Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Urgent Request for Action on Proposed Rule Affecting Federal Funding Grant Review
Reporter: Stephen J. Williams, Ph.D.
Yesterday I received an email from the Mesothelioma Applied Research Foundation (MARFA), as well as Life Sciences PA and the American Association for Cancer Research (AACR). This was on a little publicized proposed change to the NIH scientific review process allowing the Office of Management and Budget (OMB) to have direct authority over the funding of grants which had passed the rigorous scientific review process. This proposed change by the current administration could negate decision made by NIH grant review panels as well as NIH program project directors and NIH administration as well as other funding agencies.
OMB has put a deadling of July 13, 2026 for comments by the public on this proposed change so it is of urgent matter that US scientists be informed of these potential changes.
I have included the three letters below: from MARFA, Life Sciences PA, and AACR.
From the Mesothelioma Applied Research Foundation
For decades, scientific breakthroughs in mesothelioma have depended on one essential principle: research should be guided by science.
A proposed rule from the Office of Management and Budget (OMB) could weaken that principle by allowing political appointees to override scientific peer review when making federal research funding decisions. It could also allow active federally funded research projects to be terminated if deemed inconsistent with changing agency priorities.
For the mesothelioma community, the stakes are especially high.
As a rare cancer, mesothelioma research already faces significant funding challenges. Every federal grant helps advance promising discoveries, supports clinical trials, and gives patients access to new treatment options. The proposal could also restrict international scientific collaboration—partnerships that are often essential for rare disease research, where researchers must work across borders to enroll enough patients and share critical scientific knowledge.
Please take just a few minutes to submit a public comment asking OMB to protect independent scientific peer review, preserve ongoing federally funded research, and support international collaboration for rare diseases.
The OMB proposal, which is currently accepting public comments, would make significant changes to how research funding decisions are administered across federal agencies, including the NIH and NSF. The public comment period closes in just one week, Monday, July 13, 2026, and public comments can be submitted HERE. However, it is equally important for U.S. Senators and Representatives to hear directly from their constituents on matters like this. We encourage your outreach beyond the public comment period.
For decades, independent, merit-based scientific peer review has been the foundation of federal research funding. Currently, the NIH is investing over $2.5 billion in more than 4,300 research projects across the Commonwealth. These investments have helped establish Pennsylvania as a global leader in research and development for innovative therapies and technologies. The revisions proposed by OMB put in jeopardy the transparency, predictability, and scientific integrity of that process.
Federal research investments are critical to the success of Pennsylvania’s leading life sciences ecosystem. They support scientific discovery at our academic research institutions, foster crucial partnerships with industry, and help advance the therapies and technologies that improve the lives of patients in the Commonwealth, across the country, and around the world. Maintaining certainty, consistency, and confidence in this established research funding process is essential to sustaining scientific progress and continued economic growth.
Life Sciences Pennsylvania is sharing our concerns with members of the Pennsylvania Congressional delegation, as well as submitting public comment reaffirming the importance of preserving an independent, science-driven research funding system. We urge you to share your perspectives by submitting concerns to your U.S. Senators and Representatives HERE.
PHILADELPHIA – The American Association for Cancer Research (AACR) is deeply concerned that the recent action of the White House Office of Management and Budget (OMB) to propose a new set of regulations on how federal grants are awarded and managed is a major threat to the National Institutes of Health (NIH) and its lifesaving mission to accelerate progress for patients with cancer and the hundreds of other diseases that afflict millions of Americans.
AACR strongly opposes many of the changes that OMB has proposed in its recently issued rule, titled “Regulation for Federal Financial Assistance.” A considerable number of the regulations included in the rule, if finalized, will be extremely disruptive to the lifesaving research that the federal government funds and oversees, mainly through NIH.
Therefore, AACR calls on the Administration to abandon this harmful proposal, as proceeding along these lines will irreparably damage NIH, an agency that is widely revered as the world’s leading medical research enterprise for its support of the innovative discoveries and groundbreaking treatments that are increasing survival rates and enhancing the quality of life for patients.
According to OMB, the intention of these proposed revisions is to improve transparency, accountability, and oversight of federal awards while reducing administrative burden and ensuring responsible stewardship of taxpayer resources. While AACR shares these goals and supports efforts to strengthen the effectiveness, integrity, and accountability of federal grant programs, a significant number of the provisions in this proposal would in fact increase administrative complexity, create uncertainty for grant recipients, reduce transparency in funding decisions, and undermine the merit-based processes that have effectively guided federal research investments. In short, this OMB proposal is reckless and does not meet the high U.S. standards required for a meritorious, impactful research grant program.
AACR has identified several especially concerning provisions in this OMB proposal that will severely set back our nation’s medical science enterprise and delay the groundbreaking treatments that are pivotal to improving patient outcomes and saving lives:
OMB proposes to markedly expand the power of political appointees to override expert assessment of scientific merit by subjecting every federal research funding decision to political review. These politically appointed officials are unlikely to have subject-matter expertise and would also be instructed to determine whether grant proposals are aligned with the Administration’s political priorities, regardless of their scientific merit. If political appointees are required to provide oversight of federal grant decisions and are allowed or encouraged to ignore the advice of highly qualified scientists, it will threaten the significant progress in patient outcomes that has been achieved over many decades.The merit review process, in which scientific experts in a particular field are brought together to review scientific proposals and assign scores that are based on the quality of the application and its potential to advance new knowledge, has underpinned many discoveries that have led to major improvements in public health. This objective approach to scientific review establishes a foundation of trust within the broader scientific community and throughout the U.S. population. Revising the rules to establish an environment that sidesteps traditional and transparent scientific metrics will weaken overall confidence in the U.S. research enterprise. [This area corresponds to provision 200.205 in the OMB proposal.]
OMB proposes to expand agency authority to suspend or terminate awards based on changing political priorities at the agency or program goals that no longer align with the Administration’s concept of “Gold Standard Science,” which is a term the Administration uses to terminate research not because it is unsound, but because it does not fit a preferred political or methodological agenda. These suspensions and terminations could take place regardless of whether the recipient is performing the project based on the previously approved scope of work. Therefore, an active grant, including a multi-year award that is already underway, could be terminated because of a political or ideological agenda.This OMB-proposed provision would create uncertainty for researchers, institutions, and patients. As one example, this proposed change may have an adverse effect on patient accrual to cancer clinical trials, as patients with cancer may be less likely to enroll if ongoing support for these clinical trials is uncertain. Cancer research often requires years of sustained investment, and permitting political appointees to discontinue support for a grant or clinical trial after the grant or clinical trial has already been awarded or begun threatens scientific progress, wastes taxpayer resources, and destabilizes research programs and studies on which patients are relying for their survival. [This area corresponds to provisions 200.340; 200.341; and 200.342 in the OMB proposal.]
OMB proposes to create additional barriers to scientific collaboration by imposing undue restrictions on international partnerships that are often essential for making advances against cancer and other human diseases. Modern cancer science relies on global networks of researchers, clinical trial participants, data resources, and specialized expertise. Limiting these collaborations will slow the pace of discovery and innovation. As one example among many, international collaborations are vitally important for pediatric cancer research. Because childhood cancers are rare, pooling global patient data, resources, and expertise accelerates clinical trials, drives breakthroughs in drug-resistant subtypes, and bridges survival disparities across high- and low-income countries. [This area corresponds to provisions 200.202 and 200.220 in the OMB proposal.]
OMB proposes to prohibit all federal funding related to diversity, equity, and inclusion.OMB’s justification includes vague language that could be interpreted in ways that restrict research on cancer disparities, access to care, and differences in outcomes among all patient populations. Cancer touches every community, yet, sadly, its burden is not shared equally. A person’s race, ethnicity, income, ZIP code, insurance status, access to screening, ability to enroll in a clinical trial, and proximity to overall high-quality cancer care shape whether cancer is found early, treated effectively, and ultimately cured. [This area corresponds to provisions 200.218 and 200.300 in the OMB proposal.]
OMB proposes to restrict activities that are fundamental components of innovative scientific research and that are essential to how research findings are shared and translated into patient benefit. Provisions in the OMB proposal to limit funding support for scientific publications, journal subscriptions, and attendance at scientific conferences would hinder the ability of researchers to disseminate discoveries, learn about emerging advances, and establish highly productive collaborations. [This area corresponds to provisions 200.432; 200.454; and 200.461 in the OMB proposal.]
For decades, the framework that supports America’s scientific research enterprise through agencies such as NIH and the National Cancer Institute has fueled transformative discoveries in cancer prevention, detection, treatment, and survivorship. This established system has reduced the U.S. cancer death rate by 35% since 1991, resulting in more than 4.8 million U.S. lives saved. This progress has been made possible because of research funding decisions guided by the rigorous review of grant applications by scientific experts and their assessment of these grants to improve public health—NOT guided by political and ideological considerations.
If this OMB-proposed regulation is ultimately finalized, it will severely weaken the U.S. federal research grant program that has supported American innovation and medical breakthroughs for decades. It will also upend the collaborative and evidence-based model that has resulted in U.S. leadership in cancer research and medical science.
It is imperative that all US scientists respond to this potential disasterous change. NIH grant review panels take their time out of their schedule to volunteer to review grants and committ great effort and time to this labor of love. In addition, those who write the grants have spent countless hours, days and months meticulous preparing exellent grants for review. These scientists show an utmost committment to the conduct of great science and a dedication to their field of expertise. Many volunteer countless hours and resources for their research, the scientific community and for patients. And most importantly, scientists include verbage and material in grants BASED ON SOUND SCIENCE, not their opinions.
Please take some time to respond to your lawmakers before July 13, 2026
Optimism for Future Equality of Access to Healthcare in the Inaugural address as AMA President, Jesse M. Ehrenfeld, MD, MPH | AMA 2023 Annual Meeting of House of Delegates
In his inaugural address as AMA President, Jesse M. Ehrenfeld, MD, MPH, highlights the need for a more inclusive and equitable future in medicine. He shares personal experiences of discrimination and emphasizes the importance of advocacy, addressing health disparities, and fighting against disinformation to ensure equitable care for all patients.
#TUBiol5227: Biomarkers & Biotargets: Genetic Testing and Bioethics
Curator: Stephen J. Williams, Ph.D.
The advent of direct to consumer (DTC) genetic testing and the resultant rapid increase in its popularity as well as companies offering such services has created some urgent and unique bioethical challenges surrounding this niche in the marketplace. At first, most DTC companies like 23andMe and Ancestry.com offered non-clinical or non-FDA approved genetic testing as a way for consumers to draw casual inferences from their DNA sequence and existence of known genes that are linked to disease risk, or to get a glimpse of their familial background. However, many issues arose, including legal, privacy, medical, and bioethical issues. Below are some articles which will explain and discuss many of these problems associated with the DTC genetic testing market as well as some alternatives which may exist.
As you can see,this market segment appears to want to expand into the nutritional consulting business as well as targeted biomarkers for specific diseases.
Rising incidence of genetic disorders across the globe will augment the market growth
Increasing prevalence of genetic disorders will propel the demand for direct-to-consumer genetic testing and will augment industry growth over the projected timeline. Increasing cases of genetic diseases such as breast cancer, achondroplasia, colorectal cancer and other diseases have elevated the need for cost-effective and efficient genetic testing avenues in the healthcare market.
For instance, according to the World Cancer Research Fund (WCRF), in 2018, over 2 million new cases of cancer were diagnosed across the globe. Also, breast cancer is stated as the second most commonly occurring cancer. Availability of superior quality and advanced direct-to-consumer genetic testing has drastically reduced the mortality rates in people suffering from cancer by providing vigilant surveillance data even before the onset of the disease. Hence, the aforementioned factors will propel the direct-to-consumer genetic testing market overt the forecast timeline.
Nutrigenomic Testing will provide robust market growth
The nutrigenomic testing segment was valued over USD 220 million market value in 2019 and its market will witness a tremendous growth over 2020-2028. The growth of the market segment is attributed to increasing research activities related to nutritional aspects. Moreover, obesity is another major factor that will boost the demand for direct-to-consumer genetic testing market.
Nutrigenomics testing enables professionals to recommend nutritional guidance and personalized diet to obese people and help them to keep their weight under control while maintaining a healthy lifestyle. Hence, above mentioned factors are anticipated to augment the demand and adoption rate of direct-to-consumer genetic testing through 2028.
Browse key industry insights spread across 161 pages with 126 market data tables & 10 figures & charts from the report, “Direct-To-Consumer Genetic Testing Market Size By Test Type (Carrier Testing, Predictive Testing, Ancestry & Relationship Testing, Nutrigenomics Testing), By Distribution Channel (Online Platforms, Over-the-Counter), By Technology (Targeted Analysis, Single Nucleotide Polymorphism (SNP) Chips, Whole Genome Sequencing (WGS)), Industry Analysis Report, Regional Outlook, Application Potential, Price Trends, Competitive Market Share & Forecast, 2020 – 2028” in detail along with the table of contents: https://www.gminsights.com/industry-analysis/direct-to-consumer-dtc-genetic-testing-market
Targeted analysis techniques will drive the market growth over the foreseeable future
Based on technology, the DTC genetic testing market is segmented into whole genome sequencing (WGS), targeted analysis, and single nucleotide polymorphism (SNP) chips. The targeted analysis market segment is projected to witness around 12% CAGR over the forecast period. The segmental growth is attributed to the recent advancements in genetic testing methods that has revolutionized the detection and characterization of genetic codes.
Targeted analysis is mainly utilized to determine any defects in genes that are responsible for a disorder or a disease. Also, growing demand for personalized medicine amongst the population suffering from genetic diseases will boost the demand for targeted analysis technology. As the technology is relatively cheaper, it is highly preferred method used in direct-to-consumer genetic testing procedures. These advantages of targeted analysis are expected to enhance the market growth over the foreseeable future.
Over-the-counter segment will experience a notable growth over the forecast period
The over-the-counter distribution channel is projected to witness around 11% CAGR through 2028. The segmental growth is attributed to the ease in purchasing a test kit for the consumers living in rural areas of developing countries. Consumers prefer over-the-counter distribution channel as they are directly examined by regulatory agencies making it safer to use, thereby driving the market growth over the forecast timeline.
Favorable regulations provide lucrative growth opportunities for direct-to-consumer genetic testing
Europe direct-to-consumer genetic testing market held around 26% share in 2019 and was valued at around USD 290 million. The regional growth is due to elevated government spending on healthcare to provide easy access to genetic testing avenues. Furthermore, European regulatory bodies are working on improving the regulations set on the direct-to-consumer genetic testing methods. Hence, the above-mentioned factors will play significant role in the market growth.
Focus of market players on introducing innovative direct-to-consumer genetic testing devices will offer several growth opportunities
Few of the eminent players operating in direct-to-consumer genetic testing market share include Ancestry, Color Genomics, Living DNA, Mapmygenome, Easy DNA, FamilytreeDNA (Gene By Gene), Full Genome Corporation, Helix OpCo LLC, Identigene, Karmagenes, MyHeritage, Pathway genomics, Genesis Healthcare, and 23andMe. These market players have undertaken various business strategies to enhance their financial stability and help them evolve as leading companies in the direct-to-consumer genetic testing industry.
For example, in November 2018, Helix launched a new genetic testing product, DNA discovery kit, that allows customer to delve into their ancestry. This development expanded the firm’s product portfolio, thereby propelling industry growth in the market.
The following posts discuss bioethical issues related to genetic testing and personalized medicine from a clinicians and scientisit’s perspective
Question:Each of these articles discusses certain bioethical issues although focuses on personalized medicine and treatment. Given your understanding of the robust process involved in validating clinical biomarkers and the current state of the DTC market, how could DTC testing results misinform patients and create mistrust in the physician-patient relationship?
Question: If you are developing a targeted treatment with a companion diagnostic, what bioethical concerns would you address during the drug development process to ensure fair, equitable and ethical treatment of all patients, in trials as well as post market?
Articles on Genetic Testing, Companion Diagnostics and Regulatory Mechanisms
Question: What type of regulatory concerns should one have during the drug development process in regards to use of biomarker testing?From the last article on Protecting Your IP how important is it, as a drug developer, to involve all payers during the drug development process?
Can the Public Benefit Company Structure Save US Healthcare?
Curator: Stephen J. Williams, Ph.D.
UPDATED 11/05/2023
Public Benefit Corporation structure in healthcare has actually been around since the 1970s in New Yourk State, when New York City’s new Health and Hospitals Corporation took over the city Department of Hospitals and today runs 11 hospitals and four long-term care facitlites in the city. The following link to an article describes however the problems occuring with Nassau and Westchester hosptial systems, which were converted to New York PBC status in the 1990s. As the article states the financial problems in 2004 which these hospitals encountered
do not stem from their unusual status as public benefit corporations, and might have been even worse off had they not converted
The New York Times article of 2004 “At 2 Hospitals, Fiscal Troubles in the Glare of Public View” highlight in fact the growing problem that all hospitals are encountering, especially on the fiscal side. But it does highlight how to better structure these entities and why full commitment to the PBC structure is necessary.
In 2003 New York State had a record closure of hospitals, and in 2004 Nassau and WestChester were having such fiscal problems it threatened the bond status of those counties. Despite the regular problems hospitals had, critics had said there were two major contributing factors to their woes
the two agencies had not completed their transition from government operations to fully competitve hospitals
as a PBC they bear a costly mission of serving the uninsured
As a PBC the structure allows one to shed cumbersome government rules, giving them the flexibility to conduct business like other hospitals.
In addition they are no longer dependent, in fact now forced, to forgo dependence on public funding and look for independent means of investment. With their semi-independence from government the agencies also are more insulted from political pressure.
However this seemed to be the problem. These agencies were still to dependent on their local government and there was still local political influence on their boards.
UPDATED 3/15/2023
According to Centers for Medicare and Medicare Services (CMS.gov) healthcare spending per capita has reached 17.7percent of GDP with, according to CMS data:
From 1960 through 2013, health spending rose from $147 per person to $9,255 per person, an average annual increase of 8.1 percent.
the National Health Expenditure Accounts (NHEA) are the official estimates of total health care spending in the United States. Dating back to 1960, the NHEA measures annual U.S. expenditures for health care goods and services, public health activities, government administration, the net cost of health insurance, and investment related to health care. The data are presented by type of service, sources of funding, and type of sponsor.
Graph: US National Healthcare Expenditures as a percent of Gross Domestic Product from 1960 to current. Recession periods are shown in bars. Note that the general trend has been increasing healthcare expenditures with only small times of decrease for example 2020 in year of COVID19 pandemic. In addition most of the years have been inflationary with almost no deflationary periods, either according to CPI or healthcare costs, specifically.
U.S. health care spending grew 4.6 percent in 2019, reaching $3.8 trillion or $11,582 per person. As a share of the nation’s Gross Domestic Product, health spending accounted for 17.7 percent.
And as this spending grew (demand for health care services) associated costs also rose but as the statistical analyses shows there was little improvement in many health outcome metrics during the same time.
Graph of the Growth of National Health Expenditures (NHE) versus the growth of GDP. Note most years from 1960 growth rate of NHE has always been higher than GDP, resulting in a seemingly hyperinflationary effect of healthcare. Also note how there are years when this disconnect is even greater, as there were years when NHE grew while there were recessionary periods in the general economy.
It appears that US healthcare may be on the precipice of a transformational shift, but what will this shift look like? The following post examines if the corporate structure of US healthcare needs to be changed and what role does a Public Benefit Company have in this much needed transformation.
Hippocratic Oath
I swear by Apollo the physician, and Asclepius, and Hygieia and Panacea and all the gods and goddesses as my witnesses, that, according to my ability and judgement, I will keep this Oath and this contract:
To hold him who taught me this art equally dear to me as my parents, to be a partner in life with him, and to fulfill his needs when required; to look upon his offspring as equals to my own siblings, and to teach them this art, if they shall wish to learn it, without fee or contract; and that by the set rules, lectures, and every other mode of instruction, I will impart a knowledge of the art to my own sons, and those of my teachers, and to students bound by this contract and having sworn this Oath to the law of medicine, but to no others.
I will use those dietary regimens which will benefit my patients according to my greatest ability and judgement, and I will do no harm or injustice to them.
I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; and similarly I will not give a woman a pessary to cause an abortion.
In purity and according to divine law will I carry out my life and my art.
I will not use the knife, even upon those suffering from stones, but I will leave this to those who are trained in this craft.
Into whatever homes I go, I will enter them for the benefit of the sick, avoiding any voluntary act of impropriety or corruption, including the seduction of women or men, whether they are free men or slaves.
Whatever I see or hear in the lives of my patients, whether in connection with my professional practice or not, which ought not to be spoken of outside, I will keep secret, as considering all such things to be private.
So long as I maintain this Oath faithfully and without corruption, may it be granted to me to partake of life fully and the practice of my art, gaining the respect of all men for all time. However, should I transgress this Oath and violate it, may the opposite be my fate.
Translated by Michael North, National Library of Medicine, 2002.
Much of the following information can be found on the Health AffairsBlog in a post entitled
Limitations of For Profit and Non-Profit Hospitals
For profit represent ~ 25% of US hospitals and are owned and governed by shareholders, and can raise equity through stock and bond markets.
According to most annual reports, the CEOs incorrectly assume they are legally bound as fiduciaries to maximize shareholder value. This was a paradigm shift in priorities of companies which started around the mid 1980s,aphenomenon discussed below.
A by-product of this business goal, to maximize shareholder value, is that CEO pay and compensation is naturally tied to equity markets. A means for this is promoting cost efficiencies, even in the midst of financial hardships.
A clear example of the failure of this system can be seen during the 2020- current COVID19 pandemic in the US. According to the Medicare Payment Advisory Commission, four large US hospitals were able to decrease their operating expenses by $2.3 billion just in Q2 2020. This amounted to 65% of their revenue; in comparison three large NONPROFIT hospitals reduced their operating expense by an aggregate $13 million (only 1% of their revenue), evident that in lean times for-profit will resort to drastic cost cutting at expense of service, even in times of critical demands for healthcare.
Because of their tax structure and perceived fiduciary responsibilities, for-profit organizations (unlike non-profit and public benefit corporations) are not legally required to conduct community health need assessments, establish financial assistance policies, nor limit hospital charges for those eligible for financial assistance. In addition to the difference in tax liability, for-profit, unlike their non-profit counterparts, at least with hospitals, are not funded in part by state or local government. As we will see, a large part of operating revenue for non-profit university based hospitals is state and city funding.
Therefore risk for financial responsibility is usually assumed by the patient, and in worst case, by the marginalized patient populations on to the public sector.
Tax Structure Considerations of for-profit healthcare
Financials of major for-profit healthcare entities (2020 annual)
Non-profit Healthcare systems
Nonprofits represent about half of all hospitals in the US. Most of these exist as a university structure, so retain the benefits of being private health systems and retaining the funding and tax benefits attributed to most systems of higher education. And these nonprofits can be very profitable. After taking in consideration the state, local, and federal tax exemptions these nonprofits enjoy, as well as tax-free donations from contributors (including large personal trust funds), a nonprofit can accumulate a large amount of revenue after expenses. In fact 82 nonprofit hospitals had $33 billion of net asset increase year-over-year (20% increase) from 2016 to 2017. The caveat is that this revenue over expenses is usually spent on research or increased patient services (this may mean expanding the physical infrastructure of the hospital or disseminating internal grant money to clinical investigators, expanding the hospital/university research assets which could result in securing even larger amount of external funding from government sources.
And although this model may work well for intercity university/healthcare systems, it is usually a struggle for the rural nonprofit hospitals. In 2020, ten out of 17 rural hospitals that went under were nonprofits. And this is not just true in the tough pandemic year. Over the past two decades multitude of nonprofit rural hospitals had to sell and be taken over by larger for-profit entities.
Hospital consolidation has led to a worse patient experience and no real significant changes in readmission or mortality data. (The article below is how over 130 rural hospitals have closed since 2010, creating a medical emergency in rural US healthcare)
And according to the article below it is only to get worse
The authors of the Health Affairs blog feel a major disadvantage of both the for-profit and non-profit healthcare systems is “that both face limited accountability with respect to anticompettive mergers and acquisitions.”
More hospital consolidation is expected post-pandemic
Hospital deal volume is likely to accelerate due to the financial damage inflicted by the coronavirus pandemic.
The anticipated increase in volume did not show up in the latest quarter, when deals were sharply down.
The pandemic may have given hospitals leverage in coming policy fights over billing and the creation of “public option” health plans.
Hospital consolidation is likely to increase after the COVID-19 pandemic, say both critics and supporters of the merger-and-acquisition (M&A) trend.
The financial effects of the coronavirus pandemic are expected to drive more consolidation between and among hospitals and physician practices, a group of policy professionals told a recent Washington, D.C.-based web briefing sponsored by the Alliance for Health Policy.
“There is a real danger that this could lead to more consolidation, which if we’re not careful could lead to higher prices,” said Karyn Schwartz, a senior fellow at the Kaiser Family Foundation (KFF).
Schwartz cited a recent KFF analysis of available research that concluded “provider consolidation leads to higher health care prices for private insurance; this is true for both horizontal and vertical consolidation.”
Kenneth Kaufman, managing director and chair of Kaufman Hall, noted that crises tend to push financially struggling organizations “further behind.”
“I wouldn’t be surprised at all if that happens,” Kaufman said. “That will lead to further consolidation in the provider market.”
The initial rounds of federal assistance from the CARES Act, which were based first on Medicare revenue and then on net patient revenue, may fuel consolidation, said Mark Miller, PhD, executive vice president of healthcare for Arnold Ventures. That’s because the funding formulas favored organizations that already had higher revenues, he said, and provided less assistance to low-revenue organizations.
HHS has distributed $116.2 billion from the $175 billion in provider funding available through the CARES Act and the Paycheck Protection Program and Health Care Enhancement Act. The largest distributions used the two revenue formulas cited by Miller.
No surge in M&A yet
The expected burst in hospital M&A activity has yet to occur. Kaufman Hall identified 14 transactions in the second quarter of 2020, far fewer than in the same quarter in any of the four preceding years, when second-quarter transactions totaled between 19 and 31. The latest deals were not focused on small hospitals, with average seller revenue of more than $800 million — far larger than the previous second-quarter high of $409 million in 2018.
Six of the 14 announced transactions were divestitures by major for-profit health systems, including Community Health Systems, Quorum and HCA.
Kaufman Hall’s analysis of the recent deals identified another pandemic-related factor that may fuel hospital M&A: closer ties between hospitals. The analysis cited the example of Lifespan and Care New England, which had suspended merger talks in 2019. More recently, in a joint announcement, the CEOs of the two systems noted that because of the COVID-19 crisis, the two systems “have been working together in unprecedented ways” and “have agreed to enter into an exploration process to understand the pros and cons of what a formal continuation of this collaboration could look like in the future.”
The M&A outlook for rural hospitals
The pandemic has had less of a negative effect on the finances of rural hospitals that previously joined larger health systems, said Suzie Desai, senior director of not-for-profit healthcare for S&P Global.
A CEO of a health system with a large rural network told Kaufman the federal grants that the system received for its rural hospitals were much larger than the grants paid through the general provider fund.
“If that was true across the board, then the federal government recognized that many rural hospitals could be at risk of not being able to make payroll; actually running out of money,” Kaufman said. “And they seem to have bent over backwards to make sure that didn’t happen.”
Other CARES Act funding distributed to providers included:
$12.8 billion for 959 safety net hospitals
$11 billion to almost 4,000 rural healthcare providers and hospitals in urban areas that have certain special rural designations in Medicare
Telehealth has helped rural hospitals but has not been sufficient to address the financial losses inflicted by the pandemic, Desai said.
Other coming trends include a sharper cost focus
Desai expects an increasing focus “over the next couple years” on hospital costs because of the rising share of revenue received from Medicare and Medicaid. She expects increased efforts to use technology and data to lower costs.
Billy Wynne, JD, chairman of Wynne Health Group, expects telehealth restrictions to remain relaxed after the pandemic.
Also, the perceptions of the public and politicians about the financial health of hospitals are likely to give those organizations leverage in coming policy fights over changes such as banning surprise billing and creating so-called public-option health plans, Wynne said. As an example, he cited the Colorado legislature’s suspension of the launch of a public option “in part because of sensitivities around hospital finances in the COVID pandemic.”
“Once the dust settles, it’ll be interesting to see if their leverage has increased or decreased due to what we’ve been through,” Wynne said.
About the Author
Rich Daly, HFMA Senior Writer and Editor,
is based in the Washington, D.C., office. Follow Rich on Twitter: @rdalyhealthcare
The quality of care at hospitals acquired during a recent wave of consolidations has gotten worse or stayed the same, according to a study led by Harvard Medical School scientists published Jan. 2 in NEJM.
The findings deal a blow to the often-cited arguments that hospital consolidation would improve care. A flurry of earlier studies showed that mergers increase prices. Now after analyzing patient outcomes after hundreds of hospital mergers, the new research also dashes the hopes that this more expensive care might be of higher quality.
Get more HMS news here
“Our findings call into question claims that hospital mergers are good for patients—and beg the question of what we are getting from higher hospital prices,” said study senior author J. Michael McWilliams, the Warren Alpert Foundation Professor of Health Care Policy in the Blavatnik Institute at HMS and an HMS professor of medicine and a practicing general internist at Brigham and Women’s Hospital.
McWilliams noted that rising hospital prices have been one of the leading drivers of unsustainable growth in U.S. health spending.
To examine the impact of hospital mergers on quality of care, researchers from HMS and Harvard Business School examined patient outcomes from nearly 250 hospital mergers that took place between 2009 and 2013. Using data collected by the Centers for Medicare and Medicaid Services, they analyzed variables such as 30-day readmission and mortality rates among patients discharged from a hospital, as well as clinical measures such as timely antibiotic treatment of patients with bacterial pneumonia. The researchers also factored in patient experiences, such as whether those who received care at a given hospital would recommend it to others. For their analysis, the team compared trends in these indicators between 246 hospitals acquired in merger transactions and unaffected hospitals.
The verdict? Consolidation did not improve hospital performance, and patient-experience scores deteriorated somewhat after the mergers.
The study was not designed to examine the reasons behind the worsening in patient experience. Weakening of competition due to hospital mergers could have contributed, the researchers said, but deeper exploration suggested other potential mechanisms. Notably, the analysis found the decline in patient-experience scores occurred mainly in hospitals acquired by hospitals that already had a poor patient-experience score—a finding that suggests acquisitions facilitate the spread of low quality care but not of high quality care.
The researchers caution that isolated, individual mergers may have still yielded positive results—something that an aggregate analysis is not powered to capture. And the researchers could only examine measurable aspects of quality. The trend in hospital performance on these standard measures, however, appears to point to a net effect of overall decline, the team said.
“Since our study estimated the average effects of mergers, we can’t rule out the possibility that some mergers are good for patient care,” said first author Nancy Beaulieu, research associate in health care policy at HMS. “But this evidence should give us pause when considering arguments for hospitals mergers.”
The work was supported by the Agency for Healthcare Research and Quality (grant no. U19HS024072).
Co-investigators included Bruce Landon and Jesse Dalton from HMS, Ifedayo Kuye, from the University of California, San Francisco, and Leemore Dafny from Harvard Business School and the National Bureau of Economic Research.
Public benefit corporations (versus Benefit Corporate status, which is more of a pledge) are separate legal entities which exist as a hybrid, for-profit/nonprofit company but is mandated to
Pursue a general or specific public benefit
Consider the non-financial interests of its shareholders and other STAKEHOLDERS when making decision
report how well it is achieving its overall public benefit objectives
Have limited fiduciary responsibility to investors that remains IN SCOPE of public benefit goal
In essence, the public benefit corporations executives are mandated to run the company for the benefit of STAKEHOLDERS first, if those STAKEHOLDERS are the public beneficiary of the company’s goals. This in essence moves the needle away from the traditional C-Corp overvaluing the needs of shareholders and brings back the mission of the company and in the case of healthcare, the needs of its stakeholders, the consumers of healthcare.
PBCs are legal entities recognized by states rather than by the federal government. So far, in 2020 about 37 states allow companies to incorporate as a PBC. Stipulations of the charter include semiannual reporting of the public benefits bestowed by the company and how well it is achieving its public benefit mandate. There are about 3,000 US PBCs. Some companies have felt it was in their company mission and financial interest to change incorporation as a PBC.
Some well known PBCs include
Ben and Jerry’s Ice Cream
American Red Cross
Susan B. Komen Foundation
Allbirds (a shoe startup valued at $1.7 billion when made switch)
Bombas (the sock company that donates extra socks when you buy a pair)
Lemonade (a publicly traded insurance PBC that has beneficiaries select a nonprofit that the company will donate to)
Although the number of PBCs in the healthcare arena is increasing
Not many PBCs are in the area of healthcare delivery
Noone is quite sure what the economic model would look like for a healthcare delivery PBC
Some example of hospital PBC include NYC Health + Hospitals and Community First Medical Center in Chicago.
Benefits of moving a hospital to PBC Status
PBCs are held legally accountable to a predefined public benefit. For hospitals this could be delivering cost-effective quality of care and affordable to a local citizenry or an economically disadvantaged population. PBCs must produce at least an annual report on the public benefits it has achieved contrasted against a third party standard. For example a hospital could include data of Medicaid related mortality risks, data neither the C-corp nor the nonprofit 501c would have to report on. Most nonprofits and charities report their taxes on a schedule H or Form 990, which only has to report the officer’s compensation as well as monies given to charitable organizations, or other 501 organizations. The nonprofit would show a balance of zero as the donated money for that year would be allocated out for various purposes. Hospitals, even as nonprofits, are not required to submit all this data. Right now in US the ACA just requires any hospital that receives government or ACA insurance payments to report certain outcome statistics. Although varying state by state, a PBC should have a “benefit officer” to make sure the mandate is being met. In some cases a PBC benefit officer could sue the board for putting shareholder interest over the public benefit mandate.
A PBC can include community stakeholders in the articles of incorporation thus giving a voice to local community members. This would be especially beneficial for a hospital serving, say, a rural community.
PBCs do have advantages of the for-profit companies as they are not limited to non-equity forms of investment. A PBC can raise money in the equity markets or take on debt and finance it. These financial instruments are unavailable to the non-profit. Yet one interesting aspect is that PBCs require a HIGHER voting threshold by shareholders than a traditional for profit company in the ability to change their public benefit or convert their PBC back to a for-profit.
Limitations of the PBC
Little incentive financially for current and future hospitals to incorporate as a PBC. Herein lies a huge roadblock given the state of our reimbursement structure in this country. Although there may be an incentive with regard to hiring and retention of staff drawn to the organization’s social purpose. There have been, in the past, suggestions to allow hospitals that incorporate at PBC to receive some tax benefit, but this legislation has not gone through either at state or federal level. (put link to tax article).
In order for there to be value to constituents (patients) there must be strong accountability measures. This will require the utmost in ethical behavior by a board and executives. We have witnessed, through M&A by large health groups, anticompetitive and near monopoly behavior.
There are no federal guidelines but varying guidelines from state to state. There must be some federal recognition of the PBC status when it comes to healthcare, such as that the government is one of the biggest payers of US healthcare.
This is a great interview with ArcHealth, a PBC healthcare system.
Arc Health PBC is a public benefit corporation, a mission-driven for-profit company that utilizes a market-driven approach to achieving our short and long-term social goals. As a public benefit corporation, Arc Health is also a social enterprise working to further our mission of providing healthcare to rural, underserved, and indigenous communities through business practices that improve the recruitment and retention of quality healthcare providers.
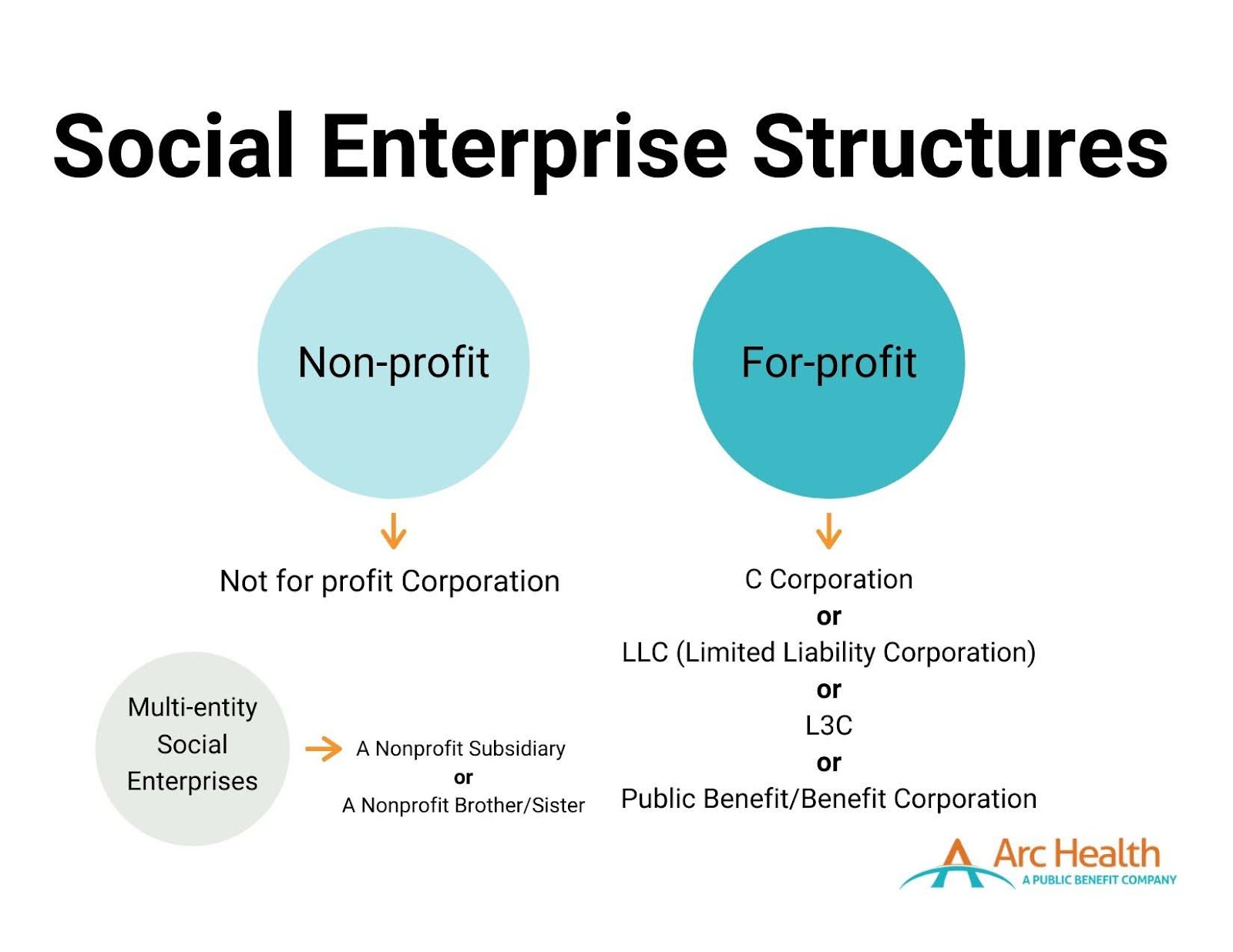
What is a Social Enterprise?
While there is no one exact definition, according to the Social Enterprise Alliance, a social enterprise is an “organization that addresses a basic unmet need or solves a social or environmental problem through a market-driven approach.” A social enterprise is not a distinct legal entity, but instead, an “ideological spectrum marrying commercial approaches with social good.” Social enterprises foster a dual-bottom-line – simultaneously seeking profits and social impact. Arc Health, like many social enterprises, seeks to be self–sustainable.
Two primary structures fall under the social enterprise umbrella: nonprofits and for-profit organizations. There are also related entities within both structures that could be considered social enterprises. Any of these listed structures can be regarded as a social enterprise depending on if and how involved they are with socially beneficial programs.
What is a Public Benefit Corporation?
Public Benefit Corporations (PBCs), also known as benefit corporations, are “for-profit companies that balance maximizing value to stakeholders with a legally binding commitment to a social or environmental mission.” PBCs operate as for-profit entities with no tax advantages or exemptions. Still, they must have a “purpose of creating general public benefit,” such as promoting the arts or science, preserving the environment, or providing benefits to underserved communities. PBCs must attain a higher degree of corporate purpose, expanded accountability, and expected transparency.
There are now over 3,000 registered PBCs, comprising approximately 0.1% of American businesses.
As a PBC, Arc Health expects to access capital through individual investors who seek financial returns, rather than through donations. Arc Health’s investors make investments with a clear understanding of the balance the company must strike between financial returns (I.e., profitability) and social purpose. Therefore, investors expect the company to be operationally profitable to ensure a financial return on their investments, while also making clear to all stakeholders and the public that generating social impact is the priority.
What is the difference between a Social Enterprise and PBC?
Social enterprises and PBCs emulate similar ideals that value the importance and need to invoke social change vis-a-vis working in a market-driven industry. Public benefit corporations fall under the social enterprise umbrella. An organization may choose to use a social enterprise model and incorporate itself as either a not-for-profit, C-Corp, PBC, or other corporate structure.
How did Arc Health Become a Public Benefit Corporation?
Arc Health was initially formed as a C-Corp. In 2019, Arc Health’s CEO and Co-Founder, Dave Shaffer, guided the conversion from a C-Corp to a PBC, incorporated in Delaware. Today, Arc Health follows guidelines and expectations for PBCs, including adhering to the State of Delaware’s requirements for PBCs.
Why is Arc Health a Social Enterprise and Public Benefit Corporation?
Arc Health believes it is essential to commit ourselves to our mission and demonstrate our dedication through our actions. We work to adhere to the core values of accountability, transparency, and purpose. As a registered public benefit company and a social enterprise, we execute our drive to achieve health equity in tangible and effective ways that the communities we work with, our stakeholders, and our providers expect of us.
90% of Americans say that companies must not only say a product or service is beneficial, but they also need to prove its benefit.
When we partner with health clinics and hospitals, we aim to provide services that enact lasting change. For example, we work with healthcare providers who desire to contribute both clinical and non-clinical skills. In 2020, Arc Health clinicians developed COVID-19 response protocols and educational materials about the vaccines. They participated in pain management working groups. They identified and followed up with kids in the community who were overdue for a well-child check. Arc Health providers should be driven by a desire to develop a long-term relationship with a healthcare service provider and participate in its successes and challenges.
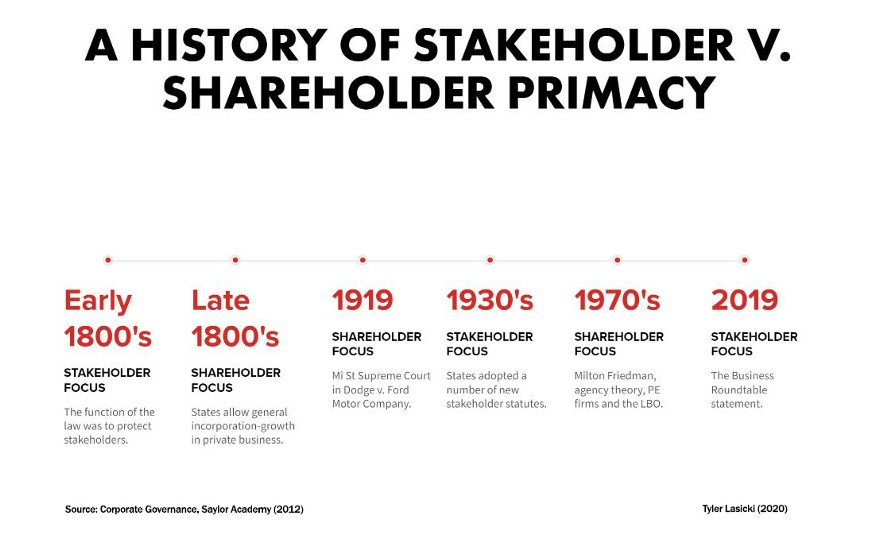
Paradigm Shift in the 1980’s: Companies Start to Emphasize Shareholders Over Stakeholders
So earlier in this post we had mentioned about a shift in philosophy at the corporate boardroom that affected how comparate thought, value, and responsibility: Companies in the 1980s started to shift their focus and value only the needs of corporate ShAREHOLDERS at the expense of their traditional STAKEHOLDERS (customers, clients). Many movies and books have been written on this and debatable if deliberate or a by-product of M&A, hostile takeovers, and the stock market in general but the effect was that the consumer was relegated as having less value, even though marketing budgets are very high. The fiduciary responsibility of the executive was now defined in terms of satisfying shareholders, who were now big huge and powerful brokerage houses, private equity, and hedge funds. A good explanation by Medium.com Tyler Lasicki is given below.
In a famous 1970 New York Times Article, Milton Friedman postulated that the CEO, as an employee of the shareholder, must strive to provide the highest possible return for all shareholders. Since that article, the United States has embraced this idea as the fundamental philosophy supporting the ultimate purpose of businesses — The Shareholders Come First.
In August of 2019, the Business Roundtable, a group made up of the most influential U.S CEOs, published a letter shifting their stance on the purpose of a corporation. Regardless of whether this piece of paper will actually result in any systematic changes has yet to be seen, however this newly stated purpose of business is a dramatic shift from the position Milton Friedman took in 1970. According to the statement, these corporations will no longer prioritize maximizing profits for shareholders, but instead turn their focus to benefiting all stakeholders — including citizens, customers, suppliers, employees, on par with shareholders.
Now the social responsibility of a company and the CEO was to maxiimize the profits even at the expense of any previous social responsibility they once had.
Small sample of the 181 Signatures attached to the Business Roundtable’s letter
What has happened over the past 50 years that has led to such a fundamental change in ideology? What has happened to make the CEO’s of America’s largest corporations suddenly change their stance on such a foundational principle of what it means to be an American business?
Since diving into this subject, I have come to find that the “American fundamental principle” of putting shareholders first is one that is actually not all that fundamental. In fact, for a large portion of our nation’s history this ideology was actually seen as the unpopular position.
Key ideological shifts in U.S. history
This post dives into a brief history of these two contrasting ideological viewpoints in an attempt to contextualize the forces behind both sides — specifically, the most recent shift (1970–2019). This basic idea of what is most important; the stakeholder or the shareholder, is the underlying reason as to why many things are the way they are today. A corporation’s priority of shareholder or stakeholder ultimately impacts employee salaries, benefits, quality of life within communities, environmental conditions, even the access to education children can receive. It affects our lives in a breadth and depth of ways and now that corporations may be changing positions (yet again) to focus on a model that prioritizes the stakeholder, it is important to understand why.
Looking forward, if stakeholder priority ends up being the popular position among American businesses, how long will it last for? What could lead to its downfall? And what will managers do to ensure a long term stakeholder-friendly business model?
It is clear to me the reasons that have led to these shifts in ideology are rather nuanced, however I want to highlight a few trends that have had a major impact on businesses changing their priorities while also providing context as to why things have shifted.
The Ascendancy of Shareholder Value
Following the 1929 stock market crash and the Great Depression, stakeholder primacy became the popular perspective within corporate America. Stakeholder primacy is the idea that corporations are to consider a wider group of interested parties (not just shareholders) whose positions need to be taken into consideration by corporate governance. According to this point of view, rather than solely being an agent for shareholders, management’s responsibilities were to be dispersed among all of its constituencies, even if it meant a reduction in shareholder value. This ideology lasted as the dominant position for roughly 40 years, in part due to public opinion and strong views on corporate responsibility, but also through state adoption of stakeholder laws.
By the mid-1970s, falling corporate profitability and stagnant share prices had been the norm for a decade. This poor economic performance influenced a growing concern in the U.S. regarding the perceived divergence between manager and shareholder interest. Many held the position that profits and share prices were suffering as a result of corporation’s increased attention on stakeholder groups.
This noticeable divergence in interests sparked many academics to focus their research on corporate management’s motivations in decision making regarding their allocation of resources. This branch of research would later be known as agency theory, which focused on the relationship between principals (shareholders) and their agents (management). Research at the time outlined how over the previous decades corporate management had pursued strategies that were not likely to optimize resources from a shareholder’s perspective. These findings were part of a seismic shift of corporate philosophy, changing priority from the stakeholders of a business to the shareholders.
By 1982, the U.S. economy started to recover from a prolonged period of high inflation and low economic growth. This recovery acted as a catalyst for change in many industries, leaving many corporate management teams to struggle in response to these changes. Their business performance suffered as a result. These distressed businesses became targets for a group of new investors…private equity firms.
Now the paradigm shift had its biggest backer…. private equity! And private equity care about ONE thing….. THEIR OWN SHARE VALUE and subsequently meaning corporate profit, which became the most important directive for the CEO.
So it is all hopeless now? Can there be a shift back to the good ‘ol days?
Well some changes are taking place at top corporate levels which may help the stakeholders to have a voice at the table, as the following IRMagazine article states.
And once again this is being led by the Business Roundtable, the same Business Roundtable that proposed the shift back in the 1970s.
n a major corporate shift, shareholder value is no longer the main objective of the US’ top company CEOs, according to the Business Roundtable, which instead emphasizes the ‘purpose of a corporation’ and a stakeholder-focused model.
The influential body – a group of chief executive officers from major US corporations – has stressed the idea of a corporation dropping the age-old notion that corporations function first and foremost to serve their shareholders and maximize profits.
Rather, the focus should be on investing in employees, delivering value to customers, dealing ethically with suppliers and supporting outside communities as the vanguard of American business, according to a Business Roundtable statement.
‘While each of our individual companies serves its own corporate purpose, we share a fundamental commitment to all of our stakeholders,’ reads the statement, signed by 181 CEOs. ‘We commit to deliver value to all of them, for the future success of our companies, our communities and our country.’
Gary LaBranche, president and CEO of NIRI, tells IR Magazine that this is part of a wider trend: ‘The redefinition of purpose from shareholder-focused to stakeholder-focused is not new to NIRI members. For example, a 2014 IR Update article by the late Professor Lynn Stout urges a more inclusive way of thinking about corporate purpose.’
NIRI has also addressed this concept at many venues, including the senior roundtable annual meeting and the NIRI Annual Conference, adds LaBranche. This trend was further seen in the NIRI policy statement on ESG disclosure, released in January this year.
Analyzing the meaning of this change in more detail, LaBranche adds: ‘The statement is a revolutionary break with the Business Roundtable’s previous position that the purpose of the corporation is to create value for shareholders, which was a long-held position championed by Milton Friedman.
‘The challenge is that Friedman’s thought leadership helped to inspire the legal and regulatory regime that places wealth creation for shareholders as the ‘prime directive’ for corporate executives.
‘Thus, commentators like Mike Allen of Axios are quick to point out that some shareholders may actually use the new statement to accuse CEOs of worrying about things beyond increasing the value of their shares, which, Allen reminds us, is the CEOs’ fiduciary responsibility.
‘So while the new Business Roundtable statement reflects a much-needed rebalancing and modernization that speaks to the comprehensive responsibilities of corporate citizens, we can expect that some shareholders will push back on this more inclusive view of who should benefit from corporate efforts and the capital that makes it happen. The new statement may not mark the dawn of a new day, but it perhaps signals the twilight of the Friedman era.’
In a similarly reflective way, Jamie Dimon, chairman and CEO of JPMorgan Chase & Co and chairman of the Business Roundtable, says: ‘The American dream is alive, but fraying. Major employers are investing in their workers and communities because they know it is the only way to be successful over the long term. These modernized principles reflect the business community’s unwavering commitment to continue to push for an economy that serves all Americans.’
Note: Mr Dimon has been very vocal for many years on corporate social responsibility, especially since the financial troubles of 2009.
Impact of New Regulatory Trends in M&A Deals
The following podcast from Pricewaterhouse Cooper Health Research Institute (called Next in Health) discusses some of the trends in healthcare M&A and is a great listen. However from 6:30 on the podcast discusses a new trend which is occuring in the healthcare company boardroom, which is this new focus on integrating companies that have proven ESG (or environmental, social, governance) functions within their organzations. As stated, doing an M&A deal with a company with strong ESG is looked favorably among regulators now.
Please click on the following link to hear a Google Podcast Next in Health episode
Heather shows the feasability of this model with multiple biotech and healthtech startups, including one founded by Mark Cuban.
Health tech unicorn Aledade recently announced that it made the strategic decision to become a public benefit corporation (PBC).
The company joins just a handful of others in healthcare that are structured this way.
So what exactly is a PBC, and why does it matter?
PBCs are a type of for-profit corporate entity that has also adopted a public benefit purpose and is currently authorized by 35 states and the District of Columbia. A PBC must consider the nonfinancial interests of its shareholders and other stakeholders when making decisions. As a public benefit corporation, companies have to weigh their social/environmental objectives alongside maximizing value for shareholders.
While PBC and B Corp. are often used interchangeably, they are not the same. A B Corp. is a certification provided to eligible companies by the nonprofit, B Lab. A PBC is an actual legal entity that bakes into its certificate of incorporation a “public benefit,” according to Rubicon Law Group.
“I don’t think that there is a trade-off between either you do things that are good for society or you make profits in your business.” —Farzad Mostashari, M.D.
PBCs also are required to provide a report to shareholders every two years that detail how well the company is achieving its overall public benefit objectives. In some states, the report must be assessed against a third-party standard and be made publicly available. Delaware PBCs are not required to report publicly or against a third-party standard.
Aledade launched in 2014 and uses data analytics to help independent doctors’ offices transition to value-based care models. The company currently partners with more than 1,000 independent primary care practices comprising over 11,000 physicians and has nearly 150 contracts covering more than 1.7 million patients and $17 billion in total healthcare spending. Last June, the company raised $123 million in a series E round, boosting its valuation to $3.1 billion.
In a blog post, Aledade CEO and co-founder Farzad Mostashari, M.D., explained the company’s reasoning behind the move and said the corporate structure of a PBC is “well suited to mission-oriented companies where alignment with stakeholders is a key driver of the business model.”
“Aledade’s public benefit purpose means that we must weigh the interests of our primary care practice partners, their patients, our employees, and those who bear the burden of rising health care costs, alongside those of our shareholders, when we make decisions,” Mostashari said in an interview. This duty extends to all significant board decisions, including decisions on whether to go public, to make acquisitions or to sell the company, he noted.
The PBC structure helps create alignment among stakeholders and build trust, he said. “I don’t think that there is a trade-off between either you do things that are good for society or you make profits in your business. That might be true for fee-for-service businesses. It’s not true for Aledade,” he said.
He added, “For businesses that are built on trust and alignment, not considering stakeholder benefits gets you neither social good nor profits. If you’re in a business like our business where it’s actually really important that everybody have faith and belief that you are doing what’s best for patients, that you are actually in it for the long-term for practices, that’s what makes us successful as a business.”
Mark Cuban Cost Plus Drugs, which launched in January 2022 to offer low-cost rivals to overpriced generic drugs, also is structured as a public benefit corporation. The company’s founder and CEO Alexander Oshmyansky started the company in 2015 as a nonprofit, according to a feature story in D Magazine. Through Y Combinator, investors told Oshmyansky that the nonprofit model wouldn’t be able to raise the needed funds. He then reworked the business model to a PBC and launched Osh’s Affordable Pharmaceuticals in 2018.
Some other companies that are biotech drug development companies that operate under the PBC model include
Even a traditional for-profit C corporation can work toward a public mission without becoming a PBC. But, in an industry like healthcare, too often the duty to maximize financial returns for shareholders or investors can be in conflict with what is best for patients, executives say.
“With a startup, it might limit the ability to sell their business to a larger company in the future because there might be some limitations on what the larger company could do with the organization.”—Jodi Daniel, a partner in Crowell & Moring’s Health Care Group
According to some healthcare experts, PBCs offer a promising alternative as a business model for healthcare companies by providing a “North Star” by which a company can navigate critical business decisions.
“I think it really helps to drive accountability,” Huang, Osmind’s chief executive, said. “I think that’s important, especially in healthcare where it’s easy sometimes to get misaligned with all the different stakeholders that are involved in the industry. We wanted to make sure we had something to be accountable to. Second, it’s ingrained in the culture. The third element of why it was so helpful for us from the beginning is just on focus and alignment. I think we can be much more clear and transparent about what we’re focused on, our values, how we try to use that transparently to influence our decisions and how we can build a business that really ties all of that together.”
In a Health Affairs article, medical researchers at Stanford, including Jimmy Qian, a co-founder of Osmind, laid out the case for why PBCs may simultaneously improve individual patient outcomes and collective benefit without sacrificing institutions’ financial stability.
PBCs are held legally accountable to a predefined public benefit, which, for hospitals, could involve delivering high-quality, affordable care to local populations. PBCs are required to produce annual benefits reports that are assessed against a third-party standard. “These reports could be used by regulatory agencies such as the Centers for Medicare and Medicaid Services (CMS) or local health authorities to evaluate whether the PBC is making progress toward its stated mission and respond accordingly,” the researchers wrote.
But are there any trade-offs?
Having a public benefit obligation could potentially “tie the hands” of board members who can’t just focus on profits and must focus on those dual responsibilities, noted Jodi Daniel, a partner in Crowell & Moring’s Health Care Group.
“Companies that transition to being a public benefit corporation are intentionally trying to ensure that that the company’s mission doesn’t get diminished over time because it’s in their charter. So it helps [the mission] to endure. But there are pros and cons to that. It is somewhat binding the future board members and executives to follow that mission,” she said.
Daniel said she has spoken with several healthcare companies recently that are weighing the possibility of transitioning to a PBC. “Companies often don’t want to necessarily limit their options in their decision-making in the future. With a startup, it might limit the ability to sell their business to a larger company in the future because there might be some limitations on what the larger company could do with the organization,” she said in an interview.
By making decisions based on interests outside of financial ones, organizations may put themselves at a margin disadvantage as compared to pure for-profit players in the space, wrote Hospitalogy founder Blake Madden.
Faddis with Veeva said the company hasn’t seen any financial or performance trade-off as a result of operating as a PBC. He noted that the move has been good for recruiting, spurred more long-term conversations with customers and has been a source of new ideas.
“Prior to the conversion, you had employees who were thinking of new products or new functionality with the mindset of getting to be commercially successful,” Faddis said. “Now, you also have people thinking about it from the angle of, ‘Does it further one of our PBC purposes and then maybe it’s also going to be commercially successful?'”
Converting to a PBC also can be a tactic to build trust, Daniel noted, especially in healthcare, and that holds the potential to drive business.
One factor that isn’t clear is whether there is sufficient oversight to hold these companies accountable to their stated public mission. Who checks to make sure companies are making progress toward their objectives to improve healthcare?
Osmind publishes its benefit corporation report on its website to make it available to the public even though it is not required to do so. “I think that really highlights the accountability piece of you need to tell the world or at least tell your shareholders how you’re really trying to uphold your public benefit,” Huang said.
Other related articles published on this Open Access Online Scientific Journal on Healthcare Issues include the following:
The coronavirus pandemic has affected almost every country in every continent however, after months of the novel advent of novel COVID-19 cases, it has become apparent that the varied clinical responses in this epidemic (and outcomes) have laid bare some of the strong and weak aspects in, both our worldwide capabilities to respond to infectious outbreaks in a global coordinated response and in individual countries’ response to their localized epidemics.
Some nations, like Israel, have initiated a coordinated government-private-health system wide action plan and have shown success in limiting both new cases and COVID-19 related deaths. After the initial Wuhan China outbreak, China closed borders and the government initiated health related procedures including the building of new hospitals. As of writing today, Wuhan has experienced no new cases of COVID-19 for two straight days.
However, the response in the US has been perplexing and has highlighted some glaring problems that have been augmented in this crisis, in the view of this writer. In my view, which has been formulated after social discussion with members in the field ,these issues can be centered on three major areas of deficiencies in the United States that have hindered a rapid and successful response to this current crisis and potential future crises of this nature.
The mistrust or misunderstanding of science in the United States
Lack of communication and connection between patients and those involved in the healthcare industry
Socio-geographical inequalities within the US healthcare system
1. The mistrust or misunderstanding of science in the United States
For the past decade, anyone involved in science, whether directly as active bench scientists, regulatory scientists, scientists involved in science and health policy, or environmental scientists can attest to the constant pressure to not only defend their profession but also to defend the entire scientific process and community from an onslaught of misinformation, mistrust and anxiety toward the field of science. This can be seen in many of the editorials in scientific publications including the journal Science and Scientific American (as shown below)
Boston rally coincides with annual American Association for the Advancement of Science (AAAS) conference and is a precursor to the March for Science in Washington, D.C.
Responding to the troubling suppression of science under the Trump administration, thousands of scientists, allies, and frontline communities are holding a rally in Boston’s Copley Square on Sunday.
“Science serves the common good,” reads the call to action. “It protects the health of our communities, the safety of our families, the education of our children, the foundation of our economy and jobs, and the future we all want to live in and preserve for coming generations.”
It continues:
But it’s under attack—both science itself, and the unalienable rights that scientists help uphold and protect.
From the muzzling of scientists and government agencies, to the immigration ban, the deletion of scientific data, and the de-funding of public science, the erosion of our institutions of science is a dangerous direction for our country. Real people and communities bear the brunt of these actions.
The rally was planned to coincide with the annual American Association for the Advancement of Science (AAAS) conference, which draws thousands of science professionals, and is a precursor to the March for Science in Washington, D.C. and in cities around the world on April 22.
However, some feel that scientists are being too sensitive and that science policy and science-based decision making may not be under that much of a threat in this country. Yet even as some people think that there is no actual war on science and on scientists they realize that the public is not engaged in science and may not be sympathetic to the scientific process or trust scientists’ opinions.
Certainly, opponents of genetically modified crops, vaccinations that are required for children and climate science have become louder and more organized in recent times. But opponents typically live in separate camps and protest single issues, not science as a whole, said science historian and philosopher Roberta Millstein of the University of California, Davis. She spoke at a standing-room only panel session at the American Association for the Advancement of Science’s annual meeting, held in Washington, D.C. All the speakers advocated for a scientifically informed citizenry and public policy, and most discouraged broadly applied battle-themed rhetoric.
In general, it appears to be a major misunderstanding by the public of the scientific process, and principles of scientific discovery, which may be the fault of miscommunication by scientists or agendas which have the goals of subverting or misdirecting public policy decisions from scientific discourse and investigation.
This can lead to an information vacuum, which, in this age of rapid social media communication,
can quickly perpetuate misinformation.
This perpetuation of misinformation was very evident in a Twitter feed discussion with Dr. Eric Topol, M.D. (cardiologist and Founder and Director of the Scripps Research Translational Institute) on the US President’s tweet on the use of the antimalarial drug hydroxychloroquine based on President Trump referencing a single study in the International Journal of Antimicrobial Agents. The Twitter thread became a sort of “scientific journal club” with input from international scientists discussing and critiquing the results in the paper.
Please note that when we scientists CRITIQUE a paper it does not mean CRITICIZE it. A critique is merely an in depth analysis of the results and conclusions with an open discussion on the paper. This is part of the normal peer review process.
Below is the original Tweet by Dr. Eric Topol as well as the ensuing tweet thread
I reviewed the cited paperhttps://t.co/E4Iw7GpVh6 an open-label, non=randomized study The endpoint was viral PCR (mostly + or -, many ND) by nasopharyngeal swab. 6 of the 36 people were asymptomatic. 6 with pneumonia (LRTI) 6 people received "H + A" pic.twitter.com/KBjR1QcZRV
Eric – a huge issue here is they only report data on 20 of the 26 patients, and of the 6 – all deteriorated! Six hydroxychloroquine-treated patients were lost in follow-up: they worsened and weee sent to the ICU! They need to do last observation carried forward for those.
— Christopher Cannon, M.D. 🇺🇦 (@cpcannon) March 21, 2020
OMG, do you realize none of the patients in the treatment arm were definitive positives to start with? They were all in the "gray zone". JFC, this study was worse than I thought when I skimmed it the first time!
Within the tweet thread it was discussed some of the limitations or study design flaws of the referenced paper leading the scientists in this impromptu discussion that the study could not reasonably conclude that hydroxychloroquine was not a reliable therapeutic for this coronavirus strain.
The lesson:The public has to realizeCRITIQUE does not mean CRITICISM.
Scientific discourse has to occur to allow for the proper critique of results. When this is allowed science becomes better, more robust, and we protect ourselves from maybe heading down an incorrect path, which may have major impacts on a clinical outcome, in this case.
2. Lack of communication and connection between patients and those involved in the healthcare industry
In normal times, it is imperative for the patient-physician relationship to be intact in order for the physician to be able to communicate proper information to their patient during and after therapy/care. In these critical times, this relationship and good communication skills becomes even more important.
Recently, I have had multiple communications, either through Twitter, Facebook, and other social media outlets with cancer patients, cancer advocacy groups, and cancer survivorship forums concerning their risks of getting infected with the coronavirus and how they should handle various aspects of their therapy, whether they were currently undergoing therapy or just about to start chemotherapy. This made me realize that there were a huge subset of patients who were not receiving all the information and support they needed; namely patients who are immunocompromised.
These are patients represent
cancer patient undergoing/or about to start chemotherapy
Patients taking immunosuppressive drugs: organ transplant recipients, patients with autoimmune diseases, multiple sclerosis patients
Patients with immunodeficiency disorders
These concerns prompted me to write a posting curating the guidance from National Cancer Institute (NCI) designated cancer centers to cancer patients concerning their risk to COVID19 (which can be found here).
Surprisingly, there were only 14 of the 51 US NCI Cancer Centers which had posted guidance (either there own or from organizations like NCI or the National Cancer Coalition Network (NCCN). Most of the guidance to patients had stemmed from a paper written by Dr. Markham of the Fred Hutchinson Cancer Center in Seattle Washington, the first major US city which was impacted by COVID19.
Also I was surprised at the reactions to this posting, with patients and oncologists enthusiastic to discuss concerns around the coronavirus problem. This led to having additional contact with patients and oncologists who, as I was surprised, are not having these conversations with each other or are totally confused on courses of action during this pandemic. There was a true need for each party, both patients/caregivers and physicians/oncologists to be able to communicate with each other and disseminate good information.
Last night there was a Tweet conversation on Twitter #OTChat sponsored by @OncologyTimes. A few tweets are included below
The Lesson: Rapid Communication of Vital Information in times of stress is crucial in maintaining a good patient/physician relationship and preventing Misinformation.
3. Socio-geographical Inequalities in the US Healthcare System
It has become very clear that the US healthcare system is fractioned and multiple inequalities (based on race, sex, geography, socio-economic status, age) exist across the whole healthcare system. These inequalities are exacerbated in times of stress, especially when access to care is limited.
Some of the passengers had to be extricated from the wrecked cars. Many of the passengers and local residents helped first responders during the rescue operation. Five local hospitals treated the injured. The derailment disrupted train service for several days.
What was not reported was the difficulties that first responders, namely paramedics had in finding an emergency room capable of taking on the massive load of patients. In the years prior to this accident, several hospitals, due to monetary reasons, had to close their emergency rooms or reduce them in size. In addition only two in Philadelphia were capable of accepting gun shot victims (Temple University Hospital was the closest to the derailment but one of the emergency rooms which would accept gun shot victims. This was important as Temple University ER, being in North Philadelphia, is usually very busy on any given night. The stress to the local health system revealed how one disaster could easily overburden many hospitals.
Over the past decade many hospitals, especially rural hospitals, have been shuttered or consolidated into bigger health systems. The graphic below shows this
Note the huge swath of hospital closures in the midwest, especially in rural areas. This has become an ongoing problem as the health care system deals with rising costs.
Lesson:Epidemic Stresses an already stressed out US healthcare system
Funding Research by Lottery?: How Lucky Do You Feel After Submitting a Grant
Reporter: Stephen J. Williams, Ph.D.
A recent article in Nature: “Science Funders Gamble on Grant Lotteries” discusses an odd twist to the anxiety most researchers feel after submitting grants to an agency. Now, along with the hours of fretting over details and verbiage in a grant application, it appears that not only great science, but the luck of the draw may be necessary to get your work funded. The article, by David Adam, discusses the funding strategy of the Health Research Council of New Zealand, which since 2015, has implemented a strategy of awarding grants through random selection. Although limited in scope and size (mainly these grants are on very highly speculative and potentially transformative research and awards are usually less that $150,000 NZD) was meant to promote the applicants in submitting more risky ideas that are usually submitted in traditional peer reviewed grants.
Random chance will create more openness to ideas that are not in the mainstream
– Margit Osterloh, economist at University of Zurich
Margit also mentions that many mid-ranking applications which are never funded could benefit from such a lottery system.
The Swiss National Science Foundation (SSFS) is also experimenting with this idea of random selection. The Health Research Council states the process in not entirely random. A computer selects the projects at random based on a random number generator. A panel then decides if they are a reasonably good and well written application.
Some researchers have felt this random process could help eliminate much bias that can be baked into the traditional peer review process. However there are many who feel the current process of peer review panels are a necessary and rigorous step in the granting process, analyzing applications which would most likely have the best chances to succeed based on the rigor of the proposed science.
However Osterloh feels that the lottery idea produces a humbling effect. As Margit said
If you know you have got a grant or a publication which is selected partly randomly, then you will know very well you are not the king of the Universe
Humility in science: a refreshing idea. However the lottery idea will not mean that scientists need not prepare a careful and well written application. Applications that are ranked very low would not be in the lottery. However, if one feels lucky, maybe the obscene hours of worrying about each sentence written, or that figures for preliminary data should be altered at the 11th hour before submission might be a thing of the past.
Real Time Coverage @BIOConvention #BIO2019: After Trump’s Drug Pricing Blueprint: What Happens Next? A View from Washington; June 3 2019 1:00 PM Philadelphia PA
Dan Todd is the Principal of Todd Strategy, LLC, a consulting firm founded in 2014 and based in Washington, DC. He provides legislative and regulatory strategic guidance and advocacy for healthcare stakeholders impacted by federal healthcare programs.
Prior to Todd Strategy, Mr. Todd was a Senior Healthcare Counsel for the Republican staff of the Senate Finance Committee, the Committee of jurisdiction for the Medicare and Medicaid programs. His areas of responsibility for the committee included the Medicare Part B and Part D programs, which includes physician, medical device, diagnostic and biopharmaceutical issues.
Before joining the Finance Committee, Mr. Todd spent several years in the biotechnology industry, where he led policy development and government affairs strategy. He also represented his companies’ interests with major trade associations such as PhRMA and BIO before federal and state representatives, as well as with key stakeholders such as physician and patient advocacy organizations.
Dan also served as a Special Assistant in the Office of the Administrator at the Centers for Medicare & Medicaid Services (CMS), the federal agency charged with the operation of the Medicare and Medicaid programs. While at CMS, Dan worked on Medicare Part B and Part D issues during the implementation of the Medicare Modernization Act from 2003 to 2005.
Cost efficiencies were never measured.
Removing drug rebates would cost 180 billion over 10 years. CBO came up with similar estimate. Not sure what Congress will do. It appears they will keep the rebates in.
House Dems are really going after PBMs; anytime the Administration makes a proposal goes right into CBO baseline estimates; negotiations appear to be in very early stages and estimates are up in the air
WH close to meet a budget cap but then broke down in next day; total confusion in DC on budget; healthcare is now held up, especially the REBATE rule; : is a shame as panel agrees cost savings would be huge
they had initiated a study to tie the costs of PartB to international drug prices; meant to get at disparity on international drug prices; they currently are only mulling the international price index; other option is to reform Part B; the proposed models were brought out near 2016 elections so not much done; unified agenda;
most of the response of Congress relatively publicly muted; a flat fee program on biologics will have big effect on how physicians and health systems paid; very cat and mouse game in DC around drug pricing
administration is thinking of a PartB “inflation cap”; committees are looking at it seriously; not a rebate; discussion of tiering of physician payments
Ways and Means Cmmtte: proposing in budget to alleve some stresses on PartB deductable amounts;
PartD: looking at ways to shore it up; insurers 80% taxpayers 20% responsible; insurers think it will increase premiums but others think will reduce catastrophic costs; big part of shift in spending in Part D has been this increase in catastrophic costs
this week they may actually move through committees on this issue; Administration trying to use the budgetary process to drive this bargain; however there will have to be offsets so there may be delays in process
Follow or Tweet on Twitter using the following @ and # (hashtags)
The U.S. Department of Health and Human Services unveiled a proposed ruletackling the initial implementation of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA).
Advanced Alternative Payment Models (APMs), including the Comprehensive Primary Care Plus and Next Generation ACO models, among others.
The Centers for Medicare & Medicaid Services expects most providers to opt for the MIPS track initially, according to CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway, M.D., who spoke on a conference call announcing the rule.
Participation in Advanced Alternative Payment models would exempt doctors from MIPS reporting requirements while also qualifying them for financial bonuses in exchange for taking on the risks related with providing “coordinated, high-quality care,” according to CMS. The agency expects both the number of physicians participating in this track and the number of payment models available to grow over time.
CMS also reports that doctors will have the flexibility to switch among various components of the Quality Payment Program as dictated by the needs of their patients or their practices.
Opinions from around the web
In this video, Gilberg, senior vice president for the Medical Group Management Association’s Government Affairs Office, discusses CMS’ Physician Value-based Payment Modifier. In 2015, Medicare will begin applying the modifier under the physician fee schedule to various providers to show value of care.
“Cost and quality … make up the value equation, in the mind of the payer, in terms of Medicare,” said Gilberg.
In addition to explaining how the modifier works, Gilberg also highlights other quality measures facing providers under the Physician Quality Reporting System and via the EHR Incentive Programs, better known as meaningful use.
When the Medicare Access and CHIP Reauthorization Act (MACRA) legislation passed in April 2015, everyone cheered the repeal of the Sustainable Growth Rate (SGR) formula for Medicare physician payment. Now, even before the MACRA regulations are even promulgated, it’s time to pay attention because Medicare physician payments in 2019 will be impacted by their performance in 2017, just a year from now.
Article ID #203: Problem of Science Doctorate Programs. Published on 4/12/2016
WordCloud Image Produced by Adam Tubman
The Problem in Biomedical Education
Henry Bourne (UCSF)
Dr. Henry Bourne has trained graduate students and postdocs at UCSF for over 40 years. In his iBiology talk, he discusses the imminent need for change in graduate education. With time to degrees getting longer, the biomedical community needs to create experimental graduate programs to find more effective and low cost ways to train future scientists and run successful laboratories. If we don’t start looking for solutions, the future of the biomedical enterprise will grow increasingly unstable.
Henry Bourne is Professor Emeritus and former chair of the Department of Pharmacology at the University of California – San Francisco. His research focused on trimeric G-proteins, G-protein coupled receptors, and the cellular signals responsible for polarity and direction-finding of human leukocytes. He is the author of several books including a memoir, Ambition and Delight, and has written extensively about graduate training and biomedical workforce issues. Now Dr. Bourne’s research focuses on the organization and founding of US biomedical research in the early 20th century.
Peer-reviewed journals retracted 110 papers over the last 2 years. Nature reports the grim details in “Publishing: the peer review scam”.
When a handful of authors were caught reviewing their own
papers, it exposed weaknesses in modern publishing systems.
Editors are trying to plug the holes.
The Hill reports that the FDA may lift its ban on blood donations from gay men. The American Red Cross has voiced its support for lifting of the ban.
Advisers for the Food and Drug Administration (FDA) will meet this week to decide whether gay men should be allowed to donate blood, the agency’s biggest step yet toward changing the 30-year-old policy.
If the FDA accepts the recommendation, it would roll back a policy that has been under strong pressure from LGBT advocates and some members of Congress for more than four years.
“We’ve got the ball rolling. I feel like this is a tide-turning vote,” said Ryan James Yezak, an LGBT activist who founded the National Gay Blood Drive and will speak at the meeting. “There’s been a lot of feet dragging and I think they’re realizing it now.”
Groups such as the American Red Cross and America’s Blood Centers also voiced support of the policy change this month, calling the ban “medically and scientifically unwarranted.”
The FDA will use the group’s recommendation to decide whether to change the policy.
“Following deliberations taking into consideration the available evidence, the FDA will issue revised guidance, if appropriate,” FDA spokeswoman Jennifer Rodriguez wrote in a statement.
This reporter has more than 20 years of Blood Bank experience. The factor in favor of the recommendation is that the HIV 1/2 and other testing is accurate enough to leave the question of donor lifestyle irrelevant. However, it remains to be seen whether the testing turnaround time is sufficient to prevent the release of units that may be contaminated prior to transfusion, which is problematic for platelets, that have short expirations. In all cases of donor infection, regardless of whether units are released, a finding leads to not releasing the product or to recall.
Democrats made a strategic mistake by passing the Affordable Care Act, Sen. Charles Schumer (N.Y.), the third-ranking member of the Senate Democratic leadership, said Tuesday.
Schumer says Democrats “blew the opportunity the American people gave them” in the 2008 elections, a Democratic landslide, by focusing on healthcare reform instead of legislation to boost the middle class.
“After passing the stimulus, Democrats should have continued to propose middle class-oriented programs and built on the partial success of the stimulus,” he said in a speech at the National Press Club.
He said the plight of uninsured Americans caused by “unfair insurance company practices” needed to be addressed, but it wasn’t the change that people wanted when they elected Barack Obama as president.
“Americans were crying out for an end to the recession, for better wages and more jobs; not for changes in their healthcare,” he said.
This reader finds the observation by Senator Schumer very perceptive, regardless of whether the observation in hindsight might have had a different political outcome. It has been noted that President Obama had a lot on his plate. Moreover, we have not seen such a poor record of legislation in my lifetime. There are underlying issues of worldview of elected officials that also contribute to the events.
THE PEER-REVIEW SCAM
BY CAT FERGUSON, ADAM MARCUS AND IVAN ORANSKY
N AT U R E | 2 7 N O V 2 0 1 4; VO L 5 1 5 : 480-82.
Most journal editors know how much effort it takes to persuade busy researchers to review a paper. That is why the editor of The Journal of Enzyme Inhibition and Medicinal Chemistry was puzzled by the reviews for manuscripts by one author — Hyung-In Moon, a medicinal-plant researcher then at Dongguk University in Gyeongju, South Korea.
The reviews themselves were not remarkable: mostly favourable, with some suggestions about how to improve the papers. What was unusual was how quickly they were completed — often within 24 hours. The turnaround was a little too fast, and Claudiu Supuran, the journal’s editor-in-chief, started to become suspicious.
In 2012, he confronted Moon, who readily admitted that the reviews had come in so quickly because he had written many of them himself. The deception had not been hard to set up. Supuran’s journal and several others published by Informa Healthcare in London
invite authors to suggest potential reviewers for their papers. So Moon provided names, sometimes of real scientists and sometimes pseudonyms, often with bogus e-mail addresses that would go directly to him or his colleagues. His confession led to the retraction of 28 papers by several Informa journals, and the resignation of an editor.
Moon’s was not an isolated case. In the past 2 years, journals have been forced to retract more than 110 papers in at least 6 instances of peer-review.
PEER-REVIEW RING
Moon’s case is by no means the most spectacular instance of peer-review rigging in recent years. That honour goes to a case that came to light in May 2013, when Ali Nayfeh, then editor-in-chief of the Journal of Vibration and Control, received some troubling news. An author who had submitted a paper to the journal told Nayfeh that he had received e-mails about it from two people claiming to be reviewers. Reviewers do not normally have direct contact with authors, and — strangely — the e-mails came from generic-looking Gmail accounts rather than from the professional institutional accounts that many academics use (see ‘Red flags in review’).
Nayfeh alerted SAGE, the company in Thousand Oaks, California, that publishes the journal. The editors there e-mailed both the Gmail addresses provided by the tipster, and the institutional addresses of the authors whose names had been used, asking for proof of identity and a list of their publications.ew rigging. What all these cases had in common was that researchers exploited vulnerabilities in the publishers’ computerized systems to dupe editors into accepting manuscripts, often by doing their own reviews. The cases involved publishing behemoths Elsevier, Springer, Taylor & Francis, SAGE and Wiley, as well as Informa, at least one of the systems — could make researchers vulnerable to even more serious identity theft. “For a piece of software that’s used by hundreds of thousands of academics worldwide, it really is appalling,” says Mark Dingemanse, a linguist at the Max Planck Institute for Psycholinguistics in Nijmegen, the Netherlands, who has used some of these programs to publish and review papers.
A 14-month investigation that came to involve about 20 people from SAGE’s editorial, legal and production departments. It showed that the Gmail addresses were each linked to accounts with Thomson Reuters’ ScholarOne, a publication-management system used by SAGE and several other publishers, including Informa. Editors were able to track every paper that the person or people behind these accounts had allegedly written or reviewed, says SAGE spokesperson Camille Gamboa. They also checked the wording of reviews, the details of author-nominated reviewers, reference lists and the turnaround time for reviews (in some cases, only a few minutes). This helped the investigators to ferret out further suspicious-looking accounts; they eventually found 130.
SAGE investigators came to realize that authors were both reviewing and citing each other at an anomalous rate. Eventually, 60 articles were found to have evidence of peer-review tampering, involvement in the citation ring or both. “Due to the serious nature of the findings, we wanted to ensure we had researched all avenues as carefully as possible before contacting any of the authors and reviewers,” says Gamboa. When the dust had settled, it turned out that there was one author in the centre of the ring: Peter Chen, an engineer then at the National Pingtung University of Education (NPUE) in Taiwan, who was a co-author on practically all of the papers in question.
PASSWORD LOOPHOLE
Moon and Chen both exploited a feature of ScholarOne’s automated processes. When a reviewer is invited to read a paper, he or she is sent an e-mail with login information. If that communication goes to a fake e-mail account, the recipient can sign into the system under whatever name was initially submitted, with no additional identity verification. Jasper Simons, vice-president of product and market strategy for Thomson Reuters in Charlottesville, Virginia, says that ScholarOne is a respected peer-review system and that it is the responsibility of journals and their editorial teams to invite properly qualified reviewers for their papers.
ScholarOne is not the only publishing system with vulnerabilities. Editorial Manager, built by Aries Systems in North Andover, Massachusetts, is used by many societies and publishers, including Springer and PLOS. The American Association for the Advancement of Science in Washington DC uses a system developed in-house for its journals Science, Science Translational Medicine and Science Signaling, but its open-access offering, Science Advances, uses Editorial Manager. Elsevier, based in Amsterdam, uses a branded version of the same product, called the Elsevier Editorial System.
Usually, editors in the United States and Europe know the scientific community in those regions well enough to catch potential conflicts of interest between authors and reviewers. But Lindsay says that Western editors can find this harder with authors from Asia — “where often none of us knows the suggested reviewers”. In these cases, the journal insists on at least one independent reviewer, identified and invited by the editors.



")