Open Abdominal Aortic Aneurysm (AAA) repair (OAR) vs. Endovascular AAA Repair (EVAR) in Chronic Kidney Disease (CKD) Patients – Comparison of Surgery Outcomes
Writer and Curator: Larry H. Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN
This is a review of the effects of CKD on increased morbidity and mortality of abdominal aortic aneurysm repair. The abdominal aorta has branches to the superior mesenteric arteries proximally, and below that both renal arteries, which also supply the adrenals (suprarenal).
Severe atherosclerosis with plaque buildup and separation of the media from the endothelium, can migrate down the addominal aorta before frank rupture of an aneurysm. Abdominal aortic aneurysm often extends from below the the renal arteries, to the internal spermatic vessels, or as far as the iliacs.


Of the visceral branches, the celiac artery and the superior and inferior mesenteric arteries are unpaired, while the suprarenals, renals, internal spermatics, and ovarian are paired. Of the parietal branches the inferior phrenics and lumbars are paired; the middle sacral is unpaired. The terminal branches are paired.
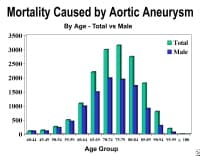
AAA is most common in men over age 65 years. If it is expanding AAA causes sudden, severe, and constant low back, flank, abdominal, or groin pain (internal spermatic branch). The presence of a pulsatile abdominal mass is virtually diagnostic but is found in less than half of all cases. At least 65% of patients with a ruptured AAA die from sudden cardiovascular collapse before arriving at a hospital.
EVAR for ruptured AAA
A study by Mehta et al assessed the effect of hemodynamic status on outcomes in 136 patients undergoing EVAR for ruptured AAAs.[1] The patients were divided into 2 groups:
(1) Hd-stable (systolic BP ≥80 mm Hg; n = 92 [68%]) and
(2) Hd-unstable (systolic BP < 80 mm Hg for >10 minutes; n = 44 [32%]).
(2) Hd-unstable (systolic BP < 80 mm Hg for >10 minutes; n = 44 [32%]).
The 30-day mortality, postoperative complications, need for secondary reinterventions, and midterm mortality were recorded. The 2 groups were found to be similar with respect to
- comorbidities,
- mean AAA maximum diameter (6.6 vs 6.4 cm),
- need for on-the-table conversion to open repair (3% vs 7%), and
- incidence of nonfatal complications (43% vs 38%) and secondary interventions (23% vs 25%).
- intraoperative need for aortic occlusion balloon,
- mean estimated blood loss,
- incidence of developing abdominal compartment syndrome (ACS), and
- mortality
were all increased in the Hd-unstable group ([1]40% vs 6%, [2]744 vs 363 mL,[3] 29% vs 4%, and [4]33% vs 18%, respectively).
Open Surgery
Requires direct access to the aorta through an abdominal or retroperitoneal approach
Endovascular: Involves gaining access to the lumen of the abdominal aorta, usually via small incisions over the femoral vessels; an endograft, typically a cloth graft with a stent exoskeleton, is placed within the lumen of the AAA, extending distally into the iliac arteries. Approximately 90% of abdominal aortic aneurysms are infrarenal.
The important surgical and endovascular anatomic considerations include associated renal and visceral artery involvement (either occlusive disease or involved in the aneurysm process) and the iliac artery (either occlusive disease or aneurysms). The length of the infrarenal aortic neck is important in helping determine the surgical approach (retroperitoneal vs transabdominal) and the location of the aortic cross clamp.
Endovascular Aneurysm Repair
Endovascular repair first became practical in the 1990s and although it is now an established alternative to open repair, its role is yet to be clearly defined. It is generally indicated in older, high-risk patients or patients unfit for open repair. However, endovascular repair is feasible for only a proportion of AAAs, depending on the morphology of the aneurysm. The main advantages over open repair are that there is less peri-operative mortality, less time in intensive care, less time in hospital overall and earlier return to normal activity. Disadvantages of endovascular repair include a requirement for more frequent ongoing hospital reviews, and a higher chance of further procedures being required. According to the latest studies, the EVAR procedure does not offer any benefit for overall survival or health-related quality of life compared to open surgery, although aneurysm-related mortality is lower.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Aorta Anatomy and Pathology in AAA
The diameter of the aorta decreases in size from its thoracic portion to the abdominal and infrarenal portions. A normal aorta shows a reduction in medial elastin layers from the thoracic area to the abdominal portion. Elastin and collagen content are also reduced. AAAs develop following degeneration of the media. The degeneration ultimately may lead to widening of the vessel lumen and loss of structural integrity.
A multidisciplinary research program supported by the US National Heart, Lung, and Blood Institute identified proteolytic degradation of aortic wall connective tissue, inflammation and immune responses, biomechanical wall stress, and molecular genetics as mechanisms important in the development of AAA. Similarly, surgical specimens of AAA reveal inflammation, with infiltration by lymphocytes and macrophages; thinning of the media; and marked loss of elastin.
Through gene microarray analysis, various genes involved in extracellular matrix degradation, inflammation, and other processes observed in AAA formation have been shown to be up-regulated, while others that may serve to prevent this occurrence are down-regulated. The combination of proteolytic degradation of aortic wall connective tissue, inflammation and immune responses, biomechanical wall stress, and molecular genetics represents a dynamic process that leads to aneurysmal deterioration of aortic tissue.
{kind=link}

1. Mehta M, Paty PS, Byrne J, Roddy SP, Taggert JB, Sternbach Y, et al. The impact of hemodynamic status on outcomes of endovascular abdominal aortic aneurysm repair for rupture. J Vasc Surg. May 2013;57(5):1255-60. [Medline].
2. Blanchard JF, Armenian HK, Friesen PP. Risk factors for abdominal aortic aneurysm: results of a case-control study. Am J Epidemiol. Mar 15 2000;151(6):575-83. [Medline].
3. Lederle FA, Johnson GR, Wilson SE, Chute EP, Littooy FN, Bandyk D, et al. Prevalence and associations of abdominal aortic aneurysm detected through screening. Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Ann Intern Med. Mar 15 1997;126(6):441-9. [Medline].
4. Wassef M, Baxter BT, Chisholm RL, Dalman RL, Fillinger MF, Heinecke J, et al. Pathogenesis of abdominal aortic aneurysms: a multidisciplinary research program supported by the National Heart, Lung, and Blood Institute. J Vasc Surg. Oct 2001;34(4):730-8. [Medline].
5. [Guideline] U.S. Preventive Services Task Force. Screening for abdominal aortic aneurysm: recommendation statement. Ann Intern Med. Feb 1 2005;142(3):198-202. [Medline]. [Full Text].
Impact of chronic kidney disease on outcomes after abdominal aortic aneurysm repair
Patel VI, Lancaster RT, Mukhopadhyay S, Aranson NJ, Conrad MF, et al.
J Vasc Surg. 2012 Nov;56(5):1206-13. http://dx.doi.org/10.1016/j.jvs.2012.04.037. Epub 2012 Aug 1.
Chronic kidney disease (CKD) is associated with increased morbidity and death after open abdominal aortic aneurysm (AAA) repair (OAR). This study highlights the effect of CKD on outcomes after endovascular AAA (EVAR) and OAR in contemporary practice.
The National Surgical Quality Improvement Program (NSQIP) Participant Use File (2005-2008) was queried by Current Procedural Terminology (American Medical Association, Chicago, Ill) code to identify EVAR or OAR patients, who were grouped by CKD class as having mild (CKD class 1 or 2), moderate (CKD class 3), or severe (CKD class 4 or 5) renal disease. Propensity score analysis was performed to match OAR and EVAR patients with mild CKD with those with moderate or severe CKD. Comparative analysis of mortality and clinical outcomes was performed based on CKD strata.
We identified 8701 patients who were treated with EVAR (n = 5811) or OAR (n = 2890) of intact AAAs. Mild, moderate, and severe CKD was present in 63%, 30%, and 7%, respectively. CKD increased (P < .01) overall mortality, with rates of 1.7% (mild), 5.3% (moderate), and 7.7% (severe) in unmatched patients undergoing EVAR or OAR. Operative mortality rates in patients with severe CKD were as high as 6.2% for EVAR and 10.3% for OAR.
Severity of CKD was associated with increasing frequency of risk factors; therefore, propensity matching to control for comorbidities was performed, resulting in similar baseline clinical and demographic features of patients with mild compared with those with moderate or severe disease.
In propensity-matched cohorts, moderate CKD increased the risk of 30-day mortality
- for EVAR (1.9% mild vs 3.2% moderate; P = .013) and
- OAR (3.1% mild vs 8.4% moderate; P < .0001).
Moderate CKD was also associated with increased morbidity in patients treated with
- EVAR (8.3% mild vs 12.8% moderate; P < .0001) or
- OAR (25.2% mild vs 32.4% moderate; P = .001).
Similarly, severe CKD increased the risk of 30-day mortality
- for EVAR (2.6% mild vs 5.7% severe; P = .0081) and
- OAR (4.1% mild vs 9.9% severe; P = .0057).
Severe CKD was also associated with increased morbidity in patients treated with
- EVAR (10.6% mild vs 19.2% severe; P < .0001) or
- OAR (31.1% mild vs 39.6% severe; P = .04).
The presence of moderate or severe CKD in patients considered for AAA repair is associated with significantly increased mortality and therefore should figure prominently in clinical decision making. The high mortality of AAA repair in patients with severe CKD is such that elective repair in such patients is not advised, except in extenuating clinical circumstances.
Related articles
- Elective Open Suprarenal Aneurysm Repair in England from 2000 to 2010 an Observational Study of Hospital Episode Statistics (plosone.org)
- The EVAR I trial: Endovascular vs. open abdominal aortic aneurysm repair [Classics Series] (2minutemedicine.com)
- Abdominal Aortic Aneurysm Genetic Risk (23andme.com)
- The EVAR II trial: Endovascular approach when unfit for open aortic aneurysm repair [Classics Series] (2minutemedicine.com)
- Red Vascular Branch Endograft System: Aortic Aneursysm (proteinbreak.wordpress.com)
Related articles published on this Open Access Online Scientific Journal
Effect of Hospital Characteristics on Outcomes of Endovascular Repair of Descending Aortic Aneurysms in US Medicare Population
Larry H. Bernstein, MD, FCAP
Abdominal Aortic Aneurysms (AAA): Albert Einstein’s Operation by Dr. Nissen
Aviva Lev-Ari, PhD, RN
No Early Symptoms – An Aortic Aneurysm Before It Ruptures – Is There A Way To Know If I Have it?
Justin D Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
First-of-Its-Kind FDA Approval for ‘AUI’ Device with Endurant II AAA Stent Graft: Medtronic Expands in Endovascular Aortic Repair in the United States
Aviva Lev-Ari, PhD, RN
Abdominal Aortic Aneurysm: Endovascular repair and open repair resulted in similar long-term survival
Aviva Lev-Ari, PhD, RN
EUROPCR 2013, Paris 5/21-5/24, 2013 Conference for Cardiolovascular Intervention and Interventional Medicine
Aviva Lev-Ari, PhD, RN
Genomics & Genetics of Cardiovascular Disease Diagnoses: A Literature Survey of AHA’s Circulation Cardiovascular Genetics, 3/2010 – 3/2013
Aviva Lev-Ari, PhD, RN and Larry Bernstein, MD, FCAP
Competition in the Ecosystem of Medical Devices in Cardiac and Vascular Repair: Heart Valves, Stents, Catheterization Tools and Kits for Open Heart and Minimally Invasive Surgery (MIS)
Aviva Lev-Ari, PhD, RN
Bioabsorbable Drug Coating Scaffolds, Stents and Dual Antiplatelet Therapy
Aviva Lev-Ari, PhD, RN
Vascular Repair: Stents and Biologically Active Implants
Larry Bernstein, MD, FCAP
Drug Eluting Stents: On MIT’s Edelman Lab’s Contributions to Vascular Biology and its Pioneering Research on DES
Larry H. Bernstein, MD, FCAP
Coronary Artery Disease – Medical Devices Solutions: From First-In-Man Stent Implantation, via Medical Ethical Dilemmas to Drug Eluting Stents
Aviva Lev-Ari, PhD, RN
Survivals Comparison of Coronary Artery Bypass Graft (CABG) and Percutaneous Coronary Intervention (PCI) / Coronary Angioplasty
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Trans-apical Transcatheter Aortic Valve Replacement in a Patient with Severe and Complex Left Main Coronary Artery Disease (LMCAD)
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Transcatheter Aortic Valve Replacement (TAVR): Postdilatation to Reduce Paravalvular Regurgitation During TAVR with a Balloon-expandable Valve
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Svelte Medical Systems’ Drug-Eluting Stent: 0% Clinically-Driven Events Through 12-Months in First-In-Man Study
Aviva Lev-Ari, PhD, RN
Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone (Justin Pearlman, Aviva Lev-Ari)
Biomaterials Technology: Models of Tissue Engineering for Reperfusion and Implantable Devices for Revascularization
Larry Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Revascularization: PCI, Prior History of PCI vs CABG
Aviva Lev-Ari, PhD, RN
http://pharmaceuticalintelligence.com/2013/04/25/revascularization-pci-prior-history-of-pci-vs-cabg/
Accurate Identification and Treatment of Emergent Cardiac Events
Larry Bernstein, MD, FCAP
FDA Pending 510(k) for The Latest Cardiovascular Imaging Technology
Aviva Lev-Ari, PhD, RN
The ACUITY-PCI score: Will it Replace Four Established Risk Scores — TIMI, GRACE, SYNTAX, and Clinical SYNTAX
Aviva Lev-Ari, PhD, RN
Nitric Oxide and it’s impact on Cardiothoracic Surgery
Tilda Barliya, PhD
CABG or PCI: Patients with Diabetes – CABG Rein Supreme
Aviva Lev-Ari, PhD, RN
To Stent or Not? A Critical Decision
Aviva Lev-Ari, PhD, RN
Endothelin Receptors in Cardiovascular Diseases: The Role of eNOS Stimulation
Aviva Lev-Ari, PhD, RN
Absorb™ Bioresorbable Vascular Scaffold: An International Launch by Abbott Laboratories
Aviva Lev-Ari, PhD, RN
Carotid Stenting: Vascular surgeons have pointed to more minor strokes in the stenting group and cardiologists to more myocardial infarctions in the CEA cohort.
Aviva Lev-Ari, PhD, RN
New Drug-Eluting Stent Works Well in STEMI
Aviva Lev-Ari, PhD, RN
Global Supplier Strategy for Market Penetration & Partnership Options (Niche Suppliers vs. National Leaders) in the Massachusetts Cardiology & Vascular Surgery Tools and Devices Market for Cardiac Operating Rooms and Angioplasty Suites
Aviva Lev-Ari, PhD, RN

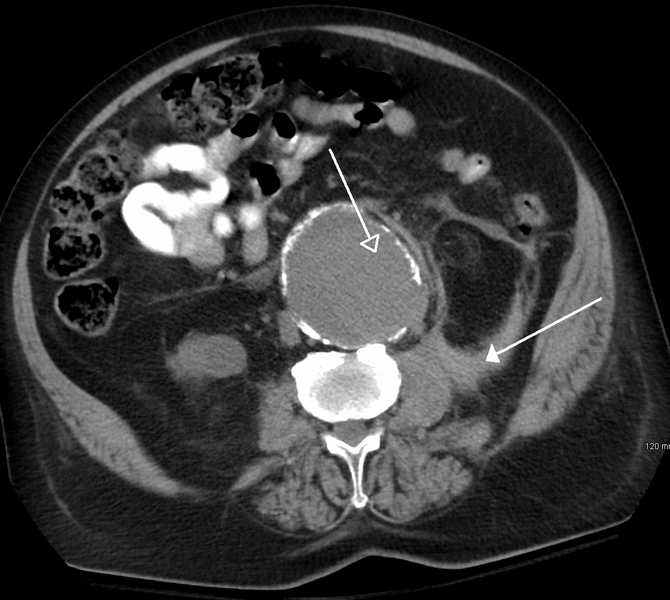
Abdominal Aortic Aneurysm in Computer Tomography (Photo credit: Wikipedia)
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette