Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
This is the first volume of the Series D: e-Books on BioMedicine – Metabolomics, Immunology, Infectious Diseases. It is written for comprehension at the third year medical student level, or as a reference for licensing board exams, but it is also written for the education of a first time bachalaureate degree reader in the biological sciences. Hopefully, it can be read with great interest by the undergraduate student who is undecided in the choice of a career.
In the Preface, I failed to disclose that the term Metabolomics applies to plants, animals, bacteria, and both prokaryotes and eukaryotes. The metabolome for each organism is unique, but from an evolutionary perspective has metabolic pathways in common, and expressed in concert with the environment that these living creatures exist. The metabolome of each has adaptive accommodation with suppression and activation of pathways that are functional and necessary in balance, for its existence. Was it William Faulkner who said in his Nobel Prize acceptance that mankind shall not merely exist, but survive? That seems to be the overlying theme for all of life. If life cannot persist, a surviving “remnant” might continue. The history of life may well be etched into the genetic code, some of which is not expressed.
This work is apportioned into chapters in a sequence that is first directed at the major sources for the energy and the structure of life, in the carbohydrates, lipids, and fats, which are sourced from both plants and animals, and depending on their balance, results in an equilibrium, and a disequilibrium we refer to as disease. There is also a need to consider the nonorganic essentials which are derived from the soil, from water, and from the energy of the sun and the air we breathe, or in the case of water-bound metabolomes, dissolved gases.
In addition to the basic essential nutrients and their metabolic utilization, they are under cellular metabolic regulation that is tied to signaling pathways. In addition, the genetic expression of the organism is under regulatory control by the interaction of RNAs that interact with the chromatin genetic framework, with exosomes, and with protein modulators.This is referred to as epigenetics, but there are also drivers of metabolism that are shaped by the interactions between enzymes and substartes, and are related to the tertiary structure of a protein. The framework for diseases in a separate chapter. Pharmaceutical interventions that are designed to modulate specific metabolic targets are addressed as the pathways are unfolded. Neutraceuticals and plant based nutrition are covered in Chapter 8.
Chapter 1: Metabolic Pathways
Chapter 2. Lipid Metabolism
Chapter 3. Cell Signaling
Chapter 4. Protein Synthesis and Degradation
Chapter 5: Sub-cellular Structure
Chapter 6: Proteomics
Chapter 7: Metabolomics
Chapter 8. Impairments in Pathological States: Endocrine Disorders; Stress Hypermetabolism and Cancer
With help from the zebrafish, a team of Australian researchers has uncovered how hematopoietic stem cells (HSC) renew themselves.
HSCs refers to stem cells present in the blood and bone marrow that are used for the replenishment of the body’s supply of blood and immune cells –
in transplants for leukemia and myeloma.
Stem cells have the potential to transform into vital cells
including muscle, bone, and blood vessels.
Understanding how HSCs form and renew themselves has potential application in the treatment of
spinal cord injuries
degenerative disorders
diabetes.
Professor Peter Currie, of the Australian Regen Med Institute at Victoria’s Monash University, led a research team to discover a crucial part of HSC’s development. Using a high-resolution microscopy, Prof. Curie’s team
caught zebrafish embyonic SCs on film as they formed.
the researchers were studying muscle mutations in the aquatic animal.
“Zebrafish make ESCs in exactly the same way as humans do, but their embryos and larvae develop free living, but the larvae are both free swimming and transparent, so one could see every cell in the body forming, including ESCs,” explained Prof. Currie.
The researchers noticed in films that a
‘buddy cell’ came along to help the ESCs form.
Called endotome cells,
they aided pre-ESCs to turn into ESCs.
Prof. Currie said that endotome cells act as helper cells for pre-ESCs ,
helping them progress to become fully fledged stem cells.
The team not only
identified some of the cells and signals
required for ESC formation, but also
pinpointed the genes required
for endotome formation in the first place.
The next step for the researchers is to
locate the signals present in the endotome cells
that trigger ESC formation in the embryo.
This may provide clues for developing
specific blood cells on demand for blood-related disorders.
Professor Currie also pointed out the discovery’s potential for
correcting genetic defects in the cell and
transplanting them back in the body to treat disorders.
The team’s work was published in the international journal Nature.
Jell-O Like Biomaterial Could Hold Key to Cancer Cell Destruction
by Estel Grace Masangkay
Scientists from Penn State University reported that a biomaterial made of tiny molecules was able to attract and destroy cancer cells.
Professor Yong Wang and bioengineering faculty at Penn State, built the tissue-like biomaterial to accomplish what chemotherapy could not –
kill every cancer cell without leaving
the possibility of a recurrence.
Prof. Wang and team built polymers
from tiny molecules called monomers. They
then wove the polymers into 3D networks
called hydrogels. Hydrogel is soft and flexible, like Jell-O, and it contains a lot of water, and
can be safely put into the body, unlike
other implants that the body often tries
to get rid of through the immune response.
“We want to make sure the materials we are using are compatible in the body.”
The researchers
attached aptamers to the hydrogels,
which release bio-chemical signal-only molecules
that draw in cancer cells.
Once attracted, the cancer cells are entrapped in the Jell-O-like substance.
What happens next is
an oligonucleotide binds to the protein-binding site of the aptamer
and triggers the release of anticancer drugs at the proper time.
“Once we trap the cancer cells, we can deliver anticancer drugs
to that specific location to kill them.
This technique would help avoid the need for systemic medications that kill not only cancer cells, but normal cells as well. Systemic chemotherapy drugs
make patients devastatingly sick and possibly
leave behind cancer cells to wreak havoc another day
If our new technique has any side effects at all, it would be only local side effects and not whole-body systemic side effects,” explained Prof. Wang.
The initial results of the research were published by Prof. Wang in the Journal of the American Chemical Society in 2012. Prof. Wang also shared the latest results of his work at the Society for Biomaterials Meeting & Exposition in April this year.
There is an explosion of work-in-progress in applications to regenerative medicine using inducible pluripotent stem cells in both endothelial and cardiomyocyte postischemic repair, and also in post bone marrow radiation restoration, with benefits and hazards. The following article is quite novel in that it deals with stem cell regulation by DNA methylation. Therefore, it deals with the essentiality of methylation of DNA in epigenetic regulation.
This is the fourth discussion of a several part series leading from the genome, to protein synthesis (1), posttranslational modification of proteins (2), examples of protein effects on metabolism and signaling pathways (3), and leading to disruption of signaling pathways in disease (4), and effects leading to mutagenesis.
Posttranslational modification is a step in protein biosynthesis. Proteins are created by ribosomes translating mRNA into polypeptide chains. These polypeptide chains undergo
PTM before becoming the mature protein product.
Regulation of somatic stem cell Function by DNA Methylation and Genomic Imprinting
Mo Li1, Na Young Kim1, Shigeo Masuda1 and Juan Carlos izpisua Belmonte1,2 1Salk institute for Biological Studies, 10010 N Torrey Pines Rd, La Jolla, CA 92037, USA. 2Center of Regenerative Medicine in Barcelona, Dr Aiguader, 88, 08003 Barcelona, Spain. Corresponding author email: mli@salk.edu
Epigenetic regulation is essential for self-renewal and differentiation of somatic stem cells, including
hematopoietic stem cells (HSCs) and
neural stem cells (NSCs).
The role of DNA methylation, a key epigenetic pathway,
in regulating somatic stem cell function
under physiological conditions and during aging
has been intensively investigated.
Accumulating evidence highlights the dynamic nature of
the DNAmethylome
during lineage commitment of somatic stem cells and
the pivotal role of DNAmethyltransferases in
stem cell self-renewal and differentiation.
Recent studies on genomic imprinting have shed light on
the imprinted gene network (IGN) in somatic stem cells,
where a subset of imprinted genes remain expressed and
are important for maintaining self-renewal of these cells.
Together with emerging technologies, elucidation of the epigenetic mechanisms regulating somatic stem cells with normal or pathological functions may contribute to the development of regenerative medicine.
In adult animals, somatic stem cells (also known as adult stem cells) are responsible for maintaining tissue homeostasis and participate in tissue regeneration under injury conditions. Self-renewal and differentiation are two important aspects of somatic stem cell function. Epigenetic mechanisms underlying these processes have been intensively investigated. With the increasing ability
to identify and manipulate somatic stem cell populations from diverse tissues,
it is possible to dissect the epigenetic pathways that are
either unique for a specific tissue or
universally important in regulating stemness and differentiation.
Epigenetic control of somatic stem cell function exists at various levels, including
DNA methylation,
histone modification, and
higher-order chromatin structure dynamics.
Here, we focus on recent progress in our understanding of how
DNA methylation regulates somatic stem cell function.
DNA Methylation and stem cell Function
The role of DNA methylation in somatic stem cell compartments has gained increasing attention. Recent evidence has shown that
DNA methylation is dynamically regulated during somatic stem cell differentiation and aging.1
A study of methylomes of human hematopoietic stem cells (HSCs) and two mature hematopoietic lineages,
including B cells and neutrophils, showed that
hypomethylated regions of lineage-specific genes often become methylated in opposing lineages, and that
progenitors display an intermediate methylation pattern
that is poised for lineage-specific resolution.2
Another study compared genome-wide promoter DNA methylation in human cord blood hematopoietic progenitor cells (HPCs) with
that in mobilized peripheral blood HPCs from aged individuals.
It was found that aged HPCs lose DNA methylation in a subset of genes that are hypomethylated in differentiated myeloid cells and
gain de novo DNA methylation at polycomb repressive complex 2 (PRC2) target sites.3
It was hypothesized that such epigenetic changes contribute to age-related loss of HSC function, such as a bias toward myeloid lineages. Recently, Beerman et al. studied the global DNA methylation landscape of HSCs in the context of
age-associated decline of HSC function.4
Over- all, the DNA methylation landscape remains stable during HSC ontogeny. However, HSCs isolated from old mice display higher global DNA methylation. Interestingly, they observed
localized DNA methylation changes in genomic regions associated with hematopoietic lineage differentiation.
These methylation changes preferentially map to genes
that are expressed in downstream progenitor and effector cells.
For example, genes that are important for the lymphoid and erythroid lineages
become methylated in “old” HSCs,
which is consistent with
the decline of lymphopoiesis and erythropoiesis during aging.
Additionally, inducing HSC proliferation by 5-fluorouracil treatment or
by limiting the number of transplantedHSCs
recapitulates the functional decline and DNA methylation changes during physiological aging.
A closer examination of the overlapping genes with significant DNA methylation changes during aging or enforced proliferation showed
an enrichment of DNA hypermethylation at PRC2 target loci,
echoing the observation by Bocker et al. in human HSCs.
Interestingly, a recent report showed that epigenetic alterations such as DNA hypermethylation that are accrued during aging,
can be fully reset by somatic reprogramming,
raising an interesting possibility that these aging-related epigenetic defects may be reserved by small molecules.5
Methylation of cytosines at CpG dinucleotides is catalyzed by three key enzymes.
DNA (cytosine-5)- methyltransferase 1 (DNMT1) is responsible for maintaining DNA methylation patterns during DNA replication
by methylating the newly synthesized hemi-methylated DNA.
The other two DNA methyltransferases, DNMT3a and DNMT3b,
are not DNA replication-dependent and can methylate fully unmethylated DNA de novo.
They are responsible for establishing new DNA methylation patterns during development.
DNMT3a, a gene required for neurogenesis,
is expressed in postnatal neural stem cells (NSCs).
In NSCs, DNMT3a methylates non-proximal promoter regions, such as gene bodies and intergenic regions. Surprisingly, rather than silencing gene expression,
DNMT3a-mediated DNA methylation in gene bodies antagonizes Polycomb-dependent repression and
facilitates the expression of neurogenic genes.6
The role of DNMT3a in HSCs has also been investigated. Both Dnmt3a and Dnmt3b are expressed in HSCs. An earlier study did not identify any defects in HSC function when Dnmt3a or Dnmt3b was removed. However,
HSCs lackingboth of these de novomethyltransferases
fail to self-renew, yet retain the capacity to differentiate.7
A more recent study re-examined
the consequences of Dnmt3a loss in HSCs and
uncovered a progressive defect in differentiation that is only manifested during serial transplantation.8
At the molecular level, while Dnmt3a loss results in the expected hypomethylation at some loci,
it counterintuitively causes hypermethylation in even more regions.8
This seemingly paradoxical result echoes the unconventional role of Dnmt3a in transcriptional activation in NSCs (as discussed above). Both cases suggest a more complex regulatory function of DNMT3a that is
beyond simply methylating DNA.
In contrast, the loss of Dnmt1 produces more dramatic and immediate phenotypes in HSCs, manifested
in premature HSC exhaustion and
block of lymphoid differentiation,
highlighting the distinct requirements for different DNA methyltransferases in HSCs.9,10
Genomic Imprinting and stemness
DNA methylation also underlies genomic imprinting, which is an
evolutionarily conserved epigenetic mechanism of ensuring appropriate gene dosage during development.
One allele of the imprinted genes is
epigenetically marked by DNA methylation to be silenced according to the parental origin.
The pattern of imprinting
is established in germ cells and maintained in somatic cells.
Imprinted genes are thought to play critical roles in organismal growth and are relatively downregulated after birth.11 Recently, a series of reports demonstrated that
a subset of imprinted genes belonging to the purported imprinted gene network (IGN)12
remain expressed in somatic stem cells and
are important for maintaining self-renewal of these cells.
Through gene expression profiling, one group identified that several members of the IGNare expressed in
murine muscle,
epidermal, and
long-term hematopoietic stem cells
as well as in human epidermal and hematopoietic stem cells.13
In particular, the paternally expressed gene 3 (Peg3) gene was shown by another group
to mark cycling and quiescent stem cells in a wide variety of mouse tissues.14
The role of imprinted genes in regulating somatic stem cell function has been examined in two types of tissues.
In bronchioalveolar stem cells (BASCs), a lung epithelial stem cell population,
expression of IGN members is required for their self-renewal.
Bmi1, a polycomb repressive complex 1 (PRC1) subunit,
is essential for controlling the expression of imprinted genes in BASCs without affecting their imprinting status.15
In Bmi1 mutant BASCs, many members of the IGN become derepressed,
including p57, H19, Dlk1, Peg3, Ndn, Mest, Gtl2, Grb10, Plagl1, and Igf2.
Knockdown of p57, which is the most differentially expressed imprinted gene between normal and mutant BASCs,
partially rescues the self-renewal defect of lung stem cells.
Interestingly, insufficient levels of p57 also inhibit self-renewal of lung stem cells. Because p57 expression
remains monoallelic in Bmi1 knockdown cells,
Bmi1 is thought to maintain an appropriate level of expression from the expressed allele of p57.15
Another IGN member- delta-like homologue 1 (Dlk1) has been shown to be important for postnatal neurogenesis. Interestingly, in this context,
Dlk1 loses its imprinting in postnatal neural stem cells and niche astrocytes.16
These studies suggest that modulating IGN may represent another
epigenetic mechanism for balancing self-renewal and differentiation in somatic stem cells.
Thus, somatic stem cells either co-opt or remodel these developmental pathways involving the IGN
to fulfill the needs of tissue homeostasis during the adult stage.
In summary, several factors participate in regulating the epigenome of somatic stem cells.
Perturbations in the epigenome of somatic stem cells,
either during organismal aging or under pathological conditions,
will tip the balance between self-renewal and differentiation of somatic stem cells (Fig. 1). A detailed understanding of the mechanisms underlying these changes will likely result in novel therapeutic approaches targeting somatic stem cells.
Figure 1. The epigenome of somatic stem cells is regulated by diverse factors.
Future perspectives The epigenetic mechanisms governing self-renewal and differentiation of somatic stem cells are likely to be complex because of the diverse needs of different tissues. It would be interesting to determine whether a common mechanism, such as the IGN, exists across different somatic stem cells. Additionally, study- ing epigenetic pathways that are specific to one type of somatic stem cell requires the isolation of these cells and their differentiated progeny, which is more practical in model organisms than in humans. Along these lines, developing robust in vitro culture methods for human somatic stem cells and protocols for differentiating these cells into specific lineages are critical for uncovering epigenetic pathways that are unique to human somatic stem cells. In recent years, the field has seen a great improvement in methods of directed differentiation of human embryonic stem cells and induced pluripotent stem cells (iPSCs). For example, it is relatively straightforward to produce high-purity cell populations that resemble neural stem cells or mesenchymal stem cells from iPSCs.17
These methodologies not only are useful for studying the normal function of somatic stem cells, but also provide an exciting opportunity for understanding the role of somatic stem cells in disease pathology and a platform to screen for drugs. A recent study under- scored the usefulness of this approach. Liu et al. studied neural stem cells derived from Parkinson’s disease human iPSCs and uncovered previously unknown defects in nuclear morphology and epigenetic regulation in these derived NSCs.18 The cellular defects only menifest in “aged” neural stem cells, which is consistent with the fact that Parkinson’s disease pri- marily manifests in old age. More importantly, this study identified neural stem cell as a potential target of therapeutic intervention for Parkinson’s disease.
Targeted modification of the human genome is another technological advancement that is on the horizon to greatly facilitate the dissection of epige- netic pathways in somatic stem cells. Although gene targeting in somatic stem cells has been historically challenging, there have been encouraging successful reports following development of new genome-e diting technologies, such as Helper-dependent adenovi- ral vectors, TALENs, and CAS9/CRISPR. With the development of these new technologies, it seems that the stage has been set for a new wave of discoveries in epigenetic mechanisms of somatic stem cells.
References
1. Li M, Liu GH, Izpisua Belmonte JC. Navigating the epigenetic landscape of pluripotent stem cells. Nat Rev Mol Cell Biol. 2012;13(8):524–535.
2. Hodges E, Molaro A, Dos Santos CO, et al. Directional DNA methylation changes and complex intermediate states accompany lineage specificity in the adult hematopoietic compartment. Mol Cell. 2011;44(1):17–28.
3. Bocker MT, Hellwig I, Breiling A, Eckstein V, Ho AD, Lyko F. Genome- wide promoter DNA methylation dynamics of human hematopoietic progen- itor cells during differentiation and aging. Blood. 2011;117(19):e182–e189.
4. Beerman I, Bock C, Garrison BS, et al. Proliferation-dependent alterations of the DNA methylation landscape underlie hematopoietic stem cell aging. Cell Stem Cell. 2013;12(4):413–425.
5. Wahlestedt M, Norddahl GL, Sten G, et al. An epigenetic component of hematopoietic stem cell aging amenable to reprogramming into a young state. Blood. 2013;121(21):4257–4264.
6. Wu H, Coskun V, Tao J, et al. Dnmt3a-dependent nonpromoter DNA methylation facilitates transcription of neurogenic genes. Science. 2010; 329(5990):444–448.
7. Tadokoro Y, Ema H, Okano M, Li E, Nakauchi H. De novo DNA meth- yltransferase is essential for self-renewal, but not for differentiation, in hematopoietic stem cells. J Exp Med. 2007;204(4):715–722.
8. Challen GA, Sun D, Jeong M, et al. Dnmt3a is essential for hematopoietic stem cell differentiation. Nat Genet. 2011;44(1):23–31.
9. Broske AM, Vockentanz L, Kharazi S, et al. DNA methylation protects hematopoietic stem cell multipotency from myeloerythroid restriction. Nat Genet. 2009;41(11):1207–1215.
10. Trowbridge JJ, Snow JW, Kim J, Orkin SH. DNA methyltransferase 1 is essential for and uniquely regulates hematopoietic stem and progenitor cells. Cell Stem Cell. 2009;5(4):442–449.
11. Wood AJ, Oakey RJ. Genomic imprinting in mammals: emerging themes and established theories. PLoS Genet. 2006;2(11):e147.
12. Lui JC, Finkielstain GP, Barnes KM, Baron J. An imprinted gene network that controls mammalian somatic growth is down-regulated during postna- tal growth deceleration in multiple organs. Am J Physiol Regul Integr Comp Physiol. 2008;295(1):R189–R196.
13. Berg JS, Lin KK, Sonnet C, et al. Imprinted genes that regulate early mam- malian growth are coexpressed in somatic stem cells. PLoS One. 2011; 6(10):e26410.
14. Besson V, Smeriglio P, Wegener A, et al. PW1 gene/paternally expressed gene 3 (PW1/Peg3) identifies multiple adult stem and progenitor cell popu- lations. Proc Natl Acad Sci U S A. 2011;108(28):11470–11475.
15. Zacharek SJ, Fillmore CM, Lau AN, et al. Lung stem cell self-renewal relies on BMI1-dependent control of expression at imprinted loci. Cell Stem Cell. 2011;9(3):272–281.
16. Ferron SR, Charalambous M, Radford E, et al. Postnatal loss of Dlk1 imprinting in stem cells and niche astrocytes regulates neurogenesis. Nature. 2011;475(7356):381–385.
17. Li W, Sun W, Zhang Y, et al. Rapid induction and long-term self-renewal of primitive neural precursors from human embryonic stem cells by small molecule inhibitors. Proc Natl Acad Sci U S A. 2011;108(20):8299–8304.
18. Liu GH, Qu J, Suzuki K, et al. Progressive degeneration of human neural stem cells caused by pathogenic LRRK2. Nature. 2012;491(7425):603–607.
Additional References in Leaders in Pharmaceutical Intelligence
Loss-of-function mutations in a gene called Pax5 have been known to drive normal blood cells to turn into leukemia cells. Such mutations are permanent, so it remained unclear whether an initial, temporary loss of function would instigate an irreversible cascade of events leading to an accumulation of undifferentiated lymphoblasts, or whether an ongoing loss of function would be needed to maintain the disease state.
With the publication of a new study, the question has become more than academic. The study, by researchers at Melbourne’s Walter and Eliza Hall Institute, has not only shown that switching off Pax5 causes cancer in a murine model of B-progenitor acute lymphoblastic leukemia (B-ALL), it has also demonstrated that switching on Pax5 essentially cures the disease.
The results of the study appeared June 15 in the journal Genes & Development, in an article entitled “Pax5 loss imposes a reversible differentiation block in B-progenitor acute lymphoblastic leukemia.” The article described how the researchers used transgenic RNAi to reversibly suppress endogenous Pax5 expression in the hematopoietic compartment of mice, which cooperates with activated signal transducer and activator of transcription 5 (STAT5) to induce B-ALL.
“In this model, restoring endogenous Pax5 expression in established B-ALL triggers immunophenotypic maturation and durable disease remission by engaging a transcriptional program reminiscent of normal B-cell differentiation,” wrote the authors. “Notably, even brief Pax5 restoration in B-ALL cells causes rapid cell cycle exit and disables their leukemia-initiating capacity.”
Institute researcher Grace Liu noted that Pax5, which is frequently “lost” in childhood B-ALL, is essential for normal development of B cells. “When Pax5 function is compromised, developing B cells can get trapped in an immature state and become cancerous,” she said. “We have shown that restoring Pax5 function, even in cells that have already become cancerous, removes this ‘block,’ and enables the cells to develop into normal white blood cells.”
Simply restoring Pax5 sufficed to normalize cancer cells. That is, re-engaging the stalled differentiation program in immature white blood cells restored normal development “despite the presence of additional oncogenic lesions.”
Institute researcher Ross Dickins, Ph.D., said that forcing B-ALL cells to resume their normal development could provide a new strategy for treating leukemia: “While B-ALL has a relatively good prognosis compared with other cancers, current treatments can last years and have major side effects. By understanding how specific genetic changes drive B-ALL, it may be possible to develop more specific treatments that act faster with fewer side effects.”
“It is very difficult to develop drugs that restore the function of genes that are lost during cancer development,” Dr. Dickins added. “However, by understanding the mechanisms by which Pax5 loss causes leukemia, we can begin to look at ways of developing drugs that could have the same effect as restoring Pax5 function.”
Pax5 is just one of about 100 genes known to suppress human tumors. Now that Pax5 has been scrutinized with genetic switch technology, the researchers speculate that similar technology could be used to characterize other tumor suppressor genes.
Epilogue: Volume 4 – Translational, Post-Translational and Regenerative Medicine in Cardiology
Larry H Bernstein, MD, FCAP, Author and Curator, Volume Four, Co-Editor
Justin Pearlman, MD, PhD, FACC, Content Consultant for Series A: Cardiovascular Diseases
Aviva Lev-Ari, PhD, RN, Co-Editor of Volume Four and Editor-in-Chief, BioMed e-Series
This completes Chapter 4 in two parts on the most dynamic developments in the regulatory pathways guiding cardiovascular dynamics and function in health and disease. I have covered key features of these in two summaries, so I shall try to look further into important expected future directions and their anticipated implications.
1. Mechanisms of Disease
Signal Transduction: Akt Phosphorylates HK-II at Thr-473 and Increases Mitochondrial HK-II Association to Protect Cardiomyocytes
Backgound: Hexokinase II binds to mitochondria and promotes cell survival.
Results: Akt phosphorylates HK-II but not the threonine 473 mutant. The phosphomimetic T473D mutant decreases its dissociation from mitochondria induced by G-6P and increases cell viability against stress.
Conclusion: Akt phosphorylates HK-II at Thr-473, resulting in increased mitochondrial HK-II and cell protection.
Significance: The Akt-HK-II signaling nexus is important in cell survival.
HK-II Phosphorylation
It has been demonstrated that an increased level of HK-II at mitochondria is protective and is increased by protective interventions but decreased under stress.
It has not been fully determined which molecular signals regulate the level of HK-II at mitochondria.
Thr-473 in HK-II is phosphorylated by Akt and this phosphorylation leads to increases in mitochondrial HK-II binding through inhibition of G-6P-dependent dissociation, conferring resistance to oxidative stress (Fig. 7).
Overexpression of WTHK-II increases mitochondrial HK-II and confers protection against hydrogen peroxide, which is enhanced significantly in HK-II T473D-expressing cells, whereas NHK-II, lacking the ability to bind to mitochondria, does not confer protection. Conversely, mitochondrial HK-II from mitochondria (Fig.6, A and B) inhibits the IGF-1-mediated increase in mitochondrial HK-II and cellular protection. Similar dose-dependent curves were obtained in mitochondrial HK-II against stress (15–25).
Gene Expression and Genetic Variation in Human Atria
Honghuang Lin PhD, Elena V. Dolmatova MD, Michael P. Morley, PhD, Kathryn L. Lunetta PhD, David D. McManus MD, ScM, et al.
Heart Rhythm 2013 http://dx.doi.org/10.1016/j.hrthm.2013.10.051
Background— The human left and right atria have different susceptibilities to develop atrialfibrillation (AF). However, the molecular events related to structural and functional changes that
enhance AF susceptibility are still poorly understood.
Objective— To characterize gene expression and genetic variation in human atria.
Results— We found that 109 genes were differentially expressed between left and right atrial tissues. A total of 187 and 259 significant cis-associations between transcript levels and genetic
variants were identified in left and right atrial tissues, respectively. We also found that a SNP at a known AF locus, rs3740293, was associated with the expression of MYOZ1 in both left and right
atrial tissues.
Conclusion— We found a distinct transcriptional profile between the right and left atrium, and extensive cis-associations between atrial transcripts and common genetic variants. Our results
implicate MYOZ1 as the causative gene at the chromosome 10q22 locus for AF.
Long-Term Caspase Inhibition Ameliorates Apoptosis, Reduces Myocardial Troponin-I Cleavage, Protects Left Ventricular Function, and Attenuates Remodeling in Rats With Myocardial Infarction
Y. Chandrashekhar, Soma Sen, Ruth Anway, Allan Shuros, Inder Anand,
This study was designed to evaluate whether in vivo caspase inhibition can prevent myocardial contractile protein degradation, improve myocardial function, and attenuate ventricular remodeling.
Apoptosis is thought to play an important role in the development and progression of heart failure (HF) after a myocardial infarction (MI). However, it is not known whether inhibiting apoptosis can attenuate left ventricular (LV) remodeling and minimize systolic dysfunction.
A 28-day infusion of caspase inhibitor was administeredimmediately after an anterior MI. In addition, five sham-operated rats given the caspase inhibitor were compared with 17 untreated sham-operated animals to study effects in non-MI rats. Left ventricular function, remodeling parameters, and hemodynamics were studied four weeks later. Myocardial caspase 3 activation and troponin-I contractile protein cleavage were studied in the non-infarct, remote LV myocardium using Western blots. Apoptosis was assessed using immunohistochemistry for activated caspase-positive cells as well as the TUNEL method. Collagen volume was estimated using morphometry.
Caspase inhibition reduced myocardial caspase 3 activation. This was accompanied by less cleavage of troponin-I, an important component of the cardiac contractile apparatus, and fewer apoptotic cardiomyocytes. Furthermore, caspase inhibition reduced LV-weight-to- body-weight ratio, decreased myocardial interstitial collagen deposition, attenuated LV remodeling, and better preserved LV systolic function after MI.
Caspase inhibition, started soon after MI and continued for four weeks, preserves myocardial contractile proteins, reduces systolic dysfunction, and attenuates ventricular remodeling.
These findings may have important therapeutic implications in post-MI HF. J Am Col Cardiol 2004;43:295–301)
Precardiac deletion of Numb and Numblike reveals renewal of cardiac progenitors
Lincoln T Shenje, Peter P Rainer , Gun-sik Cho , Dong-ik Lee , Weimin Zhong , Richard P Harvey , David A Kass , Chulan Kwon *, et al.
eLife 2014. http://dx.doi.org/10.7554/eLife.02164.001
Cardiac progenitor cells (CPCs) must control their number and fate to sustain the rapid heart growth during development, yet the intrinsic factors and environment governing these processes remain unclear. Here, we show that deletion of the ancient cell-fate regulator Numb (Nb) and its homologue Numblike (Nbl) depletes CPCs in second pharyngeal arches (PA2s) and is associated with an atrophic heart. With histological, fow cytometric and functional analyses, we fnd that CPCs remain undifferentiated and expansive in the PA2, but differentiate into cardiac cells as they exit the arch. Tracing of Nb- and Nbl-defcient CPCs by lineage-specifc mosaicism reveals that the CPCs normally populate in the PA2, but lose their expansion potential in the PA2. These fndings demonstrate that Nb and Nbl are intrinsic factors crucial for the renewal of CPCs in the PA2 and
that the PA2 serves as a microenvironment for their expansion.
2. Diagnostics and Risk Assessment
Classical and Novel Biomarkers for Cardiovascular Risk Prediction in the United States
Cardiovascular risk prediction models based on classical risk factors identified in epidemiologic cohort studies are useful in primary prevention of cardiovascular disease in individuals. This article briefly reviews aspects of
cardiovascular risk prediction in the United States and efforts to evaluate novel risk factors. Even though many novel risk markers have been found to be associated with cardiovascular disease, few appear to improve risk prediction
beyond the powerful, classical risk factors. A recent US consensus panel concluded that clinical measurement of certain novel markers for risk prediction was reasonable, namely,
hemoglobin A1c (in all adults),
microalbuminuria (in patients with hypertension or diabetes), and
C-reactive protein,
lipoprotein-associated phospholipase,
coronary calcium,
carotid intima-media thickness, and
ankle/brachial index (in patients deemed to be at intermediate cardiovascular risk, based on traditional risk factors).
Diagnostic accuracy of NT-proBNP ratio (BNP-R) for early diagnosis of tachycardia-mediated cardiomyopathy: a pilot study
Tachycardia-mediated cardiomyopathy (TMC) occurs as a consequence of prolonged high heart rate due to ventricular and supraventricular tachycardia. In animal models, rapid pacing induces severe biventricular remodeling with dilation and dysfunction [7]. On a cellular basis, cardiomyocytes exert fundamental morphological and functional roles.
When heart failure and tachycardia occur simultaneously, a useful diagnostic tool for early discrimination of patients with benign tachycardia-mediated cardiomyopathy (TMC) versus major structural heart disease (MSHD) is not available. Such a tool is required to prevent unnecessary and wearing diagnostics in patients with reversible TMC. Moreover, it could lead to early additional diagnostics and therapeutic approaches in patients with MSHD.
A total of 387 consecutive patients with supraventricular arrhythmia underwent assessment. Of these patients, 40 fulfilled the inclusion criteria
with a resting heart rate C100 bpm and an impaired left ventricular ejection fraction \40%. In all patients, successful electrical cardioversion was performed. At baseline, day 1 and weekly for 4 weeks, levels of NT-proBNP and echocardiographic parameters were evaluated.
NT-proBNP ratio (BNP-R) was calculated as a quotient of baseline NT-proBNP/follow-up NT-proBNP. After 4 weeks, cardiac catheterization was performed to identify patients with a final diagnosis of TMC versus MSHD.
Initial NT-proBNP concentrations were elevated and consecutively decreased after cardioversion in all patients studied. The area under the ROC curve for BNP-R to detect TMC was 0.90 (95% CI 0.79–1.00; p \ 0.001) after 1 week and 0.995 (95% CI 0.99–1.00; p \ 0.0001) after 4 weeks. One week after cardioversion already, a BNP-R cutoff C2.3 was useful for TMC diagnosis indicated by an accuracy of 90%, sensitivity of 84% and specificity of 95%.
BNP-R was found to be highly accurate for the early diagnosis of TMC.
Fish, marine oils, and their concentrates all serve as sources of the two marine omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), as do some products from algae.
To demonstrate an effect of EPA + DHA on heart health, a number of randomized, controlled intervention studies with clinical endpoints like overall mortality or a combination of adverse cardiac events were conducted in populations with elevated cardiovascular risk. One early intervention study with oily fish, rich in EPA + DHA, and some early studies with fish oil or fish oil concentrate or even purified EPA at doses ranging between 0.9 and 1.8 g/day indeed demonstrated effects in terms of fewer sudden cardiac deaths, fatal or non-fatal myocardial infarctions, or a combination of adverse cardiac events.
Recent meta-analyses found no significant benefits on total mortality, cardiovascular mortality, and other adverse cardiac or cardiovascular events [13–18]. This is in contrast to findings in epidemiologic studies, where intake of EPA + DHA had been found to correlate generally with an up to 50% lower incidence of adverse cardiac events [18,19], and in even sharper contrast to epidemiologic studies based on levels of EPA + DHA, demonstrating e.g., a 10-fold lower incidence of sudden cardiac death associated with high levels of the
fatty acids, as compared to low levels.
This seemingly contradictory evidence has led the American Heart Association to recommend “omega-3 fatty acids from fish or fish oil capsules (1 g/day) for cardiovascular disease risk reduction” for secondary prevention, whereas the European Society for Cardiology recommends “Fish at least twice a week, one of which to be oily fish”, but no supplements for cardiovascular prevention.
A similar picture emerges for atrial fibrillation: In epidemiologic studies, consumption of EPA + DHA or higher levels of EPA + DHA were associated with lower risk for developing atrial fibrillation, while intervention studies found no effect. Pertinent guidelines do not mention EPA + DHA. A similar picture also emerges for severe ventricular rhythm disturbances.
Why is it that trial results are at odds with results from epidemiology? What needs to be done to better translate the epidemiologic findings into trial results? The current review will try to shed some light on this issue, with a special consideration of the Omega-3 Index.
Recent large trials with eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) in the cardiovascular field did not demonstrate a beneficial effect in terms of reductions of clinical endpoints like
total mortality,
sudden cardiac arrest or
other major adverse cardiac events.
Pertinent guidelines do not uniformly recommend EPA + DHA for cardiac patients. In contrast,
in epidemiologic findings, higher blood levels of EPA + DHA were consistently associated with a lower risk for the endpoints mentioned.
The following points argue for the use of erythrocytes: erythrocyte fatty acid
composition has a low biological variability, erythrocyte fat consists almost exclusively of phospholipids, erythrocyte fatty acid composition reflects tissue fatty acid composition, pre-analytical stability, and other points. In 2004, EPA + DHA in erythrocyte fatty acids were defined as the Omega-3 Index and suggested as a risk factor for sudden cardiac death [39]. Integral to the definition was a specific and standardized analytical procedure, conforming the quality management routinely implemented in the field of clinical chemistry.
The laboratories adhering to the HS-Omega-3 Index methodology perform regular proficiency testing, as mandated in routine Clinical Chemistry labs. So far, the HS-Omega-3 Index is the only analytical procedure used in several laboratories. A standardized analytical procedure is a prerequisite to generate the data base necessary to transport a laboratory parameter from research into clinical routine. Moreover, standardization of the analytical procedure is the first important criterion for establishing a new biomarker for cardiovascular risk set forth by the American Heart Association and the US Preventive Services Task Force.
Because of low biological and analytical variability, a standardized analytical procedure, a large database and for other reasons,
blood levels of EPA + DHA are frequently assessed in erythrocytes, using the HS-Omega-3 Index methodology.
Table 1. Mean HS-Omega-3 Index values in various populations, Mean (±standard deviation (SD)). Please note that in every population studied, a lower value was found to be associated with a worse condition than a higher value. References are given, if not, unpublished, n = number of individuals measured.
All levels of fatty acids are determined by the balance of substance entering the body and those leaving the body. Neither a recent meal, even if rich in EPA + DHA, nor severe cardiac events altered the HS-Omega-3 Index. However, while long-term intake of EPA + DHA, e.g., as assessed with food questionnaires, was the main predictor of the HS-Omega-3 Index, long-term intake explained only 12%–25% of its variability. A hereditary component of 24% exists. A number of other factors correlated positively (+) or negatively (−), like age (+), body mass index (−), socioeconomic status (+), smoking (−), but no other conventional cardiac risk factors. More factors determining the level of the HS-Omega-3 Index, especially regarding efflux remain to be defined. Therefore, it is impossible to predict the HS-Omega-3 Index in an individual, as it is impossible to predict the increase in the HS-Omega-3 Index in an individual in response to a given dose of EPA + DHA. In Table 2, current evidence is presented on the relation of the HS-Omega-3 Index to CV events.
The HS-Omega-3 Index has made it possible to reclassify individuals from intermediate cardiovascular risk into the respective high risk and low risk strata, the third criterion for establishing a new biomarker for CV risk.
A low Omega-3 Index fulfills the current criteria for a novel cardiovascular risk factor.
Increasing the HS-Omega-3 Index by increased intake of EPA + DHA in randomized controlled trials improved a number of surrogate parameters for cardiovascular risk:
heart rate was reduced,
heart rate variability was increased,
blood pressure was reduced,
platelet reactivity was reduced,
triglycerides were reduced,
large buoyant low-density lipoprotein (LDL)-particles were increased and
small dense LDL-particles were reduced,
large buoyant high-density lipoproteins (HDL)2 were increased,
very low-density lipoprotein (VLDL1) + 2 was reduced,
pro-inflammatory cytokines (e.g., tumor necrosis factor alpha, interleukin-1β, interleukins-6,8,10 and monocyte chemoattractant protein-1) were reduced,
anti-inflammatory oxylipins were increased.
Importantly, in a two-year randomized double-blind angiographic intervention trial, increased erythrocyte EPA + DHA
reduced progression and increased regression of coronary lesions, an intermediate parameter.
Taken together, increasing the HS-Omega-3 Index improved surrogate and intermediate parameters for cardiovascular events. A large intervention trial with clinical endpoints based on the HS-Omega-3 Index remains to be conducted. Therefore, the fourth criterion, proof of therapeutic consequence of determining the HS-Omega- Index, is only partially fulfilled.
Neutral results of intervention trials can be explained by issues of bioavailability and trial design that surfaced after the trials were initiated.
In the future, incorporating the Omega-3 Index into trial designs by
recruiting participants with a low Omega-3 Index and
treating them within a pre-specified target range (e.g., 8%–11%),
will make more efficient trials possible and
provide clearer answers to the questions asked than previously possible.
Bioengineers at the University of California, Berkeley in a new study published in Nature say they have identified two key regulatory pathways that control how well adult stem cells repair and replace damaged tissue. They then tweaked how those stem cells reacted to those biochemical signals to revive the ability of muscle tissue in old mice to repair itself nearly as well as the muscle in the mice’s much younger counterparts. Irina Conboy, an assistant professor of bioengineering and an investigator at the Berkeley Stem Cell Center and at the California Institute for Quantitative Biosciences (QB3), led the research team conducting this study. Because the findings relate to adult stem cells that reside in existing tissue, this approach to rejuvenating degenerating muscle eliminates the ethical and medical complications associated with transplanting tissues grown from embryonic stem cells. The researchers focused on
the interplay of two competing molecular pathways that control the stem cells,
which sit next to the mature, differentiated cells that make up our working body parts. When the mature cells are damaged or wear out, the stem cells are called into action to begin the process of rebuilding.
old muscle tissue is left with
“We don’t realize it, but as we grow our bodies are constantly being remodeled,” said Conboy. “We are constantly falling apart, but we don’t notice it much when we’re young because we’re always being restored. As we age, our stem cells are prevented, through chemical signals, from doing their jobs.” The good news, the researchers said, is that
the stem cells in old tissue are still ready and able to perform their regenerative function
if they receive the appropriate chemical signals.
Studies have shown that when old tissue is placed in an environment of young blood, the stem cells behave as if they are young again. “Conversely, we have found in a study published last year that even young stem cells rapidly age when placed among blood and tissue from old mice,” said Carlson, who will stay on at UC Berkeley to expand his work on stem cell engineering.
Adult stem cells have a receptor called Notch that, when activated,
tells them that it is time to grow and divide
stem cells also have a receptor for the protein TGF-beta
that sets off a chain reaction activatingthemoleculepSmad3 and
ultimately producing cyclin-dependent kinase (CDK) inhibitors, which regulate the cell’s ability to divide.
activated Notch competeswithactivatedpSmad3 for
binding to the regulatory regions of the same CDK inhibitors in the stem cell
“We found that Notch is capable of physically kicking off pSmad3 from the promoters for the CDK inhibitors within the stem cell’s nucleus, which tells us that a precise manipulation of the balance of these pathways would allow the ability to control stem cell responses.” Notch and TGF-beta are well known in molecular biology, but Conboy’s lab is the first to connect them to the process of aging, and the first to show that they act in opposition to each other within the nucleus of the adult stem cell. Aging and the inevitable march towards death are, in part, due to the progressive decline of Notch and the increased levels of TGF-beta , producing a one-two punch to the stem cell’s capacity to effectively rebuild the body, the researchers said.
The researchers disabled the “aging pathway” that tells stem cells to stop dividing by using an established method of RNA interference that reduced levels of pSmad3. The researchers then examined the muscle of the different groups of mice one to five days after injury to compare how well the tissue repaired itself. As expected,
muscle tissue in the young mice easily replaced damaged cells with new, healthy cells. In contrast,
the areas of damaged muscle in the control group of old mice were characterized by fibroblasts and scar tissue. However,
muscles in the old mice whose stem cell “aging pathway”had been dampened showed levels of cellular regeneration that were
comparable to their much younger peers, and that were 3 to 4 times greater than those of the group of “untreated” old mice.
In the first trial of its kind in the world, 60 patients who have recently suffered a major heart attack will be injected with selected stem cells from their own bone marrow during routine coronary bypass surgery. The Bristol trial will test
whether the stem cells will repair heart muscle cells damaged by the heart attack,
by preventing late scar formation and hence impaired heart contraction.
“ Cardiac stem cell therapy aims to repair the damaged heart as it has the potential to replace the damaged tissue.” We have elected to use a very promising stem cell type selected from the patient’s own bone marrow. This approach ensures no risk of rejection or infection. It also gets around the ethical issues that would result from use of stem cells from embryonic or foetal tissue.
In this trial (known as TransACT), all patients will have bone marrow harvested before their heart operation. Then either stem cells from their own bone marrow or a placebo will be injected into the patients’ damaged hearts during routine coronary bypass surgery. The feasibility and safety of this technique has already been demonstrated. As a result of the chosen double blind placebo-controlled design, neither the patients nor the surgeon knows whether the patient is going to be injected with stem cells or placebo. This ensures that results are not biased in any way, and is the most powerful way to prove whether or not the new treatment is effective.
Under highly specific growth conditions in laboratory culture dishes, stem cells
can be coaxed into developing as new cardiomyocytes and vascular endothelial cells (Kirschstein and Skirboll, 2001).
Discoveries that have triggered the interest in the application of adult stem cells to heart muscle repair in animal models have been made by researchers in the past few years (Kirschstein and Skirboll, 2001). One study demonstrated that cardiac tissue can be regenerated in the mouse heart attack model through the introduction of adult stem cells from mouse bone marrow (Kirschstein and Skirboll, 2001). These cells were transplanted into the marrow of irradiated mice approximately 10 weeks before the recipient mice were subjected to heart attack thru tying off different major heart blood vessel, the left anterior descending (LAD) coronary artery. The survival rate was 26 percent at two to four weeks after the induced cardiac injury (Kirschstein and Skirboll, 2001). Another study of the region surrounding the damaged tissue in surviving mice showed the presence of donor-derived cardiomyocytes and endothelial cells (Kirschstein and Skirboll, 2001).
the mouse hematopoietic stem cells transplanted into the bone marrow had migrated to the border part of the damaged area, and differentiated into several types of tissue for cardiac repair.
Regenerating heart tissue through stem cell therapy
A groundbreaking study on repairing damaged heart tissue through stem cell therapy has given patients hope that they may again live active lives. An international team of Mayo Clinic researchers and collaborators has done it by discovering a way to regenerate heart tissue.
“It’s a paradigm shift,” says Andre Terzic, M.D., Ph.D., director of Mayo Clinic’s Center for Regenerative Medicine and senior investigator of the stem cell trial. “We are moving from traditional medicine, which addresses the symptoms of disease to cure disease.” Treating patients with cardiac disease has typically involved managing heart damage with medication. In collaboration with European researchers, Mayo Clinic researchers have discovered a novel way to repair a damaged heart. In Mayo Clinic’s breakthrough process,
stem cells are harvested from a patient’s bone marrow.
undergo a laboratory treatment that guides them into becoming cardiac cells,
which are then injected into the patient’s heart in an effort to grow healthy heart tissue.
The study is the first successful demonstration in people of the feasibility and safety of transforming adult stem cells into cardiac cells. Beyond heart failure, the Mayo Clinic research also is a milestone in the emerging field of regenerative medicine, which seeks to fully heal damaged tissue and organs.
Creating a heart repair kit
This image shows the process used in the clinical trials to repair damaged hearts. Cardioprogenitor cells is another term for cardiopoietic cells, those that were transformed into cardiac cells.
Transformation: The cardiopoietic cells on the left react to the cardiac environment, cluster together with like cells and form tissue.
Mayo Clinic researchers pursued this research, inspired by an intriguing discovery. In the early 2000s, they analyzed stem cells from 11 patients undergoing heart bypass surgery. The stem cells from two of the patients had an unusually high expression of certain transcription factors — the proteins that control the flow of genetic information between cells. Clinically, the two patients appeared no different from the others, yet their stem cells seemed to show unique capacity for heart repair.
That observation drove them to determine how to convert nonreparative stem cells to become reparative. Doing so required determining precisely how the human heart naturally develops, at a subcellular level. That painstaking work was led by Atta Behfar, M.D., Ph.D., a cardiovascular researcher at Mayo Clinic in Rochester, Minn. With other members of the Terzic research team, Dr. Behfar identified hundreds of proteins involved in the process of heart development (cardiogenesis). The researchers then set out to identify which of these proteins are essential in driving a stem cell to become a cardiac cell. Using computer models,
they simulated the effects of eliminating proteins one by one from the process of heart development.
That method yielded about 25 proteins.
The team then pared that number down to 8 proteins that their data indicated were essential.
The research team was then able to develop the lab procedure that guides stem cells to become heart cells.
The treated stem cells were dubbed cardiopoietic, or heart creative. A proof of principle study about guided cardiopoiesis, whose results were published in the Journal of the American College of Cardiology in 2010, demonstrated that animal models with heart disease that had been injected with caridiopoietic cells had improved heart function compared with animals injected with untreated stem cells. Hailed as “landmark work,” by the journal’s editorial writer, the study showed it was indeed possible to teach stem cells to become cardiac cells. Stem cells from each patient in the cardiopoiesis group were successfully guided to become cardiac cells. The treated cells were injected into the heart wall of each of those patients without apparent complications.
“Ihis newprocessofcardiopoiesiswas achieved in 100 percent of cases, with a very good safety profile,” Dr.Terzic says. “We are enabling the heart toregainitsinitial structure and function,” Dr.Terzic says, “and we will not stop here.” The clinicaltrialfindingsareexpectedto be published in the Journal of the American College of Cardiology in 2013. Meanwhile, research to improve the injection process and effectiveness is underway.
Stem Cells from Humans Repair Heart Damage in Monkeys
implanted graft of cardiac cells derived from human stem cells (green)
Regeneration of the heart by 4 different classes of proteins
Stem cells have shown promise in small-animal models, that is, in mice and rats. Still, it was unclear whether human embryonic-stem-cell-derived cardiomyocytes (hESC-CMs) could be produced in adequate numbers, and cryopreserved with sufficient viability, to even approach human application In a step up from small-animal models, scientists at the University of Washington used a monkey model of myocardial infarction to test how well hESC-CMs could replace damaged tissue with new heart cells and restore failing hearts to normal function. The scientists injected 1 billion heart muscle cells derived from hESC-CMs into the infarcted muscle of pigtail macaques (Macaca nemestrina). This was 10 times more of these types of cells than researchers have ever been able to generate before.
The researchers found that over subsequent weeks, the stem-cell derived heart muscle cells infiltrated into the damaged heart tissue, then matured, assembled into muscle fibers, and began to beat in synchrony with the macaque heart cells. After three months, the cells appeared to have fully integrated into the macaque heart muscle. The research team published its results April 30 in Nature, in an article entitled “Human embryonic-stem-cell-derived cardiomyocytes regenerate non-human primate hearts.” In this article, the authors indicated that their work demonstrated that
hESCs can be grown,
differentiated into cardiomyocytes, and
cryopreserved at a scale sufficient to treat a large-animal model of myocardial infarction.
“With further refinements in manufacturing, the scale up to trials in humanpatientsseemsfeasible,” the researchers wrote. “Large-animal models are important forerunners to human trials, because they impart real-world rigor to issues such as cell production, delivery, and end-point analyses, while permitting mechanistic studies not possible in patients.”
Molecule Implicated In Leukemia Also Important In Muscle Repair
The study shows that immature muscle cells require the molecule, called miR-29, to become mature, and that
the molecule is nearly missing in cells from rhabdomyosarcoma, a cancer caused by the proliferation of immature muscle cells.
Cells from human rhabdomyosarcoma tumors showed levels of the molecule that were
10 percent or less of those in normal muscle cells.
Artificially raising the level of the molecule in the cancer cells
cut their growth by half and caused them
to begin maturing, slowing down tumor growth.
MiR-29 is a type of microRNA, a family of molecules that helps regulate the proteins cells produce. Researchers say this study is unusual because
it also sheds light on the how a microRNA itself is regulated.
The gene for miR-29 is silenced by the action of a protein, called NF kappa B.
this protein is present at highlevelsinrhabdomyosarcoma cells, and
this keeps miR-29 shut off,
preventing muscle progenitor cells from maturing.
When they raised the level of the microRNA molecule in the cells,
or lowered the level of the NF kappa B protein,
the cells’ growth rate dropped two fold, and
they began taking on the appearance of mature muscle cells.
Recent years have seen major advances in understanding the structure-function relationships of G protein-coupled receptors (GPCRs). This large superfamily of transmembrane receptors comprises over 800 members in humans.
GPCRs regulate a wide variety of physiological processes including
sensation (vision, taste, and smell),
growth,
hormone responses, and
regulation of the immune and
autonomic nervous systems.
Their involvement in multiple disease pathways makes GPCRs attractive targets for drug discovery efforts.
These multifaceted proteins will be the subject of “GPCRStructure, Function and Drug Discovery,” a Global Technology Community conference scheduled to take place May 22–23 in Boston. The conference is expected to cover a broad range of topics including biased signaling, membrane protein structures, GPCR signaling dynamics, computational approaches to disease.
According to Bryan Roth, M.D., Ph.D., Michael Hooker Distinguished Professor at the University of North Carolina, Chapel Hill,
drugs that can selectively target various downstream GPCR pathways hold the most promise.
Dr. Roth’s laboratory studies approximately 360 different GPCRs with therapeutic potential using massively parallel screening methods.His research focuses on “functional selectivity,” which he describes as
“the ligand-dependent selectivity for certain signal transduction pathways in one and the same receptor.”
Dr. Roth notes that structural data have demonstrated that GPCRs exist in multiple conformations: “The structures of the 5-hydroxytryptamine 2B receptor and the recent high-resolution delta-opioid receptor structure have provided evidence for conformational rearrangements that contribute to functional selectivity.” Drugs that take advantage of this selectivity by preferentially stabilizing certain conformations may have unique therapeutic utility.
“Generally, we look at G protein versus arrestin-based signaling, although it’s also possible to examine how drugs activate one G protein-mediated signaling pathway versus another.
fluorescently tagged Arrestin and GPRC of interest
β-Arrestins constitute a major class of intracellular scaffolding proteins that regulate GPCR signaling by preventing or enhancing the binding of GPCRs to intracellular signaling molecules. Laura Bohn, Ph.D., associate professor at Scripps Florida, studies the roles that β-arrestins play in GPCR-mediated signaling.
a particular β-arrestin can play multiple, tissue-specific roles—shutting down the signaling of a receptor in one tissue while activating signaling in another.
different ligands can direct GPCR signaling to different effectors, which could result in different physiological effects,” comments Dr. Bohn. “Our challenge is in determining what signaling pathways to harness to promote certain effects, while avoiding others.”
Arrestin binding to active GPCR kinase (GRK)-phosphorylated GPCRs blocks G protein coupling
Using Designer Proteins
The multifunctional signaling abilities of β-arrestins has prompted large-scale study of their properties. Vsevolod Gurevich, Ph.D., professor of pharmacology at Vanderbilt University, studies
the structure,
function, and
biology of arrestin proteins.
β-arrestins have three main functions.
First, they prevent the coupling of GPCRs to G proteins, thereby blocking further G protein-mediated signaling (a process known as desensitization).
Second, the binding of a GCPR releases the β-arrestin’s carboxy-terminal “tail” and promotes internalization of the receptor.
Third, receptor-bound β-arrestins bind other signaling proteins, resulting in a second wave of arrestin-mediated signaling.
Dr. Gurevich’s laboratory studies β-arrestin biology through the use of three types of specially designed mutants—
enhanced phosphorylation-dependent,
receptor-specific, and
signaling-biased mutants.
an enhanced mutant of visual β-arrestin-1 partially compensates for defects of rhodopsin phosphorylation in vivo,
“Several congenital disorders are caused by mutant GPCRs that cannot be normally phosphorylated because they have lost GPCR kinase (GRK) sites. Enhanced super-active arrestins have the potential to compensate for these defects, bringing the signaling closer to normal.”
Dr. Gurevich explains the strategy involved in creating designer β-arrestins: “We identify residues critical for individual β-arrestin functions by mutagenesis, using limited structural information as a guide.
We also work on getting more structural information. In collaboration with different crystallographers, we solved the crystal structures of all four vertebrate β-arrestin subtypes in the basal state, as well as the structure of the arrestin-1-rhodopsin complex.”
Dr. Gurevich believes that designer β-arrestins “are the next step in research and therapy, moving way beyond what small molecules can achieve.
The difference in capabilities between redesigned signaling proteins, including β-arrestins, and conventional small molecule drugs is about the same as that between airplanes and horse-driven carriages.”
Dr. Gurevich observes that redesigned signaling proteins face considerable obstacles in terms of gene delivery, but that the efforts are worth it. “Using designer signaling proteins, we can tell the cell what to do in a language it cannot disobey,” asserts Dr. Gurevich.
Synthesis and Antihypertensive Screening of Novel Substituted 1,2- Pyrazoline Sulfonamide Derivatives
Avinash M. Bhagwat , Anilchandra R. Bha , Mahesh S. Palled , Anand P. Khadke , Anuradha M. Patil, et al.
Angiotensin II receptor antagonists, also known as angiotensin receptor blockers , AT1-receptor antagonists or sartans, are a group of pharmaceuticals which modulate the renin-angiotensin-aldosterone system. Their main use is in hypertension, diabetic nephropathy and congestiveheart failure. These substances are AT1-receptor antagonists which
block the activationof angiotensin II AT1 receptors.
Blockade of AT1 receptors directly causes
1 vasodilation,
2 reduces secretion of vasopressin,
3 reduces production and secretion of aldosterone, amongst other actions –
4 the combined effect of which is reduction of blood pressure.
Irbesartan is a safe and effectiveangiotensin II receptor antagonist with an affinity for the AT1 receptor that is more than 8,500times greater than its affinity for AT2 receptor. This agent has a higher bioavailability (60-80%) than other drugs in its class . In both Losartan and Irbesartan structures imidazole moiety is being present. A structure analog of losartan and Irbesartan are designed by incorporating the heterocycles like pyrazoline group. We felt it would be interesting to explore the possibilities of 1,2-pyrazoline derivatives for Angiotensin II receptor antagonistic activity.
The Irbesartan structure was a modified Losartan structure, which had all the identity of a Losartan molecule but with groups that would fit the hydrophobic cavity with a tetramethylene group and an alkyl side chain that would fit in the pocket in the AT1 receptor. The hydroxyl methyl group of Losartan being replaced with carbonyl group of Irbesartan. With a view to introduce a hydrogen bonding interaction with AT1 receptor, these structures were further modified with a view of retaining both hydrogen bonding characteristics and as well as lipophilic groups. Losartan and Irbesartan structure contains a diphenyl molecule & imidazole ring.
In Losartan and Irbesartan diphenyl molecule is attached to the nitrogen of the imidazole ring. It is interesting to to see the activity of compounds containing two phenyl rings attached at two different positions namely3,5 position of 1, 2-pyrazoline ring. The sulphonamide derivatives known for its diuretics activity which reduces renal hypertension. We use to synthesize sulphonamide and pyrazoline in one molecule to check its possible Angiotensin II receptor antagonist property. For this reason chalcones were synthesized reacted with hydrazine hydrate to yield the corresponding 1,2-pyrazoline derivatives which further condensed with sulphanilamide and formaldehyde by mannich condensation reaction.
Acute Toxicity Study (LD50)
This study was carried out in order to establish the therapeutic and toxic doses of the newly synthesized 1,2 pyrazoline derivatives. To establish LD50 of these compounds the method described by Miller & Tainter was employed.
We report new 1,2 pyrazolines which defined combination of substituents confers appropriate polarity and charge distribution for good activity. The spectral data of compounds confirms the structures.
We also report various derivatives of 1,2 pyrazolines from Chalcones to achieve the promising and selective inhibition. The synthesized 1,2 pyrazoline derivatives have resemblance to some of Angiotensin II blocking agents like Irbesartan and Losartan. Hence it was thought of carrying out Angiotensin II blocking screening by 1K-1C Goldblatt noninvasive blood pressure measurement method. As a result, the screened compounds have shown significant Angiotensin II blocking activity. Irbesartan was used as the standard drug for Angiotensin II blocking activity.
Compounds synthesized have shown the significant Angiotensin II blocking activity when compared with the control but however are not comparable to the standard Irbesartan. The results were calculated by taking mean SE and finding the ‘P’ values. Hence from the SAR studies the chloro substituted compounds PH-2 and PH-7 exhibit better Angiotensin II blocking activityamongst the synthesized compounds. The structures of all the synthesized compounds were established on the basis of M.P., TLC, IR, NMR (PMR) . The compounds synthesized were found to be non-toxic and could be synthesized in good yields. The active compounds could be taken as lead for structural and molecular modification was thought of in future.
The present work, which was undertaken is a bonafide and novel work on the synthesis of 1,2 pyrazoline derivatives. We have made an attempt in reviewing the literature on 1,2 pyrazoline derivatives for their medicinal uses with the help of chemical abstract, journals and internet surfing. For the synthesis of 1,2 pyrazoline derivatives scheme were established. Around eight derivatives were synthesized. The synthesized compounds were tested for their purity, preliminary tests, physical constants and TLC. The structure of the final compound were confirmed by IR, H-NMR spectra and GCMS. The compounds synthesized were found to be non-toxic and could be synthesized in good yields.
5. Synthetic Biology
Artists and biologists team up to ush boundaries of synthetic biology
Synthetic biologists are often accused of “playing God,” of tampering with his Creation. Well, if you’re going to Create then you might as well do so with the help of some creative individuals? That’s just what the biologists in the pages of the new book Synthetic Aesthetics, from MIT Press, aims to do. Its arrival is well-timed, with the
Alun Anderson has reviewed the new book for New Scientist. Unlike the typically defensive posture found in biotech broadly, he writes, the spirit captured by this book is “freewheeling” and collaborative, with 20 authors ranging from the arts and sciences putting their minds together to generate original ideas. Anderson notes that parts of the book “may irritate conventional scientists – some of the ideas were dreamed up while ‘performing a dance based on the myth of the Golem’, for example. But it certainly explains the key ideas of the field and leads you to many lateral conversations about what it may become.” The book is itself an offshoot of a larger project, which you can check out at its official page. It describes itself as an “experimental, international research project between synthetic biology, art, design and social science” It has roots at the University of Edinburgh, Scotland, and Stanford University, California. And the main project team is comprised of bioengineers Drew Endy (Stanford) and Alistair Elfick (Edinburgh), social scientists Jane Calvert (Edinburgh) and Pablo Schyfter (Edinburgh), and designer/artist Alexandra Daisy Ginsberg.
In the book Synthetic Aesthetics, Ginsberg provides a thought-provoking counterpoint to the engineering definition of “design”. Anderson explains in his review: An engineer might think of designing a bridge to a particular specification; a synthetic biologist of designing a microorganism with a new commercial application, pumping out green gasoline for example; but a real designer, a fashion designer, for example, is doing something else. As artist Daisy Ginsberg puts it, design “is about possibility”, the unimagined things that life could be.
Synthetic biology, she writes, has been addressing “humanity’s needs” – limitless fuel, for example – rather than “our needs as individual, diverse and complex humans”. This is refreshing: worries about the separation between the top-down design of the future and those who must live with the results are quite rare in science. These words ring true, given the intensely “problem oriented” approach to most synthetic biology research. This approach extends to the coverage of this research in the media, where even a research achievement with sweeping potential like the synthetic yeast chromosome ends up broken down into pragmatic chunks. (Yeast could mass-produce medicines! Help process fuels!) Alistair Elfick, one of the leads on the Synthetics Aesthetics project, has written a fascinating opinion piece at The Conversation to accompany the release of his book. In it, he puts forth the idea it’s time for synthetic biologists to stop thinking “like scientists,” lest they hamstring themselves.
Kenrick Vezina is Gene-ius Editor for the Genetic Literacy Project and a freelance science writer, educator, and naturalist based in the Greater Boston area.Sources:
Introduction – The Evolution of Cancer Therapy and Cancer Research: How We Got Here?
Author and Curator: Larry H Bernstein, MD, FCAP
The evolution of progress we have achieved in cancer research, diagnosis, and therapeutics has originated from an emergence of scientific disciplines and the focus on cancer has been recent. We can imagine this from a historical perspective with respect to two observations. The first is that the oldest concepts of medicine lie with the anatomic dissection of animals and the repeated recurrence of war, pestilence, and plague throughout the middle ages, and including the renaissance. In the awakening, architecture, arts, music, math, architecture and science that accompanied the invention of printing blossomed, a unique collaboration of individuals working in disparate disciplines occurred, and those who were privileged received an education, which led to exploration, and with it, colonialism. This also led to the need to increasingly, if not without reprisal, questioning long-held church doctrines.
It was in Vienna that Rokitansky developed the discipline of pathology, and his student Semelweis identified an association between then unknown infection and childbirth fever. The extraordinary accomplishments of John Hunter in anatomy and surgery came during the twelve years war, and his student, Edward Jenner, observed the association between cowpox and smallpox resistance. The development of a nursing profession is associated with the work of Florence Nightengale during the Crimean War (at the same time as Leo Tolstoy). These events preceded the work of Pasteur, Metchnikoff, and Koch in developing a germ theory, although Semelweis had committed suicide by infecting himself with syphilis. The first decade of the Nobel Prize was dominated by discoveries in infectious disease and public health (Ronald Ross, Walter Reed) and we know that the Civil War in America saw an epidemic of Yellow Fever, and the Armed Services Medical Museum was endowed with a large repository of osteomyelitis specimens. We also recall that the Russian physician and playwriter, Anton Checkov, wrote about the conditions in prison camps.
But the pharmacopeia was about to open with the discoveries of insulin, antibiotics, vitamins, thyroid action (Mayo brothers pioneered thyroid surgery in the thyroid iodine-deficient midwest), and pitutitary and sex hormones (isolatation, crystal structure, and synthesis years later), and Karl Landsteiner’s discovery of red cell antigenic groups (but he also pioneered in discoveries in meningitis and poliomyelitis, and conceived of the term hapten) with the introduction of transfusion therapy that would lead to transplantation medicine. The next phase would be heralded by the discovery of cancer, which was highlighted by the identification of leukemia by Rudolph Virchow, who cautioned about the limitations of microscopy. This period is highlighted by the classic work – “Microbe Hunters”.
John Hunter
Walter Reed
Robert Koch
goldberger 1916 Pellagra
Louis Pasteur
A multidisciplinary approach has led us to a unique multidisciplinary or systems view of cancer, with different fields of study offering their unique expertise, contributions, and viewpoints on the etiology of cancer. Diverse fields in immunology, biology, biochemistry, toxicology, molecular biology, virology, mathematics, social activism and policy, and engineering have made such important contributions to our understanding of cancer, that without cooperation among these diverse fields our knowledge of cancer would never had evolved as it has. In a series of posts “Heroes in Medical Research:” the work of researchers are highlighted as examples of how disparate scientific disciplines converged to produce seminal discoveries which propelled the cancer field, although, at the time, they seemed like serendipitous findings. In the post Heroes in Medical Research: Barnett Rosenberg and the Discovery of Cisplatin (Translating Basic Research to the Clinic) discusses the seminal yet serendipitous discoveries by bacteriologist Dr. Barnett Rosenberg, which eventually led to the development of cisplatin, a staple of many chemotherapeutic regimens. Molecular biologist Dr. Robert Ting, working with soon-to-be Nobel Laureate virologist Dr. James Gallo on AIDS research and the associated Karposi’s sarcoma identified one of the first retroviral oncogenes, revolutionizing previous held misconceptions of the origins of cancer (described in Heroes in Medical Research: Dr. Robert Ting, Ph.D. and Retrovirus in AIDS and Cancer). Located here will be a MONTAGE of PHOTOS of PEOPLE who made seminal discoveries and contributions in every field to cancer Each of these paths of discovery in cancer research have led to the unique strategies of cancer therapeutics and detection for the purpose of reducing the burden of human cancer. However, we must recall that this work has come at great cost, while it is indeed cause for celebration. The current failure rate of clinical trials at over 70 percent, has been a cause for disappointment, and has led to serious reconsideration of how we can proceed with greater success. The result of the evolution of the cancer field is evident in the many parts and chapters of this ebook. Volume 4 contains chapters that are in a predetermined order:
The concepts of neoplasm, malignancy, carcinogenesis, and metastatic potential, which encompass:
(a) How cancer cells bathed in an oxygen rich environment rely on anaerobic glycolysis for energy, and the secondary consequences of cachexia and sarcopenia associated with progression
invasion
ARTS protein and cancer
Glycolysis
Krebs cycle
Metabolic control analysis of respiration in human cancer tissue
akip1-expression-modulates-mitochondrial-function
(b) How advances in genetic analysis, molecular and cellular biology, metabolomics have expanded our basic knowledge of the mechanisms which are involved in cellular transformation to the cancerous state.
nucleotides
Methylation of adenine
ampk-and-ampk-related-kinase-ark-family-
ubiquitylation
(c) How molecular techniques continue to advance our understanding of how genetics, epigenetics, and alterations in cellular metabolism contribute to cancer and afford new pathways for therapeutic intervention.
genomic effects
LKB1AMPK pathway
mutation-frequencies-across-12-cancer-types
AMPK-activating drugs metformin or phenformin might provide protection against cancer
2. The distinct features of cancers of specific tissue sites of origin
3. The diagnosis of cancer by
(a) Clinical presentation
(b) Age of onset and stage of life
(c) Biomarker features
hairy cell leukemia
lymphoma leukemia
(d) Radiological and ultrasound imaging
Treatments
Prognostic differences within and between cancer types
We have introduced the emergence of a disease of great complexity that has been clouded in more questions than answers until the emergence of molecular biology in the mid 20th century, and then had to await further discoveries going into the 21st century. What gave the research impetus was the revelation of
1 the mechanism of transcription of the DNA into amino acid sequences
Proteins in Disease
2 the identification of stresses imposed on cellular function
NO beneficial effects
3 the elucidation of the substructure of the cell – cell membrane, mitochondria, ribosomes, lysosomes – and their functions, respectively
AKIP1 Expression Modulates Mitochondrial Function
4 the elucidation of oligonucleotide sequences
nucleotides
dna-replication-unwinding
dna-replication-ligation
dna-replication-primer-removal
dna-replication-leading-strand
dna-replication-lagging-strand
dna-replication-primer-synthesis
dna-replication-termination
5 the further elucidation of functionally relevant noncoding lncDNA
6 the technology to synthesis mRNA and siRNA sequences
Figure. RNAi and gene silencing
7 the repeated discovery of isoforms of critical enzymes and their pleiotropic properties
8. the regulatory pathways involved in signaling
Figure. Signaling Pathways Map
This is a brief outline of the modern progression of advances in our understanding of cancer. Let us go back to the beginning and check out a sequence of Nobel Prizes awarded and related discoveries that have a historical relationship to what we know. The first discovery was the finding by Louis Pasteur that fungi that grew in an oxygen poor environment did not put down filaments. They did not utilize oxygen and they produced used energy by fermentation. This was the basis for Otto Warburg sixty years later to make the comparison to cancer cells that grew in the presence of oxygen, but relied on anaerobic glycolysis. He used a manometer to measure respiration in tissue one cell layer thick to measure CO2 production in an adiabatic system.
Lavoisier Antoine-Laurent and Laplace Pierre-Simon (1783) Memoir on heat. Mémoirs de l’Académie des sciences. Translated by Guerlac H, Neale Watson Academic Publications, New York, 1982.
The Warburg apparatus is a manometric respirometer which was used for decades in biochemistry for measuring oxygen consumption of tissue homogenates or tissue slices.
The aqueous phase is vigorously shaken to equilibrate with a gas phase, from which oxygen is consumed while the evolved carbon dioxide is trapped, such that the pressure in the constant-volume gas phase drops proportional to oxygen consumption. The Warburg apparatus was introduced to study cell respiration, i.e. the uptake of molecular oxygen and the production of carbon dioxide by cells or tissues. Its applications were extended to the study of fermentation, when gas exchange takes place in the absence of oxygen. Thus the Warburg apparatus became established as an instrument for both aerobic and anaerobic biochemical studies [2, 3].
The respiration chamber was a detachable glass flask (F) equipped with one or more sidearms (S) for additions of chemicals and an open connection to a manometer (M; pressure gauge). A constant temperature was provided by immersion of the Warburg chamber in a constant temperature water bath. At thermal mass transfer equilibrium, an initial reading is obtained on the manometer, and the volume of gas produced or absorbed is determined at specific time intervals. A limited number of ‘titrations’ can be performed by adding the liquid contained in a side arm into the main reaction chamber. A Warburg apparatus may be equipped with more than 10 respiration chambers shaking in a common water bath. Since temperature has to be controlled very precisely in a manometric approach, the early studies on mammalian tissue respiration were generally carried out at a physiological temperature of 37 °C.
The Warburg apparatus has been replaced by polarographic instruments introduced by Britton Chance in the 1950s. Since Chance and Williams (1955) measured respiration of isolated mitochondria simultaneously with the spectrophotometric determination of cytochrome redox states, a water chacket could not be used, and measurements were carried out at room temperature (or 25 °C). Thus most later studies on isolated mitochondria were shifted to the artifical temperature of 25 °C.
Today, the importance of investigating mitochondrial performance at in vivo temperatures is recognized again in mitochondrial physiology. Incubation times of 1 hour were typical in experiments with the Warburg apparatus, but were reduced to a few or up to 20 min, following Chance and Williams, due to rapid oxygen depletion in closed, aqueous phase oxygraphs with high sample concentrations. Today, incubation times of 1 hour are typical again in high-resolution respirometry, with low sample concentrations and the option of reoxygenations.
Oesper P (1964) The history of the Warburg apparatus: Some reminiscences on its use. J Chem Educ 41: 294.
Koppenol WH, Bounds PL, Dang CV (2011) Otto Warburg’s contributions to current concepts of cancer metabolism. Nature Reviews Cancer 11: 325-337.
Gnaiger E, Kemp RB (1990) Anaerobic metabolism in aerobic mammalian cells: information from the ratio of calorimetric heat flux and respirometric oxygen flux. Biochim Biophys Acta 1016: 328-332. – “At high fructose concentrations, respiration is inhibited while glycolytic end products accumulate, a phenomenon known as the Crabtree effect. It is commonly believed that this effect is restricted to microbial and tumour cells with uniquely high glycolytic capacities (Sussman et al, 1980). However, inhibition of respiration and increase of lactate production are observed under aerobic conditions in beating rat heart cell cultures (Frelin et al, 1974) and in isolated rat lung cells (Ayuso-Parrilla et al, 1978). Thus, the same general mechanisms responsible for the integration of respiration and glycolysis in tumour cells (Sussman et al, 1980) appear to be operating to some extent in several isolated mammalian cells.”
Mitochondria are sometimes described as “cellular power plants” because they generate most of the cell’s supply of adenosine triphosphate (ATP), used as a source of chemical energy.[2] In addition to supplying cellular energy, mitochondria are involved in other tasks such as signaling, cellular differentiation, cell death, as well as the control of the cell cycle and cell growth.[3] The organelle is composed of compartments that carry out specialized functions. These compartments or regions include the outer membrane, the intermembrane space, the inner membrane, and the cristae and matrix. Mitochondrial proteins vary depending on the tissue and the species. In humans, 615 distinct types of proteins have been identified from cardiac mitochondria,[9Leonor Michaelis discovered that Janus green can be used as a supravital stain for mitochondria in 1900. Benjamin F. Kingsbury, in 1912, first related them with cell respiration, but almost exclusively based on morphological observations.[13] In 1913 particles from extracts of guinea-pig liver were linked to respiration by Otto Heinrich Warburg, which he called “grana”. Warburg and Heinrich Otto Wieland, who had also postulated a similar particle mechanism, disagreed on the chemical nature of the respiration. It was not until 1925 when David Keilin discovered cytochromes that the respiratory chain was described.[13]
The Clark Oxygen Sensor
Dr. Leland Clark – inventor of the “Clark Oxygen Sensor” (1954); the Clark type polarographic oxygen sensor remains the gold standard for measuring dissolved oxygen in biomedical, environmental and industrial applications . ‘The convenience and simplicity of the polarographic ‘oxygen electrode’ technique for measuring rapid changes in the rate of oxygen utilization by cellular and subcellular systems is now leading to its more general application in many laboratories. The types and design of oxygen electrodes vary, depending on the investigator’s ingenuity and specific requirements of the system under investigation.’Estabrook R (1967) Mitochondrial respiratory control and the polarographic measurement of ADP:O ratios. Methods Enzymol. 10: 41-47. “one approach that is underutilized in whole-cell bioenergetics, and that is accessible as long as cells can be obtained in suspension, is the oxygen electrode, which can obtain more precise information on the bioenergetic status of the in situ mitochondria than more ‘high-tech’ approaches such as fluorescent monitoring ofΔψm.” Nicholls DG, Ferguson S (2002) Bioenergetics 3. Academic Press, London.
Great Figures in Cancer
Dr. Elizabeth Blackburn,
j_michael_bishop onogene
Harold Varmus
Potts and Habener (PTH mRNA, Harvard MIT) JCI
JCI Fuller Albright and hPTH AA sequence
Dr. E. Donnall Thomas Bone Marrow Transplants
Dr Haraldzur Hausen EBV HPV
Dr. Craig Mello
Lee Hartwell – Hutchinson Cancer Res Center
Judah Folkman, MD
Gertrude B. Elien (1918-1999)
The Nobel Prize in Physiology or Medicine 1922
Archibald V. Hill, Otto Meyerhof
AV Hill –
“the production of heat in the muscle” Hill started his research work in 1909. It was due to J.N. Langley, Head of the Department of Physiology at that time that Hill took up the study on the nature of muscular contraction. Langley drew his attention to the important (later to become classic) work carried out by Fletcher and Hopkins on the problem of lactic acid in muscle, particularly in relation to the effect of oxygen upon its removal in recovery. In 1919 he took up again his study of the physiology of muscle, and came into close contact with Meyerhof of Kiel who, approaching the problem differently, arrived at results closely analogous to his study. In 1919 Hill’s friend W. Hartree, mathematician and engineer, joined in the myothermic investigations – a cooperation which had rewarding results.
Otto Meyerhof –
otto-fritz-meyerhof
lactic acid production in muscle contraction Under the influence of Otto Warburg, then at Heidelberg, Meyerhof became more and more interested in cell physiology. In 1923 he was offered a Professorship of Biochemistry in the United States, but Germany was unwilling to lose him. In 1929 he was he was placed in charge of the newly founded Kaiser Wilhelm Institute for Medical Research at Heidelberg. From 1938 to 1940 he was Director of Research at the Institut de Biologie physico-chimique at Paris, but in 1940 he moved to the United States, where the post of Research Professor of Physiological Chemistry had been created for him by the University of Pennsylvania and the Rockefeller Foundation. Meyerhof’s own account states that he was occupied chiefly with oxidation mechanisms in cells and with extending methods of gas analysis through the calorimetric measurement of heat production, and especially the respiratory processes of nitrifying bacteria. The physico-chemical analogy between oxygen respiration and alcoholic fermentation caused him to study both these processes in the same subject, namely, yeast extract. By this work he discovered a co-enzyme of respiration, which could be found in all the cells and tissues up till then investigated. At the same time he also found a co-enzyme of alcoholic fermentation. He also discovered the capacity of the SH-group to transfer oxygen; after Hopkins had isolated from cells the SH bodies concerned, Meyerhof showed that the unsaturated fatty acids in the cell are oxidized with the help of the sulfhydryl group. After studying closer the respiration of muscle, Meyerhof investigated the energy changes in muscle. Considerable progress had been achieved by the English scientists Fletcher and Hopkins by their recognition of the fact that lactic acid formation in the muscle is closely connected with the contraction process. These investigations were the first to throw light upon the highly paradoxical fact, already established by the physiologist Hermann, that the muscle can perform a considerable part of its external function in the complete absence of oxygen.
But it was indisputable that in the last resort the energy for muscle activity comes from oxidation, so the connection between activity and combustion must be an indirect one, and observed that in the absence of oxygen in the muscle, lactic acid appears, slowly in the relaxed state and rapidly in the active state, disappearing in the presence of oxygen. Obviously, then, oxygen is involved when muscle is in the relaxed state. http://upload.wikimedia.org/wikipedia/commons/e/e1/Glycolysis.jpg
The Nobel Prize committee had been receiving nominations intermittently for the previous 14 years (for Eijkman, Funk, Goldberger, Grijns, Hopkins and Suzuki but, strangely, not for McCollum in this period). Tthe Committee for the 1929 awards apparently agreed that it was high time to honor the discoverer(s) of vitamins; but who were they? There was a clear case for Grijns, but he had not been re-nominated for that particular year, and it could be said that he was just taking the relatively obvious next steps along the new trail that had been laid down by Eijkman, who was also now an old man in poor health, but there was no doubt that he had taken the first steps in the use of an animal model to investigate the nutritional basis of a clinical disorder affecting millions. Goldberger had been another important contributor, but his recent death put him out of consideration. The clearest evidence for lack of an unknown “something” in a mammalian diet was presented by Gowland Hopkins in 1912. This Cambridge biochemist was already well known for having isolated the amino acid tryptophan from a protein and demonstrated its essential nature. He fed young rats on an experimental diet, half of them receiving a daily milk supplement, and only those receiving milk grew well, Hopkins suggested that this was analogous to human diseases related to diet, as he had suggested already in a lecture published in 1906. Hopkins, the leader of the “dynamic biochemistry” school in Britain and an influential advocate for the importance of vitamins, was awarded the prize jointly with Eijkman. A door was opened. Recognition of work on the fat-soluble vitamins begun by McCollum. The next award related to vitamins was given in 1934 to George Whipple, George Minot and William Murphy “for their discoveries concerning liver therapy in cases of [then incurable pernicious] anemia,” The essential liver factor (cobalamin, or vitamin B12) was isolated in 1948, and Vitamin B12 was absent from plant foods. But William Castle in 1928 had demonstrated that the stomachs of pernicious anemia patients were abnormal in failing to secrete an “intrinsic factor”.
Szent-Györgyi was a Hungarian biochemist who had worked with Otto Warburg and had a special interest in oxidation-reduction mechanisms. He was invited to Cambridge in England in 1927 after detecting an antioxidant compound in the adrenal cortex, and there, he isolated a compound that he named hexuronic acid. Charles Glen King of the University of Pittsburgh reported success In isolating the anti-scorbutic factor in 1932, and added that his crystals had all the properties reported by Szent-Györgyi for hexuronic acid. But his work on oxidation reactions was also important. Fumarate is an intermediate in the citric acid cycle used by cells to produce energy in the form of adenosine triphosphate (ATP) from food. It is formed by the oxidation of succinate by the enzyme succinate dehydrogenase. Fumarate is then converted by the enzyme fumarase to malate. An enzyme adds water to the fumarate molecule to form malate. The malate is created by adding one hydrogen atom to a carbon atom and then adding a hydroxyl group to a carbon next to a terminal carbonyl group.
In the same year, Norman Haworth from the University of Birmingham in England received a Nobel prize from the Chemistry Committee for having advanced carbohydrate chemistry and, specifically, for having worked out the structure of Szent-Györgyi’s crystals, and then been able to synthesize the vitamin. This was a considerable achievement. The Nobel Prize in Chemistry was shared with the Swiss organic chemist Paul Karrer, cited for his work on the structures of riboflavin and vitamins A and E as well as other biologically interesting compounds. This was followed in 1938 by a further Chemistry award to the German biochemist Richard Kuhn, who had also worked on carotenoids and B-vitamins, including riboflavin and pyridoxine. But Karrer was not permitted to leave Germany at that time by the Nazi regime. However, the American work with radioisotopes at Lawrence Livermore Laboratory, UC Berkeley, was already ushering in a new era of biochemistry that would enrich our studies of metabolic pathways. The importance of work involving vitamins was acknowledged in at least ten awards in the 20th century.
1. Carpenter, K.J., Beriberi, White Rice and Vitamin B, University of California Press, Berkeley (2000).
2. Weatherall, M.W. and Kamminga, H., The making of a biochemist: the construction of Frederick Gowland Hopkins’ reputation. Medical History vol.40, pp. 415-436 (1996).
3. Becker, S.L., Will milk make them grow? An episode in the discovery of the vitamins. In Chemistry and Modern Society (J. Parascandela, editor) pp. 61-83, American Chemical Society,
Washington, D.C. (1983).
4. Carpenter, K.J., The History of Scurvy and Vitamin C, Cambridge University Press, New York (1986).
Transport and metabolism of exogenous fumarate and 3-phosphoglycerate in vascular smooth muscle.
The keto (linear) form of exogenous fructose 1,6-bisphosphate, a highly charged glycolytic intermediate, may utilize a dicarboxylate transporter to cross the cell membrane, support glycolysis, and produce ATP anaerobically. We tested the hypothesis that fumarate, a dicarboxylate, and 3-phosphoglycerate (3-PG), an intermediate structurally similar to a dicarboxylate, can support contraction in vascular smooth muscle during hypoxia. 3-PG improved maintenance of force (p < 0.05) during the 30-80 min period of hypoxia. Fumarate decreased peak isometric force development by 9.5% (p = 0.008) but modestly improved maintenance of force (p < 0.05) throughout the first 80 min of hypoxia. 13C-NMR on tissue extracts and superfusates revealed 1,2,3,4-(13)C-fumarate (5 mM) metabolism to 1,2,3,4-(13)C-malate under oxygenated and hypoxic conditions suggesting uptake and metabolism of fumarate. In conclusion, exogenous fumarate and 3-PG readily enter vascular smooth muscle cells, presumably by a dicarboxylate transporter, and support energetically important pathways.
Comparison of endogenous and exogenous sources of ATP in fueling Ca2+ uptake in smooth muscle plasma membrane vesicles.
A smooth muscle plasma membrane vesicular fraction (PMV) purified for the (Ca2+/Mg2+)-ATPase has endogenous glycolytic enzyme activity. In the presence of glycolytic substrate (fructose 1,6-diphosphate) and cofactors, PMV produced ATP and lactate and supported calcium uptake. The endogenous glycolytic cascade supports calcium uptake independent of bath [ATP]. A 10-fold dilution of PMV, with the resultant 10-fold dilution of glycolytically produced bath [ATP] did not change glycolytically fueled calcium uptake (nanomoles per milligram protein). Furthermore, the calcium uptake fueled by the endogenous glycolytic cascade persisted in the presence of a hexokinase-based ATP trap which eliminated calcium uptake fueled by exogenously added ATP. Thus, it appears that the endogenous glycolytic cascade fuels calcium uptake in PMV via a membrane-associated pool of ATP and not via an exchange of ATP with the bulk solution. To determine whether ATP produced endogenously was utilized preferentially by the calcium pump, the ATP production rates of the endogenous creatine kinase and pyruvate kinase were matched to that of glycolysis and the calcium uptake fueled by the endogenous sources was compared with that fueled by exogenous ATP added at the same rate. The rate of calcium uptake fueled by endogenous sources of ATP was approximately twice that supported by exogenously added ATP, indicating that the calcium pump preferentially utilizes ATP produced by membrane-bound enzymes.
Evidence for succinate production by reduction of fumarate during hypoxia in isolated adult rat heart cells.
Archives of Biochemistry and Biophysics (Impact Factor: 3.37). 01/1988; 259(2):527-35. http://dx.doi.org:/10.1016/0003-9861(87)90519-4 It has been demonstrated that perfusion of myocardium with glutamic acid or tricarboxylic acid cycle intermediates during hypoxia or ischemia, improves cardiac function, increases ATP levels, and stimulates succinate production. In this study isolated adult rat heart cells were used to investigate the mechanism of anaerobic succinate formation and examine beneficial effects attributed to ATP generated by this pathway. Myocytes incubated for 60 min under hypoxic conditions showed a slight loss of ATP from an initial value of 21 +/- 1 nmol/mg protein, a decline of CP from 42 to 17 nmol/mg protein and a fourfold increase in lactic acid production to 1.8 +/- 0.2 mumol/mg protein/h. These metabolite contents were not altered by the addition of malate and 2-oxoglutarate to the incubation medium nor were differences in cell viability observed; however, succinate release was substantially accelerated to 241 +/- 53 nmol/mg protein. Incubation of cells with [U-14C]malate or [2-U-14C]oxoglutarate indicates that succinate is formed directly from malate but not from 2-oxoglutarate. Moreover, anaerobic succinate formation was rotenone sensitive.
We conclude that malate reduction to succinate occurs via the reverse action of succinate dehydrogenase in a coupled reaction where NADH is oxidized (and FAD reduced) and ADP is phosphorylated.Furthermore, by transaminating with aspartate to produce oxaloacetate, 2-oxoglutarate stimulates cytosolic malic dehydrogenase activity, whereby malate is formed and NADH is oxidized.
In the form of malate, reducing equivalents and substrate are transported into the mitochondria where they are utilized for succinate synthesis.
1953 Hans Adolf Krebs –
” discovery of the citric acid cycle” and In the course of the 1920’s and 1930’s great progress was made in the study of the intermediary reactions by which sugar is anaerobically fermented to lactic acid or to ethanol and carbon dioxide. The success was mainly due to the joint efforts of the schools of Meyerhof, Embden, Parnas, von Euler, Warburg and the Coris, who built on the pioneer work of Harden and of Neuberg. This work brought to light the main intermediary steps of anaerobic fermentations.
In contrast, very little was known in the earlier 1930’s about the intermediary stages through which sugar is oxidized in living cells. When, in 1930, I left the laboratory of Otto Warburg (under whose guidance I had worked since 1926 and from whom I have learnt more than from any other single teacher), I was confronted with the question of selecting a major field of study and I felt greatly attracted by the problem of the intermediary pathway of oxidations.
These reactions represent the main energy source in higher organisms, and in view of the importance of energy production to living organisms (whose activities all depend on a continuous supply of energy) the problem seemed well worthwhile studying. http://www.johnkyrk.com/krebs.html
Interactive Krebs cycle
There are different points where metabolites enter the Krebs’ cycle. Most of the products of protein, carbohydrates and fat metabolism are reduced to the molecule acetyl coenzyme A that enters the Krebs’ cycle. Glucose, the primary fuel in the body, is first metabolized into pyruvic acid and then into acetyl coenzyme A. The breakdown of the glucose molecule forms two molecules of ATP for energy in the Embden Meyerhof pathway process of glycolysis.
On the other hand, amino acids and some chained fatty acids can be metabolized into Krebs intermediates and enter the cycle at several points. When oxygen is unavailable or the Krebs’ cycle is inhibited, the body shifts its energy production from the Krebs’ cycle to the Embden Meyerhof pathway of glycolysis, a very inefficient way of making energy.
Fritz Albert Lipmann –
“discovery of co-enzyme A and its importance for intermediary metabolism”.
In my development, the recognition of facts and the rationalization of these facts into a unified picture, have interplayed continuously. After my apprenticeship with Otto Meyerhof, a first interest on my own became the phenomenon we call the Pasteur effect, this peculiar depression of the wasteful fermentation in the respiring cell. By looking for a chemical explanation of this economy measure on the cellular level, I was prompted into a study of the mechanism of pyruvic acid oxidation, since it is at the pyruvic stage where respiration branches off from fermentation.
For this study I chose as a promising system a relatively simple looking pyruvic acid oxidation enzyme in a certain strain of Lactobacillus delbrueckii1. In 1939, experiments using minced muscle cells demonstrated that one oxygen atom can form two adenosine triphosphate molecules, and, in 1941, the concept of phosphate bonds being a form of energy in cellular metabolism was developed by Fritz Albert Lipmann.
In the following years, the mechanism behind cellular respiration was further elaborated, although its link to the mitochondria was not known.[13]The introduction of tissue fractionation by Albert Claude allowed mitochondria to be isolated from other cell fractions and biochemical analysis to be conducted on them alone. In 1946, he concluded that cytochrome oxidase and other enzymes responsible for the respiratory chain were isolated to the mitchondria. Over time, the fractionation method was tweaked, improving the quality of the mitochondria isolated, and other elements of cell respiration were determined to occur in the mitochondria.[13]
The most important event during this whole period, I now feel, was the accidental observation that in the L. delbrueckii system, pyruvic acid oxidation was completely dependent on the presence of inorganic phosphate. This observation was made in the course of attempts to replace oxygen by methylene blue. To measure the methylene blue reduction manometrically, I had to switch to a bicarbonate buffer instead of the otherwise routinely used phosphate. In bicarbonate, pyruvate oxidation was very slow, but the addition of a little phosphate caused a remarkable increase in rate. The phosphate effect was removed by washing with a phosphate free acetate buffer. Then it appeared that the reaction was really fully dependent on phosphate.
A coupling of this pyruvate oxidation with adenylic acid phosphorylation was attempted. Addition of adenylic acid to the pyruvic oxidation system brought out a net disappearance of inorganic phosphate, accounted for as adenosine triphosphate. The acetic acid subunit of acetyl CoA is combined with oxaloacetate to form a molecule of citrate. Acetyl coenzyme A acts only as a transporter of acetic acid from one enzyme to another. After Step 1, the coenzyme is released by hydrolysis to combine with another acetic acid molecule and begin the Krebs’ Cycle again.
Hugo Theorell –
“the nature and effects of oxidation enzymes”
From 1933 until 1935 Theorell held a Rockefeller Fellowship and worked with Otto Warburg at Berlin-Dahlem, and here he became interested in oxidation enzymes. At Berlin-Dahlem he produced, for the first time, the oxidation enzyme called «the yellow ferment» and he succeeded in splitting it reversibly into a coenzyme part, which was found to be flavin mononucleotide, and a colourless protein part. On return to Sweden, he was appointed Head of the newly established Biochemical Department of the Nobel Medical Institute, which was opened in 1937.
Succinate is oxidized by a molecule of FAD (Flavin Adenine Dinucleotide). The FAD removes two hydrogen atoms from the succinate and forms a double bond between the two carbon atoms to create fumarate.
They followed the path that became clear from intense collaborative work in California by George Beadle, by Avery and McCarthy, Max Delbruck, TH Morgan, Max Delbruck and by Chargaff that indicated that genetics would be important.
1965
François Jacob, André Lwoff and Jacques Monod –
” genetic control of enzyme and virus synthesis”.
In 1958 the remarkable analogy revealed by genetic analysis of lysogeny and that of the induced biosynthesis of ß-galactosidase led François Jacob, with Jacques Monod, to study the mechanisms responsible for the transfer of genetic information as well as the regulatory pathways which, in the bacterial cell, adjust the activity and synthesis of macromolecules. Following this analysis, Jacob and Monod proposed a series of new concepts, those of messenger RNA, regulator genes, operons and allosteric proteins.
Francois Jacob
Having determined the constants of growth in the presence of different carbohydrates, it occurred to me that it would be interesting to determine the same constants in paired mixtures of carbohydrates. From the first experiment on, I noticed that, whereas the growth was kinetically normal in the presence of certain mixtures (that is, it exhibited a single exponential phase), two complete growth cycles could be observed in other carbohydrate mixtures, these cycles consisting of two exponential phases separated by a-complete cessation of growth.
Lwoff, after considering this strange result for a moment, said to me, “That could have something to do with enzyme adaptation.”
“Enzyme adaptation? Never heard of it!” I said.
Lwoff’s only reply was to give me a copy of the then recent work of Marjorie Stephenson, in which a chapter summarized with great insight the still few studies concerning this phenomenon, which had been discovered by Duclaux at the end of the last century. Studied by Dienert and by Went as early as 1901 and then by Euler and Josephson, it was more or less rediscovered by Karström, who should be credited with giving it a name and attracting attention to its existence.
Lwoff’s intuition was correct. The phenomenon of “diauxy” that I had discovered was indeed closely related to enzyme adaptation, as my experiments, included in the second part of my doctoral dissertation, soon convinced me. It was actually a case of the “glucose effect” discovered by Dienert as early as 1900. That agents that uncouple oxidative phosphorylation, such as 2,4-dinitrophenol, completely inhibit adaptation to lactose or other carbohydrates suggested that “adaptation” implied an expenditure of chemical potential and therefore probably involved the true synthesis of an enzyme.
With Alice Audureau, I sought to discover the still quite obscure relations between this phenomenon and the one Massini, Lewis, and others had discovered: the appearance and selection of “spontaneous” mutants. We showed that an apparently spontaneous mutation was allowing these originally “lactose-negative” bacteria to become “lactose-positive”. However, we proved that the original strain (Lac-) and the mutant strain (Lac+) did not differ from each other by the presence of a specific enzyme system, but rather by the ability to produce this system in the presence of lactose. This mutation involved the selective control of an enzyme by a gene, and the conditions necessary for its expression seemed directly linked to the chemical activity of the system.
1974
Albert Claude, Christian de Duve and George E. Palade –
” the structural and functional organization of the cell”.
I returned to Louvain in March 1947 after a period of working with Theorell in Sweden, the Cori’s, and E Southerland in St. Louis, fortunate in the choice of my mentors, all sticklers for technical excellence and intellectual rigor, those prerequisites of good scientific work. Insulin, together with glucagon which I had helped rediscover, was still my main focus of interest, and our first investigations were accordingly directed on certain enzymatic aspects of carbohydrate metabolism in liver, which were expected to throw light on the broader problem of insulin action. But I became distracted by an accidental finding related to acid phosphatase, drawing most of my collaborators along with me. The studies led to the discovery of the lysosome, and later of the peroxisome.
In 1962, I was appointed a professor at the Rockefeller Institute in New York, now the Rockefeller University, the institution where Albert Claude had made his pioneering studies between 1929 and 1949, and where George Palade had been working since 1946. In New York, I was able to develop a second flourishing group, which follows the same general lines of research as the Belgian group, but with a program of its own.
1968
Robert W. Holley, Har Gobind Khorana and Marshall W. Nirenberg –
“interpretation of the genetic code and its function in protein synthesis”.
1969
Max Delbrück, Alfred D. Hershey and Salvador E. Luria –
” the replication mechanism and the genetic structure of viruses”.
1975 David Baltimore, Renato Dulbecco and Howard Martin Temin –
” the interaction between tumor viruses and the genetic material of the cell”.
1976
Baruch S. Blumberg and D. Carleton Gajdusek –
” new mechanisms for the origin and dissemination of infectious diseases” The editors of the Nobelprize.org website of the Nobel Foundation have asked me to provide a supplement to the autobiography that I wrote in 1976 and to recount the events that happened after the award. Much of what I will have to say relates to the scientific developments since the last essay. These are described in greater detail in a scientific memoir first published in 2002 (Blumberg, B. S., Hepatitis B. The Hunt for a Killer Virus, Princeton University Press, 2002, 2004).
1980
Baruj Benacerraf, Jean Dausset and George D. Snell
” genetically determined structures on the cell surface that regulate immunological reactions”.
1992
Edmond H. Fischer and Edwin G. Krebs
“for their discoveries concerning reversible protein phosphorylation as a biological regulatory mechanism”
1994
Alfred G. Gilman and Martin Rodbell –
“G-proteins and the role of these proteins in signal transduction in cells”
2011
Bruce A. Beutler and Jules A. Hoffmann –
” the activation of innate immunity“and the other half to Ralph M. Steinman – “the dendritic cell and its role in adaptive immunity”.
Renato L. Baserga, M.D.
Kimmel Cancer Center and Keck School of Medicine
Dr. Baserga’s research focuses on the multiple roles of the type 1 insulin-like growth factor receptor (IGF-IR) in the proliferation of mammalian cells. The IGF-IR activated by its ligands is mitogenic, is required for the establishment and the maintenance of the transformed phenotype, and protects tumor cells from apoptosis. It, therefore, serves as an excellent target for therapeutic interventions aimed at inhibiting abnormal growth. In basic investigations, this group is presently studying the effects that the number of IGF-IRs and specific mutations in the receptor itself have on its ability to protect cells from apoptosis.
This investigation is strictly correlated with IGF-IR signaling, and part of this work tries to elucidate the pathways originating from the IGF-IR that are important for its functional effects. Baserga’s group has recently discovered a new signaling pathway used by the IGF-IR to protect cells from apoptosis, a unique pathway that is not used by other growth factor receptors. This pathway depends on the integrity of serines 1280-1283 in the C-terminus of the receptor, which bind 14.3.3 and cause the mitochondrial translocation of Raf-1.
Another recent discovery of this group has been the identification of a mechanism by which the IGF-IR can actually induce differentiation in certain types of cells. When cells have IRS-1 (a major substrate of the IGF-IR), the IGF-IR sends a proliferative signal; in the absence of IRS-1, the receptor induces cell differentiation. The extinction of IRS-1 expression is usually achieved by DNA methylation.
Janardan Reddy, MD
Northwestern University
The central effort of our research has been on a detailed analysis at the cellular and molecular levels of the pleiotropic responses in liver induced by structurally diverse classes of chemicals that include fibrate class of hypolipidemic drugs, and phthalate ester plasticizers, which we designated hepatic peroxisome proliferators. Our work has been central to the establishment of several principles, namely that hepatic peroxisome proliferation is associated with increases in fatty acid oxidation systems in liver, and that peroxisome proliferators, as a class, are novel nongenotoxic hepatocarcinogens.
We introduced the concept that sustained generation of reactive oxygen species leads to oxidative stress and serves as the basis for peroxisome proliferator-induced liver cancer development. Furthermore, based on the tissue/cell specificity of pleiotropic responses and the coordinated transcriptional regulation of fatty acid oxidation system genes, we postulated that peroxisome proliferators exert their action by a receptor-mediated mechanism. This receptor concept laid the foundation for the discovery of
a three member peroxisome proliferator-activated receptor (PPARalpha-, ß-, and gamma) subfamily of nuclear receptors.
PPARalpha is responsible for peroxisome proliferator-induced pleiotropic responses, including
hepatocarcinogenesis and energy combustion as it serves as a fatty acid sensor and regulates fatty acid oxidation.
Our current work focuses on the molecular mechanisms responsible for PPAR action and generation of fatty acid oxidation deficient mouse knockout models. Transcription of specific genes by nuclear receptors is a complex process involving the participation of multiprotein complexes composed of transcription coactivators.
Jose Delgado de Salles Roselino, Ph.D.
Leloir Institute, Brazil
Warburg effect, in reality “Pasteur-effect” was the first example of metabolic regulation described. A decrease in the carbon flux originated at the sugar molecule towards the end metabolic products, ethanol and carbon dioxide that was observed when yeast cells were transferred from anaerobic environmental condition to an aerobic one. In Pasteur´s works, sugar metabolism was measured mainly by the decrease of sugar concentration in the yeast growth media observed after a measured period of time. The decrease of the sugar concentration in the media occurs at great speed in yeast grown in anaerobiosis condition and its speed was greatly reduced by the transfer of the yeast culture to an aerobic condition. This finding was very important for the wine industry of France in Pasteur time, since most of the undesirable outcomes in the industrial use of yeast were perceived when yeasts cells took very long time to create a rather selective anaerobic condition. This selective culture media was led by the carbon dioxide higher levels produced by fast growing yeast cells and by a great alcohol content in the yeast culture media. This finding was required to understand Lavoisier’s results indicating that chemical and biological oxidation of sugars produced the same calorimetric results. This observation requires a control mechanism (metabolic regulation) to avoid burning living cells by fast heat released by the sugar biological oxidative processes (metabolism). In addition, Lavoisier´s results were the first indications that both processes happened inside similar thermodynamics limits.
In much resumed form, these observations indicates the major reasons that led Warburg to test failure in control mechanisms in cancer cells in comparison with the ones observed in normal cells. Biology inside classical thermo dynamics poses some challenges to scientists. For instance, all classical thermodynamics must be measured in reversible thermodynamic conditions. In an isolated system, increase in P (pressure) leads to decrease in V (volume) all this in a condition in which infinitesimal changes in one affects in the same way the other, a continuum response. Not even a quantic amount of energy will stand beyond those parameters. In a reversible system, a decrease in V, under same condition, will led to an increase in P.
In biochemistry, reversible usually indicates a reaction that easily goes from A to B or B to A. This observation confirms the important contribution of E Schrodinger in his What´s Life: “This little book arose from a course of public lectures, delivered by a theoretical physicist to an audience of about four hundred which did not substantially dwindle, though warned at the outset that the subject-matter was a difficult one and that the lectures could not be termed popular, even though the physicist’s most dreaded weapon, mathematical deduction, would hardly be utilized. The reason for this was not that the subject was simple enough to be explained without mathematics, but rather that it was much too involved to be fully accessible to mathematics.”
Hans Krebs describes the cyclic nature of the citrate metabolism. Two major research lines search to understand the mechanism of energy transfer that explains how ADP is converted into ATP. One followed the organic chemistry line of reasoning and therefore, searched how the breakdown of carbon-carbon link could have its energy transferred to ATP synthesis. A major leader of this research line was B. Chance who tried to account for two carbon atoms of acetyl released as carbon dioxide in the series of Krebs cycle reactions. The intermediary could store in a phosphorylated amino acid the energy of carbon-carbon bond breakdown. This activated amino acid could transfer its phosphate group to ADP producing ATP. Alternatively, under the possible influence of the excellent results of Hodgkin and Huxley a second line of research appears.
The work of Hodgkin & Huxley indicated the storage of electrical potential energy in transmembrane ionic asymmetries and presented the explanation for the change from resting to action potential in excitable cells. This second line of research, under the leadership of P Mitchell postulated a mechanism for the transfer of oxide/reductive power of organic molecules oxidation through electron transfer as the key for energetic transfer mechanism required for ATP synthesis. Paul Boyer could present how the energy was transduced by a molecular machine that changes in conformation in a series of 3 steps while rotating in one direction in order to produce ATP and in opposite direction in order to produce ADP plus Pi from ATP (reversibility). Nonetheless, a victorious Peter Mitchell obtained the correct result in the conceptual dispute, over the B. Chance point of view, after he used E. Coli mutants to show H gradients in membrane and its use as energy source.
However, this should not detract from the important work of Chance. B. Chance got the simple and rapid polarographic assay method of oxidative phosphorylation and the idea of control of energy metabolism that bring us back to Pasteur. This second result seems to have been neglected in searching for a single molecular mechanism required for the understanding of the buildup of chemical reserve in our body. In respiring mitochondria the rate of electron transport, and thus the rate of ATP production, is determined primarily by the relative concentrations of ADP, ATP and phosphate in the external media (cytosol) and not by the concentration of respiratory substrate as pyruvate. Therefore, when the yield of ATP is high as is in aerobiosis and the cellular use of ATP is not changed, the oxidation of pyruvate and therefore of glycolysis is quickly (without change in gene expression), throttled down to the resting state. The dependence of respiratory rate on ADP concentration is also seen in intact cells. A muscle at rest and using no ATP has very low respiratory rate.
I have had an ongoing discussion with Jose Eduardo de Salles Roselino, inBrazil. He has made important points that need to be noted.
The constancy of composition which animals maintain in the environment surrounding their cells is one of the dominant features of their physiology. Although this phenomenon, homeostasis, has held the interest of biologists over a long period of time, the elucidation of the molecular basis for complex processes such as temperature control and the maintenance of various substances at constant levels in the blood has not yet been achieved. By comparison, metabolic regulation in microorganisms is much better understood, in part because the microbial physiologist has focused his attention on enzyme-catalyzed reactions and their control, as these are among the few activities of microorganisms amenable to quantitative study. Furthermore, bacteria are characterized by their ability to make rapid and efficient adjustments to extensive variations in most parameters of their environment; therefore, they exhibit a surprising lack of rigid requirements for their environment, and appears to influence it only as an incidental result of their metabolism. Animal cells on the other hand have only a limited capacity for adjustment and therefore require a constant milieu. Maintenance of such constancy appears to be a major goal in their physiology (Regulation of Biosynthetic Pathways H.S. Moyed and H EUmbarger Phys Rev,42 444 (1962)).
A living cell consists in a large part of a concentrated mixture of hundreds of different enzymes, each a highly effective catalyst for one or more chemical reactions involving other components of the cell. The paradox of intense and highly diverse chemical activity on the one hand and strongly poised chemical stability (biological homeostasis) on the other is one of the most challenging problems of biology (Biological feedback Control at the molecular Level D.E. Atkinson Science vol. 150: 851, 1965). Almost nothing is known concerning the actual molecular basis for modulation of an enzyme`s kinetic behavior by interaction with a small molecule. (Biological feedback Control at the molecular Level D.E. Atkinson Science vol. 150: 851, 1965). In the same article, since the core of Atkinson´s thinking seems to be strongly linked with Adenylates as regulatory effectors, the previous phrases seems to indicate a first step towards the conversion of homeostasis to an intracellular phenomenon and therefore, one that contrary to Umbarger´s consideration could be also studied in microorganisms.
Most biochemical studies using bacteria, were made before the end of the third upper part of log growth phase. Therefore, they could be considered as time-independent as S Luria presented biochemistry in Life an Unfinished Experiment. The sole ingredient on the missing side of the events that led us into the molecular biology construction was to consider that proteins, a macromolecule, would never be affected by small molecules translational kinetic energy. This, despite the fact that in a catalytic environment and its biological implications S Grisolia incorporated A K Balls observation indicating that the word proteins could be related to Proteus an old sea god that changed its form whenever he was subjected to inquiry (Phys Rev v 4,657 (1964).
In D.E. Atkinson´s work (Science vol 150 p 851, 1965), changes in protein synthesis acting together with factors that interfere with enzyme activity will lead to “fine-tuned” regulation better than enzymatic activity regulation alone. Comparison of glycemic regulation in granivorous and carnivorous birds indicate that when no important nutritional source of glucose is available, glycemic levels can be kept constant in fasted and fed birds. The same was found in rats and cats fed on high protein diets. Gluconeogenesis is controlled by pyruvate kinase inhibition. Therefore, the fact that it can discriminate between fasting alone and fasting plus exercise (carbachol) requirement of gluconeogenic activity (correspondent level of pyruvate kinase inhibition) the control of enzyme activity can be made fast and efficient without need for changes in genetic expression (20 minute after stimulus) ( Migliorini,R.H. et al Am J. Physiol.257 (Endocrinol. Met. 20): E486, 1989). Regrettably, this was not discussed in the quoted work. So, when the control is not affected by the absorption of nutritional glucose it can be very fast, less energy intensive and very sensitive mechanism of control despite its action being made in the extracellular medium (homeostasis).
Genomics has had a rapid growth of research into variability of human genetics in both healthy populations in the study of population migration, and in the study of genetic sequence alterations that may increase the risk of expressed human disease. This is the case for cardiology, cancer, inflammtory conditions, and gastrointestinal diseases. For the most part, genomics research in the last decade has shed light on potential therapeutic targets, but the identification of drug toxicities in late phase trials has been associated with a 70 percent failure rate in bringing new drugs to the market. Despite good technologies for investigative studies, initial work is carried out on animals and then the transferrability of the work from a “model” to man has to be assured. That is the first issue of concern.
Secondly, there is a well considered reluctance on the part of experienced and well prepared physicians to be “early” adopters to newly introduced drugs, with the apprehension that unidentified clinical problems can be expected to be unmasked. It is, however, easier to consider when a new drug belongs to an established class of medications, and it has removed known adverse effects. In this case, the adverse effects are known side effects, but not necessarily serious drug reactions that would preclude use.
A third consideration is the cost of drug development, and the cost of development is passed on to the healthcare organization in the purchasing cost. We can rest assured that the Pharmacy and Therapeutics Review Committee will not cease meeting on a regular schedule anytime soon. Further, how do the drug failures become embedded in the cost of the pharmaceutical budget passed on to the recipient. Historically, insurance is an actuarial discipline. But in the lifetime of an individual, they are bound to see a physician for acute or chronic medical attention. Only the timing cannot be predicted. As a result, dealing with the valid introduction of new medications is a big concern for both the public and the private insurer.
How does this compute for the physician provider. The practice of medicine is not quickly adaptive, as the physician’s primary concern is to do no harm. Genomics testing is not widely available, and it is for the most part not definitive for diagnostic purposes as things stand today. It may provide assessment of risk, or of survival expectation. The physician uses a step by step assessment, using the patient and family history, a focused physical exam, laboratory and radiology, proceeding to other more specialized exams. Much of the laboratory testing is based on the appearance in the circulation of changes in blood chemistry of the nature of electrolytes, circulating cells in the blood and of the blood forming organ, proteins, urea and uric acid. They are not exquisitely sensitive, but they might be sufficient for their abnormal concentrations appearing at the time the patient presents with a complaint. What tests are ordered is determioned by a need for relevant information to make a medical decision.
The relevant questions are:
1. acuity of symptoms and signs. 2. actions to be taken. 3. tests that are needed to clarify the examination findings.
once a provisional diagnosis is obtained, referrals, additional testing, and medication orders are provided based on the assessment.
Where does genetic testing fit into this? At this point, it will only be used
to confirm a restricted list of diagnoses that have a high association with the condition, and
only with the participation of a medical geneticist, when
profiling the patient and other members of the family is required.
This article presents Advances in the Treatment using Subcutaneous Erythropoietin (EPO) and Intravenous Iron (Fe) for IMPROVEMENT of Severe and Resistant Congestive Heart Failure and its resultant Anemia. The Leading Biomarker for Congestive Heart Failure is an Independent Predictor identified as an Elevated N-terminal proBNP.
FIRST ARTICLE
Anemia as an Independent Predictor of Elevated N-terminal proBNP
Salman A. Haq, MD1, Mohammad E. Alam2, Larry Bernstein, MD, FCAP3, LB Banko 1, Leonard Y. Lee, MD, FACS4, Barry I. Saul, MD, FACC5, Terrence J. Sacchi, MD, FACC6, John F. Heitner, MD, FACC7
1Cardiology Fellow, 2 Clinical Chemistry Laboratories, 3 Program Director, Cardiothoracic Surgery, 4 Division of Cardiology, Department of Medicine, New York Methodist Hospital-Weill Cornell, Brooklyn, NY
(Unpublished manuscript) Poster Presentation
SECOND ARTICLE
The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study
Donald S Silverberg, MDa; Dov Wexler, MDa; David Sheps, MDa; Miriam Blum, MDa; Gad Keren, MDa; Ron Baruch, MDa; Doron Schwartz, MDa; Tatyana Yachnin, MDa; Shoshana Steinbruch, RNa; Itzhak Shapira, MDa; Shlomo Laniado, MDa; Adrian Iaina, MDa
J Am Coll Cardiol. 2001;37(7):1775-1780. doi:10.1016/S0735-1097(01)01248-7
The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations
Donald S Silverberg, MDa; Dov Wexler, MDa; Miriam Blum, MDa; Gad Keren, MDa; David Sheps, MDa; Eyal Leibovitch, MDa; David Brosh, MDa; Shlomo Laniado, MDa; Doron Schwartz, MDa; Tatyana Yachnin, MDa; Itzhak Shapira, MDa; Dov Gavish, MDa; Ron Baruch, MDa; Bella Koifman, MDa; Carl Kaplan, MDa; Shoshana Steinbruch, RNa; Adrian Iaina, MDa
J Am Coll Cardiol. 2000;35(7):1737-1744. doi:10.1016/S0735-1097(00)00613-6
This THREE article sequence is related by investigations occurring by me, a very skilled cardiologist and his resident, and my premedical student at New York Methodist Hospital-Weill Cornell, in Brooklyn, NY, while a study had earlier been done applying the concordant discovery, which the team in Israel had though was knowledge neglected. There certainly was no interest in the problem of the effect of anemia on the patient with severe congestive heart failure, even though erythropoietin was used widely in patients with end-stage renal disease requiring dialysis, and also for patients with myelofibrosis. The high cost of EPO was only one factor, the other being a guideline to maintain the Hb concentration at or near 11 g/dl – not higher. In the first article, the authors sought to determine whether the amino terminal pro– brain type natriuretic peptide (NT-pro BNP) is affected by anemia, and to determine that they excluded all patients who had renal insufficiency and/or CHF, since these were associated with elevated NT-proBNP. It was already well established that this pro-peptide is secreted by the heart with the action as a urinary sodium retention hormone on the kidney nephron, the result being an increase in blood volume. Perhaps the adaptation would lead to increased stroke volume from increased venous return, but that is not conjectured. However, at equilibrium, one would expect there to be increased red cell production to maintain the cell to plasma volume ratio, thereby, resulting in adequate oxygen exchange to the tissues. Whether that is always possible is uncertain because any reduction in the number of functioning nephrons would make the kidney not fully responsive at the Na+ exchange level, and the NT-pro BNP would rise. This introduces complexity into the investigation, requiring a removal of confounders to establish the effect of anemia.
The other two articles are related studies by the same group in Israel. They surmised that there was evidence that was being ignored as to the effect of anemia, and the treatment of anemia was essential in addition to other treatments. They carried out a randomized trial to determine just that, a benefit to treating the anemia. But they also conjectured that an anemia with a Hb concentration below 12 g/dl has an deleterious effect on the targeted population. Treatment by intermittent transfusions could potentially provide the added oxygen-carrying capacity, but the fractionation of blood, the potential for transfusion-transmitted disease and transfusion-reactions, combined with the need for the blood for traumatic blood loss made EPO a more favorable alternative to packed RBCs. The proof-of-concept is told below. Patients randomized to receive EPO at a lower than standard dose + iron did better.
Introduction
In this article, Erythropoietin (EPO) and Intravenous Iron (Fe) as Therapeutics for Anemia in Severe and Resistant CHF: The Elevated N-terminal proBNP Biomarker we provides a summary of three articles on the topic and we shading new light on the role that Anemia Hb < 12 g% plays as a Biomarker for CHF and for
prediction of elevated BNP, known as an indicator for the following Clinical Uses:
Prognosis in newly diagnosed heart failure patients: prediction of mortality/survival1
BNP
98
22
42
94
NT-proBNP
95
37
47
93
Prognosis post myocardial infarction: prediction of mortality2
BNP
86
72
39
96
NT-proBNP
91
72
39
97
Prognosis post myocardial infarction: prediction of heart failure2
BNP
85
73
54
93
NT-proBNP
82
69
50
91
PPV, positive predictive value; NPV, negative predictive value; LVEF, left ventricular ejection fraction; NG, not given.
Reference Range
BNP:
< 100 pg/mL13
proBNP, N-terminal:
≤ 300 pg/mL
The NT-proBNP reference range is based on EDTA plasma. Other sample types will produce higher values.
Interpretive Information
Symptomatic patients who present with a BNP or NT-proBNP level within the normal reference range are highly unlikely to have CHF. Conversely, an elevated baseline level indicates the need for further cardiac assessment and indicates the patient is at increased risk for future heart failure and mortality.BNP levels increase with age in the general population, with the highest concentrations seen in those greater than 75 years of age.14 Heart failure is unlikely in individuals with a BNP level <100 pg/mL and proBNP level ≤300 pg/mL. Heart failure is very likely in individuals with a BNP level >500 pg/mL and proBNP level ≥450 pg/mL who are <50 years of age, or ≥900 pg/mL for patients ≥50 years of age. Patients in between are either hypertensive or have mild ischemic or valvular disease and should be observed closely.15BNP is increased in CHF, left ventricular hypertrophy, acute myocardial infarction, atrial fibrillation, cardiac amyloidosis, and essential hypertension. Elevations are also observed in right ventricular dysfunction, pulmonary hypertension, acute lung injury, subarachnoid hemorrhage, hypervolemic states, chronic renal failure, and cirrhosis.NT-proBNP levels are increased in CHF, left ventricular dysfunction, myocardial infarction, valvular disease, hypertensive pregnancy, and renal failure, even after hemodialysis.Although levels of BNP and NT-proBNP are similar in normal individuals, NT-proBNP levels are substantially greater than BNP levels in patients with cardiac disease due to increased stability (half-life) of NT-proBNP in circulation. Thus, results from the two tests are not interchangeable.
References
Cowie MR and Mendez GF. BNP and congestive heart failure. Prog Cardiovasc Dis. 2002;44:293-321.
Richards AM, Nicholls MG, Yandle TG, et al. Plasma N-terminal pro-brain natriuretic peptide and adrenomedullin. New neurohormonal predictors of left ventricular function and prognosis after myocardial infarction. Circulation. 1998:97:1921-1929.
Hammerer-Lercher A, Neubauer E, Muller S, et al. Head-to-head comparison of N-terminal pro-brain natriuretic peptide, brain natriuretic peptide and N-terminal pro-atrial natriuretic peptide in diagnosing left ventricular dysfunction. Clin Chim Acta. 2001;310:193-197.
McDonagh TA, Robb SD, Murdoch DR, et al. Biochemical detection of left-ventricular systolic dysfunction. Lancet. 1998;351:9-13.
Mukoyama Y, Nakao K, Hosoda K, et al. Brain natriuretic peptide as a novel cardiac hormone in humans: Evidence for an exquisite dual natriuretic peptide system, ANP and BNP. J Clin Invest. 1991;87:1402-1412.
Hunt PJ, Richards AM, Nicholls MG, et al. Immunoreactive amino-terminal pro-brain natriuretic peptide (NT-PROBNP): a new marker of cardiac impairment. Clin Endocrinol. 1997;47:287-296.
Davis M, Espiner E, Richards G, et al. Plasma brain natriuretic peptide in assessment of acute dyspnoea. Lancet. 1994;343:440-444.
Kohno M, Horio T, Yokokawa K, et al. Brain natriuretic peptide as a cardiac hormone in essential hypertension. Am J Med. 1992;92:29-34.
Bettencourt P, Ferreira A, Pardal-Oliveira N, et al. Clinical significance of brain natriuretic peptide in patients with postmyocardial infarction. Clin Cardiol. 2000;23:921-927.
Jernberg T, Stridsberg M, Venge P, et al. N-terminal pro brain natriuretic peptide on admission for early risk stratification of patients with chest pain and no ST-segment elevation. J Am Coll Cardiol. 2002;40:437-445.
Richards AM, Troughton RW. Use of natriuretic peptides to guide and monitor heart failure therapy. Clin Chem. 2012;58:62-71.
Pfister R, Scholz M, Wielckens K, et al. The value of natriuretic peptides NT-pro-BNP and BNP for the assessment of left-ventricular volume and function. A prospective study of 150 patients.Dtsch Med Wochenschr. 2002;127:2605-2609.
Redfield MM, Rodeheffer RJ, Jacobsen SJ, et al. Plasma brain natriuretic peptide concentration: impact of age and gender. J Am Coll Cardiol. 2002;40:976-982.
Weber M, Hamm C. Role of B-type natriuretic peptid (BNP) and NT-proBNP in clinical routine.Heart. 2006;92:843-849.
Anemia as an Independent Predictor of Elevated N-terminal proBNP
Salman A. Haq, MD1, Mohammad E. Alam2, Larry Bernstein, MD, FCAP3, LB Banko 1, Leonard Y. Lee, MD, FACS4, Barry I. Saul, MD, FACC5, Terrence J. Sacchi, MD, FACC6, John F. Heitner, MD, FACC7
1Cardiology Fellow, 2 Clinical Chemistry Laboratories, 3 Program Director, Cardiothoracic Surgery, 4 Division of Cardiology, Department of Medicine, New York Methodist Hospital-Weill Cornell, Brooklyn, NY
(Unpublished manuscript) Poster Presentation:
Anemia as an Independent Predictor of Elevated N-Terminal proBNP Levels in
Patients without Evidence of Heart Failure and Normal Renal Function.
Haq SA, Alam ME, Bernstein L, Banko LB, Saul BI, Lee LY, Sacchi TJ, Heitner JF.
Table 1. Patient Characteristics
Variable
No Anemia(n=138)
Anemia(n=80)
Median Age (years)
63
76
Men (%)
35
33
Creatinine (mg/dl)
0.96
1.04
Hemoglobin (g/dl)
13.7
10.2
LVEF (%)
67
63
Median NT-proBNP (pg/ml)
321.6
1896.0
A series of slide showing the determination of the representation of normal NT-proBNP range
after removal of patient confounders.
ABSTRACT
Introduction
N-terminal proBNP (NT-proBNP) has emerged as a primary tool for diagnosing congestive heart failure (CHF). Studies have shown that the level of
NT-proBNP is affected by renal insufficiency (RI) and age, independent of the diagnosis of CHF.
There is some suggestion from recent studies that
anemia may also independently affect NT-proBNP levels.
Objective
To assess the affect of anemia on NT-proBNP independent of CHF, RI, and age.
Methods
We evaluated 746 consecutive patients presenting to the Emergency Department (ED) with shortness of breath and underwent evaluation with serum NT-proBNP.
All patients underwent a trans-thoracic echocardiogram (TTE) and clinical evaluation for CHF. Patients were included in this study if they had a normal TTE (normal systolic function, mitral inflow pattern and left ventricular (LV) wall thickness) and no evidence of CHF based on clinical evaluation. Patients were excluded if they had RI (creatinine > 2 mg/dl) or a diagnosis of sepsis. Anemia was defined using the World Health Organization (W.H.O.) definition of
hemoglobin (hgb) < 13 g/dl for males and hgb < 12 g/dl for females.
Results
Of the 746 consecutive patients, 218 patients (138 anemia, 80 no anemia) met the inclusion criteria. There was a markedly significant difference between
NT- proBNP levels based on the W.H.O. diagnosis of anemia.
Patients with anemia had a
mean NT- proBNP of 4,735 pg/ml compared to 1,230 pg/ml in patients without anemia (p=0.0001).
There was a markedly
significant difference in patients who had a hgb > 12 (median 295 pg/ml) when compared to
both patients with an hgb of 10.0 to 11.9 (median 2,102 pg/ml; p = 0.0001) and
those with a hgb < 10 (median 2,131 pg/ml; p = 0.001).
Linear regression analysis comparing hgb with log NT-proBNP was statistically significant (r = 0.395; p = 0.0001). MANOVA demonstrated that
elevated NT- proBNP levels in patients with anemia was independent of age.
Conclusion
This study shows that NT-proBNP is associated with anemia independent of CHF, renal insufficiency, sepsis or age.
INTRODUCTION
B-type natriuretic peptide (BNP) is secreted from the myocardium in response to myocyte stretch. 1-2 BNP is released from the myocytes as a 76 aminoacid N-terminal fragment (NT-proBNP) and a 32-amino acid active hormone (BNP). 3 These peptides have emerged as a primary non-invasive modality for the diagnosis of congestive heart failure (CHF). 4- 7 In addition, these peptides have demonstrated prognostic significance in patients with invasive modality for the diagnosis of
congestive heart failure (CHF). 4- 7
heart failure 8-9,
stable coronary artery disease 10, and
in patients with acute coronary syndromes. 11-14
Studies have shown that the level of NT- proBNP is affected by
age and renal insufficiency (RI) independent of the diagnosis of CHF. 15,16
There is some suggestion from the literature that
anemia may also independently affect NT-proBNP levels. 17-20
Willis et al. demonstrated in a cohort of 209 patients without heart failure that anemia was associated with an elevated NT- proBNP. 17 Similarly, in 217 patients undergoing cardiac catheterization, blood samples were drawn from the descending aorta prior to contrast ventriculography for BNP measurements and
anemia was found to be an independent predictor of plasma BNP levels. 18
The objective of this study is to assess the effect of anemia on NT-proBNP independent of CHF, sepsis, age or renal insufficiency.
METHODS
Patient population
The study population consisted of 746 consecutive patients presenting to the emergency room who underwent NT-proBNP evaluation for the evaluation of dyspnea. Transthoracic echocardiogram (TTE) was available on 595 patients. Patients were included in this study if they had a normal TTE, which was defined as normal systolic function (left ventricular ejection fraction [LVEF] > 45%), normal mitral inflow pattern and normal LV wall thickness. CHF was excluded based on thorough clinical evaluation by the emergency department attending and the attending medical physician. Patients with disease states that may affect the NT- proBNP levels were also excluded:
left ventricular systolic dysfunction (LVEF < 45%),
renal insufficiency defined as a creatinine > 2 mg/dl and
sepsis (defined as positive blood cultures with two or more of the following systemic inflammatory response syndrome (SIRS) criteria: heart rate > 90 beats per minute;
body temperature < 36 (96.8 °F) or > 38 °C (100.4 °F);
hyperventilation (high respiratory rate) > 20 breaths per minute or, on blood gas, a PaCO2 less than 32 mm Hg;
white blood cell count < 4000 cells/mm3 or > 12000 cells/mm³ (< 4 x 109 or > 12 x 109 cells/L), or greater than 10% band forms (immature white blood cells). 21
The study population was then divided into two groups, anemic and non- anemic. Anemia was defined using the world health organization (W.H.O.) definition of hemoglobin (hgb) < 13 g/dl for males and < 12 g/dl for females.The data was also analyzed by dividing the patients into three groups based on hgb levels i.e. hgb > 12, hgb 10 to 11.9 and hgb < 10.
Baseline patient data
Patient’s baseline data including age, gender, ethnicity, hemoglobin (hgb), hematocrit (hct), creatinine, NT- proBNP were recorded from the electronic medical record system in our institution. Chemistry results were performed on the Roche Modular System (Indianapolis, IN), with the NT- proBNP done by chemiluminescence assay. The hemogram was performed on the Beckman Coulter GenS. All TTE’s were performed on Sonos 5500 machine. TTE data collected included LVEF, mitral inflow pattern and LV wall thickness assessment.
Statistical analysis
The results are reported in the means with p < 0.05 as the measure of significance for difference between means. Independent Student’s t-tests were done comparing NT proBNP and anemia. Univariate ANOVAs and multivariate ANOVA (MANOVA) with post hoc tests using the Bonferroni method were used to compare NT- proBNP levels with varying ranges of hgb and age using SPSS 13.0 (SPSS, Chicago, IL). A linear regression analysis was performed using SYSTAT. Calculations included Wilks’Lamda, Pillai trace and Hotelling-Lawley trace. A GOLDMineR® plot was constructed to estimate the effects of age and anemia on NT- proBNP levels. The GOLDMineR® effects plot displays the odds-ratios for predicted NT-proBNP elevation versus the predictor values. Unlike the logistic regression, the ordinal regression, which the plot is derived from, can have polychotomous as well as dichotomous values, as is the case for NT-proBNP.
RESULTS
Of the 746 consecutive patients, 218 patients met the inclusion criteria (fig 1). Baseline characteristics of patients are listed in table 1. The median age for anemic patients was 76 years and 63 years for patients without anemia. One third of patients in both groups were men. The mean hemoglobin for
anemic patients was 10.2 g/dl as compared to 13.7 g/dl for non-anemic patients.
The mean LVEF of patients with anemia was 64% as compared to 67% for non-anemic patients.
Based on the WHO definition of anemia, 138 patients were determined to be anemic while 80 patients were diagnosed as non-anemic. There was a markedly significant difference between NT-proBNP levels based on the WHO diagnosis of anemia.
Patients with anemia had a
mean NT-proBNP of 4,735 pg/ml compared to 1,230 pg/ml in patients without anemia (p = 0.0001).
Of the 218 patients in the study, 55 patients had a hgb of < 10 g/dl. Analysis using
hgb < 10 g/dl for anemia demonstrated a statistically significant difference in the NT-proBNP values.
Patients with a hgb < 10 g/dl had a mean NT- proBNP of 5,130 pg/ml
compared to 2,882 pg/ml in patients with a hgb of > 10 g/dl (p = 0.01)
The groups were also divided into three separate categories of hgb for subset analysis:
hgb > 12 g/dl,
hgb 10 to 11.9 g/dl and
hgb < 10 g/dl.
There was a markedly significant difference in
the NT- ProBNP levels of patients who had a hgb > 12 g/dl (median 295 pg/ml) when
compared to those with a hgb range of 10.0 g/dl to 11.9 g/dl (median 2,102 pg/ml) (p = 0.0001),
and also a significant difference in
NT- proBNP levels of patients with a hgb > 12 g/dl (median 295 pg/ml) when
compared to a hgb of < 10 g/dl (median 2,131 pg/ml) (p = 0.001).
However, there was no statistically significant difference in NT-proBNP levels of patients with hgb 10 g/dl to 11.9 g/dl
when compared to those with a hgb of < 10 g/dl (p = 1.0).
A scatter plot comparing hgb with log NT-proBNP and fitting of a line to the data by ordinary least squares regression was significant (p = 0.0001) and demonstrated
a correlation between anemia and NT-proBNP levels (r = 0.395) (fig. 2).
MANOVA demonstrated that elevated NT- proBNP levels in patients with anemia was independent of age (Wilks’ Lambda [p = 0.0001]). In addition, using GOLDMineR® plots (figure 3a and 3b) with a combination of age and hb scaled as predictors of elevated NT-proBNP,
both age and hgb were required as independent predictors.
What about the effect of anemia? The GOLDminer analysis of ordinal regression was carried out in a database from which renal insufficiency and CHF were removed. The anemia would appear to have an independent effect on renal insufficiency. Figure 4 is a boxplot comparison of NT – proBNP, the age normalized function NKLog (NT- proBNP)/eGFR formed from taking 1000*Log(NT- proBNP) divided by the MDRD at eGFR exceeding 60 ml/min/m2 and exceeding 30 ml/min/m2. The transformed variable substantially makes the test independent of age and renal function. The boxplot shows the medians, 97.5, 75, 25 and 2.5 percentiles. There appears to be no significance in the NKLog(NT pro-BNP)/MDRD plot. Table II compares the NT-proBNP by WHO criteria at eGFR 45, 60 and 75 ml/mln/m2 using the t-test with unequal variance assumed, and the Kolmogorov-Smirnov test for nonparametric measures of significance. The significance at 60 ml/min/m2 is marginal and nonexistent at 75 ml/min/m2. This suggests that the contribution from renal function at above 60 ml/min2 can be ignored. This is consistent with the findings using the smaller, trimmed database, but there is an interaction between
anemia, and
eGFR at levels below 60 ml/min/m2
DISCUSSION
The findings in this study indicate that
anemia was associated with elevated NT-proBNP levels independent of CHF, renal insufficiency, sepsis or age.
These findings have been demonstrated with NT-proBNP in only one previous study. Wallis et al. demonstrated that after adjusting for age, sex, BMI, GFR, LVH and valvular disease;
only age,
valvular disease and
low hemoglobin
were significantly associated with increased NT-proBNP. 18.
In our study, CHF was excluded based on both a normal TTE and a thorough clinical evaluation. In the only other study directly looking at NT- proBNP levels in anemic patients without heart failure
only 25% of patients had TTEs, with one patient having an LVEF of 40%. 17
BNP, the active molecule released after cleavage along with NT- proBNP, has also been studied in relation to blood hemoglobin levels. 18 In 263 patients undergoing cardiac catheterization blood samples were drawn from the descending aorta prior to contrast ventriculography to determine the value of BNP. Anemia was present in 217 patients. Multivariate linear regression model adjusting for
age,
gender,
body mass index,
history of myocardial infarction,
estimated creatinine clearance, and
LVEF
found hgb to be an independent predictor of BNP levels.
In our study, patients with anemia were slightly older than those without anemia. However, both MANOVA and GOLDMineR® plot demonstrated that
elevated NT-proBNP levels in patients with anemia was independent of age.
Other studies have found that BNP is dependent on renal insufficiency and age. Raymond et al. randomly selected patients to complete questionnaires regarding CHF and
then underwent pulse and blood pressure measurements,
electrocardiogram (ECG),
echocardiography and
blood sampling. 15
A total of 672 subjects were screened and 130 were determined to be normal, defined as
no CHF or ischemic heart disease,
normal LVEF,
no hypertension,
diabetes mellitus,
lung disease, and
not on any cardiovascular drugs.
They found
older age,
increasing dyspnea,
high plasma creatinine and a
LVEF < 45%
to be independently associated with an elevated NT-proBNP plasma level by multiple linear regression analysis. In another study, McCullough et al. evaluated the patients from the Breathing Not ProperlyMultinational Study
looking at the relationship between BNP and renal function in CHF. 16
Patients were excluded if they were on hemodialysis or had a estimated glomerular filteration rate (eGFR) of < 15 ml/min. They found that the BNP levels correlated significantly with the eGFR, especially in patients without CHF, suggesting
chronic increased blood volume and
increased left ventricular wall tension as a possible cause. 16
Our study was designed to exclude patients with known diseases such as CHF and renal insufficiency in order to demonstrate
the independent effect of anemia on elevated NT-proBNP levels.
The mechanism for elevated NT-proBNP levels in patients with anemia is unknown. Some possible mechanisms that have been reported in the literature include
hemodilution secondary to fluid retention in patients with CHF 18,
decreased oxygen carrying capacity with accompanying tissue hypoxia which
stimulates the cardio-renal compensatory mechanism leading to increased release of NT-proBNP. 17
The findings from our study suggest that
NT-proBNP values should not be interpreted in isolation of hemoglobin levels and
should be integrated with other important clinical findings for the diagnosis of CHF.
Further studies are warranted
to assess the relationship between anemia and plasma natriuretic peptides, and
possibly modify the NT-proBNP cutoff points for diagnosing acutely decompensated CHF in patients with anemia.
CONCLUSION
This study shows that elevated NT-proBNP levels are associated with anemia independent of
CHF,
renal insufficiency,
sepsis and
age.
NT-proBNP levels should be interpreted with caution in patients who have anemia.
REFERENCES
1. Brunea BG, Piazza LA, de Bold AJ. BNP gene expression is specifically modulated by stretch and ET-1 in a new model of isolated rat atria.Am J Physiol 1997; 273:H2678-86.
2. Wiese S, Breyer T, Dragu A, et al. Gene expression of brain natriuretic peptide in isolated atrial and ventricular human myocardium: influence of angiotensin II and diastolic fiber length. Circ 2000; 102:3074-79.
3. de Lemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet 2003; 362:316-22.
4. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent care setting. J Am Coll Cardiol 2001; 37:379-85.
5. Morrison LK, Harrison A, Krishnaswamy P, Kazanegra R, Clopton P, Maisel A. Utility of rapid natriuretic peptide assay in differentiating congestive heart failure from lung disease in patients presenting with dyspnea.
J Am Coll Cardiol 2003; 39:202-09.
6. Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002; 347:161-67.
7. Januzzi JL, Camargo CA, Anwaruddin S, et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol 2005; 95:948-954.
8. Tsutamoto T, Wada A, Meada K, et al. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: prognostic role of plasma brain natriuretic peptide concentration in patients with chronic symptomatic left ventricular dysfunction.
Circulation 1997; 96(2): 509-16.
9. Anand IS, Fisher LD, Chiang YT, et al. Changes in brain natriuretic peptide and norepinephrine over time and mortality and morbidity in the Valsartan Heart Failure Trial (Val-HEFT). Circulation 2003; 107:1278-1283.
10. Omland T, Richards AM, Wergeland R and Vik-Mo H. B-type natriuretic peptide and long term survival in patients with stable coronary artery disease.
Am J Cardiol 2005; 95:24-28.
11. Omland T, Aakvaag A, Bonarjee VV. et al. Plasma brain natriuretic peptide as an indicator of left ventricular systolic dysfunction and long term prognosis after acute myocardial infarction. Comparison with plasma atrial natriuretic peptide and N-terminal proatrial natriuretic peptide.
Circulation 1996; 93:1963-1969.
12. de Lemos JA, Morrow DA, Bently JH, et al. The prognostic value of B-type natriuretic peptide in patients with acute coronary syndromes. N Engl J Med 2001; 345:1014-1021.
13. Richards AM, Nicholls MG, Espiner EA, et al. B-type natriuretic peptides and ejection fraction for prognosis after myocardial infarction. Circulation 2003; 107:2786-2792.
14. Sabatine MS, Morrow DA, de Lemos JA, et al. Multimarker approach to risk stratification in non-ST elevation acute coronary syndromes: simultaneous assessment of troponin I, C-reactive protein and B-type natriuretic peptide.
Circulation 2002; 105:1760-1763.
15. Raymond I, Groenning BA, Hildebrandt PR, Nilsson JC, Baumann M, Trawinski J, Pedersen F. The influence of age, sex andother variables on the plasma level of N-terminal pro brain natriureticpeptide in a large sample of the general population. Heart 2003; 89:745-751.
16. McCollough PA, Duc P, Omland T, McCord J, Nowak RM, Hollander JE, et al. B-type natriuretic peptide and renal function in the diagnosis of heartfailure: an analysis from the Breathing Not Properly Multinational Study.
Am J Kidney Dis 2003; 41:571-579.
17. Willis MS, Lee ES, Grenache DG. Effect of anemia on plasma concentrations of NT-proBNP.
Clinica Chim Acta 2005; 358:175-181.
18. Wold Knudsen C, Vik-Mo H, Omland T. Blood hemoglobin is an independent predictor of B-type natriuretic peptide.
Clin Sci 2005; 109:69-74.
19. Tsuji H, Nishino N, Kimura Y, Yamada K, Nukui M, et al. Haemoglobin level influences plasma brain natriuretic peptide concentration. Acta Cardiol 2004;59:527-31.
20. Wu AH, Omland T, Wold KC, McCord J, Nowak RM, et al. Relationship of B-type natriuretic peptide and anemia in patients withand without heart failure: A substudy from the Breathing Not Properly(BNP) Multinational Study.
Am J Hematol 2005; 80:174-80.
22. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, et al. Definitions for sepsis and organ failure and guidelines for theuse of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. Chest. 1992;101(6):1644-55.
Table Legends
Table I. Clinical characteristics of the study population
Table II. Comparison of NT- proBNP means under WHO criteria at different GFR
*AF, valve disease and elevated troponin T included
r AF, valve disease and elevated troponin T removed
FIGURE LEGENDS
FIGURE 1. Study population flow chart. (see poster)
FIGURE 2. Relationship between proBNP and hemoglobin. (see above)
FIGURE 3. NT-proBNP levels in relation to anemia (see above)
Supplementary Material
Table based on LatentGOLD Statistical Innovations, Inc., Belmont, MA., 2000: Jeroen Vermunt & Jay Magidson)
4-Cluster Model
Number of cases 408
Number of parameters (Npar) 24
Chi-squared Statistics
Degrees of freedom (df) 71 p-value
L-squared (L²) 80.2033 0.21
X-squared 80.8313 0.20
Cressie-Read 76.6761 0.30
BIC (based on L²) -346.5966
AIC3 (based on L²) -132.7967
CAIC (based on L²) -417.5966
age < 51 0.0720 0.7458 0.0910 0.0912
51-70 0.3036 0.3084 0.2013 0.1867
over 70 0.3773 0.0409 0.3633 0.2186
WHO No anemia 0.4589 0.3957 0.1076 0.0378
Anemia 0.1342 0.1844 0.3742 0.3073
SECOND ARTICLE
The effect of correction of mild anemia in severe, resistant congestive heart failure using subcutaneous erythropoietin and intravenous iron: a randomized controlled study
Donald S Silverberg, MDa; Dov Wexler, MDa; David Sheps, MDa; Miriam Blum, MDa; Gad Keren, MDa; Ron Baruch, MDa; Doron Schwartz, MDa; Tatyana Yachnin, MDa; Shoshana Steinbruch, RNa; Itzhak Shapira, MDa; Shlomo Laniado, MDa; Adrian Iaina, MDa
J Am Coll Cardiol. 2001;37(7):1775-1780. doi:10.1016/S0735-1097(01)01248-7
This is a randomized controlled study of anemic patients with severe congestive heart failure (CHF) to assess the effect of correction of the anemia on cardiac and renal function and hospitalization.
BACKGROUND
Although mild anemia occurs frequently in patients with CHF, there is very little information about the effect of correcting it with erythropoietin (EPO) and intravenous iron.
METHODS
Thirty-two patients with moderate to severe CHF (New York Heart Association [NYHA] class III to IV)
who had a left ventricular ejection fraction (LVEF) of 40% despite maximally tolerated doses of CHF medications and
whosehemoglobin (Hb) levels were persistently between 10.0 and 11.5 g% were randomized into two groups.
Group A (16 patients) received subcutaneous EPO and IV iron to increase the level of Hb to at least 12.5 g%. In Group B (16 patients) the anemia was not treated. The doses of all the CHF medications were maintained at the maximally tolerated levels except for oral and intravenous (IV) furosemide, whose doses were increased or decreased according to the clinical need.
RESULTS
Over a mean of 8.2 +/- 2.6 months,
four patients in Group B andnone in Group A died of CHF-related illnesses.
The mean NYHA classimproved by 42.1% in A and worsened by 11.4% in B.
The LVEF increased by 5.5% in A and decreased by 5.4% in B.
The serum creatinine did not change in A andincreased by 28.6% in B.
The need for oral and IV furosemide decreased by 51.3% and 91.3% respectively in A and increased by 28.5% and 28.0% respectively in B.
The number of days spent in hospital compared with the same period of time before entering the studydecreased by 79.0% in A and increased by 57.6% in B.
CONCLUSIONS
When anemia in CHF is treated with EPO and IV iron, a marked improvement in cardiac and patient function is seen,
associated with less hospitalization and renal impairment and less need for diuretics. (J Am Coll Cardiol 2001;37:1775– 80)
Anemia of any cause is known to be capable of causing congestive heart failure (CHF) (1). In patients hospitalized with CHF the
mean hemoglobin (Hb) is about 12 g% (2,3),
which is considered the lower limit of normal in adults (4). Thus, anemia appears to be
common in CHF. Recently, in 142 patients in our special CHF outpatient clinic, we found that
as the CHF worsened, the mean Hb concentration decreased, from 13.7 g% in mild CHF (New York Heart Association [NYHA] class I) to 10.9 g% in severe CHF (NYHA 4), and
the prevalence of a Hb 12 g% increased from 9.1% in patients with NYHA 1 to 79.1% in those with NYHA 4 (5).
The Framingham Study has shown that anemia is an
independent risk factor for the production of CHF (6).
Despite this association of CHF with anemia,
its role is not mentioned in the 1999 U.S. guidelines for the diagnosis and treatment of CHF (7), and
many studies consider anemia to be only a rare contributing cause of hospitalization for CHF (8,9).
Recently, we performed a study in which the anemia of severe CHF that was resistant to maximally tolerated doses of standard medications
was corrected with a combination of subcutaneous (sc) erythropoietin (EPO) and intravenous iron (IV Fe) (5).
We have found this combination to be safe, effective and additive
in the correction of the anemia of chronic renal failure (CRF)in both
the predialysis period (10) and the dialysis period (11).
The IV Fe appears to be more effective than oral iron (12,13). In our previous study of CHF patients (5), the treatment resulted in
improved cardiac function,
improved NYHA functional class,
increased glomerular filtration rate,
a marked reduction in the need for diuretics and
a 92% reduction in the hospitalization rate
compared with a similar time period before the intervention. In the light of these positive results, a prospective randomized study was undertaken
to determine the effects of the correction of anemia in severe symptomatic CHF resistant to maximally tolerated CHF medication.
Abbreviations and Acronyms
CABG
coronary artery bypass graft
CHF
congestive heart failure
CRF
chronic renal failure
EPO
erythropoietin
%Fe Sat
percent iron saturation
GFR
glomerular filtration rate
Hb
hemoglobin
Hct
hematocrit
IU
international units
IV
intravenous
LVEF
left ventricular ejection fraction
NYHA
New York Heart Association
PA
pulmonary artery
sc
subcutaneous
SOLVD
Studies Of Left Ventricular Dysfunction
MATERIALS AND METHODS
Patients.Thirty-two patients with CHF were studied. Before the study, the patients were treated for least six months in the CHF clinic with
maximally tolerated doses of angiotensin-converting enzyme inhibitors, the beta-blockers bisoprolol or carvedilol, aldospirone, long-acting nitrates, digoxin and oral and intravenous (IV) furosemide.
In some patients these agents could not be given because of contraindications and in others they had to be stopped because of side effects. Despite this maximal treatment
the patients still had severe CHF (NYHA classIII), with fatigue and/or shortness of breath on even mild exertion or at rest. All had levels of
Hb in the range of 10 to 11.5 g% on at least three consecutive visits over a three-week period.
All had a LVEF of 40%.
Secondary causes of anemia including hypothyroidism, and folic acid and vitamin B12 deficiency were ruled outand
there was no clinical evidence of gastrointestinal bleeding.
The patients were randomized consecutively into two groups:
Group A, 16 patients, was treated with sc EPO and IV Fe to achieve a target Hb of at least 12.5 g%.
Group B, 16 patients, did not receive the EPO and IV Fe.
Treatment protocol for correction of anemia.
All patients in Group A received the combination of sc EPO and IV Fe. The EPO was given once a week at a starting dose of 4,000 international units (IU) per week and
the dose was increased to two or three times a week or decreased to once every few weeks as necessary
to achieve and maintain a target Hb of 12.5 g%.
The IV Fe (Venofer-Vifor International, Switzerland), a ferric sucrose product, was given in a dose of 200 mg IV in 150 ml saline over 60 min every two weeks
until the serum ferritin reached 400 g/l or
the %Fe saturation (%Fe Sat is serum iron/total iron binding capacity 100) reached 40% or
the Hb reached 12.5g%.
The IV Fe was then given at longer intervals as needed to maintain these levels.
Investigations.
Visits to the clinic were at two- to three week intervals depending on the patient’s status. This was the same frequency of visits to the CHF clinic as before then,
potassium and ferritin and %Fe Sat were performed on every visit.
blood pressure was measured by an electronic device on every visit.
LVEF was measured initially and at four- to six-month intervals by MUGA radioisotope ventriculography.
This technique measures
the amount of blood in the ventricle at the end of systole and at the end of diastole, thus giving
a very accurate assessment of the ejection fraction.
It has been shown to be an accurate and reproducible method of measuring the ejection fraction (14). Hospital records were reviewed at the end of the intervention period to compare
the number of days hospitalized during the study with
the number of days hospitalized during a similar period
when the patients were treated in the CHF clinic before the initial randomization and entry into the study.
Clinic records were reviewed to evaluate the types and doses of CHF medications used before and during the study. The mean follow-up for patients was8.2 +/-2.7 months (range 5 to 12 months). The study was done with the approval of the local ethics committee.Statistical analysis.
An analysis of variance with repeated measures (over time) was performed tocomparethe two study groups (control vs. treatment) and
to assess time trend and the interactions between the two factors.
A separate analysis was carried out for each of the outcome parameters.
The Mann-Whitney test was used to compare the change in NYHA class between two groups.
All the statistical analysis was performed by SPSS (version 10).
RESULTS
The mean age in Group A (EPO and Fe) was 75.3 +/- 14.6 years and in group B was 72.2 +/- 9.9 years. There were 11 and 12 men in Groups A and B, respectively.
Before the study the two groups were similar in
cardiac function,
comorbidities,
laboratory investigations and
medications
(Tables 1, 2 and 3), except for IV furosemide (Table 3),
which was higher in the treatment group. The mean NYHA class of Group A before the study was 3.8 0.4 and was 3.5 0.5 in Group B. The contributing factors to CHF in Groups A and B, respectively, are seen in Table 1 and were similar.
Table 1. Medical Conditions and Contributing Factors to Congestive Heart Failure in the 16 Patients Treated for the Anemia and in the 16 Controls
Table 2. The Effect of Correction of Anemia by Intravenous Iron and Erythropoietin Therapy on Various Parameters in 16 Patients in the Treatment (A) and 16 in the Control (B) Group
p values are given for analysis of variance with repeated measures and for independent t tests for comparison of baseline levels between the two groups.
BP blood pressure; Fe Sat iron saturation; Hb hemoglobin; IV intravenous; NS not stated; Std Dev. standard deviation.
The main contributing factors to CHF were considered to be
ischemic heart disease (IHD) in 11 and 10 patients respectively,
hypertension in two and two patients,
valvular heart disease in twoand two patients, and
idiopathic cardiomyopathy in one and two patients, respectively.
A significant change after treatment was observed in the two groups in the following parameters:
IV furosemide,
days in hospital,
Hb,
ejection fraction,
serum creatinine and
serum ferritin.
In addition, the interaction between the study group and time trend was significant in all measurements except for blood pressure and %Fe Sat. This interaction indicates that
the change over time was significantly different in the two groups.
Table 3. The Effect of Correction of Anemia by Intravenous Iron and Erythropoietin Therapy on Various Parameters in 16 Patients in the Treatment (A) and 16 in the Control (B) Group
p values are given for analysis of variance with repeated measures and for independent t tests for comparison of baseline levels between the two groups.
BP blood pressure; Fe Sat iron saturation; Hb hemoglobin; IV intravenous; NS not stated; Std Dev. standard deviation.
We find in the comparisons of Tables 2 and 3:
before treatment the level of oral furosemide was higher in the control group (136.2 mg/day) compared with the treatment group (132.2 mg/day).
after treatment, while the dose of oral furosemide of the treated patients was reduced to 64.4 mg/day
the dose of the nontreated patients was increased to 175 mg/day.
The same results of improvement in the treated group and deterioration in the control group are expressed in the following parameters:
IV furosemide, days in hospital,
Hb,
ejection fraction and
serum creatinine.
The NYHA class was
3.8 +/- 0.4 before treatment and 2.2 +/- 0.7 after treatment in Group A (delta mean = –1.6) and
3.5 +/- 0.7 before treatment and 3.9 +/- 0.3 after treatment in Group B. (delta mean =0.4)
The improvement in NYHA class was significantly higher (p < 0.0001) in the treatment group compared with the control group (Table 4).
Table 4. Changes from Baseline to Final New York Heart Association (NYHA) Class
Initial minus final
The improvement in NYHA class was statistically higher (p < 0.0001) in the treatment group compared with control.
There were no deaths in Group A and four deaths in Group B.
Case 1: A 71-year-old woman with severe mitral insufficiency and severe pulmonary hypertension (a pulmonary artery [PA] pressure of 75 mm Hg) had persistent NYHA 4 CHF and died during mitral valve surgery seven months after onset of the study. She was hospitalized for 21 days in the seven months before randomization and for 28 days during the seven months after randomization.
Case 2:
A 62-year-old man with a longstanding history of hypertension complicated by IHD, coronary artery bypass graft (CABG) and atrial fibrillation had persistent NYHA 4 CHF and a PA pressure of 35 mm Hg, and died from pneumonia and septic shock eight months after onset of the study. He was hospitalized for seven days in the eight months before randomization and for 21 days during the eight months after
randomization.
Case 3: A 74-year old man with IHD, CABG, chronic obstructive pulmonary disease, a history of heavy smoking and diabetes had persistent NYHA 4 CHF and a PA pressure of 28 mm Hg, and died of pulmonary edema and cardiogenic shock nine months after onset of the study. He was hospitalized for 14 days in the nine months before randomization and for 41 days during the nine months after randomization.
Case 4:
A 74-year-old man with a history of IHD, CABG, diabetes, dyslipidemia, hypertension and atrial fibrillation, had persistent NYHA 4 CHF and a PA pressure of 30 mm Hg, and died of pneumonia and septic shock six months after onset of the study. He was hospitalized for five days in the six months before randomization and for 16 days during the nine months after randomization.
DISCUSSION
Main findings.
The main finding of the present study is that the correction of
even mild anemia in patients with symptoms of very severe CHF despite being on maximally tolerated drug therapy
resulted in a significant improvement in their cardiac function and NYHA functional class.
There was also a large
reduction in the number of days of hospitalization compared with a similar period before the intervention.
all this was achieved despite a marked reduction in the dose of oral and IV furosemide.
In the group in whom the anemia was not treated, four patients died during the study. In all four cases
the CHF was unremitting and contributed to the deaths.
In addition, for the group as a whole,
the LVEF, the NYHA class and the renal function worsened.
There was also need for
increased oral and IV furosemide as well as increased hospitalization.
Study limitations.
The major limitations of this study are
the smallness of the sample size and
the fact that randomization and treatment were not done in a blinded fashion.
Nevertheless, the two groups were almost identical in
cardiac, renal and anemia status;
in the types and doses of medication they were taking before and during the intervention and
in the number of hospitalization days before the intervention.
Although the results of this study, like those of our previous uncontrolled study (5), suggest that
anemia may play an important role in the mortality and morbidity of CHF,
a far larger double-blinded controlled study should be carried out to verify our findings.
Anemia as a risk factor for hospitalization and death in CHF.
Our results are consistent with a recent analysis of 91,316 patients hospitalized with CHF (15).Anemiawas found to be a stronger predictor of
the need for early rehospitalization than was hypertension, IHD or the presence of a previous CABG.
A recent analysis of the Studies Of Left Ventricular Dysfunction (SOLVD) (16) showed that
the level of hematocrit (Hct) was an independent risk factor for mortality.
During a mean follow-up of 33 months the mortality was
22%, 27% and 34% for those with a Hct of 40, 35 to 40 and 35 respectively.
The striking response of our patients to
correction of mild anemia suggests that the failing heart may be very susceptible to anemia.
It has, in fact, been found in both animal (17) and human studies (17–19) that
the damaged heart is more vulnerable to anemia and/or ischemia than is the normal heart.
These stimuli may result in a more marked reduction in cardiac function than occurs in the normal heart and may explain why, in our study,
the patients were so resistant to high doses of CHF medications and
responded so well when the anemia was treated.
Our findings about the importance of anemia in CHF are not surprising when one considers that, in dialysis patients,
anemia has been shown to be associated with an increased prevalence and incidence of CHF (20) and that
correction of anemia in these patients is associated with improved
cardiac function (21,22),
less mortality (23,24) and
fewer hospitalizations (23,25).
Effect of improvement of CHF on CRF.
Congestive heart failure can cause progressive renal failure (26,27). Renal ischemia is found very early on
in patients with cardiac dysfunction (28,29), and
chronic ischemia may cause progression of renal failure (30). Indeed, the development of
CHF in patients with essential hypertension has been found to be one of the most powerful predictors of
the eventual development of end-stage renal disease (31).
Patients who develop CHF after a myocardial infarction experience a
fall in the glomerular filtration rate (GFR)of about 1 ml/min/month if the CHF is not treated (32).
In another recent analysis of the SOLVD study, treating the CHF with
both angiotensin-converting enzyme inhibitors and beta-blockers resulted in better preservation of the renal function than did
suggesting that the more aggressive the treatment of the CHF, the better the renal function is preserved. In the present study, as in our previous one (5), we found that the deterioration of GFR was prevented with
successful treatment of the CHF, including correction of the anemia, whereas
the renal function worsened when the CHF remained severe.
All these findings suggest that early detection and treatment of CHF and systolic and/or diastolic dysfunction from whatever cause could prevent
the deterioration not only of the cardiac function
but of the renal function as well.
This finding has very broad implications in the prevention of CRF, because most patients with advanced CRF have
either clinical evidence of CHF or at least some degree of systolic dysfunction (33).
Systolic and/or diastolic dysfunctioncan occur early on in many conditions, such as
essential hypertension (34),
renal disease of any cause (35,36) or
IHD, especially after a myocardial infarction (37).
The early detection and adequate treatment of this cardiac dysfunction, including correction of the anemia, could prevent this cardiorenal insufficiency. To detect cardiac dysfunction early on, one would need at least an echocardiogram and MUGA radio-nucleotide ventriculography. These tests should probably be done not only in patients with signs and symptoms of CHF, but in all patients where CHF or systolic and/or diastolic dysfunction are suspected, such as those with a history of heart disease or suggestive changes of ischemia or hypertrophy on the electrocardiogram, or in patients with hypertension or renal disease.
Other positive cardiovascular effects of EPO treatment.
Another possible explanation for the improved cardiac function in this study may be the direct effect that EPO itself has on improving cardiac muscle function (38,39) and myocardial cell growth (39,40) unrelated to its effect of the anemia. In fact EPO may be crucial in the formation of the heart muscle in utero (40). It may also improve endothelial function (41). Erythropoietin may besuperior to blood transfusions not only because adverse reactions to EPO are infrequent, but also because
EPO causes the production and release of young cells from the bone marrow into the blood.
These cells have an oxygen dissociation curve that is shifted to the right of the normal curve, causing the release of
much greater amounts of oxygen into the tissues than occurs normally (42).
On the other hand, transfused blood consists of older red cells with an oxygen dissociation curve that is
shifted to the left, causing the release of much less oxygen into the tissues than occurs normally (42).
The combination of IV Fe and EPO. The use of IV Fe along with EPO has been found to have an additive effect,
increasing the Hb even more than would occur with EPO alone while at the same time
allowing the dose of EPO to be reduced (10 –13).
The lower dose of EPO will be cost-saving and also reduce the chances of hypertension developing (43).
We used iron sucrose (Venofer) as our IV Fe medication because, in our experience, it is extremely well tolerated (10,11) and
has not been associated with any serious side effects in more than 1,200 patients over six years.
Implications of treatment of anemia in CHF. The correction of anemia is not a substitute for the well-documented effective therapy of CHF but seems to be an important, if not vital, addition to the therapy. It is surprising, therefore, that judging from the literature on CHF,
such an obvious treatment for improving CHF is so rarely considered.
We believe that correction of the anemia will have an important role to play in
the amelioration of cardiorenal insufficiency, and that this improvement will have
significant economic implications as well.
Acknowledgments
The authors thank Rina Issaky, Miriam Epstein, Hava Ehrenfeld and Hava Rapaport for their secretarial assistance.
Reprint requests and correspondence: Dr. D. S. Silverberg, Department of Nephrology, Tel Aviv Medical Center, Weizman 6, Tel Aviv, 64239, Israel.
THIRD ARTICLE
The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations
Donald S Silverberg, MDa; Dov Wexler, MDa; Miriam Blum, MDa; Gad Keren, MDa; David Sheps, MDa; Eyal Leibovitch, MDa; David Brosh, MDa; Shlomo Laniado, MDa; Doron Schwartz, MDa; Tatyana Yachnin, MDa; Itzhak Shapira, MDa; Dov Gavish, MDa; Ron Baruch, MDa; Bella Koifman, MDa; Carl Kaplan, MDa; Shoshana Steinbruch, RNa; Adrian Iaina, MDa
J Am Coll Cardiol. 2000;35(7):1737-1744. doi:10.1016/S0735-1097(00)00613-6
This study evaluated the prevalence and severity of anemia in patients with congestive heart failure (CHF) and
the effect of its correction on cardiac and renal function and hospitalization.
BACKGROUND
The prevalence and significance of mild anemia in patients with CHF is uncertain, and the role of erythropoietin with intravenous iron supplementation in treating this anemia is unknown.
METHODS
In a retrospective study, the records of the 142 patients in our CHF clinic were reviewed to find
the prevalence and severity of anemia (hemoglobin [Hb]12 g).
In an intervention study, 26 of these patients, despite maximally tolerated therapy of CHF for at least six months, still had had severe CHF and were also anemic. They were treated with
subcutaneous erythropoietin and intravenous iron sufficient to increase the Hb to 12 g%.
The doses of the CHF medications, except for diuretics, were not changed during the intervention period.
RESULTS
The prevalence of anemia in the 142 patients increased withthe severity of CHF,
reaching 79.1% in those with New York Heart Association class IV.
In the intervention study, the anemia of the 26 patients was treated for a mean of 7.2 5.5 months.
The mean Hb level and mean left ventricular ejection fraction increased significantly.
The mean number of hospitalizations fell by 91.9% compared with a similar period before the study.
The New York Heart Association class fell significantly,
as did the doses of oral and intravenous furosemide.
The rate of fall of the glomerular filtration rate slowed with the treatment.
CONCLUSIONS
Anemia is very common in CHF and its successful treatment is associated with a significant improvementin
cardiac function,
functional class,
renal function and
in a marked fall in the need for diuretics and hospitalization.
Abbreviations and Acronyms
ACE
Angiotensin-converting enzyme
CHF
congestive heart failure
COPD
chronic obstructive pulmonary disease
CRF
chronic renal failure
CVA
cerebrovascular accident
EPO
erythropoietin
Fe
iron
g%
grams Hb /100 ml blood
GFR
glomerular filtration rate
Hb
hemoglobin
Hct
hematocrit
IV
intravenous
LVEF
left ventricular ejection fraction
LVH
left ventriculr hypertrophy
NYHA
New York Heart Association
%Fe Sat
percent iron saturation
sc
subcutaneous
TNF
tumor becrosis factor
ACE
Angiotensin-converting enzyme
CHF
congestive heart failure
COPD
chronic obstructive pulmonary disease
CRF
chronic renal failure
CVA
cerebrovascular accident
EPO
erythropoietin
Fe
iron
g%
grams Hb /100 ml blood
GFR
glomerular filtration rate
Hb
hemoglobin
Hct
hematocrit
IV
intravenous
LVEF
left ventricular ejection fraction
LVH
left ventriculr hypertrophy
NYHA
New York Heart Association
%Fe Sat
percent iron saturation
sc
subcutaneous
TNF
tumor becrosis factor
The mean hemoglobin (Hb) in patients with congestive heart failure (CHF) is about 12 g Hb per 100 ml blood (g%) (1–3), which is considered to be the lower limit of normal in adult men and postmenopausal women (4). Thus, many patients with CHF are anemic, and
this anemia has been shown to worsen as the severity of the CHF progresses (5,6).
Severe anemia of any cause can produce CHF, and treatment of the anemia can improve it (7). In patients with chronic renal failure (CRF) who are anemic,
treatment of the anemia with erythropoietin (EPO) has improved many of the abnormalities seen in CHF,
reducing left ventricular hypertrophy (LVH) (8 –10),
preventing left ventricular dilation (11) and,
in those with reduced cardiac function, increasing the left ventricular ejection fraction (LVEF)(8 –10),
the stroke volume (12) and
the cardiac output (12).
In view of the high prevalence of anemia in CHF, it is surprising that we could find no studies in which EPO was used in the treatment of the anemia of CHF, and the use of EPO is not included in U.S. Public Health Service guide-lines of treatment of the anemia of CHF (13). In fact, anemia has been considered
only a rare contributing factor to the worsening of CHF, estimated as contributing to
no more than 0% to 1.5% of all cases (14 –16).
Perhaps for this reason, recent guidelines for the prevention and treatment of CHF do not mention treatment of anemia at all(17). If successful treatment of anemia could improve cardiac function and patient function in CHF,
this would have profound implications, because,
despite all the advances made in the treatment of CHF, it is still a major and steadily increasing cause of hospitalizations, morbidity and mortality (18 –20).
The purpose of this study is to examine
the prevalence of anemia (Hb 12 g%) in patients with different levels of severity of CHF and
to assess the effect of correction of this anemia in severe CHF patients
resistant to maximally tolerated doses of CHF medication.
A combination of subcutaneous (SC) EPO and intravenous (IV) iron (Fe) was used. We have found this combination to be additive in improving the anemia of CRF (21,22).
METHODS
Patients.
The medical records of the 142 CHF patients being treated in our special outpatient clinic devoted to CHF were reviewed to determine the prevalence and severity of anemia and CRF in these patients. These patients were referred to the clinic either from general practice or from the various wards in the hospital.
Intervention study.
Despite at least six months of treatment in the CHF clinic,
26 of the above patients had persistent, severe CHF (New York Heart Association [NYHA] class III),
had a Hb level of 12 g% and were on
angiotensin-converting enzyme [ACE] inhibitors, the
alpha-beta-blocker carvedilol,
long-acting nitrates,
digoxin,
aldactone and
oral and IV furosemide.
These 26 patients participated in an intervention study. The mean age was 71.76 8.12 years. There were 21 men and 5 women. They all had a
LVEF below 35%,
persistent fatigue and
shortness
of breath on mild to moderate exertion and often at rest, and had
required hospitalizations at least once during their follow-up in the CHF clinic for pulmonary edema.
In 18 of the 26 patients, the CHF was associated with ischemic heart disease either
alone in four patients, or
with hypertension in six,
diabetes in four,
the two together in three, or with
valvular heart disease in one.
Of the remaining eight patients,
four had valvular heart disease alone and
four had essential hypertension alone.
Secondary causes of anemia including
gastrointestinal blood loss (as assessed by history and by three negative stool occult blood examinations),
folic acid and vitamin B12 deficiency and
hypothyroidism were ruled out.
Routine gastrointestinal endoscopy was not carried out. The study passed an ethics committee.
Table 1. Initial Characteristics of the 142 Patients With CHFSeen in the CHF Clinic
CMP cardiomyopathy; LVEF left ventricular ejection fraction; NYHA New York Heart Association class.
Correction of the anemia.
All patients received the combination of SC EPO and IV Fe. The EPO was given once a week at a starting dose of 2,000 IU per week subcutaneously, and the dose was increased or decreased as necessary to achieve and maintain a target Hb of 12 g%. The IV Fe (Venofer-Vifor International, St. Gallen, Switzerland), a ferric sucrose product, was given in a dose of 200 mg IV in 150 ml saline over 60 min every week until the serum ferritin reached 400 g/liter or the percent Fe saturation (%Fe Sat: serum iron/total iron binding capacity 100) reached 40% or until the Hb reached 12 g%. The IV Fe was then given at longer intervals as needed to maintain these levels.
Medication dose.
Except for oral and IV furosemide therapy, the doses of all the other CHF medications, which were used in the maximum tolerated doses before the intervention, were kept unchanged during the intervention period.
Duration of the study.
The study lasted for a mean of 7.2 5.5 months (range four to 15 months).
Investigations.
Visits were at weekly intervals initially and then at two- to three-week intervals depending on the patient’s status. This was the same frequency of visits to the CHF clinic as before the intervention study.
A complete blood count, serum creatinine, serum ferritin and % Fe Sat were performed on every visit.
An electronic device measured the blood pressure on every visit.
The LVEF was measured by a multiple gated ventricular angiography heart scan initially and at four- to six-month intervals.
Hospital records were reviewed to compare the number of hospitalizations during the time the patients were treated for the anemia with the number of hospitalizations
during a similar period of time that they were treated in the CHF clinic
before the anemia was treated.
Clinic records were reviewed to evaluate the types and doses of CHF medications used
before and during the study.
Period of time that they were treated in the CHF clinic before the anemia was treated.
Clinic records were reviewed to evaluate the types and doses of CHF medications used before and during the study. The glomerular filtration rate (GFR) was calculated from the serum creatinine by the formula: 1/serum creatinine in mg% x 100 GFR in ml/min. The rate of change of the GFR before and during the intervention period was calculated by comparing the change in GFR per month in the year before the intervention with that during the intervention.
Statistical analysis.
Mean standard deviation was calculated. One-way analysis of variance (ANOVA) was performed to compare parameter levels between the four NYHA groups. Hochberg’s method of multiple comparisons (23) was used for pair-wise comparison between two groups. A p value of less than 0.05 was considered statistically significant. In the intervention study, the significance of the difference between the initial values and those at the end of the study for the individual parameters in the 26 treated patients was assessed by paired student’s t test; p < 0.05 was considered statistically significant. All the statistical analysis was performed by the SPSS program (Version 9, Chicago, Illinois).
RESULTS
CHF: the whole study group.
The clinical, biochemical and hematological characteristics of the 142 patients seen in the clinic are shown in Tables 1 and 2.
Sixty-seven patients (47%) had severe CHF as judged by a NYHA class of IV (Table 2).
Seventy- nine of the 142 patients (55.6%) were anemic (Hb 12 g%).
The mean Hb level fell progressively from 13.73 +/- 0.83 g% in class I NYHA to 10.90 +/- 1.70 g% in class IV NYHA (p 0.01). The percentage of patients with Hb 12 g% increased from 9.1% in class I to 79.1% in class IV.
Fifty eight patients (40.8%) had CRF as defined as a serum creatinine 1.5 mg%. The mean serum creatinine increased from 1.18 +/_ 0.38 mg% in class I NYHA, to 2.0 +/- 1.89 mg% in class IV NYHA, p 0.001. The percentage of patients with an elevated serum creatinine ( 1.5 mg%) increased from 18.2% in class I to 58.2% in class IV.
The mean ejection fraction fell from 37.67 +/- 15.74% in class I to 27.72 +/- 9.68% (p 0.005) in class IV.
Table 2. LVEF and Biochemical and Hematological Parameters by NYHA Class in 142 Patients With CHF
NYHA Class I II III IV Significantly Different Pairs*
*p 0.05 at least between the two groups by pair-wise comparison between groups.
†p 0.05 at least between the groups by ANOVA.
No. of patients
11
26
38
67
(total 142) (%)
(7.7)
(18.3)
(26.8)
(47.2)
Hb, g%†
13.73 (0.83)
13.38 (1.26)
11.95 (1.48)
10.90 (1.70)
1–3, 1–4, 2–3, 2–4
Serum creatinine,
1.18
1.22
1.32
2.00
1–2, 1–3, 1–4
mg%†
(0.38)
(0.29)
(0.38)
(1.89)
LVEF, %†
37.67 (15.74)
32.88 (12.41)
32.02 (10.99)
27.72 (9.68)
1–4, 2–4
Hb 12 g%, (%)
1 (9.1)
5 (19.2)
20 (52.6)
53 (79.1)
Serum creatinine
2
5
12
39
1.5 mg%, (%)
(18.2)
(19.2)
(31.6)
(58.2)
The intervention study: medications.
The percentage of patients receiving each CHF medication before and after the intervention period and the reasons for not receiving them are seen in Table 3.
Table 3. Number (%) of the 26 Patients Taking Each Type of Medication Before and During the Intervention Period and the Reason Why the Medication Was Not Used
Medication No. of Patients (%) Reason for Not Receiving the Medications (No. of Patients)
BP blood pressure; CRF chronic renal failure; IV intravenous.
The main reason for not receiving:
1) ACE inhibitors was the presence of reduced renal function;
2) carvedilol was the presence of chronic obstructive pulmonary disease (COPD);
3) nitrates was low blood pressure and aortic stenosis and
4) aldactone was hyperkalemia.
Table 4. Mean Dose of Each Medication Initially and at the End of the Intervention Period in the 26 Patients
No. of Patients Initial Dose ^ Final Dose^
Carvedilol (mg/day) 20 26.9 15.5 28.8 14.5
Captopril (mg/day) 7 69.6 40.0 70.7 40.4
Enalapril (mg/day) 13 25.7 12.5 26.9 12.6
Digoxin (mg/day) 25 0.10 0.07 0.10 0.07
Aldactone (mg/day) 19 61.2 49.2 59.9 47.1
Long-acting nitrates 23 53.2 13.2 54.1 14.4
Oral furosemide (mg/day) 26 200.9 120.4 78.3 41.3*
IV furosemide (mg/month) 26 164.7 178.9 19.8 47.0*
*p 0.05 at least vs. before by paired Student’s t test.
^ +/-
The mean doses of the medications are shown in Table 4.
The mean dose of oral furosemide was 200.9 +/- 120.4 mg/day before and 78.3 +/- 41.3 mg/day after the intervention (p 0.05). The dose of IV furosemide was 164.7 +/- 19.8, 178.9 mg/month before and 7.0 mg/month after the intervention (p 0.05).
The doses of the other CHF medications were almost identical in the two periods.
Clinical results.
DEATHS.
There were three deaths during the intervention period. An 83-year-old man died after eight months of respiratory failure after many years of COPD, a 65-year-old man at eight months of a CVA with subsequent pneumonia and septic shock and a 70-year-old man at four months of septicemia related to an empyema that developed after aortic valve replacement.
HEMODIALYSIS.
Three patients, a 76-year-old man, an 85-year-old woman and a 72-year-old man, required chronic hemodialysis after six, 16 and 18 months, respectively. The serum creatinines of these three patients at onset of the anemia treatment were 4.2, 3.5 and 3.6 mg%, respectively. All three had improvement in their NYHA status but
their uremia worsened as the renal function deteriorated, demanding the initiation of dialysis.
In no cases, however, was pulmonary congestion an indication for starting dialysis.
Functional results (Table 5).
During the treatment period, the NYHA class fell from a mean of 3.66 +/- 0.47 to 2.66 +/- 0.70 (p 0.05), and
24 had some improvement in their functional class.
The mean LVEF increased from 27.7 +/- 4.8 to 35.4 +/- 7.6% (p 0.001), an increase of 27.8%.
Compared with a similar period of time before the onset of the anemia treatment, the mean number of hospitalizations fell from 2.72 +/- 1.21 to 0.22 +/- 0.65 per patient (p 0.05), a decrease of 91.9%.
No significant changes were found in the mean systolic/diastolic blood pressure.
Hematological results (Table 5).
The mean hematocrit (Hct) increased from 30.14 +/- 3.12%) to 35.9 +/- 4.22% (p < 0.001).
The mean Hb increased from 10.16 +/- 0.95 g%) to 12.10 +/- 1.21 g% (p < 0.001).
The mean serum ferritin increased from 177.07 +/- 113.80 g/liter to 346.73 +/- 207.40 g/liter (p 0.005).
The mean serum Fe increased from 60.4 +/- 19.0 g% to 74 +/- .80 20.7 g% (p 0.005).
The mean %Fe Sat increased from 20.05 6.04% to 26.14 =/- 5.23% (p 0.005).
The mean dose of EPO used throughout the treatment period was 5,227 +/- 455 IU per week, and
the mean dose of IV Fe used was 185.1 +/- 57.1 mg per month.
In four of the patients,the target Hb of 12 g% was maintained despite stopping the EPO for at least four months.
Renal results (Table 5).
The changes in serum creatinine were not significant. The estimated creatinine clearance fell at a rate of 0.95 + 1.31 ml/min/month before the onset of treatment of the anemia and increased at a rate of 0.85 + 2.77 ml/min/month during the treatment period.
Table 5. The Hematological and Clinical Data of the 26 CHF Patients at Onset and at the End of the Intervention Period
————– Initial ^ Final^
Hematocrit, vol% 30.14 3.12 35.90 4.22*
Hemoglobin, g% 10.16 0.95 2.10 1.21*
Serum ferritin, g/liter 177.07 113.80 346.73 207.40*
Serum iron, g% 60.4 19.0 74.8 20.7*
% iron saturation 20.5 6.04 26.14 5.23*
Serum creatinine, mg% 2.59 0.77 2.73 1.55
LVEF, % 27.7 4.8 35.4 7.6*
No. hospitalizations/patient 2.72 1.21 0.22 0.65*
Systolic BP, mm Hg 127.1 19.4 128.9 26.4
Diastolic BP, mm Hg 73.9 9.9 74.0 12.7
NYHA (0–4) 3.66 0.47 2.66 0.70*
*p 0.05 at least vs before by paired Student’s t test. ^ +/-
BP blood pressure; LVEF left ventricular ejection fraction; NYHA New York Heart Association.
DISCUSSION
The main findings in the present study are that anemia is common in CHF patients and becomes progressively more prevalent and severe as CHF progresses. In addition, for patients with resistant CHF, the treatment of the associated anemia causes a marked improvement in their
functional status,
ejection fraction and
GFR.
All these changes were associated with a markedly
reduced need for hospitalization and
for oral and IV furosemide.
The effect of anemia on the ischemic myocardium.
We used the IV Fe together with EPO to avoid the Fe deficiency caused by the use of EPO alone (38,39).
The Fe deficiency will cause
a resistance to EPO therapy and
increase the need for higher and higher doses to maintain the Hb level (39,40).
These high doses will not only be expensive but may increase the blood pressure excessively (41). The IV Fe reduces the dose of EPO needed to correct the anemia, because
the combination of SC EPO and IV Fe has been shown to have an additive effect on correction of the anemia of CRF (21,22,39,42).
Oral Fe, however, has no such additive effect (39,42). The relatively low dose of EPO needed to control the anemia in our study may explain why
the blood pressure did not increase significantly in any patient.
We used Venofer, an Fe sucrose product, as our IV Fe supplement because, in our experience (21,22,43), it has very few side effects and, indeed, no side effects with its use were encountered in this study.
The Effect of Anemia Correction on Renal Function.
Congestive heart failure is often associated with some degree of CRF (1–3,27–29), and
this is most likely due to renal vasoconstriction and ischemia (28,29).
When the anemia is treated and the cardiac function improves,
an increase in renal blood flow and glomerular filtration is seen (7,28).
In the present study, renal function decreased as the CHF functional class worsened (Table 2). The rate of deterioration of renal function was slower during the intervention period. Treatment of anemia in CRF has been associated with
a rate of progression of the CRF that is either unchanged (30) or is slowed (31–33).
It is possible, therefore, that adequate treatment of the anemia in CHF may, in the long term, help slow down the progression of CRF.
Possible Adverse Effects of Correction of the Anemia.
There has been concern, in view of the recent Amgen study (34), that correction of the Hct to a mean 42% in hemodialysis patients might increase cardiovascular events in those receiving EPO compared with those maintained at a Hct of 30%. Although there is much uncertainty about how to interpret this study (35), there is a substantial body of evidence that shows
correction of the anemia up to a Hb of 12 g% (Hct 36%) in CRF on dialysis is safe and desirable (35–38), and
results in a reduction in mortality, morbidity and in the number and length of hospitalizations.
The same likely holds true for the anemia of CHF with or without associated CRF. Certainly, our patients’ symptoms were strikingly improved, as was their cardiac function (LVEF) and need for hospitalization and diuretics. It remains to be established
if correction of the anemia up to a normal Hb level of 14 g% might be necessary in order to further improve the patient’s clinical state.
The Role of Fe Deficiency and its Treatment in the Anemia of CHF.
We used the IV Fe together with EPO to avoid the Fe deficiency caused by the use of EPO alone (38,39). The Fe deficiency will cause
a resistance to EPO therapy and increase the need for higher and higher doses to maintain the Hb level (39,40).
These high doses will not only be expensive but may
increase the blood pressure excessively (41).
The IV Fe reduces the dose of EPO needed to correct the anemia, because the combination of SC EPO and IV Fe has been shown to have an additive effect on correction of the anemia of CRF (21,22,39,42). Oral Fe, however, has no such additive effect (39,42). The relatively low dose of EPO needed to control the anemiain our study may explain
why the blood pressure did not increase significantly in any patient.
We used Venofer, an Fe sucrose product, as our IV Fe supplement because, in our experience (21,22,43), it has very few side effects and, indeed, no side effects with its use were encountered in this study.





























































![Poster-ProBNP_final[1]](https://i0.wp.com/pharmaceuticalintelligence.com/wp-content/uploads/2013/12/poster-probnp_final1.jpg)









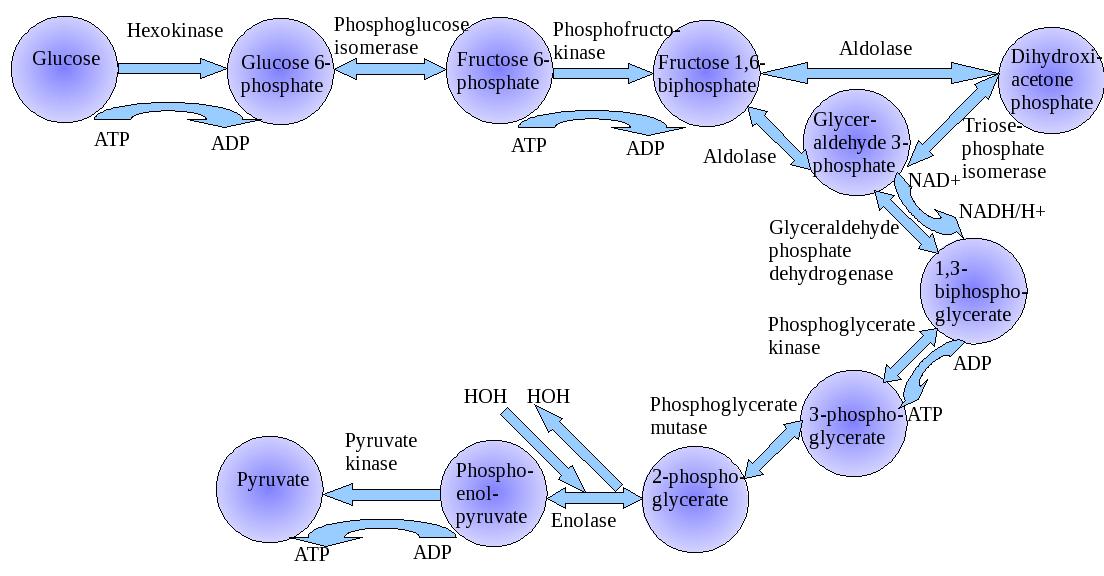{kind=link}