Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Eight Subcellular Pathologies driving Chronic Metabolic Diseases – Methods for Mapping Bioelectronic Adjustable Measurements as potential new Therapeutics: Impact on Pharmaceuticals in Use
In this curation we wish to present two breaking through goals:
Goal 1:
Exposition of a new direction of research leading to a more comprehensive understanding of Metabolic Dysfunctional Diseases that are implicated in effecting the emergence of the two leading causes of human mortality in the World in 2023: (a) Cardiovascular Diseases, and (b) Cancer
Goal 2:
Development of Methods for Mapping Bioelectronic Adjustable Measurements as potential new Therapeutics for these eight subcellular causes of chronic metabolic diseases. It is anticipated that it will have a potential impact on the future of Pharmaceuticals to be used, a change from the present time current treatment protocols for Metabolic Dysfunctional Diseases.
According to Dr. Robert Lustig, M.D, an American pediatric endocrinologist. He is Professor emeritus of Pediatrics in the Division of Endocrinology at the University of California, San Francisco, where he specialized in neuroendocrinology and childhood obesity, there are eight subcellular pathologies that drive chronic metabolic diseases.
These eight subcellular pathologies can’t be measured at present time.
In this curation we will attempt to explore methods of measurement for each of these eight pathologies by harnessing the promise of the emerging field known as Bioelectronics.
Unmeasurable eight subcellular pathologies that drive chronic metabolic diseases
Glycation
Oxidative Stress
Mitochondrial dysfunction [beta-oxidation Ac CoA malonyl fatty acid]
Insulin resistance/sensitive [more important than BMI], known as a driver to cancer development
Membrane instability
Inflammation in the gut [mucin layer and tight junctions]
Epigenetics/Methylation
Autophagy [AMPKbeta1 improvement in health span]
Diseases that are not Diseases: no drugs for them, only diet modification will help
Image source
Robert Lustig, M.D. on the Subcellular Processes That Belie Chronic Disease
These eight Subcellular Pathologies driving Chronic Metabolic Diseases are becoming our focus for exploration of the promise of Bioelectronics for two pursuits:
Will Bioelectronics be deemed helpful in measurement of each of the eight pathological processes that underlie and that drive the chronic metabolic syndrome(s) and disease(s)?
IF we will be able to suggest new measurements to currently unmeasurable health harming processes THEN we will attempt to conceptualize new therapeutic targets and new modalities for therapeutics delivery – WE ARE HOPEFUL
In the Bioelecronics domain we are inspired by the work of the following three research sources:
Michael Levin is an American developmental and synthetic biologist at Tufts University, where he is the Vannevar Bush Distinguished Professor. Levin is a director of the Allen Discovery Center at Tufts University and Tufts Center for Regenerative and Developmental Biology. Wikipedia
THE VOICE of Dr. Justin D. Pearlman, MD, PhD, FACC
PENDING
THE VOICE of Stephen J. Williams, PhD
Ten TakeAway Points of Dr. Lustig’s talk on role of diet on the incidence of Type II Diabetes
25% of US children have fatty liver
Type II diabetes can be manifested from fatty live with 151 million people worldwide affected moving up to 568 million in 7 years
A common myth is diabetes due to overweight condition driving the metabolic disease
There is a trend of ‘lean’ diabetes or diabetes in lean people, therefore body mass index not a reliable biomarker for risk for diabetes
Thirty percent of ‘obese’ people just have high subcutaneous fat. the visceral fat is more problematic
there are people who are ‘fat’ but insulin sensitive while have growth hormone receptor defects. Points to other issues related to metabolic state other than insulin and potentially the insulin like growth factors
At any BMI some patients are insulin sensitive while some resistant
Visceral fat accumulation may be more due to chronic stress condition
Fructose can decrease liver mitochondrial function
A methionine and choline deficient diet can lead to rapid NASH development
Neuroimmunology is a field that investigates the bi-directional communication between the nervous system (CNS and PNS) and the immune system. While these two physiological systems were traditionally thought to act independently and that the brain was a privileged site protected by the blood–brain barrier (BBB), researchers now appreciate the highly organized cross talk between the immune and nervous systems in health and disease. The CNS communicates with the immune system via hormonal and neural pathways. The hormonal pathway is predominantly via the HPA axis, which is the primary stress center in rodents, primates, and humans. The neural pathway is mediated via the sympathetic and parasympathetic (the vagus nerve) response. In turn, the immune system signals the CNS via cytokines released by activated immune cells in the periphery but also through activated microglia and astrocytes in the spinal cord and brain. The peripheral inflammation can lead to central proinflammatory milieu and ultimately to sickness behaviour defined as a set of behavioural changes that develop in individuals during the course of systemic inflammation (i.e., fever, lethargy, hyperalgesia). The peripheral inflammation can lead to central proinflammatory milieu and ultimately to sickness behaviour defined as a set of behavioural changes that develop in individuals during the course of systemic inflammation (i.e., fever, lethargy, hyperalgesia), Signals, originating from cellular and molecular elements of the immune system itself, constitute a level of autoregulation. There is also evidence of another more integrative level of regulation mediated by neuroendocrine signals
Pathological pain and the neuroimmune interface
The idea that pain and immunity might be associated beyond an acute response first arose from clinical observations in the 1970s that patients with chronic pain exhibited other symptoms, in addition to hyperalgesia, that parallel the classical systemic sickness response — including lethargy, depression and anxiety. The concomitance of sickness behaviors with chronic pain is therefore suggestive of underlying immune activity. Efforts to identify the origin and nature of the immune mediators involved soon followed, leading to the discovery that elevated peripheral levels of interleukin-1β (IL-1β) both induced hyperalgesia per se and mediated sickness-induced hyperalgesia1,2 . Although peripheral sensitization of pain fibers at local tissue sites of inflammation has a key role in heightening pain from those regions, these peripheral observations were soon extended with the discovery of a central nervous system (CNS) mechanism of action for IL-1β and other cytokines
Physiological pain processing
Pain (either nociceptive pain or inflammatory pain) is protective and adaptive, warning the individual to escape the pain-inducing stimulus and to protect the injured tissue site during healing. The basic scientific understanding of sensory processing and modulation has been dramatically improved by the development of pain assays that recreate some elements of clinical pain syndromes (BOX 1). Painful stimuli (for example, mechanical, thermal and chemical) are initially transduced into neuronal electrical activity and conducted from the peripheral stimulus site to the CNS along a series of well-characterized peripheral nociceptive sensory neurons (first-order primary afferent neurons). The nociceptive signal is then transmitted at central synapses through the release of a variety of neurotransmitters that have the potential to excite second-order nociceptive projection neurons in the spinal dorsal horn or hindbrain (FIG. 1). This process of nociception can occur through several mechanisms involving glutamate and neuropeptides (for example, substance P or calcitonin gene-related peptide (CGRP)). Glutamate activates postsynaptic glutamate AMPA (α-amino-3 -hydroxy-5-methyl-4-isoxazole proprionic acid) and kainate receptors on second-order nociceptive projection neurons. Interestingly, these receptor systems are not all engaged equally in response to different types of pain. Modification of the nociceptive signal can occur at the level of the spinal cord through activation of local GABAergic (that produce γ-aminobutyric acid) and glycinergic inhibitory interneurons.
10.3 Drugs that activate this novel stress response pathway, which they call the mitochondrial-to-cytosolic stress response, protected both nematodes and cultured human cells with Huntington´s disease from protein-folding damage.
New evidence has shown how coronavirus has caused much damage to the brain. There is a new evidence that shows that COVID-19 assault on the brain I has the power to be multipronged. What this means is that it can attack on certain Brain cells such as reduce the amount of blood flow that the brain needs to the brain tissue.
Along with brain damage COVID-19 has also caused strokes and memory loss. A neurologist at yell University Serena Spudich says, “Can we intervene early to address these abnormalities so that people don’t have long-term problems?”
We’re on 80% of the people who have been hospitalized due to COVID-19 have showed brain symptoms which seem to be correlated to coronavirus.
At the start of the pandemic a group of researchers speculated that coronavirus they can damage the brain by infecting the neurons in the cells which are important in the process of transmitting information. After further studies they found out that coronavirus has a harder time getting past the brains defense system and the brain barrier and that it does not affect the neurons in anyway.
An expert in this study indicated that a way in which SARS-CoV-2 may be able to get to the brain is by going through the olfactory mucosa which is the lining of the nasal cavity. It is found that this virus can be found in the nasal cavity which is why we swab the nose one getting tested for COVID-19.
Spudich quotes, “there’s not a tonne of virus in the brain”.
Recent studies indicate that SARS-CoV-2 have ability to infect astrocytes which is a type of cell found in the brain. Astrocytes do quite a lot that supports normal brain function,” including providing nutrients to neurons to keep them working, says Arnold Kriegstein, a neurologist at the University of California, San Francisco.
Astrocytes are star-shaped cells in the central nervous system that perform many functions, including providing nutrients to neurons.
Kriegstein and his fellow colleagues have found that SARS-CoV-2 I mostly infects the astrocytes over any of the other brain cells present. In this research they expose brain organoids which is a miniature brain that are grown from stem cells into the virus.
As quoted in the article” a group including Daniel Martins-de-Souza, head of proteomics at the University of Campinas in Brazil, reported6 in a February preprint that it had analysed brain samples from 26 people who died with COVID-19. In the five whose brain cells showed evidence of SARS-CoV-2 infection, 66% of the affected cells were astrocytes.”
The infected astrocytes could indicate the reasoning behind some of the neurological symptoms that come with COVID-19. Specifically, depression, brain fog and fatigue. Kreigstein quotes, “Those kinds of symptoms may not be reflective of neuronal damage but could be reflective of dysfunctions of some sort. That could be consistent with astrocyte vulnerability.”
A study that was published on June 21 they compared eight different brands of deceased people who did have COVID-19 along with 14 brains as the control. The results of this research were that they found that there was no trace of coronavirus Brain infected but they found that the gene expression was affected in some of the astrocytes.
As a result of doing all this research and the findings the researchers want to know more about this topic and how many brain cells need to be infected for there to be neurological symptoms says Ricardo Costa.
Further evidence has also been done on how SARS-CoV-2 can affect the brain by reducing its blood flow which impairs the neurons’ function which ends up killing them.
Pericytes can be found on the small blood vessels which are called capillaries and are found all throughout the body and in the brain. In a February pre-print there was a report about how SARS-CoV-2 can infect the pericyte in the brain organoids.
David Atwell, a neuroscientist at the University College London, along with his other colleagues had published a pre-print which has evidence to show that SARS-CoV-2 odes In fact pericytes behavior. I researchers saw that in the different part of the hamsters brain SARS-CoV-2 blocks the function of receptors on the pericytes which ultimately causes the capillaries found inside the tissues to constrict.
As stated in the article, It’s a “really cool” study, says Spudich. “It could be something that is determining some of the permanent injury we see — some of these small- vessel strokes.”
Attwell brought to the attention that the drugs that are used to treat high blood pressure may in fact be used in some cases of COVID-19. Currently there are two clinical trials that are being done to further investigate this idea.
There is further evidence showing that the neurological symptoms and damage could in fact be happening because of the bodies on immune system reacting or misfiring after having COVID-19.
Over the past 15 years it has become evident that people’s immune system’s make auto antibodies which attack their own tissues says Harald Prüss in the article who has a Neuroimmunologist at the German Center for neurogenerative Diseases in Berlin. This may cause neuromyelitis optica which is when you can experience loss of vision or weakness in limbs. Harald Prüss summarized that the autoantibodies can pass through the blood brain barrier and ultimately impact neurological disorders such as psychosis.
Prüss and his colleagues published a study last year that focused on them isolating antibodies against SARS-CoV-2 from people. They found that one was able to protect hamsters from lung damage and other infections. The purpose of this was to come up with and create new treatments. During this research they found that some of the antibodies from people. They found that one was able to protect hamsters from lung damage and other infections. The purpose of this was to come up with and create new treatments. During this research they found that some of the antibodies can bind to the brain tissue which can ultimately damage it. Prüss states, “We’re currently trying to prove that clinically and experimentally,” says Prüss.
Was published online in December including Prüss sorry the blood and cerebrospinal fluid of 11 people who were extremely sick with COVID-19. These 11 people had neurological symptoms as well. All these people were able to produce auto antibodies which combined to neurons. There is evidence that when the patients were given intravenous immunoglobin which is a type of antibody it was successful.
Astrocytes, pericytes and autoantibodies we’re not the only pathways. However it is likely that people with COVID-19 experience article symptoms for many reasons. As stated, In the article, Prüss says a key question is what proportion of cases is caused by each of the pathways. “That will determine treatment,” he says.
Comparing COVID-19 Vaccine Schedule Combinations, or “Com-COV” – First-of-its-Kind Study will explore the Impact of using eight different Combinations of Doses and Dosing Intervals for Different COVID-19 Vaccines
Developing Deep Learning Models (DL) for the Instant Prediction of Patients with Epilepsy
Reporter: Srinivas Sriram, Research Assistant I Research Team: Srinivas Sriram, Abhisar Anand
2021 LPBI Summer Intern in Data Science and Website Construction This article reports on a research study conducted from January 2021 to May 2021. This Research was completed before the 2021 LPBI Summer Internship that began on 6/15/2021.
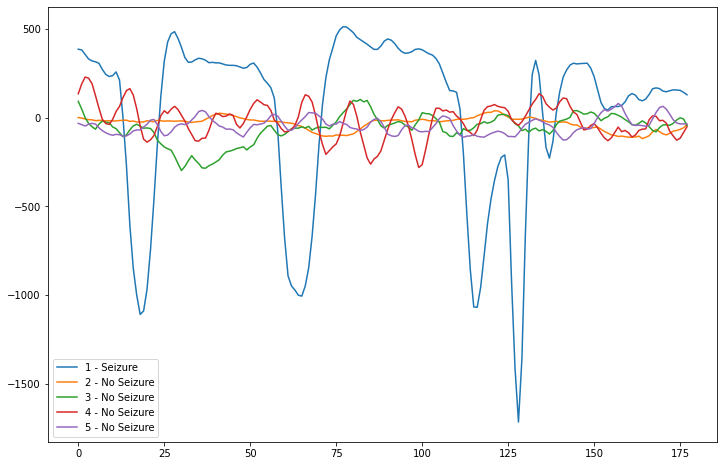
The main criterion of this study was to utilize the dataset (shown above) to develop a DL network that could accurately predict new seizures based on incoming data. To begin the study, our research group did some exploratory data analysis on the dataset and we recognized the key defining pattern of the data that allowed for the development of the DL model. This pattern of the data can be represented in the graph above, where the lines representing seizure data had major spikes in extreme hertz values, while the lines representing normal patient data remained stable without any spikes. We utilized this pattern as a baseline for our model.
Conclusions and Future Improvements:
Through our system, we were able to create a prototype solution that would predict when seizures happened in a potential patient using an accurate LSTM network and a reliable hardware system. This research can be implemented in hospitals with patients suffering from epilepsy in order to help them as soon as they experience a seizure to prevent damage. However, future improvements need to be made to this solution to allow it to be even more viable in the Healthcare Industry, which is listed below.
Needs to be implemented on a more reliable EEG headset (covers all neurons of the brain, less prone to electric disruptions shown in the prototype).
Needs to be tested on live patients to deem whether the solution is viable and provides a potential solution to the problem.
The network can always be fine-tuned to maximize performance.
A better alert system can be implemented to provide as much help as possible.
These improvements, when implemented, can help provide a real solution to one of the most common diseases faced in the world.
Background Information:
Epilepsy is described as a brain disorder diagnostic category for multiple occurrences of seizures that happen within recurrent and/or a brief timespan. According to the World Health Organization, seizure disorders, including epilepsy, are among the most common neurological diseases. Those who suffer seizures have a 3 times higher risk of premature death. Epilepsy is often treatable, especially when physicians can provide necessary treatment quickly. When untreated, however, seizures can cause physical, psychological, and emotional, including isolation from others. Quick diagnosis and treatment prevent suffering and save lives. The importance of a quick diagnosis of epilepsy has led to our research team developing Deep Learning (DL) algorithms for the sole purpose of detecting epileptic seizures as soon as they occur.
Throughout the years, one common means of detecting Epilepsy has emerged in the form of an electroencephalogram (EEG). EEGs can detect and compile “normal” and “abnormal “brain wave activity” and “indicate brain activity or inactivity that correlates with physical, emotional, and intellectual activities”. EEG waves are classified mainly by brain wave frequencies (EEG, 2020). The most commonly studied are delta, theta, alpha, sigma, and beta waves. Alpha waves, 8 to 12 hertz, are the key wave that occurs in normal awake people. They are the defining factor for the everyday function of the adult brain. Beta waves, 13 to 30 hertz, are the most common type of wave in both children and adults. They are found in the frontal and central areas of the brain and occur at a certain frequency which, if slow, is likely to cause dysfunction. Theta waves, 4 to 7 hertz, are also found in the front of the brain, but they slowly move backward as drowsiness increases and the brain enters the early stages of sleep. Theta waves are known as active during focal seizures. Delta waves, 0.5 to 4 hertz, are found in the frontal areas of the brain during deep sleep. Sigma waves, 12-16 hertz, are very slow frequency waves that occur during sleep. EEG detection of electrical brain wave frequencies can be used to detect and diagnose seizures based on their deviation from usual brain wave patterns.
In this particular research project, our research group hoped to develop a DL algorithm that when implemented on a live, portable EEG brain wave capturing device, could accurately predict when a particular patient was suffering from Epilepsy as soon as it occurred. This would be accomplished by creating a network that could detect when the brain frequencies deviated from the normal frequency ranges.
The Study:
Line Graph representing EEG Brain Waves from a Seizure versus EEG Brain Waves from a normal individual.
To expand more on the dataset, it is an EEG data set compiled by Qiuyi Wu and Ernest Fokoue (2021) from the work of medical researchers R.Andrzejak, M.D. et al. (2001) which had been made public domain through the UCI Machine Learning Repository We also confirmed fair use permission with UCI. The dataset had been gathered by Andrzejak during examinations of 500 patients with a chronic seizure disorder. R.G.Andrzejak, et al. (2001) recorded each entry in the EEG dataset used for this project within 23.6 seconds in a time-series data structure. Each row in the dataset represented a patient recorded. The continuous variables in the dataset were single EEG data points at that specific point in time during the measuring period. At the end of the dataset, was a y-variable that indicated whether or not the patient had a seizure during the period the data was recorded. The continuous variables, or the EEG data, for each patient, varied widely based on whether the patient was experiencing a seizure at that time. The Wu & Fokoue Dataset (2021) consists of one file of 11,500 rows, each with 178 sequential data points concatenated from the original dataset of 5 data folders, each including 100 files of EEG recordings of 23.6 seconds and containing 4097 data points. Each folder contained a single, original subset. Subset A contained EEG data gathering during epileptic seizure…. Subset B contained EEG data from brain tumor sites. Subset 3, from a healthy site where tumors had been located. Subsets 4 and 5 from non-seizure patients at rest with eyes open and closed, respectively.
Based on the described data, our team recognized that a Recurrent Neural Network (RNN) was needed to input the sequential data and return an output of whether the sequential data was a seizure or not. However, we realized that RNN models are known to get substantially large over time, reducing computation speeds. To help provide a solution to this issue, our group decided to implement a long-short-term memory (LSTM) model. After deciding our model’s architecture, we proceeded to train our model in two different DL frameworks inside Python, TensorFlow, and PyTorch. Through various rounds of retesting and redesigning, we were able to train and develop two accurate models in each of the models that not only performed well while learning the data while training, but also could accurately predict new data in the testing set (98 percent accuracy on the unseen data). These LSTM networks could classify normal EEG data when the brain waves are normal, and then immediately predict the seizure data based on if a dramatic spike occurred in the data.
After training our model, we had to implement our model in a real-life prototype scenario in which we utilized a Single Board Computer (SBC) in the Raspberry Pi 4 and a live capturing EEG headset in the Muse 2 Headband. The two hardware components would sync up through Bluetooth and the headband would return EEG data to the Raspberry Pi, which would process the data. Through the Muselsl API in Python, we were able to retrieve this EEG data in a format similar to the manner implemented during training. This new input data would be fed into our LSTM network (TensorFlow was chosen for the prototype due to its better performance than the PyTorch network), which would then output the result of the live captured EEG data in small intervals. This constant cycle would be able to accurately predict a seizure as soon as it occurs through batches of EEG data being fed into the LSTM network. Part of the reason why our research group chose the Muse Headband, in particular, was not only due to its compatibility with Python but also due to the fact that it was able to represent seizure data. Because none of our members had epilepsy, we had to find a reliable way of testing our model to make sure it worked on the new data. Through electrical disruptions in the wearable Muse Headband, we were able to simulate these seizures that worked with our network’s predictions. In our program, we implemented an alert system that would email the patient’s doctor as soon as a seizure was detected.
Wu, Q. & Fokoue, E. (2021). Epileptic seizure recognition data set: Data folder & Data set description. UCI Machine Learning Repository: Epileptic Seizure Recognition. Jan. 30. Center for Machine Learning and Intelligent Systems, University of California Irvine.
Nayak, C. S. (2020). EEG normal waveforms.” StatPearls [Internet]. U.S. National Library of Medicine, 31 Jul. 2020, www.ncbi.nlm.nih.gov/books/NBK539805/#.
Deep Learning extracts Histopathological Patterns and accurately discriminates 28 Cancer and 14 Normal Tissue Types: Pan-cancer Computational Histopathology Analysis
Despite heated discussion over whether it works, the FDA has approved Aduhelm, bringing a new ray of hope to the Alzheimer’s patients.
Curator and Reporter: Dr. Premalata Pati, Ph.D., Postdoc
Despite heated discussion over whether it works, the FDA has approved Aduhelm, bringing a new ray of hope to the Alzheimer’s patients.
On Monday, 7th June 2021, a controversial new Alzheimer’sDisease treatment was licensed in the United States for the first time in nearly 20 years, sparking calls for it to be made available worldwide despite conflicting evidence about its usefulness. The drug was designed for people with mild cognitive impairment, not severe dementia, and it was designed to delay the progression of Alzheimer’s disease rather than only alleviate symptoms.
The route to FDA clearance for Aducanumab has been bumpy – and contentious.
Though doctors, patients, and the organizations that assist them are in desperate need of therapies that can delay mental decline, scientists question the efficacy of the new medicine, Aducanumab or Aduhelm. In March 2019, two trials were halted because the medications looked to be ineffective. “The futility analysis revealed that the studies were most likely to fail,” said Isaacson of Weill Cornell Medicine and NewYork-Presbyterian. Biogen, the drug’s manufacturer revealed several months later that a fresh analysis with more participants found that individuals who got high doses of Aducanumab exhibited a reduction in clinical decline in one experiment. Patients treated with high-dose Aducanumab had 22% reduced clinical impairment in their cognitive health at 18 months, indicating that the advancement of their early Alzheimer’s disease was halted, according to FDA briefing documents from last year.
When the FDA’s members were split on the merits of the application in November, it was rejected. Three of its advisers went public, claiming that there was insufficient evidence that it worked in a scientific journal. They were concerned that if the medicine was approved, it might reduce the threshold for future approvals, owing to the scarcity of Alzheimer’s treatments.
Dr. Caleb Alexander, a drug safety and effectiveness expert at the Johns Hopkins Bloomberg School of Public Health, was one of the FDA advisers who was concerned that the data presented to the agency was a reanalysis after the experiment was stopped. It was “like the Texas sharpshooter fallacy,” he told the New York Times, “where the sharpshooter blows up a barn and then goes and paints a bullseye around the cluster of holes he loves.”
Some organizations, such as the non-profit Public Citizen’s Health Research Group, claimed that the FDA should not approve Aducanumab for the treatment of Alzheimer’s disease because there is insufficient proof of its efficacy.
The drug is a monoclonal antibody that inhibits the formation of amyloid protein plaques in the brain, which are thought to be the cause of Alzheimer’s disease. The majority of Alzheimer’s medications have attempted to erase these plaques.
Aducanumab appears to do this in some patients, but only when the disease is in its early stages. This means that people must be checked to see if they have the disease. Many persons with memory loss are hesitant to undergo testing because there is now no treatment available.
The few Alzheimer’s medications available appear to have limited effectiveness. When Aricept, also known as Donepezil, was approved more than 20 years ago, there was a major battle to get it. It was heralded as a breakthrough at the time – partly due to the lack of anything else. It has become obvious that it slows mental decline for a few months but makes little effect in the long run.
The findings of another trial for some patients backed up those conclusions.
Biogen submitted a Biologics License Application to the FDA in July 2020, requesting approval of the medicine.
The FDA’s decision has been awaited by Alzheimer’s disease researchers, clinicians, and patients since then.
Support for approval of the drug
Other groups, such as the Alzheimer’s Association, have supported the drug’s approval.
The Alzheimer’s Association‘s website stated on Friday, “This is a critical time, regardless of the FDA’s final judgment. We’ve never been this close to approving an Alzheimer’s drug that could affect the disease’s development rather than just the symptoms. We can keep working together to achieve our goal of a world free of Alzheimer’s disease and other dementias.”
The drug has gotten so much attention that the Knight Alzheimer Disease Research Center at Washington University in St. Louis issued a statement on Friday stating that even if it is approved, “it will still likely take several months for the medication to pass other regulatory steps and become available to patients.”
Biogen officials told KGO-TV on Monday that the medicine will be ready to ship in about two weeks and that they have identified more than 900 facilities across the United States that they feel will be medically and commercially suitable.
Officials stated the corporation will also provide financial support to qualifying patients so that their out-of-pocket payments are as low as possible. Biogen has also pledged not to raise the price for at least the next four years.
Most Medicare customers with supplemental plans, according to the firm, will have a limited or capped co-pay.
Case studies connected to the Drug Approval
Case 1
Ann Lange, one of several Chicago-area clinical trial volunteers who received the breakthrough Alzheimer’s treatment, said,
It really offers us so much hope for a long, healthy life.
Lange, 60, has Alzheimer’s disease, which she was diagnosed with five years ago. Her memory has improved as a result of the monthly infusions, she claims.
She said,
I’d forget what I’d done in the shower, so I’d scribble ‘shampoo, conditioner, face, body’ on the door. Otherwise, I’d lose track of what I’m doing “Lange remarked. “I’m not required to do that any longer.
Case 2
Jenny Knap, 69, has been receiving infusions of the Aducanumab medication for about a year as part of two six-month research trials. She told CNN that she had been receiving treatment for roughly six months before the trial was halted in 2019, and that she had recently resumed treatment.
Knap said,
I can’t say I noticed it on a daily basis, but I do think I’m doing a lot better in terms of checking for where my glasses are and stuff like that.
When Knap was diagnosed with mild cognitive impairment, a clinical precursor to Alzheimer’s disease, in 2015, the symptoms were slight but there.
Her glasses were frequently misplaced, and she would repeat herself, forgetting previous talks, according to her husband, Joe Knap.
Joe added,
We were aware that things were starting to fall between the cracks as these instances got more often
Jenny went to the Lou Ruvo Center for Brain Health at the Cleveland Clinic in Ohio for testing and obtained her diagnosis. Jenny found she was qualified to join in clinical trials for the Biogen medicine Aducanumab at the Cleveland Clinic a few years later, in early 2017. She volunteered and has been a part of the trial ever since.
It turns out that Jenny was in the placebo category for the first year and a half, Joe explained, meaning she didn’t get the treatment.
They didn’t realize she was in the placebo group until lately because the trial was blind. Joe stated she was given the medicine around August 2018 and continued until February 2019 as the trial progressed. The trial was halted by Biogen in March 2019, but it was restarted last October, when Jenny resumed getting infusions.
Jenny now receives Aducanumab infusions every four weeks at the Cleveland Clinic, which is roughly a half-hour drive from their house, with Joe by her side. Jenny added that, despite the fact that she has only recently begun therapy, she believes it is benefiting her, combined with a balanced diet and regular exercise (she runs four miles).
The hope of Aducanumab is to halt the progression of the disease rather than to improve cognition. We didn’t appreciate any significant reduction in her condition, Jenny’s doctor, Dr. Babak Tousi, who headed Aducanumab clinical studies at the Cleveland Clinic, wrote to CNN in an email.
This treatment is unlike anything we’ve ever received before. There has never been a drug that has slowed the growth of Alzheimer’s disease, he stated, Right now, existing medications like donepezil and memantine aid with symptoms but do not slow the disease’s progression.
Jenny claims that the medicine has had no significant negative effects on her.
There was signs of some very minor bleeding in the brain at one point, which was quite some time ago. It was at very low levels, in fact, Joe expressed concern about Jenny, but added that the physicians were unconcerned.
According to Tousi, with repeated therapy, “blood vessels may become leaky, allowing fluid and red blood cells to flow out to the surrounding area,” and “micro hemorrhages have been documented in 19.1% of trial participants who got” the maximal dose of therapy”.
Jenny and Joe’s attitude on the future has improved as a result of the infusions and keeping a healthy lifestyle, according to Joe. They were also delighted to take part in the trial, which they saw as an opportunity to make a positive influence in other people’s lives.
There was this apprehension of what was ahead before we went into the clinical trial, Joe recalled. “The medical aspect of the infusion gives us reason to be optimistic. However, doing the activity on a daily basis provides us with immediate benefits.”
The drug’s final commercialization announcement
Aducanumab, which will be marketed as Aduhelm, is a monthly intravenous infusion that is designed to halt cognitive decline in patients with mild memory and thinking issues. It is the first FDA-approved medication for Alzheimer’s disease that targets the disease process rather than just the symptoms.
The manufacturer, Biogen, stated Monday afternoon that the annual list price will be $56,000. In addition, diagnostic tests and brain imaging will very certainly cost tens of thousands of dollars.
The FDA approved approval for the medicine to be used but ordered Biogen to conduct a new clinical trial, recognizing that prior trials of the medicine had offered insufficient evidence to indicate effectiveness.
Biogen Inc said on Tuesday that it expects to start shipping Aduhelm, a newly licensed Alzheimer’s medicine, in approximately two weeks and that it has prepared over 900 healthcare facilities for the intravenous infusion treatment.
Other Relevant Articles
Gene Therapy could be a Boon to Alzheimer’s disease (AD): A first-in-human clinical trial proposed
Alnylam Announces First-Ever FDA Approval of an RNAi Therapeutic, ONPATTRO™ (patisiran) for the Treatment of the Polyneuropathy of Hereditary Transthyretin-Mediated Amyloidosis in Adults
Gene Therapy could be a Boon to Alzheimer’s disease (AD): A first-in-human clinical trial proposed
Reporter: Dr. Premalata Pati, Ph.D., Postdoc
A recent research work performed by the Researchers at the University of California San Diego School of Medicine has shared their first-in-human Phase I clinical trial to assess the safety and viability of gene therapy to deliver a key protein into the brains of persons with Alzheimer’s Disease (AD) or Mild Cognitive Impairment (MCI), a condition that often precedes full-blown dementia.
Mark Tuszynski, M.D., Ph.D., Professor of Neuroscience and Director of the Translational Neuroscience Institute at UC San Diego and team predicted that Gene therapy could be a boon to potential treatments for the disorders like AD and MCI.
The study provides an insight into the genetic source of these mental diseases.
The roots of mental disorders have remained an enigma for so many years. Alzheimer’s disease (AD) is an irreversible, progressive brain disorder that slowly destroys memory and thinking skills and, eventually, the ability to carry out the simplest tasks. AD is a neurodegenerative condition. A buildup of plaques and tangles in the brain, along with cell death, causes memory loss and cognitive decline. In most people with the disease, those with the late-onset type – symptoms first appear in their mid-60s. Alzheimer’s disease is the mostly appearing type of dementia in patients.
Despite decades of effort and billions of dollars of research investment, there are just mere two symptomatic treatments for AD. There is no cure or approved way to slow or stop the progression of the neurological disorder that afflicts more than 5 million Americans and is the sixth leading cause of death in the United States.
Prof. Tuszynski said gene therapy has been tested on multiple diseases and conditions, represents a different approach to a disease that requires new ways of thinking about the disease and new attempts at treatments.
The research team found that delivering the BDNF to the part of the brain that is affected earliest in Alzheimer’s disease; the entorhinal cortex and hippocampus – was able to protect from ongoing cell degeneration by reversing the loss of connections. “These trials were observed in aged rats, amyloid mice, and aged monkeys.”
The protein, calledBrain-Derived Neurotrophic Factor or BDNF, a family of growth factors found in the Brain and Central Nervous System that support the survival of existing neurons and promote growth and differentiation of new neurons and synapses. BDNF is especially important in brain regions susceptible to degeneration in AD. It is normally produced throughout life in the entorhinal cortex, an important memory center in the brain and one of the first places where the effects of AD typically appear in the form of short-term memory loss. Persons with AD have diminished levels of BDNF.
However, BDNF is a large molecule and cannot pass through the Blood-Brain Barrier. As a solution, researchers will use gene therapy in which a harmless Adeno-Associated Virus (AAV2) is modified to carry the BDNF gene and injected directly into targeted regions of the brain, where researchers hope it will prompt the production of therapeutic BDNF in nearby cells.
Precautions were taken precisely in injecting the patient to avoid exposure to surrounding degenerating neurons since freely circulating BDNF can cause adverse effects, such as seizures or epileptic conditions.
The recent research and study speculate a safe and feasible assessment of the AAV2-BDNF pathway in humans. A previous gene therapy trial from 2001 to 2012 using AAV2 and a different protein called Nerve Growth Factor (NGF) was carried out by Prof. Tuszynski and team where they observed immense growth, axonal sprouting, and activation of functional markers in the brains of participants.
He also shared that “The BDNF gene therapy trial in AD represents an advancement over the earlier NGF trial, BDNF is a more potent growth factor than NGF for neural circuits that degenerate in AD. Besides, new methods for delivering BDNF will more effectively deliver and distribute it into the entorhinal cortex and hippocampus.”
The research team hopes that the three-year-long trial will recruit 12 participants with either diagnosed AD or MCI to receive AAV2-BDNF treatment, with another 12 persons serving as comparative controls over that period.
The researchers have plans to build on recent successes of gene therapy in other diseases, including a breakthrough success in the treatment of congenital weakness in infants(spinal muscular atrophy) and blindness (Leber Hereditary Optic Neuropathy, a form of retinitis pigmentosa).”
Two brothers with MEPAN Syndrome: A Rare Genetic Disorder
Reporter: Amandeep Kaur
In the early 40s, a married couple named Danny and Nikki, had normal pregnancy and delivered their first child in October 2011. The couple was elated after the birth of Carson because they were uncertain about even conceiving a baby. Soon after birth, the parents started facing difficulty in feeding the newborn and had some wakeful nights, which they used to called “witching hours”. For initial six months, they were clueless that something was not correct with their infant. Shortly, they found issues in moving ability, sitting, and crawling with Carson. Their next half year went in visiting several behavioral specialists and pediatricians with no conclusion other than a suggestion that there is nothing to panic as children grow at different rates.
Later in early 2013, Caron was detected with cerebral palsy in a local regional center. The diagnosis was based on his disability to talk and delay in motor development. At the same time, Carson had his first MRI which showed no negative results. The parents convinced themselves that their child condition would be solved by therapies and thus started physical and occupational therapies. After two years, the couple gave birth to another boy child named Chase in 2013. Initially, there was nothing wrong with Chase as well. But after nine months, Chase was found to possess the same symptoms of delaying in motor development as his elder brother. It was expected that Chase may also be suffering from cerebral palsy. For around one year both boys went through enormous diagnostic tests starting from karyotyping, metabolic screen tests to diagnostic tests for Fragile X syndrome, lysosomal storage disorders, Friedreich ataxia and spinocerebellar ataxia. Gene panel tests for mitochondrial DNA and Oxidative phosphorylation (OXPHOS) deficiencies were also performed. No conclusion was drawn because each diagnostic test showed the negative results.
Over the years, the condition of boys was deteriorating as their movements became stiffer and ataxic, they were not able to crawl anymore. By the end of 2015, the boys had an MRI which showed some symmetric anomalies in their basal ganglia indicating a metabolic condition. The symptoms of Carson and Chase was not even explained by whole exome sequencing due to the absence of any positive result. The grievous journey of visits to neurologist, diagnostic tests and inconclusive results led the parents to rethink about anything happened erroneous due to them such as due to their lifestyle, insufficient intake of vitamins during pregnancy or exposure to toxic agents which left their sons in that situation.
During the diagnostic odyssey, Danny spent many restless and sleepless nights in searching PubMed for any recent cases with symptoms similar to his sons and eventually came across the NIH’s Undiagnosed Diseases Network (UDN), which gave a light of hope to the demoralized family. As soon as Danny discovered about the NIH’s Diseases Network, he gathered all the medical documents of both his sons and submitted the application. The submitted application in late 2015 got accepted a year later in December 2016 and they got their first appointment in early 2017 at the UDN site at Stanford. At Stanford, the boys had gone through whole-genome sequencing and some series of examinations which came back with inconclusive results. Finally, in February 2018, the family received some conclusive results which explained that the two boys suffer from MEPAN syndrome with pathogenic mutations in MECR gene.
MEPAN means Mitochondrial Enoyl CoA reductase Protein-Associated Neurodegeneration
MEPAN syndrome is a rare genetic neurological disorder
MEPAN syndrome is associated with symptoms of ataxia, optic atrophy and dystonia
The wild-type MECR gene encodes a mitochondrial protein which is involved in metabolic processes
The prevalence rate of MEPAN syndrome is 1 in 1 million
Currently, there are 17 patients of MEPAN syndrome worldwide
The symptoms of Carson and Chase of an early onset of motor development with no appropriate biomarkers and T-2 hyperintensity in the basal ganglia were matching with the seven known MEPAN patient at that time. The agonizing journey of five years concluded with diagnosis of rare genetic disorder.
Despite the advances in genetic testing and their low-cost, there are many families which still suffer and left undiagnostic for long years. To shorten the diagnostic journey of undiagnosed patients, the whole-exome and whole-genome sequencing can be used as a primary tool. There is need of more research to find appropriate treatments of genetic disorders and therapies to reduce the suffering of the patients and families. It is necessary to fill the gap between the researchers and clinicians to stimulate the development in diagnosis, treatment and drug development for rare genetic disorders.
The family started a foundation named “MEPAN Foundation” (https://www.mepan. org) to reach out to the world to educate people about the mutation in MECR gene. By creating awareness among the communities, clinicians, and researchers worldwide, the patients having rare genetic disorder can come closer and share their information to improve their condition and quality of life.
Dysregulation of ncRNAs in association with Neurodegenerative Disorders
Curator: Amandeep Kaur
Research over the years has added evidences to the hypothesis of “RNA world” which explains the evolution of DNA and protein from a simple RNA molecule. Our understanding of RNA biology has dramatically changed over the last 50 years and rendered the scientists with the conclusion that apart from coding for protein synthesis, RNA also plays an important role in regulation of gene expression.
The universe of non-coding RNAs (ncRNAs) is transcending the margins of preconception and altered the traditional thought that the coding RNAs or messenger RNAs (mRNAs) are more prevalent in our cells. Research on the potential use of ncRNAs in therapeutic relevance increased greatly after the discovery of RNA interference (RNAi) and provided important insights into our further understanding of etiology of complex disorders.
Latest research on neurodegenerative disorders has shown the perturbed expression of ncRNAs which provides the functional association between neurodegeneration and ncRNAs dysfunction. Due to the diversity of functions and abundance of ncRNAs, they are classified into Housekeeping RNAs and Regulatory ncRNAs.
The best known classes of ncRNAs are the microRNAs (miRNAs) which are extensively studied and are of research focus. miRNAs are present in both intronic and exonic regions of matured RNA (mRNA) and are crucial for development of CNS. The reduction of Dicer-1, a miRNA biogenesis-related protein affects neural development and the elimination of Dicer in specifically dopaminergic neurons causes progressive degeneration of these neuronal cells in striatum of mice.
A new class of regulatory ncRNAs, tRNAs-derived fragments (tRFs) is superabundantly present in brain cells. tRFs are considered as risk factors in conditions of neural degeneration because of accumulation with aging. tRFs have heterogenous functions with regulation of gene expression at multiple layers including regulation of mRNA processing and translation, inducing the activity of silencing of target genes, controlling cell growth and differentiation processes.
The existence of long non-coding RNAs (lncRNAs) was comfirmed by the ENCODE project. Numerous studies reported that approximately 40% of lncRNAs are involved in gene expression, imprinting and pluripotency regulation in the CNS. lncRNA H19 is of paramount significance in neural viability and contribute in epilepsy condition by activating glial cells. Other lncRNAs are highly bountiful in neurons including Evf2 and MALAT1 which play important function in regulating neural differentiation and synapse formation and development of dendritic cells respectively.
Recently, a review article in Nature mentioned about the complex mechanisms of ncRNAs contributing to neurodegenerative conditions. The ncRNA-mediated mechanisms of regulation are as follows:
Epigenetic regulation: Various lncRNAs such as BDNF-AS, TUG1, MEG3, NEAT1 and TUNA are differentially expressed in brain tissue and act as epigenetic regulators.
RNAi: RNA interference includes post-transcriptional repression by small-interfering RNAs (siRNAs) and binding of miRNAs to target genes. In a wide spectrum of neurodegenerative diseases such as Alzheimer’s disease, Parkinson disease, Huntington’s disease, Amyotrophic lateral sclerosis, Fragile X syndrome, Frontotemporal dementia, and Spinocerebellar ataxia, have shown perturbed expression of miRNA.
Alternative splicing: Variation in splicing of transcripts of ncRNAs has shown adverse affects in neuropathology of degenerative diseases.
mRNA stability: The stability of mRNA may be affected by RNA-RNA duplex formation which leads to the degradation of sense mRNA or blocking the access to proteins involved in RNA turnover and modify the progression of neurodegenerative disorders.
Translational regulation: Numerous ncRNAs including BC200 directly control the translational process of transcripts of mRNAs and effect human brain of Alzheimer’s disease.
Molecular decoys: Non-coding RNAs (ncRNAs) dilute the expression of other RNAs by molecular trapping, also known as competing endogenous RNAs (ceRNAs) which hinder the normal functioning of RNAs. The ceRNAs proportion must be equivalent to the number of target miRNAs that can be sequestered by each ncRNAs in order to induce consequential de-repression of the target molecules.
The unknown functions of numerous annotated ncRNAs may explain the underlying complexity in neurodegenerative disorders. The profiling of ncRNAs of patients suffering from neurodevelopmental and neurodegenerative conditions are required to outline the changes in ncRNAs and their role in specific regions of brain and cells. Analysis of Large-scale gene expression and functional studies of ncRNAs may contribute to our understanding of these diseases and their remarkable connections. Therefore, targeting ncRNAs may provide effective therapeutic perspective for the treatment of neurodegenerative diseases.
Elizabeth Unger from the Tian group at UC Davis, Jacob Keller from the Looger lab from HHMI, Michael Altermatt from the Gradinaru group at California Institute of Technology, and colleagues did just this, by redesigned the binding pocket of periplasmic binding proteins (PBPs) using artificial intelligence, such that it became a fluorescent sensor specific for serotonin. Not only this, the group showed that it could express and use this molecule to detect serotonin on the cell, tissue, and whole animal level.
By starting with a microbial PBP and early version of an acetyl choline sensor (iAChSnFR), the scientists used machine learning and modeling to redesign the binding site to exhibit a higher affinity and specificity to serotonin. After three repeats of mutagenesis, modeling, and library readouts, they produced iSeroSnFR. This version harbors 19 mutations compared to iAChSnFR0.6 and a Kd of 310 µM. This results in an increase in fluorescence in HEK293T cells expressing the serotonin receptor of 800%. Of over 40 neurotransmitters, amino acids, and small molecules screened, only two endogenous molecules evoked some fluorescence, but at significantly higher concentrations.
To acutely test the ability of the sensor to detect rapid changes of serotonin in the environment, the researchers used caged serotonin, a technique in which the serotonin is rapidly released into the environment with light pulses, and showed that iSeroSnFR accurately and robustly produced a signal with each flash of light. With this tool, it was then possible to move to ex-vivo mouse brain slices and detect endogenous serotonin release patterns across the brain. Three weeks after targeted injection of iSeroSnFR to specifically deliver the receptor into the prefrontal cortex and dorsal striatum, strong fluorescent signal could be detected during perfusion of serotonin or electrical stimulation.
Most significantly, this molecule was also shown to be detected in freely moving mice, a tool which could offer critical insight into the acute role of serotonin regulation during important functions such as mood and alertness. Through optical fiber placements in the basolateral amygdala and prefrontal cortex, the team measured dynamic and real-time changes in serotonin release in fear-trained mice, social interactions, and sleep wake cycles. For example, while both areas of the brain have been established as relevant to the fear response, they reliably tracked that the PFC response was immediate, while the BSA displayed a delayed response. This additional temporal resolution of neuromodulation may have important implications in neurotransmitter pharmacology of the central nervous system.
This study provided the scientific community with several insights and tools. The serotonin sensor itself will be a critical tool in the study of the central nervous system and possibly beyond. Additionally, an AI approach to mutagenesis in order to redesign a binding pocket of a receptor opens new avenues to the development of pharmacological tools and may lead to many new designs in therapeutics and research.
Connecting the Immune Response to Amyloid-β Aggregation in Alzheimer’s Disease via IFITM3
Reporter : Irina Robu, PhD
Alzheimer’s disease is a complex condition and it begins with slow aggregation of amyloid-β deposits over the course of years. This produces a mild cognitive impairment and a state of chronic inflammation enough to trigger harmful aggregation of the altered tau protein. Clearing amyloid-β from the brain hasn’t produced telling benefits to patients suggesting that it is not the key process in the development of the condition.
Recent research indicates that beta-amyloid has antiviral and antimicrobial properties, indicating a possible link between the immune response against infections and development of Alzheimer’s disease. Scientists have discovered evidence that protein interferon-induced transmembrane protein 3 (IFITM3) is involved in immune response to pathogens and play a key role in the accumulation of beta amyloid in plaques. IFITM3 is able to alter the activity of gamma-secretase enzyme, which breaks down the precursor proteins into fragments of beta-amyloid that make up plaques.
Yet it was determined that the production of IFITM3 starts in reply to activation of the immune system by invading viruses and bacteria. Indeed, researchers found that the level of IFITM3 in human brain samples correlated with levels of certain viral infections as well as with gamma-secretase activity and beta-amyloid production. Age is the number one risk factor for Alzheimer’s and the levels of both inflammatory markers and IFITM3 increased with advancing age in mice.
Innate immunity is also correlated with Alzheimer’s disease1, but the influence of immune activation on the production of amyloid beta is unknown. They were able to identify IFITM3 as γ-secretase modulatory protein, and establish a mechanism by which inflammation affects the generation of amyloid-β.
According to the current research, inflammatory cytokines induce the expression of IFITM3 in neurons and astrocytes, which binds to γ-secretase and upregulates its activity, thereby increasing the production of amyloid-β. The expression of IFITM3 is increased with ageing and in mouse models that express Alzheimer’s disease genes. IFITM3 protein is upregulated in tissue samples from a subset of patients with late-onset Alzheimer’s disease that exhibit higher γ-secretase activity. The amount of IFITM3 in the γ-secretase complex has a strong and positive correlation with γ-secretase activity in samples from patients with late-onset Alzheimer’s disease. These conclusions disclose a mechanism in which γ-secretase is controlled by neuroinflammation via IFITM3 and the risk of Alzheimer’s disease is thus amplified