Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Why do some people with COVID-19 get sicker than others? Maybe exposure to a particularly high dose of the causative virus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), accounts for the difference. Perhaps deficiencies in diet, exercise, or sleep contribute to worse illness. Although many factors govern how sick people become, a key driver of the severity of COVID-19 appears to be genetic, which is common for other human viruses and infectious agents (1). On page 579 of this issue, Wickenhagen et al. (2) show that susceptibility to severe COVID-19 is associated with a single-nucleotide polymorphism (SNP) in the human gene 2′-5′-oligoadenylate synthetase 1 (OAS1).The authors reasoned that SARS-CoV-2 should be inhibited by interferon-mediated antiviral responses, which are among the first cellular defense mechanisms produced in response to a viral infection. Interferons are a group of cytokines that induce the transcription of a large cadre of genes, many of which encode proteins with the potential to directly inhibit the invading virus. Wickenhagen et al. interrogated many hundreds of these putative antiviral proteins for their ability to suppress SARS-CoV-2 in cultured cells and found that OAS1 was particularly potent against SARS-CoV-2.OAS1 is an enzyme that is activated in the presence of double-stranded RNA, which is scattered along an otherwise singlestranded SARS-CoV-2 genome because of an assortment of RNA hairpins and other secondary structures. Once activated, OAS1 catalyzes the polymerization of adenosine triphosphate (ATP) into a second messenger, 2′-5′-oligoadenylate. This then triggers the conversion of ribonuclease L (RNaseL) into its active form so that it can cleave viral RNA, effectively blunting viral replication (3). Wickenhagen et al. found that OAS1 is expressed in respiratory tissues of healthy donors and COVID-19 patients and that it interacts with a region of the SARS-CoV-2 genome that contains double-stranded RNA secondary structures (see the figure).OAS1 exists predominantly as two isoforms in humans—a longer isoform (p46) and a shorter version (p42). Genetic variation dictates which isoform will be expressed. In humans, p46 is expressed in people who have a SNP that causes alternative splicing of the OAS1 messenger RNA (mRNA). This results in the utilization of a terminal exon that is not used to translate p42. Thus, the carboxyl terminus of the p46 OAS1 protein contains a distinct four–amino acid motif that forms a prenylation site. Prenylation is a posttranslational modification that targets proteins to membranes. In cell culture experiments, Wickenhagen et al. showed that only OAS1 p46, but not p42, could inhibit SARS-CoV-2. However, when the prenylation site of p46 was engineered into p42, this chimeric p42 protein was able to inhibit SARS-CoV-2, which strongly implicates a role for OAS1 specifically at membranes.Why are membranes important? SARS-CoV-2, like all coronaviruses, co-opts cellular membranes at the endoplasmic reticulum to form double-membrane vesicles, in which the virus replicates its genome. Thus, membrane-bound OAS1 p46 may be specifically activated by RNA viruses that form membrane-bound vesicles for replication. Indeed, the unrelated cardiovirus A, which also forms vesicular membranous structures, was inhibited by OAS1. Conversely, other respiratory RNA viruses, such as human parainfluenza virus type 3 and human respiratory syncytial virus, which do not use membrane-tethered vesicles for replication, were not inhibited by p46.Wickenhagen et al. examined a cohort of 499 COVID-19 patients hospitalized in the UK. Whereas all patients expressed OAS1, 42.5% of them did not express the antiviral p46 isoform. These patients were statistically more likely to have severe COVID-19 (be admitted to the intensive care unit). This suggests that OAS1 is an important antiviral factor in the control of SARS-CoV-2 infection and that its inability to activate RNaseL results in prolonged infections and severe disease, although other factors likely contribute. The authors also examined animals known to harbor different coronaviruses. They found evidence for prenylated OAS1 proteins in mice, cows, and camels. Notably, horseshoe bats, which are considered a possible reservoir for SARS-related coronaviruses (4), lack a prenylation motif in their OAS1 because of genomic changes that eliminated the critical four-amino acid motif. A horseshoe bat (Rhinolophus ferrumequinum) OAS1 was unable to inhibit SARS-CoV-2 infection in cell culture. Conversely, the black flying fox (Pteropus alecto)—a pteropid bat that is a reservoir for the Nipah and Hendra viruses, which can also infect humans—possesses a prenylated OAS1 that can inhibit SARS-CoV-2. These findings indicate that horseshoe bats may be genetically and evolutionarily primed to be optimal reservoir hosts for certain coronaviruses, like SARS-CoV-2.Other studies have now shown that the p46 OAS1 variant, which resides in a genomic locus inherited from Neanderthals (5–7), correlates with protection from COVID-19 severity in various populations (8, 9). These findings mirror previous studies indicating that outcomes with West Nile virus (10) and hepatitis C virus (11) infection, both of which also use membrane vesicles for replication, are also associated with genetic variation at the human OAS1 locus. Another elegant functional study complements the findings of Wickenhagen et al. by also demonstrating that prenylated OAS1 inhibits multiple viruses, including SARS-CoV-2, and is associated with protection from severe COVID-19 in patients (12).There is a growing body of evidence that provides critical understanding of how human genetic variation shapes the outcome of infectious diseases like COVID-19. In addition to OAS1, genetic variation in another viral RNA sensor, Toll-like receptor 7 (TLR7), is associated with severe COVID-19 (13–15). The effects appear to be exclusive to males, because TLR7 is on the X chromosome, so inherited deleterious mutations in TLR7 therefore result in immune cells that fail to produce normal amounts of interferon, which correlates with more severe COVID-19. Our knowledge of the host cellular factors that control SARS-CoV-2 is rapidly increasing. These findings will undoubtedly open new avenues into SARS-CoV-2 antiviral immunity and may also be beneficial for the development of strategies to treat or prevent severe COVID-19.
Degrading viral RNAOnce inside a host cell, coronaviruses form double-membrane vesicles (DMVs) to replicate their RNA genome. When anchored to membranes, 2′-5′-oligoadenylate synthetase 1 (OAS1) detects double-stranded RNA (dsRNA) secondary structure and activates ribonuclease L (RNaseL), which degrades viral RNA. The OAS1 p42 isoform lacks the prenylation motif, so it is not membrane bound and RNaseL is not activated, leading to unrestrained viral replication and correlating with severe COVID-19.GRAPHIC: KELLIE HOLOSKI/SCIENCE Source: Shroggins SCIENCE
28 Oct 2021
Vol 374, Issue 6567
pp. 535-536
DOI: 10.1126/science.abm3921
Non-toxic antiviral nanoparticles with a broad spectrum of virus inhibition
Curator and Reporter: Dr. Premalata Pati, Ph.D., Postdoc
Non-toxic antiviral nanoparticles with a broad spectrum of virus inhibition
Infectious diseases account for 20% of global deaths, with viruses accounting for over a third of these deaths (1). Lower respiratory effects and human immunodeficiency viruses (HIV) are among the top ten causes of death worldwide, both of which contribute significantly to health-care costs (2). Every year, new viruses (such as Ebola) increase the mortality toll. Vaccinations are the most effective method of avoiding viral infections, but there are only a few of them, and they are not available in all parts of the world (3). After infection, antiviral medications are the only option; unfortunately, only a limited number of antiviral medications are approved in this condition. Antiviral drugs on a big scale that can influence a wide spectrum of existing and emerging viruses are critical.
The three types of treatments currently available are small molecules (such as nucleoside analogues and peptidomimetics), proteins that stimulate the immune system (such as interferon), and oligonucleotides (for example, fomivirsen). The primary priorities include HIV, hepatitis B and C viruses, Herpes Simplex Virus (HSV), human cytomegalovirus (HCMV), and influenza virus. They work mainly on viral enzymes, which are necessary for viral replication but which differ from other host enzymes to ensure selective function. The specificity of antivirals is far from perfect because viruses rely on the biosynthesis machinery for reproduction of infected cells, which results in a widespread and inherent toxicity associated with such therapy. However, most viruses mutate rapidly due to their improper replicating mechanisms and so often develop resistance (4). Finally, since antiviral substances are targeted at viral proteins, it is challenging to build broad-based antivirals that can act with a wide range of phylogenetic and structurally different virus.
Over the last decade breakthroughs in nanotechnology have led to scientists developing incredibly specialized nanoparticles capable of traveling in specific cells through a human body. A broad spectrum of destructive viruses is being targeted and not only bind to, but also destroy, by modern computer modeling technology.
An international team of researchers led by the University of Illinois at Chicago chemistry professor Petr Kral developed novel anti-viral nanoparticles that bind to a variety of viruses, including herpes simplex virus, human papillomavirus, respiratory syncytial virus, Dengue, and lentiviruses. In contrast to conventional broad-spectrum antivirals, which just prevent viruses from invading cells, the new nanoparticles eradicate viruses. The team’s findings have been published in the journal “Nature Materials.”
The goal of this new study was to create a new anti-viral nanoparticle that could exploit the HSPG binding process to not only tightly attach with virus particles but also to destroy them. The work was done by a group of researchers ranging from biochemists to computer modeling experts until the team came up with a successful nanoparticle design that could, in principle, accurately target and kill individual virus particles.
The first step to combat many viruses consists in the attachment of heparin sulfate proteoglycan on cell surfaces to a protein (HSPG). Some of the antiviral medications already in place prevent an infection by imitating HSPG’s connection to the virus. An important constraint of these antivirals is that not only is this antiviral interaction weak, it does not kill the virus.
Kral said
We knew how the nanoparticles should bind on the overall composition of HSPG binding viral domains and the structures of the nanoparticles, but we did not realize why the various nanoparticles act so differently in terms of their both bond strength and viral entry in cells
Kral and colleagues assisted in resolving these challenges and guiding the experimentalists in fine-tuning the nanoparticle design so that it performed better.
The researchers have employed advanced computer modeling techniques to build exact structures of several target viruses and nanoparticles up to the atom’s position. A profound grasp of the interactions between individual atom groupings in viruses and nanoparticles allows the scientists to evaluate the strength and duration of prospective links between these two entities and to forecast how the bond could change over time and eventually kill the virus.
Atomistic MD simulations of an L1 pentamer of HPV capsid protein with the small NP (2.4 nm core, 100 MUP ligands). The NP and the protein are shown by van der Waals (vdW) and ribbon representations respectively. In the protein, the HSPG binding amino acids are displayed by vdW representation.
Kral added
We were capable of providing the design team with the data needed to construct a prototype of an antiviral of high efficiency and security, which may be utilized to save lives
The team has conducted several in vitro experiments following the development of a prototype nanoparticle design which have demonstrated success in binding and eventually destroying a wide spectrum of viruses, including herpes simplex, human papillomaviruses, respiratory syncytial viruses and dengue and lentiviruses.
The research is still in its early phases, and further in vivo animal testing is needed to confirm the nanoparticles’ safety, but this is a promising new road toward efficient antiviral therapies that could save millions of people from devastating virus infections each year.
Cagno, V., Andreozzi, P., D’Alicarnasso, M., Silva, P. J., Mueller, M., Galloux, M., … & Stellacci, F. (2018). Broad-spectrum non-toxic antiviral nanoparticles with a virucidal inhibition mechanism. Nature materials, 17(2), 195-203. https://www.nature.com/articles/nmat5053
Other Related Articles published in this Open Access Online Scientific Journal include the following:
Rare earth-doped nanoparticles applications in biological imaging and tumor treatment
Cryo-EM disclosed how the D614G mutation changes SARS-CoV-2 spike protein structure.
Reporter: Dr. Premalata Pati, Ph.D., Postdoc
SARS-CoV-2, the virus that causes COVID-19, has had a major impact on human health globally; infecting a massive quantity of people around 136,046,262 (John Hopkins University); causing severe disease and associated long-term health sequelae; resulting in death and excess mortality, especially among older and prone populations; altering routine healthcare services; disruptions to travel, trade, education, and many other societal functions; and more broadly having a negative impact on peoples physical and mental health.
It’s need of the hour to answer the questions like what allows the variants of SARS-CoV-2 first detected in the UK, South Africa, and Brazil to spread so quickly? How can current COVID-19 vaccines better protect against them?
Bing Chen, HMS professor of pediatrics at Boston Children’s, and colleagues analyzed the changes in the structure of the spike proteins with the genetic change by D614G mutation by all three variants. Hence they assessed the structure of the coronavirus spike protein down to the atomic level and revealed the reason for the quick spreading of these variants.
This model shows the structure of the spike protein in its closed configuration, in its original D614 form (left) and its mutant form (G614). In the mutant spike protein, the 630 loop (in red) stabilizes the spike, preventing it from flipping open prematurely and rendering SARS-CoV-2 more infectious.
Fig. 1. Cryo-EM structures of the full-length SARS-CoV-2 S protein carrying G614.
(A) Three structures of the G614 S trimer, representing a closed, three RBD-down conformation, an RBD-intermediate conformation and a one RBD-up conformation, were modeled based on corresponding cryo-EM density maps at 3.1-3.5Å resolution. Three protomers (a, b, c) are colored in red, blue and green, respectively. RBD locations are indicated. (B) Top views of superposition of three structures of the G614 S in (A) in ribbon representation with the structure of the prefusion trimer of the D614 S (PDB ID: 6XR8), shown in yellow. NTD and RBD of each protomer are indicated. Side views of the superposition are shown in fig. S8.
The mutant spikes were imaged by Cryo-Electron microscopy (cryo-EM), which has resolution down to the atomic level. They found that the D614G mutation (substitution of in a single amino acid “letter” in the genetic code for the spike protein) makes the spike more stable as compared with the original SARS-CoV-2 virus. As a result, more functional spikes are available to bind to our cells’ ACE2 receptors, making the virus more contagious.
Fig. 2. Cryo-EM revealed how the D614G mutation changes SARS-CoV-2 spike protein structure.
Say the original virus has 100 spikes,” Chen explained. “Because of the shape instability, you may have just 50 percent of them functional. In the G614 variants, you may have 90 percent that is functional. So even though they don’t bind as well, the chances are greater and you will have an infection
Forthcoming directions by Bing Chen and Team
The findings suggest the current approved COVID-19 vaccines and any vaccines in the works should include the genetic code for this mutation. Chen has quoted:
Since most of the vaccines so far—including the Moderna, Pfizer–BioNTech, Johnson & Johnson, and AstraZeneca vaccines are based on the original spike protein, adding the D614G mutation could make the vaccines better able to elicit protective neutralizing antibodies against the viral variants
Chen proposes that redesigned vaccines incorporate the code for this mutant spike protein. He believes the more stable spike shape should make any vaccine based on the spike more likely to elicit protective antibodies. Chen also has his sights set on therapeutics. He and his colleagues are further applying structural biology to better understand how SARS-CoV-2 binds to the ACE2 receptor. That could point the way to drugs that would block the virus from gaining entry to our cells.
In January, the team showed that a structurally engineered “decoy” ACE2 protein binds to SARS-CoV-2 200 times more strongly than the body’s own ACE2. The decoy potently inhibited the virus in cell culture, suggesting it could be an anti-COVID-19 treatment. Chen is now working to advance this research into animal models.
Main Source:
Abstract
Substitution for aspartic acid by glycine at position 614 in the spike (S) protein of severe acute respiratory syndrome coronavirus 2 appears to facilitate rapid viral spread. The G614 strain and its recent variants are now the dominant circulating forms. We report here cryo-EM structures of a full-length G614 S trimer, which adopts three distinct prefusion conformations differing primarily by the position of one receptor-binding domain. A loop disordered in the D614 S trimer wedges between domains within a protomer in the G614 spike. This added interaction appears to prevent premature dissociation of the G614 trimer, effectively increasing the number of functional spikes and enhancing infectivity, and to modulate structural rearrangements for membrane fusion. These findings extend our understanding of viral entry and suggest an improved immunogen for vaccine development.
Comparing COVID-19 Vaccine Schedule Combinations, or “Com-COV” – First-of-its-Kind Study will explore the Impact of using eight different Combinations of Doses and Dosing Intervals for Different COVID-19 Vaccines
From Cell Press: New Insights on the D614G Strain of COVID: Will a New Mutated Strain Delay Vaccine Development?
Reporter: Stephen J. Williams, PhD
Two recent articles in Cell Press, both peer reviewed, discuss the emergence and potential dominance of a new mutated strain of COVID-19, in which the spike protein harbors a D614G mutation.
In the first article “Making Sense of Mutation: What D614G means for the COVID-19 pandemic Remains Unclear”[1] , authors Drs. Nathan Grubaugh, William Hanage, and Angela Rasmussen discuss the recent findings by Korber et al. 2020 [2] which describe the potential increases in infectivity and mortality of this new mutant compared to the parent strain of SARS-CoV2. For completeness sake I will post this article as to not defer from their interpretations of this important paper by Korber and to offer some counter opinion to some articles which have surfaced this morning in the news.
Making sense of mutation: what D614G means for the COVID-19 pandemic remains unclear
Nathan D. Grubaugh1 *, William P. Hanage2 *, Angela L. Rasmussen3 * 1Department of Epidemiology of Microbial Diseases, Yale School of Public Health, New Haven, CT 06510, USA 2Center for Communicable Disease Dynamics, Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, MA 02115, USA 3Center for Infection and Immunity, Columbia Mailman School of Public Health, New York, NY 10032, USA Correspondence: grubaughlab@gmail.com
Abstract: Korber et al. (2020) found that a SARS-CoV-2 variant in the spike protein, D614G, rapidly became dominant around the world. While clinical and in vitro data suggest that D614G changes the virus phenotype, the impact of the mutation on transmission, disease, and vaccine and therapeutic development are largely unknown.
Introduction: Following the emergence of SARS-CoV-2 in China in late 2019, and the rapid expansion of the COVID19 pandemic in 2020, questions about viral evolution have come tumbling after. Did SARS-CoV-2 evolve to become better adapted to humans? More infectious or transmissible? More deadly? Virus mutations can rise in frequency due to natural selection, random genetic drift, or features of recent epidemiology. As these forces can work in tandem, it’s often hard to differentiate when a virus mutation becomes common through fitness or by chance. It is even harder to determine if a single mutation will change the outcome of an infection, or a pandemic. The new study by Korber et al. (2020) sits at the heart of this debate. They present compelling data that an amino acid change in the virus’ spike protein, D614G, emerged early during the pandemic, and viruses containing G614 are now dominant in many places around the world. The crucial questions are whether this is the result of natural selection, and what it means for the COVID-19 pandemic. For viruses like SARS-CoV-2 transmission really is everything – if they don’t get into another host their lineage ends. Korber et al. (2020) hypothesized that the rapid spread of G614 was because it is more infectious than D614. In support of their hypothesis, the authors provided evidence that clinical samples from G614 infections have a higher levels of viral RNA, and produced higher titers in pseudoviruses from in vitro experiments; results that now seem to be corroborated by others [e.g. (Hu et al., 2020; Wagner et al., 2020)]. Still, these data do not prove that G614 is more infectious or transmissible than viruses containing D614. And because of that, many questions remain on the potential impacts, if any, that D614G has on the COVID-19 pandemic.
The authors note that this new G614 variant has become the predominant form over the whole world however in China the predominant form is still the D614 form. As they state
“over the period that G614 became the global majority variant, the number of introductions from China where D614 was still dominant were declining, while those from Europe climbed. This alone might explain the apparent success of G614.”
Grubaugh et al. feel there is not enough evidence that infection with this new variant will lead to higher mortality. Both Korber et al. and the Seattle study (Wagner et al) did not find that the higher viral load of this variant led to a difference in hospitalizations so apparently each variant might be equally as morbid.
In addition, Grubaugh et al. believe this variant would not have much affect on vaccine development as, even though the mutation lies within the spike protein, D614G is not in the receptor binding domain of the spike protein. Korber suggest that there may be changes in glycosylation however these experiments will need to be performed. In addition, antibodies from either D614 or G614 variant infected patients could cross neutralize.
Conclusions: While there has already been much breathless commentary on what this mutation means for the COVID19 pandemic, the global expansion of G614 whether through natural selection or chance means that this variant now is the pandemic. As a result its properties matter. It is clear from the in vitro and clinical data that G614 has a distinct phenotype, but whether this is the result of bonafide adaptation to human ACE2, whether it increases transmissibility, or will have a notable effect, is not clear. The work by Korber et al. (2020) provides an early base for more extensive epidemiological, in vivo experimental, and diverse clinical investigations to fill in the many critical gaps in how D614G impacts the pandemic.
The consistent increase of G614 at regional levels may indicate a fitness advantage
G614 is associated with lower RT PCR Ct’s, suggestive of higher viral loads in patients
The G614 variant grows to higher titers as pseudotyped virions
Summary
A SARS-CoV-2 variant carrying the Spike protein amino acid change D614G has become the most prevalent form in the global pandemic. Dynamic tracking of variant frequencies revealed a recurrent pattern of G614 increase at multiple geographic levels: national, regional and municipal. The shift occurred even in local epidemics where the original D614 form was well established prior to the introduction of the G614 variant. The consistency of this pattern was highly statistically significant, suggesting that the G614 variant may have a fitness advantage. We found that the G614 variant grows to higher titer as pseudotyped virions. In infected individuals G614 is associated with lower RT-PCR cycle thresholds, suggestive of higher upper respiratory tract viral loads, although not with increased disease severity. These findings illuminate changes important for a mechanistic understanding of the virus, and support continuing surveillance of Spike mutations to aid in the development of immunological interventions.
References
Grubaugh, N.D., Hanage, W.P., Rasmussen, A.L., Making sense of mutation: what D614G means for the COVID-19 pandemic remains unclear, Cell (2020), doi: https:// doi.org/10.1016/j.cell.2020.06.040.
Korber, B., Fischer, W.M., Gnanakaran, S., Yoon, H., Theiler, J., Abfalterer, W., Hengartner, N., Giorgi, E.E., Bhattacharya, T., Foley, B., et al. (2020). Tracking changes in SARS-CoV-2 Spike: evidence that D614G increases infectivity of the COVID-19 virus. Cell 182.
Endo, A., Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group, Abbott, S., Kucharski, A.J., and Funk, S. (2020). Estimating the overdispersion in COVID-19 transmission using outbreak sizes outside China. Wellcome Open Res 5, 67.
Hu, J., He, C.-L., Gao, Q.-Z., Zhang, G.-J., Cao, X.-X., Long, Q.-X., Deng, H.-J., Huang, L.-Y., Chen, J., Wang, K., et al. (2020). The D614G mutation of SARS-CoV-2 spike protein enhances viral infectivity and decreases neutralization sensitivity to individual convalescent sera. bioRxiv 2020.06.20.161323.
Wagner, C., Roychoudhury, P., Hadfield, J., Hodcroft, E.B., Lee, J., Moncla, L.H., Müller, N.F., Behrens, C., Huang, M.-L., Mathias, P., et al. (2020). Comparing viral load and clinical outcomes in Washington State across D614G mutation in spike protein of SARS-CoV-2. Https://github.com/blab/ncov-D614G.
RNA from the SARS-CoV-2 virus taking over the cells it infects: Virulence – Pathogen’s ability to infect a Resistant Host: The Imbalance between Controlling Virus Replication versus Activation of the Adaptive Immune Response
Curator: Aviva Lev-Ari, PhD, RN – I added colors and bold face
UPDATED on 9/8/2020
What bats can teach us about developing immunity to Covid-19 | Free to read
Another duality and paradox in the Treatment of COVID-19 Patients in ICUs was expressed by Mike Yoffe, MD, PhD, David H. Koch Professor of Biology and Biological Engineering, Massachusetts Institute of Technology. Dr. Yaffe has a joint appointment in Acute Care Surgery, Trauma, and Surgical Critical Care, and in Surgical Oncology @BIDMC
on 6/29 at SOLUTIONS with/in/sight at Koch Institute @MIT
How Are Cancer Researchers Fighting COVID-19? (Part II)”Jun 29, 2020 11:30 AM EST
In COVID-19 patients: two life threatening conditions are seen in ICUs:
Blood Clotting – Hypercoagulability or Thrombophilia
Cytokine Storm – immuno-inflammatory response
The coexistence of 1 and 2 – HINDERS the ability to use effectively tPA as an anti-clotting agent while the cytokine storm is present.
Mike Yoffe’s related domain of expertise:
Signaling pathways and networks that control cytokine responses and inflammation
Misregulation of cytokine feedback loops, along with inappropriate activation of the blood clotting cascade causes dysregulation of cell signaling pathways in innate immune cells (neutrophils and macrophages), resulting in tissue damage and multiple organ failure following trauma or sepsis. Our research is focused on understanding the role of the p38-MK2 pathway in cytokine control and innate immune function, and on cross-talk between cytokines, clotting factors, and neutrophil NADPH oxidase-derived ROS in tissue damage, coagulopathy, and inflammation, using biochemistry, cell biology, and mouse knock-out/knock-in models. We recently discovered a particularly important link between abnormal blood clotting and the complement pathway cytokine C5a which causes excessive production of extracellular ROS and organ damage by neutrophils after traumatic injury.
SARS-CoV-2 infection induces low IFN-I and -III levels with a moderate ISG response
Strong chemokine expression is consistent across in vitro, ex vivo, and in vivo models
Low innate antiviral defenses and high pro-inflammatory cues contribute to COVID-19
Summary
Viral pandemics, such as the one caused by SARS-CoV-2, pose an imminent threat to humanity. Because of its recent emergence, there is a paucity of information regarding viral behavior and host response following SARS-CoV-2 infection. Here we offer an in-depth analysis of the transcriptional response to SARS-CoV-2 compared with other respiratory viruses. Cell and animal models of SARS-CoV-2 infection, in addition to transcriptional and serum profiling of COVID-19 patients, consistently revealed a unique and inappropriate inflammatory response. This response is defined by low levels of type I and III interferons juxtaposed to elevated chemokines and high expression of IL-6. We propose that reduced innate antiviral defenses coupled with exuberant inflammatory cytokine production are the defining and driving features of COVID-19.
Defining the Transcriptional Response to SARS-CoV-2 Relative to Other Respiratory Viruses
To compare the transcriptional response of SARS-CoV-2 with other respiratory viruses, including MERS-CoV, SARS-CoV-1, human parainfluenza virus 3 (HPIV3), respiratory syncytial virus (RSV), and IAV, we first chose to focus on infection in a variety of respiratory cell lines (Figure 1). To this end, we collected poly(A) RNA from infected cells and performed RNA sequencing (RNA-seq) to estimate viral load. These data show that virus infection levels ranged from 0.1% to more than 50% of total RNA reads (Figure 1A).
Discussion
In the present study, we focus on defining the host response to SARS-CoV-2 and other human respiratory viruses in cell lines, primary cell cultures, ferrets, and COVID-19 patients. In general, our data show that the overall transcriptional footprint of SARS-CoV-2 infection was distinct in comparison with other highly pathogenic coronaviruses and common respiratory viruses such as IAV, HPIV3, and RSV. It is noteworthy that, despite a reduced IFN-I and -III response to SARS-CoV-2, we observed a consistent chemokine signature. One exception to this observation is the response to high-MOI infection in A549-ACE2 and Calu-3 cells, where replication was robust and an IFN-I and -III signature could be observed. In both of these examples, cells were infected at a rate to theoretically deliver two functional virions per cell in addition to any defective interfering particles within the virus stock that were not accounted for by plaque assays. Under these conditions, the threshold for PAMP may be achieved prior to the ability of the virus to evade detection through production of a viral antagonist. Alternatively, addition of multiple genomes to a single cell may disrupt the stoichiometry of viral components, which, in turn, may itself generate PAMPs that would not form otherwise. These ideas are supported by the fact that, at a low-MOI infection in A549-ACE2 cells, high levels of replication could also be achieved, but in the absence of IFN-I and -III induction. Taken together, these data suggest that, at low MOIs, the virus is not a strong inducer of the IFN-I and -III system, as opposed to conditions where the MOI is high.
Taken together, the data presented here suggest that the response to SARS-CoV-2 is imbalanced with regard to controlling virus replication versus activation of the adaptive immune response. Given this dynamic, treatments for COVID-19 have less to do with the IFN response and more to do with controlling inflammation. Because our data suggest that numerous chemokines and ILs are elevated in COVID-19 patients, future efforts should focus on U.S. Food and Drug Administration (FDA)-approved drugs that can be rapidly deployed and have immunomodulating properties.
One of the features distinguishing SARS-CoV-2 from its more pathogenic counterpart SARS-CoV is the presence of premature stop codons in its ORF3b gene. Here, we show that SARS-CoV-2 ORF3b is a potent interferon antagonist, suppressing the induction of type I interferon more efficiently than its SARS-CoV ortholog. Phylogenetic analyses and functional assays revealed that SARS-CoV-2-related viruses from bats and pangolins also encode truncated ORF3b gene products with strong anti-interferon activity. Furthermore, analyses of more than 15,000 SARS-CoV-2 sequences identified a natural variant, in which a longer ORF3b reading frame was reconstituted. This variant was isolated from two patients with severe disease and further increased theability of ORF3b to suppress interferon induction. Thus, our findings not only help to explain the poor interferon response in COVID-19 patients, but also describe a possibility of the emergence of natural SARS-CoV-2 quasi-species with extended ORF3b that may exacerbate COVID-19 symptoms.
Highlights
ORF3b of SARS-CoV-2 and related bat and pangolin viruses is a potent IFN antagonist
SARS-CoV-2 ORF3b suppresses IFN induction more efficiently than SARS-CoV ortholog
The anti-IFN activity of ORF3b depends on the length of its C-terminus
An ORF3b with increased IFN antagonism was isolated from two severe COVID-19 cases
RNA (in green) from the SARS-CoV-2 virus is shown taking over the cells it infects.ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI
A deep dive into how the new coronavirus infects cells has found that it orchestrates a hostile takeover of their genes unlike any other known viruses do, producing what one leading scientist calls “unique” and “aberrant” changes.Recent studies show that in seizing control of genes in the human cells it invades, the virus changes how segments of DNA are read, doing so in a way that might explain why the elderly are more likely to die of Covid-19 and why antiviral drugs might not only save sick patients’ lives but also prevent severe disease if taken before infection.“It’s something I have never seen in my 20 years of” studying viruses, said virologist Benjamin tenOever of the Icahn School of Medicine at Mount Sinai, referring to how SARS-CoV-2, the virus that causes Covid-19, hijacks cells’ genomes.The “something” he and his colleagues saw is how SARS-CoV-2 blocks one virus-fighting set of genes but allows another set to launch, a pattern never seen with other viruses. Influenza and the original SARS virus (in the early 2000s), for instance, interfere with both arms of the body’s immune response — what tenOever dubs “call to arms” genes and “call for reinforcement” genes.The first group of genes produces interferons. These proteins, which infected cells release, are biological semaphores, signaling to neighboring cells to activate some 500 of their own genes that will slow down the virus’ ability to make millions of copies of itself if it invades them. This lasts seven to 10 days, tenOever said, controlling virus replication and thereby buying time for the second group of genes to act.This second set of genes produce their own secreted proteins, called chemokines, that emit a biochemical “come here!” alarm. When far-flung antibody-making B cells and virus-killing T cells sense the alarm, they race to its source. If all goes well, the first set of genes holds the virus at bay long enough for the lethal professional killers to arrive and start eradicating viruses.
“Most other viruses interfere with some aspect of both the call to arms and the call for reinforcements,” tenOever said. “If they didn’t, no one would ever get a viral illness”: The one-two punch would pummel any incipient infection into submission.
SARS-CoV-2, however, uniquely blocks one cellular defense but activates the other, he and his colleagues reported in a study published last week in Cell. They studied healthy human lung cells growing in lab dishes, ferrets (which the virus infects easily), and lung cells from Covid-19 patients. In all three, they found that within three days of infection, the virus induces cells’ call-for-reinforcement genes to produce cytokines. But it blocks their call-to-arms genes — the interferons that dampen the virus’ replication.
The result is essentially no brakes on the virus’s replication, but a storm of inflammatory molecules in the lungs, which is what tenOever calls an “unique” and “aberrant” consequence of how SARS-CoV-2 manipulates the genome of its target.
In another new study, scientists in Japan last week identified how SARS-CoV-2 accomplishes that genetic manipulation. Its ORF3b gene produces a protein called a transcription factor that has “strong anti-interferon activity,” Kei Sato of the University of Tokyo and colleagues found — stronger than the original SARS virus or influenza viruses. The protein basically blocks the cell from recognizing that a virus is present, in a way that prevents interferon genes from being expressed.
In fact, the Icahn School team found no interferons in the lung cells of Covid-19 patients. Without interferons, tenOever said, “there is nothing to stop the virus from replicating and festering in the lungs forever.”
That causes lung cells to emit even more “call-for-reinforcement” genes, summoning more and more immune cells. Now the lungs have macrophages and neutrophils and other immune cells “everywhere,” tenOever said, causing such runaway inflammation “that you start having inflammation that induces more inflammation.”
At the same time, unchecked viral replication kills lung cells involved in oxygen exchange. “And suddenly you’re in the hospital in severe respiratory distress,” he said.
In elderly people, as well as those with diabetes, heart disease, and other underlying conditions, the call-to-arms part of the immune system is weaker than in younger, healthier people, even before the coronavirus arrives. That reduces even further the cells’ ability to knock down virus replication with interferons, and imbalances the immune system toward the dangerous inflammatory response.
The discovery that SARS-CoV-2 strongly suppresses infected cells’ production of interferons has raised an intriguing possibility: that taking interferons might prevent severe Covid-19 or even prevent it in the first place, said Vineet Menachery of the University of Texas Medical Branch.
In a study of human cells growing in lab dishes, described in a preprint (not peer-reviewed or published in a journal yet), he and his colleagues also found that SARS-CoV-2 “prevents the vast amount” of interferon genes from turning on. But when cells growing in lab dishes received the interferon IFN-1 before exposure to the coronavirus, “the virus has a difficult time replicating.”
After a few days, the amount of virus in infected but interferon-treated cells was 1,000- to 10,000-fold lower than in infected cells not pre-treated with interferon. (The original SARS virus, in contrast, is insensitive to interferon.)
Ending the pandemic and preventing its return is assumed to require an effective vaccine to prevent infectionand antiviral drugs such as remdesivir to treat the very sick, but the genetic studies suggest a third strategy: preventive drugs.
It’s possible that treatment with so-called type-1 interferon “could stop the virus before it could get established,” Menachery said.
Giving drugs to healthy people is always a dicey proposition, since all drugs have side effects — something considered less acceptable than when a drug is used to treat an illness. “Interferon treatment is rife with complications,” Menachery warned. The various interferons, which are prescribed for hepatitis, cancers, and many other diseases, can cause flu-like symptoms.
But the risk-benefit equation might shift, both for individuals and for society, if interferons or antivirals or other medications are shown to reduce the risk of developing serious Covid-19 or even make any infection nearly asymptomatic.
Interferon “would be warning the cells the virus is coming,” Menachery said, so such pretreatment might “allow treated cells to fend off the virus better and limit its spread.” Determining that will of course require clinical trials, which are underway.
Other related articles in this Open Access Online Scientific Journal include the following:
Structure-guided Drug Discovery: (1) The Coronavirus 3CL hydrolase (Mpro) enzyme (main protease) essential for proteolytic maturation of the virus and (2) viral protease, the RNA polymerase, the viral spike protein, a viral RNA as promising two targets for discovery of cleavage inhibitors of the viral spike polyprotein preventing the Coronavirus Virion the spread of infection
Predicting the Protein Structure of Coronavirus: Inhibition of Nsp15 can slow viral replication and Cryo-EM – Spike protein structure (experimentally verified) vs AI-predicted protein structures (not experimentally verified) of DeepMind (Parent: Google) aka AlphaFold
Curators: Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN
Glycobiology vs Proteomics: Glycobiologists Prespective in the effort to explain the origin, etiology and potential therapeutics for the Coronavirus Pandemic (COVID-19).
Actemra, immunosuppressive which was designed to treat rheumatoid arthritis but also approved in 2017 to treat cytokine storms in cancer patients SAVED the sickest of all COVID-19 patients
The Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) Partnership on May 18, 2020: Leadership of AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Eisai, Eli Lilly, Evotec, Gilead, GlaxoSmithKline, Johnson & Johnson, KSQ Therapeutics, Merck, Novartis, Pfizer, Roche, Sanofi, Takeda, and Vir. We also thank multiple NIH institutes (especially NIAID), the FDA, BARDA, CDC, the European Medicines Agency, the Department of Defense, the VA, and the Foundation for NIH
Tweets & Retweets 2020 World Medical Innovation Forum – COVID-19, AI and the Future of Medicine, Featuring Harvard and Industry Leader Insights – MGH & BWH, Virtual Event: Monday, May 11, 8:15 a.m. – 5:15 p.m. ET
A Series of Recently Published Papers Report the Development of SARS-CoV2 Neutralizing Antibodies and Passive Immunity toward COVID19
Curator: Stephen J. Williams, Ph.D.
Passive Immunity and Treatment of Infectious Diseases
The ability of one person to pass on immunity to another person (passive immunity) is one of the chief methods we develop immunity to many antigens. For instance, maternal antibodies are passed to the offspring in the neonatal setting as well as in a mother’s milk during breast feeding. In the clinical setting this is achieved by transferring antibodies from one patient who has been exposed to an antigen (like a virus) to the another individual. However, the process of purifying the most efficacious antibody as well as its mass production is limiting due to its complexity and cost and can be prohibitively long delay during a pandemic outbreak, when therapies are few and needed immediately. Regardless, the benefits of developing neutralizing antibodies to confer passive immunity versus development of a vaccine are evident, as the former takes considerable less time than development of a safe and effective vaccine. For a good review on the development and use of neutralizing antibodies and the use of passive immunity to treat infectious diseases please read the following review:
Antibodies have been used for over a century in the prevention and treatment of infectious disease. They are used most commonly for the prevention of measles, hepatitis A, hepatitis B, tetanus, varicella, rabies, and vaccinia. Although their use in the treatment of bacterial infection has largely been supplanted by antibiotics, antibodies remain a critical component of the treatment of diptheria, tetanus, and botulism. High-dose intravenous immunoglobulin can be used to treat certain viral infections in immunocompromised patients (e.g., cytomegalovirus, parvovirus B19, and enterovirus infections). Antibodies may also be of value in toxic shock syndrome, Ebola virus, and refractory staphylococcal infections. Palivizumab, the first monoclonal antibody licensed (in 1998) for an infectious disease, can prevent respiratory syncytial virus infection in high-risk infants. The development and use of additional monoclonal antibodies to key epitopes of microbial pathogens may further define protective humoral responses and lead to new approaches for the prevention and treatment of infectious diseases.
TABLE 1
Summary of the efficacy of antibody in the prevention and treatment of infectious diseases
A Great Explanation of Active versus Passive Immunity by Dr. John Campbell, one of the pioneers in the field of immunology:Antibodies have been used for over a century in the prevention and treatment of infectious disease. They are used most commonly for the prevention of measles, hepatitis A, hepatitis B, tetanus, varicella, rabies, and vaccinia. Although their use in the treatment of bacterial infection has largely been supplanted by antibiotics, antibodies remain a critical component of the treatment of diptheria, tetanus, and botulism. High-dose intravenous immunoglobulin can be used to treat certain viral infections in immunocompromised patients (e.g., cytomegalovirus, parvovirus B19, and enterovirus infections). Antibodies may also be of value in toxic shock syndrome, Ebola virus, and refractory staphylococcal infections. Palivizumab, the first monoclonal antibody licensed (in 1998) for an infectious disease, can prevent respiratory syncytial virus infection in high-risk infants. The development and use of additional monoclonal antibodies to key epitopes of microbial pathogens may further define protective humoral responses and lead to new approaches for the prevention and treatment of infectious diseases.
However, developing successful neutralizing antibodies can still be difficult but with the latest monoclonal antibody technology, as highlighted by the following papers, this process has made much more efficient. In addition, it is not feasable to isolate antibodies from the plasma of covalescent patients in a scale that is needed for a worldwide outbreak.
When fighting off foreign invaders, our bodies make antibodies precisely produced for the task. The reason vaccines offer such long-lasting protection is they train the immune system to identify a pathogen, so immune cells remember and are ready to attack the virus when it appears. Monoclonal antibodies for coronavirus would take the place of the ones our bodies might produce to fight the disease. The manufactured antibodies would be infused into the body to either tamp down an existing infection, or to protect someone who has been exposed to the virus. However, these drugs are synthetic versions of the convalescent plasma treatments that rely on antibodies from people who have recovered from infection. But the engineered versions are easier to scale because they’re manufactured in rats, rather than from plasma donors.
The following papers represent the latest published work on development of therapeutic and prophylactic neutralizing antibodies to the coronavirus SARS-CoV2
1. Cross-neutralization of SARS-CoV-2 by a human monoclonal SARS-CoV antibody.
SARS-CoV-2 is a newly emerged coronavirus responsible for the current COVID-19 pandemic that has resulted in more than 3.7 million infections and 260,000 deaths as of 6 May 20201,2. Vaccine and therapeutic discovery efforts are paramount to curb the pandemic spread of this zoonotic virus. The SARS-CoV-2 spike (S) glycoprotein promotes entry into host cells and is the main target of neutralizing antibodies. Here we describe multiple monoclonal antibodies targeting SARS-CoV-2 S identified from memory B cells of an individual who was infected with SARS-CoV in 2003. One antibody, named S309, potently neutralizes SARS-CoV-2 and SARS-CoV pseudoviruses as well as authentic SARS-CoV-2 by engaging the S receptor-binding domain. Using cryo-electron microscopy and binding assays, we show that S309 recognizes a glycan-containing epitope that is conserved within the sarbecovirus subgenus, without competing with receptor attachment. Antibody cocktails including S309 along with other antibodies identified here further enhanced SARS-CoV-2 neutralization and may limit the emergence of neutralization-escape mutants. These results pave the way for using S309- and S309-containing antibody cocktails for prophylaxis in individuals at high risk of exposure or as a post-exposure therapy to limit or treat severe disease.
2. Potent neutralizing antibodies against SARS-CoV-2 identified by high-throughput single-cell sequencing of convalescent patients’ B cells
The COVID-19 pandemic urgently needs therapeutic and prophylactic interventions. Here we report the rapid identification of SARS-CoV-2 neutralizing antibodies by high-throughput single-cell RNA and VDJ sequencing of antigen-enriched B cells from 60 convalescent patients. From 8,558 antigen-binding IgG1+ clonotypes, 14 potent neutralizing antibodies were identified with the most potent one, BD-368-2, exhibiting an IC50 of 1.2 ng/mL and 15 ng/mL against pseudotyped and authentic SARS-CoV-2, respectively. BD-368-2 also displayed strong therapeutic and prophylactic efficacy in SARS-CoV-2-infected hACE2-transgenic mice. Additionally, the 3.8Å Cryo-EM structure of a neutralizing antibody in complex with the spike-ectodomain trimer revealed the antibody’s epitope overlaps with the ACE2 binding site. Moreover, we demonstrated that SARS-CoV-2 neutralizing antibodies could be directly selected based on similarities of their predicted CDR3H structures to those of SARS-CoV neutralizing antibodies. Altogether, we showed that human neutralizing antibodies could be efficiently discovered by high-throughput single B-cell sequencing in response to pandemic infectious diseases.
3. A human monoclonal antibody blocking SARS-CoV-2 infection
The emergence of the novel human coronavirus SARS-CoV-2 in Wuhan, China has caused a worldwide epidemic of respiratory disease (COVID-19). Vaccines and targeted therapeutics for treatment of this disease are currently lacking. Here we report a human monoclonal antibody that neutralizes SARS-CoV-2 (and SARS-CoV) in cell culture. This cross-neutralizing antibody targets a communal epitope on these viruses and may offer potential for prevention and treatment of COVID-19.
Extra References on Development of Neutralizing antibodies for COVID19 {Sars-CoV2} published this year (2020) [1-4]
Fan P, Chi X, Liu G, Zhang G, Chen Z, Liu Y, Fang T, Li J, Banadyga L, He S et al: Potent neutralizing monoclonal antibodies against Ebola virus isolated from vaccinated donors. mAbs 2020, 12(1):1742457.
Dussupt V, Sankhala RS, Gromowski GD, Donofrio G, De La Barrera RA, Larocca RA, Zaky W, Mendez-Rivera L, Choe M, Davidson E et al: Potent Zika and dengue cross-neutralizing antibodies induced by Zika vaccination in a dengue-experienced donor. Nature medicine 2020, 26(2):228-235.
Young CL, Lyons AC, Hsu WW, Vanlandingham DL, Park SL, Bilyeu AN, Ayers VB, Hettenbach SM, Zelenka AM, Cool KR et al: Protection of swine by potent neutralizing anti-Japanese encephalitis virus monoclonal antibodies derived from vaccination. Antiviral research 2020, 174:104675.
IBM Releases Novel AI-Powered Technologies to Help Health and Research Community Accelerate the Discovery of Medical Insights and Treatments for COVID-19
IBM Research has been actively developing new cloud and AI-powered technologies that can help researchers across a variety of scientific disciplines accelerate the process of discovery. As the COVID-19 pandemic unfolds, we continue to ask how these technologies and our scientific knowledge can help in the global battle against coronavirus.
Today, we are making available multiple novel, free resources from across IBM to help healthcare researchers, doctors and scientists around the world accelerate COVID-19 drug discovery: from gathering insights, to applying the latest virus genomic information and identifying potential targets for treatments, to creating new drug molecule candidates.
Though some of the resources are still in exploratory stages, IBM is making them available to qualifying researchers at no charge to aid the international scientific investigation of COVID-19.
Healthcare agencies and governments around the world have quickly amassed medical and other relevant data about the pandemic. And, there are already vast troves of medical research that could prove relevant to COVID-19. Yet, as with any large volume of disparate data sources, it is difficult to efficiently aggregate and analyze that data in ways that can yield scientific insights.
To help researchers access structured and unstructured data quickly, we are offering a cloud-based AI research resource that has been trained on a corpus of thousands of scientific papers contained in the COVID-19 Open Research Dataset (CORD-19), prepared by the White House and a coalition of research groups, and licensed databases from the DrugBank, Clinicaltrials.gov and GenBank. This tool uses our advanced AI and allows researchers to pose specific queries to the collections of papers and to extract critical COVID-19 knowledge quickly. Please note, access to this resource will be granted only to qualified researchers. To learn more and request access, please click here.
Aiding the Hunt for Treatments
The traditional drug discovery pipeline relies on a library of compounds that are screened, improved, and tested to determine safety and efficacy. In dealing with new pathogens such as SARS-CoV-2, there is the potential to enhance the compound libraries with additional novel compounds. To help address this need, IBM Research has recently created a new, AI-generative framework which can rapidly identify novel peptides, proteins, drug candidates and materials.
We have applied this AI technology against three COVID-19 targets to identify 3,000 new small molecules as potential COVID-19 therapeutic candidates. IBM is releasing these molecules under an open license, and researchers can study them via a new interactive molecular explorer tool to understand their characteristics and relationship to COVID-19 and identify candidates that might have desirable properties to be further pursued in drug development.
To streamline efforts to identify new treatments for COVID-19, we are also making the IBM Functional Genomics Platform available for free for the duration of the pandemic. Built to discover the molecular features in viral and bacterial genomes, this cloud-based repository and research tool includes genes, proteins and other molecular targets from sequenced viral and bacterial organisms in one place with connections pre-computed to help accelerate discovery of molecular targets required for drug design, test development and treatment.
Select IBM collaborators from government agencies, academic institutions and other organizations already use this platform for bacterial genomic study. And now, those working on COVID-19 can request the IBM Functional Genomics Platform interface to explore the genomic features of the virus. Access to the IBM Functional Genomics Platform will be prioritized for those conducting COVID-19 research. To learn more and request access, please click here.
Drug and Disease Information
Clinicians and healthcare professionals on the frontlines of care will also have free access to hundreds of pieces of evidence-based, curated COVID-19 and infectious disease content from IBM Micromedex and EBSCO DynaMed. Using these two rich decision support solutions, users will have access to drug and disease information in a single and comprehensive search. Clinicians can also provide patients with consumer-friendly patient education handouts with relevant, actionable medical information. IBM Micromedex is one of the largest online reference databases for medication information and is used by more than 4,500 hospitals and health systems worldwide. EBSCO DynaMed provides peer-reviewed clinical content, including systematic literature reviews in 28 specialties for comprehensive disease topics, health conditions and abnormal findings, to highly focused topics on evaluation, differential diagnosis and management.
The scientific community is working hard to make important new discoveries relevant to the treatment of COVID-19, and we’re hopeful that releasing these novel tools will help accelerate this global effort. This work also outlines our long-term vision for the future of accelerated discovery, where multi-disciplinary scientists and clinicians work together to rapidly and effectively create next generation therapeutics, aided by novel AI-powered technologies.
Grant will allow company to accelerate access to its AI solutions and use of ultrasound in COVID-19 emergency settings
TEL AVIV, Israel, May 12, 2020 /PRNewswire-PRWeb/ — DiA Imaging Analysis, a leading provider of AI based ultrasound analysis solutions, today announced that it has received a government grant from the Israel Innovation Authority (IIA) to develop solutions for ultrasound imaging analysis of COVID-19 patients using Artificial Intelligence (AI).Using ultrasound in point of care emergency settings has gained momentum since the outbreak of COVID-19 pandemic. In these settings, which include makeshift hospital COVID-19 departments and triage “tents,” portable ultrasound offers clinicians diagnostic decision support, with the added advantage of being easier to disinfect and eliminating the need to transport patients from one room to another.However, analyzing ultrasound images is a process that it is still mostly done visually, leading to a growing market need for automated solutions and decision support.As the leading provider of AI solutions for ultrasound analysis and backed by Connecticut Innovations, DiA makes ultrasound analysis smarter and accessible to both new and expert ultrasound users with various levels of experience. The company’s flagship LVivo Cardio Toolbox for AI-based cardiac ultrasound analysis enables clinicians to automatically generate objective clinical analysis, with increased accuracy and efficiency to support decisions about patient treatment and care.
The IIA grant provides a budget of millions NIS to increase access to DiA’s solutions for users in Israel and globally, and accelerate R&D with a focus on new AI solutions for COVID-19 patient management. DiA solutions are vendor-neutral and platform agnostic, as well as powered to run in low processing, mobile environments like handheld ultrasound.Recent data highlights the importance of looking at the heart during the progression of COVID-19, with one study citing 20% of patients hospitalized with COVID-19 showing signs of heart damage and increased mortality rates in those patients. DiA’s LVivo cardiac analysis solutions automatically generate objective, quantified cardiac ultrasound results to enable point-of-care clinicians to assess cardiac function on the spot, near patients’ bedside.
According to Dr. Ami Applebaum, the Chairman of the Board of the IIA, “The purpose of IIA’s call was to bring solutions to global markets for fighting COVID-19, with an emphasis on relevancy, fast time to market and collaborations promising continuity of the Israeli economy. DiA meets these requirements with AI innovation for ultrasound.”DiA has received several FDA/CE clearances and established distribution partnerships with industry leading companies including GE Healthcare, IBM Watson and Konica Minolta, currently serving thousands of end users worldwide.”We see growing use of ultrasound in point of care settings, and an urgent need for automated, objective solutions that provide decision support in real time,” said Hila Goldman-Aslan, CEO and Co-founder of DiA Imaging Analysis, “Our AI solutions meet this need by immediately helping clinicians on the frontlines to quickly and easily assess COVID-19 patients’ hearts to help guide care delivery.”
About DiA Imaging Analysis:
DiA Imaging Analysis provides advanced AI-based ultrasound analysis technology that makes ultrasound accessible to all. DiA’s automated tools deliver fast and accurate clinical indications to support the decision-making process and offer better patient care. DiA’s AI-based technology uses advanced pattern recognition and machine-learning algorithms to automatically imitate the way the human eye detects image borders and identifies motion. Using DiA’s tools provides automated and objective AI tools, helps reduce variability among users, and increases efficiency. It allows clinicians with various levels of experience to quickly and easily analyze ultrasound images.
Actemra, immunosuppressive which was designed to treat rheumatoid arthritis but also approved in 2017 to treat cytokine storms in cancer patients SAVED the sickest of all COVID-19 patients
Reporter: Aviva Lev-Ari, PhD, RN
Emergency room doctor, near death with coronavirus, saved with experimental treatment
Soon after being admitted to his own hospital with a fever, cough and difficulty breathing, he was placed on a ventilator. Five days after that, his lungs and kidneys were failing, his heart was in trouble, and doctors figured he had a day or so to live.
He owes his survival to an elite team of doctors who tried an experimental treatment pioneered in China and used on the sickest of all COVID-19 patients.
Lessons from his dramatic recovery could help doctors worldwide treat other extremely ill COVID-19 patients.
Based on the astronomical level of inflammation in his body and reports written by Chinese and Italian physicians who had treated the sickest COVID-19 patients, the doctors came to believe that it was not the disease itself killing him but his own immune system.
It had gone haywire and began to attack itself — a syndrome known as a “cytokine storm.”
The immune system normally uses proteins called cytokines as weapons in fighting a disease. For unknown reasons in some COVID-19 patients, the immune system first fails to respond quickly enough and then floods the body with cytokines, destroying blood vessels and filling the lungs with fluid.
Dr. Matt Hartman, a cardiologist, said that after four days on the immunosuppressive drug, supplemented by high-dose vitamin C and other therapies, the level of oxygen in Padgett’s blood improved dramatically. On March 23, doctors were able to take him off life support.
Four days later, they removed his breathing tube. He slowly came out of his sedated coma, at first imagining that he was in the top floor of the Space Needle converted to a COVID ward.
Responses to the #COVID-19 outbreak from Oncologists, Cancer Societies and the NCI: Important information for cancer patients
Curator: Stephen J. Williams, Ph.D.
UPDATED 3/20/2020
Among the people who are identified at risk of coronovirus 2019 infection and complications of the virus include cancer patients undergoing chemotherapy, who in general, can be immunosuppressed, especially while patients are undergoing their treatment. This has created anxiety among many cancer patients as well as their care givers and prompted many oncologist professional groups, cancer societies, and cancer centers to formulate some sort of guidelines for both the cancer patients and the oncology professional with respect to limiting the risk of infection to coronavirus (COVID19).
This information will be periodically updated and we are working to get a Live Twitter Feed to bring oncologist and cancer patient advocacy groups together so up to date information can be communicated rapidly. Please see this page regularly for updates as new information is curated.
IN ADDITION, I will curate a listing of drugs with adverse events of immunosuppression for people who might wonder if the medications they are taking are raising their risk of infections.
From the Cancer Letter:The following is a guest editorial by American Society of Clinical Oncology (ASCO) Executive Vice President and Chief Medical Officer Richard L. Schilsky MD, FACP, FSCT, FASCO. This story is part of The Cancer Letter’s ongoing coverage of COVID-19’s impact on oncology. A full list of our coverage, as well as the latest meeting cancellations, is available here.
The worldwide spread of the coronavirus (COVID-19) presents unprecedented challenges to the cancer care delivery system.
Our patients are already dealing with a life-threatening illness and are particularly vulnerable to this viral infection, which can be even more deadly for them.Further, as restrictions in daily movement and social distancing take hold, vulnerable patients may be disconnected from friends, family or other support they need as they manage their cancer.
As providers, we rely on evidence and experience when treating patients but now we face uncertainty. There are limited data to guide us in the specific management of cancer patients confronting COVID-19 and, at present, we have no population-level guidance regarding acceptable or appropriate adjustments of treatment and practice operations that both ensure the best outcome for our patients and protect the safety of our colleagues and staff.
As normal life is dramatically changed, we are all feeling anxious about the extreme economic challenges we face, but these issues are perhaps even more difficult for our patients, many of whom are now facing interruption
As we confront this extraordinary situation, the health and safety of members, staff, and individuals with cancer—in fact, the entire cancer community—is ASCO’s highest priority.
ASCO has been actively monitoring and responding to the pandemic to ensure that accurate information is readily available to clinicians and their patients. Recognizing that this is a rapidly evolving situation and that limited oncology-specific, evidence-based information is available, we are committed to sharing what is known and acknowledging what is unknown so that the most informed decisions can be made.
To help guide oncology professionals as they deal with the impact of coronavirus on both their patients and staff, ASCO has collated questions from its members, postedresponses at asco.organd assembled a compendium of additional resources we hope will be helpful as the virus spreads and the disease unfolds. We continue to receive additional questions regarding clinical care and we are updating our FAQs on a regular basis.
We hope this information is helpful even when it merely confirms that there are no certain answers to many questions. Our answers are based on the best available information we identify in the literature, guidance from public health authorities, and input received from oncology and infectious disease experts.
For patients, we have posted a blog byDr. Merry Jennifer Markham, chair of ASCO’s Cancer Communications Committee. This can be found onCancer.Net, ASCO’s patient information website, and it provides practical guidance to help patients reduce their risk of exposure, better understand COVID-19 symptoms, and locate additional information.
This blog is available both in English and Spanish. Additional blog posts addressing patient questions will be posted as new questions are received and new information becomes available.
Find below a Tweet from Dr.Markham which includes links to her article on COVID-19 for cancer patients
JNCCN: How to Manage Cancer Care during COVID-19 Pandemic
Experts from the Seattle Cancer Care Alliance (SCCA)—a Member Institution of the National Comprehensive Cancer Network® (NCCN®)—are sharing insights and advice on how to continue providing optimal cancer care during the novel coronavirus (COVID-19) pandemic. SCCA includes the Fred Hutchinson Cancer Research Center and the University of Washington, which are located in the epicenter of the COVID-19 outbreak in the United States. The peer-reviewed article sharing best practices is available for free online-ahead-of-print via open access at JNCCN.org.
Coronavirus disease 2019 (COVID-19) Resources for the Cancer Care Community
NCCN recognizes the rapidly changing medical information relating to COVID-19 in the oncology ecosystem, but understands that a forum for sharing best practices and specific institutional responses may be helpful to others. Therefore, we are expeditiously providing documents and recommendations developed by NCCN Member Institutions or Guideline Panels as resources for oncology care providers. These resources have not been developed or reviewed by the standard NCCN processes, and are provided for information purposes only. We will post more resources as they become available so check back for additional updates.
Both the resources at cancer.gov (NCI) as well as the resources from ASCO are updated as new information is evaluated and more guidelines are formulated by members of the oncologist and cancer care community and are excellent resources for those living with cancer, and also those who either care for cancer patients or their family and relatives.
Related Resources for Patients (please click on links)
@DrMarkham Dr. Markham is Chief of Heme-Onc & gyn med onc@UF | AD Med Affairs@UFHealthCancerand has collected very good information for patients concerning #Covid19
Cancer patients on chemotherapy concerned about traveling for treatment during the #COVID19 crisis may have another option. Find out about the pros and cons of taking an oral medication. https://t.co/4djwfji5WR#CTCABlog
— CTCA, part of City of Hope (@CancerCenter) March 19, 2020
UPDATED 3/20/2020 INFORMATION FROM NCI DESIGNATED CANCER CENTERS FOR PATIENTS/PROVIDERS
The following is a listing with links of NCI Designated Comprehensive Cancer Centers and some select designated Cancer Centers* which have information on infectious risk guidance for cancer patients as well as their physicians and caregivers. There are 51 NCI Comprehensive Cancer Centers and as more cancer centers formulate guidance this list will be updated.
Structure-guided Drug Discovery: (1) The Coronavirus 3CL hydrolase (Mpro) enzyme (main protease) essential for proteolytic maturation of the virus and (2) viral protease, the RNA polymerase, the viral spike protein, a viral RNA as promising two targets for discovery of cleavage inhibitors of the viral spike polyprotein preventing the Coronavirus Virion the spread of infection
Curators and Reporters: Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN
Therapeutical options to coronavirus (2019-nCoV) include consideration of the following:
(a) Monoclonal and polyclonal antibodies
(b) Vaccines
(c) Small molecule treatments (e.g., chloroquinolone and derivatives), including compounds already approved for other indications
(d) Immuno-therapies derived from human or other sources
Structure of the nCoV trimeric spike
The World Health Organization has declared the outbreak of a novel coronavirus (2019-nCoV) to be a public health emergency of international concern. The virus binds to host cells through its trimeric spike glycoprotein, making this protein a key target for potential therapies and diagnostics. Wrapp et al. determined a 3.5-angstrom-resolution structure of the 2019-nCoV trimeric spike protein by cryo–electron microscopy. Using biophysical assays, the authors show that this protein binds at least 10 times more tightly than the corresponding spike protein of severe acute respiratory syndrome (SARS)–CoV to their common host cell receptor. They also tested three antibodies known to bind to the SARS-CoV spike protein but did not detect binding to the 2019-nCoV spike protein. These studies provide valuable information to guide the development of medical counter-measures for 2019-nCoV. [Bold Face Added by ALA]
The outbreak of a novel coronavirus (2019-nCoV) represents a pandemic threat that has been declared a public health emergency of international concern. The CoV spike (S) glycoprotein is a key target for vaccines, therapeutic antibodies, and diagnostics. To facilitate medical countermeasure development, we determined a 3.5-angstrom-resolution cryo–electron microscopy structure of the 2019-nCoV S trimer in the prefusion conformation. The predominant state of the trimer has one of the three receptor-binding domains (RBDs) rotated up in a receptor-accessible conformation. We also provide biophysical and structural evidence that the 2019-nCoV S protein binds angiotensin-converting enzyme 2 (ACE2) with higher affinity than does severe acute respiratory syndrome (SARS)-CoV S. Additionally, we tested several published SARS-CoV RBD-specific monoclonal antibodies and found that they do not have appreciable binding to 2019-nCoV S, suggesting that antibody cross-reactivity may be limited between the two RBDs. The structure of 2019-nCoV S should enable the rapid development and evaluation of medical countermeasures to address the ongoing public health crisis.
SOURCE
Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation
Recent emergence of the COVID-19 coronavirus has resulted in a WHO-declared public health emergency of international concern. Research efforts around the world are working towards establishing a greater understanding of this particular virus and developing treatments and vaccines to prevent further spread.
While PDB entry 6lu7 is currently the only public-domain 3D structure from this specific coronavirus, the PDB contains structures of the corresponding enzyme from other coronaviruses. The 2003 outbreak of the closely-related Severe Acute Respiratory Syndrome-related coronavirus (SARS) led to the first 3D structures, and today there are more than 200 PDB structures of SARS proteins. Structural information from these related proteins could be vital in furthering our understanding of coronaviruses and in discovery and development of new treatments and vaccines to contain the current outbreak.
The coronavirus 3CL hydrolase (Mpro) enzyme, also known as the main protease, is essential for proteolytic maturation of the virus. It is thought to be a promising target for discovery of small-molecule drugs that would inhibit cleavage of the viral polyprotein and prevent spread of the infection.
Comparison of the protein sequence of the COVID-19 coronavirus 3CL hydrolase (Mpro) against the PDB archive identified 95 PDB proteins with at least 90% sequence identity. Furthermore, these related protein structures contain approximately 30 distinct small molecule inhibitors, which could guide discovery of new drugs. Of particular significance for drug discovery is the very high amino acid sequence identity (96%) between the COVID-19 coronavirus 3CL hydrolase (Mpro) and the SARS virus main protease (PDB 1q2w). Summary data about these closely-related PDB structures are available (CSV) to help researchers more easily find this information. In addition, the PDB houses 3D structure data for more than 20 unique SARS proteins represented in more than 200 PDB structures, including a second viral protease, the RNA polymerase, the viral spike protein, a viral RNA, and other proteins (CSV).
Public release of the COVID-19 coronavirus 3CL hydrolase (Mpro), at a time when this information can prove most vital and valuable, highlights the importance of open and timely availability of scientific data. The wwPDB strives to ensure that 3D biological structure data remain freely accessible for all, while maintaining as comprehensive and accurate an archive as possible. We hope that this new structure, and those from related viruses, will help researchers and clinicians address the COVID-19 coronavirus global public health emergency.
Update: Released COVID-19-related PDB structures include
PDB structure 6lu7 (X. Liu, B. Zhang, Z. Jin, H. Yang, Z. Rao Crystal structure of COVID-19 main protease in complex with an inhibitor N3 doi: 10.2210/pdb6lu7/pdb) Released 2020-02-05
PDB structure 6vsb (D. Wrapp, N. Wang, K.S. Corbett, J.A. Goldsmith, C.-L. Hsieh, O. Abiona, B.S. Graham, J.S. McLellan (2020) Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation Science doi: 10.1126/science.abb2507) Released 2020-02-26
PDB structure 6lxt (Y. Zhu, F. Sun Structure of post fusion core of 2019-nCoV S2 subunit doi: 10.2210/pdb6lxt/pdb) Released 2020-02-26
PDB structure 6lvn (Y. Zhu, F. Sun Structure of the 2019-nCoV HR2 Domain doi: 10.2210/pdb6lvn/pdb) Released 2020-02-26
PDB structure 6vw1
J. Shang, G. Ye, K. Shi, Y.S. Wan, H. Aihara, F. Li Structural basis for receptor recognition by the novel coronavirus from Wuhan doi: 10.2210/pdb6vw1/pdb
Released 2020-03-04
PDB structure 6vww
Y. Kim, R. Jedrzejczak, N. Maltseva, M. Endres, A. Godzik, K. Michalska, A. Joachimiak, Center for Structural Genomics of Infectious Diseases Crystal Structure of NSP15 Endoribonuclease from SARS CoV-2 doi: 10.2210/pdb6vww/pdb
Released 2020-03-04
PDB structure 6y2e
L. Zhang, X. Sun, R. Hilgenfeld Crystal structure of the free enzyme of the SARS-CoV-2 (2019-nCoV) main protease doi: 10.2210/pdb6y2e/pdb
Released 2020-03-04
PDB structure 6y2f
L. Zhang, X. Sun, R. Hilgenfeld Crystal structure (monoclinic form) of the complex resulting from the reaction between SARS-CoV-2 (2019-nCoV) main protease and tert-butyl (1-((S)-1-(((S)-4-(benzylamino)-3,4-dioxo-1-((S)-2-oxopyrrolidin-3-yl)butan-2-yl)amino)-3-cyclopropyl-1-oxopropan-2-yl)-2-oxo-1,2-dihydropyridin-3-yl)carbamate (alpha-ketoamide 13b) doi: 10.2210/pdb6y2f/pdb
Released 2020-03-04
PDB structure 6y2g
L. Zhang, X. Sun, R. Hilgenfeld Crystal structure (orthorhombic form) of the complex resulting from the reaction between SARS-CoV-2 (2019-nCoV) main protease and tert-butyl (1-((S)-1-(((S)-4-(benzylamino)-3,4-dioxo-1-((S)-2-oxopyrrolidin-3-yl)butan-2-yl)amino)-3-cyclopropyl-1-oxopropan-2-yl)-2-oxo-1,2-dihydropyridin-3-yl)carbamate (alpha-ketoamide 13b) doi: 10.2210/pdb6y2g/pdb
Released 2020-03-04
Coronavirus disease 2019 (COVID-19) is a global pandemic impacting nearly 170 countries/regions and more than 285,000 patients worldwide. COVID-19 is caused by the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), which invades cells through the angiotensin converting enzyme 2 (ACE2) receptor. Among those with COVID-19, there is a higher prevalence of cardiovascular disease and more than 7% of patients suffer myocardial injury from the infection (22% of the critically ill). Despite ACE2 serving as the portal for infection, the role of ACE inhibitors or angiotensin receptor blockers requires further investigation. COVID-19 poses a challenge for heart transplantation, impacting donor selection, immunosuppression, and post-transplant management. Thankfully there are a number of promising therapies under active investigation to both treat and prevent COVID-19. Key Words: COVID-19; myocardial injury; pandemic; heart transplant
Towler P, Staker B, Prasad SG, Menon S, Tang J, Parsons T, Ryan D, Fisher M, Williams D, Dales NA, Patane MA, Pantoliano MW (Apr 2004). “ACE2 X-ray structures reveal a large hinge-bending motion important for inhibitor binding and catalysis”. The Journal of Biological Chemistry. 279 (17): 17996–8007. doi:10.1074/jbc.M311191200. PMID14754895.
Turner AJ, Tipnis SR, Guy JL, Rice G, Hooper NM (Apr 2002). “ACEH/ACE2 is a novel mammalian metallocarboxypeptidase and a homologue of angiotensin-converting enzyme insensitive to ACE inhibitors”. Canadian Journal of Physiology and Pharmacology. 80 (4): 346–53. doi:10.1139/y02-021. PMID12025971.
Zhang, Haibo; Penninger, Josef M.; Li, Yimin; Zhong, Nanshan; Slutsky, Arthur S. (3 March 2020). “Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target”. Intensive Care Medicine. Springer Science and Business Media LLC. doi:10.1007/s00134-020-05985-9. ISSN0342-4642. PMID32125455.
^Gurwitz, David (2020). “Angiotensin receptor blockers as tentative SARS‐CoV‐2 therapeutics”. Drug Development Research. doi:10.1002/ddr.21656. PMID32129518.
ACE2 receptors have been shown to be the entry point into human cells for some coronaviruses, including the SARSvirus.[10] A number of studies have identified that the entry point is the same for SARS-CoV-2,[11] the virus that causes COVID-19.[12][13][14][15]
Some have suggested that a decrease in ACE2 could be protective against Covid-19 disease[16], but others have suggested the opposite, that Angiotensin II receptor blocker drugs could be protective against Covid-19 disease via increasing ACE2, and that these hypotheses need to be tested by datamining of clinical patient records.[17]
We need your help! Folding@home is joining researchers around the world working to better understand the 2019 Coronavirus (2019-nCoV) to accelerate the open science effort to develop new life-saving therapies. By downloading Folding@Home, you can donate your unused computational resources to the Folding@home Consortium, where researchers working to advance our understanding of the structures of potential drug targets for 2019-nCoV that could aid in the design of new therapies. The data you help us generate will be quickly and openly disseminated as part of an open science collaboration of multiple laboratories around the world, giving researchers new tools that may unlock new opportunities for developing lifesaving drugs.
2019-nCoV is a close cousin to SARS coronavirus (SARS-CoV), and acts in a similar way. For both coronaviruses, the first step of infection occurs in the lungs, when a protein on the surface of the virus binds to a receptor protein on a lung cell. This viral protein is called the spike protein, depicted in red in the image below, and the receptor is known as ACE2. A therapeutic antibody is a type of protein that can block the viral protein from binding to its receptor, therefore preventing the virus from infecting the lung cell. A therapeutic antibody has already been developed for SARS-CoV, but to develop therapeutic antibodies or small molecules for 2019-nCoV, scientists need to better understand the structure of the viral spike protein and how it binds to the human ACE2 receptor required for viral entry into human cells.
Proteins are not stagnant—they wiggle and fold and unfold to take on numerous shapes. We need to study not only one shape of the viral spike protein, but all the ways the protein wiggles and folds into alternative shapes in order to best understand how it interacts with the ACE2 receptor, so that an antibody can be designed. Low-resolution structures of the SARS-CoV spike protein exist and we know the mutations that differ between SARS-CoV and 2019-nCoV. Given this information, we are uniquely positioned to help model the structure of the 2019-nCoV spike protein and identify sites that can be targeted by a therapeutic antibody. We can build computational models that accomplish this goal, but it takes a lot of computing power.
This is where you come in! With many computers working towards the same goal, we aim to help develop a therapeutic remedy as quickly as possible. By downloading Folding@home here [LINK] and selecting to contribute to “Any Disease”, you can help provide us with the computational power required to tackle this problem. One protein from 2019-nCoV, a protease encoded by the viral RNA, has already been crystallized. Although the 2019-nCoV spike protein of interest has not yet been resolved bound to ACE2, our objective is to use the homologous structure of the SARS-CoV spike protein to identify therapeutic antibody targets.
This illustration, created at the Centers for Disease Control and Prevention (CDC), reveals ultrastructural morphology exhibited by coronaviruses. Note the spikes that adorn the outer surface of the virus, which impart the look of a corona surrounding the virion, when viewed electron microscopically. A novel coronavirus virus was identified as the cause of an outbreak of respiratory illness first detected in Wuhan, China in 2019.
Structures of the closely related SARS-CoV spike protein bound by therapeutic antibodies may help rapidly design better therapies. The three monomers of the SARS-CoV spike protein are shown in different shades of red; the antibody is depicted in green. [PDB: 6NB7 https://www.rcsb.org/structure/6nb7]
I am reposting the following Science blog post from Derrick Lowe as is and ask people go browse through the comments on his Science blog In the Pipeline because, as Dr. Lowe states that in this current crisis it is important to disseminate good information as quickly as possible so wanted the readers here to have the ability to read his great posting on this matter of Covid-19. Also i would like to direct readers to the journal Science opinion letter concerning how important it is to rebuild the trust in good science and the scientific process. The full link for the following In the Pipeline post is: https://blogs.sciencemag.org/pipeline/archives/2020/03/06/covid-19-small-molecule-therapies-reviewed
A Summary of current potential repurposed therapeutics for COVID-19 Infection from In The Pipeline: A Science blog from Derick Lowe
Let’s take inventory on the therapies that are being developed for the coronavirus epidemic. Here is a very thorough list of at Biocentury, and I should note that (like Stat and several other organizations) they’re making all their Covid-19 content free to all readers during this crisis. I’d like to zoom in today on the potential small-molecule therapies, since some of these have the most immediate prospects for use in the real world.
The ones at the front of the line are repurposed drugs that are already approved for human use, for a lot of obvious reasons. The Biocentury list doesn’t cover these, but here’s an article at Nature Biotechnology that goes into detail. Clinical trials are a huge time sink – they sort of have to be, in most cases, if they’re going to be any good – and if you’ve already done all that stuff it’s a huge leg up, even if the drug itself is not exactly a perfect fit for the disease. So what do we have? The compound that is most advanced is probably remdesivir from Gilead, at right. This has been in development for a few years as an RNA virus therapy – it was originally developed for Ebola, and has been tried out against a whole list of single-strand RNA viruses. That includes the related coronaviruses SARS and MERS, so Covid-19 was an obvious fit.
The compound is a prodrug – that phosphoramide gets cleaved off completely, leaving the active 5-OH compound GS-44-1524. It mechanism of action is to get incorporated into viral RNA, since it’s taken up by RNA polymerase and it largely seems to evade proofreading. This causes RNA termination trouble later on, since that alpha-nitrile C-nucleoside is not exactly what the virus is expecting in its genome at that point, and thus viral replication is inhibited.
There are five clinical trials underway (here’s an overview at Biocentury). The NIH has an adaptive-design Phase II trial that has already started in Nebraska, with doses to be changed according to Bayesian readouts along the way. There are two Phase III trials underway at China-Japan Friendship Hospital in Hubei, double-blinded and placebo-controlled (since placebo is, as far as drug therapy goes, the current standard of care). And Gilead themselves are starting two open-label trials, one with no control arm and one with an (unblinded) standard-of-care comparison arm. Those might read out first, depending on when they get off the ground, but will be only rough readouts due to the fast-and-loose trial design. The two Hubei trials and the NIH one will add some rigor to the process, but I’m not sure when they’re going to report. My personal opinion is that I like the chances of this drug more than anything else on this list, but it’s still unlikely to be a game-changer.
There’s an RNA polymerase inhibitor (favipiravir) from Toyama, at right, that’s in a trial in China. It’s a thought – a broad-spectrum agent of this sort would be the sort of thing to try. But unfortunately, from what I can see, it has already turned up as ineffective in in vitro tests. The human trial that’s underway is honestly the sort of thing that would only happen under circumstances like the present: a developing epidemic with a new pathogen and no real standard of care. I hold out little hope for this one, but given that there’s nothing else at present, it probably should be tried. As you’ll see, this is far from the only situation like this.
One of the screens of known drugs in China that also flagged remdesivir noted that the old antimalarial drug chloroquine seemed to be effective in vitro. It had been reported some years back as a possible antiviral, working through more than one mechanism, probably both at viral entry and intracellularly thereafter. That part shouldn’t be surprising – chloroquine’s actual mode(s) of action against malaria parasites are still not completely worked out, either, and some of what people thought they knew about it has turned out to be wrong. There are several trials underway with it at Chinese facilities, some in combination with other agents like remdesivir. Chloroquine has of course been taken for many decades as an antimalarial, but it has a number of liabilities, including seizures, hearing damage, retinopathy and sudden effects on blood glucose. So it’s going to be important to establish just how effective it is and what doses will be needed. Just as with vaccine candidates, it’s possible to do more harm with a rushed treatment than the disease is doing itself
There are several other known antiviral drugs are being tried in China, but I don’t have too much hope for those, either. The neuraminidase inhibitors such as oseltamivir (better known as Tamiflu) were tried against SARS and were ineffective; there is no reason to expect anything versus Covid-19 although these drugs are a component of some drug cocktail trials. The HIV protease therapies such as darunavir and the combination therapy Kaletra are in trials, but that’s also a rather desperate long shot, since there’s no particular reason to think that they will have any such protease inhibition against what this new virus has to offer (and indeed, such agents weren’t much help against SARS in the end, either). The classic interferon/ribavirin combination seems to have had some activity against SARS and MERS, and is in two trials from what I can see. That’s not an awful idea by any means, but it’s not a great one, either: if your viral disease has interferon/ribavirin as a front line therapy, it generally means that there’s nothing really good available. No, unless we get really lucky none of these ideas are going to slow the disease down much.
There are a few other repurposed-protease-inhibitors ideas out there, such as this one. (Edit: I had seen this paper but couldn’t track it down, so thanks to those who sent it along). This paper suggests that the TMPRSS2 protease is important for viral entry on the human-cell-side of the process, a pathway that has been noted for other coronaviruses. And it points out that there is a an approved inhibitor (in Japan) for this enzyme (camostat), so that would definitely seem to be worth a trial, probably in combination with remdesivir.
That’s about it for the existing small molecules, from what I can see. What about new ones? Don’t hold your breath, is all I can say. A drug discovery program from scratch against a new pathogen is, as many readers here well know, not a trivial exercise. As this Bloomberg article details, many such efforts in the past (small molecules and vaccines alike) have come to grief because by the time they had anything to deliver the epidemic itself had passed. Indeed, Gilead’s remdesivir had already been dropped as a potential Ebola therapy.
You will either need to have a target in mind up front or go phenotypic. For the former, what you’d see are better characterizations of the viral protease and more extensive screens against it. Two other big target areas are viral entry (which involves the “spike” proteins on the virus surface and the ACE2 protein on human cells) and viral replication. To the former, it’s worth quickly noting that ACE2 is so much unlike the more familiar ACE protein that none of the cardiovascular ACE inhibitors do anything to it at all. And targeting the latter mechanisms is how remdesivir was developed as a possible Ebola agent, but as you can see, that took time, too. Phenotypic screens are perfectly reasonable against viral pathogens as well, but you’ll need to put time and effort into that assay up front, just as with any phenotypic effort, because as anyone who does that sort of work will tell you, a bad phenotypic screen is a complete waste of everyone’s time.
One of the key steps for either route is identifying an animal model. While animal models of infectious disease can be extremely well translated to human therapy, that doesn’t happen by accident: you need to choose the right animal. Viruses in general (and coronaviruses are no exception) vary widely in their effects in different species, and not just across the gaps of bird/reptile/human and the like. No, you’ll run into things where even the usual set of small mammals are acting differently from each other, with some of them not even getting sick at all. This current virus may well have gone through a couple of other mammalian species before landing on us, but you’ll note that dogs (to pick one) don’t seem to have any problem with it.
All this means that any new-target new-chemical-matter effort against Covid-19 (or any new pathogen) is going to take years, and there is just no way around that. Update: see here for just such an effort to start finding fragment hits for the viral protease. This puts small molecules in a very bimodal distribution: you have the existing drugs that might be repurposed, and are presumably available right now. Nothing else is! At the other end, for completely new therapies you have the usual prospects of drug discovery: years from now, lots of money, low success rate, good luck to all of us. The gap between these two could in theory be filled by vaccines and antibody therapies (if everything goes really, really well) but those are very much their own area and will be dealt with in a separate post.
Either way, the odds are that we (and I mean “we as a species” here) are going to be fighting this epidemic without any particularly amazing pharmacological weapons. Eventually we’ll have some, but I would advise people, pundits, and politicians not to get all excited about the prospects for some new therapies to come riding up over the hill to help us out. The odds of that happening in time to do anything about the current outbreak are very small. We will be going for months, years, with the therapeutic options we have right now. Look around you: what we have today is what we have to work with.
Other related articles published in this Open Access Online Scientific Journal include the following:
Group of Researchers @ University of California, Riverside, the University of Chicago, the U.S. Department of Energy’s Argonne National Laboratory, and Northwestern University solve COVID-19 Structure and Map Potential Therapeutics
Reporters: Stephen J Williams, PhD and Aviva Lev-Ari, PhD, RN
Predicting the Protein Structure of Coronavirus: Inhibition of Nsp15 can slow viral replication and Cryo-EM – Spike protein structure (experimentally verified) vs AI-predicted protein structures (not experimentally verified) of DeepMind (Parent: Google) aka AlphaFold
Curators: Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN










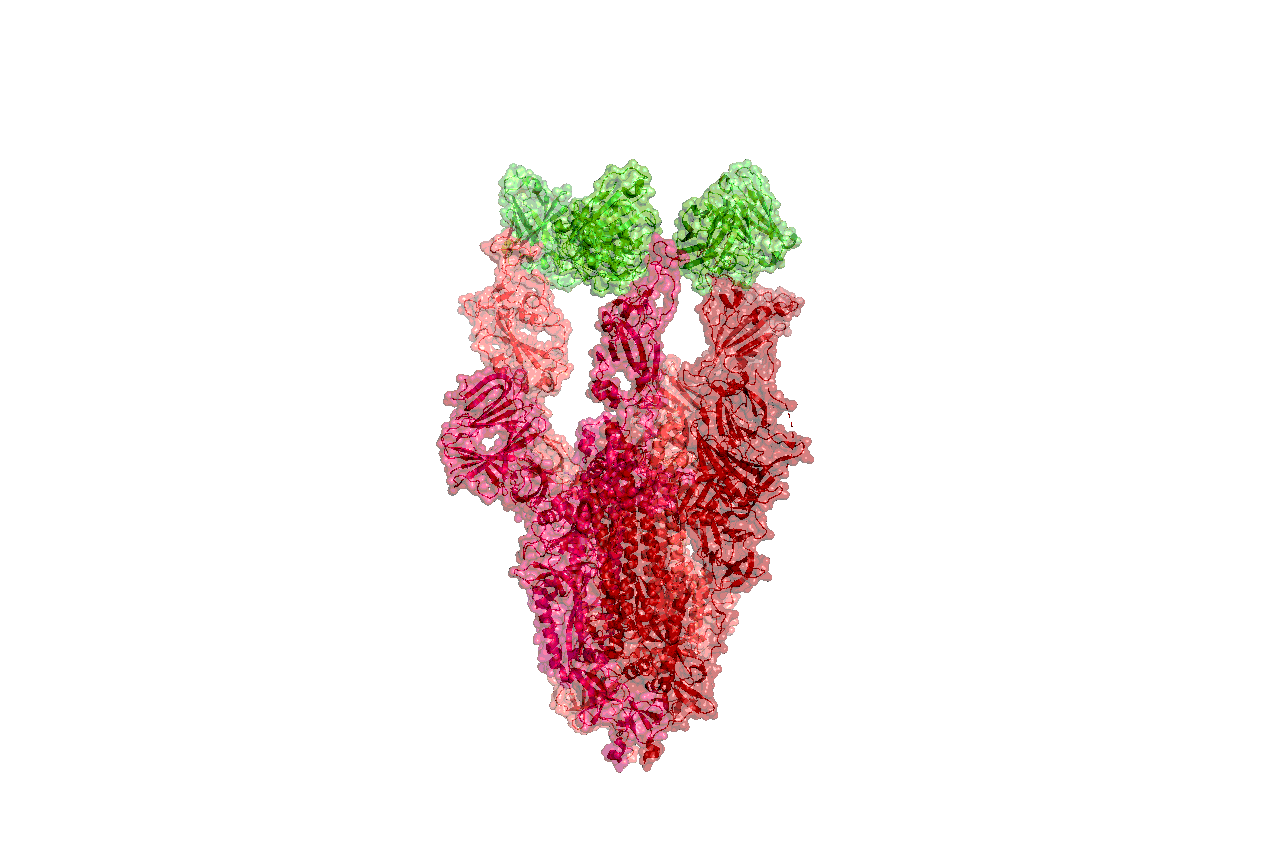




30489-X&id=fx1.jpg){kind=link}