Dr. Cambria:
An aortic aneurysm can be most simply thoughts of as a weakening or ballooning of the aorta which is the body’s major and largest blood vessel. That’s important because this ballooning or weakening can eventually lead to the aneurysm bursting, which is usually a fatal event.
Aneurysms have been referred to as the ‘silent killer’ because in most cases these aortic aneurysms cause no symptoms or problems prior to bursting. Most aortic aneurysms occur in older patients, but there are a clearly defined set of risk factors which makes certain patients at higher risk of developing aortic aneurysms. These include, most importantly, a family history of aortic aneurysm disease, and by family history I mean, if your mother or father or a brother or sister had an aortic aneurysm, you are clearly at increased risk of developing an aneurysm.
20% of the patients that we treat for aortic aneurysms have a positive family history of aneurysm disease. You are also at higher risk for developing an aortic aneurysm if you are female, if you have a history of high blood pressure, if you have been a cigarette smoker, and if you have chronic obstructive pulmonary disease or emphysema, which is in turn related to long-term cigarette smoking.
If you are at risk for developing an aortic aneurysm there are simple diagnostic x-ray studies such as ultrasounds and CAT scans to accurately diagnose number one, whether or not an aneurysm is present, and more importantly, if it is present, to measure just how large it is because that’s the single most important factor in determining whether or not your aneurysm needs to be treated.
It’s important to detect and monitor aortic aneurysms before they reach the stage of bursting because treatment is then usually successful with an expected excellent recovery. Treatment of aortic aneurysms today is very effective and involves replacing the aneurysm with an artificial blood vessel.
There are a variety of different surgical treatments, some of them including minimally invasive operations known as stent grafts, which are applied today in many patients.
Mass General has been a leader in the northeast in the successful management of aortic aneurysms. More than a decade ago, we formed the Mass General Thoracic Aortic Center, which is a team-approach of vascular surgeons, cardiac or heart surgeons, and cardiologists to effectively manage thoracic aneurysms which are often the most challenging and clinically complex to treat.
About Dr. Richard Paul Cambria, M.D.:
Richard P. Cambria, M.D. is Professor of Surgery at Harvard Medical School and Chief, Division of Vascular/Endovascular Surgery at Massachusetts General Hospital. Dr. Cambria received his medical degree from the College of Physicians and Surgeons, Columbia University, in 1977. He trained in general and vascular surgery at Massachusetts General Hospital.
http://www.empowher.com/aortic-aneurysm/content/there-are-no-early-symptoms-there-way-know-if-i-have-aortic-aneurysm-it-rupt
Education & Awards
Dr. Cambria graduated from Columbia University, New York. He has 15 awards.
| Awards |
|
|
One of America’s Leading Experts on: |
|
|
Abdominal Aortic Aneurysm |
|
|
Aortic Aneurysm |
|
|
Aortic Diseases |
|
|
Aortic Rupture |
|
|
Arterial Occlusive Diseases |
|
|
Blood Vessel Prosthesis Implantation |
|
|
Carotid Endarterectomy |
|
|
Carotid Stenosis |
|
|
Kidney Failure |
|
|
Mesenteric Vascular Occlusion |
|
|
Spinal Cord Ischemia |
|
|
Thoracic Aortic Aneurysm |
|
|
Vascular Surgical Procedures |
|
|
|
|
|
Top Ten Doctors (2012) |
|
|
Vascular Surgery, Downtown, Boston, MA |
|
http://www.vitals.com/doctors/Dr_Richard_Cambria.html#ixzz2VqxwIwMK
Publications & Research
| Dr. Cambria has contributed to 164 publications. |
| Title |
Giant Cell Aortitis of the Ascending Aorta Without Signs or Symptoms of Systemic Vasculitis is Associated with Elevated Risk of Distal Aortic Events. |
| Date |
February 2012 |
| Journal |
Arthritis and Rheumatism |
|
| Title |
Long-term Outcomes of Patients Undergoing Endovascular Infrainguinal Interventions with Single-vessel Peroneal Artery Runoff. |
| Date |
May 2011 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Management of Diseases of the Descending Thoracic Aorta in the Endovascular Era: a Medicare Population Study. |
| Date |
October 2010 |
| Journal |
Annals of Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
The Effects of Systemic Hypothermia on a Murine Model of Thoracic Aortic Ischemia Reperfusion. |
| Date |
August 2010 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Long-term Outcomes of Diabetic Patients Undergoing Endovascular Infrainguinal Interventions. |
| Date |
August 2010 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Preoperative Variables Predict Persistent Type 2 Endoleak After Endovascular Aneurysm Repair. |
| Date |
August 2010 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Surgical Management of Descending Thoracic Aortic Disease: Open and Endovascular Approaches: a Scientific Statement from the American Heart Association. |
| Date |
August 2010 |
| Journal |
Circulation |
|
| Title |
Balloon Expandable Stents Facilitate Right Renal Artery Reconstruction During Complex Open Aortic Aneurysm Repair. |
| Date |
March 2010 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Preoperative Functional Status Predicts Perioperative Outcomes After Infrainguinal Bypass Surgery. |
| Date |
March 2010 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Intermediate-term Outcomes of Endovascular Treatment for Symptomatic Chronic Mesenteric Ischemia. |
| Date |
February 2010 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
A Multicenter Clinical Trial of Endovascular Stent Graft Repair of Acute Catastrophes of the Descending Thoracic Aorta. |
| Date |
December 2009 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Effect of Pj34 on Spinal Cord Tissue Viability and Gene Expression in a Murine Model of Thoracic Aortic Reperfusion Injury. |
| Date |
December 2009 |
| Journal |
Vascular and Endovascular Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Secondary Intervention After Endovascular Abdominal Aortic Aneurysm Repair. |
| Date |
October 2009 |
| Journal |
Annals of Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Aortic Remodeling After Endovascular Repair of Acute Complicated Type B Aortic Dissection. |
| Date |
September 2009 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Significant Perioperative Morbidity Accompanies Contemporary Infrainguinal Bypass Surgery: an Nsqip Report. |
| Date |
September 2009 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Pj34, a Poly-adp-ribose Polymerase Inhibitor, Modulates Visceral Mitochondrial Activity and Cd14 Expression Following Thoracic Aortic Ischemia-reperfusion. |
| Date |
August 2009 |
| Journal |
American Journal of Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Thoracoabdominal Aneurysm Repair: Hybrid Versus Open Repair. |
| Date |
July 2009 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Successful Use of Bivalirudin for Combined Carotid Endarterectomy and Coronary Revascularization with the Use of Cardiopulmonary Bypass in a Patient with an Elevated Heparin-platelet Factor 4 Antibody Titer. |
| Date |
April 2009 |
| Journal |
Anesthesia and Analgesia |
| Excerpt |
Read excerpt
|
|
| Title |
Atherosclerotic Peripheral Vascular Disease Symposium Ii: Controversies in Carotid Artery Revascularization. |
| Date |
January 2009 |
| Journal |
Circulation |
|
| Title |
Functional Outcome After Thoracoabdominal Aneurysm Repair. |
| Date |
December 2008 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Outcomes Following Endovascular Abdominal Aortic Aneurysm Repair (evar): an Anatomic and Device-specific Analysis. |
| Date |
August 2008 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Zenith Abdominal Aortic Aneurysm Endovascular Graft. |
| Date |
August 2008 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Spinal Cord Complications After Thoracic Aortic Surgery: Long-term Survival and Functional Status Varies with Deficit Severity. |
| Date |
August 2008 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Five-year Results of Endovascular Treatment with the Gore Tag Device Compared with Open Repair of Thoracic Aortic Aneurysms. |
| Date |
June 2008 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Aortic Aneurysms. |
| Date |
May 2008 |
| Journal |
Journal of the American College of Radiology : Jacr |
|
| Title |
International Controlled Clinical Trial of Thoracic Endovascular Aneurysm Repair with the Zenith Tx2 Endovascular Graft: 1-year Results. |
| Date |
March 2008 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Contemporary Management of Descending Thoracic and Thoracoabdominal Aortic Aneurysms: Endovascular Versus Open. |
| Date |
February 2008 |
| Journal |
Circulation |
|
| Title |
Contemporary Management of Carotid Stenosis: Carotid Endarterectomy is Here to Stay. |
| Date |
January 2008 |
| Journal |
Perspectives in Vascular Surgery and Endovascular Therapy |
| Excerpt |
Read excerpt
|
|
| Title |
Long-term Durability of Open Abdominal Aortic Aneurysm Repair. |
| Date |
November 2007 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Commentary On: Mas Jl, Chatellier G, Beyssen B, Et Al. Endarterectomy Versus Stenting in Patients with Symptomatic Severe Carotid Stenosis. N Engl J Med. 2006;355:1660-1671. |
| Date |
November 2007 |
| Journal |
Perspectives in Vascular Surgery and Endovascular Therapy |
| Excerpt |
Read excerpt
|
|
| Title |
Defining the High-risk Patient for Carotid Endarterectomy: an Analysis of the Prospective National Surgical Quality Improvement Program Database. |
| Date |
October 2007 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Persistent Type 2 Endoleak After Endovascular Repair of Abdominal Aortic Aneurysm is Associated with Adverse Late Outcomes. |
| Date |
July 2007 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Restenosis After Eversion Vs Patch Closure Carotid Endarterectomy. |
| Date |
July 2007 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Surgical Revascularization Versus Endovascular Therapy for Chronic Mesenteric Ischemia: a Comparative Experience. |
| Date |
July 2007 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Comparison of Risk-adjusted 30-day Postoperative Mortality and Morbidity in Department of Veterans Affairs Hospitals and Selected University Medical Centers: Vascular Surgical Operations in Men. |
| Date |
July 2007 |
| Journal |
Journal of the American College of Surgeons |
| Excerpt |
Read excerpt
|
|
| Title |
Thoracoabdominal Aneurysm Repair: a 20-year Perspective. |
| Date |
March 2007 |
| Journal |
The Annals of Thoracic Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Stent-graft Versus Open-surgical Repair of the Thoracic Aorta: Mid-term Results. |
| Date |
January 2007 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Intermediate Results of Percutaneous Endovascular Therapy of Femoropopliteal Occlusive Disease: a Contemporary Series. |
| Date |
October 2006 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Long-term Outcomes After Endovascular Abdominal Aortic Aneurysm Repair: the First Decade. |
| Date |
October 2006 |
| Journal |
Annals of Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Poly Adenosine Diphosphate-ribose Polymerase Inhibitor Pj34 Abolishes Systemic Proinflammatory Responses to Thoracic Aortic Ischemia and Reperfusion. |
| Date |
August 2006 |
| Journal |
Journal of the American College of Surgeons |
| Excerpt |
Read excerpt
|
|
| Title |
Contemporary Results of Open Surgical Repair of Descending Thoracic Aortic Aneurysms. |
| Date |
August 2006 |
| Journal |
Seminars in Vascular Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Commentary on “extra-anatomic Visceral Revascularization and Endovascular Stent-grafting for Complex Thoracoabdominal Aortic Lesions”. |
| Date |
May 2006 |
| Journal |
Perspectives in Vascular Surgery and Endovascular Therapy |
|
| Title |
Multi-institutional Pivotal Trial of the Zenith Tx2 Thoracic Aortic Stent-graft for Treatment of Descending Thoracic Aortic Aneurysms: Clinical Study Design. |
| Date |
May 2006 |
| Journal |
Perspectives in Vascular Surgery and Endovascular Therapy |
| Excerpt |
Read excerpt
|
|
| Title |
Aortic Dissection: Perspectives in the Era of Stent-graft Repair. |
| Date |
March 2006 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
|
| Title |
Current Results of Open Surgical Repair of Descending Thoracic Aortic Aneurysms. |
| Date |
March 2006 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
|
| Title |
Late Results of Combined Carotid and Coronary Surgery Using Actual Versus Actuarial Methodology. |
| Date |
December 2005 |
| Journal |
The Annals of Thoracic Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Contemporary Results of Angioplasty-based Infrainguinal Percutaneous Interventions. |
| Date |
November 2005 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Pj34, a Poly-adp-ribose Polymerase Inhibitor, Modulates Renal Injury After Thoracic Aortic Ischemia/reperfusion. |
| Date |
October 2005 |
| Journal |
Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Safety and Efficacy of Reoperative Carotid Endarterectomy: a 14-year Experience. |
| Date |
July 2005 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Determinants of Carotid Endarterectomy Anatomic Durability: Effects of Serum Lipids and Lipid-lowering Drugs. |
| Date |
May 2005 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Early Outcomes of Endovascular Versus Open Abdominal Aortic Aneurysm Repair in the National Surgical Quality Improvement Program-private Sector (nsqip-ps). |
| Date |
May 2005 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Thoracoabdominal Aneurysm Repair: Anesthetic Management. |
| Date |
March 2005 |
| Journal |
International Anesthesiology Clinics |
|
| Title |
Endovascular Treatment of Thoracic Aortic Aneurysms: Results of the Phase Ii Multicenter Trial of the Gore Tag Thoracic Endoprosthesis. |
| Date |
March 2005 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Poly(adenosine Diphosphate Ribose) Polymerase Inhibition Modulates Spinal Cord Dysfunction After Thoracoabdominal Aortic Ischemia-reperfusion. |
| Date |
March 2005 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Current Status of Thoracoabdominal Aneurysm Repair. |
| Date |
November 2004 |
| Journal |
Advances in Surgery |
|
| Title |
Stenting for Carotid-artery Stenosis. |
| Date |
October 2004 |
| Journal |
The New England Journal of Medicine |
|
| Title |
Carotid Endarterectomy at the Millennium: What Interventional Therapy Must Match. |
| Date |
September 2004 |
| Journal |
Annals of Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Surgical Management of Popliteal Artery Embolism at the Turn of the Millennium. |
| Date |
June 2004 |
| Journal |
Annals of Vascular Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Regional Hypothermia with Epidural Cooling for Prevention of Spinal Cord Ischemic Complications After Thoracoabdominal Aortic Surgery. |
| Date |
April 2004 |
| Journal |
Seminars in Thoracic and Cardiovascular Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Preservation of Renal Function with Surgical Revascularization in Patients with Atherosclerotic Renovascular Disease. |
| Date |
February 2004 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Durability of Aortouniiliac Endografting with Femorofemoral Crossover: 4-year Experience in the Evt/guidant Trials. |
| Date |
June 2003 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Late Aortic and Graft-related Events After Thoracoabdominal Aneurysm Repair. |
| Date |
February 2003 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Surgical Treatment of Complicated Distal Aortic Dissection. |
| Date |
October 2002 |
| Journal |
Seminars in Vascular Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Thoracoabdominal Aneurysm Repair: Results with 337 Operations Performed over a 15-year Interval. |
| Date |
October 2002 |
| Journal |
Annals of Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Clinical Outcome of Internal Iliac Artery Occlusions During Endovascular Treatment of Aortoiliac Aneurysmal Diseases. |
| Date |
October 2002 |
| Journal |
Journal of Vascular and Interventional Radiology : Jvir |
| Excerpt |
Read excerpt
|
|
| Title |
Evolving Experience with Thoracic Aortic Stent Graft Repair. |
| Date |
July 2002 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Clinical Failures of Endovascular Abdominal Aortic Aneurysm Repair: Incidence, Causes, and Management. |
| Date |
July 2002 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Regarding “analysis of Predictive Factors for Progression of Type B Aortic Intramural Hematoma with Computed Tomography”. |
| Date |
July 2002 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
|
| Title |
Contemporary Management of Aortic Branch Compromise Resulting from Acute Aortic Dissection. |
| Date |
July 2001 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Endovascular Stent-graft in Abdominal Aortic Aneurysms: the Relationship Between Patent Vessels That Arise from the Aneurysmal Sac and Early Endoleak. |
| Date |
June 2001 |
| Journal |
Radiology |
| Excerpt |
Read excerpt
|
|
| Title |
Regional Hypothermia with Epidural Cooling for Spinal Cord Protection During Thoracoabdominal Aneurysm Repair. |
| Date |
April 2001 |
| Journal |
Seminars in Vascular Surgery |
| Excerpt |
Read excerpt
|
|
| Title |
Endovascular Repair of Abdominal Aortic Aneurysms: Current Status and Future Directions. |
| Date |
August 2000 |
| Journal |
Ajr. American Journal of Roentgenology |
|
| Title |
Epidural Cooling for Spinal Cord Protection During Thoracoabdominal Aneurysm Repair: A Five-year Experience. |
| Date |
July 2000 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Utility and Reliability of Endovascular Aortouniiliac with Femorofemoral Crossover Graft for Aortoiliac Aneurysmal Disease. |
| Date |
July 2000 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
| Title |
Surgical Renal Artery Reconstruction Without Contrast Arteriography: the Role of Clinical Profiling and Magnetic Resonance Angiography. |
| Date |
January 2000 |
| Journal |
Journal of Vascular Surgery : Official Publication, the Society for Vascular Surgery [and] International Society for Cardiovascular Surgery, North American Chapter |
| Excerpt |
Read excerpt
|
|
http://www.vitals.com/doctors/Dr_Richard_Cambria/credentials
http://www.vitals.com/doctors/Dr_Richard_Cambria/credentials#ixzz2VqyhFZVd
Cambria RP, Brewster DC, Lauterbach SR, Kaufman JA, Geller SC, Fan CM, Greenfield A, Hilgenberg A, Clouse WD. Evolving experience with thoracic aortic stent-graft repair. J Vasc Surg 2002:35:1129-36.
Cambria, RP, Clouse WD, Davison JK, Dunn PF, Corey M, Dorer D. Thoracoabdominal aneurysm repair: Results with 337 operations performed over a 15 year interval. Ann Surg 2002;236-471-79.
Cambria RP, Lauterbach SR, Brewster DC, Gertler JP, LaMuraglia GM, Isselbacher EM, Hilgenberg AD, Moncure AC. Contemporary management of aortic branch compromise secondary to acute aortic dissections. J Vasc Surg 2001;331185-92.
Cambria RP and Black JH. Aortic dissection perspectives for the vascular/endovascular surgeon. In Rutherford (ed) Comprehensive Vascular and Endovascular Surgery 6 th , W. B. Saunders, Inc. (in press, 2004).
Cambria RP, Marone LK, Cloud WD, Dorer, DJ, Brewster, DC, LaMuraglia, GM, Watkins, MT, Kwolek, CJ. Preservation of renal functions with surgical revascularization in patients with atherosclerotic renovascular disease. J Vasc Surg 2004; 10.023.
Abdominal Aortic Aneurysm – Case Study
by
Angela Rodriguez-Wong, MD, RVT, RPVI
Lois Eliassi, BS, RVT
http://www.navixdiagnostix.com/downloads/Navix%20-%20Q1%20’13%20Ultrasound%20Solutions.pdf
An aneurysm is defined as a focally dilated segment of an artery that is 1.5 times its normal diameter and involves all three arterial walls (intima, media and adventitia). Aneurysms can be found in the common femoral and popliteal arteries in the lower extremities, the splenic, mesenteric, and renal arteries in the abdomen, and also in the intracranial vessels. However, the most common is an abdominal aortic aneurysm (AAA) involving the aorta and iliac arteries.
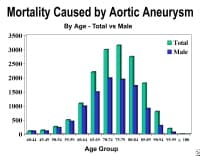
Abdominal aortic aneurysms are generally asymptomatic and are discovered accidentally either by physician palpation or by a radiologic examination such as a chest or abdominal X-ray. The risk factors that increase the probability of developing a AAA are primarily smoking and family history. An abdominal aortic aneurysm can rupture and, according to the Centers for Disease Control and Prevention, ruptured AAA was the 10th leading cause of death in males between the ages of 65-74 in the United States in 2000.
The preferred method of screening for AAA is diagnostic ultrasound. According to the Journal of Vascular Surgery, diagnostic ultrasound performed by a registered vascular technologist has a sensitivity of 100 percent and a specificity of 96 percent for the detection of an infrarenal AAA. The abdominal aorta is considered aneurysmal when it measures >3.0 cm.
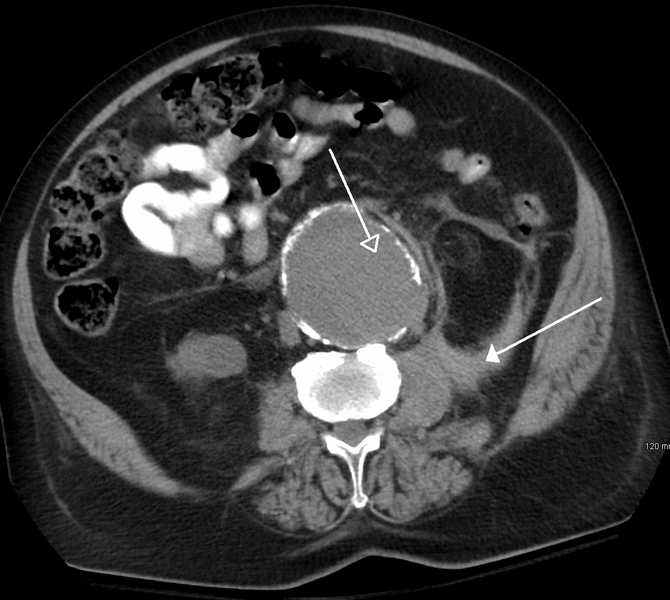
Because of its accuracy, diagnostic ultrasound not only has become an integral part in diagnosing AAA but is also an integral part in the evaluation of disease progression, the preoperative AAA evaluation, and the follow-up of AAA surgical repair. It is important to note that a rupture of an AAA is a surgical emergency and is difficult to evaluate with ultrasound due to the inability to easily demonstrate abdominal free fluid. If a rupture is suspected, it is recommended that other imaging modalities such as CT be employed to better demonstrate the ruptured aneurysm and any intra-abdominal free fluid.
Case Study –
Abdominal Aortic Aneurysm – A 77 year-old male
Angela Rodriguez-Wong, MD, RVT, RPVI
Lois Eliassi, BS, RVT
Figure 1 Distal abdominal aortic aneurysm with mural thrombus.

Figure 2 Bifurcation of the aorta.

Case Study: A 77 year-old male with a past medical history of diabetes, hypertension, arthritis, aortic valve disease and heavy smoking was referred to Eastern Vascular Diagnostic Center with a 4.2 centimeter aneurysm. The patient denied any family history of aneurysm and is allergic to intravenous contrast. A physical exam found the patient alert with a blood pressure of 100/60 mmHg, a pulse of 58 and respiration of 16. Auscultation found a bruit in the left carotid artery, clear lungs, and a regular heart rhythm with an aortic systolic murmur. The patient had a well healed sub-costal incision on his abdomen. The physician was unable to palpate the aneurysms. The patient had an aortic valve replacement in 2007 and also a cholecystectomy. On May 12, 2012, a magnetic resonance imaging (MRI) scan without contrast was performed on the patient’s abdomen. The MRI found an AAA measuring greater than 3 cm with extensive plaque near the bifurcation. The aneurysm extended into the right common iliac artery (CIA) measuring 4.2 cm and into the left CIA measuring 3.1 cm. The MRI exam did not include the pelvis, so the extent of the iliac aneurysms was not clear. On July 31, 2012, the ultrasound was performed, demonstrating normal ankle brachial index (right-1.2, left-1.1) and a AAA measuring 3.9 cm which extended into the right and left CIA. The maximum diameter of the right CIA measures 4.1 cm with mural thrombus creating a residual lumen of 2.0 cm. The maximum diameter of the left CIA measures 4.3 cm, there is also mural thrombus noted but without significant appreciable diameter reduction within the vessel. A computed tomography (CT) scan of the abdomen and pelvis without contrast was performed on July 18th confirming the infrarenal AAA with extension into the iliac arteries bilaterally.
Surgery is recommended when an AAA reaches 5.0-5.5 cm in a male and 4.5-5.0 cm in females. Surgery, depending on the aneurysm, can be an open repair or an endovascular repair. In this patient, despite the size of the AAA being 4.1 cm, the disease also involved the bilateral common iliacs prompting the need for surgical intervention. The patient was cleared by cardiology and on July 31st had an AAA and bilateral Iliac aneurysm resection with a re-implantation of the inferior mesenteric artery and an Aorta to right Hypogastric bypass to maintain pelvic perfusion.
The U.S. Preventive Services Task Force has released a statement summarizing recommendations for screening for AAA. It states that screening benefits patients who have a relatively high risk for dying from an aneurysm; major risk factors are age 65 years or older, male sex, and smoking at least 100 cigarettes in a lifetime. The guideline recommends one-time screening with ultrasound for AAA in men 65 to 75 years of age who have ever smoked. No recommendation was made for or against screening in men 65 to 75 years of age who have never smoked, and it recommended against screening women. Men with a strong family history of AAA should be counseled about the risks and benefits of screening as they approach 65 years of age.
Angela Rodriguez-Wong, MD, RVT, RPVI
awong@navixdiagnostix.com
Lois Eliassi, BS, RVT
leliassi@navixdiagnostix.com
Figure 3 Sagittal image of the right common iliac artery demonstrating the measurement of the aneurysm and the true lumen.

Figure 4 Coronal view of the left common iliac artery.

REFERENCES
1. Anderson RN. Deaths: Leading causes for 2000. Natl Vital Stat Rep. 2002;50:1–85.
2. Kent KC, Zwolak RM, Jaff MR, et al. Screening for abdominal aortic aneurysm. J Vasc Surg. 2004;39:267–9.
3. Upchurch G Jr, Schaub T. Abdominal aortic aneurysm. American Family Physician. 2006;73(7), 1198-1204. http://www.aafp.org/afp/2006/0401/p1198.html
http://www.navixdiagnostix.com/downloads/Navix%20-%20Q1%20’13%20Ultrasound%20Solutions.pdf


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}