Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Primary source: Journal of the American College of Cardiology
Source reference: Moussa I, et al “Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI)” J Am Coll Cardiol2013; 62: 1563-1570.
Additional source: Journal of the American College of Cardiology
Source reference:White H “Avatar of the universal definition of periprocedural myocardial infarction”J Am Coll Cardiol 2013; 62: 1571-1574.
Moussa reported that he had no conflicts of interest.
Stone is a consultant for Boston Scientific, Eli Lilly, Daiichi Sankyo, and AstraZeneca. The other authors reported relationships with Guerbet, The Medicines Company, Bristol-Myers Squibb/Sanofi, Merck, Maya Medical, AstraZeneca, Abbott Vascular, Regado Biosciences, Janssen Pharma, Lilly/Daiichi Sankyo, St. Jude Medical, Medtronic, Terumo, Bridgepoint/Boston Scientific, Gilead, Boston Scientific, Eli Lilly, and Daiichi Sankyo.
White is co-chairman for the Task Force for the Universal Definiton of Myocardial Infarction; has received research grants from sanofi-aventis, Eli Lilly, The Medicines Company, the NIH, Pfizer, Roche, Johnson & Johnson, Schering-Plough, Merck Sharpe & Dohme, AstraZeneca, GlaxoSmithKline, Daiichi Sankyo Pharma Development, and Bristol-Myers Squibb; and has served on advisory boards for AstraZeneca, Merck Sharpe & Dohme, Roche, and Regado Biosciences.
WASHINGTON, DC — A “clinically meaningful” definition of MI following PCI or CABG is urgently needed to replace the arbitrarily chosen “universal definition” proposed in recent years that has no relevance to patients and may be muddying clinical-trial results. Those are the conclusions of a new expert consensus document released Monday by the Society of Cardiovascular Angiography and Interventions (SCAI)[1].
The notion of a “universal definition of MI” was first proposed in 2000 and updated in 2007 and 2012. The 2012 document defines a PCI-related MI as an increase in cardiac troponin (cTn) of more than five times the upper limit of normal (ULN) during the first 48 hours postprocedure plus specific clinical or ECG features. Post-CABG, the definition is a cTn increase of >10 times the ULN, plus different clinical or ECG features.
The problem, lead author Dr Issam Moussa (Mayo Clinic, Jacksonville, FL) told heartwire, is that these cutoffs were arbitrarily chosen and not based on any hard evidence that these biomarker levels spelled a poor prognosis. Moreover, “overnight, the rate of MI went from 5% following these procedures to 20% to 30%!” he said.
The SCAI committee, in its new document, focuses on post-PCI procedures and highlights the importance of acquiring baseline cardiac biomarkers and differentiating between patients with elevated baseline CK-MB (or cTn) in whom biomarker levels are stable or falling, as well as those in whom it hasn’t been established whether biomarkers are changing.
SCAI’s Proposed Clinically Meaningful MI Definitions
Group
Definition
Normal baseline CK-MB
CK-MB rise of >10x ULN or >5x ULN with new pathologic Q-waves in at least 2 contiguous leads or new persistent left bundle branch block
OR
In the absence of baseline CK-MB, a cTn rise of >70x ULN or a rise of>35 ULN plus new pathologic Q-waves in at least 2 contiguous leads or new persistent left bundle branch block
Elevated baseline biomarkers that are stable or falling
A CK-MB or cTn rise that is equal (by an absolute increment) to the definitions described for patients with normal CK-MB at baseline.
Elevated baseline biomarkers that have not been shown to be stable or falling
A CK-MB or cTn rise that is equal (by an absolute increment) to the definitions described for patients with normal CK-MB at baseline Plus
New ST-segment elevation or depression Plus
New-onset or worsening heart failure or sustained hypotension or other signs of a clinically relevant MI.
Moussa is quick to emphasize that these new clinically meaningful definitions have limited evidence to support them—and most of what exists supports CK-MB definitions, not cTn—but that the new document is based on the best scientific evidence available.
“We don’t want to come out with a definitive statement” saying this is the final word on MI definitions,” he stressed. “There is more science that needs to be done and there remains more uncertainty. We framed this to be inclusive and also to open the field for discussion.”
His hope is that this will lead to important changes in how patients are managed and money is spent. Currently, patients with clinically meaningless biomarker elevations may become unnecessarily panicked over news that they’ve had a “heart attack,” while hospital stays may be extended and further tests ordered on the basis of these results.
Moussa et al’s proposal also has important implications for clinical trials, he continued. Currently, for studies that include periprocedural MIs as an individual end point or as part of a composite end point, the very high number of biomarker-defined “MIs” collected in the trial could potentially overwhelm the true impact of any given therapy. “You are really using an end point that is truly not relevant to patients. . . . This could really affect the whole hypothesis.”
He’s expecting some push-back from cardiologists and academics, particularly those who championed the need for the universal definition in the first place, but believes most people will welcome a clinically meaningful definition.
“I think many in the medical community will accept this because they have not really been using the universal definition in their day-to-day practice anyhow.” What’s more, the National Cardiovascular Data Registry (NCDR) does not include the reporting of MI postangiography, in part because of concerns that the universal definition of MI overestimates the true incidence of this problem. “I think many in the community will look at this definition as more reflective of the true incidence of MI after angioplasty, and if it’s accepted, they are more likely to report it to databases like NCDR and use it to reflect quality-of-care processes.”
the Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction
*Corresponding authors/co-chairpersons: Professor Kristian Thygesen, Department of Cardiology, Aarhus University Hospital, Tage-Hansens Gade 2, DK-8000 Aarhus C, Denmark. Tel: +45 7846-7614; fax: +45 7846-7619: E-mail: kristhyg@rm.dk. Professor Joseph S. Alpert, Department of Medicine, Univ. of Arizona College of Medicine, 1501 N. Campbell Ave., P.O. Box 245037, Tucson AZ 85724, USA, Tel: +1 520 626 2763, Fax: +1 520 626 0967, E-mail: jalpert@email.arizona.edu. Professor Harvey D. White, Green Lane Cardiovascular Service, Auckland City Hospital, Private Bag 92024, 1030 Auckland, New Zealand. Tel: +64 9 630 9992, Fax: +64 9 630 9915, E-mail: harveyw@adhb.govt.nz.
Reviewed by Zalman S. Agus, MD; Emeritus Professor, Perelman School of Medicine at the University of Pennsylvania and Dorothy Caputo, MA, BSN, RN, Nurse Planner
The Society for Cardiovascular Angiography and Interventions (SCAI) has released a new definition for myocardial infarction (MI) following coronary revascularization aimed at identifying only those events likely to be related to poorer patient outcomes.
In the new criteria — published as an expert consensus document inCatheterization and Cardiovascular Interventions and the Journal of the American College of Cardiology — creatine kinase-myocardial band (CK-MB) is the preferred cardiac biomarker over troponin, and much greater elevations are required to define a clinically relevant MI compared with the universal definition of MI proposed in 2007 and revised in 2012.
Also, the new definition uses the same biomarker elevation thresholds to identify MIs following both percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG), whereas the universal definition has different thresholds for events following the two procedures.
“In the universal definition of MI, they even acknowledged that their criteria were arbitrary,” Stone said in an interview. “We’ve tried to reduce the arbitrariness of the cutoff values that we selected so that the researcher, academician, clinician, hospital administrator, etc., can be confident that these levels that we’re recommending are the ones that are associated with a worse prognosis for patients suffering periprocedural complications.”
The Change
The existing universal definition for MI defines events following PCI according to an increase in cardiac troponin to greater than five times the 99th percentile upper reference limit (URL) within 48 hours when baseline levels are normal, with confirmation by electrocardiogram (ECG), imaging, or symptoms.
For CABG-related MI, the increase must be more than 10 times the 99th percentile URL within 48 hours when baseline levels are normal, with confirmation by ECG, angiography, or imaging.
But, Stone and colleagues wrote, the relationship between that degree of troponin elevation after a revascularization procedure and prognosis is not as strong as the association between a CK-MB elevation and patient outcomes.
Using a small elevation in troponin to define a post-procedure MI could find myocardial necrosis that is unlikely to be associated with poor clinical outcomes, which could have far-reaching implications, they wrote.
“Widespread adoption of an MI definition not clearly linked to subsequent adverse events such as mortality or heart failure may have serious consequences for the appropriate assessment of devices and therapies, may affect clinical care pathways, and may result in misinterpretation of physician competence,” they wrote.
To address that issue, the expert panel convened by SCAI sought to define clinically relevant MI after PCI or CABG.
A clinically relevant MI is defined in the new document based on an increase of at least 10 times the upper limit of normal in the level of CK-MB within 48 hours after a revascularization procedure when baseline levels are normal.
When the CK-MB level is not available, then an increase in troponin I or T of at least 70 times the upper limit of normal can be used to define a clinically relevant MI, according to the authors.
However, if an ECG shows new pathologic Q-waves in at least two contiguous leads or a new persistent left bundle branch block, then the thresholds can be lowered to at least five times and at least 35 times the upper limit of normal for CK-MB and troponin, respectively.
Further guidance is provided for identifying clinically relevant post-procedure MIs when the cardiac biomarker levels are elevated at baseline.
Dueling Definitions
Co-chairman of the Task Force for the Universal Definition of Myocardial Infarction, Harvey White, DSc, of Auckland City Hospital in Auckland, New Zealand, noted some limitations of the new definition, including the lack of a requirement for ischemic symptoms.
“Ischemic symptoms have always been a basic tenet of the diagnosis of MI, and it should be no different for a [PCI-related] MI,” he wrote in an accompanying editorial.
In addition, with the use of such large elevations in biomarker levels in the new definition, “there will be very few PCI-related events identified, and an opportunity to improve patient outcomes may be lost,” he wrote.
Troponin should remain the preferred biomarker over CK-MB, White argued, pointing to variability in and analytical issues with CK-MB assays, the need for sex-specific cutoffs for CK-MB levels, the need for higher thresholds of CK-MB to determine abnormalities because all individuals have circulating levels of the biomarker, and the reduced sensitivity and specificity of CK-MB.
Also, he said, CK-MB is becoming increasingly unavailable at medical centers.
“With CK-MB becoming obsolete, troponin will become the gold standard, and CK-MB will no longer have a role in defining PCI injury and infarction in clinical practice,” White wrote.
Stone admitted that troponin ultimately might be preferable to CK-MB because of its greater specificity, although the evidence does not yet support it.
“I think there’s a general desirability to move to troponins, although when you look at the data that’s out there it’s much stronger correlating CK-MB elevations to subsequent prognosis,” he said. “I think a lot of the troponin elevations are just noise or troponins are just too sensitive.”
Room for Both?
White noted in his editorial that “the rationale for the SCAI definition has been well articulated by its authors and may be appropriate in an individual trial, but it should not supplant the universal definition of MI,” he wrote.
When asked whether the new definition would replace the universal definition, Stone said there is a place for both sets of criteria.
“We would propose the clinically relevant definition be the one that is used to make most substantial decisions right now, [such as] trade-offs between efficacy and safety for new drugs and devices, in judging hospital systems and physicians, etc.,” he said. “But I do think there’s value in both, and they will both continue to evolve over time as new data becomes evident.”
Third Universal Definition of Myocardial Infarction
Improved long-term clinical outcomes in patients with ST-elevation myocardial infarction undergoing remote ischaemic conditioning as an adjunct to primary percutaneous coronary interventionEur Heart J. 2013;0:eht369v1-eht369
The role of myeloperoxidase (MPO) for prognostic evaluation in sensitive cardiac troponin I negative chest pain patients in the emergency departmentEuropean Heart Journal: Acute Cardiovascular Care. 2013;2:203-210,
An Updated Definition of Stroke for the 21st Century: A Statement for Healthcare Professionals From the American Heart Association/American Stroke AssociationStroke. 2013;44:2064-2089,
Factors Influencing the 99th Percentile of Cardiac Troponin I Evaluated in Community-Dwelling Individuals at 70 and 75 Years of AgeClin. Chem.. 2013;59:1068-1073,
Detection and management of asymptomatic myocardial injury after noncardiac surgeryEuropean Journal of Preventive Cardiology.2013;0:2047487313494294v1-2047487313494294,
Outcomes for Clinical Studies Assessing Drug and Revascularization Therapies for Claudication and Critical Limb Ischemia in Peripheral Artery DiseaseCirculation. 2013;127:1241-1250,
2013 ACCF/AHA Key Data Elements and Definitions for Measuring the Clinical Management and Outcomes of Patients With Acute Coronary Syndromes and Coronary Artery Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Acute Coronary Syndromes and Coronary Artery Disease Clinical Data Standards)Circulation. 2013;127:1052-1089,
Percutaneous Coronary Intervention Versus Optimal Medical Therapy for Prevention of Spontaneous Myocardial Infarction in Subjects With Stable Ischemic Heart DiseaseCirculation. 2013;127:769-781,
Frequency of Myocardial Infarction and Its Relationship to Angiographic Collateral Flow in Territories Supplied by Chronically Occluded Coronary ArteriesCirculation. 2013;127:703-709,
Persistent Increases in Cardiac Troponin Concentrations As Measured with High-Sensitivity Assays after Acute Myocardial InfarctionClin. Chem.. 2013;59:443-445,
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesCirculation. 2013;127:e362-e425,
This article was written in continuation to and it is addressing additional scientific matters to the content presented on this subject in the third Section titled
III. Incidence of Sepsis (circulation infection with serious consequences)
of the 7/23/2013 article on:
Cardiovascular Complications: Death from Reoperative Sternotomy after prior CABG, MVR, AVR, or Radiation; Complications of PCI; Sepsis from Cardiovascular Interventions
Justin D Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
Sepsis is generally viewed as a disease aggravated by an inappropriate immune response encountered in the afflicted individual. As an important organ system frequently compromised by sepsis and always affected by septic shock, the cardiovascular system and its dysfunction during sepsis have been studied in clinical and basic research for more than 5 decades. Although a number of mediators and pathways have been shown to be associated with myocardial depression in sepsis, the precise cause remains unclear to date. There is currently no evidence supporting global ischemia as an underlying cause of myocardial dysfunction in sepsis. A circulating myocardial depressant factor in septic shock has long been proposed, and potential candidates for a myocardial depressant factor include cytokines, prostanoids, and nitric oxide, among others. Endothelial activation and induction of the coagulatory system also contribute to the pathophysiology in sepsis.
Prompt and adequate antibiotic therapy accompanied by surgical removal of the infectious focus, if indicated and feasible, is the mainstay and also the only strictly causal line of therapy. In the presence of severe sepsis and septic shock, supportive treatment in addition to causal therapy is mandatory. We delineate some characteristics of septic myocardial dysfunction, to assess the most commonly cited and reported underlying mechanisms of cardiac dysfunction in sepsis, and to briefly outline current therapeutic strategies and possible future approaches.
Sepsis, defined by consensus conference as “the systemic inflammatory response syndrome (SIRS) that occurs during infection,” is generally viewed as a disease aggravated by the inappropriate immune response encountered in the affected individual. Morbidity and mortality are high, resulting in sepsis and septic shock being the 10th most common cause of death in the United States. The total national hospital cost invoked by severe sepsis in the United States was estimated at approximately $16.7 billion with 215 000 associated deaths annually. A study from Britain documented a 46% in-hospital mortality rate for patients presenting with severe sepsis on admission to the intensive care unit.
Current Criteria for Establishment of the Diagnosis of SIRS, Sepsis, and Septic Shock
The cardiovascular system is an important organ system frequently affected by sepsis and always affected by septic shock. Waisbren was the first to describe cardiovascular .dysfunction due to sepsis in 1951. He recognized a hyperdynamic state with full bounding pulses, flushing, fever, oliguria, and hypotension. He also described a second, smaller patient group who presented clammy, pale, and hypotensive with low volume pulses and who appeared more severely ill. The latter group might well have been volume underresuscitated, and indeed, timely and adequate volume therapy has been demonstrated to be one of the most effective supportive measures in sepsis therapy.
Under conditions of adequate volume resuscitation, the profoundly reduced systemic vascular resistance typically encountered in sepsis leads to a concomitant elevation in cardiac index that obscures the myocardial dysfunction that also occurs. As early as the mid-1980s, significant reductions in both stroke volume and ejection fraction in septic patients were observed with normal total cardiac output. The presence of cardiovascular dysfunction in sepsis is associated with a significantly increased mortality rate of 70% to 90% compared with 20% in septic patients without cardiovascular impairment.
Characteristics of Myocardial Dysfunction in Sepsis
Using portable radionuclide cineangiography, Calvin et al. were the first to demonstrate myocardial dysfunction in adequately volume-resuscitated septic patients who had decreased ejection fraction and increased end-diastolic volume index. Adding pulmonary artery catheters to serial radionuclide cineangiography, Parker and colleagues extended these observations with the 2 major findings that
(1) survivors of septic shock were characterized by increased end-diastolic volume index and decreased ejection fraction, whereas nonsurvivors typically maintained normal cardiac volumes, and
(2) these acute changes in end-diastolic volume index and ejection fraction, although sustained for several days, were reversible.
More recently, echocardiographic studies have demonstrated impaired left ventricular systolic and diastolic function in septic patients. These human studies, in conjunction with experimental studies have clearly established decreased contractility and impaired myocardial compliance as major factors that cause myocardial dysfunction in sepsis. Similar functional alterations, as discussed above, have been observed for the right ventricle.
Myocardial dysfunction in sepsis has also been analyzed with respect to its prognostic value. Parker et al. reviewing septic patients on initial presentation and at 24 hours to determine prognostic indicators, found a heart rate of <106 bpm to be the only cardiac parameter on presentation that predicted a favorable outcome. At 24 hours after presentation, a systemic vascular resistance index > 1529 dyne · s−1 · cm−5 · m−2, a heart rate < 95 bpm or a reduction in heart rate >18 bpm, and a cardiac index > 0.5 L · min−1 · m−2 suggested survival. In a prospective study, Rhodes et al. demonstrated the feasibility of a dobutamine stress test for outcome stratification, with nonsurvivors being characterized by an attenuated inotropic response.
The well-established biomarkers in myocardial ischemia and heart failure, cardiac troponin I and T, as well as B-type natriuretic peptide, have also been evaluated with regard to sepsis-associated myocardial dysfunction. B-type natriuretic peptide studies have delivered conflicting results in septic patients, confounded by pre-existing heart failure early in the course. Several small studies have reported a relationship between elevated cardiac troponin T and I and left ventricular dysfunction in sepsis, as assessed by echocardiographic ejection fraction or pulmonary artery catheter–derived left ventricular stroke work index. Cardiac troponin levels also correlated with the duration of hypotension and the intensity of vasopressor therapy. In addition, increased sepsis severity, measured by global scores such as the Simplified Acute Physiology Score II (SAPS II) or the Acute Physiology And Chronic Health Evaluation II score (APACHE II), was associated with increased cardiac troponin levels, as was poor short-term prognosis.
Despite the heterogeneity of study populations and type of troponin studied, the mentioned studies were unequivocal in concluding that elevated troponin levels in septic patients reflect higher disease severity, myocardial dysfunction, and worse prognosis. In a recent meta-analysis of 23 observational studies, Lim et al. found cardiac troponin levels to be increased in a large percentage of critically ill patients. Furthermore, in a subset of studies that permitted adjusted analysis and comprised 1706 patients, this troponin elevation was associated with an increased risk of death (odds ratio, 2.5; 95% CI, 1.9 to 3.4, P<0.001). Thus, it appears reasonable to recommend inclusion of cardiac troponins in the monitoring of patients with severe sepsis and septic shock to facilitate prognostic stratification and to increase alertness to the presence of cardiac dysfunction in individual patients.
Mechanisms Underlying Myocardial Dysfunction in Sepsis
Cardiac depression during sepsis is probably multifactorial. Nevertheless, it is important to identify individual contributing factors and mechanisms to generate worthwhile therapeutic targets. As a consequence, a vast array of mechanisms, pathways, and disruptions in cellular homeostasis have been examined in septic myocardium.
An early theory of myocardial depression in sepsis based on the hypothesis of global myocardial ischemia has no support. Septic patients have been shown to have high coronary blood flow and diminished coronary artery–coronary sinus oxygen difference. Coronary sinus blood studies in patients with septic shock have demonstrated complex metabolic alterations in septic myocardium, including increased lactate extraction, decreased free fatty acid extraction, and decreased glucose uptake. Several magnetic resonance studies in animal models of sepsis have demonstrated the presence of normal high-energy phosphate levels in the myocardium. CAD-aggravating factors encountered in sepsis encompass generalized inflammation and the activated coagulatory system. The endothelium plays a prominent role in sepsis, but little is known of the impact of preexisting, CAD-associated endothelial dysfunction in this context. In a postmortem study of 21 fatal cases of septic shock, previously undiagnosed myocardial ischemia at least contributed to death in 7 of the 21 cases (all 21 patients were males, with a mean age of 60.4 years
Myocardial Depressant Substance
Parrillo et al. first proposed a circulating myocardial depressant factor in septic shock more than 50 years ago. They quantitatively linked the clinical degree of septic myocardial dysfunction with the effect that serum, taken from respective patients, had on rat cardiac myocytes, with clinical severity correlating well with the decrease in extent and velocity of myocyte shortening. These effects were not seen when serum from convalescent patients whose cardiac function had returned to normal was applied or when serum was obtained from other critically ill, nonseptic patients. These findings were extended when ultrafiltrates from patients with severe sepsis and simultaneously reduced left ventricular stroke work index (< 30 g · m−1 · m−2) displayed cardiotoxic effects and contained significantly increased concentrations of interleukin (IL)-1, IL-8, and C3a. Recently, Mink et al. demonstrated that lysozyme c, a bacteriolytic agent believed to originate mainly from disintegrating neutrophilic granulocytes and monocytes, mediates cardiodepressive effects during Escherichia coli sepsis and, importantly, that competitive inhibition of lysozyme c can prevent myocardial depression in the respective experimental sepsis model. Additional potential candidates for myocardial depressant substance include other cytokines, prostanoids, and nitric oxide (NO).
Cytokines
Infusion of lipopolysaccharide (LPS, an obligatory component of Gram-negative bacterial cell walls) into both animals and humans partially mimics the hemodynamic effects of septic shock. Only a minority of patients with septic shock have detectable LPS levels, and the prolonged time course of septic myocardial dysfunction make the role of LPS inconsistent with LPS representing the sole myocardial depressant substance. Tumor necrosis factor-α (TNF-α) is an important early mediator of endotoxin-induced shock. TNF-α is mainly derived from activated macrophages. Studies using monoclonal antibodies directed against TNF-α or soluble TNF-α receptors failed to improve survival in septic patients. IL-1 is synthesized by monocytes, macrophages, and neutrophils in response to TNF-α and plays a crucial role in the systemic immune response. IL-1 depresses cardiac contractility by stimulating NO synthase (NOS). Transcription of IL-1 is followed by delayed transcription of IL-1 receptor antagonist (IL-1-ra), which functions as an endogenous inhibitor of IL-1. Recombinant IL-1-ra was evaluated in phase III clinical trials, which showed a tendency toward improved survival and increased survival time in a retrospective analysis of the patient subgroup with the most severe sepsis; but this initially promising therapy failed to deliver a survival benefit. IL-6, another proinflammatory cytokine, has also been implicated in the pathogenesis of sepsis and is considered a more consistent predictor of sepsis than TNF-α because of its prolonged elevation in the circulation. Although cytokines may very well play a key role in the early decrease in contractility, they cannot explain the prolonged duration of myocardial dysfunction in sepsis, unless they result in the induction or release of additional factors that in turn alter myocardial function, such as prostanoids or NO.
Prostanoids
Prostanoids are produced by the cyclooxygenase enzyme from arachidonic acid (an omega-6 derivative). The expression of cyclooxygenase enzyme-2 is induced, among other stimuli, by LPS and cytokines (cyclooxygenase enzyme-1 is expressed constitutively). Elevated levels of prostanoids such as thromboxane and prostacyclin that alter coronary autoregulation, coronary endothelial function, and intracoronary leukocyte activation, have been demonstrated in septic patients. Early animal studies with cyclooxygenase inhibitors such as indomethacin yielded very promising results. Along with other positive results, these led to an important clinical study involving 455 septic patients who were randomized to receive intravenous ibuprofen or placebo, but that study did not demonstrate improved survival for the treatment arm. Similarly, a smaller study on the effects of lornoxicam failed to provide evidence for a survival benefit through cyclooxygenase inhibition in sepsis.
Endothelin-1
Endothelin-1 upregulation has been demonstrated within 6 hours of LPS-induced septic shock. Cardiac overexpression of ET-1 triggers an increase in inflammatory cytokines (among others, TNF-α, IL-1, and IL-6), interstitial inflammatory infiltration, and an inflammatory cardiomyopathy that results in heart failure and death. The involvement of ET-1 in septic myocardial dysfunction is supported by the observation that tezosentan, a dual endothelin-A and endothelin-B receptor antagonist, improved cardiac index, stroke volume index, and left ventricular stroke work index in endotoxemic shock. However, higher doses of tezosentan exhibited cardiotoxic effects and led to increased mortality. Although ET-1 has been demonstrated to be of pathophysiological importance in a wide array of cardiac diseases through autocrine, endocrine, or paracrine effects, its biosynthesis, receptor-mediated signaling, and functional consequences in septic myocardial dysfunction warrant further investigation to assess the therapeutic potential of ET-1 receptor antagonists.
Free Radicals and Antioxidants: an Overview
The presence of free radicals in biological materials was discovered about 50 years ago. Today, there is a large body of evidence indicating that patients in hospital intensive care units (ICUs) are exposed to excessive free radicals from drugs and other substances that alter cellular reduction -oxidation (redox) balance, and disrupt normal biological functions. However, low levels of free radicals are also vital for many cell signaling events and are essential for proper cell function.
Normal cellular metabolism involves the production of ROS, and in humans, superoxide (O2 -) is the most commonly produced free radical. Phagocytic cells such as macrophages and neutrophils are prominent sources of O2 -. During an inflammatory response, these cells generate free radicals that attack invading pathogens such as bacteria and, because of this, the production of O2- by activated phagocytic cells in response to inflammation is one of the most studied free radical producing systems.
Excess free radicals can result from a variety of conditions such as tissue damage and hypoxia (limiting oxygen levels), overexposure to environmental factors (tobacco smoke, ultraviolet radiation, and pollutants), a lack of antioxidants, or destruction of free radical scavengers. When the production of damaging free radicals exceeds the capacity of the body’s antioxidant defenses to detoxify them, a condition known as oxidative stress occurs.
The hydroxyl radical (.OH) is the most reactive of the free radical molecules. OH- damages cell membranes and lipoproteins by a process termed lipid peroxidation. In fact, lipid peroxidation can be defined as the process whereby free radicals “steal” electrons from the lipids in our cell membranes, resulting in cell damage and increased production of ROS.
Catalase and glutathione peroxidase both work to detoxify O2-reactive radicals by catalyzing the formation of H2O2 derived from O2 -. The liver, kidney, and red blood cells possess high levels of catalase, which helps to detoxify chemicals in the body. The water-soluble tripeptide-thiol glutathione also plays an important role in a variety of detoxification processes. Glutathione is found in millimolar concentrations in the cell cytosol and other aqueous phases, and readily interacts with free radicals, especially the hydroxyl radical, by donating a hydrogen atom.
Adhesion Molecules
Surface-expression upregulation of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 has been demonstrated in murine coronary endothelium and cardiomyocytes after LPS and TNF-α stimulation. After cecal ligation and double puncture, myocardial intercellular adhesion molecule-1 expression increases in rats. Vascular cell adhesion molecule-1 blockade with antibodies has been shown to prevent myocardial dysfunction and decrease myocardial neutrophil accumulation, whereas both knockout and antibody blockade of intercellular adhesion molecule-1 ameliorate myocardial dysfunction in endotoxemia without affecting neutrophil accumulation. But neutrophil depletion does not protect against septic cardiomyopathy, which suggests that the cardiotoxic potential of neutrophils infiltrating the myocardium is of lesser importance in this context.
Cells and signaling pathways
It is believed that sepsis and therefore septic shock are due to the inappropriate increase in the innate immune response via circulating and tissue inflammatory cells, such as monocytes/macrophages and neutrophils. These cells normally exist in a nonactivated state but are rapidly activated in response to bacteria. Sepsis induces a dysfunction in immune cells that contributes to the development of injuries by producing mediators such as cytokines and ROS.
LPS of Gram-negative organisms induces macrophages to secrete cytokines, which in turn activate T, and B cells to upregulate the adaptive immune responses. Toll-like receptor 4 (TLR4) is the LPS receptor and its stimulation induces nuclear factor kB (NF-kB) activation. The activation of NF-kB involves phosphorylation and degradation of IkB, an inhibitor of NF-kB. The NF-kB/IkB system exerts transcriptional regulation on proinflammatory genes encoded for various adhesion molecules and cytokines. Activation of NF-kB leads to the induction of NF-kB binding elements in their promoter regions and also leads to the induction of NF-kB dependent effector genes, which produce modifications in blood flow, and aggregation of neutrophils, and platelets. This results in damaged endothelium and also coagulation abnormalities often seen in patients with sepsis and septic shock. Therefore, NF-kB is reported to be an O2 sensor in LPS-induced endotoxemia.
The sources of ROS during sepsis are:
the mitochondrial respiratory chain.
the metabolic cascade of arachidonic acid.
the protease-mediated enzyme xanthine oxidase.
granulocytes and other phagocytes activated by complement, bacteria, endotoxin, lysosomal enzymes, etc.
Other oxidases mainly NADPH oxidase.
Activated immune cells produce O2 – as a cytotoxic agent as part of the respiratory burst via the action of membrane-bound NADPH oxidase on O2.
The increase of ROS after LPS challenge has been demonstrated in different models of septic shock in peritoneal macrophages and lymphocytes. This disturbance in the balance between pro-oxidants (ROS) and antioxidants in favor of the former is characteristic of oxidative stress in immune cells in response to endotoxin. In this context,
a typical behavior of these cells under an oxidative stress situation implies changes in different immune functions such as an increase in adherence and phagocytosis and a decrease in chemotaxis. Neutrophils play a crucial role in the primary immune defense against infectious agents,which includes phagocytosis and the production of ROS. In addition, endogenous antioxidant defenses exist in a number of locations, namely intracellularly, on the cell membrane and extracellularly. The immune system is highly reliant on accurate cell-cell communication for optimal function, and any damage to the signaling systems involved will result in an impaired immune responsiveness.
Oxidative stress and modulation on GSH/GSSG (GSSG=oxidized GSH) levels also up-regulate gene expression of several other antioxidant proteins, such as manganese SOD, glutathione peroxidase, thioredoxin (Trx) and metallothionein.
Nitric Oxide
The current understanding of sepsis is a cascade of events that involves the microcirculation unevenly because of a differential effect on the large and contiguous intestinal epithelium, secondary effects on cardiopulmonary blood flows and cardiac output. This leads to a substantial body of work on therapeutic targets, either aimed at total inhibition or selective inhibition of NO synthase, and the special role of iNOS.
NO is synthesized from L-arginine by different isoenzymes of (NOS), and is implicated in a wide range of disease processes, exerting both detrimental and beneficial effects at the cellular and vascular levels. To date, three main isoforms of NOS are known:
neuronal NOS (NOS-1 or nNOS),
inducible NOS (NOS-2 or iNOS), and
endothelial NOS (NOS-3 or eNOS).
NO has been shown to play a key role in the pathogenesis of septic shock
Hyperproduction of NO induces
excessive vasodilation,
changes in vascular permeability, and
inhibition of noradrenergic nerve transmission,
all characteristics of human septic shock.
The recogniton of NO production by activated macrophages as part of the inflammatory process was an important milestone for assesing both the biological production of NO and the phenomenon of induction of NOS activity. The observation has been extended to neutrophils, lymphocytes, and other cell types. The role of NO in the pathophysiology of endotoxic shock was advanced by Thiemermann and Vane, who observed that administration of the specific NOS inhibitor N-methyl-L-arginine (L-NMMA) decreased the severe hypotension produced by administration of LPS. Other groups simultaneously reported similar results indicating that endotoxin increases NO production and prompted the idea that pharmacological inhibition of NOS may be useful in the treatment of inflammation and septic shock. However, clinical trials using L-NMMA failed to show a beneficial effect in septic shock patient. The major limitation for the use of NOS inhibitors in clinical studies is the development of pulmonary hypertension as a side effect of NOS blockade, which can be alleviated by the use of inhaled NO.
However, several compounds which modulate NO synthesis have been patented in recent years, such as various inflammatory mediators that have been implicated in the induction and activation of iNOS, particularly IFNg, TNFa, IL-1b, and platelet-activating factor (PAF) alone or synergistically. In addition to the activation of iNOS, cytokines and endotoxin may increase NO release by increasing arginine availability through the opening of the specific y+ channels and the expression of the cationic amino acid transporter (CAT), or by increasing tetrahydrobiopterin levels, a key cofactor in NO synthesis. Several experimental studies have demonstrated a decrease in NOS activity resulting in an impairment in endothelial-dependent relaxation during endotoxemia and experimental sepsis, possibly as the result of a cytokine-or hypoxia-induced shortened half-life of NOS mRNA, or of altered calcium mobilization.
Advanced Topics in Sepsis and the Cardiovascular System – Augmentation for the third Section titled:
III. Incidence of Sepsis (circulation infection with serious consequences)
NO exerts in vitro toxic effects including nuclear damage, protein and membrane phospholipid alterations, and the inhibition of mitochondrial respiration in several cell types. Mitochondrial impairment could also be considered as an adaptive phenomenon, decreasing cellular metabolism when the energy supply is limited. The toxicity of NO itself may be enhanced by the formation of ONOO- from the reaction of NO with O-2. Therefore, the multiple organ failure syndrome (MOFS) that often accompanies severe sepsis may be related to the cellular effects of excess NO or ONOO-.
Involvement of Nitrogen Species
NO reacts rapidly with ferrous iron, and at physiological concentrations, NO also binds to soluble guanylate cyclase and to another hemoprotein, cytochrome c oxidase (Complex IV), the terminal enzyme of the mitochondrial respiratory chain. NO can therefore control cellular functions via the reversible inhibition of respiration. There are a number of reactive NO species, such as
N2O3 and
ONOO-
that can also alter critical cellular components.
During the first hours after injury, iNOS-mediated NO production is upregulated, producing a burst of NO that far exceeds basal levels. This overabundance of NO produces significant cellular injury via several mechanisms.
NO may directly promote overwhelming peripheral vasodilation, resulting in vascular decomposition;
NO may upregulate the transcription NF-kB initiating an inflammatory signaling pathway that, in turn, triggers numerous inflammatory cytokines.
NO also interacts with the O-2 to yield ONOO-, a highly reactive compound that exacerbates the injury produced by either O-2 alone or NO alone.
The ONOO- generation which occurs during fluid resuscitation in the injured subject produces cellular death by enhancing DNA single strand breakage, activates the nuclear enzyme polyADP ribose synthetase (PARS), leading to cellular energy depletion and cellular necrosis. The detrimental effects of ONOO- in shock and resuscitation have been attributed to oxidation of sulfhydryl groups, the nitration of tyrosine, tryptophane, and guanine, as well as inhibition of the membrane sodium-potassium adenosine triphosphatase. PARS activation depletes NAD and thus alters electron transport, ATP synthesis, and glycolysis; and leads to DNA fragmentation and cellular apoptosis.
The activation of monocytes, macrophages and endothelial cells by LPS results in the expression of iNOS, and consequently increases the transformation of L-arginine to NO, which can combine with O2- to form ONOO-, causing tissue injury during shock, inflammation and ischemia reperfusion. NO stimulates H2O2 and O-2 production by mitochondria, increasing leakage of electrons from the respiratory chain. H2O2, in turn, participates in the upregulation of iNOS expression via NFkB activation. ONOO- has been shown to stimulate H2O2 production by isolated mitochondria. On the other hand, NO can decrease ROS-produced damage that occurs at physiological levels of NO. The high reactivity of NO with radicals might be beneficial in vivo by scavenging peroxyl radicals and inhibiting peroxidation. ONOO- may also be a signal transmitter and can mediate vasorelaxation, similarly to NO.
In sepsis, NO may exert direct and indirect effects on cardiac function. Sustained generation of NO occurs in systemic inflammatory reactions, such as septic shock with involvement in circulatory failure. In fact, myocardial iNOS activity has been reported in response to endotoxin and cytokines and inversely correlated with myocardial performance. Low-to-moderate doses of iNOS inhibitors restore myocardial contractility in hearts exposed to proinflammatory cytokines, whereas at higher doses, the effects are reversed. This finding may indicate that small amounts of NO produced by iNOS may be necessary to maintain contractility and can be cardio-protective in experimental sepsis.
A list of effects of NO in sepsis is as follows:
Inhibition of nitric oxide synthesis causes myocardial ischemia in endotoxemic rats
Nitric oxide causes dysfunction of coronary autoregulation in endotoxemic rats
Prolonged inhibition of nitric oxide synthesis in severe septic shock
Effect of L-NAME, an inhibitor of nitric oxide synthesis, on cardiopulmonary function in human septic shock: Pulmonary hypertension and reduced cardiac output during inhibition of nitric oxide synthesis in human septic shock
Effect of L-NAME, an inhibitor of nitric oxide synthesis, on plasma levels of IL-6, IL-8, TNF-a and nitrite/nitrate in human septic shock
Endothelin-1 and blood pressure after inhibition of nitric oxide synthesis in human septic shock
Distribution and metabolism of NO-nitro-L-arginine methyl ester in patients with septic shock
Pulmonary hypertension and reduced cardiac output can be major side effects of continuous NO synthase inhibition. Pulmonary vasoconstriction is undesirable because it may compromise pulmonary gas exchange and because it increases the workload on the right ventricle.
Blood pressure and systemic vascular resistance increased during infusion of the NO synthase inhibitor L-NAME, and the dosage of catecholamines was reduced. The vasoconstrictive response to L-NAME most likely was the result of blocking the NO system . In addition to the systemic effects of L-NAME, severe pulmonary vasoconstriction was observed with L-NAME.
S-Methylisothiourea sulfate (SMT) is at least 10- to 30-fold more potent as an inhibitor of inducible NOS (iNOS) in immuno-stimulated cultured macrophages (EC50, 6 ,AM) and vascular smooth muscle cells (EC50, 2 ,uM) than NG-methyl-L-arginine (MeArg) or any other NOS inhibitor yet known. The effect of SMT on iNOS activity can be reversed by excess L-arginine in a concentration-dependent manner. SMT, a potent and selective inhibitor of iNOS, may have considerable value in the therapy of circulatory shock of various etiologies and other pathophysiological conditions associated with induction of iNOS. SMT, or other iNOS-selective inhibitors, are likely to have fewer side effects which are related to the inhibition of eNOS, such as excessive vasoconstriction and organ ischemia), increased platelet and neutrophil adhesion and accumulation, and microvascular leakage.
Administration of the iron (III) complex of diethylenetriamine pentaacetic acid (DTPA iron (III), prevented death in Corynebacterium parvum 1 LPS-treated mice. Using electrochemistry, the binding of NO to DTPA iron (II) is confirmed. Treatment with DTPA iron (III) resulted in a significant decrease in mortality compared to the untreated controls. The efficacy of DTPA iron (III) increased when given to mice 2 h or more after infection. The best results were observed when DTPA iron (III) was given 5 h after infection. The iron (III) complex of diethylenetriamine pentaacetic acid (DTPA iron [III]) protected mice and baboons from the lethal effects of an infusion with live LD 100 Escherichia coli. In mice, optimal results were obtained when DTPA iron (III) was administered two or more hours after infection.
PJ34, a novel, potent PARP-1 inhibitor was found to protect against LPS induced tissue damage. PARP inhibitors protected Langendorff-perfused hearts against ischemia-reperfusion induced damages by activating the PI3-kinase–Akt pathway. The importance of the PI3-kinase–Akt pathway in LPS induced inflammatory mechanisms has gained support, raising the question whether this pathway was involved in the effect of PJ34 on LPS-induced septic shock.
Activation of the PI3-kinase–Akt/protein kinase B cytoprotective pathway is likely to contribute to the protective effects of PARP inhibitors in shock and inflammation.
Asymmetrical dimethyl arginine (ADMA) is an endogenous non-selective inhibitor of nitric oxide synthase that may influence the severity of organ failure and the occurrence of shock secondary to an infectious insult. Levels may be genetically determined by a promoter polymorphism in a regulatory gene encoding dimethylarginine dimethylaminohydrolase II (DDAH II).
ADMA levels and Sequential Organ Failure Assessment scores were directly associated on day one (p = 0.0001) and day seven (p = 0.002). The degree of acidaemia and lactaemia was directly correlated with ADMA levels at both time points (p < 0.01). On day seven, IL-6 was directly correlated with ADMA levels (p = 0.006). The variant allele with G at position -449 in the DDAH II gene was associated with increased ADMA concentrations at both time points (p < 0.05). http://pharmaceuticalintelligence.com/2012/10/20/nitric-oxide-and-sepsis-hemodynamic-collapse-and-the-search-for-therapeutic-options/ larryhbern
During sepsis, the inflammation triggers widespread coagulation in the bloodstream. A severe form of acute lung injury features pulmonary inflammation and increased capillary leak, is associated with a high mortality rate, and accounts for 100,000 deaths annually in the United States, especially associated with sepsis. Neutrophils are major effector cells at the frontier of innate immune responses, and they play a critical role in host defense against invading .microorganisms. The tissue injury appears to be related to proteases and toxic reactive oxygen radicals released from activated neutrophils. Excessive procoagulant activity is of pathophysiological significance in these disease settings. This is consistent with a pneumonia or lung injury preceding sepsis. Indeed, it is not surprising that abdominal, cardiac bypass, and post cardiac revascularization may also lead to events resembling sepsis and/or cardiovascular collapse.
The activation of the coagulation cascade is one of the earliest events initiated following tissue injury. The prime function of this complex and highly regulated proteolytic system is to generate insoluble, crosslinked fibrin strands, which bind and stabilize weak platelet hemostatic plugs, formed at sites of tissue injury. The tissue factor-dependent extrinsic pathway is the predominant mechanism by which the coagulation cascade is locally activated. The cellular effects mediated via activation of proteinase-activated receptors (PARs) may be of particular importance. In this regard, studies in PAR1 knockout mice have shown that this receptor plays a major role in orchestrating the interplay between coagulation, inflammation and lung fibrosis. The systemic inflammatory response syndrome (SIRS) is the massive inflammatory reaction resulting from systemic mediator release that may lead to multiple organ dysfunction.
For signal transduction, 01TREM-1 couples to the ITAM-containing adapter DNAX activation protein of 12 kDa (23DAP12 ). MARV and EBOV activate TREM-1 on human neutrophils, resulting in 12DAP12 phosphorylation, TREM-1 shedding, mobilization of intracellular calcium, secretion of proinflammatory cytokines, and phenotypic changes. TREM-1 is the best-characterized member of a growing family of 12DAP12-associated receptors that regulate the function of myeloid cells in innate and adaptive responses. TREM-1 (triggering receptor expressed on myeloid cells), a recently discovered receptor of the immunoglobulin superfamily, activates neutrophils and monocytes/macrophages by signaling through the adapter protein 12DAP12.
Circulating and organ-specific cell populations are activated to produce proinflammatory mediators during sepsis. Neutrophils and PBMCs bear TLR2 and TLR4, as well as other receptors, such as protein —coupled receptor, that induce increased generation of cytokines and other immunoregulatory proteins, as well as enhance release of proinflammatory mediators, including reactive oxygen species.
The expression of cytokines such as TNF-α and IL-1β is increased in sepsis, and engagement of TNF-α with type I(p55) and type II(p75) TNF receptors or IL-1β with IL-1 receptors belonging to the TLR/IL-1 receptor family produces activation of kinases (including Src, p38, extracellular signal—regulated kinase, and phosphoinositide 3–kinase) and transcriptional factors (such as nuclear factor [NF]–κB) important for further up-regulation of inflammatory proteins.
Identification of patients with cellular phenotypes characterized by increased activation of NF-κB, Akt, and protein 38, as well as discrete patterns of gene activation, may permit identification of patients with sepsis who are likely to have a worse clinical outcome In support of the hypothesis, greater nuclear accumulation of NF-κB is accompanied by higher mortality and worse clinical course in patients with sepsis. Persistent activation of NF-κB was found in nonsurvivors, with surviving patients having lower nuclear concentrations of NF-κB at early time points in their septic course than did nonsurvivors as well as more rapid return of nuclear accumulation of NF-κB. A study of surgical patients without sepsis supports the hypothesis that neutrophil phenotypes defined by NF-κB activation patterns predict clinical outcome. In that clinical series of patients undergoing repair of aortic aneurysms, higher preoperative levels of NF-κB in peripheral neutrophils were associated with death and with the development of postoperative organ dysfunction.
Insulin alleviates degradation of skeletal muscle protein by inhibiting the ubiquitin-proteasome system in septic rats
Qiyi Chen, Ning Li, Weiming Zhu, Weiqin Li, Shaoqiu Tang, et al. Chen et al. Journal of Inflammation 2011, 8:13
Hypercatabolism is common under septic conditions. Skeletal muscle is the main target organ for hypercatabolism, and this phenomenon is a vital factor in the deterioration of recovery in septic patients. In skeletal muscle, activation of the ubiquitin-proteasome system plays an important role in hypercatabolism under septic status. Insulin is a vital anticatabolic hormone and previous evidence suggests that insulin administration inhibits various steps in the ubiquitin-proteasome system. However, whether insulin can alleviate the degradation of skeletal muscle protein by inhibiting the ubiquitin-proteasome system under septic condition is unclear. This paper confirmed that mRNA and protein levels of the ubiquitin-proteasome system were upregulated and molecular markers of skeletal muscle proteolysis (tyrosine and 3-methylhistidine) simultaneously increased in the skeletal muscle of septic rats. We concluded that the ubiquitin-proteasome system is important skeletal muscle hypercatabolism in septic rats. Infusion of insulin can reverse the detrimental metabolism of skeletal muscle by inhibiting the ubiquitin-proteasome system, and the effect is proportional to the insulin infusion dose.
The International Sepsis Forum’s frontiers in sepsis: high cardiac output should be maintained in severe sepsis
Jean-Louis Vincent
Erasme Hospital, University of Brussels, Brussels, Belgium
Critical Care 2003; 7:276-278 (DOI 10.1186/cc2349)
Despite a usually normal or high cardiac output, severe sepsis is associated with inadequate tissue oxygenation, leading to organ failure and death. Some authors have suggested that raising cardiac output and oxygen delivery to predetermined supranormal values may be associated with improved
survival. While this may be of benefit in certain patients, bringing all patients to similar, supranormal values, is simplistic. It is much preferable to titrate therapy according to the needs of each individual patient. A combination of variables should be used for this purpose, in addition to a careful clinical evaluation, including not only cardiac output but also the mixed venous oxygen saturation and the blood lactate concentrations. The concept is to assess the adequacy of the cardiac output in patients with severe sepsis, enabling management strategies aimed at optimizing cardiac output to be tailored to the individual patient.
The State of US Health, 1990-2010: Burden of Diseases, Injuries, and Risk Factors
JAMA Aug 14, 2013, Vol 310, No. 6
US Burden of Disease Collaborators
We used the systematic analysis of descriptive epidemiology of 291 diseases and injuries, 1160 sequelae of these diseases and injuries, and 67 risk factors or clusters of risk factors from 1990 to 2010 for 187 countries developed for the Global Burden of Disease 2010. Disability-adjusted life-years (DALYs) were estimated as the sum of YLDs and YLLs. Deaths and DALYs related to risk factors were based on systematic reviews and meta-analyses of exposure data and relative risks for risk-outcome pairs. Healthy life expectancy (HALE) was used to summarize overall population health, accounting for both length of life and levels of ill health experienced at different ages. From 1990 to 2010, US life expectancy at birth and HALE increased, all-cause death rates at all ages decreased, and age-specific rates of years lived with disability remained stable. However, morbidity and chronic disability now account for nearly half of the US health burden, and improvements in population health in the United States have not kept pace with advances in population health in other wealthy nations. http://jama.jamanetwork.com/article.aspx?articleid=1710486HYPERLINK “http://jama.jamanetwork.com/article.aspx?articleid=1710486&goback=.gde_3267353_member_265629812#%21″&HYPERLINK “http://jama.jamanetwork.com/article.aspx?articleid=1710486&goback=.gde_3267353_member_265629812#%21″goback=%2Egde_3267353_member_265629812#%21
The Evolution of an Inflammatory Response.
Stephen F Lowry
Surgical Infections 09/2009; 10(5):419-25. · 1.80 Impact Factor
An understanding of patient-specific variation and adaptability could direct individualized biologic and management interventions for severe injury and infection. Despite more detailed appreciation of the molecular mechanisms of danger and pathogen recognition and response biology, we have much to learn about the complexity of severe injury and infection. There is a great need to extend our investigation of these mechanisms to experimental and stress-modified clinical scenarios.
Frailty and Heart Disease.
Stephan von Haehling, Stefan D Anker, Wolfram Doehner, John E Morley, Bruno Vellas
Department of Cardiology, Campus Virchow-Klinikum, Berlin, Germany.
Int j cardiol (impact factor: 7.08). 08/2013; DOI:10.1016/j.ijcard.2013.07.068
Frailty is emerging as a syndrome of pre-disability that can identify persons at risk for negative outcomes. Its presence places the individual at risk for rapid deterioration when a major event such as myocardial infarction or hospitalization occurs. In patients with cardiovascular disease, frailty is about three times more prevalent than among elderly persons without.
Pro-atrial natriuretic peptide is a prognostic marker in sepsis, similar to the APACHE II score: an observational study
Nils G Morgenthaler1, Joachim Struck1, Mirjam Christ-Crain2, Andreas Bergmann1 and Beat Müller2
1Research Department, BRAHMS AG, Biotechnology Center, Hennigsdorf/Berlin, Germany
2Department of Internal Medicine, University Hospital, Basel, Switzerland
Critical Care 2005, 9:R37-R45 (DOI 10.1186/cc3015)
Additional biomarkers in sepsis are needed to tackle the challenges of determining prognosis and optimizing selection of high-risk patients for application of therapy. In the present study, conducted in a cohort of medical intensive care unit patients, our aim was to compare the prognostic
value of mid-regional pro-atrial natriuretic peptide (ANP) levels with those of other biomarkers and physiological scores. Blood samples obtained in a prospective observational study conducted in 101 consecutive critically ill patients admitted to the intensive care unit were analyzed. The prognostic value of pro-ANP levels was compared with that of the Acute Physiology and Chronic Health Evaluation (APACHE) II score and with those of various biomarkers (i.e. C-reactive protein, IL-6 and procalcitonin). Mid-regional pro-ANP was detected in EDTA plasma from all patients using a new sandwich immunoassay. The median pro-ANP value in the survivors was 194 pmol/l (range 20–2000 pmol/l), which was significantly lower than in the nonsurvivors (median 853.0 pmol/l, range 100–2000 pmol/l; P < 0.001). On the day of admission, pro-ANP levels, but not levels of other biomarkers, were significantly higher in surviving than in nonsurviving sepsis patients (P = 0.001). In a receiver operating characteristic curve analysis for the survival of patients with sepsis, the area under the curve (AUC) for pro-ANP was 0.88, which was significantly greater than the AUCs for procalcitonin and C-reactive protein, and similar to the AUC for the APACHE II score.
Bench-to-Bedside Review: Significance and Interpretation of Elevated Troponin in Septic Patients
Raphael Favory1,2 and Remi Neviere1
1Physiology Department, School of Medicine, EA2689 University of Lille, France
2Medical Intensive Care Unit, Universitary Hospital of Lille, France
Because no bedside method is currently available to evaluate myocardial contractility independent of loading conditions, a biological marker that could detect myocardial dysfunction in the early stage of severe sepsis would be a helpful tool in the management of septic patients. Clinical and experimental studies have reported that plasma cardiac troponin levels are increased in
sepsis and could indicate myocardial dysfunction and poor outcome. The high prevalence of elevated levels of cardiac troponins in sepsis raises the question of what mechanism results in their release into the circulation.
(Note: This study is prior to the hs-troponins)
The presence of microvascular failure and regional wall motion abnormalities, which are frequently observed in positive-troponin patients, also suggest ventricular wall strain and cardiac cell necrosis. Altogether, the available studies
support the contention that cardiac troponin release is a valuable marker of myocardial injury in patients with septic shock.
Myocardial Protection in Sepsis
Simon Shakar and Brian D Lowes
University of Colorado Denver, Aurora, CO 80045, USA Critical Care 2008, 12:177 (doi:10.1186/cc6978) http://ccforum.com/content/12/5/177
Sepsis with myocardial dysfunction is seen commonly. Beta-blockers have been used successfully to treat chronic heart failure based on the premise that chronically elevated adrenergic drive is detrimental to the myocardium. However, recent reports on the acute use of beta-blockers in situations with potential hemodynamic compromise have shown the risks associated with this approach.
Myocardial injury and depression are common during sepsis and are likely multi-factorial in etiology. The adrenergic nervous system is activated in sepsis and pharmacological doses of agonists are commonly utilized during goal directed therapy to support oxygen delivery and maintain perfusion pressure. There is a large body of evidence suggesting that excessive adrenergic levels can cause myocardial damage.
Recent large prospective trials would mandate caution when using beta-blockers in acute settings of hemodynamic compromise. The COMMIT trial in acute myocardial infarction showed that metoprolol’s benefit in reducing reinfarction and arrhythmia (10 per 1,000) was offset by an increase in cardiogenic shock (11 per 1,000). This was most prominent in the first day of therapy in elderly patients with tachycardia and low blood pressure, a population reminiscent
of the one discussed in the current series. The POISE trial showed that metoprolol, started 2 to 4 hours before surgery in high risk cardiac patients, led to increased rates of death and stroke. The rates of myocardial infarction were
reduced. Hypotension was very instrumental in causing the adverse events. Interestingly, sepsis and infection were also clearly more common on metoprolol.
Myocardial depression with beta-blockers could explain the need to escalate therapy with vasoactive drugs in the current series. Gore and colleagues showed that esmolol acutely reduced cardiac output by 20% in septic patients. There was also a reduction in blood pressure and oxygen delivery. Kukin
and colleagues studied low dose beta-blockers in chronic heart failure patients. They found that even 6.25 mg of metoprolol, given orally, acutely decreased cardiac output, stroke volume and stroke work index. After 3 months and uptitration to 50 mg bid, the administration of the drug continued to cause a decrease in cardiac output and stroke work index.
Bench-to-Bedside Review: Beta-Adrenergic Modulation in Sepsis
Etienne de Montmollin, Jerome Aboab, Arnaud Mansart and Djillali Annane
Service de Réanimation Polyvalente de l’hôpital Raymond Poincaré, Garches, France
Critical Care 2009, 13:230 (doi:10.1186/cc8026 http://ccforum.com/content/13/5/230
Sepsis, despite recent therapeutic progress, still carries unacceptably high mortality rates. The adrenergic system, a key modulator of organ function and cardiovascular homeostasis, could be an interesting new therapeutic target for septic shock. beta-adrenergic regulation of the immune function in sepsis is complex and is time dependent. However, beta-2 activation as well as beta-1 blockade seems to downregulate proinflammatory response by modulating the
cytokine production profile. beta-1 blockade improves cardiovascular homeostasis in septic animals, by lowering myocardial oxygen consumption without altering organ perfusion, and perhaps by restoring normal cardiovascular variability. Beta-Blockers could also be of interest in the systemic catabolic response to sepsis, as they oppose epinephrine which is known to promote hyperglycemia, lipid and protein catabolism. Beta-1 blockade may reduce platelet aggregation and normalize the depressed fibrinolytic status induced by adrenergic stimulation. Therefore, beta-2 blockade as well as beta-2 activation improves sepsis-induced immune, cardiovascular and coagulation
dysfunctions. Beta-2 blocking, however, seems beneficial in the metabolic field. Enough evidence has been accumulated in the literature to propose beta-2 adrenergic modulation, beta-1 blockade and beta-2 activation in particular, as new promising therapeutic targets for septic dyshomeostasis, modulating favorably immune, cardiovascular, metabolic and coagulation systems.
Brain Natriuretic Peptide for Prediction of Mortality in Patients with Sepsis: a Systematic Review and Meta-Analysis
The prognostic role of brain natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NT-proBNP) in septic patients remains controversial. The purpose of this systematic review and meta-analysis was to investigate the value of elevated BNP or NT-proBNP in predicting mortality in septic patients.
PubMed, Embase and the Cochrane Central Register of Controlled Trials were searched (up to February 18, 2011). Studies were included if they had prospectively collected data on all-cause mortality in adult septic patients with either plasma BNP or NT-proBNP measurement. 12 studies with a total of 1,865 patients were included.
Elevated natriuretic peptides were significantly associated with increased risk of mortality (odds ratio (OR) 8.65, 95% confidence interval (CI) 4.94 to 15.13, P < 0.00001). The association was consistent for BNP (OR 10.44, 95% CI 4.99 to 21.58, P < 0.00001) and NT-proBNP (OR 6.62, 95% CI 2.68 to 16.34, P < 0.0001). The pooled sensitivity, specificity, positive likelihood ratio, and negative
likelihood ratio were 79% (95% CI 75 to 83), 60% (95% CI 57 to 62), 2.27 (95% CI 1.83 to 2.81) and 0.32 (95% CI 0.22 to 0.46), respectively.
Genetic Variation in Vitamin D Biosynthesis is associated with Increased Risk of Heart Failure
Genetic variation in CYP27B1 is associated with congestive heart failure in patients with hypertension.
RA Wilke, RU Simpson, BN Mukesh, SV Bhupathi, et al.
Pharmacogenomics 2009; 10(11): 1789-1797. http://dx.doi.org/10.2217/pgs.09.101
Genetic variation in vitamin D-dependent signaling is associated with congestive heart failure in human subjects with hypertension. Functional polymorphisms were selected from five candidate genes:
CYP27B1, CYP24A1, VDR, REN and ACE.
Using the Marshfield Clinic Personalized Medicine Research Project,
205 subjects with hypertension and congestive heart failure,
206 subjects with hypertension alone and
206 controls (frequency matched by age and gender) were genotyped.
In the context of hypertension, a SNP in CYP27B1 was associated with congestive heart failure (odds ratio: 2.14 for subjects homozygous for the C allele; 95% CI: 1.05–4.39).
Novel Mechanism for Disease Etiology for the Cardiac Phenotype: Modulation of Nuclear and Cytoskeletal Actin Polymerization. Lamin A/C and emerin regulate MKL1–SRF activity by modulating actin dynamics
Laminopathies, caused by mutations in the LMNA gene encoding the nuclear envelope proteins lamins A and C, represent a diverse group of diseases that include Emery–Dreifuss muscular dystrophy (EDMD), dilated cardiomyopathy (DCM), limb-girdle muscular dystrophy, and Hutchison–Gilford progeria syndrome1. Most LMNA mutations affect skeletal and cardiac muscle by mechanisms that remain incompletely understood. Loss of structural function and altered interaction of mutant lamins with (tissue-specific) transcription factors have been proposed to explain the tissue-specific phenotypes.
Altered nucleo-cytoplasmic shuttling of MKL1 was caused by altered actin dynamics in Lmna−/− and Lmna N195K/N195K mutant cells. Ectopic expression of the nuclear envelope protein emerin, which is mislocalized in Lmna mutant cells and also linked to EDMD and DCM, restored MKL1 nuclear translocation and rescued actin dynamics in mutant cells.
These findings present a novel mechanism that could provide insight into the disease aetiology for the cardiac phenotype in many laminopathies, whereby lamin A/C and emerin regulate gene expression through modulation of nuclear and cytoskeletal actin polymerization.
Heart Disease and Stroke Statistics—2011 Update
A Report From the American Heart Association
American Heart Association Statistics Committee and Stroke Statistics Subcommittee
Circulation.2011;123:e18-e209. DOI: 10.1161/CIR.0b013e3182009701
● On the basis of 2007 mortality rate data, more than 2200 Americans die of CVD each day, an average of 1 death every 39 seconds. More than 150 000 Americans killed by CVD (I00 –I99) in 2007 were 65 years of age. In 2007,
nearly 33% of deaths due to CVD occurred before the age of 75 years, which is well before the average life expectancy of 77.9 years.
● Coronary heart disease caused 1 of every 6 deaths in the United States in 2007. Coronary heart disease mortality in 2007 was 406 351. Each year, an estimated 785 000 Americans will have a new coronary attack, and 470 000 will have a recurrent attack. It is estimated that an additional 195 000 silent first myocardial infarctions occur each year. Approximately every 25 seconds, an American will have a coronary event, and approximately every minute, someone will die of one.
Prevalence and Control of Traditional Risk Factors Remains an Issue for Many Americans
● Data from the National Health and Nutrition Examination Survey (NHANES) 2005–2008 indicate that 33.5% of US adults 20 years of age have hypertension (Table 7-1). This amounts to an estimated 76 400 000 US adults with hypertension. The prevalence of hypertension is nearly equal between men and women. African American adults have among the highest rates of hypertension in the world, at 44%. Among hypertensive adults, ~ 80% are aware of their condition, 71% are using antihypertensive medication, and only 48% of those aware that they have hypertension have their condition controlled.
● Despite 4 decades of progress, in 2008, among Americans >18 years of age, 23.1% of men and 18.3% of women continued to be cigarette smokers. In 2009, 19.5% of students in grades 9 through 12 reported current tobacco use. The percentage of the nonsmoking population with detectable serum cotinine (indicating exposure to secondhand smoke) was 46.4% in 1999 to 2004, with declines occurring, and was highest for those 4 to 11 years of age (60.5%) and those 12 to 19 years of age (55.4%).
● An estimated 33 600 000 adults > 20 years of age have total serum cholesterol levels > 240 mg/dL, with a prevalence of 15.0% (Table 13-1).
● In 2008, an estimated 18 300 000 Americans had diagnosed diabetes mellitus, representing 8.0% of the adult population. An additional 7 100 000 had undiagnosed diabetes mellitus, and 36.8% had prediabetes, with abnormal
fasting glucose levels. African Americans, Mexican Americans, Hispanic/Latino individuals, and other ethnic minorities bear a strikingly disproportionate burden of diabetes mellitus in the United States (Table 16-1).
Commentary on Other Related Articles on this topic published on this Open Access Online Scientific Journal:
The immune response mechanism is the holy grail of the human defense system for health. IDO, indolamine 2, 3-dioxygenase, is a key gene for homeostasis of immune responses and producing an enzyme catabolizing the first rate-limiting step in tryptophan degradation metabolism. The hemostasis of immune system is complicated. IDO belongs to globin gene family to carry oxygen and heme.
The main function and genesis of IDO comes from the immune responses during host-microbial invasion and choice between tolerance and immunogenicity. In addition IDO has a role in vascular tone as well. In human there are three kinds of IDOs, which are IDO1, IDO2, and TDO, with distinguished mechanisms and expression profiles. , IDO mechanism includes three distinguished pathways: enzymatic acts through IFNgamma, non-enzymatic acts through TGFbeta-IFNalpha/IFNbeta and moonlighting acts through AhR/Kyn.
IDO is a key homeostatic regulator and confined in immune system mechanism for the balance between tolerance and immunity. This gene encodes indoleamine 2, 3-dioxygenase (IDO) – a heme enzyme (EC=1.13.11.52) that catalyzes the first rate-limiting step in tryptophan catabolism to N-formyl-kynurenine and acts on multiple tryptophan substrates including D-tryptophan, L-tryptophan, 5-hydroxy-tryptophan, tryptamine, and serotonin (1; 2; 3; 4).
Expression of IDO is common in antigen presenting cells (APCs), monocytes (MO), macrophages (MQs), DCs, T-cells, and some B-cells. IDO presentation in APCs is related to its role in the hierarchy and level of DC expression, but includes MOs in three DC cell subsets, CD14+CD25+, CD14++CD25+ and CD14+CD25++.
There are three types of IDO, pro-IDO like, IDO1, and IDO2. In addition, another enzyme called TDO, tryptophan 2, 3, dehydrogenase solely degrades L-Trp by a rate-limiting mechanism in liver and brain.
The IDO1 mechanism is the target for immunotherapy applications. The initial discovery of IDO in human physiology is protection of pregnancy since lack of IDO results in premature recurrent abortion. The initial rate-limiting step of tryptophan metabolism is catalyzed by either IDO or tryptophan 2, 3-dioxygenase (TDO), but the two are regulated with different mechanisms due to a His55 in TDO and a Ser167b in IDO.
IDO binds to only immune response cells, and TDO relates to NAD biosynthesis and is expressed solely in liver and brain. It has been shown that knowledge on NADH/NAD, Kyn/Trp or Trp/Kyn ratios as well as Th1/Th2, CD4/CD8 or Th17/Th_reg are equally important for assessing the metabolic state.
DCs are the orchestrator of the immune response with list of functions in uptake, processing, and presentation of antigens; activation of effector cells, such as T-cells and NK-cells; and secretion of cytokines and other immune-modulating molecules to direct the immune response.
Systemic inflammation (pneumonia, sepsis, malaria) creates hypotension and IDO expression has the effect of decreased vascular tone. Moreover, inflammation activates the endothelial coagulation activation system causing coagulopathies on patients. This reaction is namely endothelial cell activation of IDO by IFNgamma inducing Trp to Kyn conversion. Inflammation induces IDO expression in endothelial cells producing Kyn causing decrease of trp, arterial relaxation, and hypotension.
IDO, indolamine 2, 3-dioxygenase, is a key gene for homeostasis of immune responses and producing an enzyme catabolizing the first rate-limiting step in tryptophan degradation metabolism.
The mechanism of microbial response and origination of IDO is based on duplication of microbial IDO . During microbial responses, Toll-like receptors (TLRs) play a role to differentiate and determine the microbial structures as a ligand to initiate production of cytokines and pro-inflammatory agents to activate specific T helper cells. Uniqueness of TLR comes from four major characteristics of each individual TLR by ligand specificity, signal transduction pathways, expression profiles and cellular localization . Thus, TLRs are important part of the immune response signaling mechanism to initiate and design adoptive responses from innate (naïve) immune system to defend the host.
The modification of IDO+ monocytes manage towards a specific subset of T cell activation with specific TLRs are significantly important. The type of cell with correct TLR and stimuli improves or decreases the effectiveness of stimuli. .
Inhaled nitric oxide is a selective pulmonary vasodilator that improves ventilation–perfusion matching at low doses in patients with acute respiratory failure, potentially improving oxygenation and lowering pulmonary vascular resistance.
Treatment Goals for Inhaled Nitric Oxide
Improved oxygenation
Decreased pulmonary vascular resistance
Decreased pulmonary edema
Reduction or prevention of inflammation
Protection against infection
Dose-Response for Respiratory Failure in the Adult Patient – a response is defined as a 20 percent increase in oxygenation.
Dose-Response for Pulmonary Hypertension in the Adult Patient – a 30 percent decrease in pulmonary vascular resistance during the inhalation of nitric oxide (10 ppm for 10 minutes) has been used to identify an association with vascular responsiveness to agents that can be helpful in the long term.
among older Americans, more are hospitalized for HF than for any other medical condition.
Prevalence estimates for HF were determined from 1999–2008 National Health and Nutrition Examination Survey (NHANES) and US Census Bureau projected population counts for years 2012 to 2030. HF is a clinical syndrome that results from a variety of cardiac disorders.
In the Western world the top 3 causes of HF are:
coronary artery disease
valvular disease
hypertension
Stages C and D represent the symptomatic phases of HF, with stage C manageable and stage D failing medical management, resulting in marked symptoms at rest or with minimal activity despite optimal medical therapy.
Classic demographic risk factors for the development of HF include:
older age,
male gender,
ethnicity, and
low socioeconomic status.
comorbid disease states contribute to the development of HF
Ischemic heart disease
Hypertension
Diabetes mellitus, insulin resistance, and obesity are also linked to HF development,
with diabetes mellitus increasing the risk of HF by +2-fold in men and up to 5-fold in women.
Smoking remains the single largest preventable cause of disease and premature death in the United States.
Hypertension caused by Arterial Stiffening is Ineffectively Treated by Diuretics and Vasodilatation Antihypertensives
Dr Reuven Zimlichman (Tel Aviv University, Israel) http://www.theheart.org/article/1502067.do
the definitions of hypertension, as well as the risk-factor tables used to guide treatment, are no longer appropriate for a growing number of patients. New ambulatory blood-pressure-monitoring devices also measure arterial elasticity. “Unquestionably, these will improve our ability to diagnose both the status of the arteries and the changes of the arteries with time as a result of our treatment. So if we treat the patient and we see no improvement in arterial elasticity, something is not working—either the patient is not taking the medication, or our choice of medication is not appropriate, or the dose is insufficient, etc.”
Conceptual development of the subject is presented in the following nine parts:
1. Physiology of Circulation and Role of Arterial Elasticity
2. Isolated Systolic Hypertension caused by Arterial Stiffening may be inadequately treated by Diuretics or Vasodilatation Antihypertensive Medications
3. Physiology of Circulation and Compensatory Mechanism of Arterial Elasticity
4. Vascular Compliance – The Potential for Novel Therapies Novel Mechanism for Disease Etiology: Modulation of Nuclear and Cytoskeletal Actin Polymerization. Genetic Therapy targeting Vascular Conductivity, Regenerative Medicine for Vasculature Protection
5. In addition to curtailing high pressures, stabilizing BP variability is a potential target for management of hypertension
6. Mathematical Modeling: Arterial stiffening explains much of primary hypertension
7. Classification of Blood Pressure and Hypertensive Treatment Best Practice of Care in US
8. Genetic Risk for High Blood Pressure
9. Is it Hypertension or Physical Inactivity: Cardiovascular Risk and Mortality – New results in 3/2013.
Elastance in a cyclic pressure system of systole-diastole (contraction-dilation) presents impedance as a pulsatile load on the heart. Chronic exposure to elevated vascular impedance leads to impairment of lusiotropy (diastolic failure, stiff heart) and inotropy (systolic failure, weak heart).
Stiff or “lead pipe” blood vessels drop pressure precipitously to dangerously low levels in response to diuretics.
Stiff walls due to fibrosis or scar tissue have limited ability to dilate
Physiology of Circulation and Compensatory Mechanism of Arterial Elasticity
Arguably, HMG-CoA reductase inhibitors, statin therapy is a second example of a medication that helps protect vascular elasticity, both by its lipid effects and its anti-inflammatory effects.
While among other reasons for Hypertension increasing prevalence with aging, arterial stiffening is one.
Yet, stiffer vessels are more efficient at transmitting pressure to distal targets. With aging, muscle mass diminishes markedly and the contribution to circulation from skeletal muscle tissue compressions combined with competent venous valves fades.
With aging heart contractility diminishes. These issues can cause under perfusion of tissues, inadequate nutrient blood delivery (ischemia), lactic acidosis, tissue dysfunction and multi-organ failure. Hardened arteries may compensate. Thus, pharmacotherapy to increase Arterial Elasticity may be counter-indicated for patients with mild to progressive CHF.
The hypothesis that we should focus on cellular therapies to increase vascular compliance may decrease the circulation efficiency and result in worsening of cardiac right ventricular morphology and development of Dilated cardiomyopathy and hypertrophic cardiomyopathy (muscle thickening and diastolic failure), an undesirable outcome resulting from an attempt to treat the hypertension.
“Coronary” describes the crown-like position of arteries on the heart that provide its nutrient blood supply. The heart does not live off of the blood in its chambers, but rather receives its nutrient perfusion from branches of the aorta, like all other organs. The most relied on method to exam coronary artery anatomy is angiography – xray image movies obtained while the blood is opacified by injection of iodine (high atomic number to block xrays) to provide a contrast between arterial flow channel (the lumen) and the surrounding tissues. Computed tomography is providing a second-best alternative with 3D reconstructions that can be obtained less invasively (no catheters), but it often fails to see the posterior descending artery (PDA) well, and is lower in resolution (point-discrimination detail) than xray angiography (XRA). Magnetic resonance angiography (MRA) comes in as a distant third place method for examining coronary anatomy (lower quality, lower reliability), but non-invasive with no ionizing radiation. A major goal of defining coronary anatomy in individual patients is to identify coronary artery disease (CAD) and to clarify best options for management – to relieve angina and to avoid adverse consequences, e.g., heart attacks (myocardial infarction), heart failure (CHF) and death. The COURAGE trial showed that for many, aggressive medical management with statins and blood pressure control may obviate need for percutaneous or surgical interventions to control angina and minimize the risk of adverse outcomes. Patients with blockage of the left main coronary artery, or two vessel blockage including proximal left anterior descending (LAD) especially with below normal ejection fraction may be better off in the long run with bypass surgery. Therefore less invasive imaging sufficient to rule out left main disease and proximal LAD disease may suffice for decision making (except that the BARI trial results have not been overturned in favoring bypass surgery for diabetics).
On the left an overview of the coronary arteries in the anterior projection.
Coronary anatomy and anomalies
Left Main or left coronary artery (LCA)
Left anterior descending (LAD)
diagonal branches (D1, D2)
septal branches
Circumflex (Cx)
Marginal branches (M1,M2)
Right coronary artery
Acute marginal branch (AM)
AV node branch
Posterior descending artery (PDA)
RCA, LAD and Cx in the anterior projection
On the left an overview of the coronary arteries in the lateral projection.
Left Main or left coronary artery (LCA)
Left anterior descending (LAD)
diagonal branches (D1, D2)
septal branches
Circumflex (Cx)
Marginal branches (M1,M2)
Right coronary artery
Acute marginal branch (AM)
AV node branch
Posterior descending artery (PDA)
RCA, LAD and Cx in the right anterior oblique projection
On the left an overview of the coronary arteries in the lateral projection.
Left Main or left coronary artery (LCA)
Left anterior descending (LAD)
diagonal branches (D1, D2)
septal branches
Circumflex (Cx)
Marginal branches (M1,M2)
Right coronary artery
Acute marginal branch (AM)
AV node branch
Posterior descending artery (PDA)
RCA, LAD and Cx in the lateral projection
Left Coronary Artery (LCA)
The left coronary artery (LCA) is also known as the left main.
The LCA arises from the left coronary cusp.
The aortic valve has three leaflets, each having a cusp or cup-like configuration.
These are known as the left coronary cusp (L), the right coronary cusp (R) and the posterior non-coronary cusp (N).
Just above the aortic valves there are anatomic dilations of the ascending aorta, also known as the sinus of Valsalva. The left aortic sinus gives rise to the left coronary artery.
The right aortic sinus which lies anteriorly, gives rise to the right coronary artery.
The non-coronary sinus is postioned on the right side.
Left coronary (LC), right coronary (RC) and posterior non-coronary (NC) cusp
The LCA divides almost immediately into the circumflex artery (Cx) and left anterior descending artery (LAD).
On the left an axial CT-image.
The LCA travels between the right ventricle outflow tract anteriorly and the left atrium posteriorly and divides into LAD and Cx.
On the image on the left we see the left main artery dividing into
Cx with obtuse marginal branch (OM)
LAD with diagonal branches (DB)
On volume rendered images the left atrial appendage needs to be removed to get a good look on the LCA.
In 15% of cases a third branch arises in between the LAD and the Cx, known as the ramus intermedius or intermediate branch.
This intermediate branche behaves as a diagonal branch of the Cx.
Left Anterior Descending (LAD)
The LAD travels in the anterior interventricular groove and continues up to the apex of the heart.
The LAD supplies the anterior part of the septum with septal branches and the anterior wall of the left ventricle with diagonal branches.
The LAD supplies most of the left ventricle and also the AV-bundle.Mnemonic: Diagonal branches arise from the LAD.
CT image of the LAD in RAO projection
The diagonal branches come off the LAD and run laterally to supply the antero-lateral wall of the left ventricle.
The first diagonal branch serves as the boundary between the proximal and mid portion of the LAD (2).
There can be one or more diagonal branches: D1, D2 , etc.
Circumflex (Cx)
The Cx lies in the left AV groove between the left atrium and left ventricle and supplies the vessels of the lateral wall of the left ventricle.
These vessels are known as obtuse marginals (M1, M2…), because they supply the lateral margin of the left ventricle and branch off with an obtuse angle.
In most cases the Cx ends as an obtuse marginal branch, but 10% of patients have a left dominant circulation in which the Cx also supplies the posterior descending artery (PDA).Mnemonic: Marginal branches arise from the Cx and supply the lateral Margin of the left ventricle.
Circumflex and LAD seen in Lateral projection
Right Coronary Artery (RCA)
The right coronary artery arises from the anterior sinus of Valsalva and courses through the right atrioventricular (AV) groove between the right artium and right ventricle to the inferior part of the septum.
In 50-60% the first branch of the RCA is the small conus branch, that supplies the right ventricle outflow tract.
In 20-30% the conus branch arises directly from the aorta.
In 60% a sinus node artery arises as second branch of the RCA, that runs posteriorly to the SA-node (in 40% it originates from the Cx).
The next branches are some diagonals that run anteriorly to supply the anterior wall of the right ventricle.
The large acute marginal branch (AM) comes off with anacute angle and runs along the margin of the right ventricle above the diaphragm.
The RCA continues in the AV groove posteriorly and gives off a branch to the AV node.
In 65% of cases the posterior descending artery (PDA) is a branch of the RCA (right dominant circulation).
The PDA supplies the inferior wall of the left ventricle and inferior part of the septum.
RCA, LAD and LCx in Anterior projection
On the image on the far left we see the most common situation, in which the RCA comes off the right cusp and will provide the conus branch at a lower level (not shown).
On the image next to it, we see a conus branch, that comes off directly from the aorta.
LEFT: RCA comes off the right sinus of Valsalva
RIGHT: Conus artery comes off directly from the aorta
The large acute marginal branch (AM) supplies the lateral wall of the right ventricle.
In this case there is a right dominant circulation, because the posterior descending artery (PDA) comes off the RCA.
Coronary Anomalies
Coronary anomalies are uncommon with a prevalence of 1%.
Early detection and evaluation of coronary artery anomalies is essential because of their potential association with myocardial ischemia and sudden death (3).
With the increased use of cardiac-CT, we will see these anomalies more frequently.
Coronary anomalies can be differentiated into anomalies of the origin, the course and termination (Table).
The illustration in the left upper corner is the most common and clinically significant anomaly.
There is an anomalous origin of the LCA from the right sinus of Valsalva and the LCA courses between the aorta and pulmonary artery.
This interarterial course can lead to compression of the LCA (yellow arrows) resulting in myocardial ischemia.
The other anomalies in the figure on the left are not hemodynamically significant.
Interarterial LCA
On the left images of a patient with an anomalous origin of the LCA from the right sinus of Valsalva and coursing between the aorta and pulmonary artery.
Sudden death is frequently observed in these patients.
ALCAPA
On the left images of a patient with an anomalous origin of the LCA from the pulmonary artery, also known as ALCAPA.
ALCAPA results in the left ventricular myocardium being perfused by relatively desaturated blood under low pressure, leading to myocardial ischemia.
ALCAPA is a rare, congenital cardiac anomaly accounting for approximately 0.25-0.5% of all congenital heart diseases.
Approximately 85% of patients present with clinical symptoms of CHF within the first 1-2 months of life.
Myocardial bridging
Myocardial bridging is most commonly observed of the LAD (figure).
The depth of the vessel under the myocardium is more important that the lenght of the myocardial bridging.
There is debate, whether some of these myocardial bridges are hemodynamically significant.
Fistula
On the image on the left we see a large LAD giving rise to a large septal branch that terminates in the right ventricle (blue arrow).
Left to right shunt: septal branch of LAD teminates in right ventricle
Cardiology Site
by M. Abdulla
This site includes instructional movies, 3-D animation, panoramic views, online quiz, interactive video-clips, interactive heart sounds & murmurs and interactive echocardiograms.
Robin Smithuis and Tineke Wilems
Radiology department of the Rijnland Hospital Leiderdorp and the University Medical Centre Groningen, the Netherlands. http://rad.desk.nl/en/48275120e2ed5
Cardiovascular Complications: Death from Reoperative Sternotomy after prior CABG, MVR, AVR, or Radiation; Complications of PCI; Sepsis from Cardiovascular Interventions
Author, Introduction and Summary: Justin D Pearlman, MD, PhD, FACC
and
Article Curator: Aviva Lev-Ari, PhD, RN
The Curator recommends the e-Reader to read the following book on Surgical Complications:
Complications
“Essential Reading For Anyone Involved In Medicine”–Amazon.com – 2002
IIb. PAD Endovascular Interventions: Carotid Artery Endarterectomy
III. Incidence of Sepsis (circulation infection with serious consequences)
UPDATED 11/2/2013
As minimally interventional techniques improve, patients are offered a choice of invasive surgical remedies or less invasive procedures (video assisted, robotic, or percutaneous). The decision should not rest on the size of the scar or even the up front risk and discomfort, but rather should weigh all aspects of the risks and benefits. In addition to the risks and benefits for the current problem, one should also consider why the problem occurred and its likelihood of recurrence. Open chest surgery has a clear disadvantage when it comes to recurrences, as the scars from first surgery interfere with second surgery. Opening the chest (sternotomy) for a second or third time poses elevated risks analyzed herein. This article reviews data from major centers addressing the risks from repeat sternotomy and from minimally invasive cardiovascular surgeries. Any invasion of the body elevates risk of infection, which can lead to sepsis and possible death, so that risk is also addressed.
This article addresses specific reports of complications but does not cover numerous other complications that may occur, such as lung collapse, cardiogenic shock, blood loss, local infection, emboli, thrombus, stroke.
Read at the 90th Annual Meeting of The American Association for Thoracic Surgery, Toronto, Ontario, Canada, May 1–5, 2010. Received for publication April 6, 2010; revisions received July 19, 2010; accepted for publication July 30, 2010.
doi:10.1016/j.jtcvs.2010.07.086
Particular attention to protective strategies should be considered during reoperative sternotomy among patients with multiple previous sternotomies, previous mediastinal radiotherapy, and those with patent internal thoracic artery grafts. (J Thorac Cardiovasc Surg 2010;140:1028-35)
Of the 2555 patients,
1537 (60%) had undergone previous coronary artery bypass grafting,
Division of Cardiovascular Surgery, Mayo Clinic, Rochester, MN 55905, USA.
Abstract
OBJECTIVES:
A variety of protective strategies during repeat sternotomy been proposed; however, it remains unclear for which patients they are warranted.
METHODS:
We identified adults undergoing repeat median sternotomy for routine cardiac surgery at our institution between January 1, 1996, and December 31, 2007. The operative notes and perioperative outcomes were reviewed.
RESULTS:
Of the 2555 patients, 1537 (60%) had undergone previous coronary artery bypass grafting, 700 (27%) previous mitral valve surgery, and 643 (25%) previous aortic valve replacement (AVR). Sixty-one patients (2%) had prior mediastinal radiotherapy, and 424 (17%) had more than one previous sternotomy. In 231 patients, 267 injuries (9.0%) occurred. Injury occurred during sternotomy in 87 patients (33%) and during prepump dissection in 135 (51%). The hospital mortality rate was 6.5% among those without injury and 18.5% among those with injury (P < .001); when injury occurred during sternal division, the mortality rate was 25%. Injuries were more common after previous coronary artery bypass grafting (11% with previous coronary artery bypass grafting vs 7% without, P = .0012) but not previous AVR, mitral valve surgery, or aortic surgery. Injury was also more common when the current operation was AVR (10% with AVR vs 8% without, P = .04) or aortic surgery (14% vs 8%, P = .004). On multivariate analysis, previous radiotherapy (odds ratio, 4.9), a greater number of previous sternotomies (odds ratio 1.7), and a patent internal thoracic artery (odds ratio, 1.8) predicted injury. Injury was an independent risk factor of hospital death (odds ratio, 2.6).
CONCLUSIONS:
Particular attention to protective strategies should be considered during reoperative sternotomy among patients with multiple previous sternotomies, previous mediastinal radiotherapy, and those with patent internal thoracic artery grafts.
Previous operation No injury (n 1/4 2324) Injury (n 1/4 231) P value
CABG 1375 (59.2%) 162 (70.1%) .001
Aortic valve surgery 586 (25.2%) 57 (24.7%) .857
Mitral valve surgery 645 (27.8%) 55 (23.8%) .200
Tricuspid valve surgery 64 (2.8%) 9 (3.9%) .320
Aorta surgery 167 (7.2%) 20 (8.7%) .413
Current operation No injury (n 1/4 2324) Injury (n 1/4 231) P value
CABG 897 (38.6%) 104 (45.0%) .056
Aortic valve surgery 1020 (43.9%) 118 (51.1%) .036
Mitral valve surgery 821 (35.3%) 80 (34.6%) .833
Tricuspid valve surgery 414 (17.8%) 52 (22.5%) .078
Aortic surgery 232 (10.0%) 37 (16.0%) .004
DISCUSSION
The results of the present study have confirmed the significant risk of cardiovascular injury during reoperative cardiac surgery. The death rate from such injury can be 10-30%, particularly when occurring during division of the sternum. These risks are greatest among patients with multiple previous sternotomies or prior chest radiotherapy.
Current PROTOCOL at Virginia University, now suggested to be considered for adoption @Mayo Clinic:
The Mayo Clinic’s Authors write: Our findings are more consistent with those reported by Roselli and colleagues.2 The explanation of these institutional differences is unclear, although a number of practice differences are likely present between these institutions in terms of both patient substrate and surgical practice. Compared with the series from the University of Virginia, the Mayo series we have reported represents a greater percentage of total cases performed at the institution (13.5% vs 7.8%), with a somewhat greater percentage of those reoperations being for CABG (41% vs 60%). In the Mayo series, a lower percentage were first-time repeat sternotomies (83% vs 90%) and a greater percentage were the fourth time or more (2.7% vs 1.1%).
The incidence of previous radiotherapy in the University of Virginia series was not reported.
It is also unclear to what degree the differences in surgical practice, including the role of the assistant surgeons in performing the repeat sternotomy, could account for these differences. In the present retrospective study, we were unable to demonstrate an effect of experience or expertise in either the occurrence of injury or the outcome. However, it is clear to all practicing surgeons that, when injury occurs, the judgment and expertise of the operating surgeon is critical to expeditious institution of CPB or other ‘‘rescue’’ maneuvers.
Perhaps of more practical value and broad applicability, however, is the standardized approach to repeat sternotomy advocated by the group at the University of Virginia, including routine preoperative CT scanning if the procedure is the third or fourth sternotomy and insertion of a femoral arterial line by which emergent percutaneous arterial inflow cannulation can be accomplished, if necessary. In their series, emergent institution of CPB using the femoral route was instituted in 1.8% of reoperative patients, constituting 19% of the patients with injury. Most notably, in their series, no deaths occurred among these patients. Serious consideration should be given to adopting such protocols.
Our high mortality rate associated with SVG injury during sternotomy, however, supports the recommendation by others to carefully assess the course of bypass grafts by preoperative angiography. Routine preoperative CT imaging of all patients with more than one previous sternotomy has been advocated by Morishita and colleagues,3 with a demonstrable reduction in operative complications. Roselli and colleagues2 identified a lack of preparative imaging as the most common ‘‘lapse’’ in the preventive strategy among patients with injury. Our data suggest that CT scanning might be particularly helpful in the subset of patients with multiple previous sternotomies or radiotherapy and would support the institution of a policy of routine scanning for these patients.
FIGURE 1. Hospital mortality according to emergent cardiopulmonary bypass (CPB) in The Journal of Thoracic and Cardiovascular Surgery c November 2010, pp. 1032
TABLE 5. Postoperative results
No injury (n 1/4 2324) — Injury (n 1/4 231) — P value
Postoperative transfusion (U)
PRCs 4.5 7.2 6.5 8.9 .046
ICU stay (h) 102.3 228.6 146.3 +/- 346.9 <.001
Reoperation for bleeding 127 (5.5%) 21 (9.1%) .024
The Journal of Thoracic and Cardiovascular Surgery c November 2010, pp. 1032
Independent predictors for injury during repeat median sternotomy
The structures injured and the timing of injury in our study were similar to those reported by Roselli and colleagues.2 Bypass grafts were the most commonly injured and, perhaps in contrast to expectations, most injuries occurred during dissection, not during sternal division. Unlike their study, however, we found injury during sternal division to carry a greater mortality risk. We observed a remarkably high mortality rate associated with injury to the right ventricle, as did Roselli and colleagues.2 This may be particularly true in the presence of pulmonary hypertension, when attempts to repair the injury are hampered by inadequate access, progressive tearing of the ventricle secondary to traction injury, and what can be a relatively thin and friable free wall. The incidence of injury to the Internal thoracic artery (ITA) in our series (4.9%) was comparable to the 4.4%–5.3% reported by other investigators.11-14 Because the ITA was damaged more often during prepump dissection (20.7%) than during re-entry (11.5%), these data support the trend to avoid dissecting and isolating the ITA during AVR after previous CABG.12,13
FOUR CONCLUSIONS
1. On the basis of these data, we would advocate preoperative axial CT imaging to define the proximity of cardiovascular structures to the sternum of patients who have undergone more than one previous sternotomy and those who have undergone radiotherapy because these patients statistically have the greatest risk of injury.
2. We would also advocate considering percutaneous or open access of the femoral vessels, if not the institution of CPB, before sternotomy in these same patients, as well as those with significant pulmonary hypertension.
3. Because injury is common during prepump dissection, we support a philosophy of leaving patent ITA grafts undisturbed by attempts to gain control during AVR after previous CABG.
4. Finally, given the mortality rate associated with graft injury, patients with previous CABG should be considered for graft angiography or high-resolution CT.
Summary
This is a very important study on the Outcomes and the Complications involved in Cardiac Surgery @Mayo Clinic.
Study’s Objectives: A variety of protective strategies during repeat sternotomy been proposed; however, it remains unclear for which patients they are warranted.
Authors @Mayo Clinic reported:
We were unable to definitively assess the effect of any specific protective strategies on the incidence of injury. Because we do not have standardized or uniform prospective institutional policies in this regard, it was not possible to account for the confounding factor of the clinician’s judgment in the decision to use these strategies in particularly highrisk patients.
Our high mortality rate associated with saphenous vein graft (SVG) injury during sternotomy, however, supports the recommendation by others to carefully assess the course of bypass grafts by preoperative angiography.Routine preoperative CT imaging of all patients with more than one previous sternotomy has been advocated by Morishita and colleagues,3 with a demonstrable reduction in operative complications.
The reader is advised to review another article Co-Curated by us on the following related study by Mayo Clinic researches, This article examines 10-year to 15-year survivals from arterial bypass grafts using arterial vs saphenous venous grafts.
In patients undergoing isolated coronary artery bypass graft surgery with LIMA to left anterior descending artery,
arterial grafting of the non-left anterior descending vessels conferred a survival advantage at 15 years compared with Saphenous Venous grafting (SVG).
It is still unproven whether these results apply to higher-risk subgroups of patients.
Impact of Intra-procedural Stent Thrombosis during Percutaneous Coronary Intervention: Insights from the CHAMPION PHOENIX Trial ONLINE FIRST
Philippe Généreux, MD1; Gregg W. Stone, MD1; Robert A. Harrington, MD4; C. Michael Gibson, MD5; Ph. Gabriel Steg, MD6; Sorin J. Brener, MD10; Dominick J. Angiolillo, MD, PhD11; Matthew J. Price, MD12; Jayne Prats, PhD13; Laura LaSalle, MPH2; Tiepu Liu, MD, PhD12; Meredith Todd, B.Sc12; Simona Skerjanec, Pharm.D12; Christian W. Hamm, MD14; Kenneth W. Mahaffey, MD4; Harvey D. White, DSc15; Deepak L. Bhatt, MD, MPH16
Objective We sought to evaluate the clinical impact of intra-procedural stent thrombosis (IPST), a relatively new endpoint.
Background In the prospective, double-blind, active-controlled CHAMPION PHOENIX trial, cangrelor significantly reduced periprocedural and 30-day ischemic events in patients undergoing percutaneous coronary intervention (PCI), including IPST.
Methods An independent core laboratory blinded to treatment assignment performed a frame-by-frame angiographic analysis in 10,939 patients for the development of IPST, defined as new or worsening thrombus related to stent deployment anytime during the procedure. Adverse events were adjudicated by an independent, blinded clinical events committee.
Results IPST developed in 89 patients (0.8%), including 35/5470 (0.6%) and 54/5469 (1.0%) in the cangrelor and clopidogrel arms, respectively (OR [95%CI] = 0.65 [0.42,0.99], p=0.04). Compared to patients without IPST, IPST was associated with a marked increase in composite ischemia (death, myocardial infarction [MI], ischemia-driven revascularization, or new onset out-of-lab stent thrombosis [ARC]) at 48 hours and at 30 days (29.2% vs. 4.5% and 31.5% vs. 5.7%, P<0.0001 for both). After controlling for potential confounders, IPST remained a strong predictor of all adverse ischemic events at both time points.
Conclusion In the large-scale CHAMPION PHOENIX trial, the occurrence of IPST was strongly predictive of subsequent adverse cardiovascular events. The potent intravenous ADP antagonist cangrelor substantially reduced IPST, contributing to its beneficial effects at 48 hours and 30 days.
Bleeding and Vascular Complications at the Femoral Access Site Following Percutaneous Coronary Intervention (PCI): An Evaluation of Hemostasis Strategies
Dale R. Tavris, MD, MPH1, Yongfei Wang, MS2, Samantha Jacobs, BS1, Beverly Gallauresi, MPH, RN1, Jeptha Curtis, MD2, John Messenger, MD3, Frederic S. Resnic, MD, MSc4, Susan Fitzgerald, MS, RN5
Authors Affiliation
From the 1US Food and Drug Administration (FDA), Silver Spring, Maryland, 2Yale University, New Haven, Connecticut, 3University of Colorado, Boulder, Colorado, 4Brigham and Women’s Hospital, Boston, Massachusetts, and 5the American College of Cardiology, Bethesda, Maryland.
Abstract: Background. Previous research found at least one vascular closure device (VCD) to be associated with excess vascular complications, compared to manual compression (MC) controls, following cardiac catheterization. Since that time, several more VCDs have been approved by the Food and Drug Administration (FDA). This research evaluates the safety profiles of current frequently used VCDs and other hemostasis strategies. Methods. Of 1089 sites that submitted data to the CathPCI Registry from 2005 through the second quarter of 2009, a total of 1,819,611 percutaneous coronary intervention (PCI) procedures performed via femoral access site were analyzed. Assessed outcomes included bleeding, femoral artery occlusion, embolization, artery dissection, pseudoaneurysm, and arteriovenous fistula. Seven types of hemostasis strategy were evaluated for rate of “any bleeding or vascular complication” compared to MC controls, using hierarchical multiple logistic regression analysis, controlling for demographic factors, type of hemostasis, several indices of co-morbidity, and other potential confounding variables. Rates for different types of hemostasis strategy were plotted over time, using linear regression analysis.Results. Four of the VCDs and hemostasis patches demonstrated significantly lower bleeding or vascular complication rates than MC controls: Angio-Seal (odds ratio [OR], 0.68; 95% confidence interval [CI], 0.65-0.70); Perclose (OR, 0.54; CI, 0.51-0.57); StarClose (OR, 0.77; CI, 0.72-0.82); Boomerang Closure Wire (OR, 0.63; CI, 0.53-0.75); and hemostasis patches (OR, 0.70; CI, 0.67-0.74). All types of hemostasis strategy, including MC, exhibited reduced complication rates over time. All trends were statistically significant except one. Conclusions. This large, nationally representative observational study demonstrated better safety profiles for most of the frequently used VCDs, compared to MC controls.
The benefits of the transradial approach have clearly been documented in numerous studies in the past ten years.1–9 Access site bleeding complication rates are lower and early ambulation results in a significant reduction in patient morbidity and a lower total procedure cost.3,4 Both patients undergoing the procedure and staff caring for these patients overwhelmingly prefer the transradial approach.10
As a result of these benefits, there has been an increase in the use of the radial artery for interventional procedures worldwide in the past several years. This experience has led to an understanding of the problems and complications that can result from the transradial approach. The purpose of the present manuscript is to review these issues. Radial artery occlusion. Although this complication is a major concern, the consequences of radial artery occlusion are usually benign. The dual blood supply to the hand is an extremely protective mechanism (Figure 1). Hand ischemia with necrosis has occurred following prolonged cannulation of the radial artery for hemodynamic monitoring in critically ill patients; however, this complication has not been reported thus far after transradial coronary procedures.
The absence of ischemic complications is largely the result of the original recommendation by Kiemeneij that the transradial procedure be performed only in patients with a documented patent ulnar artery and palmar arch.1 This has traditionally been evaluated using the Allen’s test, but ultrasound, Doppler, and plethysmography prior to the procedure are more accurate methods.11
Plethysmography is probably the simplest and most effective method. A pulse oximetry test is performed with the probe placed on the patient’s thumb (Figure 2). The persistence of waveform and high oximetry readings after digital occlusion of the radial artery is very strong evidence that the patient will have sufficient collateral flow to prevent hand ischemia if the radial artery should become occluded as a result of the procedure. Barbeau has demonstrated the reappearance of the waveform and a high oximetry reading two minutes after initial negative results.11 This delayed recruitment of collaterals may be an additional explanation for the absence of hand ischemia with radial occlusion.
Several variables influence the incidence of radial artery occlusion. Adequate anticoagulation is extremely important. This is usually not an issue in patients undergoing interventional procedures, but the incidence of radial occlusion was as high as 30% in patients receiving only 1,000 units of heparin during diagnostic catheterization.12 The incidence of radial occlusion is reduced significantly by administering at least 5,000 units of heparin during the procedure.12,13 Due to this risk of radial occlusion, we tend to reserve the use of the radial artery for interventional procedures and “look-see” diagnostic catheterization. Elective diagnostic catheterizations are performed transradially only when there is an increased risk of femoral complications.
Catheter size has been shown to be an important predictor of post-procedure radial artery occlusion. Saito has studied the ratio of the radial artery internal diameter to the external diameter of the arterial sheath.14 The incidence of occlusion was 4% in patients with a ratio of greater than 1, as compared to 13% in those with a ratio of less than 1. Radial procedures have traditionally been performed using 6 Fr catheters, and most patients have an internal radial artery diameter larger than the 2.52 mm external 6 Fr sheath diameter.14 The incidence of radial occlusion following 6 Fr procedures is less than 5%, but the rate increases with larger sheath sizes.4,13 Virtually all interventional procedures can now be performed through large-bore, 6 Fr guide catheters, and larger-sized catheters are rarely necessary. For straightforward procedures, 5 Fr guide catheters may be utilized and are particularly useful in smaller women.
When the radial artery is utilized for hemodynamic monitoring in critically ill patients, the incidence of radial occlusion is significantly higher in patients with cannulation times greater than 24 hours, as compared to those under 20 hours.15 Since catheters are virtually always removed at the conclusion of a catheterization or interventional procedure, the time of cannulation may not be a factor. However, prolonged post-procedure compression times, particularly with high pressure using a mechanical device, may be a factor. We use sufficient pressure only to achieve hemostasis and try to remove the device as quickly as possible. Even in patients with intensive anticoagulation, it is rarely necessary to maintain mechanical compression for longer than one to two hours. A compression dressing using non-occlusive pressures can then be applied.
In summary, post-procedure radial occlusion occurs only in a small percentage of patients and is virtually always asymptomatic because of the dual blood supply to the hand. Patients with generalized vascular disease, diabetes mellitus, and those undergoing repeat procedures are more susceptible. The incidence can be minimized with appropriate anticoagulation, proper sheath selection, and avoiding prolonged high-pressure compression following the procedure. Non-occlusive radial artery injury. Recent studies have demonstrated that permanent radial artery injury without occlusion may occur following transradial intervention in some patients. Mean radial artery internal diameter as measured by ultrasound was smaller in patients undergoing repeat transradial interventional procedures as compared to the initial procedure.16 This smaller diameter was not present on the day following the procedure, but developed during a mean follow up of 4.5 months. Wakeyama et al. demonstrated with intravascular ultrasound that this progressive narrowing is due to intimal hyperplasia, presumably induced by trauma from the cannulation sheath or catheter.17 The studies in our laboratory show that this hyperplasia is usually segmental rather than diffuse and is not present in all patients with a previous transradial procedure (Figure 3). The incidence of subsequent intimal hyperplasia in patients undergoing radial procedures is yet to be determined.
The ramifications of this injury are important not only in patients undergoing repeat interventional procedures, but also in patients in whom the radial artery may be used as a conduit for coronary artery bypass surgery. At our center, this is not an issue as most procedures are performed from the right radial artery and surgeons use the left radial artery for bypass graft purposes. At present, it would seem prudent not to use a radial artery that previously has been used for a catheterization as a bypass graft. Radial artery spasm. Much of the morbidity of the transradial procedure is related to vasospasm induced by the introduction of a sheath or catheter into the radial artery. The vessel has a prominent medial layer that is largely dominated by alpha-1 adenoreceptor function.18 Thus, increased levels of circulating catecholamines are a cause of radial artery spasm. Local anesthesia and adequate sedation to control anxiety during catheter insertion are important preventative measures.
It has been demonstrated in isolated radial artery ring segments that nitroglycerin and verapamil are effective agents in preventing arterial spasm.19 Indeed, a vasodilator cocktail consisting of 3–6 mg of verapamil injected intra-arterially prior to sheath insertion is extremely effective in preventing radial artery spasm. The effect of the drug is immediate and significant arterial dilatation can be seen within minutes of its administration (Figure 4).
Intra-arterial verapamil and nitroglycerin have virtually eliminated vasospasm as a cause of significant morbidity of the procedure. It is now possible to perform transradial procedures using short sheaths and arm discomfort generally occurs only in patients with very small or tortuous radial arteries, particularly if guide catheter manipulation is excessive.
Spasm distal to the access site may be a cause of access failure. Occasionally, guide wire or guide catheter induced focal spasm may occur in a tortuous segment. Angiographic visualization of these areas is important as they generally respond to repeat verapamil administration and can be traversed with an angled hydrophilic coated guide wire. A soft-tipped coronary guide wire may also be used to cross these areas (Figure 5).
Sheath-induced spasm is also minimized by the use of sheaths with hydrophilic coating. Kiemeneij has documented that both patient discomfort and the force required to remove a sheath as measured by an automatic pull-back device was significantly less with hydrophilic coated sheaths as opposed to non-coated sheaths.20 Local access bleeding. The most important benefit of transradial procedures is the elimination of access site bleeding complications.1–4 The radial artery puncture site is located over bone and can easily be compressed with minimal pressure. Thus, bleeding from the radial access site can virtually always be prevented. Although manual pressure from an experienced operator is the ideal method to obtain hemostasis, several compression devices have been developed in an attempt to maximize operator and staff efficiency. Local hematomas may occur as a result of improper device application or device failure. It is important to emphasize that compression of the radial artery both proximally and distally to the puncture site must be performed because of retrograde flow from the palmar arch collaterals. Forearm hematoma. Bleeding may occur from a site in the radial artery remote from the access site. The most common cause is perforation of a small side branch by the guide wire in patients receiving a platelet glycoprotein IIb/IIIa inhibitor (Figure 6). Avulsion of a small radial recurrent artery arising from a radial loop is another important cause of this syndrome.21,22 Hydrophilic guidewires preferentially select this small arterial remnant in patients with a radial loop and forceful advancement of the guide catheter can result in avulsion of the vessel. Radial artery perforation has been described in 1% of patients although in our experience the incidence is substantially lower. A low threshold to perform a radial artery arteriogram when any resistance to guide wire or catheter insertion is encountered will help prevent this complication.
Recognition of this bleeding remote from the access site is important as hemostatic pressure must be applied to an area other than the access site. Hemostasis is usually easily accomplished by the application of an Ace bandage to the forearm. A blood pressure sphygmomanometer may also be utilized. The latter is inflated to systolic pressure and then gradually released over a period of one to two hours. Sealing of a perforation with a long sheath is also an option, but this is rarely necessary.22
Compartment syndrome is the most dreaded complication of radial artery hemorrhage. A large hematoma causes hand ischemia due to pressure-induced occlusion of both the radial and ulnar arteries. Fasciotomy with hematoma evacuation must be performed as an emergency procedure to prevent chronic ischemic injury. This complication is rare, occurring only once in our early experience; it should always be preventable.
Access failure. Failure to cannulate the radial artery using a 20 gauge needle and a 0.025 mm straight Terumo guide wire occurs in less than 5% of patients with an experienced operator. The importance of adequate patient sedation and local anesthesia in the prevention of radial artery spasm has previously been emphasized. In addition, meticulous attention to detail is important as the probability of failure increases as the number of unsuccessful attempts to puncture the artery increases. It should be emphasized that the puncture site is proximal to the styloid process of the radius bone. The radial artery distally usually bifurcates and becomes less superficial and attempting to puncture the vessel too distally is a common cause of access failure (Figure 7).
The radial loop is the most common congenital anomaly of the radial artery and may be a cause of access failure. It occurs in 1–2% of patients and may be unilateral or bilateral.21 Wide loops can occasionally be traversed with hydrophilic guidewires and 5 Fr catheters without excessive patient discomfort.23 However, in most cases, it is preferable to consider an alternative access site.
Radial arteries that are smaller than 2 mm in diameter are difficult to access. These are generally seen in smaller women and patients with previous radial procedures. The use of a 5 Fr guide in this situation may be an option. However, complex or difficult procedures cannot be performed through a 5 Fr guide catheter. Miscellaneous complications. Pseudoaneurysm formation may rarely occur at the radial artery access site. This is usually easily managed with thrombin injection and/or mechanical compression. However, surgery may be required. Radial artery avulsion due to intense spasm has been described but this complication should virtually never occur using contemporary techniques. Sterile abscesses rarely occur with the use of hydrophilic coated sheaths.24 Conclusion. The radial artery is an excellent access site for coronary interventions. Although technically more challenging with a definite learning curve, there are significant advantages to this approach. Complications are infrequent and many are preventable with careful technique.
Vascular complications after percutaneous coronary intervention following hemostasis with the Mynx vascular closure device versus the AngioSeal vascular closure device.
Department Cardiology, New York Medical College, Macy Pavilion, Valhalla, NY 10595, USA.
Abstract
We investigated the prevalence of vascular complications after PCI following hemostasis in 190 patients (67% men and 33% women, mean age 64 years) treated with the AngioSeal vascular closure device (St. Jude Medical, Austin, Texas) versus 238 patients (67% men and 33% women, mean age 64 years) treated with the Mynx vascular closure device (AccessClosure, Mountain View, California).
RESULTS:
Death, myocardial infarction or stroke occurred in none of the 190 patients (0%) treated with the AngioSeal versus none of 238 patients (0%) treated with the Mynx. Major vascular complications occurred in 4 of 190 patients (2.1%) treated with the AngioSeal versus 5 of 238 patients (2.1%) treated with the Mynx (p not significant). Major vascular complications in patients treated with the AngioSeal included removal of a malfunctioning device (1.1%), hemorrhage requiring intervention (0.5%) and hemorrhage with a loss of > 3g Hgb (0.5%). The major vascular complications in patients treated with the Mynx included retroperitoneal bleeding requiring surgical intervention (0.8%), pseudoaneurysm with surgical repair (0.8%) and hemorrhage with a loss of > 3g Hgb (0.4%). These complications were not significantly different between the two vascular closure devices (p = 0.77). Minor complications included hematoma > 5 cm (0.5%, n = 1) within the AngioSeal group, as well as procedure failure requiring > 30 minutes of manual compression after device deployment, which occurred in 7 out of 190 patients (3.7%) treated with the AngioSeal versus 22 of 238 patients with the Mynx (9.2%) (p = 0.033).
CONCLUSIONS:
Major vascular complications after PCI following hemostasis with vascular closure devices occurred in 2.1% of 190 patients treated with the AngioSeal vascular closure device versus 2.1% of 238 patients treated with the Mynx vascular closure device (p not significant). The Mynx vascular closure device appears to have a higher rate of device failure.
Incications and complications of invasive diagnostic procedures and percutaneous coronary interventions in the year 2003. Results of the quality control registry of the Arbeitsgemeinschaft Leitende Kardiologische Krankenhausarzte (ALKK).
The ALKK registry contains about 20% of the invasive and interventional cardiological procedures performed in Germany.
METHODS:
In 2003 a total of 82,282 consecutive diagnostic invasive and 30,689 interventional procedures from 75 hospitals were centrally collected and analyzed.
RESULTS:
The main indication for an invasive diagnostic procedure was coronary artery disease in 92.5% of cases, myocardial disease in 1.6%, impaired left ventricular function in 4.0%, valve disease in 4% and other indications in 1.9%. An acute coronary syndrome was present in 25% of the patients. The rate of severe complications in patients with a lone diagnostic invasive procedure was low (<0.5%). The indication for percutaneous coronary intervention (n=30,689) was stable angina in 44.1%, ST elevation myocardial infarction in 22.3%, non ST elevation myocardial infarction in 14.8%, unstable angina in 10.0%, silent ischemia in 2.2%, prognostic in 5.2% of patients. The majority of interventions were performed directly after the diagnostic procedure (n=23,887=78.6%). The intervention was successful in 94.6% of cases. Stent implantation was performed in 77.2%, with 1 stent in 88.4%, two stents in 7.6% and 3 or more stents in 3.3%. A drug-eluting stent was implanted in 3.6% of the cases. The complication rate after PCI was influenced by the indication for the intervention. The in-hospital mortality in patients with cardiogenic shock was 33%, while in patients with stable angina, silent ischemia and prognostic indication only 0.2% died.
CONCLUSION:
There is an increase of invasive diagnostic and interventional procedures in patients with acute coronary syndromes, with 47% of PCIs performed in these patient. PCIs were performed in 75% of the cases directly after the diagnostic procedure. The rate of stent implantation seems to have reached a plateau at around 80%, while drug-eluting stents were implanted only in a minority of cases. The complication rate is mainly dependent on the clinical presentation of the patients and the indication for PCI.
1Department of Cardiovascular Medicine, 2Department of Pathology, 3Division of Interventional Cardiology, Toho University Faculty of Medicine, Ohta City, Tokyo, Japan
Abstract: Behçet’s disease is a multisystemic vascular inflammatory disease, but concurrent cardiac diseases, such as acute myocardial infarction, are rare. Several complications may arise after coronary intervention for coronary lesions that interfere with treatment, and the incidence of coronary arterial complications due to invasive therapy remains unclear. Further, the long-term outcomes in patients with Behçet’s disease after stenting for acute myocardial infarction have not been described. The present report describes a 35-year-old Japanese man with Behçet’s disease who developed acute myocardial infarction. A coronary aneurysm developed at the stenting site of the left anterior descending coronary artery, along with stenosis in the left anterior descending segment proximal to the site. Although invasive therapy was considered, medication including immunosuppressants was selected because of the high risk of vascular complications after invasive therapy. The coronary artery disease has remained asymptomatic for the 4 years since the patient started medication. This case underscores the importance of considering the incidence of coronary arterial complications and of conservative treatment when possible.
Marso SP, Amin AP, House JA, et al; on behalf of the National Cardiovascular Data Registry. Association between use of bleeding avoidance strategies and risk of periprocedural bleeding among patients undergoing percutaneous coronary intervention. JAMA. 2010;303(21):2156-2164.
Heart Disease and Stroke Statistics — 2011 Update. American Heart Association, 2011.
Tavris DR, Gallauresi BA, Dey S, Brindis R, Mitchel K. Risk of local adverse events by gender following cardiac catheterization. Pharmacoepidemiol Drug Saf. 2007;16(2):125-131.
Tavris DR, Dey S, Gallauresi B, et al. Risk of local adverse events following cardiac catheterization by hemostasis device use — phase II. J Invasive Cardiol. 2005;17(12):644-650.
An initiative of the American College of Cardiology Foundation, the NCDR, National Cardiovascular Data Registry, is a comprehensive, outcomes-based suite of registries focused on quality improvement. www.ncdr.com.
Applegate RJ, Sacrinty MT, Kutcher MA, et al. Propensity score analysis of vascular complications after diagnostic cardiac catheterization and percutaneous coronary intervention 1998-2003. Catheter Cardiovasc Interv. 2006;67(4):556-562.
Applegate RJ, Sacrinty M, Kutcher MA, et al. Vascular complications with newer generations of Angio-Seal vascular closure devices. J Interv Cardiol. 2006;19(1):67-74.
Applegate RJ, Sacrinty MT, Kutcher MA, et al. Propensity score analysis of vascular complications after diagnostic cardiac catheterization and percutaneous coronary intervention using thrombin hemostatic patch-facilitated manual compression. J Invasive Cardiol. 2007;19(4):164-170.
Sulzbach-Hoke LM, Ratcliffe SJ, Kimmel SE, et al. Predictors of complications following sheath removal with percutaneous coronary intervention. J Cardiovasc Nurs. 2010;25(3):E1-E8.
Legrand V, Doneux P, Martinez C, et al. Femoral access management: comparison between two different vascular closure devices after percutaneous coronary intervention. Acta Cardiol. 2005;60(5):482-488.
Hermiller JB, Simonton C, Hinohara T, et al. The StarClose Vascular Closure System: interventional results from the CLIP study. Catheter Cardiovasc Interv. 2006;68(5):677-683.
Martin JL, Pratsos A, Magargee E, et al. A randomized trial comparing compression, Perclose Proglide and Angio-Seal VIP for arterial closure following percutaneous coronary intervention: the CAP trial. Catheter Cardiovasc Interv. 2008;71(1):1-5.
Deuling JH, Vermeulen RP, Anthonio RA, et al. Closure of the femoral artery after cardiac catheterization: a comparison of Angio-Seal, StarClose, and manual compression. Catheter Cardiovasc Interv. 2008;71(4):518-523.
Wong SC, Bachinsky W, Cambier P, et al; ECLIPSE Trial Investigators. A randomized comparison of a novel bioabsorbable vascular closure device versus manual compression in the achievement of hemostasis after percutaneous femoral procedures: the ECLIPSE (Ensure’s Vascular Closure Device Speeds Hemostasis Trial). JACC Cardiovasc Interv. 2009;2(8):785-793.
Arora N, Matheny ME, Sepke C, Resnic FS. A propensity analysis of the risk of vascular complications after cardiac catheterization procedures with the use of vascular closure devices. Am Heart J. 2007;153(4):606-611.
Castillo-Sang M, Tsang AW, Almaroof B, et al. Femoral artery complications after cardiac catheterization: a study of patient profile. Ann Vasc Surg. 2010;24(3):328-335.
Sanborn TA, Ebrahimi R, Manoukian SV, et al. Impact of femoral vascular closure devices and antithrombotic therapy on access site bleeding in acute coronary syndromes: the Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trial. Circ Cardiovasc Interv. 2010;3(1):57-62.
Iqtidar AF, Li D, Mather J, McKay RG. Propensity matched analysis of bleeding and vascular complications associated with vascular closure devices vs standard manual compression following percutaneous coronary intervention. Conn Med. 2011;75(1):5-10.
Marso SP, Amin AP, House JA, et al; National Cardiovascular Data Registry. Association between use of bleeding avoidance strategies and risk of periprocedural bleeding among patients undergoing percutaneous coronary intervention. JAMA. 2010;303(21):2156-2164.
Ahmed B, Piper WD, Malenka D, et al. Significantly improved vascular complications among women undergoing percutaneous coronary intervention: a report from the Northern New England Percutaneous Coronary Intervention Registry. Circ Cardiovasc Interv. 2009;2(5):423-429.
Trimarchi S, Smith DE, Share D, et al; BMC2 Registry. Retroperitoneal hematoma after percutaneous coronary intervention: prevalence, risk factors, management, outcomes, and predictors of mortality: a report from the BMC2 (Blue Cross Blue Shield of Michigan Cardiovascular Consortium) registry. JACC Cardiovasc Interv. 2010;3(8):845-850.
Vaitkus PT. A meta-analysis of percutaneous vascular closure devices after diagnostic catheterization and percutaneous coronary intervention. J Invasive Cardiol. 2004;16(5):243-246.
Koreny M, Riedmuller E, Nikfardjam M, et al. Arterial puncture closing devices compared with standard manual compression after cardiac catheterization — systematic review and meta-analysis. JAMA. 2004;291(3):350-357.
Nikolsky E, Mehran R, Halkin A, et al. Vascular complications associated with arteriotomy closure devices in patients undergoing percutaneous coronary procedures: a meta-analysis. J Am Coll Cardiol. 2004;44(6):1200-1209.
Biancari F, D’Andrea V, Di Marco C, et al. Meta-analysis of randomized trials on the efficacy of vascular closure devices after diagnostic angiography and angioplasty. Am Heart J. 2010;159(4):518-531.
Tavris DR, Dey S, Gallauresi B, et al. Risk of local adverse events following cardiac catheterization by hemostasis device use — phase II. J Invasive Cardiol. 2005;17(12): 644-650.
Frequency and Costs of Ischemic and Bleeding Complications After Percutaneous Coronary Interventions: Rationale for New Antithrombotic Therapy
Recent advances in catheter technology and antithrombotic therapy have led to a continuous improvement in outcomes of percutaneous coronary intervention (PCI). These improved outcomes have been associated with broadening of the indications for PCI, with an exponential growth in number of procedures performed, but they have also been paralleled by incremental procedure costs. The estimated costs of PCI currently range from $8,000–$13,000.1 With over 800,000 cases performed each year in the United States (US) alone, this represents over $10 billion annually for the US Healthcare System.2 Roughly half of these costs are incurred by the Center for Medicare and Medicaid Services (CMS, formerly known as the Health Care Financing Administration).3 Total costs of PCI include disposable equipment used during the procedure (balloons, catheters, stents, etc.), cardiac catheterization laboratory overhead and depreciation, nursing and pharmacy costs, laboratory costs and physician services. In addition, factors that have been found to be associated with increased PCI costs include the use of special devices such as atherectomy or vascular closure devices, the use of multiple stents, the use of platelet glycoprotein (GP) IIb/IIIa inhibitors, and the presence of certain patient demographic characteristics including advanced age, gender and other comorbidities.1,4,5 Finally, complications related to the procedure have been identified in several studies as the single most significant contributor to increased costs of PC.5–7
Methods to reduce the cost of PCI include re-use of balloon catheters,8 percutaneous revascularization performed at the same time as diagnostic catheterization,9 reduced anticoagulation, the use of new devices or pharmacological interventions to reduce restenosis and complications, and the use of competitive bidding for cardiac cath lab supplies.10 For example, the evolution of anticoagulation therapy in stented patients from a regime of post-procedural heparin and warfarin to one of thienopyridines and aspirin,11 and the subsequent reduction of length of stay from 4 days in 1995 to 2 days in 2000, have helped keep total procedure costs down.12 In addition, a reduction in complication rates appears to be a key target for cost reduction efforts. In support of this statement, in the economic assessment of the Evaluation of 7E3 for the Prevention of Ischemic Complications (EPIC) trial in high-risk patients, Mark et al. identified bleeding complications, urgent and non-urgent coronary artery bypass graft surgery (CABG), and urgent and non-urgent percutaneous transluminal coronary angioplasty (PTCA) as important correlates of incremental costs.7 Unfortunately, standard aggressive antithrombotic therapy aimed toward a reduction of ischemic complications is often associated with an increase in bleeding complications. In the analysis of the EPIC trial, the benefits of abciximab in decreasing procedure costs through a reduction of ischemic complications were offset by drug acquisition costs and by an increase in bleeding complications.7 Thus, with ischemic complications becoming more rare as a result of improvement in PCI technology and more aggressive antithrombotic therapy, bleeding has become a rather common and costly complication of PCI, with a blood transfusion estimated to add up to $8,000 to the cost of care for the PCI patient.13
Based on these premises, it appears that the next challenge in the care of PCI patients will be to determine how to continue to prevent ischemic complications without increasing the risk of bleeding. This paper examines the frequency of PCI complications in both recent clinical trials and actual practice, discusses the costs of complications, and explores improvements in patient management and particularly changes in anticoagulation therapy that might impact total costs of PCI.
Complication rates in clinical trials
Ischemic complications in clinical trials. Despite advances in PCI technology and adjunctive pharmacotherapy, data from clinical trials indicate that ischemic complications still occur in 5–15% of patients.14–19 Typically, clinical trials define ischemic complications as a combination of death, myocardial infarction (MI; both Q-wave and non-Q wave) and either urgent or any target vessel revascularization (TVR). Different definitions of MI or revascularization can make comparisons across trials difficult. However, comparisons may still be possible through the application of strict meta-analysis methodology. A recent meta-analysis combined data from 6 double-blind PCI trials conducted predominantly in North America between 1993 and 1998.20 A total of 16,546 patients were enrolled in these trials (Table 1). Protocols and case report forms for trials included in the analysis were compared to ensure reasonable consistency of study methods, patient management, data reporting and data structure. Integration of the databases from the trials enabled a direct comparison of key event rates at 7 days, using standard classifications and criteria for severity. The meta-analysis showed that the use of high-dose heparin (175 U/kg) was associated with significantly less frequent clinical ischemic events (8.1%) than lower doses of heparin (100 U/kg; 10.3%). In this same meta-analysis, event rates in patients treated with low-dose heparin (70 U/kg) plus a GP IIb/IIIa inhibitor was 6.5%.20 Although not included in this meta-analysis, it is worth noting that the incidence of death, MI and revascularization in the ESPRIT trial was 9.3% in patients treated with low-dose heparin alone (60 U/kg).21
Bleeding complications in clinical trials. In clinical trials of antiplatelet and anti-thrombotic therapy in PCI, bleeding complications are generally defined using either thrombolysis in myocardial infarction (TIMI)22 or global utilization of streptokinase or tPA outcomes (GUSTO)23 criteria (Table 2). Rates of major bleeding in clinical trials using these criteria are generally less than 2% (Table 3).14–19,21,24,25 However, these restrictive definitions may not capture all clinically significant bleeding. For example, neither the TIMI nor the GUSTO major bleeding definition includes the need for a blood transfusion as part of the criteria. Thus, a broader measure of bleeding using a combination of both major and minor bleeding defined by TIMI or GUSTO criteria appears more likely to be representative of bleeding rates in clinical practice.
In the meta-analysis of contemporary PCI trials, TIMI criteria were used to classify hemorrhagic events, permitting direct comparisons between trials. In the high-dose heparin group, the combination of TIMI major and minor bleeding occurred in 10.5% of patients compared with a rate of 10.7% in the low-dose heparin group, while the bleeding rate was 14.3% in patients receiving a combination of GP IIb/IIIa inhibitors and low-dose heparin.
As shown in Table 3, when both TIMI major and minor bleeding are combined in contemporary PCI trials, bleeding complications average 4–14%, depending on patient characteristics and the drug regime used. In addition, when transfusions are included in the definition, the frequency of bleeding complications increases substantially. For example, in NICE-3, bleeding complications were 10.5% when transfusions were included in the criteria, but only 2% of the patients experienced TIMI major bleeding.26
Notably, the only adjunctive anti-thrombotic agent shown to reduce both ischemic and bleeding complications in PCI is bivalirudin. In the Bivalirudin Angioplasty Trial,27 the risk of bleeding was decreased 62% in the bivalirudin group compared with high-dose heparin. The combined rate of TIMI major and TIMI minor bleeding in bivalirudin patients (n = 2,161) was found to be 4.3% in the meta-analysis of contemporary PCI trials with a corresponding ischemic event rate of 6.6%.20
Complications in practice
Ischemic complications in practice. Rates of ischemic complications in clinical practice are difficult to determine. Although several investigators have published data from multicenter databases, these data tend to be 3–5 years old by the time manuscripts are in print. Since trends in the published literature do show continued reduction in PCI complications over time, the frequency of complications noted in these publications may overestimate the actual rate of complications in clinical practice today. In addition, rates of complications can vary widely across institutions due to differences in practice patterns, definitions, operator skills and resource utilization. For example, in the Society for Cardiac Angiography and Interventions (SCA&I) registry, stent use among laboratories varied from 29–95%.28 Others have found lower complication rates in patients whose procedure was performed by a high-volume operator or in a high-volume institution.29 We identified 6 published reports of PCI complications in clinical practice reporting a variety of ischemic outcomes.1,28–31
Saucedo et al. prospectively collected data on 900 patients undergoing successful elective stent placement in native coronary arteries between January 1994 and December 1995.30 The purpose of this study was to evaluate the incidence and long-term clinical consequences of patients with creatine kinase (CK) myocardial isoenzyme band (CK-MB) elevations after stenting. By design, all patients in this observational study had a successful procedure defined as an increase of > 20% in luminal diameter with final percent diameter stenosis of < 50%, without the occurrence of any major complications (death, Q-wave MI and CABG). Nevertheless, 26.4% of patients had CK-MB elevations 1–5 times the upper limit of normal (ULN) and 8.5% had CK-MB elevations > 5 times ULN. In total, 3.9% of patients required a repeat diagnostic catheterization for recurrent ischemia and 1.2% required urgent target vessel revascularization. In this study, patients requiring the use of GP IIb/IIIa inhibitors were excluded.
The Northern New England group (NNE) collected data on 14,498 patients undergoing PCI between 1994 and 1996.29 In this study, outcomes included the in-hospital occurrence of death; emergency CABG (eCABG) or non-eCABG; or new MI (defined as chest pain, diaphoresis, dyspnea or hypotension associated with the development of new Q-waves or ST-T wave changes and a rise in CK to at least twice normal with a positive CK-MB). Overall, death occurred in 1.2% of patients, CABG in 2.6% (0.8% eCABG and 1.8% non-eCABG), and MI in 2%. Stents were used in 22% of patients enrolled in this registry.
In the National Cardiovascular Network database (NCN), Batchelor et al. reported complications of PCI in 109,708 patients who underwent PCI between 1994 and 1997.31 In this observational study, in-hospital mortality was defined as the occurrence of death after the procedure, MI was defined as the appearance of new Q-waves in 2 contiguous leads on a 12-lead electrocardiogram (ECG) for up to 30 days post-PCI, and repeat revascularization was defined as the need for CABG or additional PCI prior to discharge. In this study, death occurred in 1.3% of patients, Q-wave MI in 1.4% and repeat revascularization in 4.5%. Half of the patients underwent stenting in this study. Notably, this database did not record myocardial enzymes or the use of GP IIb/IIIa inhibitors.
Aronow and colleagues observed outcomes in a cohort of consecutive registry patients undergoing coronary stent placement between 1995 and 1997.32 A total of 373 patients underwent PCI during this time period, with death occurring in 9 patients (2.4%), CABG in 3 (0.8%) and MI in 19 (5.1%, including both QWMI and NQWMI). Repeat diagnostic catheterization was performed in 3.2% of patients and repeat PCI in 0.8%.
The SCA&I registry evaluated outcomes in 16,811 patients undergoing either balloon angioplasty (n = 6,121) or stenting (n = 10,690) between July 1996 and December 1998.28 In this observational analysis, 12.9% of patients received a GP IIb/IIIa inhibitor, 87% of patients enrolled in the database underwent PCI between 1997 and 1998, and 60% of the stent patients were enrolled in 1998. Outcomes reported included in-hospital death (occurring at any time during the hospitalization) and eCABG, defined as CABG occurring immediately after PCI. Death occurred in 0.4% of patients and eCABG in 0.5%.
Finally, Cohen and others recorded in-laboratory complications in 26,421 patients at 70 different centers undergoing PCI in 1998.1 In-laboratory complications were rare, with death occurring in 0.17%, cardiac arrest in 0.32%, stroke in 0.03%, ventricular fibrillation or tachycardia in 0.94%, abrupt closure in 0.71%, and eCABG in 0.53%. Overall, 72% of patients received stents and 20% received GP IIb/IIIa inhibitors.
In addition to published reports of PCI complications, data from unpublished sources can be used to determine outcomes in a more contemporary cohort of patients undergoing PCI.33 The MQ-Profile (MQ-Pro) Database [Cardinal Information Corporation (CIC), Marlborough, Massachusetts] is maintained by CIC, which sells and distributes software to US acute-care hospitals for the collection of detailed clinical and administrative data. Data from 5,373 PCI procedures performed between July 1, 1998 and June 30, 1999 were obtained from the database using International Classification of Diseases 9th Edition (ICD-9) procedure codes for PCI (36.01, 36.02, 36.05). Demographic, clinical and economic data were collected on each patient using a combination of database retrieval and chart review. In this analysis, death was defined as discharge disposition of “deceased”, MI as the presence of ECG changes consistent with MI (new Q-waves or ST-segment changes) or an increase in CK-MB of at least 2 times the testing facility’s ULN. CABG was identified by the presence of ICD-9 procedure code 36.1 and repeat PCI by either code 36.01, 36.02, or 36.05. Failed PCI was defined by the term “failed PTCA” in chart notes (for patients without a previous history of PCI) and recurrent ischemia documented by ECG changes. Death occurred in 2.0% of patients, MI in 3.1%, CABG in 1.3% and repeat PCI in 5.5%. Translated into a combined endpoint similar to those used in clinical trials, the rate of death/MI/revascularization was 11.9%.
Data from these published and unpublished observations of contemporary PCI practice indicate that while in-laboratory ischemic complications are exceedingly rare, in-hospital ischemic complications still occur in a substantial number of patients. Using an approximation of outcomes from these published and unpublished reports, mortality averages 1%, Q-wave MI occurs in 2% of patients, NQWMI in 6%, CABG in 2% and repeat PCI occurs in 3–5% of patients. It is important to underscore that although most deaths following PCI are due to underlying comorbidities (i.e., acute MI, cardiogenic shock, etc.) rather than to the procedure itself, few deaths still occur as a complication of the procedure.34,35 Extrapolated to the estimated PCI population of 800,000 cases per year, then 8,000 people will die and 64,000 will experience an MI. In addition, approximately 16,000 will require CABG and as many as 40,000 will need a repeat PCI before hospital discharge.
From the John P. Robarts Research Institute (M.P., M.E., L.J.K., J.W.F., H.J.M.B) and the Departments of Epidemiology and Biostatistics (M.E.) and Clinical Neurological Sciences (M.E., G.G.F., H.J.M.B.), University of Western Ontario, London, Ontario, Canada.
Correspondence to Dr H.J.M. Barnett, John P. Robarts Research Institute, PO Box 5015, 100 Perth Dr, London, ON N6A 5K8, Canada. E-mail barnett@rri.on.ca
Abstract
Background and Purpose—Carotid endarterectomy (CE) has been shown to be beneficial in patients with symptomatic high-grade (70% to 99%) internal carotid artery stenosis. To achieve this benefit, complications must be kept to a minimum. Complications not associated with the procedure itself, but related to medical conditions, have received little attention.
Methods—Medical complications that occurred within 30 days after CE were recorded in 1415 patients with symptomatic stenosis (30% to 99%) of the internal carotid artery. They were compared with 1433 patients who received medical care alone. All patients were in the North American Symptomatic Carotid Endarterectomy Trial (NASCET).
Results—One hundred fifteen patients (8.1%) had 142 medical complications: 14 (1%) myocardial infarctions, 101 (7.1%) other cardiovascular disorders, 11 (0.8%) respiratory complications, 6 (0.4%) transient confusions, and 10 (0.7%) other complications. Of the 142 complications, 69.7% were of short duration, and only 26.8% prolonged hospitalization. Five patients died: 3 from myocardial infarction and 2 suddenly. Medically treated patients experienced similar complications with one third the frequency. Endarterectomy was ≈1.5 times more likely to trigger medical complications in patients with a history of myocardial infarction, angina, or hypertension (P<0.05).
Conclusions—Perioperative medical complications were observed in slightly fewer than 1 of every 10 patients who underwent CE. The majority of these complications completely resolved. Most complications were cardiovascular and occurred in patients with 1 or more cardiovascular risk factors. In this selected population, the occurrence of perioperative myocardial infarction was uncommon.
The North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the European Carotid Endarterectomy Trial showed unequivocal benefit of carotid endarterectomy (CE) in symptomatic patients with high-grade internal carotid artery (ICA) stenosis (70% to 99%).12 The parallel study dealing with symptomatic patients with moderate-grade stenosis (30% to 69%) showed benefits of CE only in a carefully selected group of patients.3 Currently, CE is the most common elective peripheral vascular procedure, which in 1997 was performed in ≈130 000 patients in the United States.4
Despite benefit in the long term, CE may cause complications either by the operation itself or by concomitant medical conditions. The challenge for the future is to reduce the perioperative risk as much as possible. The incidence and type of complications that are directly related to the surgical procedure have been the subject of many reports,5678910 whereas medical complications that are not directly caused by the procedure have received less attention. The aim of the present study is to describe the incidence and type of medical complications that occurred in patients randomized into NASCET and to determine their association with baseline risk factors.
Subjects and Methods
The methods of the NASCET have been described in detail elsewhere.111 Briefly, NASCET was a randomized clinical trial designed to compare the benefit of best medical therapy alone with best medical therapy plus CE in patients with recent transient or nondisabling neurological deficit caused by cerebral or retinal ischemia in the territory of the ICA. Among the exclusions were patients with recent history (6 months) of myocardial infarction, unstable angina pectoris, atrial fibrillation, recent congestive heart failure, and valvular heart disease. For inclusion, the ICA had to have a 30% to 99% stenosis as assessed by selective carotid angiography and to be technically suitable for CE. Baseline evaluations included a detailed medical history and complete physical and neurological examination.
Surgeons were invited to join NASCET if the center had a documented CE stroke and death rate of ≤6% in a minimum of 50 consecutive cases over a 2-year period. Surgery was completed at the earliest opportunity after randomization, and patients underwent a second complete physical and neurological examination 30 days after surgery. All medical and surgical complications that caused transient or permanent disability within the 30-day period were recorded.
Medical complications consisted of myocardial infarction (based on ECG and cardiac enzyme changes), arrhythmia (requiring antiarrhythmic medication), congestive heart failure, angina pectoris, hypertension (diastolic blood pressure >100 mm Hg requiring intravenous medication), hypotension (systolic pressure <90 mm Hg requiring administration of vasopressor agent), sudden death, respiratory problems (pneumonia, atelectasis, pulmonary edema, or exacerbation of chronic obstructive pulmonary disease), renal failure (doubling of preoperative urea and/or creatinine), depression, and confusion (requiring restraint). Complications were considered mild if they were transient and did not prolong hospital stay, moderate if they were transient but caused delay in hospital discharge, and severe if they were associated with permanent disability or death.
In the present study, patients were excluded from the analyses if they had serious complications that were directly attributable to the surgical procedure, such as those due to anesthesia, thrombosis at the operative site, wound hematomas requiring surgical intervention, or deficits from a vagus nerve injury interfering with swallowing. These surgical complications are described in detail elsewhere.12 For comparative purposes, a list of complications that occurred in the medically treated arm of NASCET was compiled for the 32-day period after randomization (ie, the 30-day period plus the average 2 days that lapsed from randomization to CE in the surgical arm). In both the surgical and medical arms, patients were censored at the time of a stroke, since the subsequent medical complications are commonly the result of the stroke.
Cox proportional hazards regression modeling was used to identify baseline factors that increased the risk of perioperative medical complications. Adjusted hazard rates and adjusted hazard ratios were used to summarize the results. The estimated hazard ratio (or relative hazard) is a measure of association that can be interpreted as a relative risk. Hazard ratios with corresponding probability value of <0.05 were considered statistically significant. Adjusted hazard rates were obtained from the regression model by using the mean value for a factor being adjusted.
The modeling strategy consisted of initially fitting a “full” model, which included all factors. A “final” model was determined by eliminating all factors that were not significantly predictive of the medical complications, using a backward selection approach. The “change-in-estimate” strategy was used to determine whether the remaining factors in the final model were independent risk factors. A factor was considered an independent risk factor if the change in hazard ratios between the full and final models was <10%.
Results
A total of 1436 eligible patients were randomized to the surgical arm and 1449 to the medical arm of the NASCET. In the surgical arm, 21 patients were not operated on for various reasons.12 In the medical arm 16 patients crossed over to surgical therapy within 30 days, leaving 1433 patients for analysis. CE was performed in 1415 patients (328 patients with severe stenosis and 1087 with moderate stenosis). Of the 1415, 59 (4.2%) patients had serious surgical complications that excluded them from further analyses, and 115 (8.1%) had medical complications (Table 1⇓). Of the 142 complications, 69.7% were mild, 26.8% were moderate, and 3.5% were severe. Twenty patients had ≥2 complications. No patient had pulmonary embolus, renal failure, or depression requiring medication. Cardiovascular disorders were >4 times as common as all other conditions combined. All 5 severe complications were fatal and were caused by cardiovascular disorders: 3 patients had fatal myocardial infarction, and 2 patients died suddenly. Of the patients with fatal myocardial infarction, 2 patients had massive myocardial infarctions on the day of surgery. In the other patient, CE was prolonged (7 hours) because of intraoperative occlusion of the ICA. Twenty-four hours after CE, the patient had a myocardial infarction followed by cardiac arrest, leaving the patient in a vegetative state. The patient died 2 months later. Two patients died suddenly on days 3 and 6 after CE, and both had a history of previous myocardial infarction. All patients with fatal medical complications were male, and all had multiple cardiovascular risk factors.
North American Symptomatic Carotid Endarterectomy Trial (NASCET). Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325:445–453.
European Carotid Surgery Trialists’ Collaborative Group. MRC European Carotid Surgery Trial: interim results for symptomatic patients with severe (70–99%) or with mild (0–29%) carotid stenosis. Lancet. 1991;337:1235–1243.
Barnett HJM, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, Rankin RN, Clagett GP, Hachinski VC, Sackett DL, Thorpe KE, Meldrum HE, for the North American Symptomatic Carotid Endarterectomy Trial Collaborators. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. N Engl J Med. 1998;339:1415–1425.
Kozak LJ, Owings MF. Ambulatory and inpatient procedures in the United States, 1995. National Center for Health Statistics. Vital Health Stat 13. 1998;135:1–116.
Hertzer NR. Early complications of carotid endarterectomy: incidence, diagnosis, and management. In: Moore WS, ed. Surgery for Cerebrovascular Disease. Philadelphia, Pa: WB Saunders Co; 1996:625–649.
Young B, Moore WS, Robertson JT, Toole JF, Ernst CB, Cohen SN, Broderick JP, Dempsey RJ, Hosking JD. An analysis of perioperative surgical mortality and morbidity in the Asymptomatic Carotid Atherosclerosis Study. Stroke.1996;27:2216–2224.
Rothwell PM, Slattery J, Warlow CP. Clinical and angiographic predictors of stroke and death from carotid endarterectomy: systemic review. BMJ.1997;315:1571–1517.
North American Symptomatic Carotid Endarterectomy Trial (NASCET) Steering Committee. North American Symptomatic Carotid Endarterectomy Trial: methods, patient characteristics, and progress. Stroke. 1991;22:711–720.
Ferguson GG, Barnett HJM, Eliasziw M, Finan JW, Clagett GP, Barnes R, Barr H, Wallace C, for the North American Symptomatic Carotid Endarterectomy Trial (NASCET) Collaborators. North American Symptomatic Carotid Endarterectomy Trial (NASCET): surgical results in 1415 patients. Stroke. In press.
Adams HP Jr, Brott TG, Crowell RM, Furlan AJ, Gomez CR, Grotta J, Helgason CM, Marler JR, Woolson RF, Zivin JA, Feinberg W, Mayberg M. Guidelines for the management of patients with acute ischemic stroke: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 1994;25:1901–1914.
Feinberg WM, Albers GW, Barnett HJ, Biller J, Caplan LR, Carter LP, Hart RG, Hobson RW II, Kronmal RA, Moore WS, Robertson JT, Adams HP, Mayberg M. Guidelines for the management of transient ischemic attacks: from the Ad Hoc Committee on Guidelines for the Management of Transient Ischemic Attacks of the Stroke Council of the American Heart Association. Circulation. 1994;89:2950–2965.
Wong JH, Findlay JM, Suarez-Almazor ME. Regional performance of carotid endarterectomy: appropriateness, outcomes, and risk factors for complications.Stroke. 1997;28:891–898.
Holton P, Wood JB. The effect of bilateral removal of the carotid bodies and denervation of the carotid sinuses in two human subjects. J Physiol (Lond).1965;181:365–378.
Eliasziw M, Spence JD, Barnett HJM. Carotid endarterectomy does not affect long-term blood pressure: observations from the NASCET. Cerebrovasc Dis.1998;8:20–24.
Solomon RA, Loftus CM, Quest DO, Correll JW. Incidence and etiology if intracerebral hemorrhage following carotid endarterectomy. J Neurosurg.1986;64:29–34.
Hafner DH, Smith RB, King OW, Perdue GD, Stewart MT, Rosenthal D, Jordan WD. Massive intracerebral hemorrhage following carotid endarterectomy. Arch Surg.1987;122:305–307.
Section of Vascular and Endovascular Surgery, Boston University Medical Center, Boston, MA, USA. Alik.Farber@bmc.org
Abstract
OBJECTIVE:
Although dextran has been theorized to diminish the risk of stroke associated with carotid endarterectomy (CEA), variation exists in its use. We evaluated outcomes of dextran use in patients undergoing CEA to clarify its utility.
METHODS:
We studied all primary CEAs performed by 89 surgeons within the Vascular Study Group of New England database (2003-2010). Patients were stratified by intraoperative dextran use. Outcomes included perioperative death, stroke, myocardial infarction (MI), and congestive heart failure (CHF). Group and propensity score matching was performed for risk-adjusted comparisons, and multivariable logistic and gamma regressions were used to examine associations between dextran use and outcomes.
RESULTS:
There were 6641 CEAs performed, with dextran used in 334 procedures (5%). Dextran-treated and untreated patients were similar in age (70 years) and symptomatic status (25%). Clinical differences between the cohorts were eliminated by statistical adjustment. In crude, group-matched, and propensity-matched analyses, the stroke/death rate was similar for the two cohorts (1.2%). Dextran-treated patients were more likely to suffer postoperative MI (crude: 2.4% vs 1.0%; P = .03; group-matched: 2.4% vs 0.6%; P = .01; propensity-matched: 2.4% vs 0.5%; P = .003) and CHF (2.1% vs 0.6%; P = .01; 2.1% vs 0.5%; P = .01; 2.1% vs 0.2%; P < .001). In multivariable analysis of the crude sample, dextran was associated with a higher risk of postoperative MI (odds ratio, 3.52; 95% confidence interval, 1.62-7.64) and CHF (odds ratio, 5.71; 95% confidence interval, 2.35-13.89).
CONCLUSIONS:
Dextran use was not associated with lower perioperative stroke but was associated with higher rates of MI and CHF. Taken together, our findings suggest limited clinical utility for routine use of intraoperative dextran during CEA.
Section of Vascular Surgery Dartmouth-Hitchcock Medical Center, Lebanon, NH 03765, USA. philip.goodney@hitchcock.org
Abstract
OBJECTIVE:
This study investigated risk factors for stroke or death after carotid endarterectomy (CEA) among hospitals of varying type and size participating in a regional quality improvement effort.
METHODS:
We reviewed 2714 patients undergoing 3092 primary CEAs (excluding combined procedures or redo CEA) at 11 hospitals in Northern New England from January 2003 through December 2007. Hospitals varied in size (25 to 615 beds) and comprised community and teaching hospitals. Fifty surgeons reported results to the database. Trained research personnel prospectively collected >70 demographic and clinical variables for each patient. Multivariate logistic regression models were used to generate odds ratios (ORs) and prediction models for the 30-day postoperative stroke or death rate.
RESULTS:
Across 3092 CEAs, there were 38 minor strokes, 14 major strokes, and eight deaths (5 stroke-related) < or =30 days of the index procedure (30-day stroke or death rate, 1.8%). In multivariate analyses, emergency CEA (OR, 7.0; 95% confidence interval [CI], 1.8-26.9; P = .004), contralateral internal carotid artery occlusion (OR, 2.8; 95% CI, 1.3-6.2; P = .009), preoperative ipsilateral cortical stroke (OR, 2.4; 95% CI, 1.1-5.1; P = .02), congestive heart failure (OR, 1.6; 95% CI, 1.1-2.4, P = .03), and age >70 (OR, 1.3; 95% CI, 0.8-2.3; P = .315) were associated with postoperative stroke or death. Preoperative antiplatelet therapy was protective (OR, 0.4; 95% CI, 0.2-0.9; P = .02). Risk of stroke or death varied from <1% in patients with no risk factors to nearly 5% with patients with > or =3 risk factors. Our risk prediction model had excellent correlation with observed results (r = 0.96) and reasonable discriminative ability (area under receiver operating characteristic curve, 0.71). Risks varied from <1% in asymptomatic patients with no risk factors to nearly 4% in patients with contralateral internal carotid artery occlusion (OR, 3.2; 95% CI, 1.3-8.1; P = .01) and age >70 (OR, 2.9; 95% CI, 1.0-4.9, P = .05). Two hospitals performed significantly better than expected. These differences were not attributable to surgeon or hospital volume.
CONCLUSION:
Surgeons can “risk-stratify” preoperative patients by considering the variables (emergency procedure, contralateral internal carotid artery occlusion, preoperative ipsilateral cortical stroke, congestive heart failure, and age), reducing risk with antiplatelet agents, and informing patients more precisely about their risk of stroke or death after CEA. Risk prediction models can also be used to compare risk-adjusted outcomes between centers, identify best practices, and hopefully, improve overall results.
The patient with sepsis has severely altered physiology in a number of ways, which can influence cardiac function. Firstly, there is a
Loss of intravascular volume due to excessive third space loss that results in a decrease in preload. Systemic vascular resistance is decreased which results in a fall in afterload. In addition,
end diastolic volumes often increase and
ejection fraction falls. However, many of these changes are overcome by an
increase in heart rate that may result in an increase in cardiac output. However, it should be remembered that even in the presence of high cardiac outputs it is usually always possible to demonstrate
ventricular dysfunction in patients with sepsis. Echocardiographic studies consistently confirm that there is decreased left ventricular systolic function in humans with sepsis.
In addition, there have been many studies in animals and a few in humans which have confirmed the presence of
diastolic dysfunction – particularly in those patients that go on to die from sepsis.
In the presence of adequate fluid resuscitation there is an increase in end diastolic volume and this is probably a normal response to a decrease in contractility. However, in the non-survivors of sepsis there is a normal or low end diastolic volume that is the result of a decrease in ventricular diastolic compliance. Thus, there is a decreased end diastolic volume at the same filling pressure.
During sepsis, a
decrease in contractility results in a shift to the right of the end-systolic pressure / volume curve and if this is not compensated for results in a
a decrease in stroke volume and cardiac output.
When patients with sepsis are appropriately fluid resuscitated there is an
increase in end diastolic pressure that increases stroke volume. In addition, the
decrease in afterload will also increase stroke volume and will prevent a decrease in ejection fraction.
Alas, because there is a decrease in systolic contractility it would be expected that there would also be a decrease in diastolic stiffness which would allow cardiac output to be maintained despite the relatively low filling pressures. However, if this diastolic compliance change does not occur (as in the nonsurvivors of sepsis) then it is apparent that the ability of the ventricle to generate a stroke volume is impaired at both ends of the curve.
The cause of the altered cardiac function in sepsis remains unknown although there are many theoretical explanations. Clearly, one of the most important mechanisms which can be readily corrected is hypovolaemia.
Myocardial oedema may contribute to a decrease in contractility.
Increased circulating catecholamines can result in a decrease in diastolic compliance, particularly important since these agents are often used to improve myocardial contractility.
Increased intrathoracic pressure caused by positive pressure ventilation can also result in decreased diastolic compliance. In addition, many of the
mediators of the inflammatory response, including products of activated endothelial cells and polymorphonuclear leucocytes (e.g. nitric oxide, tumour necrosis factor and interleukins 1 and 2) have all been postulated as negative inotropes and negative lusitropes.
Another, as yet, unidentified agent which is believed to be released from the splanchnic bed –
myocardial depressant factor – is postulated to play a role.
Treatments aimed at correcting the effects of these various inflammatory mediators may be eventually found but until these approaches have been proven to be beneficial the septic patient will continue to be managed according to the physiological principles outlined by Starling.
From the Department of Medicine (M.W.M.), Division of Cardiology, Pulmonary Diseases and Vascular Medicine and the Institute of Molecular Cardiovascular Research (IMCAR) at the University Hospital (C.W.), RWTH Aachen University, Aachen, Germany.
Correspondence to Marc W. Merx, MD, Medizinische Klinik I, Universitätsklinikum der RWTH Aachen, Pauwelstraße 30, 52057 Aachen, Germany (e-mailmmerx@ukaachen.de), or Christian Weber, MD, Institut für Kardiovaskuläre Molekularbiologie, Universitätsklinikum der RWTH Aachen, Pauwelstraße 30, 52057 Aachen, Germany (e-mail cweber@ukaachen.de).
Sepsis is generally viewed as a disease aggravated by an inappropriate immune response encountered in the afflicted individual. As an important organ system frequently compromised by sepsis and always affected by septic shock, the cardiovascular system and its dysfunction during sepsishave been studied in clinical and basic research for more than 5 decades. Although a number of mediators and pathways have been shown to be associated with myocardial depression in sepsis, the precise cause remains unclear to date. There is currently no evidence supporting global ischemia as an underlying cause of myocardial dysfunction in sepsis; however, in septic patients with coexistent and possibly undiagnosed coronary artery disease, regional myocardial ischemia or infarction secondary to coronary artery disease may certainly occur.
A circulating myocardial depressant factor in septic shock has long been proposed, and potential candidates for a myocardial depressant factor include
cytokines,
prostanoids, and
nitric oxide, among others.
Endothelial activation and
induction of the coagulatory system also contribute to the pathophysiology in sepsis.
Prompt and adequate antibiotic therapy accompanied by surgical removal of the infectious focus, if indicated and feasible, is the mainstay and also the only strictly causal line of therapy. In the presence of severe sepsis and septic shock, supportive treatment in addition to causal therapy is mandatory. The purpose of this review is to delineate some characteristics of septic myocardial dysfunction, to assess the most commonly cited and reported underlying mechanisms of cardiac dysfunction in sepsis, and to briefly outline current therapeutic strategies and possible future approaches.
Sepsis, defined by consensus conference as “the systemic inflammatory response syndrome (SIRS) that occurs during infection,”1 is generally viewed as a disease aggravated by the inappropriate immune response encountered in the affected individual (for review, see Hotchkiss and Karl2 and Riedemann et al,3). The Table gives the current criteria for the establishment of the diagnosis of systemic inflammatory response syndrome, sepsis, and septic shock.1,4 Morbidity and mortality are high, resulting in sepsis and septic shock being the 10th most common cause of death in the United States.5 The incidence of sepsis and sepsis-related deaths appears to be increasing by 1.5% per year.6 In a recent study,6 the total national hospital cost invoked by severe sepsis in the United States was estimated at approximately $16.7 billion on the basis of an estimated severe sepsis rate of 751 000 cases per year with 215 000 associated deaths annually. A recent study from Britain documented a 46% in-hospital mortality rate for patients presenting with severe sepsis on admission to the intensive care unit.7
Current Criteria for Establishment of the Diagnosis of SIRS, Sepsis, and Septic Shock1,4
As an important organ system frequently affected by sepsis and always affected by septic shock, the cardiovascular system and its dysfunction during sepsis have been studied in clinical and basic research for more than 5 decades. In 1951, Waisbren was the first to describe cardiovascular dysfunction due to sepsis.8 He recognized a hyperdynamic state with full bounding pulses, flushing, fever, oliguria, and hypotension. In addition, he described a second, smaller patient group who presented clammy, pale, and hypotensive with low volume pulses and who appeared more severely ill. With hindsight, the latter group might well have been volume underresuscitated, and indeed, timely and adequate volume therapy has been demonstrated to be one of the most effective supportive measures in sepsis therapy.9
Under conditions of adequate volume resuscitation, the profoundly reduced systemic vascular resistance typically encountered in sepsis10 leads to a concomitant elevation in cardiac index that obscures the myocardial dysfunction that also occurs. However, as early as the mid-1980s, significant reductions in both stroke volume and ejection fraction in septic patients were observed despite normal total cardiac output.11 Importantly, the presence of cardiovascular dysfunction in sepsis is associated with a significantly increased mortality rate of 70% to 90% compared with 20% in septic patients without cardiovascular impairment.12 Thus, myocardial dysfunction in sepsis has been the focus of intense research activity. Although a number of mediators and pathways have been shown to be associated with myocardial depression in sepsis, the precise cause remains unclear.
The purpose of the present review is to delineate some characteristics of septic myocardial dysfunction, to assess the most commonly cited and reported underlying mechanisms of cardiac dysfunction in sepsis, and to briefly outline current therapeutic strategies and possible future approaches. This review is not intended to be all inclusive.
Characteristics of Myocardial Dysfunction in Sepsis
Using portable radionuclide cineangiography, Calvin et al13 were the first to demonstrate myocardial dysfunction in adequately volume-resuscitated septic patients with decreased ejection fraction and increased end-diastolic volume index. Adding pulmonary artery catheters to serial radionuclide cineangiography, Parker and colleagues11 extended these observations with the 2 major findings that (1) survivors of septic shock were characterized by increased end-diastolic volume index and decreased ejection fraction, whereas nonsurvivors typically maintained normal cardiac volumes, and (2) these acute changes in end-diastolic volume index and ejection fraction, although sustained for several days, were reversible. More recently, echocardiographic studies have demonstrated impaired left ventricular systolic and diastolic function in septic patients.14–16 These human studies, in conjunction with experimental studies ranging from the cellular level17 to isolated heart studies18,19 and to in vivo animal models,20–22 have clearly established decreased contractility and impaired myocardial compliance as major factors that cause myocardial dysfunction in sepsis.
Notwithstanding the functional and structural differences between the left and right ventricle, similar functional alterations, as discussed above, have been observed for the right ventricle, which suggests that right ventricular dysfunction in sepsis closely parallels left ventricular dysfunction.23–26 However, the relative contribution of the right ventricle to septic cardiomyopathy remains unknown.
Myocardial dysfunction in sepsis has also been analyzed with respect to its prognostic value. Parker et al,27 reviewing septic patients on initial presentation and at 24 hours to determine prognostic indicators, found a heart rate of <106 bpm to be the only cardiac parameter on presentation that predicted a favorable outcome. At 24 hours after presentation, a systemic vascular resistance index >1529 dyne · s−1 · cm−5 · m−2, a heart rate <95 bpm or a reduction in heart rate >18 bpm, and a cardiac index >0.5 L · min−1 · m−2 suggested survival.27 In a prospective study, Rhodes et al28 demonstrated the feasibility of a dobutamine stress test for outcome stratification, with nonsurvivors being characterized by an attenuated inotropic response. The well-established biomarkers in myocardial ischemia and heart failure, cardiac troponin I and T, as well as B-type natriuretic peptide, have also been evaluated with regard to sepsis-associated myocardial dysfunction. Although B-type natriuretic peptide studies have delivered conflicting results in septic patients (for review, see Maeder et al29), several small studies have reported a relationship between elevated cardiac troponin T and I and left ventricular dysfunction in sepsis, as assessed by echocardiographic ejection fraction30–33 or pulmonary artery catheter–derived left ventricular stroke work index.34 Cardiac troponin levels also correlated with the duration of hypotension35 and the intensity of vasopressor therapy.34In addition, increased sepsis severity, measured by global scores such as the Simplified Acute Physiology Score II (SAPS II) or the Acute Physiology And Chronic Health Evaluation II score (APACHE II), was associated with increased cardiac troponin levels,31,33 as was poor short-term prognosis.32,33,35,36 Despite the heterogeneity of study populations and type of troponin studied, the mentioned studies were univocal in concluding that elevated troponin levels in septic patients reflect higher disease severity, myocardial dysfunction, and worse prognosis. In a recent meta-analysis of 23 observational studies, Lim et al37 found cardiac troponin levels to be increased in a large percentage of critically ill patients. Furthermore, in a subset of studies that permitted adjusted analysis and comprised 1706 patients, this troponin elevation was associated with an increased risk of death (odds ratio, 2.5; 95% CI, 1.9 to 3.4, P<0.001)37; however, the underlying mechanisms clearly require further research.
Thus, it appears reasonable to recommend inclusion of cardiac troponins in the monitoring of patients with severe sepsis and septic shock to facilitate prognostic stratification and to increase alertness to the presence of cardiac dysfunction in individual patients. However, it remains to be shown whether risk stratification based on cardiac troponins can identify patients in whom aggressive therapeutic regimens might reap the greatest benefit and so translate into a survival benefit.
Mechanisms Underlying Myocardial Dysfunction in Sepsis
Cardiac depression during sepsis is probably multifactorial (Figure). Nevertheless, it is important to identify individual contributing factors and mechanisms to generate worthwhile therapeutic targets. As a consequence, a vast array of mechanisms, pathways, and disruptions in cellular homeostasis have been examined in septic myocardium.
View larger version:
Synopsis of potential underlying mechanisms in septic myocardial dysfunction. MDS indicates myocardial depressant substance.
Global Ischemia
An early theory of myocardial depression in sepsis was based on the hypothesis of global myocardial ischemia; however, septic patients have been shown to have high coronary blood flow and diminished coronary artery–coronary sinus oxygen difference.38 As in the peripheral circulation, these alterations can be attributed to disturbed flow autoregulation or disturbed oxygen utilization.39,40 Coronary sinus blood studies in patients with septic shock have also demonstrated complex metabolic alterations in septic myocardium, including increased lactate extraction, decreased free fatty acid extraction, and decreased glucose uptake.41 Furthermore, several magnetic resonance studies in animal models of sepsis have demonstrated the presence of normal high-energy phosphate levels in the myocardium.42,43 It has also been proposed that myocardial dysfunction in sepsis may reflect hibernating myocardium.44 To reach this conclusion, Levy et al44 studied a murine cecal ligation and double-puncture model and observed diminished cardiac performance, increased myocardial glucose uptake, and deposits of glycogen in a setting of preserved arterial oxygen tension and myocardial perfusion. Although all of the above-mentioned findings reflect important alterations in coronary flow and myocardial metabolism, mirroring effects observed in peripheral circulation during sepsis, there is no evidence supporting global ischemia as an underlying cause of myocardial dysfunction in sepsis. However, in septic patients with coexistent and possibly undiagnosed coronary artery disease (CAD), regional myocardial ischemia or infarction secondary to CAD may certainly occur. The manifestation of myocardial ischemia due to CAD might even be facilitated by the volatile hemodynamics in sepsis, as well as by the generalized microvascular dysfunction so frequently observed in sepsis.45 Additional CAD-aggravating factors encountered in sepsis encompass generalized inflammation and the activated coagulatory system. Furthermore, the endothelium plays a prominent role in sepsis (see below), but little is known of the impact of preexisting, CAD-associated endothelial dysfunction in this context. In a postmortem study of 21 fatal cases of septic shock, previously undiagnosed myocardial ischemia at least contributed to death in 7 of the 21 cases (all 21 patients were males, with a mean age of 60.4 years).46 It certainly appears prudent to remain wary of CAD complications while treating sepsis, especially in patients with identifiable risk factors and in view of the ever-increasing mean age of intensive care unit patients and including septic patients.
Myocardial Depressant Substance
A circulating myocardial depressant factor in septic shock was first proposed more than 50 years ago.47 Parrillo et al48 quantitatively linked the clinical degree of septic myocardial dysfunction with the effect the serum, taken from respective patients, had on rat cardiac myocytes, with clinical severity correlating well with the decrease in extent and velocity of myocyte shortening. These effects were not seen when serum from convalescent patients whose cardiac function had returned to normal was applied or when serum was obtained from other critically ill, nonseptic patients.48 In extension of these findings, ultrafiltrates from patients with severe sepsis and simultaneously reduced left ventricular stroke work index (<30 g · m−1 · m−2) displayed cardiotoxic effects and contained significantly increased concentrations of interleukin (IL)-1, IL-8, and C3a.49Recently, Mink et al50 demonstrated that lysozyme c, a bacteriolytic agent believed to originate mainly from disintegrating neutrophilic granulocytes and monocytes, mediates cardiodepressive effects during Escherichia coli sepsis and, importantly, that competitive inhibition of lysozyme c can prevent myocardial depression in the respective experimental sepsis model. Additional potential candidates for myocardial depressant substance include other cytokines, prostanoids, and nitric oxide (NO). Some of these will be discussed below.
Cytokines
Infusion of lipopolysaccharide (LPS, an obligatory component of Gram-negative bacterial cell walls) into both animals and humans51 partially mimics the hemodynamic effects of septic shock.51,52 However, only a minority of patients with septic shock have detectable LPS levels, and the prolonged time course of septic myocardial dysfunction and the chemical characteristics of LPS are not consistent with LPS representing the sole myocardial depressant substance.48,53 Tumor necrosis factor-α (TNF-α) is an important early mediator of endotoxin-induced shock.54 TNF-α is derived from activated macrophages, but recent studies have shown that TNF-α is also secreted by cardiac myocytes in response to sepsis.55 Although application of anti-TNF-α antibodies improved left ventricular function in patients with septic shock,56 subsequent studies using monoclonal antibodies directed against TNF-α or soluble TNF-α receptors failed to improve survival in septic patients.57–59 IL-1 is synthesized by monocytes, macrophages, and neutrophils in response to TNF-α and plays a crucial role in the systemic immune response. IL-1 depresses cardiac contractility by stimulating NO synthase (NOS).60 Transcription of IL-1 is followed by delayed transcription of IL-1 receptor antagonist (IL-1-ra), which functions as an endogenous inhibitor of IL-1. Recombinant IL-1-ra was evaluated in phase III clinical trials, which showed a tendency toward improved survival61 and increased survival time in a retrospective analysis of the patient subgroup with the most severe sepsis62; however, to date, this initially promising therapy has failed to deliver a statistically significant survival benefit. IL-6, another proinflammatory cytokine, has also been implicated in the pathogenesis of sepsis and is considered a more consistent predictor of sepsis than TNF-α because of its prolonged elevation in the circulation.63 Although cytokines may very well play a key role in the early decrease in contractility, they cannot explain the prolonged duration of myocardial dysfunction in sepsis, unless they result in the induction or release of additional factors that in turn alter myocardial function, such as prostanoids or NO.64,65
Prostanoids
Prostanoids are produced by the cyclooxygenase enzyme from arachidonic acid. The expression of cyclooxygenase enzyme-2 is induced, among other stimuli, by LPS and cytokines (cyclooxygenase enzyme-1 is expressed constitutively).66 Elevated levels of prostanoids such as thromboxane and prostacyclin, which have the potential to alter coronary autoregulation, coronary endothelial function, and intracoronary leukocyte activation, have been demonstrated in septic patients.67 Early animal studies with cyclooxygenase inhibitors such as indomethacin yielded very promising results.68,69Along with other positive results, these led to an important clinical study involving 455 septic patients who were randomized to receive intravenous ibuprofen or placebo.70Unfortunately, that study did not demonstrate improved survival for the treatment arm. Similarly, a more recent, smaller study on the effects of lornoxicam failed to provide evidence for a survival benefit through cyclooxygenase inhibition in sepsis.71 Animal studies aimed at elucidating possible benefits of isotype-selective cyclooxygenase inhibition have so far produced conflicting results.72,73
Endothelin-1
Endothelin-1 (ET-1; for an in-depth review of endothelin in sepsis, see Gupta et al74) upregulation has been demonstrated within 6 hours of LPS-induced septic shock.75Cardiac overexpression of ET-1 triggers an increase in inflammatory cytokines (among others, TNF-α, IL-1, and IL-6), interstitial inflammatory infiltration, and an inflammatory cardiomyopathy that results in heart failure and death.76 The involvement of ET-1 in septic myocardial dysfunction is supported by the observation that tezosentan, a dual endothelin-A and endothelin-B receptor antagonist, improved cardiac index, stroke volume index, and left ventricular stroke work index in endotoxemic shock.77 However, higher doses of tezosentan exhibited cardiotoxic effects and led to increased mortality.77Although ET-1 has been demonstrated to be of pathophysiological importance in a wide array of cardiac diseases through autocrine, endocrine, or paracrine effects, its biosynthesis, receptor-mediated signaling, and functional consequences in septic myocardial dysfunction warrant further investigation to assess the therapeutic potential of ET-1 receptor antagonists.
Nitric Oxide
NO exerts a plethora of biological effects in the cardiovascular system.78 It has been shown to modulate cardiac function under physiological and a multitude of pathophysiological conditions. In healthy volunteers, low-dose NO increases LV function, whereas inhibition of endogenous NO release by intravenous infusion of the NO synthase (NOS) inhibitor NG-monomethyl-L-arginine reduced the stroke volume index.79 Higher doses of NO have been shown to induce contractile dysfunction by depressing myocardial energy generation.80 The absence of the important NO scavenger myoglobin (Mb) in Mb knockout mice results in impaired cardiac function that is partially reversible by NOS inhibition.81 Endogenous NO contributes to hibernation in response to myocardial ischemia by reducing oxygen consumption and preserving calcium sensitivity and contractile function.82 NO also represents a potent modulator of myocardial ischemia/reperfusion injury. However, as in sepsis-related NO research, the reported effects of NO on ischemia/reperfusion injury are inconsistent owing to a multitude of confounding experimental factors.83
Sepsis leads to the expression of inducible NOS (iNOS) in the myocardium,84,85 followed by high-level NO production, which in turn importantly contributes to myocardial dysfunction, in part through the generation of cytotoxic peroxynitrite, a product of NO and superoxide (for an excellent review, see Pacher et al86). In iNOS-deficient mice, cardiac function is preserved after endotoxin challenge.87 Nonspecific NOS inhibition restores cardiac output and stroke volume after LPS injection.88 Strikingly, in septic patients, infusion of methylene blue, a nonspecific NOS inhibitor, improves mean arterial pressure, stroke volume, and left ventricular stroke work and decreases the requirement for inotropic support but, unfortunately, does not alter outcome.89 An interesting study comparing the inhibition of NO superoxide and peroxynitrite in cytokine-induced myocardial contractile failure found peroxynitrite to indeed be the most promising therapeutic target.90 It has also been proposed that the constitutively expressed mitochondrial isoform of NOS (mtNOS), the expression of which can be augmented by induction, controls rates of oxidative phosphorylation by inhibiting various steps of the respiratory chain.91 Although this hypothesis would provide a plausible explanation for the reduced coronary oxygen extraction observed during sepsis (see above), the effects of sepsis on expression of mtNOS and NO generation remain to be explored. Furthermore, the constitutively expressed endothelial NOS (eNOS), previously neglected in the context of sepsis, has been shown to be an important regulator of iNOS expression, resulting in a more stable hemodynamic status in eNOS-deficient mice after endotoxemia.92 Very recently, a functional NOS in red blood cells (rbcNOS) was identified that regulates deformability of erythrocyte membranes and inhibits activation of platelets.93 With both effect targets thus far demonstrated for rbcNOS lying at the core of microvascular dysfunction in sepsis, this discovery opens a whole new window to NO-related sepsis research. Given the existence of different NOS isoforms and their various modulating interactions, dose-dependent NO effects, and the precise balance of NO, superoxide, and thus peroxynitrite generated in subcellular compartments, further advances in our understanding of the complex NO biology and its derived reactive nitrogen species hold the promise of revealing new, more specific and effective therapeutic targets.
Adhesion Molecules
Surface-expression upregulation of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 has been demonstrated in murine coronary endothelium and cardiomyocytes after LPS and TNF-α stimulation.94 After cecal ligation and double puncture, myocardial intercellular adhesion molecule-1 expression increases in rats.95Vascular cell adhesion molecule-1 blockade with antibodies has been shown to prevent myocardial dysfunction and decrease myocardial neutrophil accumulation,94,96 whereas both knockout and antibody blockade of intercellular adhesion molecule-1 ameliorate myocardial dysfunction in endotoxemia without affecting neutrophil accumulation.94 In addition, neutrophil depletion does not protect against septic cardiomyopathy, which suggests that the cardiotoxic potential of neutrophils infiltrating the myocardium is of lesser importance in this context.94 Other aspects of adhesion molecules are discussed in conjunction with possible statin effects below.
The e-Reader is advised to consider the following expansion on the subject matter carrying the discussion to additional related clinical issues:
Therapeutic Approaches: The Present and the Future
A detailed discussion of therapeutic options in septic patients would clearly be beyond the scope of this review, and readers are kindly referred to the multiple excellent reviews published on the subject (eg, Hotchkiss and Karl,2 Annane et al,4 and Dellinger et al97). Although a number of preventive measures, such as prophylactic antibiotics, maintenance of normoglycemia, selective digestive tract decontamination, vaccines, and intravenous immunoglobulin, have shown benefit in distinct patient populations, preventive strategies with a broader aim remain elusive. Once sepsis is manifest (see the Table for criteria), prompt and adequate antibiotic therapy accompanied by surgical removal of the infectious focus, if indicated and feasible, is the mainstay and also the only strictly causal line of therapy. In the presence of severe sepsis and septic shock, supportive treatment in addition to causal therapy is mandatory. Supportive therapy encompasses early and goal-directed fluid resuscitation,9 vasopressor and inotropic therapy, red blood cell transfusion, mechanical ventilation, and renal support when indicated. It is very likely beneficial to monitor cardiac performance in these patients. A wide array of techniques are available for this purpose, ranging from echocardiography to pulmonary catheters, thermodilution techniques, and pulse pressure analysis.98 Because none of these techniques have demonstrated superiority, physicians should use the method with which they are most familiar. Whichever method is chosen, it should be applied frequently to tailor supportive therapy to the individual patient and to achieve the “gold standard” of early goal-directed therapy. In recent years, several attempts have been made to therapeutically address myocardial dysfunction in sepsis. Although the combination of norepinephrine as vasopressor and dobutamine as inotropic agent is probably the most frequently applied in septic shock, there is currently no evidence to recommend one catecholamine over the other.97 In human endotoxemia, epinephrine has been demonstrated to inhibit proinflammatory pathways and coagulation activation, as well as to augment antiinflammatory pathways,99,100 whereas no immunomodulatory or coagulant effects could be demonstrated for dobutamine in a similar setting.101 Isoproterenol has recently been applied successfully in a small group of patients with septic shock, no known history of CAD, and inappropriate mixed venous oxygen concentration despite correction of hypoxemia and anemia.102 In a cecal ligation and double-puncture model of sepsis, the β-blocker esmolol given continuously after sepsis induction improved myocardial oxygen utilization and attenuated myocardial dysfunction,103 which suggests that therapeutic strategies proven in ischemic heart failure might also hold promise in septic cardiomyopathy. However, the optimal mode of β-receptor stimulation (or indeed inhibition) to limit myocardial dysfunction remains a wide-open field for inspired investigation.
Given the generally accepted view of sepsis as a disease largely propelled by an inappropriate immune response, numerous basic research and clinical trials have been undertaken to curb the lethal toll of sepsis through modulation of this uncontrolled immune response.2,3 To date, activated protein C104 and low-dose hydrocortisone105 have emerged as the only inflammation-modulating substances that have been confirmed to be of benefit in patients with severe sepsis and septic shock. Over the past years, increasing evidence has accumulated that suggests that inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase, or statins, have therapeutic benefits independent of cholesterol lowering, termed “pleiotropic” effects. These have added a wide scope of potential targets for statin therapy that range from decreasing renal function loss106 and lowering mortality in patients with diastolic heart failure107 to prevention and treatment of stroke,108 to name just a few. These pleiotropic effects include antiinflammatory and antioxidative properties, improvement of endothelial function, and increased NO bioavailability and thus might contribute to the benefit observed with statin therapy. Notably, these important immunomodulatory effects of statins have been demonstrated to be independent of lipid lowering109 and appear to be mediated via interference with the synthesis of mevalonate metabolites (nonsteroidal isoprenoid products). Blockade of the mevalonate pathway has been shown to suppress T-cell responses,110 reduce expression of class II major histocompatibility complexes on antigen presenting cells,109 and inhibit chemokine synthesis in peripheral blood mononuclear cells.111 Furthermore, CD11b integrin expression and CD11b-dependent adhesion of monocytes have been found to be attenuated by the initiation of statin treatment in hypercholesterolemic patients.112 In this context, Yoshida et al113 have reported that statins reduce the expression of both monocytic and endothelial adhesion molecules, eg, the integrin leukocyte function-associated antigen-1 (LFA-1), via an inhibition of Rho GTPases, in particular their membrane anchoring by geranylation. In addition, mechanisms for antiinflammatory actions of statins have been revealed that are not related to the isoprenoid metabolism. For instance, Weitz-Schmidt et al114 have identified that some statins act as direct antagonists of LFA-1 owing to their capacity to bind to the regulatory site in the LFA-1 i-domain. In addition to these multifaceted antiinflammatory effects, statins may interfere with activation of the coagulation cascade, as illustrated by the suppression of LPS-induced monocyte tissue factor in vitro.115 Beyond their immunomodulatory functions, statins have been shown to exert direct antichlamydial effects during pulmonary infection with Chlamydia pneumoniae in mice,116 and a recent report suggests the benefit of statins may also extend to viral pathogens.117
Given the strong impact of statins on inflammation, statins might represent a welcome enforcement in the battle against severe infectious diseases such as sepsis. Consequently, several investigators have evaluated the role of statins in the prevention and treatment of sepsis. In a retrospective analysis, Liappis et al118 demonstrated a reduced overall and attributable mortality in patients with bacteremia who were treated concomitantly with statins. Pretreatment with simvastatin has been shown to profoundly improve survival in a polymicrobial murine model of sepsis by preservation of cardiovascular function and inhibition of inflammatory alterations.19 Encouraged by these findings, the same model was used to successfully treat sepsis in a clinically feasible fashion, ie, treatment was initiated several hours after the onset of sepsis. With different statins (atorvastatin, pravastatin, and simvastatin) being effective, the therapeutic potential of statins in sepsis appears to be a class effect.22 Recently, Steiner et al119observed that pretreatment with simvastatin can suppress the inflammatory response induced by LPS in healthy human volunteers. Furthermore, in a prospective observational cohort study in patients with acute bacterial infections performed by Almog et al,120previous treatment with statins was associated with a considerably reduced rate of severe sepsis and intensive care unit admissions. A total of 361 patients were enrolled in that study, and 82 of these patients had been treated with statins for at least 4 weeks before their admission. Severe sepsis developed in 19% of patients in the no-statin group compared with only 2.4% in patients who were taking statins. The intensive care unit admission rates were 12.2% for the no-statin group and 3.7% for the statin group. Because of the number of patients enrolled, the study was not powered to detect differences in mortality, although the large effect on sepsis rate and intensive care unit admission were at least suggestive. As the most recent development in this field, Hackam et al121 have produced an impressive observational study by initial evaluation of 141 487 cardiovascular patients, which resulted in a well-paired and homogenous study cohort of 69 168 patients after propensity-based matching. Drawing from this solid base, Hackam and coauthors were able to support the conclusion that statin therapy is associated with a considerably decreased rate of sepsis (hazard ratio, 0.81; 95% CI, 0.72 to 0.90), severe sepsis (hazard ratio, 0.83; 95% CI, 0.70 to 0.97), and fatal sepsis (hazard ratio, 0.75; 95% CI, 0.61 to 0.93). This protective effect prevailed at both high and low statin doses and for several clinically important subpopulations, such as diabetic and heart failure patients.
As has been suggested previously,122 statins might provide cumulative benefit by reducing mortality from cardiovascular and infectious diseases such as sepsis. However, statins may have detrimental effects in distinct subsets of patients. Therefore, caution should prevail, and the use of statins in patients with sepsis must be accompanied by meticulous monitoring of unexpected side effects and well-designed randomized, controlled clinical trials.
Beyond an apparent rationale for randomized trials on statins in sepsis, it is notable that the results with other immunomodulatory approaches in sepsis have yielded rather limited success. For instance, use of the anti-TNF antibody F(ab′)2 fragment afelimomab led to a significant but rather modest reduction in risk of death and to improved organ-failure scores in patients with severe sepsis and elevated IL-6 levels.123 Moreover, a selective inhibitor of group IIA secretory phospholipase A2 failed to improve clinical outcome for patients with severe sepsis, with a negative trend most pronounced among patients with cardiovascular failure.124 Hence, because none of the available strategies proven to be effective in sepsis are designed specifically to target myocardial dysfunction, one might conclude that strategies that preferentially address cardiac morbidity in sepsis may be a promising area for investigation. For instance, lipoteichoic acid, a major virulence factor in Gram-positive sepsis, causes cardiac depression by activating myocardial TNF-α synthesis via CD14 and induces coronary vascular disturbances by activating thromboxane 2 synthesis. It thus contributes to cardiac depression and may therefore be a worthwhile and cardiac-specific target.125 The implications of intensified efforts in the search for successful novel approaches to the treatment of myocardial dysfunction in sepsis may be considerable with regard to improved patient care that results in reduced mortality. This is of major significance in view of the substantial economic consequences of increasing sepsis morbidity in an aging population.
REFERENCES
in Circulation.2007; 116: 793-802 doi: 10.1161/CIRCULATIONAHA.106.678359
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RMH, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992; 101: 1644–1655.
Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001; 29: 1303–1310.
Padkin A, Goldfrad C, Brady AR, Young D, Black N, Rowan K. Epidemiology of severe sepsis occurring in the first 24 hrs in intensive care units in England, Wales, and Northern Ireland. Crit Care Med. 2003; 31: 2332–2338.
Waisbren BA. Bacteremia due to gram-negative bacilli other than the Salmonella: a clinical and therapeutic study. AMA Arch Intern Med. 1951; 88: 467–488.
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M; Early Goal-Directed Therapy Collaborative Group. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med.2001; 345: 1368–1377.
Parker MM, Shelhamer JH, Bacharach SL, Green MV, Natanson C, Frederick TM, Damske BA, Parrillo JE. Profound but reversible myocardial depression in patients with septic shock. Ann Intern Med. 1984; 100: 483–490.
Parrillo JE, Parker MM, Natanson C, Suffredini AF, Danner RL, Cunnion RE, Ognibene FP. Septic shock in humans: advances in the understanding of pathogenesis, cardiovascular dysfunction, and therapy. Ann Intern Med. 1990; 113:227–242.
Calvin JE, Driedger AA, Sibbald WJ. An assessment of myocardial function in human sepsis utilizing ECG gated cardiac scintigraphy. Chest. 1981; 80: 579–586.
Munt B, Jue J, Gin K, Fenwick J, Tweeddale M. Diastolic filling in human severe sepsis: an echocardiographic study. Crit Care Med. 1998; 26: 1829–1833.
Poelaert J, Declerck C, Vogelaers D, Colardyn F, Visser CA. Left ventricular systolic and diastolic function in septic shock. Intensive Care Med. 1997; 23: 553–560.
Ren J, Ren BH, Sharma AC. Sepsis-induced depressed contractile function of isolated ventricular myocytes is due to altered calcium transient properties. Shock.2002; 18: 285–288.
Natanson C, Fink MP, Ballantyne HK, Mac Vittie TJ, Conklin JJ, Parrillo JE. Gram-negative bacteremia produces both severe systolic and diastolic cardiac dysfunction in a canine model that simulates human septic shock. J Clin Invest.1986; 78: 259–270.
Merx MW, Liehn EA, Graf J, van de Sandt A, Schaltenbrand M, Schrader J, Hanrath P, Weber C. Statin treatment after onset of sepsis in a murine model improves survival. Circulation. 2005; 112: 117–124.
Vincent JL, Thirion M, Brimioulle S, Lejeune P, Kahn RJ. Thermodilution measurement of right ventricular ejection fraction with a modified pulmonary artery catheter. Intensive Care Med. 1986; 12: 33–38.
Dhainaut JF, Brunet F, Monsaillier JF, Villemant D, Devaux JY, Konno M, De Gournay JM, Armaganidis A, Iotti G, Huyghebaert MF. Bedside evaluation of right ventricular performance using a rapid computerized thermodilution method. Crit Care Med. 1987; 15: 148–152.
Parker MM, McCarthy KE, Ognibene FP, Parrillo JE. Right ventricular dysfunction and dilatation, similar to left ventricular changes, characterize the cardiac depression of septic shock in humans. Chest. 1990; 97: 126–131.
Parker MM, Shelhamer JH, Natanson C, Alling DW, Parrillo JE. Serial cardiovascular variables in survivors and nonsurvivors of human septic shock: heart rate as an early predictor of prognosis. Crit Care Med. 1987; 15: 923–929.
Rhodes A, Lamb FJ, Malagon I, Newman PJ, Grounds RM, Bennett ED. A prospective study of the use of a dobutamine stress test to identify outcome in patients with sepsis, severe sepsis, or septic shock. Crit Care Med. 1999; 27: 2361–2366.
Maeder M, Fehr T, Rickli H, Ammann P. Sepsis-associated myocardial dysfunction: diagnostic and prognostic impact of cardiac troponins and natriuretic peptides. Chest. 2006; 129: 1349–1366.
ver Elst KM, Spapen HD, Nguyen DN, Garbar C, Huyghens LP, Gorus FK. Cardiac troponins I and T are biological markers of left ventricular dysfunction in septic shock. Clin Chem. 2000; 46: 650–657.
Mehta NJ, Khan IA, Gupta V, Jani K, Gowda RM, Smith PR. Cardiac troponin I predicts myocardial dysfunction and adverse outcome in septic shock. Int J Cardiol.2004; 95: 13–17.
Arlati S, Brenna S, Prencipe L, Marocchi A, Casella GP, Lanzani M, Gandini C. Myocardial necrosis in ICU patients with acute non-cardiac disease: a prospective study. Intensive Care Med. 2000; 26: 31–37.
Spies C, Haude V, Fitzner R, Schroder K, Overbeck M, Runkel N, Schaffartzik W. Serum cardiac troponin T as a prognostic marker in early sepsis. Chest. 1998;113: 1055–1063.
Herbertson MJ, Werner HA, Russell JA, Iversen K, Walley KR. Myocardial oxygen extraction ratio is decreased during endotoxemia in pigs. J Appl Physiol.1995; 79: 479–486.
Solomon MA, Correa R, Alexander HR, Koev LA, Cobb JP, Kim DK, Roberts WC, Quezado ZM, Scholz TD, Cunnion RE, Hoffman WD, Bacher J, Yatsiv I, Danner RL, Banks SM, Ferrans VJ, Balaban RS, Natanson C. Myocardial energy metabolism and morphology in a canine model of sepsis. Am J Physiol Heart Circ Physiol. 1994; 266: H757–H768.
Van Lambalgen AA, van Kraats AA, Mulder MF, Teerlink T, van den Bos GC. High-energy phosphates in heart, liver, kidney, and skeletal muscle of endotoxemic rats. Am J Physiol Heart Circ Physiol. 1994; 266: H1581–H1587.
Levy RJ, Piel DA, Acton PD, Zhou R, Ferrari VA, Karp JS, Deutschman CS. Evidence of myocardial hibernation in the septic heart. Crit Care Med. 2005; 33:2752–2756.
Parrillo JE, Burch C, Shelhamer JH, Parker MM, Natanson C, Schuette W. A circulating myocardial depressant substance in humans with septic shock: septic shock patients with a reduced ejection fraction have a circulating factor that depresses in vitro myocardial cell performance. J Clin Invest. 1985; 76: 1539–1553.
Hoffmann JN, Werdan K, Hartl WH, Jochum M, Faist E, Inthorn D. Hemofiltrate from patients with severe sepsis and depressed left ventricular contractility contains cardiotoxic compounds. Shock. 1999; 13: 174–180.
Suffredini AF, Fromm RE, Parker MM, Brenner M, Kovacs JA, Wesley RA, Parrillo JE. The cardiovascular response of normal humans to the administration of endotoxin. N Engl J Med. 1989; 321: 280–287.
Reilly JM, Cunnion RE, Burch-Whitman C, Parker MM, Shelhamer JH, Parrillo JE. A circulating myocardial depressant substance is associated with cardiac dysfunction and peripheral hypoperfusion (lactic acidemia) in patients with septic shock. Chest. 1989; 95: 1072–1080.
Vincent JL, Bakker J, Marecaux G, Schandene L, Kahn RJ, Dupont E. Administration of anti-TNF antibody improves left ventricular function in septic shock patients: results of a pilot study. Chest. 1992; 101: 810–815.
Fisher CJ, Agosti JM, Opal SM, Lowry SF, Balk RA, Sadoff JC, Abraham E, Schein RM, Benjamin E; the Soluble TNF Receptor Sepsis Study Group. Treatment of septic shock with the tumor necrosis factor receptor:Fc fusion protein. N Engl J Med. 1996; 334: 1697–1702.
Abraham E, Glauser MP, Butler T, Garbino J, Gelmont D, Laterre PF, Kudsk K, Bruining HA, Otto C, Tobin E, Zwingelstein C, Lesslauer W, Leighton A; Ro 45-2081 Study Group. p55 Tumor necrosis factor receptor fusion protein in the treatment of patients with severe sepsis and septic shock: a randomized controlled multicenter trial. JAMA. 1997; 277: 1531–1538.
Abraham E, Anzueto A, Gutierrez G, Tessler S, San Pedro G, Wunderink R, Dal Nogare A, Nasraway S, Berman S, Cooney R, Levy H, Baughman R, Rumbak M, Light RB, Poole L, Allred R, Constant J, Pennington J, Porter S; NORASEPT II Study Group. Double-blind randomised controlled trial of monoclonal antibody to human tumour necrosis factor in treatment of septic shock. Lancet. 1998; 351: 929–933.
Francis SE, Holden H, Holt CM, Duff GW. Interleukin-1 in myocardium and coronary arteries of patients with dilated cardiomyopathy. J Mol Cell Cardiol. 1998;30: 215–223.
Damas P, Ledoux D, Nys M, Vrindts Y, De Groote D, Franchimont P, Lamy M. Cytokine serum level during severe sepsis in human IL-6 as a marker of severity.Ann Surg. 1992; 215: 356–362.
Schulz R, Nava E, Moncada S. Induction and potential biological relevance of a Ca2+-independent nitric oxide synthase in the myocardium. Br J Pharmacol. 1992;105: 575–580.
Liu SF, Newton R, Evans TW, Barnes PJ. Differential regulation of cyclo-oxygenase-1 and cyclo-oxygenase-2 gene expression by lipopolysaccharide treatment in vivo in the rat. Clin Sci (Lond). 1996; 90: 301–306.
Fletcher JR, Ramwell PW. Modification, by aspirin and indomethacin, of the haemodynamic and prostaglandin releasing effects of E. coli endotoxin in the dog.Br J Pharmacol. 1977; 61: 175–181.
Bernard GR, Wheeler AP, Russel JA, Schein R, Summer WR, Steinberg KP, Fulkerson WJ, Wright PE, Christmann BW, Dupont WD, Higgins SB, Swindell BB; The Ibuprofen in Sepsis Study Group. The effects of ibuprofen on the physiology and survival of patients with sepsis. N Engl J Med. 1997; 336: 912–918.
Tunctan B, Altug S, Uludag O, Demirkay B, Abacioglu N. Effects of cyclooxygenase inhibitors on nitric oxide production and survival in a mice model of sepsis. Pharmacol Res. 2003; 48: 37–48.
Reddy RC, Chen GH, Tateda K, Tsai WC, Phare SM, Mancuso P, Peters-Golden M, Standiford TJ. Selective inhibition of COX-2 improves early survival in murine endotoxemia but not in bacterial peritonitis. Am J Physiol Lung Cell Mol Physiol.2001; 281: L537–L543.
Shindo T, Kurihara H, Kurihara Y, Morita H, Yazaki Y. Upregulation of endothelin-1 and adrenomedullin gene expression in the mouse endotoxin shock model. J Cardiovasc Pharmacol. 1998; 31: S541–S544.
Yang LL, Gros R, Kabir MG, Sadi A, Gotlieb AI, Husain M, Stewart DJ. Conditional cardiac overexpression of endothelin-1 induces inflammation and dilated cardiomyopathy in mice. Circulation. 2004; 109: 255–261.
Konrad D, Oldner A, Rossi P, Wanecek M, Rudehill A, Weitzberg E. Differentiated and dose-related cardiovascular effects of a dual endothelin receptor antagonist in endotoxin shock. Crit Care Med. 2004; 32: 1192–1199.
Schulz R, Rassaf T, Massion PB, Kelm M, Balligand JL. Recent advances in the understanding of the role of nitric oxide in cardiovascular homeostasis. Pharmacol Ther. 2005; 108: 225–256.
Rassaf T, Poll LW, Brouzos P, Lauer T, Totzeck M, Kleinbongard P, Gharini P, Andersen K, Schulz R, Heusch G, Modder U, Kelm M. Positive effects of nitric oxide on left ventricular function in humans. Eur Heart J. 2006; 27: 1699–1705.
Kelm M, Schafer S, Dahmann R, Dolu B, Perings S, Decking UK, Schrader J, Strauer BE. Nitric oxide induced contractile dysfunction is related to a reduction in myocardial energy generation. Cardiovasc Res. 1997; 36: 185–194.
Merx MW, Godecke A, Flogel U, Schrader J. Oxygen supply and nitric oxide scavenging by myoglobin contribute to exercise endurance and cardiac function.FASEB J. 2005; 19: 1015–1017.
Preiser JC, Zhang H, Vray B, Hrabak A, Vincent JL. Time course of inducible nitric oxide synthase activity following endotoxin administration in dogs. Nitric Oxide. 2001; 5: 208–211.
Khadour FH, Panas D, Ferdinandy P, Schulze C, Csont T, Lalu MM, Wildhirt SM, Schulz R. Enhanced NO and superoxide generation in dysfunctional hearts from endotoxemic rats. Am J Physiol Heart Circ Physiol. 2002; 283: H1108–H1115.
Hwang TL, Yeh CC. Hemodynamic and hepatic microcirculational changes in endotoxemic rats treated with different NOS inhibitors. Hepatogastroenterology.2003; 50: 188–191.
Ferdinandy P, Danial H, Ambrus I, Rothery RA, Schulz R. Peroxynitrite is a major contributor to cytokine-induced myocardial contractile failure. Circ Res. 2000;87: 241–247.
Connelly L, Madhani M, Hobbs AJ. Resistance to endotoxic shock in endothelial nitric-oxide synthase (eNOS) knock-out mice: a pro-inflammatory role for eNOS-derived NO in vivo. J Biol Chem. 2005; 280: 10040–10046.
Raeburn CD, Calkins CM, Zimmerman MA, Song Y, Ao L, Banerjee A, Harken AH, Meng X. ICAM-1 and VCAM-1 mediate endotoxemic myocardial dysfunction independent of neutrophil accumulation. Am J Physiol Regul Integr Comp Physiol.2002; 283: R477–R486.
Raeburn CD, Calkins CM, Zimmerman MA, Song Y, Ao L, Banerjee A, Meng X, Harken AH. Vascular cell adhesion molecule-1 expression is obligatory for endotoxin-induced myocardial neutrophil accumulation and contractile dysfunction.Surgery. 2001; 130: 319–325.
Hollenberg SM, Ahrens TS, Annane D, Astiz ME, Chalfin DB, Dasta JF, Heard SO, Martin C, Napolitano LM, Susla GM, Totaro R, Vincent JL, Zanotti-Cavazzoni S. Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update. Crit Care Med. 2004; 32: 1928–1948.
van der Poll T, Coyle SM, Barbosa K, Braxton CC, Lowry SF. Epinephrine inhibits tumor necrosis factor-alpha and potentiates interleukin 10 production during human endotoxemia. J Clin Invest. 1996; 97: 713–719.
van der Poll T, Levi M, Dentener M, Jansen PM, Coyle SM, Braxton CC, Buurman WA, Hack CE, ten Cate JW, Lowry SF. Epinephrine exerts anticoagulant effects during human endotoxemia. J Exp Med. 1997; 185: 1143–1148.
Lemaire L, de Kruif M, Giebelen IA, Levi M, van der Poll T, Heesen M. Dobutamine does not influence inflammatory pathways during human endotoxemia.Crit Care Med. 2006; 34: 1365–1371.
Leone M, Boyadjiev I, Boulos E, Antonini F, Visintini P, Albanese J, Martin C. A reappraisal of isoproterenol in goal-directed therapy of septic shock. Shock. 2006;26: 353–357.
Suzuki T, Morisaki H, Serita R, Yamamoto M, Kotake Y, Ishizaka A, Takeda J. Infusion of the beta-adrenergic blocker esmolol attenuates myocardial dysfunction in septic rats. Crit Care Med. 2005; 33: 2294–2301.
Bernard GR, Vincent JL, Laterre PF, LaRosa SP, Dhainaut JF, Lopez-Rodriguez A, Steingrub JS, Garber GE, Helterbrand JD, Ely EW, Fisher CJ Jr; Recombinant Human Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) Study Group. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med. 2001; 344: 699–709.
Tonelli M, Isles C, Craven T, Tonkin A, Pfeffer MA, Shepherd J, Sacks FM, Furberg C, Cobbe SM, Simes J, West M, Packard C, Curhan GC. Effect of pravastatin on rate of kidney function loss in people with or at risk for coronary disease. Circulation. 2005; 112: 171–178.
Fukuta H, Sane DC, Brucks S, Little WC. Statin therapy may be associated with lower mortality in patients with diastolic heart failure: a preliminary report.Circulation. 2005; 112: 357–363.
Zhang L, Zhang ZG, Ding GL, Jiang Q, Liu X, Meng H, Hozeska A, Zhang C, Li L, Morris D, Zhang RL, Lu M, Chopp M. Multitargeted effects of statin-enhanced thrombolytic therapy for stroke with recombinant human tissue-type plasminogen activator in the rat. Circulation. 2005; 112: 3486–3494.
Kurakata S, Kada M, Shimada Y, Komai T, Nomoto K. Effects of different inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase, pravastatin sodium and simvastatin, on sterol synthesis and immunological functions in human lymphocytes in vitro. Immunopharmacology. 1996; 34: 51–61.
Romano M, Diomede L, Sironi M, Massimiliano L, Sottocorno M, Polentarutti N, Guglielmotti A, Albani D, Bruno A, Fruscella P, Salmona M, Vecchi A, Pinza M, Mantovani A. Inhibition of monocyte chemotactic protein-1 synthesis by statins. Lab Invest. 2000; 80: 1095–1100.
Weber C, Erl W, Weber KS, Weber PC. HMG-CoA reductase inhibitors decrease CD11b expression and CD11b-dependent adhesion of monocytes to endothelium and reduce increased adhesiveness of monocytes isolated from patients with hypercholesterolemia. J Am Coll Cardiol. 1997; 30: 1212–1217.
Yoshida M, Sawada T, Ishii H, Gerszten RE, Rosenzweig A, Gimbrone MA Jr, Yasukochi Y, Numano F. HMG-CoA reductase inhibitor modulates monocyte-endothelial cell interaction under physiological flow conditions in vitro: involvement of Rho GTPase-dependent mechanism. Arterioscler Thromb Vasc Biol. 2001; 21:1165–1171.
Colli S, Eligini S, Lalli M, Camera M, Paoletti R, Tremoli E. Vastatins inhibit tissue factor in cultured human macrophages: a novel mechanism of protection against atherothrombosis. Arterioscler Thromb Vasc Biol. 1997; 17: 265–272.
Erkkila L, Jauhiainen M, Laitinen K, Haasio K, Tiirola T, Saikku P, Leinonen M. Effect of simvastatin, an established lipid-lowering drug, on pulmonary Chlamydia pneumoniae infection in mice. Antimicrob Agents Chemother. 2005; 49: 3959–3962.
del Real G, Jimenez-Baranda S, Mira E, Lacalle RA, Lucas P, Gomez-Mouton C, Alegret M, Pena JM, Rodriguez-Zapata M, Alvarez-Mon M, Martinez A, Manes S. Statins inhibit HIV-1 infection by down-regulating Rho activity. J Exp Med. 2004;200: 541–547.
Almog Y, Shefer A, Novack V, Maimon N, Barski L, Eizinger M, Friger M, Zeller L, Danon A. Prior statin therapy is associated with a decreased rate of severe sepsis. Circulation. 2004; 110: 880–885.
Hackam DG, Mamdani M, Li P, Redelmeier DA. Statins and sepsis in patients with cardiovascular disease: a population-based cohort analysis. Lancet. 2006; 367:413–418.
Panacek EA, Marshall JC, Alberson TE, Johnson DH, Johnson S, MacArthur RD, Miller M, Barchuk WT, Fischkoff S, Kaul M, Teoh L, Van Meter L, Daum L, Lemeshow S, Hicklin G, Doig C. Efficacy and safety of the monoclonal anti-tumor necrosis factor antibody F(ab′)2 fragment afelimomab in patients with severe sepsis and elevated interleukin-6 levels. Crit Care Med. 2004; 32: 2173–2182.
Zeiher BG, Steingrub J, Laterre PF, Dmitrienko A, Fukiishi Y, Abraham E; EZZI Study Group. LY315920NA/S-5920, a selective inhibitor of group IIA secretory phospholipase A2, fails to improve clinical outcome for patients with severe sepsis.Crit Care Med. 2005; 33: 1741–1748.
Grandel U, Hopf M, Buerke M, Hattar K, Heep M, Fink L, Bohle RM, Morath S, Hartung T, Pullamsetti S, Schermuly RT, Seeger W, Grimminger F, Sibelius U. Mechanisms of cardiac depression caused by lipoteichoic acids from Staphylococcus aureus in isolated rat hearts. Circulation. 2005; 112: 691–698.
Bernstein, HL, Pearlman, JD and A. Lev-Ari Alternative Designs for the Human Artificial Heart: The Patients in Heart Failure – Outcomes of Transplant (donor)/Implantation (artificial) and Monitoring Technologies for the Transplant/Implant Patient in the Community
Pearlman, JD and A. Lev-Ari 7/17/2013 Emerging Clinical Applications for Cardiac CT: Plaque Characterization, SPECT Functionality, Angiogram’s and Non-Invasive FFR
Lev-Ari, A. 7/14/2013 Vascular Surgery: International, Multispecialty Position Statement on Carotid Stenting, 2013 and Contributions of a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD
Lev-Ari, A. 7/9/2013 Heart Transplant (HT) Indication for Heart Failure (HF): Procedure Outcomes and Research on HF, HT @ Two Nation’s Leading HF & HT Centers
Pearlman, JD and A. Lev-Ari 7/4/2013 Fractional Flow Reserve (FFR) & Instantaneous wave-free ratio (iFR): An Evaluation of Catheterization Lab Tools (Software Validation) for Ischemic Assessment (Diagnostics) – Change in Paradigm: The RIGHT vessel not ALL vessels
Lev-Ari, A. 6/3/2013 Clinical Indications for Use of Inhaled Nitric Oxide (iNO) in the Adult Patient Market: Clinical Outcomes after Use, Therapy Demand and Cost of Care
Pearlman, JD and A. Lev-Ari 5/24/2013 Imaging Biomarker for Arterial Stiffness: Pathways in Pharmacotherapy for Hypertension and Hypercholesterolemia Management
Pearlman, JD and A. Lev-Ari 5/22/2013 Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone
Lev-Ari, A. 5/17/2013 Synthetic Biology: On Advanced Genome Interpretation for Gene Variants and Pathways: What is the Genetic Base of Atherosclerosis and Loss of Arterial Elasticity with Aging
Justin D Pearlman, HL Bernstein and A. Lev-Ari 5/15/2013 Diagnosis of Cardiovascular Disease, Treatment and Prevention: Current & Predicted Cost of Care and the Promise of Individualized Medicine Using Clinical Decision Support Systems
Pearlman, JD and A. Lev-Ari 5/7/2013 On Devices and On Algorithms: Arrhythmia after Cardiac Surgery Prediction and ECG Prediction of Paroxysmal Atrial Fibrillation Onset
Lev-Ari, A. 4/28/2013 Genetics of Conduction Disease: Atrioventricular (AV) Conduction Disease (block): Gene Mutations – Transcription, Excitability, and Energy Homeostasis
Lev-Ari, A. 4/25/2013 Economic Toll of Heart Failure in the US: Forecasting the Impact of Heart Failure in the United States – A Policy Statement From the American Heart Association
Lev-Ari, A. 4/4/2013 Hypertriglyceridemia concurrent Hyperlipidemia: Vertical Density Gradient Ultracentrifugation a Better Test to Prevent Undertreatment of High-Risk Cardiac Patients
Lev-Ari, A. 4/3/2013 Fight against Atherosclerotic Cardiovascular Disease: A Biologics not a Small Molecule – Recombinant Human lecithin-cholesterol acyltransferase (rhLCAT) attracted AstraZeneca to acquire AlphaCore
Lev-Ari, A. 3/31/2013 High-Density Lipoprotein (HDL): An Independent Predictor of Endothelial Function & Atherosclerosis, A Modulator, An Agonist, A Biomarker for Cardiovascular Risk
Lev-Ari, A. and L H Bernstein 3/7/2013 Genomics & Genetics of Cardiovascular Disease Diagnoses: A Literature Survey of AHA’s Circulation Cardiovascular Genetics, 3/2010 – 3/2013
Lev-Ari, A. 11/13/2012 Peroxisome proliferator-activated receptor (PPAR-gamma) Receptors Activation: PPARγ transrepression for Angiogenesis in Cardiovascular Disease and PPARγ transactivation for Treatment of Diabetes
Lev-Ari, A. 10/19/2012 Clinical Trials Results for Endothelin System: Pathophysiological role in Chronic Heart Failure, Acute Coronary Syndromes and MI – Marker of Disease Severity or Genetic Determination?
Lev-Ari, A. 10/4/2012 Inhibition of ET-1, ETA and ETA-ETB, Induction of NO production, stimulation of eNOS and Treatment Regime with PPAR-gamma agonists (TZD): cEPCs Endogenous Augmentation for Cardiovascular Risk Reduction – A Bibliography
Lev-Ari, A. 8/29/2012 Positioning a Therapeutic Concept for Endogenous Augmentation of cEPCs — Therapeutic Indications for Macrovascular Disease: Coronary, Cerebrovascular and Peripheral
Lev-Ari, A. 8/28/2012 Cardiovascular Outcomes: Function of circulating Endothelial Progenitor Cells (cEPCs): Exploring Pharmaco-therapy targeted at Endogenous Augmentation of cEPCs
Lev-Ari, A. 8/27/2012 Endothelial Dysfunction, Diminished Availability of cEPCs, Increasing CVD Risk for Macrovascular Disease – Therapeutic Potential of cEPCs
Lev-Ari, A. 8/24/2012 Vascular Medicine and Biology: CLASSIFICATION OF FAST ACTING THERAPY FOR PATIENTS AT HIGH RISK FOR MACROVASCULAR EVENTS Macrovascular Disease – Therapeutic Potential of cEPCs
Lev-Ari, A. 7/19/2012 Cardiovascular Disease (CVD) and the Role of agent alternatives in endothelial Nitric Oxide Synthase (eNOS) Activation and Nitric Oxide Production
Lev-Ari, A. 5/29/2012 Triple Antihypertensive Combination Therapy Significantly Lowers Blood Pressure in Hard-to-Treat Patients with Hypertension and Diabetes
Protein folding: amino-acid sequence of bovine BPTI (basic pancreatic trypsin inhibitor) in one-letter code, with its folded 3D structure represented by a stick model of the mainchain and sidechains (in gray), and the backbone and secondary structure by a ribbon colored blue to red from N- to C-terminus. 3D structure from PDB file 1BPI, visualized in Mage and rendered in Raster3D. (Photo credit: Wikipedia)
The Effects of Aprotinin on Endothelial Cell Coagulant Biology
Author: Demet Sag, PhD
The Effects of Aprotinin on Endothelial Cell Coagulant Biology
Demet Sag, PhD*†, Kamran Baig, MBBS, MRCS; James Jaggers, MD, Jeffrey H. Lawson, MD, PhD
Introduction: Cardiopulmonary bypass is associated with a systemic inflammatory response syndrome, which is responsible for excessive bleeding and multisystem dysfunction. Endothelial cell activation is a key pathophysiological process that underlies this response. Aprotinin, a serine protease inhibitor has been shown to be anti-inflammatory and also have significant hemostatic effects in patients undergoing CPB. We sought to investigate the effects of aprotinin at the endothelial cell level in terms of cytokine release (IL-6), tPA release, tissue factor expression, PAR1 + PAR2 expression and calcium mobilization. Methods: Cultured Human Umbilical Vein Endothelial Cells (HUVECS) were stimulated with TNFa for 24 hours and treated with and without aprotinin (200KIU/ml + 1600KIU/ml). IL-6 and tPA production was measured using ELISA. Cellular expression of Tissue Factor, PAR1 and PAR2 was measured using flow cytometry. Intracellular calcium mobilization following stimulation with PAR specific peptides and agonists (trypsin, thrombin, Human Factor VIIa, factor Xa) was measured using fluorometry with Fluo-3AM. Results: Aprotinin at the high dose (1600kIU/mL), 183.95 ± 13.06mg/mL but not low dose (200kIU/mL) significantly reduced IL-6 production from TNFa stimulated HUVECS (p=0.043). Aprotinin treatment of TNFa activated endothelial cells significantly reduce the amount of tPA released in a dose dependent manner (A200 p=0.0018, A1600 p=0.033). Aprotinin resulted in a significant downregulation of TF expression to baseline levels. At 24 hours, we found that aprotinin treatment of TNFa stimulated cells resulted in a significant downregulation of PAR-1 expression. Aprotinin significantly inhibited the effects of the protease thrombin upon PAR1 mediated calcium release. The effects of PAR2 stimulatory proteases such as human factor Xa, human factor VIIa and trypsin on calcium release was also inhibited by aprotinin. Conclusion: We have shown that aprotinin has direct anti-inflammatory effects on endothelial cell activation and these effects may be mediated through inhibition of proteolytic activation of PAR1 and PAR2. Abstract word count: 297
INTRODUCTION Each year it is estimated that 350,000 patients in the United States, and 650,000 worldwide undergo cardiopulmonary bypass (CPB). Despite advances in surgical techniques and perioperative management the morbidity and mortality of cardiac surgery related to the systemic inflammatory response syndrome(SIRS), especially in neonates is devastatingly significant. Cardiopulmonary bypass exerts an extreme challenge upon the haemostatic system as part of the systemic inflammatory syndrome predisposing to excessive bleeding as well as other multisystem dysfunction (1). Over the past decade major strides have been made in the understanding of the pathophysiology of the inflammatory response following CPB and the role of the vascular endothelium has emerged as critical in maintaining cardiovascular homeostasis (2).
CPB results in endothelial cell activation and initiation of coagulation via the Tissue Factor dependent pathway and consumption of important clotting factors. The major stimulus for thrombin generation during CPB has been shown to be through the tissue factor dependent pathway. As well as its effects on the fibrin and platelets thrombin has been found to play a role in a host of inflammatory responses in the vascular endothelium. The recent discovery of the Protease-Activated Receptors (PAR), one of which through which thrombin acts (PAR-1) has stimulated interest that they may provide a vital link between inflammation and coagulation (3).
Aprotinin is a nonspecific serine protease inhibitor that has been used for its ability to reduce blood loss and preserve platelet function during cardiac surgery procedures requiring cardiopulmonary bypass and thus the need for subsequent blood and blood product transfusions. However there have been concerns that aprotinin may be pro-thrombotic, especially in the context of coronary artery bypass grafting, which has limited its clinical use. These reservations are underlined by the fact that the mechanism of action of aprotinin has not been fully understood. Recently aprotinin has been shown to exert anti-thrombotic effects mediated by blocking the PAR-1 (4). Much less is known about its effects on endothelial cell activation, especially in terms of Tissue Factor but it has been proposed that aprotinin may also exert protective effects at the endothelial level via protease-activated receptors (PAR1 and PAR2). In this study we simulated in vitro the effects of endothelial cell activation during CPB by stimulating Human Umbilical Vein Endothelial Cells (HUVECs) with a proinflammatory cytokine released during CPB, Tumor Necrosis Factor (TNF-a) and characterize the effects of aprotinin treatment on TF expression, PAR1 and PAR2 expression, cytokine release IL-6 and tPA secretion. In order to investigate the mechanism of action of aprotinin we studied its effects on PAR activation by various agonists and ligands.
These experiments provide insight into the effects of aprotinin on endothelial related coagulation mechanisms in terms of Tissue Factor expression and indicate it effects are mediated through Protease-Activated Receptors (PAR), which are seven membrane spanning proteins called G-protein coupled receptors (GPCR), that link coagulant and inflammatory pathways. Therefore, in this study we examine the effects of aprotinin on the human endothelial cell coagulation biology by different-dose aprotinin, 200 and 1600units. The data demonstrates that aprotinin appears to directly alter endothelial expression of inflammatory cytokines, tPA and PAR receptor expression following treatment with TNF. The direct mechanism of action is unknown but may act via local protease inhibition directly on endothelial cells. It is hoped that with improved understanding of the mechanisms of action of aprotinin, especially an antithrombotic effect at the endothelial level the fears of prothrombotic tendency may be lessened and its use will become more routine.
METHODS Human Umbilical Vein Endothelial Cells (HUVECS) used as our model to study the effects of endothelial cell activation on coagulant biology. In order to simulate the effects of cardiopulmonary bypass at the endothelial cell interface we stimulated the cells with the proinflammatory cytokine TNFa. In the study group the HUVECs were pretreated with low (200kIU/mL) and high (1600kIU/mL) dosages of aprotinin prior to stimulation with TNFa and complement activation fragments. The effects of TNFa stimulation upon endothelial Tissue Factor expression, PAR1 and PAR2 expression, and tPA and IL6 secretion were determined and compared between control and aprotinin treated cells. In order to delineate whether aprotinin blocks PAR activation via its protease inhibition properties we directly activated PAR1 and PAR2 using specific agonist ligands such thrombin (PAR1), trypsin, Factor VIIa, Factor Xa (PAR2) in the absence and presence of aprotinin.
Endothelial Cell Culture HUVECs were supplied from Clonetics. The cells were grown in EBM-2 containing 2MV bullet kit, including 5% FBS, 100-IU/ml penicillin, 0.1mg/mL streptomycin, 2mmol/L L-glutamine, 10 U/ml heparin, 30µg/mL EC growth supplement (ECGS). Before the stimulation cells were starved in 0.1%BSA depleted with FBS and growth factors for 24 hours. Cells were sedimented at 210g for 10 minutes at 4C and then resuspended in culture media. The HUVECs to be used will be between 3 and 5 passages.
Assay of IL-6 and tPA production Levels of IL-6 were measured with an ELISA based kit (RDI, MN) according to the manufacturers instructions. tPA was measured using a similar kit (American Diagnostica).
Flow CytometryThe expression of transmembrane proteins PAR1, PAR2 and tissue factor were measured by single color assay as FITC labeling agent. Prepared suspension of cells disassociated trypsin free cell disassociation solution (Gibco) to be labeled. First well washed, and resuspended into “labeling buffer”, phosphate buffered saline (PBS) containing 0.5% BSA plus 0.1% NaN3, and 5% fetal bovine serum to block Fc and non-specific Ig binding sites. Followed by addition of 5mcl of antibody to approx. 1 million cells in 100µl labeling buffer and incubate at 4C for 1 hour. After washing the cells with 200µl with wash buffer, PBS + 0.1% BSA + 0.1% NaN3, the cells were pelletted at 1000rpm for 2 mins. Since the PAR1 and PAR2 were directly labeled with FITC these cells were fixed for later analysis by flow cytometry in 500µl PBS containing 1%BSA + 0.1% NaN3, then add equal volume of 4% formalin in PBS. For tissue factor raised in mouse as monoclonal primary antibody, the pellet resuspended and washed twice more as before, and incubated at 4C for 1 hour addition of 5µl donkey anti-mouse conjugated with FITC secondary antibody directly to the cell pellets at appropriate dilution in labeling buffer. After the final wash three times, the cell pellets were resuspended thoroughly in fixing solution. These fixed and labeled cells were then stored in the dark at 4C until there were analyzed. On analysis, scatter gating was used to avoid collecting data from debris and any dead cells. Logarithmic amplifiers for the fluorescence signal were used as this minimizes the effects of different sensitivities between machines for this type of data collection.
Intracellular Calcium Measurement
Measured the intracellular calcium mobilization by Fluo-3AM. HUVECs were grown in calcium and phenol free EBM basal media containing 2MV bullet kit. Then the cell cultures were starved with the same media by 0.1% BSA without FBS for 24 hour with or without TNFa stimulation presence or absence of aprotinin (200 and 1600KIU/ml). Next the cells were loaded with Fluo-3AM 5µg/ml containing agonists, PAR1 specific peptide SFLLRN-PAR1 inhibitor, PAR2 specific peptide SLIGKV-PAR2 inhibitor, human alpha thrombin, trypsin, factor VIIa, factor Xa for an hour at 37C in the incubation chamber. Finally the media was replaced by Flou-3AM free media and incubated for another 30 minutes in the incubation chamber. The readings were taken at fluoromatic bioplate reader. For comparison purposes readings were taken before and during Fluo-3AM loading as well.
RESULTSAprotinin reduces IL-6 production from activated/stimulated HUVECS The effects of aprotinin analyzed on HUVEC for the anti-inflammatory effects of aprotinin at cultured HUVECS with high and low doses. Figure 1 shows that TNF-a stimulated a considerable increase in IL-6 production, 370.95 ± 109.9 mg/mL. If the drug is used alone the decrease of IL-6 at the low dose is 50% that is 183.95 ng/ml and with the high dose of 20% that is 338.92 from 370.95ng/ml being compared value. TNFa-aprotinin results in reduction of the IL-6 expression from 370.95ng/ml to 58.6 (6.4fold) fro A200 and 75.85 (4.9 fold) ng/ml, for A1600. After the treatment the cells reach to the below baseline limit of IL-6 expression. Aprotinin at the high dose (1600kIU/mL), 183.95 ± 13.06mg/mL but not low dose (200kIU/mL) significantly reduced IL-6 production from TNF-a stimulated HUVECS (p=0.043). Therefore, the aprotinin prevents inflammation as well as loss of blood.
Aprotinin reduces tPA production from stimulated HUVECS Whether aprotinin exerted part of its fibrinolytic effects through inhibition of tPA mediated plasmin generation examined by the effects on TNFa stimulated HUVECS. Figure 2 also demonstrates that the amount of tPA released from HUVECS under resting, non-stimulated conditions incubated with aprotinin are significantly different. Figure 2 represents that the resting level of tPA released from non-stimulated cells significantly, by 100%, increase following TNF-a stimulation for 24 hours. After application of aprotinin alone at two doses the tPA level goes down 25% of TNFa stimulated cells. However, aprotinin treatment of TNF-a activated endothelial cells significantly lower the amount of tPA release in a dose dependent manner that is low dose decreased 25 but high dose causes 50% decrease of tPA expression (A200 p=0.0018, A1600 p=0.033) This finding suggests that aprotinin exerts a direct inhibitory effect on endothelial cell tPA production.
Aprotinin and receptor expression on activated HUVECS
TF is expressed when the cell in under stress such as TNFa treatments. The stimulated HUVECs with TNF-a tested for the expression of PAR1, PAR2, and tissue factor by single color flow cytometry through FITC labeled detection antibodies at 1, 3, and 24hs.
Tissue Factor expression is reduced:
Figure 3 demonstrates that there is a fluctuation of TF expression from 1 h to 24h that the TF decreases at first hour after aprotinin application 50% and 25%, A1600 and A200 respectively. Then at 3 h the expression come back up 50% more than the baseline. Finally, at 24h the expression of TF becomes almost as same as baseline. Moreover, TNFa stimulated cells remains 45% higher than baseline after at 3h as well as at 24h.
PAR1 decreased:
Figure 4 demonstrates that aprotinin reduces the PAR1 expression 80% at 24h but there is no affect at 1 and 3 h intervals for both doses.
During the treatment with aprotinin only high dose at 1 hour time interval decreases the PAR1 expression on the cells. This data explains that ECCB is affected due to the expression of PAR1 is lowered by the high dose of aprotinin.
PAR2 is decreased by aprotinin:
Figure 5 shows the high dose of aprotinin reduces the PAR2 expression close to 25% at 1h, 50% at 3h and none at 24h. This pattern is exact opposite of PAR1 expression. Figure 5 demonstrates the 50% decrease at 3h interval only. Does that mean aprotinin affecting the inflammation first and then coagulation?
This suggests that aprotinin may affect the PAR2 expression at early and switched to PAR1 reduction later time intervals. This fluctuation can be normal because aprotinin is not a specific inhibitor for proteases. This approach make the aprotinin work better the control bleeding and preventing the inflammation causing cytokine such as IL-6.
Aprotinin inhibits Calcium fluxes induced by PAR1/2 specific agonists
The specificity of aprotinin’s actions upon PAR studied the effects of the agent on calcium release following proteolytic and non-proteolytic stimulation of PAR1 and PAR2. Figure 6A (Figure 6) shows the stimulation of the cells with the PAR1 specific peptide (SFLLRN) results in release of calcium from the cells. Pretreatment of the cells with aprotinin has no significant effect on PAR1 peptide stimulated calcium release. This suggests that aprotinin has no effect upon the non-proteolytic direct activation of the PAR 1 receptor. Yet, Figure 6B (Figure 6) demonstrates human alpha thrombin does interact with the drug as a result the calcium release drops below base line after high dose (A1600) aprotinin used to zero but low dose does not show significant effect on calcium influx. Figure 7 demonstrates the direct PAR2 and indirect PAR2 stimulation by hFVIIa, hFXa, and trypsin of cells. Similarly, at Figure 7A aprotinin has no effect upon PAR2 peptide stimulated calcium release, however, at figures 7B, C, and D shows that PAR2 stimulatory proteases Human Factor Xa, Human Factor VIIa and Trypsin decreases calcium release. These findings indicate that aprotinin’s mechanism of action is directed towards inhibiting proteolytic cleavage and hence subsequent activation of the PAR1 and PAR2 receptor complexes. The binding site of the aprotinin on thrombin possibly is not the peptide sequence interacting with receptors.
Measurement of calcium concentration is essential to understand the mechanism of aprotinin on endothelial cell coagulation and inflammation because these mechanisms are tightly controlled by presence of calcium. For example, activation of PAR receptors cause activation of G protein q subunit that leads to phosphoinositol to secrete calcium from endoplasmic reticulum into cytoplasm or activation of DAG to affect Phospho Lipase C (PLC). In turn, certain calcium concentration will start the serial formation of chain reaction for coagulation. Therefore, treatment of the cells with specific factors, thrombin receptor activating peptides (TRAPs), human alpha thrombin, trypsin, human factor VIIa, and human factor Xa, would shed light into the effect of aprotinin on the formation of complexes for pro-coagulant activity. DISCUSSION There are two fold of outcomes to be overcome during cardiopulmonary bypass (CPB): mechanical stress and the contact of blood with artificial surfaces results in the activation of pro- and anticoagulant systems as well as the immune response leading to inflammation and systemic organ failure. This phenomenon causes the “postperfusion-syndrome”, with leukocytosis, increased capillary permeability, accumulation of interstitial fluid, and organ dysfunction. CPB is also associated with a significant inflammatory reaction, which has been related to complement activation, and release of various inflammatory mediators and proteolytic enzymes. CPB induces an inflammatory state characterized by tumor necrosis factor-alpha release. Aprotinin, a low molecular-weight peptide inhibitor of trypsin, kallikrein and plasmin has been proposed to influence whole body inflammatory response inhibiting kallikrein formation, complement activation and neutrophil activation (5, 6). But shown that aprotinin has no significant influence on the inflammatory reaction to CPB in men. Understanding the endothelial cell responses to injury is therefore central to appreciating the role that dysfunction plays in the preoperative, operative, and postoperative course of nearly all cardiovascular surgery patients. Whether aprotinin increases the risk of thrombotic complications remains controversial. The anti-inflammatory properties of aprotinin in attenuating the clinical manifestations of the systemic inflammatory response following cardiopulmonary bypass are well known(15) 16) However its mechanisms and targets of action are not fully understood. In this study we have investigated the actions of aprotinin at the endothelial cell level. Our experiments showed that aprotinin reduced TNF-a induced IL-6 release from cultured HUVECS. Thrombin mediates its effects through PAR-1 receptor and we found that aprotinin reduced the expression of PAR-1 on the surface of HUVECS after 24 hours incubation. We then demonstrated that aprotinin inhibited endothelial cell PAR proteolytic activation by thrombin (PAR-1), trypsin, factor VII and factor X (PAR-2) in terms of less release of Ca preventing the activation of coagulation. So aprotinin made cells produce less receptor, PAR1, PAR2, and TF as a result there would be less Ca++ release. Our findings provide evidence for anti-inflammatory as well as anti-coagulant properties of aprotinin at the endothelial cell level, which may be mediated through its inhibitory effects on proteolytic activation of PARs. IL6 Elevated levels of IL-6 have been shown to correlate with adverse outcomes following cardiac surgery in terms of cardiac dysfunction and impaired lung function(Hennein et al 1992). Cardiopulmonary bypass is associated with the release of the pro-inflammatory cytokines IL-6, IL-8 and TNF-a. IL-6 is produced by T-cells, endothelial cells as a result monocytes and plasma levels of this cytokine tend to increase during CPB (21, 22). In some studies aprotinin has been shown to reduce levels of IL-6 post CPB(23) Hill(5). Others have failed to demonstrate an inhibitory effect of aprotinin upon pro-inflammatory cytokines following CPB(24) (25). Our experiments showed that aprotinin significantly reduced the release of IL-6 from TNF-a stimulated endothelial cells, which may represent an important target of its anti-inflammatory properties. Its has been shown recently that activation of HUVEC by PAR-1 and PAR-2 agonists stimulates the production of IL-6(26). Hence it is possible that the effects of aprotinin in reducing IL-6 may be through targeting activation of such receptors. TPA Tissue Plasminogen activator is stored, ready made, in endothelial cells and it is released at its highest levels just after commencing CPB and again after protamine administration. The increased fibrinolytic activity associated with the release of tPA can be correlated to the excessive bleeding postoperatively. Thrombin is thought to be the major stimulus for release of t-PA from endothelial cells. Aprotinin’s haemostatic properties are due to direct inhibition of plasmin, thereby reducing fibrinolytic activity as well as inhibiting fibrin degradation. Aprotinin has not been shown to have any significant effect upon t-PA levels in patients post CPB(27), which would suggest that aprotinin reduced fibrinolytic effects are not the result of inhibition of t-PA mediated plasmin generation. Our study, however demonstrates that aprotinin inhibits the release of t-PA from activated endothelial cells, which may represent a further haemostatic mechanism at the endothelial cell level. TF Resting endothelial cells do not normally express tissue factor on their cell surface. Inflammatory mediators released during CPB such as complement (C5a), lipopolysaccharide, IL-6, IL-1, TNF-a, mitogens, adhesion molecules and hypoxia may induce the expression of tissue factor on endothelial cells and monocytes. The expression of TF on activated endothelial cells activates the extrinsic pathway of coagulation, ultimately resulting in the generation of thrombin and fibrin. Aprotinin has been shown to reduce the expression of TF on monocytes in a simulated cardiopulmonary bypass circuit (28).
We found that treatment of activated endothelial cells with aprotinin significantly reduced the expression of TF after 24 hours. This would be expected to result in reduced thrombin generation and represent an additional possible anticoagulant effect of aprotinin. In a previous study from our laboratory we demonstrated that there were two peaks of inducible TF activity on endothelial cells, one immediately post CPB and the second at 24 hours (29). The latter peak is thought to be responsible for a shift from the initial fibrinolytic state into a procoagulant state. In addition to its established early haemostatic and coagulant effect, aprotinin may also have a delayed anti-coagulant effect through its inhibition of TF mediated coagulation pathway. Hence its effects may counterbalance the haemostatic derangements, i.e. first bleeding then thrombosis caused by CPB. The anti-inflammatory effects of aprotinin may also be related to inhibition of TF and thrombin generation. PARs
It has been suggested that aprotinin may target PAR on other cells types, especially endothelial cells. We investigated the role of PARs in endothelial cell activation and whether they can be the targets for aprotinin. In recent study by Day group(30) demonstrated that endothelial cell activation by thrombin and downstream inflammatory responses can be inhibited by aprotinin in vitro through blockade of protease-activated receptor 1. Our results provide a new molecular basis to help explain the anti-inflammatory properties of aprotinin reported clinically. The finding that PAR-2 can also be activated by the coagulation enzymes factor VII and factor X indicates that PAR may represent the link between inflammation and coagulation. PAR-2 is believed to play an important role in inflammatory response. PAR-2 are widely expressed in the gastrointestinal tract, pancreas, kidney, liver, airway, prostrate, ovary, eye of endothelial, epithelial, smooth muscle cells, T-cells and neutrophils. Activation of PAR-2 in vivo has been shown to be involved in early inflammatory processes of leucocyte recruitment, rolling, and adherence, possibly through a mechanism involving platelet-activating factor (PAF) We investigated the effects of TNFa stimulation on PAR-1 and PAR-2 expression on endothelial cells. Through functional analysis of PAR-1 and PAR-2 by measuring intracellular calcium influx we have demonstrated that aprotinin blocks proteolytic cleavage of PAR-1 by thrombin and activation of PAR-2 by the proteases trypsin, factor VII and factor X. This confirms the previous findings on platelets of an endothelial anti-thrombotic effect through inhibition of proteolysis of PAR-1. In addition, part of aprotinin’s anti-inflammatory effects may be mediated by the inhibition of serine proteases that activate PAR-2. There have been conflicting reports regarding the regulation of PAR-1 expression by inflammatory mediators in cultured human endothelial cells. Poullis et al first showed that thrombin induced platelet aggregation was mediated by via the PAR-1(4) and demonstrated that aprotinin inhibited the serine protease thrombin and trypsin induced platelet aggregation. Aprotinin did not block PAR-1 activation by the non-proteolytic agonist peptide, SFLLRN indicating that the mechanism of action was directed towards inhibiting proteolytic cleavage of the receptor. Nysted et al showed that TNF did not affect mRNA and cell surface protein expression of PAR-1 (35), whereas Yan et al showed downregulation of PAR-1 mRNA levels (36). Once activated PAR1 and PAR2 are rapidly internalized and then transferred to lysosomes for degradation.
Endothelial cells contain large intracellular pools of preformed receptors that can replace the cleaved receptors over a period of approximately 2 hours, thus restoring the capacity of the cells to respond to thrombin. In this study we found that after 1-hour stimulation with TNF there was a significant upregulation in PAR-1 expression. However after 3 hours and 24 hours there was no significant change in PAR-1 expression suggesting that cleaved receptors had been internalized and replenished. Aprotinin was interestingly shown to downregulate PAR-1 expression on endothelial cells at 1 hour and increasingly more so after 24 hours TNF stimulation. These findings may suggest an effect of aprotinin on inhibiting intracellular cycling and synthesis of PAR-1.
Conclusions Our study has identified the anti-inflammatory and coagulant effects of aprotinin at the endothelial cell level. All together aprotinin affects the ECCB by reducing the t-PA, IL-6, PAR1, PAR 2, TF expressions. Our data correlates with the previous foundlings in production of tPA (7, (8) 9) 10), and decreased IL-6 levels (11) during coronary artery bypass graft surgery (12-14). We have importantly demonstrated that aprotinin may target proteolytic activation of endothelial cell associated PAR-1 to exert a possible anti-inflammatory effect. This evidence should lessen the concerns of a possible prothrombotic effect and increased incidence of graft occlusion in coronary artery bypass patients treated with aprotinin. Aprotinin may also inhibit PAR-2 proteolytic activation, which may represent a key mechanism for attenuating the inflammatory response at the critical endothelial cell level. Although aprotinin has always been known as a non-specific protease inhibitor we would suggest that there is growing evidence for a PAR-ticular mechanism of action.
REFERENCES
1. Levy, J. H., and Tanaka, K. A. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg. 75: S715-720, 2003.
2. Verrier, E. D., and Morgan, E. N. Endothelial response to cardiopulmonary bypass surgery. Ann Thorac Surg. 66: S17-19; discussion S25-18, 1998.
3. Cirino, G., Napoli, C., Bucci, M., and Cicala, C. Inflammation-coagulation network: are serine protease receptors the knot? Trends Pharmacol Sci. 21: 170-172, 2000. 4. Poullis, M., Manning, R., Laffan, M., Haskard, D. O., Taylor, K. M., and Landis, R. C. The antithrombotic effect of aprotinin: actions mediated via the proteaseactivated receptor 1. J Thorac Cardiovasc Surg. 120: 370-378, 2000.
5. Hill, G. E., Alonso, A., Spurzem, J. R., Stammers, A. H., and Robbins, R. A. Aprotinin and methylprednisolone equally blunt cardiopulmonary bypass-induced inflammation in humans. J Thorac Cardiovasc Surg. 110: 1658-1662, 1995.
6. Hill, G. E., Pohorecki, R., Alonso, A., Rennard, S. I., and Robbins, R. A. Aprotinin reduces interleukin-8 production and lung neutrophil accumulation after cardiopulmonary bypass. Anesth Analg. 83: 696-700, 1996. 7. Lu, H., Du Buit, C., Soria, J., Touchot, B., Chollet, B., Commin, P. L., Conseiller, C., Echter, E., and Soria, C. Postoperative hemostasis and fibrinolysis in patients undergoing cardiopulmonary bypass with or without aprotinin therapy. Thromb Haemost. 72: 438-443, 1994.
8. de Haan, J., and van Oeveren, W. Platelets and soluble fibrin promote plasminogen activation causing downregulation of platelet glycoprotein Ib/IX complexes: protection by aprotinin. Thromb Res. 92: 171-179, 1998.
9. Erhardtsen, E., Bregengaard, C., Hedner, U., Diness, V., Halkjaer, E., and Petersen, L. C. The effect of recombinant aprotinin on t-PA-induced bleeding in rats. Blood Coagul Fibrinolysis. 5: 707-712, 1994.
10. Orchard, M. A., Goodchild, C. S., Prentice, C. R., Davies, J. A., Benoit, S. E., Creighton-Kemsford, L. J., Gaffney, P. J., and Michelson, A. D. Aprotinin reduces cardiopulmonary bypass-induced blood loss and inhibits fibrinolysis without influencing platelets. Br J Haematol. 85: 533-541, 1993.
11. Tassani, P., Augustin, N., Barankay, A., Braun, S. L., Zaccaria, F., and Richter, J. A. High-dose aprotinin modulates the balance between proinflammatory and anti-inflammatory responses during coronary artery bypass graft surgery. J Cardiothorac Vasc Anesth.14: 682-686, 2000.
12. Asehnoune, K., Dehoux, M., Lecon-Malas, V., Toueg, M. L., Gonieaux, M. H., Omnes, L., Desmonts, J. M., Durand, G., and Philip, I. Differential effects of aprotinin and tranexamic acid on endotoxin desensitization of blood cells induced by circulation through an isolated extracorporeal circuit. J Cardiothorac Vasc Anesth. 16: 447-451, 2002.
13. Dehoux, M. S., Hernot, S., Asehnoune, K., Boutten, A., Paquin, S., Lecon-Malas, V., Toueg, M. L., Desmonts, J. M., Durand, G., and Philip, I. Cardiopulmonary bypass decreases cytokine production in lipopolysaccharide-stimulated whole blood cells: roles of interleukin-10 and the extracorporeal circuit. Crit Care Med. 28: 1721-1727, 2000.
14. Greilich, P. E., Brouse, C. F., Rinder, C. S., Smith, B. R., Sandoval, B. A., Rinder, H. M., Eberhart, R. C., and Jessen, M. E. Effects of epsilon-aminocaproic acid and aprotinin on leukocyte-platelet adhesion in patients undergoing cardiac surgery. Anesthesiology. 100: 225-233, 2004.
15. Mojcik, C. F., and Levy, J. H. Aprotinin and the systemic inflammatory response after cardiopulmonary bypass. Ann Thorac Surg. 71: 745-754, 2001.
16. Landis, R. C., Asimakopoulos, G., Poullis, M., Haskard, D. O., and Taylor, K. M. The antithrombotic and antiinflammatory mechanisms of action of aprotinin. Ann Thorac Surg. 72: 2169-2175, 2001.
17. Asimakopoulos, G., Kohn, A., Stefanou, D. C., Haskard, D. O., Landis, R. C., and Taylor, K. M. Leukocyte integrin expression in patients undergoing cardiopulmonary bypass. Ann Thorac Surg. 69: 1192-1197, 2000.
18. Landis, R. C., Asimakopoulos, G., Poullis, M., Thompson, R., Nourshargh, S., Haskard, D. O., and Taylor, K. M. Effect of aprotinin (trasylol) on the inflammatory and thrombotic complications of conventional cardiopulmonary bypass surgery. Heart Surg Forum. 4 Suppl 1: S35-39, 2001.
19. Asimakopoulos, G., Thompson, R., Nourshargh, S., Lidington, E. A., Mason, J. C., Ratnatunga, C. P., Haskard, D. O., Taylor, K. M., and Landis, R. C. An anti-inflammatory property of aprotinin detected at the level of leukocyte extravasation. J Thorac Cardiovasc Surg. 120: 361-369, 2000.
20. Asimakopoulos, G., Lidington, E. A., Mason, J., Haskard, D. O., Taylor, K. M., and Landis, R. C. Effect of aprotinin on endothelial cell activation. J Thorac Cardiovasc Surg. 122: 123-128, 2001.
21. Butler, J., Chong, G. L., Baigrie, R. J., Pillai, R., Westaby, S., and Rocker, G. M. Cytokine responses to cardiopulmonary bypass with membrane and bubble oxygenation. Ann Thorac Surg. 53: 833-838, 1992.
22. Hennein, H. A., Ebba, H., Rodriguez, J. L., Merrick, S. H., Keith, F. M., Bronstein, M. H., Leung, J. M., Mangano, D. T., Greenfield, L. J., and Rankin, J. S. Relationship of the proinflammatory cytokines to myocardial ischemia and dysfunction after uncomplicated coronary revascularization. J Thorac Cardiovasc Surg. 108: 626-635, 1994.
23. Diego, R. P., Mihalakakos, P. J., Hexum, T. D., and Hill, G. E. Methylprednisolone and full-dose aprotinin reduce reperfusion injury after cardiopulmonary bypass. J Cardiothorac Vasc Anesth. 11: 29-31, 1997.
24. Ashraf, S., Tian, Y., Cowan, D., Nair, U., Chatrath, R., Saunders, N. R., Watterson, K. G., and Martin, P. G. “Low-dose” aprotinin modifies hemostasis but not proinflammatory cytokine release. Ann Thorac Surg. 63: 68-73, 1997.
25. Schmartz, D., Tabardel, Y., Preiser, J. C., Barvais, L., d’Hollander, A., Duchateau, J., and Vincent, J. L. Does aprotinin influence the inflammatory response to cardiopulmonary bypass in patients? J Thorac Cardiovasc Surg. 125: 184-190, 2003.
26. Chi, L., Li, Y., Stehno-Bittel, L., Gao, J., Morrison, D. C., Stechschulte, D. J., and Dileepan, K. N. Interleukin-6 production by endothelial cells via stimulation of protease-activated receptors is amplified by endotoxin and tumor necrosis factor-alpha. J Interferon Cytokine Res. 21: 231-240, 2001.
27. Ray, M. J., and Marsh, N. A. Aprotinin reduces blood loss after cardiopulmonary bypass by direct inhibition of plasmin. Thromb Haemost. 78: 1021-1026, 1997.
28. Khan, M. M., Gikakis, N., Miyamoto, S., Rao, A. K., Cooper, S. L., Edmunds, L. H., Jr., and Colman, R. W. Aprotinin inhibits thrombin formation and monocyte tissue factor in simulated cardiopulmonary bypass. Ann Thorac Surg. 68: 473-478, 1999.
29. Jaggers, J. J., Neal, M. C., Smith, P. K., Ungerleider, R. M., and Lawson, J. H. Infant cardiopulmonary bypass: a procoagulant state. Ann Thorac Surg. 68: 513-520, 1999.
30. Day, J. R., Taylor, K. M., Lidington, E. A., Mason, J. C., Haskard, D. O., Randi, A. M., and Landis, R. C. Aprotinin inhibits proinflammatory activation of endothelial cells by thrombin through the protease-activated receptor 1. J Thorac Cardiovasc Surg. 131: 21-27, 2006.
31. Vergnolle, N. Proteinase-activated receptor-2-activating peptides induce leukocyte rolling, adhesion, and extravasation in vivo. J Immunol. 163: 5064-5069, 1999.
32. Vergnolle, N., Hollenberg, M. D., Sharkey, K. A., and Wallace, J. L. Characterization of the inflammatory response to proteinase-activated receptor-2 (PAR2)-activating peptides in the rat paw. Br J Pharmacol. 127: 1083-1090, 1999.
33. McLean, P. G., Aston, D., Sarkar, D., and Ahluwalia, A. Protease-activated receptor-2 activation causes EDHF-like coronary vasodilation: selective preservation in ischemia/reperfusion injury: involvement of lipoxygenase products, VR1 receptors, and C-fibers. Circ Res. 90: 465-472, 2002.
34. Maree, A., and Fitzgerald, D. PAR2 is partout and now in the heart. Circ Res. 90: 366-368, 2002.
35. Nystedt, S., Ramakrishnan, V., and Sundelin, J. The proteinase-activated receptor 2 is induced by inflammatory mediators in human endothelial cells. Comparison with the thrombin receptor. J Biol Chem. 271: 14910-14915, 1996.
36. Yan, W., Tiruppathi, C., Lum, H., Qiao, R., and Malik, A. B. Protein kinase C beta regulates heterologous desensitization of thrombin receptor (PAR-1) in endothelial cells. Am J Physiol. 274: C387-395, 1998.
37. Shinohara, T., Suzuki, K., Takada, K., Okada, M., and Ohsuzu, F. Regulation of proteinase-activated receptor 1 by inflammatory mediators in human vascular endothelial cells. Cytokine. 19: 66-75, 2002.
FIGURES
Figure 1: IL-6 production following TNF-a stimulation Figure 1
Figure 2: tPA production following TNF-a stimulation Figure 2
The voice of Series A Content Consultant, Justin D Pearlman, MD, PhD, FACC
The leading cause of death and disability from any cause is cardiovascular disease, principally, heart attacks and strokes. Both the heart and brain typically allow only 10 minutes or so of inadequate blood supply before starting a committed course of permanent tissue injury, progressing in severity as time goes by without successful interruption of the disease process. Thus there is great time urgency to get patients to a definitive treatment that can stop the injury and restore adequate nutrient blood supply. Many patients can benefit from a catheterization to identify blockages and insert a small balloon within the blockage to expand the narrow channel, often followed by placement of a stent (wire cage) to maintain the expanded vessel diameter. Chemicals released over time from drug-eluting stents can prevent tissue in growth that may obstruct stents. These emergeny interventions are not always successful. There may be complications from the attempt to access an entry artery, and the blockages may not be amenable to a balloon. When such limitations are encountered, the next chance to help is surgical, with continued time pressure.
The fastest way to make the transition from a diagnostic catheterization to a timely intervention is a hybrid intervention suite that offers non-invasive imaging, catheterization and surgery all in one location. The following articles present the current state of hybrid “do it all” intervention suites. Additional articles address the risks of bad outcomes from such interventions.
Part One
Hybrid Cath Lab/OR Suite for Hybrid Surgery
In ACC.10 and i2 Summit, 59th Annual Scientific Session, 3/14-3/16, 2010, Alfred A. Bove, M.D., Ph.D., F.A.C.C., ACC President addressed the conference attendees:
Welcome to the all-new Hybrid Cath Lab/OR and 3D CV Theater. Recent developments in cardiac surgery and interventional cardiology have led to the creation of integrated, hybrid cath lab/operating rooms (OR), which provide significant advantages in the diagnosis and treatment of patients requiring cardiac procedures—helping to facilitate a rapid-response approach. These multimodality rooms are designed to support a variety of integrated surgical and endovascular procedures. We are excited to provide you with this opportunity to get a first-hand look—and feel—of the latest technologies. We hope you take the time to explore this interactive, multivendor venue. Learning is at the core of the ACC Annual Scientific Session and we invite you to expand your educational experience in this dynamic learning environment.
In the Hybrid Cath Lab/OR Suite, you’ll discover how integrating cutting edge angiographic and surgical equipment and technologies can facilitate a broad range of procedures within one location. Additionally, you will learn how hybrid suites are providing solutions that enable interventionalists and surgeons to work collaboratively to provide the best treatment options for patients. The adjoining 3D CV Theater features presentations by physicians currently performing intravascular and surgical procedures in hybrid suites. Each live presentation pairs a cardiologist with a surgeon, allowing you to hear perspectives from both sides on a variety of hybrid suite procedures and cases. In addition, the Theater offers video presentations of cases from around the world.
The ACC thanks the supporters of the Hybrid Suite for providing us with the opportunity to share this unique learning destination with you.
are perfect examples of procedures that could, and should, be carried out in a hybrid OR. High-risk patients who require less invasive interventions are the best candidates for treatment in a hybrid suite.
As cardiac surgery becomes less invasive, incisions are becoming smaller and smaller, and even totally endoscopic heart surgery is now possible. Cardiac surgeons have started to perform procedures that include catheter-based skills, such as transapical valve replacement. For these operations, surgeons need more sophisticated imaging techniques, fluoroscopy and contrast injections. The hybrid OR offers all these facilities. Perhaps the most obvious and easiest procedure that can be performed in a hybrid OR is coronary revascularization combining coronary artery bypass grafting with on-table intra-operative completion angiography for quality control. If the surgeon detects a problem during the procedure, he or she can revise the graft immediately and thereby prevent potential perioperative and long-term complications. Currently, cardiologists and cardiovascular surgeons have shown special interest in so-called hybrid coronary interventions, which are combinations of minimally invasive coronary artery bypass grafting and percutaneous coronary interventions. In these procedures, cardiovascular surgeons place a left-internal mammary artery bypass graft to the left-anterior descending artery through small incisions (MIDCAB) or completely endoscopically (TECAB), while any remaining obstructed coronary arteries are treated with stents by an interventional cardiologist. This procedure is an attractive alternative to multivessel open coronary artery bypass grafting. Transcatheter heart-valve replacement and repair are especially suited to a hybrid suite because percutaneoustransfemoral and transapical aortic valve repairs include risks that can only be treated successfully by immediate surgical intervention, such as coronary artery obstruction, aortic dissection and aortic perforations.
In addition, endovascular aortic stent grafting for the repair of abdominal aortic aneurysms is a suitable procedure for a hybrid operating room. Endovascular aneurysm repair has become an established alternative to open repair and is increasingly used for thoracic aorta repair as well. Some
emergency procedures for traumatic lesions of the thoracic aorta and
fulminant pulmonary embolism may also be performed in a hybrid OR. Several
pediatric interventions can be carried out in a hybrid suite as well, such as implantation of closure devices for atrial and ventricular septal defects in small children and
In a recent article we reported on the Change in Requirement for Surgical Support by Cath Labs for performance of Nonemergent PCI without Surgical Backup, that increases the autonomy of Interventional Cardiologists. In the Hybrid OR that change is irrelevant since the presence of a Cardiac Surgeon is a fact of the division of labor between the two types of specialties. Cardiac Surgeons are involved with percutaneous transfemoral and transapical aortic valve repairs and intervention for endoscopic aorta, AAA and Thoracic AA grafting.
Cardiovascular hybrid suite is a state-of-the-art operating room equipped with a fully functional catheterization laboratory, thus allowing surgical procedures and catheter-based interventions to be carried out in the same room. Hybrid suites provide a place where treatments traditionally available only in a cath lab and procedures only available in an operating room can be performed together to provide patients with the best available combination of therapies for cardiovascular disease. These multidisciplinary, integrated cardiovascular procedural suites bring the best of two worlds together by combining all the advantages of a modern cath lab with an up-to-date cardiovascular surgery operating room (OR).
Hybrid suites began to evolve in the mid to late 1990s, when some groups of interventional cardiologists started sharing operating rooms with cardiovascular surgeons. The appeal of the hybrid suite concept has grown as have catheter based devices (stents, coils, balloons and lasers) have been developed that enable interventional cardiologists to advance the invasiveness and effectiveness and applications of percutaneous transcatheter interventions. The interest in these suites has also increased as cardiovascular surgeons have developed a variety of techniques for
Minimally invasive procedures, such as minimally invasive direct coronary artery bypass grafting (MIDCAB) or
With the advent of more tools, interventional cardiologists are becoming more like surgeons, and with less invasive tools, cardiovascular surgeons are becoming more like interventionalists. Rather than separating surgical procedures from interventional procedures performed in traditional operating rooms and cath labs, hybrid suites provide a high-tech environment that allows cardiologists and surgeons to work together to offer patients complex, minimally invasive therapies.
Some experts believe that hybrid suites represent the wave of the future in cardiovascular care and that most heart centers will eventually install hybrid suites to offer patients the latest cardiovascular procedures safely and effectively with minimal surgical trauma. The rooms can be costly to build and equip, but if a medical center is considering building a new operating room or cath lab, setting up a hybrid suite makes sense. Medical centers that have a hybrid suite available can clearly differentiate themselves in a positive way from centers that do not have such capabilities.
The Benefits of a Hybrid Suite for Medical Centers
While building a hybrid suite is more expensive than building a traditional operating room or cath lab, a hybrid suite can potentially be used for all types of cardiovascular procedures, including
traditional cardiac and vascular surgery,
interventional coronary procedures,
endovascular aortic procedures and
electrophysiology procedures.
Hybrid suites reinforce the trend in cardiovascular care toward less invasive, comprehensive hybrid procedures. Once a hybrid suite is in place, the demand for its use will likely grow due to increasing indications and referrals for these innovative treatments, many of which are increasingly covered by third-party payers.
Interventional cath labs usually have excellent imaging capabilities but lack the sterile facilities and staff needed for a formal OR, while operating rooms frequently lack high-level imaging equipment. Some of the essential equipment for a hybrid suite includes:
• A state-of-the-art imaging system capable of performing 3D rotational angiography, CT scanning, and ultrasound is advantageous. Floor-mounted and ceiling-mounted systems are available, but many hospitals use ceiling-mounted systems because access to the patient is slightly easier. Some ceiling-mounted systems provide 3D imaging from the surgeon’s position perpendicular to the patient. However, some hospitals prefer floor-mounted systems because having mechanical parts running above the operative field may cause dust to fall, resulting in infections. An important aspect is that the C-arm can be parked away when it is not used. This especially enhances access of the anesthesia team to the patient.
• An operating table that meets the needs of both surgeons and interventionalists by electronically integrating the table with the imaging system is also essential. These tables should have retractable rails for retractors and other surgical tools. To perform 3D imaging on the operating table, the C-arm of the imaging system should allow fast and precise rotation around the patient.
• A variety of other surgical and interventional systems and equipment may also be needed, including a robotic surgical system, a heart-lung machine, an image integration system, an endoscopic imaging system, a radiology display system, an audiovisual system to move images to different monitors and an anesthesia monitoring system, including transesophageal echocardiography. Some equipment like the integrated OR table and the angiography unit need to be fixed parts of the hybrid OR. Some equipment will be mobile in order to maintain some flexibility in workflow.
Philips is one of the world’s leading technology companies, with a long history of practical innovation and visionary design. In healthcare, we are committed to understanding the human and technological needs of patients and caregivers. We believe this understanding will help us deliver solutions that not only enable more confident diagnoses and more efficient delivery of care, but also improve the overall experience of care. We offer equipment, software and services for imaging, patient monitoring, resuscitation and much more. A Hybrid OR can help make life simpler for the interdisciplinary teams who operate in this environment every day. As a world leader in cardiovascular X-ray, Philips has the experience and expertise to deliver the first class technology you need to perform minimally invasive procedures with speed, accuracy and confidence. A long history of innovation has enabled Philips to develop pioneering imaging solutions that really make a difference.
For example, Philips Allura Xper cardiovascular X-ray systems are designed to deliver enhanced imaging with superb performance for all cardiac projections, and our iE33 ultrasound system with Live 3D TEE and QLAB can assist interventional procedures and provide comprehensive quantitative information to support critical decisions. Our cardiology informatics solutions help you manage patient information throughout the cardiovascular care continuum. Philips solutions allow minimally invasive and catheter-based procedures to take place in the same suite as conventional cardiac surgery.
Phillips EchoNavigator – X-Ray and 3-D Ultrasound is described in:
Intuitive Surgical, Inc. is the global technology leader in robotic-assisted, minimally invasive surgery. The company’s da Vinci® Surgical System offers breakthrough capabilities that enable cardiac surgeons to use a minimally invasive approach and avoid median sternotomy.
Content of FDA Warning Letter, following FDA Inspection on dates 04/01/2013 – 05/30/2013 – it discussed in
MAVIG’s specialty is ceiling/boom suspension systems for lighting (exam, surgical and LED), monitor-suspension systems—single, multibank (one to eight) systems and widescreen, overhead radiation shielding and contrast injector adapters. MAVIG also manufactures radiation protection products such as aprons, gloves, table-attachable lower body shields, adjustable- and fixed-height mobile and modular barriers.
Creating a hybrid lab may be complicated, but having an experienced partner that listens makes all the difference. Toshiba’s unique blend of hybrid experience and industry recognized Infinix™-i imaging systems for the Cath Lab.
Hybrid Cath Lab/OR Suite in Leading Hospitals in the US
The Hybrid Cath Lab/OR Suite at New York Presbyterian Hospital/Columbia University Medical Center, New York, NY is presented in
Speakers at 3D CV Theater, 2010 are working in Hospitals where Hybrid Cath Lab/OR Suite are in operations at the present time. The list include the following Hospitals with a Hybrid Cath Lab/OR Suite:
Vanderbilt Medical Center, Nashville, TN
University of Maryland Heart Center, Baltimore, MD
The Heart Center at Nationwide Children’s Hospital, Columbus, Ohio
The Robotic Surgical Center, East Carolina University Department of Surgery, Greenville, N.C.
University of Washington Medicine Regional Heart Center, Seattle, WA
Brigham and Women’s Hospital, Boston, MA
Saint Joseph’s Hospital and Peachtree Cardiovascular and Thoracic Surgery, Atlanta, GA
Emory University Hospital, Atlanta, GA
Beth Israel Deaconess Medical Center, Boston, MA
Boston Medical Center, Boston, MA
Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN
Lankenau Hospital, Lancaster, PA
Cardiac Non-Invasive Laboratory at Cedars-Sinai Medical Center, Los Angeles, CA
Robotic Surgery at St. Joseph’s Hospital, Atlanta, GA
Speakers at 3D CV Theater, 2010, included the following Cardiovascular Interventionists leading the adoption process of Hybrid Surgery in Hybrid Cath Lab/OR Suite into care modalities for cardiovascular disease:
Johannes O. Bonatti, M.D., is professor of surgery and director of coronary surgery and advanced coronary interventions at the University of Maryland Heart Center, Baltimore. He received his training in general surgery and cardiac surgery at the department of surgery at Innsbruck Medical University in Austria. Prior to his arrival at the University of Maryland, he worked at this institution as an attending surgeon and associate professor. Dr. Bonatti’s main interest is the development of minimally invasive, totally endoscopic coronary artery bypass grafting (TECAB) procedures using robotic technology.
As one of the international leaders in this field, he performed the largest series of robotic TECAB on the arrested heart, including single-, double- and triple-vessel TECAB. He has published significantly on procedure development and the implementation process of completely endoscopic coronary surgery using the da Vinci robotic system. Together with colleagues from interventional cardiology, Dr. Bonatti is working on integrated concepts for treatment of coronary artery disease. He was the first to perform a simultaneous hybrid coronary intervention using TECAB and placement of a coronary stent. He is organizing international meetings on hybrid interventions in cardiovascular medicine (http://www.icrworkshop.com). He has trained heart surgeons from around the world in the use of the da Vinci robot for heart surgery and he has introduced TECAB procedures in Austria, the Czech Republic, Greece, Turkey, India and Australia.
John G. Byrne, M.D., is the William S. Stoney Professor of Cardiac Surgery at Vanderbilt University School of Medicine and chair of the department of cardiac surgery at Vanderbilt Medical Center, Nashville, TN.
Before moving to Vanderbilt, he was associate chief and residency program director in the division of cardiac surgery at Brigham and Women’s Hospital, and associate professor of surgery at Harvard Medical School, Cambridge, MA. A graduate of the University of California, Davis, he received his medical degree in 1987 from Boston University. His postdoctoral training was completed at the University of Illinois affiliated hospitals and Brigham and Women’s Hospital in Boston.
Dr. Byrne is the author of more than 100 scientific articles on cardiac surgery and related areas. His patient care emphasis is
aortic root surgery,
coronary artery disease and
valve surgery
He is board-certified in general surgery and thoracic surgery.
John P. Cheatham, M.D., is director of cardiac catheterization and interventional therapy and codirector of The Heart Center at Nationwide Children’s Hospital, Columbus, Ohio. He is also the George H. Dunlap Endowed Chair in Interventional Cardiology and professor of pediatrics and internal medicine at The Ohio State University College of Medicine. Dr. Cheatham’s area of expertise is transcatheter intervention and hybrid therapy of newborns, children and adults with complex congenital heart disease. He has pioneered several new techniques and devices in non-surgical intervention and is a leader in developing hybrid therapies. He has been a principal investigator in numerous FDA-sponsored clinical trials evaluating non-surgical closure devices and stent therapy over the past two decades. Additionally, Dr. Cheatham designed the first hybrid cardiac catheterization suites and advanced imaging equipment at Nationwide Children’s Hospital. He serves as a consultant to various medical companies and proctors new transcatheter techniques and devices to other physicians around the world. Dr. Cheatham has implemented a formal physician exchange program with two of the leading medical institutions in China. In cooperation with China Red Cross, he is also the foreign director of the International Training Center for treatment of congenital heart disease in poor children. Dr. Cheatham has written more than 120 manuscripts, 16 book chapters, 300 national and international presentations and is co-editor of the book, Complications in Percutaneous Interventions for Congenital and Structural Heart Disease. After graduating from the University of Oklahoma College of Medicine, he completed his residency at Boston Children’s Hospital, followed by a fellowship in Pediatric Cardiology at Texas Children’s Hospital in Houston.
W. Randolph Chitwood, Jr., M.D., is senior associate vice chancellor for health sciences and chief of cardiovascular services at East Carolina University Department of Surgery, Greenville, N.C. Dr. Chitwood is a leading international pioneer in minimally invasive and robotic heart surgery. The Robotic Surgical Center at East Carolina University has trained more than 350 surgeons. His research activities relate to myocardial preservation, simulation in surgery and endoscopic/robotic cardiac surgery. He was the principal investigator of the FDA robotic mitral valve trials that led to approval for use in the U.S. He is the son and grandson of “southwestern Virginia mountain doctors” who set the guidelines for his professional life. He graduated from Hampden-Sydney College and received his medical degree from the University of Virginia. After medical school, he completed the surgical residency at Duke University Medical Center under David C. Sabiston, M.D., an influential surgical educator of the era. At Duke he spent 10 years training in general and cardiothoracic surgery, as well as basic science research.
After his chief residency at Duke in 1984, he was selected to begin and head the new cardiac surgery program at the East Carolina University School of Medicine. Because of his prolific publication record as a resident and clinical acumen, his initial appointment was as a full professor of surgery. Except for a two-year hiatus as the chief of cardiothoracic surgery at the University of Kentucky, he has spent his entire career at East Carolina University, where he also served as chairman of the department of surgery. In 2003, he was named to be in charge of the development of the East Carolina Heart Institute, which now includes an integrated department of cardiovascular sciences as well as a $200 million heart hospital, outpatient, research and education center.
Larry S. Dean, M.D., is director of the University of Washington Medicine Regional Heart Center and is professor of medicine and of surgery at the University of Washington School of Medicine, Seattle. In addition to general cardiology, he is an expert in cardiac catheterization and interventional cardiology. He also conducts research on stents to keep blocked heart arteries open and on ways to prevent restenosis after stents are inserted. He is currently involved in the evaluation of percutaneous aortic valve replacement. Dr. Dean earned his M.D. from the University of Alabama School of Medicine, Birmingham, and served his internship and residency at the University of Washington. He then returned to the University of Alabama Hospital for fellowships in cardiovascular disease and in angioplasty. After nearly 15 years as a faculty member at the University of Alabama, he returned to the University of Washington to direct the Regional Heart Center. He is a fellow of the American College of Cardiology and is board-certified in internal medicine, cardiovascular disease and interventional cardiology. He is also a fellow of the American Heart Association and president-elect of the Society of Cardiovascular Angiography and Interventions.
Andrew Craig Eisenhauer, M.D., is director of the interventional cardiovascular medicine service at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School. His specialties are
interventional cardiology,
vascular medicine and
congenital and inherited diseases.
He earned his medical degree at New York University School of Medicine and served a residency at Peter Bent Brigham Hospital and a fellowship at Massachusetts General Hospital. He is certified in internal medicine, cardiovascular disease and interventional cardiology. His clinical interests are
endovascular therapy,
complex coronary disease,
peripheral vascular disease,
cerebrovascular disease,
congenital heart disease and structural heart disease
Douglas A. Murphy, M.D., is chief of cardiothoracic surgery at Saint Joseph’s Hospital and a cardiothoracic surgeon at Peachtree Cardiovascular and Thoracic Surgery, Atlanta. His areas of interest are robotically assisted heart surgery with an emphasis on repairing the mitral valve rather than replacing it. A graduate of the University of Pennsylvania Medical School, Philadelphia, he served an internship and residency at Massachusetts General Hospital, Boston, and at Emory University, Atlanta.
Khusrow Niazi, M.D., is an assistant professor at Emory University School of Medicine and director of peripheral and carotid intervention at Emory University Hospital Midtown, Atlanta. He earned his medical degree at King Edward Medical College, Lahore, Pakistan, and served an internship at Kettering Medical Center, Dayton, Ohio, and a fellowship at William Beaumont Hospital, Royal Oak, MI. He has published papers on stenting following rotational atherectomy, small vessel stenting for coronary arteries, imaging of lower extremities and treatment of peripheral arterial disease.
Jeffrey J. Popma, M.D., is director of innovations in interventional cardiology, a senior attending physician at Beth Israel Deaconess Medical Center and an associate professor of medicine at Harvard Medical School in Boston. Dr. Popma received his bachelor’s degree in economics from Stanford University, and his M.D. from Indiana University School of Medicine. He completed his internship, residency, chief residency and fellowship at University of Texas Southwestern Medical Center. He also completed an interventional cardiology fellowship at the University of Michigan. Dr. Popma is the past president of the Society for Cardiac Angiography and Intervention and is the co-chair of the ACC Interventional Council. He sits on the editorial boards of several publications, and reviews for several cardiology periodicals. Dr. Popma has more than 300 published peer-reviewed manuscripts.
Dr. Popma also directs the BIDMC Angiographic Core Laboratory and is principal investigator for more than 65 ongoing multicenter device studies within the research laboratory. Over the past 15 years, these trials have included a broad array of new technology, including bare-metal stents, drug-eluting stents, distal-protection devices, total-occlusion devices and carotid and peripheral revascularization procedures. His primary clinical interest currently is the use of percutaneous aortic valve replacement for patients with high-risk aortic stenosis.
Robert S. Poston, M.D., is chief of cardiac surgery at Boston Medical Center and associate professor of cardiothoracic surgery at Boston University School of Medicine. He has a strong background in minimally invasive cardiac bypass surgery and is a pioneer in using robotics, specifically the da Vinci Surgical System, to treat coronary artery disease. A graduate of the Johns Hopkins School of Medicine, Baltimore, Dr. Poston completed a residency in general surgery at the University of California, San Francisco, and continued his training with a research fellowship in cardiothoracic surgery at Stanford University School of Medicine, Palo Alto, CA, and a cardiothoracic residency at the University of Pittsburgh Medical Center.
Charanjit S. Rihal, M.D., is professor of medicine and director of the cardiac catheterization laboratory at Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN. A graduate of the University of Winnipeg, Dr. Rihal did his residency and fellowship at the Mayo Graduate School of Medicine and also earned an MBA at the Carlson School of Management, University of Minnesota. His medical interests are interventional cardiology, structural heart disease interventions and the management of quality and costs in healthcare.
Timothy A. Shapiro, M.D., is director of the Interventional Cardiology Fellowship Program and campus chief, interventional cardiology, at Lankenau Hospital, Lancaster, PA. A graduate of Yale University School of Medicine, he served his residency and a fellowship at the Hospital of the University of Pennsylvania.
Robert J. Siegel, M.D., is director of the Cardiac Non-Invasive Laboratory at Cedars-Sinai Medical Center, cardiology director of the Cedars-Sinai Marfan Center, and Rexford S. Kennamer, M.D., chair in cardiac ultrasound at Cedars-Sinai Medical Center, Los Angeles. Dr. Siegel is also professor of medicine in residence at the David Geffen School of Medicine at University of California, Los Angeles. He previously served as senior staff fellow in cardiac pathology at the Heart, Lung and Blood Institute of the National Institutes of Health, Bethesda, MD. Internationally recognized as one of the leading experts in the field of cardiovascular ultrasound, Dr. Siegel specializes in cardiovascular ultrasound, including transthoracic, transesophageal and intravascular methodologies. His research interests include
valvular heart disease,
therapeutic applications of ultrasound energy,
transesophageal and intraoperative echocardiography, and the
development and use of hand-held portable echocardiographic systems for clinical innovations.
In addition, he is involved with clinical research studies related to the diagnosis, assessment and management of patients with
Marfan syndrome,
hypertrophic cardiomyopathy and
pericardial and valvular heart disease.
Dr. Siegel is a fellow, and has previously served as the president of the California Chapter of the American College of Cardiology and president of the Los Angeles Society of Echocardiography. He has been active in numerous cardiovascular societies, including the American Heart Association, the American College of Cardiology and the American Society of Echocardiography. Dr. Siegel received his medical degree at Baylor College of Medicine, Houston, where he developed an interest in cardiology. He completed his medical residency at Emory University and at Los Angeles County + USC Medical Center. He completed his cardiology fellowship at Harbor-UCLA Medical Center.
Over the last two years Dr. Siegel has worked extensively with live 3D transesophageal echo in the cardiac intervention center and the operating room. He and his echocardiologist colleagues, doctors Shiota, Biner, Tolstrup and Gurudevan, have worked closely at Cedars-Sinai Medical Center in Los Angeles with the interventional cardiologists, doctors Kar and Makkar, as well as with the cardiac surgeons, doctors Trento and Fontana. They use live 3D TEE extensively for the assessment of structural heart disease. In addition, it is used on a regular basis for the guidance of percutaneous procedures for mitral valve e-clip repair, mitral balloon valvuloplasty, aortic and pulmonic valve replacement, left atrial appendage exclusion by the Watchman device as well as for ASD closure.
Sudhir P. Srivastava, M.D., president of the International College of Robotic Surgery at St. Joseph’s Hospital, Atlanta, is a pioneer in performing beating heart totally endoscopic coronary artery bypass surgeries. Previously, he was assistant professor of surgery and director of robotic and minimally invasive cardiac surgery at the University of Chicago Medical Center. Dr. Srivastava specializes in robotically assisted totally endoscopic coronary artery bypass surgery. He has performed approximately 1,000 robotic cardiothoracic surgical procedures, of which 450 have been single- and multivessel beating heart totally endoscopic coronary bypass (BH TECAB) procedures. He has keen interest in hybrid coronary revascularization in TECAB patients to achieve complete revascularization.
Dr. Srivastava has helped launch robotic revascularization programs throughout the world. He has performed numerous live BH TECAB demonstrations both in the U.S. and abroad, and continues to be a presenter and invited speaker at numerous national and international scientific meetings. He earned his medical degree at the Jawahar Lal Nehru Medical College in Ajmer, India and immigrated to the U.S. in 1972. He completed his cardiothoracic surgery residency at the hospitals associated with the University of British Columbia, Vancouver, Canada.
Francis P. Sutter, D.O., F.A.C.S., is clinical professor of surgery at Thomas Jefferson University-Jefferson Medical College, Philadelphia, and chief of cardiothoracic surgery at Lankenau Hospital, Main Line Health System, Wynnewood, PA. A graduate of Philadelphia College of Osteopathic Medicine, his surgical residency and a cardiothoracic fellowship were completed at Thomas Jefferson University Hospital.
Mark R. Vesely, M.D., is an assistant professor of medicine at the University of Maryland School of Medicine. He completed medical school at the George Washington University and postgraduate training—an internal medicine residency and fellowships in cardiovascular disease and interventional cardiology—at the University of Maryland. He is board-certified in internal medicine, cardiovascular disease, nuclear cardiology and interventional cardiology. Dr. Vesely is the associate program director of the Interventional Cardiology fellowship at University of Maryland. His special interests include the partnered approach (interventional cardiologists and cardiac surgeons) for hybrid coronary revascularization and structural heart disease interventions. Additional research interests include investigation of techniques to minimize acute myocardial infarction injury with ventricular-assist devices and adult stem cell therapies.
David X. M. Zhao, M.D., Ph.D., is an associate professor of medicine and cardiac surgery, Harry and Shelley Page Chair in Interventional Cardiology, director of the Cardiac Catheterization Laboratories and interventional cardiology director of the Interventional Cardiology Fellowship Training Program, Vanderbilt University School of Medicine, Nashville, TN. He earned his medical degree at Shanghai Medical University, Shanghai, P.R. China, and his Ph.D. in immunology at Queensland University, Brisbane, Australia. His postdoctoral training was at Zhongshan Hospital, Shanghai Medical University, Shanghai, P.R. China, The Prince Charles Hospital, Brisbane, Australia, and Brigham and Women’s Hospital, Boston.
Cardiac Surgery @ Cleveland Clinic: Traditional OR & Hybrid Cath Lab/OR Suite
Nation #1 for 19 consecutive years – The Heart Center: Miller Family Heart & Vascular Institute @ Cleveland Clinic
The Sydell and Arnold Miller Family Heart & Vascular Institute is one of the largest, most experienced cardiovascular specialty groups in the world. Our physicians are committed to providing the most advanced diagnostic and treatment options, better outcomes and improved quality of life. U.S.News & World Reporthas ranked Cleveland Clinic as the No.1 heart program in America every year since 1995.
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Comparison of the 10-year and 15-year survivals after CABG demonstrated benefit from a change in graft sources used at the Mayo Clinic and widely adapted by others: vascular grafts from the left internal mammary artery (LIMA) instead of just leg veins, for multiple grafts (up to 3), LIMA-to-LAD plus grafts using LIMA or radial artery vs LIMA/saphenous vein (SV).
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part Three
Invasive Interventions with Complications
In the following article we covered multiple etiologies for cardiovascular complications related to invasive interventions: cardiovascular and peripheral arterial or peri- and post- cardiac surgery of the open heart type.
Cardiovascular Complications: Death from Reoperative Sternotomy after prior CABG, MVR, AVR, or Radiation; Complications of PCI; Sepsis from Cardiovascular Interventions
Justin D Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
This article covers types of Cardiovascular Complications derived from the following THREE types of assault on the Human body, two related to cardiac invasive interventions, the last due to its systemic nature is taking a fatal Cardiac toll: the Sepsis condition causing cardiac failure.
2. Surgical Complication of Non-cardiac surgery type causing cardiac arrest, i.e, Surgery of Joint Replacement causing sepsis causing death or death caused by complications of surgery i.e., blood loss, viral infection, emboli, thrombus, stroke, or cardiogenic shock not related to Cardiovascular and Cardiac invasive interventions
The e-Reader is advised to consider the following expansion on the subject matter carrying the discussion to additional related clinical issues:
Larry H Bernstein, Advanced Topics in Sepsis and the Cardiovascular System at its End Stage
Bernstein, HL, Pearlman, JD and A. Lev-Ari Alternative Designs for the Human Artificial Heart: The Patients in Heart Failure – Outcomes of Transplant (donor)/Implantation (artificial) and Monitoring Technologies for the Transplant/Implant Patient in the Community
Vascular Surgery: International, Multispecialty Position Statement on Carotid Stenting, 2013 and Contributions of a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD
Author and Curator: Aviva Lev-Ari, PhD, RN
Article ID #66: Vascular Surgery: International, Multispecialty Position Statement on Carotid Stenting, 2013 and Contributions of a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD. Published on 7/14/2013
WordCloud Image Produced by Adam Tubman
Part One:
Vascular Surgery International, Multispecialty Position Statement on Carotid Stenting, 2013
Part Two:
Contributions of a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD, Chief, Division of Vascular and Endovascular Surgery Co-Director, Thoracic Aortic Center @ MGH
I. Recollection of a visit at Dr. Cambria’s Office, 2004
II. Shadowing Dr. Cambria in OR @MGH
III. Dr. Cambria: Selection of Contributions to Scientific Research on Vascular Surgery
IV. Cardiovascular Clinical Observational Experience – Aviva Lev-Ari, PhD, RN
V. Cases with Complications: CEA and CAS
Part Three:
On 8/1/2013, Cleveland Clinic Reports Equivalence between carotid endarterectomy (CEA) and open-heart surgery (OHS) and carotid artery stenting (CAS) followed by coronary artery bypass graft (CABG) surgery or non-CABG cardiac surgery
Part One:
Vascular Surgery International, Multispecialty Position Statement on Carotid Stenting, 2013 Part
No other invasive intervention procedure in the history of Vascular Surgery has stormed the profession more than the two treatment options for carotid artery partial to complete blockage than Carotid endarterectomy (CEA) and Carotid angioplasty and stenting (CAS).
The debate required evidence based resolution for the two treatment options in terms of patient outcomes and adverse events. As the title of the Position statement explained below, the verdict is non equivocal: Routine Carotid Stenting is inferior to Carotid endarterectomy (CEA) from a patient safety and outcomes.
In conclusion, current global evidence shows that, even in the best academic centers, CAS is less effective (causing more strokes) and more expensive than CEA. It is premature that some guidelines have recently added support for routine practice CAS as an alternative to CEA for
asymptomatic43,44 and
low/ average surgical risk symptomatic patients43–45
because CAS may easily be misinterpreted by readers as being equivalent for
stroke prevention46 and
historical procedural standards were cited.
CAS, for these patients, should still only be performed and paid for within well‐designed, adequately powered trials. The US Center for Medicare and Medicaid Services is doing its job and setting an excellent global example. It is protecting Medicare beneficiaries from routine practice procedures, which are currently more likely to harm them and waste finite resources47 that could be used for their advantage. Meanwhile, we need to reassess the current routine practice role of CEA and deliver optimal current medical treatment to all who need it.
Clinical Trials Results
To avoid misguidance from calls for more routine practice (nontrial) carotid angioplasty/stenting (CAS), we need to distinguish relevant facts and patients’ best interests from all else (distractions). A recent editorial by White and Jaff1 is one publication which illustrates this need particularly well. First, these authors are correct in reminding us that the responsibility of physicians is to provide best patient care, putting aside personal interest. This is inherent in any profession.2 However, misconception, bias, and conflict of interest exist. Therefore, healthcare payment organizations, such as the US Center for Medicare and Medicaid Services are important gatekeepers to facilitate patient access to interventions that are likely to help them, as opposed to all others.
It is also true that CAS and carotid endarterectomy (CEA) result in better outcomes when patients are carefully selected and skilled operators perform the procedures in experienced centers.1 We would add that key indicators (such as 30‐day periprocedural stroke/death rates) must be accurately measured in routine (real‐world) practice, particularly as stroke and death rates here may be unacceptably higher than in trials. 3–5 Therefore, it is most appropriate, as suggested by White and Jaff,1 that coverage for carotid procedures be dependent on facility accreditation and audited measurement of key standards indicators in all practices performing these procedures.
This is a priority issue. White and Jaff1 also correctly state “a major change in evidence based stroke prevention strategies will require clinical trial data.,7,8 meta‐analyses, and routine practice.9–14 Most of these data relate to low/average risk symptomatic patients and demonstrate that, for these patients, even in the best academic centers, CAS is consistently associated with significantly higher rates of stroke or death (during or after the periprocedural period) compared with CEA.
It is incorrect that CREST “failed to show a difference in overall stroke rate between CAS and CEA” as stated by White and Jaff.1 In CREST, for average surgical risk symptomatic patients, the periprocedural stroke and death rates were 6.0% for CAS versus 3.2% for CEA (hazard ratio, 1.89; 95% confidence interval, 1.11–3.21; P=0.02).8
The higher periprocedural risk of stroke or death with CAS is particularly evident in the most senior patients (>68–70 years),13,15,16 those undergoing the procedure <7 days of incident cerebral or retinal ischemic symptoms17 (when CEA has the highest stroke prevention potential),18 those undergoing CAS outside clinical trials,19 and those with certain anatomic features.20 No study has shown that CAS is more effective than CEA in preventing stroke. Further, most analyses show that CAS costs considerably more,21–24 despite calculations derived from CREST results.25 No randomized trial has been adequately powered to compare the procedural and longer term risk of CAS on stroke or death in low/average risk asymptomatic patients. However, in CREST, the direction of effect was toward nearly twice the risk (periprocedural stroke/death rate was 2.5% for CAS versus 1.4% for CEA; hazard ratio, 1.88; 95% confidence interval, 0.79–4.42; P=0.15).8 This was consistent with the significantly higher periprocedural stroke rates seen in CREST CAS‐treated symptomatic patients8 and nontrial CAS‐treated asymptomatic patients.9,26
Meanwhile, medical treatment for asymptomatic carotid disease has improved significantly since past randomized trials of medical treatment alone versus additional CEA.27–32 Medical treatment consists of identification of risk factors for heart and vascular disease and risk reduction using healthy lifestyles and appropriate drugs. Improvement in medical treatment is clear from robust analyses of all published comparable, quality stroke rate calculations (including from, and within, randomized surgical trials) of patients with 50% to 99% asymptomatic carotid stenosis. This knowledge is not, as claimed by White and Jaff,1 derived from short‐cut extrapolation from coronary artery trials. Using the same standardized rate calculations, we are now seeing an average annual rate of ipsilateral stroke of ≈0.5% with medical treatment alone.30,33,34 This is about 3X— lower than that of asymptomatic CREST CAS‐treated patients and about half the rate of asymptomatic CREST CEA‐treated patients.7,9 This low rate with medical treatment is likely to fall further with improvements in efficacy, definition, and implementation.
However, recently published rate calculations indicate that, at most, only ≈2.5% of low/average CEA risk patients with 50% to 99% asymptomatic carotid stenosis will receive a stroke prevention benefit from CEA or CAS during their remaining average 10‐year lifetime if they receive good, current medical treatment (assuming the procedural risk of stroke/death is always zero).35 This indicates that a one‐size‐fits‐all procedural approach for these asymptomatic patients is now unlikely to be beneficial overall. We need to be much more selective. Research is required to determine which asymptomatic subgroups now benefit from carotid procedures in addition to current optimal medical treatment.
We have found no direct information about the influence of current medical treatment in patients with low/average CEA risk symptomatic carotid stenosis. However, improving results for medically treated asymptomatic patients27–32 and procedural trial asymptomatic and symptomatic patients8 indicate that a 6% periprocedural risk of
stroke or
death (the current standard) is now too high.
New randomized and risk stratification studies are required using current optimal medical treatment and procedural methods.36 For example,
improved plaque37 and
thrombus identification38 or
embolic signal detection39 above and below the stenosis
may help better identify carotid plaques responsible for carotid territory ischemic symptoms. Further, the best approach for patients with high surgical risk carotid stenosis remains uncertain because risk of stroke or death has not been measured with any standard of medical treatment or adequate procedural trials. However, some registries show significantly higher risks of stroke/death with CAS compared with CEA in asymptomatic and symptomatic high surgical risk patients.40
Incidence of MI
Calls from other authors for more routine CAS on the grounds of lower periprocedural myocardial infarction (MI) rates compared with CEA are distracting.41 MI is not a measure of stroke prevention efficacy, even though it is an important procedural complication. The inclusion of periprocedural MI with stroke and death in the primary outcome measure in CREST resulted in primary outcome equivalence between CAS and CEA. However, it did not result in efficacy equivalence. In CREST, 1.1% (14/1262) of CAS patients had periprocedural clinical MI (biomarkers plus chest pain/ECG evidence) compared with 2.3% (28/1240) of CEA patients7 (P=0.03). However, periprocedural stroke was nearly twice as common (81/2502; 3.2%)7 as periprocedural clinical MI (42/2502; 1.7%) and, as mentioned above, CAS caused almost twice as many of these strokes as CEA.Further, in CREST, the mortality rate up to 4 years was equally poor for CREST patients with periprocedural stroke (20%),42 periprocedural clinical MI (19%),41 or periprocedural biomarker‐positive only MI (25%).41 Finally, nonfatal stroke was associated with a poorer quality of life at 1 year than nonfatal MI.7 Therefore, MI is a measure of carotid procedural risk (not benefit) and must be considered separately from stroke risk. Moreover, in CREST, CAS‐associated stroke was more troublesome for patients than CEA‐associated MI.
Conclusion
Calls for More Routine Carotid Stenting Are Currently Inappropriate, 3/2013
Carotid artery disease, also called carotid artery stenosis, occurs when the carotid arteries, the main blood vessels that carry oxygenated blood to the brain, become narrowed. The narrowing of the carotid arteries is most commonly related to atherosclerosis (a buildup of plaque, which is a deposit of fatty substances, cholesterol, cellular waste products, calcium, and fibrin in the inner lining of an artery). Atherosclerosis, or “hardening of the arteries,” is a vascular disease (disease of the arteries and veins). Carotid artery disease is similar to coronary artery disease, in which blockages occur in the arteries of the heart, and may cause a heart attack.
Click Image to Enlarge
To better understand how carotid artery disease affects the brain, a basic review of the anatomy of the circulation system of the brain follows.
What are the carotid arteries?
The main supply of blood to the brain is carried by the carotid arteries. The carotid arteries branch off from the aorta (the largest artery in the body) a short distance from the heart, and extend upward through the neck carrying oxygen-rich blood to the brain.
There are four carotid arteries: the right and left internal carotid arteries and the right and left external carotid arteries. One pair (external and internal) is located on each side of the neck. Just as a pulse can be felt in the wrists, a pulse can also be felt on either side of the neck over the carotid arteries.
Click to Enlarge
Why are the carotid arteries important?
Because the carotid arteries deliver blood to the brain, carotid artery disease can have serious implications by reducing the flow of oxygen to the brain. The brain needs a constant supply of oxygen in order to function. Even a brief interruption in blood supply can cause problems. Brain cells begin to die after just a few minutes without blood or oxygen. If the narrowing of the carotid arteries becomes severe enough to block blood flow, or a piece of atherosclerotic plaque breaks off and obstructs blood flow to the brain, a stroke may occur.
What causes carotid artery disease?
Atherosclerosis is the most common cause of carotid artery disease. It is unknown exactly how atherosclerosis begins or what causes it. Atherosclerosis is a slow, progressive, vascular disease that starts as early as childhood. However, the disease has the potential to progress rapidly. It is generally characterized by the accumulation of fatty deposits along the innermost layer of the arteries. If the disease process progresses, plaque formation may take place. Plaque is made up of deposits of smooth muscle cells, fatty substances, cholesterol, calcium, and cellular waste products. This thickening narrows the arteries and can decrease blood flow or completely block the flow of blood to the brain.
Risk factors associated with atherosclerosis include:
Older age
Male
Family history
Race or ethnicity
Genetic factors
Hyperlipidemia (elevated fats in the blood)
Hypertension (high blood pressure)
Smoking
Diabetes
Obesity
Diet high in saturated fat
Lack of exercise
A risk factor is anything that may directly increase or be associated with a person’s chance of developing a disease. It may be an activity, such as smoking, diet, family history, or many other things. Different diseases have different risk factors.
Although these risk factors increase a person’s risk, they do not necessarily cause the disease. Some people with one or more risk factors never develop the disease, while others develop disease and have no known risk factors. Knowing your risk factors to any disease can help to guide you into the appropriate actions, including changing behaviors and being clinically monitored for the disease.
What are the symptoms of carotid artery disease?
Carotid artery disease may be asymptomatic (without symptoms) or symptomatic (with symptoms). Asymptomatic carotid disease is the presence of a significant amount of atherosclerotic buildup without obstructing enough blood flow to cause symptoms. However, a sufficiently tight stenosis will not always cause symptoms. Symptomatic carotid artery disease may result in either a transient ischemic attack (TIA) and/or a stroke (brain attack).
A transient ischemic attack (TIA) is a sudden or temporary loss of blood flow to an area of the brain, usually lasting a few minutes to one hour. Symptoms go away entirely within 24 hours, with complete recovery. Symptoms of a TIA may include, but are not limited to, the following:
Sudden weakness or clumsiness of an arm and/or leg on one side of the body
Sudden paralysis (inability to move) of an arm and/or leg on one side of the body
Loss of coordination or movement
Confusion, decreased ability to concentrate, dizziness, fainting, and/or headache
Numbness or loss of sensation (feeling) in the face
Numbness or loss of sensation in an arm and/or leg
Temporary loss of vision or blurred vision
Inability to speak clearly or slurred speech
TIA may be related to severe narrowing or blockage or from small pieces of an atherosclerotic plaque breaking off, traveling through the bloodstream, and lodging in small blood vessels in the brain. With TIA, there is rarely permanent brain damage.
Call for medical help immediately if you suspect a person is having a TIA, as it may be a warning sign that a stroke is about to occur. Not all strokes, however, are preceded by TIAs.
Stroke is another indicator of carotid artery disease. The symptoms of a stroke are the same as for a TIA. A stroke is loss of blood flow (ischemia) to the brain that continues long enough to cause permanent brain damage. Brain cells begin to die after just a few minutes without oxygen. The area of dead cells in tissues is called an infarct.
The area of the brain that suffered the loss of blood flow will determine what the physical or mental disability may be. This may include impaired ability with movement, speech, thinking and memory, bowel and bladder function, eating, emotional control, and other vital body functions. Recovery from the specific ability affected depends on the size and location of the stroke. A stroke may result in problems, such as weakness in an arm or leg or may cause paralysis, loss of speech, or even death.
The symptoms of carotid artery disease may resemble other medical conditions or problems. Always consult your doctor for a diagnosis.
How is carotid artery disease diagnosed?
In addition to a complete medical history and physical examination, diagnostic procedures for carotid artery disease may include any, or a combination, of the following:
Auscultation (listening to) of carotid arteries. Placement of a stethoscope over the carotid artery to listen for a particular sound called a bruit (pronounced brew-ee). A bruit is an abnormal sound that is produced by blood passing through a narrowed artery. A bruit is generally considered a sign of an atherosclerotic artery; however, an artery may be diseased without producing this sound.
Carotid artery duplex scan. A type of vascular ultrasound study performed to assess the blood flow of the carotid arteries. A carotid artery duplex scan is a noninvasive (the skin is not pierced) procedure. A probe called a transducer sends out ultrasonic sound waves at a frequency too high to be heard. When the transducer (like a microphone) is placed on the carotid arteries at certain locations and angles, the ultrasonic sound waves move through the skin and other body tissues to the blood vessels, where the waves echo off of the blood cells. The transducer picks up the reflected waves and sends them to an amplifier, which makes the ultrasonic sound waves audible. Absence or faintness of these sounds may indicate an obstruction to the blood flow.
Magnetic resonance imaging (MRI). A diagnostic procedure that uses a combination of large magnets, radiofrequencies, and a computer to produce detailed images of organs and structures within the body. To have this test done, you lie inside a big tube while magnets pass around your body. It is very loud. Sometimes it is done with IV contrast injected into your veins and sometimes not.
Magnetic resonance angiography (MRA). A noninvasive diagnostic procedure that uses a combination of magnetic resonance technology (MRI) and intravenous (IV) contrast dye to visualize blood vessels. Contrast dye causes blood vessels to appear opaque on the MRI image, allowing the doctor to visualize the blood vessels being evaluated.
Computed tomography scan (also called a CT or CAT scan). A diagnostic imaging procedure that uses a combination of X-rays and computer technology to produce horizontal, or axial, images (often called slices) of the body. A CT scan shows detailed images of any part of the body, including the bones, muscles, fat, and organs. CT scans are more detailed than general X-rays. Like an MRI, it is sometimes done with IV contrast injected into your veins and sometimes not.
Angiography. An invasive procedure used to assess the degree of blockage or narrowing of the carotid arteries by taking X-ray images while a contrast dye in injected. The contrast dye helps to visualize the shape and flow of blood through the arteries as X-ray images are made.
Treatment for carotid artery disease
Specific treatment for carotid artery disease will be determined by your doctor based on:
Your age, overall health, and medical history
Extent of the disease
Your signs and symptoms
Your tolerance of specific medications, procedures, or therapies
Expectations for the course of the disease
Your opinion or preference
Carotid artery disease (asymptomatic or symptomatic) in which the narrowing of the carotid artery is less than 50 percent is most often treated medically. Asymptomatic disease with less than 70 percent narrowing may also be treated medically, depending on the individual situation.
Medical treatment for carotid artery disease may include:
Modification of risk factors. Risk factors that may be modified include smoking, elevated cholesterol levels, elevated blood glucose levels, lack of exercise, poor dietary habits, and elevated blood pressure.
Medications. Medications that may be used to treat carotid artery disease include:
Antiplatelet medications. Medications used to decrease the ability of platelets in the blood to stick together and cause clots. Aspirin, clopidogrel, and dipyridamole are examples of antiplatelet medications.
Antihyperlipidemics. Medications used to lower lipids (fats) in the blood, particularly cholesterol. Statins are a group of antihyperlipidemic medications, and include simvastatin, atorvastatin, and pravastatin, among others. Studies have shown that certain statins can decrease the thickness of the carotid artery wall and increase the size of the lumen (opening) of the artery.
Antihypertensives. Medications used to lower blood pressure. There are several different groups of medications which act in different ways to lower blood pressure.
In people with narrowing of the carotid artery greater than 50 to 69 percent, a more aggressive treatment may be recommended, particularly in people with symptoms. Surgical treatment decreases the risk for stroke after symptoms such as TIA or minor stroke, especially in people with an occlusion (blockage) of more than 70 percent who are good candidates for surgery.
Surgical treatment of carotid artery disease includes:
Carotid endarterectomy (CEA). Carotid endarterectomy is a procedure used to remove plaque and clots from the carotid arteries, located in the neck. Endarterectomy may help prevent a stroke from occurring in people with symptoms with a carotid artery narrowing of 70 percent of more.
Illustration of Carotid Endarterectomy (Click to Enlarge)
Carotid artery angioplasty with stenting (CAS). Carotid angioplasty with stenting is an option for patients who are high risk for carotid endarterectomy. This is a minimally invasive procedure in which a very small hollow tube, or catheter, is advanced from a blood vessel in the groin to the carotid arteries. Once the catheter is in place, a balloon may be inflated to open the artery and a stent is placed. A stent is a cylinder-like tube made of thin metal-mesh framework used to hold the artery open. Because there is a risk of stroke from bits of plaque breaking off during the procedure, an apparatus, called an embolic protection device, may be used. An embolic protection device is a filter (like a small basket) that is attached on a guidewire to catch any debris that may break off during the procedure.
Carotid Artery Angioplasty with Stenting (CAS) Click to Enlarge
Carotid Artery Disease and Stroke: Prevention and Treatment – John Hopkins
VIEW VIDEO –
Carotid Endarterectomy with Temporary Bypass – A Fifty year old procedure
Docteur Jean VALLA
Chirurgien Cardiovasculaire et Thoracique
AIHR/ACCA – Ancien Chirurgien des Hôpitaux Universitaires.
Membre de la Société de Chirurgie Thoracique et Cardiovasculaire de Langue Française Conventionné
Carotid artery stenosis is the narrowing of the carotid arteries. These are the main arteries in the neck that supply blood to the brain. Carotid artery stenosis, also called carotid artery disease, is a major risk factor for ischemic stroke.The narrowing is usually caused by plaque in a blood vessel. Plaque forms when cholesterol, fat and other substances build up in the inner lining of an artery.Depending on the degree of stenosis and the patient’s overall condition, carotid artery stenosis can usually be treated with surgery. The procedure is called carotid endarterectomy. It removes the plaque that caused the carotid artery to narrow. Carotid endarterectomy has proven to benefit patients with arteries stenosed (narrowed) by 70 percent or more. For people with arteries narrowed less than 50 percent, anti-clotting medicine is usually prescribed to reduce the risk of ischemic stroke.
VIEW VIDEO –
Carotid angioplasty and stenting (CAS) – Mayo Clinic
In carotid angioplasty and stenting, a long hollow tube called a catheter is inserted in the femoral artery in the groin area. The catheter is then maneuvered through the arteries until it reaches the narrowing in the carotid artery in the neck. An umbrella-shaped filter is inserted beyond the narrowing to catch any plaque or debris that may break off during the procedure. Then, a tiny balloon at the end of the catheter is inflated to push the plaque to the side and widen the vessel. A small metal coil called a stent is inserted into the vessel. The stent serves as a scaffold to help prevent the artery from narrowing again.
Contributions of a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD, Chief, Division of Vascular and Endovascular Surgery Co-Director, Thoracic Aortic Center @ MGH
I. Recollection of a visit at Dr. Cambria’s Office @MGH, 2004
The author arrived for a 4PM appointment @ MGH with a referral from NWH for a Carotid artery duplex scan that in 2004 was not performed at NWH. The consultation appointment with Dr. Kwolek CJ, a vascular surgeon trained under Dr. RP Cambria, took place in Dr. Cambria’s Office. Few minutes into the patient Medical History interview, Dr. Kwolek was called for an emergency in the OR and asked me to wait for him till he comes back. I looked around and found myself in a 14’x22′ Room, the Office of Dr. Richard Cambria @ MGH, Chief Vascular Surgery and among the Top ten in the World. Except for the glass entrance door and the wide window to the right of the entrance – 3 1/2 walls from the ceiling to one yard above the floor where completely covered with framed Awards, licenses, renewed licenses, Pictures with graduating Medical Students, Pictures with Faculty, with Patients and in the OR. I waited for Dr. Kwolek’s return for the completion of my Medical History Interview about 30 minutes. I used that time to walk along the walls in Dr. Cambria’s Office and read the framed Exhibits. It was clear to me that this Office will need, one day, in the future, to become a Museum @MGH, for most significant milestones in Vascular Surgery, a branch of Cardiothoracic Surgery. Dr. Kwolek returned and completed the interview, scheduled my Lab appointment and the next appointment to discuss the duplex scan results.
II. Shadowing Dr. Cambria in OR @MGH
Per section IV, below which described the author’s Cardiovascular Clinical Observational Experience, I recorded my Shadowing experience at the OR @MGH, including Dr. Cambria performing a CEA on a 84 year old women under going aorta valve replacement (performed by Dr. Walker) priot to a CEA performed by Dr. Cambria. It was all captivating to watch his double gloved hands performing sutures on a >95% blocked carotid artery prior to incision.
The dexterity and the speed of Dr. Cambria’s fingers’ movement, could only have reminded me of World #1 Harp Player: Nicanor Zabaleta, which I met in person, in the presence of my prominent Harp teacher, on his US Tour in 11/1989. He was awarded the Premio Nacional de Música of Spain in 1982 and six years later, in 1988, he was elected to the Real Academia de Bellas Artes de San Fernando. Dr. Cambria’s and Mr. Zabaleta’s fingers dexterity and eye hand coordination, both are of the rarest endowments in fine motor precision and perfection with Worldly finest outcomes in art, Surgery is Art, the mastering of the Harp is Art, too.
The Author in the OR — Mass General Hospital, Boston
Cardiac Surgery – Operating Room
Supervisor: Dr. J. Walker, Cardiac Surgeon
Experience: Shadowing Open Heart Surgery at MGH
1/24/2005: Carotid Artery endarterectomy operation by Dr. Richard Cambria
1/24/2005: Mitral Valve Replacement by Dr. Jennifer Walker
1/26/2005: Aorta Valve Replacement and Coronary Artery Bypass Grafting by Dr. Jennifer Walker
[Saphenous vein harvested from the leg and Radial vein harvested from the right arm]
III. Dr. Cambria: Selection of Contributions to Scientific Research on Vascular Surgery
The Author covered In Part One, Dr. Cambria’s participation in and contribution to the International, Multispecialty Position Statement on Carotid Stenting, 2013.
In Part Two Section II, I share with the e-Reader watching Dr. Cambria in the Surgical Theater performing CEA
In Part Two Section III, I am carrying with me the heavy weight of my Recollections from a Visit to his Office in 2004, my experience shadowing Dr. Cambria in the OR @MGH on 1/24/2005. Now I am giving back.
I became aware that both events have impacted favorably my 7/2013, Editorial decision, for a forthcoming book on Cardiovascular Disease in 2013. The Editorial decision is two fold:
the selection and representation of a prominent Vascular Surgery Center in the US, @MGH, and
my personal decision to select a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD @MGH.
The decision to focus on Peripheral Vascular Surgery @MGH as described in Dr. Richard P Cambria’s research had yielded one Sub-Chapter (5.5) in Chapter 5
Chapter 5
Invasive Procedures by Surgery versus Catheterization
in Volume Three in a forthcoming three volume Series of e-Books on Cardiovascular Diseases
This very Sub-Chapter, 5.5, represents milestones in Dr. Cambria as a Vascular Surgeon. His eminent profile as a Vascular Surgery Researcher, is now in:
IV. Cardiovascular Clinical Observational Experience – Aviva Lev-Ari, PhD, RN
Brigham and Women’s Hospital, Boston. MA
Cardiac ICU, Coronary Care Unit, Medical Rounds [100 hours] June 2006-November 2006
Brigham and Women’s Hospital, Boston. MA
CDIC – Cardiovascular Diagnostic and Interventional Center
Angiography & Interventional Radiology [100 hours] March 2006-August 2006
Experience shadowing the daily activities of three Physician Assistants
1. attended consultation appointments with patient candidate for procedures: fibroid embolization
2. patient candidate for intra-vertebral cement injection in fractured vertebrae in spinal column, L-9 – Kyphoplasty vertebral augmentation
3. drainage of bile leakage – biliary duct obstruction
4. attended invasive procedures in the Angiography Lab
5. attended 7:30AM department meeting on all cases scheduled for procedures in the Lab for the day
6. discussed procedure outcomes and patient follow ups with PAs
7. Shadowing PAs and Interventional Radiologists performing angiography.
– VENOUS ACCESS PROCEDURES – TUNNELED CATHETER AND PORT PLACEMENT
– DIALYSIS ACCESS MANAGEMENT – ARTERIOVENOUS FISTULA/GRAFT.
ANGIOGRAMS/ANGIOPLASTIES
Mass General Hospital, Boston
Cardiac Catheterization Lab
Supervisor: Dr. Igor Palacios, Director, Cath Lab
Experience Shadowing in the Cath Lab at MGH
1/19/2005: stenting – MI case, mitral valve opening with balloon
The cerebral hyperperfusion syndrome is a very rare complication after revascularization of the carotid artery and accompanied by postoperative or postinterventional hypertension in almost all patients. We report a case of a 77-year-old man who developed a complete aphasia and increased right-sided weakness following endovascular treatment of severe occlusive disease of the left internal carotid artery. We discuss the risk and management of cerebral hyperperfusion syndrome after carotid artery stenting.
Introduction
Neurological complications following carotid artery stenting (CAS) are usually ischemic in nature, due to embolization or occlusion of the carotid artery. However, in a small subset of patients, cerebral hyperperfusion causes postinterventional neurological dysfunction, characterized by ipsilateral headache, focal seizure activity, focal neurological deficit, and ipsilateral intracerebral edema or hemorrhage. A high clinical suspicion and early diagnosis will allow early initiation of therapy and preventing fatal brain swelling or bleeding in patients with peri- and postinterventional cerebral hyperperfusion syndrome (CHS).
Discussion
In 1981, Sundt et al. [1] described a triad of complications that included atypical migrainous phenomena, transient focal seizure activity, and intracerebral hemorrhage after CEA and used the term cerebral hyperperfusion syndrome (CHS). The first report on CHS after CAS was published by Schoser et al. [2]. They described a 59-year-old woman with ipsilateral putaminal hemorrhage that was diagnosed on the 3rd day after CAS of a high-grade stenosis of the left ICA. Outcome in this case was not fatal. The patient recovered with a mild upper limb paresis. McCabe et al. [3] were the first to report the occurrence of fatal ICH soon after CAS. Only a few hours after the procedure, neurological symptoms occurred without any prodromata (severe headache, nausea, and seizures) postulated by Sundt et al. [1] to be an obligate component of CHS. CT of the brain revealed extensive ICH and the patient died 18 days later. Abou-Chebl et al. [4] reported a retrospective single-center study on 450 patients who had been treated with CAS. Three patients (0.67%) developed ICH after the intervention. Further reports on results and complications after CAS have been published [5]. Nearly all reports on CHS after carotid revascularizations in general and CAS in particular have in common patients who had high-grade stenoses in the treated vessel.
CHS following surgical or endovascular treatment of severe carotid occlusive disease is thought to be the result of impaired cerebral autoregulation, hypertension, ischemia-reperfusion injury, oxygen-derived free radicals, baroreceptor-dysfunction, and intraprocedural ischemia [6]. Chronic cerebral hypoperfusion due to critical stenosis leads to production of vasodilatory substances. Autoregulatory failure results in the cerebral arterioles being maximally dilated over a long period of time, with subsequent loss of their ability to constrict when normal perfusion pressure is restored. The degree of microvascular dysautoregulation is proportional to the duration and severity of ischemia determined by the severity of ipsilateral stenosis and poor collateral flow.
Hypertension plays an important role in the development of CHS. In the absence of cerebral autoregulation, cerebral blood flow is directly dependent on the systemic blood pressure. The restoration of normal blood flow to chronically underperfused brain can result in edema, capillary breakthrough, and perivascular and macroscopic hemorrhages aggravated by peri- and postinterventional hypertension [6, 7]. The risk factors for CHS after CAS are summarized in Table 1.
The classic clinical presentation includes ipsilateral headache, seizures or focal neurological deficit, and ipsilateral intracerebral edema or hemorrhage. The diagnosis can be made readily with color Doppler ultrasound of the carotid artery and especially with transcranial Doppler (TCD) of the middle cerebral artery [9]. An increase in peak blood flow velocity of >100% is predictive of postinterventional hyperperfusion. Diffusion weighted MRI or single photon emission computed tomography (SPECT) could also be performed for diagnosis [10]. Angiography normally shows normal findings.
The prognosis of CHS depends on timely recognition of hyperperfusion and adequate treatment of hypertension before cerebral edema or hemorrhage develops. The prognosis following intracerebral bleeding is very poor, with mortality over 50% and significant morbidity of 80% in the survivors [4, 6]. The prognosis of CHS in patients without cerebral edema or hemorrhage is clearly better especially when they are identified and treated early. The most important aspects in preventing and treating this syndrome are early identification, careful monitoring, and control of blood pressure ideally in a high-dependency unit setting. In our special case, early diagnosis of CHS and immediate intensive medical treatment of blood pressure could prevent devastating cerebral edema or hemorrhage following CAS.
Conclusion
CHS, which is characterized by ipsilateral headache, hypertension, seizures, and focal neurological deficits, is a rare but devastating complication following carotid artery stenting. Hypertension is the most important risk factor. The diagnosis can be confirmed quickly by TCD, DWI, or SPECT. Especially peri- or postinterventional TCD monitoring should be available to identify patients with hyperperfusion who may benefit from intensive blood pressure management ideally in a specialized intensive care unit.
Abbreviations
CAS:
Carotid artery stenting
CCA:
Common carotid artery
CEA:
Carotid endarterectomy
CHS:
Cerebral hyperperfusion syndrome
CT:
Computed tomography
CVR:
Cerebrovascular reactivity
DWI:
Diffusion-weighted imaging
ICA:
Internal carotid artery
ICH:
Intracerebral haemorrhage
MRI:
Magnetic resonance imaging
SPECT:
Single photon emission computed tomography
TCD:
Transcranial Doppler.
REFERENCES
T. M. Sundt Jr., F. W. Sharbrough, and D. G. Piepgras, “Correlation of cerebral blood flow and electroencephalographic changes during carotid endarterectomy. With results of surgery and hemodynamics of cerebral ischemia,” Mayo Clinic Proceedings, vol. 56, no. 9, pp. 533–543, 1981.View at Scopus
B. G. H. Schoser, C. Heesen, B. Eckert, and A. Thie, “Cerebral hyperperfusion injury after percutaneous transluminal angioplasty of extracranial arteries,” Journal of Neurology, vol. 244, no. 2, pp. 101–104, 1997. View at Publisher · View at Google Scholar · View at Scopus
D. J. H. McCabe, M. M. Brown, and A. Clifton, “Fatal cerebral reperfusion hemorrhage after carotid stenting,” Stroke, vol. 30, no. 11, pp. 2483–2486, 1999. View at Scopus
A. Abou-Chebl, J. S. Yadav, J. P. Reginelli, C. Bajzer, D. Bhatt, and D. W. Krieger, “Intracranial hemorrhage and hyperperfusion syndrome following carotid artery stenting: risk factors, prevention, and treatment,” Journal of the American College of Cardiology, vol. 43, no. 9, pp. 1596–1601, 2004. View at Publisher · View at Google Scholar · View at Scopus
J.-H. Buhk, L. Cepek, and M. Knauth, “Hyperacute intracerebral hemorrhage complicating carotid stenting should be distinguished from hyperperfusion syndrome,” American Journal of Neuroradiology, vol. 27, no. 7, pp. 1508–1513, 2006. View at Scopus
W. F. Morrish, S. Grahovac, A. Douen et al., “Intracranial hemorrhage after stenting and angioplasty of extracranial carotid stenosis,” American Journal of Neuroradiology, vol. 21, no. 10, pp. 1911–1916, 2000. View at Scopus
R. Gupta, A. Abou-Chebl, C. T. Bajzer, H. C. Schumacher, and J. S. Yadav, “Rate, predictors, and consequences of hemodynamic depression after carotid artery stenting,” Journal of the American College of Cardiology, vol. 47, no. 8, pp. 1538–1543, 2006. View at Publisher · View at Google Scholar · View at Scopus
M. B. Sánchez-Arjona, G. Sanz-Fernández, E. Franco-Macias, and A. Gil-Peralta, “Cerebral hemodynamic changes after carotid angioplasty and stenting,” American Journal of Neuroradiology, vol. 28, pp. 640–644, 2007.
Y. Kaku, S. I. Yoshimura, and J. Kokuzawa, “Factors predictive of cerebral hyperperfusion after carotid angioplasty and stent placement,” American Journal of Neuroradiology, vol. 25, pp. 1403–1408, 2004.
Patient came to her appointment as part of a standard pre-operative evaluation for removal of a uterine myoma. She had a history of stroke with residual slurred speech, making it difficult to understand her. Accordingly, I assumed I would see some carotid stenosis, but her ultrasound showed a stunning 70-99% stenosis in her right internal carotid artery and full occlusion of her left internal carotid artery.
Flow in the common carotid arteries looked fine. The plaque itself in the internal carotid arteries was relatively hypoechoic and not easily visualized in brightness mode, so bidirectional color flow at the proximal internal carotid arteries was surprising. Adding power Doppler allowed me to conclude that there was presence of flow on the right, though minimal, and absolutely no flow in the left internal carotid artery.
Upon completion of the exam, I called the ER and spoke with the doctor, who asked me to bring Rose to the ER. Unfortunately, due to the location of the right internal carotid artery stenosis in the bony canal and total occlusion of the left internal carotid artery, surgery was not an option for clearing out the carotid plaque, but doctors believed she could continue functioning well with collateral vasculature carrying blood to her brain.
Thankfully, the patient passed her other pre-operative tests, consented to her surgery, and underwent general anesthesia with no complications. An 8-cm malignant mass was removed from her uterus and her prognosis is good.
opinion/26redberg.html. Last accessed Jan 8, 2013.
Part Three:
Cleveland Clinic Reports Equivalence between carotid endarterectomy (CEA) and open-heart surgery (OHS) and carotid artery stenting (CAS) followed by coronary artery bypass graft (CABG) surgery or non-CABG cardiac surgery
Stent first, then heart surgery, for patients with severe carotid/coronary disease
Cleveland, OH – With the absence of randomized, controlled clinical trials to address the optimal management of patients with severe carotid and coronary artery disease, a new retrospective study suggests the best tactic is a staged approach that sees the patient undergo carotid artery stenting (CAS) followed by coronary artery bypass graft (CABG) surgery or non-CABG cardiac surgery [1].
Investigators report that a combined approach that includes carotid endarterectomy (CEA) and open-heart surgery (OHS) is equivalent in terms of short-term outcomes with the staged CAS-OHS procedure. Beyond one year, however, the staged CAS-OHS approach resulted in the lowest risk of all-cause mortality, stroke, and MI when compared with a combined CEA-OHS procedure and staged CEA-OHS.
“The surgeons get very worried about doing operations on these patients because they don’t want to do a beautiful job on the bypass only to have the patient have a stroke,” lead investigator Dr Mehdi Shishehbor(Cleveland Clinic, OH) told heartwire.
Shishehbor said that when patients are undergoing open-heart surgery, whether it’s CABG or valve surgery, they are screened for carotid artery disease, given the heightened risk of stroke when undergoing heart surgery. As a result, various teams from neurology, vascular surgery, and interventional cardiology are called to address the safety of the surgery in the setting of severe carotid disease, said Shishehbor.
“These patients are the sickest of the sick in the sense that they have two conditions that are occurring concomitantly,” he said. “These are not patients who just have carotid disease. There are many patients who have moderate or mild carotid disease who undergo open-heart surgery with no problem. These are people with severe disease, those with more than 80% stenosis in one of their carotid arteries or maybe both. They also have severe coronary artery disease. These are people with left-main or three-vessel disease who are destined to undergo bypass.”
The whole point is to prevent stroke
In the study, published this week in the Journal of the American College Cardiology, the investigators reported data on 350 patients who underwent carotid revascularization and cardiac surgery. These included 45 patients who were treated with a staged CEA-OHS approach (OHS performed a median of 14 days after CEA), 110 who were treated with a staged CAS-OHS procedure (OHS performed a median of 47 days after CEA), and 195 patients treated with a combined CEA-OHS procedure. OHS is defined as CABG, CABG plus other cardiac procedures, or non-CABG cardiac surgery (isolated valve or aortic-repair surgery). In total, just 8% of procedures were non-CABG surgeries.
In a propensity-adjusted analysis analyzed by intention-to-treat, the 30-day risk of death, stroke, and MI was similar between the staged CAS-OHS and combined CEA-OHS procedures. The highest risk of the composite end point was observed in patients who underwent staged CEA-OHS.
At one year and beyond (median follow-up was 3.7 years), the staged CAS-OHS patients had the lowest risk of death, stroke, and MI. Compared with staged CEA-OHS, those treated with CAS-OHS had a 67% lower risk of death, stroke, and MI and a 65% lower risk compared with combined CEA-OHS.
Unadjusted comparison of primary/secondary end points
Event
Staged CEA-OHS,n=45 (%)
Combined CEA-OHS,n=195 (%)
Staged CAS-OHS,n=110 (%)
p
Overall 30-d risk post-OHS
31
10
10
0.003
Death
7
5
6
0.75
Stroke
2
7
2
0.11
MI
24
0.5
3
<0.001
Overall composite risk 1 y and beyond
27
39
12
<0.001
Death
38
39
11
<0.001
Stroke
2.2
1.5
0
0.37
MI
0
3.1
2.7
0.5
“In the long term, stenting [followed by OHS] definitely did better than the combined approach,” said Shishehbor. “What’s also important is that with the combined approach, the reason they didn’t do very well is because they had a higher rate of stroke in the perioperative period. . . . Remember the whole point of doing this is to prevent stroke. This is why we feel the combined approach is a little bit inferior to the staged CAS/open-heart-surgery approach. If you have a 7% risk of stroke in the 30-day perioperative period, that doesn’t appear to be the best option for the majority of patients.”
To heartwire, Shishehbor said that while the patients were well matched, the patients undergoing stenting tended to be sicker. For example, they were more likely to have symptomatic carotid stenosis and were more likely to have undergone a previous carotid revascularization. Shishehbor also said that clinical events occurring between the initial carotid artery revascularization procedure and OHS were included in the analysis. These deaths, strokes, and MIs were identified and accounted for in the data.
In an editorial accompanying the study [2], Drs Ehtisham Mahmud and Ryan Reeves (University of California, San Diego) say the work by the Cleveland Clinic group is strengthened by the propensity-adjusted analysis and long follow-up beyond the perioperative period. Most important, they say the study provides clarity for the management of patients with carotid and coronary disease.
“For patients presenting with an acute coronary syndrome requiring urgent coronary revascularization in whom waiting three to four weeks is not safe, combined CEA-OHS is the optimum revascularization strategy, though associated with higher neurological ischemic events,” write Mahmud and Reeves.
“However, for patients with a stable or an accelerating anginal syndrome who can wait three to four weeks to complete dual antiplatelet therapy [DAPT] after carotid stenting, staged CAS followed by OHS leads to superior early and long-term outcomes.”
Since completing the analysis, Shishehbor said there have been discussions with colleagues in vascular surgery, vascular medicine, cardiac surgery, and cardiology to establish the optimum way to treat patients with severe carotid and coronary disease. “The bottom line is that there will never be a randomized, clinical trial in this setting,” he told heartwire. “I hope there would be, but I doubt it. So I think papers like this are critical because we’re doing these procedures to prevent stroke. It’s important that we pick the right procedure for the right patient.”
Confounded by registry requirements
Shishehbor is also concerned about the scrutiny carotid stenting is under from the Centers for Medicare&Medicaid Services(CMS). Currently, the CMS reimburses procedures for asymptomatic patients only if they are included in one of the industry-funded and -maintained registries. He believes the scrutiny has led to a dwindling number of clinicians with the expertise capable of doing the procedure, and this is concerning, since the present analysis shows there are cohorts of asymptomatic patients who would benefit from the treatment.In addition, to be included in a registry, an asymptomatic patient must receive DAPT with aspirin andclopidogrel for four weeks. If the patient does not meet the DAPT requirements, they can’t be included in the registry. However, Shishehbor said, many of these patients have significant coronary disease and can’t wait four weeks. As a result, they are treated with a combined CEA-OHS approach, an approach that is associated with a higher risk of stroke.
Shishehbor reports serving as a speaker and consultant for Abbot Vascular, Medtronic, and Gore but waives all compensation for his work. Mahmud reports trial support from Boston Scientific and Abbott Vascular. In addition,he consults for Cordis andthe Medicines Companyand serves on the speaker‘s bureau for Medtronic. Disclosures for the coauthors are listed in the paper.
Sources
Shishehbor MH, Venkatachalam S, Sun Z, et al. A direct comparison of early and late outcomes with three approaches to carotid revascularization and open heart surgery. J Am Coll Cardiol 2013; available at: http://content.onlinejacc.org.
Mahmud E, Reeves R. Carotid revascularization prior to open heart surgery: The data driven treatment strategy. J Am Coll Cardiol 2013; available at: http://content.onlinejacc.org.
Open Abdominal Aortic Aneurysm (AAA) repair (OAR) vs. Endovascular AAA Repair (EVAR) in Chronic Kidney Disease (CKD) Patients – Comparison of Surgery Outcomes
Writer and Curator: Larry H. Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN
This is a review of the effects of CKD on increased morbidity and mortality of abdominal aortic aneurysm repair. The abdominal aorta has branches to the superior mesenteric arteries proximally, and below that both renal arteries, which also supply the adrenals (suprarenal).
Severe atherosclerosis with plaque buildup and separation of the media from the endothelium, can migrate down the addominal aorta before frank rupture of an aneurysm. Abdominal aortic aneurysm often extends from below the the renal arteries, to the internal spermatic vessels, or as far as the iliacs.
Of the visceral branches, the celiac artery and the superior and inferior mesenteric arteries are unpaired, while the suprarenals, renals, internal spermatics, and ovarian are paired. Of the parietal branches the inferior phrenics and lumbars are paired; the middle sacral is unpaired. The terminal branches are paired.
AAA is most common in men over age 65 years. If it is expanding AAA causes sudden, severe, and constant low back, flank, abdominal, or groin pain (internal spermatic branch). The presence of a pulsatile abdominal mass is virtually diagnostic but is found in less than half of all cases. At least 65% of patients with a ruptured AAA die from sudden cardiovascular collapse before arriving at a hospital.
A study by Mehta et al assessed the effect of hemodynamic status on outcomes in 136 patients undergoing EVAR for ruptured AAAs.[1] The patients were divided into 2 groups:
(1) Hd-stable (systolic BP ≥80 mm Hg; n = 92 [68%]) and
(2) Hd-unstable (systolic BP < 80 mm Hg for >10 minutes; n = 44 [32%]).
The 30-day mortality, postoperative complications, need for secondary reinterventions, and midterm mortality were recorded. The 2 groups were found to be similar with respect to
comorbidities,
mean AAA maximum diameter (6.6 vs 6.4 cm),
need for on-the-table conversion to open repair (3% vs 7%), and
incidence of nonfatal complications (43% vs 38%) and secondary interventions (23% vs 25%).
intraoperative need for aortic occlusion balloon,
mean estimated blood loss,
incidence of developing abdominal compartment syndrome (ACS), and
mortality
were all increased in the Hd-unstable group ([1]40% vs 6%, [2]744 vs 363 mL,[3] 29% vs 4%, and[4]33% vs 18%, respectively).
Requires direct access to the aorta through an abdominal or retroperitoneal approach
Endovascular: Involves gaining access to the lumen of the abdominal aorta, usually via small incisions over the femoral vessels; an endograft, typically a cloth graft with a stent exoskeleton, is placed within the lumen of the AAA, extending distally into the iliac arteries. Approximately 90% of abdominal aortic aneurysms are infrarenal.
The important surgical and endovascular anatomic considerations include associated renal and visceral artery involvement (either occlusive disease or involved in the aneurysm process) and the iliac artery (either occlusive disease or aneurysms). The length of the infrarenal aortic neck is important in helping determine the surgical approach (retroperitoneal vs transabdominal) and the location of the aortic cross clamp.
Endovascular repair first became practical in the 1990s and although it is now an established alternative to open repair, its role is yet to be clearly defined. It is generally indicated in older, high-risk patients or patients unfit for open repair. However, endovascular repair is feasible for only a proportion of AAAs, depending on the morphology of the aneurysm. The main advantages over open repair are that there is less peri-operative mortality, less time in intensive care, less time in hospital overall and earlier return to normal activity. Disadvantages of endovascular repair include a requirement for more frequent ongoing hospital reviews, and a higher chance of further procedures being required. According to the latest studies, the EVAR procedure does not offer any benefit for overall survival or health-related quality of life compared to open surgery, although aneurysm-related mortality is lower.
The diameter of the aorta decreases in size from its thoracic portion to the abdominal and infrarenal portions. A normal aorta shows a reduction in medial elastin layers from the thoracic area to the abdominal portion. Elastin and collagen content are also reduced. AAAs develop following degeneration of the media. The degeneration ultimately may lead to widening of the vessel lumen and loss of structural integrity.
A multidisciplinary research program supported by the US National Heart, Lung, and Blood Institute identified proteolytic degradation of aortic wall connective tissue, inflammation and immune responses, biomechanical wall stress, and molecular genetics as mechanisms important in the development of AAA. Similarly, surgical specimens of AAA reveal inflammation, with infiltration by lymphocytes and macrophages; thinning of the media; and marked loss of elastin.
Through gene microarray analysis, various genes involved in extracellular matrix degradation, inflammation, and other processes observed in AAA formation have been shown to be up-regulated, while others that may serve to prevent this occurrence are down-regulated. The combination of proteolytic degradation of aortic wall connective tissue, inflammation and immune responses, biomechanical wall stress, and molecular genetics represents a dynamic process that leads to aneurysmal deterioration of aortic tissue.
1. Mehta M, Paty PS, Byrne J, Roddy SP, Taggert JB, Sternbach Y, et al. The impact of hemodynamic status on outcomes of endovascular abdominal aortic aneurysm repair for rupture. J Vasc Surg. May 2013;57(5):1255-60. [Medline].
2. Blanchard JF, Armenian HK, Friesen PP. Risk factors for abdominal aortic aneurysm: results of a case-control study. Am J Epidemiol. Mar 15 2000;151(6):575-83. [Medline].
3. Lederle FA, Johnson GR, Wilson SE, Chute EP, Littooy FN, Bandyk D, et al. Prevalence and associations of abdominal aortic aneurysm detected through screening. Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Ann Intern Med. Mar 15 1997;126(6):441-9. [Medline].
4. Wassef M, Baxter BT, Chisholm RL, Dalman RL, Fillinger MF, Heinecke J, et al. Pathogenesis of abdominal aortic aneurysms: a multidisciplinary research program supported by the National Heart, Lung, and Blood Institute. J Vasc Surg. Oct 2001;34(4):730-8. [Medline].
5. [Guideline] U.S. Preventive Services Task Force. Screening for abdominal aortic aneurysm: recommendation statement. Ann Intern Med. Feb 1 2005;142(3):198-202. [Medline]. [Full Text].
Impact of chronic kidney disease on outcomes after abdominal aortic aneurysm repair
Chronic kidney disease (CKD) is associated with increased morbidity and death after open abdominal aortic aneurysm (AAA) repair (OAR). This study highlights the effect of CKD on outcomes after endovascular AAA (EVAR) and OAR in contemporary practice.
The National Surgical Quality Improvement Program (NSQIP) Participant Use File (2005-2008) was queried by Current Procedural Terminology (American Medical Association, Chicago, Ill) code to identify EVAR or OAR patients, who were grouped by CKD class as having mild (CKD class 1 or 2), moderate (CKD class 3), or severe (CKD class 4 or 5) renal disease. Propensity score analysis was performed to match OAR and EVAR patients with mild CKD with those with moderate or severe CKD. Comparative analysis of mortality and clinical outcomes was performed based on CKD strata.
We identified 8701 patients who were treated with EVAR (n = 5811) or OAR (n = 2890) of intact AAAs. Mild, moderate, and severe CKD was present in 63%, 30%, and 7%, respectively. CKD increased (P < .01) overall mortality, with rates of 1.7% (mild), 5.3% (moderate), and 7.7% (severe) in unmatched patients undergoing EVAR or OAR. Operative mortality rates in patients with severe CKD were as high as 6.2% for EVAR and 10.3% for OAR.
Severity of CKD was associated with increasing frequency of risk factors; therefore, propensity matching to control for comorbidities was performed, resulting in similar baseline clinical and demographic features of patients with mild compared with those with moderate or severe disease.
In propensity-matched cohorts, moderate CKD increased the risk of 30-day mortality
for EVAR (1.9% mild vs 3.2% moderate; P = .013) and
OAR (3.1% mild vs 8.4% moderate; P < .0001).
Moderate CKD was also associated with increased morbidity in patients treated with
EVAR (8.3% mild vs 12.8% moderate; P < .0001) or
OAR (25.2% mild vs 32.4% moderate; P = .001).
Similarly, severe CKD increased the risk of 30-day mortality
for EVAR (2.6% mild vs 5.7% severe; P = .0081) and
OAR (4.1% mild vs 9.9% severe; P = .0057).
Severe CKD was also associated with increased morbidity in patients treated with
EVAR (10.6% mild vs 19.2% severe; P < .0001) or
OAR (31.1% mild vs 39.6% severe; P = .04).
The presence of moderate or severe CKD in patients considered for AAA repair is associated with significantly increased mortality and therefore should figure prominently in clinical decision making. The high mortality of AAA repair in patients with severe CKD is such that elective repair in such patients is not advised, except in extenuating clinical circumstances.
Competition in the Ecosystem of Medical Devices in Cardiac and Vascular Repair: Heart Valves, Stents, Catheterization Tools and Kits for Open Heart and Minimally Invasive Surgery (MIS)
Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone (Justin Pearlman, Aviva Lev-Ari)
Carotid Stenting: Vascular surgeons have pointed to more minor strokes in the stenting group and cardiologists to more myocardial infarctions in the CEA cohort.
Global Supplier Strategy for Market Penetration & Partnership Options (Niche Suppliers vs. National Leaders) in the Massachusetts Cardiology & Vascular Surgery Tools and Devices Market for Cardiac Operating Rooms and Angioplasty Suites
Cardiovascular diseases comprise problems of the heart and blood vessels, including rhythm, blood supply, blood pressure, birth defects, or damage from cholesterol, tobacco, street drugs, radiation, viruses, bacteria, or fungi.
Thus the category includes heart failure (inadequate pump function), heart or vessel infection (endocarditis, vasculitis), birth defects (congenital heart disease)
Cardiovascular Diseases: Causes, Risks and Management
This book is a comprehensive review of Innovations in Cardiovascular Medicine, including the latest discoveries in
Cardiac Medical Imaging,
Regenerative Medicine,
Pharmacotherapy,
Medical Devices for Cardiac Repair,
Genomics, and opportunities for Targeted Therapy.
It is written by experts in their respective subspecialties. The e-Book’s articles have been published on the Open Access Online Scientific Journal, since April 2012. All new articles on this subject will continue to be incorporated with periodical updates.
The Journal is a scientific, medical and business, multi-expert authoring environment for information syndication in domains of Life Sciences, Medicine, Pharmaceutical and Healthcare Industries, BioMedicine, Medical Technologies & Devices. Scientific critical interpretations and original articles are written by PhDs, MDs, MD/PhDs, PharmDs, Technical MBAs as Experts, Authors, Writers (EAWs) on an Equity Sharing basis.
myocardial injury mapping by magnetic resonance contrast retention,
myocardial viability by MRI,
atheroma lipid liquid crystal characterization,
outpatient inotropic infusion therapy,
angiogenesis imaging,
multimodal in vivo stem cell imaging,
real-time velocity beam MRI,
in vivo microscopic MRI,
dobutamine stress echocardiography for low gradient valve disease,
alternative stress tests,
diagnostic electrocardiography in magnetic environments,
statistical methods to solve error propagation of large array genomics,
discovery of monocyte role in native coronary collateral development,
image tracked stem cell treatment of heart attacks,
singularity editing in differential topology.
Preface to the Three Volume Series
Cardiovascular disease has been a leading cause of death and disability and so it has also been a major focus for intense research, development, and progress. Knowledge of the causes, risks, and best practices for management continually change. That is why a dynamic electronic living textbook presents an exciting opportunity to help you keep current with the ephemeral leading edge. This book is an outgrowth of the commitment of Leaders in Pharmaceutical Business Intelligence to present the most exciting timely and pertinent advances of our day, in a continual medium to stay fresh and up to date. We hope diverse multispecialty perspectives will help you in your quest to understand, adapt and advance the leading edge of cardiovascular disease causes, risks and best practices management.
On the Diagnosis of Cardiovascular Disease: causes, manifestations, consequences and priorities
Doctors aim to spend their time on prevention, diagnosis, and disease management. More and more the time is diverted to expanding demands for documentation and bureaucratic navigation. This article focuses on the art of diagnosis, with examples based on cardiovascular diseases. Diagnosis cannot be achieved without a knowledge of the causes (etiology) of ailments, a necessary but not sufficient component of diagnosis. The causes broadly relate to nature and nurture, how our biological system develops and functions (nature), and its interactions with the outside world driven in part by behavior, diet, exposures, and activities (nurture). The nature of our individuality has been traced to the human genome, a map of code for protein products that build our structures and mediate our body part functions. Numerous blood tests have been devised to check the expression and activity level of such genomic products to identify disease and characterize its stage. The role of diet, behavior, exposures, activities or lack thereof is well established as a complicit factor in disease development and progression.
The art of diagnosis is designed to find out what is wrong. Literally, it is a flow of knowing, based on knowledge of causes of ailments, probabilities (prevalence), consequences, manifestations, priorities (which would be most urgent) and tests: CPCMPT. Review of those elements generates a list of concerns, often expressed as a “differential diagnosis” which is a prioritized list of plausible explanations for the observations, patient’s report of symptoms and findings from patient examination. The second stage of diagnosis, called the “work-up,” selects and applies tests to stratify the list of possibilities further as well as to characterize the manifestations and stage of disease. Technically, analysis of biological samples, imaging studies and intervention trials each represent tests; however, they are often viewed as distinct tools with just the former labeled as tests (biological samples include blood tests, urine tests, sputum or saliva samples, and biopsies). The primary goal of the work-up is to establish one or more specific diagnoses as the cause of ailment. The secondary goal of the work-up is to characterize the manifestations and stage of disease to define expectations and clarify options for the disease management. The third goal is to develop a management a plan to slow or stop the ailment, decrease risks of complications, slow or stop progression of disease manifestations or otherwise minimize functional impairment.
The manifestations of disease are categorized as signs and symptoms.
Signs are observable evidence of consequences,
Symptoms are subjective complaints.
A major component of diagnostic skill is the ability to identify and characterize correctly signs and symptoms of all relevant disease conditions. A second major component of diagnostic skill is the ability to select appropriate tests and interpret their significance in context, in keeping with the patient’s presentation.
When someone sees a doctor about chest pain, coronary artery disease is a prominent consideration. The most common causes of chest pain are mechanical (muscle and bone, e.g., muscle spasms, muscle and bone inflammation), but those conditions are not generally life-threatening. The consequences of blocked arteries – arrhythmia, permanent weakness of the heart, blood clots, pulmonary emboli, stroke, cardiogenic shock, death – raise the stakes and push coronary disease high in priority even when the probabilities are low. The prioritization of the differential diagnosis list has multiple considerations: urgency (how quickly it can worsen), severity of consequences, and the probabilities of a macrovascualar event (prevalence, risk factors). A ten percent risk of coronary disease typically takes precedence over a 70% likelihood of muscle spasm in terms of diagnostic testing.
The road map for the construction of our individuality as humans has been fully mapped: the human genome. Genetic variation means we are not fully determined by the mix of genes inherited from our parents. In addition to the genetic material on our 48 chromosomes, and the genetic material in mitochondria inherited from the mother, there are spontaneous changes in the genetic code, and there are modifications that affect gene expression (which codes produce gene products, quantities, rates, and post-production modifications).
The causes of cardiovascular disease are defined by Murphy’s law: what can go wrong will. However, on the nature side, most malfunctions are too severe to reach the light of day, so there is a limited list of disease mechanisms associated with sufficient viability to reach medical attention. Those mechanisms can be summarized by a mnemonic: diseases can develop new metals in-flame, a-fact externs generated (disease mechanisms: congenital, developmental, neoplastic, metabolic, inflammatory, infectious, extrinsic (e.g. stab wound), and degenerative). A taxonomy of cardiovascular diseases can be constructed in various ways: (1) itemize the major cardiovascular functions and subclassify the dysfunctions, (2) itemize by principle anatomic involvement and subclassify by pathology, (3) classify by mechanism of disease, etiology. Compendiums of cardiovascular disease may be found in: (1) French’s Differential Diagnosis, (2) Robbins and Angel Pathology, (3) Guyton’s Textbook of Physiology, as well as cardiovascular disease textbooks such as Hurst, Braunwald, Mayo Clinic, Cleveland Clinic…
Diagnosis takes many forms. The paranoid inclusive approach, manifested as “medical student syndrome”, considers any semblance of a sign or symptom vaguely similar to a disease manifestation as a frightening prospect worthy of detailed pursuit. The minimalist pragmatic approach commonly attributed to general practitioners focuses on reassurance, and pursuit of persisting complaints that match a common ailment. That approach has been summarized by the advice: when you hear hoof beats think of horses, not zebras. Specialists, on the other hand, are taught to consider all possibilities, with due consideration to urgency and treatability, so that zebras are not punished.
The healthcare system promotes the idea of generalists serving as the front line, identifying who can be managed simply, with specialists serving as finishers for more complex cases or cases requiring special skills. A flaw in that model is the need for detailed knowledge of zebras and subtle findings that may represent an urgent issue at the front line for triage. If the generalist does not know that mild symptoms from mitral valve disease or aortic valve disease may require urgent detailed assessment, patients may be referred to a specialist too late to prevent consequences that requires an earlier intervention.
Parsimony in diagnosis refers to identifying the fewest number of diagnoses that explain all the findings. The concept has been attributed to Osler, and it builds on a guiding procedure voiced in the middle ages by Occum, known as Occum’s razor: when deciding between two explanations, favor the one that requires the fewest assumptions. Parsimony is a useful guide for diagnosis of a previously healthy patient who develops a number of findings that are temporally coherent. After age 65 (official geriatrics age), physicians are taught to abandon parsimony and expect more diagnoses than findings.
A study of difficult diagnoses lead to the concept of a pivotal finding as one that has a narrow differential list. The diagnostic process is prone to errors, including cognitive biases, which may benefit from computer assistance. Intuition and analytics can be applied to reduce cognitive bias. The author developed a just-in-time social networking system within a software package called Missive(c) that enables rapid access to such tools, combining efficiency in documentation with improved quality of analysis and reports (faster and better).
Among older Americans, more are hospitalized for heart failure than for any other medical condition (diastolic failure=stiff heart, systolic failure= inadequate pumping).
Genomics – the study of the genetic basis for disease – is rapidly expanding knowledge about etiology (cause of disease), and it helps identify opportunities for accurate diagnosis and treatment. The American Heart Association journal CIRCULATION has published 348 relevant articles related to cardiovascular genomics from 2010-2013. For example, just on the subtopic of atherosclerosis (hardening of arteries), genomics offers major progress. The genetic factors that affect arterial stiffness are strongly related to a very common underlying health concern, hypertension (high blood pressure). The counterpart to genetics is environment (nature versus nurture), but genetics carries the trump cards because it determines the sensitivities to environment.
[bring here ONLY the INTRODUCTION and the Summary of each, THEN The EDITOR will provide perspective on the Research and the current STate of Cardiology in the US in 2013/2014]
Hardening of the arteries is described as atherosclerosis, or porridge-like wall changes with scarring, which leads to heart attacks, high blood pressure, stroke, and organ injury mediated by ischemia (insufficient nutrient blood supply). The causes are both nature (genetic) and nurture (behavior, diet). Specifics of the causes guide diagnosis and management.
Chapter 1.2: Genomics
The completion of the human genome map was a major accomplishment, as gene products make signals, receptors and building blocks that establish health and disease. However, it is just a stepping stone, not explaining why, where, or how the gene products are regulated and interact.
Chapter 1.3: Cardiovascular Imaging
Imaging applies a principle of physics (light transmission, sound transmission, xray transmission, magnetic resonance, radioactivity) to provide a map of interior structures and/or activities. Image processing (computing) derives further information than simple display of an observed tissue-sensitive parameter. In the case of computed tomography (CT), magnetic resonance (MRI), positron-emission tomography (PET), and single-photon emission tomography (SPECT), computer reformatting of image data is essential.
Cardiovascular disease is the leading cause of death and disability, affecting more than four times as many people as all forms of cancer combined.
Chapter 2.2: Testing for cardiovascular risk
The volunteer population of Framingham Massachusetts provided decades of data clarifying determinants of risk for cardiovascular diseases. That data helped establish the usefulness of cholesterol screening, and lead to the search for additional tests to identify risk and guide management.
Chapter 2.3: Biomarkers
Biomarkers are chemistry levels (concentrations in the blood) that identify injury or risk for injury.
As the mysteries of the human genome products are unraveled, we get closer to identifying key components. One of them is Thymosin beta 4 (Tβ4) , which plays an essential role in cardiac and blood vessel development and regeneration. It may lead to breakthroughs in angiogenesis and vasculogenesis, or new vessel development, mimicking the behavior of the lucky few who develop new vessels, or collaterals, as a natural bypass system, without requiring a surgeon to provide a blood supply to avoid or limit heart attacks.
Chapter 3.2: Image guidance of Therapy
The US government is helping to sponsor new imaging methods, while they also inhibit it by adding new taxes.
Chapter 3.3: Drug therapy
Emerging new therapies are presented, along with the biological basis.
Chapter 3.4: Cardiovascular Interventions
Technological advances enable minimally invasive solutions to problems previously addressed by surgery or autopsy.
Contributors above, need a LINK to the appropriate contributors in each volume. Table of Contents of each volume above need a LINK to the eTOCS of each volume.
Please UPDATE all links ABOVE to the appropriate locations in the respective volumes, after implementing the carry over, remove links below EXCEPT CVD1,2,3 and remove this comment of mine in RED, here
Bernstein, HL and A. Lev-Ari 5/15/2013 Diagnosis of Cardiovascular Disease, Treatment and Prevention: Current & Predicted Cost of Care and the Promise of Individualized Medicine Using Clinical Decision Support Systems
C. Genomics & Genetics of Cardiovascular Disease Diagnoses
Lev-Ari, A. and L H Bernstein 3/7/2013 Genomics & Genetics of Cardiovascular Disease Diagnoses: A Literature Survey of AHA’s Circulation Cardiovascular Genetics, 3/2010 – 3/2013
D. Genetic Base of Atherosclerosis and Loss of Arterial Elasticity with Aging
Lev-Ari, A. 5/17/2013 Synthetic Biology: On Advanced Genome Interpretation for Gene Variants and Pathways: What is the Genetic Base of Atherosclerosis and Loss of Arterial Elasticity with Aging
F. Arterial Stiffness: Pharmacotherapy for Hypertension and Hypercholesterolemia Management
Pearlman, JD and A. Lev-Ari 5/24/2013 Imaging Biomarker for Arterial Stiffness: Pathways in Pharmacotherapy for Hypertension and Hypercholesterolemia Management
Lev-Ari, A. 4/28/2013 Genetics of Conduction Disease: Atrioventricular (AV) Conduction Disease (block): Gene Mutations – Transcription, Excitability, and Energy Homeostasis
Pearlman, JD and A. Lev-Ari 5/7/2013 On Devices and On Algorithms: Arrhythmia after Cardiac Surgery Prediction and ECG Prediction of Paroxysmal Atrial Fibrillation Onset
Pearlman, JD and A. Lev-Ari 5/22/2013 Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone
Abdominal Aortic Aneurysms (AAA): Albert Einstein’s Operation by Dr. Nissen
Reporter: Aviva Lev-Ari, PhD, RN
On June 11, 2013, I received the following comment by Dr. Miranda, to my article, an Interview with Dr. Richard Cambria, Chief Vascular Surgery, MGH, Boston
Efrain Miranda, Ph.D. • It is true that abdominal aortic aneurysms (AAA) are mostly asymptomatic, until they rupture. By luck, some are identified. An example was a AAA found in Albert Einstein by Dr. Nissen when Einstein went for abdominal surgery for something completely unrelated! In my experience, I have found many AAA’s in individuals who had a totally different cause of death. http://clinanat.com/mtd/153-aneurysm
I am presenting here the the CASE of an AAA found in Albert Einstein by Dr. Nissen when Einstein went for abdominal surgery for something completely unrelated!
A Moment in History
Dr. Rudolf Nissen
(1896 – 1981)
Dr Nissen’s life is extraordinary. Born in the city of Neisse, Germany in 1896, he was the son of a local surgeon. He studied medicine in the Universities of Munich, Marburg, and Breslau. He was the pupil of the famous pathologist Albert Aschoff (discoverer of the heart’s AV node, along with Sunao Tawara).
Nissen became a professor of surgery in Berlin, and in 1933 moved to Turkey where he was placed in charge of the Department of Surgery of the University of Istanbul. In 1939 he moved to the US, first to the Massachusetts General Hospital and later to the Jewish Hospital in Brooklyn, New York. After becoming a US citizen, he moved again in 1952 to Basel, Switzerland as Chief of the Department of Surgery, where he retired in 1967. He died in 1981.
His contributions to surgery are innumerable. He wrote over 30 books and 450 journal articles. Known for the development in 1956 of what is today known as the “Nissen fundoplication” for esophageal hiatus hernia surgery, Nissen also worked with his assistant, Dr. Mario Rossetti to develop the “floppy Nissen fundoplication”, also known as the “Nissen-Rossetti procedure”. This would be enough to honor this man, still, he (with Sauerbruch) performed the first lung lobectomy and the first pneumonectomy (called then a total pneumonectomy). In 1949 he performed the first esophagectomy with a gastroesophagostomy.
His personal life is even more interesting. Drafted at 20, he fought in WWI and was wounded several times. In 1933, under the Nazi regime, he was ordered to fire all the Jewish-German assistants under his care. Being Jewish himself, he was told that he would keep his job, Nissen could not take this. He resigned his position and moved out of Germany.
Another little known fact is that he operated on Albert Einstein in 1948. He operated on Einstein because of intestinal cysts. Having found a developing abdominal aortic aneurysm, he reinforced it with cellophane, undoubtedly giving his patient a few extra years to live. Einstein died in 1955.
As a personal side note, our good friend Dr. Aaron Ruhalter scrubbed in with Dr. Nissen while serving as a surgical resident at the Brooklyn Jewish Hospital!


























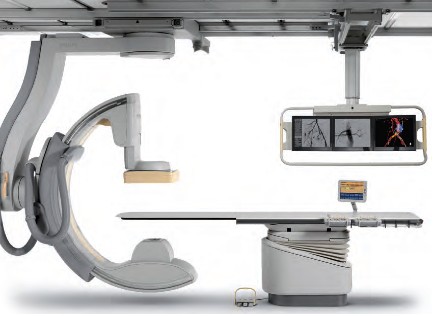










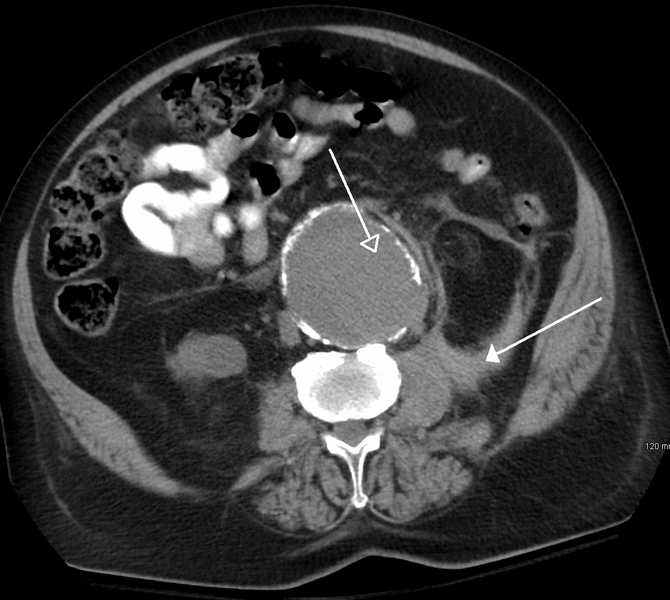





{kind=link}
{kind=link}
{kind=link}
{kind=link}
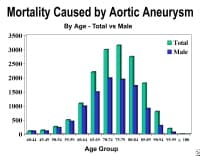{kind=link}
{kind=link}