Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
AI-Native Drug Discovery Landscape 2026 – How LPBI Group Differentiates in the New Era of Foundation Models
Curators: Aviva Lev-Ari, PhD, RN with Grok Assistence
As the race to build powerful biology foundation models intensifies, several well-funded AI-native companies have emerged with ambitious platforms for protein design, small-molecule generation, and multimodal drug discovery. While these companies bring strong technical capabilities, LPBI Group occupies a distinct and complementary position in the ecosystem.
Key AI-Native Players (2026)
Competitive Landscape Table for AI-Native in Drug Discovery
Company
Focus
Stage
LPBI Differentiation
Isomorphic Labs (DeepMind)
Protein/small molecule design using AI
Advanced (AlphaFold3 based)
LPBI offers curated multimodal training data + COM methodology (they need high-quality data to train/validate)
EvolutionaryScale
Protein design (ESM models)
Early commercial
LPBI’s strength is in clinical/therapeutic context + mechanism-of-action curation across full disease spectrum
Chai Discovery
Multimodal AI for drug discovery
Early
LPBI provides the upstream high-provenance corpus + ontology they would need for better results
Recursion Pharma
Phenotypic screening + AI
Clinical stage
LPBI’s expert-curated literature + images + COM complements their wet-lab focus
Generative AI for protein design & therapeutic optimization
Early-stage
LPBI supplies the high-provenance, expert-curated multimodal corpus and COM Tool Factory that significantly enhances model accuracy and reduces failure rates in downstream development
How LPBI Group Differentiates
LPBI Group does not compete directly in building foundation models. Instead, we provide the critical upstream layer these companies and hyperscalers urgently need:
A 9 GB private multimodal corpus of expert-curated scientific content (6,290+ articles, 48 e-Books, 7,500+ images, 300+ podcasts)
The 17-part Composition of Methods (COM) Tool Factory, including AJAUS (autonomous 24/7 refresh) and Rosetta Stone Ontology (causal mapping)
15 Subject Matter Small Language Models (SLMs) ready for concatenation into proprietary LLMs and MFMH
Proven track record of 4–5×+ uplift in novel causal relationship extraction when combined with frontier models
Strategic Positioning
While AI-native startups excel at model architecture and computation, they still face the persistent bottleneck of high-quality, causally structured, provenance-rich training data. LPBI Group’s vertically integrated assets and methodology offer a defensible moat and a true “own-both” advantage when partnered with hyperscalers or pharma companies.
This complementary role positions LPBI Group as the ideal upstream partner for the next generation of domain-aware AI in Health.
Nearly half of the global population—and 80 percent of patients in therapeutic areas such as immunology—are women. Yet, treatments are frequently developed without tailored insights for female patients, often ignoring critical biological differences such as hormonal impacts, genetic factors, and cellular sex. Historically, women’s health has been narrowly defined through the lens of reproductive organs, while for non-reproductive conditions, women were treated as “small men.” This lack of focus on sex-specific biology has contributed to significant gaps in healthcare.
A recent analysis found that women spend 25 percent more of their lives in poor health compared with men due to the absence of sex-based treatments. Addressing this disparity could not only improve women’s quality of life but also unlock over $1 trillion in annual global GDP by 2040.
Four key factors contribute to the women’s health gap: limited understanding of sex-based biological differences, healthcare systems designed around male physiology, incomplete data that underestimates women’s disease burden, and chronic underfunding of female-focused research. For instance, despite women representing 78 percent of U.S. rheumatoid arthritis patients, only 7 percent of related NIH funding in 2019 targeted female-specific studies.
However, change is happening. Companies have demonstrated how targeted R&D can drive better outcomes for women. These therapies achieved expanded FDA approvals after clinical trials revealed their unique benefits for female patients. Similarly, addressing sex-based treatment gaps in asthma, atrial fibrillation, and tuberculosis could prevent millions of disability-adjusted life years.
By closing the women’s health gap, biopharma companies can drive innovation, improve therapeutic outcomes, and build high-growth markets while addressing long-standing inequities. This untapped opportunity holds the potential to transform global health outcomes for women and create a more equitable future.
Clarivate was formed in 2016, following the acquisition of Thomson Reuters‘ Intellectual Property and Science business by Onex Corporation and Baring Private Equity Asia. Clarivate has acquired various companies since then, including, notably, ProQuest in 2021.
Clarivate (formerly CPA Global) was formerly the Intellectual Property and Science division of Thomson Reuters. Before 2008, it was known as Thomson Scientific. In 2016, Thomson Reuters struck a $3.55 billion deal in which they spun it off as an independent company, and sold it to private-equity firms Onex Corporation and Baring Private Equity Asia.
June 1, 2017: Publons, a platform for researchers to share recognition for peer review.
April 10, 2018: Kopernio, AI-tech startup providing ability to search for full-text versions of selected scientific journal articles.
October 30, 2018: TrademarkVision, provider of Artificial Intelligence (AI) trademark research applications.
September 9, 2019: SequenceBase, provider of patent sequence information and search technology to the biotech, pharmaceutical and chemical industries.
December 2, 2019: Darts-ip, provider of case law data and analytics for intellectual property (IP) professionals.
January 17, 2020: Decision Resources Group (DRG), a leading healthcare research and consulting company, providing high-value healthcare industry analysis and insights.
June 22, 2020: CustomersFirst Now, in intellectual property (“IP”) software and tech-enabled services.
October 1, 2020: CPA Global, intellectual property (“IP”) software and tech-enabled services.
December 1, 2021: ProQuest, software, data and analytics provider to academic, research and national institutions.[27]It was acquired for $5.3 billion from Cambridge Information Group in what was described as a “huge deal in the library and information publishing world”. The company said that the operational concept behind the acquisition was integrating ProQuest’s products and applications with Web of Science. Chairman of ProQuest Andy Snyder became the vice chairman of Clarivate. The Scholarly Publishing and Academic Resources Coalition, an advocacy group for open access to scholarship, voiced antitrust concerns. The acquisition had been delayed mid-year due to a Federal Trade Commission antitrust probe.
We are a leading global information services and analytics company serving the scientific research, intellectual property and life sciences end-markets. We provide structured information and analytics to facilitate the discovery, protection and commercialization of scientific research, innovations and brands. Our product porfolio includes well-established market-leading brands such as Web of Science, Derwent Innovation, Life Sciences, CompuMark and MarkMonitor (which they later divested). We believe that the stron balue proposition of our content, user interfaces, visualization and analytical tools, combined with the integration of our products and services into customers’ daily workflows, leads to our substantial customer loyalty as evidenced by their willingness to renew subscriptions with us.
Our structure, enabling a sharp focus on cross-selling opportunities within markets, is comprised of two product groups:
Science Group: consists of Web of Science and Life Science Product Lines
Intellectual Property Group: consists of Derwent, CompuMark and MarkMonitor
Corporations, government agencies, universities, law firms depend on our high-value curated content, analytics and services. Unstructured data has grown exponentially over the last decade. The trend has resulted in a critical need for unstructured data to be meaningfully filtered, analyzed and curated into relvent information that facilitates key operational and strategic decision making. Our highly curated, proprietary information created through our sourcing, aggregation, verification, translation, and categorization (ONTOLOGY) of data has resulted in our solutions being embedded in our customers’ workflow and decision-making processes.
Overview of Clarivate PLC five year strategy in 2019. Note that in 2019 the Science Group accounted for 56.2% of revenue! This was driven by their product Cortellis!
Figure. Overview of Clarivate PLC five year strategy in 2019. Note that in 2019 the Science Group accounted for 56.2% of revenue! This was driven by their product Cortellis!
Also Note nowhere in the M&A Discussion in years before 2023 was anything mentioned concerning AI or Large Language Models.
The Clarivate of Today: Built for Life Sciences with Cortellis
Clarivate PLC has integrated multiple platforms into their offering Cortellis, which integrated AI and LLM into the structured knowledge bases (see more at https://clarivate.com/products/cortellis-family/)
“Life sciences organizations are tasked, now more than ever, to discover and develop treatments that challenge the status quo, increase ROI, and improve patient lives. However, its become increasingly difficult to find, integrate and analyze the key data your teams need to make critical decisions and get your Cortellis products to patients faster.
Cortellis Competitive Intelligence: maximize ROI and improve patient outcomes
Cortellis Deals Intelligence: Portfolio Strategy and Business Development (find best deal)
Cortellis Clinical Intelligence: Clinical Trial Support and Regulatory
Cortellis Digital Health Intelligence: understand digital health ecosystem
Cortellis Drug Discovery: improve drug development speed and efficiency
MetaBase and MetaCore: integrated omics knowledge bases for drug discovery
Cortellis Regulatory: help with filings
Cortellis HTA: health tech compliance (HIPAA)
CMC Intelligence: new drug marketing
Generics Intelligence
Drug Safety Intelligence: both preclinical safety and post marketing pharmacovigilence
Watch Videos on Cortellis for Drug Discovery
Watch Video on Qiagen Site to see how Cortellis Integrates with Qiagen Omics Platform IPA with Clarivate Meta Core to gain more insights into genomic and proteomic data
Understand complex ‘omics data to accelerate your research
Discover why QIAGEN Ingenuity Pathway Analysis (IPA) is the leading pathway analysis application among the life science research community and is cited in tens of thousands of articles for the analysis, integration and interpretation of data derived from ‘omics experiments. Such experiments include:
RNA-seq
Small RNA-seq
Metabolomics
Proteomics
Microarrays including miRNA and SNP
Small-scale experiments
With QIAGEN IPA you can predict downstream effects and identify new targets or candidate biomarkers. QIAGEN Ingenuity Pathway Analysis helps you perform insightful data analysis and interpretation to understand your experimental results within the context of various biological systems.
Articles Relevant to Drug Development, Natural Language Processing in Drug Development, and Clarivate on this Open Access Scientific Journal Include:
2022 FDA Drug Approval List, 2022 Biological Approvals and Approved Cellular and Gene Therapy Products
Reporter: Aviva Lev-Ari, PhD, RN
SOURCE
Tal Bahar’s post on LinkedIn on 1/17/2023
Novel Drug Approvals for 2022
FDA’s Center for Drug Evaluation and Research (CDER)
New Molecular Entities (“NMEs”)
Some of these products have never been used in clinical practice. Below is a listing of new molecular entities and new therapeutic biological products that CDER approved in 2022. This listing does not contain vaccines, allergenic products, blood and blood products, plasma derivatives, cellular and gene therapy products, or other products that the Center for Biologics Evaluation and Research approved in 2022.
Others are the same as, or related to, previously approved products, and they will compete with those products in the marketplace. See Drugs@FDA for information about all of CDER’s approved drugs and biological products.
Certain drugs are classified as new molecular entities (“NMEs”) for purposes of FDA review. Many of these products contain active moieties that FDA had not previously approved, either as a single ingredient drug or as part of a combination product. These products frequently provide important new therapies for patients. Some drugs are characterized as NMEs for administrative purposes, but nonetheless contain active moieties that are closely related to active moieties in products that FDA has previously approved. FDA’s classification of a drug as an “NME” for review purposes is distinct from FDA’s determination of whether a drug product is a “new chemical entity” or “NCE” within the meaning of the Federal Food, Drug, and Cosmetic Act.
To treat adults with HIV whose HIV infections cannot be successfully treated with other available treatments due to resistance, intolerance, or safety considerations Press Release
To decrease the incidence of infection in patients with non-myeloid malignancies receiving myelosuppressive anti-cancer drugs associated with clinically significant incidence of febrile neutropenia
The Center for Biologics Evaluation and Research (CBER) regulates products under a variety of regulatory authorities. See the Development & Approval Process page for a description of what products are approved as Biologics License Applications (BLAs), Premarket Approvals (PMAs), New Drug Applications (NDAs) or 510Ks.
Biologics License Applications and Supplements
New BLAs (except those for blood banking), and BLA supplements that are expected to significantly enhance the public health (e.g., for new/expanded indications, new routes of administration, new dosage formulations and improved safety).
Other Applications Approved or Cleared by the Center for Biologics Evaluation and Research (CBER)
Medical devices involved in the collection, processing, testing, manufacture and administration of licensed blood, blood components and cellular products.
There are five FDA-approved CAR-T treatments for blood cancers and two gene therapies to treat rare diseases now on the market in the U.S. The late-stage pipeline could produce several more cancer CAR-Ts and gene therapies to treat a range of diseases.
One of the biggest races to watch in the cell therapy space will be that between Gilead Sciences’ Yescarta and Bristol Myers Squibb’s Breyanzi, both of which are gunning to move their CAR-Ts into earlier lines of treatment in large B-cell lymphoma (LBCL). At ASH, both companies rolled out impressive data from their trials in the second-line setting, but Gilead could have the upper hand by virtue of its three-year head start in the market, analysts said. Gilead expects to hear from the FDA on a label expansion in the second-line setting in April.
This article is part of Harvard Medical School’s continuing coverageof medicine, biomedical research, medical education and policy related to the SARS-CoV-2 pandemic and the disease COVID-19.
Harvard University and AbbVie today announced a $30 million collaborative research alliance, launching a multi-pronged effort at Harvard Medical School to study and develop therapies against emergent viral infections, with a focus on those caused by coronaviruses and by viruses that lead to hemorrhagic fever.
The collaboration aims to rapidly integrate fundamental biology into the preclinical and clinical development of new therapies for viral diseases that address a variety of therapeutic modalities. HMS has led several large-scale, coordinated research efforts launched at the beginning of the COVID-19 pandemic.
“A key element of having a strong R&D organization is collaboration with top academic institutions, like Harvard Medical School, to develop therapies for patients who need them most,” said Michael Severino, vice chairman and president of AbbVie. “There is much to learn about viral diseases and the best way to treat them. By harnessing the power of collaboration, we can develop new therapeutics sooner to ensure the world is better prepared for future potential outbreaks.”
“The cataclysmic nature of the COVID-19 pandemic reminds us how vital it is to be prepared for the next public health crisis and how critical collaboration is on every level—across disciplines, across institutions and across national boundaries,” said George Q. Daley, dean of Harvard Medical School. “Harvard Medical School, as the nucleus of an ecosystem of fundamental discovery and therapeutic translation, is uniquely positioned to propel this transformative research alongside allies like AbbVie.”
AbbVie will provide $30 million over three years and additional in-kind support leveraging AbbVie’s scientists, expertise and facilities to advance collaborative research and early-stage development efforts across five program areas that address a variety of therapeutic modalities:
Immunity and immunopathology—Study of the fundamental processes that impact the body’s critical immune responses to viruses and identification of opportunities for therapeutic intervention.
Led by Ulirich Von Andrian, the Edward Mallinckrodt Jr. Professor of Immunopathology in the Blavatnik Institute at HMS and program leader of basic immunology at the Ragon Institute of MGH, MIT and Harvard, and Jochen Salfeld, vice president of immunology and virology discovery at AbbVie.
Host targeting for antiviral therapies—Development of approaches that modulate host proteins in an effort to disrupt the life cycle of emergent viral pathogens.
Led by Pamela Silver, the Elliot T. and Onie H. Adams Professor of Biochemistry and Systems Biology in the Blavatnik Institute at HMS, and Steve Elmore, vice president of drug discovery science and technology at AbbVie.
Antibody therapeutics—Rapid development of therapeutic antibodies or biologics against emergent pathogens, including SARS-CoV-2, to a preclinical or early clinical stage.
Led by Jonathan Abraham, assistant professor of microbiology in the Blavatnik Institute at HMS, and by Jochen Salfeld, vice president of immunology and virology discovery at AbbVie.
Small molecules—Discovery and early-stage development of small-molecule drugs that would act to prevent replication of known coronaviruses and emergent pathogens.
Led by Mark Namchuk, executive director of therapeutics translation at HMS and senior lecturer on biological chemistry and molecular pharmacology in the Blavatnik Institute at HMS, and Steve Elmore, vice president of drug discovery science and technology at AbbVie.
Translational development—Preclinical validation, pharmacological testing, and optimization of leading approaches, in collaboration with Harvard-affiliated hospitals, with program leads to be determined.
This article is part of Harvard Medical School’s continuing coverage of medicine, biomedical research, medical education, and policy related to the SARS-CoV-2 pandemic and the disease COVID-19.
Less than a year ago, Harvard Medical School researchers and international colleagues unveiled a platform called VirtualFlow that could swiftly sift through more than 1 billion chemical compounds and identify those with the greatest promise to become disease-specific treatments, providing researchers with invaluable guidance before they embark on expensive and time-consuming lab experiments and clinical trials.
Propelled by the urgent needs of the pandemic, the team has now pushed VirtualFlow even further, conducting 45 screens of more than 1 billion compounds each and ranking the compounds with the greatest potential for fighting COVID-19—including some that are already approved by the FDA for other diseases.
“This was the largest virtual screening effort ever done,” said VirtualFlow co-developer Christoph Gorgulla, research fellow in biological chemistry and molecular pharmacology in the labs of Haribabu Arthanari and Gerhard Wagner in the Blavatnik Institute at HMS.
The results were published in January in the open-access journal iScience.
The team searched for compounds that bind to any of 15 proteins on SARS-CoV-2 or two human proteins, ACE2 and TMPRSS2, known to interact with the virus and enable infection.
Researchers can now explore on an interactive website the 1,000 most promising compounds from each screen and start testing in the lab any ones they choose.
The urgency of the pandemic and the sheer number of candidate compounds inspired the team to release the early results to the scientific community.
“No one group can validate all the compounds as quickly as the pandemic demands,” said Gorgulla, who is also an associate of the Department of Physics at Harvard University. “We hope that our colleagues can collectively use our results to identify potent inhibitors of SARS-CoV-2.”
In most cases, it will take years to find out whether a compound is safe and effective in humans. For some of the compounds, however, researchers have a head start.
Hundreds of the most promising compounds that VirtualFlow flagged are already FDA approved or being studied in clinical or preclinical trials for other diseases. If researchers find that one of those compounds proves effective against SARS-CoV-2 in lab experiments, the data their colleagues have already collected could save time establishing safety in humans.
Other compounds among VirtualFlow’s top hits are currently being assessed in clinical trials for COVID-19, including several drugs in the steroid family. In those cases, researchers could build on the softwarefindings to investigate how those drug candidates work at the molecular level—something that’s not always clear even when a drug works well.
It shows what we’re capable of computationally during a pandemic.
Hari Arthanari
In another effort to speed successful transitions from computer to clinic, the team has joined in Harvard’s partnership with pharmaceutical company AbbVie.
If any successful drugs eventually arise from the VirtualFlow screens, they would complement other strategies in the fight against COVID-19. For instance, drugs that halt viral replication or prevent it from entering cells could help those who cannot be vaccinated.
The nature of the screens also raises the likelihood that drugs developed against current forms of SARS-CoV-2 would work against future mutations or other coronaviruses, the authors say.
Computing power
The work was made possible in large part by about $1 million in cloud computing hours awarded by Google through a COVID-19 research grant program.
Gorgulla and colleagues used that power to screen how well the compounds bound to more than 40 sites across the 15 viral proteins as well as to the two human proteins—effectively trying 1 billion 3D puzzle pieces in 40 places each.
The team selected the sites because blocking them with compounds would either prevent SARS-CoV-2 from entering cells, prevent the virus from replicating and thus lower viral load, reduce the virus’s ability to evade or subvert our immune defenses, or disrupt viral assembly and packaging.
Many of the sites have not yet been investigated by other groups, as far as the team is aware.
“We’re exploring new avenues on how to tackle the virus. This is one of the most exciting aspects of our project,” said Gorgulla.
One benefit of studying dozens of sites on 17 proteins at once is the possibility of identifying or developing multiple drugs that, when combined, combat SARS-CoV-2 infection on different fronts. Such drug cocktails would have a better chance of halting the virus in its tracks and overcoming future mutations than a single drug that works on one protein site.
Some sites included in the screen are shared among other coronaviruses of worldwide concern. Any compound that binds to one of those sites has a “high” chance of also combating SARS, MERS, or as-yet-unknown coronavirus diseases, said Arthanari.
“We are in a position to discover pan-coronavirus drugs and help prepare for the next coronavirus pandemic, should there ever be one,” said Gorgulla.
Regardless of the outcomes, the work raises the benchmark for virtual screening and demonstrates the current power of computing in biological research.
“It shows what we’re capable of computationally during a pandemic,” said Arthanari.
The project has also brought special satisfaction to team members who don’t typically work on projects so closely tied to human health.
Tweet Collection by @pharma_BI and @AVIVA1950 and Re-Tweets for e-Proceedings 14th Annual BioPharma & Healthcare Summit, Friday, September 4, 2020, 8 AM EST to 3-30 PM EST – Virtual Edition
#USAIC20 Dr. Hal Barron, Chief Scientific Officer and President R&D, GlaxoSmithKline GWAS not easy to find which gene drives the association Functional Genomics gene by gene with phenotypes using machine learning significant help
#USAIC20 Dr. Hal Barron, Chief Scientific Officer and President R&D, GSK GWAS not easy to find which gene drives the association Functional Genomics gene by gene with phenotypes using machine learning significant help
#USAIC20 Arpa Garay, President, Global Pharmaceuticals, Commercial Analytics, Merck & Co. Data on Patients and identification who will benefit fro which therapy cultural bias risk aversion
#USAIC20 Dr. Najat Khan, Chief Operating Officer, Janssen R&D Data Sciences, Johnson & Johnson Data Validation Deployment of algorithms embed data by type early on in the crisis to understand the disease
#USAIC20 Dr. Maya Said, Chief Executive Officer, Outcomes4Me Cancer patients taking change of their care Digital Health – consumerization of Health, patient demand to be part of the decision, part the information FDA launched a Program Project Patient Voice
We’re taking a quick break at #USAIC20 before our next panel on rare diseases starts at 12:20pm EDT. USAIC would like to thank our Sponsors and Partners for supporting this year’s digital event.
#USAIC20 Dr. Roy Vagelos, Chairman of the Board, Regeneron HIV-AIDS: reverse transcriptase converted a lethal disease to a chronic disease, tried hard to make vaccine – the science was not there
#USAIC20 Dr. Roy Vagelos, Chairman of the Board, Regeneron Pharmaceuticals Congratulates Big Pharma for taking the challenge on COVID-19 Vaccine, Antibody and anti-viral Government funding Merck was independent from Government – to be able to set the price
Christopher Viehbacher, Gurnet Point Capital touches very sensitive topic at #USAIC20 He claims that we are never going to have real innovation out of big pharma! Well this isn’t new but not entirely true either… any more thoughts?
#USAIC20 Christopher Viehbacher, Managing Partner, Gurnet Point Capital Dream of every Biotech – get Big Pharma coming to acquire and pay a lot Morph and adapt
talks about various philosophies and key reasons why certain projects/molecules are killed early. My counter questions- What are chances of losing hope little early? Do small #biopharma publish negative results to aid to the knowledge pool? #USAIC20
#USAIC20 Dr. Laurie Glimcher, President & CEO, Dana-Farber Cancer Institute COlonorectal cancer is increasing immuno therapy 5 drugs marketed 30% cancer patients are treated early detection key vs metastatic 10% of cancer are inherited treatment early
#USAIC20 Rehan Verjee, President, EMD Serono Charities funding cancer research – were impacted and resources will come later and in decreased amount New opportunities support access to Medicine improve investment across the board
#USAIC20 Dr. Philip Larsen, Global Head of Research, Bayer AG Repurposing drugs as antiviral from drug screening innovating methods Cytokine storm in OCVID-19 – kinase inhibitors may be antiviral data of tested positive allows research of pathway in new ways
#USAIC20 Dr. Laurie Glimcher, President & CEO, Dana-Farber 3,000 Telemedicine session in the first week of the Pandemic vs 300 before – patient come back visits patient happy with Telemedicine team virtually need be reimbursed same rate working remotely
#USAIC20 Rehan Verjee, President, EMD Serono entire volume of clinical trials at Roche went down same at EMD delay of 6 month, some were to be initiated but was put on hold Charities funding cancer research were impacted and resources will come later smaller
#USAIC20 Dr. Laurie Glimcher, President & CEO, Dana-Farber Cancer Institute Dana Farber saw impact of COVID-19 on immunosuppressed patients coming in for Cancer Tx – switch from IV Tx to Oral 96% decrease in screenings due to Pandemic – increase with Cancer
#USAIC20 Kenneth Frazier, Chairman of the Board and Chief Executive Officer, Merck & Co. Pharma’s obligation for next generations requires investment in R&D vs Politicians running for 4 years Patients must come first vs shareholders vs R&D investment in 2011
#USAIC20 Kenneth Frazier, Chairman of the Board and Chief Executive Officer, Merck & Co. Antibiotic research at Merck – no market incentives on pricing for Merck to invest in antibiotics people will die from bacterial resistance next pandemic be bacterial
#USAIC20 Kenneth Frazier, Chairman of the Board and Chief Executive Officer, Merck & Co. Strategies of Merck = “Medicine is for the People not for Profit” – Ketruda in India is not reembureable in India and million are in need it Partnership are encouraged
Chairman Stelios Papadopoulos asks #KennethFrazier if wealthy nations will try to secure large proportion of #COVID19 drugs/vaccines. #KennethFrazie rightly mentions: pharma industry’s responsibility to balance the access to diff countries during pandemic. #USAIC20
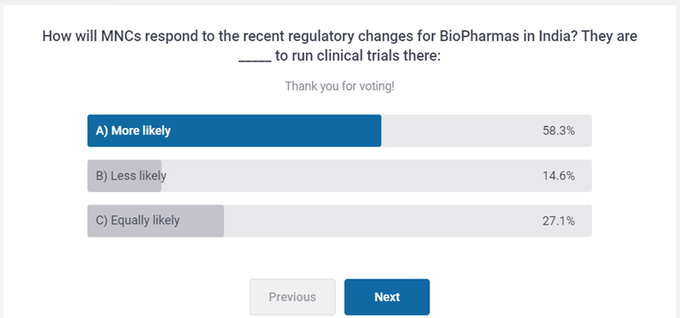
Almost 60% participants at #USAIC20 feel that MNCs are more likely to run their #clinicalTrials in #INDIA seeing changing environment here, reveals the poll. Exciting time ahead for scientific fraternity as this can substantially increase the speed of #DrugDevelopment globally
#USAIC20 Dr. Barry Bloom, Professor & former Dean, Harvard School of Public Health Vaccine in clinical trials, public need to return for 2nd shot, hesitancy Who will get the Vaccine first in the US most vulnerable of those causing transmission Pharma’s risk
#USAIC20 Dr. Barry Bloom, Professor & former Dean, Harvard School of Public Health Testing – PCR expensive does not enable quick testing is expensive result come transmission occurred Antibody testing CRISPR test based Vaccine in clinical trials
#USAIC20 Dr Andrew Plump, President of R&D, Takeda Pharmaceuticals COllaboration effort around the Globe in the Pandemic therapy solutions including Vaccines
The Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) Partnership on May 18, 2020: Leadership of AbbVie, Amgen, AstraZeneca, Bristol Myers Squibb, Eisai, Eli Lilly, Evotec, Gilead, GlaxoSmithKline, Johnson & Johnson, KSQ Therapeutics, Merck, Novartis, Pfizer, Roche, Sanofi, Takeda, and Vir. We also thank multiple NIH institutes (especially NIAID), the FDA, BARDA, CDC, the European Medicines Agency, the Department of Defense, the VA, and the Foundation for NIH
Reporter: Aviva Lev-Ari, PhD, RN
May 18, 2020
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) An Unprecedented Partnership for Unprecedented Times
It has been more than a century since the world has encountered a pandemic like coronavirus disease 2019 (COVID-19), and the rate of spread of COVID-19 around the globe and the associated morbidity and mortality have been staggering.1 To address what may be the greatest public health crisis of this generation, it is imperative that all sectors of society work together in unprecedented ways, with unprecedented speed. In this Viewpoint, we describe such a partnership.
First reported in Wuhan, China, in December 2019, COVID-19 is caused by a highly transmissible novel coronavirus, SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2). By March 2020, as COVID-19 moved rapidly throughout Europe and the US, most researchers and regulators from around the world agreed that it would be necessary to go beyond “business as usual” to contain this formidable infectious agent. The biomedical research enterprise was more than willing to respond to the challenge of COVID-19, but it soon became apparent that much-needed coordination among important constituencies was lacking.
Clinical trials of investigational vaccines began as early as January, but with the earliest possible distribution predicted to be 12 to 18 months away. Clinical trials of experimental therapies had also been initiated, but most, except for a trial testing the antiviral drug remdesivir,2 were small and not randomized. In the US, there was no true overarching national process in either the public or private sector to prioritize candidate therapeutic agents or vaccines, and no efforts were underway to develop a clear inventory of clinical trial capacity that could be brought to bear on this public health emergency. Many key factors had to change if COVID-19 was to be addressed effectively in a relatively short time frame.
On April 3, leaders of the National Institutes of Health (NIH), with coordination by the Foundation for the National Institutes of Health (FNIH), met with multiple leaders of research and development from biopharmaceutical firms, along with leaders of the US Food and Drug Administration (FDA), the Biomedical Advanced Research and Development Authority (BARDA), the European Medicines Agency (EMA), and academic experts. Participants sought urgently to identify research gaps and to discuss opportunities to collaborate in an accelerated fashion to address the complex challenges of COVID-19.
These critical discussions culminated in a decision to form a public-private partnership to focus on speeding the development and deployment of therapeutics and vaccines for COVID-19. The group assembled 4 working groups to focus on preclinical therapeutics, clinical therapeutics, clinical trial capacity, and vaccines (Figure). In addition to the founding members, the working groups’ membership consisted of senior scientists from each company or agency, the Centers for Disease Control and Prevention (CDC), the Department of Veterans Affairs (VA), and the Department of Defense.
Figure.
Accelerating COVID-19 Therapeutic Interventions and Vaccines
ACTIV’s 4 working groups, each with one cochair from NIH and one from industry, have made rapid progress in establishing goals, setting timetables, and forming subgroups focused on specific issues (Figure). The goals of the working group, along with a few examples of their accomplishments to date, include the following.
The Preclinical Working Group was charged to standardize and share preclinical evaluation resources and methods and accelerate testing of candidate therapies and vaccines to support entry into clinical trials. The aim is to increase access to validated animal models and to enhance comparison of approaches to identify informative assays. For example, through the ACTIV partnership, this group aims to extend preclinical researchers’ access to high-throughput screening systems, especially those located in the Biosafety Level 3 (BSL3) facilities currently required for many SARS-CoV-2 studies. This group also is defining a prioritization approach for animal use, assay selection and staging of testing, as well as completing an inventory of animal models, assays, and BSL 3/4 facilities.
The Therapeutics Clinical Working Group has been charged to prioritize and accelerate clinical evaluation of a long list of therapeutic candidates for COVID-19 with near-term potential. The goals have been to prioritize and test potential therapeutic agents for COVID-19 that have already been in human clinical trials. These may include agents with either direct-acting or host-directed antiviral activity, including immunomodulators, severe symptom modulators, neutralizing antibodies, or vaccines. To help achieve these goals, the group has established a steering committee with relevant expertise and objectivity to set criteria for evaluating and ranking potential candidate therapies submitted by industry partners. Following a rigorous scientific review, the prioritization subgroup has developed a complete inventory of approximately 170 already identified therapeutic candidates that have acceptable safety profiles and different mechanisms of action. On May 6, the group presented its first list of repurposed agents recommended for inclusion in ACTIV’s master protocol for adaptive clinical trials. Of the 39 agents that underwent final prioritization review, the group identified 6 agents—including immunomodulators and supportive therapies—that it proposes to move forward into the master protocol clinical trial(s) expected to begin later in May.
The Clinical Trial Capacity Working Group is charged with assembling and coordinating existing networks of clinical trials to increase efficiency and build capacity. This will include developing an inventory of clinical trial networks supported by NIH and other funders in the public and private sectors, including contract research organizations. For each network, the working group seeks to identify their specialization in different populations and disease stages to leverage infrastructure and expertise from across multiple networks, and establish a coordination mechanism across networks to expedite trials, track incidence across sites, and project future capacity. The clinical trials inventory subgroup has already identified 44 networks, with access to adult populations and within domestic reach, for potential inclusion in COVID-19 trials. Meanwhile, the survey subgroup has developed 2 survey instruments to assess the capabilities and capacities of those networks, and its innovation subgroup has developed a matrix to guide deployment of innovative solutions throughout the trial life cycle.
The Vaccines Working Group has been charged to accelerate evaluation of vaccine candidates to enable rapid authorization or approval.4 This includes development of a harmonized master protocol for adaptive trials of multiple vaccines, as well as development of a trial network that could enroll as many as 100 000 volunteers in areas where COVID-19 is actively circulating. The group also aims to identify biomarkers to speed authorization or approval and to provide evidence to address cross-cutting safety concerns, such as immune enhancement. Multiple vaccine candidates will be evaluated, and the most promising will move to a phase 2/3 adaptive trial platform utilizing large geographic networks in the US and globally.5 Because time is of the essence, ACTIV will aim to have the next vaccine candidates ready to enter clinical trials by July 1, 2020.
Corey L , Mascola JR , Fauci AS , Collins FS . A strategic approach to COVID-19 vaccine R&D. Science. Published online May 11, 2020. doi:10.1126/science.abc5312PubMedGoogle Scholar
Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) portal. National Institutes of Health. Accessed May 15, 2020. https://www.nih.gov/ACTIV
Advancing Drug Development – 12/12/2019, 8:30AM – 8:30PM at The University of Massachusetts Club, One Beacon Street, Boston, MA
Reporter: Aviva Lev-Ari, PhD, RN
4th Advancing Drug Development Forum – Making the Impossible Possible – Harnessing Small Molecule Drug Development scheduled to take place December 12th, 2019 at The University of Massachusetts Club, in Boston, Massachusetts from 8:30 AM – 8:30 PM.
Scientists are more than just chipping away and kicking down the barricades to develop complex small molecule products better and faster. Successful companies are spending quality time finding novel and clever approaches and powerful technologies to better support their knowledgeable teams. Often it takes establishing strong partnerships with 1 or more specialized service providers, cleverly combining resources – always striving to raise the bar in order to make life threatening diseases more of a chronic and tolerable disease or eradicated completely.
Hear from key opinion leaders in pharma, biotech, the investment community and innovative service providers on how they are meeting the challenges. Keep in mind, it takes being open-minded, flexible and willing sometimes to redesigning a new formulation that better enhances bioavailability, optimizes drug-delivery profiles, reduces dosing frequency, or improves the patient experience to have the potential to deliver quicker returns on investments than developing a completely new drug.
Bridging the Gap between Experimentation and Implementation
Panel Discussion
10:15 AM
Refreshment Break
10:45 AM
Cross-Talk Between Clin-Ops and Tech-Ops
Panel Discussion
11:15 AM
The Cost of Speed and Value in Drug Development
Panel Discussion
12:00 PM
Networking Luncheon
1:00 PM
Advances in the Delivery of Therapeutics to the Brain
Academic Keynote Mansoor M. Amiji, Ph.D., University Distinguished Professor, Professor of Pharmaceutical Sciences & Professor of Chemical Engineering, Northeastern University
1:30 PM
Advancing Drug Delivery and Controlled Release
Panel Discussion
2:00 PM
Drowning in DATA
2:30 PM
Disruptive AI Technologies Improving Drug Development
3:00 PM
Refreshment Break
3:30 PM
Small Specialty VS Full Service – What Makes Sense for US?
Panel Discussion
4:00 PM
Fireside Chat Michael Bonney, Executive Chair, Kaleido Biosciences Heinrich Schlieker, Ph.D., SVP Technical Operations, Sage Therapeutics
Precision Medicine has helped transform cancer care from one-size-fits-all chemotherapy to a new era, where patients’ tumors can be analyzed and therapy selected based on their genetic makeup. Until now, however, precision medicine’s impact has been far less in other therapeutic areas, many of which are ripe for transformation. Efforts are underway to bring the successes of precision medicine to neurology, immunology, ophthalmology, and other areas. This move raises key questions of how the lessons learned in oncology can be used to advance precision medicine in other fields, what types of data and tools will be important to personalizing treatment in these areas, and what sorts of partnerships and payer initiatives will be needed to support these approaches and their ultimate commercialization and use. The panel will also provide an in depth look at precision medicine approaches aimed at better understanding and improving patient care in highly complex disease areas like neurology.
Speaker panel: The big issue now with precision medicine is there is so much data and hard to put experimental design and controls around randomly collected data.
The frontier is how to CURATE randomly collected data to make some sense of it
One speaker was at a cancer meeting and the oncologist had no idea what to make of genomic reports they were given. Then there is a lack of action or worse a misdiagnosis.
So for e.g. with Artificial Intelligence algorithms to analyze image data you can see things you can’t see with naked eye but if data quality not good the algorithms are useless – if data not curated properly data is wasted
Data needs to be organized and curated.
If relying of AI for big data analysis the big question still is: what are the rates of false negative and false positives? Have to make sure so no misdiagnosis.
Please follow LIVE on TWITTER using the following @ handles and # hashtags:
Real Time Coverage @BIOConvention #BIO2019: Issues of Risk and Reproduceability in Translational and Academic Collaboration; 2:30-4:00 June 3 Philadelphia PA
Reporter: Stephen J. Williams, PhD @StephenJWillia2Article ID #267: Real Time Coverage @BIOConvention #BIO2019: Issues of Risk and Reproduceability in Translational and Academic Collaboration; 2:30-4:00 June 3 Philadelphia PA. Published on 6/3/2019
WordCloud Image Produced by Adam Tubman
Translating academic research into products and new therapies is a very risky venture as only 1% of academic research has been successfully translated into successful products.
Collaboration from Chicago area universities like U of Chicago, Northwestern, etc. First phase was enhance collaboration between universities by funding faculty recruitment and basic research. Access to core facilities across universities. Have expanded to give alternatives to company formation.
Most academic PI are not as savvy to start a biotech so they bring in biotechs and build project teams as well as developing a team of ex pharma and biotech experts. Derisk as running as one asset project. Partner as early as possible. A third of their pipeline have been successfully partnered. Work with investors and patent attorneys.
Focused on getting PIs to get to startup. Focused on oncology and vaccines and I/O. The result can be liscensing or partnership. Running around 50 to 60 projects. Creating a new company from these US PI partnerships.
Most projects from Harvard have been therapeutics-based. At Harvard they have a network of investors ($50 million). They screen PI proposals based on translateability and what investors are interested in.
In Chicago they solicit multiple projects but are agnostic on area but as they are limited they are focused on projects that will assist in developing a stronger proposal to investor/funding mechanism.
NYU goes around university doing due diligence reaching out to investigators. They shop around their projects to wet their investors, pharma appetite future funding. At Takeda they have five centers around US. They want to have more input so go into the university with their scientists and discuss ideas.
Challenges:
Takeda: Data Validation very important. Second there may be disconnect with the amount of equity the PI wants in the new company as well as management. Third PIs not aware of all steps in drug development.
Harvard: Pharma and biotech have robust research and academic does not have the size or scope of pharma. PIs must be more diligent on e.g. the compounds they get from a screen… they only focus narrowly
NYU: bring in consultants as PIs don’t understand all the management issues. Need to understand development so they bring in the experts to help them. Pharma he feels have to much risk aversion and none of their PIs want 100% equity.
Chicago: they like to publish at early stage so publication freedom is a challenge
Dr. Freedman: Most scientists responding to Nature survey said yes a reproduceability crisis. The reasons: experimental bias, lack of validation techniques, reagents, and protocols etc.
And as he says there is a great ECONOMIC IMPACT of preclinical reproducability issues: to the tune of $56 billion of irreproducable results (paper published in PLOS Biology). If can find the core drivers of this issue they can solve the problem. STANDARDS are constantly used in various industries however academic research are lagging in developing such standards. Just the problem of cell line authentication is costing $4 billion.
Dr. Cousins: There are multiple high throughput screening (HTS) academic centers around the world (150 in US). So where does the industry go for best practices in assays? Eli Lilly had developed a manual for HTS best practices and in 1984 made publicly available (Assay Guidance Manual). To date there have been constant updates to this manual to incorporate new assays. Workshops have been developed to train scientists in these best practices.
NIH has been developing new programs to address these reproducability issues. Developed a method called
“Ring Testing Initiative” where multiple centers involved in sharing reagents as well as assays and allowing scientists to test at multiple facilities.
Dr.Tong: Reproduceability of Microarrays: As microarrays were the only methodology to do high through put genomics in the early 2000s, and although much research had been performed to standardize and achieve best reproduceability of the microarray technology (determining best practices in spotting RNA on glass slides, hybridization protocols, image analysis) little had been done on evaluating the reproducibility of results obtained from microarray experiments involving biological samples. The advent of Artificial Intelligence and Machine Learning though can be used to help validate microarray results. This was done in a Nature Biotechnology paper (Nature Biotechnologyvolume28, pages827–838 (2010)) by an international consortium, the International MAQC (Microarray Quality Control) Society and can be found here
However Dr. Tong feels there is much confusion in how we define reproduceability. Dr. Tong identified a few key points of data reproduceability:
Traceability: what are the practices and procedures from going from point A to point B (steps in a protocol or experimental design)
Repeatability: ability to repeat results within the same laboratory
Replicatablilty: ability to repeat results cross laboratory
Transferability: are the results validated across multiple platforms?
The panel then discussed the role of journals and funders to drive reproduceability in research. They felt that editors have been doing as much as they can do as they receive an end product (the paper) but all agreed funders need to do more to promote data validity, especially in requiring that systematic evaluation and validation of each step in protocols are performed.. There could be more training of PIs with respect to protocol and data validation.
Other Articles on Industry/Academic Research Partnerships and Translational Research on this Open Access Online Journal Include