Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
We may not ever know’: Fauci says origin of coronavirus could remain a mystery
By Felice J. Freyer Globe Staff,Updated February 27, 2023, 6:31 p.m.
The pandemic’s true origin may never be uncovered, despite a new assessment favoring the lab leak theory from the US Department of Energy, said Dr. Anthony Fauci, former director of the National Institute of Allergy and Infectious Diseases, on Monday.
The energy department’s conclusion, first reported on Sunday by The Wall Street Journal, shows that there remains “a dichotomy of opinion” among experts but doesn’t firmly answer the question, Fauci said in an interview at the Globe’s first Health and Biotech Week event.
Based on new but undisclosed evidence, and with “low confidence,” the agency concluded the virus was probably leaked by accident from a laboratory in Wuhan, China. The FBI reached a similar conclusion in 2021, with “moderate confidence.”
But Fauci, stressing the importance of keeping “an open mind,” noted that four other intelligence agencies don’t buy the lab leak theory.
Meanwhile, evolutionary virologists have published two peer-reviewed articles showing biological evidence that “rather strongly suggests it was a natural occurrence,” he said. These virologists, using DNA evidence, demonstrated that the virus probably jumped from animals to people at a live-animal market in Wuhan.
Asked whether investigators will find a definitive answer, Fauci said, “We may not ever know.”
SOURCE
FBI Director Christopher Wray said the bureau’s assessment was that the COVID-19 virus “most likely” originated from a potential lab incident in Wuhan, China. (Fox News)
But there remains a dichotomy of opinion among experts and “we may not ever know” the origins of SARS-CoV-2, said Anthony Fauci, MD, former director of the National Institute of Allergy and Infectious Diseases, in an interview with the Boston Globe.
The body of evidence for 1 vaccine shot for people with prior Covid keeps mounting, here with the T cell response data and lack of added benefit of immune response with 2 shotshttps://t.co/0R8FPpLz34 Just out @ScienceTM
At 7:30 a.m. on 24 November, Kristian Andersen, an infectious disease researcher at Scripps Research, received a message on Slack: “This variant is completely insane.” Andrew Rambaut of the University of Edinburgh was reacting to a new SARS-CoV-2 genome sequence found in three samples collected in Botswana on 11 November and one picked up a week later in a traveler from South Africa to Hong Kong.
Andersen looked at the data and then replied: “Holy shit—that is quite something. The length of that branch …” A few minutes later he added: “Just had a look at the list of mutations—so nuts.”
They were talking about what is now called Omicron, a new variant of concern, and the long branch Andersen noticed refers to its distance to every other known virus on SARS-CoV-2’s evolutionary tree. The variant seemed to have picked up dozens of mutations, many of them known to be important in evading immunity or increasing transmissibility, with no intermediate sequences in the database of millions of viral genomes. On 23 November, after spotting the odd sequences in a global database, Tom Peacock, a virologist at Imperial College London, had already posted his own verdict on GitHub: “This could be of real concern.”
Now, once again, the world is watching as researchers work nights and weekends to learn what a new variant has in store for humanity. Is Omicron more infectious? More deadly? Is it better at reinfecting recovered people? How well does it evade vaccine-induced immunity? And where did it come from? Finding out will take time, warns Jeremy Farrar, head of the Wellcome Trust: “I’m afraid patience is crucial.”
Researchers in South Africa were already on the trail of this new variant. Several teams were independently trying to figure out why cases were spiking in Gauteng, a northern province that includes Johannesburg and Pretoria. And a private lab called Lancet had noticed that routine polymerase chain reaction (PCR) tests for SARS-CoV-2 were failing to detect a key target, the S gene, in many samples, a phenomenon previously seen with Alpha, another variant of concern. When Lancet sequenced eight of these viruses, they found out why: The genome was so heavily mutated that the test missed the gene.
Lancet shared the genomes with the Network for Genomics Surveillance in South Africa (NGS-SA), which called an urgent meeting on 23 November. “We were shocked by the number of mutations,” says Tulio de Oliveira, a virologist at the University of KwaZulu-Natal and NGS-SA’s principal investigator. After the meeting, de Oliveira says, he called South Africa’s director general of health and “asked him to inform the minister and president that a potential new variant was emerging.” The team sequenced another 100 randomly selected sequences from Gauteng in the next 24 hours. All showed the same pattern. After informing the government, de Oliveira and his colleagues presented their evidence at a press conference on the morning of 25 November. On 26 November, the World Health Organization (WHO) designated the virus a “variant of concern” and christened it Omicron. (Variant names follow the Greek alphabet but WHO skipped the letters Nu and Xi, it said, “because Nu is too easily confounded with ‘new’ and Xi was not used because it is a common surname.”)
One reason for concern about Omicron is that sequenced samples indicate it has rapidly replaced other variants in South Africa. But that picture might be skewed. For one, sequencing might have been focused on possible cases of the new variant in recent days, which could make it appear more frequent than it is. PCR data provide broader coverage and a less biased view, but there, too, samples with the S gene failure indicate a rapid rise of Omicron.
But the rising frequency could still be due in part to chance. In San Diego, a series of superspreading events at a university resulted in an explosion of one particular strain of SARS-CoV-2 earlier this year, Andersen says: “It was thousands of cases and they were all the same virus.” But the virus wasn’t notably more infectious. South Africa has seen relatively few cases recently, so a series of superspreading events could have led to the rapid increase of Omicron. “I suspect that a lot of that signal is explained by that and I desperately hope so,” Andersen says. Based on a comparison of different Omicron genomes, Andersen estimates the virus emerged sometime around late September or early October, which suggests it might be spreading more slowly than it appears to have.
The other reason to be concerned is Omicron’s confusing genome. Its spike protein, which latches on to cells on human receptors, has 30 amino acid differences from that of the original Wuhan, China, virus. In addition, amino acids have disappeared in three places and new ones appeared in one place. (Other proteins, too, have undergone changes.) Many of the changes in spike are around the receptor-binding domain, the part of the protein that makes contact with the human cell. “That is very troubling,” Farrar says. Structural biology mapping last year showed some of these changes made the virus bind to the receptor much better.
It’s hard to tell how infectious a virus is based on mutations alone, says Aris Katzourakis, an evolutionary biologist at the University of Oxford. “But if we were looking out for mutations that do affect transmissibility, it’s got all of them,” he says.
The sequence also suggests the virus could excel at evading human antibodies, says Jesse Bloom, an evolutionary biologist at the Fred Hutchinson Cancer Research Center. The human immune system produces a host of different antibodies that can neutralize SARS-CoV-2, but many of the most important ones fall into three categories that each target a slightly different site on the spike protein of the virus, simply called 1, 2, and 3. A mutation called E484K has long been worrying because it changes the shape of the site that class 2 antibodies recognize, making them less potent. Omicron carries a mutation called E484A in this site and similar changes in the sites for the other two classes of antibodies.
Bloom thinks people who recovered from COVID-19 or were vaccinated are unlikely to completely lose their ability to neutralize the virus. “But I would expect, based on this particular combination of mutations, that the drop in neutralization is larger than for all the other major variants.”
Experiments in the laboratory will have to show whether he is right. Alex Sigal, an infectious disease researcher at the Africa Health Research Institute, says he received swabs with Omicron on 24 November and has started to grow the virus. Producing enough of it to test against sera from vaccinated and recovered individuals will take a week or two, he says. Other researchers will test viruses genetically engineered to carry just the spike protein of Omicron, a process that is faster than growing the variant itself, but a bit further removed from what happens in real life.
As such studies take place, it’s crucial to closely monitor any shifts in the pandemic, Farrar says. “Do you see cases increasing not just in South Africa, but the broader South African region?” The virus has already been picked up in Belgium, the United Kingdom, and Israel, Farrar points out, and will probably be found elsewhere as well. “Do you see transmission increasing in other parts of the world around presumed index cases?” Epidemiologists will also watch for changes in disease severity—how many people are hospitalized and die. All that will take time.
In the meantime, the European Union, the United States, and many other countries have restricted travel to and from southern Africa in a bid to protect themselves. Travel restrictions are unlikely to stop the variant, Farrar says, but they can buy some time. “The question is what you then do with the time.”
Travel restrictions come with an economic and social cost, which could be a disincentive to report new variants. “I’ve heard through the grapevine that countries didn’t push sequences out very quickly [in the past] because they were worried about travel bans,” says Emma Hodcroft, a virologist at the University of Bern. “This is the opposite of what we want.”
Such considerations did not stop South African researchers, de Oliveira says. “We do risk a massive backlash in case [Omicron] does not cause a massive wave of infection and can be controlled,” he wrote in a message. “But this is a risk that I am comfortable to live with as the pandemic has caused so many deaths and suffering. [Our] hope is that our early identification will help the world.”
UPDATED on 11/8/2021
Low-dose mRNA-1273 COVID-19 vaccine generates durable memory enhanced by cross-reactive T cells
Low-dose messenger RNA (mRNA) vaccines potentially allow health providers to administer more doses from a limited vaccine supply and can be less reactogenic. Whether low-dose COVID-19 mRNA vaccines generate immune responses comparable to currently approved doses remains an open question, however. Mateus et al. report the results of a clinical trial comparing patients who received a 25-μg mRNA-1273 (Moderna) COVID-19 vaccine to 100-μg mRNA-1273 COVID-19 vaccinees and severe acute respiratory syndrome coronavirus 2–infected individuals. The low-dose Moderna vaccine generated long-lived T cell immunity that was equivalent between younger and older patients and that could be enhanced by the presence of cross-reactive T cells. Moreover, antibody and T cell responses induced by the low-dose vaccine were comparable to natural infection and about half as strong as those seen with high-dose vaccination. —STS
Structured Abstract
INTRODUCTION
Understanding human immune responses to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA vaccines is of interest for a panoply of reasons. mRNA vaccines have demonstrated impressive protection against COVID-19, but the durability of immunity has been a major unknown. Moreover, a better understanding of age-associated differences and mRNA vaccine dose response curves for dose sparing considerations is needed. Additionally, the impact of preexisting cross-reactive memory on immune responses to SARS-CoV-2 proteins remains an open question. Cross-reactive memory CD4+ T cells recognizing SARS-CoV-2 have been found in ~50% of individuals. A vaccine trial is a controlled context for testing the relevance of such cross-reactive T cells. Each of these topics was addressed in this study using blood samples from a National Institutes of Health clinical trial of 25-µg mRNA-1273 COVID-19 vaccinees as well as from 100-µg mRNA-1273 COVID-19 vaccinees and SARS-CoV-2–infected individuals.
RATIONALE
Vaccination and infection are two different paths to immunity. Comparison of vaccine-generated and infection-generated immune memory is of value. Given evidence that antibodies, CD4+ T cells, and CD8+ T cells can each participate in protective immunity against COVID-19, we measured acute and memory SARS-CoV-2 spike–specific antibodies, CD4+ T cells, and CD8+ T cells in the blood of subjects who received a low-dose (25 µg) or standard-dose (100 µg) mRNA-1273 COVID-19 vaccine. Immunological measurements were used to address the four issues described above: namely, the durability of immune memory over 7 months after vaccination, mRNA vaccine dose responses, age differences, and the impact of preexisting cross-reactive T cells.
RESULTS
Longitudinal samples from 35 volunteers immunized with 25 µg of mRNA-1273 on days 1 and 29 were used to measure SARS-CoV-2 spike–binding antibodies, receptor binding domain (RBD)–binding antibodies, SARS-CoV-2 pseudovirus (PSV) neutralizing antibodies, spike-specific CD4+ T cells, and spike-specific CD8+ T cells. Overall, substantial anti-spike, anti-RBD, and PSV neutralizing antibodies were induced in response to two 25-µg mRNA-1273 vaccinations, were maintained in 88 to 100% of vaccinees for at least 6 months after the second immunization, and were comparable in magnitude and quality to those observed 6 to 7 months after infection with SARS-CoV-2.
Spike-specific CD4+ T cells were generated by low-dose mRNA-1273 and were maintained as memory CD4+ T cells. We observed strong T follicular helper (TFH) and type 1 T helper cell polarization of these cells, which is advantageous for antiviral immunity. Spike-specific CD8+ T cells were detectable in 88% of vaccinees and maintained for at least 6 months in 67% of vaccinees. Spike-specific CD4+ or CD8+ T cell frequencies were not lower in older vaccinee groups than in 18- to 55-year-olds, either in the acute or memory phase. Thus, 25-µg mRNA-1273 vaccination induced spike antibody levels and memory T cell frequencies at 7 months after vaccination similar to those observed for COVID-19 cases 7 months after symptom onset.
Next, to assess the impact of mRNA dosing, we compared immune responses between 25-µg and 100-µg doses of mRNA-1273 vaccine. Peak anti-spike, anti-RBD, and PSV neutralizing antibody levels were about twofold higher in 100-µg vaccinees than in 25-µg vaccinees. Spike-specific CD4+ T cells responses were ~1.4-to-2.0-fold higher in 100-µg vaccinees, whereas peak CD8+ T cell responses were comparable between 25-µg and 100-µg dose regimens.
Finally, to address potential positive or negative effects of preexisting cross-reactive memory T cells, we compared 25-µg mRNA-1273 COVID-19 vaccine responses between subjects with or without measurable preexisting SARS-CoV-2 spike–reactive memory CD4+ T cells. Preexisting immunity enhanced vaccine antibody responses after a single vaccine dose, which was associated with higher spike-specific TFH cells and total spike-specific CD4+ T cell responses. Individuals with preexisting cross-reactive memory T cells also sustained higher SARS-CoV-2–neutralizing antibodies 6 months after vaccination.
CONCLUSION
The 25-µg dose of mRNA-1273 vaccine induces durable and functional T cell and antibody memory at comparable magnitude to natural infection. This work expands our understanding of immune memory to mRNA vaccine in humans, vaccine dose sparing, and possible timing of boosters. Finally, these data provide evidence that cross-reactive memory CD4+ T cells are biologically relevant and can exert a considerable positive influence on immunity generated by vaccination, with potential implications for vaccines and SARS-CoV-2 infections.
Response to low-dose mRNA-1273 vaccination over 7 months.
Immunological memory of antibodies, CD4+ T cells, and CD8+ T cells was examined after low-dose mRNA vaccination. Levels of spike-specific immune memory were then compared to immune memory observed after natural infection with SARS-CoV-2 or after full-dose vaccination. Robust immune memory comparable to natural infection but lower than after full-dose vaccination was observed. Increased vaccinee age correlated with reduced antibody levels but had no effect on cellular immune memory. Immune memory was enhanced by preexisting cross-reactive T cells. D1, day 1.
Vaccine-specific CD4+ T cell, CD8+ T cell, binding antibody, and neutralizing antibody responses to the 25-μg Moderna messenger RNA (mRNA)–1273 vaccine were examined over the course of 7 months after immunization, including in multiple age groups, with a particular interest in assessing whether preexisting cross-reactive T cell memory affects vaccine-generated immunity. Vaccine-generated spike-specific memory CD4+ T cells 6 months after the second dose of the vaccine were comparable in quantity and quality to COVID-19 cases, including the presence of T follicular helper cells and interferon-γ–expressing cells. Spike-specific CD8+ T cells were generated in 88% of subjects, with equivalent memory at 6 months post-boost compared with COVID-19 cases. Lastly, subjects with preexisting cross-reactive CD4+ T cell memory exhibited stronger CD4+ T cell and antibody responses to the vaccine, demonstrating the biological relevance of severe acute respiratory syndrome coronavirus 2–cross-reactive CD4+ T cells.
Understanding human immune responses to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA vaccines is of interest for a panoply of reasons. mRNA vaccines have demonstrated impressive protection against COVID-19 (1–7). The COVID-19 vaccine mRNA-1273, developed as a collaboration between Moderna and the National Institutes of Health Vaccine Research Center, encodes a stabilized SARS-CoV-2 full-length spike (8, 9). Durability of immunity has been, and remains, a major unknown for mRNA vaccines in humans. Encouraging reports from both Pfizer-BioNTech and Moderna indicate protective immunity of 91 and 93%, respectively, over the 6-month period after the second immunization (7 months after the first immunization) (10, 11), down modestly from the 95% maximal protection observed for each of those two vaccines within 1 to 2 months after the second immunization (1, 2). Although neutralizing antibodies are a clear correlate of immunity after two immunizations (12), the underlying mechanisms remain unclear. Moreover, those mechanisms of immunity may change as the immune response develops (e.g., after a single immunization) or as immune memory changes composition (13–15). Direct measurements of immune memory compartments in humans are necessary to provide insights into these important topics.
Infection and vaccination are two different paths to immunity. Comparison of vaccine-generated immune memory with immune memory of persons infected with SARS-CoV-2 is of value, as studies have indicated that natural immunity is 93 to 100% protective against symptomatic reinfection for 7 to 8 months (16–19), although natural immunity protection against certain variants of concern (VOCs) is likely to be lower (20). After SARS-CoV-2 infection, immunological memory has been observed for ≥8 months for CD4+ T cells, CD8+ T cells, memory B cells, and antibodies (21, 22). The immune memory in response to SARS-CoV-2 infection exhibits a relatively gradual decline that partially stabilizes within 1 year (23–26). The 100-μg mRNA-1273 vaccination has been shown to induce durable antibody responses (27), but it is unknown whether immune memory to the mRNA-1273 vaccine months after immunization is similar to or different than memory generated by SARS-CoV-2 infection. Additionally, both 25-μg- and 100-μg-dose mRNA-1273 vaccinations have been tested in clinical trials (9, 28), with 100-μg mRNA-1273 proceeding toward licensure (2, 29).
Preexisting cross-reactive memory CD4+ T cells that recognize SARS-CoV-2 have been found in ~50% of individuals pre-pandemic (30–37). There has been intense interest in understanding whether these preexisting cross-reactive memory CD4+ T cells, identified in vitro, are biologically relevant in vivo (33, 38, 39). One approach to test the relevance of such T cells in a controlled fashion is in the context of a vaccine trial, as individuals in a clinical trial are all exposed to a well-defined dose of antigen at a specific time. Additionally, exposure to a low antigen dose may be more sensitive to influence by cross-reactive memory. Thus, we examined immune responses to the 25-μg dose of the mRNA-1273 COVID-19 vaccine.
UPDATED on 9/8/2021
“..study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by #Delta#variant of #coronavirus, compared to the BNT162b2 two-dose #vaccine-induced #immunity.” https://buff.ly/3zjj15T Note; #vaccinating post-infection may provide additional protection; yet is this boost necessary, useful and long-lasting vs enhancement of protection after 2nd infection known from other endemics? #Epidemiology Pre-Covid19 Texbook knowledge stated those that show already a strong response against a challenge, i.e. vaccine, may NOT need an additional vaccination?! Thus, we could vaccinate the world insted of 10 rich counrties boosting everyone?!
Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections
Background Reports of waning vaccine-induced immunity against COVID-19 have begun to surface. With that, the comparable long-term protection conferred by previous infection with SARS-CoV-2 remains unclear.
Methods We conducted a retrospective observational study comparing three groups: (1)SARS-CoV-2-naïve individuals who received a two-dose regimen of the BioNTech/Pfizer mRNA BNT162b2 vaccine, (2)previously infected individuals who have not been vaccinated, and (3)previously infected and single dose vaccinated individuals. Three multivariate logistic regression models were applied. In all models we evaluated four outcomes: SARS-CoV-2 infection, symptomatic disease, COVID-19-related hospitalization and death. The follow-up period of June 1 to August 14, 2021, when the Delta variant was dominant in Israel.
Results SARS-CoV-2-naïve vaccinees had a 13.06-fold (95% CI, 8.08 to 21.11) increased risk for breakthrough infection with the Delta variant compared to those previously infected, when the first event (infection or vaccination) occurred during January and February of 2021. The increased risk was significant (P<0.001) for symptomatic disease as well. When allowing the infection to occur at any time before vaccination (from March 2020 to February 2021), evidence of waning natural immunity was demonstrated, though SARS-CoV-2 naïve vaccinees had a 5.96-fold (95% CI, 4.85 to 7.33) increased risk for breakthrough infection and a 7.13-fold (95% CI, 5.51 to 9.21) increased risk for symptomatic disease. SARS-CoV-2-naïve vaccinees were also at a greater risk for COVID-19-related-hospitalizations compared to those that were previously infected.
Conclusions This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity. Individuals who were both previously infected with SARS-CoV-2 and given a single dose of the vaccine gained additional protection against the Delta variant.
“Every state with a higher hospitalization rate than the country overall has a lower vaccination rate” “Every state with a higher vaccination rate than the country has a lower hospitalization rate” @WSJGraphics@karadapena@randyyeipWSJ@Brabbott42@jon_kamp
seem to assume half of cases are being diagnosed. That seems excessively high. I suspect case ascertainment is far lower; we have much more spread and are deeper into this epidemic wave than these models predict
Seems like a very confusing assumption. Through most of the pandemic pcr-confirmed infections have been assumed to be undercounts to the tune of 5x to 10x no?
On CNBC Gottlieb suggested that we are catching closer to 10% than 50% and thus there are 10x as many Delta infections. This is why he has suggested the Delta up wave will fall of in two or three weeks. He has been right most of the time. This call will be pretty easy to check.
All that matters, it seems, is that when the curve turns (as you’ve predicted) in the next 10-14 days they can laud their mitigating tactics which will probably have played a minimal role (if any) considering Delta’s already rampant spread.
10
UPDATED on 7/22/2021
UPDATED on 7/22/2021
Israel to become first in world to test Oravax oral COVID-19 vaccine
Oravax Medical is gearing up to commence clinical trials at Tel Aviv Sourasky Medical Center.
Israel is about to become the first country in the world to test the oral COVID-19 vaccine developed by Oramed Pharmaceuticals, the company’s CEO Nadav Kidron told The Jerusalem Post.
Oramed’s subsidiary, Oravax Medical, is gearing up to commence clinical trials of its vaccine at Sourasky Medical Center in Tel Aviv after receiving approval for its study protocol from the hospital’s Institutional Review Board. It is now waiting for approval from the Health Ministry, which is expected within a few weeks.
Oravax already completed GMP manufacturing in Europe of several thousand capsules that would be available for the Israeli trial and eventually in other countries.
In the U.S. the 7-day average of #Covid19 deaths is the lowest its been 𝐬𝐢𝐧𝐜𝐞 𝐌𝐚𝐫𝐜𝐡 𝟑𝟏, 𝟐𝟎𝟐𝟎! Vaccines really are amazing!
UPDATED on 4/13/2021
US recommends pausing Johnson & Johnson COVID-19 vaccine to investigate clotting reports
By Zeke Miller Associated Press,Updated April 13, 2021, 32 seconds ago
WASHINGTON (AP) — The U.S. is recommending a “pause” in using the single-dose Johnson & Johnson COVID-19 vaccine to investigate reports of potentially dangerous blood clots.
The Centers for Disease Control and Prevention and the Food and Drug Administration said Tuesday they were investigating unusual clots that occurred 6 to 13 days after vaccination. The clots occurred in veins that drain blood from the brain and occurred together with low platelets. All six cases were in women between the ages of 18 and 48; there was one death and all remained under investigation.
The reports appear similar to a rare, unusual type of clotting disorder that European authorities say is possibly linked to another COVID-19 vaccine not yet cleared in the U.S., from AstraZeneca.
Only about 9 million of the company’s doses have been delivered to states and are awaiting administration, according to CDC data.
Until now concern about the unusual blood clots has centered on the vaccine from AstraZeneca, which has not yet received authorization in the U.S. Last week, European regulators said they found a possible link between the shots and a very rare type of blood clot that occurs together with low blood platelets, one that seems to occur more in younger people.
The European Medicines Agency stressed that the benefits of receiving the vaccine outweigh the risks for most people. But several countries have imposed limits on who can receive the vaccine; Britain recommended that people under 30 be offered alternatives.
But the J&J and AstraZeneca vaccines are made with the same technology. Leading COVID-19 vaccines train the body to recognize the spike protein that coats the outer surface of the coronavirus. But the J&J and AstraZeneca vaccines use a cold virus, called an adenovirus, to carry the spike gene into the body. J&J uses a human adenovirus to create its vaccine while AstraZeneca uses a chimpanzee version.
The announcement hit U.S. stock markets immediately, with Dow futures falling almost 200 points just over two hours before the opening bell. Shares of J&J dropped almost 3%.
According to the team’s assessment, the three most notable changes to patient care in 2020 were:
1. Remote care was used more frequently by almost all patient groups.
As is to be expected, many patients were more likely to use virtual care during the pandemic than before it. This was true for patients who were Asian, Black, Hispanic, had private insurance coverage or had cardiovascular comorbidities such as hypertension or coronary artery disease.
2. Medications were prescribed less frequently.
“When comparing ordering practices between pre-COVID in-person, COVID-era in-person, COVID-era video, and COVID-era telephone visits, we found a decrease in the proportion of visits where at least one medication was ordered,” the authors wrote. “The proportion of visits where at least one medication was prescribed decreased from more than two-thirds of pre-COVID in-person visits to half of COVID-era in-person visits to only one-third of COVID-era video visits and one-quarter of COVID-era telephone visits.”
When COVID-19 daily numbers were down, the team added, it seemed that medications were often ordered more regularly.
3. Diagnostic tests were ordered less frequently.
Researchers observed the same trend when it came to ordering diagnostic and laboratory tests. Again, as it was with prescribing medications, daily COVID-19 numbers appeared to play a large role in this shift.
“It could be argued that the observed decreases in testing and prescribing were because clinicians were initially waiting for the COVID-19 pandemic to subside before advancing medical care,” the authors wrote. “Across all visits, we found that ordering practices appeared to change in association with the severity of the local COVID-19 case incidence, but we found that the differences between in-person, video, and telephone visits persisted across nearly every month of the nine-month period of study.”
The very rare brain blood cots—CVST—with the Astra Zeneca vaccine occur 50X more frequently than mRNA vaccines and are getting a lot of attention today, even before dueling press conferences of UK and EU regulators. Causality should not be in question.
Administering the AstraZeneca vaccine in Milan last month.Credit…Alessandro Grassani for The New York Times
Britain said on Wednesday that it would offer alternatives to the AstraZeneca vaccine for adults under 30 as European regulators described a “possible link” with rare blood clots, a setback for the world’s most widely used vaccine and a blow to the more than 100 countries relying on it to save lives amid a global surge in coronavirus cases.
The European regulator, the European Medicines Agency, stopped short of advising that use of the vaccine be curbed in the 27 European Union countries.
Until the announcement, Britain had never wavered in its use of the vaccine, making it a holdout in Europe even as many countries detected unusual, sometimes fatal, blood clots in some recipients. But evidence has mounted that very small numbers of Britons had also been afflicted, forcing the country to restrict a vaccine that is the backbone of its world-beating inoculation program.
The concern over the blood clots has threatened the pace of vaccinations far beyond Europe. At least 111 countries of varying income levels have administered doses of AstraZeneca’s shot, making it international aid groups’ most potent weapon in the battle to reduce deaths in the vaccine-starved global south.
British and European regulators both said it was possible that the clots were linked to the vaccine, but that more investigation was needed. European regulators described the cases as a serious but “very rare” side effect.
The agency reiterated that the overall benefits of the vaccine still outweighed the risks, but urged that health professionals and recipients of the shot be cautious about symptoms like shortness of breath, chest pain or leg swelling.
Most cases of rare blood clots were reported in women younger than 60 within two weeks of vaccination. But the regulator said that it had not concluded that age or gender were a specific risk and that it would further investigate the issue.
“This case clearly demonstrates one of the challenges posed by large scale vaccination campaigns,” Emer Cooke, the agency’s head, said in a news conference on Wednesday. “When millions of people receive these vaccines, very rare events can occur that were not identified during the clinical trials.”
No other vaccine has stirred as much controversy as the shot made by the British-Swedish company, setting off spats with the bloc over cuts in supply, its efficacy and finally over rare, but sometimes fatal, blood clots reported in some recipients.
Those concerns led several European countries to first restrict the use of AstraZeneca in older age groups, then suspend it over reports of blood clots, only to roll it out again last month after the European Medicines Agency issued a preliminary opinion that the benefits of the vaccine outweighed the risks.
As doctors reported a higher incidence of serious blood clots in younger people, some countries decided to stop administering the shot to anyone younger than 55.
Europe’s concerns over the vaccine’s side effects are also likely to threaten global inoculation efforts, with much of the developing world depending on the AstraZeneca vaccine to tackle the pandemic. The shot is the cornerstone of Covax, a program designed to make vaccine access more equitable worldwide.
The vaccine appeared to be causing an immune reaction in which antibodies bind to platelets, activating them, German doctors have said. Those platelets, in turn, were causing the formation of dangerous clots in certain parts of the body, including in veins that drain blood from the brain, leading in some cases to a rare type of stroke.
Why the antibodies develop in these people is not known, doctors have said. Some component of the vaccine, or excessive immune reaction — or both — could be the cause, they said.
No pre-existing conditions are known to make patients more vulnerable to this clotting disorder after a vaccination, European regulators said.
Confirmed US cases: 30,568,672 Confirmed US deaths: 553,517
DEATHS: Another 955 Americans died of COVID-19 yesterday, 29 percent lower than two weeks ago, according to The New York Times COVID-19 map and case count.
Deaths are rising in 6 states, Oklahoma, Missouri, Tennessee, Michigan, Utah, and Maine, as well as Washington, D.C.
INFECTIONS: New confirmed cases have now surpassed 75,000 per day. Yesterday, 77,718 more Americans were confirmed as infected, 20 percent more than two weeks ago and the most since Feb. 25.
The Times reports that over the past week, there has been an average of 65,574 new cases per day, 20 percent higher than two weeks ago.
In the past week, cases were higher in 33 states, D.C., Puerto Rico, and the Virgin Islands.
New infections have plateaued in 17 states, Guam, and the Northern Mariana Islands.
Cases are not declining anywhere in the United States.
The WHO team is expected to soon publish a 300-page final report on its investigation, after scrapping plans for an interim report on the origins of SARS-CoV-2 — the new coronavirus responsible for killing 2.7 million people globally
Doses administeredPct. of population Per 100 peopleTotalVaccinatedFully vaccinated
World
5.3
409,685,572
–
–
Israel
108
9,631,315
58%
50%
Seychelles
93
89,509
64%
28%
U.A.E.
72
6,980,466
–
–
Chile
43
8,117,316
29%
14%
U.K.
42
27,614,526
39%
2.8%
Maldives
41
212,711
–
–
Monaco
40
15,612
22%
19%
Bahrain
39
613,946
25%
14%
United States
35
115,730,008
23%
12%
Serbia
30
2,112,074
18%
12%
Malta
28
133,871
19%
8.6%
Antigua and Barbuda
25
24,164
–
–
San Marino
20
6,738
20%
–
Hungary
19
1,863,621
15%
4.3%
Show all
Note: Some countries do not provide data for the number of people who have been partially or fully vaccinated.
The data is compiled from government sources by the Our World in Data project at the University of Oxford. A vaccinated person refers to someone who has received at least one dose of a vaccine, and a fully vaccinated person has received all required doses of a vaccine. For the Pfizer-BioNTech vaccine, a person who is “fully vaccinated” has received two doses.
UPDATED on 2/22/2021
500,000 Death due to COVID-19 in the US. National Cathedral Bells are ringing 500 times.
President Biden’s chief medical advisor, Dr. Anthony Fauci, said the threshold of half a million deaths is like nothing “we have ever been through in the last 102 years, since the 1918 influenza pandemic.” U.S. deaths then were a cataclysmic 675,000, though dwarfed by a worldwide toll of some 50 million.
Mass. reports 29,959 new COVID-19 vaccinations, 26 deaths, 1,150 cases
By Martin Finucane Globe Staff,Updated February 22, 2021, 1 hour ago
The number of coronavirus vaccinations administered in Massachusetts rose by 29,959 to 1,443,848, state officials reported Monday.
The number of new vaccinations was smaller than on Sunday, when 40,983 were reported.
The total number of shots administered amounted to 85.5 percent of the 1,688,360 doses shipped to providers in the state so far, the Department of Public Health said.
The total shots administered included 1,044,210 first shots and 399,638 second shots. Those who have gotten their second shot of the currently approved two-dose vaccines are considered fully vaccinated.
Massachusetts is in the midst of a high-stakes campaign to vaccinate 4.1 million adults in an effort to bring an end to a pandemic that has sickened hundreds of thousands and caused more than 15,000 deaths in the state.
On Sunday, the US’ coronavirus death toll surpassed 500,000. While America makes up less than 5 percent of the world’s population, it accounts for more than 20 percent of the world’s deaths. Though the average number of new cases has gotten lower in recent weeks as more and more people are vaccinated, numbers are still higher than they were over the summer, and experts have reinforced that it’s important to keep pandemic precautions in place.
A leaked report by the Israeli health ministry and Pfizer indicates that vaccinations are stopping nine out of ten infections in the country. So far Israel has fully vaccinated 32 percent of its citizens using the Pfizer vaccine and has the world’s highest per capita rate of vaccinations. The study also claims that Israel could reach herd immunity by March. Outside experts caution that the report is far from conclusive, but it is certainly encouraging.
We’ve only ever eradicated one human disease—smallpox—so experts say it’s all but certain that Covid-19 is here to stay. Part of the reason diseases become endemic, or permanently present, is because people can’t get to all of the places these pathogens can shelter; in the case of Covid-19, these include bats, minks, and any humans who are unprotected. This reinforces the importance of distributing vaccines equitably worldwide to give the virus few hosts to live and mutate in.
Dr. Dan Barouch, head of the Center for Virology and Vaccine Research at Beth Israel Deaconess Medical Center., noted that the pandemic has evolved, affecting the efficacy of vaccine candidates.LANE TURNER/GLOBE STAFF
Johnson & Johnson asked the US government on Thursday to clear its one-shot coronavirus vaccine for emergency use, the first step in a regulatory process that could lead to the rollout of the third vaccine within a few weeks.
The giant health care company, which licensed technology pioneered by Beth Israel Deaconess Medical Center, has promised to deliver 100 million doses in the United States by the end of June. Because the vaccine can be administered in one shot ― unlike the other vaccines, which require two ― that would mean full coverage for 100 million people.
Dr. Paul Stoffels, Johnson & Johnson’s chief scientific officer, said in a statement that the emergency use application to the Food and Drug Administration is a “pivotal step toward reducing the burden of disease for people globally and putting an end to the pandemic.”
Johnson & Johnson filed the application six days after the New Brunswick, N.J.-based firm announced encouraging results from its late-stage global clinical trial on 43,783 volunteers. The data showed that a single shot prevented 66 percent of moderate and severe cases globally, and 72 percent in the United States.
The FDA will now assemble a packet of material, including data from the trial, that will be scrutinized by a panel of outside experts in a public hearing. A member of the advisory panel, Dr. Eric Rubin, an immunologist at the Harvard T.H. Chan School of Public Health, said he expects the committee will consider the application within two weeks. If the committee recommends authorization, the FDA is likely to act swiftly.
Dr. Anthony Fauci, President Biden’s top medical adviser on the pandemic, said in a tweet Thursday that if the FDA agrees with the committee, the vaccine “could be available in March.”
The 66 percent global effectiveness rate for the one-shot vaccine fell significantly short of the performances of the two-shot vaccines from Pfizer-BioNTech and Moderna that the FDA cleared for emergency use in December. Those vaccines prevented more than 90 percent of coronavirus cases in large trials, a remarkable showing considering that they were the first to successfully use new technology called synthetic messenger RNA.
But Dr. Dan Barouch, who runs the Center for Virology and Vaccine Research at Beth Israel, which developed different technology for the vaccine, said the pandemic has evolved, with the emergence of more resistant variants, in particular a worrisome South African strain that was detected in the United States for the first time last week.
Several vaccine experts agreed and highlighted a particularly encouraging finding in Johnson & Johnson’s announcement last week: The one-shot vaccine was highly protective against the worst cases of COVID-19. Worldwide, the shot prevented 85 percent of severe cases, and none of the vaccinated people needed hospitalization or died from COVID-19.
Fauci acknowledged last week that public health officials will likely face a “messaging challenge” to persuade people to take a vaccine that prevented 66 percent of symptomatic cases compared with roughly 95 percent.
But, he said, “If you can prevent severe disease in a high percentage of individuals [as the Johnson & Johnson vaccine did], that will alleviate so much of the stress and human suffering and death.”
He and other officials also said the Pfizer and Moderna vaccines would likely get lower efficacy results now, given the emergence of the South African strain, which appears to be more resistant to immunization.
A U.K. hospital network has become one of the first worldwide to use a digital ledger technology, similar to the one that underpins several cryptocurrencies, to track the handling of COVID-19 vaccines.
South Warwickshire NHS Foundation Trust, which is part of the government-run National Health Service and administers four hospitals in central England, has begun using the Hedera Hashgraph system to keep track of whether COVID-19 vaccines are being stored at the correct temperatures, Hedera and Everyware, a U.K. software company that is overseeing the project, said Tuesday.
The hospitals include one in Stratford-upon-Avon, the city best known for being Shakespeare’s birthplace and hometown.
In recent weeks a number of tech companies, including IBM, have proposed using blockchain technology, which is a kind of digital ledger that is maintained across a network, rather than stored in one central location, as a way to ensure data on coronavirus vaccine doses is both secure and can be shared easily across organizations that normally use different record-keeping systems. But South Warwickshire’s use of Hedera is thought to be one of the first implementations of this kind of technology for tracking vaccine handling.
Accurately tracking the status and handling of vaccine doses is particularly crucial because the inoculations produced by Pfizer and Moderna must be kept at ultralow temperatures of –70 degrees Celsius (–94 Fahrenheit) until close to the time they are to be used, while the vaccine from AstraZeneca must be kept at normal refrigerator temperatures.
Everyware has already worked with South Warwickshire to track the handling of some chemotherapy drugs, blood supplies, and ophthalmology drops that must also be kept at specific temperatures. It has done so by using Internet-connected sensors that it places in a room or within a hospital refrigerator. Doing so has helped the hospital reduce cases in which medicines had to be discarded because staff were uncertain they had been maintained at the correct temperature, Tom Screen, Everyware’s technical director, told Fortune.
“This way, we can verify the data hasn’t changed from start to finish; that the data has been in our custody and the data is valid. And we can say the analytics that you might want to run on top of this is valid,” he said.
Everyware chose the Hedera Hashgraph blockchain because it offers a very low fixed cost per piece of information added to the blockchain—just 1/100th of a U.S. penny—and can quickly handle millions of data entries, Screen said.
In contrast, many cryptocurrency-based blockchains can handle no more than one or two dozen transactions per second, and are many times more expensive, with a cost that varies as the value of the related cryptocurrency moves up and down owing to market forces.
Hedera’s Hashgraph digital ledger does not use the same kind of blockchain that Bitcoin and Ethereum do. Instead it uses a different kind of mathematical system, called a directed acyclic graph (or DAG). One benefit of this system is that it does not require nodes in the network that stores the digital ledger to solve complex mathematical puzzles as in cryptocurrency-based blockchains, which is why Hedera can offer such a low cost per piece of information added to the ledger and can process transactions so quickly.
Full-dose blood thinners decreased need for life support and improved outcome in hospitalized COVID-19 patients
In large clinical trial conducted worldwide, full dose anti-coagulation (blood thinner) treatments given to moderately ill patients hospitalized for COVID-19 reduced the requirement of vital organ support—such as the need for ventilation. A trend in possible reduction of mortality was also observed and is being further studied. With large numbers of COVID-19 patients requiring hospitalization, these outcomes could also help reduce the overload on intensive care units around the world.
Early in the pandemic, physicians around the world observed increased rates of blood clots and inflammation among COVID-19 patients which affected multiple organs and led to complications such as lung failure, heart attack and stroke. Whether providing increased doses of blood thinners routinely administered to hospitalized patients would be safe and effective was unknown at that time.
Three clinical trial platforms spanning five continents in more than 300 hospitals have been working together to test whether there is a greater benefit of full doses of heparin (blood thinners) to treat moderately ill hospitalized adults with COVID-19 compared to the lower heparin dose typically administered to prevent blood clots in hospitalized patients. Moderately ill patients are those not in intensive care and who did not receive organ support such as mechanical ventilation at trial enrollment.
Based on the interim results of more than 1,000 moderately ill patients admitted to hospital, findings showed that full doses of blood thinners, in addition to being safe, were superior to the doses normally given to prevent blood clots in hospitalized patients—with regard to the primary endpoint which is the need for ventilation or other organ supportive interventions. The trial investigators are now working as fast as possible to make the full results of the study available so clinicians can make informed decisions about treating their COVID-19 patients.
As is normal for clinical trials, these trials are overseen by independent boards that routinely review the data and are composed of experts in ethics, biostatistics, clinical trials, and blood clotting disorders. Informed by the deliberations of these oversight boards, all the trial sites have stopped enrollment.
However, research questions remain about how to further improve the clinical care of COVID-19 patients. This adaptive protocol has been designed to allow different drugs to be started, stopped or combined during the study in response to emerging scientific data. This approach enables the rapid testing of additional agents without compromising safety and the study will evolve accordingly.
The trial results reported today complement the group’s findings announced in December that routine use of full-dose anti-coagulation when started in the ICU in critically ill COVID-19 patients was not beneficial and may have been harmful in some patients.
The three international trials include: the Randomized, Embedded, Multi-factorial Adaptive Platform Trial for Community-Acquired Pneumonia (REMAP-CAP(link is external)) Therapeutic Anticoagulation; Accelerating COVID-19 Therapeutic Interventions and Vaccines-4 (ACTIV-4) Antithrombotics Inpatient; and Antithrombotic Therapy to Ameliorate Complications of COVID-19 (ATTACC). The trials, which span four continents have the common goal of assessing the benefit of full doses of blood thinners to treat moderately ill or critically ill adults hospitalized for COVID-19, compared to a lower dose often used to prevent blood clots in hospitalized patients. To meet the challenge of this pandemic, investigators worldwide joined forces to answer this question as rapidly as possible. In the United States, the ACTIV-4 trial is being led by a collaborative effort with several universities, including the University of Pittsburgh and New York University, New York City.
The trials are supported by multiple international funding organizations including Canadian Institutes of Health Research (CAN), the National Institutes of Health’s National Heart, Lung, and Blood Institute (US), the Translational Breast Cancer Research Consortium and the University of Pittsburgh Medical Center Learning While Doing Program (US), the LifeArc Foundation, National Institutes of Health Research (UK), National Health and Medical Research Council (AUS), Minderoo Foundation (AUS), and the PREPARE and RECOVER consortia (EU).
About the National Heart, Lung, and Blood Institute (NHLBI): NHLBI is the global leader in conducting and supporting research in heart, lung, and blood diseases and sleep disorders that advances scientific knowledge, improves public health, and saves lives. For more information, visit www.nhlbi.nih.gov.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
Total tests completed: 2,313,909(14,532 newly reported tests since yesterday)
Maine:
530 deaths (up 11 from yesterday)
34,963 confirmed and probable cases (up 701 from yesterday)
New Hampshire
950 deaths (up 17 from Jan. 18)
59,437 confirmed cases (up 1,573 from Jan. 18)
Vermont:
165 deaths (up 2 from yesterday)
10,471 confirmed cases (up 124 from yesterday)
Connecticut:
6,726 deaths (up 44 from yesterday)
234,134 confirmed and probable cases (up 1,915 from yesterday)
*Increases each day are calculated from the time this newsletter was sent the previous day.
Amid ongoing pandemic, Biden sworn in as president: President Biden was sworn in today as the 46th president of the United States, taking over as the country continues to battle against a pandemic that has killed more than 400,000 people nationwide. In his inaugural address, Biden said we are entering “what may well be the toughest and deadliest period of the virus. We must set aside the politics and finally face this pandemic as one nation.”
SARS-CoV-2-induced hypercytokinemia and inflammation are critically associated with COVID-19 severity. Baricitinib, a clinically approved JAK1/JAK2 inhibitor, is currently being investigated in COVID-19 clinical trials. Here, we investigated the immunologic and virologic efficacy of baricitinib in a rhesus macaque model of SARS-CoV-2 infection. Viral shedding measured from nasal and throat swabs, bronchoalveolar lavages, and tissues was not reduced with baricitinib. Type I interferon (IFN) antiviral responses and SARS-CoV-2-specific T cell responses remained similar between the two groups. Animals treated with baricitinib showed reduced inflammation, decreased lung infiltration of inflammatory cells, reduced NETosis activity, and more limited lung pathology. Importantly, baricitinib-treated animals had a rapid and remarkably potent suppression of lung macrophage production of cytokines and chemokines responsible for inflammation and neutrophil recruitment. These data support a beneficial role for, and elucidate the immunological mechanisms underlying, the use of baricitinib as a frontline treatment for inflammation induced by SARS-CoV-2 infection.
Experts disagree on one-dose vaccine, report spotlights British mutation
While the outgoing deputy director-general of the Health Ministry suggested limiting coronavirus vaccines to one dose per person, other experts were not sold on the idea.
*Increases each day are calculated from the time this newsletter was sent the previous day.
Vaccines are on the horizon, but most college students and workers are at the back of the line to get them: College students have been among the most frequently tested in Massachusetts for COVID, but they may be among the last to get vaccinated against the illness.
Bill Gates isn’t about to be contemplating his touchdown dance yet. You don’t get to devote your life to battling the world’s most intractable problems by declaring victory before a fight is over. But in a letter Gates released this morning, headlined, “These breakthroughs will make 2021 better than 2020,” it’s clear that the co-chair of the Bill and Melinda Gates Foundation is feeling pretty sanguine about the year ahead—particularly when it comes to COVID-19.
The Gates letter, which comes a month before the expected January release of the foundation’s official Annual Letter, sees a lot to be optimistic about in the recent course of the pandemic—as well as a number of things to remain wary about. Clearly, Gates takes heart in the recent emergency use authorization of both the Moderna and Pfizer-BioNTech vaccines, as well as by the straightforward and decidedly lower-tech truth that face masks and distancing remain exceedingly effective in slowing the spread of the virus as the vaccines are being rolled out.
“When I think back on the pace of scientific advances in 2020, I am stunned,” he writes. “Humans have never made more progress on any disease in a year than the world did on COVID-19 this year.”
The Gates Foundation itself can take some credit for that breakneck pace, having been funding research on the mRNA technology that underlies both the Moderna and Pfizer-BioNTech vaccines since 2014. Not only is the technique effective, it makes for an easier-to-produce vaccine, since the mRNA shot causes the body itself to produce the spike protein that elicits an antibody reaction, rather than taking the time and making the effort to manufacture it in a lab.
The following video for Dr. John Campbell explains the latest information of the new COVID-19 variant which is spreading rapidly in the UK and has been identified in many major European Union countries. Some highlights of the video include:
New variant, VUI-202012/01 is a mutation (N501Y) in the spike protein
this new mutant displays stronger transmission than previous forms of COVID19
no real data on the virulence
variant is defined by a set of 17 mutations, of which N501Y in spike protein is most common
70% more infections, increasing R value to 0.4 (R of 1.0 means not infectious)
as of 12/20/2020 60% of new cases in London are this new mutant
As of November 2020, there are reportedly 55 million people worldwide who have been infected by COVID-19, with over 1.3 million succumbing to the deadly disease. In this episode, we speak with Dr. Neville Berkman, the head of a new clinic at Hadassah Hospital Ein Kerem, specifically designed for recovered COVID-19 patients who are experiencing post-COVID complications. Find out about the state of the virus in Israel, a vaccine update and when he thinks we will be living in a COVID-free world.
The state’s seven-day positive test rate remained relatively stable at 6.0 percent for the week. (Shutterstock)
BOSTON, MA — Nearly one full week after Massachusetts took a step back in reopening — closing some industries, reducing capacity on many others and ordering stricter enforcement of indoor dining protocols — the state’s positive test average has stabilized at about 6 percent.
The state reported 3,995 new cases on Saturday — down from several recent days when the new case count was more than 5,000 — and an average positive test rate at 6.01 over the past seven days.
The seven-day positive test average as of Friday was 6.13 percent.
The seven-day positive rate average was at 3.3 on Nov. 21, rose quickly in the days after Thanksgiving before peaking at 6.2 as the majority of cities and towns in the Commonwealth moved into the state’s “high risk” category for community spread, and has stabilized over the past two weeks.
The daily report shows that of the 81,282 estimated active cases across the state, 12,482 of them are among those between 20 and 29 years old, with 10,413 cases among those in the second most prevalent age group of 30 to 39 years old.
Saturday’s report did include an increase in hospitalizations from 1,874 to 1,927. There were 383 people in intensive care statewide.
This week’s storm has contributed to varying numbers of tests being reported per day. While positive cases were down from 5,632 on Friday, the number of tests reported was also down to 80,214 from 106,034 on Friday.
Officials said up to 6 million doses of the two-shot vaccine could be shipped in the next couple of days to mostly hospitals and nursing homes across the country.
FDA Takes Additional Action in Fight Against COVID-19 By Issuing Emergency Use Authorization for Second COVID-19 Vaccine
Action Follows Thorough Evaluation of Available Safety, Effectiveness, and Manufacturing Quality Information by FDA Career Scientists, Input from Independent Experts
Today, the U.S. Food and Drug Administration issued an emergency use authorization (EUA) for the second vaccine for the prevention of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The emergency use authorization allows the Moderna COVID-19 Vaccine to be distributed in the U.S. for use in individuals 18 years of age and older.
“With the availability of two vaccines now for the prevention of COVID-19, the FDA has taken another crucial step in the fight against this global pandemic that is causing vast numbers of hospitalizations and deaths in the United States each day,” said FDA Commissioner Stephen M. Hahn, M.D. “Through the FDA’s open and transparent scientific review process, two COVID-19 vaccines have been authorized in an expedited timeframe while adhering to the rigorous standards for safety, effectiveness, and manufacturing quality needed to support emergency use authorization that the American people have come to expect from the FDA. These standards and our review process, which are the same we have used in reviewing the first COVID-19 vaccine and intend to use for any other COVID-19 vaccines, included input from independent scientific and public health experts as well as a thorough analysis of the data by the agency’s career staff.”
The FDA has determined that the Moderna COVID-19 Vaccine has met the statutory criteria for issuance of an EUA. The totality of the available data provides clear evidence that the Moderna COVID-19 Vaccine may be effective in preventing COVID-19. The data also show that the known and potential benefits outweigh the known and potential risks—supporting the company’s request for the vaccine’s use in people 18 years of age and older. In making this determination, the FDA can assure the public and medical community that it has conducted a thorough evaluation of the available safety, effectiveness, and manufacturing quality information.
The Moderna COVID-19 Vaccine contains messenger RNA (mRNA), which is genetic material. The vaccine contains a small piece of the SARS-CoV-2 virus’s mRNA that instructs cells in the body to make the virus’s distinctive “spike” protein. After a person receives this vaccine, their body produces copies of the spike protein, which does not cause disease, but triggers the immune system to learn to react defensively, producing an immune response against SARS-CoV-2.
“Guided by science and data, the agency’s career staff determined that the vaccine’s known and potential benefits clearly outweigh its known and potential risks, and although not an FDA approval, the FDA’s expectations described in our June and October guidance documents have been met,” said Peter Marks, M.D., Ph.D., Director of the FDA’s Center for Biologics Evaluation and Research. “Today’s authorization demonstrates our steadfast commitment to the health of the American people, with the assurance that our scientific standards and the integrity of our review process have been maintained. This achievement is yet another testament to the dedication of FDA’s career scientists and physicians, who have been working urgently to conduct comprehensive and rigorous evaluations of the data submitted for vaccines to prevent COVID-19.”
FDA Evaluation of Available Safety Data
Moderna COVID-19 Vaccine is administered as a series of two doses, one month apart. The available safety data to support the EUA include an analysis of 30,351 participants enrolled in an ongoing randomized, placebo-controlled study conducted in the U.S. These participants, 15,185 of whom received the vaccine and 15,166 of whom received saline placebo, were followed for a median of more than two months after receiving the second dose. The most commonly reported side effects, which typically lasted several days, were pain at the injection site, tiredness, headache, muscle pain, chills, joint pain, swollen lymph nodes in the same arm as the injection, nausea and vomiting, and fever. Of note, more people experienced these side effects after the second dose than after the first dose, so it is important for vaccination providers and recipients to expect that there may be some side effects after either dose, but even more so after the second dose. It is mandatory for ModernaTX, Inc. and vaccination providers to report the following to the Vaccine Adverse Event Reporting System (VAERS) for Moderna COVID-19 Vaccine: all vaccine administration errors, serious adverse events, cases of Multisystem Inflammatory Syndrome (MIS), and cases of COVID-19 that result in hospitalization or death.
FDA Evaluation of Available Effectiveness Data
The effectiveness data to support the EUA include an analysis of 28,207 participants in the ongoing randomized, placebo-controlled U.S. study who did not have evidence of SARS-CoV-2 infection prior to the first dose of vaccine. Among these participants, 14,134 received the vaccine and 14,073 received placebo. The vaccine was 94.1% effective in preventing COVID-19 disease among these clinical trial participants with 11 cases of COVID-19 in the vaccine group and 185 in the placebo group. At the time of the analysis of these 196 COVID-19 cases, none in the vaccine group and 30 in the placebo group were classified as severe. After the analysis of these 196 cases was completed, one severe case in the vaccine group was identified and is awaiting confirmation. At this time, data are not available to determine how long the vaccine will provide protection, nor is there evidence that the vaccine prevents transmission of SARS-CoV-2 from person to person.
Statement from NIH and BARDA on the FDA Emergency Use Authorization of the Moderna COVID-19 Vaccine
Today, the U.S. Food and Drug Administration issued an Emergency Use Authorization (EUA) to Moderna, Inc., a biotechnology company based in Cambridge, Massachusetts, for its COVID-19 vaccine, which was co-developed with scientists at the National Institutes of Health’s National Institute of Allergy and Infectious Diseases (NIAID). This innovative and monumental partnership has enabled NIH and Moderna to develop a safe and effective COVID-19 vaccine within the span of a year that will be manufactured and distributed across the U.S. The vaccine, called mRNA-1273, is a messenger RNA (mRNA) vaccine against COVID-19 encoding a prefusion stabilized form of the spike protein of SARS-CoV-2, co-developed by investigators from Moderna and NIAID’s Vaccine Research Center. The approach to stabilize the coronavirus spike protein, called S-2P, was developed by NIAID scientists and their collaborators at Scripps Research, Dartmouth College and the University of Texas at Austin. NIAID supported the early development of the mRNA-1273 vaccine, and worked with Biomedical Advanced Research and Development Authority (BARDA) scientists to support the mid- and late-stages of clinical development, with BARDA leading government support of the scale-up of manufacturing and regulatory pathway to EUA. The mRNA-1273 vaccine is the second COVID-19 vaccine in the United States to be granted an EUA. NIH Director Francis S. Collins, M.D., Ph.D., NIAID Director Anthony S. Fauci, M.D., and BARDA Director Gary Disbrow, Ph.D. released the following statements:
“It has been less than a year since the world first learned of SARS-CoV-2 and the terrible disease it can cause. To have not one but two safe and highly effective COVID-19 vaccines ready for deployment to the American public is truly a remarkable scientific achievement, and a significant step toward ending the pandemic that has caused so much suffering. The partnership to develop the mRNA-1273 vaccine is a prime example of the tremendous good that can be accomplished when the public and private sectors work together to address a serious public health problem. It is through the dedicated efforts of our federal scientists and their collaborators at Moderna and in academia, the clinical staff who conducted the vaccine’s rigorous clinical trials, and the tens of thousands of study participants who selflessly rolled up their sleeves, that another safe and highly effective vaccine to protect against COVID-19 will soon be rolled out to the American public.” – NIH Director Francis S. Collins, M.D., Ph.D.
“Several years before SARS-CoV-2 entered the public consciousness, NIAID scientists were working with Moderna to develop vaccines for other coronaviruses. That existing scientific foundation is what enabled both partners to move quickly to develop the mRNA-1273 vaccine candidate against the novel SARS-CoV-2 coronavirus. NIAID conducted the initial Phase 1 testing of the vaccine and, with the support of BARDA and other Operation Warp Speed partners, played a central role in its large-scale clinical trial. Throughout each stage of clinical testing, the Moderna vaccine proved to be safe and highly effective at preventing symptomatic COVID-19. In a study of more than 30,000 people, it demonstrated 94% efficacy, and subsequent analyses have revealed that the vaccine induces a durable immune response. There is much we still do not know about SARS-CoV-2 and COVID-19. However, we do know that this vaccine is safe and can prevent symptomatic COVID-19 and severe disease. It is my hope that all Americans will protect themselves by getting vaccinated when the vaccine becomes available to them. That is how our country will begin to heal and move forward. ” – NIAID Director Anthony S. Fauci, M.D.
“Today stands as a reminder of what can be accomplished when people come together to reach a common goal. We are working with a constant sense of urgency to bring vaccines, therapeutics and diagnostics to bear to end the crisis. As partners in Operation Warp Speed, NIAID and BARDA scientists collaborated with Moderna, adding BARDA’s expertise in late-stage clinical trials, scale-up manufacturing and regulatory requirements. By collaborating, we were able to complete these steps in parallel and accelerate the development of a safe and effective vaccine. While we celebrate today’s accomplishment, we recognize that there is still much work to do to ensure every American who wants a COVID-19 vaccine receives one. Every American has been touched in some way by this virus, and so we will continue to push forward. With continued collaboration and investment in scientific research, health security, and innovative public-private partnerships, we can achieve a safer, more prepared world.” – BARDA Director Gary Disbrow, Ph.D.
Francis Collins, M.D., is Director of the National Institutes of Health in Bethesda, Maryland.
Anthony S. Fauci, M.D., is Director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health.
Gary Disbrow, Ph.D., is Director of the Biomedical Advanced Research and Development Authority (BARDA), in the HHS Office of the Assistant Secretary for Preparedness and Response.
Federal officials gave an update Monday morning on the progress of shipments of Pfizer’s and BioNTech’s COVID-19 vaccine, saying that 145 shipments would be delivered by 2:00 PM local time around the United States.
Gen. Gustave Perna, the chief operating officer of the federal government’s Operation Warp Speed program, said personnel had worked all weekend to get the vaccine packed and shipped from Pfizer’s manufacturing site in Kalamazoo, Michigan, to states’ designated receiving sites in order that vaccinations may begin Monday.
“It went incredibly well,” Perna told reporters during a press briefing.
As of 1:00 PM on Monday, 55 shipments had been received. The remaining 95 were due to be delivered by 2:00 PM local time, Perna said.
Shipments will continue each day. It is planned that a total of 636 shipments will be delivered through Wednesday. “The shipments for tomorrow’s deliveries have already been packed and checked,” he said.
Another 581 shipments will go to states starting on Thursday and continuing through the weekend, Perna said.
By Sunday, the federal government expects to have delivered a total of 2.9 million doses of the vaccine to the states, Washington, DC, and US territories. Operation Warp Speed is holding an additional 2.9 million doses for the booster that’s due to be given 21 days later to the initial recipients, and it’s keeping 500,000 doses in reserve for contingencies.
The Post’s coronavirus coverage linked in this newsletter is free to access from this email.
The latest
The number of coronavirus cases in the United States passed 11 million on Sunday. It took 100 days for the nation to log its first 1 million cases; it took just six days to get from 10 million to 11 million.
The number of people being hospitalized with covid-19 is also higher. Fearing that the worsening crisis will lead to even more preventable deaths, the governors of several states implemented new restrictions to help slow the spread. The residents of North Dakota are now required to wear masks. Colleges, high schools, workplaces and in-person dining are closing for three weeks in Michigan. Indoor social gatherings with people outside one’s household are now prohibited in Washington, along with indoor dining at restaurants and bars.
The governors of Michigan and Washington appealed to the federal government to step in with more help for struggling businesses in light of the new restrictions. In response, White House coronavirus adviser Scott Atlas urged people to reject their states’ public health guidelines. “The only way this stops is if people rise up,” Atlas said in a tweet Sunday night.
A wide array of groups from the retail, tourism and hospitality industries are trying to battle new restrictions to preserve their ability to continue to operate. At the same time, some major retailers are buckling down with precautions that echo those they took early in the pandemic. Kroger has temporarily reverted to limiting purchases on items such as hand sanitizer, toilet paper and disinfecting wipes. Walmart stores are metering customers by only allowing a certain number inside at a time.
Moderna announced Monday that a preliminary analysis shows its experimental coronavirus vaccine is nearly 95 percent effective at preventing illness, including severe cases. The news comes a week after Pfizer and its German partner BioNTech said their candidate was 90 percent effective. U.S. leaders and health experts cheered the news, but — with wide distribution still months away — called for Americans to double down on measures to prevent the spread.
Joe Biden may have won the presidency pledging a national mask mandate and a science-based approach to controlling the pandemic, but Republicans made substantial gains in down-ballot races in the upper Midwest. Analysts say it’s likely because of their anti-restriction approach, and now GOP leaders are using it to claim a mandate for their style of pandemic management. Public health officials warn it could have disastrous consequences in the winter. Meanwhile, Biden urged President Trump to allow officials to work with the incoming administration on developing a coordinated response to the pandemic, warning that “more people may die if we don’t.”
2. Three different positivity rates that Massachusetts highlights in its daily dashboard
The lowest line on the chart is the positivity rate for testing at higher education institutions. In college testing programs, asymptomatic people can be tested repeatedly, which results in a low positivity rate. The line above it shows the rate of positive tests among all tests administered. And the top line shows the rate of positive tests when the higher education testing is removed.
4. Traces of COVID-19 found in waste water at the Massachusetts Water Resources Authority’s plant on Deer Island
The waste water is being tested for copies of the virus as part of a pilot project. The hope is to pick up early signals of future rises in infections. Results are broken down by northern and southern sections of the MWRA system.
A look into a possible future
This chart shows the University of Massachusetts’ weekly ensemble model of where the pandemic could go next for Massachusetts. Researchers at the lab combine numerous models to glean their collective wisdom and project the future several weeks ahead, in this case up to Dec. 5.
King Center on Global Development @Stanford University
We are a Stanford University research center working to improve the lives of the world’s poor.
By catalyzing Stanford’s distinctive strengths in global poverty and development research, the Stanford King Center on Global Development is working collaboratively and purposefully to turn path-breaking research into real-world results.
Since June 2020, 214 human cases of COVID-19 have been identified in Denmark with SARS-CoV-2 variants associated with farmed minks, including 12 cases with a unique variant, reported on 5 November. All 12 cases were identified in September 2020 in North Jutland, Denmark. The cases ranged in age from 7 to 79 years, and eight had a link to the mink farming industry and four cases were from the local community.
Initial observations suggest that the clinical presentation, severity and transmission among those infected are similar to that of other circulating SARS-CoV-2 viruses. However, this variant, referred to as the “cluster 5” variant, had a combination of mutations, or changes that have not been previously observed. The implications of the identified changes in this variant are not yet well understood. Preliminary findings indicate that this particular mink-associated variant identified in both minks and the 12 human cases has moderately decreased sensitivity to neutralizing antibodies. Further scientific and laboratory-based studies are required to verify preliminary findings reported and to understand any potential implications of this finding in terms of diagnostics, therapeutics and vaccines in development. In the meantime, actions are being taken by Danish authorities to limit the further spread of this variant of the virus among mink and human populations.
SARS-CoV-2, the virus which causes COVID-19, was first identified in humans in December 2019. As of 6 November, it has affected more than 48 million people causing over 1.2 million deaths worldwide. Although the virus is believed to be ancestrally linked to bats, the virus origin and intermediate host(s) of SARS-CoV-2 have not yet been identified.
Available evidence suggests that the virus is predominantly transmitted between people through respiratory droplets and close contact, but there are also examples of transmission between humans and animals. Several animals that have been in contact with infected humans, such as minks, dogs, domestic cats, lions and tigers, have tested positive for SARS-CoV-2.
Minks were infected following exposure from infected humans. Minks can act as a reservoir of SARS-CoV-2, passing the virus between them, and pose a risk for virus spill-over from mink to humans. People can then transmit this virus within the human population. Additionally, spill-back (human to mink transmission) can occur. It remains a concern when any animal virus spills in to the human population, or when an animal population could contribute to amplifying and spreading a virus affecting humans. As viruses move between human and animal populations, genetic modifications in the virus can occur. These changes can be identified through whole genome sequencing, and when found, experiments can study the possible implications of these changes on the disease in humans.
To date, six countries, namely Denmark, the Netherlands, Spain, Sweden, Italy and the United States of America have reported SARS-CoV-2 in farmed minks to the World Organisation for Animal Health (OIE).
Please watch VIDEO from Dr. John Campbell
Dr. Campbell discusses this finding in detail.
UPDATED ON 10/26/2020
Oct. 26, 2020
What you need to know today
Worldwide and nationwide (per Johns Hopkins University)
Worldwide confirmed cases: 43,374,127 (up 487,664 from yesterday*)
Worldwide deaths:1,157,284 (up 4,961 from yesterday*)
Worldwide recoveries: 29,039,929 (up 185,808 from yesterday*)
US confirmed cases: 8,687,289 (up 60,015 from yesterday*)
US deaths: 225,580 (up 383 from yesterday*)
Countries/regions affected thus far: 189
Massachusetts:
9,657 deaths among confirmed cases (up 17 from yesterday)
148,336 confirmed cases (up 1,216 from yesterday)
Total tests
Molecular (PCR): 2,652,248 (20,086 newly reported tests since yesterday)
Antigen: 174,754 (490 newly reported tests since yesterday)
Antibody: 125,973 (144 newly reported tests since yesterday)
Total tests completed: 1,067,142 (32,570 newly reported tests since Friday)
Maine:
146 deaths (up 0 from yesterday)
6,254 confirmed and probable cases (up 53 from yesterday)
Total tests completed: 587,950 (up 14,320 from Friday)
New Hampshire (as of Oct. 25)
473 deaths (up 0 from Oct. 24)
10,328 confirmed cases (up 90 from Oct. 24)
Vermont:
58 deaths (up 0 from yesterday)
2,083 confirmed cases (up 10 from yesterday)
Connecticut:
4,589 deaths (up 12 from Friday)
68,099 confirmed and probable cases (up 2,047 from Friday)
*Increases each day are calculated from the time this newsletter was sent the previous day.
The source of half of Massachusetts’ COVID-19 cases is unknown: How is the coronavirus spreading? In some cases, Massachusetts health officials have been able to contact trace and connect infections to a source. But in about half of cases, state health officials have been unable to determine the source of the infection, making it more difficult to control the spread of the virus. “For a disease like COVID, where superspreading is so important [to] prevent, not identifying the sources of infection means we’re risking not identifying superspreading events fast enough,” Dr. Sam Scarpino, an epidemiologist at Northeastern University, wrote in an e-mail.
Why are people worried about another coronavirus surge in Mass.? These charts show the answers: Experts are worried that based on the data we’re seeing from state health officials and others, Massachusetts is heading into a second surge of the coronavirus. The five charts featured in this story — based on wastewater, confirmed statewide and national coronavirus case counts, positivity rates, and hospitalizations — explain why that concern is growing.
Trump falsely calls spike in coronavirus cases a ‘fake news media conspiracy’: President Trump tweeted this morning that the latest spike in coronavirus cases nationwide is nothing more than a “fake news media conspiracy,” complaining that journalists are focusing so much on the virus ahead of the election. Trump wrongly stated that the only reason cases are rising is because testing is increasing, despite experts saying that doesn’t fully explain the rise in cases.
Calls for nationwide mask-wearing mandate grow: Dr. Scott Gottlieb, former commissioner of the Food and Drug Administration, has joined a growing chorus of public health experts who say a mask-wearing mandate could curb the spread of the coronavirus. Dr. Anthony Fauci, the nation’s top infectious disease expert, has said the same. Gottlieb wrote about the issue Sunday in the Wall Street Journal. The piece was ominously headlined: “Winter Is Coming: Time for a Mask Mandate.”
Around the region:
Massachusetts will send texts to residents in 22 high-risk coronavirus communities tonight to urge people to follow virus-related precautions.
Breast Cancer: Early Detection, Higher Risks and the Effect of COVID-19
Episode 37: Listen Now
Professor Beatrice Uziely, is the head of Oncology and Ambulatory Services at Hadassah’s Sharett Institute of Oncology, a center which serves both the population of greater Jerusalem and as a referral center for cancer patients for all over Israel and abroad. She graduated from the Hebrew University of Jerusalem with a degree in biology and graduated with a medical degree from Hebrew University-Hadassah Medical School.
After beginning her career at Hadassah, she went on to do a fellowship at the University of Southern California Norris Cancer Center before returning to Jerusalem where she has become one of the most renowned medical oncologists in Jerusalem. Her key areas of clinical interest include the connection between hormonal genetic expressions in tumors and their reaction to treatment. Invasiveness of tumors, clinical research in hormonal and chemical treatments, finding genetic markers in order to diagnose their grade and much more.
She has co-authored over 60 scientific papers and is a member of the Israel Medical Association, the Israel Society of Clinical Oncology, the American Society of Clinical Oncology and the European Society for Medical Oncology.
Dr. Paluch-Shimon is a medical oncologist with a Masters in Epidemiology from the London School of Hygiene & Tropical Medicine. She is director of the Breast Oncology Program at Hadassah University Hospital in Jerusalem, which includes a dedicated service for the care and treatment of young women with breast cancer. Dr Paluch-Shimon was the first to establish dedicated services for young women in Israel. Her key areas of clinical interest and research are breast cancer in young women, BRCA-associated breast cancer, triple negative breast cancer and neo-adjuvant therapies.
She has co-authored over 50 scientific papers and has authored ESO-ESMO international guidelines on breast cancer in young women, the ESMO clinical practice guidelines on screening and prevention of cancer in individuals with a hereditary breast and ovarian cancer syndrome. She is a member of the ESO-ESMO international consensus panel for the management of advanced breast cancer and a member of the European consensus panel on genetic testing in advanced breast cancer.
Dr. Paluch-Shimon is the subject editor for Breast Cancer for the ESMO clinical practice guidelines committee. Dr. Paluch-Shimon is currently a member of the ESMO Breast Faculty, a core faculty member in the European School of Oncology and co-chair of the European School of Oncology’s Breast Cancer in Young Women Conference. She is a graduate of the Talpiot physician leadership program (Sheba). She was a member of the Israeli Ministry of Health committee evaluating the national breast cancer screening policy and is a member of the Israeli National Cancer Council.
A panel of UC Berkeley biologists explores diverse approaches to understanding the SARS-CoV2 virus, including its ecology and evolution, mechanisms of infection, and potential therapeutic targets. Jeffery Cox, Faculty Director, Center for Emerging and Infectious Diseases, moderator Bio: http://cend.globalhealth.berkeley.edu… Diana Bautista, Professor of Cell and Developmental Biology Bio: https://mcb.berkeley.edu/faculty/cdb/… Mike Boots, Professor of Integrative Biology Bio: https://ib.berkeley.edu/people/facult… James Hurley, Professor of Biochemistry, Biophysics, and Structural Biology Bio: https://mcb.berkeley.edu/faculty/bbs/…
A panel of UC Berkeley biologists explores diverse approaches to understanding the SARS-CoV2 virus, including its ecology and evolution, mechanisms of infection, and potential therapeutic targets. Jeffery Cox, Faculty Director, Center for Emerging and Infectious Diseases, moderator Bio: http://cend.globalhealth.berkeley.edu… Diana Bautista, Professor of Cell and Developmental Biology Bio: https://mcb.berkeley.edu/faculty/cdb/… Mike Boots, Professor of Integrative Biology Bio: https://ib.berkeley.edu/people/facult… James Hurley, Professor of Biochemistry, Biophysics, and Structural Biology Bio: https://mcb.berkeley.edu/faculty/bbs/…
Subject: Lower-risk COVID-19 communities can move to next step of reopening, Baker says
Citation of a Tweet by Scott Gottlieb, MD
@ScottGottliebMD
As reported Covid cases continue to rise around the U.S., the number of Covid hospitalizations – which is an important, objective measure of total disease burden – have stopped their decline, and may be starting to increase again.
The path to a rapid, proven and widely available coronavirus vaccine will not be straightforward. There are now more than 300 experimental products, according to the World Health Organization: roughly 40 are being tested on humans, and only nine of those have reached the final stage before possible implementation: phase 3 trials.
Drug companies will be expected to hit a series of milestones before they are allowed to distribute a Covid-19 vaccine, a move experts say makes it unlikely one will be approved before the US election in November.
Wealthy countries representing just 13 per cent of the world’s population have bought more than half of the leading vaccine candidates’ promised doses, according to Oxfam, the charity.
The US government’s Biomedical Advanced Research and Development Authority is the biggest spender on vaccines, having distributed more than $10bn in funding for vaccine candidates, either via direct financing or through vaccine procurement agreements.
On a per-capita basis, the UK has built the largest and most diversified vaccine portfolio, according to data from Deutsche Bank, having pre-ordered more than five doses per citizen spread across six leading vaccine candidates. The UK is followed closely by the US, Canada and Japan.
Johnson & Johnson became the first leading pharmaceuticals company to test a single-dose Covid-19 vaccine with the launch this week of a phase 3 trial that will recruit 60,000 participants across three continents.
London is to host the world’s first Covid-19 human challenge trials — in which healthy volunteers are deliberately infected with coronavirus to assess the effectiveness of experimental vaccines. The UK government-funded studies are expected to begin in January at a secure quarantine facility in east London, according to several people involved in the project.
Colorized scanning electron micrograph of a cell (blue) heavily infected with SARS-CoV-2 virus particles (red), isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. Credit: NIAID
The novel coronavirus uses structures within its RNA to infect cells. Scientists have now identified these configurations, generating the most comprehensive atlas to date of SARS-CoV-2’s genome.
Although contained in a long, noodle-like molecule, the new coronavirus’s genome looks nothing like wet spaghetti. Instead, it folds into stems, coils, and cloverleafs that evoke molecular origami.
A team led by RNA scientist Anna Marie Pyle has now made the most comprehensive map to date of these genomic structures. In two preprints posted in July 2020 to bioRxiv.org, Pyle’s team mapped structures across the entire RNA genome of the coronavirus SARS-CoV-2, using living cells and computational analyses.
SARS-CoV-2 relies on its unique RNA structures to infect people and cause the illness COVID-19. But these structures’ contribution to infection and disease is often underappreciated, even among scientists, says Pyle, a Howard Hughes Medical Institute Investigator at Yale University.
“The general wisdom is that if we just focus on the proteins encoded in the virus’s genome, we’ll understand how SARS-CoV-2 works,” Pyle says. “But for these types of viruses, RNA structures in the genome can influence their ability to function as much as encoded proteins.”
Researchers can now begin to tease out just how these structures aid the virus—information that could ultimately lead to new treatments for COVID-19. Once scientists have identified RNA structures that carry out key tasks, for instance, it may be possible to devise ways to disrupt them—and interfere with infection.
More bang for the buck
Both DNA and its molecular relative RNA store information using a four-letter code. Within human cells, pairs of letters can form bonds spanning two strands of DNA. These strands twist together, forming the familiar double helix. RNA can form helices too, but in viruses such as SARS-CoV-2 and its relatives, it does so when a single molecule folds back on itself.
The result is not only stem-like double helices, but also three- and four-stranded structures, knot-like regions, and multi-stem junctions. Like building blocks, these simple configurations become the basis for even more complex architecture within the genome.
Nearly the entire California Senate Republican caucus was placed under mandatory quarantine this week after a coronavirus-skeptical member tested positive the virus.
This curated post shows the timeline from when the FDA announced clinical trails on convalescent therapy back in April up to their announcement of approval in August as well as some controversies surrounding the announcement of approval of this therapy for COVID19.
UPDATED ON 8/22/2020
Do-it-yourself coronavirus testing sparks kudos, and caution
By Kay Lazar Globe Staff,Updated August 22, 2020, 1 hour ago
Health care workers prepared a COVID-19 test sample before a person self-administered a test at the COVID-19 drive-through testing center at Miami-Dade County Auditorium in Miami.DAVID SANTIAGO/ASSOCIATED PRESS
Leading public health experts, frustrated with chronic delays in coronavirus testing, are on a mission to persuade federal regulators to authorize cheap, at-home tests that would deliver results in minutes and could help the country turn the corner on the pandemic.
The campaign comes as the US Food and Drug Administration recently adopted guidelines aimed at ensuring accurate results for do-it-yourself COVID-19 tests. While several companies have developed home test kits and are pushing to get them on the market, these scientists say the new thresholds are so strict that few home test kits will be able to meet them.
In pressing the FDA, these scientists argue that fast, frequent coronavirus tests, taken daily or several times a week, can be crucial to reopening schools and businesses — and keeping them open. The tests, they say, would catch silent carriers who do not show symptoms but can potentially spread the virus widely.
Dr. Anthony Fauci, Director of NIAID, addresses the AOA’s 100th House of Delegates
5,793 views
Jul 18, 2020
UPDATED ON 8/13/2020
Clinical trials of monoclonal antibodies to prevent COVID-19 now enrolling
Reporter: Stephen J. Williams, PhD
Image of an antibody binding to the surface of a virus, blocking entry into a human cell.Lisa Donohue, CoVPN
Two Phase 3, randomized, placebo-controlled, double-blind clinical trials testing whether experimental monoclonal antibodies (mAbs) can prevent infection by SARS-CoV-2 coronavirus are now enrolling healthy adults at clinical trial sites in the United States. Many of the trial sites and study investigators are part of the COVID-19 Prevention Network(link is external) (CoVPN), recently established by the National Institute of Allergy and Infectious Diseases (NIAID), one of the National Institutes of Health. SARS-CoV-2 is the virus that causes coronavirus disease 2019 (COVID-19). The trials are enrolling adults who are at risk of infection due to close contact at work or home to persons with SARS-CoV-2 infection.
“The COVID-19 Prevention Network is designed to conduct large-scale trials rapidly and efficiently,” said NIAID Director Anthony S. Fauci, M.D. “This network will allow us to test the safety and efficacy of monoclonal antibodies and other preventive measures to help identify how best to reduce the level of SARS-CoV-2 infection and ultimately end the COVID-19 pandemic.”
Monoclonal antibodies(link is external) are laboratory-made versions of proteins naturally produced by the immune system in response to invading viruses or other pathogens. Neutralizing antibodies, whether natural or monoclonal, can bind directly to portions of viruses that they use to attach to and enter cells, preventing them from initiating the infection cycle. Monoclonal antibodies may provide short-term protection from SARS-CoV-2 and could serve as important components of the COVID-19 pandemic response until vaccines become available.
One trial is being conducted jointly by NIAID and trial sponsor Regeneron Pharmaceuticals of Tarrytown, New York. It will evaluate Regeneron’s investigational double mAb combination, REGN-COV-2, which is designed to bind to two points on the SARS-CoV-2 spike protein and prevent it from entering healthy cells. The trial will enroll approximately 2,000 asymptomatic adults who are household contacts of persons with SARS-CoV-2 infection. Participants must have been in close contact (typically due to residing at the same address) with the infected person in a 96-hour window preceding administration of either REGN-CoV-2 or placebo. In addition to assessing safety, the trial will seek to define whether REGN-COV-2 can prevent infection or disease symptoms in those already infected. The efficacy assessment will be a one-month period following administration of REGN-COV-2 or placebo. All trial participants will be followed for safety for seven months after efficacy assessment period ends.
A second trial, sponsored by Eli Lilly and Company of Indianapolis, Indiana, and implemented in collaboration with NIAID, will evaluate LY-CoV555, a mAb isolated from a recovered COVID-19 patient by scientists at AbCellera (Vancouver, British Columbia, Canada) and the NIAID Vaccine Research Center, and developed by Eli Lilly and Company. This trial will assess whether LY-CoV555 can prevent SARS-CoV-2 infection among people at high risk of exposure due to residing or working in skilled nursing or assisted living facilities. Within one week of identification of a case of SARS-CoV-2 infection at a facility, study investigators will enroll trial volunteers and evaluate the prevention efficacy and safety of LY-CoV555, compared to placebo, over an 8-week period. The trial will also evaluate efficacy in preventing symptoms of a given severity in those already infected. Participants will continue to be followed for safety for an additional 16 weeks. Up to 2,400 participants will be randomized to receive intravenous infusion of either LY-CoV555 or placebo.
Additional information about this trial is available at clinicaltrials.gov using the identifier NCT04497987. Clinical investigators, hospitals or clinical sites interested in participating in one of Lilly’s clinical trials for a potential COVID-19 treatment, should call 1-877-CT-LILLY (1-877-285-4559) or email covid19potentialsite@lilly.com(link sends e-mail).
NIAID conducts and supports research—at NIH, throughout the United States, and worldwide—to study the causes of infectious and immune-mediated diseases, and to develop better means of preventing, diagnosing and treating these illnesses. News releases, fact sheets and other NIAID-related materials are available on the NIAID website.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
The death toll due to the coronavirus grew by 14 Sunday, the state reported, bringing the total confirmed dead in Massachusetts to 8,514. Confirmed cases of the disease also grew by 286, and reached a total of 112,459.
Rhode Island (as of Aug. 7):
1,014 deaths (not updated on weekends)
19,738 confirmed cases (not updated on weekends)
Total tests completed: 395,798(not updated on weekends)
Maine:
125 deaths (up 0 from yesterday*)
4,042 cases (up 16 from yesterday*)
Total tests completed: 188,569(up 2,585 from yesterday*)
New Hampshire (as of Aug. 8)
419 deaths (up 0 from Aug. 7*)
6,818 confirmed cases (up 39 from Aug. 7*)
Vermont:
58 deaths (up 0 from yesterday*)
1,459 confirmed cases (up 5 from yesterday*)
Connecticut (as of Aug. 7):
4,441 deaths (not updated on weekends)
50,320 confirmed and probable cases (not updated on weekends)
*Increases each day are calculated from the time this newsletter was sent the previous day.
Eric J. Rubin, Lindsey R. Baden, Arnold Epstein, and Stephen Morrissey
The editors are joined by health policy expert Arnold Epstein to talk about the collateral impact of Covid-19 on the care of patients with other diseases and on the U.S. health care system itself. Listen to the interview.
Subject: | 08.05.20 | J&J inks $10-per-dose vaccine supply deal; NIH to test Eli Lilly’s antibody
UPDATED ON 8/5/2020
Dr. Anthony Fauci, the nation’s top infectious disease specialist, will answer questions from Harvard Chan faculty and other COVID-19 experts, going narrow and deep on questions about the pandemic that you won’t hear anywhere else. This conversation will be moderated by Dr. Sanjay Gupta, Chief Medical Correspondent for CNN.
“When Public Health Means Business” is a multi-part series that virtually convenes luminaries from the realms of finance, industry and health to map a new path forward and ensure a better, safer future for all. Jointly presented by the Harvard T.H. Chan School of Public Health and the New England Journal of Medicine, and hosted by The Forum at the Harvard T.H. Chan School of Public Health.
The virtual Technion Board of Governors Meeting starts soon!
Meet brilliant researchers in their labs who are battling COVID-19, including Professor Naama Geva-Zatorsky, who is working on a coronavirus home test kit, and Professor Ido Kaminer, who discovered that ultraviolet light can inactivate virus particles. Enjoy a live panel discussion featuring students, and a closing address by Nobel Laureate Aaron Ciechanover.
Anthony Fauci Explains Why the US Still Hasn’t Beaten Covid
The director of NIAID talks about vaccines, school reopenings, hostility toward science, and the lessons we’ll learn when (yes, when) we recover.
Why do you think the US has done so poorly in suppressing this pandemic compared with other rich countries?
It isn’t just one single factor. Let me give you one or two that I think are important. First of all, other countries, certainly Asian countries, and certainly the European Union, when they so-called locked down—shut down, shelter in place, whatever you want to call it—they did it to about 95 percent of their countries. So they did it in full force. Some countries got hit badly, but once they locked down and turned things around, they came down to a very low baseline—down to tens or hundreds of new cases a day, not thousands. They came down and they stayed down.
Now, in the United States, when we shut down, even though it was a stress and a strain for a lot of people, we only did it to the tune of about 50 percent of the country shutting down. Our curve goes up and starts to come down. But we never came down to a reasonable baseline. We came down to about 20,000 new infections per day, and we stayed at that level for several weeks in a row. Then we started to open up—getting America “back to normal”—and started to see the cases go from 20,000 a day to 30,000, 40,000. We even hit that one point last week of 70,000 new cases a day.
So when you’re starting off with a baseline that already is very high, and then you try to open your country, and instead of listening carefully and adhering to the guidelines, some states—and I’m not going to name them—skipped over some of the checkpoints. They didn’t adhere to the guidelines, which essentially suggested a very measured, prudent way of opening step by step. In other states, the governors and mayors did it right. But in some—all you needed to do was take a look at some of the films. You see people congregating in crowds at bars with no masks on. We didn’t shut down fully, the baseline never came down to a real low level. And when we started to open up, we didn’t open up uniformly in a very strict way.
Some people have suggested that Americans can’t work together to stop a pandemic because they’re too selfish. Do you buy that?
I don’t want to be pejorative in blaming Americans. I don’t think they’re deliberately doing it. I don’t think they fully realize, and here’s why I say this: The infections taking place now, in the last few weeks, are much more disproportionately among young people. In fact, the average age of people that have gotten infected is about a decade, or a decade and a half, younger than what we saw in earlier months of the outbreak. A substantial proportion of the people who get infected—20 to 45 percent—don’t have any symptoms at all. Many of those are very young people, millennials, the people who are out there at the bars. So they look around and say, “The chance of my getting sick from this virus is much, much, much lower than an elderly person, or than somebody with an underlying condition. So I’m just gonna do what I want. If I get infected, I’ll take my chances.” The only thing about that inadvertent and maybe innocent misjudgment is that we’re starting to see that more and more young people do have serious outcomes from infection.
But what they don’t realize is that, even if they don’t get any symptoms at all, by being careless and allowing themselves to get infected, they are becoming a part of the propagation of the outbreak. They are putting other people in danger by themselves getting infected. That’s the message we have to get across: You’ve got to have some social responsibility.
It seems that there’s a hostility towards science and evidence-based thinking. How much does that worry you?
It does. Obviously, there is a bit of an anti-science trend in the United States, a pushing back on authority telling you what to do. Sometimes, in a good vein, that could be the independent spirit of the American people. That is part of our character. But on the other hand, it can work against you. And when you push back on someone telling you what to do, and you mix that with a trend of anti-authority, anti-science, then you get into trouble. Then you get into the situation we find ourselves now, where people are not acting in a way that is safeguarding their health.
LONDON, July 20 (Reuters) – AstraZeneca’s experimental COVID-19 vaccine was safe and produced an immune response in early-stage clinical trials in healthy volunteers, data showed on Monday.
The vaccine, called AZD1222 and under development by AstraZeneca and scientists at Britain’s Oxford University, did not prompt any serious side effects and elicited antibody and T-cell immune responses, according to trial results published in The Lancet medical journal.
From Lancet Editors:
An Article published in The Lancet finds promising early results on a safe COVID-19 vaccine, causing few side effects. Preliminary results from the phase 1/2 trial involving 1,077 healthy adults found that the vaccine, ChAdOx1, induced strong antibody and T cell immune responses up to day 56 of the ongoing trial. Responses may be even greater after a second dose, according to a sub-group study of 10 participants. The authors say that further clinical studies should be done with this vaccine. The current results focus on the immune response measured in the laboratory, and further testing is needed to confirm whether the vaccine effectively protects against COVID-19 infection.
Pedro M Folegatti*, Katie J Ewer*, Parvinder K Aley, Brian Angus, Stephan Becker, Sandra Belij-Rammerstorfer, Duncan Bellamy, Sagida Bibi, Mustapha Bittaye, Elizabeth A Clutterbuck, Christina Dold, Saul N Faust, Adam Finn, Amy L Flaxman, Bassam Hallis, Paul Heath, Daniel Jenkin, Rajeka Lazarus, Rebecca Makinson, Angela M Minassian, Katrina M Pollock, Maheshi Ramasamy, Hannah Robinson, Matthew Snape, Richard Tarrant, Merryn Voysey, Catherine Green*, Alexander D Douglas*, Adrian V S Hill*, Teresa Lambe*, Sarah C Gilbert*, Andrew J Pollard*, on behalf of the Oxford COVID Vaccine Trial Group†
Summary Background The pandemic of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) might be curtailed by vaccination. We assessed the safety, reactogenicity, and immunogenicity of a viral vectored coronavirus vaccine that expresses the spike protein of SARS-CoV-2.
Methods We did a phase 1/2, single-blind, randomised controlled trial in five trial sites in the UK of a chimpanzee adenovirus-vectored vaccine (ChAdOx1 nCoV-19) expressing the SARS-CoV-2 spike protein compared with a meningococcal conjugate vaccine (MenACWY) as control. Healthy adults aged 18–55 years with no history of laboratory confirmed SARS-CoV-2 infection or of COVID-19-like symptoms were randomly assigned (1:1) to receive ChAdOx1 nCoV-19 at a dose of 5×10¹⁰ viral particles or MenACWY as a single intramuscular injection. A protocol amendment in two of the five sites allowed prophylactic paracetamol to be administered before vaccination. Ten participants assigned to a non-randomised, unblinded ChAdOx1 nCoV-19 prime-boost group received a two-dose schedule, with the booster vaccine administered 28 days after the first dose. Humoral responses at baseline and following vaccination were assessed using a standardised total IgG ELISA against trimeric SARS-CoV-2 spike protein, a muliplexed immunoassay, three live SARS-CoV-2 neutralisation assays (a 50% plaque reduction neutralisation assay [PRNT50]; a microneutralisation assay [MNA50, MNA80, and MNA90]; and Marburg VN), and a pseudovirus neutralisation assay. Cellular responses were assessed using an ex-vivo interferon-γ enzyme-linked immunospot assay. The co-primary outcomes are to assess efficacy, as measured by cases of symptomatic virologically confirmed COVID-19, and safety, as measured by the occurrence of serious adverse events. Analyses were done by group allocation in participants who received the vaccine. Safety was assessed over 28 days after vaccination. Here, we report the preliminary findings on safety, reactogenicity, and cellular and humoral immune responses. The study is ongoing, and was registered at ISRCTN, 15281137, and ClinicalTrials.gov, NCT04324606.
Findings Between April 23 and May 21, 2020, 1077 participants were enrolled and assigned to receive either ChAdOx1 nCoV-19 (n=543) or MenACWY (n=534), ten of whom were enrolled in the non-randomised ChAdOx1 nCoV-19 prime-boost group. Local and systemic reactions were more common in the ChAdOx1 nCoV-19 group and many were reduced by use of prophylactic paracetamol, including pain, feeling feverish, chills, muscle ache, headache, and malaise (all p<0·05). There were no serious adverse events related to ChAdOx1 nCoV-19. In the ChAdOx1 nCoV-19 group, spike-specific T-cell responses peaked on day 14 (median 856 spot-forming cells per million peripheral blood mononuclear cells, IQR 493–1802; n=43). Anti-spike IgG responses rose by day 28 (median 157 ELISA units [EU], 96–317; n=127), and were boosted following a second dose (639 EU, 360–792; n=10). Neutralising antibody responses against SARS-CoV-2 were detected in 32 (91%) of 35 participants after a single dose when measured in MNA80 and in 35 (100%) participants when measured in PRNT50. After a booster dose, all participants had neutralising activity (nine of nine in MNA80 at day 42 and ten of ten in Marburg VN on day 56). Neutralising antibody responses correlated strongly with antibody levels measured by ELISA (R²=0·67 by Marburg VN; p<0·001).
Interpretation ChAdOx1 nCoV-19 showed an acceptable safety profile, and homologous boosting increased antibody responses. These results, together with the induction of both humoral and cellular immune responses, support largescale evaluation of this candidate vaccine in an ongoing phase 3 programme.
Also From Lancet: Note that this is another adenoviral based vaccine but from the China group
Summary Background This is the first randomised controlled trial for assessment of the immunogenicity and safety of a candidate non-replicating adenovirus type-5 (Ad5)-vectored COVID-19 vaccine, aiming to determine an appropriate dose of the candidate vaccine for an efficacy study.
Methods This randomised, double-blind, placebo-controlled, phase 2 trial of the Ad5-vectored COVID-19 vaccine was done in a single centre in Wuhan, China. Healthy adults aged 18 years or older, who were HIV-negative and previous severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection-free, were eligible to participate and were randomly assigned to receive the vaccine at a dose of 1×10¹¹ viral particles per mL or 5×10¹⁰ viral particles per mL, or placebo. Investigators allocated participants at a ratio of 2:1:1 to receive a single injection intramuscularly in the arm. The randomisation list (block size 4) was generated by an independent statistician. Participants, investigators, and staff undertaking laboratory analyses were masked to group allocation. The primary endpoints for immunogenicity were the geometric mean titres (GMTs) of specific ELISA antibody responses to the receptor binding domain (RBD) and neutralising antibody responses at day 28. The primary endpoint for safety evaluation was the incidence of adverse reactions within 14 days. All recruited participants who received at least one dose were included in the primary and safety analyses. This study is registered with ClinicalTrials.gov, NCT04341389.
Findings 603 volunteers were recruited and screened for eligibility between April 11 and 16, 2020. 508 eligible participants (50% male; mean age 39·7 years, SD 12·5) consented to participate in the trial and were randomly assigned to receive the vaccine (1×10¹¹ viral particles n=253; 5×10¹⁰ viral particles n=129) or placebo (n=126). In the 1×10¹¹ and 5×10¹⁰ viral particles dose groups, the RBD-specific ELISA antibodies peaked at 656·5 (95% CI 575·2–749·2) and 571·0 (467·6–697·3), with seroconversion rates at 96% (95% CI 93–98) and 97% (92–99), respectively, at day 28. Both doses of the vaccine induced significant neutralising antibody responses to live SARS-CoV-2, with GMTs of 19·5 (95% CI 16·8–22·7) and 18·3 (14·4–23·3) in participants receiving 1×10¹¹ and 5×10¹⁰ viral particles, respectively. Specific interferon γ enzyme-linked immunospot assay responses post vaccination were observed in 227 (90%, 95% CI 85–93) of 253 and 113 (88%, 81–92) of 129 participants in the 1×10¹¹ and 5×10¹⁰ viral particles dose groups, respectively. Solicited adverse reactions were reported by 183 (72%) of 253 and 96 (74%) of 129 participants in the 1×10¹¹ and 5×10¹⁰ viral particles dose groups, respectively. Severe adverse reactions were reported by 24 (9%) participants in the 1×10¹¹ viral particles dose group and one (1%) participant in the 5×10¹⁰ viral particles dose group. No serious adverse reactions were documented.
Interpretation The Ad5-vectored COVID-19 vaccine at 5×10¹⁰ viral particles is safe, and induced significant immune responses in the majority of recipients after a single immunisation.
UPDATED on 7/13/2020
Worldwide and nationwide (per Johns Hopkins University)
Worldwide confirmed cases: 12,995,037 (up 173,150 from yesterday*)
Worldwide deaths:570,435 (up 3,334 from yesterday*)
Worldwide recoveries: 7,157,634 (up 95,738 from yesterday*)
US confirmed cases: 3,341,838 (up 48,904 from yesterday*)
As more schools add ethics into their CS curriculum, HAI associate director Rob Reich describes Stanford’s program and its responsibility in investing in ethical innovation.
Foundation Supports Leaders in Life Science who have Refocused Work to Combat the Coronavirus Pandemic
NEW YORK, July 7, 2020 (Businesswire) – The Pershing Square Foundation (the “Foundation”) today announced that it has awarded $3 million to nineteen recipients at ten academic research institutions conducting research related to the SARS-CoV-2 virus.
As scientists across various disciplines around the world have risen to the challenge of combatting SARS-CoV-2, the Foundation worked with its network of talented cancer research scientists and physician-scientists involved in the Pershing Square Sohn Cancer Research Alliance (“PSSCRA”) to create a funding opportunity for SARS-CoV-2 research. The Foundation’s PSSCRA initiative annually awards a cancer research prize that provides funding and emboldens early-career investigators to pursue research projects at a stage when traditional funding is lacking.
“The Foundation remains committed to supporting cancer research and we are proud of the PSSCRA community that we have built over the last seven years,” said Foundation Trustee Bill Ackman. “Amid this global health crisis, we felt that we had an opportunity to quickly leverage the expertise of this exceptional scientific community to identify areas in which we could rapidly deploy funds to scientists researching SARS-CoV-2 in a way similar to our approach to funding cancer research.”
By tapping the PSSCRA community for this project, the Foundation sought to foster synergy among experts across cancer research, immunotherapy/immunology, genetics, and epigenetics to shed new light on SARS-CoV-2 research, expand basic scientific knowledge, and strengthen the arsenal for current and future health crises. Proposals were evaluated for innovation, scientific excellence, and application to the SAR-CoV-2 virus. This request for proposals built on the Foundation’s commitment to rigorous scientific research, support of risky, early-stage projects that could lead to innovation, and funding for fundamental, biological discoveries that might not otherwise receive support.
“There has never been a more important time to support scientific research and we are so thankful for our scientific community,” said Olivia Tournay Flatto, PhD, Co-Founder and Executive Director of the Pershing Square Sohn Cancer Research Alliance and President of The Pershing Square Foundation. “This community has been working tirelessly to break down the silos between institutions and build on the synergy across findings in cancer research and SARS-CoV-2. The Foundation is extremely appreciative of these scientists who are combining excellence and commitment towards understanding of human biology and disease. It is an honor to work with them.”
The grantees and research projects are (listed alphabetically by research institution):
Mikala Egeblad, PhD, Cold Spring Harbor Laboratory – “Targeting Neutrophil Extracellular Traps in COVID-19”
David Tuveson, MD, PhD, and Tobias Janowitz, MD, PhD, Cold Spring Harbor Laboratory – “Famotidine as outpatient treatment for mildly to moderately symptomatic patients with COVID-19”
Adolfo Ferrando, MD, PhD, Columbia University – “Novel antiviral PROTACs for the treatment of COVID-19, emerging viral pathogens and cancer”
Carla Kim, PhD, Harvard University and Boston Children’s Hospital – “Organoid Modeling for COVID-19″
Nina Bhardwaj, MD, PhD, Icahn School of Medicine at Mt. Sinai – “Deconvolution of SARS-Cov-2-specific immune responses in COVID-19 patients for broadly effective vaccines”
Eirini Papapetrou, MD, PhD, Icahn School of Medicine at Mt. Sinai – “Genetic Determinants of COVID-19 Disease Severity”
Benjamin Greenbaum, PhD, Matthew Hellmann, MD, and Jedd Wolchok, MD, PhD, Memorial Sloan Kettering Cancer Center – “Etiology and Immune Repertoire Evolution in SARS-CoV-2 in Patients Treated with Checkpoint Blockade Immunotherapies”
Christine Mayr, MD, PhD, Memorial Sloan Kettering Cancer Center – “A role for RNA as checkpoint for protein complex assembly”
Santosha Vardhana, MD, PhD and Omar Abdel-Wahab, MD, Memorial Sloan Kettering Cancer Center – “Leveraging cancer-driven immune dysregulation to understand and enhance anti-COVID-19 immunity”
Dafna Bar-Sagi, PhD, New York University – “Determination of the Cellular Sources of IL-6 Release and Signaling in COVID-19”
Jef Boeke, PhD, New York University – “High-throughput, Automated RT-PCR Testing for Coronavirus and Beyond”
Liam Holt, PhD, New York University and Arvin Dar, PhD, Icahn School of Medicine at Mt. Sinai – “A Synthetic Viral-Like-Particle Vaccine against SARS-CoV-2”
Agnel Sfeir, PhD, New York University – “Investigating the interplay between SARS-Cov-2 and mitochondrial function”
Ali Brivanlou, PhD, The Rockefeller University, “Capitalizing on stem cell-derived synthetic human lungs on microchips to block SARS-CoV-2”
Daniel Mucida, PhD and Sohail Tavazoie, MD, PhD, The Rockefeller University – “Mucosal immunogenetics and an oral therapy for COVID-19”
Howard Chang, MD, PhD, Stanford University, “Understanding Sex-biased Immunity to COVID-19”
John Blenis, PhD and Lewis Cantley, PhD, Weill Cornell Medicine – “Targeting cellular protein kinases as treatment for COVID-19”
Christopher Mason, PhD, Weill Cornell Medicine – “TINY COVID: Rapid, Mobile, and Point-of-care Diagnostics for SARS-CoV-2 from Saliva”
Silvia Rouskin, PhD, Whitehead Institute for Biomedical Research – “Discovery of SARS2 RNA structure-based therapeutic targets”
As part of the selection process, The Pershing Square Foundation relied on the guidance of highly accomplished leaders in academia, industry, and public health.
Since 2013, the Pershing Square Sohn Cancer Research Alliance has awarded over $22 million to 39 talented scientists. With this funding, provided at the early stage of their promising careers, the recipients are contributing to the growth of New York City as a biomedical research hub. In addition to funding, the Alliance provides Prize winners with opportunities to present their work to scientific and business audiences, helping to bridge the gap between the academic and business communities. The winners of the 2020 Pershing Square Sohn Prize for Young Investigators in Cancer Research will be announced this month.
About The Pershing Square Foundation
The Pershing Square Foundation (PSF) was established in 2006 to support exceptional leaders and innovative organizations that tackle important social issues and deliver scalable and sustainable impact across the globe. PSF has committed over $400 million in grants and social investments across a number of fields, including health and medicine, education, economic development and social justice. Since 2019, Bill Ackman and Neri Oxman have served as co-trustees of the Foundation. By investing in pioneering individuals, non-profits and mission driven companies who dare to re-imagine the possible, PSF has helped to bring about important breakthroughs — from cancer research and small-scale agriculture to criminal justice reform and educational opportunities for young people in communities around the world. For more information visit: www.pershingsquarefoundation.org.
About The Pershing Square Sohn Cancer Research Alliance
The Pershing Square Sohn Cancer Research Alliance was formed in 2013 through a $25 million commitment by The Pershing Square Foundation, which partnered with The Sohn Conference Foundation. The Alliance is dedicated to playing a catalytic role in accelerating cures for cancer by supporting innovative cancer research and by facilitating collaborations between academia and industry. Annually, the Alliance awards the Pershing Square Sohn Prize to young New York based scientists who are engaged in cutting-edge cancer research. For more information, visit https://psscra.org/.
Harvard University is closely monitoring the ongoing Coronavirus Disease 2019 (COVID-19) pandemic. Our top priority remains the health, safety, and well-being of our community, on and off campus. We are planning for several reopening stages to limit the spread of COVID-19 while ensuring the continuity of our teaching and research mission. We will continue to update the community regularly to keep you informed of additional measures.
Here are the coronavirus stories Medscape’s editors around the globe think you need to know about today:
Fauci Warns of 100K Cases a Day
Anthony Fauci, MD, head of the National Institute of Allergy and Infectious Diseases, warned US senators in a committee hearing today that the nation could see 100,000 new COVID-19 cases per day if the country does not mitigate its rising number of infections.
Fauci said it is worrisome that people continue to congregate, often without masks, and that some were “jumping over and avoiding and not paying attention to the guidelines” issued by the White House Coronavirus Task Force.
“We’re going to continue to be in a lot of trouble and there’s gonna be a lot of hurt if that does not stop,” he said.
HCQ Trial to Resume
A global randomized, controlled trial testing whether the antimalarial drugs hydroxychloroquine and chloroquine can prevent COVID-19 in healthcare workers or other high-risk workers will resume, Reuters reports. The United Kingdom’s Medicines and Healthcare Products Regulatory Agency had paused the COPCOV trial after another British trial found hydroxychloroquine to have no benefit for already infected COVID-19 patients.
“Hydroxychloroquine could still prevent infections, and this needs to be determined in a randomized controlled trial,” the trial’s coleader said. “The question whether (it) can prevent COVID-19 or not remains as pertinent as ever.”
Colchicine RCT Results
A randomized, open-label trial the authors call “hypothesis-generating” leaves open the possibility that the anti-inflammatory drug colchicine could be a treatment for COVID-19.
“While our study did not directly evaluate the mechanisms of action,” the study’s lead author told Medscape Medical News, “we believe the key lies on its anti-inflammatory properties combined with an antithrombogenic effect that was indeed observed in our cohort and has also been reported in literature.”
Subject: Fauci Warns of 100K Cases/Day, HCQ Trial to Resume
UPDATED on 6/30/2020
Remote Clinical Trial Monitoring in the time of COVID-19: Working Safer and Smarter
The Journal of Precision Medicine and the Precision Medicine Leaders’ Summits are delighted to bring you this complimentary webinar presented by Shirin Hasan of Agilent Technologies and Andrew Crenshaw of Q2 Solutions.
Data integrity and quality is integral to the success of a clinical trial. Clinical monitoring is an essential function that facilitates study conduct; to ensure data quality, study integrity, and to reinforce compliance to protocols and regulatory guidelines. With the COVID-19 pandemic, there have been ramifications on clinical trial planning and conduct. Clinical monitors are now expected to conduct many activities remotely that were once performed on-site. The regulatory guidance recently issued by major authorities (including FDA and EMA) in response to the COVID-19 pandemic supports the use of central and remote monitoring programs to maintain oversight of clinical sites. To that end, clinical affairs teams must take into account the logistics, operations, systems, secure online platforms, robustness and most importantly ensure the practicality of conducting remote clinical monitoring. We must leverage our collective knowledge and experience to chart out business continuity best practices required to support clinical trials in this new business environment.
This discussion will outline how we have implemented these controls and mitigated the risks associated with remote clinical monitoring.
The state reported on Sunday that there were 19 new deaths due to the coronavirus, bringing the death toll in Massachusetts to 8,060, while the total number of cases statewide is now almost 109,000.
Rhode Island:
927 deaths (not updated on weekends)
16,661 confirmed cases (not updated on weekends)
Total tests completed: 230,508(not updated on weekends)
Maine:
104 deaths (up 0 from yesterday*)
3,191 cases (up 37 from yesterday*)
Total tests completed: 91,587(not updated daily)
New Hampshire (as of June 27)
367 deaths (up 2 from June 26*)
5,717 confirmed cases (up 46 from June 26*)
Vermont:
56 deaths (up 0 from yesterday*)
1,202 confirmed cases (up 2 from yesterday*)
Connecticut:
4,316 deaths (up 5 from yesterday*)
46,303 confirmed and probable cases (up 97 from yesterday*)
*Increases each day are calculated from the time this newsletter was sent the previous day.
As a practicing cardiologist, Dr. Elizabeth Paratz recognizes the importance of using findings from sudden cardiac arrest/death cases to improve outcomes for other patients. This recently led her to strengthen her research skills through our GCSRT program and apply them to help create the first registry in Australia that captures multi-source surveillance data on sudden cardiac arrest and related deaths. Continue Reading
Continuing Education Course | June 29 – July 1 | Live Virtual
Clinicians need to be aware of the effect COVID-19 has on multiple organ systems. Due to these frequently changing manifestations, the complex nature of the required care and the need to preserve PPE, teamwork and communication is key in the treatment of patients with COVID-19.
Since COVID-19 requires team-based care, this course will be appealing to a broad range of clinicians. Upon completion of this course, you will be able to immediately apply the knowledge acquired to improve the care of patients with COVID-19.
The Task Force on Diversity and Inclusion’s Better Together plan outlines the School’s vision for executing across-the-board increased representation of underrepresented, historically marginalized individuals such as underrepresented minorities, women, those who identify as LGBTQ and individuals with disabilities—at all levels, particularly senior faculty and department administrators and leaders. Four themes have been identified to achieve this vision. Read Plan
Enhance Your Clinical Research Skills. Personalize Your Academic Focus.
Designed for clinicians and clinician-scientists, the GCSRT certificate program provides advanced training in the methods and conduct of clinical research to drive health care innovation and achieve better outcomes. This program will commence in December 2020.
Health care models allow policy makers—and, to varying degrees, all of us—to posit a range of “what-ifs” on issues that change the course of economies and lives. Dr. Jagpreet Chhatwal, gives insight about the challenges of building and validating the COVID-19 simulator and its real-world impact. View Article
US public health officials said they have not been ordered to slow down novel coronavirus testing efforts, despite claims from President Donald J. Trump that he had given such orders and that he believes increased testing is a mistake.
Trump said at a campaign rally in Tulsa on June 20 that he had asked officials to slow testing down, according to the Washington Post and other media sources. Then today, he tweeted[[]] “Cases are going up in the US because we are testing far more than any other country, and ever expanding. With smaller testing we would show fewer cases!”
But today the nation’s top health officials refuted the President at a House Energy and Commerce Committee hearing examining the Trump administration’s response to COVID-19.
“None of us have ever been told to slow down on testing,” said Anthony Fauci, MD, director of the National Institutes of Allergy and Infectious Diseases. “We’re going to be doing more testing, not less,” he said, adding that more testing— specifically enough to conduct surveillance—is necessary, “if you want to get your arms around and understand exactly what’s going on in community spread.”
“All of us have been and continue to be committed to increasing readily timely access to testing,” said Robert Redfield, MD, director of the Centers for Disease Control and Prevention (CDC). He agreed that surveillance testing is especially important going forward, in part because it is a way to determine how many people are asymptomatic.
The US has now performed about 27 million COVID-19 tests, averaging 500,000 tests per day, said Admiral Brett P. Giroir, MD, assistant secretary for health at the Department of Health and Human Services (HHS). Giroir, who coordinates testing for the federal government, said the aim was to conduct 40 to 50 million tests a month by the fall.
Rep. Diana DeGette (D-Colorado) asked Giroir if Trump had asked him to conduct fewer tests. “Neither the President nor anyone at the Administration has instructed or suggested we should do less testing,” he said. “We are proceeding in just the opposite—we want to do more testing of higher quality,” he said.
Giroir and Redfield also both confirmed that the CDC had developed a test that could simultaneously detect influenza A, influenza B strain and SARS-CoV-2, the virus that causes COVID-19. The agency will seek an emergency use authorization for the diagnostic. “CDC is developing that test for the public health system, but in parallel the private sector now is also in advanced development,” Redfield said.
HHS and the Food and Drug Administration (FDA) are working with multiple manufacturers to have a test available at the point of care and in labs, Giroir said.
Rising cases “disturbing”
Fauci described the progress against COVID-19 as a “mixed bag,” noting that the US has been “hit badly.” The New York metro area had done well in bringing cases down, he said.
“However, in other areas of the country we are now seeing a disturbing surge in infections,” due to in part to an increase in community spread, he said. “That is something that I’m really quite concerned about,” Fauci said.
He said it was crucial to have the manpower to run a system of testing, contacting, tracing and isolating those infected, so officials can understand where the cases are coming from. “The next couple of weeks are going to be critical in our ability to address those surges that we’re seeing in Florida, in Texas, in Arizona, and in other states,” Fauci said.
DeGette asked if it might be seen as a potential positive if the cases were mostly in younger people, who she understood did not become as ill or need hospitalization as often.
Fauci said it was too early to draw conclusions. “Deaths always lag considerably behind cases,” he said. “The concern is if those cases that infect people who end up getting sick and going to a hospital, it is conceivable you may see deaths going up,” Fauci said.
FDA, CDC: No political interference
Republicans and Democrats questioned the officials about progress on a potential COVID-19 vaccine.
Trump has promised a vaccine by year’s end—enabled by his administration’s Operation Warp Speed program—which has caused some to worry that a product might get a rushed approval, in part to boost the President’s re-election chances.
Fauci said he did not think the timeframe was unreasonable. “I feel cautiously optimistic that we will be successful in getting a vaccine,” he said. While there’s never a guarantee, Fauci continued, early data were promising. He said one vaccine would be starting phase 3 human trials in July. “There is a reasonably good chance that by the very beginning of 2021 that if we’re going to have a vaccine, we’ll have it by then,” Fauci said.
He said regulators should not approve a vaccine for emergency use unless it met FDA criteria. “I would be very disappointed if we jumped to a conclusion before we knew that a vaccine was truly safe and truly effective,” he said, adding that he would not want to live with the “perpetual ambiguity of not knowing.”
FDA Commissioner Stephen Hahn, MD said that politics would not sway an approval decision. “We will rely on the science and the data when it’s available to us,” Hahn said.
Rep. Anna Eshoo (D-California) asked if the agency had been subject to pressure from the Trump administration—especially on approving the emergency use of hydroxychloroquine. Hahn said no. “I can tell you that I have not felt political pressure at the FDA to make any decision in any specific direction,” he said.
At one point, Redfield was asked by Rep. Kathy Castor (D-Florida) how often he had met with or had spoken with Trump in the past few weeks. He would not answer, saying, that “as it relates to direct interactions, I’m going to keep those between myself and the President.”
Eshoo chided the public health officials for not pushing back on what she said was Trump’s failed leadership, which she said had led to confusion and division in the American public. “I know the agencies are talking to each other,” she said, adding, “I consider that a whisper, because the American people are not hearing you speak out.”
She honed in on Redfield. “I urge you to speak out. You’re a doctor. Put on your white jacket and speak weekly to the American people,” she said.
Rep. Tony Cardenas (D-California) picked up on the topic later, asking why the agency had not been holding regular media briefings to inform the public about the latest evidence-based information, as the CDC had done in previous epidemics.
Redfield said the agency had put out 1500 guidance documents. Before he could go any further, Cardenas interrupted.
“The President has proven very clearly that when you get in front of a podium, and you actually have a press conference, you have a higher likelihood you’re going to reach more people,” Cardenas said.
Massachusetts authorities said Sunday that 30 more people have died from COVID-19, and that public health officials have detected 125 new cases in the state. The figures came as state data show that key measurements in the fight against the novel coronavirus continued a general encouraging trend.
The state has now seen 107,061 cases of COVID-19 and 7,858 deaths, according to a Department of Public Health report that includes both probable and confirmed cases. When only confirmed cases are counted, the numbers are 102,333 cases and 7,677 deaths.
Subject: Mass. reports 125 new coronavirus cases, 30 new deaths
UPDATED on 6/21/2020
Status is reachable
Thomas Wilckens (托馬斯)
• 1st
MD #PrecisionMedicine 精密医学 thought & technology leader, Keynote Speaker, industry advisor 29.000+ Followers
1d • 1 day ago
Visualizing the History of #Pandemics – NOPE Mankind must NOT change it’s social behaviour! Why should we? Infections, disease, death is part or our lifes and this will never change. #Handwashing made always sense btw.
Visualizing the History of Pandemics
visualcapitalist.com • 4 min read
85
17 Comments
UPDATED on 6/17/2020
Headlines
A Covid-19 vaccine will only work if trials include Black participants, and that’s a challenge
Of the more than 116,000 US coronavirus deaths, almost a quarter of those victims were Black. So far, Black Americans have been inadequately represented in human trials of treatments, but experts warn fair representation will be essential for a vaccine to actually be effective.
After Beijing went almost two months without a single case, 29 communities in the city have been sent back into lockdown as new infections linked back to a giant food market have arisen. The resurgence, similar to those seen in the US, demonstrates the risks of reopening.
While Covid-19 rages on, health experts are looking ahead to future, potentially even worse, pandemics. They say it’s time to treat Covid-19 like the US government treats wars and extreme weather, and investigate the country’s response to better prepare for the next one.
Daily Distraction
You don’t need to seek out a music teacher to learn how to play an instrument. These days, you can learn it all online. Here are the best sites, apps, and YouTube channels to get you up and playing.
Subject: Coronavirus Update: Trials struggle with diversity, China deals with a second wave, and more
UPDATED on 6/16/2020
Updates on the Oxford, AstraZeneca COVID-19 Vaccine
Reporter: Stephen J. Williams, PhD
AstraZeneca CEO announces that vaccine co-developed with Oxford University may provide protection for a year. Derek Lowe column expressing doubts on the vaccine are also presented.
COVID-19: Pandemic Surgery Guidance published by a Global Consortium initiated effort by Björn L.D.M. Brücher, MD, PhD, Prof. Of Surgery, Carl-Thiem-Klinikum, Cottbus, Germany
LEAKED CDC DOCUMENTS: CORONAVIRUS IS SPIKING IN US AGAIN
ABOUT A THOUSAND AMERICANS ARE DYING EVERY DAY — A TOLL SO GRIM THAT IT’S HARD TO COMPREHEND.
BY JON CHRISTIAN / 8 HOURS AGO
Leaked documents dated to earlier this week, obtained from the U.S. Centers for Disease Control and Prevention by Yahoo News, warn that new coronavirus cases are spiking again as Americans relax their social distancing practices.
Even Dr. Anthony Fauci, the White House’s top infectious disease expert and a national figurehead against the virus, lamented this week that the outbreak has become his “worse nightmare.”
“In a period of four months, it has devastated the whole world,” he said. “And it isn’t over yet.”
Does that amount to the widely-feared “second wave” of COVID, which could lead to more mass deaths and knock down an economy that’s only starting to recover? It remains unclear — especially because the fight against the virus is going very differently in different areas of the country.
Atlantic writer James Hamblin, whose early warnings about the severity of the pandemic proved prescient, pushed back against the idea that the U.S. is experiencing a second wave. It would be more accurate, he said yesterday, to characterize COVID cases in the U.S. as “one long wave” that’s leveled out around 20,000 new cases — and, chillingly, around 1,000 deaths — per day.
James Hamblin
✔@jameshamblin
Nationally there’s no “second wave.” There’s one long wave. We’ve been in a plateau of around 20,000 cases and 1,000 deaths a day, largely among minority and vulnerable populations. Reopening will cause spikes, but calling them a second wave denies the reality of what’s going on.
Those are difficult figures to comprehend, especially when the death toll exacerbates existing inequalities. If the pandemic continues to cause a thousand deaths a day, though — or, heaven forbid, if that rate climbs substantially — it’s conceivable that the U.S. could have suffered 200,000 in just a few months.
14 states and Puerto Rico hit highest seven-day average of new coronavirus infections
Since the start of June, 14 states and Puerto Rico have recorded their highest-ever seven-day average of new coronavirus cases since the pandemic began, according to data tracked by The Washington Post: Alaska, Arizona, Arkansas, California, Florida, Kentucky, New Mexico, North Carolina, Mississippi, Oregon, South Carolina, Tennessee, Texas and Utah.
Adding to the disparity in health-care support, residents in states such as Mississippi, Florida and South Carolina are living under only minor-to-moderate restrictions — even as their average daily infection rate is rising.
As of Monday, 6/8/2020, at least 109,000 people in the United States have died of covid-19, the disease caused by the coronavirus, with more than 1.95 million cases of the virus reported.
Subject: | 06.08.20 | Eli Lilly starts second antibody test; Flu shot makers gear up for critical season
UPDATED on 6/5/2020
Residents, Fellows Face the Prospect of an Ugly Job Market
— COVID-19 could throw a wrench into career plans for some time to come
by Nicole Lou, Staff Writer, MedPage Today May 14, 2020
Around the country, unemployment has hit record highs, and medicine has not been immune to a drying up of opportunities — making this an unprecedented time particularly for the graduating class of residents and fellows.
Institutions from Harvard to the University of California system have implemented hiring freezes for the foreseeable future, where new faculty appointments are no longer allowed unless under special circumstances. For clinical and research fellowship programs not under purview of the Accreditation Council for Graduate Medical Education (ACGME), hiring is on hold.
Johns Hopkins told faculty that they can’t hire any post-doc research fellows in non-ACGME programs until July at the earliest, according to Erin Michos, MD, MHS, one of the leaders of the university’s advanced echocardiography fellowship.
“I have a post-doctoral research fellow that we offered an appointment to in February just before the COVID-19 crisis in the U.S., and then her appointment got deferred due to COVID-19, and she is completely in limbo now for the time being, unemployed. It is terrible,” she said.
Clinical fellowship positions are also in danger because these programs don’t get Medicare supplementation for fellow salaries. With all the budgetary belt-tightening, some institutions may have no choice but to limit the number of fellows they can support in the future, Michos said.
From the trainees and program directors who spoke with MedPage Today, it appeared that most contracts for this year’s graduating residents and fellows remain honored for now.
“My graduating seniors all have fellowships and I have not heard of any cancellations or changes. I have only one resident entering the job market this year and he has a job,” said Andrew Freedman, MD, program director of the urology residency program at Cedars-Sinai Medical Center in Los Angeles.
Some graduating trainees have been warned that what they signed up for may not be what they get when they arrive on campus, however.
Has the Job Changed?
Lower starting pay is something that is being asked of some new hires, Freedman has heard indirectly through anecdotes.
“I know at least one or two fellows, while they didn’t lose the job, the job changed. It was supposed to be research and became clinical,” shared Gaby Weissman, MD, program director of the cardiovascular disease fellowship at MedStar Georgetown University-Washington Hospital Center and chair of the American College of Cardiology’s Program Directors and Graduate Medical Educators Section.
“Those of us who were able to secure jobs are really thankful, but some are wondering what’s going to change with those jobs. What we want may be different from what’s possible,” said Shekinah Elmore, MD, MPH, who is graduating this year from Harvard’s radiation oncology residency program and has secured an assistant professor role at University of North Carolina at Chapel Hill, starting in the summer.
“One of the reasons I want to go there is because of the tremendous global oncology work there with a good amount of travel to Africa. What would that look like in the post-COVID era?”
It is expected that the pandemic will have ripple effects on people with chronic conditions if routine medical care is not resumed on a timely basis. With much clinical research currently halted (with the exception of COVID-19 studies), some also fear the long-term consequences in academia.
“This is especially impactful for students, residents, fellows who only have a finite time in the training to accomplish research and publications before applying for their next step” according to Michos. “Several of my trainees had their projects put on hold due to COVID-related delays, and I feel terrible for them.”
Challenges for Women, International Grads
Women are among those who would be especially hurt by a decrease in academic productivity, Michos said, noting that women in medicine already have it harder integrating work-life responsibilities even outside of a pandemic. She cited research showing that women disproportionately shoulder more childcare responsibilities and housework even among dual-earner heterosexual couples.
“Now with many daycares closed and nannies being kept away for social distancing, this has been a disaster for many families who are scrambling to find new arrangements,” she said.
“As women, how do we show our competency? It’s through our numbers, our publications, our productivity. If that slows down during this pandemic, it disproportionately is more challenging for women.”
International medical school graduates and the smaller community, rural centers where many of them practice may also find this a difficult period given the new travel and visa restrictions, Michos added.
Subject: | 06.04.20 | AstraZeneca’s massive deal for billions of COVID-19 shots; New Roche test for high-risk patients
UPDATED on 6/2/2020
Hear from Anthony Fauci, M.D., Director of the National Institute of Allergy and Infectious Diseases, and Moncef Slaoui, Ph.D., Head of U.S. Operation Warp Speed, during a special plenary session during BIO Digital on Tuesday, June 9.
During the three-part plenary A Way Forward: Winning the War on COVID through Vaccines, Fauci and Slaoui will join global thought leaders in a discussion of the novel science of COVID-19 vaccines, the long-term solution for vaccine availability, and the complex and swift moving landscape of the global pandemic.
3-Part Plenary Session: A Way Forward: Winning the War on COVID through Vaccines
Don’t miss this exciting plenary session, facilitated by Phyllis Arthur, BIO Vice President of Infectious Diseases and Diagnostics Policy. This three-part plenary session will focus on the novel science of vaccines in development as well as the challenges of clinical trials, manufacturing scale-up and global implementation.
Add this can’t-miss session to your calendar today!
Part 1: Fireside Chat with Dr. Anthony Fauci, MD
11:00 AM – 11:30 AM PDT
Join us for this personal, one-on-one conversation with Dr. Fauci as he shares his insider perspective on the COVID-19 pandemic and the science emerging in response to this unprecendented crisis.
MODERATED BY:
Part 2: Leveraging Platforms and Partnerships to Develop COVID-19 Vaccines in Record Time
11:30 AM – 12:30 PM PDT
As numerous vaccines move through clinical development there are important issues that need to be addressed. How will companies and partners conduct global clinical trials? What are the key scientific issues that must be addressed to vaccinate millions of people worldwide? This panel will discuss the complex path to clinical trials, the impact of the evolving science on their development and share their thoughts on how collaboration will bring life-saving vaccines to the world.
FEATURING SPEAKERS FROM:
Duke Margolis Center for Health Policy
FDA Center for Biologics Evaluation and Research
Johnson & Johnson
Novavax
Part 3: Global Solutions for Implementation: From Scale-up to Worldwide Access
12:30 PM – 1:30 PM PDT
The successful development of these vaccines is only the first part of a long-term response to the COVID-19 pandemic. In order to truly impact the pandemic, the global public health community will need to work together with public, private and NGO partners to implement the delivery of billions of doses of vaccines. To help speed eventual availability, many companies and their partners are pursing global manufacturing and distribution solutions even though these vaccines are in the early stages of development. This panel will discuss how the community can work together to ensure rapid and broad access to vaccines.
FEATURING:
ALSO FEATURING SPEAKERS FROM:
Coalition for Epidemic Preparedness Innovation (CEPI)
The GAVI Alliance
Merck
Moderna
Can’t-Miss Sessions on Monday
Meet BIO’s Incoming President & CEO
Incoming BIO President & Chief Executive Officer Michelle McMurry-Heath, M.D., Ph.D., will join BIO Chairman of the Board Jeremy Levin, and outgoing Chief Executive Officer and industry champion Jim Greenwood to kick off BIO Digital Week with a conversation on how the biotech sector is rising to meet the greatest public health challenge in a century.
Announcing a new BIO report that showcases state-by-state information on where the bioscience economy is the strongest and where the industry is growing. Tune in for a discussion on the latest economic numbers for the industry & better understand the COVID-19 pandemic’s impact.
Moderated by BIO’s Vice President of Infectious Diseases and Diagnostics Policy, Phyllis Arthur, this panel of top scientists and industry leaders from Takeda, Vir Biotechnology, SAB Biotherapeutics, and Regeneron will share information on the development of vital treatment options and how partnerships between industry, governments and NGOs will help speed the availability of new medicines that benefit patients.
Subject: Dr. Fauci and Dr. Slaoui to Headline BIO Digital with a Live COVID-19 Plenary Session
UPDATED on 6/1/2020
Upcoming Berkeley Conversations: COVID-19 Following is a listing of the next in our series of Berkeley Conversations: COVID-19. New events are being added regularly. If you miss the live presentations; everything is being recorded and made available for viewing at any time on the Berkeley Conversations website.
COVID-19 is threatening the health and economic security of communities around the world, with dire implications for those living in poverty. As the pandemic unfolds, the Center for Effective Global Action (CEGA) is committed to sharing practical insights that can support evidence-based responses in the Global South. This panel will feature four experts from the CEGA research community: faculty co-Directors Ted Miguel and Josh Blumenstock, along with affiliates Supreet Kaur and Paul Niehaus. Panelists will discuss ongoing and completed research that sheds light on the economic toll of the pandemic, as well as the optimal design and targeting of cash transfer programs. We hope these insights will help to inform government and NGO decision-making in the face of what could quickly become a protracted crisis.
Bats are thought to harbor hundreds of coronaviruses, as well as many other types of viruses that are highly pathogenic in humans. Dr. Cara Brook and Professor Britt Glaunsinger will provide insight into what allows bats to exist with such an array of potentially lethal viruses, how pathogens like the coronavirus jump into the human population and how the coronavirus is able to hijack a human cell to amplify itself and evade the immune system. They will also discuss the coordinated efforts across UC Berkeley to track the virus, discover exactly how it works and develop new therapies.
Speakers are: Britt Glaunsinger, Professor, Department of Plant & Microbial Biology & Class of 1963 Endowed Chair, HHMI Investigator Cara Brook, Miller Postdoctoral Fellow, Department of Integrative Biology.
The SAR-CoV-2 Virus harms blood vessel causing endothelial dysfunction negatively impacting circulation, coagulation and cardiovascular multiple functions. Treatment Protocol to include cardiovascular protective drugs and drugs controlling virus replication post entry of Host’s RNA machinery.
SAR-Cov-2 is probably a vasculotropic RNA virus affecting the blood vessels: Endothelial cell infection and endotheliitis in COVID-19
Reporter: Aviva Lev-Ari, PhD, RN – Bold face and colors are my addition
Total tests completed: 154,493(3,979 newly reported tests since Saturday)
Maine:
89 deaths (up 0 from Saturday*)
2,325 total cases (up 43 from Saturday*)
Total tests completed: 54,061(only updated on Wednesdays)
New Hampshire (as of May 30)
242 deaths (up 4 from May 29*)
4,545 confirmed cases (up 53 from May 29*)
Vermont:
55 deaths (up 0 from Saturday*)
981 confirmed cases (up 4 from Saturday*)
Connecticut:
3,944 deaths (up 32 from Saturday*)
42,201 confirmed cases (up 179 from Saturday*)
*Increases each day are calculated from the time this newsletter was sent the previous day.
The inside story of how coronavirus spread in Massachusetts: Track the coronavirus pandemic in Massachusetts to its roots and you find a story driven by heroics, ingenuity, error, pain, and a hard question: How could a state famous for health care excellence have suffered such a vast loss of human life? Also watch this short documentary, which provides an in-depth look inside the outbreak, to learn more.
Virus testing in towns across the state is a mixed bag, with eight of every 100 people having been tested: Recently released town-by-town coronavirus testing data has provided new local context about Massachusetts’ battle against the pandemic. The new data offered a glimpse of where testing has been most intensive, which includes cities that have been particularly hard hit by the pandemic, such as Chelsea and Brockton.
America is contending with a pandemic. And then widespread protests happened: The upheaval sparked by a video capturing George Floyd’s agonizing last minutes as a white police officer kneels on his neck is pulsing through an America already ragged with anger and anxiety. Emotions are raw over the toll of a pandemic that has killed more than 100,000 people across the country and cost millions of jobs.
Around the region:
Even as the coronavirus pandemic has changed expectations about how and when people will eventually gather in large crowds, plans to expand and improve the MBTA and the Boston Convention & Exhibition Center should not be abandoned, said James Rooney, president and chief executive officer of the Greater Boston Chamber of Commerce, on Sunday.
As Massachusetts continued its recovery Saturday from the coronavirus pandemic, some clergy voiced caution about opening their doors too soon, while protesters at the State House blasted Governor Charlie Baker for moving too slowly in restarting the state’s economy.
Three protests against the killing of George Floyd are taking place in Boston on Sunday, and participants are being asked to wear masks and be mindful to maintain social distancing amid the pandemic.
A Boston greeting-card startup has revised its approach, adding the machinery and personnel necessary to produce and distribute personal protective equipment. Now, thanks to one of its investors, 100,000 medical gowns are being donated to Massachusetts hospitals.
Subject: Coronavirus Now: The inside story of how COVID-19 spread in Massachusetts
5/30/2020
SARS-CoV-2 is pre-adapted to Human Transmission, branches of evolution stemming from a less well-adapted human SARS-CoV-2-like virus have been found: The Role of SARS-CoV-2 Virus Progenitors for Future Virus Disease Transmission and Pandemic Re-Emergence
Reporter and Curator: Aviva Lev-Ari, PhD, RN – all bold face and colors are my additions
Total tests completed: 132,701(2,572 newly reported tests since Saturday*)
Maine:
78 deaths (up 1 from Saturday*)
2,055 total cases (up 42 from Saturday*)
Total tests completed: 37,725(only updated on Wednesdays)
New Hampshire (as of May 23)
208 deaths (up 4 from May 22*)
4,089 confirmed cases (up 75 from May 22*)
Vermont:
54 deaths (up 0 from Saturday*)
956 confirmed cases (up 2 from Saturday*)
Connecticut:
3,693 deaths (up 18 from Saturday*)
40,468 confirmed cases (up 446 from Saturday*)
*Increases each day are calculated from the time this newsletter was sent the previous day.
In N.H., a drive-in live concert is what the new normal may look (and sound) like during the coronavirus pandemic: Tupelo Music Hall in Derry, N.H. held a socially distant concert in the parking lot Saturday afternoon – giving insight to what might become the new normal for entertainment. Most of the people spread far apart were wearing masks. So were the orange-vested attendants directing concert-goers to their “seats,” which in this case consisted of two parking spots each — one for the car, and one for whatever lawn chairs patrons pulled out of their trunks.
Much of the establishment backed Charlie Baker during the pandemic — but there has been one exception: Over the past few weeks, the Greater Boston Chamber of Commerce and Jim Rooney, its chief executive, have publicly prodded the Baker administration to be more clear and forthcoming about the reopening process, raising eyebrows in the city’s tight-knit business community that tends to work behind the scenes and air grievances privately.
New study says Massachusetts coronavirus rates are much higher than reported and could rise steeply: The estimates from Imperial College London said the virus has already infected about 13 percent of the state’s 6.9 million residents. That’s about 896,000 people, far more than the 91,662 confirmed COVID-19 cases reported by the state on Saturday but significantly short of the threshold for herd immunity.
Around the region:
In separate television appearances Sunday, US Representative William Keating and Boston Mayor Martin J. Walsh warned that the coronavirus’s impact on small businesses could force many of them to close permanently.
Whether we will continue to care about Chelsea is an open question now that the grim tallies there, and across the state, are dropping and the beaches are back, writes columnist Yvonne Abraham.
President Trump is likely to face re-election with the unemployment rate over 10%, said Eric Rosengren, president of the Boston Fed.
Eddie Sutton, who led three teams to the Final Four and was the first coach to take four schools to the NCAA Tournament, died Saturday. He was 84.
The NBA is in talks with The Walt Disney Company on a single-site scenario for a resumption of play in Central Florida in late July, the clearest sign yet that the league believes the season can continue amid the coronavirus pandemic.
How to fill the long summer ahead? Here are some safe ways for teens to volunteer.
Want to stay entertained? Here are some virtual events in music, comedy, theater, visual arts, family entertainment and more — all chosen by Globe critics and staff.
A Tufts professor – and her sisters – have released a Web comedy series coined “Old Guy,” a humorous take on ageism in the media.
Are you a small business owner? Boston Globe Media has created a Slack workspace just for you to meet other small business owners, share support, and connect with us.
Tell us how you’re coping: Here’s a list of different ways you can share your stories to better our coronavirus coverage.
Subject: Coronavirus Now: New study says Massachusetts coronavirus rates are much higher than reported
5/20/2020
Great News from the South Korean CDC! Published paper shows patients who recovered are showing immunity and are not reinfected!
Reporter: Stephen J. Williams, PhD
In the video below, Dr. John Campbell, internationally renowned immunologist and virologist from Fox Chase Cancer Center, discusses a recent paper from the south Korean CDC (not published in English yet) that shows patients who had previously been infected with COVID19 and have recovered (recovered from illness) are retesting positive merely because the high sensitivity of the PCR test used was actually detecting “dead” viral particles which were still being shed from upper airway epithelium. These patients were showing immunity to COVID19 and were not shedding live viral particles (infectious virus). In addition, the Korean CDC feels that there was not a reactivation of the virus nor was this reinfection by new virus particles, as patients had antibodies and appeared immune to further COVID19 infection. Dr. Campbell describes this as very good news. In addition he says that COVID19, unlike some influenza viruses, is a slow mutating virus and explains why this is important with respect to pathogenecity and herd immunity.
However we don’t really know how long the immunity lasts, if memory immune cells have been detected, or if this immunity is dependent on exposure to a certain viral load.
In summary, 290 patients that had recovered from COVID19 that retested positive after 10 weeks post recovery
probably retested positive due to the sensitivity of the PCR test used to detect dead virus (a sort of false positive) and
Moderna’s COVID-19 prompted an immune response similar to those seen in patients who have recovered from infection. Eight patients who received the two lowest dose levels—25 micrograms and 100 micrograms—developed neutralizing antibodies against the virus two weeks after receiving their second dose.
CAMBRIDGE, Mass.–(BUSINESS WIRE)–May 18, 2020– Moderna, Inc., (Nasdaq: MRNA) a clinical stage biotechnology company pioneering messenger RNA (mRNA) therapeutics and vaccines to create a new generation of transformative medicines for patients, today announced positive interim clinical data of mRNA-1273, its vaccine candidate against novel coronavirus (SARS-CoV-2), from the Phase 1 study led by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health (NIH).Immunogenicity data are currently available for the 25 µg and 100 µg dose level (ages 18-55) after two doses (day 43) and at the 250 µg level (ages 18-55) after one dose (day 29). Dose dependent increases in immunogenicity were seen across the three dose levels, and between prime and boost within the 25 µg and 100 µg dose levels. All participants ages 18-55 (n=15 per cohort) across all three dose levels seroconverted by day 15 after a single dose. At day 43, two weeks following the second dose, at the 25 µg dose level (n=15), levels of binding antibodies were at the levels seen in convalescent sera (blood samples from people who have recovered from COVID-19) tested in the same assay. At day 43, at the 100 µg dose level (n=10), levels of binding antibodies significantly exceeded the levels seen in convalescent sera. Samples are not yet available for remaining participants.At this time, neutralizing antibody data are available only for the first four participants in each of the 25 µg and 100 µg dose level cohorts. Consistent with the binding antibody data, mRNA-1273 vaccination elicited neutralizing antibodies in all eight of these participants, as measured by plaque reduction neutralization (PRNT) assays against live SARS-CoV-2. The levels of neutralizing antibodies at day 43 were at or above levels generally seen in convalescent sera.mRNA-1273 was generally safe and well tolerated, with a safety profile consistent with that seen in prior Moderna infectious disease vaccine clinical studies. The sole incidence of a grade 3 adverse event in the 25 µg and 100 µg dose cohorts was a single participant at 100 µg who experienced grade 3 erythema (redness) around the injection site. To date, the most notable adverse events were seen at the 250 µg dose level, comprising three participants with grade 3 systemic symptoms, only following the second dose. All adverse events have been transient and self-resolving. No grade 4 adverse events or serious adverse events have been reported.
Summary of Press Release: After two doses all participants evaluated to date across the 25 µg and 100 µg dose cohorts seroconverted with binding antibody levels at or above levels seen in convalescent sera. mRNA-1273 elicited neutralizing antibody titer levels in all eight initial participants across the 25 µg and 100 µg dose cohorts, reaching or exceeding neutralizing antibody titers generally seen in convalescent sera. The significance is that neutralizing antibody, even at the lowest dose of vaccine, was detectable in a number of subjects however this was the initial 8 subjects who received the vaccine. This study involved 60-100 subjects.
The Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) Partnership on May 18, 2020: Leadership of AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Eisai, Eli Lilly, Evotec, Gilead, GlaxoSmithKline, Johnson & Johnson, KSQ Therapeutics, Merck, Novartis, Pfizer, Roche, Sanofi, Takeda, and Vir. We also thank multiple NIH institutes (especially NIAID), the FDA, BARDA, CDC, the European Medicines Agency, the Department of Defense, the VA, and the Foundation for NIH
NIH Director: Defeating COVID-19 requires unprecedented action and collaboration
Colorized scanning electron micrograph of a VERO E6 cell (purple) exhibiting elongated cell projections and signs of apoptosis, after infection with SARS-COV-2 virus particles (pink), which were isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. NIAID
What
To respond to the generational public health crisis caused by the global COVID-19 pandemic, a swift, coordinated effort across many sectors of society is necessary, say National Institutes of Health (NIH) Director Francis S. Collins, M.D., Ph.D., and Johnson & Johnson Vice Chairman of the Executive Committee and Chief Scientific Officer Paul Stoffels, M.D. In a Viewpoint published today in JAMA(link is external), Drs. Collins and Stoffels outline the innovative efforts of Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV), a public-private initiative organized by NIH and the Foundation for the NIH. ACTIV’s partners, which include at least 18 leading biopharmaceutical companies, multiple U.S. federal agencies, and the European Medicines Agency, are developing an international strategy for an integrated research response to COVID-19.
Noting that never has a public-private biomedical research effort of this scope and scale come together with such speed and determination, Drs. Collins and Stoffels describe how ACTIV has established a collaborative framework
to prioritize therapeutic and vaccine candidates;
to streamline human clinical trials and
tap into existing trial networks; and
to coordinate regulatory processes and
leverage assets among all partners.
The authors point out that ACTIV’s industry partners have taken unprecedented steps to support a prioritization of therapeutic and vaccine candidates, no matter who has developed them, and have indicated willingness to contribute their respective clinical trial capacities, irrespective of the agent to be studied.
ACTIV has established four working groups, each with one co-chair from NIH and one from industry. They are:
The Preclinical Working Group. Charged with standardizing and sharing preclinical evaluation resources and methods, and with accelerating testing of candidate therapies and vaccines to support entry into clinical trials.
The Therapeutics Clinical Working Group. Charged with prioritizing and accelerating clinical evaluation of a long list of therapeutic candidates for COVID-19 with near-term potential.
The Clinical Trial Capacity Working Group. Charged with assembling and coordinating existing networks of clinical trials to increase efficiency and build capacity to test potential therapies and vaccines for COVID-19.
The Vaccines Working Group. Charged with accelerating evaluation of vaccine candidates to enable rapid authorization or approval.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
With all eyes on the prize for a COVID-19 vaccine, researchers are setting aggressive timetables that might be too good to be true. Despite hopes that a shot could be available this year, Novartis’ CEO is pumping the brakes––and given his past vaccines experience, he should know.
Novartis CEO Vas Narasimhan forecast Thursday that a potential COVID-19 vaccine could take until the end of 2021 to reach an approval, throwing some cold water on drugmakers with aggressive timelines for their candidates, Bloomberg reported.
In an opinion piece published in Germany’s Heraldszeitung, Narasimhan said a vaccine would be “the ultimate way to deal with this pandemic,” Bloomberg reported, and would take anywhere from “one and a half to two years.”
NIH begins clinical trial of hydroxychloroquine and azithromycin to treat COVID-19
Study enrolling adults with mild to moderate COVID-19 in the United States.
This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID’s Rocky Mountain Laboratories (RML) in Hamilton, Montana.NIAID
A clinical trial has begun to evaluate whether the malaria drug hydroxychloroquine, given together with the antibiotic azithromycin, can prevent hospitalization and death from coronavirus disease 2019 (COVID-19). The National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, is sponsoring the trial, which is being conducted by the NIAID-funded AIDS Clinical Trials Group (ACTG). Teva Pharmaceuticals is donating medications for the study.
The Phase 2b trial will enroll approximately 2,000 adults at participating ACTG sites(link is external) across the United States. Study participants must have confirmed infection with SARS-CoV-2, the virus that causes COVID-19, and be experiencing fever, cough and/or shortness of breath. The investigators anticipate that many of those enrolled will be 60 years of age or older or have a comorbidity associated with developing serious complications from COVID-19, such as cardiovascular disease or diabetes. Participants will be randomly assigned to receive short-term treatment with either hydroxychloroquine and azithromycin or matching placebos. People living with HIV and pregnant and breastfeeding women also are eligible to participate in the study. The first participant enrolled today in San Diego, California.
“We urgently need a safe and effective treatment for COVID-19. Repurposing existing drugs is an attractive option because these medications have undergone extensive testing, allowing them to move quickly into clinical trials and accelerating their potential approval for COVID-19 treatment,” said NIAID Director Anthony S. Fauci, M.D. “Although there is anecdotal evidence that hydroxychloroquine and azithromycin may benefit people with COVID-19, we need solid data from a large randomized, controlled clinical trial to determine whether this experimental treatment is safe and can improve clinical outcomes.”
Currently, there are no specific therapeutics approved by the U.S. Food and Drug Administration to treat people with COVID-19. Hydroxychloroquine is FDA-approved to prevent and treat malaria, as well as to treat the autoimmune diseases rheumatoid arthritis and lupus. Some preliminary reports have suggested that hydroxychloroquine, alone or in combination with the FDA-approved antibiotic azithromycin, may benefit people with COVID-19. Numerous clinical trials are planned or underway, including a recently launched study supported by NIH’s National Heart, Lung and Blood Institute evaluating the safety and effectiveness of hydroxychloroquine for treatment of adults hospitalized with COVID-19. On March 28, FDA issued an Emergency Use Authorization(link is external) (EUA) to allow hydroxychloroquine and medical-grade chloroquine to be distributed from the Strategic National Stockpile and prescribed by doctors to hospitalized adolescents and adults with COVID-19, as appropriate, when a clinical trial is not available or feasible.
Participants in the ACTG study, called A5395, will receive oral medications to take at home. Those randomly assigned to the experimental treatment group will take 400 milligrams (mg) of hydroxychloroquine twice on the first day and 200 mg twice daily for an additional six days. They also will take 500 mg of azithromycin on the first day and 250 mg daily for an additional four days. The control group will receive equivalent numbers of placebo pills. Neither the participants nor the study team will know who received experimental treatment or placebo until the end of the trial.
Participants will record their symptoms, adherence to treatment, and major events such as hospitalizations in a diary for 20 days. Study staff will follow up with participants by telephone during this period. When possible, participants will come to the clinical research site for an in-person visit at day 20. Additional follow-ups will be conducted by telephone three and six months after treatment starts.
The main objective of the study is to determine whether hydroxychloroquine and azithromycin can prevent hospitalization and death due to COVID-19. Additionally, investigators will evaluate the safety and tolerability of the experimental treatment for people with SARS-CoV-2 infection. While hydroxychloroquine and azithromycin are both considered safe in most people, they can cause side effects ranging from headache and nausea to, rarely, heart rhythm problems that can be life-threatening. Because of the risk of heart problems when hydroxychloroquine is used alone or combined with azithromycin, FDA cautions that use of hydroxychloroquine for COVID-19 should be limited to clinical trials or for treating certain hospitalized patients under EUA(link is external) so clinicians can monitor patients for adverse effects.
“This study will provide key data to aid responses to the COVID-19 pandemic,” said ACTG Chair Judith Currier, M.D., of the University of California, Los Angeles. “We are pleased to be able to leverage ACTG’s existing infrastructure for HIV treatment clinical trials to quickly implement this important study.”
The study team is led by Protocol Chair Davey Smith, M.D., of the University of California, San Diego. David Wohl, M.D., of the University of North Carolina at Chapel Hill, and Kara W. Chew, M.D., and Eric S. Daar, M.D., both of the University of California, Los Angeles, serve as protocol vice-chairs. The trial is expected to enroll quickly given the high incidence of COVID-19, and initial results may be available later this year.
NIAID conducts and supports research—at NIH, throughout the United States, and worldwide—to study the causes of infectious and immune-mediated diseases, and to develop better means of preventing, diagnosing and treating these illnesses. News releases, fact sheets and other NIAID-related materials are available on the NIAID website.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
Daily covid19 testing continues to increase nationally while the positivity rate continues to decline. These are hopeful signs that — at least in many parts of the nation — the epidemic is slowing. Some models show that the doubling time is now 45 days and the Ro is 1.10
The Department of Public Health (DPH) updates data on deaths and cases by city and town once a week, on Wednesdays. Click on the interactive above to see how your town or city has been affected. For more, explore a sortable table with each city and town here.
Tracking Cases, Deaths And Tests Over Time
Each day, DPH releases a dashboard of its data tracking cases and deaths by race, sex and geography. You can find more on that information on this page.
A daily look at how many beds are available in the state’s hospitals and at its new field hospitals, such as Boston Hope at the Boston Convention and Exhibition Center.
Here’s how many hospital beds are being used:
Hospitals are reporting how many confirmed and suspected coronavirus patients they are treating, including inside their ICUs. Our charts below show how the number of patients has changed over time.
Search for individual hospitals in the two charts below.
Here’s how many confirmed/suspected COVID-19 patients are in hospitals:
Here’s how many confirmed/suspected COVID-19 patients are in ICUs:
For additional details on the hospitalization charts, read more here. (Note: DPH did not provide data for April 17 or 18.) Back to top
Long-Term Care Facility Cases And Deaths
Nursing homes, assisted-living residences and rest homes are among the hardest hit amid the pandemic.
The charts below show how the number of cases, deaths and the numbers of long-term care (LTC) facilities reporting at least one case of the virus have changed over time, as well as how those factor into the overall number of cases and deaths. (Note: DPH didn’t provide data on April 20.)
Dr. Klibanski will welcome participants to the 2020 World Medical Innovation Forum, a global — and this year, virtual — gathering of more than 5,000 senior health care leaders. This annual event was established to respond to the intensifying transformation of health care and its impact on innovation. The Forum is rooted in the belief that no matter the magnitude of that change, the center of health care needs to be a shared, fundamental commitment to collaborative innovation – industry and academia working together to improve patient lives. No collaborative endeavor is more pressing than responding to the COVID-19 pandemic.
#1 | Battling COVID-19: Maps, Technology, and AI
Rochelle Walensky, MD
Chief, Infectious Disease, MGH; Professor of Medicine, Harvard Medical School
Mapping the spread of infectious diseases within communities is more important than ever as the novel coronavirus continues to sweep across the globe. Researchers are harnessing AI, technology, and advanced data analytics to map the spread of COVID-19 and identify those infected with the virus.
Total tests completed in Massachusetts: 388,389 (11,852 newly reported tests since Saturday)
*Increases each day are calculated from the time this newsletter was sent the previous day.
State by state, region by region, it’s a patchwork approach: Here’s what reopening the economy looks like: About three dozen states have issued reopening plans, according to the National Governors Association. Massachusetts has yet to unveil its own, even though restrictions on daily life to contain COVID-19 have so far kept hospitals from being overwhelmed. The stay-at-home advisory and ban on nonessential businesses is in effect until May 18, which is also the deadline for a board appointed by Governor Charlie Baker to deliver recommendations on how to restart the economy.
Karen Eggleston is a Senior Fellow, Director of the Stanford Asia Health Policy Program, and Deputy Director of the Shorenstein Asia-Pacific Research Center at the Freeman Spogli Institute for International Studies (FSI) at Stanford University.
Yong Suk Lee is the SK Center Fellow at the Freeman Spogli Institute for International Studies and Deputy Director of the Korea Program at the Walter H. Shorenstein Asia-Pacific Research Center at Stanford University.
Abstract:
Most studies of automation focus on manufacturing or use aggregate data. In one of the first studies of the service sector using establishment-level data, we examine the impact of robot adoption on staffing in nursing homes. This setting is important because robots are increasingly being adopted in many countries to address the challenges posed by population aging. Japan, in particular, has been actively developing and deploying robots in nursing homes to deal with labor shortages, and since 2015 has subsidized nursing home purchase of robots. Analyzing 2017 data from Japanese nursing homes, we document that facilities that adopt robots are larger, with more functionally-impaired residents, greater numbers of care workers and nurses, many other assistive technologies, better management practices, and located in prefectures with higher planned subsidies for robots per nursing home.
Nick Bloom is a Professor in the department of economics and Professor, by courtesy, at the Graduate School of Business. He is also the Co-Director of the Productivity, Innovation and Entrepreneurship program at the National Bureau of Economic Research (NBER), and a fellow of the Centre for Economic Performance, and the Stanford Institute for Economic Policy Research.
The King Center on Global Development is hosting a special virtual event with the Walter H. Shorenstein Asia-Pacific Research Center on the economic impact of COVID-19 in China. You will hear from four Stanford faculty members as they analyze the Chinese government’s initial response, as well as how the virus impacted urban and rural employment and the health care sectors.
COVID-19 is having a substantial impact on our students and broader research community, such as job or internship offers that are being rescinded. At the same time, many new research projects and collaborations are being launched to address the pandemic. HAI would like to create a clearinghouse for COVID-19 research collaborations and other opportunities, such as RA positions, internships, or funding opportunities.
SGLT2 Inhibitor dapagliflozin, just approved by FDA, Is Being investigated for ability to reduce respiratory failure in mild to moderate COVID-19. Experts boards warn of extreme caution though because of deadly side effects.
New study of diabetes drug for COVID-19 raises eyebrows
A just-launched study of the type 2 diabetes agent dapagliflozin (Farxiga, AstraZeneca) in patients with mild to moderate COVID-19 is raising eyebrows, given that several expert groups have advised that drugs in this class – the sodium-glucose cotransporter 2 (SGLT2) inhibitors – be stopped in all patients hospitalized with COVID-19 because of the increased risk for diabetic ketoacidosis (DKA). The randomized, double-blind, placebo-controlled, phase 3 Dapagliflozin in Respiratory Failure in Patients With COVID-19 (DARE-19) study is sponsored by AstraZeneca and Saint Luke’s Mid America Heart Institute. The trial will assess whether dapagliflozin reduces the risks of disease progression, clinical complications, and death because of COVID-19 in patients with type 2 diabetes, cardiovascular disease, and/or mild to moderate chronic kidney disease (CKD). “Dapagliflozin has demonstrated cardio- and renal-protective benefits and improved outcomes in high-risk patients with type 2 diabetes, heart failure with reduced ejection fraction, and CKD,” said the principal investigator of DARE-19, Mikhail N. Kosiborod, MD, a cardiologist at Saint Luke’s Mid America Heart Institute, Kansas City, Mo. And “patients with COVID-19 and underlying cardiometabolic disease appear to be at the highest risk of morbid complications,” he explained in an AstraZeneca statement. “Through DARE-19, we hope to decrease the severity of illness, and prevent cardiovascular, respiratory, and kidney decompensation, which are common in patients with COVID-19,” Dr. Kosiborod continued. However, advice to stop SGLT2 inhibitors in patients hospitalized with COVID-19 because of its associated DKA risk has come from several channels. These include initial guidance from Diabetes UK; experts who spoke during an American Diabetes Association webinar; and most recently, an international panel of diabetes experts. Some clinicians went so far as to say that they view the trial as potentially dangerous, while others said they could see some logic to it, as long as it is carefully managed.
The statewide death toll is 4,840 and the total number of people to test positive is up to 76,743. (Jenna Fisher/Patch)BOSTON — Another 138 people have died because of the coronavirus and 1,410 others have tested positive for the virus that causes COVID-19, according to state officials. This brings the statewide death toll to 4,840 and the total number of people to have tested positive up to 76,743.A closely watched estimate of the state’s likely death toll from the coronavirus now says Massachusetts may see nearly 7,700 deaths by August.The Seattle-based Institute for Health Metrics and Evaluation forecast has steadily risen as government policies change and the spread of the virus continues. Its prediction model forecast in March that the pandemic could take around 2,300 lives during the next four months. The April estimate put that figure around 5,625, based in part on the state’s failure to mandate social distancing measures and stay-at-home orders.
Sherlock’s quick, CRISPR-based coronavirus test gets emergency nod
5/7/2020
Scott Gottlieb, MD
@ScottGottliebMD
Daily positive cases of covid19 as a percent of total daily tests continues to fall nationally, a very good sign as covid testing expands. Declining positivity could be a leading indicator of an epidemic starting to decline. 10% is still high but it’s coming down at a steady pace
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused a global pandemic. The percentage of infected individuals who seroconvert is still an open question. In addition, it has been shown in some individuals that viral genome can still be detected at considerable time post symptom resolution. Here we investigated both seroconversion and PCR-positivity in a large cohort of convalescent serum donors in New York City. Methods: Individuals with confirmed or suspected SARS-CoV-2 infection were screened via PCR for presence of viral genome and via enzyme-linked immunosorbent assay for presence of anti SARS-CoV-2 spike antibodies.
Results: All but three confirmed SARS-CoV-2 patients seroconverted to the SARS-CoV-2 spike while only 37.4% of suspected SARS-CoV-2 patients seroconverted. PCR-positivity was detected up to 28 days from symptom resolution.
Conclusions: Here we show that the vast majority of confirmed COVID19 patients seroconvert, potentially providing immunity to reinfection. We also report that in a large proportion of individuals, viral genome can be detected via PCR in the upper respiratory tract for weeks post symptom resolution, but it is unclear if this signal represents infectious virus. [bold face by ALA]
1) I wanted share some data from a manuscript that just wen online at medrxiv.org/content/10.110…. This was spearheaded by the fantastic Dr. Ania Wajnberg in collaboration with many parts of the Mount Sinai Hospital and Icahn School of Medicine.
2) The data describes PCR and serology findings in the first 1343 plasma donors screened at Mount Sinai. Initially, there were two groups of donors: people who at some point had PCR confirmed COVID19 and people who had suspected COVID19 (but were never PCR confirmed).
3) The majority of these donors were mild cases. Now, almost all PCR-confirmed donors had antibodies, while the majority of the suspected COVID19 individuals did not. This tells us two things: a) the assay works and b) many people who think they had COVID19 might not have had it.
4) When concentrating on the PCR confirmed donors we find that at first testing not all of them make antibodies, but many have high titers (in A). When we then recall people without/with low antibody titers for second test that vast majority of them becomes positive (shown in B).
5) Keep in mind that this ELISA assay that we use here was shown to correlate well with a neutralization assay (here: medrxiv.org/content/10.110…) basically suggesting that the vast majority make neutralizing antibodies, even if they were mild cases.
6) Now, this is expected. This looks pretty normal and is basically what we see for influenza. Sometime, somebody doesn’t make antibodies (lack of seroconversion), but that is normal too. It is OK that this occurs, it happens for many other viruses at a low rate as well.
7) So, this is all good news. It still does not show that we are protected from reinfection, but it makes me feel pretty good. Now, Dr. Wajnberg found something in addition that is super interesting. Remember those reports of people testing positive again weeks after they…..
8)….recovered? Now, recently it was suggested that this is just viral fragments that are shed, not reinfection and not reactivation. Many of us have suspected this for a long time, and now we can maybe close that discussion. So, the donors were also tested by PCR when they….
9)….came in for their blood draw. And guess what? The latest PCR+ post recovery (not post-disease onset) we found so far was 28 days out. I find this extremely interesting. It is very likely that all this positivity you see below in red is genome, not infectious virus.
10) I need to go back to work, but stay tuned. I hope we will have more data for you soon. Lots of work, lots to learn. Stay home, stay safe!
Israel’s undisputed reputation as the “Start-Up Nation” has only been strengthened during the COVID-19 pandemic, as the IDF and Israeli society are working wonders, showing again that their response to life-and-death situations is proactive, solution-oriented ingenuity. While this creativity spans from AI to biotech to leading the race for a vaccine, today we’re spotlighting some of the IDF’s most resourceful repurposing, innovation, and inventions that have emerged from this global crisis to protect and save lives:
• Shayetet 13, the Israeli Navy’s Commando unit, developed a solution for civilians in need of oxygen, as COVID-19 impacts lung capacity. Naturally, the unit has extensive scuba diving experience, a practice that requires compressed oxygen devices. In the face of the coronavirus, development teams converted these operational tanks into medical, oxygen compressing systems that meet all required standards and protocols, answering a lifesaving need. Along with development and supply, the unit is managing distribution logistics!
• The IDF’s Elite Military Intelligence Directorate’s 81st Technological Unit is focused on tackling several main issues amid existing shortages: ventilators, PPE (personal protective equipment), and improved data collection. In the project “Breathing Air,” the unit converts inexpensive and simple CPAP (Continuous Positive Airway Pressure) machines, typically used by first responders for breathing assistance, into fully functioning respirators. As coronavirus attacks patients’ lungs, these machines pump air in and out, keeping sufferers alive as doctors try to fight off the virus. The system also monitors patients’ breathing and transmits this information to hospital staff. Described by doctors as “first-class invasive respirators” that are “far, far cheaper” than proper ventilators, the IDF took a simple product that already existed in high supply, overcame the challenges of emitting sterile air in proper quantities, and ensured reliable devices in the event that existing machines and ventilators ran out.
Brig. Gen. Yaniv Rotem, Head of Military R&D in Israel’s Ministry of Defense, explains some of the ways Israel has adapted its military technology to combat COVID-19, including the use of robots in hospitals that allow for doctor-patient interfacing that keep both parties safe by eliminating exposure.
• The IDF’s elite ‘Yahalom’ unit repurposed robots, originally intended to deliver heavyweight equipment to fighter forces, into coronavirus aid delivery systems. Operated at a distance via remote control, these portable and small “Probots” transport large quantities of groceries and supplies to civilians living in “hotspot” areas, easily navigating narrow spaces crowded with parked vehicles and approaching residences without generating human exposure.
• The Israel Security Agency, the Shin Bet, worked with the Health Ministry to retrace the movements of coronavirus patients by tracking cell phone and other digital data to identify, alert, and order into quarantine people unknowingly exposed to the pathogen. The practice spared untold numbers of people, as the 500 people they directed into quarantine later tested positive for the virus. This sophisticated technology was previously reserved for counterterrorism operations alone but has been revealed and deployed temporarily to save lives and curb the virus outbreak.
It’s no wonder that Israel’s status as the Start-Up Nation and an innovative trailblazer and powerhouse is often attributed to the country’s mandatory IDF service. Well-honed skills like problem-solving crises, diagnosing potential outcomes, mitigating risks, educating, and exercising life-saving practices have all proven critical and lifesaving during this crisis. Further, Israel and the IDF have impacted and lifted the world by immediately sharing their successful innovations to protect as many human lives as possible.
We at FIDF are so proud to support the heroic efforts of our men and women in uniform, so that they may continue their ingenious work, protecting all Israeli civilians, and helping those around the world over suffering from this devasting virus.
Brig. Gen. Tal Aharon joined the IDF in 1990 and holds bachelor’s and master’s degrees in Mechanical Engineering. He served in various positions in the IDF’s Technological Division of the Ground Forces before stepping into his current role as Head of the Division and has been involved in the technological development of numerous vehicles, tanks, armored personnel carriers (APCs), weapon systems, robotics, and more. Since the outbreak of COVID-19, Brig. Gen. Aharon has been leading acquirement initiatives of Medical Corps equipment and technological solutions aimed at assisting the civilian population.
Subject: IDF Innovation Saves Lives During COVID-19
5/3/2020
Development of a Vaccine at Oxford University
5/2/2020
Mass. High Technology Council COVID-19 Recovery and Return to Work Series: Framework for Restarting the MA Economy
The Massachusetts High Technology Council’s Executive Committee along with a diverse group of private sector leaders have developed a Recovery and Return to Work framework designed to restart the Commonwealth’s economy while protecting the health of residents. The framework’s essential categories are presented by Steve Pagliuca, Co-Chairman, Bain Capital and co-owner of the Boston Celtics, and Megan Greenfield, Partner, McKinsey & Co.
Coronavirus (COVID-19) Update: FDA Issues Emergency Use Authorization for Potential COVID-19 Treatment
For Immediate Release:
Today, the U.S. Food and Drug Administration issued an emergency use authorization for the investigational antiviral drug remdesivir for the treatment of suspected or laboratory-confirmed COVID-19 in adults and children hospitalized with severe disease. While there is limited information known about the safety and effectiveness of using remdesivir to treat people in the hospital with COVID-19, the investigational drug was shown in a clinical trial to shorten the time to recovery in some patients.
“FDA’s emergency authorization of remdesivir, two days after the National Institutes of Health’s clinical trial showed promising results, is a significant step forward in battling COVID-19 and another example of the Trump Administration moving as quickly as possible to use science to save lives,” said HHS Secretary Alex Azar. “NIH, FDA, and scientists across America and around the world have worked tirelessly with patients to get us this new potential treatment for COVID-19. The seamless cooperation between government and private industry under the President’s all-of-America approach to COVID-19 is getting treatment options to patients in record time.”
The emergency use authorization allows for remdesivir to be distributed in the U.S. and administered intravenously by health care providers, as appropriate, to treat suspected or laboratory-confirmed COVID-19 in adults and children hospitalized with severe disease. Severe disease is defined as patients with low blood oxygen levels or needing oxygen therapy or more intensive breathing support such as a mechanical ventilator.
“From day one, the FDA has been committed to expediting the development and availability of potential COVID-19 treatments. Today’s action is an important step in our efforts to collaborate with innovators and researchers to provide sick patients timely access to new therapies where appropriate, while at the same time supporting research to further evaluate whether they are safe and effective,” said FDA Commissioner Stephen M. Hahn, M.D. “There’s tremendous interest among all parties to identify and arm ourselves with medicines to combat COVID-19, and through our Coronavirus Treatment Acceleration Program, the FDA is working around-the-clock and using every tool at our disposal to speed these efforts.”
Based on evaluation of the emergency use authorization criteria and the scientific evidence available, it was determined that it is reasonable to believe that remdesivir may be effective in treating COVID-19, and that, given there are no adequate, approved, or available alternative treatments, the known and potential benefits to treat this serious or life-threatening virus currently outweigh the known and potential risks of the drug’s use.
The EUA also requires that fact sheets that provide important information about using remdesivir in treating COVID-19 be made available to health care providers and patients, including dosing instructions, potential side effects and drug interactions. Possible side effects of remdesivir include: increased levels of liver enzymes, which may be a sign of inflammation or damage to cells in the liver; and infusion-related reactions, which may include low blood pressure, nausea, vomiting, sweating, and shivering.
Following the declaration by the Secretary of HHS that circumstances exist justifying the emergency use of unapproved products, the FDA may issue an emergency use authorization to allow unapproved medical products or unapproved uses of approved medical products to be used in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by chemical, biological, radiological and nuclear threats when there are no adequate, approved, and available alternatives.
The issuance of an EUA is different than FDA approval. In determining whether to issue an EUA, the FDA evaluates the available evidence and carefully balances any known or potential risks of any unproven products with any known or potential benefits of making them available during the emergency.
The EUA was issued to Gilead Sciences Inc. The FDA previously allowed for study of the investigational drug under clinical trials, as well as expanded access use for individual patients and through a multi-patient expanded access program coordinated by Gilead.
The EUA will be effective until the declaration that circumstances exist justifying the authorization of the emergency use of drugs and biologics for prevention and treatment of COVID-19 is terminated and may be revised or revoked if it is determined the EUA no longer meets the statutory criteria for issuance.
The FDA, an agency within the U.S. Department of Health and Human Services, protects the public health by assuring the safety, effectiveness, and security of human and veterinary drugs, vaccines and other biological products for human use, and medical devices. The agency also is responsible for the safety and security of our nation’s food supply, cosmetics, dietary supplements, products that give off electronic radiation, and for regulating tobacco products.
The FDA didn’t leave much time to assess the positive nature of the first cut of data from a controlled study of remdesivir in severely afflicted coronavirus cases. On Friday the agency stamped their approval on Gilead’s drug, which NIAID director Anthony Fauci has already determined should become the new standard of care in treating hospitalized patients fighting off Covid-19.
After recalibrating the primary endpoint, researchers determined that the drug cut the average time to recovery to 11 days in the drug arm, compared to 15 in the control group. The drug arm mortality rate hit 8%, beating out the control group at 11%, but failed to come in at a statistically significant improvement on the first cut of the data.
The approval comes just 2 months after the outbreak truly began to rattle the US, and 3 months after the Wuhan outbreak triggered a pandemic that has killed people and shattered economies around the globe, sickening millions. The FDA’s action follows an emergency use authorization for hydroxychloroquine and chloroquine, malaria meds that have also raised safety alarms on their side effects.
Taken together, the FDA has made it clear that regulators will move first and ask questions later. In this case, there’s still much left to learn about remdesivir, including the best dose and its impact on different patient groups.
Another mystery is how Gilead plans to make money on the drug — and how much. Analysts grilled CEO Dan O’Day on that score on Thursday evening, during their Q1 call, but to no avail. All that has yet to play out.
O’Day’s emphasis on responsibility first and profits second, though, has some discounting any upside for the company.
Evan Seigerman at Credit Suisse was one of the first analysts to make a comment, noting:
We do not expect RDV to be a significant com. biz for GILD & do not model any sales.
Subject: ALERT: FDA cheers on Gilead’s remdesivir with a snap emergency OK following the first solid glimpse of positive Covid-19 data
APRIL 2020
4/29/2020
An astounding article. The drone photo is devastating. As bad as the events in the Western World are, this is so much worse …. and Africa is just starting to surge ….
And the Amazon region
Aerial view of coffins being buried at an area where new graves have been dug at the Parque Tarumã cemetery in Manaus. Photograph: Michael Dantas/AFP via Getty Images
Keeping an Academic Lab Afloat in a Pandemic – TimmermanReport.com
Two months ago, our lab at Fred Hutch was on a roll. After six years of hard work building technology platforms to discover protein drugs — infrastructure that few academic labs have — we were…
This is stunning: Nearly half of the Q1 decline in GDP can be attributed to healthcare, which is presumably delaying of elective procedures. It’s a strange reality that in the midst of a pandemic, we have a healthcare-led recession.
32 Days on a Ventilator: One Covid Patient’s Fight to Breathe Again – New York Times coverage of patient treatment at Mass General, quotes physicians Emily Rubin, Paul Currier, Yuval Raz, and Peggy Lai, nurse Kerri Voelkel, and respiratory therapists Tyler Texeira and Todd Mover
There are many big numbers associated with the coronavirus pandemic: tens of thousands have lost their lives, and millions have filed for unemployment. But there’s also much smaller story playing out — inside the cells of those who contract the virus.
This microscopic, unpredictable story is what makes the coronavirus so deadly, and developing a treatment so challenging, experts say.
Unlike bacteria or fungi, viruses cannot live on their own — they require host cells to function. When viruses use human cells as hosts, they “completely take over all of the metabolic pathways of the cell to replicate itself,” explained David Leib, chair of microbiology and immunology at Dartmouth College.
“It would be as if somebody walked into a car factory and snapped his fingers and said suddenly, ‘You’re making Twinkies!’ ” he said.
The coronavirus can attack the first cells it encounters in our nose or throat.
“It takes the virus roughly 10 minutes to get inside that cell and then to begin its replication cycle,” Leib said.
Then, he said, it takes eight to 10 hours to produce hundreds of copies of itself that go on to infect other cells in our bodies.
But while the virus is replicating and spreading, people are not necessarily aware. The World Health Organization says it can take between one and 14 days for a person to notice symptoms; the average is five days. And some people who are infected never develop symptoms.
Leib said it’s this period of time, when you do not feel sick but the virus is replicating, that makes coronavirus so dangerous and so hard to stop.
“You are a walking bottle of virus,” he said. “Any of your respiratory droplets would be quite infectious during that time, despite the fact that you feel well enough to go out and go to the store.”
After the virus breaks into your cells, some patients develop symptoms. However, many of the symptoms, including fever and aches, are actually a product of your immune system fighting off the virus rather than the virus itself.
“Many people have mild illness and after a week or so they feel a lot better,” said Shira Doron, an infectious disease doctor and epidemiologist at Tufts Medical Center.
For most people, Doron said, that mild illness seems to be it. The person’s immune system is able to see that the virus is hijacking cells and stop it.
But a small percentage of people have a second phase of the illness. They seem to be getting better until their symptoms begin escalating. The Centers for Disease Control and Prevention warns that “clinicians should be aware of the potential for some patients to rapidly deteriorate one week after illness onset.”
For many of these coronavirus cases — in which symptoms become severe — the body’s response to the virus may actually be more damaging than the virus itself.
“We actually, occasionally, find that people who are really, really sick from COVID-19, don’t even have a positive test at that point,” Doron said. “It’s not the virus really anymore that’s causing the symptoms. It’s the immune response to that invasion. We call it the cytokine storm.”
Cytokines are proteins that act like an alarm in the immune system, sending out signals and calling in reinforcements to fight an invader. In a cytokine storm, although the fight might need just one military unit, the alarm keeps going off and a massive army shows up.
“This immune overreaction is causing collateral damage. It’s like friendly fire,” explained Leib. “It’s just like any other urgent situation — an overreaction can be just as damaging as not reacting at all.”
Too many cells are recruited to fight off the invader, and the cells fail to respond effectively.
“The cells become exhausted very quickly,” said Galit Alter, a professor of medicine at the Ragon Institute of Massachusetts General Hospital, MIT and Harvard. “They’re getting stimulated so hard by all these cytokines that the cells at some point almost poop out. And they are not able to completely participate in that antiviral response.”
In the lungs, this can look like a lot of inflammation — there is fluid accumulation where there is supposed to be air. That makes it very challenging for oxygen to transfer into the blood.
Unlike humans, Leib said, bats — which experts think are the source of COVID-19 — don’t get cytokine storm. “This lack of cytokine storm in bats may explain why they don’t get sick, but we do,” he said.
Leib said one of the challenges of combating COVID-19 in humans is the fact that viruses hijack our cells.
“This is really the crux of the reason why it has been so hard to develop antiviral drugs, because almost any drug that will stop viruses dead in [their] tracks will also stop our cells dead in their tracks,” he said.
Doron, Alter and Leib emphasized how much there is still to learn about the virus. But Leib believes our best hope for fighting it is a vaccine that trains the immune system to recognize and eliminate the coronavirus before it can take hold — and before the immune system can call in that army.
Editor’s note: This is a list of selected resources on the novel coronavirus (formerly known as as 2019 n-CoV, now known as SARS-CoV-2) that causes COVID-19 disease. The list spans everything from official sources, trackers, and data sites to medical journal information hubs, background readings, and Twitter accounts. If you have suggestions for what to add here (please note, the list is not crowdsourced but carefully curated), please email sonal [at] a16z [dot] com.
Righting the Wrongs of Misinformation about the Whole Ultraviolet light Issue
I have included some of the papers which may clarify some of this confusion around ultraviolet light and COVID19. The groups of scientists and publications in question are using UV-C light to destroy viral particles in isolated plasma, not in humans. The authors were merely trying to offer a solution to blood banks like the Red Cross, who were worried that blood donations, sans the levels of available COVID testing among the general population, could destroy the viral particles in plasma and blood products they collect and use for various transfusion processes. The authors found that exposure to UV-C could be effective in destroying viral particles however it must be stated that the biological activity or infectivity of the treated purified plasma was not tested. In addition there is no safety information on the parenteral administration of riboflavin (vitamin B2) or riboflavin containing products.
What are the different types of UV Light?
Scientists categorize UV light into several different subtypes:
UV-A light (320-400nm) is UV light with the longest wavelength, and the least harmful. It is more commonly known as “black light”, and many use its ability to cause objects to emit fluorescence (a colored glowing effect) in artistic and celebratory designs. Many insects and birds can perceive this type of UV radiation visually, along with some humans in rare cases such as Aphakia (missing optic lens).
UV-B light (290-320nm) causes sunburns with prolonged exposure along with increasing the risk of skin cancer and other cellular damage. About 95% of all UV-B light is absorbed by the ozone in Earth’s atmosphere.
UV-C light (100-290nm) is extremely harmful and is almost completely absorbed by Earth’s atmosphere. It is commonly used as a disinfectant in food, air, and water to kill microorganisms by destroying their cells’ nucleic acids.
Note: DNA absorbs UV light at a peak of 260 nm and prolonged exposure to the 300 nm wavelength can damage purified DNA. UV-B transluminators are used for detection of ethidium stained DNA, however most scientists use at 365 nm in order to minimize potential damage to DNA, allowing for downstream application using the purified DNA piece including various cloning procedures. UV-B light can also damage DNA. Germicidal UV lamps emit UV-C light in this range.
Abstract BACKGROUND AND OBJECTIVE: Severe acute respiratory distress syndrome coronavirus-2 (SARS-CoV-2), the causative agent of coronavirus disease 2019 (COVID-19), is a member of the coronavirus family. Coronavirus infections in humans are typically associated with respiratory illnesses, however viral RNA has been isolated in serum from infected patients. Coronaviruses have been identified as a potential low-risk threat to blood safety. The Mirasol Pathogen Reduction Technology (PRT) System utilizes riboflavin and ultraviolet (UV) light to render blood-borne pathogens noninfectious, while maintaining blood product quality. Here we report on the efficacy of riboflavin and UV light against the pandemic virus SARS-CoV-2 when tested in both plasma and platelets units. MATERIALS AND METHODS: Stock SARS-CoV-2 was grown in Vero cells and inoculated into either plasma or platelet units. Those units were then treated with riboflavin and UV light. The infectious titers of SARS-CoV-2 were determined by plaque assay using Vero cells. A total of five (n=5) plasma and three (n=3) platelet products were evaluated in this study. RESULTS: In both experiments the measured titer of SARS-CoV-2 was below the limit of detection following treatment with riboflavin and UV light. The mean log reductions in the viral titers were ≥3.40 and ≥4.53 for the plasma units and platelet units, respectively. CONCLUSION: Riboflavin and UV light effectively reduced the titer of SARS-CoV-2 in both plasma and platelet products to below the limit of detection in tissue culture. The data suggest that the process would be effective in reducing the theoretical risk of transfusion-transmitted SARS-CoV-2.
Other papers from NCBI Pubmed on this topic include:
A paper from 1988 shows the DNA damaging effect of UV light in the 300 nm range even more than with the suspected mutagen ethidium bromide, which may be a result of ethidium bromide protecting the strand from formation of thymine dimers. DNA damage produced by ethidium bromide staining and exposure to ultraviolet light. N F Cariello, P Keohavong, B J Sanderson, and W G Thilly
4/25/2020
Updated April 24: COVID19 WHAT IF WE ARE ALL WRONG
These Treatment Guidelines have been developed to inform clinicians how to care for patients with COVID-19. Because clinical information about the optimal management of COVID-19 is evolving quickly, these Guidelines will be updated frequently as published data and other authoritative information becomes available.
The recommendations in these Guidelines are based on scientific evidence and expert opinion. Each recommendation includes two ratings: a letter (A,B, or C) that indicates the strength of the recommendation and a Roman numeral (I, II, or III) that indicates the quality of the evidence that supports the recommendation (see Table 1).
Panel Composition
Members of the COVID-19 Treatment Guidelines Panel (the Panel) were appointed by the Panel co-chairs and chosen based on their clinical experience and expertise in patient management, translational and clinical science, and/or development of treatment Guidelines. Panel members include representatives from federal agencies, health care and academic organizations, and professional societies. Federal agencies and professional societies represented on the Panel include:
American College of Chest Physicians
American College of Emergency Physicians
American Thoracic Society
Biomedical Advanced Research and Development Authority
Centers for Disease Control and Prevention
Department of Defense
Department of Veterans Affairs
Food and Drug Administration
Infectious Diseases Society of America
National Institutes of Health
Pediatric Infectious Diseases Society
Society of Critical Care Medicine
Society of Infectious Diseases Pharmacists.
The inclusion of representatives from professional societies does not imply that their societies have endorsed all elements of this document.
The names, affiliations, and conflict of interest disclosures of the Panel members, ex-officio members, and support staff are provided in the Panel Roster and Financial Disclosures.
Development of the Guidelines
Each section of the Guidelines was developed by a working group of Panel members with expertise in the section’s area of interest. Each working group was responsible for identifying relevant information and published scientific literature, and conducting a systematic, comprehensive review of that information and literature. The working groups will propose updates to the Guidelines based on the latest published research findings and evolving clinical information.
Each guideline section has been reviewed, modified as necessary, and voted on by the entire Panel. A majority vote was required for a recommendation to be included in the posted Guidelines. Panel members are required to keep all Panel deliberations and unpublished data considered during the development of the guidelines confidential.
Method of Synthesizing Data and Formulating Recommendations
The working groups critically review and synthesize the available data to develop recommendations. Aspects of the data that are considered include, but are not limited to, the type of study (e.g., case series, prospective cohort, randomized controlled trial), the quality and suitability of the methods, the number of participants, and the effect sizes observed. Each recommendation is assigned two ratings according to the scheme presented in Table 1.
Table 1. Recommendation Rating Scheme
Strength of Recommendation
Quality of Evidence for Recommendation
A: Strong recommendation for the statement
B: Moderate recommendation for the statement
C: Optional recommendation for the statement
I: One or more randomized trials with clinical outcomes and/or validated laboratory endpoints
II: One or more well-designed, nonrandomized trials or observational cohort studies
III: Expert opinion
It is important to note that at present, to develop the recommendations in these Guidelines, the Panel relied heavily on experience with other diseases, supplemented with evolving personal clinical experience with COVID-19, and incorporated the rapidly growing published scientific literature on COVID-19. When information existed in other published Guidelines that the Panel felt important to include in these Guidelines, the information was included with permission from the original sources.
Evolving Knowledge on Treatment for COVID-19
Currently there are no Food and Drug Administration (FDA)-approved drugs for COVID-19. However, an array of drugs approved for other indications, as well as multiple investigational agents, are being studied for the treatment of COVID-19 in several hundred clinical trials around the globe. These trials can be accessed at ClinicalTrials.gov. In addition, providers can access and prescribe investigational drugs or agents approved or licensed for other indications through various mechanisms, including Emergency Use Authorizations (EUA), Emergency Investigational New Drug (EIND) applications, compassionate use or expanded access programs with drug manufacturers, and/or off-label use.
For this reason, whenever possible, the Panel recommends that promising, unapproved or unlicensed treatments for COVID-19 be studied in well-designed controlled clinical trials. This includes drugs that have been approved or licensed for other indications. The Panel recognizes the critical importance of clinical research in generating evidence to address unanswered questions regarding the safety and efficacy of potential treatments for COVID-19. However, the Panel also realizes that many patients and providers who cannot access such trials are still seeking guidance about whether to use these agents.
Finally, it is important to stress that the rated treatment recommendations in these Guidelines should not be considered mandates. The choice of what to do or not to do for an individual patient is ultimately decided by the patient together with their provider.
The COVID-19 pandemic has driven big spikes in interest in telemedicine software, electronic signature tools, and Web conferencing platforms, according to recent research from TrustRadius.
The biggest increase in interest since March 9 has been in the telemedicine software category, with search impressions up 613%.
That’s followed by the electronic signature (+511%), Web conferencing (+500%), mobile app development (+366%), antivirus (+357%), remote desktop (+281%), video platforms (+265%), webinar (+226%), Web portal (+199%), and live chat (+194%) categories.
The products with the biggest spikes in interest since March 9 on the TrustRadius platform are Intermedia AnyMeeting (Web conferencing category), Google Classroom (learning management system), Blackboard Collaborate (Web conferencing), Zoom (Web conferencing), and Webex Events (webinar).
What software are people buying during COVID-19?
New Data on How COVID-19 Will Impact B2B Tech Spending | TrustRadius Blog
Coronavirus live updates: Accuracy of antibody testing questioned – Scott Gottlieb, ex-FDA Commissioner warned that the tests shouldn’t be relied upon to make “individual decisions.”
The Forum is pleased to host the following virtual symposium on Tuesday, April 21, 2020.
COVID-19: Where do we go from here? Tuesday, April 21, 2020 12-1pm ET Presented jointly by the Harvard T.H. Chan School of Public Health and the New England Journal of Medicine
Join us for a one-hour virtual symposium jointly presented by the Harvard T.H. Chan School of Public Health and the New England Journal of Medicine for a timely and important conversation with leaders in public health on COVID-19 and our next collective steps. From securing crucial supplies, to hopes for treatments and vaccines, to “reopening” society, experts will explore how best to proceed.
Subject: Reengineering masks; Truman Scholars; SLAC research; voting by mail
4/21/2020
SLAC joins the global fight against COVID-19
The lab is responding to the coronavirus crisis by imaging disease-related biomolecules, developing standards for reliable coronavirus testing and enabling other essential research.
BY MANUEL GNIDA
As part of the international response to the COVID-19 pandemic, the U.S. Department of Energy’s SLAC National Accelerator Laboratory has re-opened some of its facilities for essential research on the atomic structure of the virus and how it interacts with potential treatments and vaccines.
SLAC scientists are also leading the development of global standards to ensure reliable testing for the coronavirus, and they are participating in DOE working groups that are considering a wide range of proposals for coronavirus research, including high-throughput drug screening and novel approaches for building ventilators.
“Working with our fellow national labs, Stanford University and other partners, we’re applying our unique expertise and facilities to make a difference in the global fight against this disease,” said SLAC Director Chi-Chang Kao.
Targeting the virus on an atomic level
At the forefront of SLAC’s coronavirus research are techniques that use beams of X-rays or electrons to decipher how life’s molecular machinery works on the atomic level. This can help answer key questions about SARS-CoV-2, the virus that causes COVID-19, such as how it recognizes and infects cells, how it replicates within them, and how it spreads through our bodies. This detailed knowledge can feed into the development of vaccines and treatments with drugs or antibodies.
This animation, created with publicly available protein structure data, shows how a spike protein on the surface of novel coronavirus SARS-CoV-2 binds to a human ACE2 receptor protein, leading to infection. (Greg Pintilie/National Center for Macromolecular Imaging)
While the March 16 San Francisco Bay Area’s shelter-in-place order temporarily shut down all but essential operations at the lab, the Stanford Synchrotron Radiation Lightsource (SSRL) is operating a subset of its experimental stations to provide powerful X-rays for coronavirus-related studies.
One method they are using is X-ray crystallography, which examines biomolecules such as the spike proteins on the surface of SARS-CoV-2. These proteins dock onto receptor molecules on the surface of cells in the lungs, heart or intestines and spill the virus’s genetic material into the host cells where it replicates.
Researchers crystallize these biomolecules for analysis with SSRL’s X-rays, which produces detailed images of where each atom of the protein is located. These 3D maps can then feed into the design of targeted therapeutic interventions, for instance drugs that block spike proteins from binding to host cells.
Collaborating with researchers from other institutions, the SSRL team is working to determine the 3D structures of a number of biomolecules involved in the life cycle of SARS-CoV-2.
A robot mounts samples, stored in liquid nitrogen, into an experimental station for X-ray crystallography at SLAC’s synchrotron, SSRL. (Aina Cohen/Silvia Russi/SLAC National Accelerator Laboratory)
“We’re able to do this research and, at the same time, follow strict social distancing protocols because our experimental stations are highly automated and require only minimal staff on site,” said Aina Cohen, who co-leads SSRL’s Structural Molecular Biology Division. “Researchers can send us frozen samples to be mounted by robots into the experimental stations. The remote researchers then use our software and video tools to control the robots, view their samples, and control all the details of their experiment from their home lab, or even from their homes.”
Another method used at SSRL is small-angle X-ray scattering, which looks at how X-rays bounce off biomolecules and their complexes in solution. Thomas Weiss, who oversees the research at this experimental station, is collaborating with Gerard Wong’s lab and other scientists at the University of California, Los Angeles, as well as researchers at the University of California, San Diego, to look at how pieces of viral proteins interact with the machinery of the human immune system.Insights into these interactions could help scientists understand why SARS-CoV-2 is so infectious and causes so much inflammation – a principal reason for why it is so deadly.
LinkedIn Notification to Aviva Lev-Ari, PhD, RN on 4/20/2020
4/20/2020
With Mass General models showing a flattening curve, coronavirus patients are not expected to overwhelm the system during this week’s surge
Doctors and mathematicians at Massachusetts General Hospital, part of a little-known modeling team, are now optimistic that the number of coronavirus patients has plateaued at their institution, as well as in their larger hospital network, and will not overwhelm clinicians.
The Mass. General predictions come at a time when the state is considered a national hotspot for coronavirus and when data show 100 to 150 Massachusetts residents dying daily from the virus.
But analysts at the hospital believe that the crush of very sick patients at its doors is unlikely to get worse — and could start to ease in a week.
Subject: Mass General models show flattening curve; project system won’t be overwhelmed by coronavirus patients
4/20/2020
Dear Aviva,
Following the success of the Fierce coronavirus virtual series in March, the editorial teams beind FiercePharma and FierceHealthcare bring you the second installment in our spring virtual series, Coronavirus: Where are we now? We’ll bring together a new series of experts for a week of virtual panels to discuss our current progress against the coronavirus pandemic, and what challenges remain ahead.
View the schedule below and click here to register for the sessions of your choice.
Monday, May 4:
11:00am — 12:00pm ET | Tech’s role in managing COVID-19 patients’ recovery outside the hospital and preparing for the next virus
3:00pm — 4:00pm ET | Vaccines accelerate toward market: How fast and how far?
Tuesday, May 5:
11:00am — 12:00pm ET | Hospitals after the ‘peak’: What happens next?
3:00pm — 4:00pm ET | Clinical trial challenges amid COVID-19
Wednesday, May 6:
11:00am — 12:00pm ET | Bouncing back: Payers’ role in helping the system recover from COVID-19
3:00pm — 4:00pm ET | Outbreak scramble: Could COVID-19 change infectious disease R&D?
I hope you will join us for our Virtual Series. And as always, thank you for being a part of the Fierce community.
Subject: Fierce Coronavirus Virtual Series: Where are we now?
4/20/2020
With Mass General models showing a flattening curve, coronavirus patients are not expected to overwhelm the system during this week’s surge
Doctors and mathematicians at Massachusetts General Hospital, part of a little-known modeling team, are now optimistic that the number of coronavirus patients has plateaued at their institution, as well as in their larger hospital network, and will not overwhelm clinicians.
The Mass. General predictions come at a time when the state is considered a national hotspot for coronavirus and when data show 100 to 150 Massachusetts residents dying daily from the virus.
But analysts at the hospital believe that the crush of very sick patients at its doors is unlikely to get worse — and could start to ease in a week.
Total tests completed in Massachusetts: 162,241 (5,435 newly reported tests since yesterday)
*Increases each day are calculated from the time this newsletter was sent the previous day.
US health officials watching Mass. coronavirus outbreak closely: Massachusetts is becoming a top concern for federal officials responding to the COVID-19 outbreak as cases here climb into what Governor Charlie Baker described on Sunday as “the middle of the surge.” White House coronavirus response coordinator Dr. Deborah Birx listed Boston and Massachusetts alongside the Chicago area as places where officials were focusing their attention.
Amid a flurry of national coronavirus data, Massachusetts remains a hot spot of infection: Nationally, day after day, Massachusetts has persistently stood out by several alarming metrics, often ranking near or in the top five among states for deaths, per capita infections, and the rate of those who have tested positive for the virus. Explore how it compares to all other states.
Trump administration, congressional leaders near deal on virus aid that includes major boost for small businesses: The Trump administration and congressional leaders are closing in on a $400 billion-plus deal that could pass in the Senate as soon as Monday to renew funding for a small business loan program that recently ran out of money. The deal would also boost spending for hospitals and testing.
Around the region:
The fall semester poses a looming financial dilemma for colleges and students and their families. Colleges and universities across the country are already preparing in case students cannot come to campus in the fall.
Boston broadcasted warnings about COVID-19 from public works trucks fitted with sound equipment through the neighborhoods with the highest rates of the virus — Hyde Park, Mattapan, Dorchester, East Boston, Roxbury, and Roslindale — delivering the message to wash hands and stay inside in seven languages.
With the number of Rhode Island residents who have died from the coronavirus now at 150, Governor Gina Raimondo on Sunday once again urged people to wear a mask anytime that they’re in public.
Boston’s newest medical facility — a pop-up field hospital at the city’s cavernous convention center — has already treated more than 100 coronavirus patients in the past week and could reach capacity in the coming days.
More than 100 treatments and vaccines are in development to stem the COVID-19 pandemic, and some onlookers have worried that this sprawling and potentially duplicative effort is wasting time and resources. Hoping to bring order to the chaos, the National Institutes of Health (NIH) and major drug companies today announced a plan to stage carefully designed clinical trials of the drugs and vaccines they have decided are the highest priorities for testing and development.
The public-private partnership involves NIH, other U.S. government agencies, 16 pharma companies and biotechs, and the nonprofit Foundation for the National Institutes of Health (FNIH). It aims to develop “an international strategy” for COVID-19 research, a press release states. However, NIH Director Francis Collins told reporters during a press call today that, “It is primarily a U.S. focused effort.”
The initiative, called Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV), aims to make efficient use of NIH funding and its clinical trial networks by working with companies to evaluate data on early candidates, selecting those that have the most promise and are not already part of rigorous human tests.
AAAS Science Podcast: Why some diseases are seasonal and some are not: Coronaviruses and more
Measuring early levels of these biomarkers during acute infection will deepen our understanding of cytokine storm onset and related cardiopulmonary and neurological damage. Simoa allows measurement of trace levels of IFNα, which enables separation of bacterial from viral infections, characterization of lupus samples and now following COVID-19 patients IFNα profile and assess type I interferon treatment options. Listen to key opinion leaders discussing their views on circulating cytokines as predictive biomarkers for COVID-19 severity, early viral load quantification based on viral proteins and early measurement of IgM, IgG and IgA for seroprevalence studies.
STUDYING THE KEY ROLE OF INFLAMMATION IN DISEASE PROGRESSION AND SEVERITY
CHARACTERIZING LINKS BETWEEN VIRAL INFECTION AND NEUROLOGICAL MANIFESTATIONS
MEASURING THE EARLIEST BIOMARKERS OF MYOCARDIAL INJURY AND RISK OF ACUTE AND CHRONIC CARDIAC DISEASE
DEVELOPING NEW ULTRA-SENSITIVE ASSAYS FOR VIRAL DETECTION AND HOST RESPONSE
These studies form the basis for an educated guess at what might happen with Covid-19 patients. After being infected with SARS-CoV-2, most individuals will have an immune response, some better than others. That response, it may be assumed, will offer some protection over the medium term — at least a year — and then its effectiveness might decline.
Other evidence supports this model. A recent peer-reviewed study led by a team from Erasmus University, in the Netherlands, published data from 12 patients showing that they had developed antibodies after infection with SARS-CoV-2. Several of my colleagues and students and I have statistically analyzed thousands of seasonal coronavirus cases in the United States and used a mathematical model to infer that immunity over a year or so is likely for the two seasonal coronaviruses most closely related to SARS-CoV-2 — an indication perhaps of how immunity to SARS-CoV-2 itself might also behave.
If it is true that infection creates immunity in most or all individuals and that the protection lasts a year or more, then the infection of increasing numbers of people in any given population will lead to the buildup of so-called herd immunity. As more and more people become immune to the virus, an infected individual has less and less chance of coming into contact with a person susceptible to infection. Eventually, herd immunity becomes pervasive enough that an infected person on average infects less than one other person; at that point, the number of cases starts to go down. If herd immunity is widespread enough, then even in the absence of measures designed to slow transmission, the virus will be contained — at least until immunity wanes or enough new people susceptible to infection are born.
At the moment, cases of Covid-19 have been undercounted because of limited testing — perhaps by a factor of 10 in some places, like Italy as of late last month. If the undercounting is around this level in other countries as well, then a majority of the population in much (if not all) of the world still is susceptible to infection, and herd immunity is a minor phenomenon right now. The long-term control of the virus depends on getting a majority of people to become immune, through infection and recovery or through vaccination — how large a majority depends on yet other parameters of the infection that remain unknown.
One concern has to do with the possibility of reinfection. South Korea’s Centers for Disease Control and Prevention recently reported that 91 patients who had been infected with SARS-CoV-2 and then tested negative for the virus later tested positive again. If some of these cases were indeed reinfections, they would cast doubt on the strength of the immunity the patients had developed.
An alternative possibility, which many scientists think is more likely, is that these patients had a false negative test in the middle of an ongoing infection, or that the infection had temporarily subsided and then re-emerged. South Korea’s C.D.C. is now working to assess the merit of all these explanations. As with other diseases for which it can be difficult to distinguish a new infection from a new flare-up of an old infection — like tuberculosis — the issue might be resolved by comparing the viral genome sequence from the first and the second periods of infection.
And then there is the question of immune enhancement: Through a variety of mechanisms, immunity to a coronavirus can in some instances exacerbate an infection rather than prevent or mitigate it. This troublesome phenomenon is best known in another group of viruses, the flaviviruses, and may explain why administering a vaccine against dengue fever, a flavivirus infection, can sometimes make the disease worse.
More science on almost every aspect of this new virus is needed, but in this pandemic, as with previous ones, decisions with great consequences must be made before definitive data are in. Given this urgency, the traditional scientific method — formulating informed hypotheses and testing them by experiments and careful epidemiology — is hyper-accelerated. Given the public’s attention, that work is unusually on display. In these difficult circumstances, I can only hope that this article will seem out of date very shortly — as much more is soon discovered about the coronavirus than is known right now.
Marc Lipsitch (@mlipsitch) is a professor in the Departments of Epidemiology and Immunology and Infectious Diseases at Harvard T.H. Chan School of Public Health, where he also directs the Center for Communicable Disease Dynamics.
As of the middle of last week, the CDC had reports of more than 315,000 cases in the U.S. The new report focused on about 49,000 for which researchers had data on whether or not they worked in health care. About 9,300, or 19 percent, of them were medical professionals. That included 27 who died.
But the data varied in how complete it was, researchers said. In 12 states that did a better job reporting on whether patients worked in medicine, around 11 percent of cases were health care workers.
Compared with U.S. cases overall, larger proportions of diagnosed health care workers were women, were white, and were young or middle-aged adults. That’s consistent with the demographics of who works in health care, researchers said.
About 10 percent of the health care workers were hospitalized with symptoms, compared with 21 percent to 31 percent of overall cases. That may reflect the younger age of the workers, as well as prioritization of testing for health care employees, the report said.
Colorized scanning electron micrograph of an apoptotic cell (blue) infected with SARS-COV-2 virus particles (yellow), isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. NIAID
A new study has begun recruiting at the National Institutes of Health in Bethesda, Maryland, to determine how many adults in the United States without a confirmed history of infection with SARS-CoV-2, the virus that causes coronavirus disease 2019 (COVID-19), have antibodies to the virus. The presence of antibodies in the blood indicates a prior infection. In this “serosurvey,” researchers will collect and analyze blood samples from as many as 10,000 volunteers to provide critical data for epidemiological models. The results will help illuminate the extent to which the novel coronavirus has spread undetected in the United States and provide insights into which communities and populations are most affected.
The study will be conducted by researchers at the National Institute of Allergy and Infectious Diseases (NIAID) and the National Institute of Biomedical Imaging and Bioengineering (NIBIB), with additional support from the National Center for Advancing Translational Sciences (NCATS) and the National Cancer Institute (NCI), all parts of NIH.
“This study will give us a clearer picture of the true magnitude of the COVID-19 pandemic in the United States by telling us how many people in different communities have been infected without knowing it, because they had a very mild, undocumented illness or did not access testing while they were sick,” said Anthony S. Fauci, M.D., NIAID director. “These crucial data will help us measure the impact of our public health efforts now and guide our COVID-19 response moving forward.”
Investigators will test participants’ blood samples for the presence of SARS-CoV-2 antibodies , proteins the immune system produces to fight a specific infectious agent. A positive test result indicates previous infection. To date, reporting of U.S. cases of COVID-19 has mostly relied on molecular tests that determine the presence of the virus in a person’s airways using a noninvasive cotton swab. While these cotton swab-based tests rapidly and effectively identify active infection, they do not determine whether a person was previously infected with SARS-CoV-2 and recovered.
“An antibody test is looking back into the immune system’s history with a rearview mirror,” said Matthew J. Memoli, M.D., M.S., principal investigator of the study and director of NIAID’s Laboratory of Infectious Diseases Clinical Studies Unit. “By analyzing an individual’s blood, we can determine if that person has encountered SARS-CoV-2 previously.”
Investigators will analyze blood samples for two types of antibodies, anti-SARS-CoV-2 S protein IgG and IgM, using an ELISA (enzyme-linked immunosorbent assay) developed by researchers at NIAID and NIBIB. In blood samples found to contain antibodies against SARS-CoV-2, researchers may perform additional tests to evaluate the volunteers’ immune responses to the virus. These data may provide insight as to why these cases were less severe than those that lead to hospitalization.
Kaitlyn Sadtler, Ph.D., study lead and principal investigator for laboratory testing, holds up a microsampling device from the home blood collection kit used in the study.NIBIB
Healthy volunteers over the age of 18 from anywhere in the United States can participate and will be asked to consent to enrollment over the telephone. Individuals with a confirmed history of COVID-19 or current symptoms consistent with COVID-19 are not eligible to participate.
After enrollment, study participants will attend a virtual clinic visit, complete a health assessment questionnaire and provide basic demographic information—including race, ethnicity, sex, age and occupation—before submitting samples in one of two ways. Participants working at the NIH Bethesda campus will have blood drawn at the NIH Clinical Center. Other volunteers will participate in at-home blood sampling. Neoteryx, a medical device firm based in Torrance, California, will supply at-home blood collection kits. Researchers will ship each study participant a Mitra®Home Blood Collection Kit and provide detailed instructions on collecting a microsample of blood and mailing it back for future analysis in the laboratory.
“Researchers have considerable experience using these at-home blood collection kits to track the spread of other infectious diseases like influenza, and this method is safe, effective and easy-to-use,” said Kaitlyn Sadtler, Ph.D., study lead for laboratory testing and chief of NIBIB’s Section for Immunoengineering. “With a small finger-pick, volunteers can help scientists fight COVID-19 from their homes.”
People interested in joining this study should contact clinicalstudiesunit@nih.gov. For more information on the COVID-19 Pandemic Serum Sampling Study Launch, see the Questions and Answers. For more information on this study, please visit ClinicalTrials.gov using identifier NCT04334954. For more information on the U.S. government response to the COVID-19 pandemic, visit www.coronavirus.gov.
NIAID conducts and supports research — at NIH, throughout the United States, and worldwide — to study the causes of infectious and immune-mediated diseases, and to develop better means of preventing, diagnosing and treating these illnesses. News releases, fact sheets and other NIAID-related materials are available on the NIAID website.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
FDA quickly authorizes its second blood filtering device for COVID-19
Shortly after granting an emergency authorization to Terumo BCT’s blood filtering device for COVID-19, the FDA did the same for CytoSorbents’ system. Both are designed to strip out the immune system proteins that fuel the deadly cytokine-storm reactions associated with the disease.
Previously cleared for use in the European Union, the company’s CytoSorb purification system has been used to treat septic shock patients receiving intensive care, as well as those undergoing heart surgery or experiencing liver failure.
Now with the FDA’s blessing, the filters can be used in U.S. intensive care units for adults suffering from imminent respiratory failure, with acute lung injuries or severe COVID-19 disease.
Cytokine storms can cause severe inflammation, tissue damage and rapidly progressive shock, following a cascading release of white blood cells as the body overreacts to the coronavirus infection.
CytoSorbents describes its filters as “plug-and-play compatible” with most blood purification devices or pumps found in the ICU, such as dialysis hardware or the lung-supporting extracorporeal membrane oxygenation hardware known as ECMO machines.
“As a U.S.-based company with CytoSorb device manufacturing in New Jersey, we are eager to expand the availability of CytoSorb to U.S. hospitals and patients as a treatment option to fight cytokine storm and deadly inflammation that is believed to exacerbate COVID-19 infection,” said CytoSorbents CEO Philip Chan.
“With more than 555,000 documented coronavirus infections, the U.S. leads the world with over 22,000 deaths, and emergently needs new therapies to reduce the severity of this disease,” Chan added, as of early April 13. “This is important not just to reduce poor clinical outcomes and mortality, but to also alleviate the bottleneck for scarce resources such as ventilators and ECMO in the treatment of these critically ill patients.”
CytoSorb has previously been used in more than 80,000 treatments overseas to help treat the same kinds of complications seen in COVID-19, he said, as well as more than 200 patients with the infection itself. Its use has also been included in treatment guidelines in Italy, Panama, and China.
“Under the EUA, we plan to ramp the availability of CytoSorb in a controlled manner, to clinical centers that will work with us to generate data and leverage our knowledge of how to use the device most effectively,” Chan said.
Small Chloroquine Study Halted Over Risk of Fatal Heart Complications
A research trial of coronavirus patients in Brazil ended after patients taking a higher dose of chloroquine, one of the drugs President Trump has promoted, developed irregular heart rates.
Roughly half the study participants were given a dose of 450 milligrams of chloroquine twice daily for five days, while the rest were prescribed a higher dose of 600 milligrams for 10 days. Within three days, researchers started noticing heart arrhythmias in patients taking the higher dose. By the sixth day of treatment, 11 patients had died, leading to an immediate end to the high-dose segment of the trial.
The researchers said the study did not have enough patients in the lower-dose portion of the trial to conclude if chloroquine was effective in patients with severe disease. More studies evaluating the drug earlier in the course of the disease are “urgently needed,” the researchers said.
The role of laboratory parameters in screening of COVID-19 cases has not been definitely established. This study aimed to evaluate the accuracy of laboratory parameters in predicting cases with positive RT-PCR for COVID-19.
METHODS:
This diagnostic accuracy study was conducted on suspected COVID-19 patients, who presented to Behpooyan Clinic Medical center in Tehran (Iran) from 22 February to 14 March, 2020. Patients were divided into two groups based on the results of real time reverse transcriptase-polymerase chain reaction (RT-PCR) for COVID-19, and the accuracy of different laboratory parameters in predicting cases with positive RT-PCR was evaluated using area under the ROC curve (AUC).
RESULTS:
Two hundred cases with the mean age of 41.3± 14.6 (range: 19-78) years were studied (0.53% male). The result of RT-PCR for COVID-19 was positive in 70 (35%) cases. Patients with positive RT-PCR had significantly higher neutrophil (NEU) count (p = 0.0001), and C-reactive protein (CRP) (p = 0.04), lactate dehydrogenase (LDH) (p = 0.0001), aspartate aminotransferase (AST) (p = 0.001), alanine aminotransferase (ALT) (p = 0.0001), and Urea (p = 0.001) levels in serum. In addition, patients with positive RT-PCR had lower white blood cell (WBC) count (p = 0.0001) and serum albumin level (p = 0.0001) compared to others. ALT (AUC = 0.879), CRP (AUC = 0.870), NEU (AUC = 0.858), LDH (AUC = 0.835), and Urea (AUC = 0.835) had very good accuracy in predicting cases with positive RT-PCR for COVID-19, respectively.
CONCLUSION:
Our findings suggest that level of LDH, CRP, ALT and NEU can be used to predict the result of COVID-19 test. They can help in detection of COVID-19 patients.
Patients with positive COVID-19 had significantly higher neutrophil count CRP LDH AST ALT Urea levels in serum patients with positive COVID-19 had lower WBC count serum albumin level
CONCLUSION: Our findings suggest that level of LDH, CRP, ALT and NEU can be used to predict the result of COVID-19 test. They can help in detection of COVID-19 patients. https://ncbi.nlm.nih.gov/pubmed/32259132
4/13/2020
Pluristem Expands its Compassionate Use Program: Treated First COVID-19 Patient in U.S. Under FDA Single Patient Expanded Access Program
Cleared by FDA to proceed with the treatment in U.S. under Coronavirus Treatment Acceleration Program (CTAP)
Pluristem’s main focus: multinational clinical trial of PLX cells for treatment of complications associated with COVID-19
HAIFA, Israel, April13, 2020 – Pluristem Therapeutics Inc. (Nasdaq:PSTI) (TASE:PSTI), a leading regenerative medicine company developing a platform of novel biological therapeutic products, announced today that it has treated its first patient suffering from COVID-19 complications in the United States under the U.S. Food and Drug Administration’s (FDA) Single Patient Expanded Access Program, also called a compassionate use program, which is part of the U.S. Coronavirus Treatment Acceleration Program (CTAP), an emergency program for possible therapies that uses every available method to move new treatments to patients as quickly as possible.
The patient was treated with PLX cell therapy at Holy Name Medical Center in New Jersey, an acute care facility that is currently an active site for Pluristem’s Phase III critical limb ischemia (CLI) study. Prior to treatment with PLX, the patient was critically ill with respiratory failure due to acute respiratory distress syndrome (ARDS) and was under mechanical ventilation in an intensive care unit (ICU) for three weeks.
“We are receiving many inquiries and requests for treatment from healthcare providers and families worldwide. In parallel with our planned clinical trial, we expect to continue treating patients under compassionate use through the appropriate regulatory clearances in the United States and Israel, as well as expanding treatment under compassionate use in other countries. Our main focus remains however, the initiation of a multinational clinical study,” stated Pluristem CEO and President Yaky Yanay.
Pluristem’s main target is to initiate a multinational clinical trial as soon as possible for PLX cells in the treatment of patients suffering from complications associated with COVID-19. As the Company focus is the initiation of such clinical trial, it does not intend to provide further updates on the status of patients treated under compassionate use. Pluristem will update on the status and progress of its planned COVID-19 clinical trial program.
PLX Cells for COVID-19
PLX cells are available off-the-shelf and once commercialized, can be manufactured in large scale quantities, offering a key advantage in addressing a global pandemic. PLX cells are allogeneic mesenchymal-like cells that have immunomodulatory properties that induce the immune system’s natural regulatory T cells and M2 macrophages, and thus may prevent or reverse the dangerous overactivation of the immune system. Accordingly, PLX cells may potentially reduce the incidence and\or severity of COVID-19 pneumonia and pneumonitis leading hopefully to a better prognosis for the patients. Previous pre-clinical findings of PLX cells revealed therapeutic benefit in animal studies of pulmonary hypertension, lung fibrosis, acute kidney injury and gastrointestinal injury which are potential complications of the severe COVID-19 infection. Clinical data using PLX cells demonstrated the strong immunomodulatory potency of PLX cells in patients post major surgery. Taken together, PLX cells’ potential capabilities with the safety profile observed from clinical trials involving hundreds of patients worldwide potentially position them as a therapy for mitigating the tissue-damaging effects of COVID-19.
About Pluristem Therapeutics
Pluristem Therapeutics Inc. is a leading regenerative medicine company developing novel placenta-based cell therapy product candidates. The Company has reported robust clinical trial data in multiple indications for its patented PLX cell product candidates and is currently conducting late stage clinical trials in several indications. PLX cell product candidates are believed to release a range of therapeutic proteins in response to inflammation, ischemia, muscle trauma, hematological disorders and radiation damage. The cells are grown using the Company’s proprietary three-dimensional expansion technology and can be administered to patients off-the-shelf, without tissue matching. Pluristem has a strong intellectual property position; a Company-owned and operated GMP-certified manufacturing and research facility; strategic relationships with major research institutions; and a seasoned management team.
Subject: Fwd: Pluristem Expands its Compassionate Use Program: Treated First COVID-19 Patient in U.S. Under FDA Single Patient Expanded Access Program
4/11/2020
The C.D.C. has recommended that all Americans wear cloth masks if they go out in public. This is a shift in federal guidance reflecting new concerns that the coronavirus is being spread by infected people who have no symptoms. Until now, the C.D.C., like the W.H.O., has advised that ordinary people don’t need to wear masks unless they are sick and coughing. Part of the reason was to preserve medical-grade masks for health care workers who desperately need them at a time when they are in continuously short supply. Masks don’t replace hand washing and social distancing.
A select group of healthy Philadelphia-area volunteers will receive an experimental vaccine against the coronavirus, Inovio Pharmaceuticals of Plymouth Meeting said Monday. Inovio, which began work on its vaccine in January soon after Chinese authorities published the microbe’s genetic code, said the U.S. Food and Drug Administration had given the go-ahead to test it in humans. The study will enroll up to 40 volunteers, split between two sites: the University of Pennsylvania’s Perelman School of Medicine and the Center for Pharmaceutical Research in Kansas City, Mo. Human tests have begun on at least one other vaccine candidate, made by Cambridge, Mass.-based Moderna Inc., but most of the several dozen vaccines in development have not reached that stage. Screening of potential participants for the Inovio vaccine already has started at the Kansas City site, company officials said. Each volunteer will receive two doses of the vaccine, spaced four weeks apart. A primary goal is to make sure the vaccine, for now called INO-4800, does not cause any adverse effects. Researchers also will analyze blood samples from participants to make sure their immune systems are generating an appropriate response. The vaccine volunteers are not being exposed to the virus, at least not on purpose. But separately, scientists are doing that in animal studies. Several dozen labs and companies are at work on vaccines worldwide; none is expected to be ready before next year.
4/5/2020
Recombinant Coronavirus Vaccines Delivered via Microneedle Array
THE DRUG IS DELIVERED THROUGH A BAND-AID-LIKE PATCH — NOT A NEEDLE.
BY VICTOR TANGERMANN / 9 HOURS AGO
Researchers at the University of Pittsburgh School of Medicine announced today that they have developed a promising new COVID-19 vaccine candidate.
Early animal trials have shown promise so far, but human trials are still in the planning stages. The researchers already had a big leg up from past epidemics.
“We had previous experience on SARS-CoV in 2003 and MERS-CoV in 2014,” said Andrea Gambotto, co-senior author of the peer-reviewed paper published in the journal EBioMedicine, and associate professor of surgery at the Pittsburgh School of Medicine, in a statement.
“These two viruses, which are closely related to SARS-CoV-2, teach us that a particular protein, called a spike protein, is important for inducing immunity against the virus,” Gambotto explained. “We knew exactly where to fight this new virus.”
The vaccine dubbed “PittCoVacc” (Pittsburgh Coronavirus Vaccine) works in the same basic way as a flu shot: By injecting lab-made pieces of viral protein into the body to help it build an immunity.
When tested in mice, the researchers found that the number of antibodies capable of neutralizing the deadly SARS-CoV-2 virus surged two weeks after delivery.
Instead of being delivered through a needle, the new drug is administered through a microneedle array, a Band-Aid like patch made up of 400 tiny microneedles. Once the patch is applied, the microneedles, which are made entirely of sugar and protein dissolve, leaving no trace behind.
“We developed this to build on the original scratch method used to deliver the smallpox vaccine to the skin, but as a high-tech version that is more efficient and reproducible patient to patient,” said co-senior author Louis Falo, professor and chair of dermatology at Pitt’s School of Medicine, in the statement. “And it’s actually pretty painless — it feels kind of like Velcro.”
According to the researchers, these patches can be easily manufactured in massive “cell factories” at an industrial scale. The vaccine doesn’t even need to be refrigerated during storage or transport — a massive complication for other vaccines.
“For most vaccines, you don’t need to address scalability to begin with,” Gambotto said. “But when you try to develop a vaccine quickly against a pandemic that’s the first requirement.”
Before starting human trials, the researchers are currently applying for drug approval from the US Food and Drug Anticipation.
“Testing in patients would typically require at least a year and probably longer,” Falo said. “This particular situation is different from anything we’ve ever seen, so we don’t know how long the clinical development process will take.”
Tweets and Retweets @ COVID-19 and AI: A Virtual Conference – Human-Centered Artificial Intelligence Institute, Stanford University, 4/1/2020, 9AM PST – 3:30PM PST @StanfordHAI BY @pharma_BI and @AVIVA1950
Subject: New Guidance on Management of Acute CVD During COVID-19
UPDATED on 3/31/2020
The Mathematics of Predicting the Course of the Coronavirus
Epidemiologists are using complex models to help policymakers get ahead of the Covid-19 pandemic. But the leap from equations to decisions is a long one.
THE BASIC MATH of a computational model is the kind of thing that seems obvious after someone explains it. Epidemiologists break up a population into “compartments,” a sorting-hat approach to what kind of imaginary people they’re studying. A basic version is an SIR model, with three teams: susceptible to infection, infected, and recovered or removed (which is to say, either alive and immune, or dead). Some models also drop in an E—SEIR—for people who are “exposed” but not yet infected. Then the modelers make decisions about the rules of the game, based on what they think about how the disease spreads. Those are variables like how many people one infected person infects before being taken off the board by recovery or death, how long it takes one infected person to infect another (also known as the interval generation time), which demographic groups recover or die, and at what rate. Assign a best-guess number to those and more, turn a few virtual cranks, and let it run.
“At the beginning, everybody is susceptible and you have a small number of infected people. They infect the susceptible people, and you see an exponential rise in the infected,” says Helen Jenkins, an infectious disease epidemiologist at the Boston University School of Public Health. So far, so terrible.
The assumption for how big any of those fractions of the population are, and how fast they move from one compartment to another, start to matter immediately. “If we discover that only 5 percent of a population have recovered and are immune, that means we’ve still got 95 percent of the population susceptible. And as we move forward, we have much bigger risk of flare-ups,” Jenkins says. “If we discover that 50 percent of the population has been infected—that lots of them were asymptomatic and we didn’t know about them—then we’re in a better position.”
So the next question is: How well do people transmit the disease? That’s called the “reproductive number,” or R0, and it depends on how easily the germ jumps from person to person—whether they’re showing symptoms or not. It also matters how many people one of the infected comes into contact with, and how long they are actually contagious. (That’s why social distancing helps; it cuts the contact rate.) You might also want the “serial interval,” the amount of time it takes for an infected person to infect someone else, or the average time before a susceptible person becomes an infected one, or an infected person becomes a recovered one (or dies). That’s “reporting delay.”
And R0 really only matters at the beginning of an outbreak, when the pathogen is new and most of the population is House Susceptible. As the population fractions change, epidemiologists switch to another number: the Effective Reproductive Number, or Rt, which is still the possible number of people infected, but can flex and change over time.
SOURCES
More From WIRED on Covid-19
It’s time to do the things you keep putting off. Here’s how
A commentary in Mbio/ Hiding in :Plain Sight: an Approach to Treating Patients with Severe COVID-19 Infection
Hiding in Plain Sight: an Approach to Treating Patients with Severe COVID-19 Infection
David S. Fedson,a Steven M. Opal,b Ole Martin Rordamc
a57, chemin du Lavoir, Sergy Haut, France
bDepartment of Medicine, Warren Alpert Medical School of Brown University, Providence, Rhode Island, USA
cFyordgata 59, Trondheim, Norway
ABSTRACT
Patients with COVID-19 infection are at risk of acute respiratory disease syndrome (ARDS) and death. The tissue receptor for COVID-19 is ACE2, and higher levels of ACE2 can protect against ARDS. Angiotensin receptor blockers and statins upregulate ACE2. Clinical trials are needed to determine whether this drug combination might be used to treat patients with severe COVID-19 infection.
The severe respiratory disease that has recently emerged in China is caused by a novel coronavirus (COVID-19) (1). The virus is similar to the SARS coronavirus that spread internationally in 2003, infected more than 8,000 people, and killed almost 800. Infection with COVID-19 has now spread throughout the world, causing widespread social and economic disruption. To control its spread, Chinese officials have imposed extensive travel bans and quarantined large areas. Accelerated development of new vaccines and treatments is already under way. It is too early to know whether any of these efforts will contain the outbreak.
Thus far, patients hospitalized with severe COVID-19 infection have had pneumonia (2). Of 44,672 laboratory-confirmed patients, almost 5% have had critical illness and almost 50% of critically ill patients have died (3). The overall case fatality rate (2.3%) has been higher than that seen with seasonal influenza. Most deaths have involved older adults, many of whom have had underlying chronic illnesses. Although there is no known treatment for any coronavirus infection, investigators in China have undertaken several clinical trials. Except for corticosteroids, all of the drugs being tested target coronavirus replication. Unfortunately, very few of these antiviral drugs will be available to people who have been (or will be) infected with COVID-19. Yet, for those who develop severe disease, only one question matters: “will I live or die?” This is the question that clinical investigators should address. Could they discover a treatment that might reduce the severity of COVID-19 infection and improve patient survival?
In 2014, one of us suggested that statins might be used to treat patients with Ebola virus disease (4). A supply of a generic statin and a generic angiotensin receptor blocker (ARB) was sent to Sierra Leone. Experimental studies had shown that both drugs improved outcomes in experimental acute lung injury/acute respiratory disease syndrome (ARDS) (5–9). In Sierra Leone, local physicians treated approximately 100 Ebola patients with a combination of the two drugs. They noted “remarkable improvement” in survival. Although there was no support for a proper clinical trial, the findings from this unconventional and poorly documented treatment experience were published (10, 11). During the current Ebola outbreak in the Democratic Republic of the Congo (DRC), expensive vaccines are being used. Investigational monoclonal antibody preparations (12), but not inexpensive generic drug treatments (13), have been tested.
20 March 2020 preliminary signs that the DRC outbreak is coming under control, although the case
fatality rate is still 66%.
An approach to treating patients with severe COVID-19 infection might be hiding in plain sight. The tissue receptor for the virus is ACE2, which is also the receptor for the SARS coronavirus (1). Several years ago, investigators in the Netherlands and elsewhere showed that ARBs and statins upregulate the activity of ACE2 (14, 15), and higher levels of ACE2 are associated with a reduced severity of ARDS (16). Both statins and ARBs target the host response to infection, not the virus (9). They act largely (although not exclusively) on endothelial dysfunction, which is a common feature of many virus infections (17). Both drugs counter endothelial dysfunction by affecting the ACE2/ angiotensin-(1–7)/Mas and angiopoietin/Tie-2 signaling axes (9). Combination treatment with these two drugs appears to accelerate a return to homeostasis, allowing patients to recover on their own.
The host response is a major determinant of the pathogenesis of infectious diseases (18). We believe that investigators in China and elsewhere should undertake studies of patients with severe COVID-19 infection to determine whether targeting the host response with widely available and inexpensive generic drugs, like ARBs and statins, will improve their chances of survival. The studies would not have to be large; a successful clinical trial might require only 100 patients (9). Convincing evidence of the effectiveness of this treatment would suggest a syndromic approach to treating patients with other emerging infectious diseases, like Ebola and pandemic influenza, as well as everyday illnesses, like sepsis and pneumonia (19). The long-term benefits of these findings for global public health could be immense.
ACKNOWLEDGMENT
We declare no conflicts of interest. No funding was provided to support the
preparation of this article.
REFERENCES
1. Chen Y, Liu Q, Guo D. 2020. Emerging coronaviruses: genome structure,
replication, and pathogenesis. J Med Virol 92:418–423. https://doi.org/
10.1002/jmv.25681.
2. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z,
Xiong Y, Zhao Y, Li Y, Wang X, Peng Z. 7 February 2020. Clinical
characteristics of 138 hospitalized patients with 2019 novel coronavirusinfected
It is hard to think of a moment in the recent history of the University of California – or, indeed, in the history of our nation – as challenging and complex as this one. Across the country, normal life has been severely impacted by COVID-19. Our university community is feeling the stress and strain of this global pandemic, and my thoughts are constantly with the patients, students, faculty, and staff who are most affected. We will continue to do all that we can to protect and support our community.
In times like these, UC’s public service mission comes into sharp focus, and I couldn’t be more proud of how our community is stepping up to the challenges at hand: UC clinicians are on the front lines of this crisis treating patients; our researchers are hard at work fighting coronavirus on multiple fronts; UC students have quickly transitioned to online classes and remote study groups, all while navigating the complexities of campus shutdowns; and our faculty and staff have adopted new teaching methods and platforms in the face of the unprecedented suspension of in-classroom instruction.
Below, you can learn even more about UC’s leadership in facing the threat of COVID-19. I want to thank everyone across the University who is going the extra mile in their work, in their studies, and in simply looking out for each other and coming together as a community during a difficult time. UC has been here for its students, faculty, and staff – and for all Californians – since our founding more than 150 years ago. And the University will be here, stronger than ever, long after we emerge from this crisis together. May you all be well, and Fiat Lux.
Yours very truly,
UC medical centers launch in-house coronavirus testing and clinical trials
As has been widely reported, the ability of U.S. health providers to test and treat patients for coronavirus has lagged. Academic medical centers in California – including UC – are stepping up to help meet that challenge.
All five UC medical centers are ramping up their in-house testing while seeking commercial partnerships that will help expand our testing capacity. Meanwhile, physician scientists at UC San Diego Health, UC San Francisco, UC Irvine Health and UC Davis Health have launched a new clinical trial to assess the safety and effectiveness of an existing antiviral drug on COVID-19.
We have a long way to go, but I’m heartened by the efforts of scientists and medical professionals across California’s academic medical centers to ensure the public will be able to get the care they need.
UC experts take on COVID-19
We can face the COVID-19 threat more effectively by understanding it better. UC researchers are always working to put the best evidence-based research into the hands of decision-makers. This is no different with coronavirus – as always, UC’s research enterprise is on the front lines. Here are just a few examples:
A team of engineers and physicians at UC San Diego are developing simple, ready-to-use ventilators that can be quickly deployed to support patients in a crisis.
Lawrence Livermore and Los Alamos National Laboratories are leading members of a new national consortium that will use U.S. supercomputing resources to help scientists answer complex scientific questions about the virus in hours or days, rather than weeks or months.
A team of researchers at UC Riverside, the University of Chicago, the U.S. Department of Energy’s Argonne National Laboratory, and Northwestern University have mapped a key protein that may aid in the development of a COVID-19 vaccine.
UCLA researchers published a new study explaining how long the COVID-19 virus remains active on surfaces like cardboard, metal, and plastic.
UC San Diego physician scientist David Pride published a helpful explainer about the state of COVID-19 testing in the United States – and how UC’s academic medical centers are stepping up to develop tests that will help public health officials mitigate the spread of the virus.
UC joins together to fight the pandemic
I’ve been inspired by stories of UC students, faculty, staff, and donors who are rising to the occasion and finding creative ways to help each other in this time of crisis. This demonstrates the power of our community.
Scientists at the Innovative Genomics Institute – a partnership between UCSF and UC Berkeley and the Chan Zuckerberg Biohub – are helping one another find necessary equipment, re-agents, and volunteers to expand clinical COVID-19 testing on our campuses. The UCSF Institute for Nursing Excellence has held dozens of training sessions for UC Health staff and nurses on best practices for managing coronavirus patients. Meanwhile, medical students at UCSF have kindly volunteered to support health care workers by providing free childcare and running errands in the midst of the coronavirus response.
Generous donors have rallied to support UCSF doctors and scientists working to address COVID-19, giving more than $12 million to help UCSF respond to the pandemic. (Have resources or medical supplies to contribute? UCSF and UC San Diego Health are accepting donations.) Hundreds of donors have also contributed to UCLA’s Bruin Tech Awardfund, which provides an award of up to $1,000 to UC students who may not have the technology needed to access online classes.
We can all take immense pride in the outstanding people working diligently every single day at UC’s medical centers to take care of patients in this uniquely challenging time, whether they are health professionals, or those sanitizing our facilities and providing nourishing food.
Managing anxiety about coronavirus
Many UC experts have shared good advice about taking care of your mental health during a time of increased stress. UC San Diego and UCSF have compiled dozens of tips and resources designed to alleviate the mental and emotional strain many of us are feeling.
UC Berkeley’s Greater Good Magazine also shared eight acts of goodness amid the COVID-19 outbreak that could brighten your day. (Seeing penguins roaming a shuttered Chicago aquarium certainly made me smile.)
WHAT’S ON YOUR MIND
Recently I was asked:
Many of us are at home practicing social distancing. Any recommendations on how to keep busy and entertained?
Here are my thoughts:
First, I want to thank everyone who is practicing social distancing to help halt the spread of COVID-19. This is a crucial step to keep our communities safe, including our own medical and health center staff who are on the front lines of fighting this virus.
While you’re distancing, I recommend picking up a good book! I just started reading The Mirror & the Lightby Hilary Mantel. It’s the third and final volume in her fictional recounting of the life of Thomas Cromwell. The first two volumes were terrific, combining both literary and historical fiction. I’m already entranced by the third.
For nonfiction, I’m reading These Truths: A History of the United Statesby Jill Lepore. She’s a wonderful writer and an astute historian with keen insights into what has made our country what it is today.
When I’m tired of reading, there’s always Netflix. I can return to Cromwell’s era and watch “The Tudors.” Or, for a complete change of pace, I can stream “Better Call Saul.”
Like everyone else, I’m doing my best to entertain myself while working from home. Thank goodness for modern technology, which helps us all stay connected during these difficult times. But as the Brits would say, we will keep calm and carry on.
UPDATED ON 3/29/2020
Mayo Clinic, Amazon, others launch collaboration to increase COVID-19 testing, vaccine development
The COVID-19 Healthcare Coalition plans to leverage the strengths of healthcare organizations, technology companies, non-profits, academia, and startups to provide a focused response to the coronavirus outbreak. (Mayo Clinic)
An industry coalition of health systems, tech giants and healthcare vendors are collaborating to increase COVID-19 testing and coordinate early therapies.
The private industry effort, spearhead by Mayo Clinic’s John Halamka, M.D. and other industry leaders, plans to leverage the strengths of healthcare organizations, technology companies, non-profits, academia, and startups to provide a focused response to the coronavirus outbreak.
“Each coalition member is bringing its unique assets, sharing resources and plans, and working together to support those on the front lines in responding to COVID-19,” the COVID-19 Healthcare Coalition said in a press release.
The idea behind the effort is to crowdsource capabilities from the private sector and use data analytics and evidence-based decisions to respond to the health crisis. The coalition is seeking more industry partners to help share best practices.
Coalition members include big tech companies Amazon Web Services (AWS), Microsoft and Salesforce as well as healthcare technology vendors Arcadia.io, athenahealth, Buoy Health, Epic, and nference.
Health systems involved include HCA Healthcare, Intermountain Healthcare, Rush University System for Health, and the University of California Healthcare System.
Other industry partners are MITRE, LabCorp, Leavitt Partners, CommonWell Health Alliance, and MassChallenge.
Mitre, a national research and development center, will serve as a program manager to facilitate communication, aggregate de-identified data, from clinical insights to resource requirements like beds and ventilators, and coordinate the response across a range of organizations.
“Pandemics stress our healthcare delivery system. We are now familiar with the generalized public health measures that help contain the spread of infectious disease including social distancing, hand washing, self-quarantine, cancellation of large public events, and school closures. More targeted measures are needed and that requires coordination,” Halamka, M.D., president of Mayo Clinic Platform, wrote in a blog post.
The coalition has started focused efforts to increase COVID-19 testing capacity for the country, to coordinate early therapies, and to accelerate vaccine development, Halamka said.
“Our first task is to share learnings and encourage innovation across the coalition. We’re moving fast to support technology and policy innovations,” he wrote.
Jay Schnitzer, M.D., Mitre’s chief technology and medical officer, said applying real-time data analytics and best practice guidance to a pandemic can flatten the curve of infection and change its course, as seen with Ebola and H1N1.
“The business and research communities have mobilized to address COVID-19 and give this data analysis to the healthcare system leaders and public health officials to make evidence-based decisions that can save lives,” Schnitzer said.
The coalition set up several guiding principles: No organization will get paid for the coalition work or receive preferential advantage and each organization cooperates and openly shares their plans.
The collaborative effort plans to use data and evidence to inform decisions on people at risk of COVID-19 exposure who need diagnostic testing and healthcare delivery systems with a focus on staff, space, and supply chain.
The Global Impact of COVID-19 and Strategies for Mitigation and Suppression
Page 2 of 19
Summary
The world faces a severe and acute public health emergency due to the ongoing COVID-19 global pandemic. How individual countries respond in the coming weeks will be critical in influencing the trajectory of national epidemics. Here we combine data on age-specific contact patterns and COVID-19 severity to project the health impact of the pandemic in 202 countries. We compare predicted mortality impacts in the absence of interventions or spontaneous social distancing with what might be achieved with policies aimed at mitigating or suppressing transmission. Our estimates of mortality and healthcare demand are based on data from China and high-income countries; differences in underlying health conditions and healthcare system capacity will likely result in different patterns in low income settings.
We estimate that in the absence of interventions, COVID-19 would have resulted in 7.0 billion infections and 40 million deaths globally this year. Mitigation strategies focussing on shielding the elderly (60% reduction in social contacts) and slowing but not interrupting transmission (40% reduction in social contacts for wider population) could reduce this burden by half, saving 20 million lives, but we predict that even in this scenario, health systems in all countries will be quickly overwhelmed. This effect is likely to be most severe in lower income settings where capacity is lowest: our mitigated scenarios lead to peak demand for critical care beds in a typical low-income setting outstripping supply by a factor of 25, in contrast to a typical high-income setting where this factor is 7. As a result, we anticipate that the true burden in low income settings pursuing mitigation strategies could be substantially higher than reflected in these estimates.
Our analysis therefore suggests that healthcare demand can only be kept within manageable levels through the rapid adoption of public health measures (including testing and isolation of cases and wider social distancing measures) to suppress transmission, similar to those being adopted in many countries at the current time. If a suppression strategy is implemented early (at 0.2 deaths per 100,000 population per week) and sustained, then 38.7 million lives could be saved whilst if it is initiated when death numbers are higher (1.6 deaths per 100,000 population per week) then 30.7 million lives could be saved. Delays in implementing strategies to suppress transmission will lead to worse outcomes and fewer lives saved.
We do not consider the wider social and economic costs of suppression, which will be high and may be disproportionately so in lower income settings. Moreover, suppression strategies will need to be maintained in some manner until vaccines or effective treatments become available to avoid the risk of later epidemics. Our analysis highlights the challenging decisions faced by all governments in the coming weeks and months, but demonstrates the extent to which rapid, decisive and collective action now could save millions of lives.
SOURCE
26 March 2020 Imperial College, COVID-19 Response Team
Patrick GT Walker, Charles Whittaker, Oliver Watson et al. The Global Impact of COVID-19 and Strategies for Mitigation and Suppression. WHO Collaborating Centre for Infectious Disease Modelling, MRC Centre for Global Infectious Disease Analysis, Abdul Latif Jameel Institute for Disease and Emergency Analytics, Imperial College London (2020) doi: missing
Imperial College COVID-19 Response Team
WHO Collaborating Centre for Infectious Disease Modelling MRC Centre for Global Infectious Disease Analysis Abdul Latif Jameel Institute for Disease and Emergency Analytics Imperial College London
Subject: Re: ACC issues COVID-19 guidance for cardiologists
Dear colleagues:
I understand the serious blunder of our not having sufficient testing for Coronavirus in patients who need it. In the meantime, I am unable to understand that the hematology panel routinely widely available isn’t recommended as a necessary first step. Maybe I see this from a long career in clinical laboratory science.
The most important feature early on is a characteristic depression of the lymphocyte count, and perhaps an increase in the eosinophil count. That would be consistent in patients who might need the virus identification.
Larry H. Bernstein, MD, FCAP
This illustration, created at the Centers for Disease Control and Prevention (CDC), reveals ultrastructural morphology exhibited by coronaviruses. Note the spikes that adorn the outer surface of the virus, which impart the look of a corona surrounding the virion, when viewed electron microscopically. A novel coronavirus virus was identified as the cause of an outbreak of respiratory illness first detected in Wuhan, China in 2019.
Pinpoint Science Inc., Pinpoint Covid-19 Screening Assay – Electrical detection of SARS-CoV-2 nucleocapsid protein using nanosensors and aptamer (proof of concept) Contact
Coronavirus Disease (COVID-19): Pathophysiology, Epidemiology, Clinical Management and Public Health Response
An outbreak of a respiratory disease began in Wuhan, China in December 2019 and the causative agent was discovered in January 2020 to be a novel betacoronovirus of the same subgenus as SARS-CoV and named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Coronavirus disease 2019 (COVID-19) has rapidly disseminated worldwide, with clinical manifestations ranging from mild respiratory symptoms to severe pneumonia and a fatality rate estimated around 2%. Person to person transmission is occurring both in the community and healthcare settings. The World Health Organization (WHO) has recently declared the COVID-19 epidemic a public health emergency of international concern.
The ongoing outbreak presents many clinical and public health management challenges due to limited understanding of viral pathogenesis, risk factors for infection, natural history of disease including clinical presentation and outcomes, prognostic factors for severe illness, period of infectivity, modes and extent of virus inter-human transmission, as well as effective preventive measures and public health response and containment interventions. There are no antiviral treatment nor vaccine available but fast track research and development efforts including clinical therapeutic trials are ongoing across the world.
Managing this serious epidemic requires the appropriate deployment of limited human resources across all cadres of health care and public health staff, including clinical, laboratory, managerial and epidemiological data analysis and risk assessment experts. It presents challenges around public communication and messaging around risk, with the potential for misinformation and disinformation. Therefore, integrated operational research and intervention, learning from experiences across different fields and settings should contribute towards better understanding and managing COVID-19.
This Research Topic aims to highlight interdisciplinary research approaches deployed during the COVID-19 epidemic, addressing knowledge gaps and generating evidence for its improved management and control. It will incorporate critical, theoretically informed and empirically grounded original research contributions using diverse approaches, experimental, observational and intervention studies, conceptual framing, expert opinions and reviews from across the world. The Research Topic proposes a multi-dimensional approach to improving the management of COVID-19 with scientific contributions from all areas of virology, immunology, clinical microbiology, epidemiology, therapeutics, communications as well as infection prevention and public health risk assessment and management studies.
Submissions are welcome for the following article types: original research, review, mini-reviews, systematic reviews, research protocol, opinion and hypothesis. We particularly welcome contributions that include, but are not limited to, the following topics:
• SARS-CoV-2 genome structure, encoded proteins, replication properties, viral pathogenesis, comparative phylogenetic and viral receptor binding analysis within the betacoronavirus genus, e.g. SARS-CoV, MERS-CoV; • SARS-CoV-2 antiviral susceptibility and antigen diversity; • Natural history of COVID-19 clinical disease spectrum in different populations and analysis of intrinsic and extrinsic prognostic factors, including sero-epidemiological studies in the general population; • Host factors, including host genetics and immunological variabilities, and their association with disease severity; • Modes and dynamics of SARS-CoV-2 transmission in the household, workplace, closed community and healthcare settings, including the role of super-spreading events; • Systematic reviews and meta-analysis of COVID-19 epidemiological studies and surveillance data as well as modeling studies and analytical methods for risk assessment studies; • Effectiveness of COVID-19 infection prevention and control procedures including personal protective equipment and airborne/aerosol versus droplet isolation precautions for specific healthcare settings and epidemiological stages of the outbreak; • Effectiveness of novel public health interventions for containment or impact mitigation of the COVID-19 outbreak, including social distancing and quarantine measures; • Clinical accuracy and effectiveness of rapid SARS-CoV-2 diagnostics and serological assays; • Pre-clinical development and clinical trials of therapeutic agents for COVID-19; • Pre-clinical development and clinical trials of COVID-19 candidate vaccines; • Evaluation of methods for COVID-19 epidemiological surveillance, contact tracing studies and public health risk assessment, including digital health solutions and modeling/forecasting studies; • Clinical immunology of COVID-19, including specific antibody and cellular immune responses to SARS-CoV-2 and protective immunity. • Challenges and the potential for communication, including social media, social distancing, and ‘community spread • Community, culture, and technology-based interventions.
As this is a multidisciplinary Research Topic, we ask the authors to choose the appropriate Topic Editor for sections upon submission. For any questions please contact the editorial office (publichealth@frontiersin.org).
***Due to the exceptional nature of the COVID-19 situation, Frontiers is waiving all article publishing charges for COVID-19 related research.***
Keywords: Coronavirus, microbiology, immunology, public health, communication, risk, social media, community understanding, COVID-19, SARS-CoV-2, infection prevention and control, epidemiology, transmission studies, antiviral therapy
Important Note: All contributions to this Research Topic must be within the scope of the section and journal to which they are submitted, as defined in their mission statements. Frontiers reserves the right to guide an out-of-scope manuscript to a more suitable section or journal at any stage of peer review.
At 4 pm E.S.T. President Trump and the White House announced, after a meeting with members of the Coronavirus Task Force, that social distancing guidelines should be extended to April 30, 2020 in order to stem the rise in COVID-19 cases.
During a briefing Sunday afternoon, Trump said with the peak of the disease to hit sometime in the next two weeks and extending the guidelines will slow the spread of the virus.
“The better you do, the faster this whole nightmare will end,” he said.
The federal guidelines recommend against large group gatherings and urge older people and anyone with existing health problems to stay home. People are urged to work at home when possible and avoid restaurants, bars, non-essential travel and shopping trips.
The U.S. had more than 139,000 COVID-19 cases reported by Sunday evening, with more than 2,400 deaths. During the course of the Rose Garden briefing, reported deaths grew by several dozen and the number of cases by several thousand.
One in 3 Americans remain under state or local government orders to stay at home to slow the spread of the virus, with schools and businesses closed and public life upended.
Dr. Anthony Fauci, speaking on CNN’s “State of the Union” on Sunday, offered his prognosis as the federal government weighs rolling back guidelines on social distancing in areas that have not been as hard-hit by the outbreak at the conclusion of the nationwide 15-day effort to slow the spread of the virus.
“I would say between 100,000 and 200,000 cases,” he said, correcting himself to say he meant deaths. “We’re going to have millions of cases.” But he added “I don’t want to be held to that” because the pandemic is “such a moving target.”
What the hell is going on with coronavirus testing in the US?
The country is woefully behind where it should be, and that’s going to make it much harder to track and curtail the coronavirus’s spread.
March 25, 2020
Coronavirus is forcing a trade-off between privacy and public health
The crisis has governments and companies scrambling to decide when it’s appropriate to lift data privacy protections and AI ethics guidelines.
March 24, 2020
Your biggest questions about coronavirus, answered
Battling the spread of Covid-19 is going to be a long-haul effort. Here’s what you asked us.
March 19, 2020
Warmer weather could slow the spread of coronavirus—but not by much
Several initial analyses of transmission data suggest the pandemic could ease up in summer. But that doesn’t reduce the need for measures like social distancing.
March 19, 2020
We need more ventilators. Here’s what it will take to get them.
Manufacturers need fast-track regulatory approvals and government contracts. STAT.
March 18, 2020
This blood test can tell us how widespread coronavirus really is
A test can see if a person has ever been infected, even if they had no symptoms.
March 18, 2020
What is herd immunity and can it stop the coronavirus?
Once enough people get Covid-19, it will stop spreading on its own. But the costs will be devastating.
March 17, 2020
A new app would say if you’ve crossed paths with someone who is infected
Private Kit: Safe Paths shares information about your movements in a privacy-preserving way—and could let health officials tackle coronavirus hot spots.
March 17, 2020
We’re not going back to normal
Social distancing is here to stay for much more than a few weeks. It will upend our way of life, in some ways forever.
March 17, 2020
Amazon is hiring 100,000 new workers in the US to deal with the coronavirus boom
The hiring spree is to cope with an unprecedented surge in demand for online deliveries during the outbreak.
March 17, 2020
Here’s how social media can combat the coronavirus ‘infodemic’
With millions on lockdown, Facebook and Twitter are major sources of Covid-19 news. They’re also where misinformation thrives. How can platforms step up?
March 17, 2020
Over 24,000 coronavirus research papers are now available in one place
The data set aims to accelerate scientific research that could fight the Covid-19 pandemic.
March 16, 2020
US coronavirus testing is slowly ramping up, but way too late
Private and academic labs are rushing to fill the void left by CDC’s mistakes, hoping to slow the deadly pandemic in the US.
March 13, 2020
This is how the CDC is trying to forecast coronavirus’s spread
It has tapped one of the nation’s best flu-forecasting labs to retool its prediction algorithms for the Covid-19 pandemic.
March 13, 2020
Worst-case coronavirus scenario: 214 million Americans infected, 1.7 million dead
The worst-case figures are what would happen if no action is taken to slow the virus, which spreads person to person.
March 13, 2020
No, coronavirus is not a good argument for quitting cash
Though it’s theoretically possible, there is no evidence that physical money—or any inanimate surface, for that matter—helps the virus spread.
March 12, 2020
How to practice social distancing during the coronavirus pandemic
Not everyone can work from home or cease traveling. Here’s what you can do when circumstance forces you to be out and about during the COVID-19 outbreak.
March 13, 2020
Singapore is the model for how to handle the coronavirus
The key features: quick action, extensive testing, and relentless tracking.
March 12, 2020
AI could help with the next pandemic—but not with this one
Some things need to change if we want AI to be useful next time, and you might not like them.
March 12, 2020
Here’s how long the coronavirus can live in the air and on packages
The virus prefers steel and plastic, materials commonly found in hospitals and homes.
March 11, 2020
Chinese hackers and others are exploiting coronavirus fears for cyber espionage
Headline news and global disorder are tools hackers take advantage of to make their next breach.
March 12, 2020
Why the coronavirus outbreak is terrible news for climate change
It’ll sap funding and political will—but actually, it should.
March 9, 2020
China’s travel lockdown sharply slowed the global spread of Covid-19
March 6, 2020
A coronavirus vaccine will take at least 18 months—if it works at all
A fast-track vaccine will be tried on people soon but it uses an unproven technology.
March 10, 2020
The best, and the worst, of the coronavirus dashboards
There are dozens of sites that show you how coronavirus is spreading around the world. Here is our ranking.
March 6, 2020
South Korea is watching quarantined citizens with a smartphone app
Thousands in coronavirus lockdown will be monitored for symptoms—and tracked to make sure they stay at home and don’t become “super spreaders.”
March 6, 2020
Why the CDC botched its coronavirus testing
The first testing kits from the Centers for Disease Control had a simple fault, and red tape prevented other labs from creating their own.
March 5, 2020
Gene sleuths are tracking the coronavirus outbreak as it happens
Genetic data shows that countries are getting hit with multiple introductions of the virus.
March 4, 2020
How coronavirus turned the “dystopian joke” of FaceID masks into a reality
Thousands ordered masks that let them unlock their phones during outbreaks. But this viral art project doesn’t just work with surveillance technology—it works against it, too.
February 29, 2020
How to prepare for the coronavirus like a pro
Some of the smartest people I know are getting ready for a crisis—including me.
February 28, 2020
What are the best coronavirus treatments?
Here’s a list of promising drugs being tried on people infected with the virus.
February 25, 2020
Biologists rush to re-create the China coronavirus from its DNA code
Synthetic versions of the deadly virus could help test treatments. But what are the risks when viruses can be synthetized from scratch?
February 15, 2020
China’s coronavirus app could have unintended consequences
Tracking people to tell them whether they’ve been in close contact with a virus carrier might cause a whole new series of complicated issues.
February 13, 2020
The coronavirus is the first true social-media “infodemic”
Social media has zipped information and misinformation around the world at unprecedented speeds, fueling panic, racism … and hope.
February 12, 2020
This is what happens when you get the coronavirus
Hospitals in China are reporting their experiences with hundreds of patients so far.
February 11, 2020
Satellite images show how coronavirus brought Wuhan to a standstill
Photos taken from space show how little activity there is in Wuhan since China shut down all transportation in the city of 11 million people.
February 6, 2020
Meet the Chinese crowdsourcers fighting coronavirus censorship
Faced with information suppression and untrustworthy news, citizens in China and Hong Kong do their best to chronicle the coronavirus outbreak and sift fact from fiction.
Scientists from the University of Oxford’s Engineering Science Department and the Oxford Suzhou Centre for Advanced Research (OSCAR) have developed a rapid testing technology for the novel corona virus SARS-CoV-2 (COVID-19).
The team, led by Prof. Zhanfeng Cui and Prof. Wei Huang, have been working to improve test capabilities as the virus spreads internationally.
The new test is much faster and does not need a complicated instrument. Previous viral RNA tests took 1.5 to 2 hours to give a result. The research team has developed a new test, based on a technique which is capable of giving results in just half an hour – over three times faster than the current method.
Prof Wei Huang says: ‘The beauty of this new test lies in the design of the viral detection that can specifically recognise SARS-CoV-2 (COVID-19) RNA and RNA fragments. The test has built-in checks to prevent false positives or negatives and the results have been highly accurate.’
Additionally, the technology is very sensitive. This means that patients in early stages of infection may be identified sooner, potentially helping to reduce the spread of the coronavirus SARS-CoV-2 (COVID-19). The technology only requires a simple heat-block which maintains a constant temperature for RNA reverse transcription and DNA amplification, and the results can be read by the naked eye. This makes it potentially useful in rural area or community healthcare centres.
The technology has been validated with real clinical samples at Shenzhen Luohou People’s Hospital in China. Shenzhen Luohu People’s Hospital has applied the rapid detection kits on 16 clinic samples, including 8 positives and 8 negatives, which have been confirmed by conventional RT-PCR methods and other clinical evidence. The test results using the rapid detection kits were all successful.
Prof. Zhanfeng Cui, the Director of OSCAR, says: ‘I am proud of our team that have developed a useful technology and can make a contribution in combating CoV-19, and we are very grateful to the hospital’s medical team led by Dr Xizhou Sun, Dr Xiuming Zhang and Dr Dan Xiong for their part in testing this new technology.’
The Oxford scientists are now working to develop an integrated device so that the test can be used at clinics, airports, or even for home use.
The project was initiated by Oxford Suzhou Centre for Advanced Research (OSCAR), a University of Oxford centre in Suzhou Industrial Park. The experiments to develop the technology were performed in the Department of Engineering Science at the University of Oxford.
Cost sharing is waived for COVID-19 tests and testing related visits
If you believe you might have been exposed to COVID-19 or have symptoms such as fever, cough or difficulty breathing, call your health care provider right away. Only health care providers can order a COVID-19 test.
We are waiving cost sharing for COVID-19 testing during this national emergency. And we are waiving cost sharing for COVID-19 testing related visits during this same time, whether the testing related visit is received in a health care provider’s office, an urgent care center, an emergency department or through a telehealth visit. This coverage applies to Medicare Advantage, Medicaid and employer-sponsored plans.
The CDC remains your best resource for COVID-19
The COVID-19 situation continues to quickly evolve. Go to the CDC for the latest information on COVID-19, including how to protect yourself and what to do if you are sick.
If you believe you might have been exposed to COVID-19 or have symptoms such as fever, cough or difficulty breathing, call your health care provider right away. Only health care providers can order a COVID-19 test.
FDA authorizes CPAP machines and more as emergency ventilator alternatives
The FDA issued a wide-ranging emergency policy allowing alternative devices to be used as potentially lifesaving ventilators as shortages begin to impact hospitals’ responses to the coronavirus pandemic.
This includes modified anesthesia gas hardware and positive-pressure breathing devices as well as home continuous positive airway pressure machines used to treat sleep apnea, portable oxygen generators for chronic obstructive pulmonary disease and nasal cannulae hoses.
The agency’s broad Emergency Use Authorization enables their use for treating COVID-19 patients following a manufacturer’s official request, and the FDA will be compiling a public list of permitted devices.
In addition, the FDA told healthcare providers that certain ventilators may be able to support multiple patients at once using air tube splitters.
Earlier this week, the FDA told the industry it would allow manufacturers to modify and deploy previously cleared ventilators without needing to resubmit them for agency review and gave providers permission to use ventilators beyond their indicated shelf life.
Meanwhile, Medtronic and GE Healthcare are working to ramp up ventilator production. Medtronic, maker of the Puritan Bennett brands, said it increased global production by more than 40% and plans to more than double its total capacity. GE Healthcare said it is setting up additional manufacturing lines, increasing shifts and hiring new employees and will boost output of CT scanners, ultrasound devices, mobile X-rays and patient monitors as well.
Former FDA chief Gottlieb has dire warnings about hitting the brakes on social distancing measures
Former FDA chief Scott Gottlieb, M.D., said public policy leaders will not be able to “hit the brakes” on social distancing measures until the epidemic curve begins to drop, and that could be several weeks away. (FDA)
Hard-hit coronavirus “hot spots” like New York City are two to three weeks away from hitting peak COVID-19 cases, according to former federal official Scott Gottlieb.
Many other cities and states could be two weeks behind.
“I’m worried about Florida; I’m worried about cities like New Orleans and cities where mass transit systems were late to implement mitigation strategies like Chicago,” said Gottlieb, M.D., former Food and Drug Administration Commissioner, during a Wall Street Journal Health Forum hosted virtually this week.
Asked by WSJ reporter Anna Wilde Mathews whether the U.S. was on track to look like Italy or South Korea, Gottlieb responded: “We’re in between. We lost the chance to be South Korea, and I don’t think it will be as tragic as Italy. I certainly hope not on a per capita basis.”
To prevent hospitals from being overrun, population-based tactics such as closing businesses and schools and urging people to stay home need to continue for several weeks, Gottlieb said.
“We need to stick with these tactics, as painful as they are. There are public health implications and economic costs of these interventions. But we have to take these steps now to break the chain of transmission,” he said. “There is no public health in this country if the hospitals are overwhelmed. As long as coronavirus continues to spread in this fashion, the hospitals are not going to be functional.”
Gottlieb’s recommendations, which are in line with public health leaders such as infectious disease expert Anthony Fauci, M.D., director of the National Institute of Allergy and Infectious Diseases, contrast sharply with President Donald Trump’s call to ease restrictions. Tuesday, Trump told Fox News he hoped to have the country reopened by Easter on April 12.
“New York is not going to be there” by April 12, Gottlieb said. “You need to wait to see what happens to other American cities before making any decisions,” he said.
Technion researchers working on emergency projects to fight coronavirus
These emergency projects focus on different important aspects, such as detection and diagnostics; vaccine development; therapeutic treatments; and methods for remote care and monitoring of patients.
An employee of German biopharmaceutical company CureVac, demonstrates research workflow on a vaccine for the coronavirus (COVID-19) disease at a laboratory in Tuebingen, Germany
(photo credit: REUTERS/ANDREAS GEBERT)
Researchers from over 20 labs at the Technion-Israel Institute of Technology are working around the clock to combat the further spread of the novel coronavirus outbreak around the world.
These emergency projects focus on different important aspects, such as detection and diagnostics; vaccine development; therapeutic treatments; and even methods for remote care and monitoring of patients suffering from COVID-19, including robotic solutions.
Noteworthy examples in coronavirus diagnostics include Prof. Hossam Haick, from Technion’s Wolfson Faculty of Chemical engineering. His research is working on a diagnostic test for coronavirus carriers before they show symptoms.
In the vaccine development field, the chemical engineering faculty’s Prof. Avi Schroeder is working on a vaccine based on one developed for shrimps. If successful, the vaccine will be commercialized by his start-up company, ViAqua Theraputics. Schroeder is also working on a therapeutic treatment method by working on a drug that could treat some respiratory distress symptoms.
“Technion is at the forefront of science and technology worldwide, and during this time of crisis, we are collaborating closely with the health system and the hospitals in order to find immediate solutions to the challenges they are facing,” said Technion president Prof. Uri Sivan.
“We are working on advanced diagnostic techniques, personalized medical treatment, technologies that enable pinpointed drug delivery, treatment protocols based on machine learning and artificial intelligence, data mining and Big Data management, developing robots for remote medical care and more.
“Technion’s added value is apparent in the close interaction between medicine and engineering at our university, and in the interdisciplinary collaborations that are generating rapid and sophisticated solutions to help fight COVID-19.”
In addition, Technion researchers are collaborating with medical staff from Rambam Medical Center on numerous other emergency projects to help combat the coronavirus.
However, other research institutes in Israel are also working hard on treatments and vaccines for the virus. Earlier this week, the Kiryat Shmona-based MIGAL – Galilee Research Institute announced that they expected to begin human testing of an oral vaccine – which was based on a vaccine originally designed to prevent the Infectious Bronchitis Virus (IBV) in poultry – for the coronavirus in eight to 10 weeks.
“We are currently in intensive discussions with potential partners that can help accelerate the in-human trials phase and expedite the completion of final product development and regulatory activities,” said MIGAL CEO David Zigdon.
The coronavirus outbreak has spread throughout the world in the past few months, infecting hundreds of thousands of people and killing thousands more. At the time of writing, Israel has confirmed over two thousand cases and five deaths from COVID-19, and the country has been hard at work expanding testing and implementing containment measures.
It was an AI that first saw it coming, or so the story goes. On December 30, an artificial-intelligence company called BlueDot, which uses machine learning to monitor outbreaks of infectious diseases around the world, alerted clients—including various governments, hospitals, and businesses—to an unusual bump in pneumonia cases in Wuhan, China. It would be another nine days before the World Health Organization officially flagged what we’ve all come to know as Covid-19.
BlueDot wasn’t alone. An automated service called HealthMap at Boston Children’s Hospital also caught those first signs. As did a model run by Metabiota, based in San Francisco. That AI could spot an outbreak on the other side of the world is pretty amazing, and early warnings save lives.
But how much has AI really helped in tackling the current outbreak? That’s a hard question to answer. Companies like BlueDot are typically tight-lipped about exactly who they provide information to and how it is used. And human teams say they spotted the outbreak the same day as the AIs. Other projects in which AI is being explored as a diagnostic tool or used to help find a vaccine are still in their very early stages. Even if they are successful, it will take time—possibly months—to get those innovations into the hands of the health-care workers who need them.
The National Library of Medicine expands access to coronavirus literature through PubMed Central
Transmission electron micrograph of SARS-CoV-2 virus particles, isolated from a patient. Image captured and color-enhanced at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland.NIAID
The National Library of Medicine (NLM), part of the National Institutes of Health, is working on multiple fronts to aid in the COVID-19 response through new initiatives with the global publishing community and artificial intelligence researchers. NLM is expanding access to scientific papers on coronavirus for researchers, care providers, and the public, and for text-mining research. This work makes use of NLM’s PubMed Central® (PMC), a digital archive of peer-reviewed biomedical and life sciences literature. PMC currently provides access to nearly 6 million full-text journal articles.
Following on a statement issued by the White House Office of Science and Technology Policy (OSTP) and science policy leaders from almost a dozen other nations, NLM has stepped up its collaboration with publishers and scholarly societies to increase the number of coronavirus-related journal articles in PMC, along with available data supporting them. Submitted publications will be made available in PMC as quickly as possible after publication, in formats and with needed permissions to support text mining.
To support this initiative, NLM is adapting its standard procedures for depositing articles into PMC to provide greater flexibility that will ensure coronavirus research is readily available. NLM is also engaging with journals and publishers that do not currently participate in PMC but are in-scope for the NLM Collection. Interested publishers should contact pmc-phe@ncbi.nlm.nih.gov for information on participating in this initiative. Additional information, including a list of participating publishers and journals, is available at: https://www.ncbi.nlm.nih.gov/pmc/about/covid-19.
By making this collection of coronavirus articles more readily available in machine-readable formats, NLM aims to enable artificial intelligence researchers to develop and apply novel approaches to text mining to help answer questions about coronavirus. NLM has already made more than 10,000 full-text scholarly articles from PMC related to the coronavirus available through the COVID-19 Open Research Dataset (CORD-19). The CORD-19 dataset, the result of a request by OSTP, represents the most extensive machine-readable coronavirus literature collection available for text mining to date.
NLM will continue to aid COVID-19 response efforts by adding articles to its text-mining collection as they are published and submitted. It will also aim to bring this collection to the attention of the artificial intelligence and machine learning research communities.
The National Library of Medicine (NLM) is a leader in research in biomedical informatics and data science and the world’s largest biomedical library. NLM conducts and supports research in methods for recording, storing, retrieving, preserving, and communicating health information. NLM creates resources and tools that are used billions of times each year by millions of people to access and analyze molecular biology, biotechnology, toxicology, environmental health, and health services information. Additional information is available at https://www.nlm.nih.gov.
UCSF’s Dr. Sachin Shah compiled PubMed articles on Coronavirus into Topics. It is a very Valuable RESOURCE
3/23/2020
This NYT article on the movements of hundreds of millions of people show the Transmission routes for the 2020 Coronavirus Pandemic. IT IS THE BEST INVESTIGATING REPORTING ON THIS SUBJECT TO DATE.
The most extensive travel restrictions to stop an outbreak in human history haven’t been enough. We analyzed the movements of hundreds of millions of people to show why.
Notes: New cases are represented as seven-day averages. Japan’s count includes 696 cases and seven deaths from a cruise ship quarantined in Yokohama. France and the U.S. figures include overseas territories.
How many people have recovered or died
Source: Center for Systems Science and Engineering at Johns Hopkins University; Local governments.
Researchers at Northwestern University Feinberg School of Medicine have identifiedanew drug target for COVID-19, Xinhua reported on Sunday.
The researchers mapped the atomic structure of critical proteins in a complex, nsp10/16, representing that fourth protein structure of a potential drug target of SARS-CoV-2 determined by the scientists.
“This is a really beautiful target, because it’s a protein absolutely essential for the virus to replicate,” said lead investigator Karla Satchell.
The RNA methyltransferase is comprised of two proteins bound together, which makes it more difficult to work with.
“We need multiple drugs to treat this virus, because this disease is likely to be with us for a long time,” Satchell said, adding that “it’s not good enough for us to develop a single drug. If COVID-19 develops a resistance to one drug, then we need others.”
Investigating the New Coronavirus with Karla Satchell, PhD
Microbiologist Karla Satchell, PhD, is leading a national effort to investigate the structure biology of the components of the new coronavirus virus (2019-nCoV) and ultimately understand how to stop it from replicating in human cells through a medication or vaccine.
This work is being done with the Center for Structural Genomics of Infectious Diseases at Northwestern, which is funded by the National Institute for Allergy and Infectious Diseases.
3/23/2020
Moderna’s COVID-19 Treatment May Go to Small Group in Fall 2020; Commercial Availability Unlikely for at Least 12-18 Months – (Fidelity via NewsPoints Desk)
In a regulatory filing, Moderna clarified comments it said it had made to representatives of Goldman Sachs during a recent meeting, as reported in Fidelity.
According to Moderna, it told the investment bank that a vaccine targeting the treatment of COVID-19 “could be available to some people, possibly including healthcare professionals, in the fall of 2020,” on an emergency basis.
However, the company clarified in its statement that a commercially-available vaccine was not “likely to be available for at least 12-18 months.”
Meanwhile, CEO Stephane Bancel confirmed that it was scaling up manufacturing capacity targeting “millions of doses per month, in the potential form of individual or multi-dose vials.”
Before long, studies on SARS-CoV-2 susceptibility and the role of genetics will be published. Here at Nebula, we are monitoring the research on COVID-19 and will provide our users with timely updates. You can stay updated with the latest research discoveries by purchasing our whole-genome sequencing or uploading your existing 23andMe or AncestryDNA data.
Scientists are using genetic sequences of the coronavirus to learn where and how it is spreading. The approach relies on technology that didn’t exist just a few years ago.
Hunt For New Coronavirus Treatments Includes Gene-Silencing And Monoclonal Antibodies
IBM helps bring supercomputers into the global fight against COVID-19
By Dario Gil, Director of IBM Research
At IBM, I have the privilege of working with colleagues who have dedicated their lives and careers to advancing science and creating innovative technology that can be a force for progress in the world. Since the start of the COVID-19 pandemic we have been working closely with governments in the U.S. and worldwide to find all available options to put our technology and expertise to work to help organizations be resilient and adapt to the consequences of the pandemic, and to accelerate the process of discovery and enable the scientific and medical community to develop treatments and ultimately a cure.
Now, in collaboration with the White House Office of Science and Technology Policy and the U.S. Department of Energy and many others, IBM is helping launch the COVID-19 High Performance Computing Consortium, which will bring forth an unprecedented amount of computing power—16 systems with more than 330 petaflops, 775,000 CPU cores, 34,000 GPUs, and counting — to help researchers everywhere better understand COVID-19, its treatments and potential cures.
How can supercomputers help us fight this virus? These high-performance computing systems allow researchers to run very large numbers of calculations in epidemiology, bioinformatics, and molecular modeling. These experiments would take years to complete if worked by hand, or months if handled on slower, traditional computing platforms.
By pooling the supercomputing capacity under a consortium of partners, including IBM, Lawrence Livermore National Lab (LLNL), Argonne National Lab (ANL), Oak Ridge National Laboratory (ORNL), Sandia National Laboratory (SNL), Los Alamos National Laboratory (LANL), the National Science Foundation (NSF), NASA, the Massachusetts Institute of Technology (MIT), Rensselaer Polytechnic Institute (RPI), and multiple leading technology companies, we can offer extraordinary supercomputing power to scientists, medical researchers and government agencies as they respond to and mitigate this global emergency.
As a powerful example of the potential, IBM’s Summit, the most powerful supercomputer on the planet, has already enabled researchers at the Oak Ridge National Laboratory and the University of Tennessee to screen 8,000 compounds to find those that are most likely to bind to the main “spike” protein of the coronavirus, rendering it unable to infect host cells. They were able to recommend the 77 promising small-molecule drug compounds that could now be experimentally tested. This is the power of accelerating discovery through computation.
Now we must scale, and IBM will work with our consortium partners to evaluate proposals from researchers around the world and provide access to this supercomputing capacity for the projects that can have the most immediate impact.
I am proud to be working with my IBM colleagues and the extended scientific community to help kick-start this effort. What began just days ago with one conversation with the White House Office of Science and Technology Policy has solidified quickly into an unprecedented effort that can make a real difference. In a time of uncertainty, I want to offer this promise: IBM will continue to explore everything in our power to use our technology and expertise to drive meaningful progress in this global fight.
VOICE of Jason Zielonka, MD on Coronavirus Testing
Very interesting approach, redirecting testing based on patient self-awareness & reporting. The weakness is how asymptomatic but contagious individuals can be found …
Best implemented through the state-level health departments with cell coordination through Federal government. Keeps delivery and pickup of swabs local, where rapid response is possible.
I’ve been mulling over the @MRC_Outbreak modeling report on #COVID19 mitigation and suppression strategies since it was posted on March 16. Although mitigation through social distancing may not solve things I believe we can bring this epidemic under control. 1/19
But first, the report. @neil_ferguson, @azraghani and colleagues model COVID-19 epidemic outcomes under different intensities of non-pharmaceutical, aka social distancing, interventions. 2/19
Different mitigation scenarios that include things like school closures, isolation of symptomatic individuals and quarantine of exposed household members, result in #flatteningthecurve and reducing mortality, but under the author’s assumptions still result in an epidemic. 3/19
Given assumed severity of COVID-19 infections, this flattened epidemic is still severe, resulting in over 1 million deaths in the US and >250k deaths in GB, mostly concentrated in those over 60 and with underlying health conditions. 4/19
Alternatively, with stronger social distancing, the epidemic could be brought under control and effectively “suppressed”. However, stopping this level of social distancing would result in a fairly rapid rebound as the population would still lack immunity to the virus. 5/19
Managing this level of social distancing required for suppression while still having a functional economy and society would be difficult and it’s not at all clear that this could be maintained for the ~18 months until we have a vaccine. 6/19
This is the catch-22 as presented by the report. 7/19
However, I’m not quite that pessimistic. Although I agree that basic mitigation efforts won’t stop the epidemic, I have hope that we can solve this thing by doing traditional shoe leather epidemiology of case finding and isolation, but at scale, using modern technology. 8/19
There are two main case-based strategies that I see here, both related, as well as a supporting serological strategy. 9/19
The first strategy revolves around a massive rollout of testing capacity. We believe that a significant proportion of epidemic transmission is due to mild and maybe even asymptomatic infections (science.sciencemag.org/content/early/…). 10/19
We also believe that a significant amount of transmission may occur in the window before symptoms develop (evidence from viral load dynamics nejm.org/doi/full/10.10…, evidence from serial intervals ncbi.nlm.nih.gov/pubmed/32145466). 11/19
These transmission routes can be reduced by a huge rollout of testing capacity. If someone can be tested early in their illness before they show symptoms, they could effectively self isolate and reduce onward transmission compared to isolation when symptoms develop. 12/19
This strategy of massive testing has been a cornerstone in South Korea’s response (sciencemag.org/news/2020/03/c…) and we’re now seeing their epidemic brought under control without the stringent policies put in place elsewhere. Case counts in South Korea via @covid2019app. 13/19
This rollout of testing could be achieved through at home delivery of swabs with centralized lab-based processing combined with drive-through testing facilities. There are logistics involved in getting a result quickly, but it’s really just logistics, which can be solved. 14/19
The second, related, strategy is using cell phone location data combined with data on known positive cases to alert possible exposures to self isolate and get tested. Figure from @ChristoPhraser and colleagues who’ve considered this in detail. 15/19
This strategy targets testing capacity at most likely cases and serves to detect exposure events early, when isolation is most valuable. This cell phone location based approach is outlined carefully here: github.com/BDI-pathogens/…. 16/19
A third, supporting, strategy: as the epidemic proceeds get serological assays run on as many people as possible to systematically identify individuals who have recovered and are highly likely to possess immunity. 17/19
Individuals who have serological evidence of recovery and are no longer shedding virus can fully return to the workforce and keep society functioning (especially important for those at the clinical front lines). 18/19
Together, I believe these (and other case-based) strategies can bring down the epidemic. This is the Apollo program of our times. Let’s get to it. 19/19
Subject: Coronavirus Now: When could this pandemic end? Here’s what experts say
3/20/2020
In the last two days, major players including Bayer, Novartis, Teva and Mylan agreed to donate vast quantities of malaria med chloroquine, which President Donald Trump highlighted in a press conference Thursday as a possible treatment. Other companies including Merck KGaA, with multiple sclerosis med Rebif, and AbbVie, with HIV therapy Kaletra, have also pitted their existing drugs against the virus.
At all levels of Regeneron’s global operations, Weinreich said, researchers grasp the vastness of the pandemic’s fallout and the challenge ahead of them. Their solution? Find comfort in the work.
“There’s no escaping that it’s not business as usual, but the work is still business as usual,” Weinreich said. “We’re not compromising on the science.”
SOURCE
Inside Regeneron’s R&D war room, sleepless nights and ‘esprit de corps’ in hunt for COVID-19 therapy
BREAKING NEWS FROM HADASSAH HOSPITAL, DIRECTOR GENERAL, ZEEV ROTSTEIN:
Top of the news is that the Ministry of Health’s Central Laboratory, located at Sheba Hospital has been shut down as the Assistant Head of the Department was diagnosed with COVID-19. The Ministry of Health was in touch with Prof. Dana Wolf, Head of the Clinical Virology Laboratory at Hadassah, and asked that Hadassah replace the Central Laboratory of the State of Israel. Hadassah immediately responded to the request. We have recruited the assistance of all of our scientists and laboratory workers to fill the void left by the Central Laboratory of the State of Israel.
We have recruited volunteers, mainly doctoral students from the sciences, who will work three shifts a day (including nights and weekends) to double and even triple the number of tests we can perform.
Until yesterday, the Central Laboratory performed approximately 480 tests a day. We are trying to close the gap that has been created. To reach this goal, this morning a new robot was put into operation, in addition to PCR (polymerase chain reaction) equipment, needed for the tests, which was recruited from research laboratories. With the assistance of The Hebrew University of Jerusalem, a new area was built to collect the biological materials and then process and neutralize them through automatic systems.
Hadassah once again turned to the Ministry of Health with a request to expand screening in the general population and perform a minimum of 25,000 tests a day to minimize the possibility that home quarantine will cause coronavirus infected individuals to infect their family members, as well as to minimize its infiltration into the medical systems or other sensitive security systems.
Subject: COVID-19: Emergency Measures at Hadassah Hospital
3/19/2020
China investigating ex-Biogen employee who fled to country while sick
A statistician who was working in Massachusetts for Biogen Inc., the host of the now infamous Boston conference at the epicenter of the state’s COVID-19 outbreak, is being investigated in Beijing for allegedly flying to her native China while sick, not disclosing her exposure to coronavirus to the airline, and covering up her fever with drugs, according to reports in Chinese-based media.
your notes and enlightenment is needed as its my first….
Glycans in the viral pathology of COVID-19?
While we are constantly cautioning people from putting too much validity to the results seen in this bellow mentioned paper, it was not coming from thin air to the researchers minds.
The ABO blood groups are a result of various and different glycans on the surfaces of red blood cells and their defenition is related to immunology of blood and the core of blood typing in blood donation. It was also the hallmark of the 1930 Nobel prize of medicine.
e.g. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2766682/ in this article the authors claim and show that the ABH(O) glycan can modulate the surface of cells and their interactions to pathogens, in this case the malaia pathogen.
Glycans are involved in the interaction of the flu virus to the host cell and Tamiflu (Oseltamivir ) is based on the inhibition of that sort of interaction/modulation.
Even if true, the numbers in this paper show statistically significant difference but midly significant differences in risk profile to suggest we are to pay too much attention to the phenomena or worry, regardless of the fact these result have no significance on behavioral instructions nor would I run to check my blood type in regards to this. I would neither totally ignore the finding as it may shed light on viral pathology and infection mechanisms and understanding the later may lead us to treatment or effective vaccines. But we are still early in this path.
FDA maps out plan for trials as coronavirus starts to threaten drug research
“FDA recognizes that protocol modifications may be required, and that there may be unavoidable protocol deviations due to COVID-19 illness and/or … control measures,” the agency wrote. Among them: pausing recruitment or monitoring patients less frequently, or even virtually, rather than through hospital visits.
There are even more difficult decisions to consider, such as taking certain patients off of experimental medicines altogether if the risks outweigh the benefits. Patients who stop treatment might need extra monitoring, the FDA noted.
Trial sponsors should detail specifically how COVID-19 impacts their trials — from missed study visits or patients who drop out to contemplated protocol changes. That will keep the FDA up to date so it can understand reasons behind any “missing data” and more accurately review the drugs being tested, the agency said.
“Robust efforts by sponsors, investigators, and [review boards] to maintain the safety of trial participants and study data integrity are expected, and such efforts should be documented,” the FDA wrote. COVID-19-related trial issues are likely unavoidable, so “efforts to minimize impacts on trial integrity, and to document the reasons for protocol deviations, will be important.”
A vaccine to prevent infections of the novel coronavirus SARS-CoV-2 is likely a year or more away — at best — and treatments specifically designed to fight this virus or its complications are similarly far off.
Possible treatments, however, could already be available in the form of marketed or existing experimental drugs. Global public health officials, eager for a weapon to use in the midst of a global pandemic, are showing a willingness to be flexible in terms of the clinical trials and the evidence needed to prove treatments’ effectiveness.
Earlier this month, China OK’d the use of Actemra in patients with lung complications and high levels of interleukin-6, or IL-6, a protein that mediates inflammatory and immune response. High levels of IL-6 have been associated with a greater risk of death in patients with community-acquired pneumonia.
Actemra and Kevzara both block IL-6 and are prescribed for rheumatoid arthritis, a disorder in which an overactive immune system creates joint-damaging inflammation and pain. Actemra is similarly approved in conjunction with cancer cell therapy, which can sometimes trigger an immune reaction known as cytokine release syndrome.
The U.S.-based Kevzara trial is a two-part design that will initially evaluate fever and oxygen use in patients with acute respiratory distress syndrome, or ARDS. Two different dose levels will be used and compared to a placebo.
Longer-term, the trial hopes to measure prevention of death, use of ventilation, supplemental oxygen or hospitalization, but the design will be “adaptive” to determine the number of patients that will be followed and the endpoints to be used. ARDS often causes permanent lung damage and can lead to early death.
The trial aims to enroll 400 patients in the U.S. Regeneron’s partner Sanofi will handle international trial sites, naming Italy as one likely location for testing in coronavirus patients.
To get the trial underway quickly, Regeneron and Sanofi worked closely with the Food and Drug Administration and the Biomedical Advanced Research and Development Authority, the division of HHS involved in preparing for natural and man-made biological threats.
NIH clinical trial of investigational vaccine for COVID-19 begins
A Phase 1 clinical trial evaluating an investigational vaccine designed to protect against coronavirus disease 2019 (COVID-19) has begun at Kaiser Permanente Washington Health Research Institute (KPWHRI) in Seattle. The National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, is funding the trial. KPWHRI is part of NIAID’s Infectious Diseases Clinical Research Consortium. The open-label trial will enroll 45 healthy adult volunteers ages 18 to 55 years over approximately 6 weeks. The first participant received the investigational vaccine today.
The study is evaluating different doses of the experimental vaccine for safety and its ability to induce an immune response in participants. This is the first of multiple steps in the clinical trial process for evaluating the potential benefit of the vaccine.
The vaccine is called mRNA-1273 and was developed by NIAID scientists and their collaborators at the biotechnology company Moderna, Inc., based in Cambridge, Massachusetts. The Coalition for Epidemic Preparedness Innovations (CEPI) supported the manufacturing of the vaccine candidate for the Phase 1 clinical trial.
“Finding a safe and effective vaccine to prevent infection with SARS-CoV-2 is an urgent public health priority,” said NIAID Director Anthony S. Fauci, M.D. “This Phase 1 study, launched in record speed, is an important first step toward achieving that goal.”
Infection with SARS-CoV-2, the virus that causes COVID-19, can cause a mild to severe respiratory illness and include symptoms of fever, cough and shortness of breath. COVID-19 cases were first identified in December 2019 in Wuhan, Hubei Province, China. As of March 15, 2020, the World Health Organization (WHO) has reported 153,517 cases of COVID-19 and 5,735 deaths worldwide. More than 2,800 confirmed COVID-19 cases and 58 deaths have been reported in the United States as of March 15, according to the Centers for Disease Control and Prevention (CDC).
Currently, no approved vaccines exist to prevent infection with SARS-CoV-2.
The first treatment is Chloroquine, a medication that has been used for over 70 years to treat malaria and rheumatic illnesses such as lupus and arthritis. The bus driver who was infected with coronavirus and recovered is being treated with this medication along with other anti-viral medications.
Remdesivir, the second treatment approved, is still in the first stages of human testing and results will be available within a number of weeks, according to Ynet. Experiments with the drug began in China, the USA and additional countries, even on some severely ill patients in Israel, including the bus driver who was hospitalized in the Puria Medical Center in Tiberias. The driver saw a dramatic improvement and was even taken off a respirator.
The treatment may slow down the spread of the virus and may even stop the virus from multiplying in the body. The virus has been shown to work against MERS and SARS, viruses related to the novel coronavirus. Remdesivir succeeded in preventing monkeys from being infected with MERS in trials and led to an improvement in those who were already infected. The drug has also shown promising results against a variety of other viruses.
Kaletra, the third treatment approved, is an anti-viral medication that combines two anti-viral “protease inhibitor” medications that prevent the multiplication of HIV. The virus is already used to treat those who are carrying or ill from AIDS.
SOURCE
In Israel, Health Ministry approves experimental treatments for coronavirus
SARS-CoV-2 isan enveloped, positive-sense, single-stranded RNA β-coronavirus similar to the severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) viruses. Potential antiviral targets encoded by the viral genome include non-structural proteins (e.g., 3-chymotrypsin-like protease, papain-like protease, RNA-dependent RNA polymerase and its helicase), structural proteins (e.g., the capsid spike glycoprotein) and accessory proteins. Kaletra is thought to inhibit the 3-chymotrypsin-like protease of the SARS and MERS coronaviruses and was associated with improved clinical outcomes in a trial against SARS. Ascletis also reported that a patient with COVID-19 improved rapidly when given this HIV protease inhibitor combination.
The genomic sequence of the SARS-CoV-2 suggests that there is a high level of sequence similarity between the SARS-CoV-2, SARS and MERS proteins involved in the replication cycle.
But Erik De Clercq, of the Rega Institute for Medical Research in Leuven, Belgium, says that in searching for or designing effective drugs against COVID-19: “We should stay away from antivirals known to be acting at targets not playing a role in the replication of coronaviruses.” Such drugs include penciclovir, which is targeted at the herpesvirus DNA polymerase, and lopinavir/ritonavir, which are targeted at the HIV protease. Instead, he would favor targeting a virus-specific protein such as the RNA-dependent RNA polymerase, noting that coronaviruses do not contain or use a reverse transcriptase. George Painter, president of the Emory Institute for Drug Development, Emory University, is also cautious about the HIV protease inhibitor strategy. “It’s probably a long shot to go for drug repurposing activity against the coronavirus using HIV drugs; these were protease inhibitors that were designed specifically for HIV,” he says.
Targeting viral cellular entry via the spike glycoprotein, which mediates the virus–cell receptor interaction, is another option for repurposing. SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) and the cellular protease transmembrane protease serine 2 (TMPRSS2) to enter target cells. The marketed TMPRSS2 inhibitor camostat mesylate blocked cellular entry of the SARS-CoV-2 virus, according to an unpublished preprint. And the Janus-associated kinase (JAK) inhibitor Olumiant (baricitinib), approved for rheumatoid arthritis, was identified using machine learning algorithms on the basis of its inhibition of ACE2-mediated endocytosis. Another JAK inhibitor, Jakafi (ruxolitinib), is in trials (combined with mesenchymal stem cell infusion) for COVID-19.
The severe acute respiratory syndrome coronavirus (SARS-CoV) emerged in 2003 in China. An epidemic followed, spreading across 26 countries and infecting over 8000 people before the virus was contained. The typical symptoms of SARS are similar to the flu, including fever, headache, and overall feelings of discomfort. Severe cases of the illness were common, resulting in a mortality rate of nearly 10%. Because of the severity of the symptoms, it was possible to identify those infected with SARS-CoV and isolate them. Public health measures like social distancing were successful at containing the outbreak.
SARS and the COVID-19 pandemic
The situation is different with today’s COVID-19 pandemic. This novel coronavirus (SARS-CoV-2) can infect people who then remain largely asymptomatic. This makes it much more difficult to identify and contain those infected who continue spreading the disease. Although the mortality rate of COVID-19 is estimated to be 5 to 10 times lower than SARS, the total number of deaths has already surpassed the SARS outbreak due to failure to contain the pandemic.
However, SARS-CoV and SARS-CoV-2 also share many similarities. Both viruses originated in bats and share 80% of their genetic code. Furthermore, both viruses infect the respiratory tract using the same mechanism, and they cause similar symptoms.
While our understanding of COVID-19 is still lacking, much research on SARS has been produced in the years after 2003. Researchers have identified genetic variants that are associated with susceptibility to infection with SARS-CoV. It remains an open question whether the same genetic variants are also associated with susceptibility to SARS-CoV-2 infection given the similarities between the two coronaviruses.
To inform our users about past research on coronaviruses, we added 3 studies on SARS coronavirus infection to the Nebula Research Library. These studies give us some understanding of the links between human genetics and coronavirus infection.
Nebula Library entries on SARS
SARS coronavirus infection (Hamano, 2005)
This study explored genetic data from Vietnamese individuals and identified a genetic variant in the OAS-1 gene that is associated with susceptibility to infection with the SARS coronavirus.
SARS coronavirus infection (Ching, 2010)
This study used genetic data from Chinese individuals to demonstrate that a genetic variant is linked to a decreased susceptibility to SARS coronavirus infection. This variant is found near the MxA gene, which normally plays a role in inhibiting the replication of the SARS coronaviruses.
SARS coronavirus infection (Tu, 2015)
This study examined the genetic data of Chinese SARS patients to identify variants in 2 genes that lead to an increased risk of infection with the SARS coronavirus. One variant is in the CCL2 gene, which plays a role in attracting macrophages to an infection site. The other variant is in the MBL gene, which helps the immune system recognize molecular patterns that are commonly found on the surface of many viruses and bacteria.
New COVID-19 research
Before long, studies on SARS-CoV-2 susceptibility and the role of genetics will be published. Here at Nebula, we are monitoring the research on COVID-19 and will provide our users with timely updates. You can stay updated with the latest research discoveries by purchasing our whole-genome sequencing or uploading your existing 23andMe or AncestryDNA data.


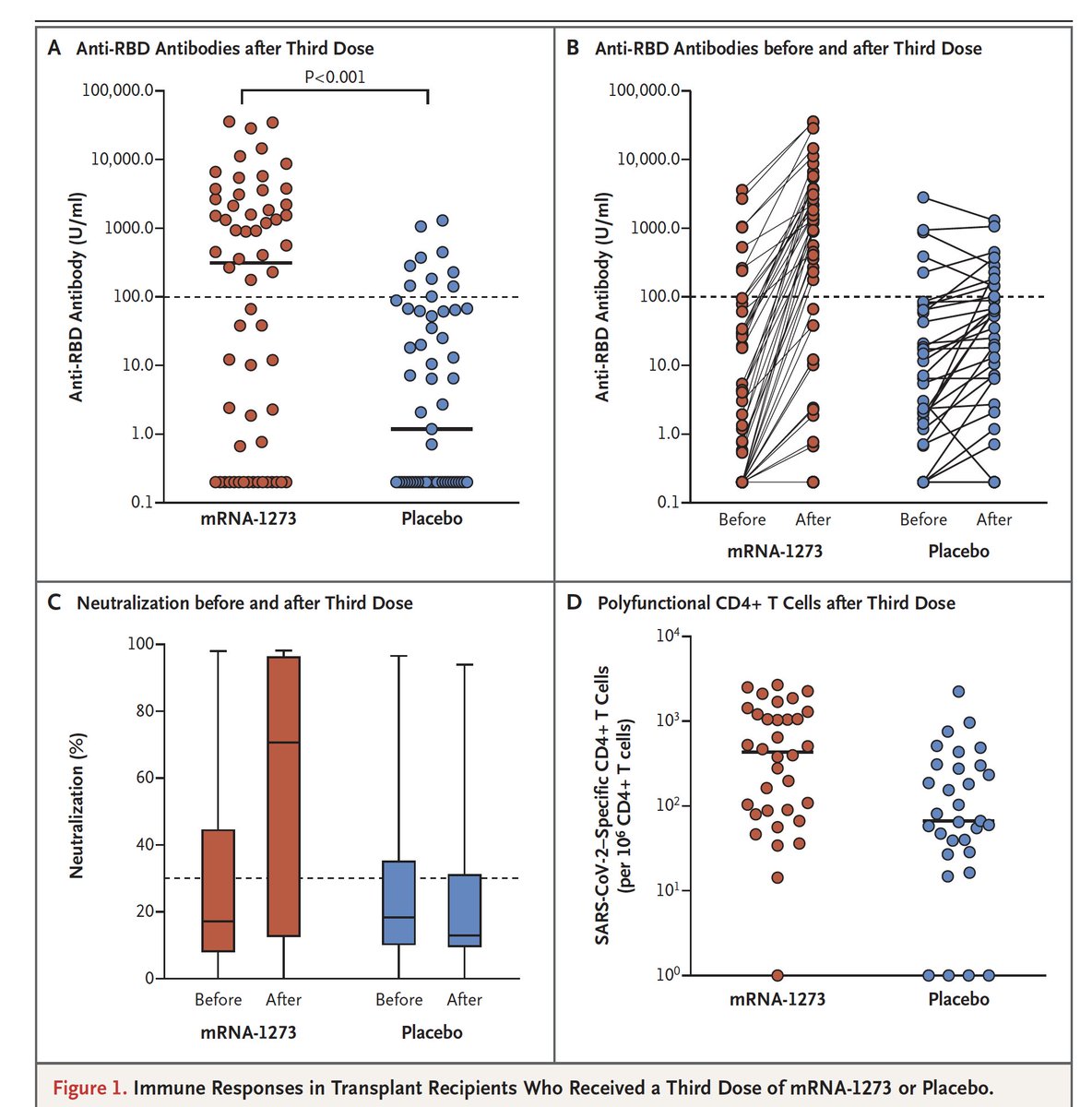


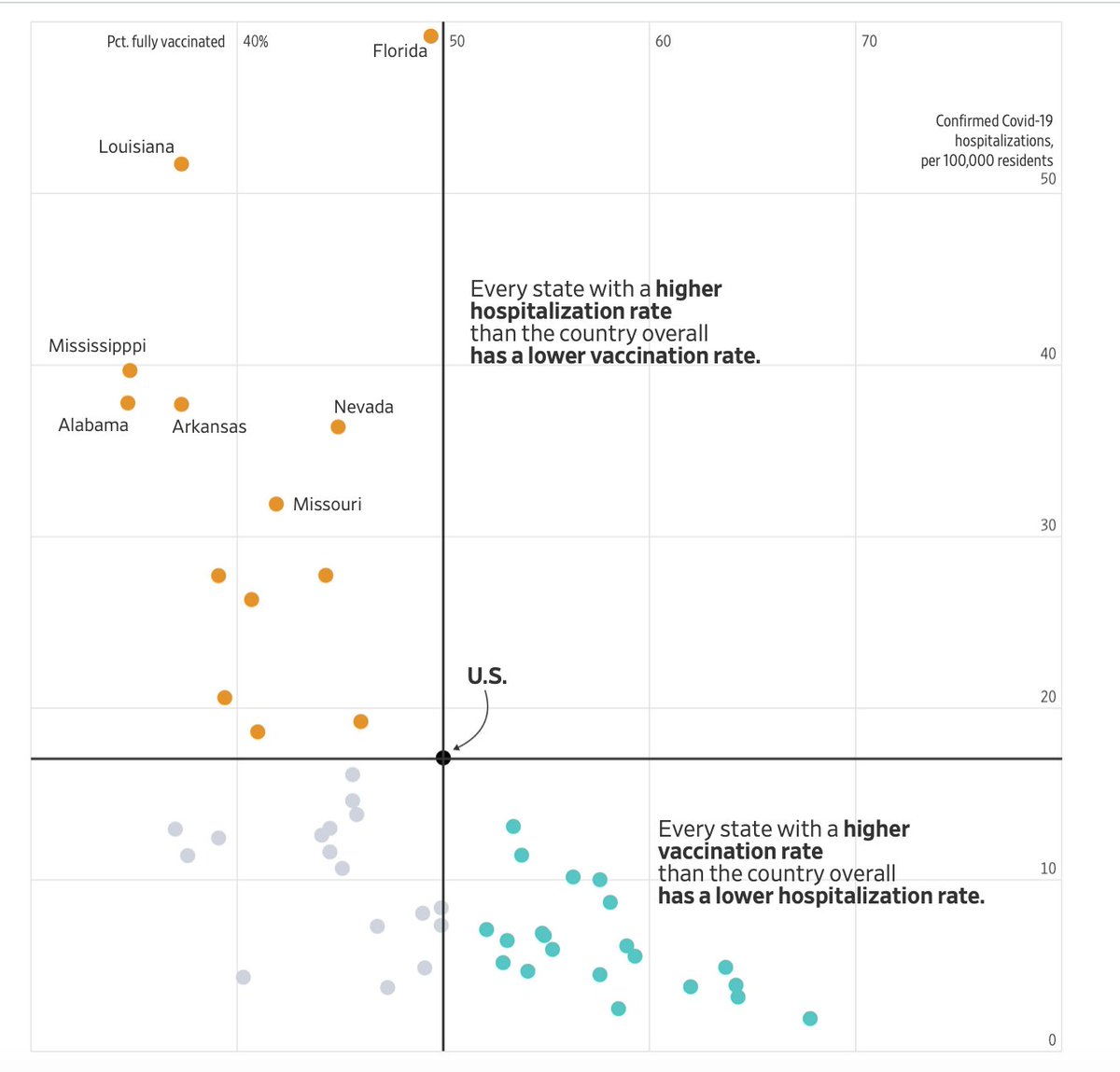


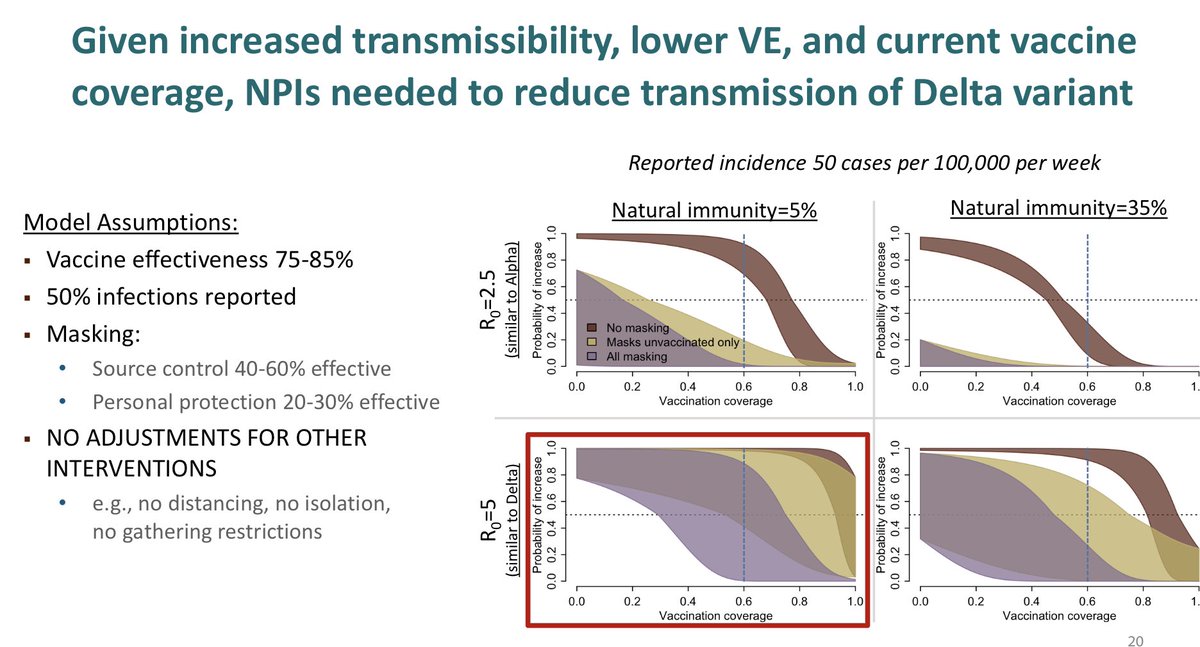











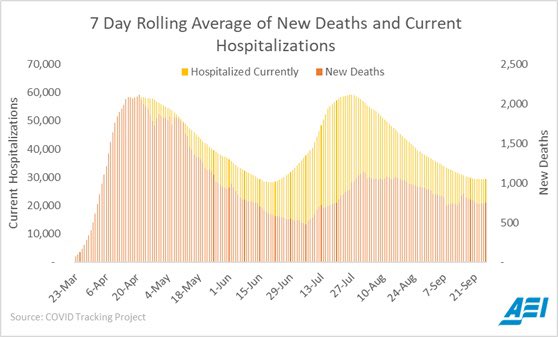
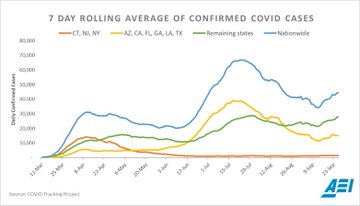
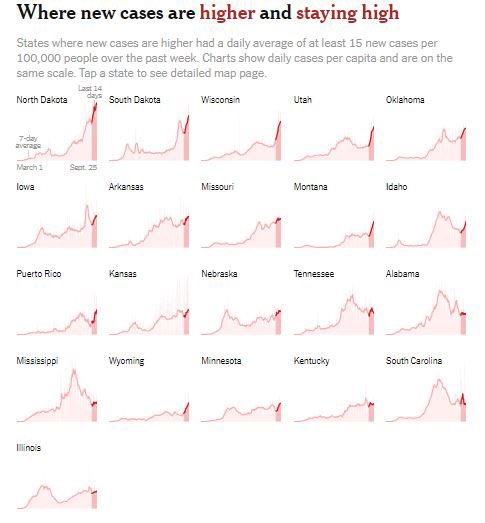
 heavily infected with SARS-CoV-2 virus particles (red), isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. Credit: NIAID")

 Image of an antibody binding to the surface of a virus, blocking entry into a human cell.Lisa Donohue, CoVPN
Image of an antibody binding to the surface of a virus, blocking entry into a human cell.Lisa Donohue, CoVPN

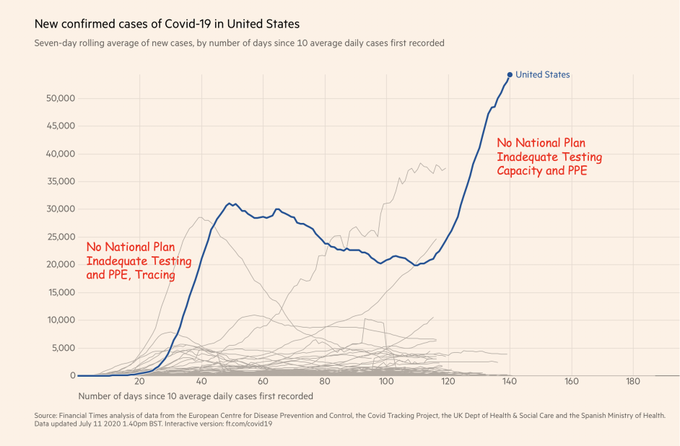






Colorized scanning electron micrograph of a VERO E6 cell (purple) exhibiting elongated cell projections and signs of apoptosis, after infection with SARS-COV-2 virus particles (pink), which were isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. NIAID

This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID’s Rocky Mountain Laboratories (RML) in Hamilton, Montana.NIAID



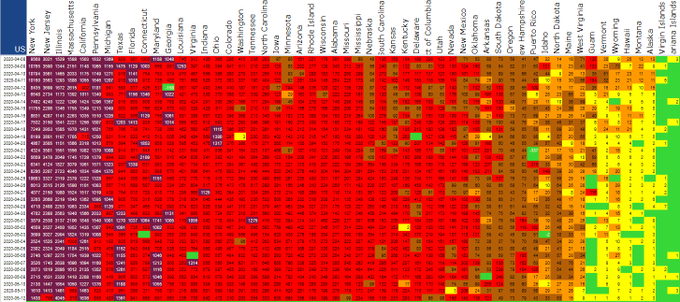
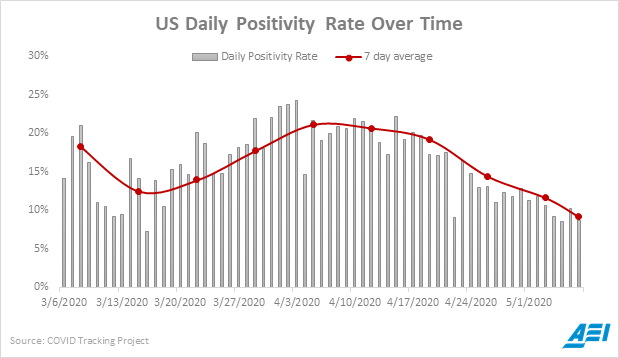









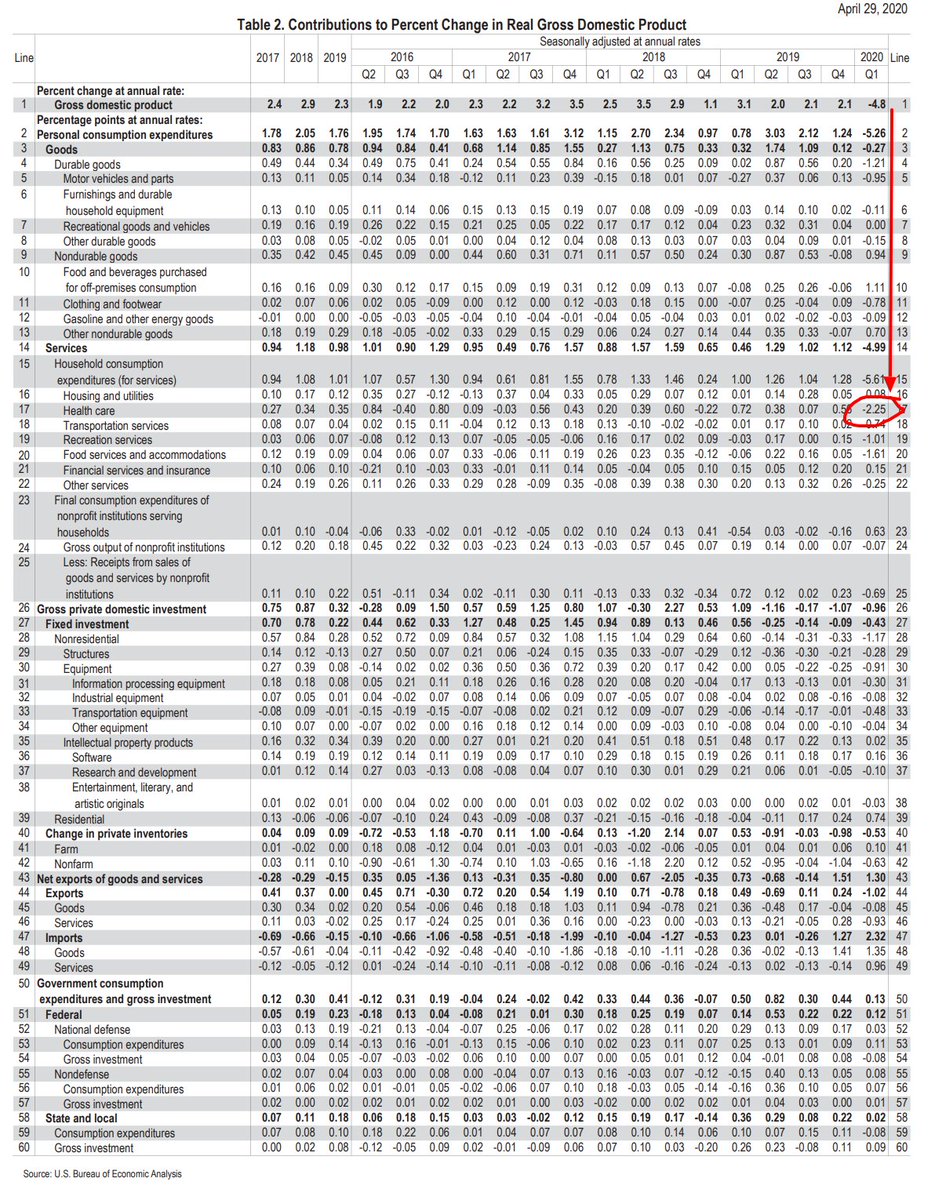





")






Kaitlyn Sadtler, Ph.D., study lead and principal investigator for laboratory testing, holds up a microsampling device from the home blood collection kit used in the study.NIBIB








































 disease at a laboratory in Tuebingen, Germany")
Transmission electron micrograph of SARS-CoV-2 virus particles, isolated from a patient. Image captured and color-enhanced at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland.NIAID



