Development of Medical Counter-measures for 2019-nCoV, CoVid19, Coronavirus
Aviva Lev-Ari, PhD, RN – March 14, 2020 to Present
- Lead Curator, e–mail Contact: AvivaLev-Ari@alum.berkeley.edu
Therapeutical options for coronavirus viral infection include the following:
(a) Monoclonal and polyclonal antibodies
- Therapeutic SARS-CoV neutralizing antibodies have been generated and could be retrieved and used again in the event of another SARS-CoV outbreak. Such antibodies would be most useful for protecting healthcare workers.
(b) Vaccines:
- recombinant attenuated viruses,
- live virus vectors – In general, it is thought that live attenuated vaccines would be the most efficacious in targeting coronaviruses.
- individual viral proteins expressed from DNA plasmids.
(c) Small molecule treatments (e.g., chloroquinolone and derivatives), including compounds already approved for other indications
(d) Immuno-therapies derived from human or other sources
(e) Other Classes: Treatment with convalescent plasma
UPDATED on 2/9/2022
Updates to COVID-19 vaccine tracker
Reporter: Aviva Lev-Ari, PhD, RN
https://pharmaceuticalintelligence.com/2022/02/09/updates-to-covid-19-vaccine-tracker/
UPDATED on 7/22/2021
Israel to become first in world to test Oravax oral COVID-19 vaccine
Oravax Medical is gearing up to commence clinical trials at Tel Aviv Sourasky Medical Center.
Israel is about to become the first country in the world to test the oral COVID-19 vaccine developed by Oramed Pharmaceuticals, the company’s CEO Nadav Kidron told The Jerusalem Post.Oramed’s subsidiary, Oravax Medical, is gearing up to commence clinical trials of its vaccine at Sourasky Medical Center in Tel Aviv after receiving approval for its study protocol from the hospital’s Institutional Review Board. It is now waiting for approval from the Health Ministry, which is expected within a few weeks.Oravax already completed GMP manufacturing in Europe of several thousand capsules that would be available for the Israeli trial and eventually in other countries.
he protocol for the inaugural Phase I/II trial that the company hopes to move forward with at Sourasky would involve 24 volunteers who have not yet been inoculated with another vaccine. Half of the group would take one capsule, and the other half would take two, Kidron said, adding that there is no placebo group because the goal is to measure the level of antibodies and other immunity indicators.“The idea here is that we want to show proof of concept: that it works for people,” he said. “I pray and hope that we will. Imagine that we could give someone an oral vaccine and they are vaccinated. This would be a revolution for the entire world.”With proof of the concept, “the whole world opens up,” Kidron said.
UPDATED on 7/2/2021
The NIH-funded adjuvant improves the efficacy of India’s COVID-19 vaccine
Curator and Reporter: Dr. Premalata Pati, Ph.D., Postdoc
UPDATED on 6/30/2021
WOLFRAM DATA REPOSITORY
https://datarepository.wolframcloud.com/
Repurposing Therapeutics for COVID-19
Vina Docking scores for drug molecules with the S-protein of SARS-CoV-2 and human human ACE2 receptor
Categories:
Types:
SOURCE
https://datarepository.wolframcloud.com/category/Health
1918 ‘Spanish Flu’ Pandemic In Chicago
Point location of influenza and pneumatic deaths and weekly mortality data recorded during 1918 ‘Spanish flu’ pandemic correlated to 1920 census data for Chicago
Categories:
Types:
keywords:
SOURCE
https://datarepository.wolframcloud.com/category/Health
Refined Genetic Graph
WWW Graph of Genetic for Link Analysis Ranking Experiments
Categories:
Types:
Genetic Sequences for the SARS-CoV-2 Coronavirus
Nucleotide sequences of the SARS-CoV-2 virus (the virus associated with the COVID-19 disease, formerly known as 2019-nCoV) including location, collection time and similar supporting data
Categories:
Types:
keywords:
- coronavirus
- sars-cov-2
- severe acute respiratory syndrome
- wuhan
- genetics
- epidemic
- outbreak
- sequence comparison
- corona
- nucleotide
- dna
- rna
- 2019-ncov
- cov-2019
- ncov2019
- 2019ncov
- 2019 ncov
- covid
- covid-19
- covid-2019
- novel coronavirus
- wuhan coronavirus
- china
- virus
- disease
- epidemiology
- public health
- variants
SOURCE
https://datarepository.wolframcloud.com/category/Health
Protein Sequences for the SARS-CoV-2 Coronavirus
Protein sequences of the SARS-CoV-2 virus (the virus associated with the COVID-19 disease, formerly known as 2019-nCoV) including location, collection time and similar supporting data
Categories:
Types:
keywords:
- coronavirus
- sars-cov-2
- severe acute respiratory syndrome
- sars coronavirus
- wuhan
- proteins
- epidemic
- outbreak
- sequence comparison
- corona
- protein
- nucleocapsid
- polyprotein
- 2019-ncov
- cov-2019
- ncov2019
- 2019ncov
- 2019 ncov
- covid
- covid-19
- covid-2019
- novel coronavirus
- wuhan coronavirus
- china
- virus
- disease
- epidemiology
- public health
Source
https://datarepository.wolframcloud.com/category/Life-Science
UPDATED on 2/12/2021
Need for Global Response to SARS-CoV-2 Viral Variants
Reporter: Aviva Lev-Ari, PhD, RN
Rise of a trio of mutated viruses hints at an increase in transmissibility, speeding the virus’ leaps from one host to the next
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 2/11/2021
Peginterferon lambda for the treatment of outpatients with COVID-19: a phase 2, placebo-controlled randomised trial
- et al.
Summary
Background
To date, only monoclonal antibodies have been shown to be effective for outpatients with COVID-19. Interferon lambda-1 is a type III interferon involved in innate antiviral responses with activity against respiratory pathogens. We aimed to investigate the safety and efficacy of peginterferon lambda in the treatment of outpatients with mild-to-moderate COVID-19.Methods
In this double-blind, placebo-controlled trial, outpatients with laboratory-confirmed COVID-19 were randomly assigned to a single subcutaneous injection of peginterferon lambda 180 μg or placebo within 7 days of symptom onset or first positive swab if asymptomatic. Participants were randomly assigned (1:1) using a computer-generated randomisation list created with a randomisation schedule in blocks of four. At the time of administration, study nurses received a sealed opaque envelope with the treatment allocation number. The primary endpoint was the proportion of patients who were negative for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA on day 7 after the injection, analysed by a χ2 test following an intention-to-treat principle. Prespecified analysis of the primary endpoint, adjusted for baseline viral load, using bivariate logistic regression was done. The trial is now complete. This trial is registered with ClinicalTrials.gov, NCT04354259.Findings
Between May 18, and Sept 4, 2020, we recruited 30 patients per group. The decline in SARS-CoV-2 RNA was greater in those treated with peginterferon lambda than placebo from day 3 onwards, with a difference of 2·42 log copies per mL at day 7 (p=0·0041). By day 7, 24 (80%) participants in the peginterferon lambda group had an undetectable viral load, compared with 19 (63%) in the placebo group (p=0·15). After controlling for baseline viral load, patients in the peginterferon lambda group were more likely to have undetectable virus by day 7 than were those in the placebo group (odds ratio [OR] 4·12 [95% CI 1·15–16·73; p=0·029). Of those with baseline viral load above 106 copies per mL, 15 (79%) of 19 patients in the peginterferon lambda group had undetectable virus on day 7, compared with six (38%) of 16 in the placebo group (OR 6·25 [95% CI 1·49–31·06]; p=0·012). Peginterferon lambda was well tolerated, and adverse events were similar between groups with mild and transient aminotransferase, concentration increases more frequently observed in the peginterferon lambda group. Two individuals met the threshold of grade 3 increase, one in each group, and no other grade 3 or 4 laboratory adverse events were reported.Interpretation
Peginterferon lambda accelerated viral decline in outpatients with COVID-19, increasing the proportion of patients with viral clearance by day 7, particularly in those with high baseline viral load. Peginterferon lambda has potential to prevent clinical deterioration and shorten duration of viral shedding.
In outpatients with COVID-19, peginterferon lambda has the potential to prevent clinical deterioration and shorten the duration of viral shedding, according to results of a double-blind, placebo-controlled trial (NCT04354259).
Reductions in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA were greater with peginterferon lambda than with placebo from day 3 onward in the phase 2 study led by Jordan J. Feld, MD, of the Toronto Centre for Liver Disease. The findings were reported in The Lancet Respiratory Medicine.
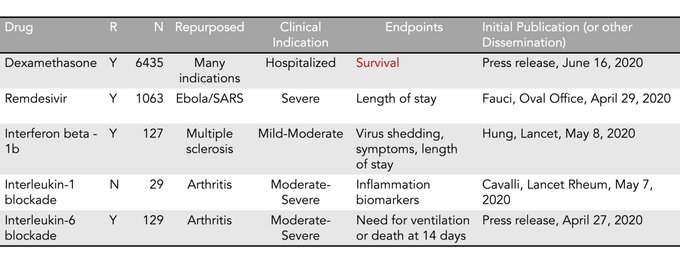
Fewer Side Effects
To date in randomized clinical trials, efficacy in treatment of COVID-19 has been shown only for remdesivir and dexamethasone in hospitalized patients, and in an interim analysis of accelerated viral clearance for a monoclonal antibody infusion in outpatients.
Activity against respiratory pathogens has been demonstrated for interferon lambda-1, a type III interferon shown to be involved in innate antiviral responses. Interferons, Feld and coauthors stated, drive induction of genes with antiviral, antiproliferative and immunoregulatory properties, and early treatment with interferons might halt clinical progression and shorten the duration of viral shedding with reduced onward transmission. In addition, interferon lambdas (type III) use a distinct receptor complex with high expression levels limited to epithelial cells in the lung, liver, and intestine, leading to fewer side effects than other interferons, including avoiding risk of promoting cytokine storm syndrome.
The researchers investigated peginterferon lambda safety and efficacy in treatment of patients with laboratory-confirmed, mild to moderate COVID-19. Sixty patients (median age 46 years, about 60% female, about 50% White) were recruited from outpatient testing centers at six institutions in Toronto, and referred to a single ambulatory site. Patients were randomly assigned 1:1 to a single subcutaneous injection of peginterferon lambda 180 mcg or placebo within 7 days of symptom onset or, if asymptomatic, of their first positive swab. Mean time from symptom onset to injection was about 4.5 days, and about 18.5% were asymptomatic. The primary outcome was the proportion of patients negative for SARS-CoV-2 RNA on day 7 after the injection.
Greater Benefit With Higher Baseline Load
A higher baseline SARS-CoV-2 RNA concentration found in the peginterferon lambda group was found to be significantly associated with day 7 clearance (odds ratio [OR] 0.69 [95% confidence interval 0.51-0.87]; P = .001). In the peginterferon lambda group, also, the mean decline in SARS-CoV-2 RNA was significantly larger than in the placebo group across all time points (days 3, 5, 7, and 14). While viral load decline was 0.81 log greater in the treatment group (P = .14) by day 3, viral load decline increased to 1.67 log copies per mL by day 5 (P = .013) and 2.42 log copies per mL by day 7 (P = .0041). At day 14, the viral decline was 1.77 log copies per mL larger in the peginterferon lambda group (P = .048).
The investigators pointed out that the difference in viral load decline between groups was greater in patients with high baseline viral load (at or above 106 copies per mL). In the peginterferon lambda high baseline viral load group, the reduction was 7.17 log copies per mL, versus 4.92 log copies per mL in the placebo group (P = .004).
SOURCE
UPDATED on 2/9/2021
Flattening the COVID-19 Curve With Natural Killer Cell Based Immunotherapies
Marisa Market1,2†, Leonard Angka1,2†, Andre B. Martel1,2,3, Donald Bastin4, Oladunni Olanubi1,2, Gayashan Tennakoon1, Dominique M. Boucher2, Juliana Ng1, Michele Ardolino1,2,5*† and Rebecca C. Auer1,2,3*†
- 1Cancer Therapeutics Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada
- 2Department of Biochemistry, Microbiology, and Immunology, University of Ottawa, Ottawa, ON, Canada
- 3Division of General Surgery, Department of Surgery, University of Ottawa, Ottawa, ON, Canada
- 4Schulich School of Medicine, University of Western Ontario, London, ON, Canada
- 5Centre for Infection, Immunity, and Inflammation, University of Ottawa, Ottawa, ON, Canada
Natural Killer (NK) cells are innate immune responders critical for viral clearance and immunomodulation. Despite their vital role in viral infection, the contribution of NK cells in fighting SARS-CoV-2 has not yet been directly investigated. Insights into pathophysiology and therapeutic opportunities can therefore be inferred from studies assessing NK cell phenotype and function during SARS, MERS, and COVID-19. These studies suggest a reduction in circulating NK cell numbers and/or an exhausted phenotype following infection and hint toward the dampening of NK cell responses by coronaviruses. Reduced circulating NK cell levels and exhaustion may be directly responsible for the progression and severity of COVID-19. Conversely, in light of data linking inflammation with coronavirus disease severity, it is necessary to examine NK cell potential in mediating immunopathology. A common feature of coronavirus infections is that significant morbidity and mortality is associated with lung injury and acute respiratory distress syndrome resulting from an exaggerated immune response, of which NK cells are an important component. In this review, we summarize the current understanding of how NK cells respond in both early and late coronavirus infections, and the implication for ongoing COVID-19 clinical trials. Using this immunological lens, we outline recommendations for therapeutic strategies against COVID-19 in clearing the virus while preventing the harm of immunopathological responses.
https://www.frontiersin.org/articles/10.3389/fimmu.2020.01512/full
Potential application of mesenchymal stem cells and their exosomes in lung injury: an emerging therapeutic option for COVID-19 patients
- Sara Al-Khawaga& Essam M. Abdelalim
Stem Cell Research & Therapy volume11, Article number: 437 (2020) Cite this article
- Abstract
The COVID-19 pandemic has negatively impacted the global public health and the international economy; therefore, there is an urgent need for an effective therapy to treat COVID-19 patients. Mesenchymal stem cells (MSCs) have been proposed as an emerging therapeutic option for the SARS-CoV-2 infection. Recently, numerous clinical trials have been registered to examine the safety and efficacy of different types of MSCs and their exosomes for treating COVID-19 patients, with less published data on the mechanism of action. Although there is no approved effective therapy for COVID-19 as of yet, MSC therapies showed an improvement in the treatment of some COVID-19 patients. MSC’s therapeutic effect is displayed in their ability to reduce the cytokine storm, enhance alveolar fluid clearance, and promote epithelial and endothelial recovery; however, the safest and most effective route of MSC delivery remains unclear. The use of poorly characterized MSC products remains one of the most significant drawbacks of MSC-based therapy, which could theoretically promote the risk for thromboembolism. Optimizing the clinical-grade production of MSCs and establishing a consensus on registered clinical trials based on cell-product characterization and mode of delivery would aid in laying the foundation for a safe and effective therapy in COVID-19. In this review, we shed light on the mechanistic view of MSC therapeutic role based on preclinical and clinical studies on acute lung injury and ARDS; therefore, offering a unique correlation and applicability in COVID-19 patients. We further highlight the challenges and opportunities in the use of MSC-based therapy
https://stemcellres.biomedcentral.com/articles/10.1186/s13287-020-01963-6
UPDATED on 2/1/2021
A Platform called VirtualFlow: Discovery of Pan-coronavirus Drugs help prepare the US for the Next Coronavirus Pandemic
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 12/21/2020
COVID-19 vaccine from AstraZeneca and University of Oxford show confusing clinical data
Amid the rollout of the two new FDA approved vaccines from Moderna and Pfizer/BioNTech with substantial display of efficacy, the AstraZeneca and University of Oxford trials reported confusing data, as the trial had analyzed data from differing dosing regimens, due to a mid-trial switch in dosing regimen and potentially a calculation error leading to incorrect dosing. The journal Science learned from an unnamed source that there may have been an error in calculation of dose leading to patients receiving only half the dose. However instead of throwing out these patients from the data analysis. it appears the whole study was reanalyzed with the different dose included. AstraZeneca has said they can produce 3 million doses if approved. In the US, Operation Warp Speed, the governments COVID relief effort, has enrolled about 11,000 out of a planned 40,000 to receive the full dose of the AZ vaccine. The AZ/Oxford vaccine should only cost $3 per dose versus $20 per dose for Moderna or Pfizer vaccine.
Source: Amid the cheering, some vaccines face questions
UPDATED on 11/16/2020
From: “Ferez S. Nallaseth, Ph.D.” <ferez.nallaseth@gmail.com>
Date: Monday, November 16, 2020 at 12:20 PM
To: Ferez Nallaseth <mocliamgelgoog2@gmail.com>
Subject: If it is helpful this is a long article dealing with the COVID-19 pandemic.
Good morning Everybody,
Hope that all is well. Please pardon the mass email. However, if in case it is of interest, this is a pre-edited version of Article from the LSINJ and the Magazine Squash Mad that has been posted on LinkedIn.
It is being prepared for publication as a White Paper or book in ayet to be selected book/journal. The article includes a select set of curated and catalogued links on the COVID19 pandemic. We have made it available as a Public Service. Although there are effective vaccines (91% and 94.5%) several caveats remain a threat to the Public Health. We hope that the article accessed through this link, contributes in some small way, to meeting this threat.
Kind regards,
Ferez
UPDATED on 10/1/2020
Coronavirus mutation-does it matter?
Reporter: Irina Robu, PhD
UPDATED on 9/30/2020
Miniproteins against the COVID-19 Spike protein may be therapeutic
Reporter: Stephen J. Williams, PhD
UPDATED on 9/9/2020
Emerging Pandemic Diseases: How We Got to COVID-19
David M. Morens1,* and Anthony S. Fauci1
1Office of the Director, National Institute of Allergy & Infectious Diseases, National Institutes of Health, Bethesda, MD, USA
*Correspondence: dm270q@nih.gov
https://doi.org/10.1016/j.cell.2020.08.021
Bradykinin Hypothesis: Potential Explanation for COVID-19
UPDATED on 9/1/2020
Why Blood Clots Are a Major Problem in Severe COVID-19
Reporter: Aviva Lev-Ari, PhD, RN
Is SARS-COV2 Hijacking the Complement and Coagulation Systems?
Reporter: Stephen J. Williams, PhD
New Etiology for COVID-19: Death results from Immune-Mediation (virus-independent immunopathology: lung and reticuloendothelial system) vs Pathogen-Mediation causing Organ Dysfunction & Hyper-Inflammation – Immunomodulatory Therapeutic Approaches (dexamethasone)
Curators: Stephen J. Williams and Aviva Lev-Ari, PhD, RN
Corticosteroid, Dexamethasone Improves Survival in COVID-19: Deaths reduction by 1/3 in ventilated patients and by 1/5 in other patients receiving oxygen only
Reporter: Aviva Lev-Ari, PhD, RN – bold face and color fonts added
SAR-Cov-2 is probably a vasculotropic RNA virus affecting the blood vessels: Endothelial cell infection and endotheliitis in COVID-19
Reporter: Aviva Lev-Ari, PhD, RN – Bold face and colors are my addition
UPDATED on 8/8/2020
Dmitry Korkin: Computational Biology of Coronavirus | AI Podcast #90 with Lex Fridman
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 7/25/2020
Severe COVID-19 in Patients experiencing Cytokine Storm: Positive Outcomes (faster respiratory recovery, a lower likelihood of mechanical ventilation, and fewer in-hospital deaths) of high dose methylprednisolone plus tocilizumab (Actemra, Genentech) vs Supportive Care Alone
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 7/24/2020
Oxford’s scientists explain the Phase I/II results for the COVID-19 vaccine
208K subscribers
UPDATED on 7/8/2020
SOURCE
From: Fierce Pharma <editors@fiercepharma.com>
Reply-To: <qx_fiercelifesciences@inbound.bamboocricket.com>
Date: Tuesday, July 7, 2020 at 12:52 PM
To: Aviva Lev-Ari <AvivaLev-Ari@alum.berkeley.edu>
Subject: | 07.07.20 | Regeneron, Novavax score COVID supply deals worth $2B total
UPDATED on 7/2/2020
TOP HEADLINES
- Chemo-induced Changes in Tumors Trigger Blood Vessel Anomalies
- Asthma Drug Salbutamol Inhibits Tau Filament Formation In Vitro
- Unprecedented Details of Tooth Enamel Structure Revealed
- SARS-CoV-2 Immunity Likely To Be Higher Than Antibody Testing Has Shown
- Deep Brain Stimulation for Parkinson’s Shows Long-term Efficacy
- Trial of Saliva Test for COVID-19 Launched
- New Strain of Swine Flu Is Something We “Need To Keep Our Eye On”
- SARS-CoV-2 Can Infect Heart Cells in a Lab Dish
- Findings From “Mini-brain” Study Suggest SARS-CoV-2 Can Infect Human Brain Cells
- How Our Brain Folds
SOURCE
From: Breaking Science News from Technology Networks <theeditor@technologynetworks.com>
Subject: SARS-CoV-2 Immunity Likely To Be Higher Than Antibody Testing Has Shown
Date: July 2, 2020 at 6:08:52 AM PDT
Reply-To: theeditor@technologynetworks.com
UPDATED on 6/28/2020
The Castleman Disease Research Network publishes Phase 1 Results of Drug Repurposing Database for COVID-19
Reporter: Stephen J. Williams, PhD
UPDATED on 6/28/2020
Corticosteroid, Dexamethasone Improves Survival in COVID-19: Deaths reduction by 1/3 in ventilated patients and by 1/5 in other patients receiving oxygen only
Reporter: Aviva Lev-Ari, PhD, RN – bold face and color fonts added
UPDATED on 6/22/2020
It’s the end of road for hydroxychloroquine in COVID-19 as Novartis, NIH and WHO pull out of trials
The road for hydroxychloroquine against COVID-19 is coming to an end. Three major clinical programs have been terminated after a U.K. trial found “no clinical benefit” for the malaria drug championed by U.S. President Donald Trump.
In the past few days, the World Health Organization (WHO), generic hydroxychloroquine (HCQ) maker Novartis and the U.S. National Institutes of Health (NIH) have all ended their HCQ COVID-19 studies in hospitalized patients in quick succession.
The WHO and NIH cited lack of benefits for patients, while Novartis blamed “acute enrollment challenges.”
Numerous investigator-sponsored trials may still be underway, but none of them has the scale of these three to yield any convincing results. Sanofi previously put a temporary halt to its own study based on safety concerns but has not since resumed recruitment, meaning the latest three terminations were likely the final judgement for HCQ’s use in COVID-19.
China first included HCQ in its COVID-19 treatment guidelines, but it was Trump who promoted the med to global attention after labeling it a “game changer.” Clinical trials were launched to prove its efficacy, and the FDA quickly doled out an emergency use authorization.
But several relatively small clinical trials, including an early one from China and a U.S. Department of Veterans Affairs study, have failed to find the drug’s worth. Its potential risk for serious side effects didn’t build confidence, either.
A controversial study in The Lancet previously led to a temporary halt of the HCQ arm in the WHO Solidarity trial, though it was soon resumed once the paper was found to be based on a dubious source of registry data and therefore was retracted by the authors.
Nevertheless, hope was still alive that a large, well-designed clinical trial would prove otherwise—until now.
Things took a rapid turn in early June. Researchers at the University of Oxford and the U.K. National Health Service said they stopped enrolling patients to the HCQ arm of a large, randomized U.K. trial dubbed Recovery after an independent data monitoring committee found “no beneficial effect” of HCQ in hospitalized patients. Specifically, the 28-day death rate for 1,542 patients who got HCQ was similar to that observed in 3,132 people on standard of care. HCQ treatment also didn’t lead to improvements in hospital stay duration or other clinical outcomes, the team said (PDF).
RELATED: FDA yanks chloroquine’s emergency OK after data show it doesn’t work against COVID-19
Days after that announcement, the FDA changed its mind and revoked HCQ’s emergency authorization. The agency based its decision on existing data, including on HCQ’s viral shedding improvement ability and those from the Recovery trial.
The WHO followed suit Wednesday by ending its HCQ study, citing its own observations and findings from the U.K. trial.
Friday, Novartis said it would discontinue its sponsored HCQ trial for COVID-19. “The recruitment challenge facing our HCQ trial has made it unlikely that the clinical team will be able to collect meaningful data in a reasonable timeframe to determine the effectiveness of HCQ in treating patients with COVID-19,” the Swiss drugmaker said in a statement.
Then, arguably adding the final nail in the HCQ COVID-19 coffin, the NIH also decided that its Orchid study of HCQ would no longer continue after a fourth interim analysis by an independent data monitoring panel found the drug provided no additional benefit over placebo control. More than 470 patients were already enrolled at that point.
SOURCE
UPDATED on 6/17/2020
We’re only 6 months into the worst pandemic in >100 years and it’s pretty impressive that a repurposed drug has now been shown to improve survival (putting aside mode of dissemination). Combos & more to come. The fatality rate should drop quite a bit by year end. That’s progress!
5:55 PM · Jun 16, 2020Twitter Web App


Replying to
It must come as a total suprise to the medical community that a very old immunosuppressive antiinflammatory, yet very, I mean very very cheap synthetic glucocorticoid saves lifes in an inflammatory disease with a “cytokine storm” sciencedirect.com/science/articl
Glucocorticoids and immune function: physiological relevance and pathogenic potential of hormonal dysfunction
Abstract
The more knowledge accumulates on the molecular action of glucocorticoids, the less appears to be known about the physiological relevance of these data. Mechanisms that determine bioactivity of glucocorticoids are largely neglected in studies on their molecular actions in immunoregulation. However, alterations of these mechanisms may contribute to the pathogenesis of acute or chronic inflammation, ranging from septic shock to autoimmune disease, or even acquired immuno deficiency syndrome. In this article, Thomas Wilckens attempts to challenge the long-standing dogma of glucocorticoids being only immunosuppressive in their action, and suggests a physiological role in which they are a prerequisite for a coordinated immune response.


Replying to

Replying to




Replying to


Replying to

Replying to
UPDATED on 6/5/2020
RAAS Inhibitors in COVID-19: A Signal of Benefit?
— No indication that ACE inhibitors, ARBs cause harm in Wuhan data
Hypertension and the discontinuation of blood pressure-lowering medications were associated with increased mortality in COVID-19, according to data from Wuhan, China.
People with high blood pressure (BP) were more likely to die during COVID-19 hospitalization (4.0% vs 1.1% without hypertension, adjusted HR 2.12, 95% CI 1.17-3.82), as were those with a history of hypertension who were not on antihypertensive medication (7.9% vs 3.2% on medications, adjusted HR 2.17, 95% CI 1.03-4.57).
Between those on renin-angiotensin-aldosterone system (RAAS) inhibitors and peers on other antihypertensives, mortality was similar (2.2% vs 3.6%, adjusted HR 0.85, 95% CI 0.28-2.58), reported Fei Li, MD, PhD, of Xijing Hospital in Xi’an, China, and colleagues in European Heart Journal.
But when data from three other groups in China were pooled in a meta-analysis, RAAS inhibitors — angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) — were associated with significantly lower risk of mortality compared to other BP-lowering drugs (RR 0.65, 95% CI 0.45-0.94).
This is “another paper with the tantalizing suggestion that RAAS inhibition might be effective in decreasing the severity of COVID-19 infection,” Harlan Krumholz, MD, of Yale School of Medicine, told MedPage Today. “We are really at the point where we need some trials to test this hypothesis. Fortunately, as before, there is no indication that these drugs cause harm associated with viral infection.”
It had been suspected that ACE inhibitors and ARBs might worsen the severity and mortality of COVID-19 by increasing expression of the ACE2 enzyme necessary for SARS-CoV-2 viral entry.
Cardiovascular societies maintain that patients with hypertension should continue their usual antihypertensive treatment with RAAS inhibitors.
Continued RAAS inhibition in COVID-19 is important because of the chronic kidney disease (CKD) that commonly accompanies hypertension, and CKD patients may require adequate BP control as part of their renal protection, according to an accompanying editorial by Luis Ruilope, MD, PhD, of Madrid’s Hospital Universitario 12 de Octubre, and colleagues.
“Furthermore, the withdrawal of RAAS blockers in these COVID-19 patients would increase the morbidity and mortality risk given the myocardial damage that may occur in COVID-19,” the editorialists added.
RAAS inhibition can also be helpful for its antithrombotic activity, Ruilope’s group noted. “In fact, hyperinflammation and derangement of the RAAS in COVID-19 could contribute to clinically suspected hypercoagulopathy and microvascular immunothrombosis.”
Li’s team performed a retrospective observational study of all 2,877 consecutive patients admitted to Huoshenshan Hospital from Feb. 5 to March 15 of this year. This emergency specialty field hospital had been built in Wuhan specifically to treat COVID-19.
Average age was around 60 years and over half of the cohort were men.
About 30% of the group had histories of hypertension, with 83.5% of those taking medications (RAAS inhibitors in more than one-quarter). Those on RAAS inhibitors shared similar medical history and baseline BP as those on the other medications.
Patients with hypertension tended to develop more severe or critical COVID-19 and require invasive mechanical ventilation, Li and colleagues reported.
The observational study was inherently limited by the potential for unmeasured confounding, according to the investigators, and stratification of patients by drug class led to groups that were not large enough for definitive comparisons.
In the meantime, the ongoing CORONACION trial is expected to provide crucial information on how people not known to be infected with SARS-CoV-2 fare on various antihypertensive drugs.
Disclosures
Li and Ruilope’s groups had no disclosures.
Primary Source
European Heart Journal
Secondary Source
European Heart Journal
SOURCE
UPDATED on 6/1/2020
SAR-Cov-2 is probably a vasculotropic RNA virus affecting the blood vessels: Endothelial cell infection and endotheliitis in COVID-19
Reporter: Aviva Lev-Ari, PhD, RN – Bold face and colors are my addition
UPDATED on 5/30/2020
SARS-CoV-2 is pre-adapted to Human Transmission, branches of evolution stemming from a less well-adapted human SARS-CoV-2-like virus have been found: The Role of SARS-CoV-2 Virus Progenitors for Future Virus Disease Transmission and Pandemic Re-Emergence
Reporter and Curator: Aviva Lev-Ari, PhD, RN – all bold face and colors are my additions
UPDATED on 5/29/2020
COVID-19: Novel Treatment Protocols using Approved drugs vs Standard of Care vs Vaccine and Antiviral new drug discovery and development – An LPBI Group Response and An LPBI Group & Affiliates Response
Curator: Aviva Lev-Ari, PhD, RN
UPDATED on 5/25/2020
T cells found in COVID-19 patients ‘bode well’ for long-term immunity | Science | AAAS
https://www.sciencemag.org/news/2020/05/t-cells-found-covid-19-patients-bode-well-long-term-immunity
Clinical Trial for the Use of Nitric Oxide to Treat Severe COVID-19 Infection
UPDATED ON 5/23/2020
RNA from the SARS-CoV-2 virus taking over the cells it infects: Virulence – Pathogen’s ability to infect a Resistant Host: The Imbalance between Controlling Virus Replication versus Activation of the Adaptive Immune Response
Curator: Aviva Lev-Ari, PhD, RN – I added colors and bold face
UPDATED ON 5/19/2020
A Series of Recently Published Papers Report the Development of SARS-CoV2 Neutralizing Antibodies and Passive Immunity toward COVID19
Curator: Stephen J. Williams, Ph.D.
UPDATED ON 5/17/2020
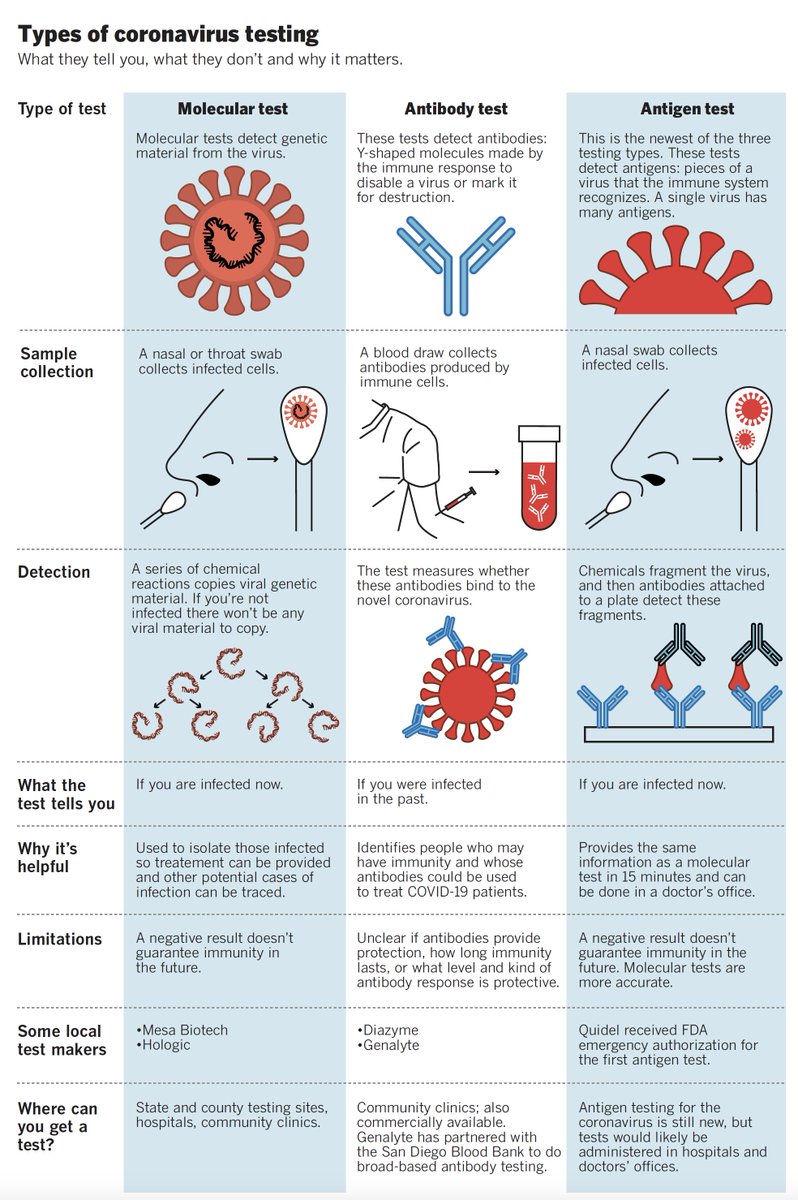
Having trouble keeping track of all the types of coronavirus tests that are out there? For a breakdown of what each test does, how it works, and why that matters, check out this graphic
and I made for
Quote Tweet
Eric Topol@EricTopol·With the recent approval of an antigen test, there are now 3 categories of #SARCoV2 testing. This is a very good infographic in today’s @sdut by @JonathanWosen @ms_gilchristShow this thread


UPDATED ON 5/16/2020
Targets of T cell responses to SARS-CoV-2 coronavirus in humans with COVID-19 disease and unexposed individuals
Highlights
- Measuring immunity to SARS-CoV-2 is key for understanding COVID19 and vaccine development
- Epitope pools detect CD4+ and CD8+ T cells in 100 and 70% of convalescent COVID patients
- T cell responses are focused not only on spike but also on M, N and other ORFs
- T cell reactivity to SARS-CoV-2 epitopes is also detected in non-exposed individuals
Summary
Understanding adaptive immunity to SARS-CoV-2 is important for vaccine development, interpreting coronavirus disease 2019 (COVID-19) pathogenesis, and calibration of pandemic control measures. Using HLA class I and II predicted peptide ‘megapools’, circulating SARS-CoV-2−specific CD8+ and CD4+ T cells were identified in ∼70% and 100% of COVID-19 convalescent patients, respectively. CD4+ T cell responses to spike, the main target of most vaccine efforts, were robust and correlated with the magnitude of the anti-SARS-CoV-2 IgG and IgA titers. The M, spike and N proteins each accounted for 11-27% of the total CD4+ response, with additional responses commonly targeting nsp3, nsp4, ORF3a and ORF8, among others. For CD8+ T cells, spike and M were recognized, with at least eight SARS-CoV-2 ORFs targeted. Importantly, we detected SARS-CoV-2−reactive CD4+ T cells in ∼40-60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.Article Info
Publication History
Accepted: May 7, 2020Received in revised form: May 4, 2020Received: April 20, 2020Publication stage
In Press Accepted Manuscript
Footnotes
Lead Contact: alex@lji.org (A.S.)
Identification
Copyright
© 2020 Elsevier Inc.ScienceDirect
Related Articles
- SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor
Hoffmann et al.CellMarch 05, 2020Open Access
- Structural and Functional Basis of SARS-CoV-2 Entry by Using Human ACE2
Wang et al.CellApril 09, 2020Open Access
- Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19
Blanco-Melo et al.CellMay 15, 2020Open Access
- Inhibition of SARS-CoV-2 Infections in Engineered Human Tissues Using Clinical-Grade Soluble Human ACE2
Monteil et al.CellApril 24, 2020Open Access
- Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein
Walls et al.CellMarch 09, 2020
SOURCE
https://www.cell.com/cell/fulltext/S0092-8674(20)30610-3
UPDATED ON 5/8/2020
remdesivir
SOURCE From: FiercePharma <editors@FiercePharma.com> Reply-To: <qx_fiercelifesciences@inbound.bamboocricket.com> Date: Friday, May 8, 2020 at 1:18 PM To: Aviva Lev-Ari <AvivaLev-Ari@alum.berkeley.edu> Subject: | 05.08.20 | Gilead faces a no-win choice on remdesivir price; missteps, access questions dog U.S. rollout |
UPDATED ON 5/4/2020
The Genome Structure of CORONAVIRUS, SARS-CoV-2
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 5/3/2020
 by JNS.org
by JNS.org
Israeli Biotech Company Starts Clinical Trials of CBD-Steroid Treatment for Virus
Stero Biotechs Announce an IP Protected Clinical Trial for COVID-19 Patients Using a CBD-Steroid Treatment
TEL AVIV, Israel, April 20, 2020 /PRNewswire/ — Stero Biotechs, an Israel-based, clinical-stage company focused on Cannabidiol (CBD) formulation research and development, in a collaboration with its main partner and shareholder, Mor Research Applications, the Tech Transfer Office (TTO) of the largest Health Maintenance Organiztaion (HMO) in Israel – Clalit, announced today a new clinical trial in the global efforts of fighting the COVID-19 virus.
The study, which will commence immediately, is a small-scale clinical trial at Rabin Medical Center Golda HaSharon Campus, treating 10 patient treatment as a ‘POC’, estimated to start in April (pending final Helsinki Committee approval). The study aims to benefit and help hospitalized patients with COVID-19 infection. The treatment cycle will be for a few weeks with a subsequent follow-up period of the same length.
Under Stero’s allowed IP and pending the success of this ‘POC’, Stero plans to scale up and expand to a phase 2a multi-center clinical trial, with an additional 40 hospitalized patients with COVID-19 Infections, under FDA clinical trial guidelines and regulations.
Stero has an extremely wide covering patent, already granted in the US. The patent has extremely wide coverage, covering over 130 Autoimmune and inflammatory diseases by name, CBD from any source (synthetic or botanic), CBD in any combination, CBD in any dosage and in any delivery system. Enhancing the therapeutic effect for Steroid treated patients with CBD is fully covered within Stero’s allowed IP.
Steroid treatment is usually the first or second line of treatment for hospitalized patients. CBD enhances the therapeutic effect of steroid treatment and treats the bio-mechanism affected by the virus. The initial study will evaluate the tolerability, safety, and efficacy of the CBD treatment, for hospitalized patients with COVID-19 Infections.
David Bassa, Founder & CEO of Stero Biotechs said: “We estimate that our CBD-based treatment can enhance the current treatment of those patients who are in life-threatening conditions. Hospitalized COVID-19 patients are mostly being treated with steroids and our study is planned to demonstrate the benefit of a combined solution with Steroid treatments. We are hopeful that this study will lead to faster benefit for the growing number of COVID-19 patients in Israel and around the world.”
About Stero Biotechs, Ltd.
STERO Biotechs Ltd., founded in 2017 and headquartered in Israel, is a clinical-stage company committed to the research and development of novel Cannabidiol (CBD) based treatment solutions that will potentially benefit millions of patients. Stero’s solution enhances the therapeutic effect of steroid treatments, allowing treatments to act more effectively. Simultaneously, the solution reduces dosage and side effects and the need for steroid therapy. STERO was granted a U.S. patent on over 130 potential indications and is planning to commence more clinical trials on various indications.
For inquiries, contact mail@sterobiotechs.com or call +972-3-617-6173
SOURCE
https://finance.yahoo.com/news/stero-biotechs-announce-ip-protected-130000539.html
Updated on 5/3/2020
https://www.nytimes.com/2020/05/01/health/coronavirus-remdesivir.html#click=https://t.co/zJU7ZQlEH4
How Remdesivir, New Hope for Covid-19 Patients, Was Resurrected
The drug failed as a treatment for hepatitis and Ebola. With federal funding, scientists trained it on the coronavirus.
By Gina Kolata
May 1, 2020
Remdesivir, an antiviral drug designed to treat both hepatitis and a common respiratory virus, seemed fated to join thousands of other failed medications after proving useless against those diseases. The drug was consigned to the pharmaceutical scrap heap, all but forgotten by the scientists who once championed it.
But on Friday, the Food and Drug Administration issued an emergency approval for remdesivir as a treatment for patients severely ill with Covid-19, the disease caused by the coronavirus.
The story of remdesivir’s rescue and transformation testifies to the powerful role played by federal funding, which allowed scientists laboring in obscurity to pursue basic research without obvious financial benefits. This research depends almost entirely on government grants.
Dr. Mark Denison of Vanderbilt University is one of a handful of researchers who discovered remdesivir’s potential. He began studying coronaviruses a quarter-century ago, a time when few scientists cared about them — the ones infecting humans caused colds, he recalled, and scientists just wanted to know how they worked.
“We were interested from the biologic perspective,” Dr. Denison recalled. “No one was interested from a therapeutic perspective.”
Neither he nor the scores of other scientists interested in coronaviruses foresaw that a new one would unleash a plague that has killed nearly a quarter-million people worldwide. The F.D.A. rushed to approve remdesivir under emergency use provisions, after a federal trial demonstrated modest improvements in severely ill patients.
The trial, sponsored by the National Institute of Allergy and Infectious Diseases, included more than 1,000 hospitalized patients and found that those receiving remdesivir recovered faster than those who got a placebo: in 11 days, versus 15 days.
But the drug did not significantly reduce fatality rates, and some critics noted that the trial’s primary endpoint — its measure of success — had been greatly simplified to emphasize time to recovery.
A half-dozen experts contacted by The Times on Thursday said the change was necessary. Officials at N.I.A.I.D. said biostaticians urging the revision had not seen the data and were not aiming for a particular result.
Dr. Anthony S. Fauci, director of the institute, said the results were “a very important proof of concept” but not a “knockout.” President Trump hailed the drug on Friday as “an important treatment” and “really promising.”
Remdesivir is approved only for severely ill patients and only temporarily; formal approval must come later. Still, some doctors laboring in intensive care units embraced the drug as an important new weapon against a virus that is killing patients worldwide.
“It’s a great first step,” said Dr. Robert Finberg, chairman of the department of medicine at the University of Massachusetts Medical School.
Little about the early history of remdesivir, manufactured by Gilead Sciences, suggested the hopes now placed upon it.
Coronaviruses hold much more RNA than scientists once theorized a virus could. Many viruses that cause epidemics rely on this type of genetic material, and almost all mutate constantly. That is why flu viruses change from year to year.
Yet coronaviruses did not change much — their mutation rate is about one-twentieth the rate of other RNA viruses.
In 2007, Dr. Denison discovered that coronaviruses have a powerful “proofreading” system. If an error occurs in copying RNA as the coronavirus replicates, it corrects the error. In lab experiments, coronaviruses that mutated were weaker, outcompeted by those without mutations.
Dr. Denison and other experts wondered if it might be possible to trick the virus with a drug that dodged the proofreading system and blocked the virus’s growing RNA chain, making it prematurely terminate.
Talking about this problem with another scientist at a meeting, Dr. Denison learned that Gilead Sciences had dozens of drugs that might do the trick. “All of these compounds had been shelved for one reason or another,” Dr. Denison said.
Most worked in lab tests to shut down coronaviruses, he found — some better than others. One of the best was GS-5734, now known as remdesivir. “I like to call it the Terminator,” Dr. Denison said.
Dr. Denison discovered remdesivir was just what they were seeking: a drug that slipped past the viruses’s powerful system to protect RNA, their genetic material. Remdesivir made growing chains of the viral RNA terminate prematurely, killing the virus.
Vials of remdesivir at a Gilead Sciences facility in La Verne, Calif.Gilead Sciences, via Reuters
Remdesivir killed every known coronavirus in Dr. Denison’s tests. Then researchers at the University of North Carolina found that the drug also killed the viruses in infected animals.
That included not just coronaviruses that cause the common cold, but also SARS and MERS — even a coronavirus that infects only mice.
But the drug failed a number of real-life tests, not just against hepatitis but also against Ebola in Africa. The drug languished, unapproved for any use — until a new coronavirus emerged.
As SARS-CoV-2, the virus that causes Covid-19, began to grow into a pandemic, many scientists realized that remdesivir might be the best solution at hand. It had already undergone animal testing and safety testing in humans.
So doctors began giving it to patients in studies without controls and even outside of studies altogether. Anecdotes fueled demand. Gilead sponsored some of these studies and gave the drug to doctors who treated hundreds of patients under compassionate use, a legal exemption permitting use of an unapproved drug to treat patients.
SOURCE
https://www.nytimes.com/2020/05/01/health/coronavirus-remdesivir.html#click=https://t.co/zJU7ZQlEH4
UPDATED on 5/1/2020
Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency
- Calvin J Gordon1,
- Egor P Tchesnokov1,
- Emma Woolner1,
- Jason K Perry2,
- Joy Y. Feng3,
- Danielle P Porter4 and
- Matthias Gotte5*
+Author Affiliations
- ↵* Corresponding author; email: gotte@ualberta.ca
Abstract
Effective treatments for coronavirus disease 2019 (COVID-19) are urgently needed to control this current pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Replication of SARS-CoV-2 depends on the viral RNA-dependent RNA polymerase (RdRp), which is the likely target of the investigational nucleotide analogue remdesivir (RDV). RDV shows broad-spectrum antiviral activity against RNA viruses, and previous studies with RdRps from Ebola virus (EBOV) and Middle East respiratory syndrome coronavirus (MERS-CoV) have revealed that delayed chain-termination is RDV’s plausible mechanism of action. Here, we expressed and purified active SARS-CoV-2 RdRp composed of the non-structural proteins nsp8 and nsp12. Enzyme kinetics indicated that this RdRp efficiently incorporates the active triphosphate form of RDV (RDV-TP) into RNA. Incorporation of RDV-TP at position i caused termination of RNA synthesis at position i+3. We obtained almost identical results with SARS-CoV, MERS-CoV, and SARS-CoV-2 RdRps. A unique property of RDV-TP is its high selectivity over incorporation of its natural nucleotide counterpart ATP. In this regard, the triphosphate forms of 2’-C–methylated compounds, including sofosbuvir, approved for the management of hepatitis C virus infection, and the broad-acting antivirals favipiravir and ribavirin, exhibited significant deficits. Furthermore, we provide evidence for the target specificity of RDV, as RDV-TP was less efficiently incorporated by the distantly related Lassa virus RdRp, and termination of RNA synthesis was not observed. These results collectively provide a unifying, refined mechanism of RDV-mediated RNA synthesis inhibition in coronaviruses and define this nucleotide analogue as a direct-acting antiviral (DAA).
Footnotes
Author contributions: C.J.G., E.P.T., and M.G. data curation; C.J.G., E.P.T., J.K.P., and M.G. software; C.J.G., E.P.T., and M.G. formal analysis; C.J.G., E.P.T., and M.G. validation; C.J.G., E.P.T., E.W., J.K.P., and M.G. investigation; C.J.G., E.P.T., and M.G. visualization; C.J.G., E.P.T., E.W., J.K.P., and M.G. methodology; E.P.T. and M.G. conceptualization; E.P.T. and M.G. writing-original draft; E.P.T., J.K.P., J.Y.F., D.P.P., and M.G. writing-review and editing; M.G. resources; M.G. supervision; M.G. funding acquisition; M.G. project administration.
- Received March 30, 2020.
- Accepted April 13, 2020.
- Published under license by The American Society for Biochemistry and Molecular Biology, Inc.
UPDATED on 4/28/2020
Researchers Map Structure of Coronavirus “Spike” Protein
The finding could help lay the groundwork for a vaccine
https://www.scientificamerican.com/article/researchers-map-structure-of-coronavirus-spike-protein/
New Images of Novel Coronavirus SARS-CoV-2 Now Available
NIAID Now | February 13, 2020
This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (blue/pink) cultured in the lab.
Credit: NIAID-RMLNIAID’s Rocky Mountain Laboratories (RML) in Hamilton, Montana, produced images of the novel coronavirus (SARS-CoV-2, previously known as 2019-nCoV) on its scanning and transmission electron microscopes on Tuesday, Feb. 11, 2020. SARS-CoV-2 causes COVID-19 disease, which has grown to be a global public health emergency since cases were first detected in Wuhan, China, in December 2019. RML investigator Emmie de Wit, Ph.D., provided the virus samples as part of her studies, microscopist Elizabeth Fischer produced the images, and the RML visual medical arts office digitally colorized the images.
Note that the images do not look much different from MERS-CoV (Middle East respiratory syndrome coronavirus, which emerged in 2012) or the original SARS-CoV (severe acute respiratory syndrome coronavirus, which emerged in 2002). That is not surprising: The spikes on the surface of coronaviruses give this virus family its name – corona, which is Latin for “crown,” and most any coronavirus will have a crown-like appearance.
These images are available to the public for free high-resolution download on the NIAID Flickr page. NIAID asks all who use the images to please credit NIAID-RML unless otherwise noted in the Flickr image description.
https://www.flickr.com/photos/niaid/49645402917/in/album-72157712914621487

Contact Information
Contact the NIAID Media Team.
Scientists know that SARS-CoV-2 is mutating
Among the thousands of samples of the long strand of RNA that makes up the coronavirus, 11 mutations have become fairly common. But as far as we know, it’s the same virus infecting people all over the world, meaning that only one “strain” of the virus exists, said Peter Thielen, a molecular biologist with the Johns Hopkins Applied Physics Laboratory.
Only one of those common mutations affects the “spike protein,” which enables the virus to infect cells in the throat and lungs. Efforts to produce antibodies that block the spike protein are central to many efforts to develop a vaccine. Since the spike protein has changed little so far, some scientists believe that’s a sign that it can’t alter itself very much and remain infectious.
There’s still a lot about the virus we don’t know. We don’t even know if people are immune to the virus if they’ve caught it already, nor how long that immunity could last, though work is well underway to understand these things.
Mr. Thielen says it is still unclear how those mutations in the genome will ultimately affect countermeasures like a vaccine.
“We just have to keep looking,” he said.
The new coronavirus is mutating, but very slowly
The new coronavirus is an RNA virus: a collection of genetic material packed inside a protein shell.
Once an RNA virus makes contact with a host, it starts to make new copies of itself that can go on to infect other cells.
RNA viruses, like the flu and measles, are more prone to changes and mutations compared with DNA viruses, such as herpes, smallpox, and human papillomavirus (HPV).
“In the world of RNA viruses, change is the norm. We expect RNA viruses to change frequently. That’s just their nature,” said Dr. Mark Schleiss, a pediatric infectious disease specialist and investigator with the Institute for Molecular Virology at the University of Minnesota.
SARS-CoV-2 is no exception, and over the past few months it has been mutating.
But the virus has mutated at a very slow pace. And when it does mutate, the new copies aren’t far off from the original virus.
“The sequences of the original isolates from China are very close to those in viruses circulating in the U.S. and the rest of the world,” said Dr. John Rose, a senior research scientist in the department of pathology at Yale Medicine who’s helping develop a COVID-19 vaccine.
SOURCE
Patient-derived mutations impact pathogenicity of SARS-CoV-2
Abstract
The sudden outbreak of the severe acute respiratory syndrome-coronavirus (SARS-CoV-2) has spread globally with more than 1,300,000 patients diagnosed and a death toll of 70,000. Current genomic survey data suggest that single nucleotide variants (SNVs) are abundant. However, no mutation has been directly linked with functional changes in viral pathogenicity. Here we report functional characterizations of 11 patient-derived viral isolates, all of which have at least one mutation. Importantly, these viral isolates show significant variation in cytopathic effects and viral load, up to 270-fold differences, when infecting Vero-E6 cells. We observed intrapersonal variation and 6 different mutations in the spike glycoprotein (S protein), including 2 different SNVs that led to the same missense mutation. Therefore, we provide direct evidence that the SARS-CoV-2 has acquired mutations capable of substantially changing its pathogenicity.
Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
This work was supported by funds from Major Project of Zhejiang Provincial Science and Technology Department #2020C03123, National Science and Technology Major Project for the Control and Prevention of Major Infectious Diseases in China (2018ZX10711001, 2018ZX10102001, 2018ZX10302206), and start-up funds from Life Sciences Institute at Zhejiang University;
Author Declarations
All relevant ethical guidelines have been followed; any necessary IRB and/or ethics committee approvals have been obtained and details of the IRB/oversight body are included in the manuscript.
SOURCE
https://www.medrxiv.org/content/10.1101/2020.04.14.20060160v2
UPDATE on 4/28/2020
How artificial intelligence is helping scientists find a coronavirus treatment
Photo/Getty ImagesAn illustration of COVID-19
More than 50,000 academic articles have been written about COVID-19 since the virus appeared in November.
The volume of new information isn’t necessarily a good thing.
Not all of the recent coronavirus literature has been peer reviewed, while the sheer number of articles makes it challenging for accurate and promising research to stand out or be further studied.
Computer science and linguistics professor James Pustejovsky is leading a Brandeis team in creating an artificial intelligence platform called Semantic Visualization of Scientific Data — or SemViz — that can sort through the growing mass of published work on coronavirus and help biologists who study the disease gain insights and notice patterns and trends across research that could lead to a treatment or cure.
Pustejovsky, an expert in theoretical and computational modeling and language, is partnering with colleagues at Tufts University, Harvard University, the University of Illinois, and Vassar College. He discussed his work with BrandeisNOW.
Can you provide a bird’s-eye view of the way you’ve applied your background as a computational linguist to current coronavirus research?
I’m a researcher who focuses on language and extracting information from large amounts of text, like the COVID-19 dataset, which now includes more than 50,000 academic articles. Biologists on the front lines of coronavirus are trying to find connections between genes, proteins and drugs, and how they interact with the virus in the cells of the human body.
SemViz combs through the existing papers and manuscripts and enables scientists to make connections and generalizations that are not obvious from reading one paper at a time.
So how might a biologist studying coronavirus actually use SemViz?
This tool gives a rapid way for biologists studying coronavirus to see a global overview of inhibitors, regulators, and activators of genes and proteins involved in the disease.
For example, what are the drugs and proteins regulating the receptor for the COVID-19 virus? This could help discover therapies that decrease the expression of the receptor for the virus in patients’ lungs. This is important because millions of people currently take blood pressure medicines that can alter this receptor and possibly increase their risk of contracting the disease.
SemViz creates a visualization landscape that helps biologists make both global and specific connections between human genes, drugs, proteins and viruses. The overall program I’m working on contains three components: two semantic visualization outputs based on the entire coronavirus research dataset, as well as a natural language-based question-answering application.
What’s the language application grid and how does it work?
It is essentially a computer-based “reading machine” that interprets tens of thousands of research articles on coronavirus and presents the results of this process to biologists in a form that is visually accessible and easily analyzed and interpreted.
It is more informative than a search engine, because it utilizes a host of language understanding tools and AI that can be applied to different domains (economics, news, science, literature) and text types (tweets, articles, books, email).
What are the implications of SemViz?
I think it’s hard to overstate the challenge brought about by information overload, particularly now with the coronavirus literature.
Biologists are interested in the mechanisms and functions of specific chemicals and proteins. SemViz can be the roadmap that scientists use to sort through large amounts of research to find these kinds of functions and relationships.
SOURCE
https://www.brandeis.edu/now/2020/april/artificial-intelligence-coronavirus.html
UPDATED on 4/24/2020
Human monoclonal antibodies block the binding of SARS-CoV-2 spike protein to angiotensin converting enzyme 2 receptor
Xiangyu Chen1 , Ren Li2,3, Zhiwei Pan1 , Chunfang Qian4 , Yang Yang1 , Renrong You5 , Jing Zhao6 , Pinghuang Liu5 , Leiqiong Gao1 , Zhirong Li1 , Qizhao Huang7 , Lifan Xu1 , Jianfang Tang1 , Qin Tian1 , Wei Yao1 , Li Hu1 , Xiaofeng Yan4 , Xinyuan Zhou 1 , Yuzhang Wu1 , Kai Deng 8 , Zheng Zhang9 , Zhaohui Qian10, Yaokai Chen4 and Lilin Ye 1
1 Institute of Immunology, PLA, Third Military Medical University, Chongqing 400038, China;
2 State Key Laboratory of Veterinary Biotechnology, Harbin Veterinary Research Institute, Chinese Academy of Agricultural Sciences, Harbin, Heilongjiang 150001, China;
3 College of Veterinary Medicine, Northeast Agricultural University, Harbin Heilongjiang 150030, China;
4 Chongqing Public Health Medical Center, Chongqing 400038, China;
5 Comparative Immunology Research Center, College of Veterinary Medicine, China Agricultural University, Beijing 100193, China;
6 Biomedical Analysis Center, Third Military Medical University, Chongqing 400038, China;
7 Cancer Center, The General Hospital of Western Theater Command, Chengdu, Sichuan 610083, China;
8 Institute of Human Virology, Zhongshan School of Medicine, Sun Yat-sen University, Guangzhou, Guangdong 510080, China;
9 Institute for Hepatology, National Clinical Research Center for Infectious Disease, Shenzhen Third People’s Hospital, Shenzhen, Guangdong 518112, China and
10 NHC Key laboratory of Systems Biology of Pathogens, Institute of Pathogen Biology, Chinese Academy of Medical Sciences and Peking Union Medical College, 100176 Beijing, China
Correspondence: Zhaohui Qian (zqian2013@sina.com) or Yaokai Chen (yaokaichen@hotmail.com) or Lilin Ye (yelilinlcmv@tmmu.edu.cn)
These authors contributed equally: Xiangyu Chen, Ren Li, Zhiwei Pan, Chunfang Qian
Cellular & Molecular Immunology _#####################_ ; https://doi.org/10.1038/s41423-020-0426-7
Cite this article
Chen, X., Li, R., Pan, Z. et al. Human monoclonal antibodies block the binding of SARS-CoV-2 spike protein to angiotensin converting enzyme 2 receptor. Cell Mol Immunol (2020). https://doi.org/10.1038/s41423-020-0426-7
Received
Accepted
Published
DOI https://doi.org/10.1038/s41423-020-0426-7
According to the World Health Organization (WHO) newly updated situation report on March 18th, 2020, the coronavirus disease 2019 (COVID-19) pandemic has confirmed 191,127 cases and claimed 7807 deaths worldwide.1 The etiological agent of COVID-19 has been identified as a novel coronavirus, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), belonging to Sarbecovirus subgenus (genus Betacoronavirus, family Coronaviridae) and showing 79.6 and 96.2% sequence identity in nucleotide to SARS-CoV and a bat coronavirus (BatCoV RaTG13), respectively.2,3,4 Like SARS-CoV infection, a substantial fraction of COVID-19 patients exhibits severe respiratory symptoms and has to be hospitalized in intensive care unit.5,6,7,8 Although the mortality rate of COVID-19 is significantly lower than that of SARS-CoV infection, SARS-CoV-2 shows much higher human-to-human transmission rate, rapidly leading to a global pandemic declared by WHO on March 11th, 2020.9
Currently, there are no approved prophylactic vaccines or therapeutic drugs that are specific to COVID-19. Blocking monoclonal antibodies (mAbs), due to their extraordinary antigen specificity, are one of the best candidates for neutralizing virus infection.10,11 Therefore, identifying and cloning blocking mAbs that can specifically target surface viral proteins to block the viral entry to host cells is a very attractive approach for preventing and treating COVID-19, in particular when effective vaccines and therapeutics are unavailable in the outbreak of the COVID-19 pandemic. We then sought to identify and clone blocking mAbs from the memory B cell repertoire of recently recovered COVID-19 patients to prevent the entry of COVID-19 virus to the host cells.
Similar to SARS-CoV, SARS-CoV-2 also utilizes highly glycosylated homotrimeric spike (S) protein for receptor binding and virus entry.3,12,13,14,15 The S protein of SARS-CoV-2 consists of two subunits, S1 and S2. To engage host cell receptor human angiotensin-converting enzyme 2 (hACE2), shared by both SARS-CoV and SARS-CoV-2, S protein undergoes dramatic conformational changes to expose the RBD and key residues for receptor binding. S protein is metastable, and binding of RBD to hACE2 receptor likely leads to the shedding of S1 protein from S2 protein, thus promoting S2-mediated virus-host membrane fusion and virus entry.16,17,18 Given the critical role of the RBD in initiating invasion of SARS-CoV-2 into host cells, it becomes a vulnerable target for neutralizing antibodies. Thus far, the human mAbs specifically target the SARS-CoV-2 RBD-hACE2 interaction have not been reported, and a monoclonal antibody targeting S1 made from immunized transgenic mice expressing human Ig variable heavy and light chains has been recently shown to neutralize both SARS-CoV-2 and SARS-CoV infection, but by an unknown mechanism that is independent of the blockade of RBD-hACE2 interaction.19
Finally, we expressed these paired plasmids encoding IgG VH and VL sequences and named these three mAbs as 311mab–31B5, 311mab–32D4 and 311mab–31B9, respectively. We first examined whether these human mAbs were able to bind to SARS-CoV-2 RBD protein by ELISA. The results showed that all three mAbs strongly and specifically bind to the RBD protein (Fig. 1f). Next, we tested whether these mAbs can block the interaction between SARS-CoV-2 RBD and hACE2. We found that both 311mab-31B5 and 311mab-32D4 could efficiently block SARS-CoV-2 RBD-hACE2 interaction (IC50 = 0.0332, and 0.0450 μg/ml, respectively), while 311mab–31B9 clone failed to inhibit such an interaction (Fig. 1g). The 31B5- and 32D4-mediated inhibition of RBD-hACE2 interaction was also evidenced by flow cytometry analysis (Fig. 1h, i). Furthermore, we determined the neutralization of these three mAbs using a SARS-CoV-2 S pseudotyped lentiviral particle.22 In line with ELISA- and flow cytometry-based blockade results, both 311mab-31B5 and 311mab-32D4 effectively neutralized pseudovirus entry to host cells ectopically expressing hACE2 (IC50 = 0.0338, and 0.0698 μg/ml, respectively). As expected, 311mab-31B9 clone failed to show any neutralization activities (Fig. 1j).
In conclusion, we have successfully cloned two human blocking mAbs using SARS-CoV-2 RBD-specific memory B cells isolated from recovered COVID-19 patients. These two mAbs can specifically bind to SARS-CoV-2 RBD, block the interaction between SARS-CoV-2 RBD and hACE2 receptor, and lead to efficient neutralization of SARS-CoV-2 S protein pseudotyped virus infection. Such human anti-SARS-CoV-2 RBD-hACE2 blocking mAbs are first reported, and hold great promise to be exploited as specific prophylactic and therapeutic agents against ongoing SARS-CoV-2 pandemic.
SOURCE
See References in following link
https://www.nature.com/articles/s41423-020-0426-7
https://www.nature.com/articles/s41423-020-0426-7.pdf
UPDATED on 4/23/2020
Gilead’s hopeful Covid-19 drug failed, errantly posted WHO report says

Daniel O’Day is the chairman and CEO of Gilead Sciences Inc.

One of the leading drug candidates against Covid-19 — Gilead Sciences Inc.’s remdesivir — apparently failed a closely watched clinical trial. But the company said the results of the study by doctors in China are inconclusive.
A mistakenly posted and now-removed draft document Thursday on the website of the World Health Organization, first reported by the health news website Stat, suggested that remdesivir failed to show improvements for Covid-19 patients or to prevent them from dying.
Foster City-based Gilead (NASDAQ: GILD), led by Chairman and CEO Daniel O’Day, said the late-stage clinical trial was stopped early because of low enrollment, muddying the study’s statistical outcomes.
“Importantly, because this study was terminated early due to low enrollment, it was underpowered to enable statistically meaningful conclusions,” Gilead spokesman Chris Ridley said in an email. “As such, the study results are inconclusive, though trends in the data suggest a potential benefit for remdesivir, particularly among patients treated early in disease.”
The confusion over the study’s data and what they mean in the grand scheme of remdesivir — a drug that failed in the clinic as a treatment for Ebola virus and is the subject of multiple doctor and company-sponsored Covid-19 trials — is part of the anxious world of Covid-19.
Along with Gilead’s drug, multiple companies are working on treatments or vaccines.
Two remdesivir trials by investigators in China were stopped early because of low enrollment, with some taking that as a positive because China has fewer Covid-19 patients and some taking it as a knock against the Gilead drug. What’s more, one site’s leaked positive results last week in a trial sponsored by the company were similarly praised and bashed.
The multiple studies of remdesivir “will help inform whom to treat, when to treat and how long to treat with remdesivir,” company spokesman Ridley said. “The studies are either fully enrolled for the primary analysis or on track to fully enroll in the near future.”


The China trial referenced in the WHO report, according to Stat, was meant to enroll 453 patients. The double-blinded study ultimately put 158 patients on remdesivir and 79 in the control arm, Stat said, who received daily infusions of the drug or placebo for 10 days.
UPDATED on 4/23/2020
Moderna Highlights Opportunity of mRNA Vaccines at its First Vaccines Day
Vaccines create significant value for healthcare systems by preventing infectious disease; despite this, the vast majority of viruses do not have commercial vaccines available, representing a large opportunity
Moderna has demonstrated neutralizing immunogenicity against all eight viruses targeted in clinical trials to date using the Company’s innovative vaccine platform
First interim analysis of Phase 1 Zika vaccine candidate (mRNA-1893) study shows that 10 µg and 30 µg dose levels seroconverted 94% and 100% of seronegative participants, respectively, and effectively boosted seropositive participants; both dose levels generally well-tolerated
NIH-led Phase 1 study of mRNA-1273, Moderna’s vaccine candidate against the novel coronavirus, continues on track with enrollment of participants at the highest dose
Virtual Vaccines Day to be held at 8:00 a.m. ET on Tuesday, April 14
About Moderna’s Prophylactic Vaccines Modality
Moderna scientists designed the Company’s prophylactic vaccines modality to prevent infectious diseases. More than 1,400 participants have been enrolled in Moderna’s infectious disease vaccine clinical studies under health authorities in the U.S., Europe and Australia. Based on clinical experience across seven Phase 1 studies, the Company has designated prophylactic vaccines a core modality and is working to accelerate the development of its vaccine pipeline.
Moderna currently has nine development candidates in its prophylactic vaccines modality, including:
Vaccines against respiratory infections
- Respiratory syncytial virus (RSV) vaccine for older adults (mRNA-1777 and mRNA-1172 or V172 with Merck)
- RSV vaccine for young children (mRNA-1345)
- Human metapneumovirus (hMPV) and parainfluenza virus type 3 (PIV3) combination vaccine (mRNA-1653)
Novel coronavirus (SARS-CoV-2) vaccine (mRNA-1273)
- Influenza H7N9 (mRNA-1851)
Vaccines against infections transmitted from mother to baby
- Cytomegalovirus (CMV) vaccine (mRNA-1647)
- Zika vaccine (mRNA-1893 with BARDA)
Vaccines against highly prevalent viral infections
- Epstein-Barr virus (EBV) vaccine (mRNA-1189)
To date, Moderna has demonstrated positive Phase 1 data readouts for seven prophylactic vaccine candidates (H10N8, H7N9, RSV, chikungunya virus, hMPV/PIV3, CMV and Zika). Moderna’s CMV vaccine candidate is currently in a Phase 2 dose-confirmation study.
Virtual Vaccines Day Today
Moderna will host a virtual Vaccines Day today, Tuesday April 14th,beginning at 8:00 a.m. ET. A live webcast will be available under “Events and Presentations” in the Investors section of the Moderna website at investors.modernatx.com. A replay of the webcast will be archived on Moderna’s website for one year following the presentation.
SOURCE
UPDATED on 4/16/2020
Updated listing of COVID-19 vaccine and therapeutic trials from NIH Clinical Trials.gov
Curator: Stephen J. Williams, PhD
UPDATED on 4/14/2020
Actemra, immunosuppressive which was designed to treat rheumatoid arthritis but also approved in 2017 to treat cytokine storms in cancer patients SAVED the sickest of all COVID-19 patients
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 4/13/2020

SOURCE
From: Ribograma Alvaro FERREIRA-ALEMAO MD PhD <ribograma@gmail.com>
Date: Monday, April 13, 2020 at 3:10 PM
To: Aviva Lev-Ari <AvivaLev-Ari@alum.berkeley.edu>
Subject: Fwd: Present Trials on COVID-19, through the world (301)
UPDATED on 4/12/2020
Considerations for Drug Interactions on QTc in Exploratory COVID-19 (Coronavirus Disease 2019) Treatment
Running Title: Roden et al.; Drug Interactions on QTc in Exploratory COVID-19 Treatment
Dan M. Roden, M.D.C.M.1 ; Robert A. Harrington, MD2 ; Athena Poppas, MD3 ; Andrea M. Russo, MD4 1 Interim Division Chief, Division of Cardiovascular Medicine; Senior Vice President for Personalized Medicine; Clinical Cardiac Electrophysiology Program Faculty, Vanderbilt University School of Medicine, Nashville, TN; 2Arthur L. Bloomfield Professor of Medicine; Chair, Department of Medicine, Stanford University, Stanford, CA; 3Chief of the Cardiology Division, Professor of Medicine, Brown University School of Medicine, Providence, RI; 4Director of Electrophysiology and Arrhythmia Services at Cooper University Hospital, Director of the CCEP Fellowship Program, Professor of Medicine at Cooper Medical School of Rowan University, Camden, NJ Dr. Harrington is president of the American Heart Association. Dr.
Hydroxychloroquine and azithromycin have been touted for potential prophylaxis or treatment for COVID-19 (coronavirus disease 2019) infection. Both drugs are listed as definite causes of torsade de pointes at crediblemeds.org. There are occasional case reports of hydroxychloroquine prolonging the QT interval and provoking torsade de pointes1-4 when used to treat systemic lupus erythematosus. Antimalarial prophylactic drugs, such as hydroxychloroquine, are believed to act on the entry and post-entry stages of SARS-CoV (severe acute respiratory syndrome–associated coronavirus) and SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) infection, likely via effects on endosomal pH and the resulting under-glycosylation of angiotensinconverting enzyme 2 receptors that are required for viral entry. 5 The widely used antibiotic azithromycin is increasingly recognized as a rare cause of QT prolongation,6,7 serious arrhythmias, 8,9 and increased risk for sudden death10; advanced age and female sex have been implicated as risk factors. Interestingly, azithromycin can also provoke non-pause–dependent polymorphic ventricular tachycardia.11,12 The FDA Perspective supported the observations that azithromycin administration leaves the patient vulnerable to QTc interval prolongation and torsade de pointes. 13 Basic electrophysiologic studies suggest that both drugs can provoke proarrhythmia via mechanisms beyond block of IKr implicated in usual cases of torsade de pointes.14,15 The effect of the combination of these agents on QT or arrhythmia risk has not been studied. There are very limited data evaluating the safety of combination therapy. Multiple randomized trials are currently being initiated. Seriously ill patients often have comorbidities that can increase risk of serious arrhythmias. These include hypokalemia, hypomagnesemia, fever,16 and an inflammatory state.17 Mechanisms to minimize arrhythmia risk include:
Electrocardiographic/QT interval monitoring:
- Withhold the drugs in patients with baseline QT prolongation (eg, QTc ≥500 msec) or with known congenital long QT syndrome.
- Monitor cardiac rhythm and QT interval; withdrawal of the drugs if QTc exceeds a preset threshold of 500 msec.
- In patients critically ill with COVID-19 infection, frequent caregiver contact may need to be minimized, so optimal electrocardiographic interval and rhythm monitoring may not be possible.
- Correction of hypokalemia to levels of >4 mEq/L and hypomagnesemia to levels of >2 mg/dL.
- Avoid other QTc prolonging agents5 whenever feasible. Safety considerations for use of hydroxychloroquine and azithromycin in clinical practice have been described.18 Some of the current COVID-19 repurposed drugs are listed in the Table.
SEE TABLE IN
Circulation
UPDATED on 4/09/2020
Worldwide trial uses AI to quickly identify ideal Covid-19 treatments
Reporter : Irina Robu, PhD
UPDATED on 3/31/2020
COVID-19 Treatment and Vaccine Tracker This document contains an aggregation of publicly available information from validated sources. It is not an endorsement of one approach or treatment over another but simply a list of all treatments and vaccines currently in development.
- Number
- Type of Product – Treatment
- FDA-Approved Indications (Treatments)
- Clinical Trials
- Ongoing for Other Diseases
- Developer/ Researcher
- Current Stage of Development
- Funding Sources
- Anticipated Timing
- Sources
LEGEND
- CCHF= Crimean-Congo Haemorrhagic Fever
- CHIKV = Chikungunya Virus
- DengV = Dengue Virus
- FMD = Foot and Mouth Disease
- EBOV = Ebola Virus
- HAV = Hepatitis A Virus
- HBV = Hepatitis B Virus
- HIV = Human Immunodeficiency Virus
- HPV = Human Papilloma Virus
- Inf = Influenza
- LASV = Lassa Fever Virus
- MARV = Marburg Virus
- MenB = Mengingitis B
- MERS = Middle East Respiratory Syndrome
- NIPV = Nipah Virus
- NORV = Norovirus
- RABV = Rabies Virus
- RSV = Respiratory Syncytial Virus
- RVF = Rift Valley Fever
-
SARS = Severe Acute Respiratory Syndrome
- SIV = Simian Immunodeficiency Virus
- TB = Tuberculosis
- VEE = Venezuelan Equine Encephalitis Virus
- VZV = Varicella Vaccine (Chickenpox)
- YFV = Yellow Fever Virus
- ZIKV = Zika Virus L
COVID-19 Treatment and Vaccine Tracker This document contains an aggregation of publicly-available information from validated sources. It is not an endorsement of one approach or treatment over another, but simply a list of all treatments and vaccines currently in development
-
Antibodies from recovered COVID-19 patients N/A Celltrion Pre-clinical Start Phase 1 ~ Sept 2020 Korea Herald 4
-
Antibodies from recovered COVID-19 patients N/A Kamada Pre-clinical BioSpace AbbVie 5
-
Antibodies from recovered COVID-19 patients N/A Vir Biotech/WuXi Biologics/Biogen Pre-clinical Stat News Vir Biotech 6
-
Antibodies from recovered COVID-19 patients N/A Lilly/Ab-Cellera (NIH Vaccines Research Center) Pre-clinical Start Phase 1 in late July 2020 Endpoints News
SOURCE
https://milkeninstitute.org/sites/default/files/2020-03/Covid19%20Tracker%20032020v3-posting.pdf
UPDATED on 3/31/2020
-
Pluristem Treated First Three COVID-19 Patients in Israel under Compassionate Use
Pluristem Treated First Three COVID-19 Patients in Israel under Compassionate Use
- Expects to treat more patients in Israel in the coming days
- Company is in discussions with regulators in the U.S and Europe to define its clinical strategy for COVID-19
HAIFA, Israel, March 30, 2020 – Pluristem Therapeutics Inc. (Nasdaq:PSTI) (TASE:PSTI), a leading regenerative medicine company developing a platform of novel biological therapeutic products, announced today that since its last update on COVID-19, it has dosed three patients in two different hospitals in Israel under a compassionate use program for the treatment of COVID-19, as approved by the Israeli Ministry of Health. Pluristem expects to enroll additional patients in Israel in the coming days and anticipates providing updates on clinical outcomes once significant data has been gathered.
All three treated patients are in a high-risk group based on age and preexisting conditions, have been experiencing severe respiratory failure, and intubation with a ventilator. Pluristem is closely following the medical condition of these patients in conjunction with the hospitals’ medical professionals delivering the care.
Pluristem is prepared for immediate ramp-up of PLX cell production with consistent batch-to-batch cell production quality through its GMP certified manufacturing facilities in order to meet potential demand.
“In this time of emergency, we are honored to be taking part in the global effort to support patients and healthcare systems. We watch with great admiration the endless efforts of the outstanding medical teams at the hospitals, and we would like to thank them for their collaboration and support. It is our hope that our mutual desire to help patients will result in improved outcomes for those hard hit by the life threating complications of COVID-19,” stated Pluristem CEO and President, Yaky Yanay. “In addition to our current activity in Israel, we are in discussions with regulators in the U.S and Europe to define our clinical strategy for COVID-19. Pluristems’ advanced manufacturing capabilities enable us to serve potential need of treating large numbers of patients under compassionate use and clinical studies across numerous countries and hospitals in accordance with our expansion program and regulatory approvals. We are facing a very different global condition right now, and the entire Pluristem team is committed to being an important part of the solution.”
PLX Cells for COVID-19
PLX cells are available off-the-shelf and once commercialized, can be manufactured in large scale quantities, offering a key advantage in addressing a global pandemic. PLX cells are allogeneic mesenchymal-like cells that have immunomodulatory properties that induce the immune system’s natural regulatory T cells and M2 macrophages, and thus may prevent or reverse the dangerous overactivation of the immune system. Accordingly, PLX cells may potentially reduce the incidence and\or severity of COVID-19 pneumonia and pneumonitis leading hopefully to a better prognosis for the patients. Previous pre-clinical findings of PLX cells revealed therapeutic benefit in animal studies of pulmonary hypertension, lung fibrosis, acute kidney injury and gastrointestinal injury which are potential complications of the severe COVID-19 infection. Clinical data using PLX cells demonstrated the strong immunomodulatory potency of PLX cells in patients post major surgery. Taken together, PLX cells’ potential capabilities with the safety profile observed from clinical trials involving hundreds of patients worldwide potentially position them as a therapy for mitigating the tissue-damaging effects of COVID-19.
The potential therapeutic effects of PLX cells for the treatment of respiratory and inflammatory complications associated with the COVID-19 are currently being studied through a collaborative agreement between Pluristem and the BIH Center for Regenerative Therapy (BCRT) and the Berlin Center for Advanced Therapies (BeCAT) at Charite’ University of Medicine Berlin.
About Pluristem Therapeutics
Pluristem Therapeutics Inc. is a leading regenerative medicine company developing novel placenta-based cell therapy product candidates. The Company has reported robust clinical trial data in multiple indications for its patented PLX cell product candidates and is currently conducting late stage clinical trials in several indications. PLX cell product candidates are believed to release a range of therapeutic proteins in response to inflammation, ischemia, muscle trauma, hematological disorders and radiation damage. The cells are grown using the Company’s proprietary three-dimensional expansion technology and can be administered to patients off-the-shelf, without tissue matching. Pluristem has a strong intellectual property position; a Company-owned and operated GMP-certified manufacturing and research facility; strategic relationships with major research institutions; and a seasoned management team.
SOURCE
From: Ofer Markman <oferm2020@gmail.com>
Date: Monday, March 30, 2020 at 10:44 AM
To: Aviva Lev-Ari <AvivaLev-Ari@alum.berkeley.edu>
Subject: Fwd: Pluristem Treated First Three COVID-19 Patients in Israel under Compassionate Use
3/30/2020
Coronavirus tracker: Novartis donates hydroxychloroquine samples to COVID study; FDA backs plasma therapy
3/29/2020
Plasma Tx Improved COVID-19 Outcomes in Sickest Patients
Question Could administration of convalescent plasma transfusion be beneficial in the treatment of critically ill patients with coronavirus disease 2019 (COVID-19)?
Findings In this uncontrolled case series of 5 critically ill patients with COVID-19 and acute respiratory distress syndrome (ARDS), administration of convalescent plasma containing neutralizing antibody was followed by an improvement in clinical status.
Meaning These preliminary findings raise the possibility that convalescent plasma transfusion may be helpful in the treatment of critically ill patients with COVID-19 and ARDS, but this approach requires evaluation in randomized clinical trials.
AbstractImportance Coronavirus disease 2019 (COVID-19) is a pandemic with no specific therapeutic agents and substantial mortality. It is critical to find new treatments.
Objective To determine whether convalescent plasma transfusion may be beneficial in the treatment of critically ill patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
Design, Setting, and Participants Case series of 5 critically ill patients with laboratory-confirmed COVID-19 and acute respiratory distress syndrome (ARDS) who met the following criteria: severe pneumonia with rapid progression and continuously high viral load despite antiviral treatment; Pao2/Fio2 <300; and mechanical ventilation. All 5 were treated with convalescent plasma transfusion. The study was conducted at the infectious disease department, Shenzhen Third People’s Hospital in Shenzhen, China, from January 20, 2020, to March 25, 2020; final date of follow-up was March 25, 2020. Clinical outcomes were compared before and after convalescent plasma transfusion.
Exposures Patients received transfusion with convalescent plasma with a SARS-CoV-2–specific antibody (IgG) binding titer greater than 1:1000 (end point dilution titer, by enzyme-linked immunosorbent assay [ELISA]) and a neutralization titer greater than 40 (end point dilution titer) that had been obtained from 5 patients who recovered from COVID-19. Convalescent plasma was administered between 10 and 22 days after admission.
Main Outcomes and Measures Changes of body temperature, Sequential Organ Failure Assessment (SOFA) score (range 0-24, with higher scores indicating more severe illness), Pao2/Fio2, viral load, serum antibody titer, routine blood biochemical index, ARDS, and ventilatory and extracorporeal membrane oxygenation (ECMO) supports before and after convalescent plasma transfusion.
Results All 5 patients (age range, 36-65 years; 2 women) were receiving mechanical ventilation at the time of treatment and all had received antiviral agents and methylprednisolone. Following plasma transfusion, body temperature normalized within 3 days in 4 of 5 patients, the SOFA score decreased, and Pao2/Fio2 increased within 12 days (range, 172-276 before and 284-366 after). Viral loads also decreased and became negative within 12 days after the transfusion, and SARS-CoV-2–specific ELISA and neutralizing antibody titers increased following the transfusion (range, 40-60 before and 80-320 on day 7). ARDS resolved in 4 patients at 12 days after transfusion, and 3 patients were weaned from mechanical ventilation within 2 weeks of treatment. Of the 5 patients, 3 have been discharged from the hospital (length of stay: 53, 51, and 55 days), and 2 are in stable condition at 37 days after transfusion.
Conclusions and Relevance In this preliminary uncontrolled case series of 5 critically ill patients with COVID-19 and ARDS, administration of convalescent plasma containing neutralizing antibody was followed by improvement in their clinical status. The limited sample size and study design preclude a definitive statement about the potential effectiveness of this treatment, and these observations require evaluation in clinical trials.
3/28/2020
Coronaviruses Replication and Pathogenicity
Coronaviruses: An Overview of Their Replication and Pathogenesis
Abstract
Coronaviruses (CoVs), enveloped positive-sense RNA viruses, are characterized by club-like spikes that project from their surface, an unusually large RNA genome, and a unique replication strategy. Coronaviruses cause a variety of diseases in mammals and birds ranging from enteritis in cows and pigs and upper respiratory disease chickens to potentially lethal human respiratory infections. Here we provide a brief introduction to coronaviruses discussing their replication and pathogenicity, and current prevention and treatment strategies. We will also discuss the outbreaks of the highly pathogenic Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and the recently identified Middle Eastern Respiratory Syndrome Coronavirus (MERS-CoV).
SARS-CoV, a group 2b β-coronavirus, was identified as the causative agent of the Severe Acute Respiratory Syndrome (SARS) outbreak that occurred in 2002–2003 in the Guangdong Province of China. It is the most severe disease caused by any coronavirus. During the 2002–2003 outbreak approximately 8098 cases occurred with 774 deaths, resulting in a mortality rate of 9%. This rate was much higher in elderly individuals, with mortality rates approaching 50% in individuals over 60 years of age. Furthermore, the outbreak resulted in the loss of nearly $40 billion dollars in economic activity, as the virus nearly shut down many activities in Southeast Asia and Toronto, Canada for several months. The outbreak began in a hotel in Hong Kong and ultimately spread to more than two dozen countries. During the epidemic, closely related viruses were isolated from several exotic animals including Himalayan palm civets and raccoon dogs [82]. However, it is widely accepted that SARS-CoV originated in bats as a large number of Chinese horseshoe bats contain sequences of SARS-related CoVs and contain serologic evidence for a prior infection with a related CoV [83,84]. In fact, two novel bat SARS-related CoVs were recently identified that are more similar to SARS-CoV than any other virus identified to date [85]. They were also found to use the same receptor as the human virus, angiotensin converting enzyme 2 (ACE2), providing further evidence that SARS-CoV originated in bats. Although some human individuals within wet animal markets, had serologic evidence of SARS-CoV infection prior to the outbreak, these individuals had no apparent symptoms [82]. Thus, it is likely that a closely related virus circulated in the wet animal markets for several years before a series of factors facilitated its spread into the larger population.
Transmission of SARS-CoV was relatively inefficient, as it only spread through direct contact with infected individuals after the onset of illness. Thus, the outbreak was largely contained within households and healthcare settings [86], except in a few cases of superspreading events where one individual was able to infect multiple contacts due to an enhanced development of high viral burdens or ability to aerosolize virus. As a result of the relatively inefficient transmission of SARS-CoV, the outbreak was controllable through the use of quarantining. Only a small number of SARS cases occurred after the outbreak was controlled in June 2003.
SARS-CoV primarily infects epithelial cells within the lung. The virus is capable of entering macrophages and dendritic cells but only leads to an abortive infection [87,88]. Despite this, infection of these cell types may be important in inducing pro-inflammatory cytokines that may contribute to disease [89]. In fact, many cytokines and chemokines are produced by these cell types and are elevated in the serum of SARS-CoV infected patients [90]. The exact mechanism of lung injury and cause of severe disease in humans remains undetermined. Viral titers seem to diminish when severe disease develops in both humans and in several animal models of the disease. Furthermore, animals infected with rodent-adapted SARS-CoV strains show similar clinical features to the human disease, including an age-dependent increase in disease severity [91]. These animals also show increased levels proinflammatory cytokines and reduced T-cell responses, suggesting a possible immunopathological mechanism of disease [92,93].
While the SARS-CoV epidemic was controlled in 2003 and the virus has not since returned, a novel human CoV emerged in the Middle East in 2012. This virus, named Middle East Respiratory Syndrome-CoV (MERS-CoV), was found to be the causative agent in a series of highly pathogenic respiratory tract infections in Saudi Arabia and other countries in the Middle East [94]. Based on the high mortality rate of ∼50% in the early stages of the outbreak, it was feared the virus would lead to a very serious outbreak. However, the outbreak did not accelerate in 2013, although sporadic cases continued throughout the rest of the year. In April 2014, a spike of over 200 cases and almost 40 deaths occurred, prompting fears that the virus had mutated and was more capable of human-to-human transmission. More likely, the increased number of cases resulted from improved detection and reporting methods combined with a seasonal increase in birthing camels. As of August 27th, 2014 there have been a total of 855 cases of MERS-CoV, with 333 deaths and a case fatality rate of nearly 40%, according to the European Center for Disease Prevention and Control.
Diagnosis, Treatment, and Prevention
In the case of SARS-CoV, several potential vaccines have been developed but none are yet approved for use. These vaccines include:
- recombinant attenuated viruses,
- live virus vectors – In general, it is thought that live attenuated vaccines would be the most efficacious in targeting coronaviruses.
- individual viral proteins expressed from DNA plasmids.
Therapeutic SARS-CoV neutralizing antibodies have been generated and could be retrieved and used again in the event of another SARS-CoV outbreak. Such antibodies would be most useful for protecting healthcare workers.
Conclusion
Over the past 50 years the emergence of many different coronaviruses that cause a wide variety of human and veterinary diseases has occurred. It is likely that these viruses will continue to emerge and to evolve and cause both human and veterinary outbreaks owing to their ability to recombine, mutate, and infect multiple species and cell types.
Future research on coronaviruses will continue to investigate many aspects of viral replication and pathogenesis. First, understanding the propensity of these viruses to jump between species, to establish infection in a new host, and to identify significant reservoirs of coronaviruses will dramatically aid in our ability to predict when and where potential epidemics may occur. As bats seem to be a significant reservoir for these viruses, it will be interesting to determine how they seem to avoid clinically evident disease and become persistently infected. Second, many of the non-structural and accessory proteins encoded by these viruses remain uncharacterized with no known function, and it will be important to identify mechanisms of action for these proteins as well as defining their role in viral replication and pathogenesis. These studies should lead to a large increase in the number of suitable therapeutic targets to combat infections. Furthermore, many of the unique enzymes encoded by coronaviruses, such as ADP-ribose-1”-phosphatase, are also present in higher eukaryotes, making their study relevant to understanding general aspects of molecular biology and biochemistry. Third, gaining a complete picture of the intricacies of the RTC will provide a framework for understanding the unique RNA replication process used by these viruses. Finally, defining the mechanism of how coronaviruses cause disease and understanding the host immunopoathological response will significantly improve our ability to design vaccines and reduce disease burden.
References
155. Bhardwaj K, Sun J, Holzenburg A, Guarino LA, Kao CC. RNA recognition and cleavage by the SARS coronavirus endoribonuclease. Journal of molecular biology. 2006;361(2):243–256. [PubMed] [Google Scholar]156. Ivanov KA, Hertzig T, Rozanov M, Bayer S, Thiel V, Gorbalenya AE, Ziebuhr J. Major genetic marker of nidoviruses encodes a replicative endoribonuclease. Proceedings of the National Academy of Sciences of the United States of America. 2004;101(34):12694–12699. [PMC free article] [PubMed] [Google Scholar]
SOURCE
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4369385/
3/26/2020
Glycobiology vs Proteomics: Glycobiologists Prespective in the effort to explain the origin, etiology and potential therapeutics for the Coronavirus Pandemic (COVID-19).
Curator: Ofer Markman, PhD
The sugars involved in a viral disease are unique in many ways when compared with the DNA/RNA or the proteins involved: they are almost totally dependent on the infected cells and thus are not affected by the viral mutation rate or by the virus at all. Nevertheless they are affected by the cells, their type and their sugar production mechanisms and in some respect to the production rate by which the virus in manufactured by the infected cells. Mutations may have nevertheless major effect not on the structures of the glycans but rather on the existence of the glycosylation site, and thus the glycan at all, but not on its structures.
This may make the gycomolecule a good target for diagnostics as stability in the molecule may mean longer life shelve of diagnostics kits.
Unique sugars are already predicted/found in the virus from certain Chinese origin, in this case an o-linked glycan/s not previously detected.
- The proximal origin of SARS-CoV-2
Kristian G. Andersen, Andrew Rambaut, W. Ian Lipkin, Edward C. Holmes & Robert F. Garry
Nature Medicine (2020)Cite this article
https://www.nature.com/articles/s41591-020-0820-9
- The covid-19 coronavirus epidemic has a natural origin, scientists say
- Emerging WuHan (COVID-19) coronavirus: glycan shield and structure prediction of spike glycoprotein and its interaction with human CD26
Naveen Vankadari & Jacqueline A. Wilce
https://www.tandfonline.com/doi/full/10.1080/22221751.2020.1739565
Nevertheless, if the virus can infect multiple cells once current cells are not going to be available for any reason those viruses may present other glycans.
Once one starts to treat the infected person via modulation of protein production or by other means the change in the dynamic of protein production vs. protein glycosylation may cause changes in protein glycosyation, including their structures, this is well known to biotechnologists producing glycoproteins in labs and production.
This may either be a problem in understanding the state of disease or an advantage as it may help following response to the treatment and help as a co-treatment diagnostics.
Early Studies include the following:
- Carbohydrate-based Diagnostics: A New Approach to COVID-19 Testing?
Mar 19, 2020 | Original story from Iceni Diagnostics
Glycans may play a role in treatment as well. TAMIFLU a case in point. Tamiflu is directed to the flu enzyme Neuraminidaze that is part of the viral structures. This approach was also explored to develop treatments.
- Pneumagen Ltd Leverages its Novel Glycan Approach to Target Coronavirus (COVID-19) Infections
March 17, 2020 PR-M03-20-NI-024
Glycans do not only effect their own involvement in treatment/diagnostics they also are effecting protein based diagnostics for this see statement by Dr. Michael Mercier of UAH
- We’re dealing with COVID-19, but what’s a virus in the first place?
23-Mar-2020 8:45 AM EDT, by University of Alabama Huntsville
https://www.newswise.com/articles/we-re-dealing-with-covid-19-but-what-s-a-virus-in-the-first-place
- The Relevance of Glycans in the Viral Pathology of COVID-19
Reporter: Ofer Markman, PhD
https://pharmaceuticalintelligence.com/2020/03/23/glycans-in-the-viral-pathology-of-covid-19/
3/23/2020
Promise of Synthetic Biology for Covid-19 Vaccine
Reporter: Irina Robu, PhD
https://pharmaceuticalintelligence.com/2020/03/23/promise-of-synthetic-biology-for-covid-19-vaccine/
3/19/2020
Testing for Positive Coronavirus Infection
Published online 2012 Mar 13. doi: 10.1002/sim.5334
Pooled testing procedures for screening high volume clinical specimens in heterogeneous populations
The Technion explained that COVID-19 is currently diagnosed using Polymerase chain reaction (PCR) testing which examines the presence of a unique genetic sequence of viruses in a single sample. The test takes a number of hours and creates a bottleneck as samples are tested individually. With pooled testing, only combined samples found to be positive will trigger individual testing.
According to Professor Roy Kishony, head of the research group at the Technion’s Faculty of Biology, “this is not a scientific breakthrough, but a demonstration of the effectivity of using the existing method and even the existing equipment to significantly increase the volume of samples tested per day.”
Kishony said that in a “joint examination of 64 samples in which only one was a positive carrier, the system identified that there was a positive sample.” Acknowledging logistical challenges, he added that the expectation was to greatly increase the volume of samples tested per day.
“This approach should reduce the chance of infection and flatten the infection curve,” he said.
At the Weizmann Institute, the university said, scientists are developing an advanced testing approach based on a process that involves fewer stages compared to existing tests, and will greatly reduce the biological risk to medical teams.
The university said it will also use its advanced laboratories to perform coronavirus tests, including the Nancy and Stephen Grand Israel National Center for Personalized Medicine (G-INCPM), a research facility established in 2016. This laboratory has a number of advanced PCR devices.
SOURCE
http://nocamels.com/2020/03/technion-weizmann-institute-coronavirus-testing/
COVID-19 (SARS-CoV-2) Virus Reactive Antibodies
|
Antibody Products |
Cat. No. |
Host |
Application |
Clonality |
Protein Structure |
Blocking Peptide |
|
3525 |
Rabbit |
ELISA |
Polyclonal |
Spike Protein |
||
|
3531 |
Rabbit |
ELISA |
Polyclonal |
Envelope Protein |
||
|
35-579 |
Mouse |
ELISA, IF, WB |
Monoclonal |
Nucleocapsid Protein |
N/A |
|
|
35-580 |
Mouse |
ELISA, IF, WB |
Monoclonal |
Nucleocapsid Protein |
N/A |
|
|
35-710 |
Mouse |
ELISA, IF |
Monoclonal |
Nucleocapsid Protein |
N/A |
|
|
35-711 |
Mouse |
ELISA, IF |
Monoclonal |
Nucleocapsid Protein |
N/A |
|
|
35-712 |
Mouse |
ELISA, IF |
Monoclonal |
Nucleocapsid Protein |
N/A |
Diagnosis of Acute Respiratory Syndrome Coronavirus 2 Infection by Detection of Nucleocapsid Protein running title: Diagnosis of COVID-19 by N antigen detection Bo Diao1#, Kun Wen2#, Jian Chen3#, Yueping Liu1 , Zilin Yuan1 ,Chao Han3 , Jiahui Chen2 , Yuxian Pan2,Li Chen4,Yunjie Dan5 , Jing Wang6 , Yongwen Chen 3 , Guohong Deng5*, Hongwei Zhou2*, Yuzhang Wu3*
https://www.medrxiv.org/content/10.1101/2020.03.07.20032524v2.full.pdf
TABLE 1 | SELECTED REPURPOSED DRUGS IN CLINICAL DEVELOPMENT TO TREAT COVID-19
Drug or cocktail Originator company Status and mechanisms Clinical trials (trial posting date) ASC09/ritonavir, lopinavir/ritonavir, with or without umifenovir Ascletis, AbbVie, Pharmstandard ASC09 is an experimental HIV-1 protease inhibitor; ritonavir and lopinavir/ritonavir are approved protease inhibitors for HIV/AIDS; umifenovir is an approved entry inhibitor against influenza At least three trials (e.g., ChiCTR2000029603, 2/6/20) ASC09/oseltamivir, ritonavir/oseltamivir, oseltamivir Ascletis, Gilead, AbbVie See above; oseltamivir is a sialidase inhibitor approved for influenza One trial (NCT04261270, 2/7/20) Azvudine Zhengzhou Granlen PharmaTech Experimental reverse transcriptase inhibitor drug against HIV-1/AIDS One trial (ChiCTR2000029853, 2/15/20) Various combinations of baloxavir marboxil/favipiravir and lopinavir/ritonavir Shionogi, Toyama Chemical Baloxavir marboxil is a Cap-dependent endonuclease inhibitor and favipiravir is a guanine analog RNA-dependent RNA polymerase inhibitor approved for influenza A and B; see above Two trials (ChiCTR2000029544, 2/3/20; ChiCTR2000029548, 2/4/20) Various combinations of darunavir/cobicistat alone or with lopinavir/ritonavir and thymosin α1 Janssen, Gilead Darunavir and cobicistat are, respectively, an HIV-1 protease inhibitor and inhibitor of cytochrome P450 (CYP)3A enzyme, approved as a combination against HIV-1/AIDS. Thymosin α1 is an immune response boosting agent Two trials (NCT04252274, 2/5/20; ChiCTR2000029541, 2/3/20) Remdesivir Gilead Phosphoramidate prodrug of an adenine analog used for Ebola and Marburg virus outbreaks (similar structure to approved HIV reverse transcriptase inhibitors) Two trials (NCT04252664, 2/5/20; NCT04257656, 2/6/20) Chloroquine or hydroxychloroquine Shanghai Zhongxi Pharmaceutical, Shanghai Ziyuan Pharmaceutical, Wuhan Wuyao Pharmaceutical Endosomal acidification fusion inhibitor At least ten trials (e.g., ChiCTR2000029826, 2/2/20; NCT04261517, 2/14/20) Methylprednisolone Generic Synthetic corticosteroid that binds to nuclear receptors to dampen proinflammatory cytokines One trial (NCT04263402, 2/10/20) Interferon alfa-2b alone or in combination with lopinavir/ritonavir and ribavirin Biogen, Merck Interferon alfa-2b is a recombinant cytokine with antiviral properties; ribavirin is a guanine derivative; as above Two trials (NCT04254874, 2/5/20; ChiCTR2000029308, 1/23/20) Camrelizumab and thymosin Incyte, Shanghai Hengrui Pharmaceutical Camrelizumab is a humanized monoclonal antibody (mAb) targeting PD-1 Two trials (ChiCTR2000029806, 2/14/20; NCT04268537, 2/14/20) Tocilizumab Chugai Pharmaceutical, Zhejiang Hisun Pharmaceutical, Jiangsu Qyun Bio-Pharmaceutical Humanized mAb targeting interleukin-6 One trial (ChiCTR2000029765, 2/13/20) The World Health Organization’s R&D Blueprint report released at the end of January considered remdesivir the most promising candidate to treat COVID-19, on the basis of its broad-spectrum activity, in vitro and in vivo data for coronaviruses and clinical safety from Ebola virus disease trials.
SOURCE
https://www.nature.com/articles/d41587-020-00003-1
| Structure-guided Drug Discovery: (1) The Coronavirus 3CL hydrolase (Mpro) enzyme (main protease) essential for proteolytic maturation of the virus and (2) viral protease, the RNA polymerase, the viral spike protein, a viral RNA as promising two targets for discovery of cleavage inhibitors of the viral spike polyprotein preventing the Coronavirus Virion the spread of infection
____________________________ |
Curators and Reporters: Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN |
Drug Discovery OptionsTherapeutics for coronavirus viral infection include the following: (a) Monoclonal and polyclonal antibodies (b) Vaccines (c) Small molecule treatments (e.g., chloroquinolone and derivatives), including compounds already approved for other indications (d) Immuno-therapies derived from human or other sources ____________________________ |
Dr. Jason Zielonka, MD – Work-in-Progress |
| Clinical Trials on CoVid19 and Coronavirus: | Dr. Jason Zielonka, MD – Work-in-Progress
Search terms CoVid19 and Coronavirus: https://clinicaltrials.gov/ct2/results/details?cond=CoVid19+coronavirus Results (all countries): 52 studies Clinicaltrials.gov is operated by NIH. It is one of 7 databases that Congress, along with ISMJE (International Society of Medical Journal Editors) identified to serve as clearing agents for trials that will be accepted for publication in ISMJE journals (basically those with the greatest circulation and largest impact factor) and whose sponsors would commit to publishing results whether positive or negative for the test treatment.. Almost all Pharma funded research and federal & foundation funded research registers with clintrials.gov. The other 6 databases are much smaller and less well known than CT.gov, so it contains the lions share of these trial registrations. ________________________________________________________ |
| Coronavirus (COVID-19): The Role of Genomics in Responding
____________________________ |
https://blog.nebula.org/role-of-genomics-coronavirus-covid-19/?utm_source=Nebula%20Genomics |
| Group of Researchers @ University of California, Riverside, the University of Chicago, the U.S. Department of Energy’s Argonne National Laboratory, and Northwestern University solve COVID-19 Structure and Map Potential Therapeutics
____________________________ |
Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN Curators |
| Predicting the Protein Structure of Coronavirus: Inhibition of Nsp15 can slow viral replication and Cryo-EM – Spike protein structure (experimentally verified) vs AI-predicted protein structures (not experimentally verified) of DeepMind (Parent: Google) aka AlphaFold
____________________________ |
Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN Curators |
| Current Drug development efforts |
https://www.clinicaltrialsarena.com/analysis/coronavirus-mers-cov-drugs/ https://www.pharmaceutical-technology.com/news/vir-biotechnology-nih-biogen-coronavirus-antibodies/ https://www.genengnews.com/a-lists/how-to-conquer-coronavirus-top-35-treatments-in-development/ https://www.biospace.com/article/mobilizing-drug-development-efforts-against-the-novel-coronavirus/ |
|
Coronavirus puts drug repurposing on the fast track |
https://www.nature.com/articles/d41587-020-00003-1 |