Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Macrocycles in new drug discovery Reporter: Larry H Bernstein, MD, FCAP Jamie Mallinson, Ian Collins Future Medicinal Chemistry, Jul 2012, Vol. 4, No. 11, Pages 1409-1438.
Natural product macrocycles and their synthetic derivatives
Compilation of References by Leaders in Pharmaceutical Business Intelligence in the Journal http://pharmaceuticalintelligence.com about
Proteomics, Metabolomics, Signaling Pathways, and Cell Regulation
Curator: Larry H Bernstein, MD, FCAP
Proteomics
The Human Proteome Map Completed
Reporter and Curator: Larry H. Bernstein, MD, FCAP
33. Cardiac Contractility & Myocardial Performance: Therapeutic Implications of Ryanopathy (Calcium Release- related Contractile Dysfunction) and Catecholamine Responses
Author, and Content Consultant to e-SERIES A: Cardiovascular Diseases: Justin Pearlman, MD, PhD, FACC
Author and Curator: Larry H Bernstein, MD, FCAP
and Article Curator: Aviva Lev-Ari, PhD, RN
8. microRNA called miRNA-142 involved in the process by which the immature cells in the bone marrow give rise to all the types of blood cells, including immune cells and the oxygen-bearing red blood cells
36. Harnessing Personalized Medicine for Cancer Management, Prospects of Prevention and Cure: Opinions of Cancer Scientific Leaders @http://pharmaceuticalintelligence.com
37. GSK for Personalized Medicine using Cancer Drugs needs Alacris systems biology model to determine the in silico
effect of the inhibitor in its “virtual clinical trial”
11. Disruption of Calcium Homeostasis: Cardiomyocytes and Vascular Smooth Muscle Cells: The Cardiac and
Cardiovascular Calcium Signaling Mechanism
Author and Curator: Larry H Bernstein, MD, FCAP, Author, and Content Consultant to e-SERIES A:
Cardiovascular Diseases: Justin Pearlman, MD, PhD, FACC and Curator: Aviva Lev-Ari, PhD, RN
12. The Centrality of Ca(2+) Signaling and Cytoskeleton Involving Calmodulin Kinases and
Ryanodine Receptors in Cardiac Failure, Arterial Smooth Muscle, Post-ischemic Arrhythmia,
Similarities and Differences, and Pharmaceutical Targets
Author and Curator: Larry H Bernstein, MD, FCAP, Author, and Content Consultant to
e-SERIES A: Cardiovascular Diseases: Justin Pearlman, MD, PhD, FACC and
Curator: Aviva Lev-Ari, PhD, RN
With help from the zebrafish, a team of Australian researchers has uncovered how hematopoietic stem cells (HSC) renew themselves.
HSCs refers to stem cells present in the blood and bone marrow that are used for the replenishment of the body’s supply of blood and immune cells –
in transplants for leukemia and myeloma.
Stem cells have the potential to transform into vital cells
including muscle, bone, and blood vessels.
Understanding how HSCs form and renew themselves has potential application in the treatment of
spinal cord injuries
degenerative disorders
diabetes.
Professor Peter Currie, of the Australian Regen Med Institute at Victoria’s Monash University, led a research team to discover a crucial part of HSC’s development. Using a high-resolution microscopy, Prof. Curie’s team
caught zebrafish embyonic SCs on film as they formed.
the researchers were studying muscle mutations in the aquatic animal.
“Zebrafish make ESCs in exactly the same way as humans do, but their embryos and larvae develop free living, but the larvae are both free swimming and transparent, so one could see every cell in the body forming, including ESCs,” explained Prof. Currie.
The researchers noticed in films that a
‘buddy cell’ came along to help the ESCs form.
Called endotome cells,
they aided pre-ESCs to turn into ESCs.
Prof. Currie said that endotome cells act as helper cells for pre-ESCs ,
helping them progress to become fully fledged stem cells.
The team not only
identified some of the cells and signals
required for ESC formation, but also
pinpointed the genes required
for endotome formation in the first place.
The next step for the researchers is to
locate the signals present in the endotome cells
that trigger ESC formation in the embryo.
This may provide clues for developing
specific blood cells on demand for blood-related disorders.
Professor Currie also pointed out the discovery’s potential for
correcting genetic defects in the cell and
transplanting them back in the body to treat disorders.
The team’s work was published in the international journal Nature.
Jell-O Like Biomaterial Could Hold Key to Cancer Cell Destruction
by Estel Grace Masangkay
Scientists from Penn State University reported that a biomaterial made of tiny molecules was able to attract and destroy cancer cells.
Professor Yong Wang and bioengineering faculty at Penn State, built the tissue-like biomaterial to accomplish what chemotherapy could not –
kill every cancer cell without leaving
the possibility of a recurrence.
Prof. Wang and team built polymers
from tiny molecules called monomers. They
then wove the polymers into 3D networks
called hydrogels. Hydrogel is soft and flexible, like Jell-O, and it contains a lot of water, and
can be safely put into the body, unlike
other implants that the body often tries
to get rid of through the immune response.
“We want to make sure the materials we are using are compatible in the body.”
The researchers
attached aptamers to the hydrogels,
which release bio-chemical signal-only molecules
that draw in cancer cells.
Once attracted, the cancer cells are entrapped in the Jell-O-like substance.
What happens next is
an oligonucleotide binds to the protein-binding site of the aptamer
and triggers the release of anticancer drugs at the proper time.
“Once we trap the cancer cells, we can deliver anticancer drugs
to that specific location to kill them.
This technique would help avoid the need for systemic medications that kill not only cancer cells, but normal cells as well. Systemic chemotherapy drugs
make patients devastatingly sick and possibly
leave behind cancer cells to wreak havoc another day
If our new technique has any side effects at all, it would be only local side effects and not whole-body systemic side effects,” explained Prof. Wang.
The initial results of the research were published by Prof. Wang in the Journal of the American Chemical Society in 2012. Prof. Wang also shared the latest results of his work at the Society for Biomaterials Meeting & Exposition in April this year.
John Carroll reports on a disappointing ruling by the FDA on AstraZeneca’s PARP1 inhibitor olaparib for maintenance therapy in women with cisplatin refractory ovarian cancer with BRCA mutation. Early clinical investigations had pointed to efficacy of PARP inhibitors in ovarian tumors carrying the BRCA mutation. The scientific rationale for using PARP1 inhibitors in BRCA1/2 deficiency was quite clear:
DNA damage can result in
1. double strand breaks (DSB)
DSB can be repaired by efficient homologous recombination (HR) or less efficient non-homologous end joining (NHEJ)
b. BRCA1 involved in RAD51 dependent HR at DSB sites
In BRCA1 deficiency DSB repaired by less efficient NHEJ
2. single strand breaks, damage (SSB)
PARP1 is activated by DNA damage and poly-ADP ribosylates histones and other proteins marking DNA for SSB repair
SSB repair usually base excision (BER) or sometimes nucleotide excision repair (NER)
B. if PARP inhibited then SSB gets converted to DSB
C. in BRCA1/2 deficient background repair is forced to less efficient NHEJ thereby perpetuating some DNA damage pon exposure to DNA damaging agent
(from Christina M Annunziata and Susan E Bates. PARP inhibitors in BRCA1/BRCA2 germline mutation carriers with ovarian and breast cancer. F1000 Biol Reports, 2010; 2:10.) Creative Commons
Dana Farber’s Dr. Ralph Scully, Ph.D., in Exploiting DNA Repair Targets in Breast Cancer (http://www.dfhcc.harvard.edu/news/news/article/5402/), explains his research investigating why multiple DNA repair pathways may have to be targeted with PARP therapy concurrent with BRCA1 deficiency.
However FDA investigators voiced their skepticism of AstraZeneca’s clinical results, namely
Small number of patients enrolled
BRCA1/2 cohort were identified retrospectively
results skewed by false benefit from “underperforming” control arm
possible inadvertent selection bias
hazard ratio suggesting improvement in progression free survival but higher risk/benefit
The FDA investigators released their report two days before an expert panel would be releasing their own report (reported in the link below from FierceBiotech)
in which the expert panel reiterated the findings of the FDA investigators. The expert panel’s job was to find if there was any clinical benefit for continuing consideration of olaparib, basically stating
“This trial has problems,” noted FDA cancer chief Richard Pazdur during the panel discussion. If investigators had “pristine evidence of a 7-month advantage in PFS, we wouldn’t be here.”
The expert panel was concerned for the above reasons as well as the reported handful of lethal cases of myelodysplastic syndrome and acute myeloid leukemia in the study, although the panel noted these patients had advanced disease before entering the trial, raising the possibility that prior drugs may have triggered their deaths.
This was certainly a disappointment as ….
it was at last year’s ASCO (2013) that investigators at Perelman School of Medicine at the University of Pennsylvania and Sheba Medical Center in Tel Hashomer, Israel presented data showing that in 193 cisplatin-refractory ovarian cancer patients carrying a BRCA1/2 mutation, 31% had a partial or complete tumor regression. In addition the study also showed good response in pancreatic and prostate cancer with tolerable side effects.
As John Carrol from FierceBiotech notes, the decision may spark renewed interest by Pfizer of a bid for AstraZeneca as the potential FDA rejection would certainly dampen AstraZeneca’s future growth and profit plans. Last month AstraZeneca’s CEO made the case to shareholders to reject the Pfizer offer by pointing to AstraZeneca’s potential beefed-up pipeline. AstraZeneca had projected olaparib as a potential $2 billion-a-year seller, although some industry analysts see sales at less than half that amount.
A company spokeswoman said the monotherapy use of olaparib for ovarian cancer assessed by the U.S. expert panel this week was only one element of a broad development program.
Please see a table of current oncology clinical trials with PARP1 inhibitors
at end of this post
However, on the same day, FierceBiotechreports some great news (at least in Europe) on the ovarian cancer front:
EU Committee for Medicinal Products for Human Use (CHMP) handed down a positive ruling on Avastin, recommending that the European Commission approve the drug for use in women with ovarian cancer that’s resistant to platinum-based chemotherapy. It’s the first biologic to receive a positive opinion from the CHMP for this hard-to-treat form of the disease.
EU had been getting pressure from British doctors to approve Avastin based on clinical trial results although it may be important to note that the EU zone seems to have an ability to recruit more numbers for clinical trials than in US. For instance an EU women’s breast cancer prevention trial had heavy recruitment in what would be considered a short time frame compared to recruitment times for the US.
Below is a table on PARP1 inhibitors in current clinical trials (obtained from NewMedicine’s Oncology KnowledgeBase™). nm|OK is a relational knowledgeBASE covering all major aspects of product development in oncolology. The database comprises 6 modules each dedicated in a specific sector within the oncology field.
PARP1 Inhibitors Currently in Clinical Trials for Ovarian Cancer
Phase I (begin 5/11, ongoing 2/14) Europe (Netherlands)– solid tumors with BRCA1 or BRCA2 mutations, locally advanced or metastatic • ovarian cancer, advanced or metastatic • fallopian tube cancer, advanced or metastatic • peritoneal cancer, advanced or metastatic
AstraZeneca Affiliate(s):
· Myriad GeneticsCurrent as of: June 26, 2014Generic Name: Olaparib Brand Name: Lynparza Other Designation: AZD2281, KU59436, KU-0059436, NSC 747856
Phase I (begin 7/05, closed 9/08) Europe (Netherlands, UK, Poland); phase II (begin 6/07, closed 2/08, completed 5/09) USA, Australia, Europe (Germany, Spain, Sweden, UK), phase II (begin 7/08, closed 2/09) USA, Australia, Europe (Belgium, Germany, Poland, Spain, UK), Israel, phase II (begin 8/08, closed 12/09, completed 3/13) USA, Australia, Canada, Europe (Belgium, France, Germany, Poland, Romania, Spain, Ukraine, UK), Israel, Russia; phase II (begin 2/10, closed 7/10) USA, Australia, Canada, Europe (Belgium, Czech Republic, Germany, Italy, Netherlands, Spain, UK), Japan, Panama, Peru (combination); MAA (accepted 9/13) EU, NDA (filed 2/14) USA– ovarian cancer, advanced or metastatic, BRCA positive • ovarian cancer, recurrent, platinum sensitive • ovarian cancer, advanced, refractory, BRCA1 or BRCA2-associatedPhase I (begin 5/08, ongoing 5/12) USA; phase II (begin 7/08, closed 10/09) Canada– breast cancer, locally advanced, BRCA1/BRCA2-associated or hereditary metastatic or inoperable • ovarian cancer, locally advanced, BRCA1/BRCA2-associated or hereditary metastatic or inoperable • breast cancer, triple-negative, BRCA-positive • ovarian cancer, high-grade serous and/or undifferentiated, BRCA-positive
Phase I (begin 10/10, ongoing 1/13) USA (combination)– ovarian cancer, inoperable or metastatic, refractory • breast cancer, inoperable or metastatic, refractory
Phase III (begin 8/13) USA, Australia, Brazil, Canada, Europe (France, Italy, Netherlands, Poland, Russia, Spain, UK), Israel, South Korea, phase III (begin 9/13) USA, Australia, Brazil, Canada, Europe (France, Germany, Italy, Netherlands, Poland, Russia, Spain, UK), Israel– ovarian cancer, serous, high grade, BRCA mutated, platinum-sensitive, relapsed, third line, maintenance • ovarian cancer, serous or endometrioid, high grade, BRCA mutated, platinum responsive (PR or CR), maintenance, first line • primary peritoneal cancer, high grade, BRCA mutated, platinum responsive (PR or CR), maintenance • fallopian tube cancer, high grade, BRCA mutated, platinum responsive (PR or
Clovis Oncology Affiliate(s):
· University of Newcastle Upon Tyne
· Cancer Research Campaign Technology
· PfizerCurrent as of: June 21, 2014Generic Name: Rucaparib Brand Name: Rucapanc Other Designation: AG140699, AG014699, AG-14,699, AG-14669, AG14699, AG140361, AG-14361, AG-014699, CO-338, PF-01367338
Phase I (begin 03, completed 05) Europe (UK) (combination), phase I (begin 2/10, closed 11/13) Europe (France, UK) (combination)– solid tumors, advanced
Phase II (begin 12/07, closed 10/13) Europe (UK)– breast cancer, advanced or metastatic, in patients carrying BRCA1 or BRCA2 mutations • ovarian cancer, advanced or metastatic, in patients carrying BRCA1 or BRCA2 mutations
Phase I/II (begin 11/11, ongoing 6/14) USA, Europe (UK)– solid tumors, metastatic, with mutated BRCA • breast cancer, metastatic, HEr2 negative, with mutated BRCA
Phase I (begin 5/11, closed 11/12, terminated 10/13) USA, phase I (begin 6/09, closed 7/12, completed 1/12) Europe (France and UK) (combination)– solid tumors, advanced, third line Phase I (begin 5/11, completed 1/13) Europe (France) (combination)– solid tumors, advanced • mantle cell lymphoma (MCL), advanced
Summary of Combination Ovarian Cancer Trials with Avastin (current and closed)
Indication in Development
ovarian cancer, advanced, recurrent, persistent • ovarian cancer, progressive, platinum resistant, second line • fallopian tube cancer, progressive, platinum resistant, second line • primary peritoneal cancer, progressive, platinum resistant, second line
Latest Status
Phase II (begin 4/02, closed 8/04) USA, phase II (begin 11/04, closed 10/05) USA; phase III (begin 10/09) Europe (Belgium, Bosnia and Herzegovina, Denmark, Finland, France, Germany, Greece, Italy, Netherlands, Norway, Portugal, Spain, Sweden), Turkey
Clinical History
Refer to the Combination Trial Module for trials of Avastin in combination with various chemotherapeutic regimens.According to results from the AURELIA clinical trial (protocol ID: MO22224; 2009-011400-33; NCT00976911), the median PFS in women with progressive platinum resistant ovarian, fallopian tube or primary peritoneal cancer treated with Avastin in combination with chemotherapy, was 6.7 months compared to 3.4 months in those treated with chemotherapy alone for an HR of 0.48 (range =0.38–0.60).. In addition, the objective response rate was 30.9% in women treated with Avastin compared to 12.6% in those on chemotherapy (p=0.001). Certain AE (Grade 2 to 5) that occurred more often in the Avastin arm compared to the chemotherapy alone arm were high blood pressure (20% versus 7%) and an excess of protein in the urine (11% versus 1%). Gastrointestinal perforations and fistulas occurred in 2% of women in the Avastin arm compared to no events in the chemotherapy arm (Pujade-Lauraine E, etal, ASCO12, Abs. LBA5002).A multicenter (n=124), randomized, open label, 2-arm, phase III clinical trial (protocol ID: MO22224; 2009-011400-33; NCT00976911; http://clinicaltrials.gov/ct2/results?term=NCT00976911 ), dubbed AURELIA, was initiated in October 2009, in Europe (Belgium, Bosnia and Herzegovina, Denmark, Finland, France, Germany, Greece, Italy, Netherlands, Norway, Portugal, Spain, and Sweden), and Turkey, to evaluate the efficacy and safety of Avastin added to chemotherapy versus chemotherapy alone in patients with epithelial ovarian, fallopian tube or primary peritoneal cancer with disease progression within 6 months of platinum therapy in the first line setting. The trials primary outcome measure is PFS. Secondary outcome measures include objective response rate, biological PFS interval, OS, QoL, and safety and tolerability. According to the protocol, all patients are treated with standard chemotherapy with IV paclitaxel (80 mg/m²) on days 1, 8, 15 and 22 of each 4-week cycle; or IV topotecan at a dose of 4 mg/m² on days 1, 8 and 15 of each 4-week cycle, or 1.25 mg/kg on days 1-5 of each 3-week cycle; or IV liposomal doxorubicin (40 mg/m²) every 4 weeks. Patients (n=179) randomized to arm 2 of the trial are treated with IV Avastin at a dose of 10 mg/kg twice weekly or 15 mg/kg thrice weekly concomitantly with the chemotherapy choice. Treatment continues until disease progression. Subsequently, patients are treated with the standard of care. Patients in arm 1 (n=182), on chemotherapy only may opt to be treated with IV Avastin (15 mg/kg) three times weekly. The trial was set up in cooperation with the Group d’Investigateurs Nationaux pour l’Etude des Cancers Ovariens (GINECO) and was conducted by the international network of the Gynecologic Cancer Intergroup (GCIG) and the pan-European Network of Gynaecological Oncological Trial Groups (ENGOT), under PI Eric Pujade-Lauraine, MD, Hopitaux Universitaires, Paris Centre, Hôpital Hôtel-Dieu (Paris, France). The trial enrolled 361 patients and was closed as of May 2012..Results were presented from a phase II clinical trial (protocol ID: CDR0000068839; GOG-0170D; NCT00022659) of bevacizumab in patients with persistent or recurrent epithelial ovarian cancer or primary peritoneal cancer that was performed by the Gynecologic Oncology Group to determine the ORR, PFS, and toxicity for this treatment. Patients must have been administered 1-2 prior cytotoxic regimens. Treatment consisted of bevacizumab (15 mg/kg) IV every 3 weeks until disease progression or prohibitive toxicity. Between April 2002 and August 2004, 64 patients were enrolled, of which 2 were excluded for wrong primary and borderline histology and 62 were evaluable (1 previous regimen=23, 2 previous regimens=39). The median disease free interval from completion of primary cytotoxic chemotherapy to first recurrence was 6.5 months. Early results demonstrated that some patients had confirmed objective responses and PFS in some was at least 6 months. Observed Grade 3 or 4 toxicities included allergy (Grade 3=1), cardiovascular (Grade 3=4; Grade 4=1), gastrointestinal (Grade 3=3), hepatic (Grade 3=1), pain (Grade 3=2), and pulmonary (Grade 4=1). As of 11/04, 36 patients were removed from the trial, including 29 for disease progression and 1 for toxicity in 33 cases reported. Preliminary evidence exists for objective responses to bevacizumab (Burger R, et al, ASCO05, Abs. 5009).An open label, single arm, 2-stage, phase II clinical trial (protocol ID: AVF2949g, NCT00097019) of bevacizumab in patients with platinum resistant, advanced (Stage III or IV), ovarian cancer or primary peritoneal cancer for whom subsequent doxorubicin or topotecan therapy also has failed was initiated in November 2004 at multiple locations in the USA to determine the safety and efficacy for this treatment.A multicenter phase II clinical trial was initiated in April 2002 to determine the 6-month PFS of patients with persistent or recurrent ovarian epithelial or primary peritoneal cancer treated with bevacizumab (protocol ID: GOG-0170D, CDR0000068839, NCT00022659). IV bevacizumab is administered over 30-90 minutes on day 1. Treatment is repeated every 21 days in the absence of disease progression or unacceptable toxicity. Patients are followed every 3 months for 2 years, every 6 months for 3 years, and then annually thereafter. A total of 22-60 patients will be accrued within 12-30 months. Robert A. Burger, MD, of Chao Family Comprehensive Cancer Center is Trial Chair.This trial was closed in August 2004.
In a followup to this original posting A Report From the Institute of Medicine of the National Academies of Sciences, Engineering, and Medicine entitled
was generated in a ViewPoint piece in JAMA which discussed their Congressional mandated report on the State of the Science in Ovarian Cancer Research, titled
Ovarian Cancers: Evolving Paradigms in Research and Care
highlights some of the research gaps felt by the committee in the current state of ovarian cancer research including:
consideration in research protocols of the multitude of histologic and morphologic subtypes of ovarian cancer, including the feeling of the committee that high grade serous OVCA originates from the distal end of the fallopian tube (espoused by Dr. Doubeau and Dr. Christopher Crum) versus originating from the ovarian surface epithelium
a call for expanded screening and prevention research with mutimodal screening including CA125 with secondary transvaginal screen
better patient education of the risk/benefit of genetic testing including BRCA1/2 as well as in consideration for PARP inhibitor therapy
treatments should be standardized and disseminated including more research in health outcomes and decision support for personalized therapy
This Perspective article can be found here: jvp160038
Some other posts relating to OVARIAN CANCER on this site include
John Carroll reports on a disappointing ruling by the FDA on AstraZeneca’s PARP inhibitor olaparib for maintenance therapy in women with cisplatin refractory ovarian cancer with BRCA mutation. Early clinical investigations had pointed to efficacy of PARP inhibitors in ovarian tumors carrying the BRCA mutation. The scientific rationale was quite clear:
Dana Farber’s Dr. Ralph Scully, Ph.D., in Exploiting DNA Repair Targets in Breast Cancer (http://www.dfhcc.harvard.edu/news/news/article/5402/), explains his research investigating why multiple DNA repair pathways may have to be targeted with PARP therapy concurrent with BRCA1 deficiency.
However FDA investigators voiced their skepticism of AstraZeneca’s clinical results, namely
Small number of patients enrolled
BRCA1/2 cohort were identified retrospectively
results skewed by false benefit from “underperforming” control arm
possible inadvertent selection bias
hazard ratio suggesting improvement in progression free survival but higher risk/benefit
The FDA investigators released their report two days before an expert panel would be releasing their own report (reported in the link below from FierceBiotech)
in which the expert panel reiterated the findings of the FDA investigators. The expert panel’s job was to find if there was any clinical benefit for continuing consideration of olaparib, basically stating
“This trial has problems,” noted FDA cancer chief Richard Pazdur during the panel discussion. If investigators had “pristine evidence of a 7-month advantage in PFS, we wouldn’t be here.”
The expert panel was concerned for the above reasons as well as the reported handful of lethal cases of myelodysplastic syndrome and acute myeloid leukemia in the study, although the panel noted these patients had advanced disease before entering the trial, raising the possibility that prior drugs may have triggered their deaths.
As John Carrol from FierceBiotech notes, the decision may spark renewed interest by Pfizer of a bid for AstraZeneca as the potential FDA rejection would certainly dampen AstraZeneca’s future growth and profit plans. Last month AstraZeneca’s CEO made the case to shareholders to reject the Pfizer offer by pointing to AstraZeneca’s potential beefed-up pipeline.
However, on the same day, FierceBiotechreports some great news (at least in Europe) on the ovarian cancer front:
EU Committee for Medicinal Products for Human Use (CHMP) handed down a positive ruling on Avastin, recommending that the European Commission approve the drug for use in women with ovarian cancer that’s resistant to platinum-based chemotherapy. It’s the first biologic to receive a positive opinion from the CHMP for this hard-to-treat form of the disease.
EU had been getting pressure from British doctors to approve Avastin based on clinical trial results although it may be important to note that the EU zone seems to have an ability to recruit more numbers for clinical trials than in US. For instance a wonen’s breast cancer prevention trial had heavy recruitment in what would be considered a short time frame compared to the US.
Can Mobile Health Apps Improve Oral-Chemotherapy Adherence? The Benefit of Gamification.
Reporter: Stephen J. Williams, PhD
Article ID #144: Can Mobile Health Apps Improve Oral-Chemotherapy Adherence? The Benefit of Gamification. Published on 6/17/2014
WordCloud Image Produced by Adam Tubman
A report on how gamification mobile applications, like CyberDoctor’s PatientPartner, may improve patient adherence to oral chemotherapy.
(includes interviews with CyberDoctor’s CEO Akhila Satish and various oncologists)
Writer/Curator: Stephen J. Williams, Ph.D.
UPDATE 5/15/2019
Please see below for an UPDATE on this post including results from the poll conducted here on the value of a gamification strategy for oral chemotherapy patient adherence as well as a paper describing a well designed development of an application specifically to address this clinical problem.
Studies have pointed to a growing need to monitor and improve medical adherence, especially with outpatient prescription drugs across many diseases, including cancer.
The trend to develop oral chemotherapies, so patients can take their medications in the convenience of their home, has introduced produced a unique problem concerning cancer patient-medication adherence. Traditionally, chemotherapies were administered by a parental (for example intravenous) route by clinic staff, however, as noted by Jennifer M Gangloff in her article Troubling Trend: Medication Adherence:
with the trend of cancer patients taking their oral medication at home, the burden of adherence has shifted from clinicians to the patients and their families.
A few highlights from Jennifer Gangloff’s article highlight the degree and scope of the problem:
There is a wide range of adherence for oral chemo– as low as 16% up to 100% adherence rates have been seen in multiple studies
High cost in lives and money: estimates in US of 125,000 deaths and $300 billion in healthcare costs due to nonadherence to oral anticancer medications
Factors not related to the patient can contribute to nonadherence including lack of information provided by the healthcare system and socioeconomic factors
Numerous methods to improve adherence issues (hospital informative seminars, talking pill bottles, reminder phone calls etc.) have met with mixed results.
More strikingly, patient adherence rates can drastically decline over treatment, with one study showing an adherence rate drop from 87% to 50% over 4 years of adjuvant tamoxifen therapy.
Tackling The Oral Chemotherapy-Patient Adherence Problem
Documented factors leading to non-adherence to oral oncology medications include
Patient feels better so stop taking the drug
Patient feels worse so stops taking the drug
Confusing and complicated dosing regimen
Inability to afford medications
Poor provider-patient relationships
Adverse effects of medication
Cognitive impairment (“chemo fog”; mental impairment due to chemotherapy
Inadequate education/instruction of discharge
There are many examples of each reason why a patient stopped taking medication. One patient was prescribed capecitabine for her metastatic breast cancer and, upon feeling nausea, started to use antacids, which precipitated toxicities as a result of increased plasma levels of capecitabine.
This review also documented the difficulties in accurately measuring patient adherence including:
Inaccuracy of self-reporting
Lack of applicability of external measurements such as pill counts
Hawthorne effect: i.e. patient pill documentation reminds them to take next dose
The group suggests that using MTM programs, especially telephony systems involving oncology nurses and pharmacists and utilizing:
Therapy support (dosing reminders)
Education
Side effect management
may be a cost-efficient methodology to improve medical adherence.
Although nurses are important intermediary educating patients about their oral chemotherapies, it does not appear that solely relying on nurses to monitor patient adherence will be sufficient, as indicated in a survey-based Japanese study.
Survey results indicated that 90% of nurses reported asking patients on oral chemotherapy about emergency contacts, side effects, and family/friend support. Nurses also provided patients with education materials on their assigned medication.
However, less than one-third of nurses asked if their patients felt confident about managing their oral chemotherapy.
“Nurses were less likely to ask adherence-related questions of patients with refilled prescriptions than of new patients,” the researchers wrote. “Regarding unused doses of anticancer agents, 35.5% of nurses reported that they did not confirm the number of unused doses when patients had refilled prescriptions.”
From the Roswell Park Cancer Institute blog post Making Mobile Health Work
US physicians are recognizing the need for the adoption of mobile in their practice but choice of apps and mobile strategies must be carefully examined before implementation. In addition, most physicians are using mobile communications as a free-complementary service and these physicians are not being reimbursed for their time.
Some companies are providing their own oncology-related mobile app services:
San Francisco, August 13, 2013 – CollabRx, Inc. (NASDAQ: CLRX), a healthcare information technology company focused on informing clinical decision making in molecular medicine, today announced a multi-year agreement with Everyday Health’s MedPage Today. The forthcoming app, which will target oncologists and pathologists, will focus on the molecular aspects of laboratory testing and therapy development. Over time, the expectation is that this app will serve as a comprehensive point of care resource for physicians and patients to obtain highly credible, expert-vetted and dynamically updated information to guide cancer treatment planning.
The McKesson Foundation’s Mobilizing for Health initiative
has awarded a grant to Partners HealthCare’s Center for Connected Health to develop a mobile health program that uses a smartphone application to help patients with cancer adhere to oral chemotherapy treatments and monitor their symptoms, FierceMobileHealthcare reports.
CancerNet announces mobile application (from cancer.net)
The report suggests that there are too many apps either offering information, suggesting behavior/lifestyle changes, or measuring compliance data but little evidence to suggest any of these are working the way they intended. The article suggests the plethora of apps may just be adding to the confusion.
MyCyberDoctor™, a True Gamification App, Shows Great Results in Improving Diabetics Medical Adherence and Health Outcome
Most of the mobile health apps discussed above, would be classified as tracking apps, because the applications simply record a patient’s actions, whether filling a prescription, interacting with a doctor, nurse, pharmacist, or going to a website to gain information. However, as discussed before, there is no hard evidence this is really impacting health outcomes.
Another type of application, termed gamification apps, rely on role-playing by the patient to affect patient learning and ultimately behavior.
An interested twist on this method was designed by Akhila Satish, CEO and developer of CyberDoctor and a complementary application PatientPartner.
As reported here, the PatientPartner application was used in the first IRB-approved mhealth clinical-trial to see if the gamification app could improve medical adherence and outcomes in diabetic patients. PatientPartner is a story-driven game in changing health behavior and biomarkers (blood glucose levels in this trial). In the clinical trial, 100 non-adherent patients with diabetes played the PatientPartner game for 15 minutes. Results were amazing, as the trial demonstrated an increase in patient adherence, with only 15 minutes of game playing.
Results from the study
Patients with diabetes who used PatientPartner showed significant improvement in three key areas – medication, diet, and exercise:
Medication adherence increased by 37%, from 58% to 95% – equivalent to three additional days of medication adherence per week.
Diet adherence increased by 24% – equivalent to two days of additional adherence a week.
Exercise adherence increased by 14% – equivalent to one additional day of adherence per week.
HbA1c (a blood sugar measure) decreased from 10.7% to 9.7%.
As mentioned in the article:
The unique, universal, non-disease specific approach allows PatientPartner to be effective in improving adherence in all patient populations.
PatientPartner is available in the iTunes store and works on the iPhone and iPod Touch. For information on PatientPartner, visit www.mypatientpartner.com.
Ms. Satish, who was named one of the top female CEO’s at the Health Conference, gratuitously offered to answer a few questions for Leaders in Pharmaceutical Business Intelligence (LPBI) on the feasibility of using such a game (role-playing) application to improve medical adherence in the oncology field.
LPBI: The results you had obtained with patient-compliance in the area of diabetes are compelling and the clinical trial well-designed. In the oncology field, due to the increase in use of oral chemotherapeutics, patient-compliance has become a huge issue. Other than diabetes, are there plans for MyCyberDoctor and PatientPartner to be used in other therapeutic areas to assist with patient-compliance and patient-physician relations?
Ms. Satish: Absolutely! We tested the application in diabetes because we wanted to measure adherence from an objective blood marker (hbA1c). However, the method behind PatientPartner- teaching patients how to make healthy choices- is universal and applicable across therapeutic areas.
LPBI: Recently, there have been a plethora of apps developed which claim to impact patient-compliance and provide information. Some of these apps have been niche (for example only providing prescription information but tied to pharmacy records and company databases). Your app seems to be the only one with robust clinical data behind it and approaches from a different angle, namely adjusting behavior using a gamefying experience and teaching the patient the importance of compliance. How do you feel this approach geared more toward patient education sets PatientPartner apart from other compliance-based apps?
Ms. Satish: PatientPartner really focuses on the how of patient decision making, rather than the specifics of each decision that is made. It’s a unique approach, and part of the reason PatientPartner works so effectively with such a short initial intervention! We are able to achieve more with less “app” time as a result of this method.
LPBI: There have been multiple studies attempting to correlate patient adherence, decision-making, and health outcome to socioeconomic status. In some circumstances there is a socioeconomic correlation while other cases such as patient-decision to undergo genetic testing or compliance to breast cancer treatment in rural areas, level of patient education may play a bigger role. Do you have data from your diabetes trial which would suggest any differences in patient adherence, outcome to any socioeconomic status? Do you feel use of PatientPartner would break any socioeconomic barriers to full patient adherence?
Ms. Satish: Within our trial, we had several different clinical sites. This helped us test the product out in a broad, socioeconomically diverse population. It is our hope that with a tool as easy to scale and use as PatientPartner we have the opportunity to see the product used widely, even in populations that are traditionally harder to reach.
LPBI: There has been a big push for the development of individual, personalized physician networks which use the internet as the primary point of contact between a primary physician and the patient. Individuals may sign up to these networks bypassing the traditional insurance-based networks. How would your application assist in these types of personalized networks?
Ms. Satish: PatientPartner can easily be plugged into any existing framework of communication between patient and provider. We facilitate patient awareness, engagement and accountability- all of which are important regardless of the network structure.
LBPI: Thank you Akhila!
A debate has begun about regulating mobile health applications, and although will be another post, I would just like to summarize a nice article in May, 2014 Oncology Times by Sarah Digiulo “Mobile Health Apps: Should They be Regulated?
In general, in the US there are HIPAA regulations about the dissemination of health related information between a patient and physician. Most of the concerns are related to personal health information made public in an open-access platform such as Twitter or Facebook.
In addition, according to Dr. Don Dizon M.D., Director of the Oncology Sexual Health Clinic at Massachusetts General Hospital, it may be more difficult to design applications directed against a vast, complex disease like cancer with its multiple subtypes than for diabetes.
Mobile Health Applications on Rise in Developing World: Worldwide Opportunity
According to International Telecommunication Union (ITU) statistics, world-wide mobile phone use has expanded tremendously in the past 5 years, reaching almost 6 billion subscriptions. By the end of this year it is estimated that over 95% of the world’s population will have access to mobile phones/devices, including smartphones.
This presents a tremendous and cost-effective opportunity in developing countries, and especially rural areas, for physicians to reach patients using mHealth platforms.
Drs. Clara Aranda-Jan Neo Mohutsiwa and Svetla Loukanova had conducted a systematic review of the literature on mHealth projects conducted in Africa[1] to assess the reliability of mobile phone and applications to assist in patient-physician relationships and health outcomes. The authors reviewed forty four studies on mHealth projects in Africa, determining their:
strengths
weaknesses
opportunities
threats
to patient outcomes using these mHealth projects. In general, the authors found that mHealth projects were beneficial for health-related outcomes and their success related to
accessibility
acceptance and low-cost
adaptation to local culture
government involvement
while threats to such projects could include
lack of funding
unreliable infrastructure
unclear healthcare system responsibilities
Dr.Sreedhar Tirunagari, an oncologist in India, agrees that mHealth, especially gamification applications could greatly foster better patient education and adherencealthough he notes that mHealth applications are not really used in India and may not be of much use for those oncology patients living in rural areas, as cell phone use is not as prevalent as in the bigger inner cities such as Delhi and Calcutta.
1) do you see a use for such apps which either track drug compliance or use gamification systems to teach patients the importance of continuing their full schedule of drug therapy
2) do you feel patient- drug compliance issues in the oncology practice is due to lack of information available to the patient or issues related to drug side effects?
“I think that Apps could help in this setting, we are in
Informatics era but..
The main question is that chronic patients are special ones.
Cancer patients have to deal with prognosis, even in therapies
with curative intent such as aromatase inhibitors are potent
Drugs that can cure; only in the future the patients know.
But meanwhile he or she has to deal with side-effects every day. A PC can help but suffer this symptoms…it. Is a real problem believe me!”
“The main app is his/her doctor”
I would like to invite all oncologists to answer the poll question ABOVE about the use of such gamification apps, like PatientPartner, for improving medical adherence to oral chemotherapy.
UPDATE 5/15/2019
The results of the above poll, although limited, revealed some interesting insights. Although only five oncologists answered the poll whether they felt gamification applications could help with oral chemotherapy patient adherence, all agreed it would be worthwhile to develop apps based on gamification to assist in the outpatient setting. In addition, one oncologist felt that the success of mobile patient adherence application would depend on the type of cancer. None of the oncologist who answered the survey thought that gamification apps would have no positive effect on patient adherence to their chemotherapy. With this in light, a recent paper by Joel Fishbein of University of Colorado and Joseph Greer from Massachusetts General Hospital, describes the development of a mobile application, in clinical trial, to promote patient adherence to their oral chemotherapy.
Mobile Applications to Promote Adherence to Oral Chemotherapy and Symptom Management: A Protocol for Design and Development
Oral chemotherapy is increasingly used in place of traditional intravenous chemotherapy to treat patients with cancer. While oral chemotherapy includes benefits such as ease of administration, convenience, and minimization of invasive infusions, patients receive less oversight, support, and symptom monitoring from clinicians. Additionally, adherence is a well-documented challenge for patients with cancer prescribed oral chemotherapy regimens. With the ever-growing presence of smartphones and potential for efficacious behavioral intervention technology, we created a mobile health intervention for medication and symptom management.
OBJECTIVE:
The objective of this study was to develop and evaluate the usability and acceptability of a smartphone app to support adherence to oral chemotherapy and symptom management in patients with cancer.
METHODS:
We used a 5-step development model to create a comprehensive mobile app with theoretically informed content. The research and technical development team worked together to develop and iteratively test the app. In addition to the research team, key stakeholders including patients and family members, oncology clinicians, health care representatives, and practice administrators contributed to the content refinement of the intervention. Patient and family members also participated in alpha and beta testing of the final prototype to assess usability and acceptability before we began the randomized controlled trial.
RESULTS:
We incorporated app components based on the stakeholder feedback we received in focus groups and alpha and beta testing. App components included medication reminders, self-reporting of medication adherence and symptoms, an education library including nutritional information, Fitbit integration, social networking resources, and individually tailored symptom management feedback. We are conducting a randomized controlled trial to determine the effectiveness of the app in improving adherence to oral chemotherapy, quality of life, and burden of symptoms and side effects. At every stage in this trial, we are engaging stakeholders to solicit feedback on our progress and next steps.
CONCLUSIONS:
To our knowledge, we are the first to describe the development of an app designed for people taking oral chemotherapy. The app addresses many concerns with oral chemotherapy, such as medication adherence and symptom management. Soliciting feedback from stakeholders with broad perspectives and expertise ensured that the app was acceptable and potentially beneficial for patients, caregivers, and clinicians. In our development process, we instantiated 7 of the 8 best practices proposed in a recent review of mobile health app development. Our process demonstrated the importance of effective communication between research groups and technical teams, as well as meticulous planning of technical specifications before development begins. Future efforts should consider incorporating other proven strategies in software, such as gamification, to bolster the impact of mobile health apps. Forthcoming results from our randomized controlled trial will provide key data on the effectiveness of this app in improving medication adherence and symptom management.
In this paper, Fishbein et al. describe the methodology of the developoment of a mobile application to promote oral chemotherapy adherence. This mobile app intervention was named CORA or ChemOtheRapy Assistant.
Of the approximately 325,000 health related apps on the market (as of 2017), the US Food and Drug Administration (FDA) have only reviewed approximately 20 per year and as of 2016 cleared only about 36 health related apps.
According to industry estimates, 500 million smartphone users worldwide will be using a health care application by 2015, and by 2018, 50 percent of the more than 3.4 billion smartphone and tablet users will have downloaded mobile health applications. However, there is not much scientific literature providing a framework for design and creation of quality health related mobile applications.
Methods
The investigators separated the app development into two phases: Phase 1 consisted of the mobile application development process and initial results of alpha and beta testing to determine acceptability among the major stakeholders including patients, caregivers, oncologists, nurses, pharmacists, pharmacologists, health payers, and patient advocates. Phase 1 methodology and results were the main focus of this paper. Phase 2 consists of an ongoing clinical trial to determine efficacy and reliability of the application in a larger number of patients at different treatment sites and among differing tumor types.
The 5 step development process in phase 1 consisted of identifying features, content, and functionality of a mobile app in an iterative process, including expert collaboration and theoretical framework to guide initial development.
There were two distinct teams: a research team and a technical team. The multidisciplinary research team consisted of the principal investigator, co-investigators (experts in oncology, psychology and psychiatry), a project director, and 3 research assistants.
The technical team consisted of programmers and project managers at Partners HealthCare Connected Health. Stakeholders served as expert consultants including oncologists, health care representatives, practice administrators, patients, and family members (care givers). All were given questionaires (HIPAA compliant) and all involved in alpha and beta testing of the product.
There were 5 steps in the development process
Implementing a theoretical framework: Patients and their family caregivers now bear the primary responsibility for their medical adherence especially to oral chemotherapy which is now more frequently administered in the home setting not in the clinical setting. Four factors were identified as the most important barriers to oral chemotherapy adherence: complexity of medication regimes, symptom burden, poor self-management of side effects, and low clinical support. These four factors were integral in the design of the mobile app and made up a conceptual framework in its design.
Conducting Initial Focus Group Interviews with key stakeholders: Stakeholders were taken from within and outside the local community. In all 32 stakeholders served as study collaborators including 8 patient/families, 8 oncologists/clinicians, 8 cancer practice administrators, and 8 representatives of the health system, community, and overall society. The goal of these focus groups were to obtain feedback on the proposed study and design included perceived importance of monitoring of adherence to oral chemotherapy, barriers to communication between patients and oncology teams regarding side effects and medication adherence, potential role of mobile apps to address barriers of quality of cancer care, potential feasibility, acceptability, and usage and feedback on the overall study design.
Creation of Wireframes (like storyboards or page designs) and Collecting Initial Feedback: The research and design team, in conjunction with stakeholder input, created content wireframes, or screen blueprints) to provide a visual guide as to what the app would look like. These wireframes also served as basis for what the patient interviews would look like on the application. A total of 10 MGH (Massachusetts General Hospital) patients (6 female, 4 male) and most with higher education (BS or higher) participated in the interviews and design of wireframes. Eight MGH clinicians participated in this phase of wireframe design.
Developing, Programming, and Refining the App: CORA was designed to be supported by PHP/MySQL databases and run on LAMP hosts (Linux, Apache, MySQL, Perl/PHP/Python) and fully HIPAA compliant. Alpha testing was conducted with various stakeholders and the app refined by the development team (technical team) after feedback.
Final beta testing and App prototype for clinical trial: The research team considered the first 5 participants enrolled in the subsequent clinical trial for finalization of the app prototype.
There were 7 updated versions of the app during the initial clinical trial phase and 4 updates addressed technical issues related to smartphone operating system upgrades.
Finally, the investigators list a few limitations in their design and study of this application. First the patient population was homogenous as all were from an academic hospital setting. Second most of the patients were of Caucasian ethnic background and most were highly educated, all of which may introduce study bias. In addition, CORA was available on smartphone and tablet only, so a larger patient population who either have no access to these devices or are not technically savvy may experience issues related to this limitation.
In addition other articles on this site related to Mobile Health applications and Health Outcomes include
Aranda-Jan CB, Mohutsiwa-Dibe N, Loukanova S: Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC public health 2014, 14:188.
The following discussion will be a review of the current interest in Avemar, a nontoxic, fermentation product of wheat germ extract, garnering interest with respect to alternative and complementary medicinal use.
Extracts from an interview by Sandra Cascio with Mate Hidvegi
Mate’s Transylvania Professor Lajos David was the organizer of the Department of Pharmacy of the University of Szeged in the 1920’s. He was elected as the Dean of the Faculty of Medicine, the first and only pharmacist who reached this high position at the University since. Dr. Hidvegy’s grandfather was a devout Roman catholic, who publicly opposed Nazi persecution of Jews during the Holocaust. One of his colleagues and, perhaps his best friend, was Albert SzentGyorgyi, the Nobel laureate who discovered vitaminC. SzentGyorgyi moved to the United States after World War II, where he turned to studies of muscle biochemistry. In his later years he turned to cancer research. He theorized that a revolutionary anticancer drug could be based upon vitamin C combined with methoxysubstituted benzoquinones, the precursors of which can be found in wheat germ. After completion of the PhD, Dr. Hidvegi spent two years with the Wheat Grain Trust in Winnipeg, Canada, before returning to Hungary in 1990. He decided to followthepathwaythat SzentGyorgyi was now engaged intocompletehisgoals.He contacted anoldfriend,GaborFodor, a brilliantchemist, also a collaborator withSzentGyorgyiincancerresearch.
He wasinvited by Hermann Esterbauer, the head of the Institute of Biochemistry at the University of Graz, to work in his laboratory. Thanks to the generosity of Professor Esterbauer, he accomplished much at Graz together with his student, Dr. Rita Farkas. It was soon after Szent-Gyorgyi’s death when, with the help of Dr. Fodor, they prepared the chemicals to make the drug Szent-Gyorgyi had intended to make, with encouragement from the great quantum biochemist, Janos Ladik. They made wheat germ extracts with the highest free benzoquinone content.This required a fermentation process to liberate the benzoquinone moieties from the chemical bonds which keep them in natural forms: in glycosides. He recalls the purple colored active molecules in the fermentation liquid. Living cells with their exo and endoenzymes are used to split bonds and make new molecules. This is also true for the manufacturing process of Avemar. This extract contains new molecules which cannot be found elsewhere.
“WhenAvemar was voted by the majority of the more than 50,000 professionals for NutrAward, it became obvious that this product is of biological efficacy plus safety, and it is based on good science.” It received the financial support needed. From this, he was able to complete the experiments and get the approval for the registration. The time arrived when he really had to give a name to the product which had only had a code name. One late night it just came: Avemar, from the Latin prayer: Ave Maria.
Avemar with widely used chemotherapeutic drugs completely inhibited the development of metastases. Exploring its whole activity profile might even take a lifetime of research. So far he has supervised Avemar research done in Hungary, Israel, the United States, Austria, Italy, Spain, Slovakia, the Czech Republic, Germany,the United Kingdom, Russia, Australia, Korea, Vietnam. It has been a good experience to see the scientific interest it has generated worldwide. In 2009, Dr. Hidvegy received an invitation from the Nobel laureate, James Watson, codiscoverer of DNA’s double helix. It was a great honor. Avemar, he hopes,will be a significant cancer drug.
Mate Hidvegi was born in Budapest, Hungary, in 1955. He studied, thentaught at what is now Budapest Universityof Technology and Economics.After finishing university, he worked in the cereal industry and was codeveloper of patented feed advisory system basedon near infrared ingredientdata. In Hungary, Hidvegi was one of the pioneers in the development oftechnologies for large scale production of instantized extracts for therapeuticuse.
Carcinogenesis vol.22 no.10 pp.1649–1652, 2001
Wheat germ extract inhibits experimental colon carcino-genesis in F-344 rats
Attila Zalatnai, Karoly Lapis, Bela Szende, Erzsebet Raso, Andros Telekes, Akos Resetar, and Mate Hidvegi
It has been demonstrated for the first time that a wheat germ extract prevents colonic cancer in laboratory animals. Four-week-old inbred male F-344 rats were used in the study. Colon carcinogenesis was induced by azoxy-methane (AOM). Ten rats served as untreated controls (group 1). For the treatment of the animals in group 2, AOM was dissolved in physiologic saline and the animals were given three weekly subcutaneous injections at 15 mg/kg body weight (b/w). In two additional groups Avemar (MSC), a fermented wheat germ extract standardized to 2,6-dimethoxy-p-benzoquinone was administered as a tentative chemo-preventive agent. MSC was dissolved in water and was given by gavage at a dose of 3 g/kg b/w once a day. In group 3, animals started to receive MSC 2 weeks prior to the first injection of AOM daily and continuously thereafter until they were killed 32 weeks later. In group 4 only the basal diet and MSC were administered. At the end of the experiment all the rats were exsanguinated under a light ether anesthesia and necropsied. Percentage of animals developing colon tumors and number of tumors per animals: group 1 – 0 and 0; group 2– 83.0 and 2.3; group 3 – 44.8 (P ≤ 0.001) and 1.3 (P ≤ 0.004); group 4 – 0 and 0. All the tumors were histologically neoplastic. The numbers of the aberrant crypt foci (ACF) per area (cm2) in group 2 were 4.85 while in group 3 the ACF numbers were 2.03 only (P ≤ 0.0001).
Table I. Macroscopic findings in the large intestines of F-344 rats treated with MSC or MSC + AOM
No. of animals w/tumorw
Average
# tumors
Average
diameter
N
1
Untreated
controls (10)
0/10
0/10
2.
AOM (47)
39/47
(83.0%)
2.3 + 0.21
(range 1–8)
2.35 +
0.25
3.
MSC +
AOM (29)
13/29
(44.8%)
1.3 + 0.17
(range 1–3)
2.21 +
0.12
4.
MSC (9)
0/9
0/9
Fig. 1. Experimental schedule. Colon carcinogenesis was induced by three consecutive s.c. doses of AOM 1 week apart in F-344 rats. Oral administration of MSC was started 2 weeks before the carcinogen treatments. All the animals were killed at the end of the experiment, e.g. on the 32nd week. (not shown)
Summing up, although the chemoprevention of colon cancers (and their pre-neoplastic lesions) has well and long been established and could be achieved by totally different compounds, the mechanisms have still remained to be clarified. This is also true for MSC.
The exact mechanism by which the fermented wheat germ concentration can prevent colon cancer is still partly unknown. MSC did inhibit the AOM-induced ACF and colon neoplasm formation, the multiplicity of the tumors, apparently acting in the initiation phase. Regarding this, we can hypothesize that MSC acts as an immunomodulator.
Wheat Germ Extract Decreases Glucose Uptake and RNARibose Formation but Increases Fatty Acid Synthesis in MIAPancreatic Adenocarcinoma Cell
LG Boros, K Lapis, B Szende, R Tömösközi-Farkas, Ádám Balogh, …., and M Hidvégi
UCLA School of Medicine, Harbor-UCLA Research and Education Institute, Torrance, Ca.; First Institute of Pathology and Experimental Cancer Research, Semmelweis Medical University, Budapest, Hungary; Central Food Research Institute, Budapest, Hungary; Department of Surgery, Albert Szent-Gyorgyi Medical and Pharmaceutical Center, School of General Medicine, University of Szeged, Szeged, Hungary; Department of Biochemistry and Molecular Biology, Institut d’Investigacions Biomediques August Pi i Sunyer, University of Barcelona, Barcelona, Spain; andDepartment of Biochemistryand Food Technology, Technical University of Budapest and Biromedicina Company, Budapest, Hungary
Pancreas 2001; 23 (2), pp. 141–147
Summary: The fermented wheat germ extract with standardized composition has potent tumor inhibitory properties. The fermented wheat germ extract controls tumor propagation. The authors show that this extract induces profound metabolic changes in cultured MIA pancreatic adenocarcinoma cells when the [1,2- 13C2] glucose isotope is used as the single tracer with biologic gas chromatography–mass spectrometry.
MIA cells treated with 0.1, 1, and 10 mg/mL wheat germ extract showed a dose-dependent decrease in cell glucose consumption, consumption, uptake of isotope into ribosomal RNA (2.4%, 9.4%, and 8.0%), and release of 13CO2 . Conversely, direct glucose oxidation and ribose recycling in the pentose cycle showed a dose-dependent increase of 1.2%, 20.7%, and 93.4%. The newly synthesized fraction of cell palmitate and the 13C enrichment of acetyl units were also increased with all doses of wheat germ extract.
The fermented wheat germ extract controls tumor propagation primarily by regulating glucose carbon redistribution between cell proliferation–related and cell differentiation–related macromolecules. Wheat germ extract treatment is likely associated with the phosphor-ylation and transcriptional regulation of metabolic enzymes that are involved in glucose carbon redistribution between cell the direct oxidative degradation of glucose,proliferation–related structural and functional macromolecules(RNA, DNA) and the direct oxidative degradation and survival of pancreatic adenocarcinoma cells in culture.
Fig 1 glu consumption of MIA pancreatic carcinoma cells in response to WGE
Figure 1. Glucose consumption of MIA pancreatic adenocarcinoma cells in response to increasing doses of fermented wheat germ extract (Avemar) treatment after 72 hours of culture. Glucose consumption (measured in milligrams) was estimated by the difference in media glucose content between Avemar-treated and control cultures. MIA cell glucose consumption was significantly inhibited in the presence of either 1 mg/mL (*p < 0.05) or 10 mg/mL (**p < 0.01) Avemar (x + SD; n = 6).
Figure 3. Ribosomal RNA synthesis of MIA pancreatic adenocarcinoma cells in response to increasing doses of fermented wheat germ extract (Avemar) treatment after 72 hours of culture. Glucose carbon incorporation into ribose isolated from ribosomal RNA is expressed as molar enrichment. The dose-dependent decrease in of rRNA after Avemar treatment indicates that ribosomal RNA synthesis is the primary site significantly affected by all doses of Avemar treatment with a maximum decrease of 29% after 10 mg/mL treatment (x + SD; n = 9; *p < 0.05, **p < 0.01).
changes in metabolic activity indicate that Avemar treatment affects cell metabolism primarily by decreasing glucose uptake and nucleic acid ribose synthesis while increasing glucose oxidation through the oxidative reactions of the pentose cycle and fatty acid synthesis from glucose carbon. The effect of Avemar treatment on lactate production and TCA cycle anapleurotic flux compared with glucose oxidation is less prominent
Fermented wheat germ extract induces apoptosis and downregulation of major histocompatibility complex class I proteins in tumor T and B cell lines
R FAJKA-BOJA, M HIDVÉGI, Y SHOENFELD, G ION, D DEMYDENKO, R TÖMÖSKÖZI-FARKAS, et al.
INTL J ONCOLOGY 2002; 20: 563-570.
Lymphocyte Signal Transduction Laboratory, Institute of Genetics, and Cytokine Group, Institute of Biochemistry, Biological Research Center of the Hungarian Academy of Sciences, Szeged; Department of Biochemistry and Food Technology, Budapest University of Technology and Economics, Budapest, Hungary; Department of Medicine ‘B’, Center for Autoimmune Diseases, Sheba Medical Center, Tel-Hashomer, Israel; Central Food Research Institute; National Institute of Oncology; Biromedicina Co., Budapest, Hungary
Abstract. The fermented wheat germ extract (code name: on cyto-fluorimeter using a monoclonal antibody to the MSC, trade name: Avemar), with standardized benzoquinone non-polymorphic region of the human MHC class I. MSC content has been shown to inhibit tumor propagation and stimulated tyrosine phosphorylation of intracellular proteins metastases formation in vivo. The aim of this study was to understand the molecular and cellular mechanisms of the anti-tumor effect of MSC. Therefore, we have designed in vitro model experiments using T and B tumor lymphocytic cell lines. As a result of the MSC treatment, cell surface MHC class I proteins was downregulated by 70-85% compared to the non-stimulated control.
Prominent apoptosis of and the influx of extracellular Ca2+ resulted in elevation of the amount of the intracellular Ca2+ concentration. 20-40% was detected upon 24 h of MSC treatment of the cell lines. Apoptosis was measured with cytofluorimetry by staining the DNA with propidium iodide and detecting the ‘sub-G ’ cell population.
Tyrosine phosphorylation of intra-cellular proteins and elevation of the intracellular Ca2+ concentration were examined using immunoblotting with anti-phosphotyrosine antibody and cytofluorimetry by means of Ca2+ sensitive fluorescence dyes, Fluo-3AM and FuraRed-AM, respectively. MSC did not induce a similar degree of apoptosis in healthy peripheral blood mononuclear cells.
Inhibition of the cellular tyrosine phosphatase activity or Ca2+ influx resulted in the opposite effect – increasing or diminishing the Avemar induced apoptosis as well as the MHC class I downregulation. The level of the cell surface MHC class I molecules was analysed with indirect immunofluorescence. The benzoquinone component (2,6-dimethoxi-p-benzoquinone) in MSC induced similar apoptosis and downregulation of the MHC class I molecules in the tumor T and B cell lines to that of MSC. These results suggest that MSC acts on lymphoid tumor cells by reducing MHC class I expression and selectively promoting apoptosis of tumor cells on a tyrosine phosphorylation and Ca2+ influx dependent way. One of the components in MSC, 2,6-dimethoxi-p-benzoquinone was shown to be an important factor in MSC mediated cell response.
Abbreviations:MHC, major histocompatibility complex;NK, natural killer;DMBQ, 2,6-dimethoxi-p-benzoquinone; FCS, fetal calf serum;PBMC, peripheral bloodmononuclear cells; TCR, T cell receptor;BCR, B cell receptor; mAb, monoclonal antibody;PMSF,phenylmethyl-sulfonylfluoride;pNPP, para-nitrophenyl-phosphate; PHA,phytohemagglutinineKey words: fermented wheat germ extract, Avemar, MSC, 2+ benzoquinone, tyrosine phosphorylation, intracellular Ca , CD45, tyrosine phosphatase, MHC class I downregulation, apoptosis
Figure 4. Apoptosis of tumor T cell lines and healthy lymphocytes upon MSC treatment. Jurkat cells were treated with 1 mg/ml MSC or .3 µg/ml DMBQ and PBMC were treated with 1 mg/ml
MSC for 24 h (A) or Jurkat cells were treated for 12 h (thick line in panel B). Control cells were left unstimulated (black bars in panel A or thin line on panel B). Apoptotic cells were enumerated
with the DNA analysis of the ‘sub-G ’ population (A) or with staining the cells with FITC1 labeled Annexin V
(B). Representative experiments are shown. The difference between the % of apoptosis in the case of treated and non-treated Jurkat cells was significant (MSC, p<0.001, n=14; DMBQ, p<0.05, n=3,
using paired, two-tailed t-test). No difference was found for PBMC (n=2).
MSC treatment causes prominent apoptosis in lymphoid tumor cells but it does not induce apoptosis of healthy resting mononuclear cells. Moreover, although MSC blocks the proliferation of PBM cells stimulated with PHA, it does not induce apoptosis in PHA stimulated cells (data not shown).
Introduction – The Evolution of Cancer Therapy and Cancer Research: How We Got Here?
Author and Curator: Larry H Bernstein, MD, FCAP
The evolution of progress we have achieved in cancer research, diagnosis, and therapeutics has originated from an emergence of scientific disciplines and the focus on cancer has been recent. We can imagine this from a historical perspective with respect to two observations. The first is that the oldest concepts of medicine lie with the anatomic dissection of animals and the repeated recurrence of war, pestilence, and plague throughout the middle ages, and including the renaissance. In the awakening, architecture, arts, music, math, architecture and science that accompanied the invention of printing blossomed, a unique collaboration of individuals working in disparate disciplines occurred, and those who were privileged received an education, which led to exploration, and with it, colonialism. This also led to the need to increasingly, if not without reprisal, questioning long-held church doctrines.
It was in Vienna that Rokitansky developed the discipline of pathology, and his student Semelweis identified an association between then unknown infection and childbirth fever. The extraordinary accomplishments of John Hunter in anatomy and surgery came during the twelve years war, and his student, Edward Jenner, observed the association between cowpox and smallpox resistance. The development of a nursing profession is associated with the work of Florence Nightengale during the Crimean War (at the same time as Leo Tolstoy). These events preceded the work of Pasteur, Metchnikoff, and Koch in developing a germ theory, although Semelweis had committed suicide by infecting himself with syphilis. The first decade of the Nobel Prize was dominated by discoveries in infectious disease and public health (Ronald Ross, Walter Reed) and we know that the Civil War in America saw an epidemic of Yellow Fever, and the Armed Services Medical Museum was endowed with a large repository of osteomyelitis specimens. We also recall that the Russian physician and playwriter, Anton Checkov, wrote about the conditions in prison camps.
But the pharmacopeia was about to open with the discoveries of insulin, antibiotics, vitamins, thyroid action (Mayo brothers pioneered thyroid surgery in the thyroid iodine-deficient midwest), and pitutitary and sex hormones (isolatation, crystal structure, and synthesis years later), and Karl Landsteiner’s discovery of red cell antigenic groups (but he also pioneered in discoveries in meningitis and poliomyelitis, and conceived of the term hapten) with the introduction of transfusion therapy that would lead to transplantation medicine. The next phase would be heralded by the discovery of cancer, which was highlighted by the identification of leukemia by Rudolph Virchow, who cautioned about the limitations of microscopy. This period is highlighted by the classic work – “Microbe Hunters”.
John Hunter
Walter Reed
Robert Koch
goldberger 1916 Pellagra
Louis Pasteur
A multidisciplinary approach has led us to a unique multidisciplinary or systems view of cancer, with different fields of study offering their unique expertise, contributions, and viewpoints on the etiology of cancer. Diverse fields in immunology, biology, biochemistry, toxicology, molecular biology, virology, mathematics, social activism and policy, and engineering have made such important contributions to our understanding of cancer, that without cooperation among these diverse fields our knowledge of cancer would never had evolved as it has. In a series of posts “Heroes in Medical Research:” the work of researchers are highlighted as examples of how disparate scientific disciplines converged to produce seminal discoveries which propelled the cancer field, although, at the time, they seemed like serendipitous findings. In the post Heroes in Medical Research: Barnett Rosenberg and the Discovery of Cisplatin (Translating Basic Research to the Clinic) discusses the seminal yet serendipitous discoveries by bacteriologist Dr. Barnett Rosenberg, which eventually led to the development of cisplatin, a staple of many chemotherapeutic regimens. Molecular biologist Dr. Robert Ting, working with soon-to-be Nobel Laureate virologist Dr. James Gallo on AIDS research and the associated Karposi’s sarcoma identified one of the first retroviral oncogenes, revolutionizing previous held misconceptions of the origins of cancer (described in Heroes in Medical Research: Dr. Robert Ting, Ph.D. and Retrovirus in AIDS and Cancer). Located here will be a MONTAGE of PHOTOS of PEOPLE who made seminal discoveries and contributions in every field to cancer Each of these paths of discovery in cancer research have led to the unique strategies of cancer therapeutics and detection for the purpose of reducing the burden of human cancer. However, we must recall that this work has come at great cost, while it is indeed cause for celebration. The current failure rate of clinical trials at over 70 percent, has been a cause for disappointment, and has led to serious reconsideration of how we can proceed with greater success. The result of the evolution of the cancer field is evident in the many parts and chapters of this ebook. Volume 4 contains chapters that are in a predetermined order:
The concepts of neoplasm, malignancy, carcinogenesis, and metastatic potential, which encompass:
(a) How cancer cells bathed in an oxygen rich environment rely on anaerobic glycolysis for energy, and the secondary consequences of cachexia and sarcopenia associated with progression
invasion
ARTS protein and cancer
Glycolysis
Krebs cycle
Metabolic control analysis of respiration in human cancer tissue
akip1-expression-modulates-mitochondrial-function
(b) How advances in genetic analysis, molecular and cellular biology, metabolomics have expanded our basic knowledge of the mechanisms which are involved in cellular transformation to the cancerous state.
nucleotides
Methylation of adenine
ampk-and-ampk-related-kinase-ark-family-
ubiquitylation
(c) How molecular techniques continue to advance our understanding of how genetics, epigenetics, and alterations in cellular metabolism contribute to cancer and afford new pathways for therapeutic intervention.
genomic effects
LKB1AMPK pathway
mutation-frequencies-across-12-cancer-types
AMPK-activating drugs metformin or phenformin might provide protection against cancer
2. The distinct features of cancers of specific tissue sites of origin
3. The diagnosis of cancer by
(a) Clinical presentation
(b) Age of onset and stage of life
(c) Biomarker features
hairy cell leukemia
lymphoma leukemia
(d) Radiological and ultrasound imaging
Treatments
Prognostic differences within and between cancer types
We have introduced the emergence of a disease of great complexity that has been clouded in more questions than answers until the emergence of molecular biology in the mid 20th century, and then had to await further discoveries going into the 21st century. What gave the research impetus was the revelation of
1 the mechanism of transcription of the DNA into amino acid sequences
Proteins in Disease
2 the identification of stresses imposed on cellular function
NO beneficial effects
3 the elucidation of the substructure of the cell – cell membrane, mitochondria, ribosomes, lysosomes – and their functions, respectively
AKIP1 Expression Modulates Mitochondrial Function
4 the elucidation of oligonucleotide sequences
nucleotides
dna-replication-unwinding
dna-replication-ligation
dna-replication-primer-removal
dna-replication-leading-strand
dna-replication-lagging-strand
dna-replication-primer-synthesis
dna-replication-termination
5 the further elucidation of functionally relevant noncoding lncDNA
6 the technology to synthesis mRNA and siRNA sequences
Figure. RNAi and gene silencing
7 the repeated discovery of isoforms of critical enzymes and their pleiotropic properties
8. the regulatory pathways involved in signaling
Figure. Signaling Pathways Map
This is a brief outline of the modern progression of advances in our understanding of cancer. Let us go back to the beginning and check out a sequence of Nobel Prizes awarded and related discoveries that have a historical relationship to what we know. The first discovery was the finding by Louis Pasteur that fungi that grew in an oxygen poor environment did not put down filaments. They did not utilize oxygen and they produced used energy by fermentation. This was the basis for Otto Warburg sixty years later to make the comparison to cancer cells that grew in the presence of oxygen, but relied on anaerobic glycolysis. He used a manometer to measure respiration in tissue one cell layer thick to measure CO2 production in an adiabatic system.
Lavoisier Antoine-Laurent and Laplace Pierre-Simon (1783) Memoir on heat. Mémoirs de l’Académie des sciences. Translated by Guerlac H, Neale Watson Academic Publications, New York, 1982.
The Warburg apparatus is a manometric respirometer which was used for decades in biochemistry for measuring oxygen consumption of tissue homogenates or tissue slices.
The aqueous phase is vigorously shaken to equilibrate with a gas phase, from which oxygen is consumed while the evolved carbon dioxide is trapped, such that the pressure in the constant-volume gas phase drops proportional to oxygen consumption. The Warburg apparatus was introduced to study cell respiration, i.e. the uptake of molecular oxygen and the production of carbon dioxide by cells or tissues. Its applications were extended to the study of fermentation, when gas exchange takes place in the absence of oxygen. Thus the Warburg apparatus became established as an instrument for both aerobic and anaerobic biochemical studies [2, 3].
The respiration chamber was a detachable glass flask (F) equipped with one or more sidearms (S) for additions of chemicals and an open connection to a manometer (M; pressure gauge). A constant temperature was provided by immersion of the Warburg chamber in a constant temperature water bath. At thermal mass transfer equilibrium, an initial reading is obtained on the manometer, and the volume of gas produced or absorbed is determined at specific time intervals. A limited number of ‘titrations’ can be performed by adding the liquid contained in a side arm into the main reaction chamber. A Warburg apparatus may be equipped with more than 10 respiration chambers shaking in a common water bath. Since temperature has to be controlled very precisely in a manometric approach, the early studies on mammalian tissue respiration were generally carried out at a physiological temperature of 37 °C.
The Warburg apparatus has been replaced by polarographic instruments introduced by Britton Chance in the 1950s. Since Chance and Williams (1955) measured respiration of isolated mitochondria simultaneously with the spectrophotometric determination of cytochrome redox states, a water chacket could not be used, and measurements were carried out at room temperature (or 25 °C). Thus most later studies on isolated mitochondria were shifted to the artifical temperature of 25 °C.
Today, the importance of investigating mitochondrial performance at in vivo temperatures is recognized again in mitochondrial physiology. Incubation times of 1 hour were typical in experiments with the Warburg apparatus, but were reduced to a few or up to 20 min, following Chance and Williams, due to rapid oxygen depletion in closed, aqueous phase oxygraphs with high sample concentrations. Today, incubation times of 1 hour are typical again in high-resolution respirometry, with low sample concentrations and the option of reoxygenations.
Oesper P (1964) The history of the Warburg apparatus: Some reminiscences on its use. J Chem Educ 41: 294.
Koppenol WH, Bounds PL, Dang CV (2011) Otto Warburg’s contributions to current concepts of cancer metabolism. Nature Reviews Cancer 11: 325-337.
Gnaiger E, Kemp RB (1990) Anaerobic metabolism in aerobic mammalian cells: information from the ratio of calorimetric heat flux and respirometric oxygen flux. Biochim Biophys Acta 1016: 328-332. – “At high fructose concentrations, respiration is inhibited while glycolytic end products accumulate, a phenomenon known as the Crabtree effect. It is commonly believed that this effect is restricted to microbial and tumour cells with uniquely high glycolytic capacities (Sussman et al, 1980). However, inhibition of respiration and increase of lactate production are observed under aerobic conditions in beating rat heart cell cultures (Frelin et al, 1974) and in isolated rat lung cells (Ayuso-Parrilla et al, 1978). Thus, the same general mechanisms responsible for the integration of respiration and glycolysis in tumour cells (Sussman et al, 1980) appear to be operating to some extent in several isolated mammalian cells.”
Mitochondria are sometimes described as “cellular power plants” because they generate most of the cell’s supply of adenosine triphosphate (ATP), used as a source of chemical energy.[2] In addition to supplying cellular energy, mitochondria are involved in other tasks such as signaling, cellular differentiation, cell death, as well as the control of the cell cycle and cell growth.[3] The organelle is composed of compartments that carry out specialized functions. These compartments or regions include the outer membrane, the intermembrane space, the inner membrane, and the cristae and matrix. Mitochondrial proteins vary depending on the tissue and the species. In humans, 615 distinct types of proteins have been identified from cardiac mitochondria,[9Leonor Michaelis discovered that Janus green can be used as a supravital stain for mitochondria in 1900. Benjamin F. Kingsbury, in 1912, first related them with cell respiration, but almost exclusively based on morphological observations.[13] In 1913 particles from extracts of guinea-pig liver were linked to respiration by Otto Heinrich Warburg, which he called “grana”. Warburg and Heinrich Otto Wieland, who had also postulated a similar particle mechanism, disagreed on the chemical nature of the respiration. It was not until 1925 when David Keilin discovered cytochromes that the respiratory chain was described.[13]
The Clark Oxygen Sensor
Dr. Leland Clark – inventor of the “Clark Oxygen Sensor” (1954); the Clark type polarographic oxygen sensor remains the gold standard for measuring dissolved oxygen in biomedical, environmental and industrial applications . ‘The convenience and simplicity of the polarographic ‘oxygen electrode’ technique for measuring rapid changes in the rate of oxygen utilization by cellular and subcellular systems is now leading to its more general application in many laboratories. The types and design of oxygen electrodes vary, depending on the investigator’s ingenuity and specific requirements of the system under investigation.’Estabrook R (1967) Mitochondrial respiratory control and the polarographic measurement of ADP:O ratios. Methods Enzymol. 10: 41-47. “one approach that is underutilized in whole-cell bioenergetics, and that is accessible as long as cells can be obtained in suspension, is the oxygen electrode, which can obtain more precise information on the bioenergetic status of the in situ mitochondria than more ‘high-tech’ approaches such as fluorescent monitoring ofΔψm.” Nicholls DG, Ferguson S (2002) Bioenergetics 3. Academic Press, London.
Great Figures in Cancer
Dr. Elizabeth Blackburn,
j_michael_bishop onogene
Harold Varmus
Potts and Habener (PTH mRNA, Harvard MIT) JCI
JCI Fuller Albright and hPTH AA sequence
Dr. E. Donnall Thomas Bone Marrow Transplants
Dr Haraldzur Hausen EBV HPV
Dr. Craig Mello
Lee Hartwell – Hutchinson Cancer Res Center
Judah Folkman, MD
Gertrude B. Elien (1918-1999)
The Nobel Prize in Physiology or Medicine 1922
Archibald V. Hill, Otto Meyerhof
AV Hill –
“the production of heat in the muscle” Hill started his research work in 1909. It was due to J.N. Langley, Head of the Department of Physiology at that time that Hill took up the study on the nature of muscular contraction. Langley drew his attention to the important (later to become classic) work carried out by Fletcher and Hopkins on the problem of lactic acid in muscle, particularly in relation to the effect of oxygen upon its removal in recovery. In 1919 he took up again his study of the physiology of muscle, and came into close contact with Meyerhof of Kiel who, approaching the problem differently, arrived at results closely analogous to his study. In 1919 Hill’s friend W. Hartree, mathematician and engineer, joined in the myothermic investigations – a cooperation which had rewarding results.
Otto Meyerhof –
otto-fritz-meyerhof
lactic acid production in muscle contraction Under the influence of Otto Warburg, then at Heidelberg, Meyerhof became more and more interested in cell physiology. In 1923 he was offered a Professorship of Biochemistry in the United States, but Germany was unwilling to lose him. In 1929 he was he was placed in charge of the newly founded Kaiser Wilhelm Institute for Medical Research at Heidelberg. From 1938 to 1940 he was Director of Research at the Institut de Biologie physico-chimique at Paris, but in 1940 he moved to the United States, where the post of Research Professor of Physiological Chemistry had been created for him by the University of Pennsylvania and the Rockefeller Foundation. Meyerhof’s own account states that he was occupied chiefly with oxidation mechanisms in cells and with extending methods of gas analysis through the calorimetric measurement of heat production, and especially the respiratory processes of nitrifying bacteria. The physico-chemical analogy between oxygen respiration and alcoholic fermentation caused him to study both these processes in the same subject, namely, yeast extract. By this work he discovered a co-enzyme of respiration, which could be found in all the cells and tissues up till then investigated. At the same time he also found a co-enzyme of alcoholic fermentation. He also discovered the capacity of the SH-group to transfer oxygen; after Hopkins had isolated from cells the SH bodies concerned, Meyerhof showed that the unsaturated fatty acids in the cell are oxidized with the help of the sulfhydryl group. After studying closer the respiration of muscle, Meyerhof investigated the energy changes in muscle. Considerable progress had been achieved by the English scientists Fletcher and Hopkins by their recognition of the fact that lactic acid formation in the muscle is closely connected with the contraction process. These investigations were the first to throw light upon the highly paradoxical fact, already established by the physiologist Hermann, that the muscle can perform a considerable part of its external function in the complete absence of oxygen.
But it was indisputable that in the last resort the energy for muscle activity comes from oxidation, so the connection between activity and combustion must be an indirect one, and observed that in the absence of oxygen in the muscle, lactic acid appears, slowly in the relaxed state and rapidly in the active state, disappearing in the presence of oxygen. Obviously, then, oxygen is involved when muscle is in the relaxed state. http://upload.wikimedia.org/wikipedia/commons/e/e1/Glycolysis.jpg
The Nobel Prize committee had been receiving nominations intermittently for the previous 14 years (for Eijkman, Funk, Goldberger, Grijns, Hopkins and Suzuki but, strangely, not for McCollum in this period). Tthe Committee for the 1929 awards apparently agreed that it was high time to honor the discoverer(s) of vitamins; but who were they? There was a clear case for Grijns, but he had not been re-nominated for that particular year, and it could be said that he was just taking the relatively obvious next steps along the new trail that had been laid down by Eijkman, who was also now an old man in poor health, but there was no doubt that he had taken the first steps in the use of an animal model to investigate the nutritional basis of a clinical disorder affecting millions. Goldberger had been another important contributor, but his recent death put him out of consideration. The clearest evidence for lack of an unknown “something” in a mammalian diet was presented by Gowland Hopkins in 1912. This Cambridge biochemist was already well known for having isolated the amino acid tryptophan from a protein and demonstrated its essential nature. He fed young rats on an experimental diet, half of them receiving a daily milk supplement, and only those receiving milk grew well, Hopkins suggested that this was analogous to human diseases related to diet, as he had suggested already in a lecture published in 1906. Hopkins, the leader of the “dynamic biochemistry” school in Britain and an influential advocate for the importance of vitamins, was awarded the prize jointly with Eijkman. A door was opened. Recognition of work on the fat-soluble vitamins begun by McCollum. The next award related to vitamins was given in 1934 to George Whipple, George Minot and William Murphy “for their discoveries concerning liver therapy in cases of [then incurable pernicious] anemia,” The essential liver factor (cobalamin, or vitamin B12) was isolated in 1948, and Vitamin B12 was absent from plant foods. But William Castle in 1928 had demonstrated that the stomachs of pernicious anemia patients were abnormal in failing to secrete an “intrinsic factor”.
Szent-Györgyi was a Hungarian biochemist who had worked with Otto Warburg and had a special interest in oxidation-reduction mechanisms. He was invited to Cambridge in England in 1927 after detecting an antioxidant compound in the adrenal cortex, and there, he isolated a compound that he named hexuronic acid. Charles Glen King of the University of Pittsburgh reported success In isolating the anti-scorbutic factor in 1932, and added that his crystals had all the properties reported by Szent-Györgyi for hexuronic acid. But his work on oxidation reactions was also important. Fumarate is an intermediate in the citric acid cycle used by cells to produce energy in the form of adenosine triphosphate (ATP) from food. It is formed by the oxidation of succinate by the enzyme succinate dehydrogenase. Fumarate is then converted by the enzyme fumarase to malate. An enzyme adds water to the fumarate molecule to form malate. The malate is created by adding one hydrogen atom to a carbon atom and then adding a hydroxyl group to a carbon next to a terminal carbonyl group.
In the same year, Norman Haworth from the University of Birmingham in England received a Nobel prize from the Chemistry Committee for having advanced carbohydrate chemistry and, specifically, for having worked out the structure of Szent-Györgyi’s crystals, and then been able to synthesize the vitamin. This was a considerable achievement. The Nobel Prize in Chemistry was shared with the Swiss organic chemist Paul Karrer, cited for his work on the structures of riboflavin and vitamins A and E as well as other biologically interesting compounds. This was followed in 1938 by a further Chemistry award to the German biochemist Richard Kuhn, who had also worked on carotenoids and B-vitamins, including riboflavin and pyridoxine. But Karrer was not permitted to leave Germany at that time by the Nazi regime. However, the American work with radioisotopes at Lawrence Livermore Laboratory, UC Berkeley, was already ushering in a new era of biochemistry that would enrich our studies of metabolic pathways. The importance of work involving vitamins was acknowledged in at least ten awards in the 20th century.
1. Carpenter, K.J., Beriberi, White Rice and Vitamin B, University of California Press, Berkeley (2000).
2. Weatherall, M.W. and Kamminga, H., The making of a biochemist: the construction of Frederick Gowland Hopkins’ reputation. Medical History vol.40, pp. 415-436 (1996).
3. Becker, S.L., Will milk make them grow? An episode in the discovery of the vitamins. In Chemistry and Modern Society (J. Parascandela, editor) pp. 61-83, American Chemical Society,
Washington, D.C. (1983).
4. Carpenter, K.J., The History of Scurvy and Vitamin C, Cambridge University Press, New York (1986).
Transport and metabolism of exogenous fumarate and 3-phosphoglycerate in vascular smooth muscle.
The keto (linear) form of exogenous fructose 1,6-bisphosphate, a highly charged glycolytic intermediate, may utilize a dicarboxylate transporter to cross the cell membrane, support glycolysis, and produce ATP anaerobically. We tested the hypothesis that fumarate, a dicarboxylate, and 3-phosphoglycerate (3-PG), an intermediate structurally similar to a dicarboxylate, can support contraction in vascular smooth muscle during hypoxia. 3-PG improved maintenance of force (p < 0.05) during the 30-80 min period of hypoxia. Fumarate decreased peak isometric force development by 9.5% (p = 0.008) but modestly improved maintenance of force (p < 0.05) throughout the first 80 min of hypoxia. 13C-NMR on tissue extracts and superfusates revealed 1,2,3,4-(13)C-fumarate (5 mM) metabolism to 1,2,3,4-(13)C-malate under oxygenated and hypoxic conditions suggesting uptake and metabolism of fumarate. In conclusion, exogenous fumarate and 3-PG readily enter vascular smooth muscle cells, presumably by a dicarboxylate transporter, and support energetically important pathways.
Comparison of endogenous and exogenous sources of ATP in fueling Ca2+ uptake in smooth muscle plasma membrane vesicles.
A smooth muscle plasma membrane vesicular fraction (PMV) purified for the (Ca2+/Mg2+)-ATPase has endogenous glycolytic enzyme activity. In the presence of glycolytic substrate (fructose 1,6-diphosphate) and cofactors, PMV produced ATP and lactate and supported calcium uptake. The endogenous glycolytic cascade supports calcium uptake independent of bath [ATP]. A 10-fold dilution of PMV, with the resultant 10-fold dilution of glycolytically produced bath [ATP] did not change glycolytically fueled calcium uptake (nanomoles per milligram protein). Furthermore, the calcium uptake fueled by the endogenous glycolytic cascade persisted in the presence of a hexokinase-based ATP trap which eliminated calcium uptake fueled by exogenously added ATP. Thus, it appears that the endogenous glycolytic cascade fuels calcium uptake in PMV via a membrane-associated pool of ATP and not via an exchange of ATP with the bulk solution. To determine whether ATP produced endogenously was utilized preferentially by the calcium pump, the ATP production rates of the endogenous creatine kinase and pyruvate kinase were matched to that of glycolysis and the calcium uptake fueled by the endogenous sources was compared with that fueled by exogenous ATP added at the same rate. The rate of calcium uptake fueled by endogenous sources of ATP was approximately twice that supported by exogenously added ATP, indicating that the calcium pump preferentially utilizes ATP produced by membrane-bound enzymes.
Evidence for succinate production by reduction of fumarate during hypoxia in isolated adult rat heart cells.
Archives of Biochemistry and Biophysics (Impact Factor: 3.37). 01/1988; 259(2):527-35. http://dx.doi.org:/10.1016/0003-9861(87)90519-4 It has been demonstrated that perfusion of myocardium with glutamic acid or tricarboxylic acid cycle intermediates during hypoxia or ischemia, improves cardiac function, increases ATP levels, and stimulates succinate production. In this study isolated adult rat heart cells were used to investigate the mechanism of anaerobic succinate formation and examine beneficial effects attributed to ATP generated by this pathway. Myocytes incubated for 60 min under hypoxic conditions showed a slight loss of ATP from an initial value of 21 +/- 1 nmol/mg protein, a decline of CP from 42 to 17 nmol/mg protein and a fourfold increase in lactic acid production to 1.8 +/- 0.2 mumol/mg protein/h. These metabolite contents were not altered by the addition of malate and 2-oxoglutarate to the incubation medium nor were differences in cell viability observed; however, succinate release was substantially accelerated to 241 +/- 53 nmol/mg protein. Incubation of cells with [U-14C]malate or [2-U-14C]oxoglutarate indicates that succinate is formed directly from malate but not from 2-oxoglutarate. Moreover, anaerobic succinate formation was rotenone sensitive.
We conclude that malate reduction to succinate occurs via the reverse action of succinate dehydrogenase in a coupled reaction where NADH is oxidized (and FAD reduced) and ADP is phosphorylated.Furthermore, by transaminating with aspartate to produce oxaloacetate, 2-oxoglutarate stimulates cytosolic malic dehydrogenase activity, whereby malate is formed and NADH is oxidized.
In the form of malate, reducing equivalents and substrate are transported into the mitochondria where they are utilized for succinate synthesis.
1953 Hans Adolf Krebs –
” discovery of the citric acid cycle” and In the course of the 1920’s and 1930’s great progress was made in the study of the intermediary reactions by which sugar is anaerobically fermented to lactic acid or to ethanol and carbon dioxide. The success was mainly due to the joint efforts of the schools of Meyerhof, Embden, Parnas, von Euler, Warburg and the Coris, who built on the pioneer work of Harden and of Neuberg. This work brought to light the main intermediary steps of anaerobic fermentations.
In contrast, very little was known in the earlier 1930’s about the intermediary stages through which sugar is oxidized in living cells. When, in 1930, I left the laboratory of Otto Warburg (under whose guidance I had worked since 1926 and from whom I have learnt more than from any other single teacher), I was confronted with the question of selecting a major field of study and I felt greatly attracted by the problem of the intermediary pathway of oxidations.
These reactions represent the main energy source in higher organisms, and in view of the importance of energy production to living organisms (whose activities all depend on a continuous supply of energy) the problem seemed well worthwhile studying. http://www.johnkyrk.com/krebs.html
Interactive Krebs cycle
There are different points where metabolites enter the Krebs’ cycle. Most of the products of protein, carbohydrates and fat metabolism are reduced to the molecule acetyl coenzyme A that enters the Krebs’ cycle. Glucose, the primary fuel in the body, is first metabolized into pyruvic acid and then into acetyl coenzyme A. The breakdown of the glucose molecule forms two molecules of ATP for energy in the Embden Meyerhof pathway process of glycolysis.
On the other hand, amino acids and some chained fatty acids can be metabolized into Krebs intermediates and enter the cycle at several points. When oxygen is unavailable or the Krebs’ cycle is inhibited, the body shifts its energy production from the Krebs’ cycle to the Embden Meyerhof pathway of glycolysis, a very inefficient way of making energy.
Fritz Albert Lipmann –
“discovery of co-enzyme A and its importance for intermediary metabolism”.
In my development, the recognition of facts and the rationalization of these facts into a unified picture, have interplayed continuously. After my apprenticeship with Otto Meyerhof, a first interest on my own became the phenomenon we call the Pasteur effect, this peculiar depression of the wasteful fermentation in the respiring cell. By looking for a chemical explanation of this economy measure on the cellular level, I was prompted into a study of the mechanism of pyruvic acid oxidation, since it is at the pyruvic stage where respiration branches off from fermentation.
For this study I chose as a promising system a relatively simple looking pyruvic acid oxidation enzyme in a certain strain of Lactobacillus delbrueckii1. In 1939, experiments using minced muscle cells demonstrated that one oxygen atom can form two adenosine triphosphate molecules, and, in 1941, the concept of phosphate bonds being a form of energy in cellular metabolism was developed by Fritz Albert Lipmann.
In the following years, the mechanism behind cellular respiration was further elaborated, although its link to the mitochondria was not known.[13]The introduction of tissue fractionation by Albert Claude allowed mitochondria to be isolated from other cell fractions and biochemical analysis to be conducted on them alone. In 1946, he concluded that cytochrome oxidase and other enzymes responsible for the respiratory chain were isolated to the mitchondria. Over time, the fractionation method was tweaked, improving the quality of the mitochondria isolated, and other elements of cell respiration were determined to occur in the mitochondria.[13]
The most important event during this whole period, I now feel, was the accidental observation that in the L. delbrueckii system, pyruvic acid oxidation was completely dependent on the presence of inorganic phosphate. This observation was made in the course of attempts to replace oxygen by methylene blue. To measure the methylene blue reduction manometrically, I had to switch to a bicarbonate buffer instead of the otherwise routinely used phosphate. In bicarbonate, pyruvate oxidation was very slow, but the addition of a little phosphate caused a remarkable increase in rate. The phosphate effect was removed by washing with a phosphate free acetate buffer. Then it appeared that the reaction was really fully dependent on phosphate.
A coupling of this pyruvate oxidation with adenylic acid phosphorylation was attempted. Addition of adenylic acid to the pyruvic oxidation system brought out a net disappearance of inorganic phosphate, accounted for as adenosine triphosphate. The acetic acid subunit of acetyl CoA is combined with oxaloacetate to form a molecule of citrate. Acetyl coenzyme A acts only as a transporter of acetic acid from one enzyme to another. After Step 1, the coenzyme is released by hydrolysis to combine with another acetic acid molecule and begin the Krebs’ Cycle again.
Hugo Theorell –
“the nature and effects of oxidation enzymes”
From 1933 until 1935 Theorell held a Rockefeller Fellowship and worked with Otto Warburg at Berlin-Dahlem, and here he became interested in oxidation enzymes. At Berlin-Dahlem he produced, for the first time, the oxidation enzyme called «the yellow ferment» and he succeeded in splitting it reversibly into a coenzyme part, which was found to be flavin mononucleotide, and a colourless protein part. On return to Sweden, he was appointed Head of the newly established Biochemical Department of the Nobel Medical Institute, which was opened in 1937.
Succinate is oxidized by a molecule of FAD (Flavin Adenine Dinucleotide). The FAD removes two hydrogen atoms from the succinate and forms a double bond between the two carbon atoms to create fumarate.
They followed the path that became clear from intense collaborative work in California by George Beadle, by Avery and McCarthy, Max Delbruck, TH Morgan, Max Delbruck and by Chargaff that indicated that genetics would be important.
1965
François Jacob, André Lwoff and Jacques Monod –
” genetic control of enzyme and virus synthesis”.
In 1958 the remarkable analogy revealed by genetic analysis of lysogeny and that of the induced biosynthesis of ß-galactosidase led François Jacob, with Jacques Monod, to study the mechanisms responsible for the transfer of genetic information as well as the regulatory pathways which, in the bacterial cell, adjust the activity and synthesis of macromolecules. Following this analysis, Jacob and Monod proposed a series of new concepts, those of messenger RNA, regulator genes, operons and allosteric proteins.
Francois Jacob
Having determined the constants of growth in the presence of different carbohydrates, it occurred to me that it would be interesting to determine the same constants in paired mixtures of carbohydrates. From the first experiment on, I noticed that, whereas the growth was kinetically normal in the presence of certain mixtures (that is, it exhibited a single exponential phase), two complete growth cycles could be observed in other carbohydrate mixtures, these cycles consisting of two exponential phases separated by a-complete cessation of growth.
Lwoff, after considering this strange result for a moment, said to me, “That could have something to do with enzyme adaptation.”
“Enzyme adaptation? Never heard of it!” I said.
Lwoff’s only reply was to give me a copy of the then recent work of Marjorie Stephenson, in which a chapter summarized with great insight the still few studies concerning this phenomenon, which had been discovered by Duclaux at the end of the last century. Studied by Dienert and by Went as early as 1901 and then by Euler and Josephson, it was more or less rediscovered by Karström, who should be credited with giving it a name and attracting attention to its existence.
Lwoff’s intuition was correct. The phenomenon of “diauxy” that I had discovered was indeed closely related to enzyme adaptation, as my experiments, included in the second part of my doctoral dissertation, soon convinced me. It was actually a case of the “glucose effect” discovered by Dienert as early as 1900. That agents that uncouple oxidative phosphorylation, such as 2,4-dinitrophenol, completely inhibit adaptation to lactose or other carbohydrates suggested that “adaptation” implied an expenditure of chemical potential and therefore probably involved the true synthesis of an enzyme.
With Alice Audureau, I sought to discover the still quite obscure relations between this phenomenon and the one Massini, Lewis, and others had discovered: the appearance and selection of “spontaneous” mutants. We showed that an apparently spontaneous mutation was allowing these originally “lactose-negative” bacteria to become “lactose-positive”. However, we proved that the original strain (Lac-) and the mutant strain (Lac+) did not differ from each other by the presence of a specific enzyme system, but rather by the ability to produce this system in the presence of lactose. This mutation involved the selective control of an enzyme by a gene, and the conditions necessary for its expression seemed directly linked to the chemical activity of the system.
1974
Albert Claude, Christian de Duve and George E. Palade –
” the structural and functional organization of the cell”.
I returned to Louvain in March 1947 after a period of working with Theorell in Sweden, the Cori’s, and E Southerland in St. Louis, fortunate in the choice of my mentors, all sticklers for technical excellence and intellectual rigor, those prerequisites of good scientific work. Insulin, together with glucagon which I had helped rediscover, was still my main focus of interest, and our first investigations were accordingly directed on certain enzymatic aspects of carbohydrate metabolism in liver, which were expected to throw light on the broader problem of insulin action. But I became distracted by an accidental finding related to acid phosphatase, drawing most of my collaborators along with me. The studies led to the discovery of the lysosome, and later of the peroxisome.
In 1962, I was appointed a professor at the Rockefeller Institute in New York, now the Rockefeller University, the institution where Albert Claude had made his pioneering studies between 1929 and 1949, and where George Palade had been working since 1946. In New York, I was able to develop a second flourishing group, which follows the same general lines of research as the Belgian group, but with a program of its own.
1968
Robert W. Holley, Har Gobind Khorana and Marshall W. Nirenberg –
“interpretation of the genetic code and its function in protein synthesis”.
1969
Max Delbrück, Alfred D. Hershey and Salvador E. Luria –
” the replication mechanism and the genetic structure of viruses”.
1975 David Baltimore, Renato Dulbecco and Howard Martin Temin –
” the interaction between tumor viruses and the genetic material of the cell”.
1976
Baruch S. Blumberg and D. Carleton Gajdusek –
” new mechanisms for the origin and dissemination of infectious diseases” The editors of the Nobelprize.org website of the Nobel Foundation have asked me to provide a supplement to the autobiography that I wrote in 1976 and to recount the events that happened after the award. Much of what I will have to say relates to the scientific developments since the last essay. These are described in greater detail in a scientific memoir first published in 2002 (Blumberg, B. S., Hepatitis B. The Hunt for a Killer Virus, Princeton University Press, 2002, 2004).
1980
Baruj Benacerraf, Jean Dausset and George D. Snell
” genetically determined structures on the cell surface that regulate immunological reactions”.
1992
Edmond H. Fischer and Edwin G. Krebs
“for their discoveries concerning reversible protein phosphorylation as a biological regulatory mechanism”
1994
Alfred G. Gilman and Martin Rodbell –
“G-proteins and the role of these proteins in signal transduction in cells”
2011
Bruce A. Beutler and Jules A. Hoffmann –
” the activation of innate immunity“and the other half to Ralph M. Steinman – “the dendritic cell and its role in adaptive immunity”.
Renato L. Baserga, M.D.
Kimmel Cancer Center and Keck School of Medicine
Dr. Baserga’s research focuses on the multiple roles of the type 1 insulin-like growth factor receptor (IGF-IR) in the proliferation of mammalian cells. The IGF-IR activated by its ligands is mitogenic, is required for the establishment and the maintenance of the transformed phenotype, and protects tumor cells from apoptosis. It, therefore, serves as an excellent target for therapeutic interventions aimed at inhibiting abnormal growth. In basic investigations, this group is presently studying the effects that the number of IGF-IRs and specific mutations in the receptor itself have on its ability to protect cells from apoptosis.
This investigation is strictly correlated with IGF-IR signaling, and part of this work tries to elucidate the pathways originating from the IGF-IR that are important for its functional effects. Baserga’s group has recently discovered a new signaling pathway used by the IGF-IR to protect cells from apoptosis, a unique pathway that is not used by other growth factor receptors. This pathway depends on the integrity of serines 1280-1283 in the C-terminus of the receptor, which bind 14.3.3 and cause the mitochondrial translocation of Raf-1.
Another recent discovery of this group has been the identification of a mechanism by which the IGF-IR can actually induce differentiation in certain types of cells. When cells have IRS-1 (a major substrate of the IGF-IR), the IGF-IR sends a proliferative signal; in the absence of IRS-1, the receptor induces cell differentiation. The extinction of IRS-1 expression is usually achieved by DNA methylation.
Janardan Reddy, MD
Northwestern University
The central effort of our research has been on a detailed analysis at the cellular and molecular levels of the pleiotropic responses in liver induced by structurally diverse classes of chemicals that include fibrate class of hypolipidemic drugs, and phthalate ester plasticizers, which we designated hepatic peroxisome proliferators. Our work has been central to the establishment of several principles, namely that hepatic peroxisome proliferation is associated with increases in fatty acid oxidation systems in liver, and that peroxisome proliferators, as a class, are novel nongenotoxic hepatocarcinogens.
We introduced the concept that sustained generation of reactive oxygen species leads to oxidative stress and serves as the basis for peroxisome proliferator-induced liver cancer development. Furthermore, based on the tissue/cell specificity of pleiotropic responses and the coordinated transcriptional regulation of fatty acid oxidation system genes, we postulated that peroxisome proliferators exert their action by a receptor-mediated mechanism. This receptor concept laid the foundation for the discovery of
a three member peroxisome proliferator-activated receptor (PPARalpha-, ß-, and gamma) subfamily of nuclear receptors.
PPARalpha is responsible for peroxisome proliferator-induced pleiotropic responses, including
hepatocarcinogenesis and energy combustion as it serves as a fatty acid sensor and regulates fatty acid oxidation.
Our current work focuses on the molecular mechanisms responsible for PPAR action and generation of fatty acid oxidation deficient mouse knockout models. Transcription of specific genes by nuclear receptors is a complex process involving the participation of multiprotein complexes composed of transcription coactivators.
Jose Delgado de Salles Roselino, Ph.D.
Leloir Institute, Brazil
Warburg effect, in reality “Pasteur-effect” was the first example of metabolic regulation described. A decrease in the carbon flux originated at the sugar molecule towards the end metabolic products, ethanol and carbon dioxide that was observed when yeast cells were transferred from anaerobic environmental condition to an aerobic one. In Pasteur´s works, sugar metabolism was measured mainly by the decrease of sugar concentration in the yeast growth media observed after a measured period of time. The decrease of the sugar concentration in the media occurs at great speed in yeast grown in anaerobiosis condition and its speed was greatly reduced by the transfer of the yeast culture to an aerobic condition. This finding was very important for the wine industry of France in Pasteur time, since most of the undesirable outcomes in the industrial use of yeast were perceived when yeasts cells took very long time to create a rather selective anaerobic condition. This selective culture media was led by the carbon dioxide higher levels produced by fast growing yeast cells and by a great alcohol content in the yeast culture media. This finding was required to understand Lavoisier’s results indicating that chemical and biological oxidation of sugars produced the same calorimetric results. This observation requires a control mechanism (metabolic regulation) to avoid burning living cells by fast heat released by the sugar biological oxidative processes (metabolism). In addition, Lavoisier´s results were the first indications that both processes happened inside similar thermodynamics limits.
In much resumed form, these observations indicates the major reasons that led Warburg to test failure in control mechanisms in cancer cells in comparison with the ones observed in normal cells. Biology inside classical thermo dynamics poses some challenges to scientists. For instance, all classical thermodynamics must be measured in reversible thermodynamic conditions. In an isolated system, increase in P (pressure) leads to decrease in V (volume) all this in a condition in which infinitesimal changes in one affects in the same way the other, a continuum response. Not even a quantic amount of energy will stand beyond those parameters. In a reversible system, a decrease in V, under same condition, will led to an increase in P.
In biochemistry, reversible usually indicates a reaction that easily goes from A to B or B to A. This observation confirms the important contribution of E Schrodinger in his What´s Life: “This little book arose from a course of public lectures, delivered by a theoretical physicist to an audience of about four hundred which did not substantially dwindle, though warned at the outset that the subject-matter was a difficult one and that the lectures could not be termed popular, even though the physicist’s most dreaded weapon, mathematical deduction, would hardly be utilized. The reason for this was not that the subject was simple enough to be explained without mathematics, but rather that it was much too involved to be fully accessible to mathematics.”
Hans Krebs describes the cyclic nature of the citrate metabolism. Two major research lines search to understand the mechanism of energy transfer that explains how ADP is converted into ATP. One followed the organic chemistry line of reasoning and therefore, searched how the breakdown of carbon-carbon link could have its energy transferred to ATP synthesis. A major leader of this research line was B. Chance who tried to account for two carbon atoms of acetyl released as carbon dioxide in the series of Krebs cycle reactions. The intermediary could store in a phosphorylated amino acid the energy of carbon-carbon bond breakdown. This activated amino acid could transfer its phosphate group to ADP producing ATP. Alternatively, under the possible influence of the excellent results of Hodgkin and Huxley a second line of research appears.
The work of Hodgkin & Huxley indicated the storage of electrical potential energy in transmembrane ionic asymmetries and presented the explanation for the change from resting to action potential in excitable cells. This second line of research, under the leadership of P Mitchell postulated a mechanism for the transfer of oxide/reductive power of organic molecules oxidation through electron transfer as the key for energetic transfer mechanism required for ATP synthesis. Paul Boyer could present how the energy was transduced by a molecular machine that changes in conformation in a series of 3 steps while rotating in one direction in order to produce ATP and in opposite direction in order to produce ADP plus Pi from ATP (reversibility). Nonetheless, a victorious Peter Mitchell obtained the correct result in the conceptual dispute, over the B. Chance point of view, after he used E. Coli mutants to show H gradients in membrane and its use as energy source.
However, this should not detract from the important work of Chance. B. Chance got the simple and rapid polarographic assay method of oxidative phosphorylation and the idea of control of energy metabolism that bring us back to Pasteur. This second result seems to have been neglected in searching for a single molecular mechanism required for the understanding of the buildup of chemical reserve in our body. In respiring mitochondria the rate of electron transport, and thus the rate of ATP production, is determined primarily by the relative concentrations of ADP, ATP and phosphate in the external media (cytosol) and not by the concentration of respiratory substrate as pyruvate. Therefore, when the yield of ATP is high as is in aerobiosis and the cellular use of ATP is not changed, the oxidation of pyruvate and therefore of glycolysis is quickly (without change in gene expression), throttled down to the resting state. The dependence of respiratory rate on ADP concentration is also seen in intact cells. A muscle at rest and using no ATP has very low respiratory rate.
I have had an ongoing discussion with Jose Eduardo de Salles Roselino, inBrazil. He has made important points that need to be noted.
The constancy of composition which animals maintain in the environment surrounding their cells is one of the dominant features of their physiology. Although this phenomenon, homeostasis, has held the interest of biologists over a long period of time, the elucidation of the molecular basis for complex processes such as temperature control and the maintenance of various substances at constant levels in the blood has not yet been achieved. By comparison, metabolic regulation in microorganisms is much better understood, in part because the microbial physiologist has focused his attention on enzyme-catalyzed reactions and their control, as these are among the few activities of microorganisms amenable to quantitative study. Furthermore, bacteria are characterized by their ability to make rapid and efficient adjustments to extensive variations in most parameters of their environment; therefore, they exhibit a surprising lack of rigid requirements for their environment, and appears to influence it only as an incidental result of their metabolism. Animal cells on the other hand have only a limited capacity for adjustment and therefore require a constant milieu. Maintenance of such constancy appears to be a major goal in their physiology (Regulation of Biosynthetic Pathways H.S. Moyed and H EUmbarger Phys Rev,42 444 (1962)).
A living cell consists in a large part of a concentrated mixture of hundreds of different enzymes, each a highly effective catalyst for one or more chemical reactions involving other components of the cell. The paradox of intense and highly diverse chemical activity on the one hand and strongly poised chemical stability (biological homeostasis) on the other is one of the most challenging problems of biology (Biological feedback Control at the molecular Level D.E. Atkinson Science vol. 150: 851, 1965). Almost nothing is known concerning the actual molecular basis for modulation of an enzyme`s kinetic behavior by interaction with a small molecule. (Biological feedback Control at the molecular Level D.E. Atkinson Science vol. 150: 851, 1965). In the same article, since the core of Atkinson´s thinking seems to be strongly linked with Adenylates as regulatory effectors, the previous phrases seems to indicate a first step towards the conversion of homeostasis to an intracellular phenomenon and therefore, one that contrary to Umbarger´s consideration could be also studied in microorganisms.
Most biochemical studies using bacteria, were made before the end of the third upper part of log growth phase. Therefore, they could be considered as time-independent as S Luria presented biochemistry in Life an Unfinished Experiment. The sole ingredient on the missing side of the events that led us into the molecular biology construction was to consider that proteins, a macromolecule, would never be affected by small molecules translational kinetic energy. This, despite the fact that in a catalytic environment and its biological implications S Grisolia incorporated A K Balls observation indicating that the word proteins could be related to Proteus an old sea god that changed its form whenever he was subjected to inquiry (Phys Rev v 4,657 (1964).
In D.E. Atkinson´s work (Science vol 150 p 851, 1965), changes in protein synthesis acting together with factors that interfere with enzyme activity will lead to “fine-tuned” regulation better than enzymatic activity regulation alone. Comparison of glycemic regulation in granivorous and carnivorous birds indicate that when no important nutritional source of glucose is available, glycemic levels can be kept constant in fasted and fed birds. The same was found in rats and cats fed on high protein diets. Gluconeogenesis is controlled by pyruvate kinase inhibition. Therefore, the fact that it can discriminate between fasting alone and fasting plus exercise (carbachol) requirement of gluconeogenic activity (correspondent level of pyruvate kinase inhibition) the control of enzyme activity can be made fast and efficient without need for changes in genetic expression (20 minute after stimulus) ( Migliorini,R.H. et al Am J. Physiol.257 (Endocrinol. Met. 20): E486, 1989). Regrettably, this was not discussed in the quoted work. So, when the control is not affected by the absorption of nutritional glucose it can be very fast, less energy intensive and very sensitive mechanism of control despite its action being made in the extracellular medium (homeostasis).
Protein folding: amino-acid sequence of bovine BPTI (basic pancreatic trypsin inhibitor) in one-letter code, with its folded 3D structure represented by a stick model of the mainchain and sidechains (in gray), and the backbone and secondary structure by a ribbon colored blue to red from N- to C-terminus. 3D structure from PDB file 1BPI, visualized in Mage and rendered in Raster3D. (Photo credit: Wikipedia)
The Effects of Aprotinin on Endothelial Cell Coagulant Biology
Author: Demet Sag, PhD
The Effects of Aprotinin on Endothelial Cell Coagulant Biology
Demet Sag, PhD*†, Kamran Baig, MBBS, MRCS; James Jaggers, MD, Jeffrey H. Lawson, MD, PhD
Introduction: Cardiopulmonary bypass is associated with a systemic inflammatory response syndrome, which is responsible for excessive bleeding and multisystem dysfunction. Endothelial cell activation is a key pathophysiological process that underlies this response. Aprotinin, a serine protease inhibitor has been shown to be anti-inflammatory and also have significant hemostatic effects in patients undergoing CPB. We sought to investigate the effects of aprotinin at the endothelial cell level in terms of cytokine release (IL-6), tPA release, tissue factor expression, PAR1 + PAR2 expression and calcium mobilization. Methods: Cultured Human Umbilical Vein Endothelial Cells (HUVECS) were stimulated with TNFa for 24 hours and treated with and without aprotinin (200KIU/ml + 1600KIU/ml). IL-6 and tPA production was measured using ELISA. Cellular expression of Tissue Factor, PAR1 and PAR2 was measured using flow cytometry. Intracellular calcium mobilization following stimulation with PAR specific peptides and agonists (trypsin, thrombin, Human Factor VIIa, factor Xa) was measured using fluorometry with Fluo-3AM. Results: Aprotinin at the high dose (1600kIU/mL), 183.95 ± 13.06mg/mL but not low dose (200kIU/mL) significantly reduced IL-6 production from TNFa stimulated HUVECS (p=0.043). Aprotinin treatment of TNFa activated endothelial cells significantly reduce the amount of tPA released in a dose dependent manner (A200 p=0.0018, A1600 p=0.033). Aprotinin resulted in a significant downregulation of TF expression to baseline levels. At 24 hours, we found that aprotinin treatment of TNFa stimulated cells resulted in a significant downregulation of PAR-1 expression. Aprotinin significantly inhibited the effects of the protease thrombin upon PAR1 mediated calcium release. The effects of PAR2 stimulatory proteases such as human factor Xa, human factor VIIa and trypsin on calcium release was also inhibited by aprotinin. Conclusion: We have shown that aprotinin has direct anti-inflammatory effects on endothelial cell activation and these effects may be mediated through inhibition of proteolytic activation of PAR1 and PAR2. Abstract word count: 297
INTRODUCTION Each year it is estimated that 350,000 patients in the United States, and 650,000 worldwide undergo cardiopulmonary bypass (CPB). Despite advances in surgical techniques and perioperative management the morbidity and mortality of cardiac surgery related to the systemic inflammatory response syndrome(SIRS), especially in neonates is devastatingly significant. Cardiopulmonary bypass exerts an extreme challenge upon the haemostatic system as part of the systemic inflammatory syndrome predisposing to excessive bleeding as well as other multisystem dysfunction (1). Over the past decade major strides have been made in the understanding of the pathophysiology of the inflammatory response following CPB and the role of the vascular endothelium has emerged as critical in maintaining cardiovascular homeostasis (2).
CPB results in endothelial cell activation and initiation of coagulation via the Tissue Factor dependent pathway and consumption of important clotting factors. The major stimulus for thrombin generation during CPB has been shown to be through the tissue factor dependent pathway. As well as its effects on the fibrin and platelets thrombin has been found to play a role in a host of inflammatory responses in the vascular endothelium. The recent discovery of the Protease-Activated Receptors (PAR), one of which through which thrombin acts (PAR-1) has stimulated interest that they may provide a vital link between inflammation and coagulation (3).
Aprotinin is a nonspecific serine protease inhibitor that has been used for its ability to reduce blood loss and preserve platelet function during cardiac surgery procedures requiring cardiopulmonary bypass and thus the need for subsequent blood and blood product transfusions. However there have been concerns that aprotinin may be pro-thrombotic, especially in the context of coronary artery bypass grafting, which has limited its clinical use. These reservations are underlined by the fact that the mechanism of action of aprotinin has not been fully understood. Recently aprotinin has been shown to exert anti-thrombotic effects mediated by blocking the PAR-1 (4). Much less is known about its effects on endothelial cell activation, especially in terms of Tissue Factor but it has been proposed that aprotinin may also exert protective effects at the endothelial level via protease-activated receptors (PAR1 and PAR2). In this study we simulated in vitro the effects of endothelial cell activation during CPB by stimulating Human Umbilical Vein Endothelial Cells (HUVECs) with a proinflammatory cytokine released during CPB, Tumor Necrosis Factor (TNF-a) and characterize the effects of aprotinin treatment on TF expression, PAR1 and PAR2 expression, cytokine release IL-6 and tPA secretion. In order to investigate the mechanism of action of aprotinin we studied its effects on PAR activation by various agonists and ligands.
These experiments provide insight into the effects of aprotinin on endothelial related coagulation mechanisms in terms of Tissue Factor expression and indicate it effects are mediated through Protease-Activated Receptors (PAR), which are seven membrane spanning proteins called G-protein coupled receptors (GPCR), that link coagulant and inflammatory pathways. Therefore, in this study we examine the effects of aprotinin on the human endothelial cell coagulation biology by different-dose aprotinin, 200 and 1600units. The data demonstrates that aprotinin appears to directly alter endothelial expression of inflammatory cytokines, tPA and PAR receptor expression following treatment with TNF. The direct mechanism of action is unknown but may act via local protease inhibition directly on endothelial cells. It is hoped that with improved understanding of the mechanisms of action of aprotinin, especially an antithrombotic effect at the endothelial level the fears of prothrombotic tendency may be lessened and its use will become more routine.
METHODS Human Umbilical Vein Endothelial Cells (HUVECS) used as our model to study the effects of endothelial cell activation on coagulant biology. In order to simulate the effects of cardiopulmonary bypass at the endothelial cell interface we stimulated the cells with the proinflammatory cytokine TNFa. In the study group the HUVECs were pretreated with low (200kIU/mL) and high (1600kIU/mL) dosages of aprotinin prior to stimulation with TNFa and complement activation fragments. The effects of TNFa stimulation upon endothelial Tissue Factor expression, PAR1 and PAR2 expression, and tPA and IL6 secretion were determined and compared between control and aprotinin treated cells. In order to delineate whether aprotinin blocks PAR activation via its protease inhibition properties we directly activated PAR1 and PAR2 using specific agonist ligands such thrombin (PAR1), trypsin, Factor VIIa, Factor Xa (PAR2) in the absence and presence of aprotinin.
Endothelial Cell Culture HUVECs were supplied from Clonetics. The cells were grown in EBM-2 containing 2MV bullet kit, including 5% FBS, 100-IU/ml penicillin, 0.1mg/mL streptomycin, 2mmol/L L-glutamine, 10 U/ml heparin, 30µg/mL EC growth supplement (ECGS). Before the stimulation cells were starved in 0.1%BSA depleted with FBS and growth factors for 24 hours. Cells were sedimented at 210g for 10 minutes at 4C and then resuspended in culture media. The HUVECs to be used will be between 3 and 5 passages.
Assay of IL-6 and tPA production Levels of IL-6 were measured with an ELISA based kit (RDI, MN) according to the manufacturers instructions. tPA was measured using a similar kit (American Diagnostica).
Flow CytometryThe expression of transmembrane proteins PAR1, PAR2 and tissue factor were measured by single color assay as FITC labeling agent. Prepared suspension of cells disassociated trypsin free cell disassociation solution (Gibco) to be labeled. First well washed, and resuspended into “labeling buffer”, phosphate buffered saline (PBS) containing 0.5% BSA plus 0.1% NaN3, and 5% fetal bovine serum to block Fc and non-specific Ig binding sites. Followed by addition of 5mcl of antibody to approx. 1 million cells in 100µl labeling buffer and incubate at 4C for 1 hour. After washing the cells with 200µl with wash buffer, PBS + 0.1% BSA + 0.1% NaN3, the cells were pelletted at 1000rpm for 2 mins. Since the PAR1 and PAR2 were directly labeled with FITC these cells were fixed for later analysis by flow cytometry in 500µl PBS containing 1%BSA + 0.1% NaN3, then add equal volume of 4% formalin in PBS. For tissue factor raised in mouse as monoclonal primary antibody, the pellet resuspended and washed twice more as before, and incubated at 4C for 1 hour addition of 5µl donkey anti-mouse conjugated with FITC secondary antibody directly to the cell pellets at appropriate dilution in labeling buffer. After the final wash three times, the cell pellets were resuspended thoroughly in fixing solution. These fixed and labeled cells were then stored in the dark at 4C until there were analyzed. On analysis, scatter gating was used to avoid collecting data from debris and any dead cells. Logarithmic amplifiers for the fluorescence signal were used as this minimizes the effects of different sensitivities between machines for this type of data collection.
Intracellular Calcium Measurement
Measured the intracellular calcium mobilization by Fluo-3AM. HUVECs were grown in calcium and phenol free EBM basal media containing 2MV bullet kit. Then the cell cultures were starved with the same media by 0.1% BSA without FBS for 24 hour with or without TNFa stimulation presence or absence of aprotinin (200 and 1600KIU/ml). Next the cells were loaded with Fluo-3AM 5µg/ml containing agonists, PAR1 specific peptide SFLLRN-PAR1 inhibitor, PAR2 specific peptide SLIGKV-PAR2 inhibitor, human alpha thrombin, trypsin, factor VIIa, factor Xa for an hour at 37C in the incubation chamber. Finally the media was replaced by Flou-3AM free media and incubated for another 30 minutes in the incubation chamber. The readings were taken at fluoromatic bioplate reader. For comparison purposes readings were taken before and during Fluo-3AM loading as well.
RESULTSAprotinin reduces IL-6 production from activated/stimulated HUVECS The effects of aprotinin analyzed on HUVEC for the anti-inflammatory effects of aprotinin at cultured HUVECS with high and low doses. Figure 1 shows that TNF-a stimulated a considerable increase in IL-6 production, 370.95 ± 109.9 mg/mL. If the drug is used alone the decrease of IL-6 at the low dose is 50% that is 183.95 ng/ml and with the high dose of 20% that is 338.92 from 370.95ng/ml being compared value. TNFa-aprotinin results in reduction of the IL-6 expression from 370.95ng/ml to 58.6 (6.4fold) fro A200 and 75.85 (4.9 fold) ng/ml, for A1600. After the treatment the cells reach to the below baseline limit of IL-6 expression. Aprotinin at the high dose (1600kIU/mL), 183.95 ± 13.06mg/mL but not low dose (200kIU/mL) significantly reduced IL-6 production from TNF-a stimulated HUVECS (p=0.043). Therefore, the aprotinin prevents inflammation as well as loss of blood.
Aprotinin reduces tPA production from stimulated HUVECS Whether aprotinin exerted part of its fibrinolytic effects through inhibition of tPA mediated plasmin generation examined by the effects on TNFa stimulated HUVECS. Figure 2 also demonstrates that the amount of tPA released from HUVECS under resting, non-stimulated conditions incubated with aprotinin are significantly different. Figure 2 represents that the resting level of tPA released from non-stimulated cells significantly, by 100%, increase following TNF-a stimulation for 24 hours. After application of aprotinin alone at two doses the tPA level goes down 25% of TNFa stimulated cells. However, aprotinin treatment of TNF-a activated endothelial cells significantly lower the amount of tPA release in a dose dependent manner that is low dose decreased 25 but high dose causes 50% decrease of tPA expression (A200 p=0.0018, A1600 p=0.033) This finding suggests that aprotinin exerts a direct inhibitory effect on endothelial cell tPA production.
Aprotinin and receptor expression on activated HUVECS
TF is expressed when the cell in under stress such as TNFa treatments. The stimulated HUVECs with TNF-a tested for the expression of PAR1, PAR2, and tissue factor by single color flow cytometry through FITC labeled detection antibodies at 1, 3, and 24hs.
Tissue Factor expression is reduced:
Figure 3 demonstrates that there is a fluctuation of TF expression from 1 h to 24h that the TF decreases at first hour after aprotinin application 50% and 25%, A1600 and A200 respectively. Then at 3 h the expression come back up 50% more than the baseline. Finally, at 24h the expression of TF becomes almost as same as baseline. Moreover, TNFa stimulated cells remains 45% higher than baseline after at 3h as well as at 24h.
PAR1 decreased:
Figure 4 demonstrates that aprotinin reduces the PAR1 expression 80% at 24h but there is no affect at 1 and 3 h intervals for both doses.
During the treatment with aprotinin only high dose at 1 hour time interval decreases the PAR1 expression on the cells. This data explains that ECCB is affected due to the expression of PAR1 is lowered by the high dose of aprotinin.
PAR2 is decreased by aprotinin:
Figure 5 shows the high dose of aprotinin reduces the PAR2 expression close to 25% at 1h, 50% at 3h and none at 24h. This pattern is exact opposite of PAR1 expression. Figure 5 demonstrates the 50% decrease at 3h interval only. Does that mean aprotinin affecting the inflammation first and then coagulation?
This suggests that aprotinin may affect the PAR2 expression at early and switched to PAR1 reduction later time intervals. This fluctuation can be normal because aprotinin is not a specific inhibitor for proteases. This approach make the aprotinin work better the control bleeding and preventing the inflammation causing cytokine such as IL-6.
Aprotinin inhibits Calcium fluxes induced by PAR1/2 specific agonists
The specificity of aprotinin’s actions upon PAR studied the effects of the agent on calcium release following proteolytic and non-proteolytic stimulation of PAR1 and PAR2. Figure 6A (Figure 6) shows the stimulation of the cells with the PAR1 specific peptide (SFLLRN) results in release of calcium from the cells. Pretreatment of the cells with aprotinin has no significant effect on PAR1 peptide stimulated calcium release. This suggests that aprotinin has no effect upon the non-proteolytic direct activation of the PAR 1 receptor. Yet, Figure 6B (Figure 6) demonstrates human alpha thrombin does interact with the drug as a result the calcium release drops below base line after high dose (A1600) aprotinin used to zero but low dose does not show significant effect on calcium influx. Figure 7 demonstrates the direct PAR2 and indirect PAR2 stimulation by hFVIIa, hFXa, and trypsin of cells. Similarly, at Figure 7A aprotinin has no effect upon PAR2 peptide stimulated calcium release, however, at figures 7B, C, and D shows that PAR2 stimulatory proteases Human Factor Xa, Human Factor VIIa and Trypsin decreases calcium release. These findings indicate that aprotinin’s mechanism of action is directed towards inhibiting proteolytic cleavage and hence subsequent activation of the PAR1 and PAR2 receptor complexes. The binding site of the aprotinin on thrombin possibly is not the peptide sequence interacting with receptors.
Measurement of calcium concentration is essential to understand the mechanism of aprotinin on endothelial cell coagulation and inflammation because these mechanisms are tightly controlled by presence of calcium. For example, activation of PAR receptors cause activation of G protein q subunit that leads to phosphoinositol to secrete calcium from endoplasmic reticulum into cytoplasm or activation of DAG to affect Phospho Lipase C (PLC). In turn, certain calcium concentration will start the serial formation of chain reaction for coagulation. Therefore, treatment of the cells with specific factors, thrombin receptor activating peptides (TRAPs), human alpha thrombin, trypsin, human factor VIIa, and human factor Xa, would shed light into the effect of aprotinin on the formation of complexes for pro-coagulant activity. DISCUSSION There are two fold of outcomes to be overcome during cardiopulmonary bypass (CPB): mechanical stress and the contact of blood with artificial surfaces results in the activation of pro- and anticoagulant systems as well as the immune response leading to inflammation and systemic organ failure. This phenomenon causes the “postperfusion-syndrome”, with leukocytosis, increased capillary permeability, accumulation of interstitial fluid, and organ dysfunction. CPB is also associated with a significant inflammatory reaction, which has been related to complement activation, and release of various inflammatory mediators and proteolytic enzymes. CPB induces an inflammatory state characterized by tumor necrosis factor-alpha release. Aprotinin, a low molecular-weight peptide inhibitor of trypsin, kallikrein and plasmin has been proposed to influence whole body inflammatory response inhibiting kallikrein formation, complement activation and neutrophil activation (5, 6). But shown that aprotinin has no significant influence on the inflammatory reaction to CPB in men. Understanding the endothelial cell responses to injury is therefore central to appreciating the role that dysfunction plays in the preoperative, operative, and postoperative course of nearly all cardiovascular surgery patients. Whether aprotinin increases the risk of thrombotic complications remains controversial. The anti-inflammatory properties of aprotinin in attenuating the clinical manifestations of the systemic inflammatory response following cardiopulmonary bypass are well known(15) 16) However its mechanisms and targets of action are not fully understood. In this study we have investigated the actions of aprotinin at the endothelial cell level. Our experiments showed that aprotinin reduced TNF-a induced IL-6 release from cultured HUVECS. Thrombin mediates its effects through PAR-1 receptor and we found that aprotinin reduced the expression of PAR-1 on the surface of HUVECS after 24 hours incubation. We then demonstrated that aprotinin inhibited endothelial cell PAR proteolytic activation by thrombin (PAR-1), trypsin, factor VII and factor X (PAR-2) in terms of less release of Ca preventing the activation of coagulation. So aprotinin made cells produce less receptor, PAR1, PAR2, and TF as a result there would be less Ca++ release. Our findings provide evidence for anti-inflammatory as well as anti-coagulant properties of aprotinin at the endothelial cell level, which may be mediated through its inhibitory effects on proteolytic activation of PARs. IL6 Elevated levels of IL-6 have been shown to correlate with adverse outcomes following cardiac surgery in terms of cardiac dysfunction and impaired lung function(Hennein et al 1992). Cardiopulmonary bypass is associated with the release of the pro-inflammatory cytokines IL-6, IL-8 and TNF-a. IL-6 is produced by T-cells, endothelial cells as a result monocytes and plasma levels of this cytokine tend to increase during CPB (21, 22). In some studies aprotinin has been shown to reduce levels of IL-6 post CPB(23) Hill(5). Others have failed to demonstrate an inhibitory effect of aprotinin upon pro-inflammatory cytokines following CPB(24) (25). Our experiments showed that aprotinin significantly reduced the release of IL-6 from TNF-a stimulated endothelial cells, which may represent an important target of its anti-inflammatory properties. Its has been shown recently that activation of HUVEC by PAR-1 and PAR-2 agonists stimulates the production of IL-6(26). Hence it is possible that the effects of aprotinin in reducing IL-6 may be through targeting activation of such receptors. TPA Tissue Plasminogen activator is stored, ready made, in endothelial cells and it is released at its highest levels just after commencing CPB and again after protamine administration. The increased fibrinolytic activity associated with the release of tPA can be correlated to the excessive bleeding postoperatively. Thrombin is thought to be the major stimulus for release of t-PA from endothelial cells. Aprotinin’s haemostatic properties are due to direct inhibition of plasmin, thereby reducing fibrinolytic activity as well as inhibiting fibrin degradation. Aprotinin has not been shown to have any significant effect upon t-PA levels in patients post CPB(27), which would suggest that aprotinin reduced fibrinolytic effects are not the result of inhibition of t-PA mediated plasmin generation. Our study, however demonstrates that aprotinin inhibits the release of t-PA from activated endothelial cells, which may represent a further haemostatic mechanism at the endothelial cell level. TF Resting endothelial cells do not normally express tissue factor on their cell surface. Inflammatory mediators released during CPB such as complement (C5a), lipopolysaccharide, IL-6, IL-1, TNF-a, mitogens, adhesion molecules and hypoxia may induce the expression of tissue factor on endothelial cells and monocytes. The expression of TF on activated endothelial cells activates the extrinsic pathway of coagulation, ultimately resulting in the generation of thrombin and fibrin. Aprotinin has been shown to reduce the expression of TF on monocytes in a simulated cardiopulmonary bypass circuit (28).
We found that treatment of activated endothelial cells with aprotinin significantly reduced the expression of TF after 24 hours. This would be expected to result in reduced thrombin generation and represent an additional possible anticoagulant effect of aprotinin. In a previous study from our laboratory we demonstrated that there were two peaks of inducible TF activity on endothelial cells, one immediately post CPB and the second at 24 hours (29). The latter peak is thought to be responsible for a shift from the initial fibrinolytic state into a procoagulant state. In addition to its established early haemostatic and coagulant effect, aprotinin may also have a delayed anti-coagulant effect through its inhibition of TF mediated coagulation pathway. Hence its effects may counterbalance the haemostatic derangements, i.e. first bleeding then thrombosis caused by CPB. The anti-inflammatory effects of aprotinin may also be related to inhibition of TF and thrombin generation. PARs
It has been suggested that aprotinin may target PAR on other cells types, especially endothelial cells. We investigated the role of PARs in endothelial cell activation and whether they can be the targets for aprotinin. In recent study by Day group(30) demonstrated that endothelial cell activation by thrombin and downstream inflammatory responses can be inhibited by aprotinin in vitro through blockade of protease-activated receptor 1. Our results provide a new molecular basis to help explain the anti-inflammatory properties of aprotinin reported clinically. The finding that PAR-2 can also be activated by the coagulation enzymes factor VII and factor X indicates that PAR may represent the link between inflammation and coagulation. PAR-2 is believed to play an important role in inflammatory response. PAR-2 are widely expressed in the gastrointestinal tract, pancreas, kidney, liver, airway, prostrate, ovary, eye of endothelial, epithelial, smooth muscle cells, T-cells and neutrophils. Activation of PAR-2 in vivo has been shown to be involved in early inflammatory processes of leucocyte recruitment, rolling, and adherence, possibly through a mechanism involving platelet-activating factor (PAF) We investigated the effects of TNFa stimulation on PAR-1 and PAR-2 expression on endothelial cells. Through functional analysis of PAR-1 and PAR-2 by measuring intracellular calcium influx we have demonstrated that aprotinin blocks proteolytic cleavage of PAR-1 by thrombin and activation of PAR-2 by the proteases trypsin, factor VII and factor X. This confirms the previous findings on platelets of an endothelial anti-thrombotic effect through inhibition of proteolysis of PAR-1. In addition, part of aprotinin’s anti-inflammatory effects may be mediated by the inhibition of serine proteases that activate PAR-2. There have been conflicting reports regarding the regulation of PAR-1 expression by inflammatory mediators in cultured human endothelial cells. Poullis et al first showed that thrombin induced platelet aggregation was mediated by via the PAR-1(4) and demonstrated that aprotinin inhibited the serine protease thrombin and trypsin induced platelet aggregation. Aprotinin did not block PAR-1 activation by the non-proteolytic agonist peptide, SFLLRN indicating that the mechanism of action was directed towards inhibiting proteolytic cleavage of the receptor. Nysted et al showed that TNF did not affect mRNA and cell surface protein expression of PAR-1 (35), whereas Yan et al showed downregulation of PAR-1 mRNA levels (36). Once activated PAR1 and PAR2 are rapidly internalized and then transferred to lysosomes for degradation.
Endothelial cells contain large intracellular pools of preformed receptors that can replace the cleaved receptors over a period of approximately 2 hours, thus restoring the capacity of the cells to respond to thrombin. In this study we found that after 1-hour stimulation with TNF there was a significant upregulation in PAR-1 expression. However after 3 hours and 24 hours there was no significant change in PAR-1 expression suggesting that cleaved receptors had been internalized and replenished. Aprotinin was interestingly shown to downregulate PAR-1 expression on endothelial cells at 1 hour and increasingly more so after 24 hours TNF stimulation. These findings may suggest an effect of aprotinin on inhibiting intracellular cycling and synthesis of PAR-1.
Conclusions Our study has identified the anti-inflammatory and coagulant effects of aprotinin at the endothelial cell level. All together aprotinin affects the ECCB by reducing the t-PA, IL-6, PAR1, PAR 2, TF expressions. Our data correlates with the previous foundlings in production of tPA (7, (8) 9) 10), and decreased IL-6 levels (11) during coronary artery bypass graft surgery (12-14). We have importantly demonstrated that aprotinin may target proteolytic activation of endothelial cell associated PAR-1 to exert a possible anti-inflammatory effect. This evidence should lessen the concerns of a possible prothrombotic effect and increased incidence of graft occlusion in coronary artery bypass patients treated with aprotinin. Aprotinin may also inhibit PAR-2 proteolytic activation, which may represent a key mechanism for attenuating the inflammatory response at the critical endothelial cell level. Although aprotinin has always been known as a non-specific protease inhibitor we would suggest that there is growing evidence for a PAR-ticular mechanism of action.
REFERENCES
1. Levy, J. H., and Tanaka, K. A. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg. 75: S715-720, 2003.
2. Verrier, E. D., and Morgan, E. N. Endothelial response to cardiopulmonary bypass surgery. Ann Thorac Surg. 66: S17-19; discussion S25-18, 1998.
3. Cirino, G., Napoli, C., Bucci, M., and Cicala, C. Inflammation-coagulation network: are serine protease receptors the knot? Trends Pharmacol Sci. 21: 170-172, 2000. 4. Poullis, M., Manning, R., Laffan, M., Haskard, D. O., Taylor, K. M., and Landis, R. C. The antithrombotic effect of aprotinin: actions mediated via the proteaseactivated receptor 1. J Thorac Cardiovasc Surg. 120: 370-378, 2000.
5. Hill, G. E., Alonso, A., Spurzem, J. R., Stammers, A. H., and Robbins, R. A. Aprotinin and methylprednisolone equally blunt cardiopulmonary bypass-induced inflammation in humans. J Thorac Cardiovasc Surg. 110: 1658-1662, 1995.
6. Hill, G. E., Pohorecki, R., Alonso, A., Rennard, S. I., and Robbins, R. A. Aprotinin reduces interleukin-8 production and lung neutrophil accumulation after cardiopulmonary bypass. Anesth Analg. 83: 696-700, 1996. 7. Lu, H., Du Buit, C., Soria, J., Touchot, B., Chollet, B., Commin, P. L., Conseiller, C., Echter, E., and Soria, C. Postoperative hemostasis and fibrinolysis in patients undergoing cardiopulmonary bypass with or without aprotinin therapy. Thromb Haemost. 72: 438-443, 1994.
8. de Haan, J., and van Oeveren, W. Platelets and soluble fibrin promote plasminogen activation causing downregulation of platelet glycoprotein Ib/IX complexes: protection by aprotinin. Thromb Res. 92: 171-179, 1998.
9. Erhardtsen, E., Bregengaard, C., Hedner, U., Diness, V., Halkjaer, E., and Petersen, L. C. The effect of recombinant aprotinin on t-PA-induced bleeding in rats. Blood Coagul Fibrinolysis. 5: 707-712, 1994.
10. Orchard, M. A., Goodchild, C. S., Prentice, C. R., Davies, J. A., Benoit, S. E., Creighton-Kemsford, L. J., Gaffney, P. J., and Michelson, A. D. Aprotinin reduces cardiopulmonary bypass-induced blood loss and inhibits fibrinolysis without influencing platelets. Br J Haematol. 85: 533-541, 1993.
11. Tassani, P., Augustin, N., Barankay, A., Braun, S. L., Zaccaria, F., and Richter, J. A. High-dose aprotinin modulates the balance between proinflammatory and anti-inflammatory responses during coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth.14: 682-686, 2000.
12. Asehnoune, K., Dehoux, M., Lecon-Malas, V., Toueg, M. L., Gonieaux, M. H., Omnes, L., Desmonts, J. M., Durand, G., and Philip, I. Differential effects of aprotinin and tranexamic acid on endotoxin desensitization of blood cells induced by circulation through an isolated extracorporeal circuit. J Cardiothorac Vasc Anesth. 16: 447-451, 2002.
13. Dehoux, M. S., Hernot, S., Asehnoune, K., Boutten, A., Paquin, S., Lecon-Malas, V., Toueg, M. L., Desmonts, J. M., Durand, G., and Philip, I. Cardiopulmonary bypass decreases cytokine production in lipopolysaccharide-stimulated whole blood cells: roles of interleukin-10 and the extracorporeal circuit. Crit Care Med. 28: 1721-1727, 2000.
14. Greilich, P. E., Brouse, C. F., Rinder, C. S., Smith, B. R., Sandoval, B. A., Rinder, H. M., Eberhart, R. C., and Jessen, M. E. Effects of epsilon-aminocaproic acid and aprotinin on leukocyte-platelet adhesion in patients undergoing cardiac surgery. Anesthesiology. 100: 225-233, 2004.
15. Mojcik, C. F., and Levy, J. H. Aprotinin and the systemic inflammatory response after cardiopulmonary bypass. Ann Thorac Surg. 71: 745-754, 2001.
16. Landis, R. C., Asimakopoulos, G., Poullis, M., Haskard, D. O., and Taylor, K. M. The antithrombotic and antiinflammatory mechanisms of action of aprotinin. Ann Thorac Surg. 72: 2169-2175, 2001.
17. Asimakopoulos, G., Kohn, A., Stefanou, D. C., Haskard, D. O., Landis, R. C., and Taylor, K. M. Leukocyte integrin expression in patients undergoing cardiopulmonary bypass. Ann Thorac Surg. 69: 1192-1197, 2000.
18. Landis, R. C., Asimakopoulos, G., Poullis, M., Thompson, R., Nourshargh, S., Haskard, D. O., and Taylor, K. M. Effect of aprotinin (trasylol) on the inflammatory and thrombotic complications of conventional cardiopulmonary bypass surgery. Heart Surg Forum. 4 Suppl 1: S35-39, 2001.
19. Asimakopoulos, G., Thompson, R., Nourshargh, S., Lidington, E. A., Mason, J. C., Ratnatunga, C. P., Haskard, D. O., Taylor, K. M., and Landis, R. C. An anti-inflammatory property of aprotinin detected at the level of leukocyte extravasation. J Thorac Cardiovasc Surg. 120: 361-369, 2000.
20. Asimakopoulos, G., Lidington, E. A., Mason, J., Haskard, D. O., Taylor, K. M., and Landis, R. C. Effect of aprotinin on endothelial cell activation. J Thorac Cardiovasc Surg. 122: 123-128, 2001.
21. Butler, J., Chong, G. L., Baigrie, R. J., Pillai, R., Westaby, S., and Rocker, G. M. Cytokine responses to cardiopulmonary bypass with membrane and bubble oxygenation. Ann Thorac Surg. 53: 833-838, 1992.
22. Hennein, H. A., Ebba, H., Rodriguez, J. L., Merrick, S. H., Keith, F. M., Bronstein, M. H., Leung, J. M., Mangano, D. T., Greenfield, L. J., and Rankin, J. S. Relationship of the proinflammatory cytokines to myocardial ischemia and dysfunction after uncomplicated coronary revascularization. J Thorac Cardiovasc Surg. 108: 626-635, 1994.
23. Diego, R. P., Mihalakakos, P. J., Hexum, T. D., and Hill, G. E. Methylprednisolone and full-dose aprotinin reduce reperfusion injury after cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 11: 29-31, 1997.
24. Ashraf, S., Tian, Y., Cowan, D., Nair, U., Chatrath, R., Saunders, N. R., Watterson, K. G., and Martin, P. G. “Low-dose” aprotinin modifies hemostasis but not proinflammatory cytokine release. Ann Thorac Surg. 63: 68-73, 1997.
25. Schmartz, D., Tabardel, Y., Preiser, J. C., Barvais, L., d’Hollander, A., Duchateau, J., and Vincent, J. L. Does aprotinin influence the inflammatory response to cardiopulmonary bypass in patients? J Thorac Cardiovasc Surg. 125: 184-190, 2003.
26. Chi, L., Li, Y., Stehno-Bittel, L., Gao, J., Morrison, D. C., Stechschulte, D. J., and Dileepan, K. N. Interleukin-6 production by endothelial cells via stimulation of protease-activated receptors is amplified by endotoxin and tumor necrosis factor-alpha. J Interferon Cytokine Res. 21: 231-240, 2001.
27. Ray, M. J., and Marsh, N. A. Aprotinin reduces blood loss after cardiopulmonary bypass by direct inhibition of plasmin. Thromb Haemost. 78: 1021-1026, 1997.
28. Khan, M. M., Gikakis, N., Miyamoto, S., Rao, A. K., Cooper, S. L., Edmunds, L. H., Jr., and Colman, R. W. Aprotinin inhibits thrombin formation and monocyte tissue factor in simulated cardiopulmonary bypass. Ann Thorac Surg. 68: 473-478, 1999.
29. Jaggers, J. J., Neal, M. C., Smith, P. K., Ungerleider, R. M., and Lawson, J. H. Infant cardiopulmonary bypass: a procoagulant state. Ann Thorac Surg. 68: 513-520, 1999.
30. Day, J. R., Taylor, K. M., Lidington, E. A., Mason, J. C., Haskard, D. O., Randi, A. M., and Landis, R. C. Aprotinin inhibits proinflammatory activation of endothelial cells by thrombin through the protease-activated receptor 1. J Thorac Cardiovasc Surg. 131: 21-27, 2006.
31. Vergnolle, N. Proteinase-activated receptor-2-activating peptides induce leukocyte rolling, adhesion, and extravasation in vivo. J Immunol. 163: 5064-5069, 1999.
32. Vergnolle, N., Hollenberg, M. D., Sharkey, K. A., and Wallace, J. L. Characterization of the inflammatory response to proteinase-activated receptor-2 (PAR2)-activating peptides in the rat paw. Br J Pharmacol. 127: 1083-1090, 1999.
33. McLean, P. G., Aston, D., Sarkar, D., and Ahluwalia, A. Protease-activated receptor-2 activation causes EDHF-like coronary vasodilation: selective preservation in ischemia/reperfusion injury: involvement of lipoxygenase products, VR1 receptors, and C-fibers. Circ Res. 90: 465-472, 2002.
34. Maree, A., and Fitzgerald, D. PAR2 is partout and now in the heart. Circ Res. 90: 366-368, 2002.
35. Nystedt, S., Ramakrishnan, V., and Sundelin, J. The proteinase-activated receptor 2 is induced by inflammatory mediators in human endothelial cells. Comparison with the thrombin receptor. J Biol Chem. 271: 14910-14915, 1996.
36. Yan, W., Tiruppathi, C., Lum, H., Qiao, R., and Malik, A. B. Protein kinase C beta regulates heterologous desensitization of thrombin receptor (PAR-1) in endothelial cells. Am J Physiol. 274: C387-395, 1998.
37. Shinohara, T., Suzuki, K., Takada, K., Okada, M., and Ohsuzu, F. Regulation of proteinase-activated receptor 1 by inflammatory mediators in human vascular endothelial cells. Cytokine. 19: 66-75, 2002.
FIGURES
Figure 1: IL-6 production following TNF-a stimulation Figure 1
Figure 2: tPA production following TNF-a stimulation Figure 2
Richard Nixon launched the so-called War on Cancer on December 23, 1971, in what was supposed to be a “moonshot” effort to cure the disease. Two years later, a Time magazine cover read, “Toward Control of Cancer.” Two decades after that, it announced, in bold red letters, “Hope in the War Against Cancer,” surmising that “a turning point” may have been reached. In 2001, its cover asked if the blood cancer drug Gleevec “is the breakthrough we’ve been waiting for.” And this past April, the newsweekly pronounced “How to Cure Cancer.” Yet roughly one hundred and forty thousand Americans have died from the disease in the last three months.
Outrage over our paltry victories against cancer informs the forthcoming book, “The Truth in Small Doses: Why We’re Losing the War on Cancer—and How to Win It,” by Clifton Leaf, who wrote a much-discussed essay on the same topic for Fortune in 2004. The title comes from a 1959 pamphlet that tells doctors to trickle out information to cancer-stricken patients, since most of them “couldn’t stand” to know the truth: the disease would kill them and there was little that could be done about it. Today, draped in ribbons of every hue, blinded by the promises of targeted therapies and antioxidants, we have, according to Leaf, neglected a basic truth: “‘the cancer problem’ is, in reality, as formidable a challenge as ever.” (Jerome Groopman discussed the progress in cancer cures, particularly immune therapy, in the magazine last year.)
Leaf is not an oncologist, but he became acquainted with the profession at an early age; he was diagnosed with Hodgkin’s disease at fifteen years old. In the book’s most poignant moment, Leaf orders his father into the corner of his hospital room to atone for having dozed off while sitting bedside. When Leaf woke up the next morning, “the biggest man I had ever known” was still standing in the corner.
As an editor at Fortune, Leaf became enthralled by the promise of Gleevec, an enzyme inhibitor that, since its release in 2001, has proven highly effective at battling chronic myeloid leukemia. Many thought a new age was coming, in which the chaotic spread of cancer would be hindered by drugs that would be precision-targeted to block the replication of rogue cells. It seemed far better than indiscriminately killing both cancerous and healthy cells, as chemotherapy had been doing for the past half-century.
But Gleevec is the exception, not the rule—and C.M.L. is a relatively simple cancer compared to solid-state tumors of the lung, colon, pancreas, or breast. Once they metastasize, most cannot be cured. Those, like Leaf, who have faced cancer have good reason for their impatience: it takes an average of thirteen years to bring a new cancer drug to market. Many of these drugs are pellets fired into cancer’s flank. A recent article in the New York Times titled “Promising New Cancer Drugs Empower the Body’s Own Defense” hailed a new melanoma drug whose median survival rate was 16.8 months. An editorial this winter in The Lancet, the august British medical journal, put the matter even more bluntly: “Has cancer medicine failed patients? In the words of cancer experts, the answer is yes.”
Leaf argues we should be closer to an all-out cure, considering our investment in the effort. The National Cancer Institute receives roughly five billion dollars per year from the federal government. If both public and private investments are to be accounted for, then Leaf estimates the United States spends about sixteen billion dollars a year on cancer research. Nor is there a lack of political will to eradicate cancer, as there is to, say, reducing carbon emissions. Leaf calls it a “bipartisan disease” that a Republican from Alabama would want defeated as much as a Democrat from Illinois. President Barack Obama said in 2009 that he would “launch a new effort to conquer a disease that has touched the life of nearly every American, including me, by seeking a cure for cancer in our time.”
In Leaf’s telling, oncology is a hidebound field averse to risk, a culture that “has grown progressively less hospitable to new voices and ideas over the past four decades.” He yearns for the likes of Sidney Farber, the unorthodox pathologist who invented chemotherapy in the late nineteen forties at Boston Children’s Hospital by injecting children stricken with acute lymphoblastic leukemia with aminopterin, which prevents cancer cells from replicating. A hero in Siddhartha Mukherjee’s “The Emperor of All Maladies,” Farber is largely responsible for the fact that childhood A.L.L. is a manageable disease today. But his methods had a high cost: he disobeyed superiors, conducted his own trial-and-error studies, and foisted unproven drugs on sick, vulnerable children.
What made Farber an iconoclast is that he wanted to cure cancer even more than he wanted to understand it. As he would come to argue, “The three hundred and twenty-five thousand patients with cancer who are going to die this year cannot wait; nor is it necessary, in order to make great progress in the cure for cancer, for us to have the full solution of all the problems of basic research…the history of Medicine is replete with examples of cures obtained years, decades, and even centuries before the mechanism of action was understood for these cures.”
Few new bold projects are being funded now, writes Leaf, noting that in 2010, the N.C.I. used the bulk of its two billion dollars in research grants on existing projects. He is as incensed that the same institutions get most of the money, writing that “in 2011, the top 43 research centers got more funding ($12 billion) than did the bottom 2,574 institutions receiving any kind of NIH support.” To some, this is the price of science that is both sound and safe. To others, it is a culture of scientific inefficiency, an I.B.M. mindset in a field that desperately yearns for Apple.
Oncologists in the field with whom I spoke agreed with this overall assessment of the War on Cancer. Andrea Hayes-Jordan, a pediatric surgical oncologist at the M. D. Anderson Cancer Center in Houston, told me that “Our strategic attacks are improving, and we are winning some battles, but not the war yet.” Silvia Formenti, who chairs the radiation oncology department at New York University’s Langone Medical Center, was even more negative in her assessment of the War on Cancer. She wrote to me in an e-mail, “We have managed to make cancer a huge business, and a national ‘terror,’ but the progress in reducing mortality is quite questionable.”
The book suggests some remedies, foremost among them preventing cancer before it strikes. At Stage 0, a cancerous growth can be detected and removed before it has diversified and spread. By the time a tumor is the size of a grape, it has as many as a billion cells. Those cells become increasingly heterogeneous, and once they break through the basement membrane that acts as a final barrier between organs and tissues, they are free to metastasize throughout the body via the bloodstream or the lymphatic system.
The book finds great promise in the chemoprevention pioneered by Dartmouth researcher Michael Sporn, who wants to treat pre-invasive lesions as seriously as full-blown cancers. This seems to fly in the face of the cautious watch-and-wait philosophy popular with many oncologists, who have become convinced (not without reason) that the cure—toxic chemotherapy, high doses of radiation—could be worse than the disease.
However, other than the breast cancer drug tamoxifen and the H.P.V. vaccine—both of which can reduce the risk of getting cancer, not cure the disease—the promise of chemoprevention remains largely unrealized. A recent paper by two preventative oncologists concluded, “There have been numerous chemoprevention trials in the past 10 years, but the number of approved chemoprevention drugs is still quite small.” Another recent study on older men with prostate cancer suggested that “watchful waiting” was often the best route, noting that many patients opted for expensive treatments they didn’t need, thus leading to impotence and incontinence. And a federal task force ruled four years ago that women should delay getting mammograms until age fifty (ten years later than the previous recommendation) because of the procedure’s own potential dangers.
Leaf acknowledges these dangers, and also points out an even more serious problem with chemoprevention: biomarkers that would signal carcinogenesis in its earliest stages have not been found. So while he is correct to highlight the potential promise of a prophylactic approach, Leaf’s own description of “the failed biomarker hunt” is, indirectly, a defense of why oncologists today are left with no choice but to wait until the disease develops.
The desire for an accelerated approach to cancer has antecedents in the AIDS activism of the nineteen-eighties. As Mukherjee describes in his book, organizations like ACT UP “made the FDA out to be a woolly bureaucratic grandfather—exacting but maddeningly slow.” That had repercussions in cancer medicine, where patients also demanded quicker access to potentially life-saving therapies. Especially en vogue by the early nineties was “megadose chemotherapy” for breast cancer, complemented by a bone marrow transplant. (The original marrow would have been destroyed by the high toxicity of the purported cure.) Yet as Mukherjee notes, by early 2000, the procedure was discovered to have been supported by fictional studies. One of its main proponents, a South African oncologist named Werner Bezwoda, had charmed his fellow practitioners with astounding results that masked the true, fatal dangers of this excessive approach. Mukherjee calls Bezwoda’s influential drug trials “a fraud, an invention, a sham,” yet he was hardly the lone cheerleader for megadose chemotherapy. Any urge to hasten the War on Cancer—however justified that urge may be—must grapple with the risk of promising anecdotes curdling into hideous truths.
Of course, some approaches are neither terribly controversial nor difficult, at least from a medical standpoint: Debu Tripathy of the University of Southern California’s Norris Cancer Center told me that he believes that ninety per cent of all lung cancers could be eliminated through the cessation of cigarette smoking. Studies have shown a link between red meat consumption and an elevated risk of cancer. Here, then, may be cancer prevention in its simplest form.
On the whole, Leaf is much less optimistic than Mukherjee. Surveying the state of cancer medicine as it was in 2005, Mukherjee concludes, “The empire of cancer was still indubitably vast…but it was losing power, fraying at its borders.” Surveying some three thousand years of humanity’s battle with cancer, Mukherjee’s is the more meditative work. Leaf’s book is more urgent, more insistent—the voice of a frightened patient who yearns for a cure, rather than of the sober oncologist concerned with getting the science right. “Emperor” is a story; “Truth” is an argument.































































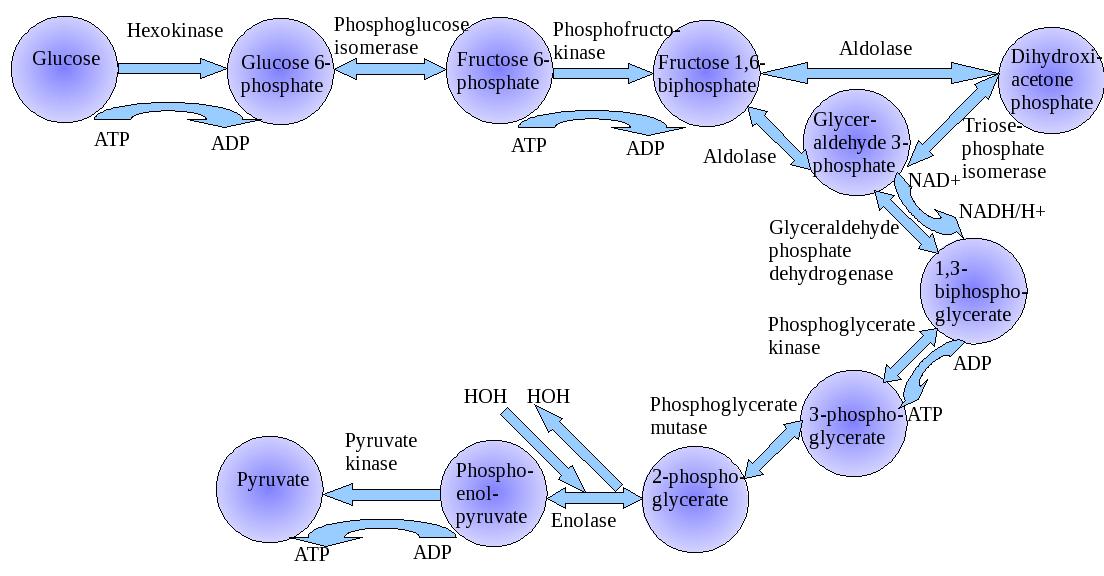{kind=link}