Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Article SELECTION from Collection of Aviva Lev-Ari, PhD, RN Scientific Articles on PULSE on LinkedIn.com for Training Small Language Models (SLMs) in Domain-aware Content of Medical, Pharmaceutical, Life Sciences and Healthcare by 15 Subjects Matter
Article selection: Aviva Lev-Ari, PhD, RN
#1 – February 20, 2016
Contributions to Personalized and Precision Medicine & Genomic Research
Non – CME – dSTRIDE™-HR: A Functional Biomarker for In Situ, ‘real-time’ Detection and Quantification of Homologous Recombination Activity.
Magda Kordon-Kiszala, PhD, CEO and co-founder,intoDNA
12:35-12:55
Epigenetic Plasticity and Tumor Evolution: Mechanisms of Resistance in Precision Oncology
Johnathan R. Whetstine, PhD, Director, Cancer Epigenetics Institute, Director, Geonomics Resource, Fox Chase Cancer Center
Title: Epigenetic plasticity a gatekeeper to generating extrachromosomal DNA amplification and rearrangements
genetic events in cancer are actually controlled not random as he says
Fox Chase Cancer Center Epigenetics Institute; 5th year goal to understand epigenetic mechanisms to understand resistance and biomarker development; bring others and break down silos; they are expanding and hiring and bringing into a network; March 5 2026 5th Annual Symposium Philadelphia Franklin Institute
DNA amplification is also chromosomal: integrated same locus or different regions or chromosomal duplication
KDM4A epigenetic demethylase controls transiet site specific DNA re-replication; can have focal control of DNA regions
you can control regional control of like EGFR amplification
can use Cy3 to find local regions
KDM3B inhibitor promotes transiet copy gains in KMT2A/MLL
EHMT2 is lysine demethylase is a driver of this copy amplification
this demethylase can change expression locally in one hour.. very fast
demethylases are very specific for their gene locus they control and so this demethylase only controls MLL gene
doxorubicin topoisomerase inhibitor can cause LOH in MLL locus and methylase inhibitor can reverse this
over twenty combinatorial regulators so this field is just budding
11:30-12:30
Companion Diagnostics in Hereditary and Chronic Diseases – Development, Regulatory Approval, and Commercialization – Non-CME Discussion
Huw Ricketts PhD, Senior Director, CLIA Business Development, QIAGEN
Tricia Carrigan, PhD, BC Biosolutions
Arushi Agarwal, MS, Partner, Health Advances
Melissa Reuter, MS, MBA, Director, Precision Medicine Program Strategy, GSK
This is a session panel Discussion on the current state of companion diagnostic development, not just in oncology. Regulatory aspects will be discussed
Arushi: There are alot of opportunities in non-oncology areas for companion diagnostics, and time to development may be an obstacle
Huw Rickets: From a development standpoint most people are not looking at the diagnostic side but more on the therapeutic side.
Tricia: There needs to be a shift in oncology drug development world, and pharma sees developing diagnostic is too expensive.
Meliisa: They try to engage early with the agencies to understand the regulatory landscape; GSK is very strong in their oncology platform but there are gaps in diagnostics and non-oncology programs
Arushi: seems in Pharma oncology and non-oncology programs seems siloed
for non-oncology many of the biomarkers may be rare… well under 25% of population
Huw: Qiagen trying to develop diagnostics for Parkinson’s but those rare genetic diseases are easier to develop
Arushi: neurodegenerative, NASH, and immuno diseases are big areas where companies are looking to make companion diagnostics
Huw: kidney disease is a big focus to develop companion diagnostics for
12:30-12:40
Non – CME – dSTRIDE™-HR: A Functional Biomarker for In Situ, ‘real-time’ Detection and Quantification of Homologous Recombination Activity.
Magda Kordon-Kiszala, PhD, CEO and co-founder,intoDNA
Tumor board Live… Molecular profiling great for identifying synthetic lethal combinations work very well… Many oncologist not accepting recommendations of molec tumor board
Tumor board Live . Oncologists don’t always accept tumor board recommendations based on molecular profiling… Dr Baptiste at first felt constrained to use single agent but WINTER combo trial with molec profiling better
Tumor board Live… Oncologist may give pushback when molecular therapeutic targets identified.. like when methylomics give a result and tumor board suggest temazolamide
Tumor board Live… Oncologist may give pushback when molecular therapeutic targets identified.. like when methylomics give a result and tumor board suggest temazolamide
Tumor board Live… Oncologist may give pushback when molecular therapeutic targets identified.. like when methylomics give a result and tumor board suggest temazolamide
Tumor board Live… Discussion of ovarian cancer case women first presented with CRC BRCA mut but failed PARP inhibitor board is looking at immunotherapy NGS IHC performed
Tumor board Live… Molecular profiling great for identifying synthetic lethal combinations work very well… Many oncologist not accepting recommendations of molec tumor board
Conference Coverage 2025 Advancing Precision Medicine Conference, Philadelphia PA October 3-4 2025
Reporter: Stephen J. Williams, PhD
The Annual Advanced Precision Medicine Conference will be held at the Pennsylvania Convention Center October 3-4 2025 in Philadelphia PA. Advancing Precision Medicine is an organization dedicated to provide education and discourse among medical professionals to advance the field of precision therapeutics and diagnostics in cancer, cardiovascular, and other diseases. The Annual symposium is held in Philadelphia.
The event will consist of two parallel tracks composed of keynote addresses, panel discussions and fireside chats which will encourage audience participation. Over the course of the two-day event leaders from industry, healthcare, regulatory bodies, academia and other pertinent stakeholders will share an intriguing and broad scope of content.
This event will consist of three immersive tracks, each crafted to explore the multifaceted dimensions of precision medicine. Delve into Precision Oncology, where groundbreaking advancements are reshaping the landscape of cancer diagnosis and treatment. Traverse the boundaries of Precision Medicine Outside of Oncology, as we probe into the intricate interplay of genetics, lifestyle, and environment across a spectrum of diseases and conditions including rare disease, cardiology, ophthalmology, and neurodegenerative disease. Immerse yourself in AI for Precision Medicine, where cutting-edge technologies are revolutionizing diagnostics, therapeutics, and patient care. Additionally, explore the emerging frontiers of Spatial Biology and Mult-Omics, where integrated approaches are unraveling the complexities of biological systems with unprecedented depth and precision.
APM is a mission-driven team dedicated to advancing clinical practice through education in precision medicine, oncology, and pathology. Our expert-led programs bring together clinicians, pathologists, pharmacists, nurses, and researchers from across the country.
What We Offer
In 2025, we’re proud to offer three specialized event series—each tailored to a different corner of the healthcare ecosystem:
Where discovery meets application – and science transforms lives.
What’s New in 2025?
Four Specialized Tracks:
Track 1 – 2025 WIN Symposium: Progress and Challenges in Precision Oncology Presented in partnership with Advancing Precision Medicine
As the official 2025 WIN Symposium, this dedicated track will explore the evolving landscape of precision oncology, highlighting both groundbreaking advances and the ongoing challenges of translating molecular insights into clinical impact. Curated by the WIN Consortium, the program will feature global leaders in cancer research, diagnostics, and therapeutic innovation—offering a comprehensive view of how precision medicine is reshaping oncology across tumor types and care settings.
Track 2 – Day 1 – Multi-Omics Integration, Day 2 – Precision Medicine Outside of Oncology
From genomics and transcriptomics to proteomics and metabolomics—this track highlights how multi-layered data is revolutionizing systems biology and clinical decision-making.
Diving into applications across cardiovascular, neurology, rare disease, infectious disease, and other therapeutic areas where precision tools are reshaping clinical practice.
Sidney Farber Professor of Medicine at Harvard Medical School and Dana-Farber Cancer Institute
Senior Physician-Scientist at Brigham and Women’s Hospital
Howard Hughes Medical Institute Investigator
William Kaelin is the Sidney Farber Professor of Medicine at Harvard Medical School and Dana-Farber Cancer Institute, Senior Physician-Scientist at Brigham and Women’s Hospital and Howard Hughes Medical Institute Investigator. He obtained his undergraduate and M.D. degrees from Duke University and completed his training in Internal Medicine at the Johns Hopkins Hospital, where he served as chief medical resident. He was a clinical fellow in Medical Oncology at the Dana-Farber Cancer Institute and later a postdoctoral fellow in David Livingston’s laboratory, during which time he was a McDonnell Scholar.
A Nobel Laureate, Dr. Kaelin received the 2019 Nobel Prize in Physiology or Medicine. He is a member of the National Academy of Sciences, the American Academy of Arts and Sciences, the National Academy of Medicine, the American Society of Clinical Investigation, and the American College of Physicians. He previously served on the National Cancer Institute Board of Scientific Advisors, the AACR Board of Trustees, and the Institute of Medicine National Cancer Policy Board. He is a recipient of the Paul Marks Prize for cancer research from the Memorial Sloan-Kettering Cancer Center; the Richard and Hinda Rosenthal Prize from the AACR; the Doris Duke Distinguished Clinical Scientist award; the 2010 Canada International Gairdner Award; ASCI’s Stanley J. Korsmeyer Award; the Scientific Grand Prix of the Foundation Lefoulon-Delalande; the Wiley Prize in Biomedical Sciences; the Steven C. Beering Award; the AACR Princess Takamatsu Award; the ASCO Science of Oncology Award; the Helis Award; the Albert Lasker Basic Medical Research Prize; the Massry Prize; the Harriet P. Dustan Award for Science as Related to Medicine from the American College of Physicians.
Dr. Kaelin’s research seeks to understand how, mechanistically, mutations affecting tumor-suppressor genes cause cancer. His laboratory is currently focused on studies of the VHL, RB-1, and p53 tumor suppressor genes. His long-term goal is to lay the foundation for new anticancer therapies based on the biochemical functions of such proteins. His work on the VHL protein helped to motivate the eventual successful clinical testing of VEGF inhibitors for the treatment of kidney cancer. Moreover, this line of investigation led to new insights into how cells sense and respond to changes in oxygen, and thus has implications for diseases beyond cancer, such as anemia, myocardial infarction, and stroke. His group also showed that leukemic transformation by mutant IDH was reversible, setting the stage for the development and approval of mutant IDH inhibitors, and discovered how thalidomide-like drugs kill myeloma cells by degrading two otherwise undruggable transcription factors,
A diverse group of more than 90 key opinion leaders will convene to explore the critical forces shaping the future of healthcare. Representing a range of disciplines—including genomics, bioinformatics, clinical research, biopharma, technology, and investment—these experts will lead discussions on the latest advancements and challenges in precision medicine.
Topics will include the evolution of genomic sequencing technologies, ethical considerations in managing patient data, the integration of AI in diagnostics, and strategies for translating innovation into clinical practice. The inclusion of investors and strategic partners will also bring a vital perspective on funding models, commercialization pathways, and the acceleration of cutting-edge therapies. Together, these voices will offer a comprehensive view of the trends transforming personalized healthcare on a global scale.
Networking Opportunities
Our precision medicine event, hosting over 500 attendees, offers invaluable networking opportunities. Bringing together professionals, researchers, and industry leaders, the event facilitates engaging discussions, knowledge-sharing, and potential partnerships, driving advancements in precision medicine.
Why Exhibit
Exhibiting at the event provides a unique opportunity to showcase your cutting-edge solutions and connect with key stakeholders in the rapidly advancing field of personalized healthcare. As an exhibitor, you’ll gain visibility among industry leaders, researchers, and professionals, allowing you to forge strategic partnerships, highlight your contributions to precision medicine, and stay at the forefront of innovations shaping the future of healthcare. Don’t miss the chance to position your company as a leader in this dynamic and transformative space, driving meaningful collaborations and contributing to the advancement of precision medicine.
Studies are showing that genetic tests are being ordered at a sufficient rate however it appears there are problems in interpretation and developing treatment plans based on omics testing results
30 % of patients in past and now currently half of all patients are not being given the proper treatment based on genomic testing results (ASCO)
E.g. only 1.5% with NTRK fusions received a NTRK based therapy (this was > 4000 patients receiving wrong therapy)
A lung oncologist may only see one patient with NTRK fusion in three years
Precision Medicine Practice Gaps
48% of oncologist surveyed agreed pathologist needs to be more informed and relevant in the decision making process with regard to tests needing to be ordered
95% said need to flip cost issues ; what does it cost not to get a test … i.e. what is the cost of the wrong therapy
We need a new commercialization model for therapeutic development for this new era of “n of one” patient
There are some tumor markers approved by FDA that cant just be measured by NGS and are correlated with a pathologic complete response
Many point mutations will have no actionable drug
Many alterations are post-genomic meaning there is a post translational component to many prognostic biomarkers
Prevalence of point mutation with no actionable mutation is a limit of NGS
It is important to look at phospho protein spectrum as a potential biomarker
Reverse phase protein proteomic analysis
Made into CLIA based array
They trained centers around the US on the technology and analysis
Basing proteomics or protein markers by traditional IHC requires much antibody validation so if the mass spectrometry field can catch up it would be very powerful
With multiple MRM.MS there is too low abundance of phosphoproteins to allow for good detection
They conducted the I-SPY2 trial for breast cancer and determining if phosphoproteins could be a good biomarker panel
They found they could predict a HER2 response better than NGS
There were patients who were predicted HER2 negative that actually had an activated HER2 signaling pathway by proteomics so NGS must have had a series of false negatives
HER2 co phosphorylation predicts pathologic complete response and predicts therapy by herceptin
They found patients classified as HER2 negative by FISH were HER2 positive by proteomics and had HER2 activation
2024 Nobel Prize in Physiology or Medicine jointly to Victor Ambros and Gary Ruvkun for the discovery of microRNA and its role in post-transcriptional gene regulation
Reporter: Aviva Lev-Ari, PhD, RN
Updated 10/22/2024
The revolution in our understanding of transcriptional regulation and dark regions of the genome
The genome of higher eukaryotes are comprised of multiple exonic and intronic regions, with coding and noncoding DNA respectively. Much of the DNA sequence between exonic regions of genes, the sequences encoding the amino acids of a polypeptide, was considered either promoter regions regulating an exonic sequence or ‘junk DNA’, which had merely separated exons and their regulatory elements. It was not considered that this dark DNA or junk DNA was important in regulating transcription of genes. It was felt that most gene regulation occurred in promoter regions by response element factors which bound to specific sequences within these regions.
MicroRNA (miRNA), originally discovered in Caenorhabditis elegans, is found in most eukaryotes, including humans [1–3]. It is predicted that miRNA account for 1-5% of the human genome and regulate at least 30% of protein-coding genes [4–8]. To date, 940 distinct miRNAs molecules have been identified within the human genome [9–12] (http://microrna.sanger.ac.uk accessed July 20, 2010). Although little is currently known about the specific targets and biological functions of miRNA molecules thus far, it is evident that miRNA plays a crucial role in the regulation of gene expression controlling diverse cellular and metabolic pathways.
MiRNA are small, evolutionary conserved, single-stranded, non-coding RNA molecules that bind target mRNA to prevent protein production by one of two distinct mechanisms. Mature miRNA is generated through two-step cleavage of primary miRNA (pri-miRNA), which incorporates into the effector complex RNA-induced silencing complex (RISC). The miRNA functions as a guide by base-pairing with target mRNA to negatively regulate its expression. The level of complementarity between the guide and mRNA target determines which silencing mechanism will be employed; cleavage of target messenger RNA (mRNA) with subsequent degradation or translation inhibition
Fig. (1). MicroRNA maturation and function.
Figure. miRNA maturation and function. Source: Macfarlane LA, Murphy PR. MicroRNA: Biogenesis, Function and Role in Cancer. Curr Genomics. 2010 Nov;11(7):537-61. doi: 10.2174/138920210793175895.
The following is an interview in the journal Journal of Cellular Biology with Dr, Victor Ambros on his discovery of miRNA.
Source: Ambros V. Victor Ambros: the broad scope of microRNAs. Interview by Caitlin Sedwick. J Cell Biol. 2013 May 13;201(4):492-3. doi: 10.1083/jcb.2014pi. PMID: 23671307; PMCID: PMC3653358.
Once, we thought we understood all there was to know about how gene expression is regulated: A cell can tinker with the expression level of a given protein’s messenger RNA by modifying the activity, abundance, and type of transcription factors in the nucleus or with the RNA’s stability once it is made. But then came a surprising story about a short RNA in C. elegans called lin-4, which didn’t encode a protein but prevented expression of the protein encoded by another gene, lin-14, through antisense binding to lin-14 mRNA (1, 2). Today, we know that lin-4 was just the first example of a large number of small RNAs, called microRNAs, which regulate the expression of various other proteins in a similar way.
Victor Ambros, whose lab published that first story about lin-4, has been studying microRNAs (3, 4) and their regulation (5, 6) ever since, pushing forward our understanding of this powerful mechanism. We called him at his office at the University of Massachusetts Medical School to get some perspective on microRNAs and his career and to learn about some of the latest developments in his lab.
“That shared discovery is one of the most precious moments in my career.”
FROM FARM TO LAB TABLE
How did you end up doing a PhD with David Baltimore?
I was the first scientist in my family. My dad was an immigrant from Poland. He came to the States just after World War II and met my mom. They got married, moved to a farm in Vermont, and started farming. My siblings and I grew up amongst the cows and pigs and helped with the haying and cutting corn, stuff like that.
When I was about nine, I got interested in science, and after that I always wanted to be a scientist. I was an amateur astronomer; I built a telescope and started to imagine that I could actually do astronomy or physics as an occupation. But I quickly changed my mind when I reached college, in part because I realized that my math skills weren’t really up to the task of being a physicist and also because I discovered molecular biology and genetics and just fell in love with both subjects. David taught one of the advanced biology classes I took as an undergraduate at MIT, and that probably had some influence on my decision to work with him. After college, I worked as a technician in David’s lab for a year. I liked it a lot and stayed on in his lab when I entered graduate school at MIT. I was lucky because I had gotten a little bit of traction on a project and continued on that as a grad student, so I ended up finishing grad school fairly efficiently.
Had you any idea at the time what the nature of the lin-4 mutant was?
The assumption was that it was a protein product. I mean, nobody ever thought that there would be any other kind of regulator. There really wasn’t any reason to imagine that there were any other kinds of molecules necessary, other than proteins, to carry out everything that’s done in a cell—especially with regard to the regulation of gene expression. The complexity of gene regulation by proteins alone was so enormous that I never imagined—and nobody I knew imagined—that we needed to look for new kinds of regulatory molecules. The realization that lin-4 was antisense to the 3′-untranslated region of lin-14 was totally the result of communication between Gary and me. That shared discovery is one of the most precious moments in my career. But at the time I didn’t realize that this might be the first example of a general mechanism for regulating gene expression because I was prone to thinking that whatever I was studying in the worm was not generally applicable. It wasn’t until genome sequences were made available that the prevalence of this mechanism became clear.
THE RIGHT CONTEXT
You’ve moved to studying processes that modulate microRNA function…
One protein we’ve studied is called Nhl-2. It’s an example of an emerging class of proteins that can modulate, positively or negatively, the RNA-induced silencing complex (RISC) that inhibits mRNAs targeted by microRNAs. This class of genes may have either general effects on RISC activity or, in some cases, more specific effects. One area of interest in the lab right now is trying to understand the specific outcomes for the regulation of particular microRNAs. Do they always interact with all their targets, or is their activity on some targets promoted or inhibited at the expense of other targets? Can their interaction with certain targets be modified depending on context? We’re using genetic and genomic approaches to identify new modulatory cofactors.
Watch Video
Victor Ambros was born in 1953 in Hanover, New Hampshire, USA. He received his PhD from Massachusetts Institute of Technology (MIT), Cambridge, MA, in 1979 where he also did postdoctoral research 1979-1985. He became a Principal Investigator at Harvard University, Cambridge, MA in 1985. He was Professor at Dartmouth Medical School from 1992-2007 and he is now Silverman Professor of Natural Science at the University of Massachusetts Medical School, Worcester, MA.
Gary Ruvkun was born in Berkeley, California, USA in 1952. He received his PhD from Harvard University in 1982. He was a postdoctoral fellow at Massachusetts Institute of Technology (MIT), Cambridge, MA, 1982-1985. He became a Principal Investigator at Massachusetts General Hospital and Harvard Medical School in 1985, where he is now Professor of Genetics.
This year’s Nobel Prize honors two scientists for their discovery of a fundamental principle governing how gene activity is regulated.
The information stored within our chromosomes can be likened to an instruction manual for all cells in our body. Every cell contains the same chromosomes, so every cell contains exactly the same set of genes and exactly the same set of instructions. Yet, different cell types, such as muscle and nerve cells, have very distinct characteristics. How do these differences arise? The answer lies in gene regulation, which allows each cell to select only the relevant instructions. This ensures that only the correct set of genes is active in each cell type.
Victor Ambros and Gary Ruvkun were interested in how different cell types develop. They discovered microRNA, a new class of tiny RNA molecules that play a crucial role in gene regulation. Their groundbreaking discovery revealed a completely new principle of gene regulation that turned out to be essential for multicellular organisms, including humans. It is now known that the human genome codes for over one thousand microRNAs. Their surprising discovery revealed an entirely new dimension to gene regulation. MicroRNAs are proving to be fundamentally important for how organisms develop and function.
Ambros and Ruvkun were interested in genes that control the timing of activation of different genetic programs, ensuring that various cell types develop at the right time. They studied two mutant strains of worms, lin-4 and lin-14, that displayed defects in the timing of activation of genetic programs during development. The laureates wanted to identify the mutated genes and understand their function. Ambros had previously shown that the lin-4 gene appeared to be a negative regulator of the lin-14 gene. However, how the lin-14 activity was blocked was unknown. Ambros and Ruvkun were intrigued by these mutants and their potential relationship and set out to resolve these mysteries.
Ambros and Ruvkun performed further experiments showing that the lin-4 microRNA turns off lin-14 by binding to the complementary sequences in its mRNA, blocking the production of lin-14 protein. A new principle of gene regulation, mediated by a previously unknown type of RNA, microRNA, had been discovered! The results were published in 1993 in two articles in the journal Cell.
Ruvkun cloned let-7, a second gene encoding a microRNA. The gene is conserved in evolution, and it is now known that microRNA regulation is universal among multicellular organisms.
Andrew Z. Fire and Craig C. Mello, awarded the Nobel Prize in 2006, described RNA interference, where specific mRNA-molecules are inactivated by adding double-stranded RNA to cells.
Mutations in one of the proteins required for microRNA production result in the DICER1 syndrome, a rare but severe syndrome linked to cancer in various organs and tissues.
Use of Systems Biology for Design of inhibitor of Galectins as Cancer Therapeutic – Strategy and Software
Curator:Stephen J. Williams, Ph.D.
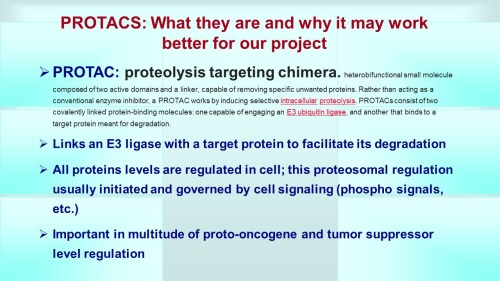
Below is a slide representation of the overall mission 4 to produce a PROTAC to inhibit Galectins 1, 3, and 9.
Using A Priori Knowledge of Galectin Receptor Interaction to Create a BioModel of Galectin 3 Binding
Now after collecting literature from PubMed on “galectin-3” AND “binding” to determine literature containing kinetic data we generate a WordCloud on the articles.
This following file contains the articles needed for BioModels generation.
From the WordCloud we can see that these corpus of articles describe galectin binding to the CRD (carbohydrate recognition domain). Interestingly there are many articles which describe van Der Waals interactions as well as electrostatic interactions. Certain carbohydrate modifictions like Lac NAc and Gal 1,4 may be important. Many articles describe the bonding as well as surface interactions. Many studies have been performed with galectin inhibitors like TDGs (thio-digalactosides) like TAZ TDG (3-deoxy-3-(4-[m-fluorophenyl]-1H-1,2,3-triazol-1-yl)-thio-digalactoside). This led to an interesting article
.
Dual thio-digalactoside-binding modes of human galectins as the structural basis for the design of potent and selective inhibitors
Human galectins are promising targets for cancer immunotherapeutic and fibrotic disease-related drugs. We report herein the binding interactions of three thio-digalactosides (TDGs) including TDG itself, TD139 (3,3′-deoxy-3,3′-bis-(4-[m-fluorophenyl]-1H-1,2,3-triazol-1-yl)-thio-digalactoside, recently approved for the treatment of idiopathic pulmonary fibrosis), and TAZTDG (3-deoxy-3-(4-[m-fluorophenyl]-1H-1,2,3-triazol-1-yl)-thio-digalactoside) with human galectins-1, -3 and -7 as assessed by X-ray crystallography, isothermal titration calorimetry and NMR spectroscopy. Five binding subsites (A-E) make up the carbohydrate-recognition domains of these galectins. We identified novel interactions between an arginine within subsite E of the galectins and an arene group in the ligands. In addition to the interactions contributed by the galactosyl sugar residues bound at subsites C and D, the fluorophenyl group of TAZTDG preferentially bound to subsite B in galectin-3, whereas the same group favored binding at subsite E in galectins-1 and -7. The characterised dual binding modes demonstrate how binding potency, reported as decreased Kd values of the TDG inhibitors from μM to nM, is improved and also offer insights to development of selective inhibitors for individual galectins.
Figures
Figure 1. Chemical structures of L3, TDG…
Figure 2. Structural comparison of the carbohydrate…
Proteolysis-targeting chimeras (PROTACs) are a promising new class of drugs that selectively degrade cellular proteins of interest. PROTACs that target oncogene products are avidly being explored for cancer therapies, and several are currently in clinical trials. Drug resistance is a substantial challenge in clinical oncology, and resistance to PROTACs has been reported in several cancer cell models. Here, using proteomic analysis, we found intrinsic and acquired resistance mechanisms to PROTACs in cancer cell lines mediated by greater abundance or production of the drug efflux pump MDR1. PROTAC-resistant cells were resensitized to PROTACs by genetic ablation of ABCB1 (which encodes MDR1) or by coadministration of MDR1 inhibitors. In MDR1-overexpressing colorectal cancer cells, degraders targeting either the kinases MEK1/2 or the oncogenic mutant GTPase KRASG12C synergized with the dual epidermal growth factor receptor (EGFR/ErbB)/MDR1 inhibitor lapatinib. Moreover, compared with single-agent therapies, combining MEK1/2 degraders with lapatinib improved growth inhibition of MDR1-overexpressing KRAS-mutant colorectal cancer xenografts in mice. Together, our findings suggest that concurrent blockade of MDR1 will likely be required with PROTACs to achieve durable protein degradation and therapeutic response in cancer.
INTRODUCTION
Proteolysis-targeting chimeras (PROTACs) have emerged as a revolutionary new class of drugs that use cancer cells’ own protein destruction machinery to selectively degrade essential tumor drivers (1). PROTACs are small molecules with two functional ends, wherein one end binds to the protein of interest, whereas the other binds to an E3 ubiquitin ligase (2, 3), bringing the ubiquitin ligase to the target protein, leading to its ubiquitination and subsequent degradation by the proteasome. PROTACs have enabled the development of drugs against previously “undruggable” targets and require neither catalytic activity nor high-affinity target binding to achieve target degradation (4). In addition, low doses of PROTACs can be highly effective at inducing degradation, which can reduce off-target toxicity associated with high dosing of traditional inhibitors (3). PROTACs have been developed for a variety of cancer targets, including oncogenic kinases (5), epigenetic proteins (6), and, recently, KRASG12C proteins (7). PROTACs targeting the androgen receptor or estrogen receptor are avidly being evaluated in clinical trials for prostate cancer (NCT03888612) or breast cancer (NCT04072952), respectively.
However, PROTACs may not escape the overwhelming challenge of drug resistance that befalls so many cancer therapies (8). Resistance to PROTACs in cultured cells has been shown to involve genomic alterations in their E3 ligase targets, such as decreased expression of Cereblon (CRBN), Von Hippel Lindau (VHL), or Cullin2 (CUL2) (9–11). Up-regulation of the drug efflux pump encoded by ABCB1—MDR1 (multidrug resistance 1), a member of the superfamily of adenosine 5′-triphosphate (ATP)–binding cassette (ABC) transporters—has been shown to convey drug resistance to many anticancer drugs, including chemotherapy agents, kinase inhibitors, and other targeted agents (12). Recently, PROTACs were shown to be substrates for MDR1 (10, 13), suggesting that drug efflux represents a potential limitation for degrader therapies. Here, using degraders (PROTACs) against bromodomain and extraterminal (BET) bromodomain (BBD) proteins and cyclin-dependent kinase 9 (CDK9) as a proof of concept, we applied proteomics to define acquired resistance mechanisms to PROTAC therapies in cancer cells after chronic exposure. Our study reveals a role for the drug efflux pump MDR1 in both acquired and intrinsic resistance to protein degraders in cancer cells and supports combination therapies involving PROTACs and MDR1 inhibitors to achieve durable protein degradation and therapeutic responses.
Fig. 1. Proteomic characterization of degrader-resistant cancer cell lines. (A) Workflow for identifying protein targets up-regulated in degrader-resistant cancer cells. Single-run proteome analysis was performed, and changes in protein levels among parent and resistant cells were determined by LFQ. m/z, mass/charge ratio. (B and C) Cell viability assessed by CellTiter-Glo in parental and dBET6- or Thal SNS 032–resistant A1847 cells treated with increasing doses of dBET6 (B) or Thal SNS 032 (C) for 5 days. Data were analyzed as % of DMSO control, presented as means ± SD of three independent assays. Growth inhibitory 50% (GI50) values were determined using Prism software. (D to G) Immunoblotting for degrader targets and downstream signaling in parental A1847 cells and their derivative dBET6-R or Thal-R cells treated with increasing doses of dBET6 or Thal SNS 032 for 4 hours. The dBET6-R and Thal-R cells were continuously cultured in 500 nM PROTAC. Blots are representative, and densitometric analyses are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 values, quantitating either (E) the dose of dBET6 that reduces BRD2, BRD3, or BRD4 or (G) the dose of Thal SNS 032 that reduces CDK9 protein levels 50% of the DMSO control treatment, were determined with Prism software. Pol II, polymerase II. (H to K) Volcano plot of proteins with increased or reduced abundance in dBET6-R (H) or Thal-R (I) A1847 cells relative to parental cells. Differences in protein log2 LFQ intensities among degrader-resistant and parental cells were determined by paired t test permutation-based adjusted P values at FDR of <0.05 using Perseus software. The top 10 up-regulated proteins in each are shown in (J) and (K), respectively. FC, fold change. (L and M) ABCB1 log2 LFQ values in dBET6-R cells from (H) and Thal-R cells from (I) compared with those in parental A1847 cells. Data are presented as means ± SD from three independent assays. By paired t test permutation-based adjusted P values at FDR of <0.05 using Perseus software, ***P ≤ 0.001. (N) Cell viability assessed by CellTiter-Glo in parental and MZ1-resistant SUM159 cells treated with increasing doses of MZ1 for 5 days. Data were analyzed as % of DMSO control, presented as means of three independent assays. GI50 values were determined using Prism software. (O and P) Immunoblotting for degrader targets and downstream signaling in parental or MZ1-R SUM159 cells treated with increasing doses of MZ1 for 24 hours. The MZ1-R cells were continuously cultured in 500 nM MZ1. Blots are representative, and densitometric analyses are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 values were determined in Prism software. (Q and R) Top 10 up-regulated proteins (Q) and ABCB1 log2 LFQ values (R) in MZ1-R cells relative to parental SUM159 cells
Fig. 2. Chronic exposure to degraders induces MDR1 expression and drug efflux activity. (A) ABCB1 mRNA levels in parental and degrader-resistant cell lines as determined by qRT-PCR. Data are means ± SD of three independent experiments. ***P ≤ 0.001 by Student’s t test. (B) Immunoblot analysis of MDR1 protein levels in parental and degrader-resistant cell lines. Blots are representative of three independent experiments. (C to E) Immunofluorescence (“IF”) microscopy of MDR1 protein levels in A1847 dBET6-R (C), SUM159 MZ1-R (D), and Thal-R A1847 cells (E) relative to parental cells. Nuclear staining by DAPI. Images are representative of three independent experiments. Scale bars, 100 μm. (F) Drug efflux activity in A1847 dBET6-R, SUM159 MZ1-R, and Thal-R A1847 cells relative to parental cells (Par.) using rhodamine 123 efflux assays. Bars are means ± SD of three independent experiments. ***P ≤ 0.001 by Student’s t test. (G) Intracellular dBET6 levels in parental or dBET-R A1847 cells transfected with a CRBN sensor and treated with increasing concentrations of dBET6. Intracellular dBET6 levels measured using the CRBN NanoBRET target engagement assay. Data were analyzed as % of DMSO control, presented as means ± SD of three independent assays. *P ≤ 0.05, **P ≤ 0.01, and ***P ≤ 0.001 by Student’s t test. (H and I) FISH analysis of representative drug-sensitive parental and drug-resistant A1847 (H) and SUM159 (I) cells using ABCB1 and control XCE 7 centromere probes. Images of interphase nuclei were captured with a Metasystems Metafer microscope workstation, and the raw images were extracted and processed to depict ABCB1 signals in magenta, centromere 7 signals in cyan, and DAPI-stained nuclei in blue. (J and K) CpG methylation status of the ABCB1 downstream promoter (coordinates: chr7.87,600,166-87,601,336) by bisulfite amplicon sequencing in parent and degrader-resistant A1847 (J) and SUM159 (K) cells. Images depict the averaged percentage of methylation for each region of the promoter, where methylation status is depicted by color as follows: red, methylated; blue, unmethylated. Schematic of the ABCB1 gene with the location of individual CpG sites is shown. Graphs are representative of three independent experiments. (L and M) Immunoblot analysis of MDR1 protein levels after short-term exposure [for hours (h) or days (d) as indicated] to BET protein degraders dBET6 or MZ1 (100 nM) in A1847 (L) and SUM159 (M) cells, respectively. Blots are representative of three independent experiments. (N to P) Immunoblot analysis of MDR1 protein levels in A1847 and SUM159 cells after long-term exposure (7 to 30 days) to BET protein degraders dBET6 (N), Thal SNS 032 (O), or MZ1 (P), each at 500 nM. Blots are representative of three independent experiments. (Q and R) Immunoblot analysis of MDR1 protein levels in degrader-resistant A1847 (Q) and SUM159 (R) cells after PROTAC removal for 2 or 7 days. Blots are representative of three independent experiments.
Fig. 3. Blockade of MDR1 activity resensitizes degrader-resistant cells to PROTACs. (A and B) Cell viability by CellTiter-Glo assay in parental and degrader-resistant A1847 (A) and SUM159 (B) cells transfected with control siRNA or siRNAs targeting ABCB1 and cultured for 120 hours. Data were analyzed as % of control, presented as means ± SD of three independent assays. ***P ≤ 0.001 by Student’s t test. (C and D) Immunoblot analysis of degrader targets after ABCB1 knockdown in parental and degrader-resistant A1847 (C) and SUM159 (D) cells. Blots are representative, and densitometric analyses using ImageJ are means ± SD of three blots, each normalized to the loading control, GAPDH. (E) Drug efflux activity, using the rhodamine 123 efflux assay, in degrader-resistant cells after MDR1 inhibition by tariquidar (0.1 μM). Data are means ± SD of three independent experiments. ***P ≤ 0.001 by Student’s t test. (F to H) Cell viability by CellTiter-Glo assay in parental and dBET6-R (F) or Thal-R (G) A1847 cells or MZ1-R SUM159 cells (H) treated with increasing concentrations of tariquidar. Data are % of DMSO control, presented as means ± SD of three independent assays. GI50 value determined with Prism software. (I to K) Immunoblot analysis of degrader targets after MDR1 inhibition (tariquidar, 0.1 μM for 24 hours) in parental and degrader-resistant A1847 cells (I and J) and SUM159 cells (K). Blots are representative, and densitometric analyses are means ± SD from three blots, each normalized to the loading control, GAPDH. (L and M) A 14-day colony formation assessed by crystal violet staining of (L) A1847 cells or (M) SUM159 cells treated with degrader (0.1 μM; dBET6 or MZ1, respectively) and MDR1 inhibitor tariquidar (0.1 μM). Images are representative of three biological replicates. (N) Immunoblotting for MDR1 in SUM159 cells stably expressing FLAG-MDR1 after selection with hygromycin. (O) Long-term 14-day colony formation assay of SUM159 cells expressing FLAG-MDR1 that were treated with DMSO, MZ1 (0.1 μM), or MZ1 and tariquidar (0.1 μM) for 14 days, assessed by crystal violet staining. Representative images of three biological replicates are shown. (P and Q) RT-PCR (P) and immunoblot (Q) analysis of ABCB1 mRNA and MDR1 protein levels, respectively, in parental or MZ1-R HCT116, OVCAR3, and MOLT4 cells.
Fig. 4. Overexpression of MDR1 conveys intrinsic resistance to degrader therapies in cancer cells. (A) Frequency of ABCB1 mRNA overexpression in a panel of cancer cell lines, obtained from cBioPortal for Cancer Genomics using Z-score values of >1.2 for ABCB1 mRNA levels (30). (B) Immunoblot for MDR1 protein levels in a panel of 10 cancer cell lines. Blots are representative of three independent experiments. (C) Cell viability by CellTiter-Glo assay in cancer cell lines expressing high or low MDR1 protein levels and treated with Thal SNS 032 for 5 days. Data were analyzed as % of DMSO control, presented as means ± SD of three independent assays. GI50 values were determined with Prism software. (D to F) Immunoblot analysis of CDK9 in MDR1-low (D) or MDR1-high (E) cell lines after Thal SNS 032 treatment for 4 hours. Blots are representative, and densitometric analyses using ImageJ are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 value determined with Prism. (G and H) Immunoblotting of control and MDR1-knockdown DLD-1 cells treated for 4 hours with increasing concentrations of Thal SNS 032 [indicated in (H)]. Blots are representative, and densitometric analysis data are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 value determined with Prism. (I) Drug efflux activity using rhodamine 123 efflux assays in DLD-1 cells treated with DMSO or 0.1 μM tariquidar. Data are means ± SD of three independent experiments. ***P ≤ 0.001 by Student’s t test. (J) Intracellular Thal SNS 032 levels, using the CRBN NanoBRET target engagement assay, in MDR1-overexpressing DLD-1 cells treated with DMSO or 0.1 μM tariquidar and increasing doses of Thal SNS 032. Data are % of DMSO control, presented as means ± SD of three independent assays. **P ≤ 0.01 and ***P ≤ 0.001 by Student’s t test. (K to N) Immunoblotting in DLD-1 cells treated with increasing doses of Thal SNS 032 (K and L) or dBET6 (M and N) alone or with tariquidar (0.1 μM) for 4 hours. Blots are representative, and densitometric analyses are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 value of Thal SNS 032 for CDK9 reduction (L) or of dBET6 for BRD4 reduction (N) determined with Prism. (O to T) Bliss synergy scores based on cell viability by CellTiter-Glo assay, colony formation, and immunoblotting in DLD-1 cells treated with the indicated doses of Thal SNS 032 (O to Q) or dBET6 (R to T) alone or with tariquidar. Cells were treated for 14 days for colony formation assays and 24 hours for immunoblotting.
Fig. 5. Repurposing dual kinase/MDR1 inhibitors to overcome degrader resistance in cancer cells. (A and B) Drug efflux activity by rhodamine 123 efflux assays in degrader-resistant [dBET-R (A) or Thal-R (B)] A1847 cells after treatment with tariquidar, RAD001, or lapatinib (each 2 μM). Data are means ± SD of three independent experiments. *P ≤ 0.05 by Student’s t test. (C and D) CellTiter-Glo assay for the cell viability of parental, dBET6-R, or Thal-R A1847 cells treated with increasing concentrations of RAD001 (C) or lapatinib (D). Data were analyzed as % of DMSO control, presented as means ± SD of three independent assays. GI50 values were determined with Prism software. (E to I) Immunoblot analysis of degrader targets in parental (E), dBET6-R (F and G), and Thal-R (H and I) A1847 cells treated with increasing concentrations of RAD001 or lapatinib for 4 hours. Blots are representative, and densitometric analyses are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 value of dBET6 for BRD4 reduction (G) or of Thal SNS 032 for CDK9 reduction (I) determined with Prism. (J) Immunoblotting for cleaved PARP in dBET6-R or Thal-R A1847 cells treated with RAD001, lapatinib, or tariquidar (each 2 μM) for 24 hours. Blots are representative of three independent blots. (K to N) Immunoblotting for BRD4 in DLD-1 cells treated with increasing doses of dBET6 alone or in combination with either RAD001 or lapatinib [each 2 μM (K and L)] or KU-0063794 or afatinib [each 2 μM (M and N)] for 4 hours. Blots are representative of three independent experiments and, in (L), are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 value for BRD4 reduction (L) determined in Prism. (O) Colony formation by DLD-1 cells treated with DMSO, dBET6 (0.1 μM), lapatinib (2 μM), afatinib (2 μM), RAD001 (2 μM), KU-0063794 (2 μM), or the combination of inhibitor and dBET6 for 14 days. Images representative of three independent assays. (P and Q) Immunoblotting for CDK9 in DLD-1 cells treated with increasing doses of Thal SNS 032 and/or RAD001 (2 μM) or lapatinib (2 μM) for 4 hours. Blots are representative, and densitometric analyses are means ± SD from three blots, each normalized to the loading control, GAPDH. DC50 value for CDK9 reduction determined with Prism (Q). (R) Colony formation in DLD-1 cells treated with DMSO, Thal SNS 032 (0.5 μM), lapatinib (2 μM), and/or RAD001 (2 μM) as indicated for 14 days.
Fig. 6. Combining MEK1/2 degraders with lapatinib synergistically kills MDR1-overexpressing KRAS-mutant CRC cells and tumors. (A and B) ABCB1 expression in KRAS-mutant CRC cell lines from cBioPortal (30) (A) and MDR1 abundance in select KRAS-mutant CRC cell lines (B). (C) Cell viability assessed by CellTiter-Glo in CRC cells treated with increasing doses of MS432 for 5 days, analyzed as % of DMSO control. GI50 value determined with Prism software. (D) Colony formation by CRC cells 14 days after treatment with 1 μM MS432. (E) MEK1/2 protein levels assessed by immunoblot in CRC lines SKCO1 (low MDR1) or LS513 (high MDR1) treated with increasing doses of MS432 for 4 hours. (F) Rhodamine 123 efflux in LS513 cells treated with DMSO, 2 μM tariquidar, or 2 μM lapatinib. (G and H) Immunoblotting analysis in LS513 cells treated with increasing doses of MS432 alone or in combination with tariquidar (0.1 μM) or lapatinib (5 μM) for 24 hours. DC50 value for MEK1 levels determined with Prism. (I) Immunoblotting in LS513 cells treated with DMSO, PD0325901 (0.01 μM), lapatinib (5 μM), or the combination for 48 hours. (J and K) Immunoblotting in LS513 cells treated either with DMSO, MS432 (1 μM), tariquidar (0.1 μM) (J), or lapatinib (5 μM) (K), alone or in combination. (L) Bliss synergy scores determined from cell viability assays (CellTiter-Glo) in LS513 cells treated with increasing concentrations of MS432, lapatinib, or the combination. (M and N) Colony formation by LS513 cells (M) and others (N) treated with DMSO, lapatinib (2 μM), MS432 (1 μM), or the combination for 14 days. (O and P) Immunoblotting in LS513 cells treated with increasing doses of MS934 alone (O) or combined with lapatinib (5 μM) (P) for 24 hours. (Q and R) Tumor volume of LS513 xenografts (Q) and the body weights of the tumor-bearing nude mice (R) treated with vehicle, MS934 (50 mg/kg), lapatinib (100 mg/kg), or the combination. n = 5 mice per treatment group. In (A) to (R), blots and images are representative of three independent experiments, and quantified data are means ± SD [SEM in (Q) and (R)] of three independent experiments; ***P ≤ 0.001 by Student’s t test.
Fig. 7. Lapatinib treatment improves KRASG12C degrader therapies in MDR1-overexpressing CRC cell lines. (A and B) Colony formation by SW1463 (A) or SW837 (B) cells treated with DMSO, LC-2 (1 μM), or MRTX849 (1 μM) for 14 days. Images representative of three independent assays. (C to E) Immunoblotting in SW1463 cells (C and D) and SW837 cells (E) treated with DMSO, LC-2 (1 μM), tariquidar (0.1 μM) (C), or lapatinib (5 μM) (D and E) alone or in combination for 48 hours. Blots are representative of three independent experiments. (F and G) Bliss synergy scores based on CellTiter-Glo assay for the cell viability of SW1463 (F) or SW837 (G) cells treated with increasing concentrations of LC-2, lapatinib, or the combination. Data are means of three experiments ± SD. (H and I) Colony formation of SW1463 (H) or SW837 (I) cells treated as indicated (−, DMSO; LC-2, 1 μM; lapatinib, 2 μM; tariquidar, 0.1 μM) for 14 days. Images representative of three independent assays. (J) Rationale for combining lapatinib with MEK1/2 or KRASG12C degraders in MDR1-overexpressing CRC cell lines. Simultaneous blockade of MDR1 and ErbB receptor signaling overcomes degrader resistance and ErbB receptor kinome reprogramming, resulting in sustained inhibition of KRAS effector signaling.
The UK Biobank (UKBB) this week unveiled to scientists the entire genomes of 200,000 people who are part of a long-term British health study.
The trove of genomes, each linked to anonymized medical information, will allow biomedical scientists to scour the full 3 billion base pairs of human DNA for insights into the interplay of genes and health that could not be gleaned from partial sequences or scans of genome markers. “It is thrilling to see the release of this long-awaited resource,” says Stephen Glatt, a psychiatric geneticist at the State University of New York Upstate Medical University.
Other biobanks have also begun to compile vast numbers of whole genomes, 100,000 or more in some cases (see table, below). But UKBB stands out because it offers easy access to the genomic information, according to some of the more than 20,000 researchers in 90 countries who have signed up to use the data. “In terms of availability and data quality, [UKBB] surpasses all others,” says physician and statistician Omar Yaxmehen Bello-Chavolla of the National Institute for Geriatrics in Mexico City.
Enabling your vision to improve public health
Data drives discovery. We have curated a uniquely powerful biomedical database that can be accessed globally for public health research. Explore data from half a million UK Biobank participants to enable new discoveries to improve public health.
This UKBB biobank represents genomes collected from 500,000 middle-age and elderly participants for 2006 to 2010. The genomes are mostly of a European descent. Other large scale genome sequencing ventures like Iceland’s DECODE, which collected over 100,000 genomes, is now a subsidiary of Amgen, and mostly behind IP protection, not Open Access as this database represents.
UK Biobank is a large-scale biomedical database and research resource, containing in-depth genetic and health information from half a million UK participants. The database is regularly augmented with additional data and is globally accessible to approved researchers undertaking vital research into the most common and life-threatening diseases. It is a major contributor to the advancement of modern medicine and treatment and has enabled several scientific discoveries that improve human health.
A summary of some large scale genome sequencing projects are show in the table below:
Biobank
Completed Whole Genomes
Release Information
UK Biobank
200,000
300,000 more in early 2023
TransOmics for Precision Medicien
161,000
NIH requires project specific request
Million Veterans Program
125,000
Non-Veterans Affairs researchers get first access
100,000 Genomes Project
120,000
Researchers must join Genomics England collaboration
All of Us
90,000
NIH expects to release 2022
Other Related Articles on Genome Biobank Projects in this Open Access Online Scientific Journal Include the Following:
Novartis uses a ‘dimmer switch’ medication to fine-tune gene therapy candidates
Reporter: Amandeep Kaur, BSc., MSc.
Using viral vectors, lipid nanoparticles, and other technologies, significant progress has been achieved in refining the delivery of gene treatments. However, modifications to the cargo itself are still needed to increase safety and efficacy by better controlling gene expression.
To that end, researchers at Children’s Hospital of Philadelphia (CHOP) have created a “dimmer switch” system that employs Novartis’ investigational Huntington’s disease medicine branaplam (LMI070) as a regulator to fine-tune the quantity of proteins generated from a gene therapy.
The investigational medicine branaplam was shown to fine-tune the expression of an erythropoietin gene therapy in mice by scientists from Children’s Hospital of Philadelphia and Novartis. (Novartis)
According to a new study published in Nature, the Xon system altered quantities of erythropoietin—which is used to treat anaemia associated with chronic renal disease—delivered to mice using viral vectors. The method has previously been licenced by Novartis, the maker of the Zolgensma gene therapy for spinal muscular atrophy.
The Xon system depends on a process known as “alternative splicing,” in which RNA is spliced to include or exclude specific exons of a gene, allowing the gene to code for multiple proteins. The team used branaplam, a small-molecule RNA-splicing modulator, for this platform. The medication was created to improve SMN2 gene splicing in order to cure spinal muscular atrophy. Novartis shifted its research to try the medication against Huntington’s disease after a trial failure.
A gene therapy’s payload remains dormant until oral branaplam is given, according to Xon. The medicine activates the expression of the therapy’s functional gene by causing it to splice in the desired way. Scientists from CHOP and the Novartis Institutes for BioMedical Research put the dimmer switch to the exam in an Epo gene therapy carried through adeno-associated viral vectors. The usage of branaplam increased mice Epo levels in the blood and hematocrit levels (the proportion of red blood cells to whole blood) by 60% to 70%, according to the researchers. The researchers fed the rodents branaplam again as their hematocrit decreased to baseline levels. The therapy reinduced Epo to levels similar to those seen in the initial studies, according to the researchers.
The researchers also demonstrated that the Xon system could be used to regulate progranulin expression, which is utilised to treat PGRN-deficient frontotemporal dementia and neuronal ceroid lipofuscinosis. The scientists emphasised that gene therapy requires a small treatment window to be both safe and effective.
In a statement, Beverly Davidson, Ph.D., the study’s senior author,said, “The dose of a medicine can define how high you want expression to be, and then the system can automatically ‘dim down’ at a pace corresponding to the half-life of the protein.”
“We may imagine scenarios in which a medication is used only once, such as to control the expression of foreign proteins required for gene editing, or only on a limited basis. Because the splicing modulators we examined are administered orally, compliance to control protein expression from viral vectors including Xon-based cassettes should be high.”
In gene-modifying medicines, scientists have tried a variety of approaches to alter gene expression. For example, methyl groups were utilised as a switch to turn on or off expression of genes in the gene-editing system CRISPR by a team of researchers from the Massachusetts Institute of Technology and the University of California, San Francisco.
Auxolytic, a biotech company founded by Stanford University academics, has described how knocking down a gene called UMPS could render T-cell therapies ineffective by depriving T cells of the nutrition uridine. Xon could also be tailored to work with cancer CAR-T cell therapy, according to the CHOP-Novartis researchers. The dimmer switch could help prevent cell depletion by halting CAR expression, according to the researchers. According to the researchers, such a tuneable switch could help CRISPR-based treatments by providing “a short burst” of production of CRISPR effector proteins to prevent undesirable off-target editing.