Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Structure-guided Drug Discovery: (1) The Coronavirus 3CL hydrolase (Mpro) enzyme (main protease) essential for proteolytic maturation of the virus and (2) viral protease, the RNA polymerase, the viral spike protein, a viral RNA as promising two targets for discovery of cleavage inhibitors of the viral spike polyprotein preventing the Coronavirus Virion the spread of infection
Curators and Reporters: Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN
Therapeutical options to coronavirus (2019-nCoV) include consideration of the following:
(a) Monoclonal and polyclonal antibodies
(b) Vaccines
(c) Small molecule treatments (e.g., chloroquinolone and derivatives), including compounds already approved for other indications
(d) Immuno-therapies derived from human or other sources
Structure of the nCoV trimeric spike
The World Health Organization has declared the outbreak of a novel coronavirus (2019-nCoV) to be a public health emergency of international concern. The virus binds to host cells through its trimeric spike glycoprotein, making this protein a key target for potential therapies and diagnostics. Wrapp et al. determined a 3.5-angstrom-resolution structure of the 2019-nCoV trimeric spike protein by cryo–electron microscopy. Using biophysical assays, the authors show that this protein binds at least 10 times more tightly than the corresponding spike protein of severe acute respiratory syndrome (SARS)–CoV to their common host cell receptor. They also tested three antibodies known to bind to the SARS-CoV spike protein but did not detect binding to the 2019-nCoV spike protein. These studies provide valuable information to guide the development of medical counter-measures for 2019-nCoV. [Bold Face Added by ALA]
The outbreak of a novel coronavirus (2019-nCoV) represents a pandemic threat that has been declared a public health emergency of international concern. The CoV spike (S) glycoprotein is a key target for vaccines, therapeutic antibodies, and diagnostics. To facilitate medical countermeasure development, we determined a 3.5-angstrom-resolution cryo–electron microscopy structure of the 2019-nCoV S trimer in the prefusion conformation. The predominant state of the trimer has one of the three receptor-binding domains (RBDs) rotated up in a receptor-accessible conformation. We also provide biophysical and structural evidence that the 2019-nCoV S protein binds angiotensin-converting enzyme 2 (ACE2) with higher affinity than does severe acute respiratory syndrome (SARS)-CoV S. Additionally, we tested several published SARS-CoV RBD-specific monoclonal antibodies and found that they do not have appreciable binding to 2019-nCoV S, suggesting that antibody cross-reactivity may be limited between the two RBDs. The structure of 2019-nCoV S should enable the rapid development and evaluation of medical countermeasures to address the ongoing public health crisis.
SOURCE
Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation
Recent emergence of the COVID-19 coronavirus has resulted in a WHO-declared public health emergency of international concern. Research efforts around the world are working towards establishing a greater understanding of this particular virus and developing treatments and vaccines to prevent further spread.
While PDB entry 6lu7 is currently the only public-domain 3D structure from this specific coronavirus, the PDB contains structures of the corresponding enzyme from other coronaviruses. The 2003 outbreak of the closely-related Severe Acute Respiratory Syndrome-related coronavirus (SARS) led to the first 3D structures, and today there are more than 200 PDB structures of SARS proteins. Structural information from these related proteins could be vital in furthering our understanding of coronaviruses and in discovery and development of new treatments and vaccines to contain the current outbreak.
The coronavirus 3CL hydrolase (Mpro) enzyme, also known as the main protease, is essential for proteolytic maturation of the virus. It is thought to be a promising target for discovery of small-molecule drugs that would inhibit cleavage of the viral polyprotein and prevent spread of the infection.
Comparison of the protein sequence of the COVID-19 coronavirus 3CL hydrolase (Mpro) against the PDB archive identified 95 PDB proteins with at least 90% sequence identity. Furthermore, these related protein structures contain approximately 30 distinct small molecule inhibitors, which could guide discovery of new drugs. Of particular significance for drug discovery is the very high amino acid sequence identity (96%) between the COVID-19 coronavirus 3CL hydrolase (Mpro) and the SARS virus main protease (PDB 1q2w). Summary data about these closely-related PDB structures are available (CSV) to help researchers more easily find this information. In addition, the PDB houses 3D structure data for more than 20 unique SARS proteins represented in more than 200 PDB structures, including a second viral protease, the RNA polymerase, the viral spike protein, a viral RNA, and other proteins (CSV).
Public release of the COVID-19 coronavirus 3CL hydrolase (Mpro), at a time when this information can prove most vital and valuable, highlights the importance of open and timely availability of scientific data. The wwPDB strives to ensure that 3D biological structure data remain freely accessible for all, while maintaining as comprehensive and accurate an archive as possible. We hope that this new structure, and those from related viruses, will help researchers and clinicians address the COVID-19 coronavirus global public health emergency.
Update: Released COVID-19-related PDB structures include
PDB structure 6lu7 (X. Liu, B. Zhang, Z. Jin, H. Yang, Z. Rao Crystal structure of COVID-19 main protease in complex with an inhibitor N3 doi: 10.2210/pdb6lu7/pdb) Released 2020-02-05
PDB structure 6vsb (D. Wrapp, N. Wang, K.S. Corbett, J.A. Goldsmith, C.-L. Hsieh, O. Abiona, B.S. Graham, J.S. McLellan (2020) Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation Science doi: 10.1126/science.abb2507) Released 2020-02-26
PDB structure 6lxt (Y. Zhu, F. Sun Structure of post fusion core of 2019-nCoV S2 subunit doi: 10.2210/pdb6lxt/pdb) Released 2020-02-26
PDB structure 6lvn (Y. Zhu, F. Sun Structure of the 2019-nCoV HR2 Domain doi: 10.2210/pdb6lvn/pdb) Released 2020-02-26
PDB structure 6vw1
J. Shang, G. Ye, K. Shi, Y.S. Wan, H. Aihara, F. Li Structural basis for receptor recognition by the novel coronavirus from Wuhan doi: 10.2210/pdb6vw1/pdb
Released 2020-03-04
PDB structure 6vww
Y. Kim, R. Jedrzejczak, N. Maltseva, M. Endres, A. Godzik, K. Michalska, A. Joachimiak, Center for Structural Genomics of Infectious Diseases Crystal Structure of NSP15 Endoribonuclease from SARS CoV-2 doi: 10.2210/pdb6vww/pdb
Released 2020-03-04
PDB structure 6y2e
L. Zhang, X. Sun, R. Hilgenfeld Crystal structure of the free enzyme of the SARS-CoV-2 (2019-nCoV) main protease doi: 10.2210/pdb6y2e/pdb
Released 2020-03-04
PDB structure 6y2f
L. Zhang, X. Sun, R. Hilgenfeld Crystal structure (monoclinic form) of the complex resulting from the reaction between SARS-CoV-2 (2019-nCoV) main protease and tert-butyl (1-((S)-1-(((S)-4-(benzylamino)-3,4-dioxo-1-((S)-2-oxopyrrolidin-3-yl)butan-2-yl)amino)-3-cyclopropyl-1-oxopropan-2-yl)-2-oxo-1,2-dihydropyridin-3-yl)carbamate (alpha-ketoamide 13b) doi: 10.2210/pdb6y2f/pdb
Released 2020-03-04
PDB structure 6y2g
L. Zhang, X. Sun, R. Hilgenfeld Crystal structure (orthorhombic form) of the complex resulting from the reaction between SARS-CoV-2 (2019-nCoV) main protease and tert-butyl (1-((S)-1-(((S)-4-(benzylamino)-3,4-dioxo-1-((S)-2-oxopyrrolidin-3-yl)butan-2-yl)amino)-3-cyclopropyl-1-oxopropan-2-yl)-2-oxo-1,2-dihydropyridin-3-yl)carbamate (alpha-ketoamide 13b) doi: 10.2210/pdb6y2g/pdb
Released 2020-03-04
Coronavirus disease 2019 (COVID-19) is a global pandemic impacting nearly 170 countries/regions and more than 285,000 patients worldwide. COVID-19 is caused by the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), which invades cells through the angiotensin converting enzyme 2 (ACE2) receptor. Among those with COVID-19, there is a higher prevalence of cardiovascular disease and more than 7% of patients suffer myocardial injury from the infection (22% of the critically ill). Despite ACE2 serving as the portal for infection, the role of ACE inhibitors or angiotensin receptor blockers requires further investigation. COVID-19 poses a challenge for heart transplantation, impacting donor selection, immunosuppression, and post-transplant management. Thankfully there are a number of promising therapies under active investigation to both treat and prevent COVID-19. Key Words: COVID-19; myocardial injury; pandemic; heart transplant
Towler P, Staker B, Prasad SG, Menon S, Tang J, Parsons T, Ryan D, Fisher M, Williams D, Dales NA, Patane MA, Pantoliano MW (Apr 2004). “ACE2 X-ray structures reveal a large hinge-bending motion important for inhibitor binding and catalysis”. The Journal of Biological Chemistry. 279 (17): 17996–8007. doi:10.1074/jbc.M311191200. PMID14754895.
Turner AJ, Tipnis SR, Guy JL, Rice G, Hooper NM (Apr 2002). “ACEH/ACE2 is a novel mammalian metallocarboxypeptidase and a homologue of angiotensin-converting enzyme insensitive to ACE inhibitors”. Canadian Journal of Physiology and Pharmacology. 80 (4): 346–53. doi:10.1139/y02-021. PMID12025971.
Zhang, Haibo; Penninger, Josef M.; Li, Yimin; Zhong, Nanshan; Slutsky, Arthur S. (3 March 2020). “Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target”. Intensive Care Medicine. Springer Science and Business Media LLC. doi:10.1007/s00134-020-05985-9. ISSN0342-4642. PMID32125455.
^Gurwitz, David (2020). “Angiotensin receptor blockers as tentative SARS‐CoV‐2 therapeutics”. Drug Development Research. doi:10.1002/ddr.21656. PMID32129518.
ACE2 receptors have been shown to be the entry point into human cells for some coronaviruses, including the SARSvirus.[10] A number of studies have identified that the entry point is the same for SARS-CoV-2,[11] the virus that causes COVID-19.[12][13][14][15]
Some have suggested that a decrease in ACE2 could be protective against Covid-19 disease[16], but others have suggested the opposite, that Angiotensin II receptor blocker drugs could be protective against Covid-19 disease via increasing ACE2, and that these hypotheses need to be tested by datamining of clinical patient records.[17]
We need your help! Folding@home is joining researchers around the world working to better understand the 2019 Coronavirus (2019-nCoV) to accelerate the open science effort to develop new life-saving therapies. By downloading Folding@Home, you can donate your unused computational resources to the Folding@home Consortium, where researchers working to advance our understanding of the structures of potential drug targets for 2019-nCoV that could aid in the design of new therapies. The data you help us generate will be quickly and openly disseminated as part of an open science collaboration of multiple laboratories around the world, giving researchers new tools that may unlock new opportunities for developing lifesaving drugs.
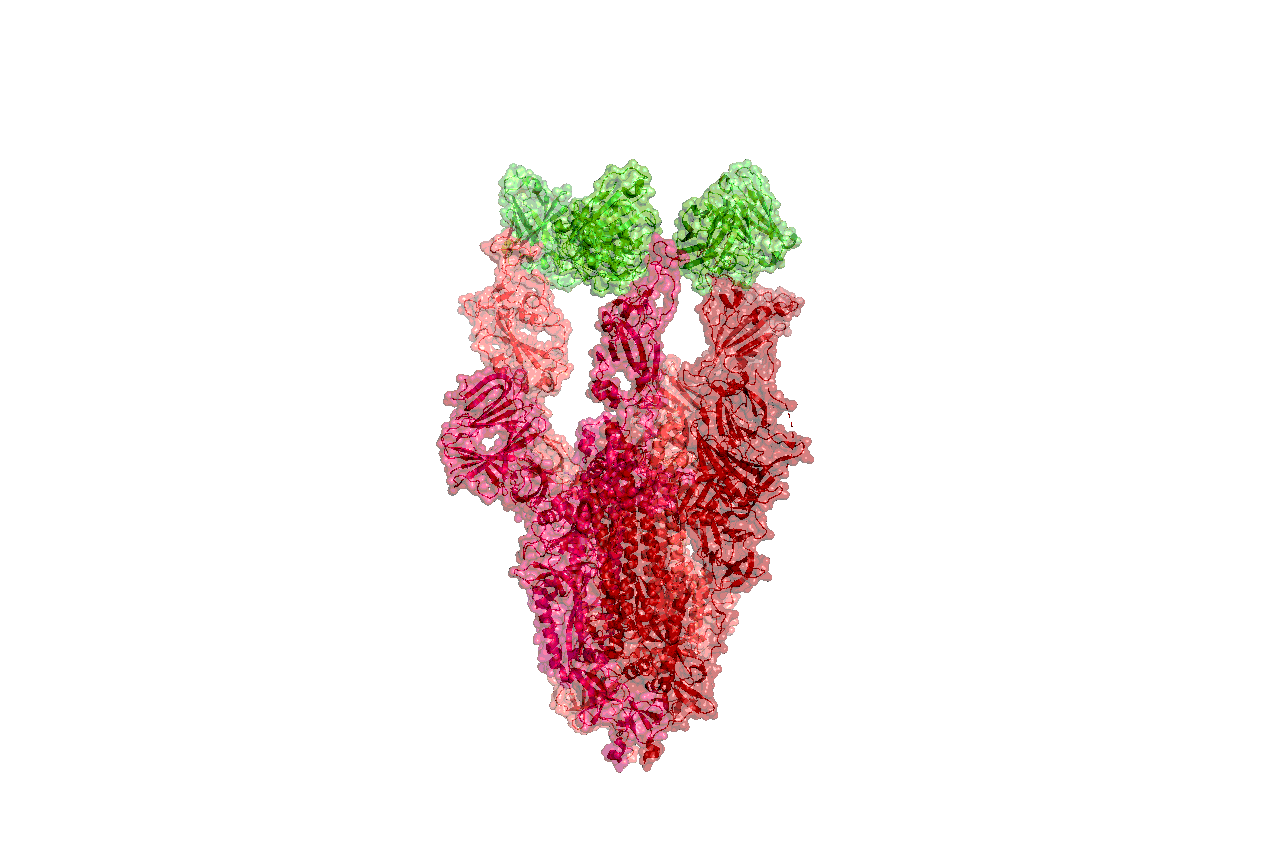
2019-nCoV is a close cousin to SARS coronavirus (SARS-CoV), and acts in a similar way. For both coronaviruses, the first step of infection occurs in the lungs, when a protein on the surface of the virus binds to a receptor protein on a lung cell. This viral protein is called the spike protein, depicted in red in the image below, and the receptor is known as ACE2. A therapeutic antibody is a type of protein that can block the viral protein from binding to its receptor, therefore preventing the virus from infecting the lung cell. A therapeutic antibody has already been developed for SARS-CoV, but to develop therapeutic antibodies or small molecules for 2019-nCoV, scientists need to better understand the structure of the viral spike protein and how it binds to the human ACE2 receptor required for viral entry into human cells.
Proteins are not stagnant—they wiggle and fold and unfold to take on numerous shapes. We need to study not only one shape of the viral spike protein, but all the ways the protein wiggles and folds into alternative shapes in order to best understand how it interacts with the ACE2 receptor, so that an antibody can be designed. Low-resolution structures of the SARS-CoV spike protein exist and we know the mutations that differ between SARS-CoV and 2019-nCoV. Given this information, we are uniquely positioned to help model the structure of the 2019-nCoV spike protein and identify sites that can be targeted by a therapeutic antibody. We can build computational models that accomplish this goal, but it takes a lot of computing power.
This is where you come in! With many computers working towards the same goal, we aim to help develop a therapeutic remedy as quickly as possible. By downloading Folding@home here [LINK] and selecting to contribute to “Any Disease”, you can help provide us with the computational power required to tackle this problem. One protein from 2019-nCoV, a protease encoded by the viral RNA, has already been crystallized. Although the 2019-nCoV spike protein of interest has not yet been resolved bound to ACE2, our objective is to use the homologous structure of the SARS-CoV spike protein to identify therapeutic antibody targets.
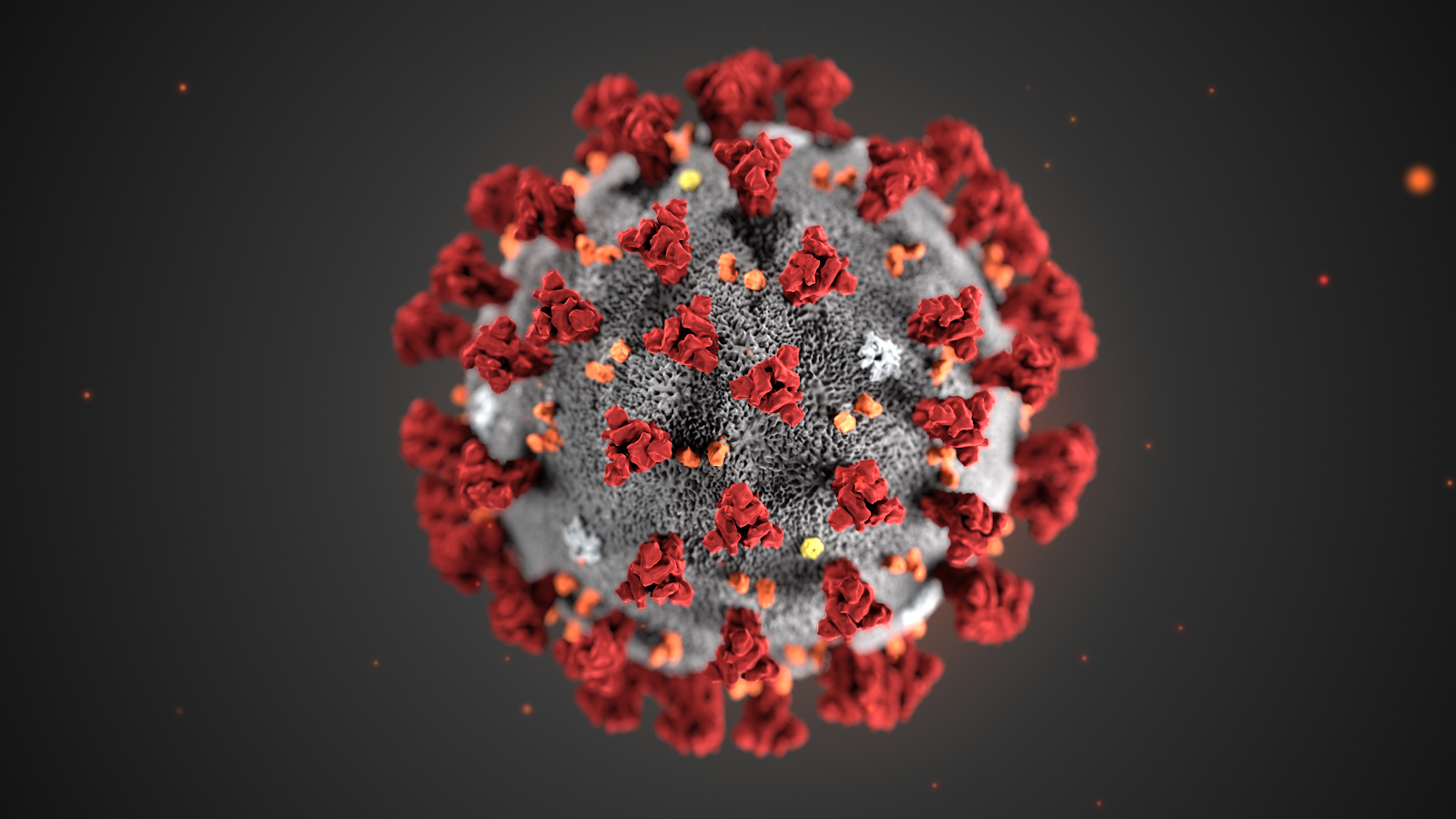
This illustration, created at the Centers for Disease Control and Prevention (CDC), reveals ultrastructural morphology exhibited by coronaviruses. Note the spikes that adorn the outer surface of the virus, which impart the look of a corona surrounding the virion, when viewed electron microscopically. A novel coronavirus virus was identified as the cause of an outbreak of respiratory illness first detected in Wuhan, China in 2019.
Structures of the closely related SARS-CoV spike protein bound by therapeutic antibodies may help rapidly design better therapies. The three monomers of the SARS-CoV spike protein are shown in different shades of red; the antibody is depicted in green. [PDB: 6NB7 https://www.rcsb.org/structure/6nb7]
I am reposting the following Science blog post from Derrick Lowe as is and ask people go browse through the comments on his Science blog In the Pipeline because, as Dr. Lowe states that in this current crisis it is important to disseminate good information as quickly as possible so wanted the readers here to have the ability to read his great posting on this matter of Covid-19. Also i would like to direct readers to the journal Science opinion letter concerning how important it is to rebuild the trust in good science and the scientific process. The full link for the following In the Pipeline post is: https://blogs.sciencemag.org/pipeline/archives/2020/03/06/covid-19-small-molecule-therapies-reviewed
A Summary of current potential repurposed therapeutics for COVID-19 Infection from In The Pipeline: A Science blog from Derick Lowe
Let’s take inventory on the therapies that are being developed for the coronavirus epidemic. Here is a very thorough list of at Biocentury, and I should note that (like Stat and several other organizations) they’re making all their Covid-19 content free to all readers during this crisis. I’d like to zoom in today on the potential small-molecule therapies, since some of these have the most immediate prospects for use in the real world.
The ones at the front of the line are repurposed drugs that are already approved for human use, for a lot of obvious reasons. The Biocentury list doesn’t cover these, but here’s an article at Nature Biotechnology that goes into detail. Clinical trials are a huge time sink – they sort of have to be, in most cases, if they’re going to be any good – and if you’ve already done all that stuff it’s a huge leg up, even if the drug itself is not exactly a perfect fit for the disease. So what do we have? The compound that is most advanced is probably remdesivir from Gilead, at right. This has been in development for a few years as an RNA virus therapy – it was originally developed for Ebola, and has been tried out against a whole list of single-strand RNA viruses. That includes the related coronaviruses SARS and MERS, so Covid-19 was an obvious fit.
The compound is a prodrug – that phosphoramide gets cleaved off completely, leaving the active 5-OH compound GS-44-1524. It mechanism of action is to get incorporated into viral RNA, since it’s taken up by RNA polymerase and it largely seems to evade proofreading. This causes RNA termination trouble later on, since that alpha-nitrile C-nucleoside is not exactly what the virus is expecting in its genome at that point, and thus viral replication is inhibited.
There are five clinical trials underway (here’s an overview at Biocentury). The NIH has an adaptive-design Phase II trial that has already started in Nebraska, with doses to be changed according to Bayesian readouts along the way. There are two Phase III trials underway at China-Japan Friendship Hospital in Hubei, double-blinded and placebo-controlled (since placebo is, as far as drug therapy goes, the current standard of care). And Gilead themselves are starting two open-label trials, one with no control arm and one with an (unblinded) standard-of-care comparison arm. Those might read out first, depending on when they get off the ground, but will be only rough readouts due to the fast-and-loose trial design. The two Hubei trials and the NIH one will add some rigor to the process, but I’m not sure when they’re going to report. My personal opinion is that I like the chances of this drug more than anything else on this list, but it’s still unlikely to be a game-changer.
There’s an RNA polymerase inhibitor (favipiravir) from Toyama, at right, that’s in a trial in China. It’s a thought – a broad-spectrum agent of this sort would be the sort of thing to try. But unfortunately, from what I can see, it has already turned up as ineffective in in vitro tests. The human trial that’s underway is honestly the sort of thing that would only happen under circumstances like the present: a developing epidemic with a new pathogen and no real standard of care. I hold out little hope for this one, but given that there’s nothing else at present, it probably should be tried. As you’ll see, this is far from the only situation like this.
One of the screens of known drugs in China that also flagged remdesivir noted that the old antimalarial drug chloroquine seemed to be effective in vitro. It had been reported some years back as a possible antiviral, working through more than one mechanism, probably both at viral entry and intracellularly thereafter. That part shouldn’t be surprising – chloroquine’s actual mode(s) of action against malaria parasites are still not completely worked out, either, and some of what people thought they knew about it has turned out to be wrong. There are several trials underway with it at Chinese facilities, some in combination with other agents like remdesivir. Chloroquine has of course been taken for many decades as an antimalarial, but it has a number of liabilities, including seizures, hearing damage, retinopathy and sudden effects on blood glucose. So it’s going to be important to establish just how effective it is and what doses will be needed. Just as with vaccine candidates, it’s possible to do more harm with a rushed treatment than the disease is doing itself
There are several other known antiviral drugs are being tried in China, but I don’t have too much hope for those, either. The neuraminidase inhibitors such as oseltamivir (better known as Tamiflu) were tried against SARS and were ineffective; there is no reason to expect anything versus Covid-19 although these drugs are a component of some drug cocktail trials. The HIV protease therapies such as darunavir and the combination therapy Kaletra are in trials, but that’s also a rather desperate long shot, since there’s no particular reason to think that they will have any such protease inhibition against what this new virus has to offer (and indeed, such agents weren’t much help against SARS in the end, either). The classic interferon/ribavirin combination seems to have had some activity against SARS and MERS, and is in two trials from what I can see. That’s not an awful idea by any means, but it’s not a great one, either: if your viral disease has interferon/ribavirin as a front line therapy, it generally means that there’s nothing really good available. No, unless we get really lucky none of these ideas are going to slow the disease down much.
There are a few other repurposed-protease-inhibitors ideas out there, such as this one. (Edit: I had seen this paper but couldn’t track it down, so thanks to those who sent it along). This paper suggests that the TMPRSS2 protease is important for viral entry on the human-cell-side of the process, a pathway that has been noted for other coronaviruses. And it points out that there is a an approved inhibitor (in Japan) for this enzyme (camostat), so that would definitely seem to be worth a trial, probably in combination with remdesivir.
That’s about it for the existing small molecules, from what I can see. What about new ones? Don’t hold your breath, is all I can say. A drug discovery program from scratch against a new pathogen is, as many readers here well know, not a trivial exercise. As this Bloomberg article details, many such efforts in the past (small molecules and vaccines alike) have come to grief because by the time they had anything to deliver the epidemic itself had passed. Indeed, Gilead’s remdesivir had already been dropped as a potential Ebola therapy.
You will either need to have a target in mind up front or go phenotypic. For the former, what you’d see are better characterizations of the viral protease and more extensive screens against it. Two other big target areas are viral entry (which involves the “spike” proteins on the virus surface and the ACE2 protein on human cells) and viral replication. To the former, it’s worth quickly noting that ACE2 is so much unlike the more familiar ACE protein that none of the cardiovascular ACE inhibitors do anything to it at all. And targeting the latter mechanisms is how remdesivir was developed as a possible Ebola agent, but as you can see, that took time, too. Phenotypic screens are perfectly reasonable against viral pathogens as well, but you’ll need to put time and effort into that assay up front, just as with any phenotypic effort, because as anyone who does that sort of work will tell you, a bad phenotypic screen is a complete waste of everyone’s time.
One of the key steps for either route is identifying an animal model. While animal models of infectious disease can be extremely well translated to human therapy, that doesn’t happen by accident: you need to choose the right animal. Viruses in general (and coronaviruses are no exception) vary widely in their effects in different species, and not just across the gaps of bird/reptile/human and the like. No, you’ll run into things where even the usual set of small mammals are acting differently from each other, with some of them not even getting sick at all. This current virus may well have gone through a couple of other mammalian species before landing on us, but you’ll note that dogs (to pick one) don’t seem to have any problem with it.
All this means that any new-target new-chemical-matter effort against Covid-19 (or any new pathogen) is going to take years, and there is just no way around that. Update: see here for just such an effort to start finding fragment hits for the viral protease. This puts small molecules in a very bimodal distribution: you have the existing drugs that might be repurposed, and are presumably available right now. Nothing else is! At the other end, for completely new therapies you have the usual prospects of drug discovery: years from now, lots of money, low success rate, good luck to all of us. The gap between these two could in theory be filled by vaccines and antibody therapies (if everything goes really, really well) but those are very much their own area and will be dealt with in a separate post.
Either way, the odds are that we (and I mean “we as a species” here) are going to be fighting this epidemic without any particularly amazing pharmacological weapons. Eventually we’ll have some, but I would advise people, pundits, and politicians not to get all excited about the prospects for some new therapies to come riding up over the hill to help us out. The odds of that happening in time to do anything about the current outbreak are very small. We will be going for months, years, with the therapeutic options we have right now. Look around you: what we have today is what we have to work with.
Other related articles published in this Open Access Online Scientific Journal include the following:
Group of Researchers @ University of California, Riverside, the University of Chicago, the U.S. Department of Energy’s Argonne National Laboratory, and Northwestern University solve COVID-19 Structure and Map Potential Therapeutics
Reporters: Stephen J Williams, PhD and Aviva Lev-Ari, PhD, RN
Predicting the Protein Structure of Coronavirus: Inhibition of Nsp15 can slow viral replication and Cryo-EM – Spike protein structure (experimentally verified) vs AI-predicted protein structures (not experimentally verified) of DeepMind (Parent: Google) aka AlphaFold
Curators: Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN
Effective humoral immune responses to infection and immunization are defined by high-affinity antibodies generated as a result of B cell differentiation and selection that occurs within germinal centers (GC). Within the GC, B cells undergo affinity maturation, an iterative and competitive process wherein B cells mutate their immunoglobulin genes (somatic hypermutation) and undergo clonal selection by competing for T cell help. Balancing the decision to remain within the GC and continue participating in affinity maturation or to exit the GC as a plasma cell (PC) or memory B cell (MBC) is critical for achieving optimal antibody avidity, antibody quantity, and establishing immunological memory in response to immunization or infection. Humoral immune responses during chronic infections are often dysregulated and characterized by hypergammaglobulinemia, decreased affinity maturation, and delayed development of neutralizing antibodies. Previous studies have suggested that poor antibody quality is in part due to deletion of B cells prior to establishment of the GC response.
In fact the impact of chronic infections on B cell fate decisions in the GC remains poorly understood. To address this question, researchers used single-cell transcriptional profiling of virus-specific GC B cells to test the hypothesis that chronic viral infection disrupted GC B cell fate decisions leading to suboptimal humoral immunity. These studies revealed a critical GC differentiation checkpoint that is disrupted by chronic infection, specifically at the point of dark zone re-entry. During chronic viral infection, virus-specific GC B cells were shunted towards terminal plasma cell (PC) or memory B cell (MBC) fates at the expense of continued participation in the GC. Early GC exit was associated with decreased B cell mutational burden and antibody quality. Persisting antigen and inflammation independently drove facets of dysregulation, with a key role for inflammation in directing premature terminal GC B cell differentiation and GC exit. Thus, the present research defines GC defects during chronic viral infection and identify a critical GC checkpoint that is short-circuited, preventing optimal maturation of humoral immunity.
Together, these studies identify a key GC B cell differentiation checkpoint that is dysregulated during chronic infection. Further, it was found that the chronic inflammatory environment, rather than persistent antigen, is sufficient to drive altered GC B cell differentiation during chronic infection even against unrelated antigens. However, the data also indicate that inflammatory circuits are likely linked to perception of antigen stimulation. Nevertheless, this study reveals a B cell-intrinsic program of transcriptional skewing in chronic viral infection that results in shunting out of the cyclic GC B cell process and early GC exit with consequences for antibody quality and hypergammaglobulinemia. These findings have implications for vaccination in individuals with pre-existing chronic infections where antibody responses are often ineffective and suggest that modulation of inflammatory pathways may be therapeutically useful to overcome impaired humoral immunity and foster affinity maturation during chronic viral infections.
One of the most contagious diseases known to humankind, measles killed an average of 2.6 million people each year before a vaccine was developed, according to the World Health Organization. Widespread vaccination has slashed the death toll. However, lack of access to vaccination and refusal to get vaccinated means measles still infects more than 7 million people and kills more than 100,000 each year worldwide as reported by WHO. The cases are on the rise, tripling in early 2019 and some experience well-known long-term consequences, including brain damage and vision and hearing loss. Previous epidemiological research into immune amnesia suggests that death rates attributed to measles could be even higher, accounting for as much as 50 percent of all childhood mortality.
Over the last decade, evidence has mounted that the measles vaccine protects in two ways. It prevents the well-known acute illness with spots and fever and also appears to protect from other infections over the long term by giving general boost to the immune system. The measles virus can impair the body’s immune memory, causing so-called immune amnesia. By protecting against measles infection, the vaccine prevents the body from losing or “forgetting” its immune memory and preserves its resistance to other infections. Researchers showed that the measles virus wipes out 11% to 73% of the different antibodies that protect against viral and bacterial strains a person was previously immune to like from influenza to herpes virus to bacteria that cause pneumonia and skin infections.
This study at Harvard Medical School and their collaborators is the first to measure the immune damage caused by the virus and underscores the value of preventing measles infection through vaccination. The discovery that measles depletes people’s antibody repertoires, partially obliterating immune memory to most previously encountered pathogens, supports the immune amnesia hypothesis. It was found that those who survive measles gradually regain their previous immunity to other viruses and bacteria as they get re-exposed to them. But because this process may take months to years, people remain vulnerable in the meantime to serious complications of those infections and thus booster shots of routine vaccines may be required.
VirScan detects antiviral and antibacterial antibodies in the blood that result from current or past encounters with viruses and bacteria, giving an overall snapshot of the immune system. Researchers gathered blood samples from unvaccinated children during a 2013 measles outbreak in the Netherlands and used VirScan to measure antibodies before and two months after infection in 77 children who’d contracted the disease. The researchers also compared the measurements to those of 115 uninfected children and adults. Researchers found a striking drop in antibodies from other pathogens in the measles-infected children that clearly suggested a direct effect on the immune system resembling measles-induced immune amnesia.
Further tests revealed that severe measles infection reduced people’s overall immunity more than mild infection. This could be particularly problematic for certain categories of children and adults, the researchers said. The present study observed the effects in previously healthy children only. But, measles is known to hit malnourished children much harder, the degree of immune amnesia and its effects could be even more severe in less healthy populations. Inoculation with the MMR (measles, mumps, rubella) vaccine did not impair children’s overall immunity. The results align with decades of research. Ensuring widespread vaccination against measles would not only help prevent the expected 120,000 deaths that will be directly attributed to measles this year alone, but could also avert potentially hundreds of thousands of additional deaths attributable to the lasting damage to the immune system.
The term ‘antibiotic’ was introduced by Selman Waksman as any small molecule, produced by a microbe, with antagonistic properties on the growth of other microbes. An antibiotic interferes with bacterial survival via a specific mode of action but more importantly, at therapeutic concentrations, it is sufficiently potent to be effective against infection and simultaneously presents minimal toxicity. Infectious diseases have been a challenge throughout the ages. From 1347 to 1350, approximately one-third of Europe’s population perished to Bubonic plague. Advances in sanitary and hygienic conditions sufficed to control further plague outbreaks. However, these persisted as a recurrent public health issue. Likewise, infectious diseases in general remained the leading cause of death up to the early 1900s. The mortality rate shrunk after the commercialization of antibiotics, which given their impact on the fate of mankind, were regarded as a ‘medical miracle’. Moreover, the non-therapeutic application of antibiotics has also greatly affected humanity, for instance those used as livestock growth promoters to increase food production after World War II.
Currently, more than 2 million North Americans acquire infections associated with antibiotic resistance every year, resulting in 23,000 deaths. In Europe, nearly 700 thousand cases of antibiotic-resistant infections directly develop into over 33,000 deaths yearly, with an estimated cost over €1.5 billion. Despite a 36% increase in human use of antibiotics from 2000 to 2010, approximately 20% of deaths worldwide are related to infectious diseases today. Future perspectives are no brighter, for instance, a government commissioned study in the United Kingdom estimated 10 million deaths per year from antibiotic resistant infections by 2050.
The increase in antibiotic-resistant bacteria, alongside the alarmingly low rate of newly approved antibiotics for clinical usage, we are on the verge of not having effective treatments for many common infectious diseases. Historically, antibiotic discovery has been crucial in outpacing resistance and success is closely related to systematic procedures – platforms – that have catalyzed the antibiotic golden age, namely the Waksman platform, followed by the platforms of semi-synthesis and fully synthetic antibiotics. Said platforms resulted in the major antibiotic classes: aminoglycosides, amphenicols, ansamycins, beta-lactams, lipopeptides, diaminopyrimidines, fosfomycins, imidazoles, macrolides, oxazolidinones, streptogramins, polymyxins, sulphonamides, glycopeptides, quinolones and tetracyclines.
The increase in drug-resistant pathogens is a consequence of multiple factors, including but not limited to high rates of antimicrobial prescriptions, antibiotic mismanagement in the form of self-medication or interruption of therapy, and large-scale antibiotic use as growth promotors in livestock farming. For example, 60% of the antibiotics sold to the USA food industry are also used as therapeutics in humans. To further complicate matters, it is estimated that $200 million is required for a molecule to reach commercialization, with the risk of antimicrobial resistance rapidly developing, crippling its clinical application, or on the opposing end, a new antibiotic might be so effective it is only used as a last resort therapeutic, thus not widely commercialized.
Besides a more efficient management of antibiotic use, there is a pressing need for new platforms capable of consistently and efficiently delivering new lead substances, which should attend their precursors impressively low rates of success, in today’s increasing drug resistance scenario. Antibiotic Discovery Platforms are aiming to screen large libraries, for instance the reservoir of untapped natural products, which is likely the next antibiotic ‘gold mine’. There is a void between phenotanypic screening (high-throughput) and omics-centered assays (high-information), where some mechanistic and molecular information complements antimicrobial activity, without the laborious and extensive application of various omics assays. The increasing need for antibiotics drives the relentless and continuous research on the foreground of antibiotic discovery. This is likely to expand our knowledge on the biological events underlying infectious diseases and, hopefully, result in better therapeutics that can swing the war on infectious diseases back in our favor.
During the genomics era came the target-based platform, mostly considered a failure due to limitations in translating drugs to the clinic. Therefore, cell-based platforms were re-instituted, and are still of the utmost importance in the fight against infectious diseases. Although the antibiotic pipeline is still lackluster, especially of new classes and novel mechanisms of action, in the post-genomic era, there is an increasingly large set of information available on microbial metabolism. The translation of such knowledge into novel platforms will hopefully result in the discovery of new and better therapeutics, which can sway the war on infectious diseases back in our favor.
Tuberculosis is one of the world’s deadliest infectious diseases, which requires six-month course of daily antibiotics. To help overcome that, a team of researchers led by MIT has devised a new way to deliver antibiotics, which they hope will make it easier to cure more patients and reduce health care costs. In their approach a coiled wire loaded with antibiotics is inserted into the patient’s stomach through a nasogastric tube. Once in the stomach, the device slowly releases antibiotics over one month, eliminating the need for patients to take pills every day.
The device is a thin, elastic wire made of nitinol that can change its shape based on temperature. The researchers can string up to 600 “pills” of various antibiotics along the wire, and the drugs are packaged in polymers whose composition can be adjusted to control the rate of drug release once the device go in the stomach. The wire is distributed to the patient’s stomach via a tube inserted through the nose, which is used regularly in hospitals for delivering medications and nutrients. When the wire reaches the higher temperatures of the stomach, it forms a coil, which stops it from passing further through the digestive system. The researchers then tested the device in pigs and found that this device could release different antibiotics at a constant rate for 28 days. Once all of the drugs are delivered, the device is recovered through the nasogastric tube using a magnet that can attract the coil.
Giovanni Traverso and Robert Langer have been working on a variety of pills and capsules that can remain in the stomach and slowly release medication after being swallowed. This type of drug delivery, can expand treatment to several chronic diseases that require daily doses of medication. One capsule that shows promise appears to be for delivering small amounts of drugs to treat HIV and malaria. After being swallowed, the capsule’s outer coating disintegrates, allowing six arms to expand, helping the device to lodge in the stomach. This device can carry about 300 milligrams of drugs which is enough for a week’s worth of HIV treatment but it falls short of the payload of 3 grams of antibiotics every day needed to treat tuberculosis.
The researchers in addition to David Collins, an economist analyzed the potential economic impact of this type of treatment. He determined that if the treatment is applied in India, costs could be reduced by about $8,000 per patient. I think that such an approach can be helpful for longer regimens required for the treatment of extensively drug-resistant TB and even hepatitis C and this approach can be an vital milestone toward addressing this problem.
The second annual PureTech Health BIG Summit brings together an elite ensemble of leading scientific researchers, investors, and CEOs and R&D leaders from major pharmaceutical, technology, and biotech companies.
The BIG Summit is designed to stimulate ideas that will have an impact on existing pipelines and catalyze future interactions among a group of delegates that represent leaders and innovators in their fields.
Please follow the discussion on Twitter using #BIGAxisSummit
By invitation only; registration is non-transferable.
For more information, please contact PureTechHealthSummit@PureTechHealth.com
Back for final sessions at #BIGAxisSummit. @PureTechH Jim Harper of Sonde Health talking about how voice data — pacing, fine motor articulation, oscillation — can point the way to objective, quantitative measures for detecting and monitoring depression.
Paul Biondi at #BIGAxisSummit : What makes big deals happen is financial, and *deep conviction* of a big future fit. Disproportionate valuation from bidders is expected.
Love this. We often reduce everything to mathematical analyses to champion or ridicule deals. Not that simple
Bob Langer (@MIT) asks how #lymphatics affected by #aging. Santambrogio: typically blame aging #immune cells for increased disease, but aging affects lymphatics too (less efficient trafficking shown). Rejuvenating these could affect several aging-related diseases #BigAxisSummit
Once herpes simplex infects a person, the virus goes into hiding inside nerve cells, hibernating there for life, periodically waking up from its sleep to reignite infection, causing cold sores or genital lesions to recur. Research from Harvard Medical School showed that the virus uses a host protein called CTCF, or cellular CCCTC-binding factor, to display this type of behavior. Researchers revealed with experiments on mice that CTCF helps herpes simplex regulate its own sleep-wake cycle, enabling the virus to establish latent infections in the body’s sensory neurons where it remains dormant until reactivated. Preventing that latency-regulating protein from binding to the virus’s DNA, weakened the virus’s ability to come out of hiding.
Herpes simplex virus’s ability to go in and out of hiding is a key survival strategy that ensures its propagation from one host to the next. Such symptom-free latency allows the virus to remain out of the reach of the immune system most of the time, while its periodic reactivation ensures that it can continue to spread from one person to the next. On one hand, so-called latency-associated transcript genes, or LAT genes, turn off the transcription of viral RNA, inducing the virus to go into hibernation, or latency. On the other hand, a protein made by a gene called ICP0 promotes the activity of genes that stimulate viral replication and causes active infection.
Based on these earlier findings, the new study revealed that this balancing act is enabled by the CTCF protein when it binds to the viral DNA. Present during latent or dormant infections, CTCF is lost during active, symptomatic infections. The researchers created an altered version of the virus that lacked two of the CTCF binding sites. The absence of the binding sites made no difference in early-stage or acute infections. Similar results were found in infected cultured human nerve cells (trigeminal ganglia) and infected mice model. The researchers concluded that the mutant virus was found to have significantly weakened reactivation capacity.
Taken together, the experiments showed that deleting the CTCF binding sites weakened the virus’s ability to wake up from its dormant state thereby establishing the evidence that the CTCF protein is a key regulator of sleep-wake cycle in herpes simplex infections.
In Nursing School at Northeastern University, 9/2005 – 12/2007, wrote a paper on Causes of Necrotiszing Tissue
In Medical-Surgical Rotation at BWH, Boston, 2006, shadowed post-surgical case of Necrotizing Fasciitis and treatment with vacuum-assisted wound closing device (VAC). Postoperative management of the surgical wound benefited from exudate removal and exact monitoring of exudate accumulation in VAC canister recorded by the Nursing staff.
In Vulnerable Populations rotation at Barbara McGinnis House in Jamaica Plain, 2006, delivered wound care to a patient with type 3 fasciitis on a lower extremity
In LTACH, Kindred Waltham Hospital, as Hospital Supervisor, 2009, supervised administration of triple IV antibiotic treatment for a patient with Type 3 Fasciitis of the lower extremity
In personal communication with Dr. T.H., OCB, Boston, 2003, he reported the cardinal importance of triple IV antibiotic treatment in curing Fasciitis in lower extremity following Hip replacement surgery.
Since ischemia and hypoxia compromise the adequate delivery of antibiotics to the infection site, conservative treatment with antibiotics alone has little value in the management of NF (58). However, they play a significant role in surgical management of the infection. Patients should be immediately treated with broad-spectrum antibiotics, when NF is suspected. The empirical usage of antibiotics is based on the microbiological classification of NF. Antibiotic treatment of a polymicrobial infection should be based on history, Gram stain, and culture. Initial treatment includes ampicillin or ampicillin–sulbactam combined with metronidazole or clindamycin (59). Anaerobic coverage is quite important for type 1 infection; metronidazole, clindamycin, or carbapenems (imipenem) are effective antimicrobials. Broad gram-negative coverage is necessary as an initial empirical therapy for patients who have recently been treated with antibiotics, or been hospitalized. In such cases, antibiotics such as ampicillin–sulbactam, piperacillin–tazobactam, ticarcillin–clavulanate acid, third or fourth generation cephalosporins, or carbapenems are used, and at a higher dosage.
Type 2 disease is treated with antibiotics against S. pyogenes and S. aureus, which usually coexist with the former. Hence, first or second generation of cephalosporins are used for the coverage of methicillin-sensitive Staphylococcus aureus (MSSA). MRSA tends to be covered by vancomycin, or daptomycin and linezolid in cases where S. aureus is resistant to vancomycin. Some studies suggest that clindamycin is superior to penicillin in managing streptococcal infections (60), but this has yet to be satisfactorily proven. Another study has proposed that clinicians should consider adding clindamycin to the beta-lactam antibiotic regimen when NF or myositis is present (61).
Type 3 NF should be managed with clindamycin and penicillin, which cover the Clostridium species. If Vibrio infection is suspected, the early use of tetracyclines (including doxycycline and minocycline) and third-generation cephalosporins is crucial for the survival of the patient, since these antibiotics have been shown to reduce the mortality rate drastically (59).
Finally, type 4 NF can be treated with amphotericin B or fluoroconazoles, but the results of this treatment are generally disappointing.
As in every empirical antibiotic therapy, the dosage should be tapered, based on the results of the initial blood, wound, and tissue cultures, but continued until the infection is under control and for at least 48 h after clinical and hemodynamic stabilization of the patient has been achieved. Antibiotics should be administered for up to 5 days after local signs and symptoms have resolved (62). The mean duration of antibiotic therapy for NF is 4–6 weeks.
Intravenous immunoglobulin (IVIG) has recently been described as a reasonable and desirable option for neutralizing streptococcal toxins (63). There is evidence that a high dose of IVIG may prove beneficial in severe streptococcal infections (64), but this has yet to be demonstrated with randomized studies.
Nursing comments:
Nutrition
Nutritional support is required from the first day of the patient’s admission to hospital (preferably the ICU), to replace lost proteins and fluid from large wounds and/or the resultant toxic shock. Metabolic demands are similar to those of other major trauma or burns, which means that the patient needs twice the basic caloric requirements.
Wound dressing and debridement
Postoperative management of abdominal wall wounds involves serial dressing changes over the following days, until the wound is free of recurrent or ongoing infection. The use of a vacuum-assisted wound closing device (VAC) can also be helpful. After surgical debridement, the use of the VAC system helps wound healing by absorbing excess exudates; reducing localized edema, and finally drawing wound edges together
Conclusion
Necrotizing fasciitis is a rare but life-threatening condition, with a high mortality rate (median mortality 32.2%) that approaches 100% without treatment. Numerous conditions are associated with this pathology, such as diabetes mellitus, immunosuppression, chronic alcohol disease, chronic renal failure, and liver cirrhosis, which can be conductive to the rapid spread of necrosis, and increase in the mortality rate. The diagnosis of NF is difficult and the differential diagnosis between NF and other necrotizing soft tissue infections more so. However, the clinician should do their utmost to secure the diagnosis of NF, as a delay in diagnosis can be fatal, and septic shock is inevitable if the disease remains untreated. The characteristic of NF is the clinical status change over time. The early clinical picture includes erythema, swelling, tenderness to palpation, and local warmth; once the infection develops, the infection site presents skin ischemia with blisters and bullae. The diagnosis of NF can be secured faster with the use of laboratory-based scoring systems, such as the LRINEC score or the FGSI score, especially in cases of Fournier’s gangrene. However, the diagnosis is definitely established by performing explorative surgery at the infected site.
Management of the infection begins with antibiotic treatment. In the majority of cases with NF (70–90%) the reasonable pathogens are two or more, suggesting the use of broad-spectrum antibiotics. The value of antibiotic treatment in NF is relatively low, and early and aggressive drainage and debridement is required. In NF of the extremities, the clinician should consider amputating the infected limb, although this will not reduce the risk of mortality. Finally, postoperative management of the surgical wound is important, along with proper nutrition of the patient. The use of VAC therapy in wound management has greatly improved the results of postoperative management.
Hepatitis B virus can cause serious, long-term health problems, such as liver disease and cancer, and can spread from mother-to-child during delivery. According to the latest estimates from the World Health Organization (WHO), approximately 257 million people in 2015 were living with the virus. Countries in Asia have a high burden of hepatitis B. There is no cure, and antiviral drugs used to treat the infection usually need to be taken for life.
To prevent infection, WHO recommends that all newborns receive their first dose of hepatitis B vaccine within 24 hours of delivery. Infants born to hepatitis B-infected mothers are also given protective antibodies called hepatitis B immune globulin (HBIG). However, mother-to-child transmission can still occur in women with high levels of virus in their blood, as well as those with mutated versions of the virus.
Tenofovir disoproxil fumarate (TDF), an antiviral drug commonly prescribed to treat hepatitis B infection, does not significantly reduce mother-to-child transmission of hepatitis B virus when taken during pregnancy and after delivery, according to a phase III clinical trial in Thailand funded by the National Institutes of Health. The study tested TDF therapy in addition to the standard preventative regimen — administration of hepatitis B vaccine and protective antibodies at birth — to explore the drug’s potential effects on mother-to-child transmission rates. The results appear in the New England Journal of Medicine.
The present study was conducted at 17 hospitals of the Ministry of Public Health in Thailand. It screened more than 2,500 women for eligibility and enrolled 331 pregnant women with hepatitis B. The women received placebo (163) or TDF (168) at intervals from 28 weeks of pregnancy to two months after delivery. All infants received standard hepatitis B preventatives given in Thailand, which include HBIG at birth and five doses of the hepatitis B vaccine by age 6 months (which differs from the three doses given in the United States). A total of 294 infants (147 in each group) were followed through age 6 months.
Three infants in the placebo group had hepatitis B infection at age 6 months, compared to zero infants in the TDF treatment group. Given the unexpectedly low transmission rate in the placebo group, the researchers concluded that the addition of TDF to current recommendations did not significantly reduce mother-to-child transmission of the virus.
According to the study, the clinical trial had enough participants to detect statistical differences if the transmission rate in the placebo group reached at least 12 percent, a rate observed in previous studies. Though the reasons are unknown, the researchers speculate that the lower transmission rate seen in the study may relate to the number of doses of hepatitis B vaccine given to infants in Thailand, lower rates of amniocentesis and Cesarean section deliveries in this study, or the lower prevalence of mutated viruses that result in higher vaccine efficacy in Thailand compared to other countries.
Includes FDA Approved Drugs for Infections and Infectious Diseases: Bacterial Infection, Viral Infection, Fungal Infection, Allergy-related Infections and Other, 1995 – 2016
VOLUME 2: covers the frontier of research on Infectious Diseases and the Human Immune System. The Immune Response, Disease Specific Immune Response, Immunodiagnostics and Immunotherapy, Immunotherapy and Autoimmunity,
Bacterial Infections, Bacteria Types, Antibactirial Therapeutics, FDA Approved Drugs for Infections and Infectious Diseases: Bacterial Infection, 1995 – 2016. Viral Infection: Virus Types, Antiviral Therapeutics, and FDA Approved Drugs for Infections and Infectious Diseases: Viral Infection, Fungal Infections, Allergy-related Infections, Other Infections,1995 – 2016,
VOLUME 3: covers the state of Science on the Historical Perspective of Immunology, Development of the Immune System, Signaling and Immunology, Cellular Immunity, Immunology and Inflammatory Response. Antibody-based Immunity, Vaccines and Microbiome, Immuno-Pharmaceutics, Cancer Immunotherapy, Immunomodulation and Neuro-Immunology.
Volume 2: Summary
The material that has been covered is a considerable material on the basic types of infections – bacterial, viral, and fungal, and diseases related to immune mechanisms. There has been a substantial coverage of the drugs and the manufacturers. This material brings to the discussion an international problem of drug resistance that applies much to bacteria, and a considerable amount of material on advances in drug development that takes into consideration protein structure and protein-protein interactions. The coverage of virus diseases brings to the forefront vaccines. However, in such cases as the influenza virus, a rapid genetic change of the virus makes the use of vaccines an issue for continuing revision.
Volume 3: Summary
The second volume is only concerned with the pathobiology of the inflammatory response, including sepsis, and it does not leave out hematopoiesis, and it lays out the difference between the B-clles and the T-cells that are related to the Toll receptor. Here we have looked closely at two immune disorders, Inflammatory Bowel Disease (Crohn’s Disease) and Rheumatoid Arthritis. Here we have discussed immunomodulation and signaling of the pathways involved, and the programmed cell death response. We have also covered the relationship of the immune response to autoimmune disorders and to cancer. The treatment of cancer now heavily leans toward the blocking of destructive processes in the immunomodulatory pathways.
Epilogue – Volume 2
Volume 2 has covered the most common bacterial and viral diseases that we find widely, or sporadically. It detailed the development of sepsis, and the immune response factor. The immune response involves local cellular invasion of lymphocytes related to initiation of T-cells and macrophages, and also the proteomic generated B-cell antibodies. These reactions are both local and systemic, as bacterial invasion is local and usually related to the tissue of residence (large intestine, oral, lung, genital). In the case of virus, the site of entry is often respiratory or by food intake, but these agents may rapidly become systemic. The other matter of the immune response is autoimmune, a reaction against the self. It is not entirely clear how this is initiated, but it has been related to failure to develop immunity in the prenatal or postnatal period. The only other possibility that might be considered would be by the mechanism of cell remodeling by an apoptotic related mechanism. The other chapters deal with therapeutics.
Epilogue – Volume 3
These two volumes have traversed a large knowledge-base. The first was directed largely at the well known bacterial, virus, fungal diseases, as well as autoimmunity. It specified recent FDA approved recommendations of pharmaceutics for these conditions. It also gives some attention to the immune response in inflammatory and autoimmune diseases, but not cancer. The second volume gives a concise history of development of Leukemias, Lymphomas pathology.