Posts Tagged ‘Invasiveness of surgical procedures’
Protected: MRI Methods and Devices: Range of Potential Applications
Posted in Medical Imaging Technology, Image Processing/Computing, MRI, CT, Nuclear Medicine, Ultra Sound, tagged Ablation, Atrial fibrillation, Invasiveness of surgical procedures, Magnetic resonance imaging, Mitral regurgitation on November 15, 2013|
Open Abdominal Aortic Aneurysm (AAA) repair (OAR) vs. Endovascular AAA Repair (EVAR) in Chronic Kidney Disease Patients – Comparison of Surgery Outcomes
Posted in Abdominal Aorta, Cardiac and Cardiovascular Surgical Procedures, Chemical Biology and its relations to Metabolic Disease, Frontiers in Cardiology and Cardiovascular Disorders, Imaging-based Cancer Patient Management, ISO 10993 for Product Registration: FDA & CE Mark for Development of Medical Devices and Diagnostics, Medical Imaging Technology, Image Processing/Computing, MRI, CT, Nuclear Medicine, Ultra Sound, Regulated Clinical Trials: Design, Methods, Components and IRB related issues, Uncategorized, tagged AAA, Abdominal aortic aneurysm, Aneurysm, Aorta, Aortic aneurysm, Endovascular aneurysm repair, Endovascular surgery, Inferior mesenteric artery, Invasiveness of surgical procedures, Larry H. Bernstein on June 28, 2013| 4 Comments »
Open Abdominal Aortic Aneurysm (AAA) repair (OAR) vs. Endovascular AAA Repair (EVAR) in Chronic Kidney Disease (CKD) Patients – Comparison of Surgery Outcomes
Writer and Curator: Larry H. Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN
This is a review of the effects of CKD on increased morbidity and mortality of abdominal aortic aneurysm repair. The abdominal aorta has branches to the superior mesenteric arteries proximally, and below that both renal arteries, which also supply the adrenals (suprarenal).
Severe atherosclerosis with plaque buildup and separation of the media from the endothelium, can migrate down the addominal aorta before frank rupture of an aneurysm. Abdominal aortic aneurysm often extends from below the the renal arteries, to the internal spermatic vessels, or as far as the iliacs.


Of the visceral branches, the celiac artery and the superior and inferior mesenteric arteries are unpaired, while the suprarenals, renals, internal spermatics, and ovarian are paired. Of the parietal branches the inferior phrenics and lumbars are paired; the middle sacral is unpaired. The terminal branches are paired.
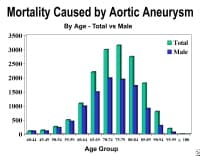
AAA is most common in men over age 65 years. If it is expanding AAA causes sudden, severe, and constant low back, flank, abdominal, or groin pain (internal spermatic branch). The presence of a pulsatile abdominal mass is virtually diagnostic but is found in less than half of all cases. At least 65% of patients with a ruptured AAA die from sudden cardiovascular collapse before arriving at a hospital.
EVAR for ruptured AAA
A study by Mehta et al assessed the effect of hemodynamic status on outcomes in 136 patients undergoing EVAR for ruptured AAAs.[1] The patients were divided into 2 groups:
(1) Hd-stable (systolic BP ≥80 mm Hg; n = 92 [68%]) and
(2) Hd-unstable (systolic BP < 80 mm Hg for >10 minutes; n = 44 [32%]).
(2) Hd-unstable (systolic BP < 80 mm Hg for >10 minutes; n = 44 [32%]).
The 30-day mortality, postoperative complications, need for secondary reinterventions, and midterm mortality were recorded. The 2 groups were found to be similar with respect to
- comorbidities,
- mean AAA maximum diameter (6.6 vs 6.4 cm),
- need for on-the-table conversion to open repair (3% vs 7%), and
- incidence of nonfatal complications (43% vs 38%) and secondary interventions (23% vs 25%).
- intraoperative need for aortic occlusion balloon,
- mean estimated blood loss,
- incidence of developing abdominal compartment syndrome (ACS), and
- mortality
were all increased in the Hd-unstable group ([1]40% vs 6%, [2]744 vs 363 mL,[3] 29% vs 4%, and [4]33% vs 18%, respectively).
Open Surgery
Requires direct access to the aorta through an abdominal or retroperitoneal approach
Endovascular: Involves gaining access to the lumen of the abdominal aorta, usually via small incisions over the femoral vessels; an endograft, typically a cloth graft with a stent exoskeleton, is placed within the lumen of the AAA, extending distally into the iliac arteries. Approximately 90% of abdominal aortic aneurysms are infrarenal.
The important surgical and endovascular anatomic considerations include associated renal and visceral artery involvement (either occlusive disease or involved in the aneurysm process) and the iliac artery (either occlusive disease or aneurysms). The length of the infrarenal aortic neck is important in helping determine the surgical approach (retroperitoneal vs transabdominal) and the location of the aortic cross clamp.
Endovascular Aneurysm Repair
Endovascular repair first became practical in the 1990s and although it is now an established alternative to open repair, its role is yet to be clearly defined. It is generally indicated in older, high-risk patients or patients unfit for open repair. However, endovascular repair is feasible for only a proportion of AAAs, depending on the morphology of the aneurysm. The main advantages over open repair are that there is less peri-operative mortality, less time in intensive care, less time in hospital overall and earlier return to normal activity. Disadvantages of endovascular repair include a requirement for more frequent ongoing hospital reviews, and a higher chance of further procedures being required. According to the latest studies, the EVAR procedure does not offer any benefit for overall survival or health-related quality of life compared to open surgery, although aneurysm-related mortality is lower.

Aorta Anatomy and Pathology in AAA
The diameter of the aorta decreases in size from its thoracic portion to the abdominal and infrarenal portions. A normal aorta shows a reduction in medial elastin layers from the thoracic area to the abdominal portion. Elastin and collagen content are also reduced. AAAs develop following degeneration of the media. The degeneration ultimately may lead to widening of the vessel lumen and loss of structural integrity.
A multidisciplinary research program supported by the US National Heart, Lung, and Blood Institute identified proteolytic degradation of aortic wall connective tissue, inflammation and immune responses, biomechanical wall stress, and molecular genetics as mechanisms important in the development of AAA. Similarly, surgical specimens of AAA reveal inflammation, with infiltration by lymphocytes and macrophages; thinning of the media; and marked loss of elastin.
Through gene microarray analysis, various genes involved in extracellular matrix degradation, inflammation, and other processes observed in AAA formation have been shown to be up-regulated, while others that may serve to prevent this occurrence are down-regulated. The combination of proteolytic degradation of aortic wall connective tissue, inflammation and immune responses, biomechanical wall stress, and molecular genetics represents a dynamic process that leads to aneurysmal deterioration of aortic tissue.

1. Mehta M, Paty PS, Byrne J, Roddy SP, Taggert JB, Sternbach Y, et al. The impact of hemodynamic status on outcomes of endovascular abdominal aortic aneurysm repair for rupture. J Vasc Surg. May 2013;57(5):1255-60. [Medline].
2. Blanchard JF, Armenian HK, Friesen PP. Risk factors for abdominal aortic aneurysm: results of a case-control study. Am J Epidemiol. Mar 15 2000;151(6):575-83. [Medline].
3. Lederle FA, Johnson GR, Wilson SE, Chute EP, Littooy FN, Bandyk D, et al. Prevalence and associations of abdominal aortic aneurysm detected through screening. Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Ann Intern Med. Mar 15 1997;126(6):441-9. [Medline].
4. Wassef M, Baxter BT, Chisholm RL, Dalman RL, Fillinger MF, Heinecke J, et al. Pathogenesis of abdominal aortic aneurysms: a multidisciplinary research program supported by the National Heart, Lung, and Blood Institute. J Vasc Surg. Oct 2001;34(4):730-8. [Medline].
5. [Guideline] U.S. Preventive Services Task Force. Screening for abdominal aortic aneurysm: recommendation statement. Ann Intern Med. Feb 1 2005;142(3):198-202. [Medline]. [Full Text].
Impact of chronic kidney disease on outcomes after abdominal aortic aneurysm repair
Patel VI, Lancaster RT, Mukhopadhyay S, Aranson NJ, Conrad MF, et al.
J Vasc Surg. 2012 Nov;56(5):1206-13. http://dx.doi.org/10.1016/j.jvs.2012.04.037. Epub 2012 Aug 1.
Chronic kidney disease (CKD) is associated with increased morbidity and death after open abdominal aortic aneurysm (AAA) repair (OAR). This study highlights the effect of CKD on outcomes after endovascular AAA (EVAR) and OAR in contemporary practice.
The National Surgical Quality Improvement Program (NSQIP) Participant Use File (2005-2008) was queried by Current Procedural Terminology (American Medical Association, Chicago, Ill) code to identify EVAR or OAR patients, who were grouped by CKD class as having mild (CKD class 1 or 2), moderate (CKD class 3), or severe (CKD class 4 or 5) renal disease. Propensity score analysis was performed to match OAR and EVAR patients with mild CKD with those with moderate or severe CKD. Comparative analysis of mortality and clinical outcomes was performed based on CKD strata.
We identified 8701 patients who were treated with EVAR (n = 5811) or OAR (n = 2890) of intact AAAs. Mild, moderate, and severe CKD was present in 63%, 30%, and 7%, respectively. CKD increased (P < .01) overall mortality, with rates of 1.7% (mild), 5.3% (moderate), and 7.7% (severe) in unmatched patients undergoing EVAR or OAR. Operative mortality rates in patients with severe CKD were as high as 6.2% for EVAR and 10.3% for OAR.
Severity of CKD was associated with increasing frequency of risk factors; therefore, propensity matching to control for comorbidities was performed, resulting in similar baseline clinical and demographic features of patients with mild compared with those with moderate or severe disease.
In propensity-matched cohorts, moderate CKD increased the risk of 30-day mortality
- for EVAR (1.9% mild vs 3.2% moderate; P = .013) and
- OAR (3.1% mild vs 8.4% moderate; P < .0001).
Moderate CKD was also associated with increased morbidity in patients treated with
- EVAR (8.3% mild vs 12.8% moderate; P < .0001) or
- OAR (25.2% mild vs 32.4% moderate; P = .001).
Similarly, severe CKD increased the risk of 30-day mortality
- for EVAR (2.6% mild vs 5.7% severe; P = .0081) and
- OAR (4.1% mild vs 9.9% severe; P = .0057).
Severe CKD was also associated with increased morbidity in patients treated with
- EVAR (10.6% mild vs 19.2% severe; P < .0001) or
- OAR (31.1% mild vs 39.6% severe; P = .04).
The presence of moderate or severe CKD in patients considered for AAA repair is associated with significantly increased mortality and therefore should figure prominently in clinical decision making. The high mortality of AAA repair in patients with severe CKD is such that elective repair in such patients is not advised, except in extenuating clinical circumstances.
Related articles
- Elective Open Suprarenal Aneurysm Repair in England from 2000 to 2010 an Observational Study of Hospital Episode Statistics (plosone.org)
- The EVAR I trial: Endovascular vs. open abdominal aortic aneurysm repair [Classics Series] (2minutemedicine.com)
- Abdominal Aortic Aneurysm Genetic Risk (23andme.com)
- The EVAR II trial: Endovascular approach when unfit for open aortic aneurysm repair [Classics Series] (2minutemedicine.com)
- Red Vascular Branch Endograft System: Aortic Aneursysm (proteinbreak.wordpress.com)
Related articles published on this Open Access Online Scientific Journal
Effect of Hospital Characteristics on Outcomes of Endovascular Repair of Descending Aortic Aneurysms in US Medicare Population
Larry H. Bernstein, MD, FCAP
Abdominal Aortic Aneurysms (AAA): Albert Einstein’s Operation by Dr. Nissen
Aviva Lev-Ari, PhD, RN
No Early Symptoms – An Aortic Aneurysm Before It Ruptures – Is There A Way To Know If I Have it?
Justin D Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
First-of-Its-Kind FDA Approval for ‘AUI’ Device with Endurant II AAA Stent Graft: Medtronic Expands in Endovascular Aortic Repair in the United States
Aviva Lev-Ari, PhD, RN
Abdominal Aortic Aneurysm: Endovascular repair and open repair resulted in similar long-term survival
Aviva Lev-Ari, PhD, RN
EUROPCR 2013, Paris 5/21-5/24, 2013 Conference for Cardiolovascular Intervention and Interventional Medicine
Aviva Lev-Ari, PhD, RN
Genomics & Genetics of Cardiovascular Disease Diagnoses: A Literature Survey of AHA’s Circulation Cardiovascular Genetics, 3/2010 – 3/2013
Aviva Lev-Ari, PhD, RN and Larry Bernstein, MD, FCAP
Competition in the Ecosystem of Medical Devices in Cardiac and Vascular Repair: Heart Valves, Stents, Catheterization Tools and Kits for Open Heart and Minimally Invasive Surgery (MIS)
Aviva Lev-Ari, PhD, RN
Bioabsorbable Drug Coating Scaffolds, Stents and Dual Antiplatelet Therapy
Aviva Lev-Ari, PhD, RN
Vascular Repair: Stents and Biologically Active Implants
Larry Bernstein, MD, FCAP
Drug Eluting Stents: On MIT’s Edelman Lab’s Contributions to Vascular Biology and its Pioneering Research on DES
Larry H. Bernstein, MD, FCAP
Coronary Artery Disease – Medical Devices Solutions: From First-In-Man Stent Implantation, via Medical Ethical Dilemmas to Drug Eluting Stents
Aviva Lev-Ari, PhD, RN
Survivals Comparison of Coronary Artery Bypass Graft (CABG) and Percutaneous Coronary Intervention (PCI) / Coronary Angioplasty
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Trans-apical Transcatheter Aortic Valve Replacement in a Patient with Severe and Complex Left Main Coronary Artery Disease (LMCAD)
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Transcatheter Aortic Valve Replacement (TAVR): Postdilatation to Reduce Paravalvular Regurgitation During TAVR with a Balloon-expandable Valve
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Svelte Medical Systems’ Drug-Eluting Stent: 0% Clinically-Driven Events Through 12-Months in First-In-Man Study
Aviva Lev-Ari, PhD, RN
Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone (Justin Pearlman, Aviva Lev-Ari)
Biomaterials Technology: Models of Tissue Engineering for Reperfusion and Implantable Devices for Revascularization
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Revascularization: PCI, Prior History of PCI vs CABG
Aviva Lev-Ari, PhD, RN
http://pharmaceuticalintelligence.com/2013/04/25/revascularization-pci-prior-history-of-pci-vs-cabg/
Accurate Identification and Treatment of Emergent Cardiac Events
Larry Bernstein, MD, FCAP
FDA Pending 510(k) for The Latest Cardiovascular Imaging Technology
Aviva Lev-Ari, PhD, RN
The ACUITY-PCI score: Will it Replace Four Established Risk Scores — TIMI, GRACE, SYNTAX, and Clinical SYNTAX
Aviva Lev-Ari, PhD, RN
Nitric Oxide and it’s impact on Cardiothoracic Surgery
Tilda Barliya, PhD
CABG or PCI: Patients with Diabetes – CABG Rein Supreme
Aviva Lev-Ari, PhD, RN
To Stent or Not? A Critical Decision
Aviva Lev-Ari, PhD, RN
Endothelin Receptors in Cardiovascular Diseases: The Role of eNOS Stimulation
Aviva Lev-Ari, PhD, RN
Absorb™ Bioresorbable Vascular Scaffold: An International Launch by Abbott Laboratories
Aviva Lev-Ari, PhD, RN
Carotid Stenting: Vascular surgeons have pointed to more minor strokes in the stenting group and cardiologists to more myocardial infarctions in the CEA cohort.
Aviva Lev-Ari, PhD, RN
New Drug-Eluting Stent Works Well in STEMI
Aviva Lev-Ari, PhD, RN
Global Supplier Strategy for Market Penetration & Partnership Options (Niche Suppliers vs. National Leaders) in the Massachusetts Cardiology & Vascular Surgery Tools and Devices Market for Cardiac Operating Rooms and Angioplasty Suites
Aviva Lev-Ari, PhD, RN

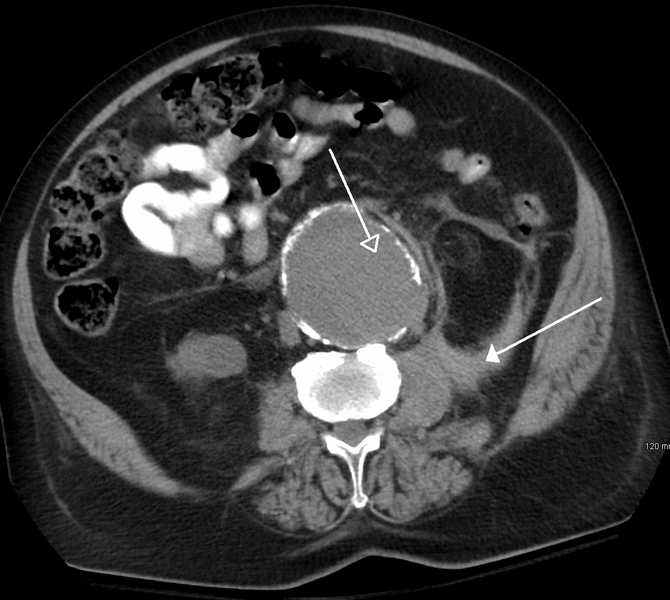
Abdominal Aortic Aneurysm in Computer Tomography (Photo credit: Wikipedia)
Effect of Hospital Characteristics on Outcomes of Endovascular Repair of Descending Aortic Aneurysms in US Medicare Population
Posted in Cardiac & Vascular Repair Tools Subsegment, FDA Regulatory Affairs, Frontiers in Cardiology and Cardiovascular Disorders, Health Economics and Outcomes Research, ISO 10993 for Product Registration: FDA & CE Mark for Development of Medical Devices and Diagnostics, Medical Devices R&D Investment, Medical Imaging Technology, Image Processing/Computing, MRI, CT, Nuclear Medicine, Ultra Sound, Regulated Clinical Trials: Design, Methods, Components and IRB related issues, Statistical Methods for Research Evaluation, Technology Transfer: Biotech and Pharmaceutical, Thoracic Aorta, tagged Aneurysm, Endovascular aneurysm repair, Harvard Medical School, Invasiveness of surgical procedures, Massachusetts General Hospital, University of Pittsburgh Medical Center, Vascular surgery on June 27, 2013| 5 Comments »
Effect of Hospital Characteristics on Outcomes of Endovascular Repair of Descending Aortic Aneurysms in US Medicare Population
Writer and Curator: Larry H. Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN
Impact of hospital volume and type on outcomes of open and endovascular repair of descending thoracic aneurysms in the United States Medicare population.
Patel VI, Mukhopadhyay S, Ergul E, Aranson N, …., Cambria RP.
Division of Vascular and Endovascular Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, Mass.
Journal of vascular surgery 2013; http://dx.doi.org/10.1016/j.jvs.2013.01.035
Open surgery for thoracic aortic aneurysm has had success, but it carries complication risks. In 2004, a much less invasive procedure, thoracic endovascular repair (TEVAR) was introduced. It eliminated a need for open surgery in many patients, but not all were suitable candidtes . The advances in endovascular technology and procedural breakthroughs since it was introduced has contributed to a dramatic transformation of the specialty of thoracic aortic surgery. The decision of which patients require open surgery is necessarily determined by the limitations of the procedure and the condition of the patient.
Thoracic endovascular aortic repair (TEVAR) is a minimally invasive alternative to conventional open surgical reconstruction for the treatment of thoracic aortic aneurysm. TEVAR procedures can be challenging and, at times, extraordinarily difficult. Meticulous assessment of anatomy and preoperative procedure planning are absolutely paramount to produce optimal outcomes. The rapidly Increased use of TEVAR has produced favorable outcomes of TEVAR compared with open abdominal repair for descending thoracic aortic aneurysms (DTAs). But the success of these procedure depends on requisite skills, and following guidelines intended for use in quality-improvement programs that assess the standard of care expected from all physicians who perform TEVAR procedures.
Currently, there is a diverse array of endografts that are commercially available to treat the thoracic aorta. Multiple studies have demonstrated excellent outcomes of thoracic endovascular aortic repair for the treatment of thoracic aortic aneurysms, with less reported perioperative morbidity and mortality in comparison with conventional open repair. Additionally, similar outcomes have been demonstrated for the treatment of type B dissections. However, the technology remains relatively novel, and larger studies with longer term outcomes are necessary to more fully evaluate the role of endovascular therapy for the treatment of thoracic aortic disease.
The MGH/Partners vascular surgeons evaluated the effect of case volume and hospital teaching status on clinical outcomes of intact DTA repair to gain an insight into whether there was a variability in DTAs outcomes based on hospital size, patient mix, number of procedures, staff characteristics, and teaching status. This study was needed for establishing the type of procedure most suited to the type of patient, and to obtain the most accurate analysis of cost requirements based on resource allocation for reimbursement purposes.
The Medicare Provider Analysis and Review (MEDPAR) data set (2004 to 2007) was queried to identify open repair or TEVAR for DTA. Hospitals were stratified by DTA volume into high volume (HV; ≥8 cases/y) or low volume (LV; <8 cases/y) and teaching or nonteaching. The effect of hospital variables on the primary study end point of 30-day mortality and secondary end points of 30-day complications and long-term survival after open repair and TEVAR DTA repair were studied using univariate testing, multivariable regression modeling, Kaplan-Meier survival analysis, and Cox proportional hazards regression modeling.
They identified 763 hospitals performing 3554 open repairs and 3517 TEVARs. Overall DTA repair increased (P < .01) from 1375 in 2004 to 1987 in 2007. The proportion of hospitals performing open repair significantly decreased from 95% in 2004 to 57% in 2007 (P < .01), whereas
- those performing TEVAR increased (P < .01) from 24% to 76%.
Overall repair type shifted from open (74% in 2004, the year before initial commercial availability of TEVAR) to TEVAR (39% open in 2007; P < .01). The fraction of open repairs at LV hospitals
- decreased from 56% in 2004 to 44% in 2007 (P < .01), whereas
- TEVAR increased from 24% in 2004 to 51% in 2007 (P < .01).
Overall mortality during the study interval for
- open repair was 15% at LV hospitals vs 11% at HV hospitals (P < .01), whereas
- TEVAR mortality was similar, at 3.9% in LV vs 5.5% in HV hospitals (P = .43).
LV was independently associated with increased mortality after open repair (odds ratio, 1.4; 95% confidence interval, 1.1-1.8; P < .01) but not after TEVAR. There was no independent effect of hospital teaching status on mortality or complications after open repair or TEVAR repair.
The total number of DTA repairs significantly increased after the introduction of TEVAR for DTA. Operative mortality for TEVAR is independent of hospital volume and type, whereas
- mortality after open surgery is lower at HV hospitals.
While the TEVAR mortality is significantly less than that of open surgery, the mortality in open surgery is higher for LV hospitals. The data suggests that TEVAR can be safely performed across a spectrum of hospitals, whereas open surgery should be performed only at HV hospitals.
- Standard of Practice for the Endovascular Treatment of Thoracic Aortic Aneurysms and Type B Dissections. Fanelli F, and Dake MD. Cardiovasc Intervent Radiol. 2009 September; 32(5): 849–860. http://dx.doi.org/10.1007/s00270-009-9668-6 PMCID: PMC2744786
- Thoracic aortic aneurysms and dissections: endovascular treatment. Baril DT, Cho JS, Chaer RA, Makaroun MS. Division of Vascular Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA. Mt Sinai J Med. 2010 May-Jun;77(3):256-69. http://dx.doi.org/10.1002/msj.20178.
Related articles
- No Early Symptoms – An Aortic Aneurysm Before It Ruptures – Is There A Way To Know If I Have it? (pharmaceuticalintelligence.com)
- Elective Open Suprarenal Aneurysm Repair in England from 2000 to 2010 an Observational Study of Hospital Episode Statistics (plosone.org)
- Abdominal Aortic Aneurysms (AAA): Albert Einstein’s Operation by Dr. Nissen (pharmaceuticalintelligence.com)
- Abdominal Aortic Aneurysm Genetic Risk (23andme.com)
- The EVAR I trial: Endovascular vs. open abdominal aortic aneurysm repair [Classics Series] (2minutemedicine.com)
- Revascularization Procedures Saving Limbs Of More Peripheral Arterial Disease Patients (medicalnewstoday.com)
- Brain aneurysm treatments now have fewer complications, better outcomes (miamiherald.com)
- The EVAR II trial: Endovascular approach when unfit for open aortic aneurysm repair [Classics Series] (2minutemedicine.com)
- SNPwatch: Three New Genetic Variants Associated with Brain Aneurysm Identified (23andme.com)
Related Articles in Pharmaceuticval Intelligence
Abdominal Aortic Aneurysms (AAA): Albert Einstein’s Operation by Dr. Nissen (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/06/11/abdominal-aortic-aneurysms-aaa-albert-einsteins-operation-by-dr-nissen/
The Heart Surgery Specialty: heart transplant, lung transplant, heart-lung transplantation, aortic valve surgery, bypass surgery, minimally invasive cardiac surgery, heart valve surgery, removal of cardiac tumors, reoperation valve surgery (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/?p=14092&preview=true
No Early Symptoms – An Aortic Aneurysm Before It Ruptures – Is There A Way To Know If I Have it?
(Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/06/10/no-early-symptoms-an-aortic-aneurysm-before-it-ruptures-is-there-a-way-to-know-if-i-have-it/
First-of-Its-Kind FDA Approval for ‘AUI’ Device with Endurant II AAA Stent Graft: Medtronic Expands in Endovascular Aortic Repair in the United States (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/30/first-of-its-kind-fda-approval-for-aui-device-with-endurant-ii-aaa-stent-graft-medtronic-expands-in-endovascular-aortic-repair-in-the-united-states/
Abdominal Aortic Aneurysm: Endovascular repair and open repair resulted in similar long-term survival
(Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2012/12/03/abdominal-aortic-aneurysm-endovascular-repair-and-open-repair-resulted-in-similar-long-term-survival/
EUROPCR 2013, Paris 5/21-5/24, 2013 Conference for Cardiolovascular Intervention and Interventional Medicine (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/29/europcr-2013-paris-521-524-2013-conference-for-cardiolovascular-intervention-and-interventional-medicine/
Genomics & Genetics of Cardiovascular Disease Diagnoses: A Literature Survey of AHA’s Circulation Cardiovascular Genetics, 3/2010 – 3/2013 (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/03/07/genomics-genetics-of-cardiovascular-disease-diagnoses-a-literature-survey-of-ahas-circulation-cardiovascular-genetics-32010-32013/
Competition in the Ecosystem of Medical Devices in Cardiac and Vascular Repair: Heart Valves, Stents, Catheterization Tools and Kits for Open Heart and Minimally Invasive Surgery (MIS) (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2012/06/22/competition-in-the-ecosystem-of-medical-devices-in-cardiac-and-vascular-repair-heart-valves-stents-catheterization-tools-and-kits-for-open-heart-and-minimally-invasive-surgery-mis/
Bioabsorbable Drug Coating Scaffolds, Stents and Dual Antiplatelet Therapy (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/29/bioabsorbable-drug-coating-scaffolds-stents-and-dual-antiplatelet-therapy/
Vascular Repair: Stents and Biologically Active Implants (larryhbern)
http://pharmaceuticalintelligence.com/2013/05/04/stents-biologically-active-implants-and-vascular-repair/
Drug Eluting Stents: On MIT’s Edelman Lab’s Contributions to Vascular Biology and its Pioneering Research on DES (larryhbern)
http://pharmaceuticalintelligence.com/2013/04/25/contributions-to-vascular-biology/
Coronary Artery Disease – Medical Devices Solutions: From First-In-Man Stent Implantation, via Medical Ethical Dilemmas to Drug Eluting Stents (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2012/08/13/coronary-artery-disease-medical-devices-solutions-from-first-in-man-stent-implantation-via-medical-ethical-dilemmas-to-drug-eluting-stents/
Survivals Comparison of Coronary Artery Bypass Graft (CABG) and Percutaneous Coronary Intervention (PCI) / Coronary Angioplasty (larryhbern)
http://pharmaceuticalintelligence.com/2013/06/23/comparison-of-cardiothoracic-bypass-and-percutaneous-interventional-catheterization-survivals/
Trans-apical Transcatheter Aortic Valve Replacement in a Patient with Severe and Complex Left Main Coronary Artery Disease (LMCAD) (larryhbern)
http://pharmaceuticalintelligence.com/2013/06/17/management-of-difficult-trans-apical-transcatheter-aortic-valve-replacement-in-a-patient-with-severe-and-complex-arterial-disease/
Transcatheter Aortic Valve Replacement (TAVR): Postdilatation to Reduce Paravalvular Regurgitation During TAVR with a Balloon-expandable Valve (larryhbern)
http://pharmaceuticalintelligence.com/2013/06/17/postdilatation-to-reduce-paravalvular-regurgitation-during-transcatheter-aortic-valve-replacement/
Svelte Medical Systems’ Drug-Eluting Stent: 0% Clinically-Driven Events Through 12-Months in First-In-Man Study (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/28/svelte-medical-systems-drug-eluting-stent-0-clinically-driven-events-through-12-months-in-first-in-man-study/
Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone (Justin Pearlman, Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/22/acute-and-chronic-myocardial-infarction-quantification-of-myocardial-viability-fdg-petmri-vs-mri-or-pet-alone/
Biomaterials Technology: Models of Tissue Engineering for Reperfusion and Implantable Devices for Revascularization (larryhbern)
http://pharmaceuticalintelligence.com/2013/05/05/bioengineering-of-vascular-and-tissue-models/
Revascularization: PCI, Prior History of PCI vs CABG (A Lev-Ari)
http://pharmaceuticalintelligence.com/2013/04/25/revascularization-pci-prior-history-of-pci-vs-cabg/
Accurate Identification and Treatment of Emergent Cardiac Events (larryhbern)
http://pharmaceuticalintelligence.com/2013/03/15/accurate-identification-and-treatment-of-emergent-cardiac-events/
FDA Pending 510(k) for The Latest Cardiovascular Imaging Technology (A Lev-Ari)
http://pharmaceuticalintelligence.com/2013/01/28/fda-pending-510k-for-the-latest-cardiovascular-imaging-technology/
The ACUITY-PCI score: Will it Replace Four Established Risk Scores — TIMI, GRACE, SYNTAX, and Clinical SYNTAX (A Lev-Ari)
http://pharmaceuticalintelligence.com/2013/01/03/the-acuity-pci-score-will-it-replace-four-established-risk-scores-timi-grace-syntax-and-clinical-syntax/
Nitric Oxide and it’s impact on Cardiothoracic Surgery (tildabarliya)
http://pharmaceuticalintelligence.com/2012/12/15/nitric-oxide-and-its-impact-on-cardiothoracic-surgery/
CABG or PCI: Patients with Diabetes – CABG Rein Supreme (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/11/05/cabg-or-pci-patients-with-diabetes-cabg-rein-supreme/
To Stent or Not? A Critical Decision (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/10/23/to-stent-or-not-a-critical-decision/
Endothelin Receptors in Cardiovascular Diseases: The Role of eNOS Stimulation (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/10/04/endothelin-receptors-in-cardiovascular-diseases-the-role-of-enos-stimulation/
Absorb™ Bioresorbable Vascular Scaffold: An International Launch by Abbott Laboratories
(Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2012/09/29/absorb-bioresorbable-vascular-scaffold-an-international-launch-by-abbott-laboratories/
Carotid Stenting: Vascular surgeons have pointed to more minor strokes in the stenting group and cardiologists to more myocardial infarctions in the CEA cohort. (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/09/21/carotid-stenting-vascular-surgeons-have-pointed-to-more-minor-strokes-in-the-stenting-group-and-cardiologists-to-more-myocardial-infarctions-in-the-cea-cohort/
New Drug-Eluting Stent Works Well in STEMI (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/08/22/new-drug-eluting-stent-works-well-in-stemi/
lobal Supplier Strategy for Market Penetration & Partnership Options (Niche Suppliers vs. National Leaders) in the Massachusetts Cardiology & Vascular Surgery Tools and Devices Market for Cardiac Operating Rooms and Angioplasty Suites (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/06/22/global-supplier-strategy-for-market-penetration-partnership-options-niche-suppliers-vs-national-leaders-in-the-massachusetts-cardiology-vascular-surgery-tools-and-devices-market-for-car/

Histopathological image of dissecting aneurysm of thoracic aorta in a patient without evidence of Marfan syndrome. The damaged aorta was surgically removed and replaced by artificial vessel. Victoria blue & HE stain. (Photo credit: Wikipedia)

Diagram of aortic aneurysm Figure A shows a normal aorta. Figure B shows a thoracic aortic aneurysm (which is located behind the heart). Figure C shows an abdominal aortic aneurysm located below the arteries that supply blood to the kidneys. (Photo credit: Wikipedia)

Thoracic aorta (Photo credit: Wikipedia)

Open Heart Surgery (Photo credit: Wikipedia)
Minimally invasive image-guided therapy for inoperable hepatocellular carcinoma
Posted in Advanced Drug Manufacturing Technology, Bio Instrumentation in Experimental Life Sciences Research, Biomarkers & Medical Diagnostics, CANCER BIOLOGY & Innovations in Cancer Therapy, Ecosystems & Industrial Concentration in the Medical Device Sector, Health Economics and Outcomes Research, Imaging-based Cancer Patient Management, Liver & Digestive Diseases Research, Medical Imaging Technology, Image Processing/Computing, MRI, CT, Nuclear Medicine, Ultra Sound, Personalized and Precision Medicine & Genomic Research, tagged Ablation, Biology, Cancer - General, Chemotherapy, focused treatment, HCC, health, Hepatocellular carcinoma, High-intensity focused ultrasound, imaging guided therapy, Invasiveness of surgical procedures, liver, liver ablation, liver cancer, liver metastasis, Magnetic resonance imaging, medicine, Personalized medicine, Radiofrequency ablation, treatment guidance, Treatment Response on April 15, 2013| 4 Comments »
Minimally invasive image-guided therapy for inoperable hepatocellular carcinoma
Curator & Reporter: Dror Nir, PhD

Large organs like the liver are good candidates for focused treatment. The following paper:
By Beatrijs A. Seinstra1, et. al. published mid-2010, gives a review of the state-of-the-art of the then available methods for local lesions’ ablation. As far as ablation techniques availability, I have found this review very much relevant to today’s technological reality. It is worthwhile noting that in the last couple of years, new imaging-based navigation and guidance applications were introduced into the market holding a promise to improve the accuracy of administrating such treatment. These are subject to clinical validation in large clinical studies. From the above mentioned publication I have chosen to highlight the parts discussing the importance of imaging-based guidance to the effective application of localized ablation-type therapies.
The clinical need:
Hepatocellular carcinoma (HCC) is a primary malignant tumor of the liver that accounts for an important health problem worldwide. Primary liver cancer is the sixth most common cancer worldwide with an incidence of 626,000 patients a year, and the third most common cause of cancer-related death [1]. Only 10–15% of HCC patients are suitable candidates for hepatic resection and liver transplantation due to the advanced stage of the disease at time of diagnosis and shortage of donors.
Immerging solution:
In order to provide therapeutic options for patients with inoperable HCC, several minimally invasive image-guided therapies for locoregional treatment have been developed. HCC has a tendency to remain confined to the liver until the disease has advanced, making these treatments particularly attractive.
Minimally invasive image-guided therapies can be divided into the group of the tumor ablative techniques or the group of image-guided catheter-based techniques. Tumor ablative techniques are either based on thermal tumor destruction, as in radiofrequency ablation (RFA), cryoablation, microwave ablation, laser ablation and high-intensity focused ultrasound (HIFU), or chemical tumor destruction, as in percutaneous ethanol injection (PEI). These techniques are mostly used for early stage disease. Image-guided catheter-based techniques rely on intra-arterial delivery of embolic, chemoembolic, or radioembolic agents [22]. These techniques enable treatment of large lesions or whole liver treatment, and are as such used for intermediate stage HCC (Figure 1).
Minimally invasive image-guided ablation techniques and intra-arterial interventions may prolong survival, spare more functioning liver tissue in comparison to surgical resection (which can be very important in cirrhotic patients), allow retreatment if necessary, and may be an effective bridge to transplantation [23–27].
During the last 2 decades, minimally invasive image-guided therapies have revolutionized the management of inoperable HCC.
The value of image guidance
Accurate imaging is of great importance during minimally invasive loco-regional therapies to efficiently guide and monitor the treatment. It enables proper placement of instruments, like the probe in case of ablation or the catheter in case of intra-arterial therapy, and accurate monitoring of the progression of the necrotic zone during ablation.
- Fluoroscopy,
- ultrasound (US),
- computed tomography (CT), and
- magnetic resonance imaging (MRI)
can all be employed. In current clinical practice, placement of the catheter in intra-arterial procedures is usually performed under fluoroscopic guidance, while ablation may be guided by ultrasound, CT or MRI.
- Ultrasound guidance allows probe insertion from every angle, offers real time visualization and correction for motion artifacts when targeting the tumor, and is low cost. However, the gas created during ablation (or ice in the case of cryoablation) hampers penetration of the ultrasound beams in tissue, causing acoustic shadowing and obscuring image details like the delineation between tumor borders and ablation zone.
- CT is also frequently used to guide minimally invasive ablation therapy, and is a reliable modality to confirm treatment results. In comparison to US, it provides increased lesion discrimination, a more reliable depiction of ablated/non-ablated interfaces, and a better correlation to pathologic size [28]. However, due to its hypervascularity, small HCCs can only be clearly visualized in the arterial phase for a short period of time. Another disadvantage of CT is the exposure of the patient and physician to ionizing radiation.
- Combining US imaging for probe placement and CT for ablation monitoring reduces this exposure. At the moment, hybrid systems are being developed, enabling combination of imaging techniques, like ultrasound and CT imaging, thereby improving the registration accuracy during treatment [29]. The interest in MRI-guided ablation is growing, as it produces a high-quality image allowing high-sensitivity tumor detection and accurate identification of the target region with multiplanar imaging.
- MRI also enables real-time monitoring of the temperature evolution during treatment [30–35]. However, MRI is an expensive technique, and MRI-guided ablation is still limited in clinical practice. Currently, the most widely used ablation technique for percutaneous treatment of focal hepatic malignancies is radiofrequency ablation (RFA), which has been shown to be safe and effective for the treatment of early stage HCC [48–50]. During RFA, a small electrode is placed within the tumor, and a high-frequency alternating electric current (approximately 400 MHz) is generated, causing ionic agitation within the tissue. ….. Most frequently ultrasound is used for image guidance (Figs. 2, 3), but there are reports of groups who use CT, MRI, or fluoroscopic imaging.

Ultrasound guided RFA. a: HCC lesion in a non-surgical patient pre-treatment (pointed out by arrow). b: Just after start treatment, electrode placed centrally in the tumor. c: Gas formation during ablation causes acoustic shadowing

Contrast-enhanced CT pre- and post-RFA. Same patient as in Fig. 2. a: Hypervascular lesion (biopsy proven HCC) in right liver lobe (pointed out by arrow) before treatment. b: Ablated lesion directly post ablation, with reactive hyperemia around the RFA lesion
References
1.
Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55:74–108PubMedCrossRef
2.
[No authors listed] (1987) Hepatocellular cancer: differences between high and low incidence regions. Lancet 2:1183–1184
3.
El-Serag HB, Davila JA, Petersen NJ, McGlynn KA (2003) The continuing increase in the incidence of hepatocellular carcinoma in the United States: an update. Ann Intern Med 139:817–823PubMed
4.
Taylor-Robinson SD, Foster GR, Arora S, Hargreaves S, Thomas HC (1997) Increase in primary liver cancer in the UK, 1979–94. Lancet 350:1142–1143PubMedCrossRef
5.
Beasley RP, Hwang LY, Lin CC, Chien CS (1981) Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22,707 men in Taiwan. Lancet 2:1129–1133PubMedCrossRef
6.
Beasley RP (1988) Hepatitis B virus. The major etiology of hepatocellular carcinoma Cancer 61:1942–1956
7.
Chen HL, Chang MH, Ni YH, Hsu HY, Lee PI, Lee CY et al (1996) Seroepidemiology of hepatitis B virus infection in children: Ten years of mass vaccination in Taiwan. JAMA 276:906–908PubMedCrossRef
8.
Chang MH, Chen CJ, Lai MS, Hsu HM, Wu TC, Kong MS et al (1997) Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N Engl J Med 336:1855–1859PubMedCrossRef
9.
Adami HO, Hsing AW, McLaughlin JK, Trichopoulos D, Hacker D, Ekbom A et al (1992) Alcoholism and liver cirrhosis in the etiology of primary liver cancer. Int J Cancer 51:898–902PubMedCrossRef
10.
Bruix J, Barrera JM, Calvet X, Ercilla G, Costa J, Sanchez-Tapias JM et al (1989) Prevalence of antibodies to hepatitis C virus in Spanish patients with hepatocellular carcinoma and hepatic cirrhosis. Lancet 2:1004–1006PubMedCrossRef
11.
Colombo M, Kuo G, Choo QL, Donato MF, Del NE, Tommasini MA et al (1989) Prevalence of antibodies to hepatitis C virus in Italian patients with hepatocellular carcinoma. Lancet 2:1006–1008PubMedCrossRef
12.
Tsukuma H, Hiyama T, Tanaka S, Nakao M, Yabuuchi T, Kitamura T et al (1993) Risk factors for hepatocellular carcinoma among patients with chronic liver disease. N Engl J Med 328:1797–1801PubMedCrossRef
13.
Pons F, Varela M, Llovet JM (2005) Staging systems in hepatocellular carcinoma. HPB (Oxford) 7:35–41
14.
Llovet JM, Fuster J, Bruix J (2004) The Barcelona approach: diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl 10:S115–S120PubMedCrossRef
15.
Bruix J, Llovet JM (2009) Major achievements in hepatocellular carcinoma. Lancet 373:614–616PubMedCrossRef
16.
Geschwind JF (2002) Chemoembolization for hepatocellular carcinoma: where does the truth lie? J Vasc Interv Radiol 13:991–994PubMedCrossRef
17.
Bruix J, Llovet JM (2002) Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology 35:519–524PubMedCrossRef
18.
Bruix J, Castells A, Bosch J, Feu F, Fuster J, Garcia-Pagan JC et al (1996) Surgical resection of hepatocellular carcinoma in cirrhotic patients: prognostic value of preoperative portal pressure. Gastroenterology 111:1018–1022PubMedCrossRef
19.
Llovet JM, Fuster J, Bruix J (1999) Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology 30:1434–1440PubMedCrossRef
20.
Thomas MB, O’Beirne JP, Furuse J, Chan AT, bou-Alfa G, Johnson P (2008) Systemic therapy for hepatocellular carcinoma: cytotoxic chemotherapy, targeted therapy and immunotherapy. Ann Surg Oncol 15:1008–1014PubMedCrossRef
21.
Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF et al (2008) Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 359:378–390PubMedCrossRef
22.
Trinchet JC, Ganne-Carrie N, Beaugrand M (2003) Review article: intra-arterial treatments in patients with hepatocellular carcinoma. Aliment Pharmacol Ther 17(Suppl 2):111–118PubMedCrossRef
23.
Lu DS, Yu NC, Raman SS, Lassman C, Tong MJ, Britten C et al (2005) Percutaneous radiofrequency ablation of hepatocellular carcinoma as a bridge to liver transplantation. Hepatology 41:1130–1137PubMedCrossRef
24.
Mazzaferro V, Battiston C, Perrone S, Pulvirenti A, Regalia E, Romito R et al (2004) Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann Surg 240:900–909PubMedCrossRef
25.
Graziadei IW, Sandmueller H, Waldenberger P, Koenigsrainer A, Nachbaur K, Jaschke W et al (2003) Chemoembolization followed by liver transplantation for hepatocellular carcinoma impedes tumor progression while on the waiting list and leads to excellent outcome. Liver Transpl 9:557–563PubMedCrossRef
26.
Yao FY, Kerlan RK, Hirose R, Davern TJ, Bass NM, Feng S et al (2008) Excellent outcome following down-staging of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat analysis. Hepatology 48:819–827PubMedCrossRef
27.
Chapman WC, Majella Doyle MB, Stuart JE, Vachharajani N, Crippin JS, Anderson CD et al (2008) Outcomes of neoadjuvant transarterial chemoembolization to downstage hepatocellular carcinoma before liver transplantation. Ann Surg 248:617–625PubMed
28.
Cha CH, Lee FT Jr, Gurney JM, Markhardt BK, Warner TF, Kelcz F et al (2000) CT versus sonography for monitoring radiofrequency ablation in a porcine liver. AJR Am J Roentgenol 175:705–711PubMed
29.
Wood BJ, Locklin JK, Viswanathan A, Kruecker J, Haemmerich D, Cebral J et al (2007) Technologies for guidance of radiofrequency ablation in the multimodality interventional suite of the future. J Vasc Interv Radiol 18:9–24PubMedCrossRef
30.
Hokland SL, Pedersen M, Salomir R, Quesson B, Stodkilde-Jorgensen H, Moonen CT (2006) MRI-guided focused ultrasound: methodology and applications. IEEE Trans Med Imaging 25:723–731PubMedCrossRef
31.
Cline HE, Hynynen K, Watkins RD, Adams WJ, Schenck JF, Ettinger RH et al (1995) Focused US system for MR imaging-guided tumor ablation. Radiology 194:731–737PubMed
32.
Hynynen K, Freund WR, Cline HE, Chung AH, Watkins RD, Vetro JP et al (1996) A clinical, noninvasive, MR imaging-monitored ultrasound surgery method. Radiographics 16:185–195PubMed
33.
Kopelman D, Inbar Y, Hanannel A, Dank G, Freundlich D, Perel A et al (2006) Magnetic resonance-guided focused ultrasound surgery (MRgFUS). Four ablation treatments of a single canine hepatocellular adenoma HPB (Oxford) 8:292–298
34.
Kopelman D, Inbar Y, Hanannel A, Freundlich D, Castel D, Perel A et al (2006) Magnetic resonance-guided focused ultrasound surgery (MRgFUS): ablation of liver tissue in a porcine model. Eur J Radiol 59:157–162PubMedCrossRef
35.
Gedroyc WM (2005) Magnetic resonance guidance of thermal ablation. Top Magn Reson Imaging 16:339–353PubMedCrossRef
36.
Livraghi T, Festi D, Monti F, Salmi A, Vettori C (1986) US-guided percutaneous alcohol injection of small hepatic and abdominal tumors. Radiology 161:309–312PubMed
37.
Shiina S, Yasuda H, Muto H, Tagawa K, Unuma T, Ibukuro K et al (1987) Percutaneous ethanol injection in the treatment of liver neoplasms. AJR Am J Roentgenol 149:949–952PubMed
38.
Lencioni R, Cioni D, Crocetti L, Bartolozzi C (2004) Percutaneous ablation of hepatocellular carcinoma: state-of-the-art. Liver Transpl 10:S91–S97PubMedCrossRef
39.
Shiina S, Teratani T, Obi S, Sato S, Tateishi R, Fujishima T et al (2005) A randomized controlled trial of radiofrequency ablation with ethanol injection for small hepatocellular carcinoma. Gastroenterology 129:122–130PubMedCrossRef
40.
Lencioni R, Bartolozzi C, Caramella D, Paolicchi A, Carrai M, Maltinti G et al (1995) Treatment of small hepatocellular carcinoma with percutaneous ethanol injection. Analysis of prognostic factors in 105 Western patients. Cancer 76:1737–1746PubMedCrossRef
41.
Livraghi T, Giorgio A, Marin G, Salmi A, De Sio I, Bolondi L et al (1995) Hepatocellular carcinoma and cirrhosis in 746 patients: long-term results of percutaneous ethanol injection. Radiology 197:101–108PubMed
42.
Di SM, Buscarini L, Livraghi T, Giorgio A, Salmi A, De Sio I et al (1997) Percutaneous ethanol injection in the treatment of hepatocellular carcinoma. A multicenter survey of evaluation practices and complication rates Scand J Gastroenterol 32:1168–1173
43.
Lencioni RA, Allgaier HP, Cioni D, Olschewski M, Deibert P, Crocetti L et al (2003) Small hepatocellular carcinoma in cirrhosis: randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Radiology 228:235–240PubMedCrossRef
44.
Lin SM, Lin CJ, Lin CC, Hsu CW, Chen YC (2004) Radiofrequency ablation improves prognosis compared with ethanol injection for hepatocellular carcinoma ≤4 cm. Gastroenterology 127:1714–1723PubMedCrossRef
45.
Lin SM, Lin CJ, Lin CC, Hsu CW, Chen YC (2005) Randomised controlled trial comparing percutaneous radiofrequency thermal ablation, percutaneous ethanol injection, and percutaneous acetic acid injection to treat hepatocellular carcinoma of 3 cm or less. Gut 54:1151–1156PubMedCrossRef
46.
Brunello F, Veltri A, Carucci P, Pagano E, Ciccone G, Moretto P et al (2008) Radiofrequency ablation versus ethanol injection for early hepatocellular carcinoma: A randomized controlled trial. Scand J Gastroenterol 43:727–735PubMedCrossRef
47.
Orlando A, Leandro G, Olivo M, Andriulli A, Cottone M (2009) Radiofrequency thermal ablation vs. percutaneous ethanol injection for small hepatocellular carcinoma in cirrhosis: meta-analysis of randomized controlled trials. Am J Gastroenterol 104:514–524PubMedCrossRef
48.
Curley SA, Izzo F, Delrio P, Ellis LM, Granchi J, Vallone P et al (1999) Radiofrequency ablation of unresectable primary and metastatic hepatic malignancies: results in 123 patients. Ann Surg 230:1–8PubMedCrossRef
49.
Curley SA, Izzo F, Ellis LM, Nicolas VJ, Vallone P (2000) Radiofrequency ablation of hepatocellular cancer in 110 patients with cirrhosis. Ann Surg 232:381–391PubMedCrossRef
50.
Goldberg SN, Gazelle GS, Solbiati L, Livraghi T, Tanabe KK, Hahn PF et al (1998) Ablation of liver tumors using percutaneous RF therapy. AJR Am J Roentgenol 170:1023–1028PubMed
Other research papers related to the management of Prostate cancer were published on this Scientific Web site:
HBV and HCV-associated Liver Cancer: Important Insights from the Genome
Harnessing Personalized Medicine for Cancer Management, Prospects of Prevention and Cure: Opinions of Cancer Scientific Leaders @ http://pharmaceuticalintelligence.com
Whole-body imaging as cancer screening tool; answering an unmet clinical need?
Personalized Medicine: Cancer Cell Biology and Minimally Invasive Surgery (MIS)
Ablation Devices Market to 2023 – Global Market Forecast and Trends Analysis by Technology, Devices & Applications
Posted in Bio Instrumentation in Experimental Life Sciences Research, Cardiac & Vascular Repair Tools Subsegment, Ecosystems & Industrial Concentration in the Medical Device Sector, Frontiers in Cardiology and Cardiovascular Disorders, Medical Devices R&D and Inventions, tagged Galil Medical, High-intensity focused ultrasound, Invasiveness of surgical procedures, Medtronic, Olympus Corporation, Radiation therapy, ultrasound, Varian Medical Systems on December 23, 2012| 5 Comments »
Ablation Devices Market to 2023 – Global Market Forecast and Trends Analysis by Technology, Devices & Applications
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 7/31/2018
Ablation devices are at present utilized as a part of shifted medicinal services ranges, for example, gynecology, dermatology, cardiology, orthopedic, neurology and a few others. Worldwide development in inclination for negligibly intrusive methodology is driving the interest for Ablation devices. Rising awareness in patient populace about accessibility and advantages from ablation treatments and defeating the cost limitations of regular medications are additionally expected to bolster the development of this market. Where regular radiation treatments have been successful and been received because of high awareness levels, developing advances, for example, hydro-mechanical removal, microwave and aqueous are expanding trusts among patients and healthcare specialist organizations.
How Big is the Global Ablation Devices Market?
The Global Ablation Devices Market is expected to exceed more than US$ 20.99 Billion by 2023 at a CAGR of 9% in the given forecast period.
The major driving factors of Global Ablation Devices Market are as follows:
- Increasing aging population
- Increasing incidence of cancer and cardiovascular diseases
- Rising adoption of minimally invasive procedures
- Development repayment scenario in established markets
- Expansion of next-generation ablation products and technologies
- Growing number of ablation procedures
- Expanding funding for the development of novel ablation device
The restraining factors of Global Ablation Devices Market are as follows:
- Healthcare cost control measures
- Strict regulatory approvals
- Challenges in therapeutic procedure
SOURCE
https://www.marketresearchengine.com/ablation-devices-market
Ablation Devices Market to 2016 – Global Market Forecast and Trends Analysis by Technology, Devices & Applications
http://www.marketsandmarkets.com/Market-Reports/ablation-devices-market-791.html
- Radiofrequency
- Cryoablation
- Microwave
- Ultrasound
- Hydrothermal
- Radiation
- Cardiac
- Cancer
- Gynecology
Ablation procedure refers to a minimally invasive surgical procedure which involves either destruction or removal of diseased or unnecessary tissue to cure the disease. It provides successful form of surgical option that has gradually become a popular alternative over invasive procedure amongst physicians and patients. The principal advantage of these procedures over surgery is short recovery time, short length scars, low risk of infection, less blood loss, and shorter hospital stays.
The global ablation devices market was valued at $7.5 billion in 2011 and is poised to grow at a CAGR of 10.5% to reach $12.4 billion by 2016. The ablation market is broadly segmented into two classes, namely, thermal and non-thermal technologies. Thermal segment consists of technologies such as electrical, radiation, light, radiofrequency, ultrasound, microwave, and hydrothermal and non-thermal segment includes cryoablation and hydromechanical. Ablation devices have applications in myriad clinical areas such as cancer / tumor, cardiac, ophthalmology, urology, gynecology and orthopedics.
Ablation procedures have witnessed significant growth in the recent years, which are attributable to factors such as growing healthcare expenditure, favorable demographics and cost effectiveness over tradition surgical procedures. Moreover, increasing applications in cancer and cardiac segment are fueling the market growth.
Factors such as advancements in technology, increasing demand for minimally invasive surgical procedures, growing baby boomers population (especially in U.S., Japan and Western European countries) are driving the market. The incidence cases of chronic diseases is expected to rise continuously in the coming years, because with increasing age, the risk of developing chronic diseases such as cancer, cardiovascular disorders, gynaecological, and orthopaedic problems increases. The ablation devices market for treating these diseases would show significant growth in the forecast period. The principal advantage of ablation procedures over surgery is short recovery time, short surgical timelines, low risk of infection, minimal damage to the healthy tissue, less blood loss, and shorter hospital stays.
Radiation therapy accounted for the largest share of 41% of the total ablation technologies market in 2011. The major driver of radiation therapy is the fact that it is applicable to any form of cancer ranging from soft tissue such as liver, lungs to bone metastases. Compared to most other techniques, radiation therapy is considered to be effective in all cancer scenarios, thus it is a single treatment for control of cancer used by most radiologists. It is expected that, radiation therapy devices will continue to enjoy the majority share in the ablation devices market for at least another decade owing to its broad scope of use, different methods of application, stable acceptance in population, and high level of awareness as compared to newly introduced ablation techniques such as hydrothermal, microwave and hydromechanical ablation.
Americas is the biggest market for ablation devices, followed by Europe. However, Asian countries represent the fastest growing markets and factors such as high patient pool, growing preferences to MIS, geographical expansion of market players, increased government investment in healthcare facilities especially in rural areas, westernization in life style and dietary habits, increasing healthcare expenditure & improving medical insurance plans are driving the ablation devices market.
Report includes company profiles of major players such as Accuray (U.S.), Alcon Laboratories Inc. (U.S.), AngioDynamics Inc. (U.S.), Arthrocare Corporation (U.S.), Atricure Inc. (U.S.), Biosense Webster (U.S.), Boston Scientific (U.S.), BSD Medical Corporation (U.S.), C.R. Bard Inc. (U.S.), ConMed Corporation (U.S.), Covidien (Ireland), Elekta AB ( Sweden), Galil Medical Ltd. (Israel), Medtronic Inc. (U.S.), Misonix Inc. (U.S.), nContact Surgical Inc. (U.S.), Olympus Corporation (Japan), Smith & Nephew (U.K.), St. Jude Medical (U.S.), Urologix Inc. (U.S.) and Varian Medical Systems Inc. (U.S.).
Scope of the Report
This research report categorizes the market for ablation devices into the following segments:
Global ablation devices market, by technology
- Thermal
- Electrical
- Radiation
- Light
- Radiofrequency
- Ultrasound
- Microwave
- Hydrothermal
- Non-thermal
- Cryoablation
- Hydromechanical
Global ablation devices market, by products
- Electrical – Electrical ablators and electronic brachytherapy
- Radiation – Brachytherapy, Intensity modulated radiation therapy, Image guided radiotherapy, Stereotactic Radiotherapy (SRT), Stereotactic body radiation therapy, Nano-radiation therapy and Proton beam therapy
- Light – Cold lasers, Excimer lasers and ultraviolet B lasers
- Radiofrequency – Temperature controlled devices, fluid cooled device and robotic navigation–catheter manipulation systems
- Ultrasound – High intensity focused ultrasound, Magnetic Resonance Imaging-Guided Focused Ultrasound (MRI-FUS), Ultrasound surgical systems and shock wave therapy
- Microwave – Microwave thermotherapy
- Hydrothermal – Endometrial hydrothermal balloon ablation devices
- Cryoablation – Tissue contact probe, cryogen spray probe and epidermal and subcutaneous cryoablation devices
Global ablation devices market, by applications
-
- Cancer
- Cardiac
- Ophthalmology
- Gynecology
- Urology
- Orthopedics
TABLE OF CONTENTS
1 INTRODUCTION
1.1 KEY TAKE AWAYS
1.2 REPORT DESCRIPTION
1.3 MARKETS COVERED
1.4 STAKEHOLDERS
1.5 RESEARCH METHODOLOGY
1.5.1 MARKET SIZE
1.5.2 MARKET SHARE
1.5.3 KEY DATA POINTS FROM SECONDARY SOURCES
1.5.4 KEY DATA POINTS FROM PRIMARY SOURCES
1.5.5 ASSUMPTIONS
2 EXECUTIVE SUMMARY
3 MARKET OVERVIEW
3.1 INTRODUCTION
3.2 ABLATION TECHNOLOGIES MARKET
3.3 ABLATION APPLICATION MARKET
3.4 MARKET DYNAMICS
3.4.1 DRIVERS
3.4.1.1 Technological advancements
3.4.1.2 Increasing procedures through minimal invasive surgery
3.4.1.3 Increasing aging population with higher risk of chronic diseases
3.4.2 RESTRAINTS
3.4.2.1 Pricing and reimbursement issues
3.4.2.2 Increasing regulatory agencies pressures
3.4.3 OPPORTUNITIES & CHALLENGES
3.4.3.1 Emerging markets
3.4.3.2 Technical and educational challenges
3.5 BURNING ISSUES
3.5.1 INCREASING RESEARCH IN CARDIAC ABLATION
3.6 MARKET SHARE ANALYSIS
4 ABLATION MARKET, BY TECHNOLOGY
4.1 INTRODUCTION
4.2 THERMAL
4.2.1 ELECTRICAL
4.2.2 RADIATION
4.2.3 RADIOFREQUENCY
4.2.4 LIGHT
4.2.5 ULTRASOUND
4.2.6 MICROWAVE
4.2.7 HYDROTHERMAL
4.3 NON-THERMAL
4.3.1 CRYOTHERAPY
4.3.2 HYDROMECHANICAL
5 ABLATION TECHNOLOGY MARKET, BY PRODUCTS
5.1 ELECTRICAL
5.1.1 ELECTRICAL ABLATORS
5.1.1.1 Argon Plasma/Beam coagulators
5.1.1.2 Irreversible electroporation
5.1.2 ELECTRONIC BRACHYTHERAPY
5.2 RADIATION
5.2.1 BRACHYTHERAPY
5.2.1.1 High-Dose-Rate (HDR) brachytherapy
5.2.1.2 Pulsed-Dose-Rate brachytherapy
5.2.1.3 Permanent seed brachytherapy or Low-Dose-Rate (LDR) brachytherapy
5.2.2 STEREOTACTIC RADIOSURGERY & STEREOTACTIC RADIOTHERAPY
5.2.3 IMAGE GUIDED RADIATION THERAPY (IGRT)
5.2.4 INTENSITY-MODULATED RADIATION THERAPY (IMRT)
5.2.5 STEREOTACTIC BODY RADIATION THERAPY (SBRT)
5.2.6 PROTON BEAM THERAPY
5.3 RADIOFREQUENCY
5.3.1 TEMPERATURE CONTROLLED RADIOFREQUENCY ABLATION DEVICES
5.3.2 FLUID COOLED RF ABLATION
5.3.3 THE ROBOTIC CATHETER MANIPULATION SYSTEM
5.4 LIGHT/LASER
5.4.1 COLD LASERS
5.4.2 EXCIMER LASERS
5.5 ULTRASOUND
5.5.1 HIGH INTENSITY FOCUSED ULTRASOUND (HIFU)
5.5.2 MAGNETIC RESONANCE GUIDED ULTRASOUND MRGFUS
5.5.3 ULTRASONIC SURGICAL SYSTEMS
5.5.4 EXTRACORPOREAL SHOCKWAVE LITHOTRIPSY
5.6 MICROWAVE ABLATION
5.6.1 MICROWAVE THERMOTHERAPY
5.7 HYDROTHERMAL ABLATION
5.7.1 ENDOMETRIAL HYDROTHERMAL BALLOON ABLATION DEVICES
5.8 CRYOABLATION
5.8.1 TISSUE CONTACT PROBE
5.8.2 TISSUE SPRAY PROBE
5.8.3 EPIDERMAL AND SUBCUTANEOUS CRYOABLATION DEVICES
6 ABLATION TECHNOLOGY MARKET, BY APPLICATIONS
6.1 INTRODUCTION
6.2 CANCER
6.3 CARDIOVASCULAR
6.4 OPHTHALMOLOGY
6.5 GYNECOLOGY
6.6 UROLOGY
6.7 ORTHOPEDICS
6.8 OTHERS
7 GEOGRAPHICAL ANALYSIS
7.1 INTRODUCTION
7.2 AMERICAS
7.3 EUROPE
7.4 ASIA-PACIFIC
7.5 ROW
8 COMPETITIVE LANDSCAPE
8.1 INTRODUCTION
8.2 MERGERS & ACQUISITIONS
8.3 AGREEMENTS, PARTNERSHIPS, COLLABORATIONS, JOINT VENTURES
8.4 NEW PRODUCT LAUNCHES
8.5 PIPELINE DEVELOPMENTS
8.6 OTHER DEVELOPMENTS
9 COMPANY PROFILES
9.1 ACCURAY INC.
9.1.1 OVERVIEW
9.1.2 FINANCIALS
9.1.3 PRODUCTS & SERVICES
9.1.4 STRATEGY
9.1.5 DEVELOPMENTS
9.2 ALCON LABORATORIES INC.
9.2.1 OVERVIEW
9.2.2 FINANCIALS
9.2.3 PRODUCTS & SERVICES
9.2.4 STRATEGY
9.2.5 DEVELOPMENTS
9.3 ANGIODYNAMICS INC.
9.3.1 OVERVIEW
9.3.2 FINANCIALS
9.3.3 PRODUCTS & SERVICES
9.3.4 STRATEGY
9.3.5 DEVELOPMENTS
9.4 ARTHROCARE CORPORATION
9.4.1 OVERVIEW
9.4.2 FINANCIALS
9.4.3 PRODUCTS & SERVICES
9.4.4 STRATEGY
9.4.5 DEVELOPMENTS
9.5 ATRICURE INC.
9.5.1 OVERVIEW
9.5.2 FINANCIALS
9.5.3 PRODUCTS & SERVICES
9.5.4 STRATEGY
9.5.5 DEVELOPMENTS
9.6 BIOSENSE WEBSTER INC.
9.6.1 OVERVIEW
9.6.2 PRODUCTS & SERVICES
9.6.3 STRATEGY
9.6.4 DEVELOPMENTS
9.7 BOSTON SCIENTIFIC CORPORATION
9.7.1 OVERVIEW
9.7.2 FINANCIALS
9.7.3 PRODUCTS & SERVICES
9.7.4 STRATEGY
9.7.5 DEVELOPMENTS
9.8 BSD MEDICAL CORPORATION
9.8.1 OVERVIEW
9.8.2 FINANCIALS
9.8.3 PRODUCTS & SERVICES
9.8.4 STRATEGY
9.8.5 DEVELOPMENTS
9.9 C.R. BARD INC.
9.9.1 OVERVIEW
9.9.2 FINANCIALS
9.9.3 PRODUCTS & SERVICES
9.9.4 STRATEGY
9.9.5 DEVELOPMENTS
9.10 CONMED CORPORATION
9.10.1 OVERVIEW
9.10.2 FINANCIALS
9.10.3 PRODUCTS & SERVICES
9.10.4 STRATEGY
9.10.5 DEVELOPMENTS
9.11 COVIDIEN PLC
9.11.1 OVERVIEW
9.11.2 FINANCIALS
9.11.3 PRODUCTS & SERVICES
9.11.4 STRATEGY
9.11.5 DEVELOPMENTS
9.12 ELEKTA AB
9.12.1 OVERVIEW
9.12.2 FINANCIALS
9.12.3 PRODUCTS & SERVICES
9.12.4 STRATEGY
9.12.5 DEVELOPMENTS
9.13 GALIL MEDICAL LTD.
9.13.1 OVERVIEW
9.13.2 FINANCIALS
9.13.3 PRODUCTS & SERVICES
9.13.4 STRATEGY
9.13.5 DEVELOPMENTS
9.14 MEDTRONIC INC.
9.14.1 OVERVIEW
9.14.2 FINANCIALS
9.14.3 PRODUCTS & SERVICES
9.14.4 STRATEGY
9.14.5 DEVELOPMENTS
9.15 MISONIX INC.
9.15.1 OVERVIEW
9.15.2 FINANCIALS
9.15.3 PRODUCTS & SERVICES
9.15.4 STRATEGY
9.15.5 DEVELOPMENTS
9.16 NCONTACT SURGICAL INC.
9.16.1 OVERVIEW
9.16.2 FINANCIALS
9.16.3 PRODUCTS & SERVICES
9.16.4 STRATEGY
9.16.5 DEVELOPMENTS
9.17 OLYMPUS CORPORATION
9.17.1 OVERVIEW
9.17.2 FINANCIALS
9.17.3 PRODUCTS & SERVICES
9.17.4 STRATEGY
9.17.5 DEVELOPMENTS
9.18 SMITH & NEPHEW
9.18.1 OVERVIEW
9.18.2 FINANCIALS
9.18.3 PRODUCTS & SERVICES
9.18.4 STRATEGY
9.18.5 DEVELOPMENTS
9.19 ST. JUDE MEDICAL INC.
9.19.1 OVERVIEW
9.19.2 FINANCIALS
9.19.3 PRODUCTS & SERVICES
9.19.4 STRATEGY
9.19.5 DEVELOPMENTS
9.20 UROLOGIX INC.
9.20.1 OVERVIEW
9.20.2 FINANCIALS
9.20.3 PRODUCTS & SERVICES
9.20.4 STRATEGY
9.20.5 DEVELOPMENTS
9.21 VARIAN MEDICAL SYSTEMS INC.
9.21.1 OVERVIEW
9.21.2 FINANCIALS
9.21.3 PRODUCTS & SERVICES
9.21.4 STRATEGY
9.21.5 DEVELOPMENTS
Please visit http://www.marketsandmarkets.com/knowledge-process-outsourcing-services.asp to specify your custom Research Requirement
SOURCE:
http://www.marketsandmarkets.com/Market-Reports/ablation-devices-market-791.html
Partial Nephrectomy: Similar outcomes for robot-aided vs. conventional surgery
Posted in Bio Instrumentation in Experimental Life Sciences Research, CANCER BIOLOGY & Innovations in Cancer Therapy, Cell Biology, Signaling & Cell Circuits, tagged Invasiveness of surgical procedures, Laparoscopic surgery, Nephrectomy, PSA, UC San Diego School of Medicine, University of Michigan on August 9, 2012| 1 Comment »
Reporter: Aviva Lev-Ari, PhD, RN
A Matched Comparison of Perioperative Outcomes of a Single Laparoscopic Surgeon Versus a Multisurgeon Robot-Assisted Cohort for Partial Nephrectomy
The Journal of Urology
Volume 188, Issue 1 , Pages 45-50, July 2012
 Jonathan S. Ellison
Jonathan S. Ellison- Jeffrey S. Montgomery
- J. Stuart Wolf Jr.
- Khaled S. Hafez
- David C. Miller
- Alon Z. Weizer

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
,
,
,
,
,
Department of Urology, University of Michigan, Ann Arbor, Michigan
Received 17 October 2011 published online 14 May 2012.
Purpose
Minimally invasive nephron sparing surgery is gaining popularity for small renal masses. Few groups have evaluated robot-assisted partial nephrectomy compared to other approaches using comparable patient populations. We present a matched pair analysis of a heterogeneous group of surgeons who performed robot-assisted partial nephrectomy and a single experienced laparoscopic surgeon who performed conventional laparoscopic partial nephrectomy. Perioperative outcomes and complications were compared.
Materials and Methods
All 249 conventional laparoscopic and robot-assisted partial nephrectomy cases from January 2007 to June 2010 were reviewed from our prospectively maintained institutional database. Groups were matched 1:1 (108 matched pairs) by R.E.N.A.L. (radius, exophytic/endophytic properties, nearness of tumor to collecting system or sinus, anterior/posterior, location relative to polar lines) nephrometry score, transperitoneal vs retroperitoneal approach, patient age and hilar nature of the tumor. Statistical analysis was done to compare operative outcomes and complications.
Results
Matched analysis revealed that nephrometry score, age, gender, tumor side and American Society of Anesthesia physical status classification were similar. Operative time favored conventional laparoscopic partial nephrectomy. During the study period robot-assisted partial nephrectomy showed significant improvements in estimated blood loss and warm ischemia time compared to those of the experienced conventional laparoscopic group. Postoperative complication rates, and complication distributions by Clavien classification and type were similar for conventional laparoscopic and robot-assisted partial nephrectomy (41.7% and 35.0%, respectively).
Conclusions
Robot-assisted partial nephrectomy has a noticeable but rapid learning curve. After it is overcome the robotic procedure results in perioperative outcomes similar to those achieved with conventional laparoscopic partial nephrectomy done by an experienced surgeon. Robot-assisted partial nephrectomy likely improves surgeon and patient accessibility to minimally invasive nephron sparing surgery.
Key Words: kidney , kidney neoplasms , nephrectomy , laparoscopy , robotics
Abbreviations and Acronyms: CLPN, conventional laparoscopic partial nephrectomy, EBL, estimated blood loss, eGFR,estimated glomerular filtration rate, ICU, intensive care unit, LOS, length of stay, RAPN, robot-assisted partial nephrectomy,SRM, small renal mass, WIT, warm ischemia time
Similar outcomes for robot-aided, conventional nephrectomy June 22, 2012 in Other Robot-assisted and conventional laparoscopic partial nephrectomies have similar outcomes and complication rates, according to a study published in the July issue of The Journal of Urology. (HealthDay) — Robot-assisted and conventional laparoscopic partial nephrectomies have similar outcomes and complication rates, according to a study published in the July issue of The Journal of Urology. Ads by Google Prostate Cancer Treatment – Expert Prostate Cancer Treatment & Care – View Video to Learn More! – http://www.TuftsMedicalCenter.tv Prostate Cancer Treatment – Learn about Watchful Waiting. Get a Second Opinion at BIDMC. – http://www.BIDMC.org Jonathan S. Ellison, M.D., from the University of Michigan in Ann Arbor, and colleagues compared perioperative outcomes and complications from conventional laparoscopic and robot-assisted partial nephrectomy cases from January 2007 to June 2010. Robot-assisted partial nephrectomies were performed by a heterogeneous group of surgeons, while a single experienced laparoscopic surgeon performed the conventional procedures. One hundred eight pairs of patients were matched by age, hilar nature of the tumor, approach, and R.E.N.A.L. (radius, exophytic/endophytic properties, nearness of tumor to collecting system or sinus, anterior/posterior, location relative to polar lines) nephrometry score. The researchers found that nephrometry score, age, gender, tumor side, and American Society of Anesthesia physical status classification were similar between the groups. Conventional laparoscopic partial nephrectomy had better operative time. Robot-assisted partial nephrectomy showed significant improvements in estimated blood loss and warm ischemia time compared to the conventional laparoscopic group. The postoperative complication rates and complication distributions by Clavien classification and type were similar for both groups (41.7 percent for the conventional group and 35.0 percent for the robot-assisted group). “Robot-assisted partial nephrectomy has a noticeable but rapid learning curve,” write the authors. “After it is overcome the robotic procedure results in perioperative outcomes similar to those achieved with conventional laparoscopic partial nephrectomy done by an experienced surgeon.” More information: Abstract Full Text (subscription or payment may be required) Journal reference: Journal of Urology
http://medicalxpress.com/news/2012-06-similar-outcomes-robot-aided-conventional-nephrectomy.html
What does your PSA score, level, reading, test mean?
By itself, a PSA reading does not mean very much. There are many possible causes of the rise in the PSA reading. The most common of these reasons is an enlarged, inflamed, or infected prostate. So a high PSA score does not necessarily indicate prostate cancer.
Unfortunately there is no failsafe test or methods at this time that can differentiate between a high PSA level caused by inflammation of the prostate or infection of the prostate or prostate cancer. At best doctors use a statistical model, which seeks to predict your chances of having prostate cancer. But that is purely a statistical construct and does not actually predict your specific and personal situation at all.
Nonetheless, an elevated PSA reading should not be ignored. It is a good indicator, certainly the best we have, and you should take precautionary action.
If you have a high PSA reading you need to return your prostate back to good health. You need to make important changes to your diet. You also need to have regular exercise. A third and equally important part of my recommendation is to take appropriate natural supplements.
I provide a roadmap in my guide “All about the Prostate”. Most men who follow my roadmap will see their PSA levels come down. It will return their prostate to good health.
INDICATION
ZYTIGA® (abiraterone acetate) in combination with prednisone is indicated for the treatment of patients with metastatic castration-resistant prostate cancer (mCRPC) who have received prior chemotherapy containing docetaxel.
IMPORTANT SAFETY INFORMATION
Contraindications – ZYTIGA® (abiraterone acetate) may cause fetal harm (Pregnancy Category X) and is contraindicated in women who are or may become pregnant.
Hypertension, Hypokalemia and Fluid Retention Due to Mineralocorticoid Excess –Use with caution in patients with a history of cardiovascular disease or with medical conditions that might be compromised by increases in hypertension, hypokalemia, and fluid retention. ZYTIGA® may cause hypertension, hypokalemia, and fluid retention as a consequence of increased mineralocorticoid levels resulting from CYP17 inhibition. Safety has not been established in patients with LVEF <50% or New York Heart Association (NYHA) Class III or IV heart failure because these patients were excluded from the randomized clinical trial. Control hypertension and correct hypokalemia before and during treatment. Monitor blood pressure, serum potassium, and symptoms of fluid retention at least monthly.
Adrenocortical Insufficiency (AI) – AI has been reported in clinical trials in patients receiving ZYTIGA® in combination with prednisone, after an interruption of daily steroids and/or with concurrent infection or stress. Use caution and monitor for symptoms and signs of AI if prednisone is stopped or withdrawn, if prednisone dose is reduced, or if the patient experiences unusual stress. Symptoms and signs of AI may be masked by adverse reactions associated with mineralocorticoid excess seen in patients treated with ZYTIGA®. Perform appropriate tests, if indicated, to confirm AI. Increased dosages of corticosteroids may be used before, during, and after stressful situations.
Hepatotoxicity – Increases in liver enzymes have led to drug interruption, dose modification, and/or discontinuation. Monitor liver function and modify, withhold, or discontinue ZYTIGA® dosing as recommended (see Prescribing Information for more information). Measure serum transaminases [alanine aminotransferase (ALT) and aspartate aminotransferase (AST)] and bilirubin levels prior to starting treatment with ZYTIGA®, every two weeks for the first three months of treatment, and monthly thereafter. Promptly measure serum total bilirubin, AST, and ALT if clinical symptoms or signs suggestive of hepatotoxicity develop. Elevations of AST, ALT, or bilirubin from the patient’s baseline should prompt more frequent monitoring. If at any time AST or ALT rise above five times the upper limit of normal (ULN) or the bilirubin rises above three times the ULN, interrupt ZYTIGA® treatment and closely monitor liver function.
Food Effect – ZYTIGA® must be taken on an empty stomach. Exposure of abiraterone increases up to 10-fold when abiraterone acetate is taken with meals. No food should be eaten for at least two hours before the dose of ZYTIGA® is taken and for at least one hour after the dose of ZYTIGA® is taken. Abiraterone Cmax and AUC0-∞ (exposure) were increased up to 17- and 10-fold higher, respectively, when a single dose of abiraterone acetate was administered with a meal compared to a fasted state.
Adverse Reactions – The most common adverse reactions (≥ 5%) are joint swelling or discomfort, hypokalemia, edema, muscle discomfort, hot flush, diarrhea, urinary tract infection, cough, hypertension, arrhythmia, urinary frequency, nocturia, dyspepsia, fractures and upper respiratory tract infection.
Drug Interactions – ZYTIGA® is an inhibitor of the hepatic drug-metabolizing enzyme CYP2D6. Avoid co-administration with CYP2D6 substrates that have a narrow therapeutic index. If an alternative cannot be used, exercise caution and consider a dose reduction of the CYP2D6 substrate. Additionally, abiraterone is a substrate of CYP3A4 in vitro. Strong inhibitors and inducers of CYP3A4 should be avoided or used with caution.
Use in Specific Populations – The safety of ZYTIGA® in patients with baseline severe hepatic impairment has not been studied. These patients should not receive ZYTIGA®.
Follow Blog via Email
Join 2,041 other subscribers-
Recent Posts
- Urgent Request for Action on Proposed Rule Affecting Federal Funding Grant Review July 7, 2026
- 2026 Tang Prize in Biopharmaceutical Science Awarded to Three Pioneers of Cellular Immunotherapy Revolutionizing Treatments for Blood Cancers and Solid Tumors July 5, 2026
- Protected: KOL on Competitive Dynamics: LPBI Group’s Founder’s Radar Screens on AI in Health, Life Sciences & BioPharma June 15, 2026
- Tumor Infiltrating Lymphocytes (TIL) as a first of kind FDA approved immunotherapy for cancer June 12, 2026
- A Systematic Analysis of Competitive Dynamics in the AI Revolution — Strategic Relevance to LPBI Group’s Mission – Alex Wissner-Gross Daily Newsletters by KOL (March 1 – June 10, 2026, to be extended to Present) June 11, 2026
- In Memoriam: Professor Yitzhak Apeloig, President and Distinguised Professor of the Technion June 4, 2026
- Top VC Investors in AI / Health AI in 2026 May 26, 2026
- Grok thinks like PhDs – Hybrid Model for Autonomous Update of Doctoral Dissertations with Original PhD Student Author editing and acceptance of Grok’s updated output. 3rd Joint article, a pilot study for Validation of an Autonomous Journal Articles Updating System (AJAUS) tested on Autonomous Update of Aviva Lev-Ari, PhD, RN Doctoral Thesis, UC, Berkeley, 1983. January 31, 2026
- 2026 World Economic Forum, 1/19 – 1/23/2026, Davos, Switzerland, LPBI Group’s KOLs interpretation of AI in Health Videos January 24, 2026
- Evolving LPBI Group’s Portfolio of Intellectual Properties (IP): From 2021 Vision to 2026 Reality January 12, 2026
Archives
Categories
Meta