Dealing with the Use of the High Sensitivity Troponin (hs cTn) Assays: Preparing the United States for High-Sensitivity Cardiac Troponin Assays
Author and Curator: Larry H Bernstein, MD, FCAP
Author and Curator: Aviva Lev-Ari, PhD, RD
In this article we shall address the two following papers:
In a previous posting I commented on the problem of hs cTn use and the on site ED performance of cardiac treadmill (done in Europe)
- prior to a decision of CT scan (not done in US).
Acute Chest Pain/ER Admission: Three Emerging Alternatives to Angiography and PCI – Corus CAD, hs cTn, CCTA
We examine the emergence of Alternatives to Angiography and PCI as most common strategy for ER admission with listed cause of Acute Chest Pain. The Goal is to use methods that will improve the process to identify for an Interventional procedure only the patients that a PCI is a must to have.
Alternative #1: Corus® CAD
Alternative #2: High-Sensitivity Cardiac Troponins in Acute Cardiac Care
Alternative #3: Coronary CT Angiography for Acute Chest Pain
After presenting the the Three alternatives, the Editorial by R.F. Redberg, Division of Cardiology,
UCSF, will be analyzed.
-
Alternative #1: First-Line Test to Help Clinicians Exclude Obstructive CAD as a Cause of the Patient’s Symptoms
Corus® CAD, a blood-based gene expression test, demonstrated high accuracy with both a high negative predictive value (96 percent) and high sensitivity (89 percent) for assessing obstructive coronary artery disease (CAD) in a population of patients referred for stress testing with myocardial perfusion imaging (MPI).
COMPASS enrolled stable patients with symptoms suggestive of CAD who had been referred for MPI at 19 U.S. sites. A blood sample was obtained in all 431 patients prior to MPI and Corus CAD gene expression testing was performed with study investigators blinded to Corus CAD test results.Following MPI, patients underwent either invasive coronary angiography orcoronary CT angiography, gold-standard anatomical tests for the diagnosis of coronary artery disease.
A Blood Based Gene Expression Test for Obstructive Coronary Artery Disease Tested in Symptomatic Non-Diabetic Patients Referred for Myocardial Perfusion Imaging: The COMPASS Study
http://pharmaceuticalintelligence.com/2012/08/14/obstructive-coronary-artery-disease-diagnosed-by-rna-levels-of-23-genes-cardiodx-heart-disease-test-wins-medicare-coverage/
-
Alternative #2: High-Sensitivity Cardiac Troponins in Acute Cardiac Care
Recommendations for the use of cardiac troponin (cTn) measurement in acute cardiac care have recently been published.[1] Subsequently, a high-sensitivity (hs) cTn T assay was introduced into routine clinical practice.[2] This assay, as others, called highly sensitive, permits measurement of cTn concentrations in significant numbers of apparently illness-free individuals. These assays can measure cTn in the single digit range of nanograms per litre (=picograms per millilitre) and some research assays even allow detection of concentrations <1 ng/L.[2–4] Thus, they provide a more precise calculation of the 99th percentile of cTn concentration in reference subjects (the recommended upper reference limit [URL]). These assays measure the URL with a coefficient of variation (CV) <10%.[2–4]The high precision of hs-cTn assays increases their ability to determine small differences in cTn over time. Many assays currently in use have a CV >10% at the 99th percentile URL limiting that ability.[5–7] However, the less precise cTn assays do not cause clinically relevant false-positive diagnosis of acute myocardial infarction (AMI) and a CV <20% at the 99th percentile URL is still considered acceptable.[8]
We believe that hs-cTn assays, if used appropriately, will improve clinical care. We propose criteria for the clinical interpretation of test results based on the limited evidence available at this time.
References
1. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B, Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J 2010;31:2197–2204.
2. Saenger AK, Beyrau R, Braun S, Cooray R, Dolci A, Freidank H, Giannitsis E, Gustafson S, Handy B, Katus H, Melanson SE, Panteghini M, Venge P, Zorn M, Jarolim P, Bruton D, Jarausch J, Jaffe AS. Multicenter analytical evaluation of a high sensitivity troponin T assay. Clin Chim Acta 2011;412:748–754.
3. Zaninotto M, Mion MM, Novello E, Moretti M, Delprete E, Rocchi MB, Sisti D, Plebani M. Precision performance at low levels and 99th percentile concentration of the Access AccuTnI assay on two different platforms. Clin Chem Lab Med 2009; 47:367–371.
4. Todd J, Freese B, Lu A, Held D, Morey J, Livingston R, Goix P. Ultrasensitive flow based immunoassays using single-molecule counting. Clin Chem 2007; 53:1990–1995.
5. van de Kerkhof D, Peters B, Scharnhorst V. Performance of Advia Centaur second-generation troponin assay TnI-Ultra compared with the first-generation cTnI assay. Ann Clin Biochem 2008; 45:316–317.
6. Lam Q, Black M, Youdell O, Spilsbury H, Schneider HG. Performance evaluation and subsequent clinical experience with the Abbott automated Architect STAT Troponin-I assay. Clin Chem 2006; 52:298–300.
7. Tate JR, Ferguson W, Bais R, Kostner K, Marwick T, Carter A. The determination of the 99th percentile level for troponin assays in an Australian reference population. Ann Clin Biochem 2008; 45:275–288.
8. Jaffe AS, Apple FS, Morrow DA, Lindahl B, Katus HA. Being rational about (im)-precision: a statement from the Biochemistry Subcommittee of the Joint European Society of Cardiology/American College of Cardiology Foundation/American Heart Association/World Heart Federation Task Force for the definition of myocardial infarction. Clin Chem 2010; 56:921–943.
SOURCE:
How to Use High-Sensitivity Cardiac Troponins in Acute Cardiac Care
Kristian Thygesen, Johannes Mair, Evangelos Giannitsis, Christian Mueller, Bertil Lindahl, Stefan Blankenberg, Kurt Huber, Mario Plebani, Luigi M. Biasucci, Marco Tubaro, Paul Collinson, Per Venge, Yonathan Hasin, Marcello Galvani, Wolfgang Koenig, Christian Hamm, Joseph S. Alpert, Hugo Katus, and Allan S. Jaffe
Eur Heart J. 2012;33(18):2252-2257.
http://www.medscape.com/viewarticle/771065
To the Editor:
Hoffmann et al. (July 26 issue)1 conclude that, among patients with low-to-intermediate-risk acute coronary syndromes, the incorporation of coronary computed tomographic angiography (CCTA) improves the standard evaluation strategy.2 However, it may be difficult to generalize their results, owing to different situations on the two sides of the Atlantic and the availability of high-sensitivity troponin T assays in Europe. In the United States, the Food and Drug Administration has still not approved a high-sensitivity troponin test, and patients in the Rule Out Myocardial Infarction/Ischemia Using Computer Assisted Tomography (ROMICAT-II) trial only underwent testing with the conventional troponin T test. As we found in the biomarker substudy in the ROMICAT-I trial, a single high-sensitivity troponin T test at the time of CCTA accurately ruled out acute myocardial infarction (negative predictive value, 100%) (Table 1TABLE 1 Results of High-Sensitivity Troponin T Testing for the Diagnosis of Acute Coronary Syndromes in ROMICAT-I.).3 In addition, patients with acute myocardial infarction can be reliably identified, with up to 100% sensitivity, with the use of two high-sensitivity measurements of troponin T within 3 hours after admission.4,5
Results of High-Sensitivity Troponin T Testing for the Diagnosis of Acute Coronary Syndromes in ROMICAT-I.).3 In addition, patients with acute myocardial infarction can be reliably identified, with up to 100% sensitivity, with the use of two high-sensitivity measurements of troponin T within 3 hours after admission.4,5
It seems plausible to assume that the incorporation of high-sensitivity troponin T assays in this trial would have outperformed CCTA. Therefore, it is important to assess the performance of such testing and compare it with routine CCTA testing in terms of length of stay in the hospital and secondary end points, especially cumulative costs and major adverse coronary events at 28 days.
References
- Hoffmann U, Truong QA, Schoenfeld DA, et al. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med 2012;367:299-308
- Redberg RF. Coronary CT angiography for acute chest pain. N Engl J Med 2012;367:375-376
- Januzzi JL Jr, Bamberg F, Lee H, et al. High-sensitivity troponin T concentrations in acute chest pain patients evaluated with cardiac computed tomography. Circulation2010;121:1227-1234
- Keller T, Zeller T, Ojeda F, et al. Serial changes in highly sensitive troponin I assay and early diagnosis of myocardial infarction. JAMA 2011;306:2684-2693
- Thygesen K, Mair J, Giannitsis E, et al. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur Heart J 2012;33:2252-2257
Author/Editor Response
In response to Karakas and Koenig: we agree that high-sensitivity troponin T assays may permit more efficient care of low-risk patients presenting to the emergency department with acute chest pain1 and may also have the potential to identify patients with unstable angina because cardiac troponin T levels are associated with the degree and severity of coronary artery disease.2 Hence, high-sensitivity troponin T assays performed early may constitute an efficient and safe gatekeeper for imaging. CCTA, however, may be useful for ruling out coronary artery disease in patients who have cardiac troponin T levels above the 99th percentile but below levels that are diagnostic for myocardial infarction. The hypothesis that high-sensitivity troponin T testing followed by CCTA, as compared with other strategies, may enable safe and more efficient treatment of patients in the emergency department who are at low-to-moderate risk warrants further assessment. The generalizability of our data to clinical settings outside the United States may also be limited because of differences in the risk profile of emergency-department populations and the use of nuclear stress imaging.3
Udo Hoffmann, M.D., M.P.H.
Massachusetts General Hospital, Boston, MA
uhoffmann@partners.org
W. Frank Peacock, M.D.
Baylor College of Medicine, Houston, TX
James E. Udelson, M.D.
Tufts Medical Center, Boston, MA
Since publication of their article, the authors report no further potential conflict of interest.
References
- Than M, Cullen L, Reid CM, et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet 2011;377:1077-1084
- Januzzi JL Jr, Bamberg F, Lee H, et al. High-sensitivity troponin T concentrations in acute chest pain patients evaluated with cardiac computed tomography. Circulation2010;121:1227-1234
- Peacock WF. The value of nothing: the consequence of a negative troponin test. J Am Coll Cardiol 2011;58:1340-1342
-
Alternative #3: Coronary CT Angiography for Acute Chest Pain
The Study concluded:
There was increased diagnostic testing and higher radiation exposure in the CCTA group, with no overall reduction in the cost of care.
Coronary CT Angiography versus Standard Evaluation in Acute Chest Pain
Udo Hoffmann, M.D., M.P.H., Quynh A. Truong, M.D., M.P.H., David A. Schoenfeld, Ph.D., Eric T. Chou, M.D., Pamela K. Woodard, M.D., John T. Nagurney, M.D., M.P.H., J. Hector Pope, M.D., Thomas H. Hauser, M.D., M.P.H., Charles S. White, M.D., Scott G. Weiner, M.D., M.P.H., Shant Kalanjian, M.D., Michael E. Mullins, M.D., Issam Mikati, M.D., W. Frank Peacock, M.D., Pearl Zakroysky, B.A., Douglas Hayden, Ph.D., Alexander Goehler, M.D., Ph.D., Hang Lee, Ph.D., G. Scott Gazelle, M.D., M.P.H., Ph.D., Stephen D. Wiviott, M.D., Jerome L. Fleg, M.D., and James E. Udelson, M.D. for the ROMICAT-II Investigators
N Engl J Med 2012; 367:299-308 July 26, 2012 http://dx.doi.org/10.1056/NEJMoa1201161
-
BACKGROUND
It is unclear whether an evaluation incorporating coronary computed tomographic angiography (CCTA) is more effective than standard evaluation in the emergency department in patients with symptoms suggestive of acute coronary syndromes.
METHODS
In this multicenter trial, we randomly assigned patients 40 to 74 years of age with symptoms suggestive of acute coronary syndromes but without ischemic electrocardiographic changes or an initial positive troponin test to early CCTA or to standard evaluation in the emergency department on weekdays during daylight hours between April 2010 and January 2012. The primary end point was length of stay in the hospital. Secondary end points included rates of discharge from the emergency department, major adverse cardiovascular events at 28 days, and cumulative costs. Safety end points were undetected acute coronary syndromes.
RESULTS
The rate of acute coronary syndromes among 1000 patients with a mean (±SD) age of 54±8 years (47% women) was 8%. After early CCTA, as compared with standard evaluation, the mean length of stay in the hospital was reduced by 7.6 hours (P<0.001) and more patients were discharged directly from the emergency department (47% vs. 12%, P<0.001). There were no undetected acute coronary syndromes and no significant differences in major adverse cardiovascular events at 28 days. After CCTA, there was more downstream testing and higher radiation exposure. The cumulative mean cost of care was similar in the CCTA group and the standard-evaluation group ($4,289 and $4,060, respectively; P=0.65).
CONCLUSIONS
In patients in the emergency department with symptoms suggestive of acute coronary syndromes, incorporating CCTA into a triage strategy improved the efficiency of clinical decision making, as compared with a standard evaluation in the emergency department, but it resulted in an increase in downstream testing and radiation exposure with no decrease in the overall costs of care. (Funded by the National Heart, Lung, and Blood Institute; ROMICAT-II ClinicalTrials.gov number, NCT01084239.)
http://www.nejm.org/doi/full/10.1056/NEJMoa1201161#t=abstract
REFERENCES
- Roe MT, Harrington RA, Prosper DM, et al. Clinical and therapeutic profile of patients presenting with acute coronary syndromes who do not have significant coronary artery disease. Circulation 2000;102:1101-1106
- Miller JM, Rochitte CE, Dewey M, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 2008;359:2324-2336
- Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008;52:1724-1732
- Marano R, De Cobelli F, Floriani I, et al. Italian multicenter, prospective study to evaluate the negative predictive value of 16- and 64-slice MDCT imaging in patients scheduled for coronary angiography (NIMISCAD-Non Invasive Multicenter Italian Study for Coronary Artery Disease). Eur Radiol 2009;19:1114-1123
- Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 2008;52:2135-2144
- Hoffmann U, Bamberg F, Chae CU, et al. Coronary computed tomography angiography for early triage of patients with acute chest pain: the ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J Am Coll Cardiol 2009;53:1642-1650
- Hollander JE, Chang AM, Shofer FS, et al. One-year outcomes following coronary computerized tomographic angiography for evaluation of emergency department patients with potential acute coronary syndrome. Acad Emerg Med 2009;16:693-698
- Rubinshtein R, Halon DA, Gaspar T, et al. Usefulness of 64-slice cardiac computed tomographic angiography for diagnosing acute coronary syndromes and predicting clinical outcome in emergency department patients with chest pain of uncertain origin. Circulation2007;115:1762-1768
- Schlett CL, Banerji D, Siegel E, et al. Prognostic value of CT angiography for major adverse cardiac events in patients with acute chest pain from the emergency department: 2-year outcomes of the ROMICAT trial. JACC Cardiovasc Imaging 2011;4:481-491
- Goldstein JA, Chinnaiyan KM, Abidov A, et al. The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J Am Coll Cardiol 2011;58:1414-1422
- Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med 2012;366:1393-1403
- Shreibati JB, Baker LC, Hlatky MA. Association of coronary CT angiography or stress testing with subsequent utilization and spending among Medicare beneficiaries. JAMA2011;306:2128-2136
- Hoffmann U, Truong QA, Fleg JL, et al. Design of the Rule Out Myocardial Ischemia/Infarction Using Computer Assisted Tomography: a multicenter randomized comparative effectiveness trial of cardiac computed tomography versus alternative triage strategies in patients with acute chest pain in the emergency department. Am Heart J2012;163:330-338
- Abbara S, Arbab-Zadeh A, Callister TQ, et al. SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 2009;3:190-204
- Gerber TC, Carr JJ, Arai AE, et al. Ionizing radiation in cardiac imaging: a science advisory from the American Heart Association Committee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention. Circulation 2009;119:1056-1065
- von Ballmoos MW, Haring B, Juillerat P, Alkadhi H. Meta-analysis: diagnostic performance of low-radiation-dose coronary computed tomography angiography. Ann Intern Med2011;154:413-420[Erratum, Ann Intern Med 2011;154:848.]
- Achenbach S, Marwan M, Ropers D, et al. Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010;31:340-346
- Than M, Cullen L, Reid CM, et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): a prospective observational validation study. Lancet 2011;377:1077-1084
In the EDITORIAL by Redberg RF. Dr. Redberg, Cardiology Division, UCSF made the following points in:
Coronary CT angiography for acute chest pain. N Engl J Med 2012;367:375-376
- Six million people present to ER annually with Acute Chest Pain, most have other diseases that Heart.
- Current diagnostic methods lead to admission to the hospital, unnecessary stays and over-treatment – improvement of outcomes is needed.
- Rule Out Myocardial Infarction Using Computer Assisted Tomography II (ROMICAT-II) 100 patients were randomly assigned to CCTA group or Standard Diagnosis Procedures Group in the ER which involved Stress Test in 74%.
CRITIQUE and Study FLAWS in MGH Study:
- ROMICAT-II enrolled patients only during “weekday daytime hours, no weekend or nights when the costs are higher.
- Assumption that a diagnostic test must be done before discharge for low-to-intermediate-risk patients is unproven and probably unwarranted.. No evidence that the tests performed let to improved outcomes.
- Events rate for patient underwent CCTA, Stress test or no testing at al were less that 1% to have an MI, no one died. Thus, it is impossible to assign a benefit to the CCTA Group. So very low rates were observed in other studies
- CCTA patients were exposed to substantial dose of Radiation, , contrast die,
- Patients underwent ECG and Negative Troponin, no evidence that additional testing further reduced the risk.
- Average age of patients: 54, 47% women.Demographic Characteristics with low incidence of CAD, NEJM, 1979; 300:1350-8
- Risk of Cancer from radiation in younger population is higher, same in women.
- Hoffmann’s Study: Radiation burden was clinically significant: Standard Evaluation Group: (4.7+-8.4 mSv), CCTA: (13.9+-10.4 mSv), exposure of 10 mSv have been projected to lead to 1 death from Cancer per 2000 persons, Arch Intern Med 2009; 169:2071-7
- Middle Age women, increased risk of Breast Cancer from radiation, Arch Intern Med 2012 June 11 (ePub ahead of Print)
- ROMICAT-II study: discharge diagnosis Acute Coronary Syndrome – less than 10%
- CCTA Group: more tests, more radiation, more interventions tht the standard-evaluation group.
- Choose Wisely Campaign – order test only when the benefit will exceed the risks
Dr. Redberd advocates ECG and Troponin, if NORMAL, no further testing.
Epicrisis on Part 1
Redberg’s conclusions are correct for the initial screening. The issue has been whether to do further testing for low or intermediate risk patients.
The most intriguing finding that is not at all surprising is that the CCTA added very little in the suspect group with small or moderate risk. My original studies using a receiver operator characteristic curve were very good, although some patients with CRF or ESRD had extremely high values. The ultra sensitive troponin threw the Area Under the ROC out the window, under the assumption that a perfect assay would exclude AMI, or any injury to the heart. The improved assay does pick up minor elevations of troponin in the absence of MI as a result of plaque rupture. It is possible that 50% of these elevations need medical attention, but then the question is an out of hospital referral or admission and further workup. I have discussed this at some length on several occasions with Dr. Jaffe at Mayo Clinic.
Many of those with minor or intermediate elevation have significant renal insufficiency, but they might also be in CKD Class 3 and not 1 or 2. The coexistence of Type 2 diabetes would go into the standard assessment, but is not mentioned in the study with respect to immediate admission or outcome 28 days after discharge.
The hs troponin I has been in daily use on the Ortho J&J (formerly Kodak) for about 2 years, and the QC standards are very high. I expected the Roche hs-TnT assay to be in use in US as well, but there may have been delays. Januzzi , Jaffe, and Fred Aplle would be involved in the evaluation in the US, but Paul Collinson in UK, Katus and Mair in Germany, and other Europena centers certainly have been using the Roche Assay.
The biggest problem in these studies is as my mentor called my attention to – the frontrunners aren’t going to support a nose-to-nose up front study. Given that a diagnosis requires more information at minimal cost, especially when diagnosis of the heart that are not MI have to be evaluated as well, it is incomprehensibe to me that such information as
- mean arterial blood pressure,
- natriuretic peptides,
- the calculated EGFR are not used in the evaluation.
It is quite impossible to clear the deck when you have patients who don’t have
- ST elevation,
- depression, or
- T-wave inversion who are seen for vague
(not to mention long QT abnormalities).
- predordial tightness or shortness of breath
- pain that resembles gall bladder.
Is this an indication of the obsolescence of the RCT.
A Retrospective Quality and Cost Driven Audit on Effect of hs cTn Assay with On-Site CT Followup. (No treadmill availability)
A retrospective multisite study showed that doing the hs cTn followed by CT on-site was a good choice for US.
I also considered the selective release of
- low- moderate-risk patients cardiology followup in a timely manner.
This report is an excellent analysis of my point by Korley and Jaffe in Medscape, and satisfies some several years discussion
I have had with Dr. Jaffe, at Mayo Clinic. He pointed out the importance of
at a discussion with Dr. Fred Apple at a meeting of the Amer Assn for Clinical Chemistry that he fully elaborates on here.
It is really a refinement of other proposals that are being discussed. It is also timely because hs cTnI is already being used
widely in the US, while there might be a holdup on the hs cTnT.
Highlights
- Need for a Universally Accepted Nomenclature
- Defining Uniform Criteria for Reference Populations
- Discriminating Between Acute and Nonacute Causes of hs-cTn Elevations
- Distinguishing Between Type 1 and Type 2 AMI
- Analytical Imprecision in Cardiac Troponin Assays
- Ruling Out AMI
- Investigating the Causes of Positive Troponin Values in Non-AMI Patients
- Risk Stratifying Patients With Nonacute Coronary Syndrome Conditions
- Conclusions
Abstract
It is only a matter of time before the use of high-sensitivity cardiac
troponin assays (hs-cTn) becomes common throughout the United
States. In preparation for this inevitability, this article raises a number
of important issues regarding these assays that deserve consideration.
These include: the need for
- the adoption of a universal nomenclature; the importance
- of defining uniform criteria for reference populations;
- the challenge of discriminating between acute and nonacute
causes of hs-cTn elevations, and
- between type 1 and type 2 acute myocardial infarction (AMI);
factors influencing the analytical precision of hs-cTn;
- ascertaining the optimal duration of the rule-out period for AMI;
- the need for further evaluation to determine the causes
of a positive hs-cTn in non-AMI patients; and
- the use of hs-cTn to risk-stratify patients with disease conditions
other than AMI.
This review elaborates on these critical issues as a means of
educating clinicians and researchers about them.
Introduction
Recently, clinicians have begun to use the recommended cut-off values
for current generation cardiac troponin (cTn) assays:
- the 99th percentile upper reference limit (URL).
Previously, there was reluctance to use these cut-off values because
- of cTn elevations from non-acute ischemic heart disease conditions.
Thus, there was a tendency to use cut-off values for troponin that equated with the
- prior gold standard diagnosis developed with less sensitive markers
- creatinine kinase-MB isoenzyme (CK-MB) or
- the lowest value at which assay achieved a 10%
coefficient of variation (CV),
which would reduce false-positive elevations (without plaque rupture).
The use of the 99th percentile URL increases the ability of these assays to detect both
- acute myocardial infarction (AMI) and
- structural cardiac morbidities.[1]
This change in practice should not be confused with
- newer-generation high-sensitivity assays.
Improvements in the analytic performance of cTn assays have resulted in
- superior sensitivity and precision.
Improved sensitivity occurs because of
- more sensitive antigen binding and detection antibodies,
- increases in the concentration of the detection probes on the tag antibodies,
- increases in sample volume, and buffer optimization.[2]
Assays now are able to measure
- 10-fold lower concentrations with high precision
(a CV <10% at the 99th percentile of the URL).
The high-sensitivity cardiac troponin T (hs-cTnT) assay is already in clinical use
throughout most of the world. It is only a matter of time before high- sensitivity
assays are approved for use in the United States. In preparation for this, as well as
- using the 99th percentile URL with contemporary assays,
there are a number of important issues that deserve consideration. Key concepts are included in (Table 1).
Table 1: Key ConceptsThere is a need to develop a universal nomenclature for troponin assays.There is a need for uniform criteria for selecting reference populations.The optimal delta criteria for distinguishing between acute and chronic cardiac injury remain unclear and are likely to be assay-specific.Distinguishing between type 1 and type 2 AMI is challenging, and
more type 2 AMIs will be detected with hsTn assays.Factors affecting the analytical precision of troponin assays (including how we collect samples) will become more important with the use of hs-cTn assays.The optimal duration for ruling out AMI remains unclear;
- novel approaches to this issue are being developed.
Elevated hs-cTn, regardless of the cause, has important
- prognostic implications and deserves additional evaluation;
Many cases of chronic elevations can be evaluated in an outpatient setting.
Hs-cTn can be used to
- risk-stratify patients with non-ACS cardiovascular comorbidities.
|
Need for a Universally Accepted Nomenclature
The literature is replete with terms used to refer to cTn assays.
We advocate the use of the term “high-sensitivity cardiac troponin assays” (hs-cTn) for
- cTn assays that v measure cardiac troponin values in
- in at least 50% of a reference population.[2,3]
This policy has now been embraced by the journal Clinical Chemistry. High-sensitivity
assays can be further categorized as well (Table 2) with respect to generations of cTn.
| Table 2. Classification of High-Sensitivity Cardiac Troponin Assays |
|
Category
|
Description
|
First Generation Able to measure cTn in
50%–75% of a reference population |
Second Generation Able to measure cTn in
75%–95% of a reference population |
Third Generation Able to measure cTn in
> 95% a reference population |
| Adapted from Apple and Collinson (3) |
- Ideally, assays should have a CV of <10% at the 99th percentile value.
Assays that do not achieve this level are less sensitive which protects against
false-positive results, and they can be used.[4]
Defining Uniform Criteria for Reference Populations
There is a lack of consistency in the types and numbers of subjects that constitute a reference
population.[2] Often, participants are included after simple screening by check list but without a
- physical examination,
- electrocardiogram, or
- laboratory testing.
At other times, a
- normal creatinine and/or a normal natriuretic peptide value is required.
- Imaging to detect structural heart disease is rarely used.
Because it is known that
- gender,
- age,
- race,
- renal function,
- heart failure, and
- structural heart disease, including
- increased left ventricular (LV) mass
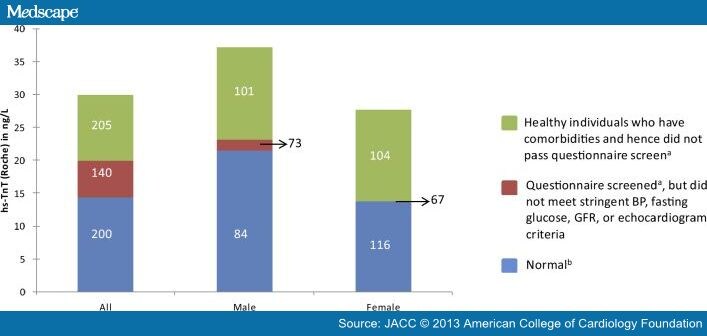
are associated with increased cTn concentrations,[5,6,7] An assay’s 99th percentile value depends on the composition of the reference group. Thus, the more criteria used, the lower the reference values (Figure 1).[5]
http://img.medscape.com/article/803/159/803159-fig1.jpg
Have no history of
- vascular disease or diabetes, and
- not taking cardioactive drugs,
Normal defined as those individuals who had
- no history of vascular or cardiovascular disease,
- diabetes mellitus,
- hypertension, or
- heavy alcohol intake and who were
- receiving no cardiac medication AND
- had blood pressure ≤140/90 mmHg;
- fasting glucose <110 mg/dL;
- eGFR >60mL/min;
- LVEF > 50%; normal lung function; and no significant
- valvular heart disease,
- LVH,
- diastolic HF, or
- regional wall-motion abnormalities on ECHO.
The appropriate reference value to use clinically also is far from a settled issue.
It might be argued that
- using a higher 99th percentile value for the elderly
- allows comparison of the patient to his or her peers, but
in raising the cut-off value, if the increases are caused by comorbidities,
- those who are particularly healthy will be disadvantaged.[8]
Gender and ethnicity are not comorbidities, and we would urge that those should be taken into account.
Regardless of the assay, there will need to be
- 99th percentile values for men that are different for women.[2]
The reference population for assay validation studies should ideally be based on –
demographic characteristics that mirror the U.S. population and include subjects whose
- blood pressure,
- serum glucose, and
- creatinine and
- natriuretic peptide values are
- within the normal reference range and
- who take no cardiac medications.
These subjects should be
- free from structural heart disease,
- documented by echocardiography,
- cardiac magnetic resonance imaging (MRI) or
- computed tomography (CT) angiography.
Meeting these criteria will be a major challenge, especially for older individuals.
A conjoint pool of samples collected with manufacturers’ support so that all methods were derived from an
- identical patient population for their reference ranges would be ideal.
[However, the method of collection and possible freeze-thaw effects is unavoidable].
One large national effort might be advantageous over multiple efforts.
Discriminating Between Acute and Nonacute Causes of hs-cTn Elevations
With the ability to precisely measure small concentrations of cTn,
- clinicians will be faced with the challenge of distinguishing patients
- who have acute problems from those with chronic elevations from other causes.
Using the fourth-generation cTnT assay, approximately 0.7% of patients in
the general population have modest elevations >99th percentile URL.[11]
In the same population, this number was 2% with the hs-cTnT assay.[6] Only
- half of them had documentation (even with imaging) of cardiac abnormalities.
If the prevalence of a positive cTnT is 2% in the general population,
- it will likely be 10% or 20% in the emergency department (ED)
- and even higher in hospitalized patients, as
- these patients often have cardiac comorbidities.
Measurement of changes in hs-cTn over time (δ hs-cTn)
- improves the specificity of hs-cTn for the diagnosis of acute cardiac injury.[12,13]
However, it does so at the cost of sensitivity. With contemporary assays, differences
- in analytical variation have been used to define an increasing pattern.
At elevated values, CV for most assays is in the range of 5% to 7%, so
- a change of 20% ensures that a given change is not caused
by analytical variation alone.[10]
At values near the 99th percentile URL, higher change values are necessary.[13] The situation with hs-cTn assays is much more complex, as follows:
| 1. Change criteria are unique for each assay. |
2. It will be easy to misclassify patients with coronary artery disease who may present with a noncardiac cause of chest pain
- but have elevated values.
They could be having unstable ischemia or elevations caused by structural cardiac abnormalities and noncardiac discomfort.
If hs-cTn is rising significantly, the issue is easy but
- if the values are not rising, a diagnosis of AMI still might be made.
- If so, some patients may be included as having AMI without a changing pattern.
- This occurred in 14% patients studied by Hammarsten et al.[14]
If patients with elevated hs-cTn without a changing pattern are not called AMI,
- should they be called patients with “unstable angina and cardiac injury” or patients with structural heart disease and noncardiac chest pain?
Perhaps both exist? |
3. The release of biomarkers is flow-dependent.Thus, there may not always be rapid access to the circulation. An area of injury distal to a totally occluded vessel (when collateral channels close) may be different in terms of the dynAMIcs of
- hs-cTn change than an intermittently occluded coronary artery.
|
4. Conjoint biological and analytical variation can be measured.
- They are assay-dependent, and the reference change values range from 35% to 85%.[2]
The use of criteria less than that (which may be what is needed clinically) will thus
likely include individuals with changes caused by
- conjoint biological and analytical variation alone.
This has been shown to be the case in
- many patients with nonacute cardiovascular diagnoses.[14,15]
|
| 5. Most evaluations have attempted to define the optimal delta, often with receiver operator curve analysis. Such an approach is based on the concept that sensitivity and specificity deserve equivalent weight.[But higher deltas improve specificity more and lower ones improve sensitivity and it is not clear that all physicians want the same tradeoffs in this regard.]ED physicians often prefer high-sensitivity so that their miss rate is low (<1%),[16] whereas hospital clinicians want increased specificity. This tension will need to be addressed in defining the optimal delta. |
6. The delta associated with AMI may be different from that associated with other cardiac injury.[14] In addition, women have less marked elevations of cTn in response to coronary artery disease[17] and in earlier studies were less apt to have elevated values.[18] Given their pathology is at times different,
- it may be that different metrics may be necessary based on gender
|
7. Some groups have assumed that if a change is of a given magnitude over 6 hours, it can be divided by 6 and the 1-h values can be used.
- This approach is not data driven, and biomarker release is more likely to be discontinuous rather than continuous.[19]
In addition, the values obtained with this approach are too small to be distinguished from a lack of change with most assays. |
These issues pose a major challenge even for defining the ideal delta change value and provide the reasons why
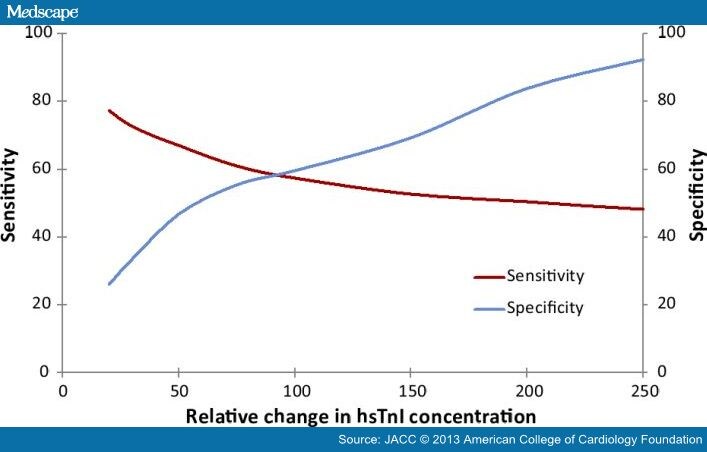
- the use of this approach will reduce sensitivity[20,21] (Figure 2).
http://img.medscape.com/article/803/159/803159-fig2.jpg
Defining the Optimal Delta: Tension Between Sensitivity and Specificity
There is a reciprocal relationship between sensitivity and specificity. With marked percentage changes,
- specificity is improved at the expense of sensitivity, and
- at lower values, the opposite occurs.
In addition, there is controversy in regard to the metrics that should be used with high-sensitivity assays.
The Australian-New Zealand group proposed
- a 50% change for hs-cTnT for values below 53 ng/l and
- a 20% change above that value.[22]
- The 20% change is much less than conjoint biological and analytical variation.
A number of publications have suggested the superiority of
- absolute δ cTn compared to relative δ cTn in discriminating between AMI and non-AMI causes of elevated cTn.[23,24,25]
- The utility of the absolute or relative δ cTn appears to depend on the initial cTn concentration, and
- the major benefit may be at higher values.[23]
A recent publication by Apple et al.[26] calculates deltas in several different ways with a contemporary assay and
- provides a template for how to do such studies optimally.[26]
If all studies were carried out in a similar fashion, it would help immensely. In the long run, institutions will need to
define the approach they wish to take. We believe this discussion is a critical one and should include
- laboratory,
- ED, and
- cardiology professionals.
Distinguishing Between Type 1 and Type 2 AMI
Although δ cTn is helpful in distinguishing between AMI and nonacute causes of Tn release,
- it may or may not be useful in discerning type 1 from type 2 AMI.
As assay sensitivity increases, it appears that the frequency of type 2 AMI increases.
Making this distinction is not easy.
Type 1 AMI is caused by a primary coronary event, usually plaque rupture.
- It is managed acutely with aggressive anticoagulation and
- revascularization (percutaneous coronary intervention or coronary artery bypass).[10]
Type 2 AMI typically evolves secondary to ischemia from an oxygen demand/supply mismatch
- severe tachycardia and
- hypo- or hypertension and the like,
- with or without a coronary abnormality.
These events usually are treated by addressing the underlying abnormalities.
They are particularly common in patients who are
- critically ill and those who
- are postoperative.[27]
However, autopsy studies from patients with postoperative AMI often manifest plaque rupture.[28]
Thus, the more important events, even if less common, may be type 1 AMIs. Type 2 events
seem more common in women, who tend to have
- more endothelial dysfunction,
- more plaque erosion, and
- less fixed coronary artery disease.[28-30]
Additional studies are needed to determine how best to make this clinical distinction.
For now, clinical judgment is recommended.
Analytical Imprecision in Cardiac Troponin Assays
All analytical problems will be more critical with hs-cTn assays. Cardiac troponin I (cTnI) and cardiac troponin T (cTnT) are measured using enzyme linked immune- sorbent assays.
- quantification of hs-cTn can be influenced by interference by reagent antibodies to analyte (cTn), leading to false- positive or negative results.[31]
- Autoantibodies to cTnI or cTnT are found in 5% to 20% of individuals and can reduce detection of cTn.[32,33]
- Additionally, fetal cTn isoforms can be re-expressed in diseased skeletal muscle and detected by the cTnT assays, resulting in false-positive values.[34]
Several strategies, including the use of
- blocking reagents,
- assay redesign, and use of
- antibody fragments,
have been used to reduce interference.[35–36]
There are differences in measured cTn values based on specimen type (serum versus heparinized plasma versus EDTA plasma).
In addition, hemolysis may affect the accuracy of cTn measurement,[37] and with blood draws from peripheral IV lines, common in ICU.
Ruling Out AMI
Studies evaluating the diagnostic performance of hs-cTn assays for the early diagnosis of AMI usually define AMI on
- the basis of a rising and/or falling pattern of current generation cTn values.[21,38]
However, defining AMI on the basis of the less sensitive current generation assay results in an underestimation of the true prevalence of AMI and
- an overestimation of negative predictive value of the experimental assay.
- shortens the time it takes to rule in all the AMIs and
- to definitively exclude AMI as it
- ignores the new AMIs more sensitively detected by the hs-cTn assay.
Thus, in the study by Hammarsten et al.,[14]
- the time to exclude all AMIs was 8.5 hours when all of the AMIs detected
with the high-sensitivity assay were included, whereas
- others that do not include these additional events report this can be done
in 3 to 4 hours.[21,29,38]
In our view, Hammarsten is correct.
This does not mean that hs-cTn cannot help in excluding AMI. Body et al.[39] reported that patients who present with undetectable values (less than the LOB of the hs-cTnT assay) were unlikely to have adverse events during follow-up. If that group of patients is added to those who present later than 6 hours, then perhaps a significant proportion of patients
- with possible acute coronary syndrome (ACS) could
- have that diagnosis excluded with the initial value.[40]
- studies need to continue to evaluate cTn values for at least 6 h
to define the frequency of additional AMIs detected in that manner.
Using follow-up evaluations of patients with small event rates
- who are likely to have additional care during the follow-up period are likely to be underpowered.
It may be that better initial risk stratification may help with this, as recently reported.[16,41]
Low-risk patients who have good follow-up after an ED visit
- may be a group that can be released as early as 2 h after presentation.[16]
Investigating the Causes of Positive Troponin Values in Non-AMI Patients
Elevated Tn values (including those obtained with high-sensitivity assays) are associated with
- a 2-fold higher risk for longer-term all-cause mortality and
- cardiovascular death than a negative troponin values.[6,42-44]
This association is dose-dependent.
- If values are rising, they are indicative of acute cardiac injury.
Those patients should be admitted because the risk is often short-term. However,
- if the values are stable, assuming the timing of any acute event would
allow detection of a changing pattern,
- the risk, although substantive, in our view, often plays out in the longer term.[44]
- Many of these individuals, assuming they are doing well clinically, can be
evaluated outside of the hospital, in our view.
- However, because such elevations are an indicator of a subclinical
cardiovascular injury, such evaluations should be early and aggressive.
Data from several studies suggest that there may well be risk far below the 99th percentile URL value.
Thus, it may evolve that patients in the upper ranges of the normal range also require some degree of cardiovascular evaluation.
Risk Stratifying Patients With Nonacute Coronary Syndrome
Conditions
Patients who have a rising pattern of values have a higher risk of mortality than those with negative values regardless of the cause.
Investigations are ongoing to determine how well results from hs-cTn testing help to risk-stratify patients with
- pulmonary embolism,[45]
- congestive heart failure,[46]
- sepsis,[47]
- hypertensive emergency,[48] and
- chronic obstructive pulmonary disease.[49]
Presently, the studies suggest that cTn values classify patients into clinically relevant risk subgroups. Studies are needed
- to evaluate the incremental prognostic benefit of hs-cTn.
Conclusions
Routine use of hs-cTn assays in the United States is inevitable. These assays hold
the promise of
- improving the sensitivity of AMI diagnoses,
- shortening the duration of AMI evaluation and
- improving the risk stratification of other noncardiac diagnoses.
However, to be able to fully realize their potential, additional studies are needed to address the
- knowledge gaps we have identified. In the interim, clinicians need to
- learn how to use the 99th% URL and
- the concept of changing values
John Adan, MD, FACC
In 2008 CMS commissioned Yale University to analyze 30 days mortality after myocardial infarction in their hospitals.
The study has been based on review of medical records. Consensus criteria for diagnosis of myocardial infarction include
- clinical symptoms,
- EKG,
- troponins,
- CK MB,
- ECHO,
- cath,
- histopathology, etc.
How the reviewed hospitals performed diagnostic coding is unknown. In clinical practice we are bombarded by consults
- for elevated troponins due to causes other than myocardial infarction, like
- pneumonia,
- accelerated hypertension,
- arrhythmias,
- renal failure, etc.
The metric started out over 19%. Now it is below 15%, on average.
CT Angiography (CCTA) Reduced Medical Resource Utilization compared to Standard Care reported in JACC
Aviva Lev-Ari, PhD, RN
http://pharmaceuticalintelligence.com/2013/05/16/ct-angiography-ccta-reduced-medical-resource-utilization-compared-
to-standard-care-reported-in-jacc/?goback=%2Egde_4346921_member_241569351

typical changes in CK-MB and cardiac troponin in Acute Myocardial Infarction (Photo credit: Wikipedia)

Phosphotungstic acid-haematoxylin staining demonstrating contraction band necrosis in an individual that had a myocardial infarction (heart attack). (Photo credit: Wikipedia)
 日本語: トロポニン(SVG修正版)")
English: Troponin(SVG Version) 日本語: トロポニン(SVG修正版) (Photo credit: Wikipedia)
Read Full Post »













 日本語: トロポニン(SVG修正版)")






















{kind=link}
{kind=link}
{kind=link}
{kind=link}