Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
The National Heart, Lung, and Blood Institute (NHLBI) convened a Working Group (WG) on August 5 to 6, 2010 in Bethesda, Maryland to discuss future directions of research in heart transplantation (HT). The WG was composed of researchers with expertise in the basic science, clinical science, and epidemiological aspects of advanced heart failure and HT.
These experts were asked to
identify the highest priority research gaps in the field and
make recommendations for future research strategies.
The WG was also asked to include approaches that capitalize on current scientific opportunities and focus on areas that requiredunique NHLBI leadership. Finally, the WG was charged with developing recommendations that would have short- and long-term impact on the field of HT. The WG participants reviewed key areas in HT and identified the most urgent knowledge gaps.
These gaps were then organized into the following 4 specific research directions:
1) enhanced phenotypic characterization of the pre-transplant population;
2) donor-recipient optimization strategies;
3) individualized immunosuppression therapy; and,
4) investigations of immune and non-immune factors affecting late cardiac allograft outcomes.
Finally, because the HT population is relatively small compared with other patient groups, the WG strongly urged concerted efforts to enroll every transplant recipient into a clinical study and to increase collaborative networks to optimize research in this field.
Forrester-classification for classification of Congestive heart failure ; Forrester-Klassifikation zur Einteilung einer akuten Herzinsuffizienz (Photo credit: Wikipedia)
Artificial heart: JARVIK-7 Heart, provided to the National Heart, Lung and Blood Institute (NHLBI) by the University of Utah. (Photo credit: Wikipedia)
Schematic of a transplanted heart with native lungs and the great vessels. (Photo credit: Wikipedia)
In Search of Clarity on Prostate Cancer Screening, Post-Surgical Followup, and Prediction of Long Term Remission
Larry H. Bernstein, MD, FCAP, Author and Curator Dror Nir, PhD, Curator Aviva Lec-Ari, PhD, RN, Curator
Article 10.8. In Search of Clarity on Prostate Cancer Screening, Post-Surgical Followup, and Prediction of Long Term Remission
There have been two important articles in the last several days giving perspectives on the current and evolving status of current and evolving diagnosis of prostate cancer (PCA) by experts Dror Nir, PhD and Aviva Lev-Ari, PhD, RN, Editor-in-Chief, http://Pharmaceuticalintelligence.com
The first article reviews the recent published update on PCA screening and diagnosis, as determined by review of the literature by an Expert Panel, in order to determine what is the current validated Evidence-Based MedicinePractice Guideline for American Urological Surgeons.
The method of review is rigorously laid out and follows the accepted standard for publication. The emphasis in the study lies in the reliance on prostate specific abtigen (PSA), which has undergone an evolutioary improvement sine 1999, although substantiation of a benefit could not be trusted until almost a decade later. The problem the is notable is the absence of discussion of improvements in cancer imaging that has also evolved in that time period, and continues to evolve with molecular probes.
Early Detection of Prostate Cancer: American Urological Association (AUA) Guideline
When reviewing the DETECTION OF PROSTATE CANCER section on the AUA website , The first thing that catches one’s attention is the image below; clearly showing two “guys” exploring with interest what could be a CT or MRI image….
But, if you bother to read the review underneath this image regarding EARLY DETECTION OF PROSTATE CANCER: AUA GUIDELINE produced by an independent group that was commissioned by the AUA to conduct a systematic review and meta-analysis of the published literature on prostate cancer detection and screening; Panel Members: H. Ballentine Carter, Peter C. Albertsen, Michael J. Barry, Ruth Etzioni, Stephen J. Freedland, Kirsten Lynn Greene, Lars Holmberg, Philip Kantoff, Badrinath R. Konety, Mohammad Hassan Murad, David F. Penson and Anthony L. Zietman – You are bound to be left with a strong feeling that something is wrong!
“The AUA commissioned an independent group to conduct a systematic review and meta-analysis of the published literature on prostate cancer detection and screening. The protocol of the systematic review was developed a priori by the expert panel. The search strategy was developed and executed by reference librarians and methodologists and spanned across multiple databases including Ovid Medline In-Process & Other Non-Indexed Citations, Ovid MEDLINE, Ovid EMBASE, Ovid Cochrane Database of Systematic Reviews, Ovid Cochrane Central Register of Controlled Trials and Scopus. Controlled vocabulary supplemented with keywords was used to search for the relevant concepts of prostate cancer, screening and detection. The search focused on DRE, serum biomarkers (PSA, PSA Isoforms, PSA kinetics, free PSA, complexed PSA, proPSA, prostate health index, PSA velocity, PSA doubling time), urine biomarkers (PCA3, TMPRSS2:ERG fusion), imaging (TRUS, MRI, MRS, MR-TRUS fusion), genetics (SNPs), shared-decision making and prostate biopsy. The expert panel manually identified additional references that met the same search criteria”
While reading through the document, I was looking for the findings related to the roll of imaging in prostate cancer screening; see highlighted above. The only thing I found: “With the exception of prostate-specific antigen (PSA)-based prostate cancer screening, there was minimal evidence to assess the outcomes of interest for other tests.”
This must mean that: Notwithstanding hundreds of men-years and tens of millions of dollars which were invested in studies aiming to assess the contribution of imaging to prostate cancer management, no convincing evidence to include imaging in the screening progress was found by a group of top-experts in a thorough and rigorously managed literature survey! And it actually lead the AUA to declare that “Nothing new in the last 20 years”…..
My interpretation of this: It says-it-all on the quality of the clinical studies that were conducted during these years, aiming to develop an improved prostate cancer workflow based on imaging. I hope that whoever reads this post will agree that this is a point worth considering!
For those who do not want to bother reading the whole AUA guidelines document here is a peer reviewed summary:
“Early Detection of Prostate Cancer: AUA Guideline; Carter HB, Albertsen PC, Barry MJ, Etzioni R, Freedland SJ, Greene KL, Holmberg L, Kantoff P, Konety BR, Murad MH, Penson DF, Zietman AL; Journal of Urology (May 2013)”
It says:
“A systematic review was conducted and summarized evidence derived from over 300 studies that addressed the predefined outcomes of interest (prostate cancer incidence/mortality, quality of life, diagnostic accuracy and harms of testing). In addition to the quality of evidence, the panel considered values and preferences expressed in a clinical setting (patient-physician dyad) rather than having a public health perspective. Guideline statements were organized by age group in years (age<40; 40 to 54; 55 to 69; ≥70).
RESULTS: With the exception of prostate-specific antigen (PSA)-based prostate cancer screening, there was minimal evidence to assess the outcomes of interest for other tests. The quality of evidence for the benefits of screening was moderate, and evidence for harm was high for men age 55 to 69 years. For men outside this age range, evidence was lacking for benefit, but the harms of screening, including over diagnosis and over treatment, remained. Modeled data suggested that a screening interval of two years or more may be preferred to reduce the harms of screening.
Prostate Cancer Molecular Diagnostic Market – the Players are: SRI Int’l, Genomic Health w/Cleveland Clinic, Myriad Genetics w/UCSF, GenomeDx and BioTheranostics
On February 6, 2013 we reported that DR. MARK RUBIN, LEADING PROSTATE CANCER AND GENOMICS EXPERT, TO LEAD CUTTING-EDGE CENTER FOR TARGETED, INDIVIDUALIZED PATIENT CARE BASED ON EACH PATIENT’S GENETICS
Genomically Guided Treatment after CLIA Approval: to be offered by Weill Cornell Precision Medicine Institute
On May 16, 2013 we reported a major breakthrough in the Prostate Cancer Screening
A Blood Test to Identify Aggressive Prostate Cancer: a Discovery @ SRI International, Menlo Park, CA
After nearly a decade, my collaborators and I have found the first marker that specifically identifies the approximately six to eight percent of prostate cancers that are considered “aggressive,” meaning they will migrate to other parts of the body, at which point they are very difficult to treat. Although we have confirmed this marker, there is much to be done before a clinical application can be developed.
Prostate Cancer MDx Competition Heating Up; New Data from Genomic Health, Myriad
May 15, 2013 By Turna Ray
Life sciences companies are gearing up for battle to capture the profitable prostate cancer molecular diagnostic market.
Genomic Health and Myriad Genetics both made presentations to the investment community last week about their genomic tests that gauge a man’s risk of prostate cancer aggressiveness. As part of its annual investor day, Myriad discussed new data on its Prolaris test, which analyzes the expression level of 46 cell cycle progression genes and stratifies men’s risk of biochemical recurrence of prostate cancer. If the test reports low gene expression, then the patient is at low risk of disease progression, while high gene expression is associated with disease progression.
Meanwhile, around the same time last week, Genomic Health launched its Oncotype DX prostate cancer test and presented data from the first validation study involving the diagnostic. The Oncotype DX prostate cancer test analyzes the expression of 17 genes within four biological pathways to gauge prostate cancer aggressiveness. The test reports a genomic prostate score from 0 to 100; the lower the score the more certain a patient can be that they can avoid treatment and continue with active surveillance. Prostate cancer patients who are deemed to be at very low risk, low risk, or intermediate risk of progressing are eligible to be tested with the Oncotype Dx test. If, based on standard clinical measures, a person’s prostate cancer is considered high risk, then he is not a candidate for Genomic Health’s test.
These molecular tests are entering the market at a time when currently available tools aren’t specific enough to distinguish between men who have an aggressive form of prostate cancer and therefore, need invasive treatments, and those that are low risk and can do well with active surveillance. According to an NIH estimate, in 2010, the annual medical costs associated with prostate cancer in the US were $12 billion.
It is estimated that each year 23 million men undergo testing for prostate specific antigen, a protein produced by the prostate gland that increases when a man has prostate cancer. Additionally, one million men get a prostate biopsy annually, while 240,000 men end up with a diagnosis for prostate cancer, and around 30,000 die from the disease. Although most of the men diagnosed with prostate cancer end up receiving surgery or radiation treatment, as many as half of these men will probably not progress, and their disease isn’t life threatening.
While PSA testing has been shown to reduce prostate cancer deaths, a man’s PSA level may be increased for reasons other than cancer. As such, broadly screening men for PSA has been controversial in the healthcare community since the test isn’t specific enough to gauge which men are at low risk of developing aggressive prostate cancer and can forgo unnecessary treatments that can have significant side effects.
Both Myriad and Genomic Health are hoping their tests will further refine prostate cancer diagnosis and help doctors gain more confidence in determining which of their patients have aggressive disease and which are at low risk.
Myriad’s advantage
In this highly competitive space, Myriad has the first mover advantage, having launched Prolaris three years ago. The company has published four studies involving the test and conducted a number of trials analyzing around 3,000 patient samples.
Researchers from UCSF and Myriad recently published the fourth validation study in the Journal of Clinical Oncology, which analyzed samples from 400 men who had undergone a radical prostatectomy. In the published study, researchers reported that 100 percent of the men whom Prolaris deemed to be at “low risk” of progression did not experience a recurrence within the five years the study was ongoing. Meanwhile, 50 percent of those the test deemed to be a “high risk” did experience recurrence during that time (PGx Reporter 3/6/2013).
New competition
Like Myriad’s BRACAnalysis test, which comprises more than 80 percent of its product revenues, Genomic Health’s Oncotype DX breast cancer recurrence tests is bringing in the majority of its product revenues. However, the company believes that its newly launched Oncotype DX prostate cancer test stands to be its largest market opportunity to date.
Last week, researchers from University of California, San Francisco, presented data from the first validation study involving the Oncotype DX prostate cancer test. The study involved nearly 400 prostate cancer patients considered low or intermediate risk by standard methods such as Gleason score and showed that when the Oncotype DX score was used in conjunction with other measures, investigators identified more patients as having very low risk disease who were appropriate for active surveillance than when they diagnosed patients without the test score.
More than one third of patients classified as low risk by standard measures in the study were deemed to be “very low risk” by Oncotype DX and therefore could choose active surveillance. Meanwhile, 10 percent of patients in the study were found by clinical measures to be at very low risk or low risk, but the Oncotype DX test deemed them as having aggressive disease that needed treatment.
Matthew Cooperberg of UCSF, who presented data from this validation study at the American Urological Association’s annual meeting last week, highlighted this feature of the Oncotype DX prostate cancer test to investors during a conference call last week. He noted that the test not only gauges which low-risk patients can confidently remain with active surveillance, but it also finds those patients who didn’t receive an accurate risk assessment based on standard clinical measures. “It’s also equally important that we identify the man who frankly should not be on active surveillance, because they’re out there,” he said.
Genomic Health has aligned its test with guidelines from the National Comprehensive Cancer Network, which has expressed concern about over-diagnosis and over-treatment in prostate cancer patients. In 2010, NCCN guidelines established a new “very low risk” category for men with clinically insignificant prostate cancer and recommended that men who fall into this category and have a life expectancy of more than 20 years should only be followed with active surveillance. In 2011, NCCN made the active surveillance criteria more stringent for men in the “very low risk” category.
In order to develop the prostate cancer test, Genomic Health collaborated with the Cleveland Clinic on six feasibility studies and selected the gene expression panel after analyzing 700 genes on tissue samples from 700 patients. The commercial test analyzes the expression of 17 genes across four biological
I am quite surprised that nothing is said about the current status of PSA for Pca, which is far advanced today, and it also needs attention. We are in the old SUFI tale about the blind men who grasped the trunk, or the tail, etc., and called it the elephant.
Robustness of ProsVue™ linear slope for prognostic identification of patients at reduced risk for prostate cancer recurrence: Simulation studies on effects of analytical imprecision and sampling time variation
Mark J. Sarno, Charles S. Davis
Clinical Biochemistry Nov 2012; 45 (16–17): 1479-1484
Highlights
► We simulate effects of analytical and sampling time variation on ProsVue slope.
► Classification switching is minimal in both stable disease and recurrence.
► We provide a framework for assessment of assays using rate of change principles
Objective
The ProsVue assay measures serum total prostate-specific antigen (PSA) over three time points post-radical prostatectomy and calculates rate of change expressed as linear slope. Slopes ≤ 2.0 pg/ml/month are associated with reduced risk for prostate cancer recurrence. However, an indicator based on measurement at multiple time points, calculation of slope, and relation of slope to a binary cutoff may be subject to effects of analytical imprecision and sampling time variation. We performed simulation studies to determine the presence and magnitude of such effects.
Design and methods
Using data from a two-site precision study and a multicenter clinical trial of 304 men, we performed simulation studies to assess whether analytical imprecision and sampling time variation can drive misclassifications or classification switching of patients with stable disease or recurrence.
Results
Analytical imprecision related to expected PSA values in a stable disease population results in ≤ 1.2% misclassifications. For populations with recurrent disease, an analysis taking into account correlation between sampling time points demonstrates that classification switching across the 2.0 pg/ml/month cutoff occurs at a rate ≤ 11%. In the narrow region of overlap between populations, classification switching maximizes at 12.3%. Lastly, sampling time variation across a wide range of scenarios results in 99.7% retention of proper classification for stable disease patients with linear slopes up to the 75th percentile of the distribution.
Conclusions
These results demonstrate the robustness of the ProsVue assay and the linear slope indicator. Further, these simulation studies provide a potential framework for evaluation of future assays that rely on the rate of change principle.
As the reviewer of this paper for Clinical Biochemistry, I have never encountered such a beautiful and rigorous evaluation that is described in the outline below:
Article Outline
1. Introduction
2. Materials and Methods
2.1. Source data
2.2. Simulation 1 – Effects of analytical imprecision in patients with stable disease
2.3. Simulations 2 and 3 – Effects of analytical imprecision in patients with PCa recurrence
2.4. Simulations 4 and 5 – Simulations in highest tertile of stable disease slopes and lowest tertile of recurrent slopes
2.5. Simulation 6 – Effects of sampling time variation
2.6. Software
3. Results
3.1. Source data for simulations
3.2. Simulation 1 – Effects of analytical imprecision in patients with stable disease
3.3. Simulations 2 and 3 – Effects of analytical imprecision in patients with PCa recurrence
3.4. Simulations 4 and 5 — Simulations in highest tertile of stable disease slopes and lowest tertile of recurrent slopes
3.5. Simulation 6 – Effects of sampling time variation
4. Discussion
5. Conclusions
References
This article is followed by another in the Urology journal.
NADiA ProsVue prostate-specific antigen slope is an independent prognostic marker for identifying men at reduced risk of clinical recurrence of prostate cancer after radical prostatectomy.
Moul JW, Lilja H, Semmes OJ, Lance RS, Vessella RL, Fleisher M, Mazzola C, Sarno MJ, Stevens B, Klem RE, McDermed JE, Triebell MT, Adams TH.
Division of Urologic Surgery and Duke Cancer Institute, Duke University Medical Center, Durham, North Carolina 27710, USA. judd.moul@duke.edu
To validate the hypothesis that men displaying serum prostate-specific antigen (PSA) slopes ≤ 2.0 pg/mL/mo after prostatectomy, measured using a new immuno-polymerase chain reaction diagnostic test (NADiA ProsVue), have a reduced risk of clinical recurrence as determined by positive biopsy, imaging findings, or death from prostate cancer.
MATERIALS AND METHODS:
From 4 clinical sites, we selected a cohort of 304 men who had been followed up for 17.6 years after prostatectomy for clinical recurrence. We assessed the prognostic value of a PSA slope cutpoint of 2.0 pg/mL/mo against established risk factors to identify men at low risk of clinical recurrence using uni- and multivariate Cox proportional hazards regression and Kaplan-Meier analyses.
RESULTS:
The univariate hazard ratio of a PSA slope >2.0 pg/mL/mo was 18.3 (95% confidence interval 10.6-31.8) compared with a slope ≤ 2.0 pg/mL/mo (P <.0001). The median disease-free survival interval was 4.8 years vs >10 years in the 2 groups (P <.0001). The multivariate hazard ratio for PSA slope with the covariates of preprostatectomy PSA, pathologic stage, and Gleason score was 9.8 (95% confidence interval 5.4-17.8), an 89.8% risk reduction for men with PSA slopes ≤ 2.0 pg/mL/mo (P <.0001). The Gleason score (<7 vs ≥ 7) was the only other significant predictor (hazard ratio 5.4, 95% confidence interval 2.1-13.8, P = .0004).
CONCLUSION:
Clinical recurrence after radical prostatectomy is difficult to predict using established risk factors. We have demonstrated that a NADiA ProsVue PSA slope of ≤ 2.0 pg/mL/mo after prostatectomy is prognostic for a reduced risk of prostate cancer recurrence and adds predictive power to the established risk factors.
NADiA ProsVue prostate-specific antigen slope is an independent prognostic marker for identifying men at reduced risk of clinical recurrence of prostate cancer after radical prostatectomy. [Urology. 2012]
Some patients who had surgery to remove the prostate may be at higher risk for recurrence. Determining the risk of recurrence is critical for these patients and their physicians in order to make the most informed decision possible about future medical management.
Physicians use post-surgical risk assessment to review a variety of parameters to help determine if the patient might develop recurrent disease. Risk factors may include:
The size and proximity of the tumor at the time of surgery (whether it has grown through the prostate walls):
Through imaging tests, physicians can determine how far cancerous tissue may have spread, with indicators such as
extracapsular extensions (ECE, beyond the prostatic capsule) and
seminal vesicle invasion (SVI, presence in the walls of the vesicles surrounding the prostate).
The presence of cancer cells at the edge of the removed tumor (known as positive margins) or in the lymph nodes outside the prostate.
A high preoperative PSA level (> 20 ng/mL).
The tumor’s Gleason Score (if it is at least 8 or higher).
However, current risk assessment relies on subjective and imprecise information. This uncertainty can have a dramatic impact on a patient’s personal experience after prostatectomy.
The newly available NADiA ProsVue test may help provide a more clear and accurate prediction of a patient’s true risk for clinical recurrence. The NADiA ProsVue test measures
the rate of change of PSA at extremely low levels over time, which can help quickly and accurately identify patients
who are at reduced risk for clinical recurrence.
In conjunction with other information, NADiA ProsVue may allow some men to avoid unnecessary treatments and anxiety after prostatectomy.
NADiA ProsVue is an in-vitro diagnostic assay for determining
rate of change of serum total prostate specific antigen (tPSA) over a period of time (slope, pg/mL per month).
The NADiA ProsVue assay is performed for patients having less than 0.1 ng/mL serum tPSA values (determined by standard-of-care assays that are FDA approved/cleared) in the first sample collected more than 6 weeks after radical prostatectomy.
What is NADiA?
NADiA stands for Nucleic Acid Detection immunoassay. Immuno-PCR, first described by Sano and Cantor in 1992 involves combining protein antigen detection by immunoassay with the detection sensitivity and precision of real-time polymerase chain reaction (qPCR). This amplified DNA-immunoassay approach is similar to that of an enzyme immunoassay, involving antibody binding reactions and intermediate washing steps. The enzyme label is replaced by a strand of DNA and detected by exponential amplification using qPCR.
NADiA employs a soluble (reporter) monoclonal antibody (MAb) labeled with an assay-specific double-stranded DNA sequence.
The presence of this DNA label does not interfere with MAb binding, nor
does the MAb interfere with DNA label amplification and detection.
The second (capturing) MAb specific for another site on the target protein (antigen) is coated onto paramagnetic microparticles.
The reporter MAb-DNA conjugate is reacted with sample in a microtiter plate format to form a first immune complex with the target antigen. The immune complex is then captured onto paramagnetic particles coated with the second capture MAb, forming an insoluble sandwich immune complex. The microparticles are washed by several cycles of magnetic capture and re-suspension to remove excess reporter MAb-DNA conjugate. The specifically bound DNA label is then detected by subjecting
suspended particles to qPCR conditions and monitoring the generations of amplicon in real time.
What are possible clinical applications?
Proteins play a crucial role in all biological functions. Identifying and measuring the quantity of specific proteins is fundamental to understanding the cause and evolution of many human disease processes. There are hundreds of thousands of proteins in the human body, but the vast majority are present at extremely low concentrations. For example, only ten (10) proteins make up 90% of the mass of plasma proteins found in human serum. Twelve (12) proteins make up another 9% of the mass. The remaining proteins comprise the final 1%. Advancing medicine through the study of proteins (known as proteomics) requires powerful and sensitive tools. http://www.irispermed.com/images/pictures/Protein_Slide_2.png
NADiA combines the specificity of an immunoassay with the detection sensitivity of qPCR and can assist efforts to provide clinical insight into many human diseases. Any disease process involving proteins below the detection limits of today’s enzyme immunoassays (EIA) is a potential target for NADiA.
NADiA ProsVue is the first of a line of assays designed to advance human healthcare in the areas of oncology and infectious disease.
NADiA® ProsVue™ is an in-vitro diagnostic assay for determining rate of change of serum total prostate specific antigen over a period of time (slope, pg/mL per month). The NADiA® ProsVue™ assay is performed for patients having less than 0.1 ng/mL serum total PSA values (determined by standard-of-care assays that are FDA approved/cleared) in the first sample collected more than 6 weeks after radical prostatectomy. ProsVue™ slope is indicated for use as a prognostic marker in conjunction with clinical evaluation as an aid in identifying those patients at reduced risk for recurrence of prostate cancer for the eight year period following prostatectomy.
The NADiA® ProsVue™ assay is not intended for the diagnosis or for the monitoring of prostate cancer.
†”Recurrence” is defined as clinical recurrence, not biochemical recurrence, and was documented by positive imaging, positive biopsy, or death due to prostate cancer.
U.S. FDA approves NADiA ProsVue prognostic test for prostate cancer
Posted on September 23, 2011 by Sitemaster
According to a media release issued
Moul et al. have now conducted a retrospective, multi-center clinical trial to further evaluate the potential prognostic value of ProsVue slope at a decision threshold of 2 pg/ml/month. (One nanogram or 1 ng = 1,000 picograms or 1,000 pg.)
The retrospective analysis was based on data from 392 prostate cancer patients who had been given radical prostatectomies between November 1991 and August 2001. To be eligible for this study, all of the following data had to be available from individual patients:
A first post-surgical PSA level of <100 pg/ml (i.e., < 0.1 ng/ml)
Full pathologic and radiographic data
Three frozen serum samples drawn between 6 weeks and 19.4 months post-surgery.
Patients were not eligible if they had received adjuvant radiotherapy and/or hormone therapy after surgery and prior to completion of the three post-surgical blood draws.
The results of this retrospective study showed that:
The average (median) PSA levels of the 392 patients was 6.3 ng/ml (range, 0 to 60.6 ng/ml)
The average (median) post-surgical Gleason score was 7.0 (range, 4 to 10).
73 patients had received neoadjuvant hormone therapy prior to their surgery.
The pathologic stages of the patients were
pT0-2, n = 228
pT3, n = 147
pT4, n = 17
116 patients had positive margins and 8 had positive lymph nodes.
The three post-surgical PSA values were based on serum drawn
after median times of 4.9, 8.6, and 12.8 months and showed median values of 10.7, 23.0 and 50.7 pg/ml, respectively.
The sensitivity, specificity, PPV and NPV for a 2 pg/mL/month ProsVue slope were 75.0, 96.6, 81.4, and 95.2, respectively.
At a median follow-up of 10.5 years, 14 patients had died of prostate cancer and 40 had died overall.
The authors conclude the the ProsVue test “provides information previously unknown” in patients in the first year post-surgery, and that a ProsVue slope of ≤ 2 pg/mL/month in that first year is highly associated with a lack of evidence of progression in long-term follow-up.
In theory, the ProsVue test may have some clinical value in the identification of patients who do not need long-term oncologic follow-up and in predicting the need for adjuvant radiation therapy. However, additional prospective studies will be necessary before this can be confirmed, and the practical clinical value of such a test would depend on whether it is significantly more accurate that data currently available from ultrasensitive PSA testing.
Additional information is available in a media release from the developer of the ProsVue test (IRIS International). According to that media release, the developer has submitted data to the FDA requesting approval to market this test.
The centers involved in this study included Duke University, Memorial Sloan-Kettering Cancer Center, Eastern Virginia Medical Center, and the University of Washington — all of which are highly reputable institutions.
NADiA ProsVue results are calculated as the linear slope of three NADiA ProsVue total PSA test results obtained on three serum samples collected between six weeks and 20 months post-radical prostatectomy.
by IRIS International, the U.S. Food & Drug Administration (FDA) has approved the company’s NADiA® ProsVue™ test as a prognostic marker that can “aid in identifying” men at reduced risk for recurrence of prostate cancer in the first 8 years after a prostatectomy
NADiA ProsVue: A prognostic test for identifying men at a reduced risk for prostate cancer recurrence following radical prostatectomy
J. Moul2, R. Lance1, J. Alter3, M. Sarno3, J. McDermed3 1 Eastern Virginia Medical School, Norfolk, USA 2 Duke Prostate Center, Durham, USA 3 Iris Molecular Diagnostics, Carlsbad, USA
Introduction: Clinical recurrence after radical prostatectomy (RP) is difficult to predict since established factors do not reliably stratify risk. We validated a pre-specified hypothesis that a post-RP NADiA® PSA slope cutpoint of ≤2.0 pg/mL/month (mo) identifies men at reduced risk of clinical recurrence as determined by positive biopsy, imaging or prostate cancer death. This study aimed to compare the prognostic strength of the ProsVue slope cutpoint vs. surgical margin status to identify men at very low risk of post-RP clinical recurrence. Methods: From a cohort of 304 men, surgical margin data was available for 234 men. PSA was measured with a Nucleic Acid Detection Immunoassay (NADiA®) having a limit of quantification of 0.00065 ng (0.65 pg) per mL. Least-squares linear PSA slope (ProsVue™) was calculated using 3 serum samples drawn 1.5-20 mo post-RP. Recurrence risk using a 2.0 pg/mL/mo ProsVue cutpoint and surgical margin status were compared by two survival methods, univariate Cox proportional hazards regression analysis (table) and Kaplan-Meier plots (figure). Results: ProsVue slope ≤2.0 pg/mL/mo was significantly associated with a reduced risk of clinical recurrence by univariate Cox analysis (HR 18.3, 95% CI, 10.6–31.8, P < 0.0001). A negative surgical margin was less significantly associated with a reduced risk of recurrence (HR 3.3, 95% CI 2.0–5.4). Median time to recurrence for men with ProsVue slope ≤2.0 pg/mL/mo and those with negative margins exceeded 17.6 years (yrs). However, median time to recurrence in men with ProsVue slope >2.0 pg/mL/mo was shorter compared to those with positive margins.
NADiA ProsVue Prostate-specific Antigen Slope Is an Independent Prognostic Marker for Identifying Men at Reduced Risk of Clinical Recurrence of Prostate Cancer After Radical Prostatectomy
Judd W. Moul, Hans Lilja, O. John Semmes, Raymond S. Lance, Robert L. Vessella, Martin Fleisher, Clarisse Mazzola, Mark J. Sarno, Barbara Stevens, Robert E. Klem, Jonathan E. McDermed, Melissa T. Triebell, Thomas H. Adams Urology Dec 2012; 80(6): 1319-1327,
Objective To validate the hypothesis that men displaying serum prostate-specific antigen (PSA) slopes ≤2.0 pg/mL/mo after prostatectomy, measured using a new immuno-polymerase chain reaction diagnostic test (NADiA ProsVue), have a reduced risk of clinical recurrence as determined by positive biopsy, imaging findings, or death from prostate cancer. Materials and Methods From 4 clinical sites, we selected a cohort of 304 men who had been followed up for 17.6 years after prostatectomy for clinical recurrence. We assessed the prognostic value of a PSA slope cutpoint of 2.0 pg/mL/mo against established risk factors to identify men at low risk of clinical recurrence using uni- and multivariate Cox proportional hazards regression and Kaplan-Meier analyses. Results The univariate hazard ratio of a PSA slope >2.0 pg/mL/mo was 18.3 (95% confidence interval 10.6-31.8) compared with a slope ≤2.0 pg/mL/mo (P <.0001). The median disease-free survival interval was 4.8 years vs >10 years in the 2 groups (P <.0001). The multivariate hazard ratio for PSA slope with the covariates of preprostatectomy PSA, pathologic stage, and Gleason score was 9.8 (95% confidence interval 5.4-17.8), an 89.8% risk reduction for men with PSA slopes ≤2.0 pg/mL/mo (P <.0001). The Gleason score (<7 vs ≥7) was the only other significant predictor (hazard ratio 5.4, 95% confidence interval 2.1-13.8, P = .0004). Conclusion Clinical recurrence after radical prostatectomy is difficult to predict using established risk factors. We have demonstrated that a NADiA ProsVue PSA slope of ≤2.0 pg/mL/mo after prostatectomy is prognostic for a reduced risk of prostate cancer recurrence and adds predictive power to the established risk factors.
Fifth–Generation Digital Immunoassay for Prostate Specific Antigen by Single Molecule Array Technology.
D.H. Wilson, D.W. Hanlon, G.K. Provuncher, L. Chang, L. Song, P.P. Patel, E.P. Ferrell, H. Lepor,A.W. Partin, D.W. Chan, L.J. Sokoll, C.D. Cheli, R.P. Thiel, D.R. Fournier, and D.C. Duffy http://dx.doi.org/10.1373/clinchem.2011.169540
Measurement of prostate specific antigen (PSA) in prostate cancer patients following radical prostatectomy (RP) has been hindered by the limit of quantification of available assays. Because radical prostatectomy removes the tissue responsible for PSA production, postsurgical PSA is typically undetectable with current assay methods. Evidence suggests, however, that more sensitive determination of PSA status following RP could improve assessment of patient prognosis and response to treatment and better target secondary therapy for those who may benefit most. We developed an investigational digital immunoassay with a 2–logs–lower limit of quantification than current ultrasensitive third–generation PSA assays. We developed reagents for a bead–based ELISA for use with high–density arrays of femtolitervolume wells. Anti–PSA capture beads with immunocomplexes and associated enzyme labels were singulated within the wells of the arrays and interrogated for the presence of enzymatic product. We characterized analytical performance, compared its accuracy with a commercially available test, and analyzed longitudinal serum samples from a pilot study of 33 RP patients. The assay exhibited a functional sensitivity (20% interassay CV) <0.05 pg/mL, total imprecision <10% from 1 to 50 pg/mL, and excellent agreement with the comparator method. All RP samples were well within the assay measurement capability. PSA concentrations following surgery were found to be predictive of prostate cancer recurrence risk over 5 years.The robust 2–log improvement in limit of quantification relative to current ultrasensitive assays and the validated analytical performance of the assay allow for accurate assessment of PSA status after RP.
Risk of prostate cancer in two age groups based on Free PSA as % of Total PSA Catalona W, Partin A, Slawin K, Brawer M, Flanigan R, Patel A, Richie J, deKernion J, Walsh P, Scardino P, Lange P, Subong E, Parson R, Gasior G, Loveland K, Southwick P (1998). “Use of the percentage of free prostate-specific antigen to enhance differentiation of prostate cancer from benign prostatic disease: a prospective multicenter clinical trial”. JAMA 279 (19) : 1542–7. doi:10.1001/jama.279.19.1542. PMID 9605898. (Photo credit: Wikipedia)
English: Human prostate specific antigen (PSA/KLK3) with bound substrate from complex with antibody (PDB id: 2ZCK) (Photo credit: Wikipedia)
Table 1. Side-effects and effects on recovery of treatments for newly diagnosed prostate cancer. The Prostate Brachytherapy Advisory Group: http://www.prostatebrachytherapyinfo.net (Photo credit: Wikipedia)
New Imaging device bears a promise for better quality control of breast-cancer lumpectomies – considering the cost impact
Author and Curator: Dror Nir, PhD
Article 11.5.2 New Imaging device bears a promise for better quality control of breast cancer lumpectomies considering the cost impact
Couple of days ago I have posted on breast-cancer mammography screening and associated costs;Not applying evidence-based medicine drives up the costs of screening for breast-cancer in the USA.Treatment of breast-cancer represents much heavier cost-burden. According to the following publication: Variability in Reexcision Following Breast Conservation Surgery made in JAMA: “Failure to achieve appropriate margins at the initial operation will require additional surgery with re-excision rate estimates ranging from 30% to 60%. These additional operations can produce considerable psychological, physical, and economic stress for patients and delay use of recommended adjuvant therapies. A high percentage (10%-36%) of women requiring reexcision undergo total mastectomy. Thus, the effect of reexcision on altering a patient’s initial treatment of choice is significant.”
Considering that ~70% of the 285,000 new patients diagnosed with breast cancer each year undergoes lumpectomy, this data represents significant cost. Not to mention morbidity, stress and reduce quality of life for the patients. In my post Optical Coherent Tomography – emerging technology in cancer patient managementI discussed the potential of OCT in controlling the quality of lumpectomies in-situ. A workflow that represents potential to reduce the costs of repeated lumpectomies.
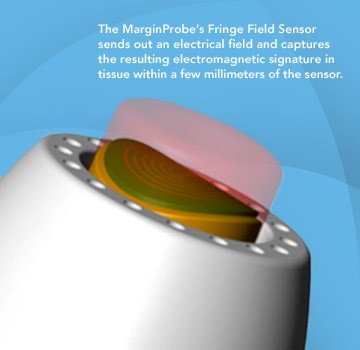
Last week, Dune Medical Devices, Inc., the company that developed the MarginProbeTM System, an intra-operative tissue assessment device to be used as accessory during lumpectomies of early-stage breast cancer, has received Premarket Approval (PMA) by the United States Food and Drug Administration.
FDA approval of the MarginProbe System was based on a 664 patient prospective, multi-center, randomized, double arm study to evaluate the effectiveness of MarginProbe in identifying cancerous tissue along the margins of removed breast tissue during initial lumpectomy procedures. MarginProbe, which uses electromagnetic “signatures” to identify healthy and cancerous tissue, was found to be over three times more effective in finding cancer on the margin during lumpectomy, compared to traditional intra-operative imaging and palpation assessment. This enabled surgeons to significantly reduce the number of patients with positive margins following initial surgery.
The following publication gives an idea on the clinical performance of MarginProbe:
“J Surg Res.2010 May 15;160(2):277-81. doi: 10.1016/j.jss.2009.02.025. Epub 2009 Mar 31.
Diagnostic performance of a novel device for real-time margin assessment in lumpectomy specimens.
Department of General Surgery, Assaf Harofeh Medical Center, Zrifin, Israel. pappo@zahav.net.il
Abstract
BACKGROUND:
Margin status in breast lumpectomy procedures is a prognostic factor for local recurrence and the need to obtain clear margins is often a cause for repeated surgical procedures. A recently developed device for real-time intraoperative margin assessment (MarginProbe; Dune Medical Devices, Caesarea, Israel), was clinically tested. The work presented here looks at the diagnostic performance of the device.
METHODS:
The device was applied to freshly excised lumpectomy and mastectomy specimens at specific tissue measurement sites. These measurement sites were accurately marked, cut out, and sent for histopathologic analysis. Device readings (positive or negative) were compared with histology findings (namely malignant, containing any microscopically detected tumor, or nonmalignant) on a per measurement site basis. The sensitivity and specificity of the device was computed for the full dataset and for additional relevant subgroups.
RESULTS:
A total of 869 tissue measurement sites were obtained from 76 patients, 753 were analyzed, of which 165 were cancerous and 588 were nonmalignant. Device performance on relatively homogeneous sites was: sensitivity 1.00 (95% CI: 0.85-1), specificity 0.87 (95% CI: 0.83-0.90). Performance for the full dataset was: sensitivity 0.70 (95% CI: 0.63-0.77), specificity 0.70 (95% CI: 0.67-0.74). Device sensitivity was estimated to change from 56% to 97% as the cancer feature size increased from 0.7 mm to 6.6 mm. Detection rate of samples containing pure DCIS clusters was not different from rates of samples containing IDC.
CONCLUSIONS:
The device has high sensitivity and specificity in distinguishing between normal and cancer tissue even down to small cancer features.
Copyright (c) 2010 Elsevier Inc. All rights reserved.
PMID: 19628225”
Imagine how cost effective breast cancer management can be if it will involve systems such as these in addition to the systems I discussed in some of my previous posts, for example: What could transform an underdog into a winner?
But one of the things that has been missed along the way is that how we do clinical research will be radically affected as well. We have this big thing about evidence-based medicine and, of course, the sanctimonious randomized, placebo-controlled clinical trial. Well, that’s great if one can do that, but often we’re talking about needing thousands, if not tens of thousands, of patients for these types of clinical trials. And things are changing so fast with respect to medicine and, for example, genomically guided interventions that it’s going to become increasingly difficult to justify these very large clinical trials.
For example, there was a drug trial for melanoma and the mutation of BRAF, which is the gene that is found in about 60% of people with malignant melanoma. When that trial was done, there was a placebo control, and there was a big ethical charge asking whether it is justifiable to have a body count. This was a matched drug for the biology underpinning metastatic melanoma, which is essentially a fatal condition within 1 year, and researchers were giving some individuals a placebo.
Would we even do that kind of trial in the future when we now have such elegant matching of the biological defect and the specific drug intervention? A remarkable example of a trial of the future was announced in May.[1] For this trial, the National Institutes of Health is working with [Banner Alzheimer’s Institute] in Arizona, the University of Antioquia in Colombia, and Genentech to have a specific mutation studied in a large extended family living in the country of Colombia in South America. There is a family of 8000 individuals who have the so-called Paisa mutation, a presenilin gene mutation, which results in every member of this family developing dementia in their 40s.
The unfortunate ending of the Tower of Babel construction project and its effect on modern imaging-based cancer patients’ management
Curator: Dror Nir, PhD
The story of the city of Babel is recorded in the book of Genesis 11 1-9. At that time, everyone on earth spoke the same language.
Picture: Pieter Bruegel the Elder: The Tower of Babel_(Vienna)
It is probably safe to assume that medical practitioners at that time were reporting the status of their patients in a standard manner. Although not mentioned, one might imagine that, at that time, ultrasound or MRI scans were also reported in a standard and transferrable manner. The people of Babel noticed the potential in uniform communication and tried to build a tower so high that it would reach the gods. Unfortunately, God did not like that, so he went down (in person) and confounded people’s speech, so that they could not understand each another. Genesis 11:7–8.
This must be the explanation for our inability to come to a consensus on reporting of patients’ imaging-outcome. Progress in development of efficient imaging protocols and in clinical management of patients is withheld due to high variability and subjectivity of clinicians’ approach to this issue.
Clearly, a justification could be found for not reaching a consensus on imaging protocols: since the way imaging is performed affects the outcome, (i.e. the image and its interpretation) it takes a long process of trial-and-error to come up with the best protocol. But, one might wonder, wouldn’t the search for the ultimate protocol converge faster if all practitioners around the world, who are conducting hundreds of clinical studies related to imaging-based management of cancer patients, report their results in a standardized and comparable manner?
Is there a reason for not reaching a consensus on imaging reporting? And I’m not referring only to intra-modality consensus, e.g. standardizing all MRI reports. I’m referring also to inter-modality consensus to enable comparison and matching of reports generated from scans of the same organ by different modalities, e.g. MRI, CT and ultrasound.
As developer of new imaging-based technologies, my personal contribution to promoting standardized and objective reporting was the implementation of preset reporting as part of the prostate-HistoScanning product design. For use-cases, as demonstrated below, in which prostate cancer patients were also scanned by MRI a dedicated reporting scheme enabled matching of the HistoScanning scan results with the prostate’s MRI results.
The MRI reporting scheme used as a reference is one of the schemes offered in a report by Miss Louise Dickinson on the following European consensus meeting : Magnetic Resonance Imaging for the Detection, Localisation, and Characterisation of Prostate Cancer: Recommendations from a European Consensus Meeting,Louise Dickinson a,b,c,*, Hashim U. Ahmed a,b, Clare Allen d, Jelle O. Barentsz e, Brendan Careyf, Jurgen J. Futterer e, Stijn W. Heijmink e, Peter J. Hoskin g, Alex Kirkham d, Anwar R. Padhani h, Raj Persad i, Philippe Puech j, Shonit Punwani d, Aslam S. Sohaib k, Bertrand Tomball,Arnauld Villers m, Jan van der Meulen c,n, Mark Emberton a,b,c,
Image of MRI reporting scheme taken from the report by Miss Louise Dickinson
The corresponding HistoScanning report is following the same prostate segmentation and the same analysis plans:
Preset reporting enabling matching of HistoScanning and MRI reporting of the same case.
It is my wish that already in the near-future, the main radiology societies (RSNA, ESR, etc..) will join together to build the clinical Imaging’s “Tower of Babel” to effectively address the issue of standardizing reporting of imaging procedures. This time it will not be destroyed…:-)
Knowing the tumor’s size and location, could we target treatment to THE ROI by applying imaging-guided intervention?
Author: Dror Nir, PhD
Article 9.6.Knowing the tumor’s size and location, could we target treatment to THE ROI by applying imaging-guided intervention?
Advances in techniques for cancer lesions’ detection and localisation [1-6] opened the road to methods of localised (“focused”) cancer treatment [7-10]. An obvious challenge on the road is reassuring that the imaging-guided treatment device indeed treats the region of interest and preferably, only it.
A step in that direction was taken by a group of investigators from Sunnybrook Health Sciences Centre, University of Toronto, Ontario, Canada who evaluate the feasibility and safety of magnetic resonance (MR) imaging–controlled transurethral ultrasound therapy for prostate cancer in humans [7]. Their study’s objective was to prove that using real-time MRI guidance of HIFU treatment is possible and it guarantees that the location of ablated tissue indeed corresponds to the locations planned for treatment. Eight eligible patients were recruited.
The setup
Treatment protocol
The result
“There was excellent agreement between the zone targeted for treatment and the zone of thermal injury, with a targeting accuracy of ±2.6 mm. In addition, the temporal evolution of heating was very consistent across all patients, in part because of the ability of the system to adapt to changes in perfusion or absorption properties according to the temperature measurements along the target boundary.”
Technological problems to be resolved in the future:
“Future device designs could incorporate urinary drainage during the procedure, given the accumulation of urine in the bladder during treatment.”
“Sufficient temperature resolution could be achieved only by using 10-mm-thick sections. Our numeric studies suggest that 5-mm-thick sections are necessary for optimal three-dimensional conformal heating and are achievable by using endorectal imaging coils or by performing the treatment with a 3.0-T platform.”
Major limitation: “One of the limitations of the study was the inability to evaluate the efficacy of this treatment; however, because this represents, to our knowledge, the first use of this technology in human prostate, feasibility and safety were emphasized. In addition, the ability to target the entire prostate gland was not assessed, again for safety considerations. We have not attempted to evaluate the effectiveness of this treatment for eradicating cancer or achieving durable biochemical non-evidence of disease status.”
References
SIMMONS (L.A.M.), AUTIER (P.), ZATURA (F.), BRAECKMAN (J.G.), PELTIER (A.), ROMICS (I.), STENZL (A.), TREURNICHT (K.), WALKER (T.), NIR (D.), MOORE (C.M.), EMBERTON (M.). Detection, localisation and characterisation of prostate cancer by Prostate HistoScanning.. British Journal of Urology International (BJUI). Issue 1 (July). Vol. 110, Page(s): 28-35
WILKINSON (L.S.), COLEMAN (C.), SKIPPAGE (P.), GIVEN-WILSON (R.), THOMAS (V.). Breast HistoScanning: The development of a novel technique to improve tissue characterization during breast ultrasound. European Congress of Radiology (ECR), A.4030, C-0596, 03-07/03/2011.
Wendie A. Berg, Kathleen S. Madsen, Kathy Schilling, Marie Tartar, Etta D. Pisano, Linda Hovanessian Larsen, Deepa Narayanan, Al Ozonoff, Joel P. Miller, and Judith E. Kalinyak Breast Cancer: Comparative Effectiveness of Positron Emission Mammography and MR Imaging in Presurgical Planning for the Ipsilateral Breast Radiology January 2011 258:1 59-72.
Anwar R. Padhani, Dow-Mu Koh, and David J. Collins Reviews and Commentary – State of the Art: Whole-Body Diffusion-weighted MR Imaging in Cancer: Current Status and Research Directions Radiology December 2011 261:3 700-718
Eggener S, Salomon G, Scardino PT, De la Rosette J, Polascik TJ, Brewster S. Focal therapy for prostate cancer: possibilities and limitations. Eur Urol 2010;58(1):57–64).
Black, Peter McL. M.D., Ph.D.; Alexander, Eben III M.D.; Martin, Claudia M.D.; Moriarty, Thomas M.D., Ph.D.; Nabavi, Arya M.D.; Wong, Terence Z. M.D., Ph.D.; Schwartz, Richard B. M.D., Ph.D.; Jolesz, Ferenc M.D. Craniotomy for Tumor Treatment in an Intraoperative Magnetic Resonance Imaging Unit. Neurosurgery: September 1999 – Volume 45 – Issue 3 – p 423
Medel, Ricky MD, Monteith, Stephen J. MD, Elias, W. Jeffrey MD, Eames, Matthew PhD, Snell, John PhD, Sheehan, Jason P. MD, PhD, Wintermark, Max MD, MAS, Jolesz, Ferenc A. MD, Kassell, Neal F. MD. Neurosurgery: Magnetic Resonance–Guided Focused Ultrasound Surgery: Part 2: A Review of Current and Future Applications. October 2012 – Volume 71 – Issue 4 – p 755–763
Bruno Quesson PhD, Jacco A. de Zwart PhD, Chrit T.W. Moonen PhD. Magnetic resonance temperature imaging for guidance of thermotherapy. Journal of Magnetic Resonance Imaging, Special Issue: Interventional MRI, Part 1, Volume 12, Issue 4, pages 525–533, October 2000
Introducing smart-imaging into radiologists’ daily practice.
Author and Curator: Dror Nir, PhD
Article 11.3.1 Introducing smart imaging into radiologists daily practice
Radiology congresses are all about imaging in medicine. Interestingly, radiology originates from radiation. It was the discovery of X-ray radiation at the beginning of the 20th century that opened the road to “seeing” the inside of the human body without harming it (at that time that meant cutting into the body).
Radiology meetings are about sharing experience and knowhow on imaging-based management patients. The main topic is always image-interpretation: the bottom line of clinical radiology! This year’s European Congress of Radiology (ECR) dedicated few of its sessions to recent developments in image-interpretation tools. I chose to discuss the one that I consider contributing the most to the future of cancer patients’ management.
In the refresher course dedicated to computer application the discussion was aimed at understanding the question “How do image processing and CAD impact radiological daily practice?” Experts’ reviews gave the audience some background information on the following subjects:
A. The link between image reconstruction and image analysis.
B. Semantic web technologies for sharing and reusing imaging-related information
C. Image processing and CAD: workflow in clinical practice.
I find item A to be a fundamental education item. Not once did I hear a radiologist saying: “I know this is the lesion because it’s different on the image”. Being aware of the computational concepts behind image rendering, even if it is at a very high level and lacking deep understanding of the computational processes, will contribute to more balanced interpretations.
Item B is addressing the dream of investigators worldwide. Imagine that we could perform a web search and find educating, curated materials linking visuals and related clinical information, including standardized pathology reporting. We would only need to remember that search engines used certain search methods and agree, worldwide, on the method and language to be used when describing things. Having such tools is a pre-requisite to successful pharmaceutical and bio-tech development.
I find item C strongly linked to A, as all methods for better image interpretation must fit into a workflow. This is a design goal that is not trivial to achieve. To understand what I mean by that, try to think about how you could integrate the following examples in your daily workflow: i.e. what kind of expertise is needed for execution, how much time it will take, do you have the infrastructure?
In the rest of this post, I would like to highlight, through examples that were discussed during ECR 2012, the aspect of improving cancer patients’ clinical assessment by using information fusion to support better image interpretation.
Adding up quantitative information from MR spectroscopy (quantifies biochemical property of a target lesion) and Dynamic Contrast Enhanced MR imaging (highlights lesion vasculature).
Image provided by: Dr. Pascal Baltzer, director of mammography at the centre for radiology at Friedrich Schiller University in Jena, Germany
Registration of images generated by different imaging modalities (Multi-modal imaging registration).
The following examples: Fig 2 demonstrates registration of a mammography image of a breast lesion to an MRI image of this lesion. Fig3 demonstrates registration of an ultrasound image of a breast lesion scanned by an Automatic Breast Ultrasound (ABUS) system and an MRI image of the same lesion.
Images provided by members of the HAMAM project (an EU, FP7 funded research project: Highly Accurate Breast Cancer Diagnosis through Integration of Biological Knowledge, Novel Imaging Modalities, and Modelling): http://www.hamam-project.org
Multi-modality image registration is usually based on the alignment of image-features apparent in the scanned regions. For ABUS-MRI matching these were: the location of the nipple and the breast thickness; the posterior of the nipple in both modalities; the medial-lateral distance of the nipple to the breast edge on ultrasound; and an approximation of the ribcage using a cylinder on the MRI. A mean accuracy of 14mm was achieved.
Also from the HAMAM project, registration of ABUS image to a mammography image:
registration of ABUS image to a mammography image, Image provided by members of the HAMAM project (an EU, FP7 funded research project: Highly Accurate Breast Cancer Diagnosis through Integration of Biological Knowledge, Novel Imaging Modalities, and Modelling): http://www.hamam-project.org
Automatic segmentation of suspicious regions of interest seen in breast MRI images
Segmentation of suspicious the lesions on the image is the preliminary step in tumor evaluation; e.g. finding its size and location. Since lesions have different signal/image characteristics to the rest of the breast tissue, it gives hope for the development of computerized segmentation techniques. If successful, such techniques bear the promise of enhancing standardization in the reporting of lesions size and location: Very important information for the success of the treatment step.
Roberta Fusco of the National Cancer Institute of Naples Pascal Foundation, Naples/IT suggested the following automatic method for suspicious ROI selection within the breast using dynamic-derived information from DCE-MRI data.
Automatic segmentation of suspicious ROI in breast MRI images, image provided by Roberta Fusco of the National Cancer Institute of Naples Pascal Foundation, Naples/IT
Her algorithm includes three steps (Figure 2): (i) breast mask extraction by means of automatic intensity threshold estimation (Otsu Thresh-holding) on the parametric map obtained through the sum of intensity differences (SOD) calculated pixel by pixel; (ii) hole-filling and leakage repair by means of morphological operators: closing is required to fill the holes on the boundaries of breast mask, filling is required to fill the holes within the breasts, erosion is required to reduce the dilation obtained by the closing operation; (iii) suspicious ROIs extraction: a pixel is assigned to a suspicious ROI if it satisfies two conditions: the maximum of its normalized time-intensity curve should be greater than 0.3 and the maximum signal intensity should be reached before the end of the scan time. The first condition assures that the pixels within the ROI have a significant contrast agent uptake (thus excluding type I and type II curves) and the second condition is required for the time-intensity pattern to be of type IV or V (thus excluding type III curves).
It is generally agreed by radiologists and oncologists that in order to provide a comprehensive work-flow that complies with the principles of personalized medicine, future cancer patients’ management will heavily rely on “smart imaging” applications. These could be accompanied by highly sensitive and specific bio-markers, which are expected to be delivered by pharmaceutical companies in the upcoming decade. In the context of this post, smart imaging refers to imaging systems that are enhanced with tissue characterization and computerized image interpretation applications. It is expected that such systems will enable gathering of comprehensive clinical information on cancer tumors, such as location, size and rate of growth.
What is the main incentive for promoting cancer patients’ management based on smart imaging?
It promises to enable personalized cancer patient management by providing the medical practitioner with a non-invasive and non-destructive tool to detect, stage and follow up cancer tumors in a standardized and reproducible manner. Furthermore, applying smart imaging that provides valuable disease-related information throughout the management pathway of cancer patient will eventually result in reducing the growing burden of health-care costs related to cancer patients’ treatment.
Let’s briefly review the segments that are common to all cancer patients’ pathway: screening, treatment and costs.
Screening for cancer:It is well known that one of the important factors in cancer treatment success is the specific disease staging. Often this is dependent on when the patient is diagnosed as a cancer patient. In order to detect cancer as early as possible, i.e. before any symptoms appear, leaders in cancer patients’ management came up with the idea of screening. To date, two screening programs are the most spoken of: the “officially approved and budgeted” breast cancer screening; and the unofficial, but still extremely costly, prostate cancer screening. After 20 years of practice, both are causing serious controversies:
In trend analysis of WHO mortality data base [1], the authors, Autier P, Boniol M, Gavin A and Vatten LJ, argue that breast cancer mortality in neighboring European countries with different levels of screening but similar access to treatment is the same: “The contrast between the time differences in implementation of mammography screening and the similarity in reductions in mortality between the country pairs suggest that screening did not play a direct part in the reductions in breast cancer mortality”.
In prostate cancer mortality at 11 years of follow-up [2], the authors,Schröder FH et. al. argue regarding prostate cancer patients’ overdiagnosis and overtreatment: “To prevent one death from prostate cancer at 11 years of follow-up, 1055 men would need to be invited for screening and 37 cancers would need to be detected”.
The lobbying campaign (see picture below) that AdmeTech (http://www.admetech.org/) is conducting in order to raise the USA administration’s awareness and get funding to improve prostate cancer treatment is a tribute to patients’ and practitioners’ frustration.
Treatment: Current state of the art in oncology is characterized by a shift in the decision-making process from an evidence-based guidelines approach toward personalized medicine. Information gathered from large clinical trials with regard to individual biological cancer characteristics leads to a more comprehensive understanding of cancer.
Quoting from the National cancer institute (http://www.cancer.gov/) website: “Advances accrued over the past decade of cancer research have fundamentally changed the conversations that Americans can have about cancer. Although many still think of a single disease affecting different parts of the body, research tells us through new tools and technologies, massive computing power, and new insights from other fields that cancer is, in fact, a collection of many diseases whose ultimate number, causes, and treatment represent a challenging biomedical puzzle. Yet cancer’s complexity also provides a range of opportunities to confront its many incarnations”.
Personalized medicine, whether it uses cytostatics, hormones, growth inhibitors, monoclonal antibodies, and loco-regional medical devices, proves more efficient, less toxic, less expensive, and creates new opportunities for cancer patients and health care providers, including the medical industry.
To date, at least 50 types of systemic oncological treatments can be offered with much more quality and efficiency through patient selection and treatment outcome prediction.
Figure taken from presentation given by Prof. Jaak Janssens at the INTERVENTIONAL ONCOLOGY SOCIETY meeting held in Brussels in October 2011
For oncologists, recent technological developments in medical imaging-guided tissue acquisition technology (biopsy) create opportunities to provide representative fresh biological materials in a large enough quantity for all kinds of diagnostic tests.
Health-care economics: We are living in an era where life expectancy is increasing while national treasuries are over their limits in supporting health care costs. In the USA, of the nation’s 10 most expensive medical conditions, cancer has the highest cost per person. The total cost of treating cancer in the U.S. rose from about $95.5 billion in 2000 to $124.6 billion in 2010, the National Cancer Institute (www.camcer.gov) estimates. The true sum is probably higher as this estimate is based on average costs from 2001-2006, before many expensive treatments came out; quoting from www.usatoday.com : “new drugs often cost $100,000 or more a year. Patients are being put on them sooner in the course of their illness and for a longer time, sometimes for the rest of their lives.”
With such high costs at stake, solutions to reduce the overall cost of cancer patients’ management should be considered. My experience is that introducing smart imaging applications into routine use could contribute to significant savings in the overall cost of cancer patients’ management, by enabling personalized treatment choice and timely monitoring of tumors’ response to treatment.










")
")

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}