Genomics and Metabolomics Advances in Cancer
Writer and Curator: Larry H. Bernstein, MD, FCAP
UPDATED 6/01/2019
UPDATED 9/26/2021
Genomics
Unraveling the clonal hierarchy of somatic genomic aberrations
D Prandi, SC Baca, A Romanel, CE Barbieri, Juan-Miguel Mosquera, et al.
Genome Biology 2014, 15:439
http://genomebiology.com/2014/15/8/439
Defining the chronology of molecular alterations may identify milestones in carcinogenesis. To unravel the temporal evolution of aberrations from clinical tumors, we developed CLONET, which upon estimation of tumor admixture and ploidy infers the clonal hierarchy of genomic aberrations. Comparative analysis across 100 sequenced genomes from prostate, melanoma, and lung cancers established diverse evolutionary hierarchies, demonstrating the early disruption of tumor-specific pathways. The analyses highlight the diversity of clonal evolution within and across tumor types that might be informative for risk stratification and patient selection for targeted therapies. CLONET addresses heterogeneous clinical samples seen in the setting of precision medicine.
The Transcription Factor Titration Effect Dictates Level of Gene Expression
RC Brewster, FM Weinert, HG Garcia, D Song, M Rydenfelt, and R Phillips
Cell, Mar 13, 2014;156: 1312–1323
http://dx.doi.org/10.1016/j.cell.2014.02.022
Models of transcription are often built around a picture of RNA polymerase and transcription factors (TFs) acting on a single copy of a promoter. However, most TFs are shared between multiple genes with varying binding affinities. Beyond that, genes often exist at high copy number—in multiple identical copies on the chromosome or on plasmids or viral vectors with copy numbers in the hundreds. Using a thermodynamic model, we characterize the interplay between TF copy number and the demand for that TF. We demonstrate the parameter-free predictive power of this model as a function of the copy number of the TF and the number and affinities of the available specific binding sites; such predictive control is important for the understanding of transcription and the desire to quantitatively design the output of genetic circuits. Finally, we use these experiments to dynamically measure plasmid copy number through the cell cycle.
Telomere dynamics in human mesenchymal stem cells after exposure to acute oxidative stress
M Harbo, S Koelvraa, N Serakinci, L Bendixa
DNA Repair 2012. http://dx.doi.org/10.1016/j.dnarep.2012.06.003
A gradual shortening of telomeres due to replication can be measured using the standard telomere restriction fragments (TRF) assay and other methods by measuring the mean length of all the telomeres in a cell. In contrast, stress-induced telomere shortening, which is believed to be just as important for causing cellular senescence, cannot be measured properly using these methods. Stress-induced telomere shortening caused by, e.g. oxidative damage happens in a stochastic manner leaving just a few single telomeres critically short. It is now possible to visualize these few ultra-short telomeres due to the advantages of the newly developed Universal single telomere length assay (STELA), and we therefore believe that this method should be considered the method of choice when measuring the length of telomeres after exposure to oxidative stress. In order to test our hypothesis, cultured human mesenchymal stem cells, either primary or hTERT immortalized, were exposed to sub-lethal doses of hydrogen peroxide, and the short term effect on telomere dynamics was monitored by Universal STELA and TRF measurements. Both telomere measures were then correlated with the percentage of senescent cells estimated by senescence-associated β-galactosidase staining. The exposure to acute oxidative stress resulted in an increased number of ultra-short telomeres, which correlated strongly with the percentage of senescent cells, whereas a correlation between mean telomere length and the percentage of senescent cells was absent. Based on the findings in the present study, it seems reasonable to conclude that Universal STELA is superior to TRF in detecting telomere damage caused by exposure to oxidative stress. The choice of method should therefore be considered carefully in studies examining stress-related telomere shortening as well as in the emerging field of lifestyle studies involving telomere length measurements.
tDNA insulators and the emerging role of TFIIIC in genome organization
Kevin Van Bortle and Victor G. Corces
Transcription Dec 12, 2012; 3(6): 1-8. www.landesbioscience.com
Recent findings provide evidence that tDNAs function as chromatin insulators from yeast to humans. TFIIIC, a transcription factor that interacts with the B-box in tDNAs as well as thousands of ETC sites in the genome, is responsible for insulator function. Though tDNAs are capable of enhancer-blocking and barrier activities for which insulators are defined, new insights into the relationship between insulators and chromatin structure suggest that TFIIIC serves a complex role in genome organization. We review the role of tRNA genes and TFIIIC as chromatin insulators, and highlight recent findings that have broadened our understanding of insulators in genome biology.
Structure and organization of insulators in eukaryotes. (A) From yeast to mammals, in organisms in which it has been studied, the TFIIIC protein interacts with the B-box sequence in tRNA genes or sites in the genome named ETC sites.
Synthetic CpG islands reveal DNA sequence determinants of chromatin structure
E Wachter, T Quante, C Merusi, A Arczewska, F Stewart, S Webb, A Bird
eLife 2014;3:e03397. http://dx.doi.org:/10.7554/eLife.03397.001
The mammalian genome is punctuated by CpG islands (CGIs), which differ sharply from the bulk genome by being rich in G + C and the dinucleotide CpG. CGIs often include transcription initiation sites and display ‘active’ histone marks, notably histone H3 lysine 4 methylation. In embryonic stem cells (ESCs) some CGIs adopt a ‘bivalent’ chromatin state bearing simultaneous ‘active’ and ‘inactive’ chromatin marks. To determine whether CGI chromatin is developmentally programmed at specific genes or is imposed by shared features of CGI DNA, we integrated artificial CGI-like DNA sequences into the ESC genome. We found that bivalency is the default chromatin structure for CpG-rich, G + C-rich DNA. A high CpG density alone is not sufficient for this effect, as A + T-rich sequence settings invariably provoke de novo DNA methylation leading to loss of CGI signature chromatin. We conclude that both CpG-richness and G + C-richness are required for induction of signature chromatin structures at CGIs.
Locus-specific mutation databases: pitfalls and good practice based on the p53 experience
Thierry Soussi, Chikashi Ishioka, Mireille Claustres and Christophe Béroud
NATURE REVIEWS | CANCER JAN 2006; 6: 83-90.
Between 50,000 and 60,000 mutations have been described in various genes that are associated with a wide variety of diseases. Reporting, storing and analysing these data is an important challenge as such data provide invaluable information for both clinical medicine and basic science.
The practical value of mutation analysis All studies performed to date show that mutations are, in general, not randomly distributed. Hot-spot regions have been demonstrated, corresponding to a region of DNA that is susceptible to mutations (such as CpG dinucleotides), a codon encoding a key residue in the biological function of the protein, or both (BOX 1). Identification of these hot-spot regions and natural mutants is essential to define crucial regions in an unknown protein.
Locus-specific databases have been developed to exploit this huge volume of data. The p53 mutation database is a paradigm, as it constitutes the largest collection of somatic mutations (22,000). However, there are several biases in this database that can lead to serious erroneous interpretations. We describe several rules for mutation database management that could benefit the entire scientific community.
Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles
A Subramaniana, P Tamayo, VK Mootha, S Mukherjee, BL Ebert, et al.
PNAS Oct 25, 2005; 102(43): 15545–15550
http://pnas.org/cgi/doi/10.1073/pnas.0506580102
Although genomewide RNA expression analysis has become a routine tool in biomedical research, extracting biological insight from such information remains a major challenge. Here, we describe a powerful analytical method called Gene Set Enrichment Analysis (GSEA) for interpreting gene expression data. The method derives its power by focusing on gene sets, that is, groups of genes that share common biological function, chromosomal location, or regulation. We demonstrate how GSEA yields insights into several cancer-related data sets, including leukemia and lung cancer. Notably, where single-gene analysis finds little similarity between two independent studies of patient survival in lung cancer, GSEA reveals many biological pathways in common. The GSEA method is embodied in a freely available software package, together with an initial database of 1,325 biologically defined gene sets.
Mutational landscape and significance across 12 major cancer types
C Kandoth, MD McLellan, F Vandin, Kai Ye, B Niu, C Lu, et al.
NATURE OCT 2013; 502: 333-337. http://dx.doi.org:/10.1038/nature12634
The Cancer Genome Atlas (TCGA) has used the latest sequencing and analysis methods to identify somatic variants across thousands of tumours. Here we present data and analytical results for point mutations and small insertions/deletions from 3,281 tumours across 12 tumour types as part of the TCGA Pan-Cancer effort. We illustrate the distributions of mutation frequencies, types and contexts across tumour types, and establish their links to tissues of origin, environmental/ carcinogen influences, and DNA repair defects. Using the integrated data sets, we identified 127 significantly mutated genes from well-known(for example, mitogen-activated protein kinase, phosphatidylinositol-3-OH kinase,Wnt/b-catenin and receptor tyrosine kinase signalling pathways, and cell cycle control) and emerging (for example, histone, histone modification, splicing, metabolism and proteolysis) cellular processes in cancer. The average number of mutations in these significantly mutated genes varies across tumour types; most tumours have two to six, indicating that the numberof driver mutations required during oncogenesis is relatively small. Mutations in transcriptional factors/regulators show tissue specificity, whereas histone modifiers are often mutated across several cancer types. Clinical association analysis identifies genes having a significant effect on survival, and investigations of mutations with respect to clonal/subclonal architecture delineate their temporal orders during tumorigenesis. Taken together, these results lay the groundwork for developing new diagnostics and individualizing cancer treatment.
Molecular insights into RNA and DNA helicase evolution from the determinants of specificity for a DEAD-box RNA helicase
Anna L. Mallam, David J. Sidote and Alan M. Lambowitz
eLife 2014; http://dx.doi.org:/10.7554/eLife.04630
How different helicase families with a conserved catalytic ‘helicase core’ evolved to function on varied RNA and DNA substrates by diverse mechanisms remains unclear. Here, we used Mss116, a yeast DEAD-box protein that utilizes ATP to locally unwind dsRNA, to investigate helicase specificity and mechanism. Our results define the molecular basis for the substrate specificity of a DEAD-box protein. Additionally, they show that Mss116 has ambiguous substrate-binding properties and interacts with all four NTPs and both RNA and DNA. The efficiency of unwinding correlates with the stability of the ‘closed-state’ helicase core, a complex with nucleotide and nucleic acid that forms as duplexes are unwound. Crystal structures reveal that core stability is modulated by family-specific interactions that favor certain substrates. This suggests how present-day helicases diversified from an ancestral core with broad specificity by retaining core closure as a common catalytic mechanism while optimizing substrate-binding interactions for different cellular functions.
Identification of human TERT elements necessary for telomerase recruitment to telomeres
Jens C Schmidt, Andrew B Dalby, Thomas R Cech
eLife 2014; http://dx.doi.org/10.7554/eLife.03563
Human chromosomes terminate in telomeres, repetitive DNA sequences bound by the shelterin complex. Shelterin protects chromosome ends, prevents recognition by the DNA damage machinery, and recruits telomerase. A patch of amino acids, termed the TEL-patch, on the OB-fold domain of the shelterin component TPP1 is essential to recruit telomerase to telomeres. In contrast, the site on telomerase that interacts with the TPP1 OB-fold is not well defined. Here we identify separation-of-function mutations in the TEN-domain of human telomerase reverse transcriptase (hTERT) that disrupt the interaction of telomerase with TPP1 in vivo and in vitro but have very little effect on the catalytic activity of telomerase. Suppression of a TEN-domain mutation with a compensatory charge-swap mutation in the TEL-patch indicates that their association is direct. Our findings define the interaction interface required for telomerase recruitment to telomeres, an important step towards developing modulators of this interaction as therapeutics for human disease.
Metabolomics
Single Cell Profiling of Circulating Tumor Cells: Transcriptional Heterogeneity and Diversity from Breast Cancer Cell Lines
MN Mindrinos, G Bhanot, SH Dairkee, RW Davis, SS Jeffrey
PLoS ONE 7(5): e33788. http://dx.doi.org:/doi:10.1371/journal.pone.0033788
Background: To improve cancer therapy, it is critical to target metastasizing cells. Circulating tumor cells (CTCs) are rare cells found in the blood of patients with solid tumors and may play a key role in cancer dissemination. Uncovering CTC phenotypes offers a potential avenue to inform treatment. However, CTC transcriptional profiling is limited by leukocyte contamination; an approach to surmount this problem is single cell analysis. Here we demonstrate feasibility of performing high dimensional single CTC profiling, providing early insight into CTC heterogeneity and allowing comparisons to breast cancer cell lines widely used for drug discovery.
Methodology/Principal Findings: We purified CTCs using the MagSweeper, an immunomagnetic enrichment device that isolates live tumor cells from unfractionated blood. CTCs that met stringent criteria for further analysis were obtained from 70% (14/20) of primary and 70% (21/30) of metastatic breast cancer patients; none were captured from patients with nonepithelial cancer (n = 20) or healthy subjects (n = 25). Microfluidic-based single cell transcriptional profiling of 87 cancer associated and reference genes showed heterogeneity among individual CTCs, separating them into two major subgroups, based on 31 highly expressed genes. In contrast, single cells from seven breast cancer cell lines were tightly clustered together by sample ID and ER status. CTC profiles were distinct from those of cancer cell lines, questioning the suitability of such lines for drug discovery efforts for late stage cancer therapy.
Conclusions/Significance: For the first time, we directly measured high dimensional gene expression in individual CTCs without the common practice of pooling such cells. Elevated transcript levels of genes associated with metastasis NPTN, S100A4, S100A9, and with epithelial mesenchymal transition: VIM, TGFß1, ZEB2, FOXC1, CXCR4, were striking compared to cell lines. Our findings demonstrate that profiling CTCs on a cell-by-cell basis is possible and may facilitate the application of ‘liquid biopsies’ to better model drug discovery
Simplifying Disease Complexity part 6 – Bringing Metabolomics into Practice
Dr. Kirk Beebe, Director of Application Science, Metabolon, Inc.
n the previous editions of this 6-part series, we’ve explored numerous example of how metabolomics is bringing success to areas such as cancer, metabolic disease, cardiovascular, and rare disease research. Although we did not devote attention to every area of biology or therapeutic area, the intent of this broad series was not only to convey how metabolomics can be used in a specific area of research (e.g. cancer), but actually, how metabolomics is a central science for interrogating any biological question. So, although it may seem like an oversimplification, to understand whether metabolomics could be used in a research setting one need only ask themselves, “Do I have a biological question that would benefit from a hypothesis-free approach?, am I interested in exploring my system for potential new discoveries? Or do I need a biomarker/better biomarker?
As described in our first part, metabolites have been and continue to be a staple for clinical and in vivo decision making (e.g. cholesterol, glucose, bilirubin, creatinine, thyroid hormone, newborn screening for inborn errors of metabolism (IEMs)). In short, this utility is fundamental to the foundations of biology since metabolism is central to all kingdoms of life and contemporary biology is driven to maintain metabolic homeostasis to maintain the phenotype. An unappreciated point that we leave this series with is that this fundamental nature (the connection of metabolism to the phenotype) confers an important advantage of metabolism for deriving biomarkers and understanding the underlying physiology.
Metabolites are a diagnostic data stream.
Whether a phenotype is driven by a single mutation or a combination of genetic differences, environmental influences or the microbiota, metabolism provides a systems-level diagnostic.
That is, no matter the source of the physiological or phenotypic change (i.e. genes, microbiota, environmental), the change will almost invariably register within metabolism. Thus, modern metabolomic approaches offer the opportunity to more deeply interrogate the “metabolome” to discover more sensitive and specific biomarkers and understand the basis of disease and drug response.
As such, metabolomics has the potential to be able to integrate systems on a number of levels. It is useful through its ability to enrich genomics, transcriptomics and proteomics, thus integrating a number of data streams that provide knowledge and contribute to informed decision-making and patient management1. Using metabolomics, individual tissues can be queried but less invasive sample types (e.g., blood, urine, feces, and/or saliva) can also yield biomarkers and mechanistic insight. The integration of the individual tissues at the level of these more accessible samples can offer an overview of the entire system and inform on important biological pathways. Finally, although the focus of this series was on what metabolomics can bring to biomarker and other related research areas, it should be noted that a combination of metabolomics with other scientific approaches will undoubtedly broaden insight and produce verifiable, validatable biomarkers that track with efficacy and therapy.
As we close this series, we hope that we have conveyed 4 critical points – 1) metabolism is central to biology and hence, key in research and biomarker discovery, 2) the reason for this is due to the fundamental nature of metabolism being central to the development of all life and being the focal point of contemporary biology’s drive to maintain homeostasis, 3) metabolomic is the most powerful way to survey metabolism by offering a simultaneous read-out if hundreds of reactions and pathways, and 4) metabolomics as a practical tool has only recently emerged.
And it is on this last point that we leave the reader with some final considerations. We imagine that, after careful review of the information outlined in this series, many readers will be motivated to explore the use of metabolomics in their research. However, as outlined throughout this series, mature technologies have only recently arisen. Nevertheless, there are many laboratories that perform some version of “metabolomics”. Although the experimental goal often dictates the precise approach, there are 5 critical features that a metabolomic technology must harbor in order for it to achieve a similar purpose as mature omic technologies (e.g. DNA sequencers) in terms of depth of coverage and data quality. These minimally include:
- Must be based on an authenticated chemical library
2. Must have procedures for eliminated noise from the data
5. Must have a mechanism to identify novel metabolites
6. Must have robust QC process from sample preparation through statistical analysis
4. Must provide a mechanism to abstract information/interpret the data
References
- Eckhart, A.D., Beebe, K. & Milburn, M. Metabolomics as a key integrator for “omic” advancement of personalized medicine and future therapies. Clin Transl Sci 5, 285-288
(2012).
- Evans, A., Mitchell, M., Dai, H. & DeHaven, C.D. Categorizing Ion –Features in Liquid Chromatography/Mass Spectrometry Metobolomics Data. Metabolomics 2 (2012).
- DeHaven, C.D., Evans, A., Dai, H. & Lawton, K.A. in Metabolomics. (ed. U. Roessner) (InTech, 2012).
- Dehaven, C.D., Evans, A.M., Dai, H. & Lawton, K.A. Organization of GC/MS and LC/MS metabolomics data into chemical libraries. J Cheminform 2, 9 (2010).
- Evans, A.M., DeHaven, C.D., Barrett, T., Mitchell, M. & Milgram, E. Integrated, nontargeted ultrahigh performance liquid chromatography/electrospray ionization tandem mass spectrometry platform for the identification and relative quantification of the small-molecule complement of biological systems. Anal Chem 81, 6656-6667 (2009).
Prediction of intracellular metabolic states from extracellular metabolomic data
MK Aurich, G Paglia, Ottar Rolfsson, S Hrafnsdottir, M Magnusdottir, MM, et al.
Metabolomics Aug 14, 2014; http://dx.doi.org:/10.1007/s11306-014-0721-3
http://link.springer.com/article/10.1007/s11306-014-0721-3/fulltext.html#Sec1

intra- extracellular metabolites
Metabolic models can provide a mechanistic framework to analyze information-rich omics data sets, and are increasingly being used to investigate metabolic alternations in human diseases. An expression of the altered metabolic pathway utilization is the selection of metabolites consumed and released by cells. However, methods for the inference of intracellular metabolic states from extracellular measurements in the context of metabolic models remain underdeveloped compared to methods for other omics data. Herein, we describe a workflow for such an integrative analysis emphasizing on extracellular metabolomics data. We demonstrate, using the lymphoblastic leukemia cell lines Molt-4 and CCRF-CEM, how our methods can reveal differences in cell metabolism. Our models explain metabolite uptake and secretion by predicting a more glycolytic phenotype for the CCRF-CEM model and a more oxidative phenotype for the Molt-4 model, which was supported by our experimental data. Gene expression analysis revealed altered expression of gene products at key regulatory steps in those central metabolic pathways, and literature query emphasized the role of these genes in cancer metabolism. Moreover, in silico gene knock-outs identified unique control points for each cell line model, e.g., phosphoglycerate dehydrogenase for the Molt-4 model. Thus, our workflow is well suited to the characterization of cellular metabolic traits based on extracellular metabolomic data, and it allows the integration of multiple omics data sets into a cohesive picture based on a defined model context.

Metabolome Informatics Research

Identification of Metabolites in the Normal Ovary and Their Transformation in Primary and Metastatic Ovarian Cancer MOC vs EOC
Genomics and Cancer
Identification of Gene Networks Associated with Acute Myeloid Leukemia by Comparative Molecular Methylation and Expression Profiling
M Dellett, KA O’Hagan, HA Alexandra Colyer and KI Mills
Biomarkers in Cancer 2010:2 43–55 http://www.la-press.com.
Around 80% of acute myeloid leukemia (AML) patients achieve a complete remission, however many will relapse and ultimately die of their disease. The association between karyotype and prognosis has been studied extensively and identified patient cohorts as having favourable [e.g. t(8; 21), inv (16)/t(16; 16), t(15; 17)], intermediate [e.g. cytogenetically normal (NK-AML)] or adverse risk [e.g. complex karyotypes]. Previous studies have shown that gene expression profiling signatures can classify the sub-types of AML, although few reports have shown a similar feature by using methylation markers. The global methylation patterns in 19 diagnostic AML samples were investigated using the Methylated CpG Island Amplification Microarray (MCAM) method and CpG island microarrays containing 12,000 CpG sites. The first analysis, comparing favourable and intermediate cytogenetic risk groups, revealed significantly differentially methylated CpG sites (594 CpG islands) between the two subgroups. Mutations in the NPM1 gene occur at a high frequency (40%) within the NK-AML subgroup and are associated with a more favourable prognosis in these patients. A second analysis comparing the NPM1 mutant and wild-type research study subjects again identified distinct methylation profiles between these two subgroups. Network and pathway analysis revealed possible molecular mechanisms associated with the different risk and/or mutation sub-groups. This may result in a better classification of the risk groups, improved monitoring targets, or the identification of novel molecular therapies.
Molecular Imaging of Proteases in Cancer
Yunan Yang, Hao Hong, Yin Zhang and Weibo Cai
Cancer Growth and Metastasis 2009:2 13–27. http://www.la-press.com
Proteases play important roles during tumor angiogenesis, invasion, and metastasis. Various molecular imaging techniques have been employed for protease imaging: optical (both fluorescence and bioluminescence), magnetic resonance imaging (MRI), single-photon emission computed tomography (SPECT), and positron emission tomography (PET). In this review, we will summarize the current status of imaging proteases in cancer with these techniques. Optical imaging of proteases, in particular with fluorescence, is the most intensively validated and many of the imaging probes are already commercially available. It is generally agreed that the use of activatable probes is the most accurate and appropriate means for measuring protease activity. Molecular imaging of proteases with other techniques (i.e. MRI, SPECT, and PET) has not been well-documented in the literature which certainly deserves much future effort. Optical imaging and molecular MRI of protease activity has very limited potential for clinical investigation. PET/SPECT imaging is suitable for clinical investigation; however the optimal probes for PET/SPECT imaging of proteases in cancer have yet to be developed. Successful development of protease imaging probes with optimal in vivo stability, tumor targeting efficacy, and desirable pharmacokinetics for clinical translation will eventually improve cancer patient management. Not limited to cancer, these protease-targeted imaging probes will also have broad applications in other diseases such as arthritis, atherosclerosis, and myocardial infarction.
Evolutionarily conserved genetic interactions with budding and fission yeast MutS identify orthologous relationships in mismatch repair-deficient cancer cells
E Tosti, JA Katakowski, S Schaetzlein, Hyun-Soo Kim, CJ Ryan, M Shales, et al.
Genome Medicine 2014, 6:68. http://genomemedicine.com/content/6/9/68
Background: The evolutionarily conserved DNA mismatch repair (MMR) system corrects base-substitution and insertion-deletion mutations generated during erroneous replication. The mutation or inactivation of many MMR factors strongly predisposes to cancer, where the resulting tumors often display resistance to standard chemotherapeutics. A new direction to develop targeted therapies is the harnessing of synthetic genetic interactions, where the simultaneous loss of two otherwise non-essential factors leads to reduced cell fitness or death. High-throughput screening in human cells to directly identify such interactors for disease-relevant genes is now widespread, but often requires extensive case-by-case optimization. Here we asked if conserved genetic interactors (CGIs) with MMR genes from two evolutionary distant yeast species (Saccharomyces cerevisiae and Schizosaccharomyzes pombe) can predict orthologous genetic relationships in higher eukaryotes.
Methods: High-throughput screening was used to identify genetic interaction profiles for the MutSα and MutSβ heterodimer subunits (msh2Δ, msh3Δ, msh6Δ) of fission yeast. Selected negative interactors with MutSβ (msh2Δ/msh3Δ) were directly analyzed in budding yeast, and the CGI with SUMO-protease Ulp2 further examined after RNA interference/drug treatment in MSH2-deficient and -proficient human cells.
Results: This study identified distinct genetic profiles for MutSα and MutSβ, and supports a role for the latter in recombinatorial DNA repair. Approximately 28% of orthologous genetic interactions with msh2Δ/msh3Δ are conserved in both yeasts, a degree consistent with global trends across these species. Further, the CGI between budding/fission yeast msh2 and SUMO-protease Ulp2 is maintained in human cells (MSH2/SENP6), and enhanced by Olaparib, a PARP inhibitor that induces the accumulation of single-strand DNA breaks. This identifies SENP6 as a promising new target for the treatment of MMR-deficient cancers.
Conclusion: Our findings demonstrate the utility of employing evolutionary distance in tractable lower eukaryotes to predict orthologous genetic relationships in higher eukaryotes. Moreover, we provide novel insights into the genome maintenance functions of a critical DNA repair complex and propose a promising targeted treatment for MMR deficient tumors.
Cancer Genome Landscapes
B Vogelstein, N Papadopoulos, VE Velculescu, S Zhou, LA Diaz Jr., KW Kinzler, et al.
Science 339, 1546 (2013); http://dx.doi.org:/10.1126/science.1235122
Over the past decade, comprehensive sequencing efforts have revealed the genomic landscapes of common forms of human cancer. For most cancer types, this landscape consists of a small number of “mountains” (genes altered in a high percentage of tumors) and a much larger number of “hills” (genes altered infrequently). To date, these studies have revealed ~140 genes that, when altered by intragenic mutations, can promote or “drive” tumorigenesis. A typical tumor contains two to eight of these “driver gene” mutations; the remaining mutations are passengers that confer no selective growth advantage. Driver genes can be classified into 12 signaling pathways that regulate three core cellular processes: cell fate, cell survival, and genome maintenance. A better understanding of these pathways is one of the most pressing needs in basic cancer research. Even now, however, our knowledge of cancer genomes is sufficient to guide the development of more effective approaches for reducing cancer morbidity and mortality.
Approaches for establishing the function of regulatory genetic variants involved in disease
Julian Charles Knight
Genome Medicine 2014, 6:92. http://genomemedicine.com/content/6/10/92
The diversity of regulatory genetic variants and their mechanisms of action reflect the complexity and context-specificity of gene regulation. Regulatory variants are important in human disease and defining such variants and establishing mechanism is crucial to the interpretation of disease-association studies. This review describes approaches for identifying and functionally characterizing regulatory variants, illustrated using examples from common diseases. Insights from recent advances in resolving the functional epigenomic regulatory landscape in which variants act are highlighted, showing how this has enabled functional annotation of variants and the generation of hypotheses about mechanism of action. The utility of quantitative trait mapping at the transcript, protein and metabolite level to define association of specific genes with particular variants and further inform disease associations are reviewed. Establishing mechanism of action is an essential step in resolving functional regulatory variants, and this review describes how this is being facilitated by new methods for analyzing allele-specific expression, mapping chromatin interactions and advances in genome editing. Finally, integrative approaches are discussed together with examples highlighting how defining the mechanism of action of regulatory variants and identifying specific modulated genes can maximize the translational utility of genome-wide association studies to understand the pathogenesis of diseases and discover new drug targets or opportunities to repurpose existing drugs to treat them.
Biomarkers
TRIM29 as a Novel Biomarker in Pancreatic Adenocarcinoma
Hongli Sun, Xianwei Dai, and Bing Han
Disease Markers 2014, Article ID 317817, 7 pages
http://dx.doi.org/10.1155/2014/317817
Background and Aim. Tripartite motif-containing 29 (TRIM29) is structurally a member of the tripartite motif family of proteins and is involved in diverse human cancers. However, its role in pancreatic cancer remains unclear.
Methods. The expression pattern of TRIM29 in pancreatic ductal adenocarcinoma was assessed by immunocytochemistry. Multivariate logistic regression analysis was used to investigate the association between TRIM29 and clinical characteristics. In vitro analyses by scratch wound healing assay and invasion assays were performed using the pancreatic cancer cell lines.
Results. Immunohistochemical analysis showed TRIM29 expression in pancreatic cancer tissues was significantly higher (𝑛 = 186) than that in matched adjacent nontumor tissues. TRIM29 protein expression was significantly correlated with lymph node metastasis (𝑃 = 0.019). Patients with positive TRIM29 expression showed both shorter overall survival and shorter recurrence-free survival than those with negative TRIM29 expression. Multivariate analysis revealed that TRIM29 was an independent factor for pancreatic cancer over survival (HR = 2.180, 95% CI: 1.324–4.198, 𝑃 = 0.011). In vitro, TRIM29 knockdown resulted in inhibition of pancreatic cancer cell proliferation, migration, and invasion.
Conclusions. Our results indicate that TRIM29 promotes tumor progression and may be a novel prognostic marker for pancreatic ductal adenocarcinoma.
Bioinformatic identification of proteins with tissue-specific expression for biomarker discovery
I Prassas, CC Chrystoja, S Makawita1, and EP Diamandis
BMC Medicine 2012, 10:39. http://www.biomedcentral.com/1741-7015/10/39
Background: There is an important need for the identification of novel serological biomarkers for the early detection of cancer. Current biomarkers suffer from a lack of tissue specificity, rendering them vulnerable to nondisease-specific increases. The present study details a strategy to rapidly identify tissue-specific proteins using bioinformatics.
Methods: Previous studies have focused on either gene or protein expression databases for the identification of candidates. We developed a strategy that mines six publicly available gene and protein databases for tissue-specific proteins, selects proteins likely to enter the circulation, and integrates proteomic datasets enriched for the cancer secretome to prioritize candidates for further verification and validation studies.
Results: Using colon, lung, pancreatic and prostate cancer as case examples, we identified 48 candidate tissuespecific biomarkers, of which 14 have been previously studied as biomarkers of cancer or benign disease. Twenty six candidate biomarkers for these four cancer types are proposed.
Conclusions: We present a novel strategy using bioinformatics to identify tissue-specific proteins that are potential cancer serum biomarkers. Investigation of the 26 candidates in disease states of the organs is warranted
The Serum Glycome to Discriminate between Early-Stage Epithelial Ovarian Cancer and Benign Ovarian Diseases
K Biskup, E Iona Braicu, J Sehouli, R Tauber, and V Blanchard
Disease Markers 2014, Article ID 238197, 10 pages
http://dx.doi.org/10.1155/2014/238197
Epithelial ovarian cancer (EOC) is the sixth most common cause of cancer deaths in women because the diagnosis occurs mostly when the disease is in its late-stage. Current diagnostic methods of EOC show only a moderate sensitivity, especially at an early-stage of the disease; hence, novel biomarkers are needed to improve the diagnosis. We recently reported that serum glycome modifications observed in late-stage EOC patients by MALDI-TOF-MS could be combined as a glycan score named GLYCOV that was calculated from the relative areas of the 11 N-glycan structures that were significantly modulated. Here, we evaluated the ability of GLYCOV to recognize early-stage EOC in a cohort of 73 individuals comprised of 20 early-stage primary serous EOC, 20 benign ovarian diseases (BOD), and 33 age-matched healthy controls. GLYCOV was able to recognize stage I EOC whereas CA125 values were statistically significant only for stage II EOC patients. In addition, GLYCOV was more sensitive and specific compared to CA125 in distinguishing early-stage EOC from BOD patients, which is of high relevance to clinicians as it is difficult for them to diagnose malignancy prior to operation.
The Clinicopathological Significance of miR-133a in Colorectal Cancer
Timothy Ming-Hun Wan, Colin Siu-Chi Lam, Lui Ng, Ariel Ka-Man Chow, et al.
Disease Markers 2014, Article ID 919283, 8 pages http://dx.doi.org/10.1155/2014/919283
This study determined the expression of microRNA-133a (MiR-133a) in colorectal cancer (CRC) and adjacent normal mucosa samples and evaluated its clinicopathological role in CRC. The expression of miR-133a in 125 pairs of tissue samples was analyzed by quantitative real-time polymerase chain reaction (qRT-PCR) and correlated with patient’s clinicopathological data by statistical analysis. Endogenous expression levels of several potential target genes were determined by qRT-PCR and correlated using Pearson’s method. MiR-133a was downregulated in 83.2% of tumors compared to normal mucosal tissue. Higher miR-133a expression in tumor tissues was associated with development of distant metastasis, advanced Dukes and TNM staging, and poor survival. The unfavorable prognosis of higher miR-133a expression was accompanied by dysregulation of potential miR-133a target genes, LIM and SH3 domain protein 1 (LASP1), Caveolin-1 (CAV1), and Fascin-1 (FSCN1). LASP1 was found to possess a negative correlation (𝛾 = −0.23), whereas CAV1 exhibited a significant positive correlation (𝛾 = 0.27), and a stronger correlation was found in patients who developed distant metastases (𝛾 = 0.42). In addition, a negative correlation of FSCN1 was only found in nonmetastatic patients. In conclusion, miR-133a was downregulated in CRC tissues, but its higher expression correlated with adverse clinical characteristics and poor prognosis.
The Clinical Significance of PR, ER, NF-𝜅B, and TNF-𝛼 in Breast Cancer
Xian-Long Zhou, Wei Fan, Gui Yang, and Ming-Xia Yu
Disease Markers 2014, Article ID 494581, 7 pages http://dx.doi.org/10.1155/2014/494581
Objectives. To investigate the expression of estrogen (ER), progesterone receptors (PR), nuclear factor-𝜅B (NF-𝜅B), and tumor necrosis factor-𝛼 (TNF-𝛼) in human breast cancer (BC), and the correlation of these four parameters with clinicopathological features of BC.
Methods and Results. We performed an immunohistochemical SABC method for the identification of ER, PR, NF-𝜅B, and TNF-𝛼 expression in 112 patients with primary BC.The total positive expression rate of ER, PR, NF-𝜅B, and TNF-𝛼 was 67%, 76%, 84%, and 94%, respectively. The expressions of ER and PR were correlated with tumor grade, TNM stage, and lymph node metastasis (𝑃 < 0.01, resp.), but not with age, tumor size, histological subtype, age at menarche, menopause status, number of pregnancies, number of deliveries, and family history of cancer. Expressions of ER and PR were both correlated with NF-𝜅B and TNF-𝛼 expression (𝑃 < 0.05, resp.). Moreover, there was significant correlation between ER and PR (𝑃 < 0.0001) as well as between NF-𝜅B and TNF-𝛼 expression (𝑃 < 0.05).
Conclusion. PR and ER are highly expressed, with significant correlation with NF-𝜅B and TNF-𝛼 expression in breast cancer. The important roles of ER and PR in invasion and metastasis of breast cancer are probably associated with NF-𝜅B and TNF-𝛼 expression.
Serum Protein Profile at Remission Can Accurately Assess Therapeutic Outcomes and Survival for Serous Ovarian Cancer
J Wang, A Sharma, SA Ghamande, S Bush, D Ferris, W Zhi, et la.
PLoS ONE 8(11): e78393. http://dx.doi.org:/10.1371/journal.pone.0078393
Background: Biomarkers play critical roles in early detection, diagnosis and monitoring of therapeutic outcome and recurrence of cancer. Previous biomarker research on ovarian cancer (OC) has mostly focused on the discovery and validation of diagnostic biomarkers. The primary purpose of this study is to identify serum biomarkers for prognosis and therapeutic outcomes of ovarian cancer. Experimental Design: Forty serum proteins were analyzed in 70 serum samples from healthy controls (HC) and 101 serum samples from serous OC patients at three different disease phases: post diagnosis (PD), remission (RM) and recurrence (RC). The utility of serum proteins as OC biomarkers was evaluated using a variety of statistical methods including survival analysis.
Results: Ten serum proteins (PDGF-AB/BB, PDGF-AA, CRP, sFas, CA125, SAA, sTNFRII, sIL-6R, IGFBP6 and MDC) have individually good area-under-the-curve (AUC) values (AUC = 0.69–0.86) and more than 10 three-marker combinations have excellent AUC values (0.91–0.93) in distinguishing active cancer samples (PD & RC) from HC. The mean serum protein levels for RM samples are usually intermediate between HC and OC patients with active cancer (PD & RC). Most importantly, five proteins (sICAM1, RANTES, sgp130, sTNFR-II and sVCAM1) measured at remission can classify, individually and in combination, serous OC patients into two subsets with significantly different overall survival (best HR = 17, p,1023).
Conclusion: We identified five serum proteins which, when measured at remission, can accurately predict the overall survival of serous OC patients, suggesting that they may be useful for monitoring the therapeutic outcomes for ovarian cancer.
Serum Clusterin as a Tumor Marker and Prognostic Factor for Patients with Esophageal Cancer
Wei Guo, Xiao Ma, Christine Xue, Jianfeng Luo, Xiaoli Zhu, et al.
Disease Markers 2014, Article ID 168960, 7 pages http://dx.doi.org/10.1155/2014/168960
Background. Recent studies have revealed that clusterin is implicated in many physiological and pathological processes, including tumorigenesis. However, the relationship between serum clusterin expression and esophageal squamous cell carcinoma (ESCC) is unclear.
Methods. The serum clusterin concentrations of 87 ESCC patients and 136 healthy individuals were examined. An independent-samples Mann-Whitney 𝑈 test was used to compare serum clusterin concentrations of ESCC patients to those of healthy controls. Univariate analysis was conducted using the log-rank test and multivariate analyses were performed using the Cox proportional hazards model. Results. In healthy controls, the mean clusterin concentration was 288.8 ± 75.1 𝜇g/mL, while in the ESCC patients, the mean clusterin concentration was higher at 412.3±159.4 𝜇g/mL (𝑃 < 0.0001). The 1-, 2-, and 4-year survival rates for the 87 ESCC patients were 89.70%, 80.00%, and 54.50%. Serum clusterin had an optimal diagnostic cut-off point (serum clusterin concentration = 335.5 𝜇g/mL) for esophageal squamous cell carcinoma with sensitivity of 71.26% and specificity of 77.94%. And higher serum clusterin concentration (>500 𝜇g/mL) indicated better prognosis (𝑃 = 0.030).
Conclusions. Clusterin may play a key role during tumorigenesis and tumor progression of ESCC and it could be applied in clinical work as a tumor marker and prognostic factor.
Septin 9 methylated DNA is a sensitive and specific blood test for colorectal cancer
JD Warren, Wei Xiong, AM Bunker, CP Vaughn, LV Furtado, et al.
BMC Medicine 2011, 9:133. http://www.biomedcentral.com/1741-7015/9/133
Background: About half of Americans 50 to 75 years old do not follow recommended colorectal cancer (CRC) screening guidelines, leaving 40 million individuals unscreened. A simple blood test would increase screening compliance, promoting early detection and better patient outcomes. The objective of this study is to demonstrate the performance of an improved sensitivity blood-based Septin 9 (SEPT9) methylated DNA test for colorectal cancer. Study variables include clinical stage, tumor location and histologic grade.
Methods: Plasma samples were collected from 50 untreated CRC patients at 3 institutions; 94 control samples were collected at 4 US institutions; samples were collected from 300 colonoscopy patients at 1 US clinic prior to endoscopy. SEPT9 methylated DNA concentration was tested in analytical specimens, plasma of known CRC cases, healthy control subjects, and plasma collected from colonoscopy patients.
Results: The improved SEPT9 methylated DNA test was more sensitive than previously described methods; the test had an overall sensitivity for CRC of 90% (95% CI, 77.4% to 96.3%) and specificity of 88% (95% CI, 79.6% to 93.7%), detecting CRC in patients of all stages. For early stage cancer (I and II) the test was 87% (95% CI, 71.1% to 95.1%) sensitive. The test identified CRC from all regions, including proximal colon (for example, the cecum) and had a 12% false-positive rate. In a small prospective study, the SEPT9 test detected 12% of adenomas with a false-positive rate of 3%.
Conclusions: A sensitive blood-based CRC screening test using the SEPT9 biomarker specifically detects a majority of CRCs of all stages and colorectal locations. The test could be offered to individuals of average risk for CRC who are unwilling or unable to undergo colonoscopy.
Matrix Metalloproteinases in Cancer: Prognostic Markers and Therapeutic Targets
Pia Vihinen And Veli-Matti K¨Ah¨Ari
Int. J. Cancer 2002; 99: 157–166 http://dx.doi.org:/10.1002/ijc.10329
Degradation of extracellular matrix is crucial for malignant tumour growth, invasion, metastasis and angiogenesis. Matrix metalloproteinases (MMPs) are a family of zinc-dependent neutral endopeptidases collectively capable of degrading essentially all matrix components. Elevated levels of distinct MMPs can be detected in tumour tissue or serumof patients with advanced cancer and their role as prognostic indicators in cancer is studied. In addition, therapeutic intervention of tumour growth and invasion based on inhibition of MMP activity is under intensive investigation and several MMP inhibitors are in clinical trials in cancer. In this review, we discuss the current view on the feasibility of MMPs as prognostic markers and as targets for therapeutic intervention in cancer.
Mass Spectrometric Screening of Ovarian Cancer with Serum Glycans
Jae-Han Kim, Chang Won Park, Dalho Um, Ki Hwang Baek, Yohahn Jo, et al.
Disease Markers 2014, Article ID 634289, 9 pages
http://dx.doi.org/10.1155/2014/634289
development of novel biomarkers based on the glycomic analysis. In this study, N-linked glycans from human serum were quantitatively profiled by matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry (MS) and compared between healthy controls and ovarian cancer patients. A training set consisting of 40 healthy controls and 40 ovarian cancer cases demonstrated an inverse correlation between 𝑃 value of ANOVA and area under the curve (AUC) of each candidate biomarker peak from MALDI-TOF MS, providing standards for the classification. A multi-biomarker panel composed of 15 MALDI-TOF MS peaks resulted in AUC of 0.89, 80∼90% sensitivity, and 70∼83% specificity in the training set. The performance of the biomarker panel was validated in a separate blind test set composed of 23 healthy controls and 37 ovarian cancer patients, leading to 81∼84% sensitivity and 83% specificity with cut-off values determined by the training set. Sensitivity of CA-125, the most widely used ovarian cancer marker, was 74%in the training set and 78% in the test set, respectively. These results indicate that MALDI-TOF MS-mediated serum N-glycan analysis could provide critical information for the screening of ovarian cancer.
Large, Collaborative Lung Cancer Trial Goes for Precision Medicine Goal
News | June 30, 2014 | Lung Cancer Targets
By Anna Azvolinsky, PhD
In a new biomarker-focused clinical trial, five therapies will be tested to develop new, precision medicine approaches to treat squamous cell lung cancer. The Lung Cancer Master Protocol (Lung-MAP)/SWOG S1400 phase 2/3 clinical trial, brings together the National Cancer Institute (NCI), the Foundation for the National Institutes of Health (FNIH), SWOG Cancer Research, five pharmaceutical companies (Amgen, AstraZeneca, Genentech, MedImmune, and Pfizer), Foundation Medicine (a molecular informatics company), and Friends of Cancer Research, a non-profit foundation.
The trial aims to enroll about 10,000 patients total and will cost about $160 million, of which the NCI is contributing $25 million.
Lung-MAP is unique as this is the first public-private partnership in drug development that includes the NCI, the Food and Drug Administration (FDA), U.S. oncology cooperative groups, and a number of patient advocacy groups according to one of the study investigators, David Gandara, MD, chair of the SWOG lung committee, and thoracic oncologist at the UC Davis Cancer Center. “Funds are made available for every aspect of the trial,” said Gandara. “There is nothing in the history of oncology or drug development like it.”
The clinical trial seeks to identify molecular aberrations in patients with advanced squamous cell lung cancer that can be targeted either by existing therapies or through the development of new ones. The innovation of this trial is a master protocol that will rely on the strength of numbers—up to 1000 patients per year at more than 200 sites throughout the U.S. for more than 200 cancer-related genetic alterations. Testing results will then dictate which experimental trial arm is most appropriate for which patient. Unlike a trial that seeks to enroll patients harboring just one mutation, which limits the access for many patients, the Lung-MAP design better ensures that a patient who is screened will be eligible for a targeted therapy trial arm.
This type of umbrella trial design is particularly suitable for squamous cell lung cancer. Thus far, has not been defined by one or several driver mutations. Instead, these tumors are made of a spectrum of genetic aberrations that are each relatively rare within the squamous lung cancer patient population, making enrollment into targeted therapy clinical trials difficult. According to the NCI, Lung-MAP “aims to establish a model of clinical testing that more efficiently meets the needs of both patients and drug developers,” facilitating more efficient matching of a patient to an investigational targeted therapy trial.
Lung-MAP was specifically designed for squamous cell lung cancer because this lung cancer subtype represents the greatest unmet need for new treatment, Gandara told OncoTherapy Network:
“All of the dramatic advances that have been made in the treatment of lung cancer over the last ten years have occurred in adenocarcinoma, a lung cancer subtype with several recently recognized and ‘druggable oncogenes’ such as EGFR mutations or ALK translocations. However, there have been essentially no advances in squamous cell lung cancer.”
But, recent genome-wide studies have identified several gene alterations in squamous cell lung cancer that are also druggable, including PI3K, FGFR, and CDK mutations, said Gandara. The trial is initially testing four targeted therapies: Genentech’s GDC-0032 (a PI3 kinase inhibitor), Pfizer’s palbociclib (an oral cyclin-dependent-kinase 4/6 inhibitor, AZD4547), an oral fibroblast growth factor receptor inhibitor from AstraZeneca, and rilotumumab, Amgen’s antibody against the human hepatocyte growth factor.
The fifth agent is, MEDI4736, an immune checkpoint inhibitor antibody targeting PD-L1. Patients whose tumors do not harbor a mutation suitable for targeting with one of the four targeted therapies will be enrolled in the MED4736 sub-study.
Once a patient is matched to a specific trial sub-study, randomization will determine whether the patient receives the experimental therapy or standard of care chemotherapy. The planned trial endpoints for each sub-study are overall survival and progression-free survival.
“I cannot overemphasize the importance of the FDA’s participation in this project, since each of these sub-studies is designed to result in approval of a paired biomarker and new drug if that sub-study meets the requirements for improved effectiveness,” said Gandara.
– See more at: http://www.oncotherapynetwork.com/lung-cancer-targets/large-collaborative-lung-cancer-trial-goes-precision-medicine-goal
The BATTLE Trial: Personalizing Therapy for Lung Cancer
Kim, RS. Herbst, II. Wistuba, JJ Lee, GR. Blumenschein Jr., A Tsao, DJ. Stewart, et al.
Authors’ Affiliations: 1Departments of Thoracic/Head and Neck Medical Oncology, 2Pathology, 3Biostatistics, and 4Diagnostic Radiology, The University of Texas MD Anderson Cancer Center, Houston, Texas; 5Winship Cancer Center, Emory University, Atlanta, Georgia; 6Dana-Farber Cancer Institute, Boston, Massachusetts; and 7University of Maryland, Baltimore, Maryland.
Corresponding Author:
Waun K. Hong, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd., Houston, TX 77030. Phone: 713-794-1441; Fax: 1-713-792-4654; E-mail:whong@mdanderson.org
The Biomarker-integrated Approaches of Targeted Therapy for Lung Cancer Elimination (BATTLE) trial represents the first completed prospective, biopsy-mandated, biomarker-based, adaptively randomized study in 255 pretreated lung cancer patients. Following an initial equal randomization period, chemorefractory non–small cell lung cancer (NSCLC) patients were adaptively randomized to erlotinib, vandetanib, erlotinib plus bexarotene, or sorafenib, based on relevant molecular biomarkers analyzed in fresh core needle biopsy specimens. Overall results include a 46% 8-week disease control rate (primary end point), confirm prespecified hypotheses, and show an impressive benefit from sorafenib among mutant-KRAS patients. BATTLE establishes the feasibility of a new paradigm for a personalized approach to lung cancer clinical trials.
(ClinicalTrials.gov numbers:NCT00409968, NCT00411671, NCT00411632, NCT00410059, and NCT00410189.
Significance: The BATTLE study is the first completed prospective, adaptively randomized study in heavily pretreated NSCLC patients that mandated tumor profiling with “real-time” biopsies, taking a substantial step toward realizing personalized lung cancer therapy by integrating real-time molecular laboratory findings in delineating specific patient populations for individualized treatment. Cancer Discovery; 1(1); 44–53. © 2011 AACR.
Read the Commentary on this article by Sequist et al., p. 14
Read the Commentary on this article by Rubin et al., p. 17
This article is highlighted in the In This Issue feature, p. 4
Pharmacometabolomics in Drug Discovery & Development: Applications and Challenges
Yang and F. Marotta
Metabolomics 2012, 2:5 http://dx.doi.org/10.4172/2153-0769.1000e122
Recently, the concept of pharmaco-metabolomics is mentioned more frequently as an emerging discipline to study the effect of drugs on the whole pattern of small endogenous molecules and in applying the profiles of metabolomics for drug development. For the latter part, metabolomics is majorly used to differentiate patients into responder or non-responder groups in an effort to decrease large inter-individual variation in clinical trials. It is a novel approach that combines metabolite profile and chemo-metrics to model and predict drug targets, efficacy, pharmacokinetics and toxicity on both individual and population basis. It attracts many scientists’ attention because of its intrinsic advantages and promising potentials in drug discovery and development. Considering personalized drug treatment is the desired goal for current drug development, pharmaco-metabolomics provide an effective and inexpensive strategy to evaluate drug efficacy and toxicology, which may make personalized medicine realistic both from scientific and financial perspectives. Furthermore, the FDA also realized that metabolomics coupling with other “Omics” approaches could be a valuable tool in evaluating general toxicology and could eventually replace the use of animals after addressing certain challenges.
Networking metabolites and diseases
Pascal Braun, Edward Rietman, and Marc Vidal
PNAS July 22, 2008; 105(29): 9849–9850
Diseasome and Drug-Target Network
Recently, Goh et al. constructed a ‘‘diseasome’’ network in which two diseases are linked to each other if they share at least one gene, in which mutations are associated with both diseases. In the resulting network, related disease families cluster tightly together, thus phenotypically defining functional modules. Importantly, for the first time this study applied concepts from network biology to human diseases, thus opening the door for discovering causal relationships between disregulated networks and resulting ailments.
Subsequently Yilderim et al. linked drugs to protein targets in a drug–target network, which could then be overlaid with the diseasome network. One notable finding was the recent trend toward the development of new compounds directly targeted at disease gene products, whereas previous drugs, often found by trial and error, appear to target proteins only indirectly related to the actual disease molecular mechanisms. An important question that remains in this emerging field of network analysis consists of investigating the extent to which directly targeting the product of mutated genes is an efficient approach or whether targeting network properties instead, and thereby accounting for indirect nonlinear effects of system perturbations by drugs, may prove more fruitful. However, to answer such questions it is important to have a good understanding of the various influences that can lead to diseases.
UPDATED 6/01/2019
Combined hereditary and somatic mutations of replication error repair genes result in rapid onset of ultra-hypermutated cancers
from Nat Genet. 2015 Mar;47(3):257-62. doi: 10.1038/ng.3202. Epub 2015 Feb 2.
Shlien A1, Campbell BB2, de Borja R3, Alexandrov LB4, Merico D5, Wedge D4, Van Loo P6, Tarpey PS4, Coupland P7, Behjati S4, Pollett A8, Lipman T9, Heidari A9, Deshmukh S9, Avitzur N9, Meier B10, Gerstung M4, Hong Y10, Merino DM3, Ramakrishna M4, Remke M11, Arnold R3, Panigrahi GB3, Thakkar NP12, Hodel KP13, Henninger EE13, Göksenin AY13, Bakry D14, Charames GS15, Druker H16, Lerner-Ellis J17, Mistry M2, Dvir R18, Grant R14, Elhasid R18, Farah R19, Taylor GP20, Nathan PC14, Alexander S14, Ben-Shachar S21, Ling SC22, Gallinger S23, Constantini S24, Dirks P25, Huang A26, Scherer SW27, Grundy RG28, Durno C29, Aronson M30, Gartner A10, Meyn MS31, Taylor MD25, Pursell ZF13, Pearson CE12, Malkin D32, Futreal PA4, Stratton MR4, Bouffet E26, Hawkins C33, Campbell PJ34, Tabori U35; Biallelic Mismatch Repair Deficiency Consortium.
Abstract: DNA replication-associated mutations are repaired by two components: polymerase proofreading and mismatch repair. The mutation/consequences of disruption to both repair components in humans are not well studied. We sequenced cancer genomes from children with inherited biallelic mismatch repair deficiency (bMMRD). High-grade bMMRD brain tumors exhibited massive numbers of substitution mutations (>250/Mb), which was greater than all childhood and most cancers (>7,000 analyzed). All ultra-hypermutated bMMRD cancers acquired early somatic driver mutations in DNA polymerase ɛ or δ. The ensuing mutation signatures and numbers are unique and diagnostic of childhood germ-line bMMRD (P < 10(-13)). Sequential tumor biopsy analysis revealed that bMMRD/polymerase-mutant cancers rapidly amass an excess of simultaneous mutations (∼600 mutations/cell division), reaching but not exceeding ∼20,000 exonic mutations in <6 months. This implies a threshold compatible with cancer-cell survival. We suggest a new mechanism of cancer progression in which mutations develop in a rapid burst after ablation of replication repair.
Genetic changes which occur in spontaneous arising somatic cancers include point mutations, copy number alterations and rearrangements and in general result from a defective DNA repair mechanisms during proliferation/replication over many years however as most somatic cancers are heterogeneous it is difficult to pinpoint the exact repair defects which may be ultimately responsible for such genetic aberrations.
However, early-onset cancers (e.g. pediatric cancers) in patients with hereditary DNA repair defects offer a good view of the mutation types and secondary pathways that drive oncogenesis. bMMRD is a childhood cancer syndrome characterized by early-onset cancers in various organs and caused by biallelic mutations. In this study, genomes from 17 inherited cancers, by exomic sequencing and microarrays, were analyzed and compared to non-neoplastic tissue genomes from matched patients. Brain cancers from these patients had an extremely high number of point mutations compared to other childhood cancers and adult cancers.
Mismatch repair was defective in all these cancers therefore it appeared that secondary mutations are required to cause the ultrahypermutated state. The most frequently mutated gene was POLE (polymerase epsilon), affecting the proofreading ability of this DNA polymerase. The genomes of tumors with mutant POLE had signature mutational spectrum and the signature occurred early but these signatures had been found in endometrial and colorectal cancers. The authors concluded, based on serial analysis of other brain cancers with bMMRD and the observation that recurrent brain cancers accumulated mutations over a relatively short period, once the proofreading capability of pol epsilon is compromised in MMR deficient cells there is no defense against rapid and catastrophic accumulations of mutations. This rapid accumulation of mutations apparently do not lead to apoptosis but rather rapid tumor initiation, and generating multiple subclones of tumor cells.
UPDATED 9/26/2021
Metabolic Profiling Reveals a Dependency of Human Metastatic Breast Cancer on Mitochondrial Serine and One-Carbon Unit Metabolism
Source: https://pubmed.ncbi.nlm.nih.gov/31941752/
Abstract
Breast cancer is the most common cancer among American women and a major cause of mortality. To identify metabolic pathways as potential targets to treat metastatic breast cancer, we performed metabolomics profiling on the breast cancer cell line MDA-MB-231 and its tissue-tropic metastatic subclones. Here, we report that these subclones with increased metastatic potential display an altered metabolic profile compared with the parental population. In particular, the mitochondrial serine and one-carbon (1C) unit pathway is upregulated in metastatic subclones. Mechanistically, the mitochondrial serine and 1C unit pathway drives the faster proliferation of subclones through enhanced de novo purine biosynthesis. Inhibition of the first rate-limiting enzyme of the mitochondrial serine and 1C unit pathway, serine hydroxymethyltransferase (SHMT2), potently suppresses proliferation of metastatic subclones in culture and impairs growth of lung metastatic subclones at both primary and metastatic sites in mice. Some human breast cancers exhibit a significant association between the expression of genes in the mitochondrial serine and 1C unit pathway with disease outcome and higher expression of SHMT2 in metastatic tumor tissue compared with primary tumors. In addition to breast cancer, a few other cancer types, such as adrenocortical carcinoma and kidney chromophobe cell carcinoma, also display increased SHMT2 expression during disease progression. Together, these results suggest that mitochondrial serine and 1C unit metabolism plays an important role in promoting cancer progression, particularly in late-stage cancer. IMPLICATIONS: This study identifies mitochondrial serine and 1C unit metabolism as an important pathway during the progression of a subset of human breast cancers.
ntroduction
The majority of breast cancer patients die from metastatic disease. The process of cancer metastasis involves local invasion into surrounding tissue, dissemination into the bloodstream, extravasation, and eventual colonization of a new tissue. Following a period of dormancy, small numbers of micrometastases eventually proliferate into large macrometastases, or secondary tumors.
Previous studies have illuminated several themes of metabolic reprogramming that occur during metastasis (1–8). However, the majority of these reported site-specific metabolic features of metastatic cancer cells. We reason that breast cancer cells that leave the primary tumor and successfully establish new lesions at distal sites would encounter similar metabolic stresses during metastasis. By performing comparative metabolomics on the MDA-MB-231 human breast cancer cell line and its tissue-tropic metastatic subclones, we uncovered that the catabolism of the non-essential amino acid serine through the mitochondrial one-carbon (1C) unit pathway is an important driver of proliferation in a subset of metastatic breast cancers that closely resembles the molecular features of MDA-MB-231 cells. Emerging evidence shows that the non-essential amino acid serine is essential for cancer cell survival and proliferation. The genomic regions containing PHGDH are amplified in breast cancer and melanoma, diverting 3PG to serine synthesis (9,10). We also reported that PHGDH is upregulated upon amino acid starvation by the transcription factor ATF4 (11). On one hand, serine serves as a precursor for the synthesis of protein, lipids, nucleotides and other amino acids, which are necessary for cell division and growth. On the other hand, serine catabolism through the mitochondrial 1C unit pathway is critical for maintaining cellular redox control under stress conditions (12,13). In mitochondria, serine catabolism is initiated by serine hydroxymethyltransferase 2 (SHMT2). SHMT2 catalyzes a reversible reaction converting serine to glycine, with concurrent generation of the 1C unit donor methylene-THF, which is further oxidized by downstream enzymes MTHFD2 and MTHFD1L to produce NAD(P)H and formate. Subsequent export of formate from the mitochondria can then be re-assimilated into the cytosolic folate pool to support anabolic reactions. All three mitochondrial serine and 1C unit pathway enzymes (SHMT2, MTHFD2 and MTHFD1L) are upregulated in breast tumor samples compared to normal tissues (13,14). However, due to lack of functional investigations targeting this pathway in in vitro and in vivo breast cancer models, it remains unclear whether the mitochondrial 1C unit pathway represents a good target for treating metastatic breast cancer.
In this study, we report that enzymes in the mitochondrial serine and 1C unit pathway are even further upregulated specifically in subclones of the aggressive breast cancer cell line MDA-MB-231 that have been selected in vivo for the ability to preferentially metastasize to specific organs. We demonstrate that SHMT2 inhibition suppresses proliferation more strongly in these highly metastatic subclones compared to the parental population in vitro. Knockdown of SHMT2 also impairs breast cancer growth in vivo at both the primary and metastatic sites. In addition, we find that the expression of mitochondrial 1C unit pathway enzymes significantly associates with poor disease outcome in a subset of human breast cancer patients, potentiating its role as a therapeutic target or biomarker in advanced cancer. Finally, SHMT2 expression increases in breast invasive carcinoma, adrenocortical carcinoma, chromophobe renal cell carcinoma and papillary renal cell carcinoma during tumor progression, particularly in late stage tumors, suggesting that inhibitors targeting SHMT2 may hold promise for treating these late stage cancers when other therapeutic options become limited.
Materials and Methods
Cell lines
All of the paired parental and metastatic subclones were generated in Dr. Joan Massagué’s laboratory (Memorial Sloan-Kettering Cancer Center) (15–17). Cells were cultured in DMEM/F12 with 10% fetal bovine serum (Sigma) with 1% penicillin/streptomycin. All cells lines were tested every three to six months and found negative for mycoplasma (MycoAlert Mycoplasma Detection Kit; Lonza). These cell lines were not authenticated by the authors. All cell lines used in experiments were passaged no more than ten times from time of thawing.
RNAi
Stable 831-BrM,1833-BoM, and 4175-LM cell lines expressing shRNA against SHMT2, MTHFD2, and c-Myc were generated through infection with lentivirus and 1 μg/mL puromycin selection. shRNA-expressing virus was obtained using a previously published method (13). Pooled populations were tested for on-target knockdown by immunoblot.
Immunoblot
The following antibodies were used: SHMT1, SHMT2 (Sigma), MTHFD2, MTHFD1L, c-Myc, Actin (Cell Signaling Technologies).
RNA Isolation, Reverse Transcription, and Real-Time PCR
Total RNA was isolated from tissue culture plates according to the TRIzol Reagant (Invitrogen) protocol. 3 μg of total RNA was used in the reverse transcription reaction using the SuperScript III (Invitrogen) protocol. Quantitative PCR amplification was performed on the Prism 7900 Sequence Detection System (Applied Biosystems) using Taqman Gene Expression Assays (Applied Biosystems). Gene expression data were normalized to 18S rRNA.
In vivo Tumor Growth Assays
All procedures involving animals and their care were approved by the Institutional Animal Care and Use Committee of Stanford University in accordance with institutional and National Institutes of Health guidelines. For orthotopic growth studies, 4175-LM shNT and 4175-LM shSHMT2 cells (1 × 106 cells in 0.1 mL of PBS, n = 8 per group) were injected into the flanks of NU/J 10-week-old female mice (The Jackson Laboratory). Tumors were measured with calipers over a 50-day time course. Volumes were calculated using the formula width2 × length × 0.5.
For lung metastasis assays, 4175-LM shNT and 4175-LM shSHMT2 cells (0.2 × 105 cells, n = 8 per group) were injected via tail vein into 6–8 week-old female NOD SCID mice. Mice were imaged weekly using the Xenogen IVIS 200 (PerkinElmer, Waltham, MA). Briefly, mice were injected intraperitoneally with 100 μg/g of D-luciferin (potassium salt; PerkinElmer) on the day of imaging. 8 min later, mice were anesthetized in an anesthesia-induction chamber using a mixture of 3% isoflurane (Fluriso, VetOne) in O2. Anesthesia was maintained with a mixture of 2% isoflurane in O2 inside the imaging chamber. Using Living Image (PerkinElmer, Waltham, MA), images were acquired (Exposure time, auto; F stop. 1.2; Binning, medium) from both dorsal and ventral sides of mice and a total photon flux (p/sec/cm2/sr) per animal was calculated by averaging the signal acquired from the dorsal and ventral side. After 4 weeks, surviving mice were sacrificed and lungs snap frozen in liquid N2 prior to homogenization in TRIzol for RNA extraction.
Metabolite Profiling and Mass Spectrometry
For total metabolite analysis, parental and metastatic cell lines were seeded in 60mm culture dishes in DMEM/F12 supplemented with 10% dialyzed fetal bovine serum. Media was refreshed 2 hours prior to harvesting by washing 3x with PBS before quenching with 800mL of −80 C 80:20 methanol:water. Extracts were spun down, supernatants collected, dried and resuspended in water before LC-MS analysis. Samples were analyzed by reversed-phase ion-pairing chromatography coupled with negative-mode electrospray-ionization high-resolution MS on a stand-alone ThermoElectron Exactive orbitrap mass spectrometer (18). Peak picking and quantification were conducted using MAVEN analysis software. Heatmap was generated in R. Multiple testing correction and q-value generation were performed in PRISM software (GraphPad).
For [2,3,3-2H]serine labeling experiments, parental and metastatic cells were cultured in RPMI medium lacking glucose, serine, and glycine (TEKnova) supplemented with 2 g/L glucose and 0.03 g/L [2,3,3-2H]serine (Cambridge Isotope Laboratories) for up to 24 hours before harvesting. Cells were washed twice with ice-cold PBS prior to extraction with 400 μL of 80:20 acetonitrile:water over ice for 15 min. Cells were scraped off plates to be collected with supernatants, sonicated for 30s, then spun down at 1.5 × 104 RPM for 10 min. 200 μL of supernatant was taken out for LC-MS/MS analysis immediately.
Quantitative LC-ESI-MS/MS analysis of [2,3,3-2H]serine-labeled cell extracts was performed using an Agilent 1290 UHPLC system equipped with an Agilent 6545 Q-TOF mass spectrometer (Santa Clara, CA, US). A hydrophilic interaction chromatography method (HILIC) with an BEH amide column (100 × 2.1 mm i.d., 1.7 μm; Waters) was used for compound separation at 35 °C with a flow rate of 0.3ml/min. The mobile phase A consisted of 25 mM ammonium acetate and 25mM ammonium hydroxide in water and mobile phase B was acetonitrile. The gradient elution was 0–1 min, 85 % B; 1–12 min, 85 % B → 65 % B; 12– 12.2 min, 65 % B-40%B; 12.2–15 min, 40%B. After the gradient, the column was re-equilibrated at 85%B for 5min. The overall runtime was 20 min and the injection volume was 5 μL. Agilent Q-TOF was operated in negative mode and the relevant parameters were as listed: ion spray voltage, 3500 V; nozzle voltage, 1000 V; fragmentor voltage, 125 V; drying gas flow, 11 L/min; capillary temperature, 325 °C, drying gas temperature, 350 °C; and nebulizer pressure, 40 psi. A full scan range was set at 50 to 1600 (m/z). The reference masses were 119.0363 and 980.0164. The acquisition rate was 2 spectra/s. Isotopologues extraction was performed in Agilent Profinder B.08.00 (Agilent Technologies). Retention time (RT) of each metabolite was determined by authentic standards (Supplementary Table S1). The mass tolerance was set to +/−15 ppm and RT tolerance was +/− 0.2 min. Natural isotope abundance was corrected using Agilent Profinder software (Agilent Technologies).
Cell Line Classification
Cell line expression and copy number data were downloaded from the COSMIC cell line dataset (https://cancer.sanger.ac.uk/cell_lines), and all cell lines were classified using different cell line classifiers, including PAM50 and scmod2 using the package genefu from Bioconductor; and iC10 using package iC10 (19–22). The MDA-MB-231 parental and metastatic subclones were classified as Basal (posterior probability of 0.516), ER-Her2- (posterior probability of 0.997), IC4 (posterior probability of 0.999).
Outcome Analysis
METABRIC clinical and expression data was downloaded from EGA (EGAS00000000083) (21). Outcome analysis was performed in IC4 samples only (N=342) in order to mimic the phenotype of the MDA-MB-231 breast cancer cell line. Survival analysis was performed over disease specific survival (DSS) censored to 20 years. Gene high/low categorization was performed using the maxstat algorithm, which determines the optimal threshold for separating high and low expression (from the surv cutpoint function of package survminer). Cox Proportional Hazard multivariate models use continuous expression adjusted by age, grade, size, number of lymph nodes, ER, PR and Her2 status. Kaplan-Meier plots were generated using the package survcomp, and Cox Proportional Hazards were generated using the package rms.
Immunohistochemical Staining and Quantification for SHMT2
Human primary breast cancer tissue and paired lymph node metastases were obtained from Biomax.us. Tumors were graded by Biomax.us pathologists according to the Nottingham grading system with respect to degree of glandular duct formation, nuclear pleomorphism, and nuclear fission counting. Each feature was scored from 1–3, and the total score was used to determine the following grades: Grade 1 (total score 3–5; low grade or well differentiated), Grade 2 (total score 6–7; intermediate grade or moderately differentiated), Grade 3 (total score 8–9; high grade or poorly differentiated). Standard immunohistochemical methods were performed as previously described (23). The primary anti-human SHMT2 antibody (Sigma) was used at a concentration of 1:3000. Images were acquired on a Leica DMi8 system (Leica Microsystems) and quantified for positive SHMT2 signal intensity by ImageJ software.
SHMT2 Expression Analysis by Individual Cancer Stage
SHMT2 expression data across every annotated TCGA cancer data set was queried and downloaded from the UALCAN database (http://ualcan.path.uab.edu/index.html) (24).
Statistical Analyses
All statistical tests were performed using the paired or unpaired Student’s t test by PRISM software. Values with a p value of < 0.05 were considered significant.
Results
Metastatic breast cancer cells exhibit altered metabolic profiles
To identify common metabolic pathways reprogrammed in metastatic breast cancer cells during cancer progression, we performed metabolomic profiling of the human triple negative breast cancer cell line MDA-MB-231 and its metastatic subpopulations (Fig. 1A and andB).B). This cell line was derived from the pleural effusion of a patient with widespread metastatic disease years after primary tumor removal (25), and the subclones of this cell line with higher metastasis rate and preference to the bone, lung, or brain were previously isolated by in vivo selection (15–17) (831-BrM: brain metastasis. 1833-BoM: bone metastasis. 4175-LM: lung metastasis).

Metastatic breast cancer subclones display an altered metabolic profile. (A) Schematic of targeted metabolomics workflow. Brain (831-BrM), bone (1833-BoM), and lung (4175-LM) metastatic subclones from tissue-tropic subpopulations were generated following IV injection of a parental population of MDA-MB-231 (231-Parental) cells into the tail vein or heart. Stable cell lines were passaged in culture prior to metabolite extraction for LC-MS/MS. (B) LC-MS profile of the 231-Parental, 831-BrM, and 1833-BoM cell lines. Cell lines were plated in biological triplicates prior to metabolite extraction. Signals were normalized to the mean signal of each metabolite across all samples, log2 transformed, and clustered.
At the time of initial metabolomics comparison, the lung metastatic subclone 4175-LM did not recover well in culture, so we profiled the 831-BrM and 1833-BoM metastatic subclones along with the parental population. We observed multiple metabolites involved in a plethora of metabolic pathways that were differentially enriched or depleted in the metastatic 831-BrM and 1833-BoM subclones compared to the parental population of MDA-MB-231 (231-Parental) cells (Fig. 1B). Following correction for false discovery rate, the levels of twenty-four metabolites were significantly altered in both 831-BrM and 1833-BoM cells compared to 231-Parental cells (Supplementary Table S2). Metabolites significantly enriched in metastatic subclones included the glycolytic intermediate dihydroxyacetone-phosphate (which is reversibly isomerized to glyceraldehyde-3-phosphate), the tricarboxylic acid (TCA) cycle intermediate succinate, amino acids such as proline and asparagine, and the pentose-phosphate pathway product 5-phosphoribosyl-1-pyrophosphate. These observations are consistent with prior observations of perturbations in lower glycolysis and the TCA cycle observed in other cell line models (notably murine 4T1 cells), suggesting common metabolic developments during metastasis of breast cancers in both mice and humans (1–3,5,6). Additionally, enrichment of asparagine has been reported to promote metastatic cancer cell phenotypes by epithelial-to-mesenchymal transition (8). Nonetheless, the most significantly depleted class of metabolites in 831-BrM and 1833-BoM cells compared to 231-Parental cells were free purine nucleotides, suggesting alterations in purine metabolism in metastatic cells (Fig. 1B).
c-Myc is important for breast cancer cell proliferation
We wondered whether reduced levels of purines reflected decreased synthesis or higher consumption in the metastatic subclones. Because it was previously reported that the oncogenic transcription factor c-Myc induces the expression of nucleotide biosynthesis genes and that c-Myc amplification and overexpression is a common event in triple-negative breast cancer (26–28), we wondered if the relative differences in purine abundance could be explained by altered c-Myc protein levels in our cell line system. Indeed, 831-BrM, 1833-BoM, and 4175-LM cells overexpressed c-Myc compared to 231-Parental cells (Fig. 2A). Since sufficiency of free nucleotides can act as an important checkpoint for cell division (29), we then compared the proliferation rates of parental and metastatic subclones. Accordingly, 831-BrM, 1833-BoM, and 4175-LM cells proliferated faster than 231-Parental cells in vitro (Fig. 2B), suggesting that the higher consumption rate is the cause of lower purine levels in the metastatic subclones.

c-Myc drives proliferation in metastatic breast cancer cell subclones. (A) IB for c-Myc from whole-cell extracts of parental and metastatic subclones. (B) Proliferation of parental cells and metastatic subclones over 3 days (mean ± SD, n = 3). (C) 3 day proliferation of 231-Parental, 831-BrM, 1833-BoM, and 4175-LM cells expressing either a nontargeting (shNT) or c-Myc targeting (shMyc) vectors. (mean ± SD, n = 3).
Because the role of c-Myc in metastasis is still unclear, with evidence suggesting it plays both pro-metastatic and anti-metastatic functions in breast cancer depending on the genetic context (30,31), we tested the sensitivity of parental and metastatic subclones to c-Myc inhibition. Small hairpin RNA (shRNA)–mediated knockdown of c-Myc reduced cell proliferation in all four cell lines, although the degree of inhibition was stronger in 831-BrM and 1833-BoM cells (Fig. 2C, Supplementary Fig. S1). Parental cells expressing a non-targeting shRNA showed elevated c-Myc expression, possibly due to puromycin selection. These data suggest that c-Myc is an important mediator of cell proliferation, and c-Myc overexpression provided a proliferative advantage at least in brain and bone-metastatic subclones.
Identification of serine and one-carbon unit pathway elevation in metastatic subclones
The products of several metabolic pathways feed into nucleotide synthesis, including ribulose-5-phosphate from the pentose phosphate pathway, and one-carbon (1C) units and glycine from the serine and 1C unit pathway. It is also known that c-Myc can promote the expression of serine and glycine metabolism genes in cancer cells (32,33). We performed expression analyses of the metastatic subclones and found elevated levels of the key mitochondrial enzymes serine hydroxymethyltransferase 2 (SHMT2), methylenetetrahydrofolate dehydrogenase 2 (MTHFD2), and methylenetetrahydrofolate dehydrogenase 1-like (MTHFD1L), in contrast to the downregulated expression of the cytosolic isoenzyme serine hydroxymethyltransferase 1 (SHMT1) (Fig. 3A–C). Consistent with previous reports in other cell types, knockdown of c-Myc in parental and metastatic breast cancer subclones diminished MTHFD2 and MTHFD1L protein expression, suggesting these enzymes are c-Myc-regulated (Supplementary Fig. S1). SHMT2 expression did not reduce upon c-Myc knockdown, suggesting that SHMT2 expression was regulated by other transcription factors. To determine whether c-Myc and mitochondrial 1C unit pathway enzyme overexpression was a common co-occurrence in other cancer metastasis models, we checked protein expression levels in the parental and metastatic subpopulations of other human cell line systems derived from lung adenocarcinoma or ER+ breast carcinoma patients (34,35). There was a clear correlation of SHMT2, MTHFD2, and MTHFD1L expression with c-Myc expression among all the cell lines tested. The brain metastatic subclones of lung adnocacinoma cell lines PC9 and H2030 had increased MTHFD2 expression, though we could not find another system that also displayed overexpression of c-Myc and all the three mitochondrial 1C unit pathway enzymes in metastatic subclones relative to their corresponding parental cells (Supplementary Fig. S2). Taken together with the observations of higher serine and glycine levels in 831-BrM and 1833-BoM cells compared to 231-Parental cells (Fig. 1B), these data suggest that the role of c-Myc in regulating mitochondrial serine and 1C unit metabolism in metastatic cancer may be tissue-specific.

The mitochondrial serine and one-carbon unit pathway is upregulated in metastatic breast cancer subclones. (A) Schematic of the cytosolic and mitochondrial serine and one-carbon unit pathway. (B) qPCR for serine and one-carbon unit pathway genes (mean ± SD, n = 3, *P < 0.05 **P < 0.01 ***P < 0.001 ****P < 0.0001 by two-tailed Student’s t test, compared to expression in parental cells). (C) IB for serine and one-carbon unit pathway enzymes from whole-cell extracts of parental cells and metastatic subclones. (D) Schematic diagram of incorporation of 2H (D) from [2,3,3-2H]serine onto glycine, one-carbon units, and purines. (E) SHMT flux estimated by relative abundance of labeled glycine from serine (mean ± SD, n = 3, **P < 0.01 by two-tailed Student’s t test). (F) Fractional labeling of [2,3,3-2H]serine onto GTP and ATP (mean ± SD, n = 3, *P < 0.05 **P < 0.01 ***P < 0.001 by two-tailed Student’s t test).
Metastatic subclones display increased mitochondrial serine and one-carbon unit pathway activity
We next asked if higher expression of mitochondrial serine and 1C unit pathway enzymes might indeed reflect higher pathway activity. Serine can be catabolized in both the mitochondrial and cytosolic branch of the 1C unit pathway. Since cancer cells predominately express the mitochondrial serine catabolic enzymes over the cytosolic enzymes, serine is generally catabolized in the mitochondria in cancer cells (13,14,36). Serine hydroxyl-methyltransferase 2 (SHMT2) initiates this reaction by converting serine to glycine while donating a carbon group to tetrahydrafolate (THF) to generate methylene-THF. Subsequent oxidation of methylene-THF by MTHFD2 and MTHFD1L generates NAD(P)H and formate. Formate can cross the mitochondrial membrane to provide 1C units for anabolic reactions such as nucleotide synthesis (37).
We hypothesized that the reason metastatic cells upregulate the serine and 1C unit pathway is to enhance nucleotide synthesis to fuel cell proliferation. Indeed, most cancer cells have been reported to utilize serine as the predominant source of 1C units for biosynthesis (38). We performed [2,3,3-2H]serine tracing to examine 1C unit pathway flux to glycine and purine nucleotides. In cells grown in media containing [2,3,3-2H]serine, the cytosolic pathway generates methylene-THF (me-THF) mass heavy by 2 (M+2) and 10-formyl-THF mass heavy by 1 (M+1), while 10-formyl-THF derived from mitochondrial formate exchange to the cytosol is strictly M+1. [2,3,3-2H]serine labeling onto the metabolites glycine and purine nucleotide triphosphates produced from the mitochondrial pathway thereby produces glycine M+1 and purines either M+1 or M+2 (Fig. 3D). Time course experiments were performed in 4175-LM cells to determine the optimal steady state labeling conditions for glycine and ATP from serine: 2 hours and 24 hours respectively (Supplementary Fig. S3). We observed higher SHMT flux in metastatic subclones, as the relative abundance of M+1 glycine was approximately 1.5-fold higher in 4175-LM cells compared to 231-Parental cells, indicating that higher purine turnover in metastatic cells was fueled by higher SHMT flux (Fig. 3E). Importantly, while robust fractions of ATP and GTP were labeled in parental cells, the metastatic subclones displayed even higher labeling fractions from serine (Fig. 3F). These results demonstrate that upregulation of serine catabolism through the mitochondrial 1C unit pathway promotes de novo purine synthesis in metastatic breast cancer cells.
Serine catabolism is necessary for metastatic cancer cell proliferation in vitro
To address the extent to which mitochondrial serine catabolism is necessary for cell proliferation, 231-Parental, 831-BrM, 1833-BoM, and 4175-LM cells were infected with lentivirus expressing shRNAs against SHMT2 (shSHMT2) or a nontargeting control (shNT). Intriguingly, knockdown of SHMT2 protein expression with two different shRNAs drastically suppressed proliferation of the metastatic subclones significantly, with a reduced effect in 231-Parental cells (Fig. 4A and andB).B). In contrast, knockdown of the downstream enzyme of the mitochondrial serine and 1C unit pathway, MTHFD2, suppressed proliferation to a lesser extent (Supplementary Fig. S4A and B). To evaluate the therapeutic potential of targeting 1C unit metabolism to block metastatic growth, we treated cells with a small-molecule inhibitor of SHMT called SHIN1 (39). In vitro, metastatic subclones were sensitive to SHIN1 with an EC50 in the 100–500 nM range (Supplementary Fig. S5). There was no obvious enhancement of SHIN1 sensitivity in 831-BrM, 1833-BoM, and 4175-LM cells compared to 231-Parental cells, possibly because SHIN1 inhibits both SHMT2 and SHMT1 (Fig. 4C). Importantly, inhibition of cell proliferation in the presence of SHIN1 could be rescued by the supplementation of formate (2 mM), a source of cellular 1C units (Fig. 4C). These results indicate that the major role of elevated mitochondrial serine catabolism is to generate 1C units for cytosolic purine biosynthesis in the metastatic subclones. Thus, targeting SHMT activity may be a promising way to restrict nucleotide availability to block metastatic breast cancer cell proliferation.

Metastatic subclones are particularly sensitive to SHMT2 inhibition. (A) 3 day proliferation of 231-Parental, 831-BrM,1833-BoM, and 4175-LM cells expressing either a nontargeting (shNT) or SHMT2 targeting (shSHMT2) vectors. Relative proliferation was calculated relative to average proliferation of shNT cells (mean ± SD, n = 3). (B) IB for SHMT2 in parental and metastatic subclones. (C) 3 day proliferation of parental and metastatic cells with 2 μM SHIN1, in RPMI with or without 2 mM formate and dialyzed FBS (mean ± SD, n = 3, ***P < 0.001 ****P < 0.0001 by two-tailed Student’s t test). Counts were normalized to the proliferation of 231-Parental cells in media without SHIN1 and formate treatment. (D) Growth of 4175-LM shNT and shSHMT2 tumors in the mammary fat pad of nude mice (mean ± SEM, n = 8, **P < 0.01 by two-tailed Student’s t test). (E) Quantification of luminescence signal in the lungs of mice 3 weeks post injection of either 4175-LM shNT or shSHMT2 cells (mean ± SEM, **P < 0.01 by two-tailed Student’s t test, shNT;n = 8 shSHMT2;n = 7). (F) qPCR analysis of hGAPDH expression in the lungs of mice 4 weeks post injection of either 4175-LM shNT or shSHMT2 cells (mean ± SEM, *P < 0.05 by two-tailed Student’s t test, shNT;n = 6 shSHMT2;n = 7).
SHMT2 knockdown impairs primary and metastatic growth in vivo
We then interrogated the effect of reducing mitochondrial 1C unit pathway activity in two different models of cancer growth in vivo. 4175-LM cells were chosen due to the relative ease of monitoring, measuring, and collecting tissue from lung metastasis compared to brain and bone metastasis. For the first model, we monitored breast cancer growth at the primary tumor site. SHMT2 knockdown significantly impaired the growth of 4175-LM cells in the mammary fat pads of immunodeficient mice (Fig. 4D, Supplementary Fig. S6). For the second model, we induced breast cancer metastasis to the lung by intravenous tail vein injection. Because 4175-LM cells express firefly luciferase (16), we tracked tumor growth in the lung by bioluminescence imaging (BLI). Both BLI and quantification of human GAPDH (hGAPDH) expression from resected mouse lungs revealed a roughly two-fold reduction of lung tumor burden in mice injected with shSHMT2 cells compared to shNT cells (Fig. 4E and andF,F, Supplementary Fig. S7A). While on average, shSHMT2 tumors had reduced human SHMT2 (hSHMT2) expression compared to shNT tumors, some shSHMT2 tumors appeared to have reacquired hSHMT2 expression (Supplementary Fig. S7B and C). These data suggest that SHMT2 is necessary for metastatic growth in vivo.
Mitochondrial serine and 1C unit pathway genes are associated with more aggressive metastatic disease in some human breast cancer patients
To further explore the relevancy of mitochondrial one-carbon unit metabolism in human breast cancer metastasis, we examined the expression of SHMT1, SHMT2, MTHFD2, and MTHFD1L in the METABRIC dataset of human breast cancer patients (21). We retrospectively inferred metastatic recurrence in patients by examining the frequency of disease-specific survival (DSS) up to 20 years. Patients were separated into two groups based on the maxstat algorithm (see Materials and Methods). Patients with high SHMT2 expression were significantly more likely to succumb to metastatic recurrent disease, while patients with high expression of the cytosolic isozyme SHMT1 were significantly protected from metastatic relapse (Fig. 5A, Supplementary Fig. S8). Using three different breast cancer subtype clustering analyses based on gene expression (PAM50, IC10, SCMOD2), we classified the MDA-MB-231 cell line as basal, IC4 (copy number flat), and ER−Her2− (20,21). We have previously described IC4 as consisting of a mixture of ER− tumors with lymphocytic infiltration and ER+ tumors with abundant stroma. Accordingly, further analysis of the IC4 patient subgroup following adjustment for covariates of age, grade, size, number of lymph nodes, ER, PR and Her2 status revealed a significant association of MTHFD1, MTHFD1L, MTHFD2, and SHMT2 expression with worse survival and SHMT1 expression with better survival (Fig. 5B). Finally, we stained a tissue microarray panel of human breast invasive ductal carcinoma and matched lymph node metastases and found significantly higher expression of SHMT2 in metastatic cancer cells comparing to the primary tumors (Fig. 5C and andD).D). Together, these data suggest that SHMT2 and other mitochondrial 1C unit pathway enzymes may be used as prognostic markers that indicate worse patient outcome, while cytosolic SHMT1 expression may indicate better survival rate in the IC4 patient subgroup.

Mitochondrial serine and one-carbon unit pathway enzyme expression correlates with poor survival in human breast cancer. (A) Kaplan-Meier plot for SHMT1 (left) and SHMT2 (right) expression associated with disease-specific survival (DSS) in the human IC4 patient subgroup (METABRIC). (B) Forest plot for the hazard of individual 1C unit pathway genes adjusted for covariates (age, grade, size, number of lymph nodes, ER, PR and Her2 status) in the IC4 subgroup (n=343). (C) Representative SHMT2 staining (at 40x) of human breast invasive ductal carcinoma and matched metastatic carcinoma tissue samples (LN = lymph node). (D) Quantification of SHMT2 intensity by IHC in metastatic lesions compared to primary tumors (mean ± SD, n = 33 per group, *P < 0.05 by two-tailed Student’s t test).
Relevance of SHMT2 expression in the progression and aggressiveness of other cancer types
To evaluate the contribution of mitochondrial 1C unit metabolism to the progression of other cancer types, we queried SHMT2 expression in TCGA datasets through the UALCAN portal (24). In addition to breast invasive carcinoma (BRCA), we identified adrenocortical carcinoma (ACC), head and neck squamous cell carcinoma (HNSC), kidney chromophobe cell carcinoma (KICH), and kidney renal papillary cell carcinoma (KIRP) as cancer types in which SHMT2 expression progressively increased as a function of stage (Fig. 6). Notably, gain of SHMT2 expression in BRCA and HNSC tended to occur early on in cancer progression, whereas in KICH, SHMT2 upregulation may occur only during the very late stage. A few cancer types such as mesothelioma (MESO) and ovarian serous cystadenocarcinoma (OV) showed the opposite trend: a progressive loss of SHMT2 expression with increasing cancer stage (Supplementary Fig. 9). Collectively, these data present the possibility that there exist additional cancer types in which mitochondrial 1C unit metabolism promotes progression and aggressiveness.

Box plots depicting the average expression level (transcripts per million) of SHMT2 in normal tissue (N) and as a function of cancer stage (stage 1 = S1; stage 2 = S2; stage 3 = S4; stage 4 = S4). Statistically significant differences between pairwise comparisons are highlighted in red. Abbreviations for cancer types are explained as follows: ACC (adrenocortical carcinoma), BRCA (breast invasive carcinoma), HNSCC (head and neck squamous cell carcinoma), KICH (kidney chromophobe carcinoma), KIRP (kidney renal papillary cell carcinoma).
Discussion
For breast cancer, common metastatic sites include the brain, bone, liver, and lung. At the cellular level, the original heterogeneous population of cancer cells from the primary tumor undergo a selection process whereby those clones with alterations (carrying both genetic lesions and epigenetic modifications) favoring fitness and plasticity are enriched. These adaptations, in turn, equip cells with the ability to withstand standard treatments such as chemotherapy and radiation therapy, ultimately leading to cancer progression and metastatic recurrence (40). While many previous studies have elucidated a role for molecular processes such as epithelial to mesenchymal transition and invasion and migration of cancer cells, our understanding of how metabolic pathway alterations shape metastatic growth is still limited. It is important to note that the MDA-MB-231 cells we studied were isolated from a pleural population that already metastasizes well in vivo. Our metabolomics profiling of the even more highly metastatic triple-negative breast cancer subclones suggested alterations in both glycolysis and the TCA cycle during the late stages of cancer progression, consistent with findings from other groups of heightened mitochondrial metabolism in metastatic cells (2,3,5,6). We further discovered elevated catabolism of serine in the mitochondria of our metastatic subclones. A previous study in isogenic murine 4T1 breast cancer cell lines found that transformed cells showed higher levels of nucleotides than nontransformed cells, and that “more metastatic” lines had even more nucleotides than “less metastatic” ones (1). In contrast, we found lower levels of free purines in metastatic variants of human MDA-MB-231 cell lines compared to the parental population (Fig. 1B). This discrepancy may be attributed to different oncogenic contexts in 4T1 cells versus MDA-MB-231 cells or inherent differences in purine metabolism between murine and human cells. Due to the difficulty of obtaining pure metastatic tumor tissue from in vivo studies, the metabolomic analysis were performed using established cell lines in vitro. Microenvironmental factors from metastatic niche, such as hypoxia and nutrient starvation, also regulate cancer cell metabolism. Since mitochondrial 1C unit metabolism can utilize both NAD+ and NADP+, cancer cells with upregulation of mitochondrial 1C unit metabolism may gain metabolic flexibility to sustain proliferation under stress conditions. When cells engage active respiration, the mitochondrial 1C unit pathway can utilize NAD+ to generate 1C units; under hypoxia or starvation conditions, when the NAD+/NADH ratio decreases, elevated mitochondrial ROS leads to an increased NADP+/NADPH ratio, which can also drive the 1C unit pathway and purine synthesis. Further investigations comparing the metabolic profile changes under these stress conditions may provide more insight into potential links between metabolic stresses and the evolution of metastatic cancer cells.
The role of serine in cancer growth has drawn increasing interest over the years ever since the identification of PHGDH amplifications in melanoma and breast cancer (9,10). A variety of mechanisms have been proposed to explain why increased serine synthesis and serine catabolism could promote tumorigenesis, including rerouting glucose carbon flux, maintenance of compartment-specific NAD(P)+/NAD(P)H ratios, and the control of metabolites such as acetyl-coA, α-ketoglutarate, or 2-hydroxyglutarate (12,41,42). Moreover, a previous study had implicated SHMT2 and a neutral amino acid importer of serine and glycine (ASCT2) as prognostic biomarkers for breast cancer (43). Our study is the first to directly evaluate the therapeutic potential of targeting SHMT2 in metastatic breast cancer using both genetic and pharmaceutical approaches. Intriguingly, genetic knockdown of SHMT2 strongly inhibited the proliferation of metastatic cells, while treatment with a dual SHMT1/SHMT2 inhibitor suppressed proliferation of both parental and metastatic subclones. This discrepancy may be explained by prior observations that while MDA-MB-231 cells preferentially utilize the mitochondrial pathway for 1C unit production, inhibition of individual mitochondrial enzymes can lead to a switch to the cytosolic pathway (36). We thus speculate that 231-Parental cells may be more adept at switching to cytosolic serine catabolism, and for reasons still unclear, the metastatic subclones are less flexible. Consistent with observations in colon cancer xenografts (36), SHMT2 knockdown in the lung metastatic subclone slowed, but not completely suppressed, tumor growth in the mammary fat pad and lung. In addition, we found that in the IC4 subset of human breast cancer patients, the expression of mitochondrial one-carbon unit enzymes is positively associated with more aggressive disease. Thus, interrogating the expression status of mitochondrial one-carbon unit enzymes through transcriptional or proteomic methods holds prognostic value in the metastatic setting, and warrants the need for further development of drugs that selectively inhibit serine catabolism for treating the metastasis of triple-negative breast cancer.
What causes the upregulation of mitochondrial serine catabolic flux in highly metastatic cancer cells? We provide evidence that a crucial oncogenic event promotes the ability of metastatic breast cancer subclones to catabolize serine faster than parental cells: c-Myc activation. c-Myc overexpression is known to be associated with up to 40% of breast cancers, with hyperactive c-Myc enriched particularly in the basal-like subtype (27,44). These observations are consistent with our findings of the MDA-MB-231 cell line as basal-like and its metastatic subclones expressing even higher levels of c-Myc than the parental population (Fig. 2A). We found that c-Myc was required for the maintenance of the mitochondrial serine and 1C unit pathway genes MTHFD2 and MTHFD1L, consistent with previous reports that c-Myc supports serine/glycine metabolism at the transcriptional level in other cell types (32,33). These results suggest a model for breast cancer metastasis in which a small fraction of c-Mychigh expressing cells from the primary tumor acquire the ability to upregulate serine catabolism to fuel growth in metastatic tissue sites. Alternatively, high c-Myc expression and the linked ability to upregulate serine catabolism may be intrinsic properties of stem-like metastasis-initiating cells that are enriched in breast cancer cell populations selected for high metastatic activity in mice. As one of the key oncogenic transcription factors, there is increasing evidence that c-Myc plays multiple roles during the metastatic process. c-Myc knockdown reduces invasion and migration of MDA-MB-231 cells (30). Moreover, a recent study corroborated our findings of elevated c-Myc levels in brain-metastatic derivatives of human breast cancer cells and demonstrated its necessity for the invasive growth of brain metastases (45). Our study highlights the role of c-Myc in enhancing 1C unit pathway activity and proliferation, which is also important for metastatic growth. Since SHMT2 expression was not reduced by c-Myc shRNA, it is likely that other tumor-promoting factors, such as ATF4 and NRF2, also play important roles in late stage cancer progression by modulating 1C unit metabolism. Intriguingly, a recent report showed that TGF-β signaling induces the expression of SHMT2 (46). Given the critical role of TGF-β in promoting metastasis (47,48), it may be interesting to further investigate whether serine and 1C unit pathway metabolic reprogramming is controlled by TGF-ß signaling in metastatic subpopulations of human breast cancer cells.











































{kind=link}
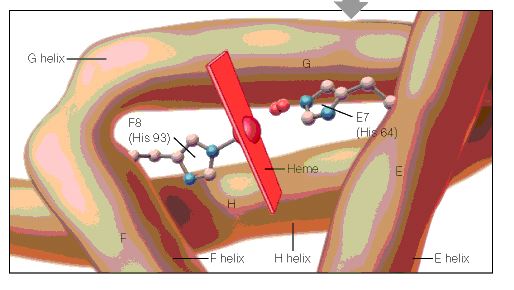{kind=link}
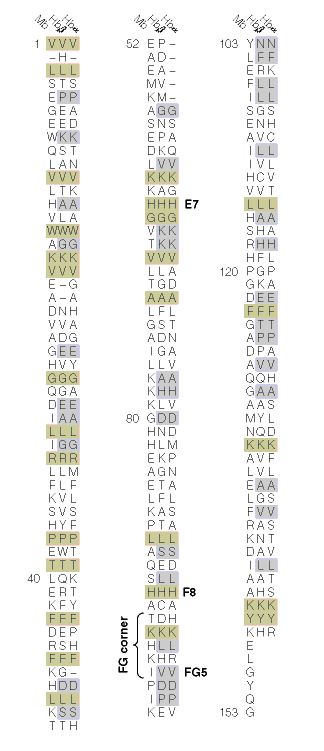{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}