Nonhematologic Cancer Stem Cells [11.2.3]
Writer and Curator: Larry H. Bernstein, MD, FCAP
Nonhematologic Stem Cells
11.2.3.1 C8orf4 negatively regulates self-renewal of liver cancer stem cells via suppression of NOTCH2 signalling
Pingping Zhu, Yanying Wang, Ying Du, Lei He, Guanling Huang, et al.
Nature Communications May 2015; 6(7122). http://dx.doi.org:/10.1038/ncomms8122
Liver cancer stem cells (CSCs) harbor self-renewal and differentiation properties, accounting for chemotherapy resistance and recurrence. However, the molecular mechanisms to sustain liver CSCs remain largely unknown. In this study, based on analysis of several hepatocellular carcinoma (HCC) transcriptome datasets and our experimental data, we find that C8orf4 is weakly expressed in HCC tumors and liver CSCs. C8orf4 attenuates the self-renewal capacity of liver CSCs and tumor propagation. We show that NOTCH2 is activated in liver CSCs. C8orf4 is located in the cytoplasm of HCC tumor cells and associates with the NOTCH2 intracellular domain, which impedes the nuclear translocation of N2ICD. C8orf4 deletion causes the nuclear translocation of N2ICD that triggers the NOTCH2 signaling, which sustains the stemness of liver CSCs. Finally, NOTCH2 activation levels are consistent with clinical severity and prognosis of HCC patients. Altogether, C8orf4 negatively regulates the self-renewal of liver CSCs via suppression of NOTCH2 signaling.
Like stem cells, CSCs are characterized by self-renewal and differentiation simultaneously9. Not surprisingly, CSCs share core regulatory genes and developmental pathways with normal tissue stem cells. Accumulating evidence shows that NOTCH, Hedgehog and Wnt signaling pathways are implicated in the regulation of CSC self-renewal4. NOTCH signaling modulates many aspects of metazoan development and tissue stemness10, 11. NOTCH receptors contain four members (NOTCH1–4) in mammals, which are activated by engagement with various ligands. The aberrant NOTCH signaling was first reported to be involved in the tumorigenesis of human T-cell leukaemia12, 13. Recently, a number of studies have reported that the NOTCH signaling pathway is implicated in regulating self-renewal of breast stem cells and mammary CSCs14, 15. However, how the NOTCH signaling regulates the liver CSC self-renewal remains largely unknown.
C8orf4, also called thyroid cancer 1 (TC1), was originally cloned from a papillary thyroid carcinoma and its surrounding normal thyroid tissue16. C8orf4 is ubiquitously expressed across a wide range of vertebrates with the sequence conservation across species. A number of studies have reported that C8orf4 is highly expressed in several tumors and implicated in tumorigenesis17, 18, 19. In addition, C8orf4 augments Wnt/β-catenin signaling in some cancer cells20, 21, suggesting it may be involved in the regulation of self-renewal of CSCs. However, the biological function of C8orf4 in the modulation of liver CSC self-renewal is still unknown. Here we show that C8orf4 is weakly expressed in HCC and liver CSCs. NOTCH2 signaling is highly activated in HCC tumors and liver CSCs. C8orf4 negatively regulates the self-renewal of liver CSCs via suppression of NOTCH2 signaling.
C8orf4 is weakly expressed in HCC tissues and liver CSCs
To search for driver genes in the oncogenesis of HCC, we performed genome-wide analyses using several online-available HCC transcriptome datasets by R language and Bioconductor approaches. After analysing gene expression profiles of HCC tumor and peri-tumor tissues, we identified >360 differentially expressed genes from both Park’s cohort (GSE36376; ref. 22) and Wang’s cohort (GSE14520; refs 23, 24). Of these changed genes, we focused on C8orf4, which was weakly expressed in HCC tumors derived from both Park’s cohort (GSE36376) and Wang’s cohort (GSE14520) (Fig. 1a). Lower expression of C8orf4 was further confirmed in HCC samples by quantitative reverse transcription–PCR (qRT–PCR) and immunoblotting (Fig. 1b,c). In this study, HCC patient samples we used included all subtypes of HCC. In addition, these observations were further validated by immunohistochemical (IHC) staining (Fig. 1d). These data indicate that C8orf4 is weakly expressed in HCC tumor tissues.

C8orf4 is weakly expressed in HCC tumours and liver CSCs
Figure 1. C8orf4 is weakly expressed in HCC tumours and liver CSCs
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f1.jpg
(a)C8orf4 is weakly expressed in HCC patients. Using R language and Bioconductor methods, we analyzed C8orf4 expression in HCC tumor and peri-tumor tissues provided by Park’s cohort (GSE36376) and Wang’s cohort (GSE14520) datasets. (b,c) C8orf4 expression levels were verified in HCC patient samples by quantitative RT–PCR (qRT–PCR) (b) and immunoblotting (c). β-actin served as a loading control. 18S: 18S rRNA. (d) HCC samples were assayed by immunohistochemical staining. Scale bar—left: 50 μm; right: 20 μm. (e) C8orf4 is weakly expressed in CD13+CD133+ cells sorted from Huh7 cells and primary HCC samples. C8orf4 messenger RNA (mRNA) was measured by qRT–PCR. Six HCC samples got similar results. (f) C8orf4 is much more weakly expressed in oncospheres than non-sphere tumor cells. Non-sphere: Huh7 or HCC primary cells that failed to form spheres. (g) HCC sample tissues were co-stained with anti-C8orf4 and anti-CD13 or anti-CD133 antibodies, then counterstained with DAPI for confocal microscopy. White arrows indicate CD13+ or CD133+ cells. Scale bars: 20 μm. For a,b, data are shown as box and whisker plot. Boxes represent interquartile range (IQR); upper and lower edge corresponds to the 75th and 25th percentiles, respectively. Horizontal lines within boxes represent median levels of gene intensity. Whiskers below and above boxes extend to the 5th and 95th percentiles, respectively. For e and f, Student’s t-test was used for statistical analysis, *P<0.05;**P<0.01, data are shown as mean ± standard deviation. Data are representative of at least three independent experiments. P, peri-tumor; T, tumor.
Notably, C8orf4 was also weakly expressed in embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs) by analysis of its expression profiles derived from online datasets (GSE14897; ref. 25 and GSE25417; ref. 26) (Supplementary Fig. 1a,b). C8orf4 was also lowly expressed in normal liver stem cells (Supplementary Fig. 1c,d), suggesting that C8orf4 may be involved in the regulation of self-renewal of liver stem cells. Thus, we propose that C8orf4 might play a role in the maintenance of liver CSCs. Since CD13 and CD133 were widely used as liver CSC surface markers, we sorted CD13+CD133+ cells from Huh7 and Hep3B HCC cell lines as well as HCC samples, serving as liver CSCs. We observed that C8orf4 was weakly expressed in liver CSCs enriched from both HCC cell lines and patient samples (Fig. 1e). Six HCC samples were analyzed for these experiments. Similar results were obtained in CD13+CD133+ cells from Hep3B cells. Furthermore, we performed sphere formation experiments using Huh7 cells and HCC primary sample cells, and detected expression levels of C8orf4. We observed that C8orf4 was dramatically reduced in the oncospheres generated by both HCC cell lines and patient samples (Fig. 1f). In addition, we noticed that C8orf4 expression was negatively correlated with liver CSC markers such as CD13 and CD133 in HCC samples (Fig. 1g), suggesting lower expression of C8orf4 in liver CSCs. Moreover, C8orf4 was mainly located in the cytoplasm of tumour cells. Altogether, C8orf4 is weakly expressed in HCC tumor tissues and liver CSCs.
C8orf4 negatively regulates self-renewal of liver CSCs
We then wanted to look at whether C8orf4 plays a critical role in the self-renewal maintenance of liver CSCs. C8orf4 was knocked out in Huh7 cells through a CRISPR/Cas9 system (Fig. 2a). TwoC8orf4-knockout (KO) cell strains were established and C8orf4 was completely deleted in these two strains. C8orf4 deletion dramatically enhanced oncosphere formation (Fig. 2b). We co-stained SOX9, a widely used progenitor marker, and Ki67, a well-known proliferation marker, in C8orf4 KO sphere cells. We found that SOX9 was strongly stained in C8orf4 KO sphere cells (Supplementary Fig. 2a). In contrast, Ki67 staining was not significantly altered in C8orf4 KO sphere cells versus WT sphere cells. We also digested sphere cells and examined the SOX9 and Ki67 expression by flow cytometry. Similar results were achieved (Supplementary Fig. 2b). Importantly, through serial passage of CSC sphere cells, similar observations were obtained in the fourth generation oncosphere assay (Supplementary Fig. 2c,d). These data suggest that C8orf4 is involved in the regulation of liver CSC self-renewal.
(not shown)
Figure 2: C8orf4 knockout enhances self-renewal of liver CSCs.
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f2.jpg
- C8orf4-deficient Huh7 cells were established using a CRISPR/Cas9 system. T7 endonuclease I cleavage confirmed the efficiency of sgRNA (left panel, white arrowheads), and C8orf4-knockout efficiency was confirmed by western blot (right panel). Two knockout cell lines were used. C8KO#1:C8orf4KO#1; C8KO#2: C8orf4KO#2. (b) C8orf4-deficient cells enhanced sphere formation activity. Calculated ratios are shown in the right panel. (c) C8orf4-deficient or WT Huh7 cells (1 × 106) were injected into BALB/c nude mice. Tumor sizes were observed every 5 days. (d) C8orf4 deficiency enhances tumor-initiating capacity. Diluted cell numbers of Huh7 cells were implanted into BALB/c nude mice for tumor initiation. Percentages of tumor-formation mice were calculated (left panel), and frequency of tumor-initiating cells was calculated using extreme limiting dilution analysis (right panel). Error bars represent the 95% confidence intervals of the estimation. (e) Expression levels of CD13 andCD133 were analyzed in C8orf4-knockout Huh7 cells. (f) C8orf4 was silenced in HCC primary cells and C8orf4 depletion enhanced sphere formation activity. Calculated ratios are shown at the right panel. Three HCC specimens obtained similar results. (g) C8orf4-overexpressing Huh7 cells were established (left panel). C8orf4-overexpressing Huh7 cells and control Huh7 cells were cultured for sphere formation. (h,i) Xenograft tumor growth (h) and frequency of tumor-initiating cells (i) for C8orf4-overexpressing Huh7 cells were analyzed as c,d. (j) C8orf4 overexpression reduces expression of CD133 and CD13 in Huh7 cells. (k) C8orf4 was transfected in HCC primary cells and cultured for sphere formation. Three HCC patient samples obtained similar results. Scale bars: b,f,g,k, 500 μm. Student’s t-test was used for statistical analysis, *P<0.05; **P<0.01; ***P<0.001, data are shown as mean ± standard deviation. Data represent at least three independent experiments. oeC8orf4, overexpression of C8orf4; oeVec, overexpression vector.
In addition, C8orf4-deficient Huh7 cells overtly increased xenograft tumour growth (Fig. 2c). We then performed sphere formation and digested oncospheres formed by C8orf4-deficient or WT cells into single-cell suspension, then subcutaneously implanted 1 × 104, 1 × 103, 1 × 102 and 10 cells into BALB/c nude mice. Tumour formation was examined for tumour-initiating capacity at the third month. C8orf4 deficiency remarkably enhanced tumour-initiating capacity and liver CSC ratios (Fig. 2d). In addition, C8orf4 deletion significantly enhanced expression levels of the liver CSC markers such as CD13 and CD133 (Fig. 2e). We also silenced C8orf4 in HCC primary cells using a lentivirus infection system and established C8orf4-silenced cells. Two pairs of short hairpin RNA (shRNA) sequences obtained similar knockdown efficiency. C8orf4 knockdown remarkably promoted sphere formation and xenograft tumour growth (Fig. 2f and Supplementary Fig. 2e). These data indicate that C8orf4 deletion potentiates the self-renewal of liver CSCs.
We next overexpressed C8orf4 in Huh7 cells and HCC primary cells using lentivirus infection. We observed that C8orf4 overexpression in Huh7 cells remarkably reduced sphere formation and xenograft tumour growth (Fig. 2g,h). In addition, C8orf4 overexpression remarkably reduced tumour-initiating capacity and expression of liver CSC markers (Fig. 2i,j). Similar results were observed by C8orf4 overexpression in HCC primary cells (Fig. 2k). We tested three HCC samples with similar results. Overall, C8orf4 negatively regulates the maintenance of liver CSC self-renewal and tumour propagation.
C8orf4 suppresses NOTCH2 signaling in liver CSCs
To further determine the underlying mechanism of C8orf4 in the regulation of liver CSCs, we analyzed three major self-renewal signaling pathways, including Wnt/β-catenin, Hedgehog and NOTCH pathways, in C8orf4-deleted Huh7 cells and HCC primary cells. We found that only NOTCH target genes were remarkably upregulated in C8orf4-deficient cells (Fig. 3a), whereasC8orf4 deficiency did not significantly affect the Wnt/β-catenin or the Hedgehog pathway. Given that the NOTCH family receptors have four members, we wanted to determine which NOTCH member was involved in the C8orf4-mediated suppression of liver CSC stemness. We noticed that only NOTCH2 was highly expressed in both Huh7 cells and HCC samples (Fig. 3b). In addition, this result was also confirmed by analysis of NOTCH expression levels derived from Wang’s cohort (GSE14520) and Petel’s cohort (E-TABM-36; ref. 27) (Fig. 3c). Moreover, we analysed expression profiles of C8orf4 and NOTCH target genes using Park’s cohort (GSE36376) and Wurmbach’s cohort (GSE6764; ref. 28). These cohort datasets provided several Notch signaling and its target genes. HEY1, NRARP and HES6 genes were highly expressed in HCC tumour tissues (GSE6764; ref. 28), which were further confirmed in HCC samples by real-time PCR (Supplementary Fig. 3a,b). Furthermore, HEY1, NRARP and HES6 genes have been reported to be relatively specific NOTCH target genes. We then examined these three genes as the NOTCH2 target genes throughout this study. We found that the C8orf4 expression level was negatively correlated with the expression levels of HEY1 and HES6, suggesting that C8orf4 inhibited NOTCH signaling in HCC patients (Fig. 3d). Finally these results were further confirmed in HCC samples by qRT-PCR (Fig. 3e). To further explore the activation status of NOTCH2 signaling in liver CSCs, we examined the expression levels of NOTCH downstream target genes in oncospheres and CD13+CD133+ cells derived from both Huh7 cells and HCC cells. We observed that NOTCH target genes were highly expressed in liver CSCs (Fig. 3f,g). These observations were verified by immunoblotting (Fig. 3h). In addition, the expression levels of NRARP, HES6 and HEY1 were positively related to the expression levels of EpCAM and CD133 derived from Zhang’s cohort (GSE25097; ref. 29) and Wang’s cohort (GSE14520; Supplementary Fig. 3c,d). These data suggest that the NOTCH2 signaling plays a critical role in the maintenance of self-renewal of liver CSCs.
(not shown)
Figure 3: C8orf4 suppresses NOTCH2 signaling in liver CSCs.
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f3.jpg
(a) C8orf4 deficiency or depletion activates NOTCH signaling. The indicated major stemness signalling pathways were analysed in C8orf4-knockout Huh7 cells (left panel) and C8orf4-silenced primary cells of HCC samples (right panel). (b) Four receptor members of NOTCH family were examined in both Huh7 cells (left panel) and 29 pairs of HCC samples (right panel). (c) NOTCH receptors were analyzed from Wang’s cohort (left panel) and Petel’s cohort (right panel) datasets. (d) HEY1 and HES6 were highly expressed in C8orf4low samples by analysis of Park’s cohort (upper panel) and Wurmbach’s cohort (lower panel). (e) Expression levels of HEY1 and HES6 along with C8orf4 were analysed in HCC samples by qRT–PCR. (f,g) Expression levels of NRARP, HEY1 and HES6 in spheres generated by Huh7 cells and HCC primary cells (f) and in CD13+CD133+ cells sorted from Huh7 cells and HCC primary cells (g). Non-sphere: Huh7 cells or HCC cells that failed to form spheres. (h) HEY1, HES6 and NRARP expression in sphere and non-sphere cells was detected by immunoblotting. β-actin was used as a loading control. For c,d, data are shown as box and whisker plot. Box: interquartile range (IQR); horizontal line within box: median; whiskers: 5–95 percentile. For a,b,f,g, Student’s t-test was used for statistical analysis, *P<0.05;**P<0.01; ***P<0.001, data are shown as mean ± standard deviation. Data are representative of at least three independent experiments.
C8orf4 interacts with NOTCH2 that is critical for liver CSCs
On ligand–receptor binding, the NOTCH receptor experiences a proteolytic cleavage by metalloprotease and γ-secretase, releasing a NOTCH extracellular domain (NECD) and a NOTCH intracellular domain (NICD), respectively30. Then the active NICD undergoes nuclear translocation and activates the expression of NOTCH downstream target genes31.Then we constructed the NOTCH2 extracellular domain (N2ECD) and intracellular domain (N2ICD) and examined the interaction with C8orf4 via a yeast two-hybrid approach. Interestingly, we found that C8orf4 interacted with N2ICD, but not N2ECD (Fig. 4a). The interaction was validated by co-immunoprecipitation (Fig. 4b). Through domain mapping, the ankyrin repeat domain of NOTCH2 was essential and sufficient for its association with C8orf4 (Fig. 4c). Taken together, C8orf4 interacts with the N2ICD domain of NOTCH2.
Figure 4: C8orf4 interacts with NOTCH2 that is required for the self-renewal maintenance of liver CSCs.

C8orf4 interacts with NOTCH2 that is required for the self-renewal maintenance of liver CSCs
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f4.jpg
(a) C8orf4 interacts with N2ICD. Yeast strain AH109 was co-transfected with Gal4 DNA-binding domain (BD) fused C8orf4 and Gal4-activating domain (AD) fused N2ICD. p53 and large T antigen were used as a positive control. (b) Recombinant Flag-N2ICD and GFP–C8orf4 were incubated for co-immunoprecipitation. (c) The ankyrin repeat AR domain is essential and sufficient for the interaction of C8orf4 with N2ICD. Various N2ICD truncation constructs were co-transfected with GFP–C8orf4 for domain mapping. NLS: nuclear location signal. (d) NOTCH2 was knocked down in Huh7 cells and detected by qRT–PCR and immunoblotting. (e) NOTCH2-silenced Huh7 cells were cultured for sphere formation assays. Two pairs of shRNAs against NOTCH2 obtained similar results. (f,g) Xenograft tumor growth (f) and frequency of tumor-initiating cells (g) for NOTCH2-silenced Huh7 cells were analyzed. (h) NOTCH2 was silenced in HCC primary cells and NOTCH2 depletion declined sphere formation activity. Three HCC specimens obtained similar results. (i) Sphere formation capacity was examined in differently treated HCC primary cells. (j) HCC primary cells were treated with indicated lentivirus and implanted into BALB/c nude mice for xenograft tumor growth assays. Scale bars: e,h,i, 500 μm, Student’s t-test was used for statistical analysis, *P<0.05; **P<0.01; ***P<0.001, data are shown as mean ± standard deviation. Data are representative of at least three independent experiments. IB, immunoblotting; IP, immunoprecipitation; NS, not significant.
To further verify the role of NOTCH2 in the maintenance of liver CSC self-renewal, we knocked down NOTCH2 in Huh7 cells and established stably depleted cell lines by two pairs of NOTCH2 shRNAs (Fig. 4d). NOTCH2 knockdown dramatically reduced sphere formation (Fig. 4e), as well as attenuated xenograft tumor growth and tumor-initiating capacity (Fig. 4f,g). Similar observations were achieved in NOTCH2-depleted HCC primary cells (Fig. 4h). In addition, we found that simultaneous knockdown of NOTCH2 and overexpression of C8orf4 failed to reduce sphere formation capacity compared with individual knockdown of NOTCH2 (Fig. 4i), suggesting that NOTCH2 and C8orf4 affected sphere formation through the same pathway. Meanwhile, C8orf4 knockdown failed to rescue the sphere formation ability of NOTCH2-depleted HCC primary cells (Fig. 4i). Similar observations were obtained in Huh7 cells (Supplementary Fig. 4). Finally, NOTCH2 depletion in C8orf4-silenced Huh7 cells or HCC primary cells also abrogated the C8orf4 depletion-mediated enhancement of xenograft tumor growth (Fig. 4j), suggesting that C8orf4 acted as upstream of NOTCH2 signaling. These data suggest that C8orf4 suppresses the liver CSC stemness through inhibiting the NOTCH2 signaling pathway.
C8orf4 blocks nuclear translocation of N2ICD
As shown in Fig. 1g, C8orf4 was mainly localized in the cytoplasm in tumor cells of HCC samples. To confirm these observations, we stained C8orf4 in several HCC cell lines and noticed that C8orf4 also resided in the cytoplasm of Huh7 cells and Hep3B cells (Fig. 5a and Supplementary Fig. 5a). These results were further validated by cellular fractionation (Fig. 5b). Importantly, C8orf4 KO led to nuclear translocation of N2ICD (Fig. 5c). In addition, we also examined the intracellular location of N2ICD in Huh7 spheres. We found that C8orf4 deletion caused complete nuclear translocation of N2ICD in oncosphere cells (Fig. 5d,e), while N2ICD was mainly located in the cytoplasm of WT oncosphere cells. However, we found that C8orf4 KO did not affect subcellular localization of β-catenin (Supplementary Fig. 5b,c). Through luciferase assays, C8orf4 transfection did not significantly influence promoter transcription activity of Wnt target genes such as TCF1, LEF and SOX4 (Supplementary Fig. 5d). These data indicate that C8orf4 resides in the cytoplasm of HCC cells and inhibits nuclear translocation of N2ICD.

C8orf4 deletion causes the nuclear translocation of N2ICD
Figure 5: C8orf4 deletion causes the nuclear translocation of N2ICD.
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f5.jpg
(a) C8orf4 resides in the cytoplasm of Huh7 cells. Huh7 cells were permeabilized and stained with anti-C8orf4 antibody, then counterstained with PI for confocal microscopy. (b) Cellular fractionation was performed and detected by immunoblotting. (c,d) C8orf4 knockout causes the nuclear translocation of N2ICD. C8orf4-deficient Huh7 cells (c) and sphere cells (d) were permeabilized and stained with anti-C8orf4 and anti-N2ICD antibodies, then counterstained with DAPI followed by confocal microscopy. (e) Cellular fractionation was performed in C8orf4-deficient sphere and WT sphere cells followed by immunoblotting. (f) C8orf4-deficient Huh7 cells were implanted into BALB/c nude mice. Xenograft tumors were analyzed by immunohistochemical staining. Red arrowheads denote nuclear translocation of N2ICD. (g) C8orf4-overexpressing Huh7 cells were permeabilized for immunofluorescence staining. (h) Cellular fractionation was performed in C8orf4-overexpressing Huh7 cells for immunoblotting. (i,j) C8orf4 was overexpressed in N2ICD-overexpressing Huh7 cells followed by immunofluorescence staining (i) and immunoblotting (j). (k) NOTCH target genes were measured in cells treated as in i by real-time PCR. Scale bars: a,c,d,g,i, 10 μm; f, 40 μm. Student’s t-test was used for statistical analysis, **P<0.01;***P<0.001, data are shown as mean±s.d.. Data represent at least three independent experiments.
To further determine whether C8orf4 inhibits the NOTCH2 signaling in the propagation of xenograft tumors, we examined the distribution of N2ICD and NOTCH2 target gene activation inC8orf4-deficient xenograft tumor tissues. We found that C8orf4-deficient tumors displayed much more nuclear translocation of N2ICD compared with WT tumors (Fig. 5f). Expectedly, C8orf4-deficient tumors showed elevated expression levels of NOTCH2 target genes such as HEY1, HES6 and NRARP (Supplementary Fig. 5e). Furthermore, C8orf4 overexpression blocked the nuclear translocation of N2ICD (Fig. 5g,h). Consequently, C8orf4-overexpressing tumors showed much less N2ICD nuclear translocation and reduced expression levels of NOTCH2 target genes compared with control tumors (Supplementary Fig. 5f,g). Of note, C8orf4 overexpression in N2ICD-overexpressing Huh7 cells still blocked nuclear translocation of N2ICD (Fig. 5i,j). Consequently, C8orf4 overexpression abolished the activation of Notch2 signaling (Fig. 5k). These results suggest that C8orf4 deletion causes the nuclear translocation of N2ICD leading to activation of NOTCH2 signaling.
NOTCH2 signalling is required for the stemness of liver CSCs
To further verify the role of NRARP and HEY1 in the maintenance of liver CSC self-renewal, we knocked down these two genes in Huh7 cells and established stably depleted cell lines by two pairs of shRNAs. As expected, NRARP knockdown dramatically reduced sphere formation (Fig. 6a,b). NRARP knockdown also attenuated tumor-initiating capacity and liver CSC ratios (Fig. 6c). Similar results were achieved in NRARP-silenced HCC primary cells (Fig. 6d,e). Similarly, HEY1 silencing remarkably reduced sphere formation derived from Huh7 and HCC primary cells (Fig. 6f–i), as well as declined xenograft tumor growth and tumor-initiating capacity (Supplementary Fig. 6a,b). In sum, NOTCH2 signaling is required for the maintenance of liver CSC self-renewal.
(not shown)
Figure 6: Depletion of NRARP and HEY1 impairs stemness of liver CSCs.
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f6.jpg
(a,b) NRARP-silenced Huh7 cells were established (a) and showed reduced sphere formation capacity (b). Two pairs of shRNAs against NRARP obtained similar results. (c) NRARP-silenced Huh7 cells decline tumour-initiating capacity (left panel) and reduce liver CSC frequency (right panel). Error bars represent the 95% confidence intervals of the estimation. (d,e) NRARP was knocked down in HCC primary cells (d) and sphere formation was detected (e). Three HCC samples were tested with similar results. (f,g) HEY1-silenced Huh7 cells were established (f) and sphere formation was assayed (g). Two pairs of shRNAs against HEY1 obtained similar results. (h,i) HEY1 was knocked down in HCC primary cells (h) and HEY1 depletion impaired sphere formation capacity (i). Three HCC samples were tested with similar results. Scale bars: b,e,g,i, 500 μm. For a,b,d–i, Student’s t-test was used for statistical analysis, *P<0.05; **P<0.01; ***P<0.001, data are shown as mean ± standard deviation. Data are representative of at least three independent experiments.
NOTCH2 signaling is correlated with HCC severity
As shown above, the NOTCH2 signaling was highly activated in liver CSCs and involved in the regulation of liver CSC stemness. We further examined the relationship of NOTCH2 signaling with the progression of HCC. First, we analyzed NOTCH2 activation levels in HCC tumor tissues and peri-tumor tissues derived from Park’s cohort (GSE36376). We observed that HEY1, HES6 and NRARP were highly expressed in the tumor tissues of HCC patients (Fig. 7a). Consistently, high expression levels of HEY1, HES6 and NRARP in HCC tumors were validated by Zhang’s cohort (GSE25097) (Fig. 7b). Importantly, high expression of these three genes was confirmed in HCC samples through quantitative RT–PCR (Fig. 7c), as well as immunoblotting (Fig. 7d). To confirm a causative link between low C8orf4 expression level and nuclear N2ICD, we examined 93 HCC samples (31 peri-tumor, 37 early stage of HCC patients and 25 advanced stage of HCC patients) with immunohistochemistry staining. We observed that nuclear staining of N2ICD appeared in ~10% tumor cells in the majority of early HCC patients we tested (Fig. 7e,f). In advanced HCC patients, nuclear staining of N2ICD in tumor cells increased to ~30% in almost all the advanced HCC patients we examined. Consequently, HEY1 staining existed in ~10% tumor cells with scattered distribution and increased to 30% tumor cells in the advanced HCC patients (Fig. 7e). Consistently, low expression of C8orf4 was well correlated with activation of NOTCH2 signaling (Fig. 7e,f).

NOTCH2 activation levels are consistent with clinical severity and prognosis of HCC patients
Figure 7: NOTCH2 activation levels are consistent with clinical severity and prognosis of HCC patients.
http://www.nature.com/ncomms/2015/150519/ncomms8122/images_article/ncomms8122-f7.jpg
(a,b) NOTCH target genes were highly expressed in HCC tumour tissues derived from Park’s cohort (a) and Zhang’s cohort (b). (c) High expression levels of NOTCH target genes in HCC tumor tissues were verified by qRT–PCR. (d) HEY1 expression in HCC tumor tissues was detected by western blot. (e) IHC staining for N2ICD, C8orf4 and HEY1. These images represent 93 HCC samples. Scale bars, 50 μm. (f) IHC images were calculated using Image-Pro Plus 6. (g) Expression levels of NOTCH target genes were elevated in HCC tumors and advanced HCC patients derived from Wang’s cohort. (h) HEY1 expression level was positively correlated with prognosis prediction of HCC patients analyzed by Petel’s cohort and Wang’s cohort. HCC samples were divided into two groups according to HEY1 expression levels followed by Kaplan–Meier survival analysis. For a–c, data are shown as box and whisker plot, Box: interquartile range (IQR); horizontal line within box: median; whiskers: 5–95 percentile. For f,g, Student’s t-test was used for statistical analysis, *P<0.05; **P<0.01; ***P<0.001; data are shown as mean ± standard deviation. Experiments were repeated at least three times. aHCC, advanced HCC; CL, cirrhosis liver; eHCC, early HCC; IL, inflammatory liver; NL, normal liver; NS, not significant.
Serial passages of colonies or sphere formation in vitro, as well as transplantation of tumor cells, are frequently used to assess the long-term self-renewal capacities of CSCs32. We used HCC primary cells for serial passage growth in vitro and tested the expression levels of C8orf4, HEY1 and SOX9. We found that C8orf4 expression was gradually reduced over serial passages in oncosphere cells (Supplementary Fig. 7a). Consequently, the expression of NOTCH2 targets such as HEY1 and SOX9 was gradually increased in oncosphere cells during serial passages (Supplementary Fig. 7b). In addition, N2ICD nuclear translocation appeared in oncosphere cells with high expression of HEY1 plus low expression of C8orf4 (termed as C8orf4−/N2ICDnuc/HEY1+cells) (Supplementary Fig. 7c). These data suggest that the C8orf4−/N2ICDnuc/HEY1+ fraction cells represent a subset of liver CSCs.
Through analyzing Wang’s cohort (GSE54238), we noticed that the NOTCH2 activation levels were positively correlated with the development and progression of HCC (Fig. 7g). By contrast, the NOTCH2 pathway was not activated in inflammation liver, cirrhosis liver and normal liver (Fig. 7f). Consistently, similar observations were achieved by analysis of Zhang’s cohort (GSE25097) (Supplementary Fig. 7d). In addition, the NOTCH2 activation levels were consistent with clinicopathological stages of HCC patients derived from Wang’s cohort (GSE14520) (Supplementary Fig. 7e). Finally, HCC patients with higher expression of HEY1 displayed worse prognosis derived from Petel’s cohort (E-TABM-36) and Wang’s cohort (GSE14520) (Fig. 7h). These two cohorts (E-TABM-36 and GSE14520) have survival information of HCC patients. Taken together, the NOTCH2 activation levels in tumor tissues are consistent with clinical severity and prognosis of HCC patients.
Discussion
CSC have been identified in many solid tumors, including breast, lung, brain, liver, colon, prostate and bladder cancers4, 6, 33. CSCs have similar characteristics associated with normal tissue stem cells, including self-renewal, differentiation and the ability to form new tumors. CSCs may be responsible for cancer relapse and metastasis due to their invasive and drug-resistant capacities34. Thus, targeting CSCs may become a promising therapeutic strategy to deadly malignancies35, 36. However, it remains largely unknown about hepatic CSC biology. In this study, we used CD13 and CD133 to enrich CD13+CD133+
subpopulation cells as liver CSCs. Based on analysis of several online-available HCC transcriptome datasets, we found that C8orf4 is weakly expressed in HCC tumors as well as in CD13+CD133+ liver CSCs. NOTCH2 signaling is required for the maintenance of liver CSC self-renewal. C8orf4 resides in the cytoplasm of tumor cells and interacts with N2ICD, blocking the nuclear translocation of N2ICD. Lower expression of C8orf4 causes nuclear translocation of N2ICD that activates NOTCH2 signaling in liver CSCs. NOTCH2 activation levels are consistent with clinical severity and prognosis of HCC patients. Therefore, C8orf4 negatively regulates self-renewal of liver CSCs via suppression of NOTCH2 signaling.
Elucidating signaling pathways that maintains self-renewal of liver CSCs is pivotal for the understanding of hepatic CSC biology and the development of novel therapies against HCC. Several signaling pathways, such as Wnt/β-catenin, transforming growth factor-beta, AKT and STAT3 pathways, have been defined to be implicated in the regulation of liver CSCs37. Not surprisingly, some liver CSC subsets and normal tissue stem cells may share core regulatory genes and common signaling pathways. The NOTCH signaling pathway plays an important role in development via cell-fate determination, proliferation and cell survival38, 39. The NOTCH family receptors contain four members in mammals (NOTCH1–4), which are activated by binding to their corresponding ligands. A large body of evidence provides that NOTCH signaling is implicated in carcinogenesis40. However, the role of NOTCH signaling in liver cancer is controversial. A previous study reported that NOTCH1 signaling suppresses tumor growth of HCC41. Recently, several reports showed that NOTCH signaling enhances liver tumor initiation42, 43, 44. Importantly, a recent study showed that various NOTCH receptors have differential functions in the development of liver cancer45. Here we demonstrate that NOTCH2 signaling is activated in HCC tumor tissues and liver CSCs, which is required for the maintenance of liver CSC self-renewal.
C8orf4, also known as TC1, was originally cloned from a papillary thyroid cancer16, 46. The copy number variations of C8orf4 are associated with acute myeloid leukemia and other hematological malignancies19, 47. C8orf4 has been reported to be implicated in various cancers. C8orf4 was highly expressed in thyroid cancer, gastric cancer and breast cancer16, 20, 46. C8orf4 has been reported to enhance Wnt/β-catenin signaling in cancer cells that is associated with poor prognosis20, 21. However, C8orf4 is downregulated in colon cancer48. In this study, we show that C8orf4 is weakly expressed in HCC tumor tissues and liver CSCs. Our observations were confirmed by two HCC cohort datasets. Importantly, C8orf4 negatively regulates the NOTCH2 signaling to suppress the self-renewal of liver CSCs. Therefore, C8orf4 may exert distinct functions in the regulation of various malignancies.
NOTCH receptors consist of noncovalently bound extracellular and transmembrane domains. Once binding with membrane-bound Delta or Jagged ligands, the NOTCH receptors undergoes a proteolytic step by metalloprotease and γ-secretase, generating NECD and NICD fragments11, 31. The NICD, a soluble fragment, is released in the cytoplasm on proteolysis. Then the NICD translocates to the nucleus and binds to the transcription initiation complex, leading to activation of NOTCH-associated target genes49. However, it is largely unclear how the NICD is regulated during NOTCH signaling activation. Here we show that N2ICD binds to C8orf4 in the cytoplasm of liver non-CSC tumor cells, which impedes the nuclear translocation of N2ICD. By contrast, in liver CSCs, lower expression of C8orf4 causes the nuclear translocation of N2ICD, leading to activation of NOTCH signaling.
CSCs or tumour-initiating cells, behave like tissue stem cells in that they are capable of self-renewal and of giving rise to hierarchical organization of heterogeneous cancer cells4. Thus, CSCs harbour the stem cell properties of self-renewal and differentiation. Actually, the CSC model cannot account for tumorigenesis in all tumours. CSCs could undergo genetic evolution, and the non-CSCs might switch to CSC-like cells4. These results highlight the dynamic nature of CSCs, suggesting that the clonal evolution and CSC models can act in concert for tumorigenesis. Furthermore, low C8orf4 expression in tumor cells results in overall Notch2 activation, which then may have more of a progenitor signature and be more aggressive. These cells would likely have a growth advantage in non-adherent conditions and express many of the stemness markers. The dynamic nature of CSCs or persistent NOTCH2 activation may contribute to the high number of C8orf4−/N2ICDnuc/HEY1+ cells in advanced HCC tumors and correlation in the patient cohort.
A recent study showed that NOTCH2 and its ligand Jag1 are highly expressed in human HCC tumors, suggesting activation of NOTCH2 signaling in HCC45. In addition, inhibiting NOTCH2 or Jag1 dramatically reduces tumor burden and growth. However, suppression of NOTCH3 has no effect on tumor growth. Dill et al.43 reported that Notch2 is an oncogene in HCC. Notch2-driven HCC are poorly differentiated with a high expression level of the progenitor marker Sox9, indicating a critical role of Notch2 signaling in liver CSCs. Here we found that NOTCH2 and its target genes such as NRARP, HEY1 and HES6 are highly expressed in HCC samples. In addition, depletion of NRARP and HEY1 impairs the stemness maintenance of liver CSCs and tumor propagation. Moreover, the expression levels of NRARP, HEY1 and HES6 in tumors are positively correlated with clinical severity and prognosis of HCC patients. Finally, the NOTCH2 activation status is positively related to the clinicopathological stages of HCC patients. Altogether, C8orf4 and NOTCH2 signaling can be detected for the diagnosis and prognosis prediction of HCC patients, as well as used as targets for eradicating liver CSCs for future therapy.
11.2.3.2 Quantifying the Landscape for Development and Cancer from a Core Cancer Stem Cell Circuit
The authors developed a landscape and path theoretical framework to investigate the global natures and dynamics for a core cancer stem cell gene network. The landscape exhibits four basins of attraction, representing cancer stem cell, stem cell, cancer and normal cell states. They also uncovered certain key genes and regulations responsible for determining the switching between different states. [Cancer Res]
Chunhe Li and Jin Wang
Cancer Res May 13, 2015; 75(10).
http://dx.doi.org:/10.1158/0008-5472.CAN-15-0079
Cancer presents a serious threat to human health. The understanding of the cell fate determination during development and tumor genesis remains challenging in current cancer biology. It was suggested that cancer stem cell (CSC) may arise from normal stem cells, or be transformed from normal differentiated cells. This gives hints on the connection between cancer and development. However, the molecular mechanisms of these cell type transitions and the CSC formation remain elusive. We quantified landscape, dominant paths and switching rates between cell types from a core gene regulatory network for cancer and development. Stem cell, CSC, cancer, and normal cell types emerge as basins of attraction on associated landscape. The dominant paths quantify the transition processes among CSC, stem cell, normal cell and cancer cell attractors. Transition actions of the dominant paths are shown to be closely related to switching rates between cell types, but not always to the barriers in between, due to the presence of the curl flux. During the process of P53 gene activation, landscape topography changes gradually from a CSC attractor to a normal cell attractor. This confirms the roles of P53 of preventing the formation of CSC, through suppressing self-renewal and inducing differentiation. By global sensitivity analysis according to landscape topography and action, we identified key regulations determining cell type switchings and suggested testable predictions. From landscape view, the emergence of the CSCs and the associated switching to other cell types are the results of underlying interactions among cancer and developmental marker genes. This indicates that the cancer and development are intimately connected. This landscape and flux theoretical framework provides a quantitative way to understand the underlying mechanisms of CSC formation and interplay between cancer and development. Major Findings: We developed a landscape and path theoretical framework to investigate the global natures and dynamics for a core cancer stem cell gene network. Landscape exhibits four basins of attraction, representing CSC, stem cell, cancer and normal cell states. We quantified the kinetic rate and paths between different attractor states. We uncovered certain key genes and regulations responsible for determining the switching between different states.
11.2.3.3 IMP3 Promotes Stem-Like Properties in Triple-Negative Breast Cancer by Regulating SLUG
Scientists observed that insulin-like growth factor-2 mRNA binding protein 3 (IMP3) expression is significantly higher in tumor initiating than in non-tumor initiating breast cancer cells and demonstrated that IMP3 contributes to self-renewal and tumor initiation, properties associated with cancer stem cells. [Oncogene]
S Samanta, H Sun, H L Goel, B Pursell, C Chang, A Khan, et al.
Oncogene , (18 May 2015) |
http://dx.doi.org:/10.1038/onc.2015.164
IMP3 (insulin-like growth factor-2 mRNA binding protein 3) is an oncofetal protein whose expression is prognostic for poor outcome in several cancers. Although IMP3 is expressed preferentially in triple-negative breast cancer (TNBC), its function is poorly understood. We observed that IMP3 expression is significantly higher in tumor initiating than in non-tumor initiating breast cancer cells and we demonstrate that IMP3 contributes to self-renewal and tumor initiation, properties associated with cancer stem cells (CSCs). The mechanism by which IMP3 contributes to this phenotype involves its ability to induce the stem cell factor SOX2. IMP3 does not interact with SOX2 mRNA significantly or regulate SOX2 expression directly. We discovered that IMP3 binds avidly to SNAI2 (SLUG) mRNA and regulates its expression by binding to the 5′ UTR. This finding is significant because SLUG has been implicated in breast CSCs and TNBC. Moreover, we show that SOX2 is a transcriptional target of SLUG. These data establish a novel mechanism of breast tumor initiation involving IMP3 and they provide a rationale for its association with aggressive disease and poor outcome.
11.2.3.4 Type II Transglutaminase Stimulates Epidermal Cancer Stem Cell Epithelial-Mesenchymal Transition
Researchers investigated the role of type II transglutaminase (TG2) in regulating epithelial mesenchymal transition (EMT) in epidermal cancer stem cells. They showed that TG2 knockdown or treatment with TG2 inhibitor, resulted in a reduced EMT marker expression, and reduced cell migration and invasion. [Oncotarget]
ML Fisher, G Adhikary, W Xu, C Kerr, JW Keillor, RL Ecker
Oncotarget May 08, 2015;
Type II transglutaminase (TG2) is a multifunctional protein that has recently been implicated as having a role in ECS cell survival. In the present study we investigate the role of TG2 in regulating epithelial mesenchymal transition (EMT) in ECS cells. Our studies show that TG2 knockdown or treatment with TG2 inhibitor, results in a reduced EMT marker expression, and reduced cell migration and invasion. TG2 has several activities, but the most prominent are its transamidase and GTP binding activity. Analysis of a series of TG2 mutants reveals that TG2 GTP binding activity, but not the transamidase activity, is required for expression of EMT markers (Twist, Snail, Slug, vimentin, fibronectin, N-cadherin and HIF-1α), and increased ECS cell invasion and migration. This coupled with reduced expression of E-cadherin. Additional studies indicate that NFϰB signaling, which has been implicated as mediating TG2 impact on EMT in breast cancer cells, is not involved in TG2 regulation of EMT in skin cancer. These studies suggest that TG2 is required for maintenance of ECS cell EMT, invasion and migration, and suggests that inhibiting TG2 GTP binding/G-protein related activity may reduce skin cancer tumor survival.
Epidermal squamous cell carcinoma (SCC) is among the most common cancers and the frequency is increasing at a rapid rate [1,2]. SCC is treated by surgical excision, but the rate of recurrence approaches 10% and the recurrent tumors are aggressive and difficult to treat [2]. We propose that human epidermal cancer stem (ECS) cells survive at the site of tumor excision, that these cells give rise to tumor regrowth, and that therapies targeted to kill ECS cells constitute a viable anti-cancer strategy. An important goal in this context is identifying and inhibiting activity of key proteins that are essential for ECS cell survival. Working towards this goal, we have developed systems for propagation of human ECS cells [3]. These cells display properties of cancer stem cells including self-renew and high level expression of stem cell marker proteins [3].
In the present study we demonstrate that ECS cells express proteins characteristic of cells undergoing EMT (epithelial-mesenchymal transition). EMT is a morphogenetic process whereby epithelial cells lose epithelial properties and assume mesenchymal characteristics [4]. The epithelial cells lose cell-cell contact and polarity, and assume a mesenchymal migratory phenotype. There are three types of EMT. This first is an embryonic process, during gastrulation, when the epithelial sheet gives rise to the mesoderm [5]. The second is a growth factor and cytokine-stimulated EMT that occurs at sites of tissue injury to facilitate wound repair [6]. The third is associated with epithelial cancer cell acquisition of a mesenchymal migratory/invasive phenotype. This process mimics normal EMT, but is not as well controlled and coordinated [4, 7, 8]. A number of transcription factors (ZEB1, ZEB2, snail, slug, and twist) that are expressed during EMT suppress expression of epithelial makers, including E-cadherin, desmoplakin and claudins [4]. Snail proteins also activate expression of vimentin, fibronectin and metalloproteinases [4]. Snail factors are not present in normal epithelial cells, but are present in the tumor cells and are prognostic factors for poor survival [4].
An important goal is identifying factors that provide overarching control of EMT in cancer stem cells. In this context, several recent papers implicate type II transglutaminase (TG2) as a regulator of EMT [9–12]. TG2, the best studied transglutaminase, was isolated in 1957 from guinea pig liver extract as an enzyme involved in the covalent crosslinks proteins via formation of isopeptide bonds [13]. However, subsequent studies reveal that TG2 also serves as a scaffolding protein, regulates cell adhesion, and modulates signal transduction as a GTP binding protein that participates in G protein signaling [14]. TG2 is markedly overexpressed in cancer cells, is involved in cancer development [15–18], and has been implicated in maintaining and enhancing EMT in breast and ovarian cancer [10, 12, 19, 20]. The G protein function may have an important role in these processes [10, 21–23].
In the present manuscript we study the role of TG2 in regulating EMT in human ECS cells. Our studies show that TG2 is highly enriched in ECS cells. We further show that these cells express EMT markers and that TG2 is required to maintain EMT protein expression. TG2 knockdown, or treatment with TG2 inhibitor, reduces EMT marker expression and ECS cell survival, invasion and migration. TG2 GTP binding activity is absolutely required for maintenance of EMT protein expression and EMT-related responses. However, in contrast to breast cancer [9, 10], we show that TG2 regulation of EMT is not mediated via NFκB signaling.
TG2 is required for expression of EMT markers
EMT is a property of tumor stem cells that confers an ability to migrate and invade surrounding tissue [24–26]. We first examined whether ECS cells express EMT markers. Non-stem cancer cells and ECS cells, derived from the SCC-13 cancer cell line, were analyzed for expression of EMT markers. Fig. 1A shows that a host of EMT transcriptional regulators, including Twist, Snail and Slug, are increased in ECS cells (spheroid) as compared to non-stem cancer cells (monolayer). This is associated with increased levels of vimentin, fibronectin and N-cadherin, which are mesenchymal proteins, and reduced expression of E-cadherin, an epithelial marker. HIF-1α, an additional marker frequently associated with EMT, is also elevated. We next examined whether TG2 is required to maintain EMT marker expression. SCC-13 cell-derived ECS cells were grown in the presence of control- or TG2-siRNA, to reduce TG2, and the impact on EMT marker level was measured. Fig. 1B shows that loss of TG2 is associated with reduced expression of Twist, Snail, vimentin and HIF-1α. To further assess the role of TG2, we utilized SCC13-Control-shRNA and SCC13-TG2-shRNA2 cell lines. These lines were produced by infection of SCC-13 cells with lentiviruses encoding control- or TG2-specific shRNA. Fig. 1C shows that SCC13-TG2-shRNA2 cells express markedly reduced levels of TG2 and that this is associated with reduced expression of EMT associated transcription factors and target proteins, and increased expression of E-cadherin. To confirm this, we grew SCC13-Control-shRNA and SCC13-TG2-shRNA2 cells as monolayer cultures for immunostain detection of EMT markers. As shown in Fig. 2A, TG2 levels are reduced in TG2-shRNA expressing cells, and this is associated with the anticipated changes in epithelial and mesenchymal marker expression.
Tumor cells that express EMT markers display enhanced migration and invasion ability [24–26]. We therefore examined the impact of TG2 reduction on these responses. To measure invasion, control-shRNA and TG2-shRNA cells were monitored for ability to move through matrigel. Fig. 2B shows that loss of TG2 reduces movement through matrigel by 50%. We further show that this is associated with a reduction in cell migration using a monolayer culture wound closure assay. The control cells close the wound completely within 14 h, while TG2 knockdown reduces closure rate (Fig. 2C).
TG2 inhibitor reduces EMT marker expression and EMT functional responses
NC9 is a recently developed TG2-specific inhibitor [27, 28]. We therefore asked whether pharmacologic inhibition of TG2 suppresses EMT. SCC-13 cells were treated with 0 or 20 μM NC9. Fig. 3A shows that NC9 treatment reduces EMT transcription factor (Twist, Snail, Slug) and EMT marker (vimentin, fibronectin, N-cadherin, HIF-1α) levels. Consistent with these changes, the level of the epithelial marker, E-cadherin, is elevated. Fig. 3B and 3C show that pharmacologic inhibition of TG2 activity also reduces EMT biological response. Invasion (Fig. 3B) and cell migration (Fig. 3C) are also reduced.
Identification of TG2 functional domain required for EMT
We next performed studies to identify the functional domains and activities required for TG2 regulation of EMT. TG2 is a multifunctional enzyme that serves as a scaffolding protein, as a transamidase, as a kinase, and as a GTP binding protein [21]. The two best studied functions are the transamidase and GTP binding/G-protein related activities [21]. Transamidase activity is observed in the presence of elevated intracellular calcium, while GTP binding-related signaling is favored by low calcium conditions (reviewed in [21]). To identify the TG2 activity required for EMT, we measured the ability of wild-type and mutant TG2 to restore EMT in SCC13-TG2-shRNA2 cells, which have reduced TG2 expression (Fig. 4A). SCC13-TG2-shRNA2 cells display reduced expression of EMT markers including Twist, Snail, Slug, vimentin, fibronectin, N-cadherin and HIF-1α, and increased expression of the epithelial maker, E-cadherin, as compared to SCC13-Control-shRNA cells. Expression of wild-type TG2, or the TG2-C277S or TG2-W241A mutants, restores marker expression in SCC13-TG2-shRNA2 cells (Fig. 4A). TG2-C277S and TG2-W241A lack transamidase activity [10,29–31]. In contrast, TG2-R580A, which lacks G-protein activity [29–31], and TG2-Y516F, which retains only partial G-protein activity [30], do not efficiently restore marker expression. These findings suggest that the TG2 GTP binding function is required for EMT.
We next assayed the ability of the TG2 mutants to restore EMT functional responses-invasion and migration. Fig. 4B, 4C shows that wild-type TG2, TG2-C277S and TG2-W241A restore the ability of SCC13-TG2-shRNA2 cells to invade matrigel, but TG2-R580A and Y516F are less active. Fig. 4D shows a similar finding for cell migration, in that the TG2-R580A and Y517F mutant are only partially able to restore SCC13-TG2-shRNA2 cell migration. These findings suggest that TG2 GTP binding/G-protein related activity is required for EMT-related migration and invasion by skin cancer cells.
Role of TG2 in regulating EMT in A431 cells
The number of available epidermis-derived squamous cell carcinoma cell lines is limited, and so we compared our findings with A431 cells. A431 cells are squamous cell carcinoma cells established from human vulvar skin. A431 cells were grown as monolayer (non-stem cancer cells) and spheroids (ECS cells) and after 10 d the cells were harvested and assayed for expression of TG2 and EMT makers. Fig. 5A shows that TG2 levels are elevated in ECS cells and that this is associated with increased levels of mesenchymal markers, including Twist, Snail, Slug, vimentin, fibronectin, N-cadherin and HIF-1α. In contrast, E-cadherin levels are reduced. We next examined the impact of TG2 knockdown on EMT marker expression. Fig. 5B shows that mesenchymal markers are globally reduced and E-cadherin level is increased. As a biological endpoint of EMT, we examine the impact of TG2 knockdown on spheroid formation and found that TG2 loss leads to reduced spheroid formation (Fig. 5C). We next examined the impact of NC9 treatment on EMT and found a reduction in EMT markers expression associated with an increase in epithelial (E-cadherin) marker level (Fig. 5D). This loss of EMT marker expression is associated with reduced matrigel invasion (Fig. 5E), reduced spheroid formation (Fig. 5F) and reduced cell migration (Fig. 5G).
Role of NFκB
Previous studies in breast [18, 32–36], ovarian cancer [12, 37, 38], and epidermoid carcinoma [11] indicate that NFκB signaling mediates TG2 impact on EMT. We therefore assessed the role of NFκB in skin cancer cells. As shown in Fig. 6A, the increase in TG2 level observed in ECS cells (spheroids) is associated with reduced NFκB level. In addition, NFκB level is increased in TG2 knockdown cells (Fig. 6B). Thus, increased NFκB is not associated with increased TG2. We next assessed the impact of NFκB knockdown on TG2 control of EMT marker expression. Fig. 6C shows that TG2 is required for increased expression of EMT markers (HIF-1α, snail, twist, N-cadherin, vimentin and fibronectin) and reduced expression of the E-cadherin epithelial marker; however, knockdown of NFκB expression does not interfere with TG2 regulation of these endpoints. We next examined the effect of TG2 knockdown on NFκB and IκBα localization. The fluorescence images in Fig. 6D suggest that TG2 knockdown with TG2-siRNA does not alter the intracellular localization of NFκB or IκBα. This is confirmed by subcellular fractionation assay (Fig. 6E) which compares NFκB level in SCC13-TG2-Control and SCC13-TG2-shRNA2 (TG2 knockdown) cells. We also monitored NFκB subcellular distribution following treatment with NC9, the TG2 inhibitor. Fig. 6F shows that cytoplasmic/nuclear distribution of NFκB is not altered by NC9. Finally, we monitored the impact of TG2 expression on NFκB binding to a canonical NFκB-response element. Increased NFκB binding to the response element is a direct measure of NFκB activity [10]. Fig. 6G shows that overall binding is reduced in nuclear (N) extract prepared from ECS cells (spheroids) as compared to non-stem cancer cells (monolayer), and that NFkB binding, as indicated by gel supershift assay, is also slightly reduced in ECS cell extracts. These findings indicate that NFkB binding is slightly reduced in ECS cells, which are TG2-enriched (Fig. 1A).
We next monitored the role of NFκB on biological endpoints of EMT. Fig. 7A and 7B show that TG2 knockdown reduces migration through matrigel, but NFκB knockdown has no impact. Likewise, TG2 knockdown reduces wound closure, but NFκB knockdown does not. These findings suggest that NFκB does not mediate the pro-EMT actions of TG2 in epidermal squamous cell carcinoma.
The metastatic cascade, from primary tumor to metastasis, is a complex process involving multiple pathways and signaling cascades [39–41]. Cells that complete the metastatic cascade migrate away from the primary tumor through the blood to a distant site and there form a secondary tumor. Identifying the mechanisms that allow cells to survive this journey and form secondary tumors is an important goal. The processes involved in epithelial-mesenchymal transition (EMT) are important cancer therapy targets, as EMT is associated with enhanced cancer cell migration and stem cell self-renewal. EMT regulators, including Snail, Twist, Slug, are increased in expression in EMT and control expression of genes associated with the EMT phenotype [42].
TG2 is required for EMT
We have characterized a population of ECS cells derived from epidermal squamous cell carcinoma [3]. The present studies show that these cells, which display enhanced migration and invasion, possess elevated levels of TG2. Moreover, these cells are enriched in expression of transcription factors associated with EMT (Snail, Slug, and Twist, HIF-1α) as well as mesenchymal structural proteins including vimentin, fibronectin and N-cadherin. Consistent with a shift to mesenchymal phenotype, E-cadherin, an epithelial marker, is reduced in level. Additional studies show that TG2 knockdown results in a marked reduction in EMT marker expression and that this is associated with reduced ability of the cells to migrate to close a scratch wound and reduced movement in matrigel invasion assays. We also examined the impact of treatment with a TG2 inhibitor. NC9 is an irreversible active site inhibitor of TG2, that locks the enzyme in an open conformation [28, 43–45]. NC9 treatment of ECS cells results in decreased levels of Snail, Slug and Twist. These transcription factors suppress E-cadherin expression [46] and their decline in level is associated with increased levels of E-cadherin. NC9 inhibition of TG2 also reduces expression of vimentin, fibronectin and N-cadherin, and these changes are associated with reduced cell migration and reduced invasion through matrigel.
(Figures are not shown)
We also examined the role of TG2 in A431 squamous cell carcinoma cells derived from the vulva epithelium. TG2 is elevated in A431-derived ECS cells, as are EMT markers, and knockdown of TG2, with TG2-siRNA, reduces EMT marker expression and spheroid formation. Studies with NC9 indicate that NC9 inhibits A431 spheroid formation, EMT, migration and invasion. These studies indicate that TG2 is also required for EMT and migration and invasion in A431 cells. Based on these findings we conclude that TG2 is essential for EMT, migration and invasion, and is likely to contribute to metastasis in squamous cell carcinoma.
TG2 GTP binding activity is required for EMT
TG2 is a multifunctional enzyme that can act as a transamidase, GTP binding protein, protein disulfide isomerase, protein kinase, protein scaffold, and DNA hydrolase [21, 29, 44, 47]. The two most studied functions are the transamidase and GTP binding functions [29, 44, 47]. To identify the TG2 activity responsible for induction of EMT, we studied the ability of TG2 mutants to restore EMT in SCC13-TG2-shRNA2 cells, which express low levels of TG2 and do not express elevated levels of EMT markers or display EMT-related biological responses. These studies show that wild-type TG2 restores EMT marker expression and the ability of the cells to migrate on plastic and invade matrigel. TG2 mutants that retain GTP binding activity (TG2-C277S and TG2-W241A) also restore EMT. In contrast, TG2-R580A, which lacks GTP binding function, does not restore EMT. This evidence suggests that the GTP binding function is essential for TG2 induction of the EMT phenotype in ECS cells. Recent reports suggest that the TG2 is important for maintenance of stem cell survival in breast [9, 10, 17] and ovarian [12, 38, 48] cancer cells. Moreover, our findings are in agreement of those of Mehta and colleagues who reported that the TG2 GTP binding function, but not the crosslinking function, is required for TG2 induction of EMT in breast cancer cells [10].
TG2, NFκB signaling and EMT
To gain further insight into the mechanism of TG2 mediated EMT, we examined the role of NFκB. NFκB has been implicated as mediating EMT in breast, ovarian, and pancreatic cancer; however, NFκB may have a unique role in epidermal squamous cell carcinoma. In keratinocytes, NFκB has been implicated in keratinocyte dysplasia and hyperproliferation [49]. However, inhibition of NFκB function has also been shown to predispose murine epidermis to cancer [50]. Here we show that TG2 levels are elevated and NFκB levels are reduced in ECS cells as compared to non-stem cancer cells, and that TG2 knockdown is associated with increased NFκB level. In addition, TG2 knockdown, or inhibition of TG2 by treatment with NC9, does not altered the nuclear/cytoplasmic distribution of NFκB. We further show that elevated levels of TG2 in spheroid culture results in a slight reduction in NFκB binding to the NFκB response element, as measured by gel mobility supershift assay. These molecular assays strongly suggest that NFκB does not mediate the action of TG2 in epidermal cancer stem cells. Moreover, knockdown of NFκB-p65 in TG2 positive cells does not result in a reduction in Snail, Slug and Twist, or mesenchymal marker proteins expression, and concurrent knockdown of TG2 and NFκB does not reduce EMT marker protein levels beyond that of TG2 knockdown alone. These findings suggest that NFκB is not an intermediary in TG2-stimulated EMT in ECS cells. This is in contrast to the required role of NFκB in mediating TG2 induction of cell survival and EMT in breast cancer cells [18, 32, 33] and ovarian cancer [12, 37, 38] and epidermoid carcinoma [11].
11.2.3.5 CD24+ Ovarian Cancer Cells are Enriched for Cancer Initiating Cells and Dependent on JAK2 Signaling for Growth and Metastasis
Investigators showed that CD24+ and CD133+ cells have increased tumorsphere forming capacity. CD133+ cells demonstrated a trend for increased tumor initiation while CD24+ cells vs CD24– cells, had significantly greater tumor initiation and tumor growth capacity. [Mol Cancer Ther]
D Burgos-Ojeda, R Wu, K McLean, Yu-Chih Chen, M Talpaz, et al.
Molec Cancer Ther May 12, 2015; 14(5)
http://dx.doi.org:/10.1158/1535-7163.MCT-14-0607
Ovarian cancer is known to be composed of distinct populations of cancer cells, some of which demonstrate increased capacity for cancer initiation and/or metastasis. The study of human cancer cell populations is difficult due to long requirements for tumor growth, inter-patient variability and the need for tumor growth in immune-deficient mice. We therefore characterized the cancer initiation capacity of distinct cancer cell populations in a transgenic murine model of ovarian cancer. In this model, conditional deletion of Apc, Pten, and Trp53 in the ovarian surface epithelium (OSE) results in the generation of high grade metastatic ovarian carcinomas. Cell lines derived from these murine tumors express numerous putative stem cell markers including CD24, CD44, CD90, CD117, CD133 and ALDH. We show that CD24+ and CD133+ cells have increased tumor sphere forming capacity. CD133+ cells demonstrated a trend for increased tumor initiation while CD24+ cells vs CD24- cells, had significantly greater tumor initiation and tumor growth capacity. No preferential tumor initiating or growth capacity was observed for CD44+, CD90+, CD117+, or ALDH+ versus their negative counterparts. We have found that CD24+ cells, compared to CD24- cells, have increased phosphorylation of STAT3 and increased expression of STAT3 target Nanog and c-myc. JAK2 inhibition of STAT3 phosphorylation preferentially induced cytotoxicity in CD24+ cells. In vivo JAK2 inhibitor therapy dramatically reduced tumor metastases, and prolonged overall survival. These findings indicate that CD24+ cells play a role in tumor migration and metastasis and support JAK2 as a therapeutic target in ovarian cancer.
11.2.3.6 EpCAM-Antibody-Labeled Noncytotoxic Polymer Vesicles for Cancer Stem Cells-Targeted Delivery of Anticancer Drug and siRNA
Researchers designed and synthesized a novel anti-epithelial cell adhesion molecule (EpCAM)-monoclonal-antibody-labeled cancer stem cells (CSCs)-targeting, noncytotoxic and pH-sensitive block copolymer vesicle as a nano-carrier of anticancer drug and siRNA. [Biomacromolecules]
Jing Chen , Qiuming Liu , Jiangang Xiao , and Jianzhong Du
Biomacromolecules May 19, 2015. (just published)
http://dx.doi.org:/10.1021/acs.biomac.5b00551
Cancer stem cells (CSCs) have the capability to initiate tumor, to sustain tumor growth, to maintain the heterogeneity of tumor, and are closely linked to the failure of chemotherapy due to their self-renewal and multilineage differentiation capability with an innate resistance to cytotoxic agents. Herein, we designed and synthesized a novel anti-EpCAM (epithelial cell adhesion molecule)-monoclonal-antibody-labeled CSCs-targeting, noncytotoxic and pH-sensitive block copolymer vesicle as a nano-carrier of anticancer drug and siRNA (to overcome CSCs drug resistance by silencing the expression of oncogenes). This vesicle shows high delivery efficacy of both anticancer drug doxorubicin hydrochloride (DOX∙HCl) and siRNA to the CSCs because it is labeled by the monoclonal antibodies to the CSCs-surface-specific marker. Compared to non-CSCs-targeting vesicles, the DOX∙HCl or siRNA loaded CSCs-targeting vesicles exhibited much better CSCs killing and tumor growth inhibition capabilities with lower toxicity to normal cells (IC50,DOX decreased by 80%), demonstrating promising potential applications in nanomedicine.
11.2.3.7 Survival of Skin Cancer Stem Cells Requires the Ezh2 Polycomb Group Protein
Investigators showed that Ezh2 is required for epidermal cancer stem (ECS) cell survival, migration, invasion and tumor formation, and that this is associated with increased histone H3 trimethylation on lysine 27, a mark of Ezh2 action. They also showed that Ezh2 knockdown or treatment with Ezh2 inhibitors, GSK126 or EPZ-6438, reduced Ezh2 level and activity, leading to reduced ECS cell spheroid formation, migration, invasion and tumor growth. [Carcinogenesis]
G Adhikary, D Grun, S Balasubramanian, C Kerr, J Huang and RL Eckert
Carcinogenesis (2015)
http://dx.doi.org:/10.1093/carcin/bgv064
Polycomb group (PcG) proteins, including Ezh2, are important candidate stem cell maintenance proteins in epidermal squamous cell carcinoma. We previously showed that epidermal cancer stem cells (ECS cells) represent a minority of cells in tumors, are highly enriched in Ezh2 and drive aggressive tumor formation. We now show that Ezh2 is required for ECS cell survival, migration, invasion and tumor formation, and that this is associated with increased histone H3 trimethylation on lysine 27, a mark of Ezh2 action. We also show that Ezh2 knockdown or treatment with Ezh2 inhibitors, GSK126 or EPZ-6438, reduces Ezh2 level and activity, leading to reduced ECS cell spheroid formation, migration, invasion and tumor growth. These studies indicate that epidermal squamous cell carcinoma cells contain a subpopulation of cancer stem (tumor-initiating) cells that are enriched in Ezh2, that Ezh2 is required for optimal ECS cell survival and tumor formation, and that treatment with Ezh2 inhibitors may be a strategy for reducing epidermal cancer stem cell survival and suppressing tumor formation.
11.2.3.8 Inhibition of STAT3, FAK and Src mediated signaling reduces cancer stem cell load, tumorigenic potential and metastasis in breast cancer
R Thakur, R Trivedi, N Rastogi, M Singh & DP Mishra
Scientific Reports May 14, 2015; 5(10194)
http://dx.doi.org:/10.1038/srep10194
Cancer stem cells (CSCs) are responsible for aggressive tumor growth, metastasis and therapy resistance. In this study, we evaluated the effects of Shikonin (Shk) on breast cancer and found its anti-CSC potential. Shk treatment decreased the expression of various epithelial to mesenchymal transition (EMT) and CSC associated markers. Kinase profiling array and western blot analysis indicated that Shk inhibits STAT3, FAK and Src activation. Inhibition of these signaling proteins using standard inhibitors revealed that STAT3 inhibition affected CSCs properties more significantly than FAK or Src inhibition. We observed a significant decrease in cell migration upon FAK and Src inhibition and decrease in invasion upon inhibition of STAT3, FAK and Src. Combined inhibition of STAT3 with Src or FAK reduced the mammosphere formation, migration and invasion more significantly than the individual inhibitions. These observations indicated that the anti-breast cancer properties of Shk are due to its potential to inhibit multiple signaling proteins. Shk also reduced the activation and expression of STAT3, FAK and Src in vivo and reduced tumorigenicity, growth and metastasis of 4T1 cells. Collectively, this study underscores the translational relevance of using a single inhibitor (Shk) for compromising multiple tumor-associated signaling pathways to check cancer metastasis and stem cell load.
Breast cancer is the most common endocrine cancer and the second leading cause of cancer-related deaths in women. In spite of the diverse therapeutic regimens available for breast cancer treatment, development of chemo-resistance and disease relapse is constantly on the rise. The most common cause of disease relapse and chemo-resistance is attributed to the presence of stem cell like cells (or CSCs) in tumor tissues1, 2. CSCs represent a small population within the tumor mass, capable of inducing independent tumors in vivo and are hard to eradicate2. Multiple signaling pathways including Receptor Tyrosine Kinase (RTKs), Wnt/β-catenin, TGF-β, STAT3, Integrin/FAK, Notch and Hedgehog signaling pathway helps in maintaining the stem cell programs in normal as well as in cancer cells3, 4, 5, 6. These pathways also support the epithelial-mesenchymal transition (EMT) and expression of various drug transporters in cancer cells. Cells undergoing EMT are known to acquire stem cell and chemo-resistant traits7. Thus, the induction of EMT programs, drug resistance and stem cell like properties are interlinked7. Commonly used anti-cancer drugs eradicate most of the tumor cells, but CSCs due to their robust survival mechanisms remain viable and lead to disease relapse8. Studies carried out on patient derived tumor samples and in vivo mouse models have demonstrated that the CSCs metastasize very efficiently than non-CSCs9, 10, 11. Therefore, drugs capable of compromising CSCs proliferation and self-renewal are urgently required as the inhibition of CSC will induce the inhibition of tumor growth, chemo-resistance, metastasis and metastatic colonization in breast cancer.
Shikonin, a natural dietary component is a potent anti-cancer compound12, 13. Previous studies have shown that Shk inhibits the cancer cell growth, migration, invasion and tumorigenic potential12. Shk has good bioavailability, less toxicity and favorable pharmacokinetic and pharmacodynamic profiles in vivo12. In a recent report, it was shown that the prolonged exposure of Shk to cancer cells does not cause chemo-resistance13.Other studies have shown that it inhibits the expression of various key inflammatory cytokines and associated signaling pathways12, 14. It decreases the expression of TNFα, IL12, IL6, IL1β, IL2, IFNγ, inhibits ERK1/2 and JNK signaling and reduces the expression of NFκB and STAT3 transcription factors14, 15. It inhibits proteasome and also modulates the cancer cell metabolism by inhibiting tumor specific pyurvate kinase-M214,15, 16. Skh causes cell cycle arrest and induces necroptosis in various cancer types14. Shk also inhibits the expression of MMP9, integrin β1 and decreases invasive potential of cancer cells14, 17. Collectively, Shk modulates various signaling pathways and elicits anti-cancer responses in a variety of cancer types.
In breast cancer, Shk has been reported to induce the cell death and inhibit cell migration, but the mechanisms responsible for its effect are not well studied18, 19. Signaling pathways modulated by Shk in cancerous and non-cancerous models have previously been shown important for breast cancer growth, metastasis and tumorigenicity20. Therefore in the current study, we investigated the effect of Shk on various hallmark associated properties of breast cancer cells, including migration, invasion, clonogenicity, cancer stem cell load and in vivo tumor growth and metastasis.
Shk inhibits cancer hallmarks in breast cancer cell lines and primary cells
We first examined the effect of Shk on various cancer hallmark capabilities (proliferation, invasion, migration, colony and mammosphere forming potential) in breast cancer cells. MTT assay was used to find out effect of Shk on viability of breast cancer cells. Semi-confluent cultures were exposed to various concentrations of Shk for 24 h. Shk showed specific anti-breast cancer activity with IC50 values ranging from 1.38 μM to 8.3 μM in MDA-MB 231, MDA-MB 468, BT-20, MCF7, T47D, SK-BR-3 and 4T1 cells (Fig. 1A). Whereas the IC50 values in non-cancerous HEK-293 and human PBMCs were significantly higher indicating that it is relatively safe for normal cells (Fig. S1A). Shk was found to induce necroptotic cell death consistent with previous reports (Fig. S1B). Treatment of breast cancer cells for 24 h with 1.25 μM, 2.5 μM and 5.0 μM of Shk significantly reduced their colony forming potential (Fig. 1B). To check the effect of Shk on the heterogeneous cancer cell population, we tested it on patient derived primary breast cancer cells. Shk reduced the viability and colony forming potential of primary breast cancer cells in dose dependent manner (Fig. 1C,D). Further we checked its effects on migration and invasion of breast cancer cells. Shk (2.5 μM) significantly inhibited the migration of MDA-MB 231, MDA-MB 468, MCF7 and 4T1 cells (Fig. 1E). It also inhibited the cell invasion in dose dependent manner (Fig. 1F and S1C, S1D, S1E,S1F). We further examined its effect on mammosphere formation. MDA-MB 231, MDA-MB 468, MCF7 and 4T1 cell mammosphere cultures were grown in presence or absence of 1.25 μM, 2.5 μM and 5.0 μM Shk for 24 h. After 8 days of culture, a dose dependent decrease in the mammosphere forming potential of these cells was observed (Figs. 1G,H). Collectively, these results indicated that Shk effectively inhibits the various hallmarks associated with aggressive breast cancer.
(not shown)
Figure 1: Shk inhibits multiple cancer hallmarks
Shk reduces cancer stem cell load in breast cancer
As Shk exhibited strong anti-mammosphere forming potential; therefore it was further examined for its anti-cancer stem cell (CSC) properties. Cancer stem cell loads in breast cancer cells were assessed using Aldefluor assay which measures ALDH1 expression. MDA-MB 231 cells with the highest number of ALDH1+ cells were selected for further studies (Fig. S2A). We also checked the correlation between ALDH1 expression and mammosphere formation. Sorted ALDH1+ cells were subjected to mammosphere cultures. ALDH1+ cells formed highest number of mammospheres compared to ALDH1-/low and parent cell population, indicating that ALDH1+ cells are enriched in CSCs (Fig. S2B). Shk reduced the Aldefluor positive cells in MDA-MB 231 cells after 24 h of treatment (Fig. 2A,B). Next, we examined the effect of Shk on the expression of stem cell (Sox2, Oct3/4, Nanog, AldhA1 and c-Myc) and EMT (Snail, Slug, ZEB1, Twist, β-Catenin) markers, associated with the sustenance of breast CSCs. Shk (2.5 μM) treatment for 24 h reduced the expression of these markers (Fig. 2C and S2D). Shk also reduced protein expression of these markers in dose dependent manner (Fig. 2D,E and S2C).
(not shown)
Figure 2: Shk decreases stem cell load in breast cancer cells and enriched CD44+,CD24−/low breast cancer stem cells.
To further confirm anti-CSC properties of Shk, we checked the effect of shikonin on the load of CD44+ CD24− breast CSCs in MCF7 cells grown on matrigel. Shikonin reduced CD44+ CD24− cell load in dose dependent manner after 24 h of treatment (Fig S2E). We also tested its effects on the enriched CSC population. CD44+ CD24− cells were enriched from MCF7 cells using MagCellect CD24− CD44+ Breast CSC Isolation Kit (Fig. S2F). Enriched CSCs formed highest number of mammosphere in comparison to parent MCF7 cell population or negatively selected CD24+ cells (Fig. S2G). Enriched CSCs were treated with indicated doses of Shk (0.625 μM, 1.25 μM and 2.5 μM) for 24 h and were either analyzed for ALDH1 positivity or subjected to colony or mammosphere formation. 2.5 μM dose of Shk reduced ALDH1+ cells by 50% and inhibited colony and mammosphere formation (Fig. S2H, 2F, 2G and 2H). Shk also reduced the mRNA expression of CSC markers in CD44+ CD24− cells and patient derived primary cancer cells (Fig. 2I,J). These results collectively indicated that Shk inhibits CSC load and associated programs in breast cancer.
Shk is a potent inhibitor of STAT3 and poorly inhibits FAK and Src
To identify the molecular mechanism responsible for anti-cancer properties of Shk, we used a human phospho-kinase antibody array to study a subset of phosphorylation events in MDA-MB 231 cells after 6h of treatment with 2.5 μM Shk. Amongst the 46 phospho-antibodies spotted on the array, the relative extent of phosphorylation of three proteins decreased to about ≳ 2 fold (STAT3, 3.3 fold; FAK, 2.5 fold and Src, 1.8 fold) upon Shk treatment (Fig. 3A,B). These proteins (STAT3, FAK and Src) are known to regulate CSC proliferation and self renewal21, 22, 23. Therefore, we focused on these proteins and the result of kinase-array was confirmed by western blotting. Shk effectively inhibits STAT3 at early time point (1 h) while activation of FAK and Src decreased on or after 3 h (Fig. 3C) confirming Shk as a potent inhibitor of STAT3. Shk also reduced the protein expression of STAT3, FAK and Src at 24 h (Fig. 3C).
(not shown)
Figure 3. Shk inhibits STAT3, FAK and Src signaling pathways.
We also observed that Shk does not inhibit JAK2 at initial time-points (Fig. 3C). This raised a possibility that Shk either regulates STAT3 independent of JAK2 or it binds directly to STAT3. To check the first probability, we activated STAT3 by treating the cells with IL6 (100 ng ml−1) for 1 h followed by treatment with Shk (2.5 μM) for 1 h. Both immunofluorescence and western-blotting results showed that Shk inhibited activated STAT3 without inhibiting JAK2 (Fig. S3A, S3B) confirming that Shk inhibits JAK2 mediated activation of STAT3 possibly by binding directly to STAT3. For further confirmation, we performed an in silico molecular docking analysis to examine binding of Shk with the STAT3 SH2 domain. In a major conformational cluster, Shk occupied Lys-707, Lys-709 and Phe-710 binding sites in the STAT3 SH2 domain similar to the STAT3 standard inhibitor S3I-201 (Fig. S3C and S3D). The binding energy of Shk to STAT3 was −4.20 kcal mol−1. Collectively, these results showed that Shk potently inhibits STAT3 activation and also attenuates FAK and Src activation.
STAT3, Src and FAK are differentially expressed and activated in breast CSCs (BCSCs)
STAT3 and FAK are known to play an important role in proliferation and self-renewal of CSCs in various cancer types including breast cancer21, 22, 24. Src also support CSC phenotype in some cancer types, but there are limited reports of its involvement in breast cancer25. Therefore, we checked the expression and activation of STAT3, FAK and Src in CSCs and non-CSCs. Here we used two methods to enrich the CSCs and non-CSCs. In the first method, the MDA-MB 231 cells were subjected to mammosphere formation for 96 h. After 96 h, mammosphere and non-mammosphere forming cells were clearly visible (Fig. 4A). These mammosphere and non-mammosphere forming cells were separated by using a 70 micron cell strainer. Mammospheres were subjected to two subculture cycles to enrich CSCs. With each passage, the viable single cells (non-mammosphere forming cells) and mammospheres were collected in RIPA lysis buffer and western blotting was done (Fig. 4B). We found that the activation and expression of the STAT3, FAK and Src is higher in enriched mammosphere cultures (Fig. 4C). In the second method, CD44+ CD24− cells were isolated from MCF7 cultures using MagCellect Breast CSC Isolation Kit. STAT3, FAK and Src activation and their mRNA and protein expression were assessed in enriched CSCs and were compared to parent MCF7 cell population. STAT3, FAK and Src all were differentially activated in CSCs (Fig. 4E). High mRNA as well as protein expressions of all the three genes was also observed in CSCs (Fig. 4D,E). Collectively, these results indicate that STAT3, FAK and Src are over expressed and activated in BCSCs.
Figure 4: STAT3, FAK and Src are differentially activated and expressed in breast cancer cells.
- Representative picture indicating mammosphere and single suspended cells. (B) Schematic outline of mammosphere enrichment. (C) Protein expression and activation of STAT3, FAK and Src was determined in single suspended cells (non-mammosphere forming cells) and mammospheres by western blot. The full size blots corresponding to the cropped blot images are given in S10. (D) Gene expression of STAT3, FAK and Src was determined in MCF7 parent population and CD44+ CD24−/low MCF7 cells using PCR. The full agarose gel images corresponding to the cropped images are given in Fig. S10. (E) Protein expression and activation of STAT3, FAK and Src was in CD44+ 24− cells and parent population.

STAT3, FAK and Src are differentially activated and expressed in breast cancer cells.
http://www.nature.com/srep/2015/150514/srep10194/images_article/srep10194-f4.jpg
STAT3 is important for mammosphere formation and CSC programs in breast cancer
As our results indicated that the expression and activation of STAT3, FAK and Src is high in BCSCs and Shk is capable of inhibiting these signaling proteins; therefore to find out functional relevance of each protein and associated effects on their pharmacological inhibition by Shk, we used specific inhibitors against these three. Effect of these inhibitors was first tested on the mammosphere forming potential of MDA-MB 231, MDA-MB 468 and MCF7 cells. A drastic reduction in the mammosphere formation was observed upon STAT3 inhibition. FAK and Src inhibition also reduced the primary and secondary mammosphere formation but STAT3 inhibition showed most potent effect (Fig. 5A and S4). Further, we also checked the effect of these inhibitors on the expression of various CSC and EMT related markers in MDA-MB 231 cells. STAT3 inhibition decreased the expression of most of the CSC and EMT markers (Fig. 5B). These two findings indicated that STAT3 inhibition is more effective in reducing mammosphere forming potential and weakens major CSC programs and the anti-CSC potential of Shk is possibly due to its strong STAT3 inhibitory effect.
(not shown)

STAT3, FAK and Src activation status correlates with mammosphere forming potential in breast cancer
Figure 5: STAT3, FAK and Src activation status correlates with mammosphere forming potential in breast cancer.
http://www.nature.com/srep/2015/150514/srep10194/carousel/srep10194-f5.jpg
(A) Bar graph represents number of mammospheres formed from 2500 cells in presence and absence of indicated treatments. MDA-MB 231, MDA-MB 468 and MCF7 24 h mammosphere cultures were treated with Shk (2.5 μM), FAK inhibitor (FAK inhibitor 14; 2.5 μM), Src inhibitor (AZM 475271; 10 μM) and STAT3 inhibitor (WP1066; 10 μM). After 24 h, treatments were removed and cells were allowed to grow in fresh mammosphere culture media for 8 days. (B) Expression of various stem cell and EMT related transcription factors and markers were detected using western blotting in MDA-MB 231 cells with or without indicated treatments. The full size blots corresponding to the cropped blot images are given in Fig. S10. (C) MDA-MB 231, MDA-MB 468 and MCF7 cells were pre-treated with either IL6 (100 ng ml−1), Fibronectin (1 μg ml−1) or EGF (25 ng ml−1) for two population doublings and subjected to mammosphere formation. Bar graph represents average of three independent experiments. (D) MCF7 cells were pre-treated with either IL6 (100 ng ml−1), Fibronectin (1 μg ml−1) or EGF (25 ng ml−1) for two population doublings and subjected to mammosphere formation. After 24 h, cells were treated with DMSO (untreated) or Shk (treated) as indicated in the bar graph. Data are shown as the mean ±SD. (*) p < 0.05 and (**) p < 0.01.
To further check the involvement of these pathways in CSCs, we cultured MDA-MB 231, MDA-MB 468 and MCF7 cells in the presence of either IL6 (100ng ml−1), EGF (25 ng ml−1) or Fibronectin (1 μg ml−1) coated surface for two population doublings. Cells were then subjected to mammosphere formation. In IL6 pre-treated cultures, there was a sharp rise in mammosphere formation, indicating that the STAT3 activation shifts CSC and non-CSC dynamics towards CSCs (Fig. 5C). IL6 is previously known to induce the conversion of non-CSC to CSC via STAT3 activation26. In MCF7 cells, mammosphere forming potential after IL6 pre-treatment increased nearly by three fold. Therefore, we further checked the effectiveness of Shk on mammosphere forming potential in pre-treated MCF7 cells. It was found that Shk inhibits mammosphere formation most effectively in IL6 pre-treated cultures (Fig. 5D). However, in EGF and Fibronectin pre-treated cultures, Shk was relatively less effective. This was possibly due to its weak FAK and Src inhibitory potential. Collectively, these results illustrated that STAT3 activation is significantly correlated with the mammosphere forming potential of breast cancer cells and its inhibition by a standard inhibitor or Shk potently reduce the mammosphere formation.
Shk inhibit CSCs load by disrupting the STAT3-Oct3/4 axis
In breast cancer, STAT3 mediated expression of Oct3/4 is a major regulator of CSC self-renewal26, 27. As we observed that both Shk and STAT3 inhibitors decreased the Oct3/4 expression (Figs. 2C and 5B), we further checked the effect of STAT3 activation on ALDH1+ CSCs and Oct3/4 expression. On IL6 pre-treatment, number of ALDH1+ cells increased in all three (MDA-MB 231, MDA-MB 468 and MCF7) cancer cells (Fig. 6A). MCF7 cells showed highest increase. Therefore, to check the effect of STAT3 inhibition on CSC load, we incubated IL6 pre-treated MCF7 cells with Shk and STAT3 inhibitor for 24 h and analyzed for ALDH1 positivity. It was observed that both Shk and STAT3 inhibitor reduced the IL6 induced ALDH1 positivity from 10% to < 2% (Fig. 6B). These results suggested that Shk induced inhibition of STAT3 and decrease in BCSC load is interlinked. We further checked the effect of STAT3 activation status on Oct3/4 expression in MDA-MB 231, MDA-MB 468 and MCF7 cells. We observed that expression of Oct3/4 increases with the increase in STAT3 activation (Fig. 6C–E).
(not shown)
Figure 6: STAT3 activation status and its effect on cancer stem cell load
STAT3 transcriptional activity is important in maintaining CSC programs28, 29. Therefore, we also examined the effect of Shk on STAT3 promoter activity. STAT3 reporter assay was performed in presence of IL6 and Shk; it was found that Shk reduced the promoter activity of STAT3 in a dose dependent manner (Fig. S5). Collectively, these results showed that Shk mediated STAT3 inhibition are responsible for decrease in CSC load and Oct3/4 associated stem cell programs.
Shk inhibits mammosphere formation, migration and invasion through inhibition of STAT3, FAK and Src in breast cancer cells
As the earlier results (Fig. 1) showed that Shk inhibits cell migration and invasion in breast cancer cells, we further examined the effect of STAT3, FAK and Src inhibitors on cell migration and invasion in MDA-MB 231 cells. It was found that STAT3 inhibitor poorly inhibits cell migration while both Src and FAK inhibitors were effective in reducing cell migration (Fig. 7A). All the three inhibitors decreased the cell invasion and MMP9 expression significantly (Fig. 7B and S6). It was also observed that effect of all these inhibitors, except STAT3 inhibitor on mammosphere formation and FAK inhibitor on cell migration, were not comparable to that of Shk. Shk inhibited all these properties more effectively than individual inhibition of STAT3, FAK and Src. This made us to assume that the ability of Shk to inhibit multiple signaling molecules simultaneously is the reason behind its potent anti-cancer effect. To check this notion, we combined STAT3, FAK and Src inhibitors with each other and examined the effect of combinations on invasion, migration and mammosphere forming potential in MDA-MB 231 cells. We observed further decrease in cell migration and invasion on combining STAT3 and FAK, STAT3 and Src, or FAK and Src (Figs. 7A,B). Combination of FAK and Src was not very effective in inhibiting mammosphere formation in MDA-MB 231 cells and CD44+ CD24− MCF7 CSCs. However, their combination with STAT3 decreased the mammosphere forming potential equivalent to that of Shk (Fig. 7C,D). We also compared the mammosphere forming potential of Shk with Salinomycin (another anti-CSC agent) and found that at 2.5 μM dose of Shk was almost two times more potent than Salinomycin (Fig. S7). Collectively, these results indicated that Shk inhibits multiple signaling proteins (STAT3, FAK and Src) to compromise various aggressive breast cancer hallmarks.
Figure 7: Combination of FAK, Src and STAT3 inhibitors is more potent than individual inhibition against various cancer hallmarks.

combination-of-fak-src-and-stat3-inhibitors-is-more-potent-than-individual-inhibition-against-various-cancer-hallmarks
http://www.nature.com/srep/2015/150514/srep10194/images_article/srep10194-f7.jpg
- Cell migration and (B) cell invasion potential of MDA-MB 231 cells was assessed in the presence of Shk (2.5 μM), FAK inhibitor (FAK inhibitor 14; 2.5 μM), Src inhibitor (AZM 475271; 10 μM) and STAT3 inhibitor (WP1066; 10 μM). Various combinations of these inhibitors were also used STAT3+FAK inhibitor (WP1066; 10 μM + FAK inhibitor 14; 2.5 μM), STAT3 + Src Inhibitor (WP1066; 10 μM + AZM 475271; 10 μM) and FAK+Src Inhibitor (FAK inhibitor 14; 2.5 μM + AZM 475271; 10 μM). Cell migration and cell invasion was assessed through scratch cell migration assay and transwell invasion after 24 h of treatments. (C,D) Mammosphere forming potential of MDA-MB 231 cells and CD44+ CD24−/low enriched MCF7 cells was assessed in presence of similar combination of STAT3+FAK inhibitor (WP1066; 10 μM + FAK inhibitor 14; 2.5 μM), STAT3 + Src Inhibitor (WP1066; 10 μM+ AZM 475271; 10 μM) and FAK + Src Inhibitor (FAK inhibitor 14; 2.5 μM + AZM 475271; 10 μM). Cells were subjected to mammosphere cultures for 24 h and treated with the indicated inhibitors for next 24 h, followed by media change and growth of mammospheres were monitored for next 8 days. Data are shown as the mean ±SD. (**) p < 0.01.
Shk inhibits breast cancer growth, metastasis and decreases tumorigenicity
To explore whether Shk may have therapeutic potential for breast cancer treatment in vivo, we tested Shk against 4T1-induced breast cancer syngenic mouse model. 4T1 cells (mouse breast cancer cells) are capable of growing fast and metastasize efficiently in vivo30. Prior to the in vivo experiments, we checked the effect of Shk on ALDH1 positivity and on activation of STAT3, FAK and Src in 4T1 cells in vitro. Shk effectively decreased the ALDH1+ cells and inhibited STAT3, FAK and Src in 4T1 cells in vitro (Fig. S8A and S8B). For in vivo tumor generation, 1 × 106 cells were injected subcutaneously in the fourth nipple mammary fat pad of BALB/c mice. When the average size of tumors reached around 50 mm3, mice were divided into three groups, vehicle and two Shk treated groups each received either 2.5 mg Kg−1 or 5.0 mg Kg−1 Shk. Shk was administered via the intraperitoneal injection on every alternate day. It significantly suppressed the tumor growth in 4T1 induced syngenic mouse model (Fig. 8A). The average reduction in 4T1 tumor growth was 49.78% and 89.73% in 2.5 mg Kg−1 and 5.0 mg Kg−1 groups respectively compared with the vehicle treated group (Fig. 8A). No considerable change in body weight of the treated group animals was observed (Fig. S9A). We further examined the effect of Shk on the tumor initiating potential of breast cancer cells. 4T1 induced tumors were excised from the control and treatment groups on the second day after 4th dose of Shk was administered. Tumors were dissociated; cells were allowed to adhere and then re-injected into new animals for secondary tumor formation. Growth of secondary tumors was monitored till day 15 post-reinjection. Shk treated groups showed a marked decrease in secondary tumor formation (Fig. 8D). We also observed a drastic reduction in the number of metastatic nodules in the lungs of treatment group animals (Fig. 8F). The reduction in the metastatic load was not proportional to the decrease in tumor sizes; however within the treatment group, some animals with small tumors were carrying higher number of metastatic nodules. As FAK is an important mediator of cancer metastasis and metastatic colonization, we further examined the effects of Shk on metastatic colonization. For this, 1 × 105 4T1 cells were injected to BALB/c mice through tail vein. Animals were divided into three groups, as indicated above. Shk and vehicle were administered through intraperitoneal injections at alternate days starting from the 2nd day post tail vein injections till 33rd day. The average reduction in total number of metastatic nodules was 88.6% – 90.5% in Shk treated mice compared to vehicle control (Fig. 8F). An inset picture (Fig. 8A lower panel) represents lung morphology of vehicle control and treated groups. We further examined the activation and expression status of STAT3, FAK and Src between vehicle control and treated group tumors. There were low expression and activation of STAT3, FAK and Src in treated tumors as compared to the vehicle control (Fig. 8B,C). Similar trend was observed in ALDH1 expressions (Fig. 8B). Further, the mice tumor sections were subjected to immunohistochemistry, immunofluorescence and hematoxylin and eosin (H&E) staining to study histology and expression of key proteins being examined in this study. Fig. 8G shows representative images of H&E staining, proliferating cell nuclear antigen (PCNA), terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL), STAT3 and Oct3/4 immunostaining. PCNA expression was low while TUNEL positive cells were high in tumor tissues of Shk treated groups. STAT3 and Oct3/4 expression was low in Shk treated groups. These results collectively demonstrated that Shk modulates the expression and activation of STAT3, FAK and Src in vivo and is effective in suppressing tumorigenic potential and metastasis in syngenic mouse model.
Figure 8: Shk inhibits breast cancer growth, tumorigenicity and metastasis in vivo.

Shk inhibits breast cancer growth, tumorigenicity and metastasis in vivo
http://www.nature.com/srep/2015/150514/srep10194/images_article/srep10194-f8.jpg
- Shk inhibited 4T1 tumor growth. Bar graph represents the average tumor volumes in vehicle control and Shk treated tumor bearing mice (n = 6). (*) p < 0.05 and (**) p < 0.01. Inset picture of upper panel represents tumor sizes and lower pane represents lung morphology in vehicle control and Shk treatment groups. (B) Western blot examination of indicated proteins for their expression and activation in vehicle control and treated tumor groups. The full size blots corresponding to the cropped blot images are given in Fig. S10. (C) Gene expression of stem cell and EMT markers in tumor tissues excised from the vehicle control and Shk treated groups (n = 3). (D) Number of secondary tumors formed after injecting indicated cell dilutions from Vehicle treated and Shk treated 4T1 tumors. (E) Number of lung nodules formed in mice injected with 4T1 mouse mammary tumor cells in the mammary fat pad and administered with 2.5 mg Kg−1 Shk or vehicle control on every alternate day for 3 weeks (n = 6). (F) Number of lung nodules in mice injected with 4T1 mouse mammary tumor cells through tail vein and administered with 2.5 mg Kg−1 Shk or vehicle control on every alternate day for 3 weeks. (n = 8) (G) Representative panel of the histological H&E staining, immunofluorescence staining for the STAT3, Oct3/4, cell proliferation marker PCNA and DNA damage indicator-TUNEL staining of tumor sections from vehicle and treatment groups.
Recent studies have shown that aggressiveness, therapy resistance and disease relapse in breast cancer is attributed to a small population of CSCs involved in continuous self-renewal and differentiation through signaling pathways similar to that of the normal stem cells31. Therapeutic targeting of CSCs therefore, has profound clinical implications for cancer treatment31. Recent studies indicated that therapies / agents targeting both differentiated cancer cells and CSCs may possibly have significant therapeutic advantages32. Therefore, it is imperative to look for novel therapeutic agents with lesser side effects urgently for effective targeting of CSCs. In search of novel, nontoxic anti-CSC agents, attention has been focused on natural agents in recent times33,34. In this study, we have used a natural napthoquinone compound, Shk with established antitumorigenic, favorable pharmacokinetic and toxicity profiles and report for the first time its potent anti-CSC properties. Shk significantly inhibits breast cancer cell proliferation in vitro, ex vivoand in vivo. It decreases the cell migration and invasion of breast cancer cells in vivo, as well as inhibits tumorigenicity, metastasis and metastatic colonization in a syngenic mouse model of breast cancer in vivo. These finding suggest a strong potential of Shk in breast cancer therapy.
We assessed the effect of Shk on the CSC load in breast cancer cells through various functional assays (tumorsphere in vitro and syngenic mouse model of breast cancer in vivo) and quantification of specific stem cell markers. In breast cancer, CD44+ CD24− cells and ALDH1+ cells are considered to be BCSCs21, 25. Shk significantly decreased the mammosphere formation (Fig. 1H, S1G and 2H), ALDH1+ cell and CD44+ CD24− cell loads in vitro (Fig. 2B, S2E and S2H). It also reduced the expression of CSC markers (Oct3/4, Sox2, Nanog, c-Myc and Aldh1) in vivo andin vitro (Fig. 2C,D, S2C and S2D). These genes are known to regulate stem cell programs and in cancer, they are established promoters and regulators of CSC phenotype35, 36, 37, 38, 39, 40. Decrease in the expression of these genes on Shk treatment indicates its potential to suppress CSC programs. Tumor initiating potential (tumorigenicity) is the bona fide measure of CSCs. Reduction in the tumorigenic potential of cells isolated form Shk treated tumors indicates in vivoanti-CSC effects of Shk.
We further demonstrated that Shk is a potent inhibitor of STAT3 and it also inhibits FAK and Src (Fig. 3A–C). Its STAT3 inhibitory property was found to be responsible for its anti-CSC effects (Figs. 6B and 7B). STAT3 and FAK inhibitors are previously known to compromise CSC growth41,42. Here, we found that pharmacological inhibition of STAT3 was more effective in compromising CSC load than FAK and Src inhibitions (Fig. 5A). STAT3 activation through IL6 increases mammosphere formation more significantly than Src and FAK activation through EGF and Fibronectin (Fig. 5C). This indicates that IL6-STAT3 axis is a key regulator of BCSC dynamics.
11.2.3.9 Ovatodiolide Sensitizes Aggressive Breast Cancer Cells to Doxorubicin Anticancer Activity, Eliminates Their Cancer Stem Cell-Like Phenotype, and Reduces Doxorubicin-Associated Toxicity
Investigators evaluated the usability of ovatodiolide (Ova) in sensitizing triple negative breast cancer (TNBC) cells to doxorubicin (Doxo), cytotoxicity, so as to reduce Doxo effective dose and consequently its adverse effects. Ova-sensitized TNBC cells also lost their cancer stem cell-like phenotype evidenced by significant dissolution and necrosis of formed mammospheres, as well as their terminal differentiation. [Cancer Lett]
11.2.3.10 Glabridin Inhibits Cancer Stem Cell-Like Properties of Human Breast Cancer Cells: An Epigenetic Regulation of miR-148a/SMAd2 Signaling
The authors report that glabridin (GLA) attenuated the cancer stem cell (CSC)-like properties through microRNA-148a (miR-148a)/transforming growth factor beta-SMAD2 signal pathway in vitro and in vivo. In MDA-MB-231 and Hs-578T breast cancer cell lines, GLA enhanced the expression of miR-148a through DNA demethylation. [Mol Carcinog]
11.2.3.11 Ginsenoside Rh2 Inhibits Cancer Stem-Like Cells in Skin Squamous Cell Carcinoma
The effects of ginsenoside Rh2 (GRh2) on Lgr5-positive cancer stem cells (CSCs) were determined by flow cytometry and by tumor sphere formation. Scientists found that GRh2 dose-dependently reduced skin squamous cell carcinoma viability, possibly through reduced the number of Lgr5-positive CSCs. [Cell Physiol Biochem]
Liu S. Chen M. Li P. Wu Y. Chang C. Qiu Y. Cao L. Liu Z. Jia C.
Cell Physiol Biochem 2015;36:499-508
http://dx.doi.org:/10.1159/000430115
Background/Aims: Treatments targeting cancer stem cells (CSCs) are most effective cancer therapy, whereas determination of CSCs is challenging. We have recently reported that Lgr5-positive cells are cancer stem cells (CSCs) in human skin squamous cell carcinoma (SCC). Ginsenoside Rh2 (GRh2) has been shown to significantly inhibit growth of some types of cancers, whereas its effects on the SCC have not been examined. Methods: Here, we transduced human SCC cells with lentivirus carrying GFP reporter under Lgr5 promoter. The transduced SCC cells were treated with different doses of GRh2, and then analyzed cell viability by CCK-8 assay and MTT assay. The effects of GRh2 on Lgr5-positive CSCs were determined by fow cytometry and by tumor sphere formation. Autophagy-associated protein and β-catenin were measured by Western blot. Expression of short hairpin small interfering RNA (shRNA) for Atg7 and β-catenin were used to inhibit autophagy and β-catenin signaling pathway, respectively, as loss-of-function experiments. Results: We found that GRh2 dose-dependently reduced SCC viability, possibly through reduced the number of Lgr5-positive CSCs. GRh2 increased autophagy and reduced β-catenin signaling in SCC cells. Inhibition of autophagy abolished the effects of GRh2 on β-catenin and cell viability, while increasing β-catenin abolished the effects of GRh2 on autophagy and cell viability. Conclusion: Taken together, our data suggest that GRh2 inhibited SCC growth, possibly through reduced the number of Lgr5-positive CSCs. This may be conducted through an interaction Carcinoma account for more than 80% of all types of cancer worldwide, and squamous cell carcinoma (SCC) is the most frequent carcinoma. Skin SCC causes a lot of mortality yearly, which requires a better understanding of the molecular carcinogesis of skin SCC for developing efficient therapy [1,2]. Ginsenoside Rh2 (GRh2) is a characterized component in red ginseng, and has proven therapeutic effects on inflammation [3] and a number of cancers [4,5,6,7,8,9,10,11,12,13,14], whereas its effects on the skin SCC have not been examined.
Cancer stem cells (CSCs) are cancer cells with great similarity to normal stem cells, e.g., the ability to give rise to various cell types in a particular cancer [15,16]. CSCs are highly tumorigenic, compared to other non-CSCs. CSCs appear to persist in tumors as a distinct population and CSCs are believed to be responsible for cancer relapse and metastasis after primary tumor resection [15,16,17,18]. Recently, the appreciation of the critical roles of CSCs in cancer therapy have been continuously increasing, although the identification of CSCs in a particular cancer is still challenging.
To date, different cell surface proteins have been used to isolate CSCs from a variety of cancers by flow cytometry. Among these markers for identification of CSCs, the most popular ones are prominin-1 (CD133), side population (SP) and increased activity of aldehyde dehydrogenase (ALDH). CD133 is originally detected in hematopoietic stem cells, endothelial progenitor cells and neuronal and glial stem cells. Later on, CD133 has been shown to be expressed in the CSCs from some tumors [19,20,21,22,23], but with exceptions [24]. SP is a sub-population of cells that efflux chemotherapy drugs, which accounts for the resistance of cancer to chemotherapy. Hoechst (HO) has been experimentally used for isolation of SP cells, while the enrichment of CSCs by SP appears to be limited [25]. Increased activity of ALDH, a detoxifying enzyme responsible for the oxidation of intracellular aldehydes [26,27], has also been used to identify CSCs, using aldefluor assay [28,29]. However, ALDH has also been detected in other cell types, which creates doubts on the purity of CSCs using ALDH method [30,31]. Moreover, all these methods appear to be lack of cancer specificity.
The Wnt target gene Lgr5 has been recently identified as a stem cell marker of the intestinal epithelium, and of the hair follicle [32,33]. Recently, we reported that Lgr5 may be a potential CSC marker for skin SCC [34]. We detected extremely high Lgr5 levels in the resected skin SCC specimen from the patients. In vitro, Lgr5-positive SCC cells grew significantly faster than Lgr5-negative cells, and the fold increase in growth of Lgr5-positive vs Lgr5-negative cells is significantly higher than SP vs non-SP, or ALDH-high vs ALDH-low, or CD133-positive vs CD133-negative cells. Elimination of Lgr5-positive SCC cells completely inhibited cancer cell growth in vitro.
Here, we transduced human SCC cells with lentivirus carrying GFP reporter under Lgr5 promoter. The transduced SCC cells were treated with different doses of GRh2, and then analyzed cell viability by CCK-8 assay and MTT assay. The effects of GRh2 on Lgr5-positive CSCs were determined by flow cytometry and by tumor sphere formation. Autophagy-associated protein and β-catenin were measured by Western blot. Expression of short hairpin small interfering RNA (shRNA) for autophagy-related protein 7 (Atg7) and β-catenin were used to inhibit autophagy and β-catenin signaling pathway, respectively, as loss-of-function experiments. Atg7 was identified based on homology to Pichia pastoris GSA7 and Saccharomyces cerevisiae APG7. In the yeast, the protein appears to be required for fusion of peroxisomal and vacuolar membranes. The protein shows homology to the ATP-binding and catalytic sites of the E1 ubiquitin activating enzymes. Atg7 is a mediator of autophagosomal biogenesis, and is a putative regulator of autophagic function [35,36,37,38]. We found that GRh2 dose-dependently reduced SCC viability, possibly through reduced the number of Lgr5-positive CSCs. GRh2 increased autophagy and reduced β-catenin signaling in SCC cells. Inhibition of autophagy abolished the effects of GRh2 on β-catenin and cell viability, while increasing β-catenin abolished the effects of GRh2 on autophagy and cell viability.
Transduction of SCC cells with GFP under Lgr5 promoter
We have recently shown that Lgr5 is CSC marker for skin SCC [34]. In order to examine the role of GRh2 on SCC cells, as well as a possible effect on CSCs, we transduced human skin SCC cells A431 [34] with a lentivirus carrying GFP reporter under Lgr5 promoter (Fig. 1A). The Lgr5-positive cells were green fluorescent in culture (Fig. 1B), and could be analyzed or isolated by flow cytometry, based on GFP (Fig. 1C).
(not shown)
Fig. 1. Transduction of SCC cells with GFP under Lgr5 promoter. (A) The structure of lentivirus carrying GFP reporter under Lgr5 promoter. (B) The pLgr5-GFP-transduced A431 cells in culture. Lgr5-positive cells were green fluorescent. Nuclear staining was done by DAPI. (C) Representative flow chart for analyzing pLgr5-GFP-transduced A431 cells by flow cytometry based on GFP. Gated cells were Lgr5-positive cells. Scar bar is 20µm.
GRh2 dose-dependently inhibits SCC cell growth
Then, we examined the effect of GRh2 on the viability of SCC cells. We gave GRh2 at different doses (0.01mg/ml, 0.1mg/ml and 1mg/ml) to the cultured pLgr5-GFP-transduced A431 cells. We found that from 0.01mg/ml to 1mg/ml, GRh2 dose-dependently deceased the cell viability in either a CCK-8 assay (Fig. 2A), or a MTT assay (Fig. 2B). Next, we questioned whether GRh2 may have a specific effect on CSCs in SCC cells. Thus, we analyzed GFP+ cells, which represent Lgr5-positive CSCs in pLgr5-GFP-transduced A431 cells after GRh2 treatment. We found that GRh2 dose-dependently deceased the percentage of GFP+ cells, by representative flow charts (Fig. 2C), and by quantification (Fig. 2D). We also examined the capability of the GRh2-treated cells in the formation of tumor sphere. We found that GRh2 dose-dependently deceased the formation of tumor sphere-like structure, by quantification (Fig. 2E), and by representative images (Fig. 2F). Together, these data suggest that GRh2 dose-dependently inhibited SCC cell growth, possibly through inhibition of CSCs.
Fig. 2. GRh2 dose-dependently inhibits SCC cell growth. We gave GRh2 at different doses (0.01mg/ml, 0.1mg/ml and 1mg/ml) to the cultured pLgr5-GFP-transduced A431 cells. (A-B) GRh2 dose-dependently deceased the cell viability in either a CCK-8 assay (A), or a MTT assay (B). (C-D) GFP+ cells after GRh2 treatment were analyzed by flow cytometry, showing that GRh2 dose-dependently deceased the percentage of GFP+ cells, by representative flow charts (C), and by quantification (D). The capability of the GRh2-treated cells to form tumor sphere-like structures was examined, shown by quantification (E), and by representative images (F). *p
http://www.karger.com/Article/ShowPic/430115?image=000430115_f02.JPG
GRh2 treatment decreases β-catenin and increases autophagy in SCC cells
We analyzed the molecular mechanisms underlying the cancer inhibitory effects of GRh2 on SCC cells. We thus examined the growth-regulatory proteins in SCC. From a variety of proteins, we found that GRh2 treatment dose-dependently decreases β-catenin, and dose-dependently upregulated autophagy-related proteins Beclin, Atg7 and increased the ratio of LC3 II to LC3 I, by quantification (Fig. 3A), and by representative Western blots (Fig.3B). Since β-catenin signaling is a strong cell-growth stimulator and autophagy can usually lead to stop of cell-growth and cell death, we feel that the alteration in these pathways may be responsible for the GRh2-mediated suppression of SCC growth.
(not shown)
Figure 3. GRh2 treatment decreases β-catenin and increases autophagy in SCC cells.
http://www.karger.com/Article/ShowPic/430115?image=000430115_f03.JPG
Inhibition of autophagy abolishes the effects of GRh2 on β-catenin
In order to find out the relationship between β-catenin and autophagy in this model, we inhibited autophagy using a shRNA for Atg7, and examined its effect on the changes of β-catenin by GRh2. First, the inhibition of Atg7 in A431 cells by shAtg7 was confirmed by RT-qPCR (Fig. 4A), and by Western blot (Fig. 4B). Inhibition of Atg7 resulted in abolishment of the effects of GRh2 on other autophagy-associated proteins (Fig. 4B), and resulted in abolishment of the inhibitory effect of GRh2 on β-catenin (Fig. 4B). Moreover, the effects of GRh2 on cell viability were completely inhibited (Fig. 4C). Together, inhibition of autophagy abolishes the effects of GRh2 on β-catenin. Thus, the regulation of GRh2 on β-catenin needs autophagy-associated proteins.
Fig. 4. Inhibition of autophagy abolishes the effects of GRh2 on β-catenin.
A431 cells were transfected with shRNA for Atg7, or scrambled sequence (scr) as a control. (A) RT-qPCR for Atg7. (B) Quantification of β-catenin, Beclin, Atg7 and LC3 by Western blot. (C) Cell viability by CCK-8 assay. *p
http://www.karger.com/Article/ShowPic/430115?image=000430115_f04.JPG
Overexpression of β-catenin abolishes the effects of GRh2 on autophagy
Next, we inhibited the effects of GRh2 on β-catenin by overexpression of β-catenin in A431 cells. First, the overexpression of β-catenin in A431 cells was confirmed by RT-qPCR (Fig. 5A), and by Western blot (Fig. 5B). Overexpression of β-catenin resulted in abolishment of the effects of GRh2 on autophagy-associated proteins (Fig. 5B). Moreover, the effects of GRh2 on cell viability were completely inhibited (Fig. 5C). Together, inhibition of β-catenin signaling abolishes the effects of GRh2 on autophagy. Thus, the regulation of GRh2 on autophagy needs β-catenin signaling. This model is thus summarized in a schematic (Fig. 6), suggesting that GRh2 may target both β-catenin signaling and autophagy, which interacts with each other in the regulation of SCC cell viability and growth.
http://www.karger.com/Article/ShowPic/430115?image=000430115_f05.JPG
Fig. 5. Overexpression of β-catenin abolishes the effects of GRh2 on autophagy. A431 cells were transfected with β-catenin, or scrambled sequence (scr) as a control. (A) RT-qPCR for β-catenin. (B) Quantification of β-catenin, Beclin, Atg7 and LC3 by Western blot. (C) Cell viability by CCK-8 assay. *p
http://www.karger.com/Article/ShowPic/430115?image=000430115_f06.JPG
Fig. 6. Schematic of the model. GRh2 may target both β-catenin signaling and autophagy, which interacts with each other in the regulation of SCC cell viability and growth.
Understanding the cancer molecular biology of skin SCC and identification of an effective treatment are both critical for improving the current therapy [1]. Lgr5 has been recently identified as a novel stem cell marker of the intestinal epithelium and the hair follicle, in which Lgr5 is expressed in actively cycling cells [32,33]. Moreover, we recently showed that Lgr5-positive are CSCs in skin SCC [34]. Thus, specific targeting Lgr5-positive cells may be a promising therapy for skin SCC.
In the current study, we analyzed the effects of GRh2 on the viability of SCC. Importantly, we not only found that GRh2 dose-dependently decreases SCC cell viability, but also dose-dependently decreased the number of Lgr5-positive CSCs in SCC cells. These data suggest that the CSCs in SCC may be more susceptible for the GRh2 treatment, and the decreases in CSCs may result in the decreased viability in total SCC cells. This point was supported by following mechanism studies. Activated β-catenin signaling by WNT/GSK3β prevents degradation of β-catenin and induces its nuclear translocation [39]. Nuclear β-catenin thus activates c-myc, cyclinD1 and c-jun to promote cell proliferation, and activates Bcl-2 to inhibit apoptosis [39]. High β-catenin levels thus are a signature of CSCs. Therefore, it is not surprising that CSCs are more affected than other cells when GRh2 targets β-catenin signaling.
In addition, GRh2 appears to target autophagy. Although altered metabolism may be beneficial to the cancer cells, it can create an increased demand for nutrients to support cell growth and proliferation, which creates metabolic stress and subsequently induces autophagy, a catabolic process leading to degradation of cellular components through the lysosomal system [40]. Cancer cells use autophagy as a survival strategy to provide essential biomolecules that are required for cell viability under metabolic stress [40]. However, autophagy not only results in a staring in cell growth, but also may result in cell death [40]. Increases in autophagy may substantially decrease cancer cell growth. Thus, GRh2 has its inhibitory effect on skin SCC cells through a combined effect on cell proliferation (by decreasing β-catenin) and autophagy [40].
Interestingly, our data suggest an interaction between β-catenin and autophagy. This finding is consistent with previous reports showing that autophagy negatively modulates Wnt/β-catenin signaling by promoting Dvl instability [41,42], and with other studies showing that β-catenin regulates autophagy [38,43,44].
Of note, we have checked other SCC lines and essentially got same results. Together with our previous reports showing that Lgr5-positive cells are CSCs in skin SCC [34], these findings thus highlight a future engagement of Lgr5-directed GRh2 therapy, which could be performed in a sufficiently frequent manner, to substantially improve the current treatment for skin SCC.
Normal vs Cancer Thyroid Stem Cells: The Road to Transformation
The authors discuss new insights into thyroid stem cells as a potential source of cancer formation in light of the available information on the oncogenic role of genetic modifications that occur during thyroid cancer development. Understanding the fine mechanisms that regulate tumor transformation may provide new ground for clinical intervention in terms of prevention, diagnosis and therapy. [Oncogene] Abstract |
|
Cancer Stem Cells: A Potential Target for Cancer Therapy
The identification of cancer stem cells (CSCs) and a better understanding of the complex characteristics of CSCs will provide invaluable diagnostic, therapeutic and prognostic targets for clinical application. The authors introduce the dysregulated properties of CSCs in cancers and discuss the possible challenges in targeting CSCs for cancer treatment. [Cell Mol Life Sci] Abstract |
|
Targeting Cancer Stem Cells Using Immunologic Approaches
Wicha, M; Chang, A; Yingxin, X; Xiaolian, Z; Ning, N; Liu, Shuang, Q, L; Pan, Q |
Stem Cells |
2015-04-15 |
4.15 | Apr 22 |
Targeting Notch, Hedgehog, and Wnt Pathways in Cancer Stem Cells: Clinical Update
Ivy, P; Takebe, N |
Nat Rev Clin Oncol |
2015-04-07 |
4.14 | Apr 15 |
Hypoxia-Inducible Factors in Cancer Stem Cells and Inflammation
Liu, Y; Peng, G |
Trends Pharmacol Sci |
2015-04-06 |
4.14 | Apr 15 |
NANOG in Cancer Stem Cells and Tumor Development: An Update and Outstanding Questions
Tang, D; Chao, HP; Wang, J; Yang, Tao; Jeter, C |
Stem Cells |
2015-03-26 |
4.12 | Apr 1 |
Two Genes Control Breast Cancer Stem Cell Proliferation and Tumor Properties
When mothers breastfeed their babies, they depend upon a unique interaction of genes and hormones to produce milk and deliver it to their hungry little tyke. Unfortunately, this same cocktail of genes and hormones can also lead to breast cancer, especially if the mother has her first pregnancy after age 30.
A medical research group at the Medical College of Georgia at Georgia Regents University has established that a gene called DNMT1 plays a central role in the maintenance of the breast (mammary gland) stem cells that enable normal rapid growth of the breasts during pregnancy. This same gene, however, can also maintain those cancer stem cells that enable breast cancer. According to their work, the DNMT1 gene is highly expressed in the most common types of breast cancer.
Also, another gene called ISL1, which encodes a protein that puts the brakes on the growth of breast stem cells, is nearly silent in the breasts during pregnancy and in breast cancer stem cells.
Dr. Muthusamy Thangaraju, a biochemist at the Medical College of Georgia, who is the corresponding author of this study, which was published in the journal Nature Communications, said, “DNMT1 directly regulates ISL1. If the DNMT1 expression is high, this ISL1 gene is low.” Thangaraju and his team first observed the connection between DNMT1 and ISL1 when they knocked out the DNMT1 gene mice and noted an increase in the expression of ISL1. These results inspired them to examine the relationship of these two genes in human breast cancer cells.
Thangaraju and his co-workers discovered that ISL1 is silent in most human breast cancers. Furthermore, they demonstrated that restoring higher levels of ISL1 to human breast cancer cells dramatically reduced cancer stem cell populations, the growth of these cells, and their ability to spread throughout the tissue; all of which are hallmarks of cancer.
Conversely, Thangaraju and his team knocked out the DNMT1 gene in a breast-cancer mouse model, the breast will not develop as well. However, according to Thangaraju, this same deletion will also prevent the formation of about 80 percent of breast tumors. In fact, DNMT1 also down-graded super-aggressive, triple-negative breast cancers, which are negative for the estrogen receptor (ER-), progesterone receptor (PR-), and HER2 (HER2-).
The findings from this work also point toward new therapeutic targets for breast cancer and new strategies to diagnose early breast cancer. For example, a blood test for ISL1 might provide a marker for the presence of early breast cancer. Additionally, the anti-seizure medication valproic acid is presently being used in combination with chemotherapy to treat breast cancer, and this drug increases the expression of ISL1. This might explain why valproic acid works for these patients, according to Thangaraju. Workers in Thangaraju’s laboratory are already screening other small molecules that might work as well or better than valproic acid.
Mammary stem cells maintain the breasts during puberty as well as pregnancy, which are both periods of dynamic breast cell growth. During pregnancy, breasts may generate 300 times more cells as they prepare for milk production. Unfortunately, these increased levels of cell growth might also include the production of tumor cells, and the mutations that lead to breast cancer increase in frequency with age. If the developing fetus dies before she comes to term, immature breast cells that were destined to become mature mammary gland cells can more easily become cancer, according to Rajneesh Pathania, a GRU graduate student who is the first author of this study.
DNMT1 is essential for maintaining a variety of stem cell types, such as hematopoietic stem cells, which produce all types of blood cells. However, the role of DNMT1 in the regulation of breast-specific stem cells that make mammary gland tissue and may enable breast cancer has not been studied to this point.
For reasons that are unclear, there is an increased risk of breast cancer if the first pregnancy occurs after age 30 or if mothers lose their baby during pregnancy or have an abortion. Women who never have children also are at increased risk, but multiple term pregnancies further decrease the risk, according to data compiled and analyzed by the American Cancer Society.
Theories to explain these phenomena include the coupling of the hormone-induced maturation of breast cells that occurs during pregnancy with an increase in the potential to produce breast cancer stem cells. Most breast cancers thrive on estrogen and progesterone, which are both highly expressed during pregnancy and help fuel stem cell growth. During pregnancy, stem cells also divide extensively and as their population increases, DNMT1 levels also increase.
In five different types of human breast cancer, researchers found high levels of DNMT1 and ISL1 turned off. Even in a laboratory dish, when they reestablished normal expression levels of ISL1, human breast cancer cells and stem cell activity were much reduced, Thangaraju said.
Like this:
Like Loading...
Read Full Post »






















 : 0.74 and 0.70, respectively). Expression of p16INK4a was observed in all endometrial biopsies. Compared with Ki-67 expression and detection of high-risk human papillomavirus, p16INK4a was less likely to be positive in samples from women with negative, reactive, and atypical biopsies. Although expression of p16INK4ain endometrial epithelium may be problematic in terms of screening, the potential of p16INK4a as a screening test warrants investigation.
: 0.74 and 0.70, respectively). Expression of p16INK4a was observed in all endometrial biopsies. Compared with Ki-67 expression and detection of high-risk human papillomavirus, p16INK4a was less likely to be positive in samples from women with negative, reactive, and atypical biopsies. Although expression of p16INK4ain endometrial epithelium may be problematic in terms of screening, the potential of p16INK4a as a screening test warrants investigation. , and for analysis was grouped into the negative category. For Ki-67, the results were also reported in a semiquantitative fashion as cells in the lower 1/3 of the epithelium staining (i.e., usually basilar cell staining), cells in the middle 1/3–2/3 staining, or cells in the upper 1/3 staining (
, and for analysis was grouped into the negative category. For Ki-67, the results were also reported in a semiquantitative fashion as cells in the lower 1/3 of the epithelium staining (i.e., usually basilar cell staining), cells in the middle 1/3–2/3 staining, or cells in the upper 1/3 staining ( 1+ staining (24 of 208 -original diagnosis, 12 of 112 recut diagnosis). 57% of the CIN I cases had
1+ staining (24 of 208 -original diagnosis, 12 of 112 recut diagnosis). 57% of the CIN I cases had 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
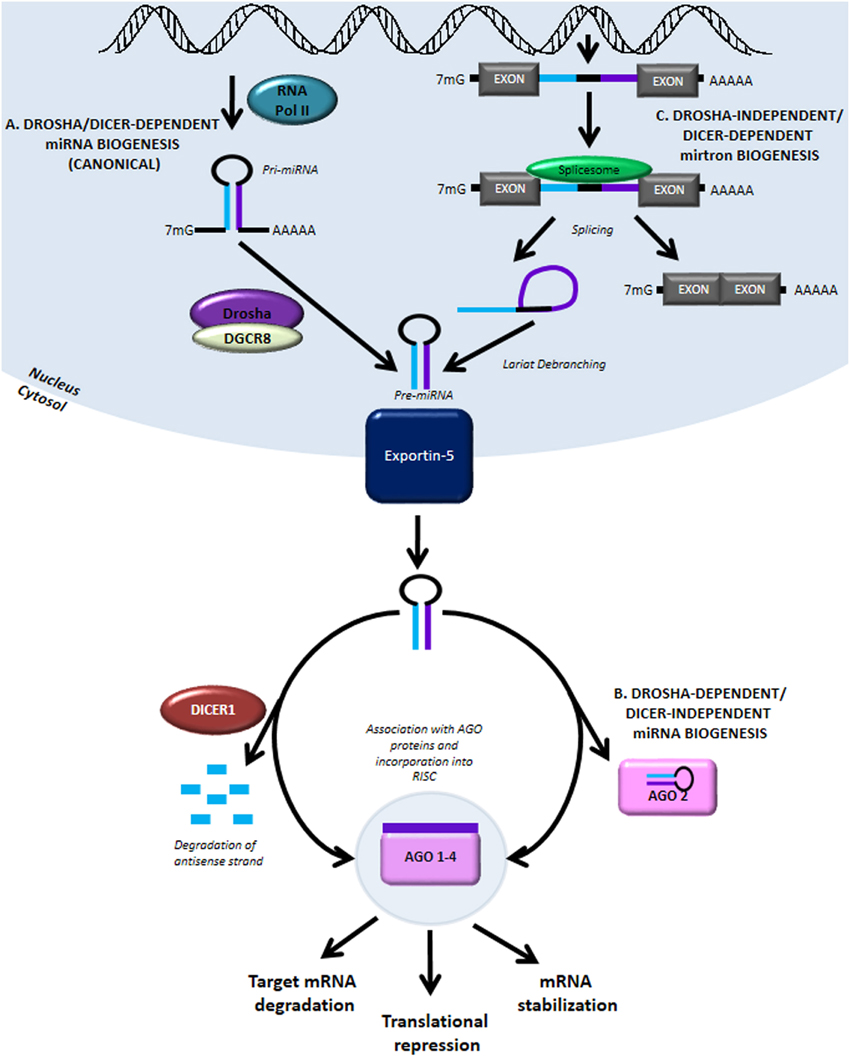{kind=link}
{kind=link}
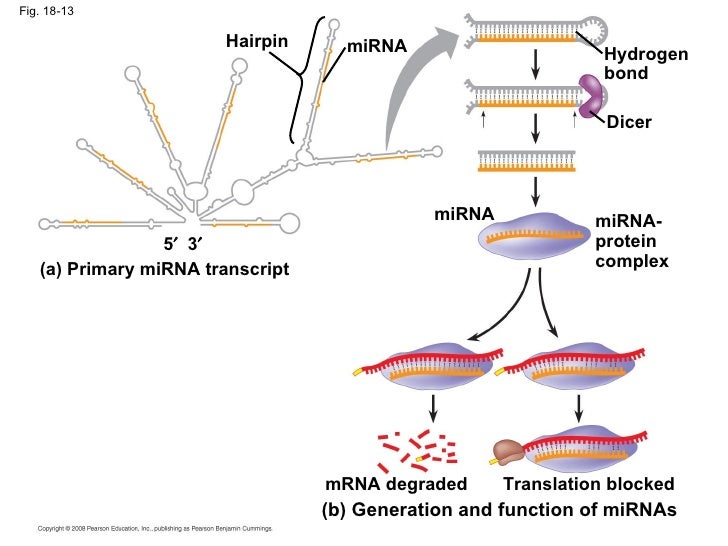{kind=link}
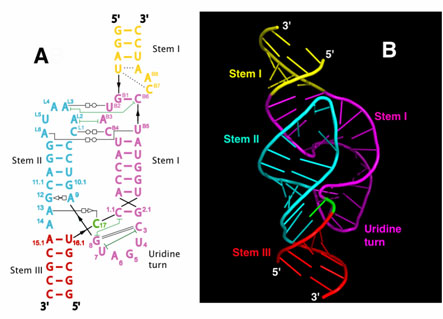{kind=link}
{kind=link}
{kind=link}
{kind=link}
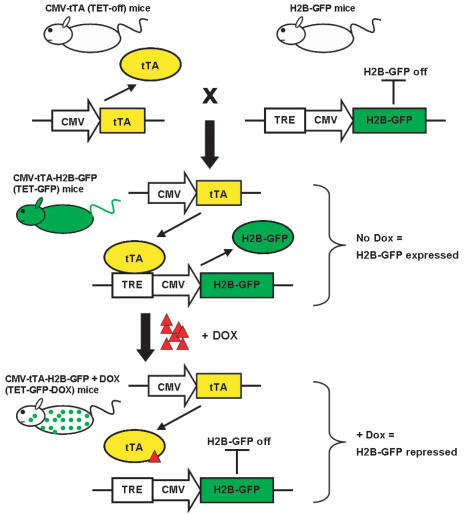{kind=link}
{kind=link}