Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
The purpose of surgery is typically to remove the entire tumor, along with some of the healthy tissue around it, called the margin. If the tumor cannot be removed entirely, “debulking” surgery may be performed. Debulking surgery is a procedure in which the goal is to remove as much of the tumor as possible. Side effects of surgery include weakness, fatigue, and pain for the first few days following the procedure.
Chemotherapy
Chemotherapy is the use of drugs to kill tumor cells, usually by stopping the cells’ ability to grow and divide. Systemic chemotherapy is delivered through the bloodstream to reach tumor cells throughout the body. A chemotherapy regimen (schedule) usually consists of a specific number of cycles given over a set period of time. A patient may receive one drug at a time or combinations of different drugs at the same time. The side effects of chemotherapy depend on the individual and the dose used, but they can include fatigue, risk of infection, nausea and vomiting, loss of appetite, and diarrhea. These side effects usually go away once treatment is finished.
Radiation therapy is the use of high-energy x-rays or other particles to kill tumor cells. The most common type of radiation treatment is called external-beam radiation therapy, which is radiation given from a machine outside the body. When radiation treatment is given using implants, it is called internal radiation therapy or brachytherapy. A radiation therapy regimen usually consists of a specific number of treatments given over a set period of time. Side effects from radiation therapy may include fatigue, mild skin reactions, upset stomach, and loose bowel movements. Most side effects go away soon after treatment is finished.
Hormone therapy
The goal of hormone therapy is often to lower the levels of hormones in the body. Hormone therapy may be given to help stop the tumor from growing or to relieve symptoms caused by the tumor. In addition, for thyroid cancer, hormone therapy will be given if the thyroid gland has been removed, to replace the hormone that is needed by the body to function properly.
Immunotherapy (also called biologic therapy) is designed to boost the body’s natural defenses to fight the tumor. It uses materials made either by the body or in a laboratory to bolster, target, or restore immune system function. Examples of immunotherapy include cancer vaccines, monoclonal antibodies, and interferons. Alpha interferon is a form of biologic therapy given as an injection under the skin. This is sometimes used to help relieve symptoms caused by the tumor, but it can have severe side effects including fatigue, depression, and flu-like symptoms.
Targeted therapy is a treatment that targets the tumor’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This type of treatment blocks the growth and spread of tumor cells while limiting damage to normal cells, usually leading to fewer side effects than other cancer medications.
Recent studies show that not all tumors have the same targets. To find the most effective treatment, the doctor may run tests to identify the genes, proteins, and other factors in the tumor. As a result, doctors can better match each patient with the most effective treatment whenever possible.
Depending on the type of endocrine tumor, targeted therapy may be a possible treatment option. For instance, targeted therapies, such as sunitinib (Sutent) and everolimus (Afinitor), have been approved for treating advanced islet cell tumors. Early results of clinical trials (research studies) with targeted therapy drugs for other types of endocrine tumors are promising, but more research is needed to prove they are effective.
Recurrent endocrine tumor
Once the treatment is complete and there is a remission (absence of symptoms; also called “no evidence of disease” or NED). Many survivors feel worried or anxious that the tumor will come back. If the tumor does return after the original treatment, it is called a recurrent tumor. It may come back in the same place (called a local recurrence), nearby (regional recurrence), or in another place (distant recurrence). When this occurs, a cycle of testing will begin again to learn as much as possible about the recurrence. Often the treatment plan will include the therapies described above (such as surgery, chemotherapy, and radiation therapy) but may be used in a different combination or given at a different pace. People with a recurrent tumor often experience emotions such as disbelief or fear. Patients are encouraged to talk with their health care team about these feelings and ask about support services to help them cope.
Metastatic endocrine tumor
If a cancerous tumor has spread to another location in the body, it is called metastatic cancer. A treatment plan that includes a combination of surgery, chemotherapy, radiation therapy, hormone therapy, immunotherapy, or targeted therapy may be recommended if required.
In addition to treatment to slow, stop, or eliminate the cancer (also called disease-directed treatment), an important part of cancer care is relieving a person’s symptoms and side effects. It includes supporting the patient with his or her physical, emotional, and social needs, an approach called palliative or supportive care. People often receive disease-directed therapy and treatment to ease symptoms at the same time.
Sarcoma is a general class of cancers of mesenchymal cells that form connective tissues. Sarcoma can start in any part of the body and can be formed in the bones or in soft tissues. Sarcomas are rare cancers as compared to the more common epithelial cancers (carcinomas). Around 15,000 new cases of sarcomas diagnosed in the United States every year. Both children and adults can develop a sarcoma, however, while in adults it accounts for only about 1% of all cancers, sarcoma represents around 15% of all cancers in children.
There are tens of different types of sarcomas. This fact makes a particular type of sarcoma to be even rarer. Being sarcoma an uncommon cancer, it is strongly recommended for patients diagnosed with sarcoma to get consultant and treatment for the disease in sarcoma centers, or at list be treated by an oncologist physician that had experienced with sarcomas.
As stated, sarcomas are cancers of connective tissues, namely tissues that connect the body, holding it together. These tissues include: bones, cartilage, muscle, nerve, blood and lymph vessels, and fat. Therefore, sarcomas nomenclature is based according to the normal tissue type they most closely resemble (as opposed to carcinomas where the nomenclature is based upon the organ or part of the body where cancer is originated). Few examples: Osteosarcoma (OS) – cancer of bones origin; Chondrosarcoma – cancer of cells that produce cartilage; Fibrosarcoma – cancer derived from fibrous connective tissues cells; Rhabdomyosarcoma (RMS) – cancer from skeletal muscle progenitors; Liposarcoma – cancer that arises in fat cells, etc.
Watch a Dana-Farber Cancer Institute – About Sarcoma Video
Soft tissues sarcoma (STS)
Among sarcomas, the group of soft tissues sarcoma (STS) is the largest one, consists of many different types of cancers that origin in soft connective tissues that support and connect overall body parts. STSs account for less than 1% of all new cancer cases where about 11,000 new cases are diagnosed each year in the US, and about 4,000 people are dying from it each year. STS can occur almost anywhere in the body: about 60% of STSs occur in an arm or leg, 30% in the trunk (torso) or abdomen, and 10% in the head or neck. Because there are many different types of STS, it is more of a family of related cancer diseases then a single one. The specific types of STS are often named according to the normal tissue cells they most closely resemble (see introduction), however, some STSs do not look like any type of normal tissue and are thought to arise from stem cells. In addition to their tissue resemblance name, STS are characterized with grades and stages (Table I) where low-grade STSs are often local tumors that grow more slowly and are treated surgically (although radiation therapy or chemotherapy may be used occasionally), and intermediate – and high-grade STSs are tumors that are more likely to metastasize and are treated with a combination of surgery, chemotherapy and/or radiation therapy.
Figure 1. STS of the thigh muscle just above the knee.
In their early stages, STSs usually do not stimulate any symptoms and can grow unnoticed. This is because STSs are grown within soft connective tissues which are elastic and flexible, thus the tumor can develop quite large before being felt and cause any symptoms. The first noticeable symptom is usually a painless lump or swelling, however, since most lumps are not sarcoma they are often misdiagnosed. Eventually, the tumor interferes with normal body activities and cause pain by pressing against nerves and muscles, or if the sarcoma is located at the abdomen the tumor can induce abdominal pains or constipation. Therefore, when STS is suspected it should be examined for any unusual lumps growing to define whether they are malignant even if symptoms are not present, preferred by a sarcoma specialist. There are no standard screening tests for sarcoma. Usually a biopsy of the suspected tumor is taken to evaluate if indeed it is malignant and to define its type and grade. In addition, molecular testing of the tumor could be performed to identify specific genes unique to the tumor. Finally, imaging tests may be used to find out whether the cancer has metastasized.
Prognosis and current treatment
The five-year survival rate for localized-low grade sarcomas is 83%; 54% for intermediate sarcomas (spread to regional lymph nodes); and 16% for high grade STSs that have spread to distant parts of the body to form metastasis. Survival is depended also on tumor size, location, type, mitotic rate, and whether it is superficial or deep.
Surgery
Treatment options depend on the type and stage of cancer, possible side effects, and the patient’s preferences and overall health. Treatment can be a long and arduous process for many patients. Usually STSs are treated with surgery whenever it is possible. Should the tumor is not removable by surgery it may be possible to control its growth with radiation therapy. For a sarcoma that can be surgically removed, radiation therapy and/or chemotherapy may be given before or after surgery to reduce tumor recurrence. Small STSs can usually be effectively eliminated by surgery alone. However, sarcomas larger than 5 cm are often treated with a combination of surgery and radiation therapy or chemotherapy before surgery – to shrink the tumor and make its removal easier, or during and after surgery – to eradicate any remaining microscopic tumor cells. In addition, radiation and chemotherapy pre-surgical treatment might facilitate less surgery, preserving the limbs if the tumor is located in the arms or legs (limb-sparing surgery). Historically, STSs were treated with amputation; however, nowadays at least 90% of tumors are removed using limb-sparing surgery. In intermediate-high stages, chemotherapy and radiation therapy may also be used to reduce the size of the sarcoma or relieve pain and other symptoms.
Radiotherapy
The most commonly used radiation form is external beam radiation. Another mean of post surgically radiation is brachytherapy. This technique allows for high doses of radiation over a short period of time. The decision to use radiation before and/or after surgery is not standardized and may be changed on an individual case basis; Table II describes the choices of using radiation with surgery.
Table II: The advantages and disadvantages of the timing of radiotherapy
Proton therapy (also called proton beam therapy), a type of radiation treatment that uses protons rather than x-rays is also being adapted to treat sarcoma. This mode of radiotherapy allows target the radiation much more focused at the tumor site and thus is much protective to surrounding healthy tissue. This procedure however, is currently only available in a few specialized cancer centers in the US. In addition, particle therapy treatment with heavier charged particles such as carbon ions is being used and studied for the treatment of sarcomas in Japan and Germany.
Chemotherapy
Chemotherapy is often used when a sarcoma has already spread and can be given before surgery or, after surgery as adjuvant chemotherapy to destroy any microscopic tumor cells remained after surgery. In addition, when a tumor is considered non-operable, cycles of chemotherapy could be performed in order to shrink the tumor and make it necrotic to enable its removal by operation.
Different drugs are used to treat different subtypes of sarcoma. The types of chemotherapy that are used alone or in combination for most STSs include doxorubicin and ifosfamide that are the most common chemotherapy drugs employed for STS, as well as other ordinary chemotherapy drugs. The drug trabectedin, approved for use in Europe, is given for patients with advanced STS when conventional chemotherapy fails. Trabectedin has been shown to have high activity levels in the treatment of a specific subtype of liposarcoma (myxoid/round cell liposarcoma). Other chemotherapy drugs that are only used for certain subtypes of STS include: paclitaxel, docetaxel for Angiosarcoma; as well as vincristine, etoposide, actinomycin, and cyclophosphamide for Rhabdomyosarcoma and Ewing sarcoma.
Experimental chemotherapy drugs include Eribulin, a drug approved for treatment of breast cancer that has shown promising results in early clinical trials. In addition, new versions of sarcoma standard chemotherapy that cause fewer side effects are being studied in ongoing clinical trials. For instance, the three new versions of ifosfamide: palifosfamide, glufosfamide, and TH-302.
Targeted therapy
As genetic and molecular cancer research has evolved, targeted treatment to sarcoma became available. Targeted treatment to sarcoma intends to inhibit the growth and spread of cancer cells by hitting specific proteins, mainly by blocking the action of protein kinases.
Imatinib, a tyrosine-kinase inhibitor was approved in 2002 by the FDA for the treatment of gastrointestinal stromal tumor (GIST) in advanced stages and it is now the standard first-line treatment for GIST. In 2006, sunitinib multi-target receptor tyrosine kinase (RTK) inhibitor was also approved for the treatment of GIST when imatinib fails. Imatinib has been approved recently for use for patients with GIST after initial surgery, to try to prevent recurrence of the tumor. Imatinib is approved also for the treatment of advanced stage dermatofibrosarcoma protuberans (DFSP). Pazopanib, another multi-targeted inhibitor of receptor tyrosine kinase, has also been approved for patients with advanced STS as well as for use in sarcomas other than liposarcoma and GIST in conditions where standard chemotherapy is not working. Regorafenib is a new kinase inhibitor with significant activity in patients with advanced GIST who have already been treated with imatinib and suntinib. The FDA is currently reviewing a phase III clinical trial of this drug.
Closing remarks
Research efforts are made in order to elucidate new sarcoma-specific molecular targets. Studying sarcomas unique genetic fingerprints and understanding their value to sarcoma, not only can assist developing new drugs, but also may help better prediction of patients’ prognosis. To find the most effective treatment, tests to identify the genes, proteins, and other sarcoma-associated factors need to be developed and performed to give a better matched treatment for each patient. However, being sarcoma a highly diverse group of cancers make these efforts a hard task. These issues will be discussed further in future post(s) to be published in Pharmaceutical Intelligence.
“A research team from Stanford University’s School of Medicine is now one step closer to uncovering a cancer treatment that could be applicable across the board in killing every kind of cancer tumor” (1). It appeared that their antibody-drug against the CD47 protein, enabled the shrinking of all tumor cells. After completing their animal studies the researchers now move into a human phase clinical trials. CD47 has been previously studied and evaluated for its role in multiple cells, some of this data however, is somewhat controversy. So where do we stand?
CD47
CD47 (originally named integrin-associated protein (IAP)) is a cell surface protein of the immunoglobulin (Ig) superfamily, which is heavily glycosylated and expressed by virtually all cells in the body and overexpressed in many types of cancer including breast, ovarian, colon, prostate and others (3). CD47 was first recognized as a 50 kDa protein associated and copurified with the Alpha-v-Beta-3 integrin in placenta and neutrophil granulocytes and later shown to have the capacity to regulate integrin function and the responsiveness of leukocytes to RGD-containing extracellular matrix proteins. CD47 has also been shown to be identical to the OA-3/OVTL3 antigen highly expressed on most ovarian carcinomas (4,5).
CD47 consists of an extracellular IgV domain, a five times transmembrane-spanning domain, and a short alternatively spliced cytoplasmic tail. In both humans and mice, the cytoplasmic tail can be found as four different splice isoforms ranging from 4 to 36 amino acids, showing different tissue expression patterns (3).
CD47 interactions (3, 6):
Thrombospondin-1 (TSP-1) – a secreted glycoprotein that plays a role in vascular development and angiogenesis. Binding of TSP-1 to CD47 influences several fundamental cellular functions including cell migration and adhesion, cell proliferation or apoptosis, and plays a role in the regulation of angiogenesis and inflammation.
Signal-regulatory protein-alpha (SIRPα) – an inhibitory transmembrane receptor present on myeloid cells. The CD47/SIRPα interaction leads to bidirectional signaling, resulting in different cell-to-cell responses including inhibition of phagocytosis, stimulation of cell-cell fusion, and T-cell activation.
Integrins – several membrane integrins, most commonly integrin avb3. These interactions result in CD47/integrin complexes that effect a range of cell functions including adhesion, spreading and migration
These interactions with multiple proteins and cells types create several important functions, which include:
Cell proliferation – cell proliferation is heavily dependent on cell type as both activation and loss of CD47 can result in enhanced proliferation. For example, activation of CD47 with TSP-1 in wild-type cells inhibits proliferation and reduces expression of stem cell transcription factors. In cancer cells however, activation of CD47 with TSP-1 increases proliferation of human U87 and U373 astrocytoma. it is likely that CD47 promotes proliferation via the PI3K/Akt pathway in cancerous cells but not normal cells (7). Loss of CD47 allows sustained proliferation of primary murine endothelial cells and enables these cells to spontaneously reprogram to form multipotent embryoid body-like clusters (8).
Apoptosis – Ligation of CD47 by anti-CD47mAbs was found to induce apoptosis in a number of different cell types (3). For example: Of the two SIRP-family members known to bind the CD47 IgV domain (SIRPα and SIRPγ), SIRPα as a soluble Fc-fusion protein does not induce CD47-dependent apoptosis, hile SIRPα or SIRPγ bound onto the surface of beads induces apoptosis through CD47 in Jurkat T cells and the myelomonocytic cell line U937.
Migration – CD47 role on cell migration was first demonstrated in neutrophils, these effects were shown to be dependent on avb3 integrins, which interact with and are activated by CD47 at the plasma membrane. In cancer, Blocking CD47 function has been shown to inhibit migration and metastasis in a variety of tumor models. Blockade of CD47 by neutralizing antibodies reduced migration and chemotaxis in response to collagen IV in melanoma, prostate cancer and ovarian cancer-derived cells (9).
Angiogenesis – The mechanism of the anti-angiogenic activity of CD47 is not fully understood, but introduction of CD47 antibodies and TSP-1 have been shown to inhibit nitric oxide (NO)-stimulated responses in both endothelial and vascular smooth muscle cells (10). More so, CD47 signaling influences the SDF-1 chemokine pathway, which plays a role in angiogenesis (11). (12)
Inflammatory response – Interactions between endothelial cell CD47 and leukocyte SIRPγ regulate T cell transendothelial migration (TEM) at sites of inflammation. CD47 also functions as a marker of self on murine red blood cells which allows RBC to avoid phagocytosis. Tumor cells can also evade macrophage phagocytosis through the expression of CD47 (2, 13).
It appears that CD47 ligation induce different responses, depending on cell type and partner for ligation.
Therapeutic and clinical aspect of CD47 in human cancer:
CD47 is overexpressed in many types of human cancers and its known function as a “don’t eat me” signal, suggests the potential for targeting the CD47-SIRPα pathway as a common therapy for human malignancies (2,13). Upregulation of CD47 expression in human cancers also appears to influence tumor growth and dissemination. First, increased expression of CD47 in several hematologic malignancies was found to be associated with a worse clinical prognosis, and in ALL to predict refractoriness to standard chemotherapies (13, 14-16). Second, CD47 was demonstrated to regulate tumor metastasis and dissemination in both MM and NHL (13, 17).
Efforts have been made to develop therapies inhibiting the CD47-SIRPα pathway, principally through blocking monoclonal antibodies directed against CD47, but also possibly with a recombinant SIRPα protein that can also bind and block CD47.
Chao MP et al. 2012 Combination strategies targeting CD47 in cancer
While monotherapies targeting CD47 were efficacious in several pre-clinical tumor models, combination strategies involving inhibition of the CD47-SIRPα pathway offer even greater therapeutic potential. Specifically, antibodies targeting CD47-SIRPα can be included in combination therapies with other therapeutic antibodies, macrophage-enhancing agents, chemo-radiation therapy, or as an adjuvant therapy to inhibit metastasis (13).
For example, anti-SIRPα antibody was found to potentiate antibody-dependent cellular cytotoxicity (ADCC) mediated by the anti-Her2/Neu antibody trastuzumab against breast cancer cells (18). CD47–SIRPα interactions and SIRPα signaling negatively regulate trastuzumab-mediated ADCC in vitro and antibody-dependent elimination of tumor cells in vivo
More so, chemo-radiation therapy-mediated upregulation of cell surface calreticulin may potentially augment the activity of anti-CD47 antibody. However, this approach may also lead to increased toxicity as cell surface calreticulin is expressed on non-cancerous cells undergoing apoptosis, a principle effect of chemo-radiation therapy (19).
Highlights:
Phagocytic cells, macrophages, regulate tumor growth through phagocytic clearance
CD47 binds SIRPα on phagocytes which delivers an inhibitory signal for phagocytosis
A blocking anti-CD47 antibody enabled phagocytic clearance of many human cancers
Phagocytosis depends on a balance of anti-(CD47) and pro-(calreticulin) signals
Anti-CD47 antibody synergized with an FcR-engaging antibody, such as rituximab
Summary
Evasion of immune recognition is a major mechanism by which cancers establish and propagate disease. Recent data has demonstrated that the innate immune system plays a key role in modulating tumor phagocytosis through the CD47-SIRPα pathway. Careful development of reagents that can block the CD47/SIRPα interaction may indeed be useful to treat many forms of cancer without having too much of a negative side effect in terms of inducing clearance of host cells. Therapeutic approaches inhibiting this pathway have demonstrated significant efficacy, leading to the reduction and elimination of multiple tumor types.
Dr. Weissman says: “We are now hopeful that the first human clinical trials of anti-CD47 antibody will take place at Stanford in mid-2014, if all goes well. Clinical trials may also be done in the United Kingdom”. These clinical trials must be designed so that the data they generate will produce a valid scientific result!!!
2. Willingham SB, Volkmer JP, Gentles AJ, Sahoo D, Dalerba P, Mitra SS, Wang J, Contreras-Trujillo H, Martin R, Cohen JD, Lovelace P, Scheeren FA, Chao MP, Weiskopf K, Tang C, Volkmer AK, Naik TJ, Storm TA, Mosley AR, Edris B, Schmid SM, Sun CK, Chua MS, Murillo O, Rajendran P, Cha AC, Chin RK, Kim D, Adorno M, Raveh T, Tseng D, Jaiswal S, Enger PØ, Steinberg GK, Li G, So SK, Majeti R, Harsh GR, van de Rijn M, Teng NN, Sunwoo JB, Alizadeh AA, Clarke MF, Weissman IL. The CD47-signal regulatory protein alpha (SIRPa) interaction is a therapeutic target for human solid tumors. Proc Natl Acad Sci U S A. 2012 Apr 24;109(17):6662-6667. http://www.pnas.org/content/early/2012/03/20/1121623109
3. Oldenborg PL. CD47: A Cell Surface Glycoprotein Which Regulates Multiple Functions of Hematopoietic Cells in Health and Disease. ISRN Hematology Volume 2013 (2013), Article ID 614619, 19 pages. http://www.hindawi.com/isrn/hematology/2013/614619/
4. G. Campbell, P. S. Freemont, W. Foulkes, and J. Trowsdale, “An ovarian tumor marker with homology to vaccinia virus contains an IgV- like region and multiple transmembrane domains,”Cancer Research, vol. 52, no. 19, pp. 5416–5420, 1992. http://cancerres.aacrjournals.org/content/52/19/5416.long
5. L. G. Poels, D. Peters, Y. van Megen et al., “Monoclonal antibody against human ovarian tumor-associated antigens,” Journal of the National Cancer Institute, vol. 76, no. 5, pp. 781–791, 1986. http://www.ncbi.nlm.nih.gov/pubmed/3517452
7. Sick E, Boukhari A, Deramaudt T, Rondé P, Bucher B, André P, Gies JP, Takeda K (February 2011). “Activation of CD47 receptors causes proliferation of human astrocytoma but not normal astrocytes via an Akt-dependent pathway”. Glia59 (2): 308–319. http://www.ncbi.nlm.nih.gov/pubmed/21125662
9. Shahan TA, Fawzi A, Bellon G, Monboisse JC, Kefalides NA. “Regulation of tumor cell chemotaxis by type IV collagen is mediated by a Ca(2+)-dependent mechanism requiring CD47 and the integrin alpha(V)beta(3)”. J. Biol. Chem 2000.275 (7): 4796–4802. http://www.jbc.org/content/275/7/4796
10. Isenberg JS, Ridnour LA, Dimitry J, Frazier WA, Wink DA, Roberts DD. “CD47 is necessary for inhibition of nitric oxide-stimulated vascular cell responses by thrombospondin-1”. J. Biol. Chem 2006. 281 (36): 26069–26080. http://www.jbc.org/content/281/36/26069
11. Smadja DM, d’Audigier C, Bièche I, Evrard S, Mauge L, Dias JV, Labreuche J, Laurendeau I, Marsac B, Dizier B, Wagner-Ballon O, Boisson-Vidal C, Morandi V, Duong-Van-Huyen JP, Bruneval P, Dignat-George F, Emmerich J, Gaussem P. “Thrombospondin-1 is a plasmatic marker of peripheral arterial disease that modulates endothelial progenitor cell angiogenic properties”. Arterioscler. Thromb. Vasc. Biol 2011. 31 (3): 551–559. http://atvb.ahajournals.org/content/31/3/551
14. Majeti R, Chao MP, Alizadeh AA, Pang WW, Jaiswal S, Gibbs KD, Jr, van Rooijen N, Weissman IL. Cd47 is an adverse prognostic factor and therapeutic antibody target on human acute myeloid leukemia stem cells. Cell. 2009;138(2):286–299. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2726837/
15. Chao MP, Alizadeh AA, Tang C, Jan M, Weissman-Tsukamoto R, Zhao F, Park CY, Weissman IL, Majeti R. Therapeutic antibody targeting of cd47 eliminates human acute lymphoblastic leukemia.Cancer Res. 2011;71 (4):1374–1384. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3041855/
16. Chao MP, Alizadeh AA, Tang C, Myklebust JH, Varghese B, Gill S, Jan M, Cha AC, Chan CK, Tan BT, Park CY, et al. Anti-cd47 antibody synergizes with rituximab to promote phagocytosis and eradicate non-hodgkin lymphoma. Cell. 2010;142(5):699–713. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2943345/
17. Chao MP, Tang C, Pachynski RK, Chin R, Majeti R, Weissman IL. Extranodal dissemination of non-hodgkin lymphoma requires cd47 and is inhibited by anti-cd47 antibody therapy. Blood.2011;118(18):4890–4901. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3208297/
18. Zhao XW, van Beek EM, Schornagel K, Van der Maaden H, Van Houdt M, Otten MA, Finetti P, Van Egmond M, Matozaki T, Kraal G, Birnbaum D, et al. Cd47-signal regulatory protein-alpha (sirpalpha) interactions form a barrier for antibody-mediated tumor cell destruction. Proc Natl Acad Sci U S A.2011;108(45):18342–18347. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3215076/
19. Obeid M, Tesniere A, Ghiringhelli F, Fimia GM, Apetoh L, Perfettini JL, Castedo M, Mignot G, Panaretakis T, Casares N, Metivier D, et al. Calreticulin exposure dictates the immunogenicity of cancer cell death. Nat Med. 2007;13(1):54–61. http://www.ncbi.nlm.nih.gov/pubmed/17187072
Other related articles on this Open Access Online Scientific Journal include the following:
ByBeatrijs A. Seinstra1, et. al. published mid-2010, gives a review of the state-of-the-art of the then available methods for local lesions’ ablation. As far as ablation techniques availability, I have found this review very much relevant to today’s technological reality. It is worthwhile noting that in the last couple of years, new imaging-based navigation and guidance applications were introduced into the market holding a promise to improve the accuracy of administrating such treatment. These are subject to clinical validation in large clinical studies. From the above mentioned publication I have chosen to highlight the parts discussing the importance of imaging-based guidance to the effective application of localized ablation-type therapies.
The clinical need:
Hepatocellular carcinoma (HCC) is a primary malignant tumor of the liver that accounts for an important health problem worldwide. Primary liver cancer is the sixth most common cancer worldwide with an incidence of 626,000 patients a year, and the third most common cause of cancer-related death [1]. Only 10–15% of HCC patients are suitable candidates for hepatic resection and liver transplantation due to the advanced stage of the disease at time of diagnosis and shortage of donors.
Immerging solution:
In order to provide therapeutic options for patients with inoperable HCC, several minimally invasive image-guided therapies for locoregional treatment have been developed. HCC has a tendency to remain confined to the liver until the disease has advanced, making these treatments particularly attractive.
Minimally invasive image-guided therapies can be divided into the group of the tumor ablative techniques or the group of image-guided catheter-based techniques. Tumor ablative techniques are either based on thermal tumor destruction, as in radiofrequency ablation (RFA), cryoablation, microwave ablation, laser ablation and high-intensity focused ultrasound (HIFU), or chemical tumor destruction, as in percutaneous ethanol injection (PEI). These techniques are mostly used for early stage disease. Image-guided catheter-based techniques rely on intra-arterial delivery of embolic, chemoembolic, or radioembolic agents [22]. These techniques enable treatment of large lesions or whole liver treatment, and are as such used for intermediate stage HCC (Figure 1).
Minimally invasive image-guided ablation techniques and intra-arterial interventions may prolong survival, spare more functioning liver tissue in comparison to surgical resection (which can be very important in cirrhotic patients), allow retreatment if necessary, and may be an effective bridge to transplantation [23–27].
During the last 2 decades, minimally invasive image-guided therapies have revolutionized the management of inoperable HCC.
The value of image guidance
Accurate imaging is of great importance during minimally invasive loco-regional therapies to efficiently guide and monitor the treatment. It enables proper placement of instruments, like the probe in case of ablation or the catheter in case of intra-arterial therapy, and accurate monitoring of the progression of the necrotic zone during ablation.
can all be employed. In current clinical practice, placement of the catheter in intra-arterial procedures is usually performed under fluoroscopic guidance, while ablation may be guided by ultrasound, CT or MRI.
Ultrasound guidance allows probe insertion from every angle, offers real time visualization and correction for motion artifacts when targeting the tumor, and is low cost. However, the gas created during ablation (or ice in the case of cryoablation) hampers penetration of the ultrasound beams in tissue, causing acoustic shadowing and obscuring image details like the delineation between tumor borders and ablation zone.
CT is also frequently used to guide minimally invasive ablation therapy, and is a reliable modality to confirm treatment results. In comparison to US, it provides increased lesion discrimination, a more reliable depiction of ablated/non-ablated interfaces, and a better correlation to pathologic size [28]. However, due to its hypervascularity, small HCCs can only be clearly visualized in the arterial phase for a short period of time. Another disadvantage of CT is the exposure of the patient and physician to ionizing radiation.
Combining US imaging for probe placement and CT for ablation monitoring reduces this exposure. At the moment, hybrid systems are being developed, enabling combination of imaging techniques, like ultrasound and CT imaging, thereby improving the registration accuracy during treatment [29]. The interest in MRI-guided ablation is growing, as it produces a high-quality image allowing high-sensitivity tumor detection and accurate identification of the target region with multiplanar imaging.
MRI also enables real-time monitoring of the temperature evolution during treatment [30–35]. However, MRI is an expensive technique, and MRI-guided ablation is still limited in clinical practice. Currently, the most widely used ablation technique for percutaneous treatment of focal hepatic malignancies is radiofrequency ablation (RFA), which has been shown to be safe and effective for the treatment of early stage HCC [48–50]. During RFA, a small electrode is placed within the tumor, and a high-frequency alternating electric current (approximately 400 MHz) is generated, causing ionic agitation within the tissue. ….. Most frequently ultrasound is used for image guidance (Figs. 2, 3), but there are reports of groups who use CT, MRI, or fluoroscopic imaging.
Ultrasound guided RFA. a: HCC lesion in a non-surgical patient pre-treatment (pointed out by arrow). b: Just after start treatment, electrode placed centrally in the tumor. c: Gas formation during ablation causes acoustic shadowing
Contrast-enhanced CT pre- and post-RFA. Same patient as in Fig. 2. a: Hypervascular lesion (biopsy proven HCC) in right liver lobe (pointed out by arrow) before treatment. b: Ablated lesion directly post ablation, with reactive hyperemia around the RFA lesion
References
1.
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55:74–108PubMedCrossRef
2.
[No authors listed] (1987) Hepatocellular cancer: differences between high and low incidence regions. Lancet 2:1183–1184
3.
El-Serag HB, Davila JA, Petersen NJ, McGlynn KA (2003) The continuing increase in the incidence of hepatocellular carcinoma in the United States: an update. Ann Intern Med 139:817–823PubMed
4.
Taylor-Robinson SD, Foster GR, Arora S, Hargreaves S, Thomas HC (1997) Increase in primary liver cancer in the UK, 1979–94. Lancet 350:1142–1143PubMedCrossRef
5.
Beasley RP, Hwang LY, Lin CC, Chien CS (1981) Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22,707 men in Taiwan. Lancet 2:1129–1133PubMedCrossRef
6.
Beasley RP (1988) Hepatitis B virus. The major etiology of hepatocellular carcinoma Cancer 61:1942–1956
7.
Chen HL, Chang MH, Ni YH, Hsu HY, Lee PI, Lee CY et al (1996) Seroepidemiology of hepatitis B virus infection in children: Ten years of mass vaccination in Taiwan. JAMA 276:906–908PubMedCrossRef
8.
Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS et al (1997) Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N Engl J Med 336:1855–1859PubMedCrossRef
9.
Adami HO, Hsing AW, McLaughlin JK, Trichopoulos D, Hacker D, Ekbom A et al (1992) Alcoholism and liver cirrhosis in the etiology of primary liver cancer. Int J Cancer 51:898–902PubMedCrossRef
10.
Bruix J, Barrera JM, Calvet X, Ercilla G, Costa J, Sanchez-Tapias JM et al (1989) Prevalence of antibodies to hepatitis C virus in Spanish patients with hepatocellular carcinoma and hepatic cirrhosis. Lancet 2:1004–1006PubMedCrossRef
11.
Colombo M, Kuo G, Choo QL, Donato MF, Del NE, Tommasini MA et al (1989) Prevalence of antibodies to hepatitis C virus in Italian patients with hepatocellular carcinoma. Lancet 2:1006–1008PubMedCrossRef
12.
Tsukuma H, Hiyama T, Tanaka S, Nakao M, Yabuuchi T, Kitamura T et al (1993) Risk factors for hepatocellular carcinoma among patients with chronic liver disease. N Engl J Med 328:1797–1801PubMedCrossRef
13.
Pons F, Varela M, Llovet JM (2005) Staging systems in hepatocellular carcinoma. HPB (Oxford) 7:35–41
14.
Llovet JM, Fuster J, Bruix J (2004) The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl 10:S115–S120PubMedCrossRef
15.
Bruix J, Llovet JM (2009) Major achievements in hepatocellular carcinoma. Lancet 373:614–616PubMedCrossRef
16.
Geschwind JF (2002) Chemoembolization for hepatocellular carcinoma: where does the truth lie? J Vasc Interv Radiol 13:991–994PubMedCrossRef
17.
Bruix J, Llovet JM (2002) Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology 35:519–524PubMedCrossRef
18.
Bruix J, Castells A, Bosch J, Feu F, Fuster J, Garcia-Pagan JC et al (1996) Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology 111:1018–1022PubMedCrossRef
19.
Llovet JM, Fuster J, Bruix J (1999) Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 30:1434–1440PubMedCrossRef
20.
Thomas MB, O’Beirne JP, Furuse J, Chan AT, bou-Alfa G, Johnson P (2008) Systemic therapy for hepatocellular carcinoma: cytotoxic chemotherapy, targeted therapy and immunotherapy. Ann Surg Oncol 15:1008–1014PubMedCrossRef
21.
Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF et al (2008) Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 359:378–390PubMedCrossRef
22.
Trinchet JC, Ganne-Carrie N, Beaugrand M (2003) Review article: intra-arterial treatments in patients with hepatocellular carcinoma. Aliment Pharmacol Ther 17(Suppl 2):111–118PubMedCrossRef
23.
Lu DS, Yu NC, Raman SS, Lassman C, Tong MJ, Britten C et al (2005) Percutaneous radiofrequency ablation of hepatocellular carcinoma as a bridge to liver transplantation. Hepatology 41:1130–1137PubMedCrossRef
24.
Mazzaferro V, Battiston C, Perrone S, Pulvirenti A, Regalia E, Romito R et al (2004) Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann Surg 240:900–909PubMedCrossRef
25.
Graziadei IW, Sandmueller H, Waldenberger P, Koenigsrainer A, Nachbaur K, Jaschke W et al (2003) Chemoembolization followed by liver transplantation for hepatocellular carcinoma impedes tumor progression while on the waiting list and leads to excellent outcome. Liver Transpl 9:557–563PubMedCrossRef
26.
Yao FY, Kerlan RK, Hirose R, Davern TJ, Bass NM, Feng S et al (2008) Excellent outcome following down-staging of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat analysis. Hepatology 48:819–827PubMedCrossRef
27.
Chapman WC, Majella Doyle MB, Stuart JE, Vachharajani N, Crippin JS, Anderson CD et al (2008) Outcomes of neoadjuvant transarterial chemoembolization to downstage hepatocellular carcinoma before liver transplantation. Ann Surg 248:617–625PubMed
28.
Cha CH, Lee FT Jr, Gurney JM, Markhardt BK, Warner TF, Kelcz F et al (2000) CT versus sonography for monitoring radiofrequency ablation in a porcine liver. AJR Am J Roentgenol 175:705–711PubMed
29.
Wood BJ, Locklin JK, Viswanathan A, Kruecker J, Haemmerich D, Cebral J et al (2007) Technologies for guidance of radiofrequency ablation in the multimodality interventional suite of the future. J Vasc Interv Radiol 18:9–24PubMedCrossRef
30.
Hokland SL, Pedersen M, Salomir R, Quesson B, Stodkilde-Jorgensen H, Moonen CT (2006) MRI-guided focused ultrasound: methodology and applications. IEEE Trans Med Imaging 25:723–731PubMedCrossRef
31.
Cline HE, Hynynen K, Watkins RD, Adams WJ, Schenck JF, Ettinger RH et al (1995) Focused US system for MR imaging-guided tumor ablation. Radiology 194:731–737PubMed
32.
Hynynen K, Freund WR, Cline HE, Chung AH, Watkins RD, Vetro JP et al (1996) A clinical, noninvasive, MR imaging-monitored ultrasound surgery method. Radiographics 16:185–195PubMed
33.
Kopelman D, Inbar Y, Hanannel A, Dank G, Freundlich D, Perel A et al (2006) Magnetic resonance-guided focused ultrasound surgery (MRgFUS). Four ablation treatments of a single canine hepatocellular adenoma HPB (Oxford) 8:292–298
34.
Kopelman D, Inbar Y, Hanannel A, Freundlich D, Castel D, Perel A et al (2006) Magnetic resonance-guided focused ultrasound surgery (MRgFUS): ablation of liver tissue in a porcine model. Eur J Radiol 59:157–162PubMedCrossRef
35.
Gedroyc WM (2005) Magnetic resonance guidance of thermal ablation. Top Magn Reson Imaging 16:339–353PubMedCrossRef
36.
Livraghi T, Festi D, Monti F, Salmi A, Vettori C (1986) US-guided percutaneous alcohol injection of small hepatic and abdominal tumors. Radiology 161:309–312PubMed
37.
Shiina S, Yasuda H, Muto H, Tagawa K, Unuma T, Ibukuro K et al (1987) Percutaneous ethanol injection in the treatment of liver neoplasms. AJR Am J Roentgenol 149:949–952PubMed
38.
Lencioni R, Cioni D, Crocetti L, Bartolozzi C (2004) Percutaneous ablation of hepatocellular carcinoma: state-of-the-art. Liver Transpl 10:S91–S97PubMedCrossRef
39.
Shiina S, Teratani T, Obi S, Sato S, Tateishi R, Fujishima T et al (2005) A randomized controlled trial of radiofrequency ablation with ethanol injection for small hepatocellular carcinoma. Gastroenterology 129:122–130PubMedCrossRef
40.
Lencioni R, Bartolozzi C, Caramella D, Paolicchi A, Carrai M, Maltinti G et al (1995) Treatment of small hepatocellular carcinoma with percutaneous ethanol injection. Analysis of prognostic factors in 105 Western patients. Cancer 76:1737–1746PubMedCrossRef
41.
Livraghi T, Giorgio A, Marin G, Salmi A, De Sio I, Bolondi L et al (1995) Hepatocellular carcinoma and cirrhosis in 746 patients: long-term results of percutaneous ethanol injection. Radiology 197:101–108PubMed
42.
Di SM, Buscarini L, Livraghi T, Giorgio A, Salmi A, De Sio I et al (1997) Percutaneous ethanol injection in the treatment of hepatocellular carcinoma. A multicenter survey of evaluation practices and complication rates Scand J Gastroenterol 32:1168–1173
43.
Lencioni RA, Allgaier HP, Cioni D, Olschewski M, Deibert P, Crocetti L et al (2003) Small hepatocellular carcinoma in cirrhosis: randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology 228:235–240PubMedCrossRef
44.
Lin SM, Lin CJ, Lin CC, Hsu CW, Chen YC (2004) Radiofrequency ablation improves prognosis compared with ethanol injection for hepatocellular carcinoma ≤4 cm. Gastroenterology 127:1714–1723PubMedCrossRef
45.
Lin SM, Lin CJ, Lin CC, Hsu CW, Chen YC (2005) Randomised controlled trial comparing percutaneous radiofrequency thermal ablation, percutaneous ethanol injection, and percutaneous acetic acid injection to treat hepatocellular carcinoma of 3 cm or less. Gut 54:1151–1156PubMedCrossRef
46.
Brunello F, Veltri A, Carucci P, Pagano E, Ciccone G, Moretto P et al (2008) Radiofrequency ablation versus ethanol injection for early hepatocellular carcinoma: A randomized controlled trial. Scand J Gastroenterol 43:727–735PubMedCrossRef
47.
Orlando A, Leandro G, Olivo M, Andriulli A, Cottone M (2009) Radiofrequency thermal ablation vs. percutaneous ethanol injection for small hepatocellular carcinoma in cirrhosis: meta-analysis of randomized controlled trials. Am J Gastroenterol 104:514–524PubMedCrossRef
48.
Curley SA, Izzo F, Delrio P, Ellis LM, Granchi J, Vallone P et al (1999) Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg 230:1–8PubMedCrossRef
49.
Curley SA, Izzo F, Ellis LM, Nicolas VJ, Vallone P (2000) Radiofrequency ablation of hepatocellular cancer in 110 patients with cirrhosis. Ann Surg 232:381–391PubMedCrossRef
50.
Goldberg SN, Gazelle GS, Solbiati L, Livraghi T, Tanabe KK, Hahn PF et al (1998) Ablation of liver tumors using percutaneous RF therapy. AJR Am J Roentgenol 170:1023–1028PubMed
Other research papers related to the management of Prostate cancer were published on this Scientific Web site:
Harnessing Personalized Medicine for Cancer Management, Prospects of Prevention and Cure: Opinions of Cancer Scientific Leaders @ http://pharmaceuticalintelligence.com
Acute lymphoblastic leukemia (ALL) is a malignant disorder of lymphoid progenitor cells was previously discussed for the genetic origin and the prognostic factors used in clinical trials (1). We will now focus on the treatment options with emphasis on the bone marrow transplantation (2).
According to the National Cancer Institute (NCI), the treatment of childhood ALL usually has 3 phases (3a):
Induction Therapy: The goal is to kill leukemia cells in both the blood and the bone marrow and induce a remission.
Consolidation/Intensification Therapy: It begins once the leukemia is in remission. The goal is to kill any remaining leukemia cells that may not be active but may regrow and cause relapse.
Maintenance Therapy: The goal is to kill any remaining leukemia cells that may regrow and cause relapse. In this phase the different cancer treatments are usually been given at lower doses than those in the previous phases.
Four types of cancer treatment are used:
Chemotherapy – The way the chemotherapy is given depends on the child’s risk group. Children with high-risk ALL receive more anticancer drugs, higher doses of anticancer drugs, and receive treatment for a longer time than children with standard-risk ALL.. The full list of approved drug (3b)
Radiation Therapy– is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. External radiation therapy may be used to treat childhood ALL that has spread, or may spread, to the brain and spinal cord.
Chemotherapy with stem cell transplantation– A method inwhich stem cells (immature blood cells) are removed from the blood or bone marrow of a donor. After the patient receives treatment, the donor’s stem cells are given to the patient through an infusion. These reinfused stem cells grow into (and restore) the patient’s blood cells. Stem cell transplant is rarely used as initial treatment for children and teenagers with ALL. It is used more often as part of treatment for ALL that relapses
Targeted Therapy – Tyrosine Kinase Inhibitors (TKIs) are targeted therapy drugs that block the enzyme, tyrosine kinase, which causes stem cells to become more white blood cells or blasts than the body needs. For example, imatinib mesylate (Gleevec) is a TKI used in the treatment of children with Philadelphia chromosome-positive ALL. However, because patients can develop resistance to these drugs, new tyrosine kinase inhibitors are being investigated. For example, nilotinib (AMN-107) is being studied for patients with Philadelphia chromosome positive ALL who are resistant to imatinib
Bone Marrow or Peripheral Blood Stem cell Transplant for ALL
Stem cell transplants (SCT) offer a way for doctors to use high doses of chemo. Although the drugs destroy the patient’s bone marrow, transplanted stem cells can restore the bone marrow’s ability to make blood. Stem cells for a transplant come from either the blood or from the bone marrow. Bone marrow transplants were more common in the past, but they have largely been replaced by peripheral blood stem cell transplant (PBSCT).
Types of Transplants (4).
The stem cells can come from either the patient (an autologoustransplant) or from a matched donor (an allogeneictransplant).
Allogeneic stem cell transplant: In an allogeneic transplant, the stem cells come from someone else – usually a donor whose tissue type is a very close match to the patient’s. The donor may be a brother or sister if they are a good match. Less often, an unrelated donor may be found. An allogeneic transplant is the preferred type of transplant for ALL when it is available.
“Mini-transplant”: “mini-transplant” (also called a non-myeloablative transplant or reduced-intensity transplant), where they get lower doses of chemo and radiation that do not destroy all the cells in their bone marrow. They then are given the donor stem cells. These cells enter the body and form a new immune system, which sees the leukemia cells as foreign and attacks them (a graft-versus-leukemia effect). This is not a standard treatment for ALL, and is being studied to find out how useful it may be.
Autologous stem cell transplant: In an autologous transplant, a patient’s own stem cells are removed from his or her bone marrow or blood. They are frozen and stored while the person gets treatment (high-dose chemo and/or radiation). The stem cells are then given back to the patient after treatment.
One problem with autologous transplants is that it is hard to separate normal stem cells from leukemia cells in the bone marrow or blood samples. Even after treating the stem cells in the lab to try to kill or remove any leukemia cells, there is the risk of returning some leukemia cells with the stem cell transplant
Stem cell transplants and side effects (4):
Early side effects: Early side effects are much the same as those caused by any other type of high-dose chemo, such as nausea, vomiting, loss of appetite, mouth sores, and hair loss. Because of the high doses of chemo used, these can sometimes be severe.
Infection resulting from a weakened immune system is the most common side effect. Because the stem cell procedure is done more swiftly, the risk period is shorter than with bone marrow transplantation. The risk for infection is most critical during the first 6 weeks following the transplant, but it takes 6 – 12 months post-transplant for a patient’s immune system to fully recover. Immune systems of patients with graft-versus-host disease can take even longer to function normally. Low red cell count and platelet counts are also early-side effects that when happens are treated with blood transfusion.
A rare but serious side effect of stem cell transplant is called veno-occlusive disease of the liver (VOD). In this disease, the high doses of chemo given for the transplant damage the liver. Symptoms include weight gain (from fluid collecting), liver swelling, and yellowing of the skin and eyes (jaundice). When severe, it can lead to liver failure, kidney failure, and even death.
Long-term side effects: Some side effects can last for a long time, or may not happen until years after the transplant. These long-term side effects can include the following:
Acute/Chronic Graft-versus-host disease (GVHD), which occurs only in a donor transplant
Organ damage: lungs ( shortness of breath), ovaries (infertility and loss of menstrual period), thyroid, eyes (cataract), bone etc.
Developing another type of leukemia or other cancer several years later.
ALL (and AML), Bone Marrow transplant and Clinical Trials
Back in the early 80’s, chemotherapy was shown to cure a substantial portions of patients with ALL. Yet some patients had high risk of relapse when treated using conventional regimens, due to patient- and disease-related variables. Bone marrow transplantation (BMT) was found to have encouraging results depending on the circumstances, yet the relative role between chemo and BMT to high-risk patients was controversial.
It was believed that the factors which predict poor outcome with chemo do not adversely affect the transplant outcome, yet this assumption was not based on comparing similar predicting factors . More so, the prognostic factors for outcome after BMT were not well-defined and the optimal regimen for transplant was not agreed upon. Thus, researches aimed to identify the characteristics and factors affecting good outcome after transplantation for ALL in first and second remission.
For this, 690 patients with HLA-identical sibling receiving allogeneic BMT either after first or second complete remission (CR). Numerous factors were accounted for including; age, sex, donor-recipient sex match, chemo regimen and presence of GVHD.
Of the many factors evaluated, several were highly significant in BMT outcome:
GVHD – It may have both favorable and unfavorable effect on the outcome. On one hand it may reduce leukemia relapse but on the other hand it may increase transplant-related mortality.
Conditioning chemo regimens – most chemo regimens had negative effects of the BTM outcome. By, since the study group included only a small number of patients and these studies were conducted before the new chemo types/regimes using high-does etoposide, this factor may need to be reevaluated.
Donor-recipient sex match – This factor was found to be highly significant in female receiving donors from male-matched donors. These patients had higher risk of relapse and treatment failure. This was probably due to host sensitization to the H-Y antigens. This data is also needed to be handled with cautious due to the small number of patients.
Immune phenotype – Blood cell type and leukocyte levels at the beginning of the treatment is a another crucial factor. Higher leukocyte levels and non-T cell phenotype resulted in adverse outcome which led to remission.
Patient age – Age did not play a role when comparing the outcome after first relapse, but was found to be more favorable for younger ages (<16) when comparing the outcome after second relapse.
First relapse – a failure of first therapy override any other variable. The medical situation ( on/off chemo) at the time of a first relapse is highly important. If relapse occurred while OFF chemo, patients had better prognosis.
A recent study conducted by Wing Leung, M.D., Ph.D from St. Jude Children Hospital shows that that transplantation offers real hope of survival to patients with high-risk leukemia that is not curable with intensive chemotherapy. Bone marrow transplant survival more than doubled in recent years for young, high-risk leukemia patients who lacked genetically matched donors (5).
Five years after transplantation, survival was 65 percent for the 37 St. Jude patients with high-risk ALL treated at the hospital between 2000 and 2007, compared to 28 percent for the 57 St. Jude ALL patients who underwent treatment between 1991 and 1999. For AML patients, success rates grew from 34 % to 74%.
Dr. Leung explains that historically, transplant patients fared best and suffered fewer complications when the donors were relatives who carried the same six proteins on their white blood cells. Known as HLA proteins, they serve as markers to help the immune system distinguish between an individual’s healthy tissue and diseased cells that should be eliminated.
However, St. Jude investigators pioneered the use of haploidentical transplants (=partially genetically matched donors such as parents), demonstrating that careful matching of patients and donors and proper processing of the hematopoietic donor cells enhances the anti-cancer effect of transplantation without significantly increasing side effects.
The process involves careful testing and HLA screening of potential donors to identify the one whose immune system is likely to mount the most aggressive attack against remaining leukemia cells using specialized immune cells known as natural killer cells (5).
Dr. Leung further explains that the odds of finding a good haploidentical donor are 70 to 80 percent, compared to about a 25 percent chance of having a matched sibling donor, Leung said. The likelihood of finding a genetically identical, unrelated donor ranges from about 60 to 90 percent depending on the patient’s race or ethnicity.
Summary
Previous study have identified several factors that may affect the outcome of BMT in high-risk patients and included GVHD, blood count, chemo regimen prior to the transplantation, donor-sex matched and others. In a more recent study, however, the results indicated that all patients with very high-risk leukemia should be considered as candidates for HCT (Allogeneic hematopoietic cell transplantation) early in the course of diagnosis or relapse treatment, regardless of the availability of a matched donor or the intensity of prior chemotherapy. HLA typing, donor search, and transplant center referral should be performed as soon as possible. Patients with persistent minimal residual disease (MRD) or hematologic relapse while on therapy are also considered candidates for HCT in current protocols. There are several major differences between previous years study-analyses and this current one that needs to be taken into consideration before including or excluding each of them. [A]; 24% of the allogeneic HCTs in patients younger than 20 years worldwide were performed using cord blood grafts vs the previous bone marrow transplant procedure, [B] differences chemo-regimens between the previous and current years, [C] different transplant approaches evolved simultaneously, and therefore it is difficult to conduct retrospective analyses and [D] matching in HLA-C was not required for unrelated donor HCTs before 2008 in several institutes and therefore outcomes after contemporary 8 of 8 loci-matched transplantations may even be better than those favorable rates reported.
The data reported within is highly important and may increase patients survival rates and increased quality of lives. It is therefore necessary that different clinical-trial centers will re-evaluate current protocols and consider this new approach.
REFERENCES:
1. Acute Lymphoblastic Leukemia (ALL) and Nanotechnology. Author Tilda Barliya PhD
5. W. Leung, D. Campana, J. Yang, D. Pei, E. Coustan-Smith, K. Gan, J. E. Rubnitz, J. T. Sandlund, R. C. Ribeiro, A. Srinivasan, C. Hartford, B. M. Triplett, M. Dallas, A. Pillai, R. Handgretinger, J. H. Laver, C.-H. Pui. High success of hematopoietic cell transplantation regardless of donor source in children with very high-risk leukemia. Blood, 2011; DOI: 10.1182/blood-2011-01-333070
6. AJ Barrett, MM Horowitz, RP Gale, JC Biggs, BM Camitta, KA Dicke, E Gluckman, RA Good, RH Herzig, and MB Lee. Marrow transplantation for acute lymphoblastic leukemia: factors affecting relapse and survival. Blood August 1, 1989vol. 74 no. 2 862-871
7. FujiiH, Tradeau JD., Teachey DT., Fish JD., Grupp SA., Schlts KR and Reid GS. In vivo control of acute lymphoblastic leukemia by immunostimulatory CpG oligonucleotides. Blood 2007, 109: 2008-2013.
9. O. Ringde´n, M. Labopin, A. Bacigalupo, W. Arcese, U.W. Schaefer, R. Willem. Transplantation of Peripheral Blood Stem Cells as Compared With Bone Marrow From HLA-Identical Siblings in Adult Patients With Acute Myeloid Leukemia and Acute Lymphoblastic Leukemia. Journal of Clinical Oncology 2002, Vol 20, No 24 (December 15),: pp 4655-4664.
10. Bunin N, Carston M, Wall D, Adams R, Casper J, Kamani N, King R, and the National Marrow Donor Program Working Group. Unrelated marrow transplantation for children with acute lymphoblastic leukemia in second remission. Blood 2002, May 1, vol 99: 3151-3157. http://bloodjournal.hematologylibrary.org/content/99/9/3151.full.pdf+html
11. Mehmet Uzunel, Jonas Mattsson, Marie Jaksch, Mats Remberger, and Olle Ringde´n. The significance of graft-versus-host disease and pretransplantation minimal residual disease status to outcome after allogeneic stem cell transplantation in patients with acute lymphoblastic leukemia. Blood 2001 98: 1982-1985. http://bloodjournal.hematologylibrary.org/content/98/6/1982.full.pdf+html
12. Marina Cetkovic-Cvrlje, Bertram A. Roers, Barbara Waurzyniak, Xing-Ping Liu, and Fatih M. Uckun. Targeting Janus kinase 3 to attenuate the severity of acute graft-versus-host disease across the major histocompatibility barrier in mice. Blood 2001 98: 1607-1613. http://bloodjournal.hematologylibrary.org/content/98/5/1607.full.pdf+html
13. Kate A. Wheeler, Susan M. Richards, Clifford C. Bailey, Brenda Gibson, Ian M. Hann, Frank G. H. Hill, and Judith M. Chessells for the Medical Research Council Working Party on Childhood Leukaemia. Bone marrow transplantation versus chemotherapy in the treatment of very high–risk childhood acute lymphoblastic leukemia in first remission: results from Medical Research Council UKALL X and XI. Blood 2000 96: 2412-2418. http://bloodjournal.hematologylibrary.org/content/96/7/2412.full.pdf+html
14. O. Ringde´n, M. Remberger, T. Ruutu, J. Nikoskelainen, L. Volin, L. Vindeløv, T. Parkkali, S. Lenhoff, B. Sallerfors, L. Mellander, P. Ljungman, and N. Jacobsen, for the Nordic Bone Marrow Transplantation Group. Increased Risk of Chronic Graft-Versus-Host Disease, Obstructive Bronchiolitis, and Alopecia With Busulfan Versus Total Body Irradiation: Long-Term Results of a Randomized Trial in Allogeneic Marrow Recipients With Leukemia. 1999 93: 2196-2201. http://bloodjournal.hematologylibrary.org/content/93/7/2196.full.pdf+html
15. Christopher J.C. Knechtli, Nicholas J. Goulden, Jeremy P. Hancock, Victoria L.G. Grandage, Emma L. Harris, Russell J. Garland, Claire G. Jones, Anthony W. Rowbottom, Linda P. Hunt, Ann F. Green, Emer Clarke, Alan W. Lankester, Jacqueline M. Cornish, Derwood H. Pamphilon, Colin G. Steward, and Anthony Oakhill. Minimal Residual Disease Status Before Allogeneic Bone Marrow Transplantation Is an Important Determinant of Successful Outcome for Children and Adolescents With Acute Lymphoblastic Leukemia. Blood 1998 92: 4072-4079. http://bloodjournal.hematologylibrary.org/content/92/11/4072.full.pdf+html
16. Daniel J. Weisdorf, Amy L. Billett, Peter Hannan, Jerome Ritz, Stephen E. Sallan, Michael Steinbuch, and Norma K.C. Ramsay. Autologous Versus Unrelated Donor Allogeneic Marrow Transplantation for Acute Lymphoblastic Leukemia. Blood 1997 90: 2962-2968. http://bloodjournal.hematologylibrary.org/content/90/8/2962.full.pdf+html
Personalized Medicine: Clinical Aspiration of Microarrays
Reporter, Writer: Stephen J. Williams, Ph.D.
In this month’s Science, Mike May (at http://www.sciencemag.org/site/products/lst_20130215.xhtml) describes some of the challenges and successes in introducing microarray analysis to the clinical setting. Traditionally used for investigational research, microarray is now being developed, customized and used for biomarker analysis, prognostic and predictive value, in a disease-specific manner.
Challenges in data interpretation
In an interview with Seth Crosby, director of the Genome Technology Access Center at Washington University School of Medicine in St. Louis, “the biggest challenge” in moving microarray to the clinical setting is data interpretation. The current technology makes it possible to evaluate expression of thousands of genes from a patient’s sample however as Crosby describes is assigning clinical relevance to the data. For example Crosby explains that Washington University had validated a panel of 45 oncology genes by next generation sequencing and are using these genes to develop diagnostic tests to screen patient tumors for the purpose of determining a personalized therapeutic strategy. Seth Crosby noted it took “hundreds of Ph.D. and M.D. hours” to sift through the hundreds of papers to determine which genes were relevant to a specific cancer type. However, he notes, that once we better understand which changes in the patient’s genome are related to a specific disease we will be able to narrow down the list and be able to produce both economical and more disease-relevant microarrays.
Is this aberration pathogenic or not?
Microarrays are becoming an invaluable tool in cytogenetics, as eluded by Andy Last, executive vice president of the genetic analysis business unit atAffymetrix. Certain diseases like Down syndrome have well characterized chromosomal alterations like additions or deletions of parts or entire chromosomes. According to Affymetrix, the most common use of microarrays is for determining copy number variation. However according to James Clough, vice president of clinical and genomic services at Oxford Gene Technology, given the hundreds of syndromes associated with chromosomal rearrangements, the challenge will be to determine if a small chromosomal aberration has pathologic significance, given that microarray affords much higher diagnostic yield and speed of analysis than traditional microscopic techniques. To address this challenge, Oxford Gene Technologies, PerkinElmer, Affymetrix, and Agilent all have custom designed microarrays to evaluate disease specific copy number and SNP (single nucleotide polymorphism) microarrays. For example PerkinElmer designed OncoChip™ to evaluate copy number variation in more than 1.800 cancer genes. Agilent makes microarrays that evaluates both copy number variation such as its CGH (comparative genomic hybridization) plus SNP microarrays. Patricia Barco, product manager for cytogenetics at Agilent, notes these arrays can be used in prenatal and postnatal research and cancer, and “can be customized from more than 28 million probes in our library”.
Custom Tools and Software to Handle the Onslaught of Big Data
There is a need for FDA approved diagnostic tools based on microarrays. Pathwork Diagnostic’s has one such tool (the Pathwork Tissue of Origin test), which uses 2,000 transcript markers and a proprietary computational algorithm to determine from expression analysis, the tissue of origin of a patient’s tumor. Pathwork also provides a fast, custom turn-around analytical service for pathologists who encounter difficult to interpret samples. Illumina provides the Infinium HumanCore BeadChip family of microarrays, which can determine genetic variations for purposes of biological tissue banking. This system uses a set of over 300,000 SNP probes plus 240,000 exome-based markers.
Tools have also been developed to validate microarray results. A common validation strategy is the use of quantitative real-time PCR to verify the expression changes seen on the microarray. Life Technologies developed the TaqMan OpenArray Real Time PCR plates, which have 3,072 wells and can be custom-formatted using their library of eight million validated TaqMan assays.
Making Sense of the Big Data: Bridging the Knowledge Gap using Bioinformatics
The use of microarray has spurned industries devoted to developing the bioinformatics software to analyze the massive amounts of data and provide clinical significance. For example companies such as Expression Analysis use their bioinformatics software to provide pathway analysis for microarray data in order to translate the data into the biology. Using such strategies can also validate the design of microarrays for various diseases.
Foundation Medicine, Inc., a molecular information company, provides cancer genomics test solutions. It offers FoundationOne, an informative genomic profile to identify a patient’s individual molecular alterations and match them with relevant targeted therapies and clinical trials. The company’s product enables physicians to recommend treatment options for patients based on the molecular subtype of their cancer.
Cancer research has rapidly embraced high throughput technologies into its research, using various microarray, tissue array, and next generation sequencing platforms. The result has been a rapid increase in cancer data output and data types. Now more than ever, having the bioinformatic skills and knowledge of available bioinformatic resources specific to cancer is critical. The CBW will host a 5-day workshop covering the key bioinformatics concepts and tools required to analyze cancer genomic data sets. Participants will gain experience in genomic data visualization tools which will be applied throughout the development of the skills required to analyze cancer -omic data for gene expression, genome rearrangement, somatic mutations and copy number variation. The workshop will conclude with analyzing and conducting pathway analysis on the resultant cancer gene list and integration of clinical data.
Successful Examples of Clinical Ventures Integrating Bioinformatics in Cancer Treatment Decision –Making
The University of Pavia, Italy developed a fully integrated oncology bioinformatics workflow as described on their website and at the ESMO 2012 Congress meeting:
ONCO-I2B2 PROJECT: A BIOINFORMATICS TOOL INTEGRATING –OMICS AND CLINICAL DATA TO SUPPORT TRANSLATIONAL RESEARCH
Abstract:
2530
Congress:
ESMO 2012
Type:
Abstract
Topic:
Translational research
Authors:
A. Zambelli, D. Segagni, V. Tibollo, A. Dagliati, A. Malovini, V. Fotia, S. Manera, R. Bellazzi; Pavia/IT
Body
The ONCO-i2b2 project, supported by the University of Pavia and the Fondazione Salvatore Maugeri (FSM), aims at supporting translational research in oncology and exploits the software solutions implemented by the Informatics for Integrating Biology and the Bedside (i2b2) research centre, an initiative funded by the NIH Roadmap National Centres for Biomedical Computing. The ONCO-i2b2 software is designed to integrate the i2b2 infrastructure with the FSM hospital information system and the Bruno Boerci Biobank, in order to provide well-characterized cancer specimens along with an accurate patients clinical data-base. The i2b2 infrastructure provides a web-based access to all the electronic medical records of cancer patients, and allow researchers analyzing the vast amount of biological and clinical information, relying on a user-friendly interface. Data coming from multiple sources are integrated and jointly queried.
In 2011 at AIOM Meeting we reported the preliminary experience of the ONCO-i2b2 project, now we’re able to present the up and running platform and the extended data set. Currently, more than 4400 specimens are stored and more than 600 of breast cancer patients give the consent for the use of specimens in the context of clinical research, in addition, more than 5000 histological reports are stored in order to integrate clinical data.
Within the ONCO-i2b2 project is possible to query and merge data regarding:
• Anonymous patient personal data;
• Diagnosis and therapy ICD9-CM subset from the hospital information system;
• Histological data (tumour SNOMED and TNM codes) and receptor profile testing (Her2, Ki67) from anatomic pathology database;
• Specimen molecular characteristics (DNA, RNA, blood, plasma and cancer tissues) from the Bruno Boerci Biobank management system.
The research infrastructure will be completed by the development of new set of components designed to enhance the ability of an i2b2 hive to utilize data generated by NGS technology, providing a mechanism to apply custom genomic annotations. The translational tool created at FSM is a concrete example regarding how the integration of different information from heterogeneous sources could bring scientific research closer to understand the nature of disease itself and to create novel diagnostics through handy interfaces.
Disclosure
All authors have declared no conflicts of interest.
Cancer Bioinformatics: Recovery Act Investment Report
November 2009
Public Health Burden of Cancer
Cancer is the second leading cause of death in the United States after heart disease. In 2009, it is estimated that nearly 1.5 million new cases of invasive cancer will be diagnosed in this country and more than 560,000 people will die of the disease.
Over the past five years, NCI’s Center for Biomedical Informatics and Information Technology (CBIIT) has led the effort to develop and deploy the cancer Biomedical Informatics Grid® (caBIG) in partnership with the broader cancer community. The caBIG network is designed to enable the integration and exchange of data among researchers in the laboratory and the clinic, simplify collaboration, and realize the potential of information-based (personalized) medicine in improving patient outcomes. caBIG has connected major components of the cancer community, including NCI-designated Cancer Centers, participating institutions of the NCI Community Cancer Centers Program (NCCCP), and numerous large-scale scientific endeavors, as well as basic, translational, and clinical researchers at public and private institutions across the United States and around the world. Beyond cancer research, caBIG capabilities—infrastructure, standards, and tools—provide a prototype for linking other disease communities and catalyzing a new 21st-century biomedical ecosystem that unifies research and care. ARRA funding will allow NCI to accelerate the ongoing development of the Cancer Knowledge Cloud and Oncology Electronic Health Records (EHRs) initiatives, thereby providing for continued job creation in the areas of biomedical informatics development and application as well as healthcare delivery.
The caBIG Cancer Knowledge Cloud: Extending the Research Infrastructure
The Cancer Knowledge Cloud is a virtual biomedical capability that utilizes caBIG tools, infrastructure, and security frameworks to integrate distributed individual and organizational data, software applications, and computational capacity throughout the broad cancer research and treatment community. The Cancer Knowledge Cloud connects, integrates, and facilitates sharing of the diverse primary data generated through basic and clinical research and care delivery to enable personalized medicine. The cloud includes information generated through large-scale research projects such as The Cancer Genome Atlas (TCGA), the cancer Human Biobank (caHUB) tissue acquisition network, the NCI Functional Biology Consortium, the NCI Patient Characterization Center, and the NCI Preclinical Development Pipeline, academic and industry counterparts to these projects, and clinical observations (from entities such as the NCCCP) captured in oncology-extended Electronic Health Records. Through the use of the caBIG Data Sharing and Security Framework, the Cloud will support appropriate sharing of information, supporting in silico hypothesis generation and testing, and enabling a learning healthcare system.
A caBIG-Based Rapid-Learning Healthcare System: Incorporating Oncology-Extended Electronic Healthcare Records (EHRs)
The 21st-century Cancer Knowledge Cloud will connect individuals, organizations, institutions, and their associated information within an information technology-enabled cycle of discovery, development, and clinical care—the paradigm of a rapid-learning healthcare system. This will transform these disconnected sectors into a system that is personalized, preventive, pre-emptive, and patient-participatory. To be realized, this model requires the adoption of standards-based EHRs. Presently, however, no certified oncology-based EHR exists, and fewer than 3 percent of oncologists with outpatient-based practices utilize EHRs. caBIG has recently established a collaboration with the American Society of Clinical Oncology (ASCO) to develop an oncology-specific EHR (caEHR) specification based on open standards already in use in the oncology community that will utilize caBIG standards for interoperability. NCI will implement an open-source version of this specification to validate the specification and to provide a free alternative to sites that choose not to purchase a commercial system. The launch customer for the caEHR will be NCCCP participating sites. NCI will work with appropriate entities to provide a mechanism for certifying that caEHR implementations are consistent with the NCI/ASCO specification.
Bards Cancer Institute has another clinical bioinformatics program to support their clinical efforts:
Clinical Bioinformatics Program in Oncology at Barts Cancer Institute at Barts and the London School of Medicine
Bioinformatics is a new interdisciplinary area involving biological, statistical and computational sciences. Bioinformatics will enable cancer researchers not only to manage, analyze, mine and understand the currently accumulated, valuable, high-throughput data, but also to integrate these in their current research programs. The need for bioinformatics will become ever more important as new technologies increase the already exponential rate at which cancer data are generated.
What we do
We work alongside clinical and basic scientists to support the cancer projects within BCI. This is an ideal partnership between scientific experts, who know the research questions that will be relevant from a cancer biologist or clinician’s perspective, and bioinformatics experts, who know how to develop the proposed methods to provide answers.
We also conduct independent bioinformatics research, focusing on the development of computational and integrative methods, algorithms, databases and tools to tackle the analysis of the high volumes of cancer data.
We also are actively involved in the development of bioinformatics educational courses at BCI. Our courses offer a unique opportunity for biologists to gain a basic understanding in the use of bioinformatics methods to access and harness large complicated high-throughput data and uncover meaningful information that could be used to understand molecular mechanisms and develop novel targeted therapeutics/diagnostic tools.
Developing Criteria for Genomic Profiling in Lung Cancer:
A Report from U.S. Cancer Centers
In a report by Pao et. al., a group of clinicians organized a meeting to standardize some protocols for the integration of microarray and genomic data from lung cancer patients into the clinical setting.[1] There has been ample evidence that adenocarcinomas could be classified into “clinically relevant molecular subsets” based on distinct genomic changes. For example EGFR (epidermal growth factor receptor) exon 19 deletions and exon 21 point mutations predict sensitivity to tyrosine kinase inhibitors (TKIs) like gefitinib, whereas exon 20 insertions predict primary resistance[2].
However, as the authors note, “mutational profiling has not been widely accepted or adopted into practice in thoracic oncology”.
Therefore, a multi-institutional workshop was held in 2009 among participants from Massachusetts General Hospital (MGH) Cancer Center, Memorial Sloan-Kettering Cancer Center (MSKCC), the Dana-Farber/Bingham & Women’s Cancer Center (DF/BWCC), the M.D. Anderson Cancer Center (VICC), and the Vanderbilt-Ingram Cancer Center (VICC) to discuss their institutes molecular profiling programs with emphasis on:
·Organization/workflow
·Mutation detection technologies
·Clinical protocols and reporting
·Patient consent
In addition to the aforementioned challenges, the panel discussed further issues for developing improved science-driven criteria for determining targeted therapies including:
1)Including pathologists into criteria development as pathology departments are usually the main repositories for specimens
2)Developing integrated informatics systems
3)Standardizing new target validation methodology across cancer centers
AMPK Is a Negative Regulator of the Warburg Effect and Suppresses Tumor Growth In Vivo
Reporter-Curator: Stephen J. Williams, Ph.D.
Word Cloud by Daniel Menzin
There has been a causal link between alterations in cellular metabolism and the cancer phenotype. Reorganization of cellular metabolism, marked by a shift from oxidative phosphorylation to aerobic glycolysis for cellular energy requirements (Warburg effect), is considered a hallmark of the transformed cell. In addition, if tumors are to survive and grow, cancer cells need to adapt to environments high in metabolic stress and to avoid programmed cell death (apoptosis). Recently, a link between cancer growth and metabolism has been supported by the discovery that the LKB1/AMPK signaling pathway as a tumor suppressor axis[1].
LKB1/AMPK/mTOR Signaling Pathway
The Liver Kinase B1 (LKB1)/AMPK AMP-activated protein kinase/mammalian Target of Rapamycin Complex 1 (mTORC1) signaling pathway links cellular metabolism and energy status to pathways involved in cell growth, proliferation, adaption to energy stress, and autophagy. LKB1 is a master control for 14 other kinases including AMPK, a serine-threonine kinase which senses cellular AMP/ATP ratios. In response to cellular starvation, AMPK is allosterically activated by AMP, leading to activation of ATP-generating pathways like fatty acid oxidation and blocking anabolic pathways, like lipid and cholesterol synthesis (which consume ATP). In addition, AMPK regulates cell growth, proliferation, and autophagy by regulating the mTOR pathway. AMPK activates the tuberous sclerosis complex 1/2, which ultimately inhibits mTORC1 activity and inhibits protein translation. This mTOR activity is dis-regulated in many cancers.
LKB1/AMPK in Cancer
Somatic mutations of the STK11 gene encoding LKB1 are detected in lung and cervical cancers
Therefore LKB1 may be a strong tumor suppressor
Pharmacologic activation of LKB1/AMPK with metformin can suppress cancer cell growth
In a recent Cell Metabolism paper[2], Brandon Faubert and colleagues describe how AMPK activity reduces aerobic glycolysis and tumor proliferation while loss of AMPK activity promotes tumor proliferation by shifting cells to aerobic glycolysis and increasing anabolic pathways in a HIF1-dependent manner.
The paper’s major findings were as follows:
Loss of AMPKα1 cooperates with the Myc oncogene to accelerate lymphomagenesis
Inhibiting HIF-1α reverses the metabolic effects of AMPKα loss
HIF-1α mediates the growth advantage of tumors with reduced AMPK signaling
Summary
AMPK is a metabolic sensor that helps maintain cellular energy homeostasis. Despite evidence linking AMPK with tumor suppressor functions, the role of AMPK in tumorigenesis and tumor metabolism is unknown. Here we show that AMPK negatively regulates aerobic glycolysis (the Warburg effect) in cancer cells and suppresses tumor growth in vivo. Genetic ablation of the α1 catalytic subunit of AMPK accelerates Myc-induced lymphomagenesis. Inactivation of AMPKα in both transformed and nontransformed cells promotes a metabolic shift to aerobic glycolysis, increased allocation of glucose carbon into lipids, and biomass accumulation. These metabolic effects require normoxic stabilization of the hypoxia-inducible factor-1α (HIF-1α), as silencing HIF-1α reverses the shift to aerobic glycolysis and the biosynthetic and proliferative advantages conferred by reduced AMPKα signaling. Together our findings suggest that AMPK activity opposes tumor development and that its loss fosters tumor progression in part by regulating cellular metabolic pathways that support cell growth and proliferation.
Below is the graphical abstract of this paper.
(Photo credit reference(2; Faubert et. al) permission from Elsevier)
However, this regulation of tumor promotion by AMPK may be more complicated and dependent on the cellular environment.
Nissam Hay from the University of Illinois College of Medicine, Chicago, Illinois, USA and his co-workers Sang-Min Jeon and Navdeep Chandel were investigating the mechanism through which LKB1/AMPK regulate the balance between cancer cell growth and apoptosis under energy stress[3]. In their system, the loss of function of either of these proteins makes cells more sensitive to apoptosis in low glucose environments, and cells deficient in either AMPK or LKB1 were shown to be resistant to oncogenic transformation. Whereas previous studies showed (as above) AMPK opposes tumor proliferation in a HIF1-dependent manner, their results showed AMPK could promote tumor cell survival during periods of low glucose or altered redox status.
The researchers incubated LKB1-deficient cancer cells in the presence of either glucose or one of the non-metabolizable glucose analogues 2-deoxyglucose (2DG) and 5-thioglucose (5TG), and found that 2DG, but not 5TG, induced the activation of AMPK and protected the cells from apoptosis, even in cells that were deficient in LKB1.
The authors demonstrated that glucose deprivation depleted NADPH levels, increased H2O2 levels and increased cell death, and that this was accelerated in cells deficient in the enzyme glucose-6-phosphate dehydrogenase. Anti-oxidants were also found to inhibit cell death in cells deficient in either AMPK or LKB1.
Knockdown or knockout of either LKB1 or AMPK in cancer cells significantly increased levels of H2O2 but not of peroxide (O2–) during glucose depletion. The glucose analogue 2DG was able to activate AMPK and maintain high levels of NADPH and low levels of H2O2 in these cells.
The nucleotide coenzyme NADPH is generated in the pentose phosphate pathway and mitochondrial metabolism, and consumed in H2O2 elimination and fatty acid synthesis. If glucose is limited mitochondrial metabolism becomes the major source of NADPH, supported by fatty acid oxidation. AMPK is known to be a regulator of fatty acid metabolism through inhibition of two acetyl-CoA carboxylases, ACC1 and ACC2.
Short interfering RNAs (siRNAs) to knock down levels of both ACC1 and ACC2 in A549 cancer cells and found that only ACC2 knockdown significantly increased peroxide accumulation and apoptosis, while over-expression of mutant ACC1 and ACC2 in LKB1-proficient cells increased H2O2 and apoptosis.
Therefore, it was concluded AMPK acts to promote early tumor growth and prevent apoptosis in conditions of energy stress through inhibiting acetyl-CoA carboxylase activity, thus maintaining NADPH levels and preventing the build-up of peroxide in glucose-deficient conditions.
This may appear to be conflicting with the previous report in this post however, it is possible that these reports reflect differences in the way cells respond to various cellular stresses, be it hypoxia, glucose deprivation, or changes in redox status. Therefore a complex situation may arise:
AMPK promotes tumor progression under glucose starvation
AMPK can oppose tumor proliferation under a normoxic, HIF1-dependent manner
Could AMPK regulation be different in cancer stem cells vs. non-stem cell?
References:
1. Green AS, Chapuis N, Lacombe C, Mayeux P, Bouscary D, Tamburini J: LKB1/AMPK/mTOR signaling pathway in hematological malignancies: from metabolism to cancer cell biology. Cell Cycle 2011, 10(13):2115-2120.
2. Faubert B, Boily G, Izreig S, Griss T, Samborska B, Dong Z, Dupuy F, Chambers C, Fuerth BJ, Viollet B et al: AMPK is a negative regulator of the Warburg effect and suppresses tumor growth in vivo. Cell metabolism 2013, 17(1):113-124.
3. Jeon SM, Chandel NS, Hay N: AMPK regulates NADPH homeostasis to promote tumour cell survival during energy stress. Nature 2012, 485(7400):661-665.
Other posts on this site related to Warburg Effect and Cancer include:
In the last post of Melanoma titled “In focus: Melanoma Genetics”, I discussed the clinical characteristics and the genetics involved in Melanoma. This post would discuss melanoma therapeutics, both current and novel.
According to the American Cancer Society, more than 76,000 new cases and more than 9100 deaths from melanoma were reported in the United States in 2012[1] Melanoma develops from the malignant transformation of melanocytes, the pigment-producing cells that reside in the basal epidermal layer in human skin. Although most melanomas arise in the skin, they may also arise from mucosal surfaces or at other sites to which neural crest cells migrate.
Melanoma therapeutics
Surgical treatment of cutaneous melanoma employs specific surgical margins depending on the depth of invasion of the tumor and there are specific surgical treatment guidelines of primary, nodal, and metastatic melanoma that surgeons adhere to while treatment. Melanoma researchers have been focusing on developing adjuvant therapies for that would increase the survival post-surgery.
Chemotherapy
Among traditional chemotherapeutic agents, only dacarbazine is FDA approved for the treatment of advanced melanoma (Eggermont AM and Kirkwood JM, Eur J Cancer, Aug 2004;40(12):1825-36). Dacarbazine is a triazene derivative and alkylates and cross-links DNA during all phases of the cell cycle, resulting in disruption of DNA function, cell cycle arrest, and apoptosis. Currently, 17 clinical trials are underway to test the efficacy and effectiveness of dacarbazine against melanoma as either a single agent or in combination chemotherapy regimens with other anti-cancer chemotherapeutic agents such as cisplatin, paclitaxel. Temozolomide is a triazene analog of dacarbazine and is approved for the treatment of malignant gliomas. At physiologic pH, it is converted to a short-lived active cytotoxic compound, monomethyl triazeno imidazole carboxamide (MTIC). MTIC methylates DNA at the O6 and N7 positions of guanine, resulting in inhibition of DNA replication. Unlike dacarbazine, which is metabolized to MITC only in the liver, temozolomide is metabolized to MITC at all sites. Temozolomide is administered orally and penetrates well into the central nervous system. Temozolomide is being tested in many combination regimens for patients with melanoma metastatic to the brain (Douglas JG and Margolin K, Semin Oncol, Oct 2002;29(5):518-24).
Immunotherapy
Melanoma and the immune system are closely related. Hence, immunotherapy has been explored in the treatment of the disease. The two most widely investigated immunotherapy drugs for melanoma are Interferon (IFN)-alpha and Interleukin-2 (IL-2).
The role of IFNalpha-2b in the adjuvant therapy of patients with localized melanoma at high risk for relapse was established by the results of three large randomized trials conducted by the US Intergroup; all three trials demonstrated an improvement in relapse-free survival and two in overall survival. One of these trials, a large randomized multicenter trial performed by the Eastern Cooperative Oncology Group (ECOG), in high-risk melanoma patients showed significant improvements in relapse-free and overall survival with adjuvant IFN-α-2b therapy, compared with standard observation (ECOG 1684). The results of the study led to FDA approval of IFN-α-2b for treatment of melanoma. This study was performed on patients with deep primary tumors without lymph node involvement and node-positive melanomas. In other studies, little antitumor activity has been demonstrated in IFN-α-2b–treated metastatic stage IV melanoma.
Recombinant IL-2 showed an overall response rate of 15-20% in metastatic melanoma and was capable of producing complete and durable remissions in about 6% of patients treated. Based upon these data, the US FDA has approved the use of high-dose IL-2 for the therapy of patients with metastatic melanoma. Aldesleukin (Brand name: Proleukin) is a recombinant analog of the endogenous cytokine interleukin-2 (IL-2). It binds to and activates the IL-2 receptor (IL-2R), followed by heterodimerization of the IL-2R beta and gamma(c) cytoplasmic chains; activation of Jak3; and phosphorylation of tyrosine residues on the IL-2R beta chain, resulting in an activated receptor complex (NCI). The activated complex recruits several signaling molecules that act as substrates for regulatory enzymes associated with the complex. It is administered intravenously and stimulates lymphokine-activating killer (LAK) cells, natural killer (NK) cells and the production of cytokines such as gamma interferon (nm|OK). Several clinical trials are currently underway using Aldesleukin to determine the efficacy of combination treatment in melanoma patients.
Another anti-cancer immunotherapeuty-based mechanism involved inhibition of inhibitory signal of cytotoxic T lymphocyte-associated antigen 4 (CTLA-4), a molecule on T-cells that plays a critical role in regulating natural immune responses. Ipilimumab (Brand name: Yervoy) was by FDA for melanoma treatment. It is a human monoclonal antibody (MAb) T-cell potentiator that specifically blocks CTLA-4. It is approved for inoperable advanced (Stage III) or metastatic (Stage IV) melanoma in newly diagnosed or previously treated patients (nm|OK). The approval, March 25, 2011, was based on a randomized (3:1:1) double-blind double-dummy clinical trial (MDX010-20) in patients with unresectable or metastatic melanoma who had received at least one prior systemic treatment for melanoma. Patients were randomly assigned to receive either ipilimumab, 3 mg/kg intravenously, in combination with the tumor vaccine (n=403); ipilimumab plus vaccine placebo (n=137); or tumor vaccine with placebo (n=136). Patients treated with ipilimumab alone had a median overall survival (OS) of 10 months while those treated with tumor vaccine had a median OS of 6 months. The trial also demonstrated a statistically significant improvement in OS for patients treated with the combination of ipilimumab plus tumor vaccine compared with patients treated with tumor vaccine alone. For more information on the trial, check the clinical trials website, www.clinicaltrials.gov
Signaling pathway inhibitors
Approximately 90% of BRAF gene mutations involve valine (V) to glutamic acid (E) mutation at number 600 residue (V600E). The resulting oncogene product, BRAF (V600E) kinase is highly active and exhibits elevated MAPK pathway. The BRAF(V600E) gene mutation occurs in approximately 60% of melanomas indicating that it could be therapeutically relevant.Vemurafenib (Brand name: Zelboraf) is a novel small-molecule inhibitor of BRAF (V600E) kinase. It selectively binds to the ATP-binding site and inhibits the activity of BRAF (V600E) kinase. Vemurafebib inhibits over active MAPK pathway by inhibiting the mutated BRAF kinase, thereby reducing tumor cell proliferation (NCI). Encouraging results of phase III randomized, open-label, multicenter trial were reported recently at the 2011 ASCO meeting (Chapman PB, et al, ASCO 2011, Abstract LBA4). The trial compared the novel BRAF inhibitor vemurafenib with dacarbazine in patients with BRAF-mutated melanoma. Previously untreated, unresectable stage IIIC or stage IV melanoma that tested positive for BRAF mutation were randomized (1:1) to vemurafenib or dacarbazine. The response rate (RR) was significantly high (48.4%) in vemurafenib treated patients as compared to 5.5% in dacarbazine among the 65% of patients evaluable for RR to date. In addition, vemurafenib was associated with significantly improved OS and PFS compared to dacarbazine in patients with previously untreated BRAF (V600E) mutation bearing patients with metastatic melanoma.
Biochemotherapy
Biochemothreapy combine traditional chemotherapy with immunotherapies, such as IL-2 and IFN-α-2b. These combination therapies seemed promising in phase II trials, however, seven large studies failed to show statistically significant increased overall survival rates for various biochemotherapy regimens in patients with stage IV metastasis (Margolin KA, et al, Cancer, 1 Aug 2004;101(3):435-8). Owing to inconsistent results of the available studies with regard to benefit including RR, OS and progression time, and consistently high toxicity rates, clinical practice guideline do not recommend biochemotherapy for the treatment of metastatic melanoma (Verma S, et al, Curr Oncol, April 2008; 15(2): 85–89).
Vaccines
The use of therapeutic vaccines is an ongoing area of research, and clinical trials of several types of vaccines (whole cell, carbohydrate, peptide) are being conducted in patients with intermediate and late-stage melanoma. Vaccines are also being tested in patients with metastatic melanoma to determine their immune effects and to define their activity in combination with other immunotherapeutic agents such as IL-2 or IFNalpha (Agarwala S, Am J Clin Dermatol, 2003;4(5):333-46). In fact, recently investigators at the Indiana University Health Goshen Center for Cancer Care (Goshen, IN) conducted a randomized, multicenter phase III trial involving 185 patients with stage IV or locally advanced stage III cutaneous melanoma. The patients were assigned into treatment groups with IL-2 alone or with vaccine (gp100) followed by IL-2. The vaccine-IL-2 group had a significantly improved OR as compared to the IL-2-only group (16% Vs. 6%) and longer progression free survival (2.2 months Vs. 1.6 months). The median overall survival was also longer in the vaccine-interleukin-2 group than in the interleukin-2-only group (17.8 months Vs. 11.1 months). Thus, a combination of vaccine and immunotherapy showed a better response rate and longer progression-free survival than with interleukin-2 alone in patients with advanced melanoma (Schwartzentruber DJ, et al, N Engl J Med, 2 Jun 2011;364(22):2119-27).
Which Treatment When?
Earlier, there were essentially two main options for patients suffering from advanced melanoma, dacarbazine and IL-2. Dacarbazine, a chemotherapeutic agent produces modest improvements in survival or symptomatic benefits in most patients. Interleukin-2 -based drugs, on the other hand, induce long-term remissions in a small group of patients but are highly toxic. Recently, FDA approved ipilimumab and vemurafenib for patients with metastatic melanoma. Apart from these, therapies are also aiming at starving the tumor by inhibiting angiogenesis or depleting nutrients essential for cancer growth. Of the antiangiogenic compounds, VEGFR inhibitors SU5416 and AG-013736 demonstrated broad-spectrum antitumor activity in mice bearing xenografts of human cancer cell lines originating from various tissues, including melanoma. In addition, several trials are currently underway to test the efficacy of the drugs in combination. In the future, personalized medicine-based recommendations of novel and existing drugs for melanoma patients might be the way to go.
NEW YORK (Reuters) – Michael Weitz was out of options. The Californian had endured chemotherapy, radiation and surgery but his lung cancer still spread to his bones and brain. He was entered into a Phase I study – the earliest stage of human testing for a new medicine – of crizotinib. The drug works for about 4 percent of advanced lung cancer patients with a mutated form of a protein called ALK.
Weitz, now 55, is cancer-free after three years of taking the drug now sold by Pfizer as Xalkori after an unusually swift development process.
It typically has taken a decade and $1 billion to bring a new treatment to market. But in the last two years a handful of cancer drugs – including Onyx Pharmaceutical Inc’s Kyprolis for multiple myeloma, Roche’s Zelboraf for melanoma, and Pfizer’s Xalkori – were approved in about half that time because of improved genetic screening, more definitive Phase I trials and the dire need for new, effective treatments.
“We hope to be able to shave years off the time it takes to get final approval and save hundreds of millions of dollars per drug,” said Robert Schneider, director of translational cancer research at New York University Cancer Institute.
Smoking lung cancer (Photo credit: Wikipedia)
High rates of lung cancer (indicated in this map by brown colors) are highly correlated with the Stroke Belt. (Photo credit: Wikipedia)
‘Triple negative breast cancer’ or TNBC, as the name suggests, is a classification of breast cancers lacking the expression of estrogen receptor (ER) and progesterone receptor expression as well as amplification of the human epidermal growth factor receptor 2 (HER2).
Unlike other breast cancer types, treating TNBC is a challenge mainly because of the absence of well-defined molecular targets and because of disease heterogeneity. Currently, neoadjuvant chemotherapies are in use to treat TNBC patients. Some, around 30%, patients respond completely to neoadjuvant chemotherapy and have good outcomes after surgery. However, if there is a residual disease after therapy, outcomes are poor.
Therefore, current focus of the field is to first understand the complexity of the disease, both at genomic and molecular level and look for targets. Also, several combination chemotherapies are currently under trial to determine the efficacy, overall response rate, progression-free survival and other relevant factors for patients suffering with different forms of TNBC.
Recently, in the San Antonio Breast Cancer Symposium (SABCS 2012), several abstarcts related to TNBC research, both clinical and pre-clinical. Here is a compilation of some of the abstracts and their relevance in the field of TNBC research:
Triple Negative Breast Cancer: Subtypes, Molecular Targets, and Therapeutic Approaches, Pietenpol JA, Vanderbilt-Ingram Cancer Center; Vanderbilt University School of Medicine (Nashville, TN), Abstract no. ES2-2.
In order to better understand the complexity of TNBC, an integrative and comprehensive genomic and molecular analysis is required. The analysis would give important cues to developing and administering effective therapeutic agents. The group has compiled an extensive number of TNBC gene expression profiles and initiated molecular subtyping of the disease. Differential GE was used to designate 25 TNBC cell line models representative of the following subtypes:
two basel-like TNBC subtypes with cell cycle and DDR gene expression signatures (BL1 and BL2);
two mesenchymal subtypes with high expression of genes involved in differentiation and growth factor pathways (M and MSL);
an immunomodulatory (IM) type;
a luminal subtype driven by androgen signaling (LAR)
The pharmacological drugs were chosen on the basis of the genetic pathways active in the cell lines with the abovementioned TNBC subtypes. It was observed that BL1 and BL2 subtype cell lines respond to cisplatin. Mesenchymal, basal, and luminal subtype lines with aberrations in PI3K signaling and have the greatest sensitivity to PI3K inhibitors.
The LAR subtype cell lines express AR and are uniquely sensitive to bicalutamide (AR antagonist). The experiment was a proof-of-concept that the best therapy could be based on TNBC subtypes.
The group has also developed a web-based subtyping tool referred to as “TNBCtype,” for candidate TNBC tumor samples using our gene expression metadata and classification methods. The approach would enable alignment of TNBC patients to appropriate targeted therapies.
The Clonal and Mutational Composition of Triple Negative Breast Cancers: Aparicio S, University of British Columbia (Vancouver, BC), Canada. Abstract no. ES2-3.
The abstract is on the same lines, TNBC heterogeneity that is. The concept of clonal heterogeneity in cancers, the spatial and temporal variation in clonal composition, is the focal point of the discussion. The group has developed next generation sequencing approaches and applied them to the understanding of mutational and clonal composition of primary TNBC. They have demonstrated that both mutational composition and clonal structure of primary TNBC is in fact a complete spectrum, a notion that is far from the previous one that stated TNBC to be a distinct disease. The authors add “clonal analysis suggests a means by which the genetic complexity might be reduced by following patient evolution over time and space.” The specific implications of the mutational and transcriptome landscapes of TNBC in relation to possible disease biologies were discussed in the symposium.
Profiling of triple-negative breast cancers after neoadjuvant chemotherapy identifies targetable molecular alterations in the treatment-refractory residual disease:
Balko JM, etal, Vanderbilt University (Nashville, TN); Foundation Medicine, (Cambridge, MA); Instituto Nacional de Enfermedades Neoplásicas, Lima, Peru
In the absence of hormone receptors and hence lack of targets, Neoadjuvant chemotherapy (NAC) is increasingly used in patients with TNBC. NAC can induce a pathologic complete response (pCR) in ∼30% of patients which portends a favorable prognosis. In contrast, patients with residual disease (RD) in the breast at surgical resection exhibit worse outcomes. The authors hypothesize that “profiling residual TNBC after NAC would identify molecularly targetable lesions in the chemotherapy resistant component of the tumor and that the persistent tumor cells would mirror micro-metastases which ultimately recur in such patients.” The researchers utilized targeted next generation sequencing (NGS) for 182 oncogenes and tumor suppressors in a CLIA certified lab (Foundation Medicine, Cambridge, MA) and gene expression profiling (NanoString) of the RD after NAC in 102 patients with TNBC. The RD was stained for Ki67, which has been reported to predict outcome after NAC in unselected breast cancers. Out of the 89 evaluable post-NAC tumors, 57 (64%) were basal-like; 19% HER2-enriched; 6% luminal A; 6% luminal B and 5% normal-like. Of 81 tumors evaluated by NGS, 89% demonstrated mutations in TP53, 27% were MCL1-amplified, and 21% were MYC-amplified.
Several pathways were found to be altered:
PI3K/mTOR pathway (AKT1-3, PIK3CA, PIK3R1, RAPTOR, PTEN, and TSC1)
Cell cycle genes (amplifications of CDK2, CDK4, and CDK6, CCND1-3, and CCNE1); loss of RB
DNA repair pathway (BRCA1/2, ATM)
Ras/MAPK pathway (KRAS, RAF1, NF1)
Sporadic growth factor receptor (amplifications occurred in EGFR, KIT, PDGFRA, PDGFRB, MET, FGFR1, FGFR2, and IGF1R.
NGS identified 7 patients with ERBB2 gene amplification. NGS could assist in the identification of ERBB2-overexpressing tumors misclassified at the time of diagnosis.
Amplifications of MYC were independently associated with poor recurrence-free survival (RFS) and overall survival (OS). In contrast to the earlier notion, high post-NAC Ki67 score did not predict poor RFS or OS in this predominantly TNBC cohort.
The authors concluded that “the diversity of lesions in residual TNBCs after NAC underscores the need for powerful and broad molecular approaches to identify actionable molecular alterations and, in turn, better inform personalized therapy of this aggressive disease.”
Identification of Novel Synthetic-Lethal Targets for MYC-Driven Triple-Negative Breast Cancer: Goga A, etal, UCSF (San Francisco, CA), Abstract No. S3-8
Reiterating the greatest challenge of the TNBC treatment, no targeted agents currently exist against TNBC. The group at UCSF has discovered that TNBC frequently express high levels of the MYC proto-oncogene. The discovery has led them to identify new “synthetic-lethal” strategies to selectively kill TNBC with MYC overexpression. “Synthetic lethality arises when a combination of mutations in two or more genes leads to cell death, whereas a mutation in only one of these genes has little effect. Using this strategy, we can take advantage of the elevated MYC signaling in TNBC to selectively kill them, while sparing normal tissues in which MYC is expressed at much lower levels”
The researchers performed a shRNA synthetic-lethal screen in the human mammary epithelial cells (HMEC), to identify new molecules, such as cell cycle kinases, which when inhibited can preferentially kill TNBC cells. A high-throughput screen of ∼2000 shRNAs, that target the human kinome (∼ 600 kinases) when performed, led to the identification of 13 kinases whose inhibition by >1 shRNAs gave rise to >50% inhibition of cell growth. ARK5 and GSK3A were the two other kinases that were shown to have a synthetic-lethal interaction with MYC. Since these two kinases have been identified in other studies, it gives validity to the ability to the methods of Goga etal in identifying synthetic-lethal targets. The group is currently characterizing and validating the 11 novel targets identified in this screen, using human cancer cell lines as well as mouse cancer models to determine the impact of inhibiting these targets on triple-negative breast cancer development and proliferation.

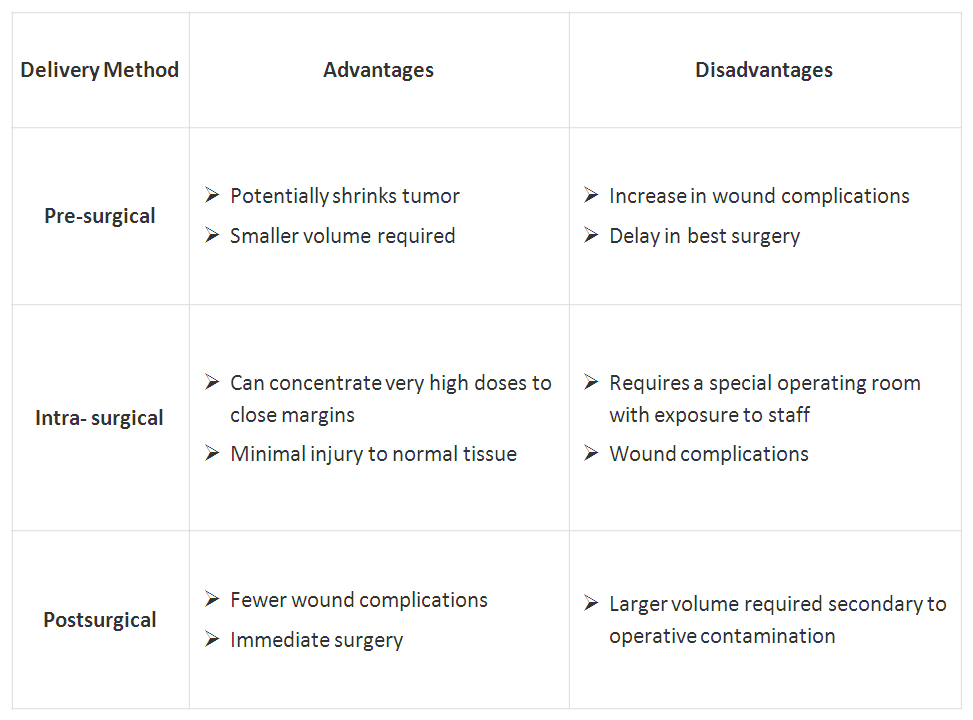 Click on table to enlarge
Click on table to enlarge











