Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Although first originated in 2003, the world of bioprinting is still very new and ambiguous. Nevertheless, as the need for organ donation continues to increase worldwide, and organ and tissue shortages prevail, a handful of scientists have started utilizing this cutting-edge science and technology for various areas of regenerative medicine to possibly fill that organ-shortage void.
Among these scientists is Ibrahim Tarik Ozbolat, an associate professor of Engineering Science and Mechanics Department and the Huck Institutes of the Life Sciences at Penn State University, who’s been studying bioprinting and tissue engineering for years.
While Ozbolat is not the first to originate 3D bioprinting research, he’s the first one at Penn State University to spearhead the studies at Ozbolat Lab, Leading Bioprinting Research.
“Tissue engineering is a big need. Regenerative medicine, biofabrication of tissues and organs that can replace the damage or diseases is important,” Ozbolat told R&D Magazine after his seminar presentation at Interphex last week in New York City, titled 3D Bioprinting of Living Tissues & Organs.”
3D bioprinting is the process of creating cell patterns in a confined space using 3D-printing technologies, where cell function and viability are preserved within the printed construct.
Recent progress has allowed 3D printing of biocompatible materials, cells and supporting components into complex 3D functional living tissues. The technology is being applied to regenerative medicine to address the need for tissues and organs suitable for transplantation. Compared with non-biological printing, 3D bioprinting involves additional complexities, such as the choice of materials, cell types, growth and differentiation factors, and technical challenges related to the sensitivities of living cells and the construction of tissues. Addressing these complexities requires the integration of technologies from the fields of engineering, biomaterials science, cell biology, physics and medicine, according to nature.com.
“If we’re able to make organs on demand, that will be highly beneficial to society,” said Ozbolat. “We have the capability to pattern cells, locate them and then make the same thing that exists in the body.”
Additive manufacturing, otherwise known as three-dimensional (3D) printing, is driving major innovations in many areas, such as engineering, manufacturing, art, education and medicine. Recent advances have enabled 3D printing of biocompatible materials, cells and supporting components into complex 3D functional living tissues. 3D bioprinting is being applied to regenerative medicine to address the need for tissues and organs suitable for transplantation. Compared with non-biological printing, 3D bioprinting involves additional complexities, such as the choice of materials, cell types, growth and differentiation factors, and technical challenges related to the sensitivities of living cells and the construction of tissues. Addressing these complexities requires the integration of technologies from the fields of engineering, biomaterials science, cell biology, physics and medicine. 3D bioprinting has already been used for the generation and transplantation of several tissues, including multilayered skin, bone, vascular grafts, tracheal splints, heart tissue and cartilaginous structures. Other applications include developing high-throughput 3D-bioprinted tissue models for research, drug discovery and toxicology.
3D printing is increasingly permitting the direct digital manufacture (DDM) of a wide variety of plastic and metal items. While this in itself may trigger a manufacturing revolution, far more startling is the recent development of bioprinters. These artificially construct living tissue by outputting layer-upon-layer of living cells. Currently all bioprinters are experimental. However, in the future, bioprinters could revolutionize medical practice as yet another element of the New Industrial Convergence.
Bioprinters may be constructed in various configurations. However, all bioprinters output cells from a bioprint head that moves left and right, back and forth, and up and down, in order to place the cells exactly where required. Over a period of several hours, this permits an organic object to be built up in a great many very thin layers.
In addition to outputting cells, most bioprinters also output a dissolvable gel to support and protect cells during printing. A possible design for a future bioprinter appears below and in the sidebar, here shown in the final stages of printing out a replacement human heart. Note that you can access larger bioprinter images on the Future Visions page. You may also like to watch my bioprinting video.
Bioprinting Pioneers
Several experimental bioprinters have already been built. For example, in 2002 Professor Makoto Nakamura realized that the droplets of ink in a standard inkjet printer are about the same size as human cells. He therefore decided to adapt the technology, and by 2008 had created a working bioprinter that can print out biotubing similar to a blood vessel. In time, Professor Nakamura hopes to be able to print entire replacement human organs ready for transplant. You can learn more about this groundbreaking work here or read this message from Professor Nakamura. The movie below shows in real-time the biofabrication of a section of biotubing using his modified inkjet technology.
Another bioprinting pioneer is Organovo. This company was set up by a research group lead by Professor Gabor Forgacs from the University of Missouri, and in March 2008 managed to bioprint functional blood vessels and cardiac tissue using cells obtained from a chicken. Their work relied on a prototype bioprinter with three print heads. The first two of these output cardiac and endothelial cells, while the third dispensed a collagen scaffold — now termed ‘bio-paper’ — to support the cells during printing.
Since 2008, Organovo has worked with a company called Invetech to create a commercial bioprinter called the NovoGen MMX. This is loaded with bioink spheroids that each contain an aggregate of tens of thousands of cells. To create its output, the NovoGen first lays down a single layer of a water-based bio-paper made from collagen, gelatin or other hydrogels. Bioink spheroids are then injected into this water-based material. As illustrated below, more layers are subsequently added to build up the final object. Amazingly, Nature then takes over and the bioink spheroids slowly fuse together. As this occurs, the biopaper dissolves away or is otherwise removed, thereby leaving a final bioprinted body part or tissue.
As Organovo have demonstrated, using their bioink printing process it is not necessary to print all of the details of an organ with a bioprinter, as once the relevant cells are placed in roughly the right place Nature completes the job. This point is powerfully illustrated by the fact that the cells contained in a bioink spheroid are capable of rearranging themselves after printing. For example, experimental blood vessels have been bioprinted using bioink spheroids comprised of an aggregate mix of endothelial, smooth muscle and fibroblast cells. Once placed in position by the bioprint head, and with no technological intervention, the endothelial cells migrate to the inside of the bioprinted blood vessel, the smooth muscle cells move to the middle, and the fibroblasts migrate to the outside.
In more complex bioprinted materials, intricate capillaries and other internal structures also naturally form after printing has taken place. The process may sound almost magical. However, as Professor Forgacs explains, it is no different to the cells in an embryo knowing how to configure into complicated organs. Nature has been evolving this amazing capability for millions of years. Once in the right places, appropriate cell types somehow just know what to do.
In December 2010, Organovo create the first blood vessels to be bioprinted using cells cultured from a single person. The company has also successfully implanted bioprinted nerve grafts into rats, and anticipates human trials of bioprinted tissues by 2015. However, it also expects that the first commercial application of its bioprinters will be to produce simple human tissue structures for toxicology tests. These will enable medical researchers to test drugs on bioprinted models of the liver and other organs, thereby reducing the need for animal tests.
In time, and once human trials are complete, Organovo hopes that its bioprinters will be used to produce blood vessel grafts for use in heart bypass surgery. The intention is then to develop a wider range of tissue-on-demand and organs-on-demand technologies. To this end, researchers are now working on tiny mechanical devices that can artificially exercise and hence strengthen bioprinted muscle tissue before it is implanted into a patient.
Organovo anticipates that its first artificial human organ will be a kidney. This is because, in functional terms, kidneys are one of the more straight-forward parts of the body. The first bioprinted kidney may in fact not even need to look just like its natural counterpart or duplicate all of its features. Rather, it will simply have to be capable of cleaning waste products from the blood. You can read more about the work of Organovoand Professor Forgac’s in this article from Nature.
Regenerative Scaffolds and Bones
A further research team with the long-term goal of producing human organs-on-demand has created the Envisiontec Bioplotter. Like Organovo’s NovoGen MMX, this outputs bio-ink ’tissue spheroids’ and supportive scaffold materials including fibrin and collagen hydrogels. But in addition, the Envisontech can also print a wider range of biomaterials. These include biodegradable polymers and ceramics that may be used to support and help form artificial organs, and which may even be used as bioprinting substitutes for bone.
Talking of bone, a team lead by Jeremy Mao at the Tissue Engineering and Regenerative Medicine Lab at Columbia University is working on the application of bioprinting in dental and bone repairs. Already, a bioprinted, mesh-like 3D scaffold in the shape of an incisor has been implanted into the jaw bone of a rat. This featured tiny, interconnecting microchannels that contained ‘stem cell-recruiting substances’. In just nine weeks after implantation, these triggered the growth of fresh periodontal ligaments and newly formed alveolar bone. In time, this research may enable people to be fitted with living, bioprinted teeth, or else scaffolds that will cause the body to grow new teeth all by itself. You can read more about this development in this article from The Engineer.
In another experient, Mao’s team implanted bioprinted scaffolds in the place of the hip bones of several rabbits. Again these were infused with growth factors. As reported inThe Lancet, over a four month period the rabbits all grew new and fully-functional joints around the mesh. Some even began to walk and otherwise place weight on their new joints only a few weeks after surgery. Sometime next decade, human patients may therefore be fitted with bioprinted scaffolds that will trigger the grown of replacement hip and other bones. In a similar development, a team from Washington State University have also recently reported on four years of work using 3D printers to create a bone-like material that may in the future be used to repair injuries to human bones.
In Situ Bioprinting
The aforementioned research progress will in time permit organs to be bioprinted in a lab from a culture of a patient’s own cells. Such developments could therefore spark a medical revolution. Nevertheless, others are already trying to go further by developing techniques that will enable cells to be printed directly onto or into the human body in situ. Sometime next decade, doctors may therefore be able to scan wounds and spray on layers of cells to very rapidly heal them.
Already a team of bioprinting researchers lead by Anthony Alata at the Wake Forrest School of Medicine have developed a skin printer. In initial experiments they have taken 3D scans of test injuries inflicted on some mice and have used the data to control a bioprint head that has sprayed skin cells, a coagulant and collagen onto the wounds. The results are also very promising, with the wounds healing in just two or three weeks compared to about five or six weeks in a control group. Funding for the skin-printing project is coming in part from the US military who are keen to develop in situ bioprinting to help heal wounds on the battlefield. At present the work is still in a pre-clinical phase with Alata progressing his research usig pigs. However, trials of with human burn victims could be a little as five years away.
The potential to use bioprinters to repair our bodies in situ is pretty mind blowing. In perhaps no more than a few decades it may be possible for robotic surgical arms tipped with bioprint heads to enter the body, repair damage at the cellular level, and then also repair their point of entry on their way out. Patients would still need to rest and recuperate for a few days as bioprinted materials fully fused into mature living tissue. However, most patients could potentially recover from very major surgery in less than a week.
Researchers from Harvard Medical School and Massachusetts General Hospital have completed the first stage of an important collaboration aimed at understanding the intricate variables of neuropsychiatric disease—something that currently eludes clinicians and scientists.
The research team, led by Isaac Kohane at HMS and Roy Perlis at Mass General, has created a neuropsychiatric cellular biobank—one of the largest in the world.
It contains induced pluripotent stem cells, or iPSCs, derived from skin cells taken from 100 people with neuropsychiatric diseases such as schizophrenia, bipolar disorder and major depression, and from 50 people without neuropsychiatric illness.
In addition, a detailed profile of each patient, obtained from hours of in-person assessment as well as from electronic medical records, is matched to each cell sample.
As a result, the scientific community can now for the first time access cells representing a broad swath of neuropsychiatric illness. This enables researchers to correlate molecular data with clinical information in areas such as variability of drug reactions between patients. The ultimate goal is to help treat, with greater precision, conditions that often elude effective management.
The cell collection and generation was led by investigators at Mass General, who in collaboration with Kohane and his team are working to characterize the cell lines at a molecular level. The cell repository, funded by the National Institutes of Health, is housed at Rutgers University.
“This biobank, in its current form, is only the beginning,” said Perlis, director of the MGH Psychiatry Center for Experimental Drugs and Diagnostics and HMS associate professor of psychiatry. “By next year we’ll have cells from a total of four hundred patients, with additional clinical detail and additional cell types that we will share with investigators.”
A current major limitation to understanding brain diseases is the inability to access brain biopsies on living patients. As a result, researchers typically study blood cells from patients or examine post-mortem tissue. This is in stark contrast with diseases such as cancer, for which there are many existing repositories of highly characterized cells from patients.
The new biobank offers a way to push beyond this limitation.
A Big Step Forward
While the biobank is already a boon to the scientific community, researchers at MGH and the HMS Department of Biomedical Informatics will be adding additional layers of molecular data to all of the cell samples. This information will include whole genome sequencing and transcriptomic and epigenetic profiling of brain cells made from the stem cell lines.
Collaborators in the HMS Department of Neurobiology, led by Michael Greenberg, department chair and Nathan Marsh Pusey Professor of Neurobiology, will also work to examine characteristics of other types of neurons derived from these stem cells.
“This can potentially alter the entire way we look at and diagnose many neuropsychiatric conditions,” said Perlis.
One example may be to understand how the cellular responses to medication correspond to the patient’s documented responses, comparing in vitro with in vivo. “This would be a big step forward in bringing precision medicine to psychiatry,” Perlis said.
“It’s important to recall that in the field of genomics, we didn’t find interesting connections to disease until we had large enough samples to really investigate these complex conditions,” said Kohane, chair of the HMS Department of Biomedical Informatics.
“Our hypothesis is that here we will require far fewer patients,” he said. “By measuring the molecular functioning of the cells of each patient rather than only their genetic risk, and combining that all that’s known of these people in terms of treatment response and cognitive function, we will discover a great deal of valuable information about these conditions.”
Added Perlis, “In the early days of genetics, there were frequent false positives because we were studying so few people. We’re hoping to avoid the same problem in making cellular models, by ensuring that we have a sufficient number of cell lines to be confident in reporting differences between patient groups.”
The generation of stem cell lines and characterization of patients and brain cell lines is funded jointly by the the National Institute of Mental Health, the National Human Genome Research Institute and a grant from the Centers of Excellence in Genomic Science program.
On C.T.E. and Athletes, Science Remains in Its Infancy
Alzheimer’s disease is the most common form of dementia, characterized by two pathological hallmarks: amyloid-β plaques and neurofibrillary tangles1. The amyloid hypothesis of Alzheimer’s disease posits that the excessive accumulation of amyloid-β peptide leads to neurofibrillary tangles composed of aggregated hyperphosphorylated tau2, 3. However, to date, no single disease model has serially linked these two pathological events using human neuronal cells. Mouse models with familial Alzheimer’s disease (FAD) mutations exhibit amyloid-β-induced synaptic and memory deficits but they do not fully recapitulate other key pathological events of Alzheimer’s disease, including distinct neurofibrillary tangle pathology4, 5. Human neurons derived from Alzheimer’s disease patients have shown elevated levels of toxic amyloid-β species and phosphorylated tau but did not demonstrate amyloid-β plaques or neurofibrillary tangles6, 7, 8, 9, 10, 11. Here we report that FAD mutations in β-amyloid precursor protein and presenilin 1 are able to induce robust extracellular deposition of amyloid-β, including amyloid-β plaques, in a human neural stem-cell-derived three-dimensional (3D) culture system. More importantly, the 3D-differentiated neuronal cells expressing FAD mutations exhibited high levels of detergent-resistant, silver-positive aggregates of phosphorylated tau in the soma and neurites, as well as filamentous tau, as detected by immunoelectron microscopy. Inhibition of amyloid-β generation with β- or γ-secretase inhibitors not only decreased amyloid-β pathology, but also attenuated tauopathy. We also found that glycogen synthase kinase 3 (GSK3) regulated amyloid-β-mediated tau phosphorylation. We have successfully recapitulated amyloid-β and tau pathology in a single 3D human neural cell culture system. Our unique strategy for recapitulating Alzheimer’s disease pathology in a 3D neural cell culture model should also serve to facilitate the development of more precise human neural cell models of other neurodegenerative disorders.
Figure 2: Robust increases of extracellular amyloid-β deposits in 3D-differentiated hNPCs with FAD mutations.close
a, Thin-layer 3D culture protocol. HC, histochemistry; IF, immunofluorescence; IHC, immunohistochemistry. b, Amyloid-β deposits in 6-week differentiated control and FAD ReN cells in 3D Matrigel (green, GFP; blue, 3D6; scale bar, …
In the March 28th, 2016 issue of the journal Nature Medicine, Mark Tuszynski and his colleagues from the University of California, San Diego, in collaboration with colleagues from Japan and Wisconsin, report that they were able to successfully coax stem cell-derived neurons to regenerate damaged corticospinal tracts in rats. Furthermore, this regeneration produced observable, functional benefits.
What is the “corticospinal tract” you ask? The corticospinal tracts are part of the “pyramidal tracts” that include the corticospinal and corticobulbar tracts. The pyramidal tracts are the main controllers of voluntary movement and connect their nerve fibers eventually to cells that serve voluntary muscles and allow them to contract. We call such nerves “motor nerves,” and the corticospinal nerve tracts are among the most important of the motor nerve tracts.
These neural tracts are collectively called “pyramidal tracts” because they pass through a small area of the brain stem known as the pyramids, which lie on the ventral side of the medulla oblongata. Both pyramidal tracts originate in the forebrain; specifically from the so-called “motor cortex” of the forebrain. The motor cortex lies just in front of the central sulcus of the forebrain. In the motor cortex, lies thousands of “upper motor neurons” that extend their axons down to the brain stem and spinal cord.
In the brain stem, the majority of these corticospinal tracts crossover (or decussate) to the other side of the brain stem and travel down the opposite side of the spinal cord. The corticospinal axons extend all the way down the spinal cord, until they make a connection (synapse) with a “lower motor neuron” that extends its axon to the skeletal muscles that it will direct to contract. The corticobulbar tract contains nerves that conduct nerve impulses from cranial nerves and these help the muscles of the face and neck contract, and are involved in facial expressions, swallowing, chewing, and so on.
Damage to the upper motor neurons as a result of a stroke can rob a person of the ability to move, since the muscles that are attached to the upper motor neurons cannot receive any signals to contract. Likewise, damage to the axonal tracts (also known as nerve fibers) can paralyze a patient and rob them of their ability to move.
“We humans use corticospinal axons for voluntary movement,” said Tuszynski. “In the absence of regeneration of this system in previous studies, I was doubtful that most therapies taken to humans would improve function. Now that we can regenerate the most important motor system for humans, I think that the potential for translation is more promising.”
Novel use of EPR spectroscopy to study in vivo protein structure
α-synuclein is a protein found abundantly throughout the brain. It is present mainly at the neuron ends where it is thought to play a role in ensuring the supply of synaptic vesicles in presynaptic terminals, which are required for the release of neurotransmitters to relay signals between neurons. It is critical for normal brain function.
However, α-synuclein is also the primary protein component of the cerebral amyloid deposits characteristic of Parkinson’s disease and its precursor is found in the amyloid plaques of Alzheimer’s disease. Although α-synuclein is present in all areas of the brain, these disease-state amyloid plaques only arise in distinct areas.
Imaging of isolated samples of α-synuclein in vitro indicate that it does not have the precise 3D folded structure usually associated with proteins. It is therefore classed as an intrinsically disordered protein. However, it was not known whether the protein also lacked a precise structure in vivo.
There have been reports that it can form helical tetramers. Since the 3D structure of a biological protein is usually precisely matched to the specific function it performs, knowing the structure of α-synuclein within a living cell will help elucidate its role and may also improve understanding of the disease states with which it is associated.
If α-synuclein remains disordered in vivo, it may be possible for the protein to achieve different structures, and have different properties, depending on its surroundings.
Techniques for determining protein structure
It has long been known that elucidating the structure of a protein at an atomic level is fundamental for understanding its normal function and behavior. Furthermore, such knowledge can also facilitate the development of targeted drug treatments. Unfortunately, observing the atomic structure of a protein in vivo is not straightforward.
X-ray diffraction is the technique usually adopted for visualizing structures at atomic resolution, but this requires crystals of the molecule to be produced and this cannot be done without separating the molecules of interest from their natural environment. Such processes can modify the protein from its usual state and, particularly with complex structures, such effects are difficult to predict.
The development of nuclear magnetic resonance (NMR) spectroscopy improved the situation by making it possible for molecules to be analyzed under in vivo conditions, i.e. same pH, temperature and ionic concentration.
More recently, increases in the sensitivity of NMR and the use of isotope labelling have enabled determinations of the atomic level structure and dynamics of proteins to be determined within living cells1. NMR has been used to determine the structure of a bacterial protein within living cells2 but it is difficult to achieve sufficient quantities of the required protein within mammalian cells and to keep the cells alive for NMR imaging to be conducted.
Electron paramagnetic resonance (EPR) spectroscopy for determining protein structure
Recently, researchers have managed to overcome these obstacles by using in-cell NMR and electron paramagnetic resonance (EPR) spectroscopy. EPR spectroscopy is a technique that is similar to NMR spectroscopy in that it is based on the measurement and interpretation of the energy differences between excited and relaxed molecular states.
In EPR spectroscopy it is electrons that are excited, whereas in NMR signals are created through the spinning of atomic nuclei. EPR was developed to measure radicals and metal complexes, but has also been utilized to study the dynamic organization of lipids in biological membranes3.
EPR has now been used for the first time in protein structure investigations and has provided atomic-resolution information on the structure of α-synuclein in living mammalians4,5.
Bacterial forms of the α-synuclein protein labelled with 15N isotopes were introduced into five types of mammalian cell using electroporation. Concentrations of α-synuclein close to those found in vivo were achieved and the 15N isotopes allowed the protein to be clearly defined from other cellular components by NMR. The conformation of the protein was then determined using electron paramagnetic resonance (EPR).
The results showed that within living mammalian cells α-synuclein remains as a disordered and highly dynamic monomer. Different intracellular environments did not induce major conformational changes.
Summary
The novel use of EPR spectroscopy has resolved the mystery surrounding the in vivo conformation of α-synuclein. It showed that α-synuclein maintains its disordered monomeric form under physiological cell conditions. It has been demonstrated for the first time that even in crowded intracellular environments α-synuclein does not form oligomers, showing that intrinsic structural disorder can be sustained within mammalian cells.
References
Freedberg DI and Selenko P. Live cell NMR Annu. Rev. Biophys. 2014;43:171–192.
Sakakibara D, et al. Protein structure determination in living cells by in-cell NMR spectroscopy. Nature 2009;458:102–105.
Yashroy RC. Magnetic resonance studies of dynamic organisation of lipids in chloroplast membranes. Journal of Biosciences 1990;15(4):281.
Alderson TA and Bax AD. Parkinson’s Disease. Disorder in the court. Nature 2016; doi:10.1038/nature16871.
Theillet FX, et al. Structural disorder of monomeric α-synuclein persists in mammalian cells. Nature 2016; doi:10.1038/nature16531.
The corticospinal tract (CST) is the most important motor system in humans, yet robust regeneration of this projection after spinal cord injury (SCI) has not been accomplished. In murine models of SCI, we report robust corticospinal axon regeneration, functional synapse formation and improved skilled forelimb function after grafting multipotent neural progenitor cells into sites of SCI. Corticospinal regeneration requires grafts to be driven toward caudalized (spinal cord), rather than rostralized, fates. Fully mature caudalized neural grafts also support corticospinal regeneration. Moreover, corticospinal axons can emerge from neural grafts and regenerate beyond the lesion, a process that is potentially related to the attenuation of the glial scar. Rat corticospinal axons also regenerate into human donor grafts of caudal spinal cord identity. Collectively, these findings indicate that spinal cord ‘replacement’ with homologous neural stem cells enables robust regeneration of the corticospinal projection within and beyond spinal cord lesion sites, achieving a major unmet goal of SCI research and offering new possibilities for clinical translation.
Scientists build a living cellular organism with a genome smaller than any known in nature.
By Ruth Williams | March 24, 2016
By stripping down the genome of a mycoplasma bacterium to the minimal genes required for life,Craig Venter and colleagues have created a new organism with the smallest genome of any known cellular life form. The work, published in Sciencetoday (March 24), is the closest scientists have come to creating a cell in which every gene and protein is fully understood—but they are not quite there yet.
“In biology, as we’ve been trying to do genetic and biological engineering, we’re frustrated by the fact that . . . evolution has given us a real mess—it’s really just bubble gum and sticks, piecing together whatever works,” said biomedical engineer Chris Voigt of MIT who was not involved in the study. “This [work] is one of the first attempts at a grand scale to go in and try to clean up some of the mess . . . so that we can better understand the genetics.”
The quest to synthesize a minimal genome with only the essential genes for life is one researchers at the J. Craig Venter Institute (JCVI) in San Diego have been doggedly pursuing for the better part of two decades. Clyde Hutchison, an investigator at JCVI and lead author of the new study, explained the motivation: “We want to understand at a mechanistic level how a living cell grows and divides,” he told The Scientist, and yet, “there is no cell that exists where the function of every gene is known.” Possession of such fundamental knowledge, he added, would also put researchers “in a better position to engineer cells to make specific products,” like pharmaceuticals, Hutchinson said.
The team’s starting point was the bacterium Mycoplasma genitalium, which has the smallest known genome of any living cell with just 525 genes. However, it also has a very slow growth rate, making it difficult to work with. To practice synthesizing genomes and building new organisms, the team therefore turned to M. genitalium’s cousins, M. mycoides and M. capricolum, which have bigger genomes and faster growth rates. In 2010, Venter’s team successfully synthesized a version of the M. mycoides genome (JCVI-syn1.0) and placed it into the cell of a M. capricolum that had had its own genome removed. This was the first cell to contain a fully synthetic genome capable of supporting replicative life.
With the genome synthesis and transfer skills mastered, the next step was to make the genome smaller, explained Hutchison. One approach would be to delete the genes one by one and see which the cells could live without. But “we thought we knew enough, that it would be that much faster to design the genome, build it, and install it in a cell,” said Hutchison. The problem was, “we weren’t completely right about that,” he said. “It took quite a bit longer than we thought.”
Using JCVI-syn1.0 as their starting material, the researchers initially designed a minimal genome based on information from the literature and from mutagenesis studies that suggested which genes were likely essential. They divided this genome into eight overlapping segments and tested each one in combination with the complementary seven-eighths of the standard JCVI-syn1.0 genome. All but one of the designed segments failed to sustain viable cells.
Going back to the drawing board, the team decided to perform mutagenesis experiments on JCVI-syn1.0 to determine, categorically, which genes were required for life. Their experiments revealed that the genes fell into three groups: essential, nonessential, and quasiessential—those that aren’t strictly required, but without which growth is severely impaired. The failure to include these quasiessential genes in the initial design explained in large part why it had failed, explained Hutchison. “The concept of a minimal genome seems simple, but when you get into it, it’s a little more complicated,” he said. “There’s a trade-off between genome size and growth rate.”
Equipped with this knowledge, the team redesigned, synthesized, and tested new genome segments retaining the quasiessential genes. Three iterative cycles of testing later, the team had a genome that successfully supported life.
“This is a really pioneering next step in the use of synthetic biology,” said Leroy Hood, president of the Institute for Systems Biology in Seattle who also did not participate in the research.
Ultimately the team removed 428 genes from the JCVI-syn1.0 genome to create JCVI-syn3.0 with 473 genes (438 protein-coding genes and 35 RNA genes)—considerably fewer than the 525 genes of M. genitalium. Interestingly, the functions of around one-third of the genes (149) remain unknown. “I was surprised it was that high,” said Hood, “but I also think we kid ourselves about how much we know about the genomes of organisms. There’s still an enormous amount of dark matter.”
Some of these genes of unknown function appear to be conserved in higher eukaryotes, said Hutchison. “Those, in a way, are the most exciting,” he said, “because they might represent some new undescribed function that has spread through other life forms.”
C.A. Hutchison III et al., “Design and synthesis of a minimal bacterial genome,” Science, 351: 1414, 2016.
Design and synthesis of a minimal bacterial genome
A goal in biology is to understand the molecular and biological function of every gene in a cell. One way to approach this is to build a minimal genome that includes only the genes essential for life. In 2010, a 1079-kb genome based on the genome of Mycoplasma mycoides (JCV-syn1.0) was chemically synthesized and supported cell growth when transplanted into cytoplasm. Hutchison IIIet al. used a design, build, and test cycle to reduce this genome to 531 kb (473 genes). The resulting JCV-syn3.0 retains genes involved in key processes such as transcription and translation, but also contains 149 genes of unknown function.
INTRODUCTION In 1984, the simplest cells capable of autonomous growth, the mycoplasmas, were proposed as models for understanding the basic principles of life. In 1995, we reported the first complete cellular genome sequences (Haemophilus influenza, 1815 genes, and Mycoplasma genitalium, 525 genes). Comparison of these sequences revealed a conserved core of about 250 essential genes, much smaller than either genome. In 1999, we introduced the method of global transposon mutagenesis and experimentally demonstrated that M. genitalium contains many genes that are nonessential for growth in the laboratory, even though it has the smallest genome known for an autonomously replicating cell found in nature. This implied that it should be possible to produce a minimal cell that is simpler than any natural one. Whole genomes can now be built from chemically synthesized oligonucleotides and brought to life by installation into a receptive cellular environment. We have applied whole-genome design and synthesis to the problem of minimizing a cellular genome. RATIONALE Since the first genome sequences, there has been much work in many bacterial models to identify nonessential genes and define core sets of conserved genetic functions, using the methods of comparative genomics. Often, more than one gene product can perform a particular essential function. In such cases, neither gene will be essential, and neither will necessarily be conserved. Consequently, these approaches cannot, by themselves, identify a set of genes that is sufficient to constitute a viable genome. We set out to define a minimal cellular genome experimentally by designing and building one, then testing it for viability. Our goal is a cell so simple that we can determine the molecular and biological function of every gene.
RESULTS Whole-genome design and synthesis were used to minimize the 1079–kilobase pair (kbp) synthetic genome of M. mycoides JCVI-syn1.0. An initial design, based on collective knowledge of molecular biology in combination with limited transposon mutagenesis data, failed to produce a viable cell. Improved transposon mutagenesis methods revealed a class of quasi-essential genes that are needed for robust growth, explaining the failure of our initial design. Three more cycles of design, synthesis, and testing, with retention of quasi-essential genes, produced JCVI-syn3.0 (531 kbp, 473 genes). Its genome is smaller than that of any autonomously replicating cell found in nature. JCVI-syn3.0 has a doubling time of ~180 min, produces colonies that are morphologically similar to those of JCVI-syn1.0, and appears to be polymorphic when examined microscopically. CONCLUSION The minimal cell concept appears simple at first glance but becomes more complex upon close inspection. In addition to essential and nonessential genes, there are many quasi-essential genes, which are not absolutely critical for viability but are nevertheless required for robust growth. Consequently, during the process of genome minimization, there is a trade-off between genome size and growth rate. JCVI-syn3.0 is a working approximation of a minimal cellular genome, a compromise between small genome size and a workable growth rate for an experimental organism. It retains almost all the genes that are involved in the synthesis and processing of macromolecules. Unexpectedly, it also contains 149 genes with unknown biological functions, suggesting the presence of undiscovered functions that are essential for life. JCVI-syn3.0 is a versatile platform for investigating the core functions of life and for exploring whole-genome design.
Four design-build-test cycles produced JCVI-syn3.0.
(A) The cycle for genome design, building by means of synthesis and cloning in yeast, and testing for viability by means of genome transplantation. After each cycle, gene essentiality is reevaluated by global transposon mutagenesis. (B) Comparison of JCVI-syn1.0 (outer blue circle) with JCVI-syn3.0 (inner red circle), showing the division of each into eight segments. The red bars inside the outer circle indicate regions that are retained in JCVI-syn3.0. (C) A cluster of JCVI-syn3.0 cells, showing spherical structures of varying sizes (scale bar, 200 nm).
Abstract
We used whole-genome design and complete chemical synthesis to minimize the 1079–kilobase pair synthetic genome of Mycoplasma mycoides JCVI-syn1.0. An initial design, based on collective knowledge of molecular biology combined with limited transposon mutagenesis data, failed to produce a viable cell. Improved transposon mutagenesis methods revealed a class of quasi-essential genes that are needed for robust growth, explaining the failure of our initial design. Three cycles of design, synthesis, and testing, with retention of quasi-essential genes, produced JCVI-syn3.0 (531 kilobase pairs, 473 genes), which has a genome smaller than that of any autonomously replicating cell found in nature. JCVI-syn3.0 retains almost all genes involved in the synthesis and processing of macromolecules. Unexpectedly, it also contains 149 genes with unknown biological functions. JCVI-syn3.0 is a versatile platform for investigating the core functions of life and for exploring whole-genome design.
The late Cambridge Mayor Alfred Vellucci welcomed Life Sciences Labs to Cambridge, MA – June 1976
Reporter: Aviva Lev-Ari, PhD, RN
How Cambridge became the Life Sciences Capital
Worth watching is the video below, which captures the initial Cambridge City Council hearing on recombinant DNA research from June 1976. The first speaker is the late Cambridge mayor Alfred Vellucci.
Vellucci hoped to pass a two-year moratorium on gene splicing in Cambridge. Instead, the council passed a three-month moratorium, and created a board of nine Cambridge citizens — including a nun and a nurse — to explore whether the work should be allowed, and if so, what safeguards would be necessary. A few days after the board was created, the pro and con tables showed up at the Kendall Square marketplace.
At the time, says Phillip Sharp, an MIT professor, Cambridge felt like a manufacturing town that had seen better days. He recalls being surrounded by candy, textile, and leather factories. Sharp hosted the citizens review committee at MIT, explaining what the research scientists there planned to do. “I think we built a relationship,” he says.
By early 1977, the citizens committee had proposed a framework to ensure that any DNA-related experiments were done under fairly stringent safety controls, and Cambridge became the first city in the world to regulate research using genetic material.
Testosterone treatment improved primarily sexual function than walking or vitality in older men with low testosterone levels
Reporter and Curator: Dr. Sudipta Saha, Ph.D.
A preliminary study of testosterone therapy in older men with low levels of the hormone and clinical conditions to which low testosterone might contribute, found that restoring levels to those of healthy young men improved sexual function. Treatment had a smaller effect on other aspects of health, such as the ability to walk or the sense of vitality.
A high proportion of older men have testosterone levels well below those found in healthy younger men. In most cases, these low levels are not due to diseases known to affect testosterone levels, such as testicular or pituitary conditions. Many of these men also have symptomatic problems that could be related to low testosterone, including diminished sexual function, decreased mobility and fatigue.
For a long time, there has been interest in whether testosterone is an appropriate therapy for aging-related conditions in men. This study clarifies questions about some of its potential benefits. The study did not find a pattern of increased cardiovascular disease risk. Clarifying the risks requires further study.
Participants included 790 men age 65 and older with serum testosterone levels consistently well below the average for young healthy men. They were randomized to receive testosterone gel applied to the skin or a placebo gel daily. Serum testosterone concentration was measured at one, two, three, six, nine and 12 months. The men were also closely monitored for prostate and cardiovascular problems. In addition to low testosterone, the presence of at least one of three conditions (low sexual function, difficulty in walking or low vitality) was required for eligibility to participate in the T Trials (Testosterone Trials).
Sexual function — In men with low sexual function, testosterone treatment increased sexual activity, sexual desire and erectile function more than placebo treatment.
Physical function — In men with difficulty in walking, testosterone treatment did not significantly affect walking ability, as measured by the distance they could walk in six minutes (a common test of walking ability). However, in all men, walking speed and distance did improve among those who received testosterone compared with placebo.
Vitality — In the group of men with symptoms of low vitality and fatigue, testosterone treatment did not significantly affect fatigue symptoms, but had modest favorable effects on mood.
The trials’ results indicate that, for older men with low sexual function, testosterone treatment can contribute to improved function. In contrast, though, the results don’t indicate that testosterone treatment for older men with low walking ability or vitality will improve these conditions to a great extent. Older men should consult their physicians if considering a testosterone treatment.
Using Zinc Finger Nuclease Technology to Generate CRX-Reporter Human Embryonic Stem Cells as a Tool to Identify and Study the Emergence of Photoreceptors Precursors During Pluripotent Stem Cell Differentiation
Joseph Collin1, Carla B Mellough1, Birthe Dorgau1, Stefan Przyborski2, Inmaculada Moreno-Gimeno3 and Majlinda Lako1,*
The purpose of this study was to generate human embryonic stem cell (hESC) lines harboring the green fluorescent protein (GFP) reporter at the endogenous loci of the Cone-Rod Homeobox (CRX) gene, a key transcription factor in retinal development. Zinc finger nucleases (ZFNs) designed to cleave in the 3′ UTR of CRX were transfected into hESCs along with a donor construct containing homology to the target region, eGFP reporter, and a puromycin selection cassette. Following selection, polymerase chain reaction (PCR) and sequencing analysis of antibiotic resistant clones indicated targeted integration of the reporter cassette at the 3′ of the CRX gene, generating a CRX-GFP fusion. Further analysis of a clone exhibiting homozygote integration of the GFP reporter was conducted suggesting genomic stability was preserved and no other copies of the targeting cassette were inserted elsewhere within the genome. This clone was selected for differentiation towards the retinal lineage. Immunocytochemistry of sections obtained from embryoid bodies and quantitative reverse transcriptase PCR of GFP positive and negative subpopulations purified by fluorescence activated cell sorting during the differentiation indicated a significant correlation between GFP and endogenous CRX expression. Furthermore, GFP expression was found in photoreceptor precursors emerging during hESC differentiation, but not in the retinal pigmented epithelium, retinal ganglion cells, or neurons of the developing inner nuclear layer. Together our data demonstrate the successful application of ZFN technology to generate CRX-GFP labeled hESC lines, which can be used to study and isolate photoreceptor precursors during hESC differentiation. Stem Cells2016;34:311–321
A New Tool for Photoreceptor Production to Treat Vision Loss
The production of replacement cells from human pluripotent stem cell (hPSC) sources has great potential for the treatment of certain forms of vision impairment and blindness. The production of functional stem cell-derived retinal-pigmented epithelium (RPE) is already a notable success, although the equivalent success in photoreceptor cell production has so far lagged behind, due partly to the lack of robust human cell surface markers to allow their purification.
To get round this problem, canny researchers from the laboratory of Majlinda Lako (Newcastle University, United Kingdom) have used zinc finger nuclease (ZFN) gene editing technology to create a reporter embryonic stem cell (ESC) line suitable for the enhanced production of photoreceptor cells [1].
The authors targeted a green fluorescent protein (GFP) reporter into the endogenous locus of the Cone-Rod Homeobox (CRX) transcription factor gene which is known to be selectively expressed post-mitotic retinal photoreceptor precursors. The integration of this reporter into hESCs did not negatively affect genomic stability or pluripotency and, following 3D differentiation to form laminated neural retina [2], GFP expression faithfully mimicked the known expression patterns of CRX (See Figure).
In-depth expression analysis of CRX-positive cells then demonstrated the restriction of GFP-CRX to only two cell types within the 90-day differentiation protocol: RECOVERIN-expressing photoreceptor precursors situated in the developing outer nuclear layer of the optic cup and a subpopulation of non-proliferative retinal progenitors. Importantly, the study detected the expression of genes known to be activated by CRX, so suggesting that GFP-targeting does not affect the functionality of the transcription factor.
In conclusion, the authors have created a CRX-GFP-labeled hESC line which can be used to identify, purify, and study photoreceptor precursors during hESC differentiation, in the hope of improving differentiation protocols, discovering cell surface markers, and developing clinically applicable strategies for transplantation. A great tool for those working towards generating treatments for vision impairment and blindness.
References
Collin J, Mellough CB, Dorgau B, et al. Using Zinc Finger Nuclease Technology to Generate CRX-Reporter Human Embryonic Stem Cells as a Tool to Identify and Study the Emergence of Photoreceptors Precursors During Pluripotent Stem Cell Differentiation. STEM CELLS 2016;34:311-321.
Mellough CB, Collin J, Khazim M, et al. IGF-1 Signaling Plays an Important Role in the Formation of Three-Dimensional Laminated Neural Retina and Other Ocular Structures From Human Embryonic Stem Cells. Stem Cells 2015;33:2416-2430.
Stem Cells Regenerate Human Lens After Cataract Surgery, Restoring Vision
Approach may have broad therapeutic implications on tissue and organ repair
The clouded lens of a cataract in human eye. Photo courtesy of Wikimedia
Researchers at University of California, San Diego School of Medicine and Shiley Eye Institute, with colleagues in China, have developed a new, regenerative medicine approach to remove congenital cataracts in infants, permitting remaining stem cells to regrow functional lenses.
The treatment, which has been tested in animals and in a small, human clinical trial, produced much fewer surgical complications than the current standard-of-care and resulted in regenerated lenses with superior visual function in all 12 of the pediatric cataract patients who received the new surgery.
The findings are published in the March 9 online issue of Nature.
Congenital cataracts – lens clouding that occurs at birth or shortly thereafter – is a significant cause of blindness in children. The clouded lens obstructs the passage of light to the retina and visual information to the brain, resulting in significant visual impairment. Current treatment is limited by the age of the patient and related complications. Most pediatric patients require corrective eyewear after cataract surgery.
“An ultimate goal of stem cell research is to turn on the regenerative potential of one’s own stem cells for tissue and organ repair and disease therapy,” said Kang Zhang, MD, PhD, chief of Ophthalmic Genetics, founding director of the Institute for Genomic Medicine and co-director of Biomaterials and Tissue Engineering at the Institute of Engineering in Medicine, both at UC San Diego School of Medicine.
In the new research, Zhang and colleagues relied upon the regenerative potential of endogenous stem cells. Unlike other stem cell approaches that involve creating stem cells in the lab and introducing them back into the patient, with potential hurdles like pathogen transmission and immune rejection, endogenous stem cells are stem cells already naturally in place at the site of the injury or problem. In the case of the human eye, lens epithelial stem cells or LECs generate replacement lens cells throughout a person’s life, though production declines with age.
Current cataract surgeries largely remove LECs within the lens; the lingering cells generate disorganized regrowth in infants and no useful vision. After confirming the regenerative potential of LECs in animal models, the researchers developed a novel minimally invasive surgery method that preserves the integrity of the lens capsule – a membrane that helps give the lens its required shape to function – and a way to stimulate LECs to grow and form a new lens with vision.
In subsequent tests in animals with cataracts and in a small human trial, they found the new surgical technique allowed pre-existing LECs to regenerate functional lenses. In particular, the human trial involved 12 infants under the age of 2 treated with the new method and 25 similar infants receiving current standard surgical care. The latter control group experienced a higher incidence of post-surgery inflammation, early-onset ocular hypertension and increased lens clouding.
The scientists reported fewer complications and faster healing among the 12 infants who underwent the new procedure and, after three months, a clear, regenerated biconvex lens in all of the patients’ eyes.
“The success of this work represents a new approach in how new human tissue or organ can be regenerated and human disease can be treated, and may have a broad impact on regenerative therapies by harnessing the regenerative power of our own body,” said Zhang, who also has an appointment at Veterans Affairs San Diego Healthcare System.
Zhang said he and colleagues are now looking to expand their work to treating age-related cataracts. Age-related cataracts is the leading cause of blindness in the world. More than 20 million Americans suffer from cataracts, and more than 4 million surgeries are performed annually to replace the clouded lens with an artificial plastic version, called an intraocular lens.
Despite technical advances, a large portion of patients undergoing surgery are left with suboptimal vision post-surgery and are dependent upon corrective eyewear for driving a car and/or reading a book. “We believe that our new approach will result in a paradigm shift in cataract surgery and may offer patients a safer and better treatment option in the future.”
Co-authors on the study include Haotian Lin, Hong Ouyang, Shan Huang, Zhenzhen Liu, Shuyi Chen, Xialin Liu, Lixia Luo, Baoxin Chen, Jiangna Chen, Fu Shang, Xuri Li, Yujuan Wang, Zheng Zhong, and senior author Yishi Liu, Sun Yat-sen University, China; Jie Zhu, Danni Lin, Sherrina Patel, Frances Wu, Christopher Chung, Cindy Wen, Jin Zhu, Austin Qiu, David Granet, Christopher Heichel, Michal Krawczyk, Dorota Skowronska-Krawczyk, Maryam Jafari, William Shi, Daniel Chen, Sheng Zhong, Liangfang Zhang, Jiayi Hou, and Shaochen Chen, UC San Diego; Guiqun Cao, Gen Li, Huimin Cai, and Yanxin Xu, Sichuan University, China; Rui Hou, Guangzhou KangRui Biological Pharmaceutical Technology Company, China; Robert A.J. Singer, Sean Morrison, Ying Zhang, and Richard L. Maas, University of Texas Southwestern Medical Center.
Funding for this research came, in part, from the 973 Program (National Basic Research Program of China); a Major International Joint Research Project (No. 81320108008); 863 Program (State High-Tech Development Plan of China); the National Natural Science Foundation of China; the State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yatsen University; Research to Prevent Blindness; and the Howard Hughes Medical Institute.
The repair and regeneration of tissues using endogenous stem cells represents an ultimate goal in regenerative medicine. To our knowledge, human lens regeneration has not yet been demonstrated. Currently, the only treatment for cataracts, the leading cause of blindness worldwide, is to extract the cataractous lens and implant an artificial intraocular lens. However, this procedure poses notable risks of complications. Here we isolate lens epithelial stem/progenitor cells (LECs) in mammals and show that Pax6 and Bmi1 are required for LEC renewal. We design a surgical method of cataract removal that preserves endogenous LECs and achieves functional lens regeneration in rabbits and macaques, as well as in human infants with cataracts. Our method differs conceptually from current practice, as it preserves endogenous LECs and their natural environment maximally, and regenerates lenses with visual function. Our approach demonstrates a novel treatment strategy for cataracts and provides a new paradigm for tissue regeneration using endogenous stem cells.
Characterization and differentiation of rabbit LECs.
a, LECs were positive for PAX6 (green) and SOX2 (red). b, Lentoid formation (green arrows) with positive αA-crystallin and β-crystallin staining on day 15 of LEC differentiation. c, Left panel, phase-contrast photograph of a lentoid bod…
Lens regeneration in macaque models after minimally invasive surgery.
a, Slit-lamp microscopy showed regenerating lens tissue grew from the peripheral to the central lens in a circular symmetrical pattern 2–3 months after surgery, reaching the centre at 5 months post-surgery. Five months after surgery, di…
Functional characteristics of regenerated human lenses
a, Lens thickness increased significantly 6 and 8 months after surgery (1.9 ± 0.3 and 3.7 ± 0.3 mm, respectively, *P < 0.01), n = 24. b, Lens refractive power increased significantly 6 and 8 months after surgery (5.1 ± 0.5 and 19.0 ± 0…
Conditional deletion of Bmi-1 led to decrease in Pax6+ and Sox2+ cells and cataract formation
A, Loss of Bmi-1 reduced the Pax6+ and Sox2+ LECs population. a, Representative images of haematoxylin and eosin-stained lens sections from Bmi1fl/fl control mice andNestin-cre;Bmi1fl/fl mice. b, Representative images of Bmi-1 (red) st…
Stem Cells Regenerate Human Lens After Cataract Surgery and Restore Vision
Collaboration between scientists from mainland China, the University of California, San Diego School of Medicine and Shiley Eye Institute have developed a new, stem cell-based technique that permits remaining stem cells to regrow functional lenses after the diseased lens was removed. This treatment was initially tested in laboratory animals, but it has now been tested in a small human clinical trial. This procedure produced far fewer surgical complications than the current standard-of-care. The real boost is that this regenerative procedure resulted in regenerated lenses that had superior visual qualities in all 12 of the pediatric cataract patients who served as subjects for this clinical trial.
Kang Zhang, MD, PhD, chief of Ophthalmic Genetics, founding director of the Institute for Genomic Medicine and co-director of Biomaterials and Tissue Engineering at the Institute of Engineering in Medicine, both at UC San Diego School of Medicine, said: “An ultimate goal of stem cell research is to turn on the regenerative potential of one’s own stem cells for tissue and organ repair and disease therapy.” Zhang and his colleagues published their work in the journal Nature.
Cataracts are cloudiness over the lens of the eye that blurs vision. The lens consists mostly of water and protein. When the protein aggregates, it clouds the lens and reduces the light that reaches the retina. This clouding may become severe enough to cause blurred vision. Most age-related cataracts develop from protein clumpings. You do not have to be older to suffer from cataracts. Congenital cataracts occur at birth or shortly after birth. Scarring of the retina or prenatal damage to the eye can cause congenital cataracts. Congenital cataracts are a significant cause of blindness in children. Current treatment for congenital cataracts is limited by the age of the patient. Most pediatric patients require corrective eyewear after cataract surgery.
To address this medical need, Zhang and colleagues examined the regenerative potential of endogenous stem cells on the lens. Unlike other stem cell approaches that involve creating stem cells in the lab and introducing them back into the patient, Zhang decided to use stem cells that are already in place at the site of the injury to do the heavy lifting. In the human eye, lens epithelial stem cells or LECs generate replacement lens cells throughout a person’s life, even though their production declines with age.
Unfortunately, current cataract surgeries essentially remove LECs within the lens. Whatever cells might be left over produce disorganized regrowth in infants and no useful vision. Zhang and his colleagues first confirmed that LECs had regenerative potential. To confirm this, they used laboratory animals. With that knowledge in hand, Zhang and his collaborators devised a novel, minimally invasive surgical procedure that removes the cloudy lens, but manages to maintain the integrity of the membrane that gives the lens its required shape (the lens capsule). With the lens capsule in place, the LECs were activated to replace the missing lens.
Once again, Zhang and his team ensured that their technique worked in animals before they ever tried it on a human patient. Animals with cataracts whose lenses were extirpated, but whose lens capsules were left intact, regenerated new lenses that were devoid of cataracts and provided excellent sight. With their technique honed and ready, Zhang and others tested their procedure on very young human infants in a small human trial. They discovered that their new surgical technique allowed pre-existing LECs to efficiently regenerate functional lenses. In particular, the human trial involved 12 infants under the age of 2 treated with the new method developed by Zhang and others, and 25 similar infants receiving current standard surgical care.
The results were stark: the control group experienced a higher incidence of post-surgery inflammation, early-onset ocular hypertension and increased lens clouding, but those infants who received Zhang’s new procedure showed fewer complications and faster healing. After three months, the 12 infants who underwent the new procedure had a clear, regenerated biconvex lens in all of their eyes.
“The success of this work represents a new approach in how new human tissue or organ can be regenerated and human disease can be treated, and may have a broad impact on regenerative therapies by harnessing the regenerative power of our own body,” said Zhang.
Zhang indicated that he and his colleagues are now looking to apply what they learned in this project to tackling the issue of age-related cataracts. Age-related cataracts are the leading cause of blindness in the world. Over 20 million Americans suffer from cataracts, and more than 4 million surgeries are performed annually to replace the clouded lens with an artificial plastic lens (intraocular lens).
Despite technical advances, a large portion of patients undergoing surgery are left with suboptimal vision post-surgery and are dependent upon corrective eyewear for driving a car and/or reading a book. “We believe that our new approach will result in a paradigm shift in cataract surgery and may offer patients a safer and better treatment option in the future,” said an optimistic Zhang.
Lens stem cells may reside outside the lens capsule: an hypothesis
In this paper, we consider the ocular lens in the context of contemporary developments in biological ideas. We attempt to reconcile lens biology with stem cell concepts and a dearth of lens tumors. Historically, the lens has been viewed as a closed system, in which cells at the periphery of the lens epithelium differentiate into fiber cells. Theoretical considerations led us to question whether the intracapsular lens is indeed self-contained. Since stem cells generate tumors and the lens does not naturally develop tumors, we reasoned that lens stem cells may not be present within the capsule. We hypothesize that lens stem cells reside outside the lens capsule, in the nearby ciliary body. Our ideas challenge the existing lens biology paradigm. We begin our discussion with lens background information, in order to describe our lens stem cell hypothesis in the context of published data. Then we present the ciliary body as a possible source for lens stem cells, and conclude by comparing the ocular lens with the corneal epithelium.
Lens background The vertebrate lens is a transparent cellular structure, specialized to focus and transmit light. The lens is composed of two cell types – epithelial cells that form a single cuboidal layer on the anterior surface, and elongated fiber cells that form the posterior bulk of the lens (Figure 1). A capsule of extracellular matrix components encompasses the lens.
The lens grows slowly throughout life, primarily via cell division in the germinative zone. The germinative zone is a narrow cellular region that rings the lens epithelium toward the periphery of the anterior lens surface. Newly formed cells within the germinative zone elongate and migrate along the inner capsular surface toward the lens equator, forming new lens fiber cells as they continue to elongate and migrate posteriorly beyond the equator. These new fiber cells add to the periphery of the existing fiber cell mass, displacing older fiber cells toward the interior of the expanding lens [1-3]. Central fiber cells are retained for life. Historically, the adult lens has been viewed as a closed system, in which all lens precursor cells or stem cells reside within the capsular confines.
Lens stem cells We use the following definition of lens stem cells – cells with prolonged self-renewing capacity, that produce one or more differentiated cell types with limited proliferative capabilities [4,5]. In general, stem cells are small, undifferentiated cells that reside in contact with a basement membrane in a protected location known as a stem cell niche.
Infrequent stem cell divisions result in one of two cell outcomes. The new cell either remains in its niche as a stem cell, or leaves as a progenitor cell that migrates from the niche to participate in cell differentiation events. Progenitor cells destined for differentiation increase in number through multiple, finite cell divisions as transit amplifying cells [5-7].
A lifetime of cell division in the lens implies the existence of a lens stem cell population. Typically stem cells reside in a protected niche, which for surface or exposed epithelia is a pigment protected and well vascularized location [8,9]. The lens lacks both pigment and a vascular system. An additional point is that tumors often arise from stem cells [10,11], yet the lens does not develop tumors [12,13]. How might these incongruities be reconciled? We hypothesize that the lens is not a closed system. Specifically, lens stem cells may reside outside the lens capsule. If the adult lens does not contain its own stem cell population, we asked where lens stem cells could exist. The pigmented, vascularized ciliary body lies in close proximity to the lens germinative zone, located outside of the lens capsule [14- 17]. We propose that the ciliary body could serve as a potential source of stem cells for the lens. We will discuss the ciliary body in more detail below.
Lens cell lineage If cell migration occurs within the anterior portions of the lens epithelium, the direction of this migration has not been conclusively determined. There is some circumstantial support (enumerated below) for transit amplifying cells of the germinative zone to supply precursors of new epithelial cells, as well as fiber cells. 1) As organisms age, the volume of the lens increases through new fiber cell addition at the lens equator. The growing lens maintains an epithelial cell monolayer over its expanding anterior surface area. While individual lens epithelial cells increase in average size with advancing age, some epithelial cell division is required to maintain the observed cell coverage [23]. New cells are needed in particular toward the periphery of the anterior epithelial region. Transit amplifying cells of the germinative zone are well positioned to fill this need. 2) Apoptosis of lens epithelial cells has been observed in normal and cataractous lenses [28,29]. Extrapolation of estimated apoptosis rates and cell division rates in the central epithelium suggests that replacement epithelial cells originate toward the lens epithelial periphery and migrate centripetally. 3) Injury of cells in the central lens epithelium resulted in increased DNA synthesis within 24 hours in the lens germinative zone. At later time points (four days), DNA synthesis was also observed in more central epithelial cells surrounding the wound [30]. One possible interpretation of these central epithelium wounding studies is that cells from the germinative zone may routinely migrate centripetally to replace damaged epithelial cells. By analogy, limbal cells are the recognized source of new corneal epithelial cells, and central corneal wounding was demonstrated to stimulate limbal cell proliferation [31-33]. 4) In vitro lens cell migration studies performed in an electric field provided indirect support for centripetal migration of lens epithelial cells in vivo [34]. 5) Several other researchers have proposed centripetal migration of lens epithelial cells based on their own diverse experimental observations [35-38].
If transit amplifying cells in the germinative zone provide replacement cells for the anterior epithelium, then cells of the germinative zone would possess differentiation potential for two different lens cell types – epithelial cells and fiber cells. Individual cells may have the potential to differentiate either as epithelial or fiber cells. Alternatively, two distinct precursor cell populations may reside within the lens germinative zone.
Lens stem cell hypothesis While circumstantial evidence implicates the germinative zone as the source of new cells for lens epithelium as well as for fiber cells, results from a recent study seem to contradict these ideas. …
Ciliary body, a possible source of lens stem cells If the encapsulated lens does not contain its own stem cell population, we asked where lens stem cells could reside. The ciliary body is a pigmented and vascularized tissue, that lies physically close to the lens germinative zone [14- 16,41]. The ciliary body represents the anterior extension of the choroid, and is situated between the choroid and the iris. The epithelium of the ciliary body consists of two cell layers, an inner non-pigmented epithelium, and an outer pigmented epithelium in intimate contact with capillaries [16]. The ciliary epithelial layers represent anterior extensions of the inner non-pigmented neural retina and the outer pigmented retinal epithelium, respectively. (The terms ‘inner’ and ‘outer’ are used in reference to the ocular globe interior.) A recognized stem cell population – the retinal stem cells – resides in the ciliary body [42-44]. …
Posterior capsule opacification If the continuity of the lens capsule is breached, however, extralenticular cell migration into the area delimited by the lens capsule likely occurs. Cataract extraction disrupts the lens capsule. Subsequent cell growth and migration on the remaining capsule lead to complications in 25% of adult patients (and nearly 100% of pediatric patients) that again compromise vision [71-73]. These complications, known as after-cataract or posterior capsule opacification, are believed to primarily involve proliferation and migration of lens epithelial cells left behind during cataract surgery [74-77]. There is also evidence that cells originating in non-lens ocular tissues participate in cell aggregates within the remaining capsule [78-80].
In posterior capsule opacification, the majority of aberrant cell growth is attributed to lens cells originating within the capsule. However, if our hypothesis is correct that lens stem cells normally reside outside the lens capsule, then much of this aberrant growth may actually arise from lens progenitor cells that migrate to the capsule after the cataract surgery.
Analogies to corneal epithelium If our lens literature summary seems contrived to explain an improbable lens stem cell hypothesis, consider the corneal epithelium. Like the lens, the corneal epithelium is a transparent, avascular ocular tissue, specialized to focus and transmit light [81]. One major difference between cornea and lens is that the cornea also provides a protective surface for the eye. In its protective role at the environment interface, the corneal epithelium has well developed tissue replacement capabilities to repair normal wear and minor injuries [82,83]. In contrast, lens cell division occurs on a more limited scale.
Conclusion In light of concepts that have evolved in stem cell literature in recent years, we re-examine the ocular lens in the context of features common to other biological tissues. Since the lens grows throughout life and does not naturally develop tumors, we ask whether lens stem cells could reside in a more typical stem cell niche, one that is pigmented and vascularized. We hypothesize that lens stem cells reside outside the lens capsule in nearby pigmented ocular tissue, the ciliary body. Here, we present our review of the lens literature from this novel perspective.
Stem cells are unspecialized cells that have been a major focus of the field of regenerative medicine, opening new frontiers and regarded as the future of medicine. The ophthalmology branch of the medical sciences was the first to directly benefit from stem cells for regenerative treatment. The success stories of regenerative medicine in ophthalmology can be attributed to its accessibility, ease of follow-up and the eye being an immune-privileged organ. Cell-based therapies using stem cells from the ciliary body, iris and sclera are still in animal experimental stages but show potential for replacing degenerated photoreceptors. Limbal, corneal and conjunctival stem cells are still limited for use only for surface reconstruction, although they might have potential beyond this. Iris pigment epithelial, ciliary body epithelial and choroidal epithelial stem cells in laboratory studies have shown some promise for retinal or neural tissue replacement. Trabecular meshwork, orbital and sclera stem cells have properties identical to cells of mesenchymal origin but their potential has yet to be experimentally determined and validated. Retinal and retinal pigment epithelium stem cells remain the most sought out stem cells for curing retinal degenerative disorders, although treatments using them have resulted in variable outcomes. The functional aspects of the therapeutic application of lenticular stem cells are not known and need further attention. Recently, embryonic stem cell-derived retinal pigment epithelium has been used for treating patients with Stargardts disease and age-related macular degeneration. Overall, the different stem cells residing in different components of the eye have shown some success in clinical and animal studies in the field of regenerative medicine.
Pluripotency, the capacity to differentiate into multiple lineages, and proliferation are two characteristic attributes of stem cells. These cells are capable of replacing damaged or diseased cells under certain circumstances. Regenerative medicine or stem cell-based therapy has now reached a state where ocular tissues damaged by disease or injury can be repaired and/or regenerated. The ease of access for the therapeutic procedure as well as follow-up together with its immune-privileged status makes the eye an ideal organ for studying regenerative medicine. Such therapy involves various procedures where stem cells are injected into both the cellular and extracellular matrix microenvironments [1]. Corneal epithelial cell transplantation has been the most widely used stem cell-based therapy following bone marrow transplantation.
Stem cell-based treatment in ophthalmology follows either a cell replacement therapy strategy or a strategy involving trophic factor-based guidance cues. Throughout treatment, outcomes depend on our in-depth knowledge of the disease, the source of stem cells, the mode of treatment and the plausible mechanism driving the therapeutic outcome [2]. …
Cornea (limbus and stroma)
The cornea is at the outermost surface of the eye and safeguards transparency, which is crucial for vision. The corneal stem cell population is located in the periphery of the cornea, in the limbus; these cells are termed limbal epithelial stem cells (LESCs) [3–6]. Stroma comprises 90% of the volume of the cornea and, unlike the self-renewal of epithelia, the homeostasis of stroma is not based on a cycle of cell death and mitotic renewal.
Identification and isolation
Stem cells in the corneal epithelium are located in the basal layer of the limbal region at the corneal periphery, called the palisades of Vogt [3]. These are visualized in small clusters and are closely associated with the stromal matrix and the basement membrane, thereby assisting in cell-cell, cell-extracellular matrix and paracrine signaling communication. The corneal epithelial basal layer is composed mostly of transient amplifying cells at various stages of maturity. …
Therapeutic implications
LESC deficiency is pathological, either partially or completely, and is caused by either mechanical injury or chemical and thermal burns or acquired by diseases such as aniridia and Stevens Johnson syndrome. Treatment of such conditions involves LESC transplantation therapy. LESCs from the healthy eye in unilateral cases of ocular disease are expanded ex vivo for therapeutic purposes using protocols involving amniotic membrane or fibrin in the presence or absence of growth-arrested 3 T3 fibroblast feeder layers. Alternative, experimental sources for LESCs for cell-based therapy include buccal mucosal epithelial cells, hair follicle stem cells, and human embryonic stem cells (ESCs) [17,18]. Among non-limbal cell types, cultured oral mucosal cells and conjunctival epithelial cells have been transplanted to treat limbal stem cell deficiency in humans [19,20]. …
Conjunctiva
The conjunctiva, apart from being a barrier to pathogenic entry, is a highly vascularized connective tissue that provides channels for proper flow of nutrients and fluids. Conjunctival cells undergo renewal similar to the corneal epithelium, but the source of the stem cells for this remains elusive [23].
Identification and isolation
Conjunctival stem cells can differentiate into either mucin-producing goblet cells or an epithelial cell. The dividing basal cells migrate from the bulbar conjunctiva to the corneal surface and differentiate. Conjunctival epithelial cells are negative for CK3 and CK12 but positive for CK19. The stem cells residing in the fornical niche can differentiate into epithelial cells as well as goblet cells, as shown in clonal culture assays. This provides strong evidence that the stem cell population for conjunctiva renewal is in the fornix region [24,25]. …
Iris
The iris divides the space between the cornea and lens into anterior and posterior halves. The stroma and the vasculature of the iris are developed from the anterior region of the optic cup [28].
Identification and isolation
Iris pigment epithelial cells have the ability to grow in spheres and express markers of neural stem/progenitor cells such as Nestin, Msi and Pax6. Studies from mouse iris have revealed that these cells can also be differentiated to neuronal as well as glial lineages and express markers such as Chx10, Rho, Otx2 and Olig2 [29].
Ciliary body
The ciliary body produces the aqueous humor and is involved in regulating the aqueous flow, blood flow, intra-ocular pressure and maintenance of the immune-privileged status of the anterior chamber [31].
Identification and isolation
Ciliary body stem cells are derived from ciliary epithelium and undergo lineage-specific differentiation to retinal tissues. The ciliary-derived progenitor cell population expresses neuronal/retinal markers such as Nestin, Chx10 and Pax6. Ciliary epithelial cells can be cultured in vitro, forming neurospheres expressing transcription factors (Sox 2 and Pax 6) and retinal markers (Lhx2, Dach1, Six 3) [32]. …
Trabecular meshwork
The trabecular meshwork (TM) is a tissue between the cornea and iris in the anterior region that is responsible for drainage of aqueous fluid. The balance between aqueous secretion and outflow determines intraocular pressure, which is a risk factor for the development of glaucoma. TM cells help to remove debris in the circulating aqueous humor [38].
Identification and isolation
TM cells express vimentin, non-muscle actin, aquaporin-1, acetylated and acetoacetylated alpha-2 adrenergic receptor, matrix GLA protein and chitinase-3-like-1 [39–41]. Recently, the isolation and characterization of TM cells have been widely studied. These studies suggest that TM cells have stem cell-like properties, expressing mesenchymal cell-associated markers such as CD73, CD90, and CD105, and the ability to differentiate into adipocytes, osteocytes, and chondrocytes [38,42]. Further, studies showed that TM stem cells isolated as a side population or as clones expressed specific stem cell markers such as ABCG2, Notch1, OCT-3/4, AnkG, and MUC1 [38]. These stem cells could differentiate into the TM lineage and expressed AQP1, CHI3L1, and TIMP3 markers and had a phagocytic function [38,42].
Lens
The lens is composed of the lens capsule, epithelium and fibers and, like the cornea, is transparent. Lens stem cells are hypothesized to reside in the lens capsule, although they have not yet been identified. It is plausible that they come from the ciliary body, which is anatomically close to the lens [46].
Identification and isolation
Lens capsule regeneration has been shown to occur in lower vertebrates from cells residing in the ciliary body. The lens stem cells might thus reside in the lens capsule [47,48]. Lens stem cells have not yet been identified.
Therapeutic implications
Lens progenitor cells have been derived from human ESCs as well as induced pluripotent stem cells (iPSCs) [48]. Lens stem cells are presumed to have a role in maintaining the lens transparency and might be important in cataractogenesis or other lens abnormalities.
Retina
The retina represents the connecting link between visual input and image processing in the brain. Retinal diseases mostly result in irreversible damage to the visual pathway. Several studies in animal models have achieved some amount of success using transplantation of photoreceptors, endothelial cells and retinal pigment epithelium (RPE) [17,48].
Therapeutic implications
Recently, safety and efficacy results were obtained from a clinical trial of subretinal transplantation of RPE cells derived from human ESCs. Several groups have shown the capacity of human ESCs to differentiate into RPE with variable success rates [56]. Recently, the differentiation efficacy was increased 30-fold by adding vitamin B3 and activin A protein [51]. Murine disease models such as Leber’s congenital amaurosis rat have been used to study transplantation with differentiated retinal precursors; no teratoma formation was observed but the curative outcome needs to be followed up [57].
Transplantation of stem cell-, stem cell precursor- and iPSC-derived photoreceptors has resulted in functional recovery in animal models of retinal degeneration. Studies by several groups have demonstrated integration of photoreceptor precursors derived from postnatal retinas into degenerated mouse retina [52,53,58,59]. Tucker and colleagues [60] demonstrated that adult fibroblast-derived iPSCs differentiated into retinal precursor cells expressing retinal as well as photoreceptor markers (Pax6, CRX, recoverin and rhodopsin). Moreover, research has progressed from differentiating ESCs into photoreceptor lineages to determining the type of cell and day of culture required for successful transplantation [61–63]. Investigating methods to improve and support transplantation, Tucker and colleagues [64] demonstrated that a xeno-free substrate and extracellular matrix-coated dishes resulted in similar differentiation of iPSCs to retinal cells.
Choroid
The choroid is derived from mesoderm and neuroectoderm. Choroidal stem cells obtained from murine studies reveal mesenchymal stem cell properties, expressing markers such as Sca-1, CD90.2, CD44, CD105, CD73, ABCG2, Six2, Notch1 and Pax6. We are still far from understanding their proliferative and differentiation potential [70].
Sclera
The sclera is continuous with the cornea and is composed of fibrous material with viscoelastic properties. It is responsible for maintaining ocular pressure. Scleral stem cells have a mesenchymal origin and express ABCG2, Six2, Pax6 and Notch1 [70].
We provide comprehensive detail on the localization of ocular stem cells and explain the therapeutic potential of each. Ocular diseases can be classified into vascular defects, anatomical defects and neurodegenerative defects. In order to address these defects, regenerative medicine using cell replacement strategies could be highly beneficial and effective. Identification of the proper sources of stem cells is the first step towards this, followed by their isolation and characterization. Ophthalmology is the only branch of medical science that has so far gained from the field of regenerative medicine. Limbal stem cell transplantation is the only other cell-based transplantation procedure, other than bone marrow transfusion, that has been approved for patient care.
Tables 1 and and22 provide summaries of the present and future prospects of stem cells for ocular therapy. Figure 1 depicts the locations of stem cells and their clinical application status. Figures 2 and and33 highlight stem cell sources used in ocular cell therapies for specific diseases. In order to harness the potential of stem cell-based therapy to provide and restore sight in blind patients, the safety of the cells needs to be studied in detail. For the successful utilization of stem cells for therapeutic purposes, small molecules can be incorporated with or conjugated to them before transplantation to promote specific differentiation pathways [76]. These cells serve to replace damaged cells and produce cytokines, growth factors, and other trophic molecules [77]. Fundamental studies are needed to unravel the roles of the Ivy league signaling pathways such as the Notch, WNT, Jak-Stat, tyrosine kinase, and Sonic hedgehog pathways. Also, alternative sources of stem cells need to be explored for their ability to integrate into the visual network. Basic researchers and ophthalmologists worldwide share optimism that stem cell therapy will in the future provide a means to restore vision.
There are different results related to betatrophin and its characteristic to induce insulin and/or expand the pancreas beta cells. All the experiments so far were performed in mice. Some of the authors like Elisabeth Kugelberg from Harvard University agrees that betatrophin can induce insulin and expansion of secreting beta cells in mice (E. Kugelberg , 2014). Levitsky et al., 2014, come to the conclusion that betatrophin stimulate growth of beta cells in mice, while Gusarova et al., 2014, said that Betatrophin doesn’t control cell expansion in mice ( Gusarova et al., 2014) All three results are based on experiments on mice.
To make sure what are the characteristics of betatrophin in human pancreatic beta cells I suggest to try to determine the concentration and effect on those concentrations on immortal beta cells from human, CM cell line (insulinoma-obtained from ascitic fluid of cancer patients ) ( they are not producing any insulin under the glucose stimulation, therefore they may be a good for our model if they respond to betatrophin) TRM-1 (foetal Human SV40 T antigen)-Express small amount of insulin, not responsive to glucose stimulation) and finally Blox5 ( foetal Human SV40 T –antigen) which Exhibit glucose responsive. and Low insulin content.Blox5 may be the second good cell line to experiment, because they are responsive to glucose and they may be responsive to betatrophin as well.
If we found that those cell lines are inducing insulin then we may try primary beta cells. There is an article of 2013 (Ilie and Ilie, 2013) in which there is a possibility of regeneration of beta cells in vivo by neogenesis from adult pancreas. We can use their model to see if betatrophin indeed induce insulin in those cells. ( see the article attached)
On the other hand there are possibilities of growing beta cells directly onto pancreatic duct as it shows below:
Xenotransplantation of Human Cardiomyocyte Progenitor Cells Does Not Improve Cardiac Function in a Porcine Model of Chronic Ischemic Heart Failure. Results f…
It is known that in patients with Type 1 diabetes the immune system attacks the pancreas, and the monitoring of blood sugar becomes really difficult. Lately the research showed a possibility of replacing the pancreatic islets cells with healthy cells to take over glucose monitoring and insulin release. However the immune system attacked the transplanted cells, patients being obliged to take immunosuppressant drugs for the rest of their life.
Now , a new advance in this type of research by Boston Children’s Hospital designed a material that was used to encapsulate human islet before transplanted them. In animal testing it was showed that the encapsulated human cells could cure diabetes for up to six months without provoking an immune response.
This approach “has the potential to provide diabetics with a new pancreas that is protected from the immune system, which allow them to control their blood sugar without taking drugs. That’s the dream” says Daniel Anderson, The Samuel A Goldblith Associate Professor in MIT’s Department of Chemical Engineering, A member of MIT’s Koch Institute for integrative Cancer research and Institute for Medical Engineering and Science (IMES), and a research fellow in the department of Anesthesiology at Boston Children’s Hospital
The JDRF director Julia Greenstein, Anderson, Langer and colleagues explored a chemical derivative originally isolated from brown algae to encapsulate the cells without harming them, allowing sugar and proteins to go through, thus permitted to test the glucose level after transplantation of the encapsulated cells. The research was published in Nature Medicine and Nature Biotechnology. Researchers from Harvard University, University of Illinois at Chicago and Joslin Diabetes Center and University of Massachusetts Medical school also contributed to this research.
Previous research has shown that when alginate capsules are implanted in primates and humans, scar tissue builds up around the capsules, making the device ineffective. MIT/Children Hospital try to modify alginate make it less likely to provoke this kind of immune response.
With The Courtesy of The Researchers
“We decided to take an approach where you cast a very wide net and see what you can catch,” says Arturo Vegas, a former MIT and Boston Children’s Hospital postdoc who is now an assistant professor at Boston University. Vegas is the first author of the Nature Biotechnology paper and co-first author of the Nature Medicine paper. “We made all these derivatives of alginate by attaching different small molecules to the polymer chain, in hopes that these small molecule modifications would somehow give it the ability to prevent recognition by the immune system.”
800 alginate derivatives were screened . Further, the known triazole thiomorpholine dioxide (TMTD) have been chosen to be tested in diabetic mice. They chose a strain of mice with a strong immune system and implanted human islet cells encapsulated in TMTD into a region of the abdominal cavity known as the intraperitoneal space.
The pancreatic islet cells used in this study were generated from human stem cells using a technique recently developed by Douglas Melton, a professor at Harvard University who is an author of the Nature Medicine paper.
Following implantation, the cells immediately began producing insulin in response to blood sugar levels and were able to keep blood sugar under control for the length of the study, 174 days.
“The really exciting part of this was being able to show, in an immune-competent mouse, that when encapsulated these cells do survive for a long period of time, at least six months,” says Omid Veiseh, a senior postdoc at the Koch Institute and Boston Children’s hospital, co-first author of the Nature Medicine paper, and an author of the Nature Biotechnology paper. “The cells can sense glucose and secrete insulin in a controlled manner, alleviating the mice’s need for injected insulin.”
The researchers also found that 1.5-millimeter diameter capsules made from their best materials (but not carrying islet cells) could be implanted into the intraperitoneal space of nonhuman primates for at least six months without scar tissue building up.
“The combined results from these two papers suggests that these capsules have real potential to protect transplanted cells in human patients,” says Robert Langer, the David H. Koch Institute Professor at MIT, a senior research associate at Boston’s Children Hospital, and co-author on both papers. “We are so pleased to see this research in cell transplantation reach these important milestones.”
Cherie Stabler, an associate professor of biomedical engineering at the University of Florida, says this approach is impressive because it tackles all aspects of the problem of islet cell delivery, including finding a source of cells, preventing an immune response, and developing a suitable delivery material.
“It’s such a complex, multipronged problem that it’s important to get people from different disciplines to address it,” says Stabler, who was not involved in the research. “This is a great first step towards a clinically relevant, cell-based therapy for Type I diabetes.”
At this point the researchers are thinking of using their new material in non human primates and eventually performing clinical trials in diabetic patients. “Our goal is to continue to work hard to translate these promising results into a therapy that can help people,” Anderson says.
“Being insulin-independent is the goal,” Vegas says. “This would be a state-of-the-art way of doing that, better than any other technology could. Cells are able to detect glucose and release insulin far better than any piece of technology we’ve been able to develop.”
In their research they found out that the new material works best with molecules containing triazole group- a ring containing two atoms of Carbon and three of N. However, they suspect that in this particular case it may interfere with the immune system’s ability to recognize the material as foreign.
The work was supported, in part, by the JDRF, the Leona M. and Harry B. Helmsley Charitable Trust, the National Institutes of Health, and the Tayebati Family Foundation.
Other authors of the papers include MIT postdoc Joshua Doloff; former MIT postdocs Minglin Ma and Kaitlin Bratlie; MIT graduate students Hok Hei Tam and Andrew Bader; Jeffrey Millman, an associate professor at Washington University School of Medicine; Mads Gürtler, a former Harvard graduate student; Matt Bochenek, a graduate student at the University of Illinois at Chicago; Dale Greiner, a professor of medicine at the University of Massachusetts Medical School; Jose Oberholzer, an associate professor at the University of Illinois at Chicago; and Gordon Weir, a professor of medicine at the Joslin Diabetes Center.


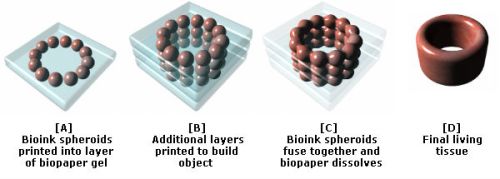



![Robust increases of extracellular amyloid-[bgr] deposits in 3D-differentiated hNPCs with FAD mutations.](https://i0.wp.com/www.nature.com/nature/journal/v515/n7526/carousel/nature13800-f2.jpg?resize=121%2C200)











 1
1


















{kind=link}
{kind=link}
{kind=link}
{kind=link}