COVID-19: Novel Treatment Protocols using Approved drugs vs Standard of Care vs Vaccine and Antiviral new drug discovery and development – An LPBI Group Response and An LPBI Group & Affiliates Response
Curator: Aviva Lev-Ari, PhD, RN
On 5/26/2020 LPBI organized a Symposium on New Therapeutics for COVID-19
AGENDA included presentations by:
- Dr. Raphael Nir, PhD, CSO, SBH, Sciences, Inc. – Drug Concept to mitigate Cytokine Storm in COVID-19 – ATTACHMENT
- Dr. Ajay Gupta, MD, Professor & Entrepreneur – Rhinitis drug approved in Japan – REPURPOSED for COVID-19 and Application for FDA Approval
- Dr. Yigal Blum, PhD, ex-SRI Int’l VP and Entrepreneur – AMORPHOUS CALCIUM CARBONATE (ACC) TREATMENT FOR COVID-19
- Dr. Orna Harel, PhD, Managing Partner, Agbiopro – Representation for – Prof. Saul Yedgar on the concept and state of preclinical efforts for COVID-19 drug development
- Aviva Lev-Ari, PhD, RN – The Potential of REVIVAL of Drug Discovery Initiative and Explorations of Joint Ventures with Biotech companies – An Interim Phase toward POST Coronavirus Pandemic Exit
DISCUSSION – Where and What is the INTERFACE between what our External Relations attempt to accomplish and the Capabilities of LPBI Group’s Team
In the concluding remarks, Dr. Lev-Ari discussed the importance of TREATMENT PROTOCOLS vs. one Therapeutics at a time vs. Combination Drug therapies.
Dr. Lev-Ari pointed the Symposium attendees to the following two points:
1. The State of Science been endorsed by LPBI Group
RNA from the SARS-CoV-2 virus taking over the cells it infects: Virulence – Pathogen’s ability to infect a Resistant Host: The Imbalance between Controlling Virus Replication versus Activation of the Adaptive Immune Response
Curator: Aviva Lev-Ari, PhD, RN – I added colors and bold face
https://pharmaceuticalintelligence.com/2020/05/23/rna-from-the-sars-cov-2-virus-taking-over-the-cells-it-infects-virulence-pathogens-ability-to-infect-a-resistant-host-the-imbalance-between-controlling-virus-replication-versus-activation-of-the/
2. LPBI Group’s Position for Treatment Protocol(s)
- T cells found in COVID-19 patients ‘bode well’ for long-term immunity | Science | AAAS
https://www.sciencemag.org/news/2020/05/t-cells-found-covid-19-patients-bode-well-long-term-immunity
- Clinical Trial for the Use of Nitric Oxide to Treat Severe COVID-19 Infection
https://pharmaceuticalintelligence.com/2020/04/14/clinical-trial-for-the-use-of-nitric-oxide-to-treat-severe-covid-19/
In continuation to 5/26/2020 Symposium on New Therapeutics for COVID-19, we will follow up with an AGENDA for 6/16/2020
Part I: Therapeutics for COVID-19
- Prof. Saul Yedgar – Holder of US Patents on Rhinitis, anti-inflatation and other indications – 40 minutes
- Dr. Ajay Gupta, MD – Rhinitis drug approved in Japan – FDA Application for Approval of Repurpusing to COVID-19 in the US – 40 minutes
- Discussion – 20 minutes
On 5/29/2020 Dr. Lev-Ari read the article, COVID-19 Critical Care
STORY AT-A-GLANCE
- Despite the fact that many critical care specialists are using treatment protocols that differ from standard of care, information about natural therapeutics in particular are still being suppressed by the media and is not received by critical care physicians
- Five critical care physicians have formed the Front Line COVID-19 Critical Care Working Group (FLCCC). The group has developed a highly effective treatment protocol known as MATH+
- Of the more than 100 hospitalized COVID-19 patients treated with the MATH+ protocol as of mid-April, only two died. Both were in their 80s and had advanced chronic medical conditions
- The protocols call for the use of intravenous methylprednisolone, vitamin C and subcutaneous heparin within six hours of admission into the hospital, along with high-flow nasal oxygen. Optional additions include thiamine, zinc and vitamin D
- COVID-19 kills by triggering hyperinflammation, hypercoagulation and hypoxia. The MATH+ protocol addresses these three core pathological processes
COVID-19 Early Intervention Protocol
According to Kory, the FLCCCs MATH+ protocol has been delivered to the White House on four occasions, yet no interest has been shown. Worse, he says they continue to be stonewalled by the U.S. Centers for Disease Control and the National Institute for Health. Why?
Isn’t saving lives, right now, and by any means possible, more important than pushing for a vaccine? If the MATH+ protocol works with near-100% effectiveness, a vaccine may not even be necessary. The MATH+ protocol gets its name from:
Intravenous Methylprednisolone High-dose intravenous Ascorbic acid
Plus optional treatments Thiamine, zinc and vitamin D
Full dose low molecular weight Heparin
Kory’s testimony transcript reviews and summarizes the MATH+ protocol, and explains why the timing of the treatment is so important. As explained by Kory, there are two distinct yet overlapping phases of COVID-19 infection.
- Phase 1 is the viral replication phase. Typically, patients will only experience mild symptoms, if any, during this phase. At this time, it’s important to focus on antiviral therapies.
- In Phase 2, the hyperinflammatory immune response sets in, which can result in organ failures (lungs, brain, heart and kidneys). The MATH+ protocol is designed to treat this active phase, but it needs to be administered early enough.
The MATH+ Protocol
The MATH+ protocol7 calls for the use of three medicines, all of which need to be started within six hours of hospital admission:
- Intravenous methylprednisolone, to suppress the immune system and prevent organ damage from cytokine storms — For mild hypoxia, 40 milligrams (mg) daily until off oxygen; moderate to severe illness, 80 mg bolus followed by 20 mg per day for seven days. On Day 8, switch to oral prednisone and taper down over the next six days.
- Intravenous ascorbic acid (vitamin C), to control inflammation and prevent the development of leaky blood vessels in the lungs — 3 grams/100 ml every six hours for up to seven days.
- Subcutaneous heparin (enoxaparin), to thin the blood and prevent blood clots — For mild to moderate illness, 40 mg to 60 mg daily until discharged.
Optional additions include thiamine, zinc and vitamin D. In addition to these medications, the protocol calls for high-flow nasal oxygen to avoid mechanical ventilation, “which itself damages the lungs and is associated with a mortality rate approaching nearly 90% in some centers,” Kory notes.8
Together, this approach addresses the three core pathological processes seen in COVID-19, namely hyperinflammation, hypercoagulability of the blood, and hypoxia (shortness of breath due to low oxygenation).
COVID-19 Should Not Be Treated as ARDS
In the video, Dr. Paul Marik points out that it’s crucial for doctors to treat each patient as an individual case, as COVID-19 is not conventional acute respiratory distress syndrome (ARDS).
If the patient is assumed to have ARDS and placed on a ventilator, you’re likely going to damage their lungs. Indeed, research has now shown that patients placed on mechanical ventilation have far higher mortality rates than patients who are not ventilated. While not discussed here, some doctors are also incorporating hyperbaric oxygen treatment in lieu of ventilation, with great success.
The reason for this is because the primary problem is inflammation, not fluid in the lungs. So, Marik says, they need anti-inflammatory drugs. “It’s not the virus that is hurting the host, it’s the acute inflammatory dysregulated response,” he says. “That’s why you need to use vitamin C and steroids.” He points out that steroids play a crucial role, as it creates synergy with vitamin C.
COVID-19 patients also have a hypercoagulation problem, so they need anticoagulants. In addition to using the proper medication, they must also be treated early. “You have to intervene early and aggressively to prevent them from deteriorating,” Marik says.
Methylprednisolone May Be a Crucial Component
Kory expresses concerns over the fact that health organizations around the world are warning doctors against the use of corticosteroids, calling this a “tragic error”9 as “COVID-19 is a steroid-responsive disease.”10 In his testimony, he points out:11
“Sorin Draghici, CEO of Advaita Bioinformatics, just reported12 that their incredibly sophisticated Artificial Intelligence platform called iPathwayGuide, using cultured human cell lines infected with COVID-19, is able to map all the human genes which are activated by this virus …
Note almost all the activated genes are those that express triggers of inflammation. With this knowledge of the specific COVID inflammatory gene activation combined with knowledge of the gene suppression activity of all known medicines they were able to match the most effective drug for COVID-19 human gene suppression, and that drug is methylprednisolone.
This must be recognized, as the ability of other corticosteroids to control inflammation in COVID-19 was much less impactful. This is, we believe, an absolutely critical and historic finding. Many centers are using similar but less effective agents such as dexamethasone or prednisone.”
As noted by Kory in his senate testimony, Marik, chief of pulmonary and critical care medicine at the Eastern Virginia Medical School in Norfolk, Virginia, is a member of the FLCCC.13 You may recall that Marik was the one who in 2017 announced he had developed an extraordinarily effective treatment against sepsis.
Marik’s sepsis protocol also calls for intravenous vitamin C and a steroid, in this case hydrocortisone, along with thiamine. I for one am not surprised that the two protocols are so similar, seeing how sepsis is also a major cause of death in severe COVID-19 cases.
Safe and Effective Treatments Must Not Be Ignored
As noted by Marik in the video, COVID-19 is not regular ARDS and should not be treated as such. What kills people with COVID-19 is the inflammation, and steroids in combination with vitamin C work synergistically together to control and regulate that inflammation. The heparin, meanwhile, addresses the hypercoagulation that causes blood clots, which is a unique feature of COVID-19. As for the “lack of studies” supporting their protocol, FLCCC notes:14
“A number of official guidelines, such as those of the WHO and several other U.S. agencies, recommend limiting treatment for … critically ill patients to ‘supportive care only’ — and to allow the therapies described here to be studied in randomized controlled trials where half of the patients would receive placebo and where the results would come in months or years.
Our physicians agree that while a randomized controlled trial (RCT), under normal circumstances, might be considered, the early provisions of MATH+, which must be given within hours of critical illness, would inevitably be delayed by such a study design, rendering the validity of the RCT questionable.
Furthermore, while the results of an RCT would not be available for months or more, well-designed observational studies of the protocol could yield timely feedback during this pandemic, to improve the treatment process much more quickly.”
I believe this information needs to be shared far and wide, if we are to prevent more people from dying unnecessarily. More and more, as doctors are starting to speak openly about their clinical findings, we’re seeing that there are quite a few different ways to tackle this illness without novel antivirals or vaccines, using older, inexpensive and readily available medications that are already known to be safe.
References
A Response by LPBI Group and a Potential Response by LPBI Group and its Affiliates
LPBI Group’s Components in Novel Treatment Protocol Definition
- Forthcoming by Stephen J. Williams, PhD – Immuno-theraphy boosting Protocol
based on
T cells found in COVID-19 patients ‘bode well’ for long-term immunity | Science | AAAS
https://www.sciencemag.org/news/2020/05/t-cells-found-covid-19-patients-bode-well-long-term-immunity
- Forthcoming by Aviva Lev-Ari, PhD, RN and Stephen J. Williams, PhD – Nitric Oxide Inhaler OR Bystolic® (nebivolol) www.bystolicpro.com
- Two alternatives per stage of COVID-19 infections: Severe or Moderate
Featured snippet from the web





https://www.researchgate.net/publication/221979500
Nebivolol: Impact on cardiac and endothelial function and clinical utility
Article in Vascular Health and Risk Management · March 2012
DOI: 10.2147/VHRM.S20669 · Source: PubMed
Jorge Eduardo Toblli1, Federico DiGennaro1, Jorge Fernando Giani2, Fernando Pablo Dominici2
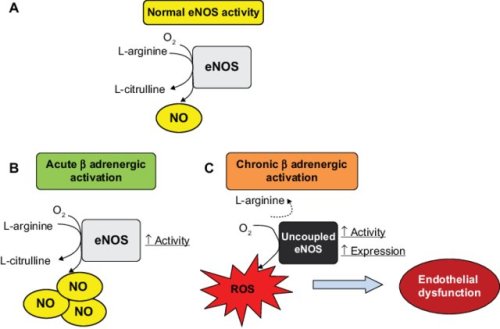
1Hospital Aleman, 2Instituto de Química y Fisicoquímica Biológicas (IQUIFIB), Facultad de Farmacia y Bioquímica, Facultad de Medicina, Universidad de Buenos Aires, Buenos Aires, ArgentinaAbstract: Endothelial dysfunction is a systemic pathological state of the endothelium characterized by a reduction in the bioavailability of vasodilators, essentially nitric oxide, leading to impaired endothelium-dependent vasodilation, as well as disarrangement in vascular wall metabolism and function. One of the key factors in endothelial dysfunction is overproduction of reactive oxygen species which participate in the development of hypertension, atherosclerosis, diabetes, cardiac hypertrophy, heart failure, ischemia-reperfusion injury, and stroke. Because impaired endothelial activity is believed to have a major causal role in the pathophysiology of vascular disease, hypertension, and heart failure, therapeutic agents which modify this condition are of clinical interest. Nebivolol is a third-generation β-blocker with high selectivity for β1-adrenergic receptors and causes vasodilation by interaction with the endothelial L-arginine/nitric oxide pathway. This dual mechanism of action underscores several hemodynamic qualities of nebivolol, which include reductions in heart rate and blood pressure and improvements in systolic and diastolic function. Although nebivolol reduces blood pressure to a degree similar to that of conventional β-blockers and other types of antihypertensive drugs, it may have advantages in populations with difficult-to-treat hypertension, such as patients with heart failure along with other comorbidities, like diabetes and obesity, and elderly patients in whom nitric oxide-mediated endothelial dysfunction may be more pronounced. Furthermore, recent data indicate that nebivolol appears to be a cost-effective treatment for elderly patients with heart failure compared with standard care. Thus, nebivolol is an effective and well tolerated agent with benefits above those of traditional β-blockers due to its influence on nitric oxide release, which give it singular hemodynamic effects, cardioprotective activity, and a good tolerability profile. This paper reviews the pharmacology structure and properties of nebivolol, focusing on endothelial dysfunction, clinical utility, comparative efficacy, side effects, and quality of life in general with respect to the other antihypertensive agents.
Keywords: beta-blockers, nebivolol, oxidative stress, endothelial function, cardiovascular protection, nitric oxide
SOURCE
l-nebivolol is responsible for beta-3 adrenergic receptor agonist activity that stimulates endothelial nitric oxide synthase, increasing nitric oxide levels; leading to vasodilation, decreased peripheral vascular resistance, increased stroke volume, ejection fraction, and cardiac output
- BYSTOLIC (nebivolol) [package insert]. Irvine, CA: Allergan USA, Inc.
- Data on file. Allergan, Inc.
- Germino FW. Efficacy and tolerability of nebivolol monotherapy by baseline systolic blood pressure: a retrospective analysis of pooled data from two multicenter, 12-week, randomized, double-blind, placebo-controlled, parallel-group, dose-ranging studies in patients with mild to moderate essential hypertension. Clin Ther. 2009;31:1946-1956.
- Lacourcière Y, Lefebvre J, Poirier L, Archambault F, Arnott W. Treatment of ambulatory hypertensives with nebivolol or hydrochlorothiazide alone and in combination: a randomized, double-blind, placebo-controlled, factorial-design trial. Am J Hypertens. 1994;7:137-145.
- Lewin A, Punzi H, Luo X, Stapff M. Nebivolol monotherapy for patients with systolic stage II hypertension: results of a randomized, placebo-controlled trial [published online ahead of print January 25, 2013]. Clin Ther. doi.10.1016/j.clinthera.2012.12.015.
- Saunders E, Smith WB, DeSalvo KB, Sullivan WA. The efficacy and tolerability of nebivolol in hypertensive African American patients. J Clin Hypertens. 2007;9:866-875.
- Neutel JM, Smith DH, Gradman AH. Adding nebivolol to ongoing antihypertensive therapy improves blood pressure and response rates in patients with uncontrolled stage l-ll hypertension. J Hum Hypertens. 2010;24:64-73.
- Weber MA, Basile J, Stapff M, Khan B, Zhou D. Blood pressure effects combined with β-blocker and angiotensin-converting enzyme inhibitor therapy compared with the individual agents: a placebo-controlled study with nebivolol and lisinopril. J Clin Hypertens. 2012;14:588-592.
- Source: Managed Markets Insight and Technology, LLC™, a trademark of MMIT Database, as of January 2019. Data are subject to change.
- U.S. Department of Health and Human Services Food and Drug Administration. Guidance for Industry Hypertension Indication: Drug Labeling for Cardiovascular Outcome Claims. March 2011. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM075072.pdf. Accessed March 2019.
- Punzi H, Lewin A, Lukić T, Goodin T, Wei Chen. Efficacy and safety of nebivolol in Hispanics with stage I-II hypertension: a randomized placebo-controlled trial. Ther Adv Cardiovasc Dis. 2010;4(6):349-357.
- Giles TD, Khan BV, Lato J, Brener L, Ma Y, Lukic T. Nebivolol monotherapy in younger adults (younger than 55 years) with hypertension: a randomized, placebo-controlled trial. J Clin Hypertens (Greenwich). 2013;15:687-693.
- Kamp O, Sieswerda GT, Visser CA. Comparison of effects on systolic and diastolic left ventricular function of nebivolol versus atenolol in patients with uncomplicated essential hypertension. Am J Cardiol. 2003;92(3):344-348.
based on
- Clinical Trial for the Use of Nitric Oxide to Treat Severe COVID-19 Infection
https://pharmaceuticalintelligence.com/2020/04/14/clinical-trial-for-the-use-of-nitric-oxide-to-treat-severe-covid-19/
-
LPBI Group’s Affiliates:
If you wish your Therapeutic solution to be included in the NEW DEFINITION of Treatment Protocol(s), then propose your component for inclusion in the Novel Treatment Protocol to be discussed on June 16, 2020
LPBI Group’s Affiliates Components in the Novel Treatment Protocol(s) Definition
- Prof. Saul Yedgar – Holder of US Patents on Rhinitis, anti-inflammation and other indications – 40 minutes
- Dr. Ajay Gupta, MD – Rhinitis drug approved in Japan – FDA Application for Approval of Repurposing to COVID-19 in the US – 40 minutes
- Dr. Raphael Nir, PhD, CSO, SBH, Sciences, Inc. – Drug Concept to mitigate Cytokine Storm in COVID-19
- Dr. Yigal Blum, PhD, ex-SRI Int’l VP and Entrepreneur – AMORPHOUS CALCIUM CARBONATE (ACC) TREATMENT FOR COVID-19
References on Nitric Oxide on PharmaceuticalIntellige.com – Open Access Online Scientific Journal include 299 articles
https://pharmaceuticalintelligence.com/?s=Nitric+Oxide
Of note
- Clinical Trial for the Use of Nitric Oxide to Treat Severe COVID-19 Infection
https://pharmaceuticalintelligence.com/2020/04/14/clinical-trial-for-the-use-of-nitric-oxide-to-treat-severe-covid-19/
Included in the 299 articles
- Transposon-mediated Gene Therapy improves Pulmonary Hemodynamics and attenuates Right Ventricular Hypertrophy: eNOS gene therapy reduces Pulmonary vascular remodeling and Arterial wall hyperplasia
Reporter: Aviva Lev-Ari, PhD, RN
- Endothelin Receptors in Cardiovascular Diseases: The Role of eNOS Stimulation
Author and Curator of an Investigator Initiated Study: Aviva Lev-Ari, PhD, RN
- Inhibition of ET-1, ETA and ETA-ETB, Induction of NO production, stimulation of eNOS and Treatment Regime with PPAR-gamma agonists (TZD): cEPCs Endogenous Augmentation for Cardiovascular Risk Reduction – A Bibliography
Curator of an Investigator Initiated Study: Aviva Lev-Ari, PhD, RN
- Cardiovascular Disease (CVD) and the Role of Agent Alternatives in endothelial Nitric Oxide Synthase (eNOS) Activation and Nitric Oxide Production
Curator and Investigator Initiated Study: Aviva Lev-Ari, PhD, RN
Leave a Reply