Coronary Reperfusion Therapies: CABG vs PCI – Mayo Clinic preprocedure Risk Score (MCRS) for Prediction of in-Hospital Mortality after CABG or PCI
Author and Curator: Larry H. Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN
Published on Mar 27, 2012
Mayo Clinic cardiologist Charanjit Rihal, M.D. discusses a recent study conducted by Mayo Clinic that focuses on predicting operator outcomes in coronary angioplasty procedures.
“We’ve been interested in prediction of outcomes after coronary angioplasty and stent procedures for some time,” says Dr. Rihal. “Almost ten years ago, we published a paper called ‘The Mayo Clinic Risk Score for Prediction of Adverse Events following Coronary Angioplasty and Stent Procedures’. We’ve since refined into the ‘New Mayo Clinic Risk Score’, which includes seven key variables that predict bad outcomes following PCI procedures.”
The study, which was presented at the 2012 ACC Annual Scientific Session & Expo, presents a novel application of the Mayo Clinic Risk Score to predict operator specific outcomes in coronary angioplasty procedures.
“We looked at the outcomes of over 8000 procedures performed by 21 Mayo Clinic interventional cardiologists as predicted by the Mayo Clinic Risk Score,” says Dr. Rihal. “On an individual basis, we were able to calculate the expected mortality and adverse event rate and compare that to the actual observed mortality and adverse event rate. We were able to show that in our clinical practice of PCI, this risk score was very useful as a performance measure.
In a pleasant surprise, the study also discovered an outlier whose outcomes for instances of adverse event rates were much better than expected. “We don’t know exactly why this operator has such good results,” remarks Dr. Rihal, “But that will be the next phase of this analysis. We can compare procedural, pre-procedural, and post procedural practices of this operator and see if there are things that are translatable to the rest of us.”
VIEW VIDEO
- age,
- creatinine,
- ejection fraction,
- myocardial infarction < or = 24 hours,
- shock,
- congestive heart failure
- peripheral vascular disease
- diabetes mellitus (37.1%)
- hypertension (80.5%)
- peripheral vascular disease (15.3%)
- renal disease (creatinine > or = 1.4 mg/dL; 11.8%).
- age
- estimated creatinine clearance (which has been improved substantially by the Mayo Clinic)
- EF
- AMI < 24 hrs
- Decompensated CHF or shock
- PVD, or carotid artery disease, or PAD
- MAP
- Age falls into interval classes that would suffice for use as classification variables.
- Creatinine is a measurement that is a continuous variable, but I call attention to the fact that eGFR would be preferred, as physicians tend to look at the creatinine roughly in relationship to age, gender, and body size or BMI.
- The laboratory contribution as powerful information is underutilized.
- stable CHF and
- decompensated CHF, or degrees in between?
- Survivals Comparison of Coronary Artery Bypass Graft (CABG) and Percutaneous Coronary Intervention (PCI) / Coronary Angioplasty (emberbranch.wordpress.com)
- Risks of Coronary Artery Bypass Surgery (everydayhealth.com)
- Heart Attack Treatment Options (everydayhealth.com)
- Cabbage Surgery Overview (surgery.answers.com)
- Comparison of cardiothoracic bypass and percutaneous interventional catheterization survivals (pharmaceuticalintelligence.com)
- Functional Flow Reserve in Diagnostic Coronary Angiography Changes Decisions in 25 Percent of Cases (medindia.net)
- High incidence of acute coronary occlusion in patients without protocol positive ST segment elevation referred to an open access primary angioplasty programme. (zedie.wordpress.com)
- Bioresorbable Drug-Eluting Scaffolds Emerging As The Dominant Device Of The Future For Percutaneous Coronary Interventions (medicalnewstoday.com)
Other related articles were published on this Open Access Online Scientific Journal, including:
Survivals Comparison of Coronary Artery Bypass Graft (CABG) and Percutaneous Coronary Intervention (PCI) / Coronary Angioplasty
Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Competition in the Ecosystem of Medical Devices in Cardiac and Vascular Repair: Heart Valves, Stents, Catheterization Tools and Kits for Open Heart and Minimally Invasive Surgery (MIS) (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2012/06/22/competition-in-the-ecosystem-of-medical-devices-in-cardiac-and-vascular-repair-heart-valves-stents-catheterization-tools-and-kits-for-open-heart-and-minimally-invasive-surgery-mis/
Bioabsorbable Drug Coating Scaffolds, Stents and Dual Antiplatelet Therapy (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/29/bioabsorbable-drug-coating-scaffolds-stents-and-dual-antiplatelet-therapy/
Vascular Repair: Stents and Biologically Active Implants (larryhbern)
http://pharmaceuticalintelligence.com/2013/05/04/stents-biologically-active-implants-and-vascular-repair/
Drug Eluting Stents: On MIT’s Edelman Lab’s Contributions to Vascular Biology and its Pioneering Research on DES (larryhbern)
http://pharmaceuticalintelligence.com/2013/04/25/contributions-to-vascular-biology/
Coronary Artery Disease – Medical Devices Solutions: From First-In-Man Stent Implantation, via Medical Ethical Dilemmas to Drug Eluting Stents (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2012/08/13/coronary-artery-disease-medical-devices-solutions-from-first-in-man-stent-implantation-via-medical-ethical-dilemmas-to-drug-eluting-stents/
Survivals Comparison of Coronary Artery Bypass Graft (CABG) and Percutaneous Coronary Intervention (PCI) / Coronary Angioplasty (larryhbern)
http://pharmaceuticalintelligence.com/2013/06/23/comparison-of-cardiothoracic-bypass-and-percutaneous-interventional-catheterization-survivals/
Trans-apical Transcatheter Aortic Valve Replacement in a Patient with Severe and Complex Left Main Coronary Artery Disease (LMCAD) (larryhbern)
http://pharmaceuticalintelligence.com/2013/06/17/management-of-difficult-trans-apical-transcatheter-aortic-valve-replacement-in-a-patient-with-severe-and-complex-arterial-disease/
Transcatheter Aortic Valve Replacement (TAVR): Postdilatation to Reduce Paravalvular Regurgitation During TAVR with a Balloon-expandable Valve (larryhbern)
http://pharmaceuticalintelligence.com/2013/06/17/postdilatation-to-reduce-paravalvular-regurgitation-during-transcatheter-aortic-valve-replacement/
Svelte Medical Systems’ Drug-Eluting Stent: 0% Clinically-Driven Events Through 12-Months in First-In-Man Study (Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/28/svelte-medical-systems-drug-eluting-stent-0-clinically-driven-events-through-12-months-in-first-in-man-study/
Acute and Chronic Myocardial Infarction: Quantification of Myocardial Perfusion Viability – FDG-PET/MRI vs. MRI or PET alone (Justin Pearlman, Aviva Lev-Ari)
http://pharmaceuticalintelligence.com/2013/05/22/acute-and-chronic-myocardial-infarction-quantification-of-myocardial-viability-fdg-petmri-vs-mri-or-pet-alone/
Biomaterials Technology: Models of Tissue Engineering for Reperfusion and Implantable Devices for Revascularization (larryhbern)
http://pharmaceuticalintelligence.com/2013/05/05/bioengineering-of-vascular-and-tissue-models/
Revascularization: PCI, Prior History of PCI vs CABG (A Lev-Ari)
http://pharmaceuticalintelligence.com/2013/04/25/revascularization-pci-prior-history-of-pci-vs-cabg/
Accurate Identification and Treatment of Emergent Cardiac Events (larryhbern)
http://pharmaceuticalintelligence.com/2013/03/15/accurate-identification-and-treatment-of-emergent-cardiac-events/
FDA Pending 510(k) for The Latest Cardiovascular Imaging Technology (A Lev-Ari)
http://pharmaceuticalintelligence.com/2013/01/28/fda-pending-510k-for-the-latest-cardiovascular-imaging-technology/
The ACUITY-PCI score: Will it Replace Four Established Risk Scores — TIMI, GRACE, SYNTAX, and Clinical SYNTAX (A Lev-Ari)
http://pharmaceuticalintelligence.com/2013/01/03/the-acuity-pci-score-will-it-replace-four-established-risk-scores-timi-grace-syntax-and-clinical-syntax/
CABG or PCI: Patients with Diabetes – CABG Rein Supreme (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/11/05/cabg-or-pci-patients-with-diabetes-cabg-rein-supreme/
New Drug-Eluting Stent Works Well in STEMI (A Lev-Ari)
http://pharmaceuticalintelligence.com/2012/08/22/new-drug-eluting-stent-works-well-in-stemi/

Three coronary artery bypass grafts, a LIMA to LAD and two saphenous vein grafts – one to the right coronary artery (RCA) system and one to the obtuse marginal (OM) system. (Photo credit: Wikipedia)

Forrester-classification for classification of Congestive heart failure ; Forrester-Klassifikation zur Einteilung einer akuten Herzinsuffizienz (Photo credit: Wikipedia)







")







 3D computer generated image of chromosomes. Image: cdascher/iStock
3D computer generated image of chromosomes. Image: cdascher/iStock Christine SeidmanThe team focused their gene-mutation search on the exome — the small fraction of each person’s genome that encodes proteins, where disease-causing mutations are most likely to occur. Children with and without congenital heart disease had about the same number of de novomutations — on average, slightly less than one protein-altering mutation each. However, the locations of those mutations were markedly different in the two groups.
Christine SeidmanThe team focused their gene-mutation search on the exome — the small fraction of each person’s genome that encodes proteins, where disease-causing mutations are most likely to occur. Children with and without congenital heart disease had about the same number of de novomutations — on average, slightly less than one protein-altering mutation each. However, the locations of those mutations were markedly different in the two groups.




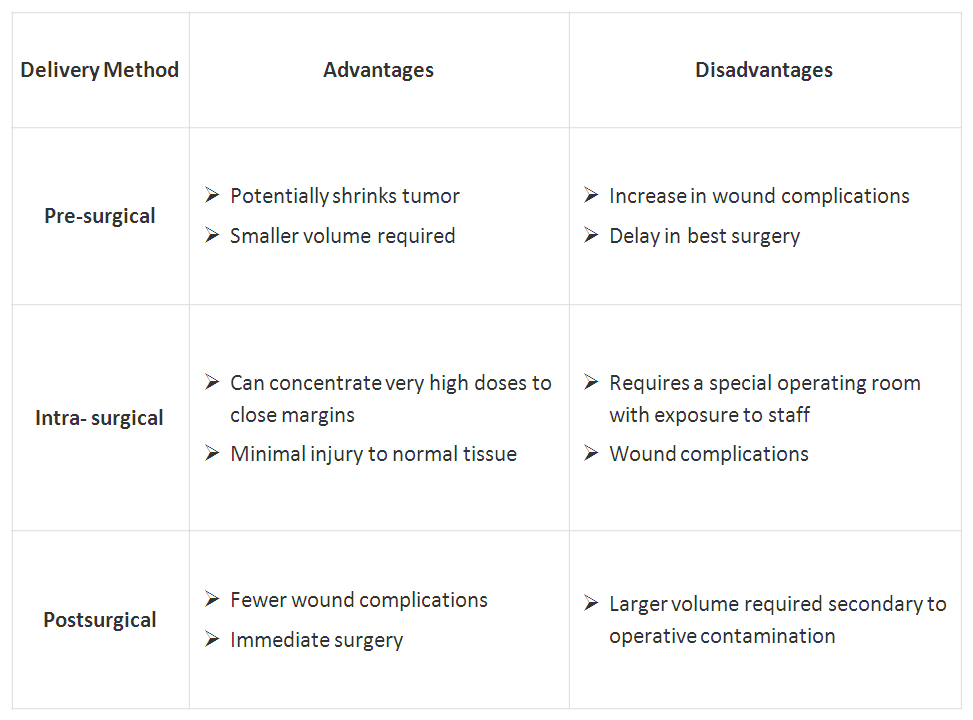 Click on table to enlarge
Click on table to enlarge

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}