Synopsis for AI & Machine Learning in Clinical Trials, APRIL 12, 2018 PFIZER INNOVATION RESEARCH LAB – CAMBRIDGE, MA
Reporter: Aviva Lev-Ari, PhD, RN
Recap Book
Aviva Lev-Ari, PhD, RN, Director and Founder of LPBI Group, will attend and cover in Real Time the Conference
@pharma_BI
@AVIVA1950
- Tweets for AI and Machine Learning in Clinical Trials April 12th, 2018 hosted at Pfizer’s Innovation Research Lab in Cambridge, MA @AVIVA1950 @pharma_BI
https://pharmaceuticalintelligence.com/2018/04/12/tweets-for-ai-and-machine-learning-in-clinical-trials-april-12th-2018-hosted-at-pfizers-innovation-research-lab-in-cambridge-ma-aviva1950-pharma_bi/

About Aviva Lev-Ari, PhD, RN and LPBI Group

AI and Machine Learning in Clinical Trials
April 12th, 2018 hosted at Pfizer’s Innovation Research Lab in Cambridge, MA
1 Portland St, Cambridge, MA 02139
With case studies from Pfizer, Novartis, Merck, AstraZeneca, MIT, Takeda, Sanofi & more, you will not
want to miss the latest in leveraging AI and Machine Learning in Clinical Trials.
#Pfizer #Merck #Sanofi #AstraZeneca #Novartis #Takeda #BMS #Biogen #GSK #MIT #Medable #Saama #RapidMiner
100+ innovators, data scientists, informatics, senior clinical trials execs & tech experts will convene to
discuss advances in artificial intelligence, machine learning, & clinical study data analytics.
Faculty of Advisors and Speakers:
Dan Karlin, Head of Digital Medical, Informatics, Regulatory Strategy, Pfizer
Joseph Lehar, Exec. Dir, Computational Biology, Merck
David Tester, Head, Data Sciences & Engineering, Chief Data Office, Sanofi
Bhaskar Dutta, Principal Scientist, Advanced Analytics Center, AstraZeneca
Jonas Dorn, Project Manager, Digital Health, Novartis
Jyoti Shah, Assoc. Dir, Data Development, Merck
Raj Bandaru, Sr. Director, Data Sciences Strategy, Sanofi
Ronald Dorenbos, Assoc. Dir, Materials Innovation, Takeda
Zeshan Farooqui, Sr. Clinical Site Manager, BMS
Shwen Gwee, Head, Digital Strategy, Global Clinical Ops, Biogen
Munther Baara, Head, New Clinical Paradigm, Pfizer
Shyamal Patel, Sr. Manager, PfIRe Lab, Pfizer
Bill Tobia, Lead Clinical Research Instructor, GSK
Regina Barzilay, Delta Electronics Professor, MIT
Amir Lahav, Digital Innovation Lead, Pfizer
Michelle Longmire, CEO, Medable
Karim Damji, SVP Product and Marketing, Saama
Malai Sankarasubbu, VP, AI Innovation, Saama
Ingo Mierswa, Founder/President, RapidMiner
You can take a look at the latest agenda here: http://panagorapharma.com/ai/schedule/
You can register at the following link using the promo code BOSTONBIOTECH25 for 25% off
registrations: https://panagorapharma.com/ai/registration/
If you have any other questions, you can reach out to the organizer:
Doug Lavender
CoFounder
PanAgora Pharma
Doug@panagoraconferences.com
Phone: 203-253- 6401
CORE THEMES:
1. An Exploration of Machine Learning for Clinical Study Data
2. Natural Language Processing (NLP) for Patient Voice Analysis via Social Channels
3. Machine Learning and Artificial Intelligence for Recruitment
4. The Potential of Machine Learning and AI for Adverse Event Identification
5. Real-time Patient Data Analysis
AGENDA for Thursday, April 12th, 2018
8:00 – 9:00 am Conference Registration Open in Pfizer Lobby – 1 Portland Street, Cambridge, MA
9:00 – 9:10 am Opening Remarks from Conference Chairman
Robert “Joe” Mather, Executive Director, Head of Digital Collaborations, Pfizer
9:10 – 9:50 am KEYNOTE PANEL: AI & ML to Support Clinical Trials – Where do we begin?
The internet of things, mHealth, wearable and sensor-enabled devices present an
unprecedented opportunity for accelerated data collection. What does it mean for life
sciences – are we prepared to handle the influx of data, and create valuable visibility to
accelerate trials? Where should we start? What are the best current applications? How can
we leverage AI and Machine Learning for Adverse Event Identification?
David Tester, Head, Data Science & Engineering, Chief Data Office, Sanofi
- Do exploratory AI & ML outside the context of Clinical Trials 1st
Joseph Lehar, Executive Director, Computational Biology, Merck
- Oncology – images of response to treatment are complex, Pathology is assisted by AI
- AI can assist in cell classification
- Biggest opportunity of AI %& ML in Immunology, use non invasive medium even behavioral indicators
- Informed Consent in Clinical Trials
- Development of AI models to avoid bias
- Monitoring the Trials identify signals
Bhaskar Dutta, Principal Scientist, Advanced Analytics Center, AstraZeneca
- Structure exploration in first study, signals used in second study
- Even in Informatics groups there can be and there is resistance to acceptance of AI and ML
- 80%-90% clean the data holistic data view integration and Privacy
- pooling data sets across companies for benefits of sampling: Parkinson Disease case
- Patients Voice in a Biomarker study as partners vs Patients as Customers
Moderator: Robert “Joe” Mather, Exec. Dir, Head of Digital Collaborations, Pfizer
- Data sharing across the organization
- How the audience feel about sharing code not only data
9:50 – 10:20 am CASE STUDY: Making Sense of Sensor Data: A Case Study in Data Quality Evaluation
Bhaskar Dutta, Principal Scientist, Advanced Analytics Center, AstraZeneca
- Making sense of sensor data – 40 clinical data scientists and expanding
- Tactical impact, Strategic build, Horizon Scanning &evaluaiton capabilities, Quantitative Solutions
- % of Healthcare spending of GDP: LOWER THE % BY DIGITAL TECHNOLOGIES
- Improve adherence no need of new drugs
- 70% of Patients are interested in Monitoring their Health digitally
- wearable sensors – will increase the quality of monitoring
- Burden of Chronic disease: i.e., Asthma (23Millions), Diabetes (29Million)
- COst direct and Indirect
- Patient Needs
- Challenging in using digital solutions: Lack of integration,
- Values: to Patients, to HCP, Pharma: Drug discovery, Drug Cost
- Digital-solutions Lifecycle: Pharma perspective: Need characterization, device sensor characterization,
- at AstraZeneca: Project – iPREDICT – individualize PREdiction of DIsease Control using digital sensor Technology
- Device Brands and their Price to Consumer: ZephyrBioPatch, Garmin Vivosmart, MS Band 2, GoBe, HealthPatch MD, BodyGardian, BioPatch
- Usability Survey: Ease of setting up, Ease of use, 1st impression, comfort, likely to recommend
- Data capturing: Missing, quality of recording – data quality evaluation: signal to noise ratio
- poor compliance
- Data Privacy – GPS data is the most PRIVATE: de-identification of IDs, GPS can generate identifiable data
- Integration with other data streams
- Six different Groups: Patient cnetrality, Applications Usability,
- They are hiring in the MD area
10:20 – 10:50 am Using AI and Machine Learning to Improve Clinical Trials
• Clinical trial dedicated mobile apps can improve patient experience in clinical trials and
increase data collection and yield,
• Advanced analytics on patient data
§ HIPAA compliance, data collection & analysis
Michelle Longmire, CEO, Medable
- Enabling Direct personalized medicine
- current process: 1-5 drugs >$2Bil, 12 years
- Apply AI in a Case study on mild cognitive impairment:
- Recruitment,
- Trial (drug efficacy)
- Endpoint (crude assessment)
- AI – From Engagement to Insight:
- Trial Process, – identify Patients in populations before onset of disease
- Discovery, – Adaptive Trials
- Transformation – Digitome, Digital Biomarkers
- Input: Patient reported data – to measure daily progress
- Probabilistic condition for algorithm development
- Input: Smartphone sensors: 6-minute walk
- Input: Contextual data – Location, air quality, weather, disease & crime
- Input: VOICE: Google Home, Amazon Alexa, Apple: Siri
- Input: Devices: fitbit, Tomtom, biovation – Swiss company – 6 paramenters per second: Cognition applications
- Bayesian Nets: Conditional probabilities
- Deep learning: Pathern in data : Problem/data
- Partnering with other Medical Centers
MEDABLE INSIGHT: Signature of Digitome
- AI platform
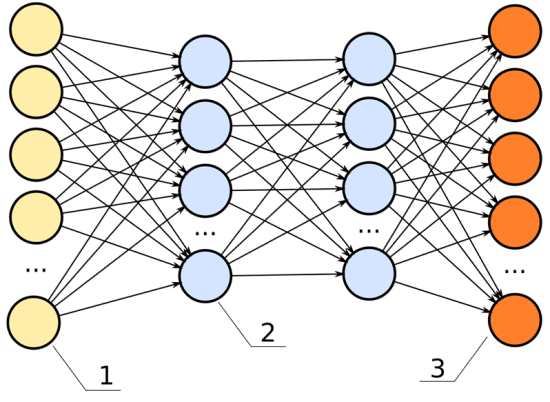
- Choose form anumber of Neural Networks (NN) ‘pattern’ to allow
- Train Multiple NN, Time series Data, Visualization: View Data
- Cerebrum Demo: Correlate patterns
10:50 – 11:10 am NETWORKING COFFEE AND REFRESHMENT BREAK
11:10 – 11:40 am CASE STUDY: Machine Learning for Clinical Study Data
Shyamal Patel, Sr. Manager, PfIRe Lab, Pfizer
SEE Digital Biomarkers Journal
- DIGITAL biomarkers: from algorithms to Endpoints
- Algorithms (gait speed, HR)–>> Biomarkers (Change is stat is it change in Disease stage?)–>>> Endpoints (relevant for target)
- Wearable devices are tight coupled on body for continuous monitoring
- smartphone: Sensor
- connect devices
- iPhone – Sensor packed powerhouse: Movement, Location, Context, Emotion (Camera, microphone)
- 70% of data is unstructured: Text, image, video – SOURCE: IBM
- Why use AI for building digital biomarkers: AI: Data _ Answers =Rules vs classic Programming: Data + rules = Answers
- AI enables:
- Learn efficintly large data sets
- make updates when more data becomes available
- Deploy at scale across platforms
DEEP Learning: automated driving, Object recognition, robotics, speech recognition
Case Study 1: Implement Heuristic algorithms (published in literature) Evaluate Performance (agreement with clinical ratings under controlled conditions) Train Machine Learning Models (Annotation as ground truth) to AI models
- detect hand tremor – Quantify Tremor
Outcomes:
- achieve significant reduction in false positive rate
- strong agreement with ratings provided by trained clinical raters
Case Study 2: Mining the sound signal for biomarkers
Outcomes:
- 85% accuracy in hackaton
Evaluating AI driven Digital Biomarkers:
Accuracy – Problem: Over fitting
Speed
Explainability – How does the model works? – understand the trade offfs
Scalability – do not be a hammer looking for a nail
11:40 – 12:10 pm Accelerating Clinical Trials using Natural Language Understanding
Pharma has a big text problem. Lots of useful information buried in unstructured data
formats that is difficult to use. Natural Language Understanding will help to turn what was
once unusable data into meaningful insights that can be applied to the clinical trial
development continuum. NLU engines also open up the possibility for users to have a more
interactive relationship with their vast data stores using speech or chat messaging in a
conversational experience
Come and see how we are using Natural Language Understanding to solve problems:
• Adverse events in the real world and clinical trials
• Better matched patients for on-going clinical trials
• Hidden associations from interactions between physiology, therapies, and clinical
outcomes
Karim Damji, SVP Product, Saama
Malai Sankarasubbu, VP of AI Research, Saama
- Too many variations
- ADE – Adverse Drug Event extraction from Biomedical Text
Data Manager: Delivers Clinical Data Analytics as a Service using Saama platform
Implementation of dashboard: Smart Assistant for Clinical Operations:
- Initiate a conversation over multiple natural channels of engagement
- Identify intent and entity Need for NLU engine !!!!!
- Intent extractor
- Entity Extractor
- Conversation Experience (CX): One question per one answer – not a good CX
Saama: ChatBot Voice interaction
- Rank studies on Pancreatic Cancer in ClinicalTrials.gov by Inclusion vs Exclusion Criteria
- Entity extraction and Patinet matching for EHR Data
- Protein
- Chemical compound
- Organism
- Environment
- Tissue
- Disease/phenotype
- Gene Ontology Term
12:10 – 12:40 pm CASE STUDY: Bringing Digital Health and Artificial Intelligence to Merck
Merck is building up digital health capabilities to increase patient engagement, improve trial
performance, and develop clearer disease phenotypes. I will describe some efforts across
the organization in this area & provide examples of smart trials / AI collaborations underway.
Joseph Lehar, Executive Director, Computational Biology, Merck
- Digital health innovations at Merck
- quantitative phyenotypes – clearer disease signals
- trial performance – more effective and more efficient
- Patient outcomes – Better ones
- Data analytics & Infrastructure – enabling 1,2,3
- Smart trials: pacient-centric studies
- Pilot studies: Smart dosing, sampling and analytics
- at home vs at clinic
- smart pill packs daily blood spot for PK/DNA, e-Diary
- less expensive sampling
- Key findings: More trials should have smart monitoring
- Future expansion: Better, more relevant, wider: Less invasive , Apply to active clinical trials , scale up to larger populations
- Collaborate with big Technology companies on AI
- Flexible, scientific partnerships
- Projects with like success sooner
- Projects underway or being actively planned
- Value-based models on Trials outcomes
- Cross functional collaborations: Organizations, Projects: i.e., Oncology, Objectives
12:40 – 1:00 pm SINEQUA PRESENTATION
Jeff Evernham, Sinequa
evernham@sinequa.com
- Content of the data: Expand, Link, Enrich, Improve
- Data set Index
- Row IndexStructured and Unstructured (Textual)
- DIscovery: Common variables across all data sets
- Cognitive Analytics: SEARCH, NLP, Integrated ML
- Single study –>> Multiple Studies –> numerical variables –>> Enriched categorical variables Unstructured data
1:00 – 1:50 pm EXECUTIVE NETWORKING LUNCHEON
1:50 – 2:15 pm CASE STUDY: We want to teach a machine to think like a physician, but how do we tell how
a physician thinks?
Inter- and intra-rater variability can severely impact the data quality of our clinical trials. If we
could teach machine learning algorithms to assess patients like experienced physicians, we
would have every patient assessed the exact same way across all the sites in a clinical trial.
As a bonus, we could make these medical assessments available in underserved areas of the
world. However, how can we train a machine learning algorithm on data annotated by
humans, if we know that those human annotations are unreliable? We will present a
framework, and the journey that led us to it, that allows combining the judgments of
multiple human raters into one consensus scale and thus provide high quality ground truth,
an aspect of machine learning that doesn’t always get the attention it deserves.
Jonas Dorn, Digital Solutions Director, Novartis
- Rater consistency is limited given by n-Raters to K-Patients – Human consistency is limited: Disease severity score assigned
- ML –>> Scores are generated
- What is ground truth to be considered GOOD?
- Comparative video rating
- Converting ranking into scores, “true Score”
- True score + uncertainty + rater consistency – compare realization – compare realization to threshold, comes with uncertainty
- Combine all rating by all doctores = continuous consensus score (with uncertainties) vs Coarse ratings (raw/consensus)
- Create consistent score through comparisons
- Conclusion: Humans are bad at absolute ratings but good at comparison
- Comparison-based enable virtual rating
2:15 – 2:45 pm PANEL DISCUSSION: Hearing the Voice of the Patient – How Ambient Listening Devices and Artificial Intelligence Can Improve the Clinical Trial Experience
The healthcare industry, and in particular, the clinical research sector, has recently focused
its attention on achieving “patient-centricity”. Driven by the desire to better engage clinical
trial volunteers, coupled by the need to demonstrate value-added medical products, this
has become much more than the latest buzz word. However, once the trial begins, the
patient oftentimes may feel isolated in the process – quite simply, they need to ask
questions and receive answers that they can understand. Is this an opportunity to effectively & efficiently use ambient listening devices?
How can we leverage AI and Machine Learning for the detection of adverse events, using NLP and other strategies for analysis?
Amir Lahav, Digital Innovation Lead, Rare Disease Research Unit, Pfizer
- speech technology – voice activated mechanism
- voice recording for Ataxia Patients – for interaction with Patients
- Accustic pattern recognition analysis of Human voice detects Asthman or CVD in Patient : voice for detection of disease: Stroke Patient,
Zeshan Farooqui, Sr. Clinical Site Manager, Bristol-Myers Squibb
Malai Sankarasubbu, VP of AI Research, Saama
Moderated by: Bill Tobia, Lead Clinical Research Instructor, GSK
Voice of patient on audio technology
2:45 – 3:15 pm CASE STUDY: Clinical Data Integration from Translational Modeling Using Machine
Learning
Raj Bandaru, Sr. Director, Sr. Director, Translational Informatics, Sanofi
- Clinical Data Integration for Translational Modeling
- Challenges of Data Discovery Integration of Clinical Data
- Automated Data Cataloging
- Data DIscovery – 80% effort
- Crawler – Bayesian machine learning – >> data Catalog (Index) –>> Meta Data (Information) –>>> Elastic Data– >> synonyms and hierarchhical search –>. Ontologies and Access Management
- Probabilistic model –>> no need for complete ontologies
- self learning, self maintaining, meta data management, Data on demand, LOW of no IT support, cost a fraction of dat integration projects
- GOAL: develop a classifier that predicts data class and relevnce to the question being asked
- Metadata driven Risk-based De-Identification Strategy: Internal Use, External Use
- Data Analytics Ask a question using Amazon Alexa
- Data science and knowledge management Team
2:50 – 3:10PM Moving beyond Actigraphy: Using AI to make sense of multi-parameter wearable sensor data
Chris Economos, VP of Business Development, PhysIQ – AI for Personalized Anomaly Detection
- Contnuous Biosensor Data +Deep Learning to Potentially DIagnose Heart Hailure Likelihood of Heart FAilure derived from Activity Alone: Heart Failure vs Normal Vs Cancer Treatment vs COPD
- Activity + HR: Heart Failure vs Normal Vs Cancer Treatment vs COPD
- “baseline” vs “estimates”
- the difference is “Residuals”
- Actual, RR, HR, Higher than Expected: Deterioration vs Improvement
- Chris Economos, VP of Business Development, PhysIQ Case Study: Phase 3 Cardiovascular Clinical Trial: 600 patients, 97 sites, 14 countries, 9 languages 2 CROs
- All Causes Hospitalization vs Worsening HF Hospitalization
- Application of AI to data detection of exacerbation
3:15 – 3:35 pm NETWORKING COFFEE AND REFRESHMENT BREAK
3:35 – 4:05 pm Learning Disease Progression and Patient Stratification Models from Images and Text
Regina Barzilay, Delta Electronics Professor, MIT EECS, MIT Koch Institute for
Integrative Cancer Research
- Predict recurrences, sensitivity to Treatment, LCIS – Lobar Carcinoma In-Situ
- Enabling New Science – NLP Atypia – 7000 cases
- Reducing Over-treatment – 87% excision are of benign tissue
- 31% cancers were visible a year prior to cancer
- Interpretable Neural Models
- Multi-Task Representation Learning: Small sample size: Task “N” Tumor Size change GOALS: Correlate similar tasks
4:05 – 4:25 pm How AI will transform Clinical Trials
Ronald Dorenbos, Associate Director, Materials & Innovation, Takeda
- Patient’s Perspective: AI can help patients to get better faster, present the disease
- Future of clinical Trials: Personalization, Patients becoming the point-of-care, Adherence, Healthier Life Style
- patient acceptance and adoption of digital health and AI are growing
- In Pharma: SImulation Modeling, Predicting reaction to therapies Virtual Clinical Trials
4:25 – 5:00 pm PANEL DISCUSSION: How to make all the Data Machine Learnable?
Raj Bandaru, Sr. Director, Data Sciences Strategy, Sanofi
- advises to use models that will signal noise vs clean the data upfront with endless effort
Jonas Dorn, Digital Solutions Director, Novartis
- Cleaning data MUST be done before modeling
- At present AI will not change the WOrld as fast, future of AI will move slowly
Ingo Mierswa, Founder and President, RapidMiner
- missing data is not an excuse, it worth a chance
- Data Engineering and Data modeling is separate in hands of two groups, optimal modeling requires one group, cooperation and validation both groups need be involved along the entire cycle
- Support the RIGHT to own the data
Jyoti Shah, Associate Director, Data Development, Merck
- A lot of data and high quality of Data
- Digital technology – data collected by machine becomes part of the process
- Patients Centers will disctate the pace of AI adoption, they want to own data
Moderated by: Munther Baara, Head, New Clinical Paradigm, Pfizer
5:00 – 6:30 pm Networking Drinks Reception / END OF CONFERENCE
SOURCE
http://panagorapharma.com/ai/schedule/
Read Full Post »
")