Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Article SELECTION from Collection of Aviva Lev-Ari, PhD, RN Scientific Articles on PULSE on LinkedIn.com for Training Small Language Models (SLMs) in Domain-aware Content of Medical, Pharmaceutical, Life Sciences and Healthcare by 15 Subjects Matter
Article selection: Aviva Lev-Ari, PhD, RN
#1 – February 20, 2016
Contributions to Personalized and Precision Medicine & Genomic Research
Resitu Medical Sets Stage for Breakthrough in Breast Tumour Removal
Curator: Dr. Sudipta Saha, Ph.D.
Resitu Medical, a Swedish company specializing in minimally invasive breast tumour removal, has announced the appointment of Stefan Sowa as its new Chief Executive Officer. Strategic leadership is being strengthened as the company moves towards commercialization in both European and American markets.
A novel electrosurgical device, designed to excise entire breast lesions during the biopsy procedure, is being developed by Resitu. The device is intended to minimize the need for open surgery by allowing intact removal of tissue with minimal bleeding, guided by real-time ultrasound imaging. Preclinical studies are currently being conducted, and preparations for FDA clearance and CE marking are underway.
ISO 13485 certification for the design, development, manufacturing, and sales of the device has been successfully obtained. Investment has been secured from major shareholders, including Novoaim, ALMI Invest Stockholm, and STOAF, to support the finalization of the product and the initiation of serial production for clinical trials.
Through the use of its technology, false negatives are hoped to be reduced, while patient outcomes and diagnostic accuracy are expected to be significantly improved. The burden on healthcare systems may also be alleviated by minimizing the need for recalls and secondary biopsies.
Positive attention has been garnered at major medical conferences, with workshops hosted at events such as the Uppsala Breast Meeting, and favourable media coverage has been achieved. With Stefan Sowa at the helm, Resitu’s innovative device is poised to transform breast cancer management practices globally.
#TUBiol5227: Biomarkers & Biotargets: Genetic Testing and Bioethics
Curator: Stephen J. Williams, Ph.D.
The advent of direct to consumer (DTC) genetic testing and the resultant rapid increase in its popularity as well as companies offering such services has created some urgent and unique bioethical challenges surrounding this niche in the marketplace. At first, most DTC companies like 23andMe and Ancestry.com offered non-clinical or non-FDA approved genetic testing as a way for consumers to draw casual inferences from their DNA sequence and existence of known genes that are linked to disease risk, or to get a glimpse of their familial background. However, many issues arose, including legal, privacy, medical, and bioethical issues. Below are some articles which will explain and discuss many of these problems associated with the DTC genetic testing market as well as some alternatives which may exist.
As you can see,this market segment appears to want to expand into the nutritional consulting business as well as targeted biomarkers for specific diseases.
Rising incidence of genetic disorders across the globe will augment the market growth
Increasing prevalence of genetic disorders will propel the demand for direct-to-consumer genetic testing and will augment industry growth over the projected timeline. Increasing cases of genetic diseases such as breast cancer, achondroplasia, colorectal cancer and other diseases have elevated the need for cost-effective and efficient genetic testing avenues in the healthcare market.
For instance, according to the World Cancer Research Fund (WCRF), in 2018, over 2 million new cases of cancer were diagnosed across the globe. Also, breast cancer is stated as the second most commonly occurring cancer. Availability of superior quality and advanced direct-to-consumer genetic testing has drastically reduced the mortality rates in people suffering from cancer by providing vigilant surveillance data even before the onset of the disease. Hence, the aforementioned factors will propel the direct-to-consumer genetic testing market overt the forecast timeline.
Nutrigenomic Testing will provide robust market growth
The nutrigenomic testing segment was valued over USD 220 million market value in 2019 and its market will witness a tremendous growth over 2020-2028. The growth of the market segment is attributed to increasing research activities related to nutritional aspects. Moreover, obesity is another major factor that will boost the demand for direct-to-consumer genetic testing market.
Nutrigenomics testing enables professionals to recommend nutritional guidance and personalized diet to obese people and help them to keep their weight under control while maintaining a healthy lifestyle. Hence, above mentioned factors are anticipated to augment the demand and adoption rate of direct-to-consumer genetic testing through 2028.
Browse key industry insights spread across 161 pages with 126 market data tables & 10 figures & charts from the report, “Direct-To-Consumer Genetic Testing Market Size By Test Type (Carrier Testing, Predictive Testing, Ancestry & Relationship Testing, Nutrigenomics Testing), By Distribution Channel (Online Platforms, Over-the-Counter), By Technology (Targeted Analysis, Single Nucleotide Polymorphism (SNP) Chips, Whole Genome Sequencing (WGS)), Industry Analysis Report, Regional Outlook, Application Potential, Price Trends, Competitive Market Share & Forecast, 2020 – 2028” in detail along with the table of contents: https://www.gminsights.com/industry-analysis/direct-to-consumer-dtc-genetic-testing-market
Targeted analysis techniques will drive the market growth over the foreseeable future
Based on technology, the DTC genetic testing market is segmented into whole genome sequencing (WGS), targeted analysis, and single nucleotide polymorphism (SNP) chips. The targeted analysis market segment is projected to witness around 12% CAGR over the forecast period. The segmental growth is attributed to the recent advancements in genetic testing methods that has revolutionized the detection and characterization of genetic codes.
Targeted analysis is mainly utilized to determine any defects in genes that are responsible for a disorder or a disease. Also, growing demand for personalized medicine amongst the population suffering from genetic diseases will boost the demand for targeted analysis technology. As the technology is relatively cheaper, it is highly preferred method used in direct-to-consumer genetic testing procedures. These advantages of targeted analysis are expected to enhance the market growth over the foreseeable future.
Over-the-counter segment will experience a notable growth over the forecast period
The over-the-counter distribution channel is projected to witness around 11% CAGR through 2028. The segmental growth is attributed to the ease in purchasing a test kit for the consumers living in rural areas of developing countries. Consumers prefer over-the-counter distribution channel as they are directly examined by regulatory agencies making it safer to use, thereby driving the market growth over the forecast timeline.
Favorable regulations provide lucrative growth opportunities for direct-to-consumer genetic testing
Europe direct-to-consumer genetic testing market held around 26% share in 2019 and was valued at around USD 290 million. The regional growth is due to elevated government spending on healthcare to provide easy access to genetic testing avenues. Furthermore, European regulatory bodies are working on improving the regulations set on the direct-to-consumer genetic testing methods. Hence, the above-mentioned factors will play significant role in the market growth.
Focus of market players on introducing innovative direct-to-consumer genetic testing devices will offer several growth opportunities
Few of the eminent players operating in direct-to-consumer genetic testing market share include Ancestry, Color Genomics, Living DNA, Mapmygenome, Easy DNA, FamilytreeDNA (Gene By Gene), Full Genome Corporation, Helix OpCo LLC, Identigene, Karmagenes, MyHeritage, Pathway genomics, Genesis Healthcare, and 23andMe. These market players have undertaken various business strategies to enhance their financial stability and help them evolve as leading companies in the direct-to-consumer genetic testing industry.
For example, in November 2018, Helix launched a new genetic testing product, DNA discovery kit, that allows customer to delve into their ancestry. This development expanded the firm’s product portfolio, thereby propelling industry growth in the market.
The following posts discuss bioethical issues related to genetic testing and personalized medicine from a clinicians and scientisit’s perspective
Question:Each of these articles discusses certain bioethical issues although focuses on personalized medicine and treatment. Given your understanding of the robust process involved in validating clinical biomarkers and the current state of the DTC market, how could DTC testing results misinform patients and create mistrust in the physician-patient relationship?
Question: If you are developing a targeted treatment with a companion diagnostic, what bioethical concerns would you address during the drug development process to ensure fair, equitable and ethical treatment of all patients, in trials as well as post market?
Articles on Genetic Testing, Companion Diagnostics and Regulatory Mechanisms
Question: What type of regulatory concerns should one have during the drug development process in regards to use of biomarker testing?From the last article on Protecting Your IP how important is it, as a drug developer, to involve all payers during the drug development process?
Can the Public Benefit Company Structure Save US Healthcare?
Curator: Stephen J. Williams, Ph.D.
UPDATED 11/05/2023
Public Benefit Corporation structure in healthcare has actually been around since the 1970s in New Yourk State, when New York City’s new Health and Hospitals Corporation took over the city Department of Hospitals and today runs 11 hospitals and four long-term care facitlites in the city. The following link to an article describes however the problems occuring with Nassau and Westchester hosptial systems, which were converted to New York PBC status in the 1990s. As the article states the financial problems in 2004 which these hospitals encountered
do not stem from their unusual status as public benefit corporations, and might have been even worse off had they not converted
The New York Times article of 2004 “At 2 Hospitals, Fiscal Troubles in the Glare of Public View” highlight in fact the growing problem that all hospitals are encountering, especially on the fiscal side. But it does highlight how to better structure these entities and why full commitment to the PBC structure is necessary.
In 2003 New York State had a record closure of hospitals, and in 2004 Nassau and WestChester were having such fiscal problems it threatened the bond status of those counties. Despite the regular problems hospitals had, critics had said there were two major contributing factors to their woes
the two agencies had not completed their transition from government operations to fully competitve hospitals
as a PBC they bear a costly mission of serving the uninsured
As a PBC the structure allows one to shed cumbersome government rules, giving them the flexibility to conduct business like other hospitals.
In addition they are no longer dependent, in fact now forced, to forgo dependence on public funding and look for independent means of investment. With their semi-independence from government the agencies also are more insulted from political pressure.
However this seemed to be the problem. These agencies were still to dependent on their local government and there was still local political influence on their boards.
UPDATED 3/15/2023
According to Centers for Medicare and Medicare Services (CMS.gov) healthcare spending per capita has reached 17.7percent of GDP with, according to CMS data:
From 1960 through 2013, health spending rose from $147 per person to $9,255 per person, an average annual increase of 8.1 percent.
the National Health Expenditure Accounts (NHEA) are the official estimates of total health care spending in the United States. Dating back to 1960, the NHEA measures annual U.S. expenditures for health care goods and services, public health activities, government administration, the net cost of health insurance, and investment related to health care. The data are presented by type of service, sources of funding, and type of sponsor.
Graph: US National Healthcare Expenditures as a percent of Gross Domestic Product from 1960 to current. Recession periods are shown in bars. Note that the general trend has been increasing healthcare expenditures with only small times of decrease for example 2020 in year of COVID19 pandemic. In addition most of the years have been inflationary with almost no deflationary periods, either according to CPI or healthcare costs, specifically.
U.S. health care spending grew 4.6 percent in 2019, reaching $3.8 trillion or $11,582 per person. As a share of the nation’s Gross Domestic Product, health spending accounted for 17.7 percent.
And as this spending grew (demand for health care services) associated costs also rose but as the statistical analyses shows there was little improvement in many health outcome metrics during the same time.
Graph of the Growth of National Health Expenditures (NHE) versus the growth of GDP. Note most years from 1960 growth rate of NHE has always been higher than GDP, resulting in a seemingly hyperinflationary effect of healthcare. Also note how there are years when this disconnect is even greater, as there were years when NHE grew while there were recessionary periods in the general economy.
It appears that US healthcare may be on the precipice of a transformational shift, but what will this shift look like? The following post examines if the corporate structure of US healthcare needs to be changed and what role does a Public Benefit Company have in this much needed transformation.
Hippocratic Oath
I swear by Apollo the physician, and Asclepius, and Hygieia and Panacea and all the gods and goddesses as my witnesses, that, according to my ability and judgement, I will keep this Oath and this contract:
To hold him who taught me this art equally dear to me as my parents, to be a partner in life with him, and to fulfill his needs when required; to look upon his offspring as equals to my own siblings, and to teach them this art, if they shall wish to learn it, without fee or contract; and that by the set rules, lectures, and every other mode of instruction, I will impart a knowledge of the art to my own sons, and those of my teachers, and to students bound by this contract and having sworn this Oath to the law of medicine, but to no others.
I will use those dietary regimens which will benefit my patients according to my greatest ability and judgement, and I will do no harm or injustice to them.
I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; and similarly I will not give a woman a pessary to cause an abortion.
In purity and according to divine law will I carry out my life and my art.
I will not use the knife, even upon those suffering from stones, but I will leave this to those who are trained in this craft.
Into whatever homes I go, I will enter them for the benefit of the sick, avoiding any voluntary act of impropriety or corruption, including the seduction of women or men, whether they are free men or slaves.
Whatever I see or hear in the lives of my patients, whether in connection with my professional practice or not, which ought not to be spoken of outside, I will keep secret, as considering all such things to be private.
So long as I maintain this Oath faithfully and without corruption, may it be granted to me to partake of life fully and the practice of my art, gaining the respect of all men for all time. However, should I transgress this Oath and violate it, may the opposite be my fate.
Translated by Michael North, National Library of Medicine, 2002.
Much of the following information can be found on the Health AffairsBlog in a post entitled
Limitations of For Profit and Non-Profit Hospitals
For profit represent ~ 25% of US hospitals and are owned and governed by shareholders, and can raise equity through stock and bond markets.
According to most annual reports, the CEOs incorrectly assume they are legally bound as fiduciaries to maximize shareholder value. This was a paradigm shift in priorities of companies which started around the mid 1980s,aphenomenon discussed below.
A by-product of this business goal, to maximize shareholder value, is that CEO pay and compensation is naturally tied to equity markets. A means for this is promoting cost efficiencies, even in the midst of financial hardships.
A clear example of the failure of this system can be seen during the 2020- current COVID19 pandemic in the US. According to the Medicare Payment Advisory Commission, four large US hospitals were able to decrease their operating expenses by $2.3 billion just in Q2 2020. This amounted to 65% of their revenue; in comparison three large NONPROFIT hospitals reduced their operating expense by an aggregate $13 million (only 1% of their revenue), evident that in lean times for-profit will resort to drastic cost cutting at expense of service, even in times of critical demands for healthcare.
Because of their tax structure and perceived fiduciary responsibilities, for-profit organizations (unlike non-profit and public benefit corporations) are not legally required to conduct community health need assessments, establish financial assistance policies, nor limit hospital charges for those eligible for financial assistance. In addition to the difference in tax liability, for-profit, unlike their non-profit counterparts, at least with hospitals, are not funded in part by state or local government. As we will see, a large part of operating revenue for non-profit university based hospitals is state and city funding.
Therefore risk for financial responsibility is usually assumed by the patient, and in worst case, by the marginalized patient populations on to the public sector.
Tax Structure Considerations of for-profit healthcare
Financials of major for-profit healthcare entities (2020 annual)
Non-profit Healthcare systems
Nonprofits represent about half of all hospitals in the US. Most of these exist as a university structure, so retain the benefits of being private health systems and retaining the funding and tax benefits attributed to most systems of higher education. And these nonprofits can be very profitable. After taking in consideration the state, local, and federal tax exemptions these nonprofits enjoy, as well as tax-free donations from contributors (including large personal trust funds), a nonprofit can accumulate a large amount of revenue after expenses. In fact 82 nonprofit hospitals had $33 billion of net asset increase year-over-year (20% increase) from 2016 to 2017. The caveat is that this revenue over expenses is usually spent on research or increased patient services (this may mean expanding the physical infrastructure of the hospital or disseminating internal grant money to clinical investigators, expanding the hospital/university research assets which could result in securing even larger amount of external funding from government sources.
And although this model may work well for intercity university/healthcare systems, it is usually a struggle for the rural nonprofit hospitals. In 2020, ten out of 17 rural hospitals that went under were nonprofits. And this is not just true in the tough pandemic year. Over the past two decades multitude of nonprofit rural hospitals had to sell and be taken over by larger for-profit entities.
Hospital consolidation has led to a worse patient experience and no real significant changes in readmission or mortality data. (The article below is how over 130 rural hospitals have closed since 2010, creating a medical emergency in rural US healthcare)
And according to the article below it is only to get worse
The authors of the Health Affairs blog feel a major disadvantage of both the for-profit and non-profit healthcare systems is “that both face limited accountability with respect to anticompettive mergers and acquisitions.”
More hospital consolidation is expected post-pandemic
Hospital deal volume is likely to accelerate due to the financial damage inflicted by the coronavirus pandemic.
The anticipated increase in volume did not show up in the latest quarter, when deals were sharply down.
The pandemic may have given hospitals leverage in coming policy fights over billing and the creation of “public option” health plans.
Hospital consolidation is likely to increase after the COVID-19 pandemic, say both critics and supporters of the merger-and-acquisition (M&A) trend.
The financial effects of the coronavirus pandemic are expected to drive more consolidation between and among hospitals and physician practices, a group of policy professionals told a recent Washington, D.C.-based web briefing sponsored by the Alliance for Health Policy.
“There is a real danger that this could lead to more consolidation, which if we’re not careful could lead to higher prices,” said Karyn Schwartz, a senior fellow at the Kaiser Family Foundation (KFF).
Schwartz cited a recent KFF analysis of available research that concluded “provider consolidation leads to higher health care prices for private insurance; this is true for both horizontal and vertical consolidation.”
Kenneth Kaufman, managing director and chair of Kaufman Hall, noted that crises tend to push financially struggling organizations “further behind.”
“I wouldn’t be surprised at all if that happens,” Kaufman said. “That will lead to further consolidation in the provider market.”
The initial rounds of federal assistance from the CARES Act, which were based first on Medicare revenue and then on net patient revenue, may fuel consolidation, said Mark Miller, PhD, executive vice president of healthcare for Arnold Ventures. That’s because the funding formulas favored organizations that already had higher revenues, he said, and provided less assistance to low-revenue organizations.
HHS has distributed $116.2 billion from the $175 billion in provider funding available through the CARES Act and the Paycheck Protection Program and Health Care Enhancement Act. The largest distributions used the two revenue formulas cited by Miller.
No surge in M&A yet
The expected burst in hospital M&A activity has yet to occur. Kaufman Hall identified 14 transactions in the second quarter of 2020, far fewer than in the same quarter in any of the four preceding years, when second-quarter transactions totaled between 19 and 31. The latest deals were not focused on small hospitals, with average seller revenue of more than $800 million — far larger than the previous second-quarter high of $409 million in 2018.
Six of the 14 announced transactions were divestitures by major for-profit health systems, including Community Health Systems, Quorum and HCA.
Kaufman Hall’s analysis of the recent deals identified another pandemic-related factor that may fuel hospital M&A: closer ties between hospitals. The analysis cited the example of Lifespan and Care New England, which had suspended merger talks in 2019. More recently, in a joint announcement, the CEOs of the two systems noted that because of the COVID-19 crisis, the two systems “have been working together in unprecedented ways” and “have agreed to enter into an exploration process to understand the pros and cons of what a formal continuation of this collaboration could look like in the future.”
The M&A outlook for rural hospitals
The pandemic has had less of a negative effect on the finances of rural hospitals that previously joined larger health systems, said Suzie Desai, senior director of not-for-profit healthcare for S&P Global.
A CEO of a health system with a large rural network told Kaufman the federal grants that the system received for its rural hospitals were much larger than the grants paid through the general provider fund.
“If that was true across the board, then the federal government recognized that many rural hospitals could be at risk of not being able to make payroll; actually running out of money,” Kaufman said. “And they seem to have bent over backwards to make sure that didn’t happen.”
Other CARES Act funding distributed to providers included:
$12.8 billion for 959 safety net hospitals
$11 billion to almost 4,000 rural healthcare providers and hospitals in urban areas that have certain special rural designations in Medicare
Telehealth has helped rural hospitals but has not been sufficient to address the financial losses inflicted by the pandemic, Desai said.
Other coming trends include a sharper cost focus
Desai expects an increasing focus “over the next couple years” on hospital costs because of the rising share of revenue received from Medicare and Medicaid. She expects increased efforts to use technology and data to lower costs.
Billy Wynne, JD, chairman of Wynne Health Group, expects telehealth restrictions to remain relaxed after the pandemic.
Also, the perceptions of the public and politicians about the financial health of hospitals are likely to give those organizations leverage in coming policy fights over changes such as banning surprise billing and creating so-called public-option health plans, Wynne said. As an example, he cited the Colorado legislature’s suspension of the launch of a public option “in part because of sensitivities around hospital finances in the COVID pandemic.”
“Once the dust settles, it’ll be interesting to see if their leverage has increased or decreased due to what we’ve been through,” Wynne said.
About the Author
Rich Daly, HFMA Senior Writer and Editor,
is based in the Washington, D.C., office. Follow Rich on Twitter: @rdalyhealthcare
The quality of care at hospitals acquired during a recent wave of consolidations has gotten worse or stayed the same, according to a study led by Harvard Medical School scientists published Jan. 2 in NEJM.
The findings deal a blow to the often-cited arguments that hospital consolidation would improve care. A flurry of earlier studies showed that mergers increase prices. Now after analyzing patient outcomes after hundreds of hospital mergers, the new research also dashes the hopes that this more expensive care might be of higher quality.
Get more HMS news here
“Our findings call into question claims that hospital mergers are good for patients—and beg the question of what we are getting from higher hospital prices,” said study senior author J. Michael McWilliams, the Warren Alpert Foundation Professor of Health Care Policy in the Blavatnik Institute at HMS and an HMS professor of medicine and a practicing general internist at Brigham and Women’s Hospital.
McWilliams noted that rising hospital prices have been one of the leading drivers of unsustainable growth in U.S. health spending.
To examine the impact of hospital mergers on quality of care, researchers from HMS and Harvard Business School examined patient outcomes from nearly 250 hospital mergers that took place between 2009 and 2013. Using data collected by the Centers for Medicare and Medicaid Services, they analyzed variables such as 30-day readmission and mortality rates among patients discharged from a hospital, as well as clinical measures such as timely antibiotic treatment of patients with bacterial pneumonia. The researchers also factored in patient experiences, such as whether those who received care at a given hospital would recommend it to others. For their analysis, the team compared trends in these indicators between 246 hospitals acquired in merger transactions and unaffected hospitals.
The verdict? Consolidation did not improve hospital performance, and patient-experience scores deteriorated somewhat after the mergers.
The study was not designed to examine the reasons behind the worsening in patient experience. Weakening of competition due to hospital mergers could have contributed, the researchers said, but deeper exploration suggested other potential mechanisms. Notably, the analysis found the decline in patient-experience scores occurred mainly in hospitals acquired by hospitals that already had a poor patient-experience score—a finding that suggests acquisitions facilitate the spread of low quality care but not of high quality care.
The researchers caution that isolated, individual mergers may have still yielded positive results—something that an aggregate analysis is not powered to capture. And the researchers could only examine measurable aspects of quality. The trend in hospital performance on these standard measures, however, appears to point to a net effect of overall decline, the team said.
“Since our study estimated the average effects of mergers, we can’t rule out the possibility that some mergers are good for patient care,” said first author Nancy Beaulieu, research associate in health care policy at HMS. “But this evidence should give us pause when considering arguments for hospitals mergers.”
The work was supported by the Agency for Healthcare Research and Quality (grant no. U19HS024072).
Co-investigators included Bruce Landon and Jesse Dalton from HMS, Ifedayo Kuye, from the University of California, San Francisco, and Leemore Dafny from Harvard Business School and the National Bureau of Economic Research.
Public benefit corporations (versus Benefit Corporate status, which is more of a pledge) are separate legal entities which exist as a hybrid, for-profit/nonprofit company but is mandated to
Pursue a general or specific public benefit
Consider the non-financial interests of its shareholders and other STAKEHOLDERS when making decision
report how well it is achieving its overall public benefit objectives
Have limited fiduciary responsibility to investors that remains IN SCOPE of public benefit goal
In essence, the public benefit corporations executives are mandated to run the company for the benefit of STAKEHOLDERS first, if those STAKEHOLDERS are the public beneficiary of the company’s goals. This in essence moves the needle away from the traditional C-Corp overvaluing the needs of shareholders and brings back the mission of the company and in the case of healthcare, the needs of its stakeholders, the consumers of healthcare.
PBCs are legal entities recognized by states rather than by the federal government. So far, in 2020 about 37 states allow companies to incorporate as a PBC. Stipulations of the charter include semiannual reporting of the public benefits bestowed by the company and how well it is achieving its public benefit mandate. There are about 3,000 US PBCs. Some companies have felt it was in their company mission and financial interest to change incorporation as a PBC.
Some well known PBCs include
Ben and Jerry’s Ice Cream
American Red Cross
Susan B. Komen Foundation
Allbirds (a shoe startup valued at $1.7 billion when made switch)
Bombas (the sock company that donates extra socks when you buy a pair)
Lemonade (a publicly traded insurance PBC that has beneficiaries select a nonprofit that the company will donate to)
Although the number of PBCs in the healthcare arena is increasing
Not many PBCs are in the area of healthcare delivery
Noone is quite sure what the economic model would look like for a healthcare delivery PBC
Some example of hospital PBC include NYC Health + Hospitals and Community First Medical Center in Chicago.
Benefits of moving a hospital to PBC Status
PBCs are held legally accountable to a predefined public benefit. For hospitals this could be delivering cost-effective quality of care and affordable to a local citizenry or an economically disadvantaged population. PBCs must produce at least an annual report on the public benefits it has achieved contrasted against a third party standard. For example a hospital could include data of Medicaid related mortality risks, data neither the C-corp nor the nonprofit 501c would have to report on. Most nonprofits and charities report their taxes on a schedule H or Form 990, which only has to report the officer’s compensation as well as monies given to charitable organizations, or other 501 organizations. The nonprofit would show a balance of zero as the donated money for that year would be allocated out for various purposes. Hospitals, even as nonprofits, are not required to submit all this data. Right now in US the ACA just requires any hospital that receives government or ACA insurance payments to report certain outcome statistics. Although varying state by state, a PBC should have a “benefit officer” to make sure the mandate is being met. In some cases a PBC benefit officer could sue the board for putting shareholder interest over the public benefit mandate.
A PBC can include community stakeholders in the articles of incorporation thus giving a voice to local community members. This would be especially beneficial for a hospital serving, say, a rural community.
PBCs do have advantages of the for-profit companies as they are not limited to non-equity forms of investment. A PBC can raise money in the equity markets or take on debt and finance it. These financial instruments are unavailable to the non-profit. Yet one interesting aspect is that PBCs require a HIGHER voting threshold by shareholders than a traditional for profit company in the ability to change their public benefit or convert their PBC back to a for-profit.
Limitations of the PBC
Little incentive financially for current and future hospitals to incorporate as a PBC. Herein lies a huge roadblock given the state of our reimbursement structure in this country. Although there may be an incentive with regard to hiring and retention of staff drawn to the organization’s social purpose. There have been, in the past, suggestions to allow hospitals that incorporate at PBC to receive some tax benefit, but this legislation has not gone through either at state or federal level. (put link to tax article).
In order for there to be value to constituents (patients) there must be strong accountability measures. This will require the utmost in ethical behavior by a board and executives. We have witnessed, through M&A by large health groups, anticompetitive and near monopoly behavior.
There are no federal guidelines but varying guidelines from state to state. There must be some federal recognition of the PBC status when it comes to healthcare, such as that the government is one of the biggest payers of US healthcare.
This is a great interview with ArcHealth, a PBC healthcare system.
Arc Health PBC is a public benefit corporation, a mission-driven for-profit company that utilizes a market-driven approach to achieving our short and long-term social goals. As a public benefit corporation, Arc Health is also a social enterprise working to further our mission of providing healthcare to rural, underserved, and indigenous communities through business practices that improve the recruitment and retention of quality healthcare providers.
What is a Social Enterprise?
While there is no one exact definition, according to the Social Enterprise Alliance, a social enterprise is an “organization that addresses a basic unmet need or solves a social or environmental problem through a market-driven approach.” A social enterprise is not a distinct legal entity, but instead, an “ideological spectrum marrying commercial approaches with social good.” Social enterprises foster a dual-bottom-line – simultaneously seeking profits and social impact. Arc Health, like many social enterprises, seeks to be self–sustainable.
Two primary structures fall under the social enterprise umbrella: nonprofits and for-profit organizations. There are also related entities within both structures that could be considered social enterprises. Any of these listed structures can be regarded as a social enterprise depending on if and how involved they are with socially beneficial programs.
What is a Public Benefit Corporation?
Public Benefit Corporations (PBCs), also known as benefit corporations, are “for-profit companies that balance maximizing value to stakeholders with a legally binding commitment to a social or environmental mission.” PBCs operate as for-profit entities with no tax advantages or exemptions. Still, they must have a “purpose of creating general public benefit,” such as promoting the arts or science, preserving the environment, or providing benefits to underserved communities. PBCs must attain a higher degree of corporate purpose, expanded accountability, and expected transparency.
There are now over 3,000 registered PBCs, comprising approximately 0.1% of American businesses.
As a PBC, Arc Health expects to access capital through individual investors who seek financial returns, rather than through donations. Arc Health’s investors make investments with a clear understanding of the balance the company must strike between financial returns (I.e., profitability) and social purpose. Therefore, investors expect the company to be operationally profitable to ensure a financial return on their investments, while also making clear to all stakeholders and the public that generating social impact is the priority.
What is the difference between a Social Enterprise and PBC?
Social enterprises and PBCs emulate similar ideals that value the importance and need to invoke social change vis-a-vis working in a market-driven industry. Public benefit corporations fall under the social enterprise umbrella. An organization may choose to use a social enterprise model and incorporate itself as either a not-for-profit, C-Corp, PBC, or other corporate structure.
How did Arc Health Become a Public Benefit Corporation?
Arc Health was initially formed as a C-Corp. In 2019, Arc Health’s CEO and Co-Founder, Dave Shaffer, guided the conversion from a C-Corp to a PBC, incorporated in Delaware. Today, Arc Health follows guidelines and expectations for PBCs, including adhering to the State of Delaware’s requirements for PBCs.
Why is Arc Health a Social Enterprise and Public Benefit Corporation?
Arc Health believes it is essential to commit ourselves to our mission and demonstrate our dedication through our actions. We work to adhere to the core values of accountability, transparency, and purpose. As a registered public benefit company and a social enterprise, we execute our drive to achieve health equity in tangible and effective ways that the communities we work with, our stakeholders, and our providers expect of us.
90% of Americans say that companies must not only say a product or service is beneficial, but they also need to prove its benefit.
When we partner with health clinics and hospitals, we aim to provide services that enact lasting change. For example, we work with healthcare providers who desire to contribute both clinical and non-clinical skills. In 2020, Arc Health clinicians developed COVID-19 response protocols and educational materials about the vaccines. They participated in pain management working groups. They identified and followed up with kids in the community who were overdue for a well-child check. Arc Health providers should be driven by a desire to develop a long-term relationship with a healthcare service provider and participate in its successes and challenges.
Paradigm Shift in the 1980’s: Companies Start to Emphasize Shareholders Over Stakeholders
So earlier in this post we had mentioned about a shift in philosophy at the corporate boardroom that affected how comparate thought, value, and responsibility: Companies in the 1980s started to shift their focus and value only the needs of corporate ShAREHOLDERS at the expense of their traditional STAKEHOLDERS (customers, clients). Many movies and books have been written on this and debatable if deliberate or a by-product of M&A, hostile takeovers, and the stock market in general but the effect was that the consumer was relegated as having less value, even though marketing budgets are very high. The fiduciary responsibility of the executive was now defined in terms of satisfying shareholders, who were now big huge and powerful brokerage houses, private equity, and hedge funds. A good explanation by Medium.com Tyler Lasicki is given below.
In a famous 1970 New York Times Article, Milton Friedman postulated that the CEO, as an employee of the shareholder, must strive to provide the highest possible return for all shareholders. Since that article, the United States has embraced this idea as the fundamental philosophy supporting the ultimate purpose of businesses — The Shareholders Come First.
In August of 2019, the Business Roundtable, a group made up of the most influential U.S CEOs, published a letter shifting their stance on the purpose of a corporation. Regardless of whether this piece of paper will actually result in any systematic changes has yet to be seen, however this newly stated purpose of business is a dramatic shift from the position Milton Friedman took in 1970. According to the statement, these corporations will no longer prioritize maximizing profits for shareholders, but instead turn their focus to benefiting all stakeholders — including citizens, customers, suppliers, employees, on par with shareholders.
Now the social responsibility of a company and the CEO was to maxiimize the profits even at the expense of any previous social responsibility they once had.
Small sample of the 181 Signatures attached to the Business Roundtable’s letter
What has happened over the past 50 years that has led to such a fundamental change in ideology? What has happened to make the CEO’s of America’s largest corporations suddenly change their stance on such a foundational principle of what it means to be an American business?
Since diving into this subject, I have come to find that the “American fundamental principle” of putting shareholders first is one that is actually not all that fundamental. In fact, for a large portion of our nation’s history this ideology was actually seen as the unpopular position.
Key ideological shifts in U.S. history
This post dives into a brief history of these two contrasting ideological viewpoints in an attempt to contextualize the forces behind both sides — specifically, the most recent shift (1970–2019). This basic idea of what is most important; the stakeholder or the shareholder, is the underlying reason as to why many things are the way they are today. A corporation’s priority of shareholder or stakeholder ultimately impacts employee salaries, benefits, quality of life within communities, environmental conditions, even the access to education children can receive. It affects our lives in a breadth and depth of ways and now that corporations may be changing positions (yet again) to focus on a model that prioritizes the stakeholder, it is important to understand why.
Looking forward, if stakeholder priority ends up being the popular position among American businesses, how long will it last for? What could lead to its downfall? And what will managers do to ensure a long term stakeholder-friendly business model?
It is clear to me the reasons that have led to these shifts in ideology are rather nuanced, however I want to highlight a few trends that have had a major impact on businesses changing their priorities while also providing context as to why things have shifted.
The Ascendancy of Shareholder Value
Following the 1929 stock market crash and the Great Depression, stakeholder primacy became the popular perspective within corporate America. Stakeholder primacy is the idea that corporations are to consider a wider group of interested parties (not just shareholders) whose positions need to be taken into consideration by corporate governance. According to this point of view, rather than solely being an agent for shareholders, management’s responsibilities were to be dispersed among all of its constituencies, even if it meant a reduction in shareholder value. This ideology lasted as the dominant position for roughly 40 years, in part due to public opinion and strong views on corporate responsibility, but also through state adoption of stakeholder laws.
By the mid-1970s, falling corporate profitability and stagnant share prices had been the norm for a decade. This poor economic performance influenced a growing concern in the U.S. regarding the perceived divergence between manager and shareholder interest. Many held the position that profits and share prices were suffering as a result of corporation’s increased attention on stakeholder groups.
This noticeable divergence in interests sparked many academics to focus their research on corporate management’s motivations in decision making regarding their allocation of resources. This branch of research would later be known as agency theory, which focused on the relationship between principals (shareholders) and their agents (management). Research at the time outlined how over the previous decades corporate management had pursued strategies that were not likely to optimize resources from a shareholder’s perspective. These findings were part of a seismic shift of corporate philosophy, changing priority from the stakeholders of a business to the shareholders.
By 1982, the U.S. economy started to recover from a prolonged period of high inflation and low economic growth. This recovery acted as a catalyst for change in many industries, leaving many corporate management teams to struggle in response to these changes. Their business performance suffered as a result. These distressed businesses became targets for a group of new investors…private equity firms.
Now the paradigm shift had its biggest backer…. private equity! And private equity care about ONE thing….. THEIR OWN SHARE VALUE and subsequently meaning corporate profit, which became the most important directive for the CEO.
So it is all hopeless now? Can there be a shift back to the good ‘ol days?
Well some changes are taking place at top corporate levels which may help the stakeholders to have a voice at the table, as the following IRMagazine article states.
And once again this is being led by the Business Roundtable, the same Business Roundtable that proposed the shift back in the 1970s.
n a major corporate shift, shareholder value is no longer the main objective of the US’ top company CEOs, according to the Business Roundtable, which instead emphasizes the ‘purpose of a corporation’ and a stakeholder-focused model.
The influential body – a group of chief executive officers from major US corporations – has stressed the idea of a corporation dropping the age-old notion that corporations function first and foremost to serve their shareholders and maximize profits.
Rather, the focus should be on investing in employees, delivering value to customers, dealing ethically with suppliers and supporting outside communities as the vanguard of American business, according to a Business Roundtable statement.
‘While each of our individual companies serves its own corporate purpose, we share a fundamental commitment to all of our stakeholders,’ reads the statement, signed by 181 CEOs. ‘We commit to deliver value to all of them, for the future success of our companies, our communities and our country.’
Gary LaBranche, president and CEO of NIRI, tells IR Magazine that this is part of a wider trend: ‘The redefinition of purpose from shareholder-focused to stakeholder-focused is not new to NIRI members. For example, a 2014 IR Update article by the late Professor Lynn Stout urges a more inclusive way of thinking about corporate purpose.’
NIRI has also addressed this concept at many venues, including the senior roundtable annual meeting and the NIRI Annual Conference, adds LaBranche. This trend was further seen in the NIRI policy statement on ESG disclosure, released in January this year.
Analyzing the meaning of this change in more detail, LaBranche adds: ‘The statement is a revolutionary break with the Business Roundtable’s previous position that the purpose of the corporation is to create value for shareholders, which was a long-held position championed by Milton Friedman.
‘The challenge is that Friedman’s thought leadership helped to inspire the legal and regulatory regime that places wealth creation for shareholders as the ‘prime directive’ for corporate executives.
‘Thus, commentators like Mike Allen of Axios are quick to point out that some shareholders may actually use the new statement to accuse CEOs of worrying about things beyond increasing the value of their shares, which, Allen reminds us, is the CEOs’ fiduciary responsibility.
‘So while the new Business Roundtable statement reflects a much-needed rebalancing and modernization that speaks to the comprehensive responsibilities of corporate citizens, we can expect that some shareholders will push back on this more inclusive view of who should benefit from corporate efforts and the capital that makes it happen. The new statement may not mark the dawn of a new day, but it perhaps signals the twilight of the Friedman era.’
In a similarly reflective way, Jamie Dimon, chairman and CEO of JPMorgan Chase & Co and chairman of the Business Roundtable, says: ‘The American dream is alive, but fraying. Major employers are investing in their workers and communities because they know it is the only way to be successful over the long term. These modernized principles reflect the business community’s unwavering commitment to continue to push for an economy that serves all Americans.’
Note: Mr Dimon has been very vocal for many years on corporate social responsibility, especially since the financial troubles of 2009.
Impact of New Regulatory Trends in M&A Deals
The following podcast from Pricewaterhouse Cooper Health Research Institute (called Next in Health) discusses some of the trends in healthcare M&A and is a great listen. However from 6:30 on the podcast discusses a new trend which is occuring in the healthcare company boardroom, which is this new focus on integrating companies that have proven ESG (or environmental, social, governance) functions within their organzations. As stated, doing an M&A deal with a company with strong ESG is looked favorably among regulators now.
Please click on the following link to hear a Google Podcast Next in Health episode
Heather shows the feasability of this model with multiple biotech and healthtech startups, including one founded by Mark Cuban.
Health tech unicorn Aledade recently announced that it made the strategic decision to become a public benefit corporation (PBC).
The company joins just a handful of others in healthcare that are structured this way.
So what exactly is a PBC, and why does it matter?
PBCs are a type of for-profit corporate entity that has also adopted a public benefit purpose and is currently authorized by 35 states and the District of Columbia. A PBC must consider the nonfinancial interests of its shareholders and other stakeholders when making decisions. As a public benefit corporation, companies have to weigh their social/environmental objectives alongside maximizing value for shareholders.
While PBC and B Corp. are often used interchangeably, they are not the same. A B Corp. is a certification provided to eligible companies by the nonprofit, B Lab. A PBC is an actual legal entity that bakes into its certificate of incorporation a “public benefit,” according to Rubicon Law Group.
“I don’t think that there is a trade-off between either you do things that are good for society or you make profits in your business.” —Farzad Mostashari, M.D.
PBCs also are required to provide a report to shareholders every two years that detail how well the company is achieving its overall public benefit objectives. In some states, the report must be assessed against a third-party standard and be made publicly available. Delaware PBCs are not required to report publicly or against a third-party standard.
Aledade launched in 2014 and uses data analytics to help independent doctors’ offices transition to value-based care models. The company currently partners with more than 1,000 independent primary care practices comprising over 11,000 physicians and has nearly 150 contracts covering more than 1.7 million patients and $17 billion in total healthcare spending. Last June, the company raised $123 million in a series E round, boosting its valuation to $3.1 billion.
In a blog post, Aledade CEO and co-founder Farzad Mostashari, M.D., explained the company’s reasoning behind the move and said the corporate structure of a PBC is “well suited to mission-oriented companies where alignment with stakeholders is a key driver of the business model.”
“Aledade’s public benefit purpose means that we must weigh the interests of our primary care practice partners, their patients, our employees, and those who bear the burden of rising health care costs, alongside those of our shareholders, when we make decisions,” Mostashari said in an interview. This duty extends to all significant board decisions, including decisions on whether to go public, to make acquisitions or to sell the company, he noted.
The PBC structure helps create alignment among stakeholders and build trust, he said. “I don’t think that there is a trade-off between either you do things that are good for society or you make profits in your business. That might be true for fee-for-service businesses. It’s not true for Aledade,” he said.
He added, “For businesses that are built on trust and alignment, not considering stakeholder benefits gets you neither social good nor profits. If you’re in a business like our business where it’s actually really important that everybody have faith and belief that you are doing what’s best for patients, that you are actually in it for the long-term for practices, that’s what makes us successful as a business.”
Mark Cuban Cost Plus Drugs, which launched in January 2022 to offer low-cost rivals to overpriced generic drugs, also is structured as a public benefit corporation. The company’s founder and CEO Alexander Oshmyansky started the company in 2015 as a nonprofit, according to a feature story in D Magazine. Through Y Combinator, investors told Oshmyansky that the nonprofit model wouldn’t be able to raise the needed funds. He then reworked the business model to a PBC and launched Osh’s Affordable Pharmaceuticals in 2018.
Some other companies that are biotech drug development companies that operate under the PBC model include
Even a traditional for-profit C corporation can work toward a public mission without becoming a PBC. But, in an industry like healthcare, too often the duty to maximize financial returns for shareholders or investors can be in conflict with what is best for patients, executives say.
“With a startup, it might limit the ability to sell their business to a larger company in the future because there might be some limitations on what the larger company could do with the organization.”—Jodi Daniel, a partner in Crowell & Moring’s Health Care Group
According to some healthcare experts, PBCs offer a promising alternative as a business model for healthcare companies by providing a “North Star” by which a company can navigate critical business decisions.
“I think it really helps to drive accountability,” Huang, Osmind’s chief executive, said. “I think that’s important, especially in healthcare where it’s easy sometimes to get misaligned with all the different stakeholders that are involved in the industry. We wanted to make sure we had something to be accountable to. Second, it’s ingrained in the culture. The third element of why it was so helpful for us from the beginning is just on focus and alignment. I think we can be much more clear and transparent about what we’re focused on, our values, how we try to use that transparently to influence our decisions and how we can build a business that really ties all of that together.”
In a Health Affairs article, medical researchers at Stanford, including Jimmy Qian, a co-founder of Osmind, laid out the case for why PBCs may simultaneously improve individual patient outcomes and collective benefit without sacrificing institutions’ financial stability.
PBCs are held legally accountable to a predefined public benefit, which, for hospitals, could involve delivering high-quality, affordable care to local populations. PBCs are required to produce annual benefits reports that are assessed against a third-party standard. “These reports could be used by regulatory agencies such as the Centers for Medicare and Medicaid Services (CMS) or local health authorities to evaluate whether the PBC is making progress toward its stated mission and respond accordingly,” the researchers wrote.
But are there any trade-offs?
Having a public benefit obligation could potentially “tie the hands” of board members who can’t just focus on profits and must focus on those dual responsibilities, noted Jodi Daniel, a partner in Crowell & Moring’s Health Care Group.
“Companies that transition to being a public benefit corporation are intentionally trying to ensure that that the company’s mission doesn’t get diminished over time because it’s in their charter. So it helps [the mission] to endure. But there are pros and cons to that. It is somewhat binding the future board members and executives to follow that mission,” she said.
Daniel said she has spoken with several healthcare companies recently that are weighing the possibility of transitioning to a PBC. “Companies often don’t want to necessarily limit their options in their decision-making in the future. With a startup, it might limit the ability to sell their business to a larger company in the future because there might be some limitations on what the larger company could do with the organization,” she said in an interview.
By making decisions based on interests outside of financial ones, organizations may put themselves at a margin disadvantage as compared to pure for-profit players in the space, wrote Hospitalogy founder Blake Madden.
Faddis with Veeva said the company hasn’t seen any financial or performance trade-off as a result of operating as a PBC. He noted that the move has been good for recruiting, spurred more long-term conversations with customers and has been a source of new ideas.
“Prior to the conversion, you had employees who were thinking of new products or new functionality with the mindset of getting to be commercially successful,” Faddis said. “Now, you also have people thinking about it from the angle of, ‘Does it further one of our PBC purposes and then maybe it’s also going to be commercially successful?'”
Converting to a PBC also can be a tactic to build trust, Daniel noted, especially in healthcare, and that holds the potential to drive business.
One factor that isn’t clear is whether there is sufficient oversight to hold these companies accountable to their stated public mission. Who checks to make sure companies are making progress toward their objectives to improve healthcare?
Osmind publishes its benefit corporation report on its website to make it available to the public even though it is not required to do so. “I think that really highlights the accountability piece of you need to tell the world or at least tell your shareholders how you’re really trying to uphold your public benefit,” Huang said.
Other related articles published on this Open Access Online Scientific Journal on Healthcare Issues include the following:
Despite heated discussion over whether it works, the FDA has approved Aduhelm, bringing a new ray of hope to the Alzheimer’s patients.
Curator and Reporter: Dr. Premalata Pati, Ph.D., Postdoc
Despite heated discussion over whether it works, the FDA has approved Aduhelm, bringing a new ray of hope to the Alzheimer’s patients.
On Monday, 7th June 2021, a controversial new Alzheimer’sDisease treatment was licensed in the United States for the first time in nearly 20 years, sparking calls for it to be made available worldwide despite conflicting evidence about its usefulness. The drug was designed for people with mild cognitive impairment, not severe dementia, and it was designed to delay the progression of Alzheimer’s disease rather than only alleviate symptoms.
The route to FDA clearance for Aducanumab has been bumpy – and contentious.
Though doctors, patients, and the organizations that assist them are in desperate need of therapies that can delay mental decline, scientists question the efficacy of the new medicine, Aducanumab or Aduhelm. In March 2019, two trials were halted because the medications looked to be ineffective. “The futility analysis revealed that the studies were most likely to fail,” said Isaacson of Weill Cornell Medicine and NewYork-Presbyterian. Biogen, the drug’s manufacturer revealed several months later that a fresh analysis with more participants found that individuals who got high doses of Aducanumab exhibited a reduction in clinical decline in one experiment. Patients treated with high-dose Aducanumab had 22% reduced clinical impairment in their cognitive health at 18 months, indicating that the advancement of their early Alzheimer’s disease was halted, according to FDA briefing documents from last year.
When the FDA’s members were split on the merits of the application in November, it was rejected. Three of its advisers went public, claiming that there was insufficient evidence that it worked in a scientific journal. They were concerned that if the medicine was approved, it might reduce the threshold for future approvals, owing to the scarcity of Alzheimer’s treatments.
Dr. Caleb Alexander, a drug safety and effectiveness expert at the Johns Hopkins Bloomberg School of Public Health, was one of the FDA advisers who was concerned that the data presented to the agency was a reanalysis after the experiment was stopped. It was “like the Texas sharpshooter fallacy,” he told the New York Times, “where the sharpshooter blows up a barn and then goes and paints a bullseye around the cluster of holes he loves.”
Some organizations, such as the non-profit Public Citizen’s Health Research Group, claimed that the FDA should not approve Aducanumab for the treatment of Alzheimer’s disease because there is insufficient proof of its efficacy.
The drug is a monoclonal antibody that inhibits the formation of amyloid protein plaques in the brain, which are thought to be the cause of Alzheimer’s disease. The majority of Alzheimer’s medications have attempted to erase these plaques.
Aducanumab appears to do this in some patients, but only when the disease is in its early stages. This means that people must be checked to see if they have the disease. Many persons with memory loss are hesitant to undergo testing because there is now no treatment available.
The few Alzheimer’s medications available appear to have limited effectiveness. When Aricept, also known as Donepezil, was approved more than 20 years ago, there was a major battle to get it. It was heralded as a breakthrough at the time – partly due to the lack of anything else. It has become obvious that it slows mental decline for a few months but makes little effect in the long run.
The findings of another trial for some patients backed up those conclusions.
Biogen submitted a Biologics License Application to the FDA in July 2020, requesting approval of the medicine.
The FDA’s decision has been awaited by Alzheimer’s disease researchers, clinicians, and patients since then.
Support for approval of the drug
Other groups, such as the Alzheimer’s Association, have supported the drug’s approval.
The Alzheimer’s Association‘s website stated on Friday, “This is a critical time, regardless of the FDA’s final judgment. We’ve never been this close to approving an Alzheimer’s drug that could affect the disease’s development rather than just the symptoms. We can keep working together to achieve our goal of a world free of Alzheimer’s disease and other dementias.”
The drug has gotten so much attention that the Knight Alzheimer Disease Research Center at Washington University in St. Louis issued a statement on Friday stating that even if it is approved, “it will still likely take several months for the medication to pass other regulatory steps and become available to patients.”
Biogen officials told KGO-TV on Monday that the medicine will be ready to ship in about two weeks and that they have identified more than 900 facilities across the United States that they feel will be medically and commercially suitable.
Officials stated the corporation will also provide financial support to qualifying patients so that their out-of-pocket payments are as low as possible. Biogen has also pledged not to raise the price for at least the next four years.
Most Medicare customers with supplemental plans, according to the firm, will have a limited or capped co-pay.
Case studies connected to the Drug Approval
Case 1
Ann Lange, one of several Chicago-area clinical trial volunteers who received the breakthrough Alzheimer’s treatment, said,
It really offers us so much hope for a long, healthy life.
Lange, 60, has Alzheimer’s disease, which she was diagnosed with five years ago. Her memory has improved as a result of the monthly infusions, she claims.
She said,
I’d forget what I’d done in the shower, so I’d scribble ‘shampoo, conditioner, face, body’ on the door. Otherwise, I’d lose track of what I’m doing “Lange remarked. “I’m not required to do that any longer.
Case 2
Jenny Knap, 69, has been receiving infusions of the Aducanumab medication for about a year as part of two six-month research trials. She told CNN that she had been receiving treatment for roughly six months before the trial was halted in 2019, and that she had recently resumed treatment.
Knap said,
I can’t say I noticed it on a daily basis, but I do think I’m doing a lot better in terms of checking for where my glasses are and stuff like that.
When Knap was diagnosed with mild cognitive impairment, a clinical precursor to Alzheimer’s disease, in 2015, the symptoms were slight but there.
Her glasses were frequently misplaced, and she would repeat herself, forgetting previous talks, according to her husband, Joe Knap.
Joe added,
We were aware that things were starting to fall between the cracks as these instances got more often
Jenny went to the Lou Ruvo Center for Brain Health at the Cleveland Clinic in Ohio for testing and obtained her diagnosis. Jenny found she was qualified to join in clinical trials for the Biogen medicine Aducanumab at the Cleveland Clinic a few years later, in early 2017. She volunteered and has been a part of the trial ever since.
It turns out that Jenny was in the placebo category for the first year and a half, Joe explained, meaning she didn’t get the treatment.
They didn’t realize she was in the placebo group until lately because the trial was blind. Joe stated she was given the medicine around August 2018 and continued until February 2019 as the trial progressed. The trial was halted by Biogen in March 2019, but it was restarted last October, when Jenny resumed getting infusions.
Jenny now receives Aducanumab infusions every four weeks at the Cleveland Clinic, which is roughly a half-hour drive from their house, with Joe by her side. Jenny added that, despite the fact that she has only recently begun therapy, she believes it is benefiting her, combined with a balanced diet and regular exercise (she runs four miles).
The hope of Aducanumab is to halt the progression of the disease rather than to improve cognition. We didn’t appreciate any significant reduction in her condition, Jenny’s doctor, Dr. Babak Tousi, who headed Aducanumab clinical studies at the Cleveland Clinic, wrote to CNN in an email.
This treatment is unlike anything we’ve ever received before. There has never been a drug that has slowed the growth of Alzheimer’s disease, he stated, Right now, existing medications like donepezil and memantine aid with symptoms but do not slow the disease’s progression.
Jenny claims that the medicine has had no significant negative effects on her.
There was signs of some very minor bleeding in the brain at one point, which was quite some time ago. It was at very low levels, in fact, Joe expressed concern about Jenny, but added that the physicians were unconcerned.
According to Tousi, with repeated therapy, “blood vessels may become leaky, allowing fluid and red blood cells to flow out to the surrounding area,” and “micro hemorrhages have been documented in 19.1% of trial participants who got” the maximal dose of therapy”.
Jenny and Joe’s attitude on the future has improved as a result of the infusions and keeping a healthy lifestyle, according to Joe. They were also delighted to take part in the trial, which they saw as an opportunity to make a positive influence in other people’s lives.
There was this apprehension of what was ahead before we went into the clinical trial, Joe recalled. “The medical aspect of the infusion gives us reason to be optimistic. However, doing the activity on a daily basis provides us with immediate benefits.”
The drug’s final commercialization announcement
Aducanumab, which will be marketed as Aduhelm, is a monthly intravenous infusion that is designed to halt cognitive decline in patients with mild memory and thinking issues. It is the first FDA-approved medication for Alzheimer’s disease that targets the disease process rather than just the symptoms.
The manufacturer, Biogen, stated Monday afternoon that the annual list price will be $56,000. In addition, diagnostic tests and brain imaging will very certainly cost tens of thousands of dollars.
The FDA approved approval for the medicine to be used but ordered Biogen to conduct a new clinical trial, recognizing that prior trials of the medicine had offered insufficient evidence to indicate effectiveness.
Biogen Inc said on Tuesday that it expects to start shipping Aduhelm, a newly licensed Alzheimer’s medicine, in approximately two weeks and that it has prepared over 900 healthcare facilities for the intravenous infusion treatment.
Other Relevant Articles
Gene Therapy could be a Boon to Alzheimer’s disease (AD): A first-in-human clinical trial proposed
Alnylam Announces First-Ever FDA Approval of an RNAi Therapeutic, ONPATTRO™ (patisiran) for the Treatment of the Polyneuropathy of Hereditary Transthyretin-Mediated Amyloidosis in Adults
Fighting Chaos with care, community trust, engagement must be cornerstones of pandemic response
Reporter: Amandeep Kaur, BSc, MSc (Exp. 6/2021)
According to the Global Health Security Index released by Johns Hopkins University in October 2019 in collaboration with Nuclear Threat Initiative (NTI) and The Economist Intelligence Unit (EIU), the United States was announced to be the best developed country in the world to tackle any pandemic or health emergency in future.
The table turned within in one year of outbreak of the novel coronavirus COVID-19. By the end of March 2021, the country with highest COVID-19 cases and deaths in the world was United States. According to the latest numbers provided by World Health Organization (WHO), there were more than 540,000 deaths and more than 30 million confirmed cases in the United States.
Joia Mukherjee, associate professor of global health and social medicine in the Blavatnik Institute at Harvard Medical School said,
“When we think about how to balance control of an epidemic over chaos, we have to double down on care and concern for the people and communities who are hardest hit”.
She also added that U.S. possess all the necessary building blocks required for a health system to work, but it lacks trust, leadership, engagement and care to assemble it into a working system.
Mukherjee mentioned about the issues with the Index that it undervalued the organized and integrated system which is necessary to help public meet their needs for clinical care. Another necessary element for real health safety which was underestimated was conveying clear message and social support to make effective and sustainable efforts for preventive public health measures.
Mukherjee is a chief medical officer at Partners In Health, an organization focused on strengthening community-based health care delivery. She is also a core member of HMS community members who play important role in constructing a more comprehensive response to the pandemic in all over the U.S. With years of experience, they are training global health care workers, analyzing the results and constructing an integrated health system to fight against the widespread health emergency caused by coronavirus all around the world.
Mukherjee encouraged to strengthen the consensus among the community to constrain this infectious disease epidemic. She suggested that validation of the following steps are crucial such as testing of the people with symptoms of infection with coronavirus, isolation of infected individuals by providing them with necessary resources and providing clinical treatment and care to those people who are in need. Mukherjee said, that community engagement and material support are not just idealistic goal rather these are essential components for functioning of health care system during an outburst of coronavirus.
Continued alertness such as social distancing and personal contact with infected individual is important because it is not possible to rapidly replace the old-school public health approaches with new advanced technologies like smart phone applications or biomedical improvements.
Public health specialists emphasized that the infection limitation is the only and most vital strategy for controlling the outbreak in near future, even if the population is getting vaccinated. It is crucial to slowdown the spread of disease for restricting the natural modification of more dangerous variants as that could potentially escape the immune protection mechanism developed by recently generated vaccines as well as natural immune defense systems.
Making Crucial connections
The treatment is more expensive and complicated in areas with less health facilities, said Paul Farmer, the Kolokotrones University Professor at Harvard and chair of the HMS Department of Global Health and Social Medicine. He called this situation as treatment nihilism. Due to shortage of resources, the maximum energy is focused in public health care and prevention efforts. U.S. has resources to cope up with the increasing demand of hospital space and is developing vaccines, but there is a form of containment nihilism- which means prevention and infection containment are unattainable- said by many experts.
Farmer said, integration of necessary elements such as clinical care, therapies, vaccines, preventive measures and social support into a single comprehensive plan is the best approach for a better response to COVID-19 disease. He understands the importance of community trust and integrated health care system for fighting against this pandemic, as being one of the founders of Partners In Health and have years of experience along with his colleagues from HMS and PIH in fighting epidemics of HIV, Ebola, cholera, tuberculosis, other infectious and non-infectious diseases.
PIH launched the Massachusetts Community Tracing Collaborative (CTC), which is an initiative of contact tracing statewide in partnership with several other state bodies, local boards of Health system and PIH. The CTC was setup in April 2020 in U.S. by Governor Charlie Baker, with leadership from HMS faculty, to build a unified response to COVID-19 and create a foundation for a long-term movement towards a more integrated community-based health care system.
The contact tracing involves reaching out to individuals who are COVID-19 positive, then further detect people who came in close contact with infected individuals and screen out people with coronavirus symptoms and encourage them to seek testing and take necessary precautions to break the chain of infection into the community.
In the initial phase of outbreak, the CTC group comprises of contact tracers and health care coordinators who spoke 23 different languages, including social workers, public health practitioners, nurses and staff members from local board health agencies with deep links to the communities they are helping. The CTC worked with 339 out of 351 state municipalities with local public health agencies relied completely on CTC whereas some cities and towns depend occasionally on CTC backup. According to a report, CTC members reached up to 80 percent of contact tracking in hard-hit and resource deprived communities such as New Bedford.
Putting COVID-19 in context
Based on generations of experience helping people surviving some of the deadliest epidemic and endemic outbreaks in places like Haiti, Mexico, Rwanda and Peru, the staff was alert that people with bad social and economic condition have less space to get quarantined and follow other public health safety measures and are most vulnerable people at high risk in the pandemic situation.
Infected individuals or individuals at risk of getting infected by SARS-CoV-2 had many questions regarding when to seek doctor’s help and where to get tested, reported by contact tracers. People were worried about being evicted from work for two weeks and some immigrants worried about basic supplies as they were away from their family and friends.
The CTC team received more than 7,000 requests for social support assistance in the initial three months. The staff members and contact tracers were actively connecting the resourceful individuals with the needy people and filling up the gap when there was shortage in their own resources.
Farmer said, “COVID is a misery-seeking missile that has targeted the most vulnerable.”
The reality that infected individuals concerned about lacking primary household items, food items and access to childcare, emphasizes the urgency of rudimentary social care and community support in fighting against the pandemic. Farmer said, to break the chain of infection and resume society it is mandatory to meet all the elementary needs of people.
“What kinds of help are people asking for?” Farmer said and added “it’s important to listen to what your patients are telling you.”
An outbreak of care
The launch of Massachusetts CTC with the support from PIH, started receiving requests from all around the country to assist initiating contact tracing procedures. In May, 2020 the organization announced the launch of a U.S. public health accompaniment to cope up with the asked need.
The unit has included team members in nearly 24 states and municipal health departments in the country and work in collaboration with local organizations. The technical support on things like choosing and implementing the tools and software for contact tracing was provided by PIH. To create awareness and provide new understanding more rapidly, a learning collaboration was established with more than 200 team members from more than 100 different organizations. The team worked to meet the needs of population at higher risk of infection by advocating them for a stronger and more reliable public health response.
The PIH public health team helped to train contact trackers in the Navajo nation and operate to strengthen the coordination between SARS-CoV-2 testing, efforts for precaution, clinical health care delivery and social support in vulnerable communities around the U.S.
“For us to reopen our schools, our churches, our workplaces,” Mukherjee said, “we have to know where the virus is spreading so that we don’t just continue on this path.”
The WHO team is expected to soon publish a 300-page final report on its investigation, after scrapping plans for an interim report on the origins of SARS-CoV-2 — the new coronavirus responsible for killing 2.7 million people globally
A brain aneurysm is a bulge that forms in the blood vessel of your brain that could lead to severe health issues and possibly death. Brain aneurysm affect about one in 50 Americans and can lead to serious medical emergencies including stroke and brain damage. Current treatments for brain aneurysm are limited and very invasive and can vary from person to person.
Researchers at Lawrence Livermore National Laboratory and their collaborators were able to replicate an aneurysm in vitro by 3D printing blood vessels with human cerebral cells. One of the leading engineers, William Hynes performed an endovascular repair procedure on the printed aneurysm by inserting a catheter into blood vessel and tightly packed platinum coils inside the aneurysm sac. Afterward, the scientists introduced blood plasma into the aneurysm and identified the formation of blood clot where the coils were located and they were able to observe the post-op healing process of the endothelial cells within the vessels.
One thing that was obvious to the LLNL scientists is that computer modeling is an important step to developing patient-specific care for aneurysms based on patient’s blood vessel geometry, blood pressure and other factors. They also determined that it takes time for the new surgical technology to move from laboratory to the clinic.
The idea is if they can replicate the aneurysms as much as needed using animal models or 3D printing, they can help find better options for aneurysms with uncontrollable geometries. Since, the most common treatment for aneurysms is the endovascular metal coiling approach, researchers believe that by taking out the guesswork out of aneurysms treatment researchers can design more predictive 3D models that takes patient geometry into account.
Hynes teamed with former LLNL scientist Duncan Maitland and Amanda Randles, a former Lab computational scientist to verify if Randles’s flow dynamic model compares with the real world. At low flow rates, scientist saw little movement of blood into the aneurysm, while an increased flow rate, resulted in a circular flow of blood throughout the aneurysm, as would be predictable in a true brain aneurysm.
Using the data obtained from the flow dynamic model in combination with the 3D printing platform, researchers developed a potential tool for surgeons to pre-select the best coil types desirable to fully pack an aneurysm to obtain the best treatment outcome, and perform “test runs” of procedures before attempting them on the human patient.
Unlike animal models, LLNL’s platform allows scientists to directly measure the fluid dynamics inside the vessels and aneurysm while maintaining biological relevance.
In addition to patient-specific care and serving as a testbed for surgical training, researchers mentioned that the platform can improve the understanding of basic biology and the post-surgery healing response. Even though the results are promising, researchers mentioned that there is long way before their platform is applicable in a clinical environment setting.
When dermatologist Jenna Lester learned that rashes on skin and toes were a symptom of Covid-19, she started searching the medical literature for images of what the rashes looked like on Black skin so she’d recognize it in her Black patients. She couldn’t find a single picture.
“I was frustrated because we know Covid-19 is disproportionately impacting communities of color,” said Lester, an assistant professor of dermatology at the University of California, San Francisco who recently published her analysis. “I felt like I was seeing a disparity being built right before my eyes.”
The dearth of images in the Covid-19 literature is just the newest example of the glaring lack of representation of Black and brown skin that has persisted in dermatology research journals and textbooks for decades. The issue is coming under closer scrutiny now as dermatologists, like many physicians, grapple more openly with systemic racism and the health disparities it is causing in their field.
“Black Lives Matter is forcing a lot of people to look inward and say, ‘Where are our shortcomings?’” said Nada Elbuluk, an associate professor of clinical dermatology at the University of Southern California and the founder of a diversity and inclusion program in her department. “Dermatology is no different.”
The discrimination in her specialty extends beyond images and gaps in training, to restrictive insurance coverage for skin conditions that affect people with heavily pigmented skin, and to the many dermatologists who don’t accept patients with Medicaid.
It may be no surprise that a field that focuses on skin is now reckoning with skin color. In dermatology, where images are critical for diagnoses, the lack of images of darker skin poses a roadblock to proper treatment and medical education. Skin conditions that involve redness or pinkness in light skin can be subtler or harder to see in dark skin, and physicians who haven’t been adequately trained with such images are prone to misdiagnose people of color. “We absolutely need a diversity of images,” said Elbuluk.
An analysis of textbooks by Jules Lipoff, an assistant professor of clinical dermatology at the University of Pennsylvania, showed the percentage of images of dark skin ranged from 4% to 18%. “We are not teaching (and possibly not learning) skin of color,” Lester wrote in a separate analysis she conducted. Many worry the field’s shift toward using artificial intelligence to aid diagnosis of disease will further deepen the divide, because the machine learning algorithms are trained with datasets consisting primarily of fair-skinned images.
Dermatologist Jenna Lester treats Geoffry Blair Hutto at the UCSF skin of color clinic.COURTESY BARBARA RIES, UCSF
It gets worse. While many textbooks depict the vast majority of skin diseases using light skin, there is one notable exception: Black skin is more often used to depict sexually transmitted diseases, a glaring example of stereotyping that is all the more painful given the U.S. government’s complicity in the notorious Tuskegee experiments that left syphilis untreated for decades in a group of poor, Black men.
Lipoff’s analysis, published this year, showed many dermatology textbooks had zero images of dark skin with acne, psoriasis, or dermatitis. When it came to syphilis, however, many books relied heavily on images of dark skin. Lester’s analysis found that while 28% of images of infectious diseases used images of darker skin, the number of depictions of dark skin was twice as high for infections that were sexually transmitted.
“In the textbooks I used in medical school, every penis was a Black penis showing an STD. We’ve got to stop that,” said Susan Taylor, a pioneer in the push for better dermatologic care for patients with dark skin and the Sandra Lazarus professor of dermatology at the Perelman School of Medicine at the University of Pennsylvania.
Considered a trailblazer in the field of dermatology, Taylor established the nation’s first “Skin of Color” dermatology clinic at Mount Sinai in New York in the late 1990s. In 2004, she founded the Skin of Color Society to help educate fellow dermatologists about how to treat patients of color, push for research and clinical trials to include people with darker skin, and mentor and encourage medical students of color to enter dermatology, where only 3% of practitioners are Black and 4% are Hispanic. “These are really abysmal numbers,” Taylor said. “That’s got to change.”
Taylor is also the lead author of the textbook Dermatology for Skin of Color, a guide considered invaluable by many dermatologists. But even those who rely on the book say it’s frustrating that a separate book on dark skin is still required — when as a nation we are just a few decades away from a majority of residents having skin of color.
“This is the white patient treated as the default and the Black patient as the asterisk,” said Lipoff. “You can’t make skin of color a lecture that students get once a year. It can’t be ‘otherized’ or put in a separate textbook.”
Taylor agrees. “Nothing would make me happier than to not have to publish another edition of that book,” she said.
Dermatologists say the lack of images is one reason why many conditions, including Lyme disease, spider bites, and cancers can go misdiagnosed or underdiagnosed in darker skinned patients, sometimes with dangerous results. The five-year melanoma survival rate for Black patients is just 70% compared with 94% for white patients.
The mother of a mixed-race 13-year-old from Connecticut said she was told by her child’s pediatrician when she was 8 that the white patches on her skin were pityriasis alba, a skin rash that’s usually not considered a serious condition. She was given a lotion, but the skin patches never went away. “I kept going online and looking at things but I couldn’t see anyone with issues that looked like hers,” said the mother, who didn’t want her name used to protect the girl’s privacy. “And the doctor was casual about it.”
Partly because of insurance issues, and partly because the mother thought there was nothing to worry about, it took five years before her daughter’s white patches were properly diagnosed: She had T-cell lymphoma, a cancer. While she will require maintenance light therapy for life, her overall prognosis is good. But her case highlights the difficult and sometimes frightening challenge many patients of color face to get a proper dermatologic diagnosis.
“Black Lives Matter is forcing a lot of people to look inward and say, ‘Where are our shortcomings?’ Dermatology is no different.”
When Ellen Buchanan Weiss noticed patches on the dark brown skin of her toddler son, she wondered if it was eczema, or something more serious. “I Googled it and noticed immediately the pictures were all of white skin,” she said. “I Googled other conditions and it was the same. No matter what I searched, there were almost no images of dark skin.”
The patches did turn out to be eczema and were easily treated. Still, the disparity bothered her for months. About a year ago, Weiss, a stay-at-home mom in Raleigh, N.C., decided to create an Instagram account called “Brown Skin Matters.” She posted images of skin conditions in darker skin next to images of the same condition in white skin and asked followers to send in more photos. The account exploded almost immediately.
“I’ve had tons of medical schools, physicians, nurses, and pharmacists all contact me saying this was useful,” she said. “I never thought this was going to become a diagnostic tool.”
Instagram is not exactly the best platform for making medical diagnoses, so Weiss is now working with medical experts to help create a more rigorous and searchable web-based tool for diagnosis of skin diseases in darker skin. It still floors Weiss that she, a person with no medical background, is at the center of it. “It’s curious to me, and troubling, that this is 2020 and this gap is still here,” she said. “Some large medical institution should have been taking care of this, not me.”
Comparison of atopic dermatitis in infants with darkly pigmented versus lightly pigmented skin, from the widely used textbook, Dermatology.COURTESY BOLOGNIA JL, SCHAFFER JV, AND CERRONI L, EDS. DERMATOLOGY. 4TH ED. ELSEVIER
Bolognia said she is extremely sensitive about not stigmatizing people of color by using only images of darkly pigmented skin to illustrate sexually transmitted diseases or drug users. “I noticed this as a student, the images of STDs were nearly all of patients with darkly pigmented skin, but the people I saw with syphilis were often fair-skinned,” she said. “I wondered about the possibility that pictures were being taken of individuals who were less likely to say no.”
The issue of textbooks failing to adequately represent skin of color is not a new one. Yet Lipoff’s study compared today’s textbooks with those of 15 years ago and found little has changed. Jean Bolognia, a professor of dermatology at the Yale School of Medicine, has spent more than two decades editing the widely used textbook, Dermatology; she said providing a wide spectrum of skin tones is critical and something she’s worked hard to include, though she acknowledged there’s more work to do.
“I’m not saying it’s perfect, but we’ve been working really hard for over 15 years to show the whole spectrum,” said Bolognia, who is now working on the fifth edition of the textbook. “I feel you can always do better and I realize I don’t have enough images of Asian skin, so that is something I’m addressing.”Related:
The field’s other widely used textbook is Andrews’ Diseases of the Skin. That book’s lead author, William James, is a longtime champion of diversity in dermatology, according to his colleagues at Penn, who include Taylor and Lipoff. James said representing a variety of skin tones was an important issue, but said authors were challenged by limits placed on the number of photos by textbook publishers and because findings of redness or pinkness can be hard to see in images of darker skin. “Deciding if an entity is represented at all, or more than once, is always difficult,” he said in an email.
James said his textbook includes more photos of Black skin than white skin in conditions that are more common in Black patients, and noted that eight of 14 photos of syphilis are in lighter skin.
Agrowing number of dermatologists are following Taylor’s lead and opening skin of color clinics that provide care for darker-skinned patients. Lester opened one at UCSF last year. Elbuluk has worked at or founded three skin of color clinics throughout her training and early career, including at Penn, NYU Medical School, and, in 2018, at USC, where she hopes to also spur much-needed clinical research on darker skin. “It’s surprising to me when large cities don’t have these,” Elbuluk said.
There are many reasons why people of color, particularly those who do not have private health insurance, lack access to dermatologists. Lipoff, who has examined the issue, said many dermatologists do not take Medicaid. Racial bias that discourages the treatment of Black patients, he said, is literally built into the physician reimbursement system. Many conditions that affect darker skin are often not covered by insurance because they are considered cosmetic.
Meanwhile, the highest revenue procedures, Lipoff said, include those for the diagnosis and treatment of skin cancer, which is more likely to occur in white patients. This difference in how procedures are valued and reimbursed, he said, is a perfect example of structural racism that drives practices to directly and indirectly focus on white patients and marginalize Black patients. “If Black patients earned practices three times the revenue,” he said, “the disparity would disappear overnight.”
“It’s curious to me, and troubling, that this is 2020 and this gap is still here. Some large medical institution should have been taking care of this, not me.”
Until it does, physicians who run skin of color clinics are hoping to address the lack of care, and poor care, Black and brown patients have received. The clinics are a welcome addition to people like Dar Bray, a 45-year-old behavioral therapist and darker-skinned Black man from Los Angeles.
Bray had dealt for years with deep and persistent scars caused by acne, trying bleaching creams and expensive cosmetic products, all with no success. “I went to so many doctors who didn’t know what to do with my skin. All the pictures they had on their wall were fair-skinned people,” Bray said. “It didn’t feel like racism, it felt like just plain ignorance.”
Seeing Elbuluk, he said, was immediately different. Bray is now undergoing chemical peels to remove scarring and using simple (and inexpensive) cleansers and moisturizers, and says he sees a huge improvement in his skin. He’s also wearing sunscreen, something no physician had ever told him was necessary; like many, he had believed the myth “Black don’t crack.” “When I went to the beach, I never wore sunscreen,” he said. “Now I have years of sun damage.”
Mistrust of white physicians led Gregory Hines, a 63-year-old longshoreman who lives in Oakland, to go years without seeing a doctor about growths under his arm, on his back, and on his neck, even as they puffed up and became, in his words “kind of weird and ugly.”
“I experience it a lot, going to doctors — especially white, male doctors — they assume they know more than you. They assume they already know what your problem is the minute you walk through the door,” he said.
When he heard UCSF’s Skin of Color clinic had opened, he was willing to give it a try. “When Dr. Lester walked in, I said, ‘Whoa, this is great,’” he said. “I wanted a Black doctor who understands Black skin.”
Lester ended up removing the masses, one of which was nearly as large as a golf ball, and sent them for tests to see if they were cancerous. Fortunately, they were not.
Lester is the only Black dermatologist in San Francisco. She’s hoping that will change after her current crop of residents decides where they will establish their practices. Her Black patients, she said, are often shocked when she walks in the door.
“I’ve had patients ask if they can take a picture with me to show their grandkids,” she said. “They want to talk all about me and how I got here, and I have to say, ‘No, this time is for you.’”
National Cancer Institute Director Neil Sharpless says mortality from delays in cancer screenings due to COVID19 pandemic could result in tens of thousands of extra deaths in next decade
Reporter: Stephen J Williams, PhD
UPDATED: 08/14/2023
A Cross Sectional Study Reveals What Oncologists Had Feared: Cancer Screenings During Pandemic Has Decreased, leading to Decreased Early Detection
As discussed in many articles here on COVID-19 and cancer, during the pandemic many oncologists were worried that people slowed getting their cancer screenings due to health risks due to the COVID-19 outbreak. Governmental agencies went as far to project upticks in future cancer rates, as preventative screening rates were down due to closed hospitals, shuttered services, or patient trepidation during the height of the pandemic. As many oncologists voiced, a decrease in cancer screenings might lead to missing out on the early stages of the disease, when most treatable. Now, reported in a Lancet cross-sectional analysis by investigators at ACS and University of Texas Southwest (1), we have the first indication of the effects of this decrease in preventative screening, namely decreased early detection and diagnosis.
The authors used data from the US National Cancer Database, a nationwide hospital-based cancer registry, to perform a cross sectional nationwide assessment of the prevalence of new cancer diagnosis before, during, and after the height of the pandemic (March 1 2020 to December 31, 2020). Newly diagnosed cases of first primary malignant cancer between Jan1, 2018 to Dec 31, 2020 were identified and monthly and annual counts and stage distributions were caluculated andpresented as adjusted odds ratios (aORs). They also used the period from 2018 to Jan 2020 as a baseline or prepandemic level of newly diagnosed cancer.
Results of this analysis identified 2,404,050 adults with newly diagnosed cancer during study period 2018 to 2020. The monthly number of new cancer diagnoses (all stages) decreased significantly after the start of the COVID-19 pandemic in March 2020. However new cancer diagnosis returned to pre-pandemic levels by end of 2020. The decrease in diagnosis was largest for stage I diseases however the odds of being diagnosed with late stage IV disease were higher in 2020 than in 2019. When the authors stratified the cohorts based on sociodemographic groups, interestingly those most affected (with lowest diagnosis rates during the pandemic) were those living in socioeconomic deprived areas, hispanics, asian americans, pacific Islanders, and uninsured individuals.
The authors’ interpretations are a warning: Substantial cancer underdiagnosis and decreases in the proportion of early stage diagnoses occurred during 2020 in the USA, particularly among medically underserved individuals. Monitoring the long-term effects of the pandemic on morbidity, survival, and mortality is warranted.
Evidence before this study
We searched PubMed using the terms “COVID”, “pandemic”, and “cancer” for studies published in English between
March 1, 2020, and Nov 30, 2022. Health care was disrupted during the emergence of the COVID-19 pandemic. In the USA, rapid decreases in screening were reported for nearly all types of cancer screening services after the declaration of the COVID-19 national emergency. Decreased screening, and delayed and forgone routine check-ups or health-care visits, can lead to underdiagnosis of cancer, especially for early stage disease for which treatment is most effective. Several studies have identified reduced use of diagnostic procedures and decreases in the number of newly diagnosed patients during 2020 in the USA. However, these studies were done in selected populations, in specific geographical areas, or for only a single cancer type, limiting understanding of the COVID-19 pandemic on cancer burden nationally.
Added value of this study
Using a recently released nationwide cancer registry dataset, we comprehensively evaluated changes in cancer diagnoses and stage distribution during the first year of the COVID-19 pandemic by cancer type and key sociodemographic factors in the USA.
Implications of all the available evidence
Along with existing evidence, our findings should help to inform future policy and cancer care delivery interventions to improve access to care for underserved populations. Research is warranted to monitor the long-term effects of the underdiagnosis of early stage cancer identified in this study on morbidity, mortality, and disparities in health outcomes.
Results
The main results from the paper are summarized below:
Between 2020 and 2019, annual stage I diagnoses decreased by 17·2% (95% CI 16·8–17·6), and annual stage IV diagnoses decreased 9·8% (9·2–10·5). Notably, by race and ethnicity, the largest percentage reduction in stage I diagnoses was among Hispanic individuals and Asian American and Pacific Islander individuals, and the largest percentage reduction in stage IV diagnoses was among non-Hispanic Black and non-Hispanic White individuals. Diagnoses of lung cancer, colorectal cancer, melanoma, and non-Hodgkin lymphoma had the largest percentage reduction among both stage I (>18%) and stage IV (>10%) diagnoses; cancers of the prostate, cervix, liver, oesophagus, stomach, and thyroid also had large percentage reductions in stage I diagnoses (>20).
After adjusting for sociodemographic and clinical factors, the stage distribution of new diagnoses changed in 2020 compared with 2019 (table 3). Specifically, the aOR for being diagnosed with stage I disease versus stage II–IV disease in 2020 compared with 2019 was 0·946 (95% CI 0·939–0·952), and the aOR for being diagnosed with stage IV disease versus stage I–III disease in 2020 compared with 2019 was 1·074 (1·066–1·083).
These results also confirmed results seen in other studies coming from Europe (2,3, 4).
References
Han X, Yang NN, Nogueira L, Jiang C, Wagle NS, Zhao J, Shi KS, Fan Q, Schafer E, Yabroff KR, Jemal A. Changes in cancer diagnoses and stage distribution during the first year of the COVID-19 pandemic in the USA: a cross-sectional nationwide assessment. Lancet Oncol. 2023 Aug;24(8):855-867. doi: 10.1016/S1470-2045(23)00293-0. PMID: 37541271.
Kuzuu K, Misawa N, Ashikari K, et al. Gastrointestinal cancer stage at diagnosis before and during the COVID-19 pandemic in Japan. JAMA Netw Open 2021; 4: e2126334. DOI: 10.1001/jamanetworkopen.2021.26334
Linck PA, Garnier C, Depetiteville MP, et al. Impact of the COVID-19 lockdown in France on the diagnosis and staging of breast cancers in a tertiary cancer centre. Eur Radiol 2022; 32: 1644–51. DOI: 10.1007/s00330-021-08264-3
Mynard N, Saxena A, Mavracick A, et al. Lung cancer stage shift as a result of COVID-19 lockdowns in New York City, a brief report. Clin Lung Cancer 2022; 23: e238–42. DOI: 10.1016/j.cllc.2021.08.010
This story is part of The Cancer Letter’s ongoing coverage of COVID-19’s impact on oncology. A full list of our coverage, as well as the latest meeting cancellations, is available here.
The COVID-19 pandemic will likely cause at least 10,000 excess deaths from breast cancer and colorectal cancer over the next 10 years in the United States.
Scenarios run by NCI and affiliated modeling groups predict that delays in screening for and diagnosis of breast and colorectal cancers will lead to a 1% increase in deaths through 2030. This translates into 10,000 additional deaths, on top of the expected one million deaths resulting from these two cancers.
“For both these cancer types, we believe the pandemic will influence cancer deaths for at least a decade,” NCI Director Ned Sharpless said in a virtual joint meeting of the Board of Scientific Advisors and the National Cancer Advisory Board June 15. “I find this worrisome as cancer mortality is common. Even a 1% increase every decade is a lot of cancer suffering.
“And this analysis, frankly, is pretty conservative. We do not consider cancers other than those of breast and colon, but there is every reason to believe the pandemic will affect other types of cancer, too. We did not account for the additional non-lethal morbidity from upstaging, but this could also be significant and burdensome.”
An editorial by Sharpless on this subject appears in the journal Science.
The early analyses, conducted by the institute’s Cancer Intervention and Surveillance Modeling Network, focused on breast and colorectal cancers, because these are common, with relatively high screening rates.
CISNET modelers created four scenarios to assess long-term increases in cancer mortality rates for these two diseases:
The pandemic has no effect on cancer mortality
Delayed screening—with 75% reduction in mammography and, colorectal screening and adenoma surveillance for six months
Delayed diagnosis—with one-third of people delaying follow-up after a positive screening or diagnostic mammogram, positive FIT or clinical symptoms for six months during a six-month period
Combination of scenarios two and three
Treatment scenarios after diagnosis were not included in the model. These would be: delays in treatment, cancellation of treatment, or modified treatment.
“What we did is show the impact of the number of excess deaths per year for 10 years for each year starting in 2020 for scenario four versus scenario one,” Eric “Rocky” Feuer, chief of the NCI’s Statistical Research and Applications Branch in the Surveillance Research Program, said to The Cancer Letter.
Feuer is the overall project scientist for CISNET, a collaborative group of investigators who use simulation modeling to guide public health research and priorities.
“The results for breast cancer were somewhat larger than for colorectal,” Feuer said. “And that’s because breast cancer has a longer preclinical natural history relative to colorectal cancer.”
Modelers in oncology are creating a global modeling consortium, COVID-19 and Cancer Taskforce, to “support decision-making in cancer control both during and after the crisis.” The consortium is supported by the Union for International Cancer Control, The International Agency for Research on Cancer, The International Cancer Screening Network, the Canadian Partnership Against Cancer, and Cancer Council NSW, Australia.
A spike in cancer mortality rates threatens to reverse or slow down—at least in the medium term—the steady trend of reduction of cancer deaths. On Jan. 8, the American Cancer Society published its annual estimates of new cancer cases and deaths, declaring that the latest data—from 2016 to 2017—show the “largest ever single-year drop in overall cancer mortality of 2.2%.” Experts say that innovation in lung cancer treatment and the success of smoking cessation programs are driving the sharp decrease (The Cancer Letter, Feb. 7, 2020).
The pandemic is expected to have broader impact, including increases in mortality rates for other cancer types. Also, variations in severity of COVID-19 in different regions in the U.S. will influence mortality metrics.
“There’s some other cancers that might have delays in screening—for example cervical,prostate, and lungcancer, although lung cancer screening rates are still quite low and prostate cancer screening should only be conducted on those who determine that the benefits outweigh the harms,” Feuer said. “So, those are the major screening cancers, but impacts of delays in treatment, canceling treatment or alternative treatments—could impact a larger range of cancer sites.
“This model assumes a moderate disruption which resolves after six months, and doesn’t consider non-lethal morbidities associated with the delay. One thing I think probably is occurring is regional variation in these impacts,” Feuer said. “If you’re living in New York City where things were ground zero for some of the worst impact early on, probably delays were larger than other areas of the country. But now, as we’re seeing upticks in other areas of the country, there may be in impact in these areas as well”
How can health care providers mitigate some of these harms? For example, for people who delayed screening and diagnosis, are providers able to perform triage, so that those at highest risk are prioritized?
“From a strictly cancer control point of view, let’s get those people who delayed screening, or followup to a positive test, or treatment back on schedule as soon as possible,” Feuer said. “But it’s not a simple calculus, because in every situation, we have to weigh the harms and benefits. As we come out of the pandemic, it tips more and more to, ‘Let’s get back to business with respect to cancer control.’
“Telemedicine doesn’t completely substitute for seeing patients in person, but at least people could get the advice they need, and then are triaged through their health care providers to indicate if they really should prioritize coming in. That helps the individual and the health care providerweigh the harms and benefits, and try to strategize about what’s best for any individual.”
If the pandemic continues to disrupt routine care, cancer-related mortality rates would rise beyond the predictions in this model.
“I think this analysis begins to help us understand the costs with regard to cancer outcomes of the pandemic,” Sharpless said. “Let’s all agree we will do everything in our power to minimize these adverse effects, to protect our patients from cancer suffering.”
UPDATED: 10/11/2021
Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak
Source:
MengyuanDai, DianboLiu, MiaoLiu, FuxiangZhou, GuilingLi, ZhenChen, ZhianZhang, HuaYou, MengWu, QichaoZheng, YongXiong, HuihuaXiong, ChunWang, ChangchunChen, FeiXiong, YanZhang, YaqinPeng, SipingGe, BoZhen, TingtingYu, LingWang, HuaWang, YuLiu, YeshanChen, JunhuaMei, XiaojiaGao, ZhuyanLi, LijuanGan, CanHe, ZhenLi, YuyingShi, YuwenQi, JingYang, Daniel G.Tenen, LiChai, Lorelei A.Mucci, MauricioSantillana and HongbingCai. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak
The novel COVID-19 outbreak has affected more than 200 countries and territories as of March 2020. Given that patients with cancer are generally more vulnerable to infections, systematic analysis of diverse cohorts of patients with cancer affected by COVID-19 is needed. We performed a multicenter study including 105 patients with cancer and 536 age-matched noncancer patients confirmed with COVID-19. Our results showed COVID-19 patients with cancer had higher risks in all severe outcomes. Patients with hematologic cancer, lung cancer, or with metastatic cancer (stage IV) had the highest frequency of severe events. Patients with nonmetastatic cancer experienced similar frequencies of severe conditions to those observed in patients without cancer. Patients who received surgery had higher risks of having severe events, whereas patients who underwent only radiotherapy did not demonstrate significant differences in severe events when compared with patients without cancer. These findings indicate that patients with cancer appear more vulnerable to SARS-CoV-2 outbreak.
Significance: Because this is the first large cohort study on this topic, our report will provide much-needed information that will benefit patients with cancer globally. As such, we believe it is extremely important that our study be disseminated widely to alert clinicians and patients.
Introduction
A new acute respiratory syndrome coronavirus, named SARS-CoV-2 by the World Health Organization (WHO), has rapidly spread around the world since its first reported case in late December 2019 from Wuhan, China (1). As of March 2020, this virus has affected more than 200 countries and territories, infecting more than 800,000 individuals and causing more than 40,000 deaths (2).
With more than 18 million new cases per year globally, cancer affects a significant portion of the population. Individuals affected by cancer are more susceptible to infections due to coexisting chronic diseases, overall poor health status, and systemic immunosuppressive states caused by both cancer and anticancer treatments (3). As a consequence, patients with cancer who are infected by the SARS-CoV-2 coronavirus may experience more difficult outcomes than other populations. Until now, there is still no systematic evaluation of the effects that the SARS-CoV-2 coronavirus has of patients with cancer in a representative population. A recent study reported a higher risk of severe events in patients with cancer when compared with patients without cancer (4); however, the small sample size of SARS-CoV-2 patients with cancer used in the study limited how representative it was of the whole population and made it difficult to conduct more insightful analyses, such as comparing clinical characteristics of patients with different types of cancer, as well as anticancer treatments (5, 6).
Using patient information collected from 14 hospitals in Hubei Province, China, the epicenter of the 2019–2020 COVID-19 outbreak, we describe the clinical characteristics and outcomes [death, intensive care unit (ICU) admission, development of severe/critical symptoms, and utilization of invasive mechanical ventilation] of patients affected by the SARS-CoV-2 coronavirus for 105 hospitalized patients with cancer and 536 patients without cancer. We document our findings for different cancer types and stages, as well as different types of cancer treatments. We believe the information and insights provided in this study will help improve our understanding of the effects of SARS-CoV-2 in patients with cancer.
Results
Patients Characteristics
In total, 105 COVID-19 patients with cancer were enrolled in our study for the time period January 1, 2020, to February 24, 2020, from 14 hospitals in Wuhan, China. COVID-19 patients without cancer matched by the same hospital, hospitalization time, and age were randomly selected as our control group. Our patient population included 339 females and 302 males. Patients with cancer [median = 64.00, interquartile range (IQR) = 14.00], when compared with those without cancer (median = 63.50, IQR = 14.00) had similar age distributions (by design), experienced more in-hospital infections [20 (19.04%) of 105 patients vs. 8 (1.49%) of 536 patients;P < 0.01], and had more smoking history [36 (34.28%) of 105 patients vs. 46 (8.58%) of 536 patients; P < 0.01], but had no significant differences in sex, other baseline symptoms, and other comorbidities (Table 1). With respect to signs and symptoms upon admission, COVID-19 patients with cancer were similar to those without cancer except for a higher prevalence of chest distress [15 (14.29%) of 105 patients vs. 36 (6.16%) of 536 patients; P = 0.02].
Characteristics of COVID-19 patients with and without cancer
Clinical Outcomes
Compared with COVID-19 patients without cancer, patients with cancer had higher observed death rates [OR, 2.34; 95% confidence interval (CI), (1.15–4.77); P = 0.03], higher rates of ICU admission [OR, 2.84; 95% CI (1.59–5.08); P < 0.01], higher rates of having at least one severe or critical symptom [OR, 2.79; 95% CI, (1.74–4.41); P < 0.01], and higher chances of needing invasive mechanical ventilation (Fig. 1A). We also conducted survival analysis on occurrence of any severe condition which included death, ICU admission, having severe symptoms, and utilization of invasive mechanical ventilation (see cumulative incidence curves in Fig. 1B). In general, patients with cancer deteriorated more rapidly than those without cancer. These observations are consistent with logistic regression results (Supplementary Fig. S1), after adjusting for age, sex, smoking, and comorbidities including diabetes, hypertension, and chronic obstructive pulmonary disease (COPD). According to our multivariate logistic regression results, patients with cancer still had an excess OR of 2.17 (P = 0.06) for death (Supplementary Fig. S1A), 1.99 (P < 0.01) for experiencing any severe symptoms (Supplementary Fig. S1B), 3.13 (P < 0.01) for ICU admission (Supplementary Fig. S1C), and 2.71 (P = 0.04) for utilization of invasive mechanical ventilation (Supplementary Fig. S1D; Supplementary Table S1). The consistency of observed ORs between the multivariate regression model and unadjusted calculation reassures the association between cancer and severe events even in the presence of other factors such as age differences.
Severe conditions in patients with and without cancer, and patients with different types, stages, and treatments of cancer. Severe conditions include death, ICU admission, having severe/critical symptoms, and usage of invasive mechanical ventilation. Incidence and survival analysis of severe conditions among COVID-19 patients with cancer and without cancer (A and B), among patients with different types of cancer (C and D), among patients with metastatic and nonmetastatic cancers (E and F), among patients with lung cancer, other cancers than lung with lung metastasis, and other cancers than lung without lung metastasis (G and H), and patients receiving different types of cancer treatments (I and J). P values indicate differences between cancer subgroups versus patients without cancer. For A, C, E, G, I, *, P < 0.05; **, P < 0.01. OR, 95% CI, and P values between different subgroups are listed in Supplementary Table S2. For B, D, F, H, J, HR, 95% CI, and P values are listed in Supplementary Table S3.
Cancer Types
Information regarding potential risks of severe conditions in SARS-CoV-2 associated with each type of cancer was calculated. We compared different conditions among cancer types (Table 2). Lung cancer was the most frequent cancer type [22 (20.95%) of 105 patients], followed by gastrointestinal cancer [13 (12.38%) of 105 patients], breast cancer [11 (10.48%) of 105 patients], thyroid cancer [11 (10.48%) of 105 patients], and hematologic cancer [9 (8.57%) of 105 patients]. As shown in Fig. 1C and D and Supplementary Table S2, patients with hematologic cancer including leukemia, lymphoma, and myeloma have a relatively high death rate [3 (33.33%) of 9 patients], high ICU admission rate [4 (44.44%) of 9 patients], high risks of severe/critical symptoms [6 (66.67%) of 9 patients], and high chance of utilization of invasive mechanical ventilation [2 (22.22%) of 9 patients]. Patients with lung cancer had the second-highest risk levels, with death rate [4 (18.18%) of 22 patients], ICU admission rate [6 (27.27%) of 22 patients], risks of severe/critical symptoms [11 (50.00%) of 22 patients], and the chance of utilization of invasive mechanical ventilation [4 (18.18%) of 22 patients; Table 2].
Severe events in 105 patients with cancer for each type of cancer
Cancer Stage
We found that patients with metastatic cancer (stage IV) had even higher risks of death [OR, 5.58; 95% CI (1.71–18.23); P = 0.01], ICU admission [OR, 6.59; 95% CI (2.32–18.72); P < 0.01], having severe conditions [OR, 5.97; 95% CI (2.24–15.91); P < 0.01], and use of invasive mechanical ventilation [OR, 55.42; 95% CI (13.21–232.47); P < 0.01]. In contrast, patients with nonmetastatic cancer did not demonstrate statistically significant differences compared with patients without cancer, with all P > 0.05 (Fig. 1E and F; Supplementary Tables S2 and S3). In addition, when compared with patients without cancer, patients with lung cancer or other cancers with lung metastasis also showed higher risks of death, ICU admission rates, higher critical symptoms, and use of invasive mechanical ventilation, with all P values below 0.01, but other cancers without lung metastasis had no statistically significant differences (all P values > 0.05; Fig. 1G and H; Supplementary Table S3) when compared with patients without cancer.
Cancer Treatments
Among the 105 COVID-19 patients with cancer in our study, 13 (12.26%) had radiotherapy, 17 (14.15%) received chemotherapy, 8 (7.62%) received surgery, 4 (3.81%) had targeted therapy, and 6 (5.71%) had immunotherapy within 40 days before the onset of COVID-19 symptoms. All of the targeted therapeutic drugs were EGFR–tyrosine kinase inhibitors for treatment of lung cancer, and all of the immunotherapy drugs were PD-1 inhibitors for the treatment of lung cancer. A patient with cancer may have more than one type of therapy. Our observation suggested that patients who received immunotherapy tended to have high rates of death [2 (33.33%) of 6 patients] and high chances of developing critical symptoms [4 (66.67%) of 6 patients]. Patients who received surgery demonstrated higher rates of death [2 (25.00%) of 8 patients], higher chances of ICU admission [3 (37.50%) of 8 patients], higher chances of having severe or critical symptoms [5 (62.50%) of 8 patients], and higher use of invasive ventilation [2 (25.00%) of 8 patients] than other treatments excluding immunotherapy. However, patients with cancer who received radiotherapy did not show statistically significant differences in having any severe events when compared with patients without cancer, with all P values > 0.10 (Fig. 1I and J). Clinical details on the cancer diagnoses and cancer treatments are summarized in Supplementary Table S4.
Timeline of Severe Events
To evaluate the time-dependent evolution of the disease, we conducted the timeline of different events for COVID-19 patients with cancer (Fig. 2A) and COVID-19 patients without cancer (Fig. 2B) with death and other severe events marked in the figure. COVID-19 patients with cancer had a mean length of stay of 27.01 days (SD 9.52) and patients without cancer had a mean length of stay of 17.75 days (SD 8.64); the difference is significant (Wilcoxon test, P < 0.01). To better clarify the contributing factors that might influence outcomes, we also included logistic regression of COVID-19 patients with cancer adjusted by immunosuppression levels in Supplementary Table S5. However, no significant association between immunosuppression and severe outcomes was observed from the analysis (with all P > 0.05).
Timeline of events for COVID-19 patients. A, Timeline of events in COVID-19 patients with cancer. B, Timeline of events in COVID-19 patients without cancer. For visualization purposes, patients without timeline information are excluded and only 105 COVID-19 patients without cancer are shown.
Discussion
The findings in this study suggest that patients with cancer infected with SARS-CoV-2 tend to have more severe outcomes when compared with patients without cancer. Patients with hematologic cancer, lung cancer, and cancers in metastatic stages demonstrated higher rates of severe events compared with patients without cancer. In addition, patients who underwent cancer surgery showed higher death rates and higher chances of having critical symptoms.
The SARS-CoV-2 virus has spread rapidly globally; thus, many countries have not been ready to handle the large volume of people affected by this outbreak due to a lack of knowledge about how this coronavirus affects the general population. To date, reports on the general population infected with SARS-CoV-2 suggest elderly males have a higher incidence and death rate (7, 8). Limited information is known about the outcome of patients with cancer who contract this highly communicable disease. Cancer is among the top causes of death. Asia, Europe, and North America have the highest incidence of cancer in the world (9), and at the moment of the writing of this study the SARS-CoV-2 virus is mainly spreading in these three areas (referred from https://www.cdc.gov/media/releases/2020/s0226-Covid-19-spread.html; https://www.nytimes.com/2020/02/27/world/coronavirusnews.html). Although COVID-19 patients with cancer may share some epidemiologic features with the general population with this disease, they may also have additional clinical characteristics. Therefore, we conducted this study on patients with cancer with coexisting COVID-19 disease to evaluate the potential effect of COVID-19 on patients with cancer.
On the basis of our analysis, COVID-19 patients with cancer tend to have more severe outcomes when compared with the noncancer population. Although COVID-19 is reported to have a relatively low death rate of 2% to 3% in the general population (10), patients with cancer and COVID-19 not only have a nearly 3-fold increase in the death rate than that of COVID-19 patients without cancer, but also tend to have much higher severity of their illness. Altogether, these findings suggest that patients with cancer are a much more vulnerable population in the current COVID-19 outbreak. Our findings are consistent with those presented in a previous study based on 18 patients with cancer (4). Because of the limited number of patients with cancer in the previous study, the authors concluded that among patients with cancer, age is the only risk factor for the severity of the illness. On the basis of our data on 105 patients with cancer, we have discovered additional risk factors, including cancer types, cancer stage, and cancer treatments, which may contribute to the severity of the disease among patients with cancer.
Our data demonstrate that the severity of SARS-CoV-2 infection in patients is significantly affected by the types of tumors. From our analysis, patients with hematologic cancer have the highest severity and death rates among all patients with cancer, and lung cancer follows second. Patients with hematologic cancer in our study include patients with leukemia, myeloma, and lymphoma, who have a more compromised immune system than patients with solid tumors (11). These patients all had a rapidly deteriorating clinical course once infected with COVID-19. Because malignant or dysfunctional plasma cells, lymphocytes, or white blood cells in general in hematologic malignancies have decreased immunologic function (12–14), this could be the main reason why patients with hematologic cancer have very high severity and death rates. All patients with hematologic cancer are prone to the complications of serious infection (12–14), which can exacerbate the condition which could have worsened in patients with COVID-19. In our study, 55.56% of patients with hematologic cancer had severe immunosuppression, which may be the main reason for deteriorated outcomes. Although the small sample size limits representativity of the observation, we believe our finding can serve as an informative starting point for further investigation when a larger cohort from a wide range of healthcare providers becomes available. Among solid tumors, lung cancer is the highest risk category disease in patients with SARS-CoV-2 infection (Fig. 1C). Decreased lung function and severe infection in patients with lung cancer could contribute to the worse outcome in this subpopulation (15, 16).
In our analysis, we classified the SARS-CoV-2 infection–related high risk factors based on death, severe or critical illness, ICU admission, and the utilization of invasive mechanical ventilation. Using these parameters, we detected a multi-fold increase in risk in the cancer population, in contrast to the noncancer population. If there were primary or metastatic tumors in the lungs, patients were more prone to a deteriorated course in a short time. Intriguingly, when patients with cancer had only early-stage disease without metastasis, we did not observe any difference between the cancer and noncancer population in terms of COVID-19–related death rate or severity (Fig. 1E). The stage of cancer diagnosis seemed to play a significant role in the severity and death rate of COVID-19.
Patients with cancer received a wide range of treatments, and we also found that different types of treatments had different influences on severity and death when these patients contracted COVID-19. Recently, immunotherapy has assumed a very important role in treating tumors, which aids in treatment of cancer by blocking the immune escape of cancer cells. But in our study, in contrast to patients with cancer with other treatments, patients with immunotherapy had the highest death rate and the highest severity of illness, a very puzzling finding. According to pathologic studies on the patients with COVID-19, there were desquamation of pneumocytes and hyaline membrane formation, implying that these patients had acute respiratory distress syndrome (ARDS; ref. 17). ARDS induced by cytokine storm is reported to be the main reason for death of SARS-CoV-2–infected patients (18). It is possible that in this setting, immunotherapy induces the release of a large amount of cytokines, which can be toxic to normal cells, including lung epithelial cells (19–21), and therefore lead to a more severe illness. However, in this study the number of patients with immunotherapy was too small; further research with a large case population needs to be conducted in the future.
In addition, COVID-19 patients with cancer who are under active treatment or not under active treatment do not show differences in their outcomes, and there is a significant difference between COVID-19 patients with cancer but not with active treatment and patients without cancer (Supplementary Table S2). These results indicate that COVID-19 patients with both active treatment and just cancer history have a higher risk of developing severe events than noncancer COVID-19 patients. The possible reasons could be due to some known cancer-related complications, for example, anemia, hypoproteinaemia, or dyspnea in early phase of COVID-19 (22). We considered that cancer had a lifetime effect on patients and that cancer survivors always need routine follow-up after primary resection. Therefore, in clinical COVID-19 patient management, equivalent attention needs to be paid to those with cancer whether they are under active therapeutics or not during the outbreak of COVID-19.
This study has several limitations. Although the cohort of COVID-19 patients with cancer is one of the largest in Hubei province, China, the epicenter of the initial outbreak, a larger cohort from the whole country or even from multiple countries will be more representative. Large-scale national and international research collaboration will be necessary to achieve this. At the initial stage of the outbreak, data collection and research activities were not a priority of the hospitals. Therefore, it was not possible to record and collect some data that are potentially informative for our analysis in a timely manner. In addition, due to the urgency of clinical treatment, medical data used in this study were largely disconnected from the patients’ historical electronic medical records, which are mostly stored with a different healthcare provider than the medical center providing COVID-19 care. This left us with limited information about each patient.
Our study is the midsize cohort study on this topic and will provide much-needed information on risk factors of this population. We hope that our findings will help countries better protect patients with cancer affected by the ongoing COVID-19 pandemic.
Methods
Study Design and Patients
We conducted a multicenter study focusing on the clinical characteristics of confirmed cases of COVID-19 patients with cancer in 14 hospitals in Hubei province, China; all of the 14 hospitals served as government-designated hospitals for patients diagnosed with COVID-19. SARS-CoV-2–infected patients without cancer matched by the same hospital and hospitalization time were randomly selected as our control group. In addition, as age is one of the major predictors of severity of respiratory diseases like COVID-19 (4), we excluded from our analysis 117 younger COVID-19 patients without cancer so that median ages of patients with cancer (median = 64.0, IRQ = 14.00) and patients without cancers (median = 63.5, IQR = 14.00) would be comparable.
End Points and Assessments
There were four primary outcomes analyzed in this study: death, admission into the ICU, development of severe or critical symptoms, and utilization of invasive mechanical ventilation. The clinical definition of severe/critical symptoms follows the 5th edition of the 2019Novel Coronavirus Disease (COVID-19) Diagnostic Criteria published by the National Health Commission in China, including septic shock, ARDS, acute kidney injury, disseminated intravascular coagulation, and rhabdomyolysis.
Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System
Source:
VikasMehta, SanjayGoel, RafiKabarriti, DanielCole, MendelGoldfinger, AnaAcuna-Villaorduna, KithPradhan, RajaThota, StanReissman, Joseph A.Sparano, Benjamin A.Gartrell, Richard V.Smith, NitinOhri, MadhurGarg, Andrew D.Racine, ShalomKalnicki, RomanPerez-Soler, BalazsHalmos and AmitVerma. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System
Patients with cancer are presumed to be at increased risk from COVID-19 infection–related fatality due to underlying malignancy, treatment-related immunosuppression, or increased comorbidities. A total of 218 COVID-19–positive patients from March 18, 2020, to April 8, 2020, with a malignant diagnosis were identified. A total of 61 (28%) patients with cancer died from COVID-19 with a case fatality rate (CFR) of 37% (20/54) for hematologic malignancies and 25% (41/164) for solid malignancies. Six of 11 (55%) patients with lung cancer died from COVID-19 disease. Increased mortality was significantly associated with older age, multiple comorbidities, need for ICU support, and elevated levels of D-dimer, lactate dehydrogenase, and lactate in multivariate analysis. Age-adjusted CFRs in patients with cancer compared with noncancer patients at our institution and New York City reported a significant increase in case fatality for patients with cancer. These data suggest the need for proactive strategies to reduce likelihood of infection and improve early identification in this vulnerable patient population.
Significance: COVID-19 in patients with cancer is associated with a significantly increased risk of case fatality, suggesting the need for proactive strategies to reduce likelihood of infection and improve early identification in this vulnerable patient population.
Introduction
The novel coronavirus COVID-19, or severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), has spread rapidly throughout the world since its emergence in December 2019 (1). The virus has infected approximately 2.9 million people in more than 200 countries with more than 200,000 deaths at the time of writing (2). Most recently, the United States has become the epicenter of this pandemic, reporting an estimated 956,000 cases of COVID-19 infection, with the largest concentration in New York City (NYC) and its surrounding areas (approximately >203,000 cases or 35% of all U.S. infections; ref. 3).
Early data suggests that 14% to 19% of infected patients will develop significant sequelae with acute respiratory distress syndrome, septic shock, and/or multiorgan failure (1, 4, 5), and approximately 1% to 4% will die from the disease (2). Recent meta-analyses have demonstrated an almost 6-fold increase in the odds of mortality for patients with chronic obstructive pulmonary disease (COPD) and a 2.5-fold increase for those with diabetes, possibly due to the underlying pulmonary and immune dysfunction (6, 7). Given these findings, patients with cancer would ostensibly be at a higher risk of developing and succumbing to COVID-19 due to immunosuppression, increased coexisting medical conditions, and, in cases of lung malignancy, underlying pulmonary compromise. Patients with hematologic cancer, or those who are receiving active chemotherapy or immunotherapy, may be particularly susceptible because of increased immunosuppression and/or dysfunction.
According the NCI, there were approximately 15.5 million cancer survivors and an estimated 1,762,450 new cases of cancer diagnosed in the United States in 2019 (8). Early case series from China and Italy have suggested that patients with malignancy are more susceptible to severe infection and mortality from COVID-19 (9–12), a phenomenon that has been noted in other pandemics (13). Many of these descriptive studies have included small patient cohorts and have lacked cancer site–specific mortality data or information regarding active cancer treatment. As New York has emerged as the current epicenter of the pandemic, we sought to investigate the risk posed by COVID-19 to our cancer population with more granular data regarding cancer type and active treatment, and identify factors that placed patients with cancer at highest risk of fatality from COVID-19.
Results
Outcomes of 218 Cancer Patients with COVID-19 Show High Overall Mortality with Tumor-Specific Patterns
A total of 218 patients with cancer and COVID-19 were treated in Montefiore Health System (New York, NY) from March 18, 2020, to April 8, 2020. These included 164 (75%) patients with solid tumors and 54 (25%) with hematologic malignancies. This cohort included 127 (58%) males and 91 (42%) females. The cohort was predominantly composed of adult patients (215/218, 98.6%) with a median age of 69 years (range 10–92 years).
Sixty-one (28%) patients expired as a result of COVID-19disease at the time of analysis (Table 1). The mortality was 25% among all patients with solid tumors and was seen to occur at higher rates in patients with lung cancers (55%), gastrointestinal (GI) cancers [colorectal (38%), pancreatic (67%), upper GI (38%)], and gynecologic malignancies (38%). Genitourinary (15%) and breast (14%) cancers were associated with relatively lower mortality with COVID-19 infection.
Hematologic malignancies were associated with higher rate of mortality with COVID-19 (37%). Myeloid malignancies [myelodysplastic syndromes (MDS)/acute myeloid leukemia (AML)/myeloproliferative neoplasm (MPN)] showed a trend for higher mortality compared with lymphoid neoplasms [non-Hodgkin lymphoma (NHL)/chronic lymphoid leukemia (CLL)/acute lymphoblastic leukemia (ALL)/multiple myeloma (MM)/Hodgkin lymphoma; Table 1]. Rates of ICU admission and ventilator use were slightly higher for hematologic malignancies than solid tumors (26% vs. 19% and 11% vs. 10%, respectively), but this did not achieve statistical significance.
Disease Characteristics of Cancer Patients with COVID-19 Demonstrate the Effect of Age, Comorbidities, and Laboratory Biomarkers on Mortality
Analysis of patient characteristics with mortality did not show any gender bias (Table 2). Older age was significantly associated with increased mortality, with median age of deceased cohort at 76 years when compared with 66 years for the nondeceased group (P = 0.0006; Cochran-Armitage test). No significant associations between race and mortality were seen.
Disease characteristics of patients with cancer with COVID-19 and association with mortality
COVID-19 disease severity, as evident from patients who needed ICU care and ventilator support, was significantly associated with increased mortality. Interestingly, active disease (<1 year) and advanced metastatic disease showed a trend for increased mortality, but the association did not achieve statistical significance (P = 0.09 and 0.06, respectively). Active chemotherapy and radiotherapy treatment were not associated with increased case fatality. Very few patients in this cohort were on immunotherapy, and this did not show any associations with mortality.
Analysis of comorbidities demonstrated increased risk of dying from COVID-19 in patients with cancer with concomitant heart disease [hypertension (HTN), coronary artery disease (CAD), and congestive heart failure (CHF)] and chronic lung disease (Table 2). Diabetes and chronic kidney disease were not associated with increased mortality in univariate analysis (Table 2).
We also analyzed laboratory values obtained prior to diagnosis of COVID-19 and during the time of nadir after COVID-19 positivity in our cancer cohort. Relative anemia pre–COVID-19 was associated with increased mortality, whereas pre-COVID platelet and lymphocyte counts were not (Table 3).Post–COVID-19 infection, lower hemoglobin levels, higher total white blood cell (WBC) counts, and higher absolute neutrophil counts were associated with increased mortality (Table 3). Analysis of other serologic biomarkers demonstrated that elevated D-dimer, lactate, and lactate dehydrogenase (LDH) in patients were significantly correlated with dying (Table 3).
Laboratory values of cancer patients with COVID-19 and association with mortality
Next, we conducted multivariate analyses and used variables that showed a significant association with mortality in univariate analysis (P < 0.05 in univariate was seen with age, ICU admission, hypertension, chronic lung disease, CAD, CHF, baseline hemoglobin, nadir hemoglobin, WBC counts, D-dimer, lactate, and LDH). Gender was forced in the model and we used a composite score of comorbidities from the sum of indicators for diabetes mellitus (DM), HTN, chronic lung disease, chronic kidney disease, CAD, and CHF capped at a maximum of 3. In the multivariate model (Supplementary Table S1), we observed that older age [age < 65; OR, 0.23; 95% confidence interval (CI), 0.07–0.6], higher composite comorbidity score (OR, 1.52; 95% CI, 1.02–2.33), ICU admission (OR, 4.83; 95% CI, 1.46–17.15), and elevated inflammatory markers (D-dimer, lactate, and LDH) were significantly associated with mortality after multivariate comparison in patients with cancer and COVID-19.
Interaction with the Healthcare Environment was a Prominent Source of Exposure for Patients with Cancer
A detailed analysis of deceased patients (N = 61; Supplementary Table S2) demonstrated that many were either nursing-home or shelter (n = 22) residents, and/or admitted as an inpatient or presented to the emergency room within the 30 days prior to their COVID-19 positive test (21/61). Altogether, 37/61 (61%) of the deceased cohort were exposed to the healthcare environment at the outset of the COVID-19 epidemic. Few of the patients in the cohort were on active oncologic therapy. The vast majority had a poor Eastern Cooperative Oncology Group performance status (ECOG PS; 51/61 with an ECOG PS of 2 or higher) and carried multiple comorbidities.
Patients with Cancer Demonstrate a Markedly Increased COVID-19 Mortality Rate Compared with Noncancer and All NYC COVID-19 Patients
An age- and sex-matched cohort of 1,090 patients at a 5:1 ratio of noncancer to cancer COVID-19 patients from the same time period and from the same hospital system was also obtained after propensity matching and used as control to estimate the increased risk posed to our cancer population (Table 4). We observed case fatality rates (CFR) were elevated in all age cohorts in patients with cancer and achieved statistical significance in the age groups 45–64 and in patients older than 75 years of age.
Comparison of cancer and COVID-19 mortality with all NYC cases (official NYC numbers up to 5 p.m., April 12, 2020) and a control group from the same healthcare facility
To also compare our CFRs with a larger dataset from the greater NYC region, we obtained official case numbers from New York State (current up to April 12, 2020; ref. 3). In all cohorts, the percentage of deceased patients was found to rise sharply with increasing age (Table 4). Strikingly, CFRs in cancer patients with COVID-19 were significantly, many-fold higher in all age groups when compared with all NYC cases (Table 4).
Discussion
To our knowledge, this is the first large report of COVID-19 CFRs among patients with cancer in the United States. The overall case fatality among COVID-19–infected patients with cancer in an academic center located within the current epicenter of the global pandemic exceeded 25%. In addition, striking tumor-specific discrepancies were seen, with marked increased susceptibility for those with hematologic malignancies and lung cancer. CFRs were 2 to 3 times the age-specific percentages seen in our noncancer population and the greater NYC area for all COVID-19 patients.
Our results seem to mirror the typical prognosis of the various cancer types. Among the most common malignancies within the U.S. population (lung, breast, prostate, and colorectal), there was 55% mortality among patients with lung cancer, 14% for breast cancer, 20% for prostate cancer, and 38% for colorectal cancer. This pattern reflects the overall known lethality of these cancers. The percent annual mortality (ratio of annual deaths/new diagnosis) is 59.3% for lung cancer, 15.2% for breast cancer, 17.4% for prostate cancer, and 36% for colorectal cancer (8). This suggests that COVID-19 infection amplifies the risk of death regardless of the cancer type.
Patients with hematologic malignancies demonstrate a higher mortality than those with solid tumors. These patients tend to be treated with more myelosuppressive therapy, and are often severely immunocompromised because of underlying disease. There is accumulating evidence that one major mechanism of injury may be a cytokine-storm syndrome secondary to hyperinflammation, which results in pulmonary damage. Patients with hematologic malignancy may potentially be more susceptible to cytokine-mediated inflammation due to perturbations in myeloid and lymphocyte cell compartments (14).
Many of the predictive risk factors for mortality in our cancer cohort were similar to published data among all COVID-19 patients. A recent meta-analysis highlighted the association of chronic diseases including hypertension (OR, 2.29), diabetes (OR, 2.47), COPD (OR, 5.97), cardiovascular disease (OR, 2.93), and cerebrovascular disease (OR, 3.89) with a risk for developing severe COVID-19 infection among all patients (15). In our cancer patient dataset, a large proportion of patients had at least one of these concurrent risk factors. In a univariate model, we observed significant associations of death from COVID-19 infection in patients with hypertension, chronic lung disease, coronary heart disease, and congestive heart failure. Serologic predictors in our dataset predictive for mortality included anemia at time of infection, and elevated LDH, D-dimer, and lactic acid, which correlate with available data from all COVID-19 patients.
Rapidly accumulating reports suggest that age and race may play a role in the severity of COVID-19 infection. In our cancer cohort, the median age of the patients succumbing to COVID-19 was 76 years, which was 10 years older than patients who have remained alive. The CDC has reported a disproportionate number of African Americans are affected by COVID-19 in the United States, accounting for 33% of all hospitalized patients while constituting only 13% of the U.S. population (15). However, the racial breakdown of our patients was proportional to the Bronx population as a whole, and race was not a significant predictor of mortality in our univariate or multivariate models. Our data might argue that the increased mortality noted in the larger NYC populations might also likely be driven by socioeconomic and health disparities in addition to underlying biological factors. Overall mortality with COVID-19 has been higher in the Bronx, which is a socioeconomically disadvantaged community with a mean per capita income of $19,721 (16, 17). Our patients with cancer were predominantly from the Bronx and potentially had increased mortality in part due to socioeconomic factors and comorbidities. Even after accounting for the increased mortality seen in COVID-19 in the Bronx, the many-fold magnitude increase in death rates within our cancer cohort can potentially be attributed to the vulnerability of oncology patients. This was evident in the comparison with a control group from the same hospital system that demonstrated a significant association of cancer with mortality in patients between 45 and 64 years of age and older than 75 years of age.
Interaction with the healthcare environment prior to widespread knowledge of the epidemic within NYC was a prominent source of exposure for our patients with cancer. Many of those who succumbed to COVID-19 infection were older and frail with significant impairment of pulmonary and/or immunologic function. These findings could be utilized to risk-stratify patients with cancer during this pandemic, or in future viral airborne outbreaks, and inform mitigation practices for high-risk individuals. These strategies could include early and aggressive social distancing, resource allocation toward more outpatient-based care and telemedicine, testing of asymptomatic high-risk patients, and institution of strict infection-control measures. Indeed, such strategies were implemented early in the pandemic at our center, possibly explaining the relatively low number of infected patients on active therapy.
There were several limitations to our study. Data regarding do not resuscitate or intubate orders were not included in the analysis and could have significantly affected the decision-making and mortality surrounding these patients. Although an attempt was made to control for those receiving active cancer treatment or with additional comorbidities, we could not fully account for the patients’ preexisting health conditions prior to COVID-19 infection. Differential treatment paradigms for COVID-19 infection and sequelae were not controlled for in our analysis. Because of the limited follow-up, the full clinical course of these patients may not be included. Future comparative studies to noncancer patients will be needed to fully ascertain the risk posed to oncology patients. Finally, though our data does include those who were tested and discharged within our health system, we cannot fully account for those who were tested in nonaffiliated outpatient settings, which may potentially bias our study to more severe cases. We also acknowledge that the mortality rate is highly dependent on the breadth of testing, and therefore understand that more widespread detection of viral infection would likely alter the results.
Our data suggest significant risk posed to patients with cancer infected with COVID-19, with an observed significant increase in mortality. The highest susceptibility appears to be in hematologic or lung malignancies, suggesting that proactive strategies to reduce likelihood of infection and improve early identification of COVID-19 positivity in the cancer patient population are clearly warranted. Overall, we hope and expect that our data from the current epicenter of the COVID-19 epidemic will help inform other healthcare systems, patients with cancer, and the public about the particular vulnerability of patients with cancer to this disease.
For more Articles on COVID-19 please see our Coronavirus Portal at
Article ID #273: Live Notes and Conference Coverage in Real Time. COVID19 And The Impact on Cancer Patients Town Hall with Leading Oncologists; April 4, 2020. Published 4/4/2020
This update is the video from the COVID-19 Series 4.
UPDATED 4/08/2020 see below
The Second in a Series of Virtual Town Halls with Leading Oncologist on Cancer Patient Care during COVID-19 Pandemic: What you need to know
The second virtual Town Hall with Leading International Oncologist, discussing the impact that the worldwide COVID-19 outbreak has on cancer care and patient care issues will be held this Saturday April 4, 2020. This Town Hall Series is led by Dr. Roy Herbst and Dr. Hossain Borghaei who will present a panel of experts to discuss issues pertaining to oncology practice as well as addressing physicians and patients concerns surrounding the risk COVID-19 presents to cancer care. Some speakers on the panel represent oncologist from France and Italy, and will give their views of the situation in these countries.
Speakers include:
Roy S. Herbst, MD, PhD, Ensign Professor of Medicine (Medical Oncology) and Professor of Pharmacology; Chief of Medical Oncology, Yale Cancer Center and Smilow Cancer Hospital; Associate Cancer Center Director for Translational Research, Yale Cancer Center
Hossain Borghaei, DO, MS , Chief of Thoracic Medical Oncology and Director of Lung Cancer Risk Assessment, Fox Chase Cancer Center
Giuseppe Curigliano, MD, PhD, University of Milan and Head of Phase I Division at IEO, European Institute of Oncology
Paolo Ascierto, MD National Tumor Institute Fondazione G. Pascale, Medical oncologist from National Cancer Institute of Naples, Italy
Dr. Jack West from City of Hope talked about telemedicine: Coordination of the patient experience, which used to be face to face now moved to a telemedicine alternative. For example a patient doing well on personalized therapy, many patients are well suited for a telemedicine experience. A benefit for both patient and physician.
Dr. Rohit Kumar: In small cancer hospitals, can be a bit difficult to determine which patient needs to come in and which do not. For outpatients testing for COVID is becoming very pertinent as these tests need to come back faster than it is currently. For inpatients the issue is personal protection equipment. They are starting to reuse masks after sterilization with dry heat. Best to restructure the system of seeing patients and scheduling procedures.
Dr. Christopher Manley: hypoxia was an issue for COVID19 patients but seeing GI symptoms in 5% of patients. Nebulizers have potential to aerosolize. For patients in surgery prep room surgical masks are fine. Ventilating these patients are a challenge as hypoxia a problem. Myocarditis is a problem in some patients. Diffuse encephalopathy and kidney problems are being seen. So Interleukin 6 (IL6) inhibitors are being used to reduce the cytokine storm presented in patients suffering from COVID19.
Dr. Hope Rugo from UCSF: Breast cancer treatment during this pandemic has been challenging, even though they don’t use too much immuno-suppressive drugs. How we decide on timing of therapy and future visits is crucial. For early stage breast cancer, neoadjuvant therapy is being used to delay surgeries. Endocrine therapy is more often being used. In patients that need chemotherapy, they are using growth factor therapy according to current guidelines. Although that growth factor therapy might antagonize some lung problems, there is less need for multiple visits.
For metastatic breast cancer, high risk ER positive are receiving endocrine therapy and using telemedicine for followups. For chemotherapy they are trying to reduce the schedules or frequency it is given. Clinical trials have been put on hold, mostly pharmokinetic studies are hard to carry out unless patients can come in, so as they are limiting patient visits they are putting these type of clinical studies on hold.
Dr. Harriet Kluger: Melanoma community of oncologists gathered together two weeks ago to discuss guidelines and best practices during this pandemic. The discussed that there is a lack of data on immunotherapy long term benefit and don’t know the effectiveness of neoadjuvant therapy. She noted that many patients on BRAF inhibitors like Taflinar (dabrafenib) or Zelboraf (vemurafenib) might get fevers as a side effect from these inhibitors and telling them to just monitor themselves and get tested if they want. Yale has also instituted a practice that, if a patient tests positive for COVID19, Yale wants 24 hours between the next patient visit to limit spread and decontaminate.
Marianne Davies: Blood work is now being done at satellite sites to limit number of in person visits to Yale. Usually they did biopsies to determine resistance to therapy but now relying on liquid biopsies (if insurance isn’t covering it they are working with patient to assist). For mesothelioma they are dropping chemotherapy that is very immunosuppressive and going with maintenance pembrolizumab (Keytruda). It is challenging in that COPD mimics the symptoms of COVID and patients are finding it difficult to get nebulizers at the pharmacy because of shortages; these patients that develop COPD are also worried they will not get the respirators they need because of rationing.
Dr. Barbara Burtness: Head and neck cancer. Dr. Burtness stresses to patients that the survival rate now for HPV positive head and neck is much better and leaves patients with extra information on their individual cancers. She also noted a registry or database that is being formed to track data on COVID in patients undergoing surgery and can be found here at https://globalsurg.org/covidsurg/
About CovidSurg
There is an urgent need to understand the outcomes of COVID-19 infected patients who undergo surgery.
Capturing real-world data and sharing international experience will inform the management of this complex group of patients who undergo surgery throughout the COVID-19 pandemic, improving their clinical care.
CovidSurg has been designed by an international collaborating group of surgeons and anesthetists, with representation from Canada, China, Germany, Hong Kong, Italy, Korea, Singapore, Spain, United Kingdom, and the United States.
Dr. Burtness had noted that healthcare care workers are at high risk of COVID exposure during ear nose and throat (ENT) procedures as the coronavirus resides in the upper respiratory tract. As for therapy for head and neck cancers, they are staying away from high dose cisplatin because of the nephrotoxicity seen with high dose cisplatin. An alternative is carboplatin which generally you do not see nephrotoxicity as an adverse event (a weekly carboplatin). Changing or increasing dose schedule (like 6 weeks Keytruda) helps reduce immunologic problems related to immunosupression and patients do not have to come in as often.
Italy and France
Dr. Paolo Ascierto: with braf inhibitors, using in tablet form so patients can take from home. Also they are moving chemo schedules for inpatients so longer dosing schedules. Fever still a side effect from braf inhibitors and they require a swab to be performed to ascertain patient is COVID19 negative. Also seeing pneumonitis as this is an adverse event from checkpoint inhibitors so looking at CT scans and nasal swab to determine if just side effect of I/O drugs or a COVID19 case. He mentioned that their area is now doing okay with resources.
Dr. Guiseppe Curigliano mentioned about the redesign of the Italian health system with spokes and hubs of health care. Spokes are generalized medicine while the hubs represent more specialized centers like CV hubs or cancer hubs. So for instance, if a melanoma patient in a spoke area with COVID cases they will be referred to a hub. He says they are doing better in his area
In the question and answer period, Dr. West mentioned that they are relaxing many HIPAA regulations concerning telemedicine. There is a website on the Centers for Connective Health Policy that shows state by state policy on conducting telemedicine. On immuno oncology therapy, many in the panel had many questions concerning the long term risk to COVID associated with this type of therapy. Fabrice mentioned they try to postpone use of I/O and although Dr. Kluger said there was an idea floating around that PD1/PDL1 inhibitors could be used as a prophylactic agent more data was needed.
Please revisit this page as the recording of this Town Hall will be made available next week.
UPDATED 4/08/2020
Below find theLIVE RECORDING and TAKEAWAYSby the speakers
Town Hall Takeaways
Utilize Telehealth to Its Fullest Benefit
· Patients doing well on targeted therapy or routine surveillance are well suited to telemedicine
· Most patients are amenable to this, as it is more convenient for them and minimizes their exposure
· A patient can speak to multiple specialists with an ease that was not previously possible
· CMS has relaxed some rules to accommodate telehealth, though private insurers have not moved as quickly, and the Center for Connected Health Policy maintains a repository of current state-by-state regulations: https://www.cchpca.org/
Practice Management Strategies
· In the face of PPE shortages, N95 masks can be decontaminated using UV light, hydrogen peroxide, or autoclaving with dry heat; the masks can be returned to the original user until the masks are no longer suitable for use
· For blood work or scans, the use of external satellite facilities should be explored
· Keep pumps outside of the room so nurses can attend to them quickly
· Limit the use of nebulizers, CPAPs, and BiPAPs due to risk of aerosolization
· Caution is urged in the presence of cardiac complications, as ventilated patients may appear to improve, only to suffer severe myocarditis and cardiac arrest following extubation
· When the decision is made to intubate, intubate quickly, as less invasive methods result in aerosolization and increased risks to staff
Study the Lessons of Europe
· The health care system in Italy has been reorganized into “spokes” and “hubs,” with a number of cancer hubs; if there is a cancer patient in a spoke hospital with many COVID patients, this patient may be referred to a hub hospital
· Postpone adjuvant treatments whenever possible
· Oral therapies, which can be managed at home, are preferred over therapies that must be administered in a healthcare setting
· Pneumonitis patients without fevers may be treated with steroids, but nasal swab testing is needed in the presence of concomitant fever
· Any staff who are not needed on site should be working from home, and rotating schedules can be used to keep people healthy
· Devise an annual epidemic control plan now that we have new lessons from COVID
We Must Be Advocates for Our Cancer Patients
· Be proactive with other healthcare providers on behalf of patients with a good prognosis
· Consider writing letters for cancer patients for inclusion into their chart, or addendums on notes, then encourage patients to print these out, or give it to them during their visit
· The potential exists for a patient to be physiologically stable on a ventilator, but intolerant of decannulation; early discussions are necessary to determine reasonable expectations of care
· Be sure to anticipate a second wave of patients, comprised of cancer patients for whom treatments and surgery have been delayed!
Tumor-Specific Learnings
Ø Strategies in Breast Cancer:
· In patients with early-stage disease, promote the use of neoadjuvant therapy where possible to delay the need for surgery
· For patients with metastatic disease in the palliative setting, transition to less frequent chemotherapy dosing if possible
· While growth factors may pose a risk in interstitial lung disease, new guidelines are emerging
· The use of BRAF/MEK inhibitors can cause fevers that are drug-related, and access to an alternate clinic where patients can be assessed is a useful resource
Ø Strategies in Lung Cancer:
· For patients who are stable on an oral, targeted therapy, telehealth check-in is a good option
· For patients who progress on targeted therapies, increased use of liquid biopsies when appropriate can minimize use of bronchoscopy suites and other resources
· For patients on pembrolizumab monotherapy, consider switching to a six-week dosing of 400 mg
· Many lung cancer patients worry about “discrimination” should they develop a COVID infection; it is important to support patients and help manage expectations and concerns
UPDATED 5/11/2020
Townhall on COVID-19 and Cancer Care with Leading Oncologists Series 4
Addressing the Challenges of Cancer Care in the Community
")




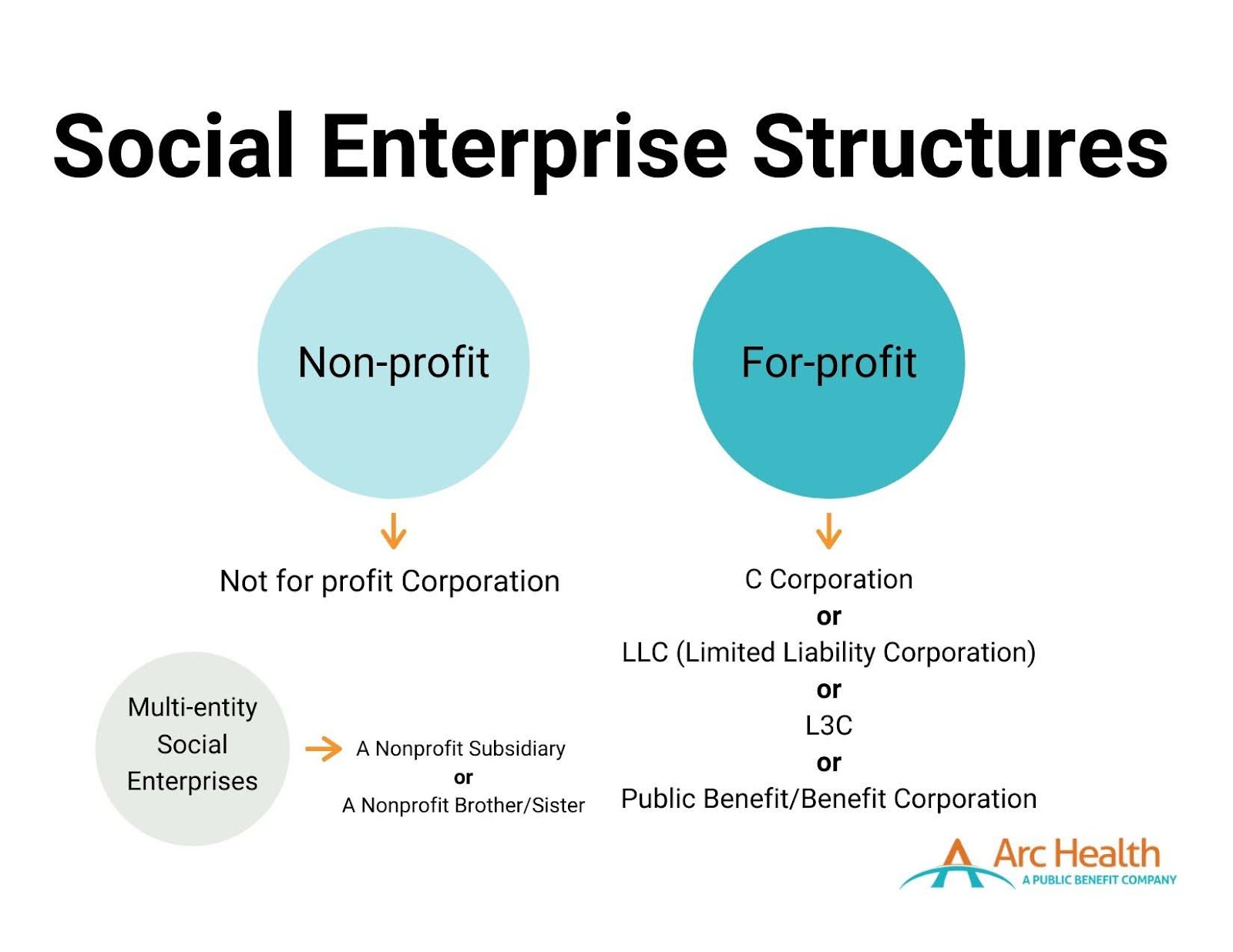



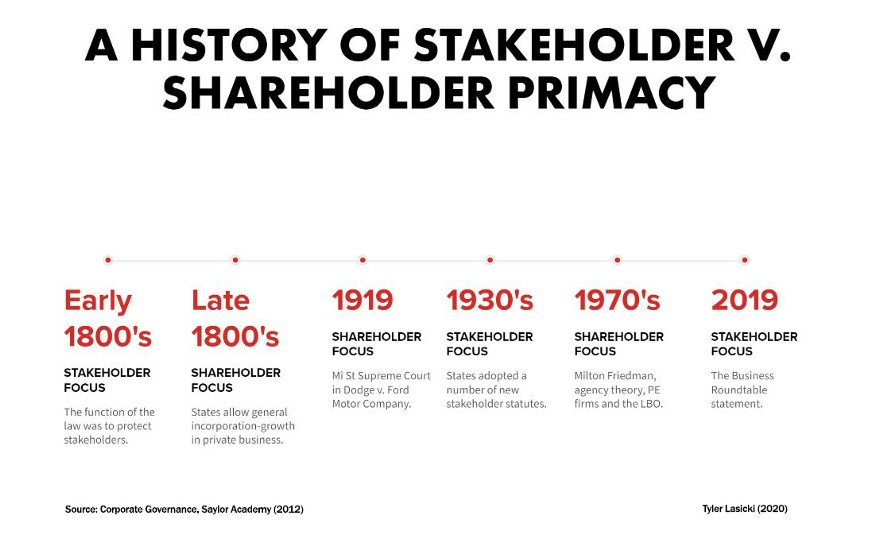










{kind=link}
{kind=link}