Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
4:00 A New Era of Personalized Therapy: Using Tumor Neoantigens to Unlock the Immune System
Matthew J. Goldstein, M.D., Ph.D., Director, Translational Medicine, Neon Therapeutics, Inc.
Neon Therapeutics, Inc. launched in 2015 to focus on advancing neoantigen biology to improve cancer patient care. A neoantigen-based product engine will allow Neon to develop further treatment modalities including next-generation vaccines and T cell therapies targeting both personalized as well as shared neoantigens. The company’s first trial will launch later this year investigating the combination of a personalized, vaccine with nivolumab in advanced Melanoma, NSCLC, and Bladder Cancer.
4:30 Emerging Innate Immune Targets for Enhancing Adaptive Anti-Tumor Responses
Michael Rosenzweig, Ph.D., Executive Director, Biology-Discovery, IMR Early Discovery, Merck Research Laboratories
Novel cancer immunotherapies targeting T cell checkpoint proteins have emerged as powerful tools to induce profound, durable regression and remission of many types of cancer. Despite these advances, multiple studies have demonstrated that not all patients respond to these therapies, and the ability to predict which patients may respond is limited. Harnessing the innate immune system to augment the adaptive anti-tumor response represents an attractive target for therapy, which has the potential to enhance both the percentage and rate of response to checkpoint blockade.
5:00 Reading Tea Leaves:
The Dilemma of Prediction and Prognosis in Immunotherapy
Morganna Freeman, D.O., Associate Director, Melanoma & Cutaneous Oncology Program, The Angeles Clinic and Research Institute
With the rapid expansion of immunotherapeutics in oncology, scientifically significant advances have been made with both the depth and duration of antitumor responses. However, not all patients benefit, or quickly relapse, thus much scientific inquiry has been devoted to appropriate patient selection and how such obstacles might be overcome. While more is known about potential biomarkers, accurate prognostication persists as a knowledge gap, and efforts to bridge it will be discussed here.
Personalized Immunotherapy | The Immuno-Oncology Summit
August 30-31, 2016 | Marriott Long Wharf Hotel – Boston, MA
Fueled with advances in genomic technologies, personalized oncology promises to innovate cancer therapy and target the previously undruggable space. Developments in immune checkpoint inhibitors, cancer vaccines, and adoptive T-cell therapies, as well as biomarker-driven immuno-oncology clinical trials, are enabling the next generation of cancer therapy. Cambridge Healthtech Institute’s Inaugural Personalized Immunotherapy meeting brings together clinical immuno-oncologists and thought leaders from pharmaceutical and biotech companies, and leading academic teams to share research and case studies in implementing patient-centric approaches to using the immune system to beat cancer.
TUMOR NEOANTIGENS FOR PERSONALIZED IMMUNOTHERAPY
Basics of Personalized Immunotherapy: What Is a Good Antigen?
Pramod K. Srivastava, M.D., Ph.D., Professor, Immunology and Medicine, Director, Carole and Ray Neag Comprehensive Cancer Center, University of Connecticut School of Medicine
Novel Antibodies against Immunogenic Neoantigens
Philip M. Arlen, M.D., President & CEO, Precision Biologics, Inc.
PD-1 Blockade in Tumors with Mismatch-Repair Deficiency
Luis Alberto Diaz, M.D., Associate Professor, Oncology, Johns Hopkins Sidney Kimmel Comprehensive Cancer Center
PERSONALIZED IMMUNOTHERAPY WITH CANCER VACCINES
Cancer Vaccines in the Era of Checkpoint Inhibitors
Keith L. Knutson, Ph.D., Professor, Immunology, Mayo Clinic
Developing Therapeutic Cancer Vaccine Strategies for Prostate Cancer
Ravi Madan, M.D., Clinical Director, Genitourinary Malignancies Branch, National Cancer Institute, National Institutes of Health
Getting Very Personal: Fully Individualized Tumor Neoantigen-Based Vaccine Approaches to Cancer Therapy
Karin Jooss, Ph.D., CSO, Gritstone Oncology
Approaches to Assess Tumor Mutation Load for Selecting Patients for Cancer Immunotherapy
John Simmons, Ph.D., Manager, Research Services, Personal Genome Diagnostics
In situ Vaccination for Lymphoma
Joshua Brody, M.D., Director, Lymphoma Immunotherapy Program, Icahn School of Medicine at Mount Sinai
Immunotherapy Using Ad5 [E1-, E2b-] Vector Vaccines in the Cancer MoonShot 2020 Program
Frank R. Jones, Ph.D., Chairman & CEO, Etubics Corporation
PERSONALIZED CELL THERAPY
Integration of Natural Killer-Based Therapy into the Treatment of Lymphoma
Andrew M. Evens, D.O., Professor and Chief, Hematology/Oncology, Tufts University School of Medicine; Director, Tufts Cancer Center
Dendritic Cells: Personalized Cancer Vaccines and Inducers of Multi-Epitope-Specific T Cells for Adoptive Cell Therapy
Pawel Kalinski, M.D., Ph.D., Professor, Surgery, Immunology, and Bioengineering, University of Pittsburgh School of Medicine, University of Pittsburgh Cancer Institute
Mesothelin-Targeted CAR T-Cell Therapy for Solid Tumors
Prasad S. Adusumilli, M.D., FACS, Deputy Chief of Translational & Clinical Research, Thoracic Surgery, Memorial Sloan-Kettering Cancer Center
Synthetic Regulation of T Cell Therapies Adds Safety and Enhanced Efficacy to Previously Unpredicted Therapies
David M. Spencer, Ph.D., CSO, Bellicum Pharmaceuticals
Long-Term Relapse-Free Survival of Patients with Acute Myeloid Leukemia (AML) Receiving a Telomerase- Engineered Dendritic Cell Immunotherapy
Jane Lebkowski, Ph.D., President & CSO, Research and Development, Asterias Biotherapeutics
Activated and Exhausted Tumor Infiltrating B Cells in Non-Small Cell Lung Cancer Patients Present Antigen and Influence the Phenotype of CD4 Tumor Infiltrating T Cells
Tullia Bruno, Ph.D., Research Assistant Professor, Immunology, University of Pittsburgh
About the Immuno-Oncology Summit
CHI’s 4th Annual Immuno-Oncology Summit has been designed to support a coordinated effort by industry players to bring commercial immunotherapies and immunotherapy combinations through clinical development and into the market. This weeklong, nine-meeting set will include topics ranging from early discovery through clinical development as well as emerging areas such as oncolytic virotherapy. Overall, this event will provide a focused look at how researchers are applying new science and technology in the development of the next generation of effective and safe immunotherapies.
Cambridge Healthtech Institute, 250 First Avenue, Suite 300, Needham, MA 02494 healthtech.com
Tel: 781-972-5400 | Fax: 781-972-5425
This email is being sent to sjwilliamspa@comcast.net. This email communication is for marketing purposes. If it is not of interest to you, please disregard and we apologize for any inconvenience this may have caused.
Visit www.chicorporate.com/corporate_unsubscribe.aspx to update usage.
GE Healthcare has acquired Biosafe Group SA, a supplier of Integrated Cell Bioprocessing Systems for Cell Therapy and Regenerative Medicine Industry
Reporter and Curator: Dr. Sudipta Saha, Ph.D.
Researchers of University of Texas at San Antonio, USA, have developed a new, non-invasive method which can kill cancer cells in two hours, an advance that may significantly help people with inoperable or hard-to-reach tumours, as well as young children stricken with the deadly disease.
The method involves injecting a chemical compound, nitrobenzaldehyde, into the tumour and allowing it to diffuse into the tissue. A beam of light is then aimed at the tissue, causing the cells to become very acidic inside and, essentially, commit suicide. Within two hours, up to 95 per cent of the targeted cancer cells are estimated to be dead.
The method was tested against triple negative breast cancer, one of the most aggressive types of cancer and one of the hardest to treat. The prognosis for triple negative breast cancer is usually very poor. One treatment in the laboratory was able to stop the tumour from growing and doubled the chances of survival in the mice.
According to the researchers all forms of cancer attempt to make cells acidic on the outside and attract the attention of blood vessels as an attempt to get rid of the acid. But, instead, the cancer cells latches onto the blood vessel and uses it to make the tumour grow bigger.
Chemotherapy treatments target all cells in the body, and certain chemotherapeutics try to keep cancer cells acidic as a way to kill the cancer. This is what causes many cancer patients to lose their hair and become weak. This method however, is more precise and can target just the tumour.
This research is presently extended on drug-resistant cancer cells to make this therapy as strong as possible. The researchers also started to develop a nanoparticle that can be injected into the body to target metastasised cancer cells. The nanoparticle is activated with a wavelength of light which can pass harmlessly through skin, flesh and bone and still activate the nanoparticle.
This non-invasive method will help cancer patients with tumours in areas that have proven problematic for surgeons, such as the brain stem, aorta or spine. It could also help people who have received the maximum amount of radiation treatment and can no longer cope with the scarring and pain that goes along with it, or children who are at risk of developing mutations from radiation as they grow older.
Nuha Buchanan Kadri, Matthew Gdovin, Nizar Alyassin, Justin Avila, Aryana Cruz, Louis Cruz, Steve Holliday, Zachary Jordan, Cameron Ruiz and Jennifer Watts. Photodynamic acidification therapy to reduce triple negative breast cancer growth in vivo. Journal of Clinical Oncology, Vol 34, No 15_suppl (May 20 Supplement), 2016: e12574.
Vectorisation Of Immune Checkpoint Inhibitor Antibodies
Reporter: David Orchard-Webb, PhD
The FDA approved ipilimumab (anti-CTLA-4) and nivolumab (anti-PD-1) combination in October 2015 for the treatment of advanced melanoma. The antibodies have recently been approved in the UK for the same indication. Over half of patients respond to the combination [1]. These drugs belong to the class of monoclonal antibodies known as immune checkpoint inhibitors. The binding of anti-CTLA-4 antibodies to activated T cells prevents the surface CTLA-4 receptor from binding CD80 and/or CD86 on antigen presenting cells (APCs). Normally CTLA-4 binding to APCs deactivates the T-cell. Antibodies against programmed cell death protein 1 (PD-1) work by a similar mechanism to CTLA-4. These drugs are delivered by repeated intravenous injections (iv) [2].
Oncolytic viruses are an emerging class of immunotherapeutics that actively stimulate the immune system by releasing tumour antigens via lysis and by virtue of anti-viral immunity. The first FDA approved oncolytic virus (Imlygic), developed by Amgen/ BioVex, was given the green light in October 2015 for advanced melanoma patients delivered via direct tumour injection. The mechanism of action of oncolytic viruses is highly complementary with checkpoint inhibitor antibodies and multiple trials combining these two classes of agent are under way.
At the recent American Association for Cancer Research (AACR) annual meeting in New Orleans, Louisiana, the oldest biotechnology company in France – Transgene, presented preclinical data concerning oncolytic vaccinia viruses that express whole antibody (mAb), Fragment antigen-binding (Fab) or single-chain variable fragment (scFv) against mouse PD-1 [3]. These combinations proved superior over virus alone in mouse xenografts of melanoma and fibrosarcoma cell lines. Transgene claim that “these results pave the way for next generation of oncolytic vaccinia armed with immunomodulatory therapeutic proteins such as mAbs” (Figure 1) [3].
Figure 1: The convergence of therapeutics based on oncolytic viruses and monoclonal antibodies against immune checkpoint inhibotor proteins. Image Source:Eric Molina. No changes were made. Creative Commons Attribution 2.0 Generic (CC BY 2.0).
The combination of immune checkpoint inhibitors and oncolytic virus as a single molecular entity clearly has advantages in terms of manufacturing cost effectiveness. In addition viral vectors have the capacity for perfect specificity to tumours which has potential safety advantages.
The retina is responsible for capturing images from the visual field. Retinitis pigmentosa, which refers to a group of inherited diseases that cause retinal degeneration, causes a gradual decline in vision because retinal photoreceptor cells (rods and cones) die. Images on the left are courtesy of the National Eye Institute, NIH; image on the right is courtesy of Robert Fariss, Ph.D., and Ann Milam, Ph.D., National Eye Institute, NIH.
Metabolomics, the comprehensive evaluation of the products of cellular processes, can provide new findings and insight in a vast array of diseases and dysfunctions. Though promising, metabolomics lacks the standing of genomics or proteomics. It is, in a manner of speaking, the new kid on the “omics” block.
Even though metabolomics is still an emerging discipline, at least some quarters are giving it a warm welcome. For example, metabolomics is being advanced by the Common Fund, an initiate of the National Institutes of Health (NIH). The Common Fund has established six national metabolomics cores. In addition, individual agencies within NIH, such as the National Institute of Environmental Health Sciences (NIEHS), are releasing solicitations focused on growing more detailed metabolomics programs.
Whether metabolomic studies are undertaken with or without public support, they share certain characteristics and challenges. Untargeted or broad-spectrum studies are used for hypotheses generation, whereas targeted studies probe specific compounds or pathways. Reproducibility is a major challenge in the field; many studies cannot be reproduced in larger cohorts. Carefully defined guidance and standard operating procedures for sample collection and processing are needed.
While these challenges are being addressed, researchers are patiently amassing metabolomic insights in several areas, such as retinal diseases, neurodegenerative diseases, and autoimmune diseases. In addition, metabolomic sleuths are availing themselves of a growing selection of investigative tools.
A Metabolomic Eye on Retinal Degeneration
The retina has one of the highest metabolic activities of any tissue in the body and is composed of multiple cell types. This fact suggests that metabolomics might be helpful in understanding retinal degeneration. At least, that’s what occurred to Ellen Weiss, Ph.D., a professor of cell biology and physiology at the University of North Carolina School of Medicine at Chapel Hill. To explore this possibility, Dr. Weiss began collaborating with Susan Sumner, Ph.D., director of systems and translational sciences at RTI International.
Retinal degeneration is often studied through the use of genetic-mouse models that mimic the disease in humans. In the model used by Dr. Weiss, cells with a disease-causing mutation are the major light-sensing cells that degenerate during the disease. Individuals with the same or a similar genetic mutation will initially lose dim-light vision then, ultimately, bright-light vision and color vision.
Wild-type and mutant phenotypes, as well as dark- and light-raised animals, were compared, since retinal degeneration is exacerbated by light in this genetic model. Retinas were collected as early as day 18, prior to symptomatic disease, and analyzed. Although data analysis is ongoing, distinct differences have emerged between the phenotypes as well as between dark- and light-raised animals.
“There is a clear increase in oxidative stress in both light-raised groups but to a larger extent in the mutant phenotype,” reports Dr. Weiss. “There are global changes in metabolites that suggest mitochondrial dysfunction, and dramatic changes in lipid profiles. Now we need to understand how these metabolites are involved in this eye disease and the relevance of these perturbations.”
For example, the glial cells in the retina that upregulate a number of proteins in response to stress to attempt to save the retina are as likely as the light-receptive neurons to undergo metabolic changes.
“One of the challenges in metabolomics studies is assigning the signals that represent the metabolites or compounds in the samples,” notes Dr. Sumner. “Signals may be ‘unknown unknowns,’ compounds that have never been identified before, or ‘known unknowns,’ compounds that are known but that have not yet been assigned in the biological matrix.”
Internal and external libraries, such as the Human Metabolome Dictionary, are used to match signals. Whether or not a match exists, fragmentation patterns are used to characterize the metabolite, and when possible a standard is obtained to confirm identity. To assist with this process, the NIH Common Fund supports Metabolite Standard Synthesis Cores (MSSCs). RTI International holds an MSSC contract in addition to being a NIH-designated metabolomics core.
Mitochondrial Dysfunction in Alzheimer’s Disease
Alzheimer’s disease (AD) is difficult to diagnose early due to its asymptomatic phase; accurate diagnosis occurs only in postmortem brain tissue. To evaluate familial AD, a rare inherited form of the disease, the laboratory of Eugenia Trushina, Ph.D., associate professor of neurology and associate professor of pharmacology at the Mayo Clinic, uses mouse models to study the disease’s early molecular mechanisms.
Synaptic loss underlies cognitive dysfunction. The length of neurons dictates that mitochondria move within the cell to provide energy at the site of the synapses. An initial finding was that very early on mitochondrial trafficking was affected reducing energy supply to synapses and distant parts of the cell.
During energy production, the major mitochondrial metabolite is ATP, but the organelle also produces many other metabolites, molecules that are implicated in many pathways. One can assume that changes in energy utilization, production, and delivery are associated with some disturbance.
“Our goal,” explains Dr. Trushina, “was to get a proof of concept that we could detect in the blood of AD patients early changes of mitochondria dysfunction or other changes that could be informative of the disease over time.”
A Mayo Clinic aging study involves a cohort of patients, from healthy to those with mild cognitive impairment (MCI) through AD. Patients undergo an annual battery of tests including cognitive function along with blood and cerebrospinal fluid sampling. Metabolic signatures in plasma and cerebrospinal fluid of normal versus various disease stages were compared, and affected mitochondrial and lipid pathways identified in MCI patients that progressed to AD.
“Last year we published on a new compound that goes through the blood/brain barrier, gets into mitochondria, and very specifically, partially inhibits mitochondrial complex I activity, making the cell resistant to oxidative damage,” details Dr. Trushina. “The compound was able to either prevent or slow the disease in the animal familial models.
“Treatment not only reduced levels of amyloid plaques and phosphorylated tau, it also restored mitochondrial transport in neurons. Now we have additional compounds undergoing investigation for safety in humans, and target selectivity and engagement.”
“Mitochondria play a huge role in every aspect of our lives,” Dr. Trushina continues. “The discovery seems counterintuitive, but if mitochondria function is at the heart of AD, it may provide insight into the major sporadic form of the disease.”
Distinguishing Types of Asthma
In children, asthma generally manifests as allergy-induced asthma, or allergic asthma. And allergic asthma has commonalities with allergic dermatitis/eczema, food allergies, and allergic rhinitis. In adults, asthma is more heterogeneous, and distinct and varied subpopulations emerge. Some have nonallergic asthma; some have adult-onset asthma; and some have obesity-, occupational-, or exercise-induced asthma.
Adult asthmatics may have markers of TH2 high verus TH2 low asthma (T helper 2 cell cytokines) and they may respond to various triggers—environmental antigens, occupational antigens, irritants such as perfumes and chlorine, and seasonal allergens. Exercise, too, can trigger asthma.
One measure that can phenotype asthmatics is nitric oxide, an exhaled breath biomarker. Nitric oxide is a smooth muscle relaxant, vasodilator, and bronchodilator that can have anti-inflammatory properties. There is a wide range of values in asthmatics, and a number of values are needed to understand the trend in a particular patient. L-arginine is the amino acid that produces nitric oxide when converted to L-citrulline, a nonessential amino acid.
According to Nicholas Kenyon, M.D., a pulmonary and critical care specialist who is co-director of the University of California, Davis Asthma Network (UCAN), some metabolomic studies suggest that there is a state of L-arginine depletion during asthma attacks or in severe asthma suggesting a lack of substrate to produce nitric oxide. Dr. Kenyon is conducting clinical work on L-arginine supplementation in a double-blind cross-over intervention trial of L-arginine versus placebo. The 50-subject study in severe asthmatics should be concluded in early 2017.
Many new biologic therapies are coming to market to treat asthma; it will be challenging to determine which advanced therapy to provide to which patient. Therapeutics mostly target severe asthma populations and are for patients with evidence of higher numbers of eosinophils in the blood and lung, which include anti-IL-5 and (soon) anti-IL-13, among others.
Tools Development
Waters is developing metabolomics applications that use multivariate statistical methods to highlight compounds of interest. Typically these applications combine separation procedures, accomplished by means of liquid chromatography or gas chromatography (LC or GC), with detection methods that rely on mass spectrometry (MS). To support the identification, quantification, and analysis of LC-MS data, the company provides bioinformatics software. For example, Progenesis QI software can interrogate publicly available databases and process information about isotopic patterns, retention times, and collision cross-sections.
Mass spectrometry (MS) is the gold standard in metabolomics and lipidomics. But there is a limit to what accurate mass and resolution can achieve. For example, neither isobaric nor isomeric species are resolvable solely by MS. New orthogonal analytical tools will allow more confident identifications.
To improve metabolomics separations before MS detection, a post-ionization separation tool, like ion mobility, which is currently used to support traditional UPLC-MS and MS imaging metabolomics protocols, becomes useful. The collision-cross section (CCS), which measures the shape of molecules, can be derived, and it can be used as an additional identification coordinate.
Other new chromatographic tools are under development, such as microflow devices and UltraPerformance Convergence Chromatography (UPC2), which uses liquid CO2 as its mobile phase, to enable new ways of separating chiral metabolites. Both UPC2 and microflow technologies have decreased solvent consumption and waste disposal while maintaining UPLC-quality performance in terms of chromatographic resolution, robustness, and reproducibility.
Informatics tools are also improving. In the latest versions of Waters’ Progenesis software, typical metabolomics identification problems are resolved by allowing interrogation of publicly available databases and scoring according to accurate mass, isotopic pattern, retention time, CCS, and either theoretical or experimental fragments.
MS imaging techniques, such as MALDI and DESI, provide spatial information about the metabolite composition in tissues. These approaches can be used to support and confirm traditional analyses without sample extraction, and they allow image generation without the use of antibodies, similar to immunohistochemistry.
“Ion-mobility tools will soon be implemented for routine use, and the use of extended CCS databases will help with metabolite identification,” comments Giuseppe Astarita Ph.D., principal scientist, Waters. “More applications of ambient ionization MS will emerge, and they will allow direct-sampling analyses at atmospheric pressure with little or no sample preparation, generating real-time molecular fingerprints that can be used to discriminate among phenotypes.”
Microflow Technology
Microflow technology offers sensitivity and robustness. For example, at the Proteomics and Metabolomics Facility, Colorado State University, peptide analysis was typically performed using nanoflow chromatography; however, nanoflow chromatography is slow and technically challenging. Moving to microflow offered significant improvements in robustness and ease-of-use and resulted in improved chromatography without sacrificing sensitivity.
Conversely, small molecule applications were typically performed with analytical-scale chromatography. While this flow regime is extremely robust and fast, it can sometimes be limited in sensitivity. Moving to microflow offered significant improvements in sensitivity, 5- to 10-fold depending on the compound, without sacrificing robustness.
But broad-scale microflow adoption is hampered by a lack of available column chemistries and legacy HPLC or UPLC infrastructure that is not conducive to low-flow operation.
“We utilize microflow technology on all of our tandem quadrupole instruments for targeted quantitative assays,” says Jessica Prenni, Ph.D., director, Proteomics and Metabolomics Facility, Colorado State University. “All of our peptide quantitation is exclusively performed with microflow technology, and many of our small molecule assays. Application examples include endocannabinoids, bile acids and plant phytohormone panels.”
Compound annotation and comparability and transparency in data processing and reporting is a challenge in metabolomics research. Multiple groups are actively working on developing new tools and strategies; common best practices need to be adopted.
The continued growth of open-source spectral databases and new tools for spectral prediction from compound databases will dramatically impact the ability for metabolomics to result in novel discoveries. The move to a systems-level understanding through the combination of various omics data also will have a huge influence and be enabled by the continued development of open-source and user-friendly pathway-analysis tools.
Where Trackless Terrain Once Challenged Biomarker Development, Clearer Paths Are Emerging
Fusion detection can be carried out with traditional opposing primer-based library preparation methods, which require target- and fusion-specific primers that define the region to be sequenced. With these methods, primers are needed that flank the target region and the fusion partner, so only known fusions can be detected. An alternative method, ArcherDX’ Anchored Multiplex PCR (AMP), can be used to detect the target of interest, plus any known and unknown fusion partners. This is because AMP uses target-specific unidirectional primers, along with reverse primers, that hybridize to the sequencing adapter that is ligated to each fragment prior to amplification.
In time, the narrow, tortuous paths followed by pioneers become wider and straighter, whether the pioneers are looking to settle new land or bring new biomarkers to the clinic.
In the case of biomarkers, we’re still at the stage where pioneers need to consult guides and outfitters or, in modern parlance, consultants and technology providers. These hardy souls tend to congregate at events like the Biomarker Conference, which was held recently in San Diego.
At this event, biomarker experts discussed ways to avoid unfortunate detours on the trail from discovery and development to clinical application and regulatory approval. Of particular interest were topics such as the identification of accurate biomarkers, the explication of disease mechanisms, the stratification of patient groups, and the development of standard protocols and assay platforms. In each of these areas, presenters reported progress.
Another crucial subject is the integration of techniques such as next-generation sequencing (NGS). This particular technique has been instrumental in advancing clinical cancer genomics and continues to be the most feasible way of simultaneously interrogating multiple genes for driver mutations.
Enriching nucleic acid libraries for target genes of interest prior to NGS greatly enhances the sensitivity of detecting mutations, as the enriched regions are sequenced multiple times. This is particularly useful when analyzing clinical samples, which generate low amounts of poor-quality nucleic acids.
Most target-enrichment strategies require prior knowledge of both ends of the target region to be sequenced. Therefore, only gene fusions with known partners can be amplified for downstream NGS assays.
Archer’s Anchored Multiplex PCR (AMP™) technology overcomes this limitation, as it can enrich for novel fusions, while only requiring knowledge of one end of the fusion pair. At the heart of the AMP chemistry are unique Molecular Barcode (MBC) adapters, ligated to the 5′ ends of DNA fragments prior to amplification. The MBCs contain universal primer binding sites for PCR and a molecular barcode for identifying unique molecules. When combined with 3′ gene-specific primers, MBCs enable amplification of target regions with unknown 5′ ends.
“Tagging each molecule of input nucleic acid with a unique molecular barcode allows for de-duplication, error correction, and quantitative analysis, resulting in high sequencing consensus. With its low error rate and low limits of detection, AMP is revolutionizing the field of cancer genomics.”
In a proof-of-concept study, a single-tube 23-plex panel was designed to amplify the kinase domains of ALK, RET, ROS1, and MUSK genes by AMP. This enrichment strategy enabled identification of gene fusions with multiple partners and alternative splicing events in lung cancer, thyroid cancer, and glioblastoma specimens by NGS.
Over the last decade, the Biomarker/Translational Research Laboratory has focused on developing clinical genotyping and fluorescent in situ hybridization (FISH) assays for rapid personalized genomic testing.
“Initially, we analyzed the most prevalent hotspot mutations, about 160 in 25 cancer genes,” continued Dr. Borger. “However, this approach revealed mutations in only half of our patients. With the advent of NGS, we are able to sequence 190 exons in 39 cancer genes and obtain significantly richer genetic fingerprints, finding genetic aberrations in 92% of our cancer patients.”
Using multiplexed approaches, Dr. Borger’s team within the larger Center for Integrated Diagnostics (CID) program at MGH has established high-throughput genotyping service as an important component of routine care. While only a few susceptible molecular alterations may currently have a corresponding drug, the NGS-driven analysis may supply new information for inclusion of patients into ongoing clinical trials, or bank the result for future research and development.
“A significant impediment to discovery of clinically relevant genomic signatures is our current inability to interconnect the data,” explained Dr. Borger. “On the local level, we are striving to compile the data from clinical observations, including responses to therapy and genotyping. Globally, it is imperative that comprehensive public databases become available to the research community.”
This image, from the Massachusetts General Hospital Cancer Center, shows multicolor fluorescence in situ hybridization (FISH) analysis of cells from a patient with esophagogastric cancer. Remarkably, the FISH analysis revealed that co-amplification of the MET gene (red signal) and the EGFR gene (green signal) existed simultaneously in the same tumor cells. A chromosome 7 control probe is shown in blue.
Tumor profiling at MGH have already yielded significant discoveries. Dr. Borger’s lab, in collaboration with oncologists at the MGH Cancer Center, found significant correlations between mutations in the genes encoding the metabolic enzymes isocitrate dehydrogenase (IDH1 and IDH2) and certain types of cancers, such as cholangiocarcinoma and acute myelogenous leukemia (AML).
Historically, cancer signatures largely focus on signaling proteins. Discovery of a correlative metabolic enzyme offered a promise of diagnostics based on metabolic byproducts that may be easily identified in blood. Indeed, the metabolite 2-hydroxyglutarate accumulates to high levels in the tissues of patients carrying IDH1 and IDH2 mutations. They have reported that circulating 2-hydroxyglutarate as measured in the blood correlates with tumor burden, and could serve as an important surrogate marker of treatment response. …..
Researchers Uncover How ‘Silent’ Genetic Changes Drive Cancer
“Traditionally, it has been hard to use standard methods to quantify the amount of tRNA in the cell,” says Tavazoie. The lead authors of the article, Hani Goodarzi, formerly a postdoc in the lab and now a new assistant professor at UCSF, and research assistant Hoang Nguyen, devised and applied a new method that utilizes state-of-the-art genomic sequencing technology to measure the amount of tRNAs in different cell types.
The team chose to compare breast tissue from healthy individuals with tumor samples taken from breast cancer patients–including both primary tumors that had not spread from the breast to other body sites, and highly aggressive, metastatic tumors.
They found that the levels of two specific tRNAs were significantly higher in metastatic cells and metastatic tumors than in primary tumors that did not metastasize or healthy samples. “There are four different ways to encode for the protein building block arginine,” explains Tavazoie. “Yet only one of those–the tRNA that recognizes the codon CGG–was associated with increased metastasis.”
The tRNA that recognizes the codon GAA and encodes for a building block known as glutamic acid was also elevated in metastatic samples.
The team hypothesized that the elevated levels of these tRNAs may in fact drive metastasis. Working in mouse models of primary, non-metastatic tumors, the researchers increased the production of the tRNAs, and found that these cells became much more invasive and metastatic.
They also did the inverse experiment, with the anticipated results: reducing the levels of these tRNAs in metastatic cells decreased the incidence of metastases in the animals.
How do two tRNAs drive metastasis? The researchers teamed up with members of the Rockefeller University proteomics facility to see how protein expression changes in cells with elevated levels of these two tRNAs.
“We found global increases in many dozens of genes,” says Tavazoie, “so we analyzed their sequences and found that the majority of them had significantly increased numbers of these two specific codons.”
According to the researchers, two genes stood out among the list. Known as EXOSC2 and GRIPAP1, these genes were strongly and directly induced by elevated levels of the specific glutamic acid tRNA.
“When we mutated the GAA codons to GAG– a “silent” mutation because they both spell out the protein building block glutamic acid–we found that increasing the amount of tRNA no longer increased protein levels,” explains Tavazoie. These proteins were found to drive breast cancer metastasis.
The work challenges previous assumptions about how tRNAs function and suggests that tRNAs can modulate gene expression, according to the researchers. Tavazoie points out that “it is remarkable that within a single cell type, synonymous changes in genetic sequence can dramatically affect the levels of specific proteins, their transcripts, and the way a cell behaves.”
Testing Blood Metabolites Could Help Tailor Cancer Treatment
Scientists have found that measuring how cancer treatment affects the levels of metabolites – the building blocks of fats and proteins – can be used to assess whether the drug is hitting its intended target.
This new way of monitoring cancer therapy could speed up the development of new targeted drugs – which exploit specific genetic weaknesses in cancer cells – and help in tailoring treatment for patients.
Scientists at The Institute of Cancer Research, London, measured the levels of 180 blood markers in 41 patients with advanced cancers in a phase I clinical trial conducted with The Royal Marsden NHS Foundation Trust.
They found that investigating the mix of metabolic markers could accurately assess how cancers were responding to the targeted drug pictilisib.
Their study was funded by the Wellcome Trust, Cancer Research UK and the pharmaceutical company Roche, and is published in the journal Molecular Cancer Therapeutics.
Pictilisib is designed to specifically target a molecular pathway in cancer cells, called PI3 kinase, which has key a role in cell metabolism and is defective in a range of cancer types.
As cancers with PI3K defects grow, they can cause a decrease in the levels of metabolites in the bloodstream.
The new study is the first to show that blood metabolites are testable indicators of whether or not a new cancer treatment is hitting the correct target, both in preclinical mouse models and also in a trial of patients.
Using a sensitive technique called mass spectrometry, scientists at The Institute of Cancer Research (ICR) initially analysed the metabolite levels in the blood of mice with cancers that had defects in the PI3K pathway.
They found that the blood levels of 26 different metabolites, which were low prior to therapy, had risen considerably following treatment with pictilisib. Their findings indicated that the drug was hitting its target, and reversing the effects of the cancer on mouse metabolites.
Similarly, in humans the ICR researchers found that almost all of the metabolites – 22 out of the initial 26 – once again rose in response to pictilisib treatment, as seen in the mice.
Blood levels of the metabolites began to increase after a single dose of pictilisib, and were seen to drop again when treatment was stopped, suggesting that the effect was directly related to the drug treatment.
Metabolites vary naturally depending on the time of day or how much food a patient has eaten. But the researchers were able to provide the first strong evidence that despite this variation metabolites can be used to test if a drug is working, and could help guide decisions about treatment.
New Metabolic Pathway Reveals Aspirin-Like Compound’s Anti-Cancer Properties
Researchers at the Gladstone Institutes say they have found a new pathway by which salicylic acid, a key compound in the nonsteroidal anti-inflammatory drugs aspirin and diflunisal, stops inflammation and cancer.
In a study (“Salicylate, Diflunisal and Their Metabolites Inhibit CBP/p300 and Exhibit Anticancer Activity”) published in eLife, the investigators discovered that both salicylic acid and diflunisal suppress two key proteins that help control gene expression throughout the body. These sister proteins, p300 and CREB-binding protein (CBP), are epigenetic regulators that control the levels of proteins that cause inflammation or are involved in cell growth.
By inhibiting p300 and CBP, salicylic acid and diflunisal block the activation of these proteins and prevent cellular damage caused by inflammation. This study provides the first concrete demonstration that both p300 and CBP can be targeted by drugs and may have important clinical implications, according to Eric Verdin, M.D., associate director of the Gladstone Institute of Virology and Immunology .
“Salicylic acid is one of the oldest drugs on the planet, dating back to the Egyptians and the Greeks, but we’re still discovering new things about it,” he said. “Uncovering this pathway of inflammation that salicylic acid acts upon opens up a host of new clinical possibilities for these drugs.”
Earlier research conducted in the laboratory of co-author Stephen D. Nimer, M.D., director of Sylvester Comprehensive Cancer Center at the University of Miami Miller School of Medicine, and a collaborator of Verdin’s, established a link between p300 and the leukemia-promoting protein AML1-ETO. In the current study, scientists at Gladstone and Sylvester worked together to test whether suppressing p300 with diflunisal would suppress leukemia growth in mice. As predicted, diflunisal stopped cancer progression and shrunk the tumors in the mouse model of leukemia. ……
Novel Protein Agent Targets Cancer and Host of Other Diseases
Researchers at Georgia State University have designed a new protein compound that can effectively target the cell surface receptor integrin v3, mutations in which have been linked to a number of diseases. Initial results using this new molecule show its potential as a therapeutic treatment for an array of illnesses, including cancer.
The novel protein molecule targets integrin v3 at a novel site that has not been targeted by other scientists. The researchers found that the molecule induces apoptosis, or programmed cell death, of cells that express integrin v3. This integrin has been a focus for drug development because abnormal expression of v3 is linked to the development and progression of various diseases.
“This integrin pair, v3, is not expressed in high levels in normal tissue,” explained senior study author Zhi-Ren Liu, Ph.D., professor in the department of biology at Georgia State. “In most cases, it’s associated with a number of different pathological conditions. Therefore, it constitutes a very good target for multiple disease treatment.”
“Here we use a rational design approach to develop a therapeutic protein, which we call ProAgio, which binds to integrin αvβ3 outside the classical ligand-binding site,” the authors wrote. “We show ProAgio induces apoptosis of integrin αvβ3-expressing cells by recruiting and activating caspase 8 to the cytoplasmic domain of integrin αvβ3.”
The findings from this study were published recently in Nature Communications in an article entitled “Rational Design of a Protein That Binds Integrin αvβ3 Outside the Ligand Binding Site.” …..
“We took a unique angle,” Dr. Lui noted. “We designed a protein that binds to a different site. Once the protein binds to the site, it directly triggers cell death. When we’re able to kill pathological cells, then we’re able to kill the disease.”
The investigators performed extensive cell and molecular testing that confirmed ProAgio interacts and binds well with integrin v3. Interestingly, they found that ProAgio induces apoptosis by recruiting caspase 8—an enzyme that plays an essential role in programmed cell death—to the cytoplasmic area of integrin v3. ProAgio was much more effective in inducing cell death than other agents tested.
Noncoding RNAs Not So Noncoding
Bits of the transcriptome once believed to function as RNA molecules are in fact translated into small proteins.
In 2002, a group of plant researchers studying legumes at the Max Planck Institute for Plant Breeding Research in Cologne, Germany, discovered that a 679-nucleotide RNA believed to function in a noncoding capacity was in fact a protein-coding messenger RNA (mRNA).1 It had been classified as a long (or large) noncoding RNA (lncRNA) by virtue of being more than 200 nucleotides in length. The RNA, transcribed from a gene called early nodulin 40 (ENOD40), contained short open reading frames (ORFs)—putative protein-coding sequences bookended by start and stop codons—but the ORFs were so short that they had previously been overlooked. When the Cologne collaborators examined the RNA more closely, however, they found that two of the ORFs did indeed encode tiny peptides: one of 12 and one of 24 amino acids. Sampling the legumes confirmed that these micropeptides were made in the plant, where they interacted with a sucrose-synthesizing enzyme.
Five years later, another ORF-containing mRNA that had been posing as a lncRNA was discovered inDrosophila.2,3 After performing a screen of fly embryos to find lncRNAs, Yuji Kageyama, then of the National Institute for Basic Biology in Okazaki, Japan, suppressed each transcript’s expression. “Only one showed a clear phenotype,” says Kageyama, now at Kobe University. Because embryos missing this particular RNA lacked certain cuticle features, giving them the appearance of smooth rice grains, the researchers named the RNA “polished rice” (pri).
Turning his attention to how the RNA functioned, Kageyama thought he should first rule out the possibility that it encoded proteins. But he couldn’t. “We actually found it was a protein-coding gene,” he says. “It was an accident—we are RNA people!” The pri gene turned out to encode four tiny peptides—three of 11 amino acids and one of 32—that Kageyama and colleagues showed are important for activating a key developmental transcription factor.4
Since then, a handful of other lncRNAs have switched to the mRNA ranks after being found to harbor micropeptide-encoding short ORFs (sORFs)—those less than 300 nucleotides in length. And given the vast number of documented lncRNAs—most of which have no known function—the chance of finding others that contain micropeptide codes seems high.
Overlooked ORFs
From the late 1990s into the 21st century, as species after species had their genomes sequenced and deposited in databases, the search for novel genes and their associated mRNAs duly followed. With millions or even billions of nucleotides to sift through, researchers devised computational shortcuts to hunt for canonical gene and mRNA features, such as promoter regions, exon/intron splice sites, and, of course, ORFs.
ORFs can exist in practically any stretch of RNA sequence by chance, but many do not encode actual proteins. Because the chance that an ORF encodes a protein increases with its length, most ORF-finding algorithms had a size cut-off of 300 nucleotides—translating to 100 amino acids. This allowed researchers to “filter out garbage—that is, meaningless ORFs that exist randomly in RNAs,” says Eric Olsonof the University of Texas Southwestern Medical Center in Dallas.
Of course, by excluding all ORFs less than 300 nucleotides in length, such algorithms inevitably missed those encoding genuine small peptides. “I’m sure that the people who came up with [the cut-off] understood that this rule would have to miss anything that was shorter than 100 amino acids,” saysNicholas Ingolia of the University of California, Berkeley. “As people applied this rule more and more, they sort of lost track of that caveat.” Essentially, sORFs were thrown out with the computational trash and forgotten.
Aside from statistical practicality and human oversight, there were also technical reasons that contributed to sORFs and their encoded micropeptides being missed. Because of their small size, sORFs in model organisms such as mice, flies, and fish are less likely to be hit in random mutagenesis screens than larger ORFs, meaning their functions are less likely to be revealed. Also, many important proteins are identified based on their conservation across species, says Andrea Pauli of the Research Institute of Molecular Pathology in Vienna, but “the shorter [the ORF], the harder it gets to find and align this region to other genomes and to know that this is actually conserved.”
As for the proteins themselves, the standard practice of using electrophoresis to separate peptides by size often meant micropeptides would be lost, notes Doug Anderson, a postdoc in Olson’s lab. “A lot of times we run the smaller things off the bottom of our gels,” he says. Standard protein mass spectrometry was also problematic for identifying small peptides, says Gerben Menschaert of Ghent University in Belgium, because “there is a washout step in the protocol so that only larger proteins are retained.”
But as researchers take a deeper dive into the function of the thousands of lncRNAs believed to exist in genomes, they continue to uncover surprise micropeptides. In February 2014, for example, Pauli, then a postdoc in Alex Schier’s lab at Harvard University, discovered a hidden code in a zebrafish lncRNA. She had been hunting for lncRNAs involved in zebrafish development because “we hadn’t really anticipated that there would be any coding regions out there that had not been discovered—at least not something that is essential,” she says. But one lncRNA she identified actually encoded a 58-amino-acid micropeptide, which she called Toddler, that functioned as a signaling protein necessary for cell movements that shape the early embryo.5
Then, last year, Anderson and his colleagues reported another. Since joining Olson’s lab in 2010, Anderson had been searching for lncRNAs expressed in the heart and skeletal muscles of mouse embryos. He discovered a number of candidates, but one stood out for its high level of sequence conservation—suggesting to Anderson that it might have an important function. He was right, the RNA was important, but for a reason that neither Anderson nor Olson had considered: it was in fact an mRNA encoding a 46-amino-acid-long micropeptide.6
“When we zeroed in on the conserved region [of the gene], Doug found that it began with an ATG [start] codon and it terminated with a stop codon,” Olson says. “That’s when he looked at whether it might encode a peptide and found that indeed it did.” The researchers dubbed the peptide myoregulin, and found that it functioned as a critical calcium pump regulator for muscle relaxation.
With more and more overlooked peptides now being revealed, the big question is how many are left to be discovered. “Were there going to be dozens of [micropeptides]? Were there going to be hundreds, like there are hundreds of microRNAs?” says Ingolia. “We just didn’t know.”
Little things mean a lot. To any biologist, this time-worn maxim is old news. But it’s worth revisiting. As several articles in this issue of The Scientist illustrate, how researchers define and examine the “little things” does mean a lot.
Consider this month’s cover story, “Noncoding RNAs Not So Noncoding,” by TS correspondent Ruth Williams. Combing the human genome for open reading frames (ORFs), sequences bracketed by start and stop codons, yielded a protein-coding count somewhere in the neighborhood of 24,000. That left a lot of the genome relegated to the category of junk—or, later, to the tens of thousands of mostly mysterious long noncoding RNAs (lncRNAs). But because they had only been looking for ORFs that were 300 nucleotides or longer (i.e., coding for proteins at least 100 amino acids long), genome probers missed so-called short ORFs (sORFs), which encode small peptides. “Their diminutive size may have caused these peptides to be overlooked, their sORFs to be buried in statistical noise, and their RNAs to be miscategorized, but it does not prevent them from serving important, often essential functions, as the micropeptides characterized to date demonstrate,” writes Williams.
How little things work definitely informs another field of life science research: synthetic biology. As the functions of genes and gene networks are sussed out, bioengineers are using the information to design small, synthetic gene circuits that enable them to better understand natural networks. In “Synthetic Biology Comes into Its Own,” Richard Muscat summarizes the strides made by synthetic biologists over the last 15 years and offers an optimistic view of how such networks may be put to use in the future. And to prove him right, just as we go to press, a collaborative group led by one of syn bio’s founding fathers, MIT’s James Collins, has devised a paper-based test for Zika virus exposure that relies on a freeze-dried synthetic gene circuit that changes color upon detection of RNAs in the viral genome. The results are ready in a matter of hours, not the days or weeks current testing takes, and the test can distinguish Zika from dengue virus. “What’s really exciting here is you can leverage all this expertise that synthetic biologists are gaining in constructing genetic networks and use it in a real-world application that is important and can potentially transform how we do diagnostics,” commented one researcher about the test.
Moving around little things is the name of the game when it comes to delivering a package of drugs to a specific target or to operating on minuscule individual cells. Mini-scale delivery of biocompatible drug payloads often needs some kind of boost to overcome fluid forces or size restrictions that interfere with fine-scale manipulation. To that end, ingenious solutions that motorize delivery by harnessing osmotic changes, magnets, ultrasound, and even bacterial flagella are reviewed in “Making Micromotors Biocompatible.”
Cilengitide, a cyclic RGD pentapeptide, is currently in clinical phase III for treatment of glioblastomas and in phase II for several other tumors. This drug is the first anti-angiogenic small molecule targeting the integrins αvβ3, αvβ5 and α5β1. It was developed by us in the early 90s by a novel procedure, the spatial screening. This strategy resulted in c(RGDfV), the first superactive αvβ3 inhibitor (100 to 1000 times increased activity over the linear reference peptides), which in addition exhibited high selectivity against the platelet receptor αIIbβ3. This cyclic peptide was later modified by N-methylation of one peptide bond to yield an even greater antagonistic activity in c(RGDf(NMe)V). This peptide was then dubbed Cilengitide and is currently developed as drug by the company Merck-Serono (Germany).
This article describes the chemical development of Cilengitide, the biochemical background of its activity and a short review about the present clinical trials. The positive anti-angiogenic effects in cancer treatment can be further increased by combination with “classical” anti-cancer therapies. Several clinical trials in this direction are under investigation.
Integrins are heterodimeric receptors that are important for cell-cell and cell-extracellular matrix (ECM) interactions and are composed of one α and one β-subunit [1, 2]. These cell adhesion molecules act as transmembrane linkers between their extracellular ligands and the cytoskeleton, and modulate various signaling pathways essential in the biological functions of most cells. Integrins play a crucial role in processes such as cell migration, differentiation, and survival during embryogenesis, angiogenesis, wound healing, immune and non-immune defense mechanisms, hemostasis and oncogenic transformation [1]. The fact that many integrins are also linked with pathological conditions has converted them into very promising therapeutic targets [3]. In particular, integrins αvβ3, αvβ5 and α5β1 are involved in angiogenesis and metastasis of solid tumors, being excellent candidates for cancer therapy [4–7].
There are a number of different integrin subtypes which recognize and bind to the tripeptide sequence RGD (arginine, glycine, aspartic acid), which represents the most prominent recognition motif involved in cell adhesion. For example, the pro-angiogenic αvβ3 integrin binds various RGD-containing proteins, including fibronectin (Fn), fibrinogen (Fg), vitronectin (Vn) and osteopontin [8]. It is therefore not surprising that this integrin has been targeted for cancer therapy and that RGD-containing peptides and peptidomimetics have been designed and synthesized aiming to selectively inhibit this receptor [9, 10].
One classical strategy used in drug design is based on the knowledge about the structure of the receptor-binding pocket, preferably in complex with the natural ligand. However, this strategy, the so-called “rational structure-based design”, could not be applied in the field of integrin ligands since the first structures of integrin’s extracellular head groups were not described until 2001 for αvβ3 [11] (one year later, in 2002 the structure of this integrin in complex with Cilengitide was also reported [12]) and 2004 for αIIbβ3 [13]. Therefore, initial efforts in this field focused on a “ligand-oriented design”, which concentrated on optimizing RGD peptides by means of different chemical approaches in order to establish structure-activity relationships and identify suitable ligands.
We focused our interest in finding ligands for αvβ3 and based our approach on three chemical strategies pioneered in our group: 1) Reduction of the conformational space by cyclization; 2) Spatial screening of cyclic peptides; and 3)N-Methyl scan.
The combination of these strategies lead to the discovery of the cyclic peptidec(RGDf(NMe)V) in 1995. This peptide showed subnanomolar antagonistic activity for the αvβ3 receptor, nanomolar affinities for the closely related integrins αvβ5 and α5β1, and high selectivity towards the platelet receptor αIIbβ3. The peptide was patented together with Merck in 1997 (patent application submitted in 15.9.1995, opened in 20.3.1997) [14] and first presented with Merck’s agreement at the European Peptide Symposium in Edinburgh (September 1996) [15]. The synthesis and activity of this molecule was finally published in 1999 [16]. This peptide is now developed by Merck-Serono, (Darmstadt, Germany) under the name “Cilengitide” and has recently entered Phase III clinical trials for treating glioblastoma [17]. …..
The discovery 30 years ago of the RGD motif in Fn was a major breakthrough in science. This tripeptide sequence was also identified in other ECM proteins and was soon described as the most prominent recognition motif involved in cell adhesion. Extensive research in this direction allowed the description of a number of bidirectional proteins, the integrins, which were able to recognize and bind to the RGD sequence. Integrins are key players in the biological function of most cells and therefore the inhibition of RGD-mediated integrin-ECM interactions became an attractive target for the scientific community.
However, the lack of selectivity of linear RGD peptides represented a major pitfall which precluded any clinical application of RGD-based inhibitors. The control of the molecule’s conformation by cyclization and further spatial screening overcame these limitations, showing that it is possible to obtain privileged bioactive structures, which enhance the biological activity of linear peptides and significantly improve their receptor selectivity. Steric control imposed in RGD peptides together with their biological evaluation and extensive structural studies yielded the cyclic peptide c(RGDfV), the first small selective anti-angiogenic molecule described. N-Methylation of this cyclic peptide yielded the much potentc(RGDf(NMe)V), nowadays known as Cilengitide.
The fact that brain tumors, which are highly angiogenic, are more susceptible to the treatment with integrin antagonists, and the positive synergy observed for Cilengitide in combination with radio-chemotherapy in preclinical studies, encouraged subsequent clinical trials. Cilengitide is currently in phase III for GBM patients and in phase II for other types of cancers, with to date a promising therapeutic outcome. In addition, the absence of significant toxicity and excellent tolerance of this drug allows its combination with classical therapies such as RT or cytotoxic agents. The controlled phase III study CENTRIC was launched in 2008, with primary outcome measures due on September 2012. The results of this and other clinical studies are expected with great hope and interest.
Integrins are heterodimeric, transmembrane receptors that function as mechanosensors, adhesion molecules and signal transduction platforms in a multitude of biological processes. As such, integrins are central to the etiology and pathology of many disease states. Therefore, pharmacological inhibition of integrins is of great interest for the treatment and prevention of disease. In the last two decades several integrin-targeted drugs have made their way into clinical use, many others are in clinical trials and still more are showing promise as they advance through preclinical development. Herein, this review examines and evaluates the various drugs and compounds targeting integrins and the disease states in which they are implicated.
Integrins are heterodimeric cell surface receptors found in nearly all metazoan cell types, composed of non-covalently linked α and β subunits. In mammals, eighteen α-subunits and eight β-subunits have been identified to date 1. From this pool, 24 distinct heterodimer combinations have been observed in vivo that confer cell-to-cell and cell-to-ligand specificity relevant to the host cell and the environment in which it functions 2. Integrin-mediated interactions with the extracellular matrix (ECM) are required for the attachment, cytoskeletal organization, mechanosensing, migration, proliferation, differentiation and survival of cells in the context of a multitude of biological processes including fertilization, implantation and embryonic development, immune response, bone resorption and platelet aggregation. Integrins also function in pathological processes such as inflammation, wound healing, angiogenesis, and tumor metastasis. In addition, integrin binding has been identified as a means of viral entry into cells 3. ….
Combination of cilengitide and radiation therapy and temozolomide. The addition of cilengitide to radiotherapy and temozolomide based treatment regimens has shown promising preliminary results in ongoing Phase II trials in both newly diagnosed and progressive glioblastoma multiforme 139–140. In addition to the Phase II objectives sought, these trials are significant in that they represent progress that has made in determining tumor drug uptake and in identifying a subset of patients that may benefit from treatment. In a Phase II trial enrolling 52 patients with newly diagnosed glioblastoma multiforme receiving 500 mg cilengitide twice weekly during radiotherapy and in combination with temozolomide for 6 monthly cycles following radiotherapy, 69% achieved 6 months progression free survival compared to 54 % of patients receiving radiotherapy followed by temozolomide alone. The one-year overall survival was 67 and 62 % of patients for the cilengitide combination group and the radiotherapy and temozolomide group, respectively. Non-hematological grade 3-4 toxcities were limited, and included symptoms of fatigue, asthenia, anorexia, elevated liver function tests, deep vein thrombosis and pulmonary embolism in across a total of 5.7% of the patients. Grade 3-4 hematological malignancies were more common and included lymphopenia (53.8%), thrombocytopenia (13.4%) and neutropenia (9.6%). This trial is significant in the fact that is has provided the first evidence correlating a molecular biomarker with response to treatment. Decreased methylguanine methyltransferase (MGMT) expression was associated with favorable outcome. Patients harboring increased MGMT promoter methylation appeared to benefit more from combined treatment with cilengitide than did patients lacking promoter methylation. The significance of the MGMT promoter methylation in predicting response is likely due to inclusion of temozolomide in the treatment combination.
A similar Phase II study evaluating safety and differences in overall survival among newly diagnosed glioblastoma multiforme patients receiving radiation therapy combined with temozolomide and varying doses of cilengitide is nearing completion. Preliminary reports specify that initial safety run-in studies in 18 patients receiving doses 500, 1000 and 2000 mg cilengitide found no dose limiting toxicities. Subsequently 94 patients were randomized to receive standard therapy plus 500 or 2000 mg cilengitide. Median survival time in both cohorts was 18.9 months. At 12 months the overall survival was 79.5 % (89/112 patients).
In the last two decades great progress has been made in the discovery and development of integrin targeted therapeutics. Years of intense research into integrin function has provided an understanding of the potential applications for the treatment of disease. Advances in structural characterization of integrin-ligand interactions has proved beneficial in the design and development of potent, selective inhibitors for a number of integrins involved in platelet aggregation, inflammatory responses, angiongenesis, neovascularization and tumor growth.
The αIIbβ3 integrin antagonists were the first inhibitors to make their way into clinical use and have proven to be effective and safe drugs, contributing to the reduction of mortality and morbidity associated with acute coronary syndromes. Interestingly, the prolonged administration of small molecules targeting this integrin for long-term prevention of thrombosis related complications have not been successful, for reasons that are not yet fully understood. This suggests that modulating the intensity, duration and temporal aspects of integrin function may be more effective than simply shutting off integrin signaling in some instances. Further research into the dynamics of platelet activation and thrombosis formation may elucidate the mechanisms by which integrin activation is modulated.
The introduction of α4 targeted therapies held great promise for the treatment of inflammatory diseases. The development of Natalizumab greatly improved the quality of life for multiple sclerosis patients and those suffering with Crohn’s Disease compared to previous treatments, but the role in asthma related inflammation could not be validated. Unfortunately for MS and Crohn’s patients, immune surveillance in the central nervous system was also compromised as a direct effect α4β7 antagonism, with potentially lethal effects. Thus Natalizumab and related α4β7 targeting drugs are now limited to patients refractory to standard therapies. The design and development of α4β1 antagonists for the treatment of Crohn’s Disease may offer benefit with decreased risks. The involvement of these integrins in fetal development also raises concerns for widespread clinical use.
Integrin antagonists that target angiogenesis are progressing through clinical trials. Cilengitide has shown promising results for the treatment of glioblastomas and recurrent gliomas, cancers with notoriously low survival and cure rates. The greatest challenge facing the development of anti-angiogenic integrin targeted therapies is the overall lack of biomarkers by which to measure treatment efficacy.
Mapping the ligand-binding pocket of integrin α5β1 using a gain-of-function approach
Integrin α5β1 is a key receptor for the extracellular matrix protein fibronectin. Antagonists of human α5β1 have therapeutic potential as anti-angiogenic agents in cancer and diseases of the eye. However, the structure of the integrin is unsolved and the atomic basis of fibronectin and antagonist binding by α5β1 is poorly understood. Here we demonstrate that zebrafish α5β1 integrins do not interact with human fibronectin or the human α5β1 antagonists JSM6427 and cyclic peptide CRRETAWAC. Zebrafish α5β1 integrins do bind zebrafish fibronectin-1, and mutagenesis of residues on the upper surface and side of the zebrafish α5 subunit β-propeller domain shows that these residues are important for the recognition of RGD and synergy sites in fibronectin. Using a gain-of-function analysis involving swapping regions of the zebrafish α5 subunit with the corresponding regions of human α5 we show that blades 1-4 of the β-propeller are required for human fibronectin recognition, suggesting that fibronectin binding involves a broad interface on the side and upper face of the β-propeller domain. We find that the loop connecting blades 2 and 3 of the β-propeller (D3-A3 loop) contains residues critical for antagonist recognition, with a minor role played by residues in neighbouring loops. A new homology model of human α5β1 supports an important function for D3-A3 loop residues Trp-157 and Ala-158 in the binding of antagonists. These results will aid the development of reagents that block α5β1 functions in vivo.
Structural Basis of Integrin Regulation and Signaling
Integrins are cell adhesion molecules that mediate cell-cell, cell-extracellular matrix, and cellpathogen interactions. They play critical roles for the immune system in leukocyte trafficking and migration, immunological synapse formation, costimulation, and phagocytosis. Integrin adhesiveness can be dynamically regulated through a process termed inside-out signaling. In addition, ligand binding transduces signals from the extracellular domain to the cytoplasm in the classical outside-in direction. Recent structural, biochemical, and biophysical studies have greatly advanced our understanding of the mechanisms of integrin bidirectional signaling across the plasma membrane. Large-scale reorientations of the ectodomain of up to 200 Å couple to conformational change in ligand-binding sites and are linked to changes in α and β subunit transmembrane domain association. In this review, we focus on integrin structure as it relates to affinity modulation, ligand binding, outside-in signaling, and cell surface distribution dynamics.
The immune system relies heavily on integrins for (a) adhesion during leukocyte trafficking from the bloodstream, migration within tissues, immune synapse formation, and phagocytosis; and (b) signaling during costimulation and cell polarization. Integrins are so named because they integrate the extracellular and intracellular environments by binding to ligands outside the cell and cytoskeletal components and signaling molecules inside the cell. Integrins are noncovalently associated heterodimeric cell surface adhesion molecules. In vertebrates, 18 α subunits and 8 β subunits form 24 known αβ pairs (Figure 1). This diversity in subunit composition contributes to diversity in ligand recognition, binding to cytoskeletal components and coupling to downstream signaling pathways. Immune cells express at least 10 members of the integrin family belonging to the β2, β7, and β1 subfamilies (Table 1). The β2 and β7 integrins are exclusively expressed on leukocytes, whereas the β1 integrins are expressed on a wide variety of cells throughout the body. Distribution and ligand-binding properties of the integrins on leukocytes are summarized in Table 1. For reviews, see References 1 and 2. Mutations that block expression of the β2 integrin subfamily lead to leukocyte adhesion deficiency, a disease associated with severe immunodeficiency (3).
As adhesion molecules, integrins are unique in that their adhesiveness can be dynamically regulated through a process termed inside-out signaling or priming. Thus, stimuli received by cell surface receptors for chemokines, cytokines, and foreign antigens initiate intracellular signals that impinge on integrin cytoplasmic domains and alter adhesiveness for extracellular ligands. In addition, ligand binding transduces signals from the extracellular domain to the cytoplasm in the classical outside-in direction (outside-in signaling). These dynamic properties of integrins are central to their proper function in the immune system. Indeed, mutations or small molecules that stabilize either the inactive state or the active adhesive state—and thereby block the adhesive dynamics of leukocyte integrins—inhibit leukocyte migration and normal immune responses.
Novel Discoveries in Molecular Biology and Biomedical Science, Volume 2 (Volume Two: Latest in Genomics Methodologies for Therapeutics: Gene Editing, NGS and BioInformatics, Simulations and the Genome Ontology), Part 1: Next Generation Sequencing (NGS)
Novel Discoveries in Molecular Biology and Biomedical Science
Curator: Larry H. Bernstein, MD, FCAP
UPDATED on 6/1/2016
The following is a collection of current articles on noncoding DNA, synthetic genome engineering, protein regulation of apoptosis, drug design, and geometrics.
No longer ‘junk DNA’ — shedding light on the ‘dark matter’ of the genome
A new tool called “LIGR-Seq” enables scientists to explore in depth what non-coding RNAs actually do in human cells May 23, 2016
he LIGR-seq method for global-scale mapping of RNA-RNA interactions in vivo to reveal unexpected functions for uncharacterized RNAs that act via base-pairing interactions (credit: University of Toronto)
What used to be dismissed by many as “junk DNA” has now become vitally important, as accelerating genomic data points to the importance of non-coding RNAs (ncRNAs) — a genome’s messages that do not specifically code for proteins — in development and disease.
But our progress in understanding these molecules has been slow because of the lack of technologies that allow for systematic mapping of their functions.
Now, professor Benjamin Blencowe’s team at the University of Toronto’s Donnelly Centre has developed a method called “LIGR-seq” that enables scientists to explore in depth what ncRNAs do in human cells.
The study, described in Molecular Cell, was published on May 19, along with two other papers, in Molecular Cell and Cell, respectively, from Yue Wan’s group at the Genome Institute of Singapore and Howard Chang’s group at Stanford University in California, who developed similar methods to study RNAs in different organisms.
Of the 3 billion letters in the human genome, only two per cent make up the protein-coding genes. The genes are copied, or transcribed, into messenger RNA (mRNA) molecules, which provide templates for building proteins that do most of the work in the cell. Much of the remaining 98 per cent of the genome was initially considered by some as lacking in functional importance. However, large swaths of the non-coding genome — between half and three quarters of it — are also copied into RNA.
So then what might the resulting ncRNAs do? That depends on whom you ask. Some researchers believe that most ncRNAs have no function, that they are just a by-product of the genome’s powerful transcription machinery that makes mRNA. However, it is emerging that many ncRNAs do have important roles in gene regulation — some ncRNAs act as carriages for shuttling the mRNAs around the cell, or provide a scaffold for other proteins and RNAs to attach to and do their jobs.
But the majority of available data has trickled in piecemeal or through serendipitous discovery. And with emerging evidence that ncRNAs could drive disease progression, such as cancer metastasis, there was a great need for a technology that would allow a systematic functional analysis of ncRNAs.
“Up until now, with existing methods, you had to know what you are looking for because they all require you to have some information about the RNA of interest. The power of our method is that you don’t need to preselect your candidates; you can see what’s occurring globally in cells, and use that information to look at interesting things we have not seen before and how they are affecting biology,” says Eesha Sharma, a PhD candidate in Blencowe’s group who, along with postdoctoral fellow Tim Sterne-Weiler, co-developed the method.
The human RNA-RNA interactome, showing interactions detected by LIGR-seq (credit: University of Toronto)
The new ‘‘LIGation of interacting RNA and high-throughput sequencing’’ (LIGR-seq) tool captures interactions between different RNA molecules. When two RNA molecules have matching sequences — strings of letters copied from the DNA blueprint — they will stick together like Velcro. With LIGR-seq, the paired RNA structures are removed from cells and analyzed by state-of-the-art sequencing methods to precisely identify the RNAs that are stuck together.
“Most researchers in the life sciences agree that there’s an urgent need to understand what ncRNAs do. This technology will open the door to developing a new understanding of ncRNA function,” says Blencowe, who is also a professor in the Department of Molecular Genetics.
Not having to rely on pre-existing knowledge will boost the discovery of RNA pairs that have never been seen before. Scientists can also, for the first time, look at RNA interactions as they occur in living cells, in all their complexity, unlike in the juices of mashed up cells that they had to rely on before. This is a bit like moving on to explore marine biology from collecting shells on the beach to scuba-diving among the coral reefs, where the scope for discovery is so much bigger.
Actually, ncRNAs come in multiple flavors: there’s rRNA, tRNA, snRNA, snoRNA, piRNA, miRNA, and lncRNA, to name a few, where prefixes reflect the RNA’s place in the cell or some aspect of its function. But the truth is that no one really knows the extent to which these ncRNAs control what goes on in the cell, or how they do this.
Discoveries
Nonetheless, the new technology developed by Blencowe’s group has been able to pick up new interactions involving all classes of RNAs and has already revealed some unexpected findings.
The team discovered new roles for small nucleolar RNAs (snoRNAs), which normally guide chemical modifications of other ncRNAs. It turns out that some snoRNAs can also regulate stability of a set of protein-coding mRNAs. In this way, snoRNAs can also directly influence which proteins are made, as well as their abundance, adding a new level of control in cell biology.
And this is only the tip of the iceberg; the researchers plan to further develop and apply their technology to investigate the ncRNAs in different settings.
“We would like to understand how ncRNAs function during development. We are particularly interested in their role in the formation of neurons. But we will also use our method to discover and map changes in RNA-RNA interactions in the context of human diseases,” says Blencowe.
Abstract of Global Mapping of Human RNA-RNA Interactions
The majority of the human genome is transcribed into non-coding (nc)RNAs that lack known biological functions or else are only partially characterized. Numerous characterized ncRNAs function via base pairing with target RNA sequences to direct their biological activities, which include critical roles in RNA processing, modification, turnover, and translation. To define roles for ncRNAs, we have developed a method enabling the global-scale mapping of RNA-RNA duplexes crosslinked in vivo, “LIGation of interacting RNA followed by high-throughput sequencing” (LIGR-seq). Applying this method in human cells reveals a remarkable landscape of RNA-RNA interactions involving all major classes of ncRNA and mRNA. LIGR-seq data reveal unexpected interactions between small nucleolar (sno)RNAs and mRNAs, including those involving the orphan C/D box snoRNA, SNORD83B, that control steady-state levels of its target mRNAs. LIGR-seq thus represents a powerful approach for illuminating the functions of the myriad of uncharacterized RNAs that act via base-pairing interactions.
Understanding the unknown functions of these genes may lead to the creation of new diagnostic tests for clinical laboratories and anatomic pathology groups
Once again, J. Craig Venter, PhD, is charting new ground in gene sequencing andgenomic science. This time his research team has built upon the first synthetic cell they created in 2010 to build a more sophisticated synthetic cell. Their findings from this work may give pathologists and medical laboratory scientists new tools to diagnose disease.
Recently the research team at the J. Craig Venter Institute (JCVI) and Synthetic Genomics, Inc. (SGI) published their latest findings. Among the things they learned is that science still does not understand the functions of about a third of the genes required for their synthetic cells to function.
JCVI-syn3.0 Could Radically Alter Understanding of Human Genome
Based in La Jolla, Calif., and Rockville, Md., JCVI is a not-for-profit research institute aiming to advance genomics. Building upon its first synthetic cell—Mycoplasma mycoides (M. mycoides) JCVI-syn1.0, which JCVI constructed in 2010—the same team of scientists created the first minimal synthetic bacterial cell, which they calledJCVI-syn3.0. This new artificial cell contains 531,560 base pairs and just 473 genes, which means it is the smallest genome of any organism that can be grown in laboratory media, according to a JCVI-SGI statement.
For pathologists and medical laboratory leaders, the creation of a synthetic life form is a milestone toward better understanding genome sequencing and how this new knowledge may help advance both diagnostics and therapeutics.
“What we’ve done is important because it is a step toward completely understanding how a living cell works,” Clyde Hutchison III, PhD, told New Scientist. “If we can really understand how the cell works, then we will be able to design cells efficiently for the production of pharmaceutical and other useful products.” Hutchison is Professor Emeritus of Microbiology and Immunology at the University of North Carolina at Chapel Hill, Distinguished Professor at the J. Craig Venter Institute, a member of the National Academy of Sciences, and a fellow of the American Academy of Arts and Sciences.
Clyde Hutchison, III, PhD (above), Professor Emeritus of Microbiology and Immunology at the University of North Carolina at Chapel Hill and Distinguished Professor at the J. Craig Venter Institute, stated that his team’s “goal is to have a cell for which the precise biological function of every gene is known.” (Photo credit: JCVI.)
Understanding a Gene’s True Purpose
According to the JCVI researchers, 149 genes have no known purpose. They are, however, necessary for life and health.
“We know about two-thirds of the essential biology, and we’re missing a third,” stated J. Craig Venter, PhD, Founder and CEO of JCVI, in a story published by MedPage Today.
This knowledge is based upon decades of research. JCVI seeks to create a minimal cell operating system to understand biology, while also providing what the JCVI statement called a “chassis for use in industrial applications.”
What Do these Genes Do Anyway?
The JCVI team found that among most genes’ biological functions:
“JCVI-syn3.0 is a working approximation of a minimal cellular genome—a compromise between a small genome size and a workable growth rate for an experimental organism. It retains almost all the genes that are involved in the synthesis and processing of macromolecules. Unexpectedly, it also contains 149 genes with unknown biological functions, suggesting the presence of undiscovered functions that are essential for life,” the researchers told the journal Science.
More research is needed, the scientists say, into the 149 genes that appear to lack specific biologic functions.
Unlocking Mystery of the 149 Genes Could Lead to Advances in Genomic Science
“Finding so many genes without a known function is unsettling, but it’s exciting because it’s left us with much still to learn. It’s like the ‘dark matter’ of biology,” said Alistair Elfick, PhD, Chair of Synthetic Biological Engineering, University of Edinburgh, UK, in the New Scientist article.
Studies such as JCVI’s research is key to broadening understanding and framing appropriate questions about scientific, ethical, and economic implications of synthetic biology.
The creation of a synthetic cell will have a profound and positive impact on understanding of biology and how life works, JCVI said.
Such research may inspire new whole genome synthesis tools and semi-automated processes that could dramatically affect clinical laboratory procedures. It also could lead to new techniques and tools for advanced vaccine and pharmaceuticals, JCVI pointed out.
No single technique has set the molecular biology field ablaze with excitement and potential like the CRISPR-Cas9 genome editing system has following its introduction only a few short years ago. The following articles represent the flexibility of this technique to potentially treat a host of genetic disorders and possibly even prevent the onset of disease.
Scientists recently convened at the CRISPR Precision Gene Editing Congress, held in Boston, to discuss the new technology. As with any new technique, scientists have discovered that CRISPR comes with its own set of challenges, and the Congress focused its discussion around improving specificity, efficiency, and delivery.
With a staggering number of papers published in the past several years involving the characterization and use of the CRISPR/Cas9 gene editing system, it is surprising that researchers are still finding new features of the versatile molecular scissor enzyme.
If a Cas9 nuclease variant could be engineered that was less grabby, it might loosen its grip on DNA sequences throughout the genome—except those sequences representing on-target sites. That’s the assumption that guided a new investigation by researchers at Massachusetts General Hospital.
The gene-editing technology known as CRISPR-Cas9 is starting to raise expectations in the therapeutic realm. In fact, CRISPR-Cas9 and other CRISPR systems are moving so close to therapeutic uses that the technology’s ethical implications are starting to attract notice.
Published: Tuesday, May 24, 2016 A comparison of synthetic gene-activating Cas9 proteins can help guide research and development of therapeutic approaches.
The CRISPR-Cas9 system has come to be known as the quintessential tool that allows researchers to edit the DNA sequences of many organisms and cell types. However, scientists are also increasingly recognizing that it can be used to activate the expression of genes. To that end, they have built a number of synthetic gene activating Cas9 proteins to study gene functions or to compensate for insufficient gene expression in potential therapeutic approaches.
“The possibility to selectively activate genes using various engineered variants of the CRISPR-Cas9 system left many researchers questioning which of the available synthetic activating Cas9 proteins to use for their purposes. The main challenge was that all had been uniquely designed and tested in different settings; there was no side-by-side comparison of their relative potentials,” said George Church, Ph.D., who is Core Faculty Member at the Wyss Institute for Biologically Inspired Engineering at Harvard University, leader of its Synthetic Biology Platform, and Professor of Genetics at Harvard Medical School. “We wanted to provide that side-by-side comparison to the biomedical research community.”
In a study published on 23 May in Nature Methods, the Wyss Institute team reports how it rigorously compared and ranked the most commonly used artificial Cas9 activators in different cell types from organisms including humans, mice and flies. The findings provide a valuable guide to researchers, allowing them to streamline their endeavors.
The team also included Wyss Core Faculty Member James Collins, Ph.D., who also is the Termeer Professor of Medical Engineering & Science and Professor of Biological Engineering at the Massachusetts Institute of Technology (MIT)’s Department of Biological Engineering and Norbert Perrimon, Ph.D., a Professor of Genetics at Harvard Medical School.
Gene activating Cas9 proteins are fused to variable domains borrowed from proteins with well-known gene activation potentials and engineered so that the DNA editing ability is destroyed. In some cases, the second component of the CRISPR-Cas9 system, the guide RNA that targets the complex to specific DNA sequences, also has been engineered to bind gene-activating factors.
“We first surveyed seven advanced Cas9 activators, comparing them to each other and the original Cas9 activator that served to provide proof-of-concept for the gene activation potential of CRISPR-Cas9. Three of them, provided much higher gene activation than the other candidates while maintaining high specificities toward their target genes,” said Marcelle Tuttle, Research Fellow at the Wyss and a co-lead author of the study.
The team went on to show that the three top candidates were comparable in driving the highest level of gene expression in cells from humans, mice and fruit flies, irrespective of their tissue and developmental origins. The researchers also pinpointed ways to further maximize gene activation employing the three leading candidates.
“In some cases, maximum possible activation of a target gene is necessary to achieve a cellular or therapeutic effect. We managed to cooperatively enhance expression of specific genes when we targeted them with three copies of a top performing activator using three different guide RNAs,” said Alejandro Chavez, Ph.D., a Postdoctoral Fellow and the study’s co-first author.
“The ease of use of CRISPR-Cas9 offers enormous potential for development of genome therapeutics. This study provides valuable new design criteria that will help enable synthetic biologists and bioengineers to develop more effective targeted genome engineering technologies in the future,” said Wyss Institute Founding Director Donald Ingber, M.D., Ph.D., who is the Judah Folkman Professor of Vascular Biology at Harvard Medical School and the Vascular Biology Program at Boston Children’s Hospital, and also Professor of Bioengineering at the Harvard John A. Paulson School of Engineering and Applied Sciences.
Engineering T Cells to Functionally Cure HIV-1 Infection
Despite the ability of antiretroviral therapy to minimize human immunodeficiency virus type 1 (HIV-1) replication and increase the duration and quality of patients’ lives, the health consequences and financial burden associated with the lifelong treatment regimen render a permanent cure highly attractive. Although T cells play an important role in controlling virus replication, they are themselves targets of HIV-mediated destruction. Direct genetic manipulation of T cells for adoptive cellular therapies could facilitate a functional cure by generating HIV-1–resistant cells, redirecting HIV-1–specific immune responses, or a combination of the two strategies. In contrast to a vaccine approach, which relies on the production and priming of HIV-1–specific lymphocytes within a patient’s own body, adoptive T-cell therapy provides an opportunity to customize the therapeutic T cells prior to administration. However, at present, it is unclear how to best engineer T cells so that sustained control over HIV-1 replication can be achieved in the absence of antiretrovirals. This review focuses on T-cell gene-engineering and gene-editing strategies that have been performed in efforts to inhibit HIV-1 replication and highlights the requirements for a successful gene therapy–mediated functional cure.
Automated top-down design technique simplifies creation of DNA origami nanostructures
Nanoparticles for drug delivery and cell targeting, nanoscale robots, custom-tailored optical devices, and DNA as a storage medium are among the possible applications
May 27, 2016
The boldfaced line, known as a spanning tree, follows the desired geometric shape of the target DNA origami design method, touching each vertex just once. A spanning tree algorithm is used to map out the proper routing path for the DNA strand. (credit: Public Domain)
MIT, Baylor College of Medicine, and Arizona State University Biodesign Institute researchers have developed a radical new top-down DNA origami* design method based on a computer algorithm that allows for creating designs for DNA nanostructures by simply inputting a target shape.
DNA origami (using DNA to design and build geometric structures) has already proven wildly successful in creating myriad forms in 2- and 3- dimensions, which conveniently self-assemble when the designed DNA sequences are mixed together. The tricky part is preparing the proper DNA sequence and routing design for scaffolding and staple strands to achieve the desired target structure. Typically, this is painstaking work that must be carried out manually.
The new algorithm, which is reported together with a novel synthesis approach in the journal Science, promises to eliminate all that and expands the range of possible applications of DNA origami in biomolecular science and nanotechnology. Think nanoparticles for drug delivery and cell targeting, nanoscale robots in medicine and industry, custom-tailored optical devices, and most interesting: DNA as a storage medium, offering retention times in the millions of years.**
Shape-shifting, top-down software
Unlike traditional DNA origami, in which the structure is built up manually by hand, the team’s radical top-down autonomous design method begins with an outline of the desired form and works backward in stages to define the required DNA sequence that will properly fold to form the finished product.
“The Science paper turns the problem around from one in which an expert designs the DNA needed to synthesize the object, to one in which the object itself is the starting point, with the DNA sequences that are needed automatically defined by the algorithm,” said Mark Bathe, an associate professor of biological engineering at MIT, who led the research. “Our hope is that this automation significantly broadens participation of others in the use of this powerful molecular design paradigm.”
The algorithm, which is known as DAEDALUS (DNA Origami Sequence Design Algorithm for User-defined Structures) after the Greek craftsman and artist who designed labyrinths that resemble origami’s complex scaffold structures, can build any type of 3-D shape, provided it has a closed surface. This can include shapes with one or more holes, such as a torus.
A simplified version of the top-down procedure used to design scaffolded DNA origami nanostructures. It starts with a polygon corresponding to the target shape. Software translates a wireframe version of this structure into a plan for routing DNA scaffold and staple strands. That enables a 3D DNA-based atomic-level structural model that is then validated using 3D cryo-EM reconstruction. (credit: adapted from Biodesign Institute images)
With the new technique, the target geometric structure is first described in terms of a wire mesh made up of polyhedra, with a network of nodes and edges. A DNA scaffold using strands of custom length and sequence is generated, using a “spanning tree” algorithm — basically a map that will automatically guide the routing of the DNA scaffold strand through the entire origami structure, touching each vertex in the geometric form once. Complementary staple strands are then assigned and the final DNA structural model or nanoparticle self-assembles, and is then validated using 3D cryo-EM reconstruction.
The software allows for fabricating a variety of geometric DNA objects, including 35 polyhedral forms (Platonic, Archimedean, Johnson and Catalan solids), six asymmetric structures, and four polyhedra with nonspherical topology, using inverse design principles — no manual base-pair designs needed.
To test the method, simpler forms known as Platonic solids were first fabricated, followed by increasingly complex structures. These included objects with nonspherical topologies and unusual internal details, which had never been experimentally realized before. Further experiments confirmed that the DNA structures produced were potentially suitable for biological applications since they displayed long-term stability in serum and low-salt conditions.
Biological research uses
The research also paves the way for designing nanoscale systems mimicking the properties of viruses, photosynthetic organisms, and other sophisticated products of natural evolution. One such application is a scaffold for viral peptides and proteins for use as vaccines. The surface of the nanoparticles could be designed with any combination of peptides and proteins, located at any desired location on the structure, in order to mimic the way in which a virus appears to the body’s immune system.
The researchers demonstrated that the DNA nanoparticles are stable for more than six hours in serum, and are now attempting to increase their stability further.
The nanoparticles could also be used to encapsulate the CRISPR-Cas9 gene editing tool. The CRISPR-Cas9 tool has enormous potential in therapeutics, thanks to its ability to edit targeted genes. However, there is a significant need to develop techniques to package the tool and deliver it to specific cells within the body, Bathe says.
This is currently done using viruses, but these are limited in the size of package they can carry, restricting their use. The DNA nanoparticles, in contrast, are capable of carrying much larger gene packages and can easily be equipped with molecules that help target the right cells or tissue.
The most exciting aspect of the work, however, is that it should significantly broaden participation in the application of this technology, Bathe says, much like 3-D printing has done for complex 3-D geometric models at the macroscopic scale.
* DNA origami brings the ancient Japanese method of paper folding down to the molecular scale. The basics are simple: Take a length of single-stranded DNA and guide it into a desired shape, fastening the structure together using shorter “staple strands,” which bind in strategic places along the longer length of DNA. The method relies on the fact that DNA’s four nucleotide letters—A, T, C, & G stick together in a consistent manner — As always pairing with Ts and Cs with Gs.
The DNA molecule in its characteristic double stranded form is fairly stiff, compared with single-stranded DNA, which is flexible. For this reason, single stranded DNA makes for an ideal lace-like scaffold material. Further, its pairing properties are predictable and consistent (unlike RNA).
** A single gram of DNA can store about 700 terabytes of information — an amount equivalent to 14,000 50-gigabyte Blu-ray disks — and could potentially be operated with a fraction of the energy required for other information storage options.
Essential role of miRNAs in orchestrating the biology of the tumor microenvironment
MicroRNAs (miRNAs) are emerging as central players in shaping the biology of the Tumor Microenvironment (TME). They do so both by modulating their expression levels within the different cells of the TME and by being shuttled among different cell populations within exosomes and other extracellular vesicles. This review focuses on the state-of-the-art knowledge of the role of miRNAs in the complexity of the TME and highlights limitations and challenges in the field. A better understanding of the mechanisms of action of these fascinating micro molecules will lead to the development of new therapeutic weapons and most importantly, to an improvement in the clinical outcome of cancer patients. Keywords: Exosomes, microRNAs, Tumor microenvironment, Cancer
While cancer treatment and survival have improved worldwide, the need for further understanding of the underlying tumor biology remains. In recent years, there has been a significant shift in scientific focus towards the role of the tumor microenvironment (TME) on the development, growth, and metastatic spread of malignancies. The TME is defined as the surrounding cellular environment enmeshed around the tumor cells including endothelial cells, lymphocytes, macrophages, NK cells, other cells of the immune system, fibroblasts, mesenchymal stem cells (MSCs), and the extracellular matrix (ECM). Each of these components interacts with and influences the tumor cells, continually shifting the balance between pro- and anti-tumor phenotype. One of the predominant methods of communication between these cells is through extracellular vesicles and their microRNA (miRNA) cargo. Extracellular vesicles (EVs) are between 30 nm to a few microns in diameter, are surrounded by a phospholipid bilayer membrane, and are released from a variety of cell types into the local environment. There are three well characterized groups of EVs: 1) exosomes, typically 30–100 nm, 2) microvesicles (or ectosomes), typically 100–1000 nm, and 3) large oncosomes, typically 1–10 μm. Each of these categories has a distinctly unique biogenesis and purpose in cellcell communication despite the fact that current laboratory methods do not always allow precise differentiation. EVs are found to be enriched with membrane-bound proteins, lipid raft-associated and cytosolic proteins, lipids, DNA, mRNAs, and miRNAs, all of which can be transferred to the recipient cell upon fusion to allow cell-cell communications [1]. Of these, miRNAs have been of particular interest in cancer research, both as modifiers of transcription and translation as well as direct inhibitors or enhancers of key regulatory proteins. These miRNAs are a large family of small non-coding RNAs (19–24 nucleotides) and are known to be aberrantly expressed, both in terms of content as well as number, in both the tumor cells and the cells of the TME. Synthesis of these mature miRNA is a complex process, starting with the transcription of long, capped, and polyadenylated pri-miRNA by RNA polymerase II. These are cropped into a 60–100 nucleotide hairpinstructure pre-miRNA by the microprocessor, a heterodimer of Drosha (a ribonuclease III enzyme) and DGCR8 (DiGeorge syndrome critical region gene 8). The premiRNA is then exported to the cytoplasm by exportin 5, cleaved by Dicer, and separated into single strands by helicases. The now mature miRNA are incorporated into the RNA-induced silencing complex (RISC), a cytoplasmic effector machine of the miRNA pathway. The primary mechanism of action of the mature miRNA-RISC complex is through their binding to the 3’ untranslated region, or less commonly the 5’ untranslated region, of target mRNA, leading to protein downregulation either via translational repression or mRNA degradation. More recently, it has been shown that miRNAs can also upregulate the expression of target genes [2]. MiRNA genes are mostly intergenic and are transcribed by independent promoters [3] but can also be encoded by introns, sharing the same promoter of their host gene [4]. MiRNAs undergo the same regulatory mechanisms of any other protein coding gene (promoter methylation, histone modifications, etc.…) [5, 6]. Interestingly, each miRNA may have contradictory effects both within varying tumor cell lines and within different cells of the TME. In this review, we provide a state-of-the-art description of the key role that miRNAs have in the communication between tumor cells and the TME and their subsequent effects on the malignant phenotype. Finally, this review has made every effort to clarify, whenever possible, whether the reference is to the −3p or the -5p miRNA. Whenever such clarification has not been provided, this indicates that it was not possible to infer such information from the cited bibliography.
Angiogenesis and miRNAs Cellular plasticity, critical in the development of malignancy, includes the many diverse mechanisms elicited by cancer cells to increase their malignant potential and develop increasing treatment resistance. One such mechanism, angiogenesis, is critical to the development of metastatic disease, affecting both the growth of malignant cells locally and their survival at distant sites. In the last ten years, miRNAs, often packaged in tumor cell-derived exosomes, have emerged as important contributors to the complicated regulation and balance of pro- and anti-angiogenic factors.
Most commonly, miRNAs derived from cancer cells have oncogenic activity, promoting angiogenesis and tumor growth and survival. The most-well characterized of the pro-angiogenic miRNAs, the miR-17-92 cluster encoding six miRNAs (miR-17, −18a, −19a, −19b, −20a, and −92a), is found on chromosome 13, and is highly conserved among vertebrates [7]. The complex and multifaceted functions of the miR-17-92 cluster are summarized in Fig. 1. Amplification, both at the genetic and RNA level, of miR-17-92 was initially found in several lymphoma cell lines and has subsequently been observed in multiple mouse tumor models [7].
Central role of the miR-17-92 cluster in the biology of the TME. The miR-17-92 cluster encoding miR-17, −18a, −19b, −20a, and -92a is upregulated in multiple tumor types and interacts with various components of the TME to finely “tune” the TME through a complex combination of pro- and anti-tumoral effects
Most commonly, miRNAs derived from cancer cells have oncogenic activity, promoting angiogenesis and tumor growth and survival. The most-well characterized of the pro-angiogenic miRNAs, the miR-17-92 cluster encoding six miRNAs (miR-17, −18a, −19a, −19b, −20a, and −92a), is found on chromosome 13, and is highly conserved among vertebrates [7]. The complex and multifaceted functions of the miR-17-92 cluster are summarized in Fig. 1. Amplification, both at the genetic and RNA level, of miR-17-92 was initially found in several lymphoma cell lines and has subsequently been observed in multiple mouse tumor models [7]. Up-regulation of this particular locus has further been confirmed in miRnome analysis across multiple different tumor types, including lung, breast, stomach, prostate, colon, and pancreatic cancer [8]. The miR-17-92 cluster is directly activated by Myc and modulates a variety of downstream transcription factors important in cell cycle regulation and apoptosis including activation of E2F family and Cyclin-dependent kinase inhibitor (CDKN1A) and downregulation of BCL2L11/BIM and p21 [7]. In addition to promoting cell cycle progression and inhibiting apoptosis, the miR-17-92 cluster also downregulates thrombospondin-1 (Tsp1) and connective tissue growth factor (CTGF), important antiangiogenic proteins [7]. Similarly, microvesicles from colorectal cancer cells contain miR-1246 and TGF-β which are transferred to endothelial cells to silence promyelocytic leukemia protein (PML) and activate Smad 1/5/8 signaling promoting proliferation and migration [9]. Likewise, lung cancer cell line derived microvesicles contain miR-494, in response to hypoxia, which targets PTEN in the endothelial cells promoting angiogenesis through the Akt/eNOS pathway [10]. Lastly, exosomal miR-135b from multiple myeloma cells suppresses the HIF-1/FIH-1 pathway in endothelial cells, increasing angiogenesis [11]. A summary of the studies showing the functions of exosomal miRNAs in shaping the biology of the TME is provided in Table 1.
Table 1
Actions of exosomal miRNAs exchanged between cells of the TME
The most common target of anti-angiogenic therapy is VEGF, and not unsurprisingly, multiple miRNAs (including miR-9, miR-20b, miR-130, miR-150, and miR-497) promote angiogenesis through the induction of the VEGF pathway. The most studied of these is the up-regulation of miR-9 which has been linked to a poor prognosis in multiple tumor types, including breast cancer, non-small cell lung cancer, and melanoma [12]. The two oncogenes MYC and MYCN activate miR-9 and cause E-cadherin downregulation resulting in the upregulated transcription of VEGF [13]. In addition, miR-9 has been shown to upregulate the JAK-STAT pathway, supporting endothelial cell migration and tumor angiogenesis [13]. Both amplification of miR-20b and miR-130 as well as miR-497 suppression regulate VEGF through hypoxia inducible factor 1α (HIF-1α) supporting increased angiogenesis [14, 15, 16, 17]. …..
The pivotal discovery in 2012 by Mitra et al. laid the ground-work for our current knowledge on the interactions between tumor-derived miRNAs and fibroblasts. In combination, the down-regulation of miR-214 and miR-31 and the up-regulation of miR-155 trigger the reprogramming of quiescent fibroblasts to CAFs [32]. As expected, the reverse regulation of these miRNAs reduced the migration and invasion of co-cultured ovarian cancer cells [32]. While the pathway of miR-155’s involvement in CAF biology is still being elucidated, the pathways of miR-214 and miR-31 have been established. In endometrial cancer, miR-31 was found to target the homeobox gene SATB2, leading to enhanced tumor cell migration and invasion [33]. MiR-214 similarly has an inverse correlation with its chemokine target, C-C motif Ligand 5 (CCL5) [32]. CCL5 secretion has been associated with enhanced motility, invasion, and metastatic potential through NF-κB-mediated MMP9 activation and through generation and differentiation of myeloid-derived suppressor cells (MDSCs) [34, 35, 36]. Furthermore, miR-210 and miR-133b overexpression and miR-149 suppression have been subsequently found to independently trigger the conversion to CAFs, possibly through paracrine stimulation, and to additionally promote EMT in prostate and gastric cancer, respectively [37, 38,39]. MiR-210 additionally enlists monocytes and encourages angiogenesis [37]. …
Another function of CAFs is the destruction of the ECM and its remodeling with a tumor-supportive composition and structure which includes modulation of specific integrins and metalloproteinases as some of the most studied miRNA targets. The 23 matrix metalloproteinases (MMPs) are critical in the ECM degradation, disruption of the growth signal balance, resistance to apoptosis, establishment of a favorable metastatic niche, and promotion of angiogenesis [54]. As expected, miRNAs have been found to regulate the actions of MMPs, together working to promote cancer cell growth, invasiveness, and metastasis. In HCC, MMP2 and 9 expression is up-regulated by miR-21 via PTEN pathway downregulation. Similarly, in cholangiocarcinoma it was observed that reduced levels of miR-138 induced up-regulation of RhoC, leading to increased levels of the same two MMPs [55, 56]. ….
As has been shown throughout this review, miRNAs have an important and varied effect on human carcinogenesis by shaping the biology of the TME towards a more permissive pro-tumoral phenotype. The complex events leading to such an outcome are currently quite universally defined as the “educational” process of cancer cells on the surrounding TME. While the initial focus was on the direction from the cancer cell to the surrounding TME, increasingly interest is centered on the implications of a more dynamic bidirectional exchange of genetic information. MiRNAs represent only part of the cargo of the extracellular vesicles, but an increasing scientific literature points towards their pivotal role in creating the micro-environmental conditions for cancer cell growth and dissemination. The nearby future will have to address several questions still unanswered. First, it is absolutely necessary to clarify which miRNAs and to what extent they are involved in this process. The contradictory results of some studies can be explained by the differences in tumor-types and by different concentrations of miRNAs used for functional studies. Understanding whether different concentrations of the same miRNA elicit different target effects and therefore changes the biology of the TME, will represent a significant consideration in the development of this field. It is certainly very attractive (especially in an attempt to develop new and desperately needed better cancer biomarkers) to think that concentrations of miRNAs within the TME are reflected systemically in the circulating levels of that same miRNA, however this has not yet been irrefutably demonstrated. Moreover, the study of the paracrine interactions among different cell populations of the TME and their reciprocal effects has been limited to two, maximum three cell populations. This is still way too far from describing the complexity of the TME and only the development of new tridimensional models of the TME will be able to cast a more conclusive light on such complexity. Finally, the pharmacokinetics of miRNA-containing vesicles is in its infancy at best, and needs to be further developed if the goal is development of new therapies based on the use of exosomic miRNAs. Therefore, the future of miRNA research, particularly in its role in the TME, holds still a lot of questions that need answering. However, for these exact same reasons, this is an incredibly exciting time for research in this field. We can envision a not too far future in which these concerns will be satisfactorily addressed and our understanding of the role of miRNAs within the TME will allow us to use them as new therapeutic weapons to successfully improve the clinical outcome of cancer patients.
Researchers at the Walter and Eliza Hall Institute in Australia have discovered a new way to trigger cell death that could lead to drugs to treat cancer and autoimmune disease.
Programmed cell death (a.k.a. apoptosis) is a natural process that removes unwanted cells from the body. Failure of apoptosis can allow cancer cells to grow unchecked or immune cells to inappropriately attack the body.
The protein known as Bak is central to apoptosis. In healthy cells, Bak sits in an inert state but when a cell receives a signal to die, Bak transforms into a killer protein that destroys the cell.
Triggering the cancer-apoptosis trigger
Institute researchers Sweta Iyer, PhD, Ruth Kluck, PhD, and colleagues unexpectedly discovered that an antibody they had produced to study Bak actually bound to the Bak protein and triggered its activation. They hope to use this discovery to develop drugs that promote cell death.
The researchers used information about Bak’s three-dimensional structure to find out precisely how the antibody activated Bak. “It is well known that Bak can be activated by a class of proteins called ‘BH3-only proteins’ that bind to a groove on Bak. We were surprised to find that despite our antibody binding to a completely different site on Bak, it could still trigger activation,” Kluck said. “The advantage of our antibody is that it can’t be ‘mopped up’ and neutralized by pro-survival proteins in the cell, potentially reducing the chance of drug resistance occurring.”
Drugs that target this new activation site could be useful in combination with other therapies that promote cell death by mimicking the BH3-only proteins. The researchers are now working with collaborators to develop their antibody into a drug that can access Bak inside cells.
Their findings have just been published in the open-access journal Nature Communications. The research was supported by the National Health and Medical Research Council, the Australian Research Council, the Victorian State Government Operational Infrastructure Support Scheme, and the Victorian Life Science Computation Initiative.
Abstract of Identification of an activation site in Bak and mitochondrial Bax triggered by antibodies
During apoptosis, Bak and Bax are activated by BH3-only proteins binding to the α2–α5 hydrophobic groove; Bax is also activated via a rear pocket. Here we report that antibodies can directly activate Bak and mitochondrial Bax by binding to the α1–α2 loop. A monoclonal antibody (clone 7D10) binds close to α1 in non-activated Bak to induce conformational change, oligomerization, and cytochrome c release. Anti-FLAG antibodies also activate Bak containing a FLAG epitope close to α1. An antibody (clone 3C10) to the Bax α1–α2 loop activates mitochondrial Bax, but blocks translocation of cytosolic Bax. Tethers within Bak show that 7D10 binding directly extricates α1; a structural model of the 7D10 Fab bound to Bak reveals the formation of a cavity under α1. Our identification of the α1–α2 loop as an activation site in Bak paves the way to develop intrabodies or small molecules that directly and selectively regulate these proteins.
“Cure” is a word that’s dominated the rhetoric in the war on cancer for decades. But it’s a word that medical professionals tend to avoid. While the American Cancer Society reports that cancer treatment has improved markedly over the decades and the five-year survival rate is impressively high for many cancers, oncologists still refrain from declaring their cancer-free patients cured. Why?
Patients are declared cancer-free (also called complete remission) when there are no more signs of detectable disease.
However, minuscule clusters of cancer cells below the detection level can remain in a patient’s body after treatment. Moreover, such small clusters of straggler cells may undergo metastasis, where they escape from the initial tumor into the bloodstream and ultimately settle in a distant site, often a vital organ such as the lungs, liver or brain.
When a colony of these metastatic cells reaches a detectable size, the patient is diagnosed with recurrent metastatic cancer. About one in three breast cancer patients diagnosed with early-stage cancer later develop metastatic disease, usually within five years of initial remission.
By the time metastatic cancer becomes evident, it is much more difficult to treat than when it was originally diagnosed.
What if these metastatic cells could be detected earlier, before they established a “foothold” in a vital organ? Better yet, could these metastatic cancer cells be intercepted, preventing them them from lodging in a vital organ in the first place?
The implant is a tiny porous polymer disc (basically a miniature sponge, no larger than a pencil eraser) that can be inserted just under a patient’s skin. Implantation triggers the immune system’s “foreign body response,” and the implant starts to soak up immune cells that travel to it. If the implant can catch mobile immune cells, then why not mobile metastatic cancer cells?
We gave implants to mice specially bred to model metastatic breast cancer. When the mice had palpable tumors but no evidence of metastatic disease, the implant was removed and analyzed.
Cancer cells were indeed present in the implant, while the other organs (potential destinations for metastatic cells) still appeared clean. This means that the implant can be used to spot previously undetectable metastatic cancer before it takes hold in an organ.
For patients with cancer in remission, an implant that can detect tumor cells as they move through the body would be a diagnostic breakthrough. But having to remove it to see if it has captured any cancer cells is not the most convenient or pleasant detection method for human patients.
Detecting cancer cells with noninvasive imaging
There could be a way around this, though: a special imaging method under development at Northwestern University called Inverse Spectroscopic Optical Coherence Tomography (ISOCT). ISOCT detects molecular-level differences in the way cells in the body scatter light. And when we scan our implant with ISOCT, the light scatter pattern looks different when it’s full of normal cells than when cancer cells are present. In fact, the difference is apparent when even as few as 15 out of the hundreds of thousands of cells in the implant are cancer cells.
There’s a catch – ISOCT cannot penetrate deep into tissue. That means it is not a suitable imaging technology for finding metastatic cells buried deep in internal organs. However, when the cancer cell detection implant is located just under the skin, it may be possible to detect cancer cells trapped in it using ISOCT. This could offer an early warning sign that metastatic cells are on the move.
This early warning could prompt doctors to monitor their patients more closely or perform additional tests. Conversely, if no cells are detected in the implant, a patient still in remission could be spared from unneeded tests.
The ISOCT results show that noninvasive imaging of the implant is feasible. But it’s a method still under development, and thus it’s not widely available. To make scanning easier and more accessible, we’re working to adapt more ubiquitous imaging technologies like ultrasound to detect tiny quantities of tumor cells in the implant.
Besides providing a way to detect tiny numbers of cancer cells before they can form new tumors in other parts of the body, our implant offers an even more intriguing possibility: diverting metastatic cells away from vital organs, and sequestering them where they cannot cause any damage.
In our mouse studies, we found that metastatic cells got caught in the implant before they were apparent in vital organs. When metastatic cells eventually made their way into the organs, the mice with implants still had significantly fewer tumor cells in their organs than implant-free controls. Thus, the implant appears to provide a therapeutic benefit, most likely by taking the metastatic cells it catches out of the circulation, preventing them from lodging anywhere vital.
Interestingly, we have not seen cancer cells leave the implant once trapped, or form a secondary tumor in the implant. Ongoing work aims to learn why this is. Whether the cells can stay safely immobilized in the implant or if it would need to be removed periodically will be important questions to answer before the implant could be used in human patients.
What the future may hold
For now, our work aims to make the implant more effective at drawing and detecting cancer cells. Since we tested the implant with metastatic breast cancer cells, we also want to see if it will work on other types of cancer. Additionally, we’re studying the cells the implant traps, and learning how the implant interacts with the body as a whole. This basic research should give us insight into the process of metastasis and how to treat it.
In the future (and it might still be far off), we envision a world where recovering cancer patients can receive a detector implant to stand guard for disease recurrence and prevent it from happening. Perhaps the patient could even scan their implant at home with a smartphone and get treatment early, when the disease burden is low and the available therapies may be more effective. Better yet, perhaps the implant could continually divert all the cancer cells away from vital organs on its own, like Iron Man’s electromagnet that deflects shrapnel from his heart.
This solution is still not a “cure.” But it would transform a formidable disease that one out of three cancer survivors would otherwise ultimately die from into a condition with which they could easily live.
New PSA Test Examines Protein Structures to Detect Prostate Cancers
5/16/2016 by Cleveland Clinic
A promising new test is detecting prostate cancer more precisely than current tests, by identifying molecular changes in the prostate specific antigen (PSA) protein, according to Cleveland Clinic research presented today at the American Urological Association annual meeting.
The study – part of an ongoing multicenter prospective clinical trial – found that the IsoPSATM test can also differentiate between high-risk and low-risk disease, as well as benign conditions.
Although widely used, the current PSA test relies on detection strategies that have poor specificity for cancer – just 25 percent of men who have a prostate biopsy due to an elevated PSA level actually have prostate cancer, according to the National Cancer Institute – and an inability to determine the aggressiveness of the disease.
The IsoPSA test, however, identifies prostate cancer in a new way. Developed by Cleveland Clinic, in collaboration with Cleveland Diagnostics, Inc., IsoPSA identifies the molecular structural changes in protein biomarkers. It is able to detect cancer by identifying these structural changes, as opposed to current tests that simply measure the protein’s concentration in a patient’s blood.
“While the PSA test has undoubtedly been one of the most successful biomarkers in history, its limitations are well known. Even currently available prostate cancer diagnostic tests rely on biomarkers that can be affected by physiological factors unrelated to cancer,” said Eric Klein, M.D., chair of Cleveland Clinic’s Glickman Urological & Kidney Institute. “These study results show that using structural changes in PSA protein to detect cancer is more effective and can help prevent unneeded biopsies in low-risk patients.”
The clinical trial involves six healthcare institutions and 132 patients, to date. It examined the ability of IsoPSA to distinguish patients with and without biopsy-confirmed evidence of cancer. It also evaluated the test’s precision in differentiating patients with high-grade (Gleason = 7) cancer from those with low-grade (Gleason = 6) disease and benign findings after standard ultrasound-guided biopsy of the prostate.
Substituting the IsoPSA structure-based composite index for the standard PSA resulted in improvement in diagnostic accuracy. Compared with serum PSA testing, IsoPSA performed better in both sensitivity and specificity.
“We took an ‘out of the box’ approach that has shown success in detecting prostate cancer but also has the potential to address other clinically important questions such as clinical surveillance of patients after treatment,” said Mark Stovsky, M.D., staff member, Cleveland Clinic Glickman Urological & Kidney Institute’s Department of Urology. Stovsky has a leadership position (Chief Medical Officer) and investment interest in Cleveland Diagnostics, Inc. “In general, the clinical utility of prostate cancer early detection and screening tests is often limited by the fact that biomarker concentrations may be affected by physiological processes unrelated to cancer, such as inflammation, as well as the relative lack of specificity of these biomarkers to the cancer phenotype. In contrast, clinical research data suggests that the IsoPSA assay can interrogate the entire PSA isoform distribution as a single stand-alone diagnostic tool which can reliably identify structural changes in the PSA protein that correlate with the presence or absence and aggressiveness of prostate cancer.”
Point of Care, Highly Accurate Cervical Cancer Screening
Fifty-five million times a year, American women go to their gynecologist for a Pap Smear. After waiting a few weeks for the results, more than 3.5 million of them are called back to the physician for a follow up visualization of the cervix. Beyond the stress related to possibly having cancer, the women are then subjected to a colposcopic exam, and all too often, a painful biopsy. Then more stressful waiting for a final diagnosis from the pathologist.
Cervical cancer develops slowly, allowing for successful treatment, when identified on time. Regions with high screening compliancy have low mortality rates from this cancer. In the US, for instance, where screening rates are close to 90%, only 4,200 women die from cervical cancer, annually, or 2.6 women per 100,000. However, the screening process in the developed world is long, complicated and not optimized.
In developing regions however, cervical cancer is a leading cause of women death. Over 85% of the total deaths from this cancer are in developing countries. Regions suffering from low screening rates include not only Africa, India and China, but many Eastern European countries as well. According to an OECD report from 2014, the cervical cancer screening rates in Romania and Hungary are as low as 14.6% and 36.7% respectively. The mortality rates in these countries are high, 16 in 100,000 women in Romania and 7.7 in 100,000 in Hungary.
The current screening process for cervical cancer detection is long, beginning with a Pap or HPV test. Cytology results take weeks to receive. A positive result requires follow-up testing by colposcopy and often biopsy. In countries where there is little access to medical care, or where screening compliancy is low, the chances of successful detection via this multi-step process are small. Developing regions and non-compliant countries require a point of care diagnostic method, which eliminates the need for return visits.
Additional limitations to cervical cancer screening are the low sensitivity and specificity rates of Pap tests and the high false positive rates of HPV test, leading to unnecessary colposcopies. Both cytology and colposcopy testing are highly dependent on operator proficiency for accurate diagnosis.
Biop has developed a new technology for the optimization of this process, into one, three minute, painless optical scan. The vaginal probe uses advanced optical, imaging and non-imaging technologies to identify and classify epithelium based cancers and pre-cancerous lesions. The probe is inserted into the vaginal canal, and scans the entire cervix. The resulting images and optical signatures created from the light, and captured by the sensors, are analyzed by the proprietary algorithm. The result is two pictures, on the physician’s screen; a high resolution photograph of the patient’s cervix, immediately next to a hot/cold map indicating a precise classification and location of any diseased lesions.
Deep learning applied to drug discovery and repurposing
Deep neural networks for drug discovery (credit: Insilico Medicine, Inc.)
Scientists from Insilico Medicine, Inc. have trained deep neural networks (DNNs) to predict the potential therapeutic uses of 678 drugs, using gene-expression data obtained from high-throughput experiments on human cell lines from Broad Institute’s LINCS databases and NIH MeSH databases.
The supervised deep-learning drug-discovery engine used the properties of small molecules, transcriptional data, and literature to predict efficacy, toxicity, tissue-specificity, and heterogeneity of response.
“We used LINCS data from Broad Institute to determine the effects on cell lines before and after incubation with compounds, co-author and research scientist Polina Mamoshina explained to KurzweilIAI.
“We used gene expression data of total mRNA from cell lines extracted and measured before incubation with compound X and after incubation with compound X to identify the response on a molecular level. The goal is to understand how gene expression (the transcriptome) will change after drug uptake. It is a differential value, so we need a reference (molecular state before incubation) to compare.”
The research is described in a paper in the upcoming issue of the journal Molecular Pharmaceutics.
Helping pharmas accelerate R&D
Alex Zhavoronkov, PhD, Insilico Medicine CEO, who coordinated the study, said the initial goal of their research was to help pharmaceutical companies significantly accelerate their R&D and increase the number of approved drugs. “In the process we came up with more than 800 strong hypotheses in oncology, cardiovascular, metabolic, and CNS spaces and started basic validation,” he said.
The team measured the “differential signaling pathway activation score for a large number of pathways to reduce the dimensionality of the data while retaining biological relevance.” They then used those scores to train the deep neural networks.*
“This study is a proof of concept that DNNs can be used to annotate drugs using transcriptional response signatures, but we took this concept to the next level,” said Alex Aliper, president of research, Insilico Medicine, Inc., lead author of the study.
Via Pharma.AI, a newly formed subsidiary of Insilico Medicine, “we developed a pipeline for in silico drug discovery — which has the potential to substantially accelerate the preclinical stage for almost any therapeutic — and came up with a broad list of predictions, with multiple in silico validation steps that, if validated in vitro and in vivo, can almost double the number of drugs in clinical practice.”
Despite the commercial orientation of the companies, the authors agreed not to file for intellectual property on these methods and to publish the proof of concept.
Deep-learning age biomarkers
According to Mamoshina, earlier this month, Insilico Medicine scientists published the first deep-learned biomarker of human age — aiming to predict the health status of the patient — in a paper titled “Deep biomarkers of human aging: Application of deep neural networks to biomarker development” by Putin et al, in Aging; and an overview of recent advances in deep learning in a paper titled “Applications of Deep Learning in Biomedicine” by Mamoshina et al., also in Molecular Pharmaceutics.
Insilico Medicine is located in the Emerging Technology Centers at Johns Hopkins University in Baltimore, Maryland, in collaboration with Datalytic Solutions and Mind Research Network.
* In this study, scientists used the perturbation samples of 678 drugs across A549, MCF-7 and PC-3 cell lines from the Library of Integrated Network-Based Cellular Signatures (LINCS) project developed by the National Institutes of Health (NIH) and linked those to 12 therapeutic use categories derived from MeSH (Medical Subject Headings) developed and maintained by the National Library of Medicine (NLM) of the NIH.
To train the DNN, scientists utilized both gene level transcriptomic data and transcriptomic data processed using a pathway activation scoring algorithm, for a pooled dataset of samples perturbed with different concentrations of the drug for 6 and 24 hours. Cross-validation experiments showed that DNNs achieve 54.6% accuracy in correctly predicting one out of 12 therapeutic classes for each drug.
One peculiar finding of this experiment was that a large number of drugs misclassified by the DNNs had dual use, suggesting possible application of DNN confusion matrices in drug repurposing. FutureTechnologies Media Group | Video presentation Insilico medicine
Abstract of Deep learning applications for predicting pharmacological properties of drugs and drug repurposing using transcriptomic data
Deep learning is rapidly advancing many areas of science and technology with multiple success stories in image, text, voice and video recognition, robotics and autonomous driving. In this paper we demonstrate how deep neural networks (DNN) trained on large transcriptional response data sets can classify various drugs to therapeutic categories solely based on their transcriptional profiles. We used the perturbation samples of 678 drugs across A549, MCF-7 and PC-3 cell lines from the LINCS project and linked those to 12 therapeutic use categories derived from MeSH. To train the DNN, we utilized both gene level transcriptomic data and transcriptomic data processed using a pathway activation scoring algorithm, for a pooled dataset of samples perturbed with different concentrations of the drug for 6 and 24 hours. When applied to normalized gene expression data for “landmark genes,” DNN showed cross-validation mean F1 scores of 0.397, 0.285 and 0.234 on 3-, 5- and 12-category classification problems, respectively. At the pathway level DNN performed best with cross-validation mean F1 scores of 0.701, 0.596 and 0.546 on the same tasks. In both gene and pathway level classification, DNN convincingly outperformed support vector machine (SVM) model on every multiclass classification problem. For the first time we demonstrate a deep learning neural net trained on transcriptomic data to recognize pharmacological properties of multiple drugs across different biological systems and conditions. We also propose using deep neural net confusion matrices for drug repositioning. This work is a proof of principle for applying deep learning to drug discovery and development.
A novel nanoscale organic transistor-based biosensor that can detect molecules associated with neurodegenerative diseases and some types of cancer has been developed by researchers at the National Nanotechnology Laboratory (LNNano) in Brazil.
The transistor, mounted on a glass slide, contains the reduced form of the peptide glutathione (GSH), which reacts in a specific way when it comes into contact with the enzyme glutathione S-transferase (GST), linked to Parkinson’s, Alzheimer’s and breast cancer, among other diseases.
Sensitive water-gated copper phthalocyanine (CuPc) thin-film transistor (credit: Rafael Furlan de Oliveira et al./Organic Electronics)
“The device can detect such molecules even when they’re present at very low levels in the examined material, thanks to its nanometric sensitivity,” explained Carlos Cesar Bof Bufon, Head of LNNano’s Functional Devices & Systems Lab (DSF).
Bufon said the system can be adapted to detect other substances by replacing the analytes (detection compounds). The team is working on paper-based biosensors to further lower the cost, improve portability, and facilitate fabrication and disposal.
The research is published in the journal Organic Electronics.
Abstract of Water-gated phthalocyanine transistors: Operation and transduction of the peptide–enzyme interaction
The use of aqueous solutions as the gate medium is an attractive strategy to obtain high charge carrier density (1012 cm−2) and low operational voltages (<1 V) in organic transistors. Additionally, it provides a simple and favorable architecture to couple both ionic and electronic domains in a single device, which is crucial for the development of novel technologies in bioelectronics. Here, we demonstrate the operation of transistors containing copper phthalocyanine (CuPc) thin-films gated with water and discuss the charge dynamics at the CuPc/water interface. Without the need for complex multilayer patterning, or the use of surface treatments, water-gated CuPc transistors exhibited low threshold (100 ± 20 mV) and working voltages (<1 V) compared to conventional CuPc transistors, along with similar charge carrier mobilities (1.2 ± 0.2) x 10−3 cm2 V−1 s−1. Several device characteristics such as moderate switching speeds and hysteresis, associated with high capacitances at low frequencies upon bias application (3.4–12 μF cm−2), indicate the occurrence of interfacial ion doping. Finally, water-gated CuPc OTFTs were employed in the transduction of the biospecific interaction between tripeptide reduced glutathione (GSH) and glutathione S-transferase (GST) enzyme, taking advantage of the device sensitivity and multiparametricity.
The study offers understanding of potential therapeutic targets.
Building on data from The Cancer Genome Atlas (TCGA) project, a multi-institutional team of scientists have completed the first large-scale “proteogenomic” study of breast cancer, linking DNA mutations to protein signaling and helping pinpoint the genes that drive cancer. Conducted by members of the National Cancer Institute’s Clinical Proteomic Tumor Analysis Consortium (CPTAC), including Baylor College of Medicine, Broad Institute of MIT and Harvard, Fred Hutchinson Cancer Research Center, New York University Langone Medical Center, and Washington University School of Medicine, the study takes aim at proteins, the workhorses of the cell, and their modifications to better understand cancer.
Appearing in the Advance Online Publication of Nature, the study illustrates the power of integrating genomic and proteomic data to yield a more complete picture of cancer biology than either analysis could do alone. The effort produced a broad overview of the landscape of the proteome (all the proteins found in a cell) and the phosphoproteome (the sites at which proteins are tagged by phosphorylation, a chemical modification that drives communication in the cell) across a set of 77 breast cancer tumors that had been genomically characterized in the TCGA project. Although the TCGA produced an extensive catalog of somatic mutations found in cancer, the effects of many of those mutations on cellular functions or patients’ outcomes are unknown.
In addition, not all mutated genes are true “drivers” of cancer — some are merely “passenger” mutations that have little functional consequence. And some mutations are found within very large DNA regions that are deleted or present in extra copies, so winnowing the list of candidate genes by studying the activity of their protein products can help identify therapeutic targets. “We don’t fully understand how complex cancer genomes translate into the driving biology that causes relapse and mortality,” said Matthew Ellis, director of the Lester and Sue Smith Breast Center at Baylor College of Medicine and a senior author of the paper.
“These findings show that proteogenomic integration could one day prove to be a powerful clinical tool, allowing us to traverse the large knowledge gap between cancer genomics and clinical action.” In this study, the researchers at the Broad Institute analyzed breast tumors using accurate mass, high-resolution mass spectrometry, a technology that extends the coverage of the proteome far beyond the coverage that can be achieved by traditional antibody-based methods. This allowed them to scale their efforts and quantify more than 12,000 proteins and 33,000 phosphosites, an extremely deep level of coverage.
Scripps scientists have designed a drug candidate that decreases growth of breast cancer cells.
In a development that could lead to a new generation of drugs to precisely treat a range of diseases, scientists from the Florida campus of The Scripps Research Institute (TSRI) have for the first time designed a drug candidate that decreases the growth of tumor cells in animal models in one of the hardest to treat cancers—triple negative breast cancer.
“This is the first example of taking a genetic sequence and designing a drug candidate that works effectively in an animal model against triple negative breast cancer,” said TSRI Professor Matthew Disney. “The study represents a clear breakthrough in precision medicine, as this molecule only kills the cancer cells that express the cancer-causing gene—not healthy cells. These studies may transform the way the lead drugs are identified—by using the genetic makeup of a disease.”
The study, published by the journal Proceedings of the National Academy of Sciences, demonstrates that the Disney lab’s compound, known as Targaprimir-96, triggers breast cancer cells to kill themselves via programmed cell death by precisely targeting a specific RNA that ignites the cancer.
Short-Cut to Drug Candidates
While the goal of precision medicine is to identify drugs that selectively affect disease-causing biomolecules, the process has typically involved time-consuming and expensive high-throughput screens to test millions of potential drug candidates to identify those few that affect the target of interest. Disney’s approach eliminates these screens.
The new study uses the lab’s computational approach called Inforna, which focuses on developing designer compounds that bind to RNA folds, particularly microRNAs.
MicroRNAs are short molecules that work within all animal and plant cells, typically functioning as a “dimmer switch” for one or more genes, binding to the transcripts of those genes and preventing protein production. Some microRNAs have been associated with diseases. For example, microRNA-96, which was the target of the new study, promotes cancer by discouraging programmed cell death, which can rid the body of cells that grow out of control.
In the new study, the drug candidate was tested in animal models over a 21-day course of treatment. Results showed decreased production of microRNA-96 and increased programmed cell death, significantly reducing tumor growth. Since targaprimir-96 was highly selective in its targeting, healthy cells were unaffected.
In contrast, Disney noted, a typical cancer therapeutic targets and kills cells indiscriminately, often leading to side effects that can make these drugs difficult for patients to tolerate.
Benjamin Zealley and Aubrey D.N.J. de Grey Commentary on Some Recent Theses Relevant to Combating Aging: June 2015
Cancer Autoantibody Biomarker Discovery and Validation Using Nucleic Acid Programmable Protein Array Jie Wang, PhD, Arizona State University
Currently in the United States, many patients with cancer do not benefit from population-based screening due to challenges associated with the existing cancer screening scheme. Blood-based diagnostic assays have the potential to detect diseases in a non-invasive way. Proteins released from small early tumors may only be present intermittently and are diluted to tiny concentrations in the blood, making them difficult to use as biomarkers. However, they can induce autoantibody (AAb) responses, which can amplify the signal and persist in the blood even if the antigen is gone. Circulating autoantibodies are a promising class of molecules that have the potential to serve as early detection biomarkers for cancers. This PhD thesis aims to screen for autoantibody biomarkers for the early detection of two deadly cancers, basal-like breast cancer and lung adenocarcinoma. First, a method was developed to display proteins in both native and denatured conformations on a protein array. This method adopted a novel protein tag technology, called a HaloTag, to immobilize proteins covalently on the surface of a glass slide. The covalent attachment allowed these proteins to endure harsh treatment without becoming dissociated from the slide surface, which enabled the profiling of antibody responses against both conformational and linear epitopes. Next, a plasma screening protocol was optimized to increase significantly the signal-to-noise ratio of protein array–based AAb detection. Following this, the AAb responses in basal-like breast cancer were explored using nucleic acid programmable protein arrays (NAPPA) containing 10,000 full-length human proteins in 45 cases and 45 controls. After verification in a large sample set (145 basal-like breast cancer cases, 145 controls, 70 non-basal breast cancer) by enzyme-linked immunosorbent assay (ELISA), a 13-AAb classifier was developed to differentiate patients from controls with a sensitivity of 33% at 98% specificity. A similar approach was also applied to the lung cancer study to identify AAbs that distinguished lung cancer patients from computed tomography–positive benign pulmonary nodules (137 lung cancer cases, 127 smoker controls, 170 benign controls). In this study, two panels of AAbs were discovered that showed promising sensitivity and specificity. Six out of eight AAb targets were also found to have elevated mRNA levels in lung adenocarcinoma patients using TCGA data. These projects as a whole provide novel insights into the association between AAbs and cancer, as well as general B cell antigenicity against self-proteins.
Comment: There are two widely supported models for cancer development and progression—the clonal evolution (CE) model and the cancer stem cell (CSC) model. Briefly, the former claims that most or all cells in a tumor contribute to its maintenance; as newer and more aggressive clones develop by random mutation, they become responsible for driving growth. The range of different mutational profiles generated is assumed to be large enough to account for disease recurrence after therapy (due to rare resistant clones) and metastasis (clones arising with the ability to travel to distant sites). The CSC model instead asserts that a small number of mutated stem cells are the origin of the primary cell mass, drive metastasis through the intermittent release of undifferentiated, highly mobile progeny, and account for recurrence due to a generally quiescent metabolic profile conferring potent resistance to chemotherapy. In either case, the immunological visibility of an early tumor may be highly sporadic. Clones arising early in CE differ little in proteomic terms from healthy host cells; those that do trigger a response are unlikely to have acquired robust resistance to immune attack, so are destroyed quickly in favor of their stealthier brethren. Likewise, CSCs share some of the immune privilege of normal stem cells and, due to their inherent ability to produce differentiated progeny with distinct proteomic signatures, are partially protected from attacks on their descendants. Consequently, such well-hidden cells may remain in the body for years to decades. The autoantibody panel developed in this study for basal-like breast cancer exhibits exceptional specificity despite a comparatively small training set. Given its ease of application, this suggests great promise for a more exhaustively trained classifier as a populationlevel screening tool.
Condition-Specific Differential Sub-Network Analysis for Biological Systems Deepali Jhamb, PhD, Indiana University
Biological systems behave differently under different conditions. Advances in sequencing technology over the last decade have led to the generation of enormous amounts of condition-specific data. However, these measurements often fail to identify low-abundance genes and proteins that can be biologically crucial. In this work, a novel textmining system was first developed to extract condition-specific proteins from the biomedical literature. The literaturederived data was then combined with proteomics data to construct condition-specific protein interaction networks. Furthermore, an innovative condition-specific differential analysis approach was designed to identify key differences, in the form of sub-networks, between any two given biological systems. The framework developed here was implemented to understand the differences between limb regenerationcompetent Ambystoma mexicanum and regeneration-deficient Xenopus laevis. This study provides an exhaustive systems-level analysis to compare regeneration competent and deficient sub-networks to show how different molecular entities inter-connect with each other and are rewired during the formation of an accumulation blastema in regenerating axolotl limbs. This study also demonstrates the importance of literature-derived knowledge, specific to limb regeneration, to augment the systems biology analysis. Our findings show that although the proteins might be common between the two given biological conditions, they can have a high dissimilarity based on their biological and topological properties in the sub-network. The knowledge gained from the distinguishing features of limb regeneration in amphibians can be used in future to induce regeneration chemically in mammalian systems. The approach developed in this dissertation is scalable and adaptable to understanding differential sub-networks between any two biological systems. This methodology will not only facilitate the understanding of biological processes and molecular functions that govern a given system, but will also provide novel intuitions about the pathophysiology of diseases/conditions.
Comment: We have long advocated a principle of directly comparing young and old bodies as a means to identify the classes of physical damage that accumulate in the body during aging. This approach circumvents our ignorance of the full etiology of each particular disease manifestation, a phenomenally difficult question given the ethical issues of experimenting on human subjects, the lengthy ‘‘incubation time’’ of aging-related diseases, and the complex interconnections between their risk factors—innate and environmental. Repairing such damage has the potential to prevent pathology before symptoms appear, an approach now becoming increasingly mainstream.11 However, a naı¨ve comparison faces a number of difficulties, even given a sufficiently large sample set to compensate for inter-individual variation. Most importantly, the causal significance of a given species cannot be reliably determined from its simple prevalence.12 The catalytic nature of cell biology means that those entities whose abundance changes the most profoundly in absolute terms are quite unlikely to be the drivers of that change and may even spontaneously revert to baseline levels in the absence of on-going stimulation. Meanwhile, functionality is often heavily influenced independently of abundance by post-translational modifications that may escape direct detection. Sub-network analysis uses computational means to identify groups of genes and/or proteins that vary in a synchronized way with some parameter, indicating functional connectivity. The application of methods such as those developed here to the comparison of a wide range of younger and older conditions will facilitate the identification of processes—not merely individual factors—that are impaired with age, and thus will help greatly in identifying the optimal points for intervention.
Development of a Light Actuated Drug Delivery-on-Demand System Chase Linsley, PhD, University of California, Los Angeles
The need for temporal–spatial control over the release of biologically active molecules has motivated efforts to engineer novel drug delivery-on-demand strategies actuated via light irradiation. Many systems, however, have been limited to in vitro proof-of-concept due to biocompatibility issues with the photo-responsive moieties or the light wavelength, intensity, and duration. To overcome these limitations, the objective of this dissertation was to design a light-actuated drug delivery-on-demand strategy that uses biocompatible chromophores and safe wavelengths of light, thereby advancing the clinical prospects of light-actuated drug delivery-on-demand systems. This was achieved by: (1) Characterizing the photothermal response of biocompatible visible light and near-infrared-responsive chromophores and demonstrating the feasibility and functionality of the light actuated on-demand drug delivery system in vitro; and (2) designing a modular drug delivery-on-demand system that could control the release of biologically active molecules over an extended period of time. Three biocompatible chromophores—Cardiogreen, Methylene Blue, and riboflavin—were identified and demonstrated significant photothermal response upon exposure to near-infrared and visible light, and the amount of temperature change was dependent upon light intensity, wavelength, as well as chromophore concentration. As a proof-of-concept, pulsatile release of a model protein from a thermally responsive delivery vehicle fabricated from poly(N-isopropylacrylamide) was achieved over 4 days by loading the delivery vehicle with Cardiogreen and irradiating with near-infrared light. To extend the useful lifetime of the light-actuated drug delivery-on-demand system, a modular, reservoir-valve system was designed. Using poly(ethylene glycol) as a reservoir for model small molecule drugs combined with a poly(N-isopropylacrylamide) valve spiked with chromophore-loaded liposomes, pulsatile release was achieved over 7 days upon light irradiation. Ultimately, this drug delivery strategy has potential for clinical applications that require explicit control over the presentation of biologically active molecules. Further research into the design and fabrication of novel biocompatible thermally responsive delivery vehicles will aid in the advancement of the light-actuated drug delivery-on-demand strategy described here. Comment: Our combined comments on this thesis and the next one appear after the next abstract.
Light-Inducible Gene Regulation in Mammalian Cells Lauren Toth, PhD, Duke University
The growing complexity of scientific research demands further development of advanced gene regulation systems. For instance, the ultimate goal of tissue engineering is to develop constructs that functionally and morphologically resemble the native tissue they are expected to replace. This requires patterning of gene expression and control of cellular phenotype within the tissue-engineered construct. In the field of synthetic biology, gene circuits are engineered to elucidate mechanisms of gene regulation and predict the behavior of more complex systems. Such systems require robust gene switches that can quickly turn gene expression on or off. Similarly, basic science requires precise genetic control to perturb genetic pathways or understand gene function. Additionally, gene therapy strives to replace or repair genes that are responsible for disease. The safety and efficacy of such therapies require control of when and where the delivered gene is expressed in vivo.
Unfortunately, these fields are limited by the lack of gene regulation systems that enable both robust and flexible cellular control. Most current gene regulation systems do not allow for the manipulation of gene expression that is spatially defined, temporally controlled, reversible, and repeatable. Rather, they provide incomplete control that forces the user to choose to control gene expression in either space or time, and whether the system will be reversible or irreversible. The recent emergence of the field of optogenetics—the ability to control gene expression using light—has made it possible to regulate gene expression with spatial, temporal, and dynamic control. Light-inducible systems provide the tools necessary to overcome the limitations of other gene regulation systems, which can be slow, imprecise, or cumbersome to work with. However, emerging light-inducible systems require further optimization to increase their efficiency, reliability, and ease of use.
Initially, we engineered a light-inducible gene regulation system that combines zinc finger protein technology and the light-inducible interaction between Arabidopsis thaliana plant proteins GIGANTEA (GI) and the light oxygen voltage (LOV) domain of FKF1. Zinc finger proteins (ZFPs) can be engineered to target almost any DNA sequence through tandem assembly of individual zinc finger domains that recognize a specific 3-bp DNA sequence. Fusion of three different ZFPs to GI (GI-ZFP) successfully targeted the fusion protein to the specific DNA target sequence of the ZFP. Due to the interaction between GI and LOV, co-expression of GI-ZFP with a fusion protein consisting of LOV fused to three copies of the VP16 transactivation domain (LOV-VP16) enabled blue-light dependent recruitment of LOV-VP16 to the ZFP target sequence. We showed that placement of three to nine copies of a ZFP target sequence upstream of a luciferase or enhanced green fluorescent protein (eGFP) transgene enabled expression of the transgene in response to blue light. Gene activation was both reversible and tunable on the basis of duration of light exposure, illumination intensity, and the number of ZFP binding sites upstream of the transgene. Gene expression could also be patterned spatially by illuminating the cell culture through photomasks containing various patterns.
Although this system was useful for controlling the expression of a transgene, for many applications it is useful to control the expression of a gene in its natural chromosomal position. Therefore, we capitalized on recent advances in programmed gene activation to engineer an optogenetic tool that could easily be targeted to new, endogenous DNA sequences without re-engineering the light inducible proteins. This approach took advantage of CRISPR/Cas9 technology, which uses a gene-specific guide RNA (gRNA) to facilitate Cas9 targeting and binding to a desired sequence, and the light-inducible heterodimerizers CRY2 and CIB1 from Arabidopsis thaliana to engineer a lightactivated CRISPR/Cas9 effector (LACE) system. We fused the full-length (FL) CRY2 to the transcriptional activator VP64 (CRY2FL-VP64) and the amino-terminal fragment of CIB1 to the amino, carboxyl, or amino and carboxyl terminus of a catalytically inactive Cas9. When CRY2-VP64 and one of the CIBN/dCas9 fusion proteins are expressed with a gRNA, the CIBN/dCas9 fusion protein localizes to the gRNA target. In the presence of blue light, CRY2FL binds to CIBN, which translocates CRY2FL-VP64 to the gene target and activates transcription. Unlike other optogenetic systems, the LACE system can be targeted to new endogenous loci by solely manipulating the specificity of the gRNA without having to re-engineer the light-inducible proteins. We achieved light-dependent activation of the IL1RN, HBG1/2, or ASCL1 genes by delivery of the LACE system and four gene-specific gRNAs per promoter region. For some gene targets, we achieved equivalent activation levels to cells that were transfected with the same gRNAs and the synthetic transcription factor dCas9-VP64. Gene activation was also shown to be reversible and repeatable through modulation of the duration of blue light exposure, and spatial patterning of gene expression was achieved using an eGFP reporter and a photomask.
Finally, we engineered a light-activated genetic ‘‘on’’ switch (LAGOS) that provides permanent gene expression in response to an initial dose of blue light illumination. LAGOS is a lentiviral vector that expresses a transgene only upon Cre recombinase–mediated DNA recombination. We showed that this vector, when used in conjunction with a light-inducible Cre recombinase system, could be used to express MyoD or the synthetic transcription factor VP64- MyoD in response to light in multiple mammalian cell lines, including primary mouse embryonic fibroblasts. We achieved light-mediated up-regulation of downstream myogenic markers myogenin, desmin, troponin T, and myosin heavy chains I and II as well as fusion of C3H10T1/2 cells into myotubes that resembled a skeletal muscle cell phenotype. We also demonstrated LAGOS functionality in vivo by engineering the vector to express human VEGF165 and human ANG1 in response to light. HEK 293T cells stably expressing the LAGOS vector and transiently expressing the light-inducible Cre recombinase proteins were implanted into mouse dorsal window chambers. Mice that were illuminated with blue light had increased micro-vessel density compared to mice that were not illuminated. Analysis of human vascular endothelial growth factor (VEGF) and human ANG1 levels by enzyme-linked immunosorbent assay (ELISA) revealed statistically higher levels of VEGF and ANG1 in illuminated mice compared to non-illuminated mice.
In summary, the objective of this work was to engineer robust light-inducible gene regulation systems that can control genes and cellular fate in a spatial and temporal manner. These studies combine the rapid advances in gene targeting and activation technology with natural light-inducible plant protein interactions. Collectively, this thesis presents several optogenetic systems that are expected to facilitate the development of multicellular cell and tissue constructs for use in tissue engineering, synthetic biology, gene therapy, and basic science both in vitro and in vivo.
Comment: Although it is easy to characterize technological progress as following in the wake of scientific discoveries, the reverse is almost equally true; advances in technique open the door to types of experiment previously intractable or impossible. Such is currently the case for the field of optically controlled biotechnology, which has exploded into prominence, particularly over the last half-decade. Light of an appropriate wavelength can penetrate mammalian tissues to a depth of up to a couple of centimeters, rendering much of the living body accessible to optical study and control—still more if the detector/source is integrated into an endoscopic or fiber optic probe. Techniques borrowed from the semiconductor industry allow patterns of illumination to be controlled down to the nanometer scale, ideal for addressing individual cells. The highly controlled time course of such experiments, as compared to traditional means of gene activation, such as the addition of a chemical agent to the medium, eliminates confounding variables, and simplifies data analysis. Furthermore, this level of immediate control opens the door to closed-loop systems where the activity of entities under optical control can be continuously tuned in relation to some parameter(s). In the first of these two illuminating theses, a vehicle is developed that permits light-driven release of a small molecule. Such a system could be employed to target a systemically administered antibiotic or anti-neoplastic agent to a site of infection or cancer while sparing other bodily tissues from toxicity. Because most modern drugs cannot be produced in the body, even given arbitrarily good control of cellular biochemistry, this technique will have lasting value in numerous clinical contexts. In the second thesis, the level of precision achieved is even more profound; the CRISPR/Cas9 system has received much recent attention13 in its own right for its capacity to target arbitrary genetic sequences without an arduous protein-engineering step. The LACE system described stands to permit genetic manipulation with almost arbitrarily good spatial, temporal, and genomic site-specific control, using only means available to a typical university laboratory.
Targeting T Cells for the Immune-Modulation of Human Diseases Regina Lin, PhD, Duke University
Dysregulated inflammation underlies the pathogenesis of a myriad of human diseases ranging from cancer to autoimmunity. As coordinators, executers, and sentinels of host immunity, T cells represent a compelling target population for immune-modulation. In fact, the antigen-specificity, cytotoxicity, and promise of long-lived of immune-protection make T cells ideal vehicles for cancer immunotherapy. Interventions for autoimmune disorders, on the other hand, aim to dampen T cell–mediated inflammation and promote their regulatory functions. Although significant strides have been made in targeting T cells for immune modulation, current approaches remain less than ideal and leave room for improvement. In this dissertation, I seek to improve on current T cell-targeted immunotherapies, by identifying and pre-clinically characterizing their mechanisms of action and in vivo therapeutic efficacy.
CD8+ cytotoxic T cells have potent anti-tumor activity and therefore are leading candidates for use in cancer immunotherapy. The application of CD8+ T cells for clinical use has been limited by the susceptibility of ex vivo– expanded CD8+ T cells to become dysfunctional in response to immunosuppressive microenvironments. To enhance the efficacy of adoptive cell transfer therapy (ACT), we established a novel microRNA (miRNA)-targeting approach that augments CTL cytotoxicity and preserves immunocompetence. Specifically, we screened for miRNAs that modulate cytotoxicity and identified miR-23a as a strong functional repressor of the transcription factor Blimp-1, which promotes CTL cytotoxicity and effector cell differentiation. In a cohort of advanced lung cancer patients, miR- 23a was up-regulated in tumor-infiltrating CD8+ T cells, and its expression correlated with impaired anti-tumor potential of patient CD8+ T cells. We determined that tumor-derived transforming growth factor-b (TGF-b) directly suppresses CD8+ T cell immune function by elevating miR-23a and down-regulating Blimp-1. Functional blockade of miR-23a in human CD8+ T cells enhanced granzyme B expression; and in mice with established tumors, immunotherapy with just a small number of tumor-specific CD8+ T cells in which miR-23a was inhibited robustly hindered tumor progression. Together, our findings provide a miRNA-based strategy that subverts the immunosuppression of CD8+ T cells that is often observed during adoptive cell transfer tumor immunotherapy and identify a TGF-bmediated tumor immune-evasion pathway
Having established that miR-23a-inhibition can enhance the quality and functional resilience of anti-tumor CD8+ T cells, especially within the immune-suppressive tumor microenvironment, we went on to interrogate the translational applicability of this strategy in the context of chimeric antigen receptor (CAR)-modified CD8+ T cells. Although CAR T cells hold immense promise for ACT, CAR T cells are not completely curative due to their in vivo functional suppression by immune barriers—such as TGF-b—within the tumor microenvironment. Because TGF-b poses a substantial immune barrier in the tumor microenvironment, we sought to investigate whether inhibiting miR-23a in CAR T cells can confer immune competence to afford enhanced tumor clearance. To this end, we retrovirally transduced wild-type and miR-23a–deficient CD8+ T cells with the EGFRvIII-CAR, which targets the PepvIII tumorspecific epitope expressed by glioblastomas (GBM). Our in vitro studies demonstrated that while wild-type EGFRvIIICAR T cells were vulnerable to functional suppression by TGF-b, miR-23a abrogation rendered EGFRvIII-CAR T cells immune-resistant to TGF-b. Rigorous preclinical studies are currently underway to evaluate the efficacy of miR-23adeficient EGFRvIII-CAR T cells for GBM immunotherapy.
Last, we explored novel immune-suppressive therapies by the biological characterization of pharmacological agents that could target T cells. Although immune-suppressive drugs are classical therapies for a wide range of autoimmune diseases, they are accompanied by severe adverse effects. This motivated our search for novel immunesuppressive agents that are efficacious and lack undesirable side effects. To this end, we explored the potential utility of subglutinol A, a natural product isolated from the endophytic fungus Fusarium subglutinans. We showed that subglutinol A exerts multimodal immune-suppressive effects on activated T cells in vitro. Subglutinol A effectively blocked T cell proliferation and survival, while profoundly inhibiting pro-inflammatory interferon-c (IFN-c) and interleukin-17 (IL-17) production by fully differentiated effector Th1 and Th17 cells. Our data further revealed that subglutinol A might exert its anti-inflammatory effects by exacerbating mitochondrial damage in T cells, but not in innate immune cells or fibroblasts. Additionally, we demonstrated that subglutinol A significantly reduced lymphocytic infiltration into the footpad and ameliorated footpad swelling in the mouse model of Th1-driven delayed-type hypersensitivity. These results suggest the potential of subglutinol A as a novel therapeutic for inflammatory diseases.
Comment: Immunotherapy is among the most promising approaches to cancer treatment, having the specificity and scope to selectively target transformed cells wherever they may reside within the body and the potential to install a permanent defense against disease recurrence. By the time a typical cancer is clinically diagnosed, however, it has already found means to survive a prolonged period of potential immune attack. The mechanisms by which tumors evade immune surveillance are beginning to be elucidated,15,16 and include both direct suppression of effector cells and progressive editing of the host’s immune repertoire to disfavor future attack. It is inherently difficult to interfere with these defenses directly, due to the selection pressures in genetically heterogeneous neoplastic tissue. Much effort is thus being focused on methods for rendering therapeutically delivered immune cells resistant to their effects. The cytokine TGF-b is paradoxically known to function as both a tumor suppressor in healthy tissue and as a tumorderived species associated with multiple cancer-promoting activities, including enhanced immune evasion. This work identifies the pathway by which TGF-b compromises cytotoxic T cell function in the tumor microenvironment, and demonstrates an effective method for blocking this signal. In many clinical cases, however, editing of the patient’s immune repertoire has already removed or rendered anergic those immune cells able to recognize their cancer. Thus, the finding that blocking TGF-b signaling also appears to enhance the effectiveness of CAR-modified T cells— engineered with an antibody fragment targeting them with high affinity to a particular tumor-associated epitope—is a welcome addition to these already promising results.
Novel Fibonacci and non-Fibonacci structure in the sunflower: results of a citizen science experiment
Jonathan Swinton, Erinma Ochu, The MSI Turing’s Sunflower Consortium
This citizen science study evaluates the occurrence of Fibonacci structure in the spirals of sunflower (Helianthus annuus) seedheads. This phenomenon has competing biomathematical explanations, and our core premise is that observation of both Fibonacci and non-Fibonacci structure is informative for challenging such models. We collected data on 657 sunflowers. In our most reliable data subset, we evaluated 768 clockwise or anticlockwise parastichy numbers of which 565 were Fibonacci numbers, and a further 67 had Fibonacci structure of a predefined type. We also found more complex Fibonacci structures not previously reported in sunflowers. This is the third, and largest, study in the literature, although the first with explicit and independently checkable inclusion and analysis criteria and fully accessible data. This study systematically reports for the first time, to the best of our knowledge, seedheads without Fibonacci structure. Some of these are approximately Fibonacci, and we found in particular that parastichy numbers equal to one less than a Fibonacci number were present significantly more often than those one more than a Fibonacci number. An unexpected further result of this study was the existence of quasi-regular heads, in which no parastichy number could be definitively assigned.
Introduction
Fibonacci structure can be found in hundreds of different species of plants [1]. This has led to a variety of competing conceptual and mathematical models that have been developed to explain this phenomenon. It is not the purpose of this paper to survey these: reviews can be found in [1–4], with more recent work including [5–10]. Instead, we focus on providing empirical data useful for differentiating them.
These models are in some ways now very mathematically satisfying in that they can explain high Fibonacci numbers based on a small number of plausible assumptions, though they are not so satisfying to experimental scientists [11]. Despite an increasingly detailed molecular and biophysical understanding of plant organ positioning [12–14], the very parsimony and generality of the mathematical explanations make the generation and testing of experimental hypotheses difficult. There remains debate about the appropriate choice of mathematical models, and whether they need to be central to our understanding of the molecular developmental biology of the plant. While sunflowers provide easily the largest Fibonacci numbers in phyllotaxis, and thus, one might expect, some of the stronger constraints on any theory, there is a surprising lack of systematic data to support the debate. There have been only two large empirical studies of spirals in the capitulum, or head, of the sunflower: Weisse [15] and Schoute [16], which together counted 459 heads; Schoute found numbers from the main Fibonacci sequence 82% of the time and Weise 95%. The original motivation of this study was to add a third replication to these two historical studies of a widely discussed phenomenon. Much more recently, a study of a smaller sample of 21 seedheads was carried out by Couder [17], who specifically searched for non-Fibonacci examples, whereas Ryan et al. [18] studied the arrangement of seeds more closely in a small sample of Helianthus annuus and a sample of 33 of the related perennial H. tuberosus.
Neither the occurrence of Fibonacci structure nor the developmental biology leading to it are at all unique to sunflowers. As common in other species, the previous sunflower studies found not only Fibonacci numbers, but also the occasional occurrence of the double Fibonacci numbers, Lucas numbers and F4 numbers defined below [1]. It is worth pointing out the warning of Cooke [19] that numbers from these sequences make up all but three of the first 17 integers. This means that it is particularly valuable to look at specimens with large parastichy numbers, such as the sunflowers, where the prevalence of Fibonacci structure is at its most striking.
Neither Schoute nor Weisse reported their precise technique for assigning parastichy numbers to their samples, and it is noteworthy that neither author reported any observation of non-Fibonacci structure. One of the objectives of this study was to rigorously define Fibonacci structure in advance and to ensure that the assignment method, though inevitably subjective, was carefully documented.
This paper concentrates on the patterning of seeds towards the outer rim of sunflower seedheads. The number of ray florets (the ‘petals’, typically bright yellow) or the green bracts behind them tends to have a looser distribution around a Fibonacci number. In the only mass survey of these, Majumder & Chakravarti [20] counted ray florets on 1002 sunflower heads and found a distribution centred on 21.
This citizen science study evaluates the occurrence of Fibonacci structure in the spirals of sunflower (Helianthus annuus) seedheads. This phenomenon has competing biomathematical explanations, and our core premise is that observation of both Fibonacci and non-Fibonacci structure is informative for challenging such models. We collected data on 657 sunflowers. In our most reliable data subset, we evaluated 768 clockwise or anticlockwise parastichy numbers of which 565 were Fibonacci numbers, and a further 67 had Fibonacci structure of a predefined type. We also found more complex Fibonacci structures not previously reported in sunflowers. This is the third, and largest, study in the literature, although the first with explicit and independently checkable inclusion and analysis criteria and fully accessible data. This study systematically reports for the first time, to the best of our knowledge, seedheads without Fibonacci structure. Some of these are approximately Fibonacci, and we found in particular that parastichy numbers equal to one less than a Fibonacci number were present significantly more often than those one more than a Fibonacci number. An unexpected further result of this study was the existence of quasi-regular heads, in which no parastichy number could be definitively assigned.
Incorporation of irregularity into the mathematical models of phyllotaxis is relatively recent: [17] gave an example of a disordered pattern arising directly from the deterministic model while more recently the authors have begun to consider the effects of stochasticity [10,21]. Differentiating between these models will require data that go beyond capturing the relative prevalence of different types of Fibonacci structure, so this study was also designed to yield the first large-scale sample of disorder in the head of the sunflower.
The Fibonacci sequence is the sequence of integers 1,2,3,5,8,13,21,34,55,89,144… in which each member after the second is the sum of the two preceding. The Lucas sequence is the sequence of integers 1,3,4,7,11,18,29,47,76,123… obeying the same rule but with a different starting condition; the F4 sequence is similarly 1,4,5,9,14,23,37,60,97,…. The double Fibonacci sequence 2,4,6,10,16,26,42,68,110,… is double the Fibonacci sequence. We say that a parastichy number which is any of these numbers has Fibonacci structure. The sequencesF5=1,5,6,11,17,28,45,73,… and F8=1,8,9,17,26,43,69,112… also arise from the same rule, but as they had not been previously observed in sunflowers we did not include these in the pre-planned definition of Fibonacci structure for parsimony. One example of adjacent pairs from each of these sequences was, in fact, observed but both examples are classified as non-Fibonacci below. A parastichy number which is any of 12,20,33,54,88,143 is also not classed as having Fibonacci structure but is distinguished as a Fibonacci number minus one in some of the analyses, and similarly 14,22,35,56,90,145 as Fibonacci plus one.
When looking at a seedhead such as in figure 1 the eye naturally picks out at least one family of parastichies or spirals: in this case, there is a clockwise family highlighted in blue in the image on the right-hand side.
Figure 5 plots the individual pairs observed. On the reference line, the ratio of the numbers is equal to the golden ratio so departures from the line mark departures from Fibonacci structure, which are less evident in the more reliable photoreviewed dataset. It can be seen from table 3 that Fibonacci pairings dominate the dataset.
Observed pairings of Fibonacci types of clockwise and anticlockwise parastichy numbers. Other means any parastichy number which neither has Fibonacci structure nor is Fibonacci ±1. Of all the Fibonacci ±1/Fibonacci pairs, only sample 191, a (21,20) pair, was not close to an adjacent Fibonacci pair.
One typical example of a Fibonacci pair is shown in figure 6, with a double Fibonacci case infigure 1 and a Lucas one in figure 7. There was no photoreviewed example of an F4 pairing. The sole photoreviewed assignment of a parastichy number to the F4 sequence was the anticlockwise parastichy number 37 in sample 570, which was relatively disordered. The clockwise parastichy number was 55, lending support to the idea this may have been a perturbation of a (34,55) pattern. We also found adjacent members of higher-order Fibonacci series. Figures 8 and 9 each show well-ordered examples with parastichy counts found adjacent in the F5 and F8 series, respectively: neither of these have been previously reported in the sunflower.
Sunflower 095. An (89,55) example with 89 clockwise parastichies and 55 anticlockwise ones, extending right to the rim of the head. Because these are clear and unambiguous, the other parastichy families which are visible towards the centre are not counted here.
Sunflower 667. Anticlockwise parastichies only, showing competing parastichy families which are distinct but in some places overlapping.
Our core results are twofold. First, and unsurprisingly, Fibonacci numbers, and Fibonacci structure more generally, are commonly found in the patterns in the seedheads of sunflowers. Given the extent to which Fibonacci patterns have attracted pseudo-scientific attention [33], this substantial replication of limited previous studies needs no apology. We have also published, for the first time, examples of seedheads related to the F5 and F8 sequences but by themselves they do not add much to the evidence base. Our second core result, though, is a systematic survey of cases where Fibonacci structure, defined strictly or loosely, did not appear. Although not common, such cases do exist and should shed light on the underlying developmental mechanisms. This paper does not attempt to shed that light, but we highlight the observations that any convincing model should explain. First, the prevalence of Lucas numbers is higher than those of double Fibonacci numbers in all three large datasets in the literature, including ours, and there are sporadic appearances of F4, F5 and F8 sequences. Second, counts near to but not exactly equal to Fibonacci structure are also observable: we saw a parastichy count of 54 more often than the most common Lucas count of 47. Sometimes, ambiguity arises in the counting process as to whether an exact Fibonacci-structured number might be obtained instead, but there are sufficiently many unambiguous cases to be confident this is a genuine phenomenon. Third, among these approximately Fibonacci counts, those which are a Fibonacci number minus one are significantly more likely to be seen than a Fibonacci number plus one. Fourth, it is not uncommon for the parastichy families in a seedhead to have strong departures from rotational symmetry: this can have the effect of yielding parastichy numbers which have large departures from Fibonacci structure or which are completely uncountable. This is related to the appearance of competing parastichy families. Fifth, it is common for the parastichy count in one direction to be more orderly and less ambiguous than that in the other. Sixth, seedheads sometimes possess completely disordered regions which make the assignment of parastichy numbers impossible. Some of these observations are unsurprising, some can be challenged by different counting protocols, and some are likely to be easily explained by the mathematical properties of deformed lattices, but taken together they pose a challenge for further research.
It is in the nature of this crowd-sourced experiment with multiple data sources that it is much easier to show variability than it is to find correlates of that variability. We tried a number of cofactor analyses that found no significant effect of geography, growing conditions or seed type but if they do influence Fibonacci structure, they are likely to be much easier to detect in a single-experimenter setting.
We have been forced by our results to extend classifications of seedhead patterns beyond structured Fibonacci to approximate Fibonacci ones. Clearly, the more loose the definition of approximate Fibonacci, the easier it is to explain away departures from model predictions. Couder [17] found one case of a (54,87) pair that he interpreted as a triple Lucas pair 3×(18,29). While mathematically true, in the light of our data, it might be more compellingly be thought of as close to a (55,89) ideal than an exact triple Lucas one. Taken together, this need to accommodate non-exact patterns, the dominance of one less over one more than Fibonacci numbers, and the observation of overlapping parastichy families suggest that models that explicitly represent noisy developmental processes may be both necessary and testable for a full understanding of this fascinating phenomenon. In conclusion, this paper provides a testbed against which a new generation of mathematical models can and should be built.
Researchers find weaker immune response to viral infections in children with mitochondrial disorders
One of the first human studies on how mitochondrial function impacts immune cells to guide future treatments. Mitochondria convert food and oxygen into energy. Genomic variants in more than 350 genes have been linked to mitochondrial disorders.NHGRI In a new study, National Institutes of Health (NIH) researchers found that altered B cell function in children with mitochondrial disorders led to a weaker and less diverse antibody response to viral infections. The study, published in Frontiers in Immunology, was led by researchers at the National Human Genome Research Institute (NHGRI), who analyzed the gene activities of immune cells in children with mitochondrial disorders and found that B cells, which produce antibodies to fight viral infections, are less able to survive cellular stress.
“Our work is one of the first examples to study how B cells are affected in mitochondrial disease by looking at human patients,” said Eliza Gordon-Lipkin, M.D., assistant research physician in NHGRI’s Metabolism, Infection and Immunity Section and co-first author of the paper.
Mitochondria are important components of nearly every cell in the body because they convert food and oxygen into energy. Genomic variants in more than 350 genes have been linked to mitochondrial disorders with varied symptoms depending on which cells are affected.
“For children with mitochondrial disorders, infections can be life threatening or they can worsen the progression of their disorder,” said Peter McGuire, M.B.B.Ch., NHGRI investigator, head of the Metabolism, Infection and Immunity Section and senior author of the study. “We wanted to understand how immune cells differ in these patients and how that influences their response to infections.”
Around 1 in 5,000 people worldwide have a mitochondrial disorder. Examples of mitochondrial disorders are Leigh’s syndrome, which primarily affects the nervous system, and Kearns-Sayre syndrome, which primarily affects the eyes and heart. While mitochondrial disorders are known to affect organs such as the heart, liver, and brain, less is known how they affect the immune system. Using a genomic technique called single-cell RNA sequencing, which analyzes gene activity in different cell types, researchers studied immune cells found in blood. These cells include different types of white blood cells that help the body fight infections. During stressful conditions, these cells produce a microRNA called mir4485. MicroRNAs are small strings of RNA that help control when and where genes are turned on and off. mir4485 controls cellular pathways that help cells survive.
“We think that B cells in these patients undergo cellular stress when they turn into plasma cells and produce antibodies, and these B cells then try to survive by producing the microRNA to cope,” said Dr. McGuire. “But the B cells are too fragile due to their limited energy, so they are unable to survive the stressful conditions.”
Researchers used a technique called VirScan to look at all past viral infections, assess how well the immune system fought those infections and see the effects of B cells and plasma cells on antibody production. With a weaker antibody response, the immune systems in children with mitochondrial disorders are less able to recognize and neutralize invading viruses and clear infections. Researchers aim to use the results of this study to guide future treatment of patients with mitochondrial disorders, noting that more translational studies are needed in this research area.
Reference: Gordon-Lipkin et al. Primary oxidative phosphorylation defects lead to perturbations in the human B cell repertoire. Frontiers in Immunology. DOI: 10.3389/fimmu.2023.1142634. (2023)
Regulatory T (TReg) cells are essential for maintaining peripheral tolerance, preventing autoimmune diseases and limiting chronic inflammatory diseases. However, they also limit beneficial responses by suppressing sterilizing immunity and limiting antitumour immunity. Given that TReg cells can have both beneficial and deleterious effects, there is considerable interest in determining their mechanisms of action. In this Review, we describe the basic mechanisms used by TReg cells to mediate suppression and discuss whether one or many of these mechanisms are likely to be crucial for TReg-cell function. In addition, we propose the hypothesis that effector T cells may not be ‘innocent’ parties in this suppressive process and might in fact potentiate TReg-cell function.
This schematic depicts the various regulatory T (Treg)-cell mechanisms arranged into four groups centred around four basic modes of action. ‘Inhibitory cytokines’ include interleukin-10 (IL-10), interleukin-35 (IL-35) and transforming growth factor-β (TGF-β). ‘Cytolysis’ includes granzyme-A- and granzyme-B-dependent and perforin-dependent killing mechanisms. ‘Metabolic disruption’ includes high affinity IL-2 receptor α (CD25)-dependent cytokine-deprivation-mediated apoptosis, cyclic AMP (cAMP)-mediated inhibition, and CD39- and/or CD73-generated, adenosine–purinergic adenosine receptor (A2A)-mediated immunosuppression. ‘Targeting dendritic cells’ includes mechanisms that modulate DC maturation and/or function such as lymphocyte activation gene-3 (LAG3; also known as CD223)–MHC-class-II-mediated suppression of DC maturation, and cytotoxic T lymphocyte antigen-4 (CTLA4)–CD80/CD86-mediated induction of indoleamine 2,3-dioxygenase (IDO), which is an immunosuppressive molecule, by DCs.
Model for how effector T cells might boost Treg-cell function
This occurs in three stages. (a) Initial regulatory T (Treg)-cell activation induces production of regulatory factors such as interleukin-35 (IL-35). (b) Treg cells ‘sense’ the presence of recently activated effector T cells through a receptor–ligand interaction (cell surface or soluble). (c) This in turn boosts or potentiates Treg-cell function resulting in the enhanced production of regulatory mediators, such as IL-35, and perhaps the induction of new mediators.
Regulatory T (Treg) cells are essential for maintaining peripheral tolerance, preventing autoimmune diseases and limiting chronic inflammatory diseases. However, they also limit beneficial responses by suppressing sterilizing immunity and limiting anti-tumour immunity. Given that Treg cells can have both beneficial and deleterious effects, there is considerable interest in determining their mechanisms of action. In this Review, we discuss the basic mechanisms used by Treg cells to mediate suppression, and discuss whether one or many of these mechanisms are likely to be crucial for Tregcell function. In addition, we present the hypothesis that effector T cells may not be ‘innocent’ parties in this suppressive process and might in fact potentiate Treg-cell function.
Several sophisticated regulatory mechanisms are used to maintain immune homeostasis, prevent autoimmunity and moderate inflammation induced by pathogens and environmental insults. Chief amongst these are regulatory T (Treg) cells that are now widely regarded as the primary mediators of peripheral tolerance. Although Treg cells play a pivotal role in preventing autoimmune diseases, such as type 1 diabetes1,2, and limiting chronic inflammatory diseases, such as asthma and inflammatory bowel disease (IBD)3,4, they also block beneficial responses by preventing sterilizing immunity to certain pathogens5,6 and limiting anti-tumour immunity7. A seminal advance in the analysis of Treg cells came with the identification of a key transcription factor, forkhead box P3 (FOXP3), that is required for their development, maintenance and function8,9. Mice and patients that lack FOXP3 develop a profound autoimmune-like lymphoproliferative disease that graphically emphasizes the importance of Treg cells in maintaining peripheral tolerance10-12 (BOX 1). Although FOXP3 has been proposed as the master regulator of Treg cells that controls the expression of multiple genes that mediate their regulatory activity13,14, this has been recently challenged raising the possibility that other transcriptional events may operate upstream of and/or concurrently with FOXP3 to mediate Treg-cell development15.
While Foxp3 has proven to be an invaluable marker for murine Treg cells, its role in human Treg cells is less straightforward (see BOX 2 for a discussion of Treg-cell markers). Humans that lack FOXP3 develop immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX), a severe autoimmune disease that presents early in infancy. Although FOXP3 appears to be required for human Treg-cell development and function, expression of FOXP3 alone is clearly not sufficient as a significant percentage of human activated T cells express FOXP3 and yet do not possess regulatory activity16-20. Furthermore, induction of FOXP3 in human T cells by transforming growth factor-β (TGFβ) does not confer a regulatory phenotype, in contrast to their murine counterparts20. Consequently, FOXP3 is not a good marker for human Treg cells (BOX 2). Whether this distinction is due to intrinsic differences between mouse and human FOXP3 and/or a requirement for an additional cofactor/ transcription factor is an important question that needs to be resolved.
Significant progress has been made over the last few years in delineating the molecules and mechanisms that Treg cells use to mediate suppression21,22. In this Review, we outline our current understanding of the mechanisms used by Treg cells to mediate suppression, and the challenges that lie ahead in defining their mode of action. We also discuss whether Treg cells are likely to depend on one, a few or many of these mechanisms. In addition, we propose that effector T cells may have a significant role in boosting and/or modulating Treg-cell function. Unless stated, we focus here primarily on the mechanisms that are used by thymus-derived natural CD4+CD25+ FOXP3+ Treg cells.
Basic mechanisms of Treg-cell function Defining the mechanisms of Treg-cell function is clearly of crucial importance. Not only would this provide insight into the control processes of peripheral tolerance but it would probably provide a number of potentially important therapeutic targets. Although this quest has been ongoing since interest in Treg cells was reignited in 199523, there has been significant progress in the last few years. From a functional perspective, the various potential suppression mechanisms of Treg cells can be grouped into four basic ‘modes of action’: suppression by inhibitory cytokines, suppression by cytolysis, suppression by metabolic disruption, and suppression by modulation of dendritic-cell (DC) maturation or function (FIG. 1).
Suppression by inhibitory cytokines Inhibitory cytokines, such as interleukin-10 (IL-10) and TGFβ, have been the focus of considerable attention as a mechanism of Treg-cell-mediated suppression. There has also been significant interest in their ability to generate induced (also known as adaptive) Treg-cell populations, either naturally in vivo or experimentally as a potential therapeutic modality (BOX 3). Although the general importance of IL-10 and TGFβ as suppressive mediators is undisputed, their contribution to the function of thymus-derived, natural Treg cells is still a matter of debate24. This is partly due to the general perception that Treg cells function in a contactdependent manner25,26. Indeed, in vitro studies using neutralizing antibodies or T cells that are unable to produce or respond to IL-10 and TGFβ suggested that these cytokines may not be essential for Treg-cell function25-28. However, this contrasts with data from in vivo studies29,30.
In allergy and asthma models, evidence suggests that both natural and antigen-specific Treg cells control disease in a manner that is, in part, dependent on IL-1029 and in some reports dependent on both IL-10 and TGFβ 31. Adoptive transfer of allergen-specific Treg cells induced significant IL-10 production by CD4+ effector T cells in the lung following allergen challenge and this Treg-cell-mediated control of disease was reversed by treatment with an IL-10- receptor-specific antibody32. However, suppression of allergic inflammation and airway hyper-reactivity, and increased production of IL-10 still occurred following transfer of IL-10- deficient Treg cells, suggesting that Treg cells can suppress the Th2-driven response to allergens in vivo through an IL-10-dependent mechanism, but that the production of IL-10 by Treg cells themselves is not required for the suppression observed. This contrasts with a recent study suggesting that the Treg-cell-specific ablation of IL-10 expression resulted in increased lung allergic inflammation and hyperreactivity33.
This scenario might occur in other disease models. For instance, the effects of IL-10 can only be partially attributed to Treg-cell-derived IL-10 in the immune response to hepatitis B virus34 and in the allograft tolerance response elicited by splenocytes exposed to non-inherited maternal antigens35. Recently, it was also shown that IL-10 is crucial for the control of various infections in which Treg cells have been reported to be involved including Mycobacterium tuberculosis36, Toxoplasma gondii37, Leishmania major38, and Trichinella spiralis39. However, Treg cells were not the source of IL-10 in all of these infection models.
By contrast, several studies have shown that IL-10 production by Treg cells is essential for the prevention of colitis in mouse models of IBD40. Moreover, it appears that the tumour microenvironment promotes the generation of FOXP3+ Treg cells that mediate IL-10- dependent, cell-contact independent, suppression41. Similarly, in UV-radiation-induced carcinogenesis, IL-10 production by Treg cells appears to be important for blocking anti-tumour immunity42. IL-10 produced by Treg cells also appears to be crucial for IL-10-mediated tolerance in a model of hepatitis induced by concanavalin A43 and tolerance to bacterial and viral superantigens44. In addition, recent papers suggest new roles for Treg-cell-derived IL-10 in the induction of feto-maternal tolerance45 and B-cell-enhanced recovery from experimental autoimmune encephalomyelitis46. Collectively, the picture that appears to be emerging is that the relative importance of Treg-cell-derived IL-10 is very dependent on the target organism or disease and on the experimental system. Furthermore, the Treg-cell-specific deletion of IL-10 did not result in the development of spontaneous systemic autoimmunity, but did result in enhanced pathology in the colon of older mice and in the lungs of mice with induced airway hypersensitivity, suggesting that the function of Treg-cell-derived IL-10 may be restricted to controlling inflammatory responses induced by pathogens or environmental insults33.
While some early in vitro studies using neutralizing antibodies to TGFβ or Treg cells lacking TGFβ 25,47 indicated that TGFβ was not required for natural Treg-cell function, other studies, both in vitro and in vivo suggested a critical role for Treg-cell surface bound TGFβ 48,49. Therefore, the importance of TGFβ for natural Treg-cell function has also been a controversial topic. Indeed, there has been considerably more focus recently on the importance of TGFβ in the development of induced Treg cells and perhaps in Treg-cell maintenance in general (BOX 3). However, there are studies that suggest that TGFβ produced by Treg cells may directly participate in effector T-cell suppression. For instance, effector T cells that are resistant to TGFβ-mediated suppression cannot be controlled by Treg cells in an IBD model50. In addition, TGFβ produced by Treg cells has been found to be important in the control of the host immune response to M. tuberculosis36, suppression of allergic responses31 and prevention of colitis in an IBD model51. Interestingly, TGFβ produced by Treg cells has also been implicated in limiting anti-tumour immunity in head and neck squamous-cell carcinoma52 and in follicular lymphoma53 by rendering T cells unresponsive to the tumour. TGFβ also appears to limit the anti-tumour activity of cytokine-induced killer cells54.
Membrane-tethered TGFβ can also mediate suppression by Treg cells in a cell-cell contactdependent manner48. Treg cells can control islet infiltration of CD8+ T cells and delay the progress of diabetes through membrane-tethered TGFβ 49. However, experiments using mice deficient in TGFβ-receptor (TGFβR) signalling in effector T cells or using TGFβ or TGFβR blocking reagents failed to show that membrane-tethered TGFβ is required for natural Treg cell development or function47. More recently, however, interest in membrane-tethered TGFβ has re-surfaced with the description of a previously unappreciated role for it in the tumour microenvironment. TGFβ associated with tumour exosome membranes appears to enhance the suppressive function of Treg cells and skew T cells away from their effector functions and towards regulatory functions55. Furthermore, ovalbumin-induced airway inflammation can be attenuated by heme oxygenase-1 through membrane-tethered TGFβ and IL-10 secretion by Treg cells56, a process that activates the Notch1–HES1 (hairy and enhancer of split 1) axis in target cells57. Thus, in light of the most current data, it now appears that soluble and/or membrane-tethered TGFβ may have a previously unappreciated role in natural Treg-cell function.
Recently, a new inhibitory cytokine, IL-35, has been described that is preferentially expressed by Treg cells and is required for their maximal suppressive activity58. IL-35 is a novel member of the IL-12 heterodimeric cytokine family and is formed by the pairing of Epstein–Barr virus induced gene 3 (Ebi3), which normally pairs with p28 to form IL-27, and p35 (also known as Il12a), which normally pairs with p40 to form IL-12. Both Ebi3 and Il12a are preferentially expressed by murine Foxp3+ Treg cells58,59, but not resting or active effector T cells, and are significantly upregulated in actively suppressing Treg cells58. As predicted for a heterodimeric cytokine, both Ebi3−/− and Il12a−/− Treg cells had significantly reduced regulatory activity in vitro and failed to control homeostatic proliferation and cure IBD in vivo. This precise phenocopy suggested that IL-35 is required for the maximal suppressive activity of Treg cells. Importantly IL-35 was not only required but sufficient, as ectopic expression of IL-35 conferred regulatory activity on naive T cells and recombinant IL-35 suppressed T cell proliferation in vitro58. Although IL-35 is an exciting addition to the Treg-cell portfolio, there is clearly much that remains to be defined about this cytokine and its contribution to Treg-cell function. For instance, it remains to be determined if IL-35 suppresses the development and/or function of other cell types such as DCs and macrophages.
It is now clear that three inhibitory cytokines, IL-10, IL-35 and TGFβ, are key mediators of Treg-cell function. Although they are all inhibitory, the extent to which they are utilized in distinct pathogenic/homeostatic settings differs suggesting a non-overlapping function, which needs further refinement.
……….
How many mechanisms do Treg cells need? Although efforts to define the suppressive mechanisms used by Treg cells continue, an important question looms large. Is it likely that all these molecules and mechanisms will be crucial for Treg-cell function? There are three broad possibilities.
One, a single, overriding suppressive mechanism is required by all Treg cells Until the entire mechanistic panoply of Treg cells is defined, one cannot completely rule out this possibility. However, this possibility would seem unlikely as none of the molecules and/ or mechanisms that have been defined to date, when blocked or deleted, result in the complete absence of regulatory activity — a consequence that one might predict would result in a ‘Scurfy-like’ phenotype (BOX 1). So, although Treg cells that lack a single molecule, for instance IL-10, IL-35 or granzyme B, exhibit significantly reduced suppressor function, a scurfy phenotype does not ensue. Given that none of the current Treg-cell mechanisms can exclusively claim this distinction, it seems unlikely that any ‘unknown’ molecules or mechanisms could do so either.
Two, multiple, non-redundant mechanisms are required for maximal Treg-cell function In the studies conducted to date, Treg cells that lack various suppressive molecules have been shown to be functionally defective. This favours a scenario where there are multiple mechanisms that can be used by Treg cells but they are non-redundant, with each molecule contributing to the mechanistic whole. At present, this possibility would seem plausible. Indeed, this is supported by the recent analysis of mice possessing a Treg-cell-specific ablation of IL-10 expression, in which enhanced pathology was observed following environmental insult33. One would predict that at some point we should be able to generate knockout mice that lack a particular set of genes which results in a complete loss of Treg-cell activity. For this to be truly non-redundant, this list would probably be restricted and small (2–4 genes).
Three, multiple, redundant mechanisms are required for maximal Treg-cell function With the plethora of regulatory mechanisms described to date and the possibility of more yet to be identified, it is conceivable that there are multiple mechanisms that function redundantly. Such a redundant system would help to mitigate against effector T-cell escape from regulatory control. Also, given the very small size of the Treg-cell population, a sizable arsenal may be required at the height of an effector T-cell attack. Of course, it is possible that a semi-redundant scenario exists.
These possibilities have been discussed from the perspective of there being a single homogeneous Treg-cell population. However, as for helper T cell subsets it remains possible that a few or even many different Treg-cell subsets exist24. Each of these may rely on one or multiple regulatory mechanisms. Several recent studies have provided support for both phenotypic and functional heterogeneity amongst Treg cells. For instance, it has recently been shown that a small sub-population of Treg cells express the chemokine receptor CCR6, which is associated with T cells possessing an effector-memory phenotype102. CCR6+ Treg cells appeared to accumulate in the central nervous systems of mice with experimental autoimmune encephalomyelitis (EAE) suggesting that they may have a prevalent role in controlling responses in inflamed tissues. Heterogeneous expression of HLA-DR has also been suggested to mark different subpopulations of functionally distinct human Treg cells103. Indeed, HLADR positive Treg cells were found to be more suppressive than their DR negative counterparts. One might speculate that their enhanced inhibitory activity is due to DR-mediated ligation of the inhibitory molecule LAG3 expressed by activated effector T cells95,96.
So, if multiple suppressor mechanisms exist, how might these be integrated and used productively by Treg cells in vivo? We would propose the following possible models21. First, a ‘hierarchical’ model in which Treg cells possess many mechanisms that could be used but only one or two that are really crucial and consistently important in a variety of regulatory settings. Second, a ‘contextual’ model where different mechanisms become more or less important depending on the background or context in which the Treg cells reside and the type of target cell that they have to repress. For example, some cell types may be inhibited primarily by cytokines, whereas others are most effectively suppressed through lysis by Treg cells. Alternatively, different mechanisms may be more effective in different tissue compartments or in different disease settings. This notion is supported by the recent analysis of mice in which IL-10 expression was specifically ablated in Treg cells33. Whereas Treg-cell-derived IL-10 was not required for the systemic control of autoimmunity, it did seem to be required from the control of inflammatory events at mucosal interfaces such as the lungs and colon. As a clear picture of the available Treg-cell weaponry emerges, an important challenge will be to determine their relative importance and contribution to Treg-cell function in different disease models.
A hypothesis: effector T cells potentiate Treg-cell function? Most cellular interactions within the immune system are bidirectional, with molecular signals moving in both directions even though the interaction has broader unidirectional intentions (for example, CD4+ T-cell help). However, to date the general perception is that Treg cells suppress and effector T cells capitulate. We hypothesize that this is in fact an incomplete picture and that effector T cells have a very active role in their own functional demise. Three recent observations support this view. First, we have recently examined the molecular signature of activated Treg cells in the presence and absence of effector T cells and were surprised to find that it was strikingly different, with hundreds of genes differentially modulated as a consequence of the presence of effector T cells (C.J.W. and D.A.A.V., unpublished observations). Second, we have shown that Ebi3 and Il12a mRNA are markedly upregulated in Treg cells that were co-cultured with effector T cells, supporting the idea that effector T cells may provide signals which boost IL-35 production in trans58. Third, we found that Treg cells were able to mediate suppression of effector T cells across a permeable membrane when placed in direct contact with effector T cells in the upper chamber of a Transwell™ plate (L.W.C. and D.A.A.V., unpublished observations). Interestingly, this suppression was IL-35 dependent, as Ebi3−/− Treg cells were unable to mediate this ‘long-distance’ suppression. Collectively, these data suggest that it is the ‘induction’, rather than the ‘function’, of Treg-cell suppression that is contact-dependent and that effector T cells have an active role in potentiating Treg-cellmediated suppression. Therefore, we hypothesize that receptor–ligand interactions between the co-cultured CD4+ effector T cells and Treg cells initiate a signalling pathway that leads to enhanced IL-35 secretion and regulatory activity (FIG. 2). While the molecule that mediates this enhanced Treg-cell suppression is unknown, it is possible that IL-2 may serve this function104. Given the contrasting genetic profiles of activated Treg cells in the presence and absence of effector T cells, it seems possible that this interaction may boost the expression of other regulatory proteins. It may well be that effector T cells unwittingly perform the ultimate act of altruism.
Concluding remarks Although significant progress has been made over the last few years in defining the mechanisms that Treg cells use to mediate their suppressive function, there is clearly much that remains to be elucidated and many questions persist. First, are there more undiscovered mechanisms and/ or molecules that mediate Treg-cell suppression? What is clear is that the transcriptional landscape of Treg cells is very different from naive or activated effector T cells. There are literally thousands of genes that are upregulated (or downregulated) in Treg cells compared with effector T cells. Although it seems unlikely that all or many of these will be crucial for Treg-cell function, it is quite possible that a few undiscovered genes might be important. It should be noted that although we are discussing mechanisms here, it is clear that some of these molecules may perform key Treg-cell functions, such as Treg-cell homing and homeostasis, which are likely to indirectly influence their suppressive capacity in vivo but don’t directly contribute to their inhibitory activity. It is also possible that some of these unknown molecules may represent more specific markers for the characterization and isolation of Treg cells, a particularly important issue for the analysis and use of human Treg cells (BOX 2).
Second, which mechanisms are most important? An important but potentially complex challenge will be to determine if a few mechanisms are important in many Treg-cell settings or whether different mechanisms are required in different cellular scenarios. At present it is difficult to assess this objectively as these mechanisms have predominantly been elucidated in different labs using distinct experimental systems and thus none have really been compared in side-by-side experiments. Furthermore, only recently have conditional mutant mice been examined that have a regulatory component specifically deleted in Treg cells33.
It almost goes without saying that although defining the Treg-cell mode of action is of great academic importance, it is also essential in order to develop effective approaches for the clinical manipulation of Treg cells. Given the capacity of Treg cells to control inflammation and autoimmunity, and their implication in blocking effective anti-tumour immunity and preventing sterilizing immunity, it seems probable that a clear understanding of how Treg cells work will present definitive opportunities for therapeutic intervention.
Mice that carry a spontaneous loss-of-function mutation (known as Scurfy mice) or a deletion of Foxp3 develop a fatal autoimmune-like disease with hyperresponsive CD4+ T cells9,12. More recently Foxp3:diptheria toxin receptor (DTR) knockin mice have allowed for the selective depletion of Treg cells following DT treatment105. These mice have been invaluable for dissecting the role of Foxp3 in Treg-cell function. Given the profound phenotype in these mice, there is a general expectation that genetic disruption of any key Treg-cell inhibitory molecule or mechanism would probably result in a Scurfy-like phenotype. Of course, it is also possible that deletion of a key Treg-cell gene may be more synonymous with DT-mediated Treg-cell depletion where Foxp3 may still serve to prevent expression of proinflammatory cytokines105. Nonetheless, this has lead to the notion that if mutant mice don’t have a Scurfy-like or a Treg-cell-depleted phenotype, then the disrupted gene probably isn’t important for Treg-cell function. This may not necessarily be correct. Indeed, it is possible that no mouse lacking a Treg-cell inhibitory effector molecule will ever be generated that develops a profound, spontaneous autoimmune disease21. It should be noted that mutant mice that are Helicobacter spp. and/or Citrobacter rodentium positive may have an exacerbated phenotype, as several studies have shown that opportunistic enteric bacteria can significant exacerbate gut pathology4. Ultimately, the occurrence of disease in knockout mice will depend on whether Treg cells rely on a single or multiple suppressive mechanisms. Given the number of genes induced or modulated by FOXP3, it is probable that a programme of intrinsic and extrinsic regulation is induced that involves multiple proteins9,13. Therefore, it would not be surprising if deletion of a single molecule does not provoke the profound Scurfy-like phenotype seen in mice that lack Foxp3.
Box 2. Treg-cell markers
Identifying discriminatory cell surface markers for the characterization and isolation of Treg cells has always been a critical goal. Although excellent markers exist for murine Treg cells, this goal has remained elusive for human Treg cells. Traditionally, murine and human Treg cells have been characterized as CD4+CD25+ (also known as interleukin-2 receptor α (IL-2Rα)). Indeed, murine Treg cells can be effectively isolated based on staining for CD4+CD25+CD45RBlow expression. However, the purity of isolated human Treg cells has always been an issue because T cells up-regulate CD25 upon activation106. Indeed, during the influenza or allergy season a substantial proportion of human CD4+ T cells can express CD25. Although the identification of forkhead box P3 (Foxp3) as a key regulator of Treg-cell development and function has facilitated their identification in the mouse8, many activated (non-regulatory) human T cells express FOXP3, precluding it as a useful marker for human Treg cells16-20. Consequently, the search for Treg-cell-specific cellsurface markers, particularly in humans, has continued in earnest with a growing number of candidates proposed (reviewed by Zhao and colleagues107). For instance, it was shown that the expression of CD127 (also known as IL-7R) is down-regulated on Treg cells and that this could be used to increase the purity of human Treg-cell isolation. Indeed, there is a 90% correlation between CD4+CD25+CD127low T cells and FOXP3 expression108, 109. In addition, it was recently found that Treg cells expressed a higher level of folate receptor 4 (FR4) compared with activated effector T cells110. It is also important to recognize that Treg cells, like their T helper cell counterparts, may be heterogeneous and thus a collection of cell surface markers could facilitate their isolation and functional characterization. Indeed, such heterogeneity has recently been described based on differential expression of HLA-DR or CCR6102,103. However, the general use of both markers remains to be fully established so it is quite probable that the search for better Treg-cell markers will continue for some time.
Box 3 Induced or adaptive Treg cells: development and mode of action
Naturally occurring FOXP3+CD4+CD25+ Treg cells develop in the thymus and display a diverse T-cell receptor (TCR) repertoire that is specific for self-antigens111,112. However, Treg cells can also be ‘induced’, ‘adapted’ or ‘converted’ from effector T cells during inflammatory processes in peripheral tissues, or experimentally generated as a possible therapeutic29,113,114. For instance, T regulatory 1 cells (Tr1) and T helper 3 cells (Th3) can be generated experimentally by, and mediate their suppressive activity through interleukin-10 (IL-10) and transforming growth factor-β (TGFβ), respectively114,115. Typically, these regulatory populations do not express FOXP3. In vivo, it has recently been suggested that stimulation of mouse effector T cells by CD103+ dendritic cells (DCs) in the presence of TGFβ and retinoic acid induces the generation of Foxp3+ T cells in the gutassociated lymphoid tissue (GALT)116-121. Furthermore, Treg cells can be preferentially induced in the periphery by exposure to αVβ8-integrin-expressing DCs122 or suppressor of cytokine signalling 3 (Socs3) −/− DCs123. Interestingly, independent of its role in generating induced Treg cells, TGFβ may also have an important role in helping to maintain Foxp3 expression in natural Treg cells124, a process that can be blocked by IL-4 or interferon-γ (IFNγ) 125. In contrast to mouse T cells, FOXP3 induction by TCR stimulation in the presence of TGFβ in human T cells does not confer a regulatory phenotype20. The mechanism of action of adaptive Treg cells may not necessarily be restricted to suppressive cytokines. Indeed, human adaptive Treg cells (CD4+CD45RA+ T cells stimulated with CD3- and CD46-specific antibodies) have also been shown to express granzyme B and killing target cells in a perforin-dependent manner126. Treg cells often have a restricted specificity for particular cell types, tumours or foreign antigens127. Therefore, induced Treg cells may be ideally suited to respond to infectious agents. This may also be of particular importance in the GALT and in the tumour microenvironment where TGFβ drives the conversion of induced Treg cells118,128. A significant challenge in deciphering data from in vivo experiments is to assess the contribution of natural Treg cells versus induced Treg cells, and to determine whether inhibitory molecules, such as IL-10 or TGFβ, were derived from the former or the latter (or elsewhere).
Aberrant PD-L1 expression through 3′-UTR disruption in multiple cancers.
Successful treatment of many patients with advanced cancer using antibodies against programmed cell death 1 (PD-1; also known as PDCD1) and its ligand (PD-L1; also known as CD274) has highlighted the critical importance of PD-1/PD-L1-mediated immune escape in cancer development1, 2, 3, 4, 5, 6. However, the genetic basis for the immune escape has not been fully elucidated, with the exception of elevated PD-L1 expression by gene amplification and utilization of an ectopic promoter by translocation, as reported in Hodgkin and other B-cell lymphomas, as well as stomach adenocarcinoma6, 7, 8, 9, 10. Here we show a unique genetic mechanism of immune escape caused by structural variations (SVs) commonly disrupting the 3′ region of the PD-L1 gene. Widely affecting multiple common human cancer types, including adult T-cell leukaemia/lymphoma (27%), diffuse large B-cell lymphoma (8%), and stomach adenocarcinoma (2%), these SVs invariably lead to a marked elevation of aberrant PD-L1 transcripts that are stabilized by truncation of the 3′-untranslated region (UTR). Disruption of the Pd-l1 3′-UTR in mice enables immune evasion of EG7-OVA tumour cells with elevated Pd-l1 expression in vivo, which is effectively inhibited by Pd-1/Pd-l1 blockade, supporting the role of relevant SVs in clonal selection through immune evasion. Our findings not only unmask a novel regulatory mechanism of PD-L1 expression, but also suggest that PD-L1 3′-UTR disruption could serve as a genetic marker to identify cancers that actively evade anti-tumour immunity through PD-L1 overexpression.
Viruses are a dominant driver of protein adaptation in mammals.
Viruses interact with hundreds to thousands of proteins in mammals, yet adaptation against viruses has only been studied in a few proteins specialized in antiviral defense. Whether adaptation to viruses typically involves only specialized antiviral proteins or affects a broad array of virus-interacting proteins is unknown. Here, we analyze adaptation in ~1300 virus-interacting proteins manually curated from a set of 9900 proteins conserved in all sequenced mammalian genomes. We show that viruses (i) use the more evolutionarily constrained proteins within the cellular functions they interact with and that (ii) despite this high constraint, virus-interacting proteins account for a high proportion of all protein adaptation in humans and other mammals. Adaptation is elevated in virus-interacting proteins across all functional categories, including both immune and non-immune functions. We conservatively estimate that viruses have driven close to 30% of all adaptive amino acid changes in the part of the human proteome conserved within mammals. Our results suggest that viruses are one of the most dominant drivers of evolutionary change across mammalian and human proteomes.
Purdue scientists use adaptors to advance CAR-T therapy
Chimeric antigen receptor (CAR) T cells, developed in the 1990s, are a genetically engineered type of T cell that can target a specific cancer. Now, scientists at Purdue University say they’ve made improvements in this strategy–overcoming the several limitations of traditional CAR-T therapy.
Purdue professor of chemistry Philip Low and his team presented their findings at the American Association for Cancer Research meeting in New Orleans last month.
T cells are a type of immune cell that recognizes and clears the body of invading cells or pathogens, like cancer. They are fine-tuned by the immune system in order to specifically target and kill these foreign invaders–but cancer cells may respond by jumping these safety barriers.
CAR-T therapy was therefore proposed and has been recently used for cancer treatment. It has been hailed for its promising remission rates after early stage clinical trials for acute lymphoblastic leukemia.
“The problem is that the traditional engineered T-cell treatment can be too effective, sometimes killing tumor cells too fast and triggering a toxic reaction in a patient, and sometimes not stopping once the tumor has been destroyed and continuing to seek out and destroy healthy cells important to bodily functions,” Low said in a university news release. “We have found a potential way to control the engineered immune cells to overcome the limitations posed by CAR T-cell therapy.”
They did this by teaming up with Endocyte ($ECYT) scientist Haiyan Chu and designing CAR T cells that require activation by a small molecule adaptor before proceeding. In this way, they can carefully control the amount of active CAR T cells in the circulation.
So far, they have only tried the novel therapy in animal models, but when they tested it in mice they observed antitumor activity only when both the CAR T cells and the correct adaptor molecules were present.
Low believes it will allow clinicians to target multiple cancer subtypes at once. “Most tumors are heterogeneous and contain cancer cells that express different characteristics, including having different tumor-specific proteins on their surface,” he said in the release. “The cancer-targeting molecule on the adaptor we designed can be swapped out to target different molecules on other unrelated cancer cell surfaces. The idea is that a mixture of these adaptors can be given to a patient so that a single CAR T cell clone can be targeted to all of the relevant cancer subtypes in a patient.”
“In the past a new CAR T cell had to be designed for each desired cancer target,” Low said. “This system uses the same blind CAR T cell for all treatments. The adaptor molecule is what needs to be changed, and it is far easier to manipulate and swap pieces in and out of it than the T cells.”
A graphic depicting the activation and inactivation of CAR T cells through a small molecule adaptor is shown. Philip S. Low, Purdue’s Ralph C. Corley Distinguished Professor of Chemistry and director of the Purdue Center for Drug Discovery, and graduate student Yong Gu Lee led a team that designed new engineered CAR T cells that must be activated and targeted by a small molecule adaptor before they can kill cancer cells. The system has the potential to control the engineered cells to overcome existing limitations in CAR T-cell therapy. CREDIT Purdue University image courtesy of Yong Gu Lee
Purdue University researchers may have figured out a way to call off a cancer cell assassin that sometimes goes rogue and assign it a larger tumor-specific “hit list.”
T cells are the immune system’s natural defense against cancer and other harmful entities in the human body. However, the cells must be activated and taught by the immune system to recognize cancer cells in order to seek out and destroy them. Unfortunately, many types of cancer manage to thwart this process.
In the 1990s scientists found a way to genetically engineer T cells to recognize a specific cancer. These engineered T cells, called chimeric antigen receptor, or CAR, T cells, have been recently used as treatment for cancer, said Philip S. Low, Purdue’s Ralph C. Corley Distinguished Professor of Chemistry and director of the Purdue Center for Drug Discovery who led the work.
“The problem is that the traditional engineered T-cell treatment can be too effective, sometimes killing tumor cells too fast and triggering a toxic reaction in a patient, and sometimes not stopping once the tumor has been destroyed and continuing to seek out and destroy healthy cells important to bodily functions,” Low said. “We have found a potential way to control the engineered immune cells to overcome the limitations posed by CAR T-cell therapy.”
Low and Purdue graduate student Yong Gu Lee collaborated with Endocyte Inc. scientist Haiyan Chu to design genetically engineered CAR T cells that must be activated and targeted by a small molecule adaptor before they can kill cancer cells. The technology has been tested in animal models but no human trials have been performed. A poster presentation describing the work was presented Tuesday (April 19, 2016) at the American Association for Cancer Research annual meeting in New Orleans.
“While the traditional CAR T cells could remain and replicate in the human body for many years, the adaptors we have created are expected to be excreted fairly quickly,” Lee said. “By controlling the level of adaptors in the system, we can control the numbers and potencies of active CAR T cells. Those that aren’t stimulated by an adaptor molecule are blind and do not recognize or target any cells. Eventually, if they remain inactive for a while, they should die and be eliminated from the body.”
A study in mice showed the anti-tumor activity was induced only when both the engineered CAR T cell and the correct adaptor molecules were present.
The system also offers the potential to treat multiple cancer subtypes at once, Low said.
“Most tumors are heterogeneous and contain cancer cells that express different characteristics, including having different tumor-specific proteins on their surface,” he said. “The cancer-targeting molecule on the adaptor we designed can be swapped out to target different molecules on other unrelated cancer cell surfaces. The idea is that a mixture of these adaptors can be given to a patient so that a single CAR T cell clone can be targeted to all of the relevant cancer subtypes in a patient.”
The adaptor molecule serves as a bridge between the CAR T-cell and the cancer cell. It is made with a yellow dye called fluorescein isothiocyanate on one end, to which the engineered CAR T cells have been designed to bind, and a cancer-targeting molecule on the other.
Low’s research has focused on the design and synthesis of technologies for targeted delivery of therapeutic and imaging agents to treat cancer, inflammatory and autoimmune diseases, and infectious diseases.
He has developed molecules that target folate-receptors and prostate-specific membrane antigen on the surfaces of cancer cells. Approximately 85 percent of ovarian cancers; 80 percent of endometrial and lung cancers; and 50 percent of breast, kidney and colon cancers express folate receptors on their cellular surfaces. Prostate-specific membrane antigen receptors are found on nearly 90 percent of all prostate cancers. Other tumor-specific ligands developed by Low’s lab can target each of the other major human cancers, he said.
Each CAR T cell has thousands of receptors on its surface to which an adaptor molecule can bind. One CAR T cell could have a variety of adaptor molecules bound to its surface and the cancer cell it targets will depend on which of those adaptors first encounters a targeted cancer cell. Once the CAR T cell binds to a cancer cell, it begins the process of destroying it. When that process is complete, the CAR T cell is released and can bind to a new cancer cell, he said.
“In the past a new CAR T cell had to be designed for each desired cancer target,” Low said. “This system uses the same blind CAR T cell for all treatments. The adaptor molecule is what needs to be changed, and it is far easier to manipulate and swap pieces in and out of it than the T cells.”
In addition to Low, Chu and Lee, members of the research group include Purdue postdoctoral research associates at the time of the study Srinivasarao Tenneti and Ananda Kumar Kanduluru.
Drug discovery is one of the priorities within Purdue Moves, an initiative designed to broaden the university’s global impact and enhance educational opportunities for its students. All of the moves fall into four broad categories: science, technology, engineering and math (STEM) leadership; world-changing research; transformative education; and affordability and accessibility.
The Purdue University Center for Drug Discovery supports more than 100 faculty in six colleges with research focused on several major disease categories: cancer; diabetes, obesity and cardiovascular; immune and infectious disease; and neurological disorders and trauma.
The center and drug discovery initiative builds upon Purdue’s strengths along all points of the drug discovery pipeline, including 14 core units to provide shared resources for analysis, screening, synthesis and testing of potential therapeutic compounds.
With more than 44 Purdue-developed compounds at various stages of preclinical development, and 16 in human clinical trials, Purdue is among the most productive universities in the world of drug discovery.
The center also is aligned with the university’s recently announced $250 million investment in the life sciences.
Endocyte Inc., a Purdue Research Park-based company that develops receptor-targeted therapeutics for the treatment of cancer and autoimmune diseases, funded the study, holds exclusive rights to the technology and assisted Purdue researchers in the development of the technology. Low is a founder and chief science officer of Endocyte Inc. and serves on the Endocyte board of directors.
Yong Gu Lee, Haiyan Chu, Srinivasarao Tenneti, Ananda Kumar Kanduluru, Philip S. Low
Chimeric antigen receptor (CAR) T cells show significant potential for treating cancer due to their tumor-specific activation and ability to focus their killing activity on cells that express a tumor antigen. Unfortunately, this promising therapeutic technology is still limited by: (1) an inability to control the rate of cytokine release and tumor lysis; (2) the absence of an “off switch” that can terminate cytotoxic activity when tumor eradication is complete; (3) a failure to eliminate tumor cells that do not express the targeted antigen; and (4) a requirement to generate a different CAR T cell for each unique tumor antigen. In order to address these limitations, we have exploited a low molecular weight bi-specific adaptor molecule that must bridge between the CAR T cell and its targeted tumor cell by simultaneously binding to the chimeric antigen receptor on the CAR T cell and the unique antigen on the tumor. Using this bispecific adaptor, one can control CAR T cell cytotoxicity by adjusting the concentration and rate of administration of the adaptor. Because the half life of the adapter is <20 minutes in vivo, termination of CAR T cell killing can be accomplished by cessation of adapter administration. Moreover, when heterogeneous tumors containing cells that express orthogonal antigens must be treated, the same CAR T cell can be targeted to multiple antigens by attachment of the same CAR ligand to the appropriate selection of tumor-specific ligands. Finally, when the targeted tumor antigen is also expressed at low levels on normal cells, tumor specificity can be achieved by adjusting the affinity of the tumor-specific ligand to enable CAR T cell engagement only when a highly multivalent interaction is possible. To experimentally demonstrate the aforementioned benefits of using low molecular weight bispecific adaptors, CAR T cells were constructed by fusing an anti-fluorescein isothiocyanate (FITC) scFv to a CD3 zeta chain containing the intracellular domain of CD137 (i.e. CAR4-1BBZ T cells). Then, to enable their tumor-specific cytotoxicity, a bispecific adaptor molecule comprised of fluorescein linked to a small organic ligand with high affinity and specificity for a tumor-specific antigen (FITC-SMC) was synthesized. For these studies, the tumor-specific ligands were: i) folate for recognition of the folate receptor that is over-expressed on ~1/3 of human cancers, ii) DUPA for binding to prostate specific membrane antigen that is over-expressed on prostate cancers, and iii) NK-1R ligand that is over-expressed on neuroendocrine tumors. The ability of the same clone of CAR4-1BBZ T cells to eliminate tumors expressing each of the above antigens was then demonstrated by administration of the desired FITC-SMC to mice injected with the CAR4-1BBZ T cells. Our data show that anti-tumor activity: i) is only induced when both CAR4-1BBZ T cells and the correct antigen-specific FITC-SMC are present, ii) anti-tumor activity and toxicity can be sensitively controlled by adjusting the dosing of FITC-SMC, and iii) treatment of antigenically heterogeneous tumors can be achieved by administration of a mixture of the desired FITC-SMCs. Taken together, these data show that many of the limitations of CAR T cell technology can be addressed by use of a bi-specific adaptor molecule to mediate tumor cell recognition and killing.
CTLA-4 found in dendritic cells suggests New cancer treatment possibilities
Both dendritic cells and T cells are important in triggering the immune response, whereas antigen presenting dendritic cells act as the “general” leading T cells “soldiers” to chase and eliminate enemies in the battle against cancer. The well-known immune checkpoint break, CTLA-4, is believed to be present only in T cells (and cells of the same lineage). However, a new study published in Stem Cells and Development suggests that CTLA-4 also presents in dendritic cells. It further explores the mechanism on how turning off the dendritic cells in the immune response against tumors.
Dendritic Cell-Secreted Cytotoxic T-Lymphocyte-Associated Protein-4 Regulates the T-cell Response by Downmodulating Bystander Surface B7.
The remarkable functional plasticity of professional antigen-presenting cells (APCs) allows the adaptive immune system to respond specifically to an incredibly diverse array of potential pathogenic insults; nonetheless, the specific molecular effectors and mechanisms that underpin this plasticity remain poorly characterized. Cytotoxic T-lymphocyte-associated protein-4 (CTLA-4), the target of the blockbuster cancer immunotherapeutic ipilimumab, is one of the most well-known and well-studied members of the B7 superfamily and negatively regulates T cell responses by a variety of known mechanisms. Although CTLA-4 is thought to be expressed almost exclusively among lymphoid lineage hematopoietic cells, a few reports have indicated that nonlymphoid APCs can also express the CTLA-4 mRNA transcript and that transcript levels can be regulated by external stimuli. In this study, we substantially build upon these critical observations, definitively demonstrating that mature myeloid lineage dendritic cells (DC) express significant levels of intracellular CTLA-4 that they constitutively secrete in microvesicular structures. CTLA-4(+) microvesicles can competitively bind B7 costimulatory molecules on bystander DC, resulting in downregulation of B7 surface expression with significant functional consequences for downstream CD8(+) T-cell responses. Hence, the data indicate a previously unknown role for DC-derived CTLA-4 in immune cell functional plasticity and have significant implication for the design and implementation of immunomodulatory strategies intended to treat cancer and infectious disease.
Non-invasive strategy to guide personalized cancer immunotherapy
Cancer immunotherapy is the rising hope to offer ultimate solutions for cancer. Neoantigens, derived from products of mutated genes in tumor cells, are found to be closely related to the efficacy of cancer immunotherapies. A non-invasive approach to identify unique, patient-specific neoantigens has been advanced by Dr. Steven Rosenberg’s group. A recent article published in Nature Medicine reported that a small population of circulating CD8+PD-1+ tumor-reactive T lymphocytes can be used to identify neoantigens, in addition to tumor-infiltrating T cells. The study paves the way for designing personalized cancer immunotherapy with a novel non-invasive approach.
Detection of lymphocytes that target tumor-specific mutant neoantigens-derived from products encoded by mutated genes in the tumor-is mostly limited to tumor-resident lymphocytes, but whether these lymphocytes often occur in the circulation is unclear. We recently reported that intratumoral expression of the programmed cell death 1 (PD-1) receptor can guide the identification of the patient-specific repertoire of tumor-reactive CD8(+) lymphocytes that reside in the tumor. In view of these findings, we investigated whether PD-1 expression on peripheral blood lymphocytes could be used as a biomarker to detect T cells that target neoantigens. By using a high-throughput personalized screening approach, we identified neoantigen-specific lymphocytes in the peripheral blood of three of four melanoma patients. Despite their low frequency in the circulation, we found that CD8(+)PD-1(+), but not CD8(+)PD-1(-), cell populations had lymphocytes that targeted 3, 3 and 1 unique, patient-specific neoantigens, respectively. We show that neoantigen-specific T cells and gene-engineered lymphocytes expressing neoantigen-specific T cell receptors (TCRs) isolated from peripheral blood recognized autologous tumors. Notably, the tumor-antigen specificities and TCR repertoires of the circulating and tumor-infiltrating CD8(+)PD-1(+) cells appeared similar, implying that the circulating CD8(+)PD-1(+) lymphocytes could provide a window into the tumor-resident antitumor lymphocytes. Thus, expression of PD-1 identifies a diverse and patient-specific antitumor T cell response in peripheral blood, providing a novel noninvasive strategy to develop personalized therapies using neoantigen-reactive lymphocytes or TCRs to treat cancer.
PD-1 identifies the patient-specific CD8+ tumor-reactive repertoire infiltrating human tumors
Adoptive transfer of tumor-infiltrating lymphocytes (TILs) can mediate regression of metastatic melanoma; however, TILs are a heterogeneous population, and there are no effective markers to specifically identify and select the repertoire of tumor-reactive and mutation-specific CD8+ lymphocytes. The lack of biomarkers limits the ability to study these cells and develop strategies to enhance clinical efficacy and extend this therapy to other malignancies. Here, we evaluated unique phenotypic traits of CD8+ TILs and TCR β chain (TCRβ) clonotypic frequency in melanoma tumors to identify patient-specific repertoires of tumor-reactive CD8+lymphocytes. In all 6 tumors studied, expression of the inhibitory receptors programmed cell death 1 (PD-1; also known as CD279), lymphocyte-activation gene 3 (LAG-3; also known as CD223), and T cell immunoglobulin and mucin domain 3 (TIM-3) on CD8+ TILs identified the autologous tumor-reactive repertoire, including mutated neoantigen-specific CD8+ lymphocytes, whereas only a fraction of the tumor-reactive population expressed the costimulatory receptor 4-1BB (also known as CD137). TCRβ deep sequencing revealed oligoclonal expansion of specific TCRβ clonotypes in CD8+PD-1+ compared with CD8+PD-1– TIL populations. Furthermore, the most highly expanded TCRβ clonotypes in the CD8+ and the CD8+PD-1+ populations recognized the autologous tumor and included clonotypes targeting mutated antigens. Thus, in addition to the well-documented negative regulatory role of PD-1 in T cells, our findings demonstrate that PD-1 expression on CD8+ TILs also accurately identifies the repertoire of clonally expanded tumor-reactive cells and reveal a dual importance of PD-1 expression in the tumor microenvironment.
Cancer immunotherapy has experienced major progress in the last decade. Adoptive transfer of ex vivo–expanded tumor-infiltrating lymphocytes (TILs) can cause substantial regression of metastatic melanoma (1, 2). Blockade of the interaction of cytotoxic T lymphocyte antigen 4 (CTLA-4; also known as CD152) or programmed cell death 1 receptor (PD-1; also known as CD279) with their ligands using blocking antibodies alone or in combination have been shown to unleash an otherwise-ineffective immune response against melanoma (3–7), renal cell carcinoma (3), and non–small cell lung cancer (3). The antitumor responses observed in these clinical trials support the presence of naturally occurring tumor-reactive CD8+ T cells and their immunotherapeutic potential. In the particular case of TIL therapy, persistence of transferred tumor-specific T cell clones is associated with tumor regression (8). Moreover, retrospective clinical studies have shown an association of autologous tumor recognition by TILs and clinical response (9, 10), which suggests that enrichment of tumor-reactive cells could enhance clinical efficacy. However, the identification of the diverse repertoire of tumor-reactive cells limits the ability to study these cells, enhance clinical efficacy, and extend this therapy to other malignancies.
Melanoma TILs represent a heterogeneous population that can target a variety of antigens, including melanocyte differentiation antigens, cancer germline antigens, self-antigens overexpressed by the tumor, and mutated tumor neoantigens (11). The latter appear to be of critical importance for the antitumor responses observed after transfer of TILs, given the substantial regression of metastatic melanoma in up to 72% of patients in phase 2 clinical trials, in the absence of any autoimmune side effects in the great majority of patients (2). This contrasts with the modest antitumor activity but high prevalence of severe autoimmune manifestations observed after transfer of peripheral blood gene-engineered T cells expressing TCRs targeting shared melanocyte differentiation antigens MART1 and gp100 (12,13). Furthermore, T cells targeting mutated neoepitopes are not subject to negative selection in the thymus and may constitute the predominant naturally occurring tumor-reactive population in cancer patients. In support of this notion, a recent study reported the frequent detection and dominance of T cell populations targeting mutated epitopes in melanoma-derived TILs (14). Conversely, T cells targeting shared melanocyte differentiation antigens and cancer germline antigens in bulk melanoma TILs were represented at a strikingly low frequency (15). These findings have shifted our interest from the more accessible and commonly studied T cells targeting melanocyte differentiation antigens to T cells targeting unique patient-specific mutations. However, the often rare availability of autologous tumor cell lines necessary to study these reactivities, and the hurdles associated with the identification of the unique mutations targeted, have thus far hindered immunobiological studies of these T cell populations in the tumor.
Naturally occurring tumor-reactive cells are exposed to their antigen at the tumor site. Thus, the immunobiological characterization of T cells infiltrating tumors represents a unique opportunity to study their function and to identify the patient-specific repertoire of tumor-reactive cells. TCR stimulation triggers simultaneous upregulation of both costimulatory and coinhibitory receptors, which can either promote or inhibit T cell activation and function. Expression of the inhibitory receptors PD-1, CTLA-4, lymphocyte-activation gene 3 (LAG-3; also known as CD223), and T cell immunoglobulin and mucin domain 3 (TIM-3) is regulated in response to activation and throughout differentiation (16, 17). Chronic antigen stimulation has been shown to induce coexpression of inhibitory receptors and is associated with T cell hyporesponsiveness, termed exhaustion (18). Exhaustion in response to persistent exposure to antigen was first delineated in a murine model of chronic lymphocytic choriomeningitis virus (19), but has been observed in multiple human chronic viral infections (20–22) as well as in tumor-reactive MART1-specific TILs (23, 24), and has provided the rationale for restoring immune function using immune checkpoint blockade. Conversely, 4-1BB (also known as CD137) is a costimulatory member of the TNF receptor family that has emerged as an important mediator of survival and proliferation, particularly in CD8+ T cells (25–27). 4-1BB is transiently expressed upon TCR stimulation, and its expression has been used to enrich for antigen-specific T cells in response to acute antigen stimulation (28). However, expression of this marker has not been extensively explored in CD8+ lymphocytes infiltrating human tumors. In addition to changes in the expression of cosignaling receptors on the surface of T cells, antigen-specific stimulation typically results in clonal expansion. TCR sequence immunoprofiling can be used to monitor T cell responses to a given immune challenge even without a priori knowledge of the specific epitope targeted, through determination of the abundance of specific clonotypes (29, 30). However, there is limited knowledge regarding the TCR repertoire and the frequency of tumor-reactive clonotypes infiltrating human tumors.
We hypothesized that the assessment of unique phenotypic traits expressed by CD8+ TILs and TCR β chain (TCRβ; encoded by TRB) clonotypic immunoprofiling of lymphocytes infiltrating the tumor could provide a powerful platform to study antitumor T cell responses and evaluated their usefulness in identifying the diverse repertoire of tumor-reactive cells. Despite the accepted negative regulatory role of PD-1 in T cells, our findings establish that expression of PD-1 on CD8+ melanoma TILs accurately identifies the repertoire of clonally expanded tumor-reactive, mutation-specific lymphocytes and suggest that cells derived from this population play a critical role in tumor regression after TIL administration.
PD-1 was initially described to be expressed on a T cell hybridoma undergoing cell death (37). Its negative effect on T cell responses was first delineated in PD-1 knockout mice (38, 39). Since then, PD-1 expression and coexpression of other inhibitory receptors such as CTLA-4, TIM-3, BTLA, CD160, LAG-3, and 2B4 have become a hallmark of chronically stimulated T cells during chronic infection or in the tumor microenvironment. This altered phenotype, and the interaction of these receptors with their corresponding ligands on target cells, is associated with impaired proliferation and effector function frequently referred to as exhaustion (18, 24, 40). Expression of PD-1 in patients with chronic viral infections correlates with disease progression (22, 41). Additionally, CD8+ lymphocytes targeting melanoma differentiation antigens in the tumor express PD-1, CTLA-4, TIM-3, and LAG-3 and exhibit impaired IFN-γ and IL-2 secretion (23, 24), supporting a negative regulatory role of PD-1 and inhibitory receptors in naturally occurring T cell responses to cancer and providing a rationale for the treatment of cancer with immune checkpoint inhibitors.
In the present study, we found that expression of PD-1 on CD8+ melanoma TILs captured the diverse repertoire of clonally expanded tumor-reactive lymphocytes. TCRβ sequencing revealed that tumor-reactive and mutation-specific clonotypes were highly expanded in the CD8+ population and preferentially expanded in the PD-1+ population. This is consistent with the TCR stimulation-driven expression of this receptor on T cells (42). The inhibitory receptors TIM-3 and LAG-3 and the costimulatory receptor 4-1BB were also expressed on CD8+PD-1+ TILs and could also be used to enrich for tumor-reactive cells. PD-1 was consistently expressed at a higher frequency and was found to be more comprehensive at identifying the diverse repertoire of tumor-reactive cells infiltrating melanoma tumors, although the less frequent PD-1–/TIM-3+ and PD-1–/LAG-3+ subpopulations could also represent tumor-reactive cells (Supplemental Figure 4 and Supplemental Table 6). Additionally, previous studies from our laboratory showing coexpression of PD-1 and CTLA-4 (23), and our preliminary data supporting coexpression of PD-1 and ICOS (Supplemental Figure 5), suggest that other receptors may also be used to distinguish tumor-reactive cells. Our present results further support immunotherapeutic intervention using immune checkpoint blockade using PD-1, TIM-3, and LAG-3 blocking antibodies or 4-1BB agonistic antibody to restore the function of tumor-reactive lymphocytes, which is currently being actively pursued in the clinic (3, 4, 6, 7, 43). The potential cooperative mechanisms of inhibition of these receptors when engaged with their ligands (44, 45) suggests that the combined targeting of different inhibitory receptors can further enhance antitumor efficacy, as already shown with the combination of anti–PD-1 and anti–CTLA-4 (5). Our present results demonstrate that PD-1 identifies the clonally expanded CD8+ tumor-reactive population and suggest that expression of PD-1 on CD8+TILs could function as a potential predictive biomarker of antitumor efficacy using immune checkpoint inhibitors.
Naturally occurring tumor-reactive cells play a pivotal role in mediating antitumor responses after TIL transfer. Currently, expansion of TILs for patient treatment involves nonspecific growth of TILs from tumor fragments in IL-2, and the diversity and frequency of antitumor T cells present in the final T cell product used for treatment remains largely uncharacterized. Prospective clinical studies have reported that in vitro recognition of autologous tumor by TILs is associated with a higher probability of clinical response (9, 10), which suggests that enrichment of tumor-reactive cells could enhance clinical efficacy. This is consistent with the idea that both tumor-reactive and non–tumor-reactive cells may compete for cytokines in vivo, especially in the absence of vaccination. However, the isolation of the patient-specific repertoire of tumor-reactive cells is not possible with current technologies (14, 28, 46–50). Our findings established that expression of PD-1, TIM-3, LAG-3, and 4-1BB in CD8+ TILs can be used to enrich for tumor-reactive cells, regardless of the specific antigen targeted. One potential concern with isolating T cells expressing inhibitory receptors for therapy is that these cells may be exhausted or functionally impaired (23, 24, 44, 51, 52). However, we found that PD-1+, TIM-3+, and LAG-3+ CD8+ cells expanded in IL-2 were capable of secreting IFN-γ and lyse tumor in vitro. This supports the notion that immune dysfunction associated with coexpression of inhibitory receptors on CD8+ TILs can be reversed (21, 41, 51, 53), and may enable the reproducible enrichment of tumor-reactive cells for patient treatment. Notably, in a preliminary experiment (n= 8 nonresponders; 14 responders), there was no association between the frequency of expression of any of the markers studied in the CD8+ TILs in the fresh tumor and the clinical response to TILs derived from these tumor samples. However, the fresh tumors included in this study belonged to patients treated in several TIL protocols over the course of 10 years, and TILs were generated from these tumors using different methods, which makes these data difficult to interpret. In addition, the frequency of cells initially expressing PD-1 in the tumor may not reflect the frequency of the PD-1 derived cells in the infusion bag. For example, a low frequency of PD-1+ cells may be highly enriched during the process of TIL culture as a result of the presence of tumor cells. Although in vivo antitumor activity of tumor-isolated TILs based on PD-1 expression requires testing in a clinical trial, the observation that the overwhelming majority of tumor-reactive cells were derived from cells expressing PD-1 suggests that cells expressing PD-1 and inhibitory receptors in the tumor play a critical role in tumor regression after TIL administration.
The functional implications of selecting PD-1–, LAG-3–, TIM-3–, or 4-1BB–expressing T cells to enrich for tumor-reactive cells for patient treatment remain unclear. Although previous studies have reported differential expression of PD-1, LAG-3, and TIM-3 throughout differentiation (17), or preferential expression of TIM-3 in IFN-γ–secreting cells (54), our preliminary results have failed to show consistent phenotypic or functional differences between PD-1+, LAG-3+, TIM-3+, and 4-1BB+ selected TILs, including cytokine secretion, proliferation, and susceptibility to apoptosis (data not shown). We found that PD-1 expression was almost completely lost in the PD-1+ derived populations upon in vitro culture in IL-2. Conversely, TIM-3 and LAG-3 expression increased in the TIM-3– and LAG-3– populations after expansion. Overall, there were no differences in the expression of PD-1, TIM-3, or LAG-3 between any the populations after expansion. Thus, in agreement with previous reports (55, 56), we conclude that expansion in IL-2 alters the expression of these markers and compromises the potential use of inhibitory receptors to select for tumor-reactive cells after in vitro expansion. Recent work in animal models suggests that chronic antigen stimulation (57–59) or a tolerizing microenvironment (60) may lead to permanent epigenetic changes in T cells, raising the possibility that the restoration of function observed in previously exhausted or tolerized cells in presence of cytokines may only be transient. These results have not yet been corroborated in human tumor-specific cells. However, given that the overwhelming majority of tumor-reactive cells appear to derive from cells expressing PD-1 in the tumor, studying permanent versus transient reversion of exhaustion may have important implications for adoptive cell transfer of TILs.
Tumor-reactive cells can also be found infiltrating other tumor malignancies, such as renal cell carcinoma (61) or ovarian (62), cervical (63), or gastrointestinal tract cancers (64), albeit at lower frequencies. Our findings provide alternatives to enrich and study tumor-reactive CD8+ TILs through selection of cells expressing the cell surface receptors PD-1, LAG-3, TIM-3, and 4-1BB, a hypothesis that we are actively investigating. Additionally, our present findings showed that the frequency of a specific clonotype in the CD8+ and PD-1+ populations can be used to predict its ability to recognize tumor and isolate tumor-specific TCRs, thus providing means to overcome potential irreversible functional impairments of TILs (52).
2 reports with opposing results have generated controversy regarding which may be the optimal marker for the identification of the tumor-reactive repertoire, PD-1 or 4-1BB. In one report studying PD-1 expression in the tumor, the authors showed promising although inconsistent ability to enrich for shared melanoma-reactive cells (55). In a more recent article studying the role of 4-1BB in fresh ovarian TILs, Ye et al. concluded that expression of 4-1BB, but not PD-1, on lymphocytes defines the population of tumor-reactive cells in the tumor (65). The results of Ye et al. appear to contradict our present findings, showing that expression of PD-1 rather than 4-1BB more comprehensively identifies the repertoire of tumor-reactive cells in the tumor. However, these inconsistencies can be explained by different experimental approaches undertaken to study the immunobiology of TILs. First, Ye et al. found that expression of 4-1BB in fresh ovarian TILs and tumor-associated lymphocytes was low, and thus exposed the tumor to IL-7 and IL-15 (65). In the 1 patient sample in which the authors enriched for tumor-reactive cells from fresh ovarian TILs or tumor-associated lymphocytes exposed to IL-7 and IL-15, expression of 4-1BB was dependent on in vitro activation, but no longer represented the natural expression of 4-1BB in the fresh tumor. Second, with the exception of the 1 experiment described above, the enrichment experiments reported were carried out with melanoma or ovarian TIL lines expanded in IL-2 and cocultured with tumor cell lines in vitro. It is well known that IL-2 can change the activation status and also the expression of inhibitory receptors on T cells (data not shown and ref. 56). Thus, the experiment comparing expression of PD-1 and 4-1BB performed by Ye et al. (65) addressed the significance of these receptors after in vitro coculture of a highly activated melanoma TIL line with a tumor cell line, rather than the role of PD-1 and 4-1BB expression in CD8+ lymphocytes in the fresh tumor. Finally, both Inozume et al. and Ye et al. used matched HLA-A2 cell lines to assess tumor reactivity (55, 65). However, the use of HLA-matched tumor cell lines does not enable the assessment of reactivities against unique mutations that are present only in the autologous tumor cell line. In our current study, we used fresh melanoma tumors for all our experiments, and these were rested in the absence of cytokines to preserve the phenotype of TILs. Moreover, we used autologous tumor cell lines to assess tumor recognition. We believe that our experimental approach overcomes the limitations described above, enabling us to conclude that tumor-reactive cells can be detected in both the PD-1+/4-1BB+ and PD-1+/4-1BB– CD8+ TIL populations.
In summary, expression of PD-1 in CD8+ TILs in the fresh tumor identified and selected for the diverse patient-specific repertoire of tumor-reactive cells, including mutation-specific cells. In addition, analysis of the CD8+ TIL TCRβ repertoire in 2 melanomas showed that the frequency of a specific TCRβ clonotype in the CD8+ and PD-1+ populations could be used to predict its ability to recognize the autologous tumor. The use of inhibitory receptors and the frequency of individual TCRs to prospectively identify and select the diverse repertoire of tumor-reactive cells holds promise for the personalized treatment of cancer with T cell therapies, but may also facilitate the dissection and understanding of the immune response in human cancer patients.
Anti-PD-1 is poised to be a blockbuster, which other immune-checkpoint targeting drugs are on the horizon?
Clinical studies of anti-immune-checkpoint protein therapeutics have shown not only an improved overall survival, but also a long-term durable response, compared to chemotherapy and genomically-targeted therapy. To expand the success of immune-checkpoint therapeutics into more tumor types and improving efficacy in difficult-to-treat tumors, additional targets involved in checkpoint-blockade need to be explored, as well as testing the synergy between combining approaches.
Currently, CTLA-4 and PD-1/PD-L1 are furthest along in development, and have shown very promising results in metastatic melanoma patients. This is just a fraction of targets involved in the checkpoint-blockade pathway. Several notable targets include:
LAG-3 – Furthest along in clinical development with both a fusion protein and antibody approach, antibody apporach being tested in combination with anti-PD-1
TIM-3 – Also in clinical development. Pre-clinical studies indicate that it co-expresses with PD-1 on tumor-infiltrating lymphocytes. Combination with anti-PD-improves anti-tumor response
VISTA – Antibody targeting VISTA was shown to improve anti-tumor immune response in mice
In addition, there are also co-stimulatory factors that are also being explored as viable therapeutic targets
OX40 – Both OX40 and 4-1BB are part of the TNF-receptor superfamily. Phase I data shows acceptable safety profile, and evidence of anti-tumor response in some patients
4-1BB – Phase I/II data on an antibody therapeutic targeting OX40 shows promising clinical response for melanoma, renal cell carcinoma and ovarian cancer.
Inducible co-stimulator (ICOS) – Member of the CD28/B7 family. Its expression was found to increase upon T-cell activation. Anti-CTLA-4 therapy increases ICOS-positive effector T-cells, indicating that it may work in synergy with anti-CTLA-4. Clinical trials of anti-ICOS antibody are planned for 2015.
Targeting single immune-checkpoint proteins has proven to be clinically effective at treating specific tumor types; can targeting two different proteins synergize effects?
Despite the success of targeting immune-checkpoint proteins, such as CTLA-4, PD-1, LAG-3, TIM-3 among others, percentages of patient response vary and rarely exceed 50%. It is highly tempting to speculate a strategy of dual-targeting of these checkpoint proteins. A recent presentation at the Keystone Symposium for Tumor Immunology: Multidisciplinary Science Driving Combination Therapy detailed findings of dual-targeting two immune-checkpoint proteins in mouse tumor models. Their key findings are summarized below:
Dual-targeting PD-1 and LAG-3 demonstrates superior efficacy over blocking either target alone
In addition to previous reported data on superior dual-targeting efficacy against fibrosarcoma (Sa1N) and colorectal adenosarcoma (MC38) tumor types1, anti-tumor activity against myeloma (SC J558L) and B-cell lymphoma (A20) hematological tumor types were also reported to be effacious.2
These exciting pre-clinical findings may result in further exploration of dual-targeting antibodies in the clinic, either as combination of existing antibody therapies, or as a new bi-specific antibody therapeutic.
Camelid single domain antibodies are a novel bi-specific antibody platform that may be used to develop a new generation of dual-targeting antibodies against multiple immune-checkpoint proteins.
New insight behind the success of fighting cancer by targeting immune checkpoint proteins
Immune checkpoint blockade has proven to be highly successful in the clinic at treating aggressive and difficult-to-treat forms of cancer. The mechanism of the blockade, targeting CTLA-4 and PD-1 receptors which act as on/off switches in T cell-mediated tumor rejection, is well understood. However, little is known about the tumor antigen recognition profile of these affected T-cells, once the checkpoint blockade is initiated.
In a recent published study, the authors used genomics and bioinformatics approaches to identify critical epitopes on 3-methylcholanthrene induced sarcoma cell lines, d42m1-T3 and F244. CD8+ T cells in anti-PD-1 treated tumor bearing mice were isolated and fluorescently labeled with tetramers loaded with predicted mutant epitopes. Out of 66 predicted mutants, mLama4 and mAlg8 were among the highest in tetramer-positive infiltrating T-cells. To determine whether targeting these epitopes alone would yield similar results as anti-PD-1 treatment, vaccines against these two epitopes were developed and tested in mice. Prophylactic administration of the combined vaccine against mLama4 and mAlg8 yielded an 88% survival in tumor bearing mice, thus demonstrating that these two epitopes are the major antigenic targets from checkpoint-blockade and therapies against these two targets are similarly efficacious.
In addition to understanding the mechanism, identification of these tumor-specific mutant antigens is the first step in discovering the next wave of cancer immunotherapies via vaccines or antibody therapeutics. Choosing the right antibody platform can speed the discovery of a new therapeutics against these new targets. Single domain antibodies have the advantage of expedited optimization, flexibility of incorporating multiple specificity and functions, superior stability, and low COG over standard antibody approaches.
Myeloid-derived-suppressor cells as regulators of the immune system
Dmitry I. Gabrilovich and Srinivas Nagaraj Nat Rev Immunol. 2009 March ; 9(3): 162–174. http://dx.doi.org:/10.1038/nri2506
Myeloid-derived suppressor cells (MDSCs) are a heterogeneous population of cells that expands during cancer, inflammation and infection, and that has a remarkable ability to suppress T-cell responses. These cells constitute a unique component of the immune system that regulates immune responses in healthy individuals and in the context of various diseases. In this Review, we discuss the origin, mechanisms of expansion and suppressive functions of MDSCs, as well as the potential to target these cells for therapeutic benefit.
The first observations of suppressive myeloid cells were described more than 20 years ago in patients with cancer1-3. However, the functional importance of these cells in the immune system has only recently been appreciated due to accumulating evidence that has demonstrated their contribution to the negative regulation of immune responses during cancer and other diseases. It is now becoming increasingly clear that this activity is contained within a population known as myeloid-derived suppressor cells (MDSCs). Features common to all MDSCs are their myeloid origin, immature state and a remarkable ability to suppress T-cell responses (Box 1). In addition to their suppressive effects on adaptive immune responses, MDSCs have also been reported to regulate innate immune responses by modulating the cytokine production of macrophages4. Non-immunological functions of MDSC have also been described, such as the promotion of tumour angiogenesis, tumour-cell invasion and metastasis. However, as a discussion of these aspects of MDSC biology is beyond the scope of this article, the reader is referred to another recent Review on this topic5.
MDSCs represent an intrinsic part of the myeloid-cell lineage and are a heterogeneous population that is comprised of myeloid-cell progenitors and precursors of myeloid cells. In healthy individuals, immature myeloid cells (IMCs) generated in bone marrow quickly differentiate into mature granulocytes, macrophages or dendritic cells (DCs). In pathological conditions such as cancer, various infectious diseases, sepsis, trauma, bone marrow transplantation or some autoimmune disorders, a partial block in the differentiation of IMCs into mature myeloid cells results in an expansion of this population. Importantly, the activation of these cells in a pathological context results in the upregulated expression of immune suppressive factors such as arginase (encoded by ARG1) and inducible nitric oxide synthase (iNOS; also known as NOS2) and an increase in the production of NO (nitric oxide) and reactive oxygen species (ROS). Together, this results in the expansion of an IMC population that has immune suppressive activity; these cells are now collectively known as MDSCs. In this
Origin and subsets of MDSCs It is important to note that MDSCs that are expanded in pathological conditions (see later) are not a defined subset of myeloid cells but rather a heterogeneous population of activated IMCs that have been prevented from fully differentiating into mature cells. MDSCs lack the expression of cell-surface markers that are specific for monocytes, macrophages or DCs and are comprised of a mixture of myeloid cells with granulocytic and monocytic morphology6. Early studies showed that 1–5% of MDSCs are able to form myeloid-cell colonies7-9 and that about one third of this population can differentiate into mature macrophages and DCs in the presence of appropriate cytokines in vitro and in vivo7-9. In mice, MDSCs are characterized by the co-expression of the myeloid lineage differentiation antigen Gr1 (also known as Ly6G) and CD11b (also known as αM-integrin)10. Normal bone marrow contains 20–30% of cells with this phenotype, but these cells make up only a small proportion (2–4%) of spleen cells and are absent from the lymph nodes in mice (Fig. 1). In humans, MDSCs are most commonly defined as CD14-CD11b+ cells or, more narrowly, as cells that express the common myeloid marker CD33 but lack the expression of markers of mature myeloid and lymphoid cells and the MHC-class-II molecule HLA-DR11, 12. MDSCs have also been identified within a CD15+ population in human peripheral blood13. In healthy individuals, immature myeloid cells with described above phenotype comprise ∼0.5% of peripheral blood mononuclear cells.
Recently, the morphological heterogeneity of these cells has been defined more precisely in part based on their expression of Gr1. Notably, Gr1-specific antibodies bind to both Ly6G and Ly6C, which are encoded by separate genes. However, these epitopes are recognized by different antibodies specific for each individual epitopes: anti-Ly6C and anti-Ly6G. Granulocytic MDSCs have a CD11b+Ly6G+Ly6Clow phenotype, whereas MDSCs with monocytic morphology are CD11b+Ly6G-Ly6Chigh 6,14. Importantly, evidence indicates that these two subpopulations may have different functions in cancer and infectious and autoimmune diseases15-17. During the analysis of ten different experimental tumour models, we found that both of these subsets of MDSCs were expanded. In most cases, however, the expansion of the granulocytic MDSC population was much greater than that of the monocytic subset6 and, interestingly, the two subpopulations used different mechanisms to suppress Tcell function (see later). In addition, the ability to differentiate into mature DCs and macrophages in vitro has been shown to be restricted to monocytic MDSCs6.
In recent years, several other surface molecules have been used to identify additional subsets of suppressive MDSCs, including CD80 (also known as B7.1)18, CD115 (the macrophage colony-stimulating factor receptor)19, 20 and CD124 (the IL-4 receptor α-chain)20. In our own studies, we observed that many MDSCs in tumour-bearing mice co-express CD115 and CD1246; however, direct comparison of MDSCs from tumour-bearing mice and Gr1+CD11b+ cells from naive mice showed that they expressed similar levels of CD115 and CD124. In addition, sorted CD115+ or CD124+ MDSCs from EL-4 tumour-bearing mice had the same ability to suppress T-cell proliferation on a per cell basis as did CD115- or CD124-MDSCs. This suggests that, although these molecules are associated with MDSCs, they might not be involved in the immunosuppressive function of these cells in all tumour models.
Overall, current data suggest that MDSCs are not a defined subset of cells but rather a group of phenotypically heterogeneous myeloid cells that have common biological activity.
MDSCs in pathological conditions MDSCs were first characterized in tumour-bearing mice or in patients with cancer. Inoculation of mice with transplantable tumour cells, or the spontaneous development of tumours in transgenic mice with tissue-restricted oncogene expression, results in a marked systemic expansion of these cells (Fig. 1 and Table 1). In addition, up to a tenfold increase in MDSC numbers was detected in the blood of patients with different types of cancer11, 12, 21, 22. In many mouse tumour models, as many as 20–40% of nucleated splenocytes are represented by MDSCs (in contrast to the 2-4% seen in normal mice). In addition, these cells are found in tumour tissues and in the lymph nodes of tumour-bearing mice.
Although initial observations and most of the current information regarding the role of MDSCs in immune responses has come from studies in the cancer field, accumulating evidence has shown that MDSCs also regulate immune responses in bacterial and parasitic infections, acute and chronic inflammation, traumatic stress, surgical sepsis and transplantation. A systemic expansion of both the granulocytic and monocytic subset of MDSCs was observed in mice primed with Mycobacterium tuberculosis as part of complete Freund’s adjuvant (CFA). Acute Trypanosoma cruzi infection, which induces T-cell activation and increased production of interferon-γ (IFNγ), also leads to the expansion of MDSCs23, 24. A similar expansion of MDSCs has been reported during acute toxoplasmosis25, polymicrobial sepsis26, acute infection with Listeria monocytogenes or chronic infection with Leishmania major27 and infection with helminths28,29, 30, Candida albicans31 or Porphyromonas gingivalis32.
MDSC expansion is also associated with autoimmunity and inflammation. In experimental autoimmune encephalomyelitis (EAE), a mouse model of multiple sclerosis, an increase in CD11b+Ly6ChiLy6G− MDSCs was observed in the spleen and blood and these cells were found to enter the central nervous system during the inflammatory phase of the disease16. A significant increase in the number of MDSCs was also detected in experimental autoimmune uveoretinitis, an animal model of human intraocular inflammatory disease33, in the skin and spleens of mice that were repeatedly treated with a contact sensitizer to induce an inflammatory response34 and in inflammatory bowel diseases35. MDSCs were also found to infiltrate the spleen and suppress T-cell function in a model of traumatic stress36. Finally, a significant transient increase in MDSC numbers was also demonstrated in normal mice following immunization with different antigens such as ovalbumin or peptide together with CFA, a recombinant vaccinia virus expressing interleukin-2 (IL-2) or staphylococcal enterotoxin A 8, 37, 38. Therefore, current information clearly indicates that the expansion of an immunosuppressive MDSC population is frequently observed in many pathological conditions.
Expansion and activation of MDSCs Studies have demonstrated that the MDSC population is influenced by several different factors (Table 1), which can be divided into two main groups. The first group includes factors that are produced mainly by tumour cells and promote the expansion of MDSC through stimulation of myelopoiesis and inhibiting of the differentiation of mature myeloid cells. The second group of factors is produced mainly by activated T cells and tumour stroma, and is involved in directly activating MDSCs. Mechanisms of MDSC expansion—Factors that induce MDSC expansion can include cyclooxygenase-2 (COX2), prostaglandins 39-41, stem-cell factor (SCF)39, macrophage colony-stimulating factor (M-CSF), IL-642, granulocyte/macrophage colony-stimulating factor (GM-CSF)41 and vascular endothelial growth factor (VEGF) 43 (Table 1). The signalling pathways in MDSCs that are triggered by most of these factors converge on Janus kinase (JAK) protein family members and signal transducer and activator of transcription 3 (STAT3) (Fig. 2), which are signalling molecules that are involved in cell survival, proliferation, differentiation and apoptosis44. STAT3 is arguably the main transcription factor that regulates the expansion of MDSCs. MDSCs from tumour-bearing mice have markedly increased levels of phosphorylated STAT3 compared with IMCs from naive mice45. Exposure of haematopoietic progenitor cells to tumour-cell-conditioned medium resulted in the activation of JAK2 and STAT3 and was associated with an expansion of MDSCs in vitro, whereas inhibition of STAT3 expression in haematopoietic progenitor cells abrogated the effect of tumour-derived factors on MDSC expansion46. Ablation of STAT3 expression in conditional knockout mice or selective STAT3 inhibitors markedly reduced the expansion of MDSCs and increased T-cell responses in tumour-bearing mice45, 47. STAT3 activation is associated with increased survival and proliferation of myeloid progenitor cells, probably through upregulated expression of STAT3 target genes including B-cell lymphoma XL, (BCL-XL), cyclin D1, MYC and survivin. So, abnormal and persistent activation of STAT3 in myeloid progenitors prevents their differentiation into mature myeloid cells and thereby promotes MDSC expansion.
Recent findings suggest that STAT3 also regulates MDSC expansion through inducing the expression of S100A8 and S100A9 proteins. In addition, it has been shown that MDSCs also express receptors for these proteins on their cell surface. S100A8 and S100A9 belong to the family of S100 calcium-binding proteins that have been reported to have an important role in inflammation48. STAT3-dependent upregulation of S100A8 and S100A9 expression by myeloid progenitor cells prevented their differentiation and resulted in the expansion of MDSCs in the spleens of tumor-bearing and naive S100A9-transgenic mice. By contrast, MDSCs did not expand in the peripheral blood and spleens of mice deficient for S100A9 following challenge with tumour cells or CFA49. In a different study, S100A8 and S100A9 proteins were shown to promote MDSC migration to the tumour site through binding to carboxylated N-glycan receptors expressed on the surface of these cells 50. Blocking the binding of S100A8 and S100A9 to their receptors on MDSCs in vivo with a carboxylated glycan-specific antibody reduced MDSC levels in the blood and secondary lymphoid organs of tumour-bearing mice50. In human colon tumour tissue, and in a mouse model of colon cancer, myeloid progenitor cells expressing S100A8 and S100A9 have been shown to infiltrate regions of dysplasia and adenoma. Furthermore, administration of a carboxylated glycan-specific monoclonal antibody (mAbGB3.1) was found to markedly reduced chronic inflammation and tumorigenesis51. Although the mechanisms involved require further study, these studies suggest that S100A9 and/or S100A8 proteins have a crucial role in regulating MDSC expansion, and may provide a link between inflammation and immune suppression in cancer.
Mechanisms of MDSC activation—Recently, it has become clear that the suppressive activity of MDSCs requires not only factors that promote their expansion but those that induce their activation. The expression of these factors, which are produced mainly by activated T cells and tumour stromal cells, is induced by different bacterial or viral products or as a result of tumour cell death 26. These factors, which include IFNγ, ligands for Toll-like receptors (TLRs), IL-13, IL-4 and transforming growth factor-β (TGFβ), activate several different signalling pathways in MDSCs that involve STAT6, STAT1, and nuclear factor-κB (NF-κB) (Fig. 2).
Blockade of IFNγ, which is produced by activated T cells, abolishes MDSC-mediated T-cell suppression17, 52. STAT1 is the major transcription factor activated by IFNγ-mediated signalling and, in the tumour microenvironment, the upregulation of ARG1 and iNOS expression in MDSCs involved a STAT1-dependent mechanism. Indeed, MDSCs from Stat1-/- mice failed to up regulate ARG1 and iNOS expression and therefore did not inhibit Tcell responses53. Consistent with other findings, IFNγ produced by activated T cells and by MDSCs triggered iNOS expression and synergized with IL-4Rα and ARG1 pathways that have been implicated in the suppressive function of MDSCs20.
An important role for the signalling pathway that involves IL-4 receptor α-chain (IL-4Rα) and STAT6 (which is activated by the binding of either IL-4 or IL-13 to IL-4Rα) in MDSC activation has been demonstrated in several studies. It has been shown that ARG1 expression is induced by culturing freshly isolated MDSCs or cloned MDSC lines with IL-454. In addition, IL-4 and IL-13 upregulate arginase activity, which increases the suppressive function of MDSCs55. In line with these observations, other experiments have shown that STAT6 deficiency prevents signalling downstream of the IL-4Rα and thereby blocks the production of ARG1 by MDSCs56. In addition, the IL-4Rα–STAT6 pathway was also found to be involved in IL-13-induced TGFβ1 production by MDSCs in mice with sarcoma, which resulted in decreased tumour immunosurveillance57. This could be regulated by neutralizing both TGFβ and IL-1357. However, in breast tumor model IL-4Rα knockout mice retain high levels of MDSC after surgery56. In a different study that evaluated the separate role of TGFβ (not involving study of IL-4Rα) TGFβ-specific blocking antibody failed to reverse T-cell anergy in B-cell lymphoma in vitro58. It is possible that, the IL4Rα–STAT6 pathway might not be involved in promoting tumour immunosuppression in all tumour models.
TLRs have a central role in the activation of innate immune responses. Polymicrobial sepsis induced by the ligation and puncture of the caecum, which releases microbial products into the peritoneum and systemic circulation, was shown to result in an expansion of the MDSC population in the spleen that was dependent on the TLR adaptor molecule myeloid differentiation primary-response gene 88 (MyD88)26. However, wild-type mice and mice lacking a functional TLR4 protein had comparable expansion of the MDSC during polymicrobial sepsis, which suggests that signalling through TLR4 is not required for MDSC expansion and that MyD88-dependent signalling pathways that are triggered by other TLRs probably contribute to the expansion of MDSCs in sepsis26. This indicates that the activation of MDSCs is a fundamental outcome of the host innate immune response to pathogens that express TLR ligands.
It is important to note that an increase in the production and/or recruitment of IMCs in the context of acute infectious diseases or following vaccination does not necessarily represent an expansion of an immunosuppressive MDSC population. It is likely that under pathological conditions, the expansion of a suppressive MDSC population is regulated by two different groups of factors that have partially overlapping activity: those that induce MDSC expansion and those that induce their activation (which leads to increased levels of ROS, arginase, and/ or NO). This two-tiered system may allow for flexibility in the regulation of these cells under physiological and pathological conditions.
Mechanisms of MDSC suppressive activity Most studies have shown that the immunosuppressive functions of MDSCs require direct cell– cell contact, which suggests that they act either through cell-surface receptors and/or through the release of short-lived soluble mediators. The following sections describe the several mechanisms that have been implicated in MDSC-mediated suppression of T-cell function.
Arginase and iNOS—Historically, the suppressive activity of MDSCs has been associated with the metabolism of L-arginine. L-arginine serves as a substrate for two enzymes: iNOS, which generates NO, and arginase, which converts L-arginine into urea and L-ornithine. MDSCs express high levels of both arginase and iNOS, and a direct role for both of these enzymes in the inhibition of T-cell function is well established; this has been reviewed recently59, 60. Recent data suggest that there is a close correlation between the availability of arginine and the regulation of T-cell proliferation11, 61. The increased activity of arginase in MDSCs leads to enhanced L-arginine catabolism, which depletes this non-essential amino acid from the microenvironment. The shortage of L-arginine inhibits T-cell proliferation through several different mechanisms, including decreasing their CD3ζ expression62 and preventing their upregulation of the expression of the cell cycle regulators cyclin D3 and cyclin-dependent kinase 4 (CDK4)63. NO suppresses T-cell function through a variety of different mechanisms that involve the inhibition of JAK3 and STAT5 in T cells64, the inhibition of MHC class II expression 65 and the induction of T-cell apoptosis66.
ROS—Another important factor that contributes to the suppressive activity of MDSCs is ROS. Increased production of ROS has emerged as one of the main characteristics of MDSCs in both tumour-bearing mice and patients with cancer6, 10, 13, 53, 67-70. Inhibition of ROS production by MDSCs isolated from mice and patients with cancer completely abrogated the suppressive effect of these cells in vitro10, 13, 67. Interestingly, ligation of integrins expressed on the surface of MDSCs was shown to contribute to increased ROS production following the interaction of MDSCs with T cells10. In addition, several known tumour-derived factors, such as TGFβ, IL-10, IL-6, IL-3, platelet-derived growth factor (PDGF) and GM-CSF, can induce the production of ROS by MDSCs (for review see Ref 71).
The involvement of ROS and NO in mechanisms of MDSC suppression are not restricted to neoplastic conditions, as inflammation and microbial products are also known to induce the development of a MDSC population that produces ROS and NO following interactions with activated T cells15. Similar findings were observed in models of EAE16 and acute Toxoplasmosis infection 16. In addition, it has been observed that MDSCs mediated their suppressive function through IFNγ-dependent NO production in an experimental model of Trypanosoma cruzi infection23.
Peroxynitrite—More recently, it has emerged that peroxynitrite (ONOO-) is a crucial mediator of MDSC-mediated suppression of T-cell function. Peroxynitrite is a product of a chemical reaction between NO and superoxide anoion (O2-) and is one of the most powerful oxidants produced in the body. It induces the nitration and nitrosylation of the amino acids cystine, methionine, tryptophan and tyrosine72. Increased levels of peroxynitrite are present at sites of MDSC and inflammatory-cell accumulation, including sites of ongoing immune reactions. In addition, high levels of peroxynitrite are associated with tumour progression in many types of cancer72, 73,74-78, which has been linked with T-cell unresponsiveness. Bronte and colleagues reported that human prostate adenocarcinomas were infiltrated by terminallydifferentiated CD8+ T cells that were in an unresponsive state. High levels of nitrotyrosine were present in the T cells, which suggested the production of peroxynitrites in the tumour environment. Inhibiting the activity of arginase and iNOS, which are expressed in malignant but not in normal prostate tissue and are key enzymes of L-arginine metabolism,, led to decreased tyrosine nitration and restoration of T-cell responsiveness to tumour antigens79. In addition, we have demonstrated that peroxynitrite production by MDSCs during direct contact with T cells results in nitration of the T-cell receptor (TCR) and CD8 molecules, which alters the specific peptide binding of the T cells and renders them unresponsive to antigen-specific stimulation. However, the T cells maintained their responsiveness to nonspecific stimuli80. This phenomenon of MDSC induced antigen-specific T-cell unresponsiveness was also observed in vivo in tumour-bearing mice53.
Subset-specific suppressive mechanisms?—Recent findings indicate that different subsets of MDSC might use different mechanisms by which to suppress T-cell proliferation. As described earlier, two main subsets of MDSCs have been identified: a granulocytic subset and a monocytic subset. The granulocytic subset of MDSC was found to express high levels of ROS and low levels of NO, whereas the monocytic subset expressed low levels of ROS and high levels of NO and both subsets expressed ARG16 (Fig.3). Interestingly, both populations suppressed antigen-specific T-cell proliferation to an equal extent, despite their different mechanisms of action. Consistent with these observations, Movahedi et al. also reported two distinct MDSC subsets in tumour-bearing mice, one that consisted of mononuclear cells that resembled inflammatory monocytes and a second that consisted of polymorphonuclear cells that were similar to immature granulocytes. Again, both populations were found to suppress antigen-specific T-cell responses, although by using distinct effector molecules and signalling pathways. The suppressive activity of the granulocytic subset was ARG1-dependent, in contrast to the STAT1- and iNOS-dependent mechanism of the monocyte fraction17. Finally, the same trend was observed in Trypanosoma cruzii infection. In this case, monocytic MDSCs produced NO and strongly inhibited T-cell proliferation, and granulocytic MDSCs produced low levels of NO and did not inhibit T-cell proliferation, although they did produce superoxide15. The biological significance of such functional dichotomy of these two MDSC subsets remains to be elucidated. Induction of TReg cells—Recently, the ability of MDSCs to promote the de novo development of FOXP3+ regulatory T (TReg) cells in vivo has been described18, 19. The induction of TReg cells by MDSCs was found to require the activation of tumour-specific Tcells and the presence of IFNγ and IL-10 but was independent of NO19. In mice bearing 1D8 ovarian tumours, the induction of TReg cells by MDSCs required the expression of cytotoxic lymphocyte antigen 4 (CTLA-4; also known as CD152) by MDSCs18. In a mouse model of lymphoma, MDSCs were shown to induce TReg-cell expansion through a mechanism that required arginase and the capture, processing and presentation of tumour-associated antigens by MDSCs, but not TGFβ58. By contrast, Movahedi et al. found that the percentage of TReg cells was invariably high throughout tumour growth and did not relate to the kinetics of expansion of the MDSC population, suggesting that MDSCs were not involved in TReg-cell expansion17. Furthermore, in a rat model of kidney allograft tolerance that was induced with a CD28-specific antibody, MDSCs that were co-expressing CD80 and CD86 were found to have a limited effect on the expansion of the TReg-cell population81. Although further work is required to resolve these discrepancies and to determine the physiological relevance of these studies, it seems possible that MDSCs are involved in TReg-cell differentiation through the production of cytokines or direct cell–cell interactions. Furthermore, MDSCs and TReg cells might be linked in a common immunoregulatory network (see later).
Tissue-specific effects on MDSCs A major unresolved question in this field is whether MDSCs mediate antigen-specific or nonspecific suppression of T-cell responses. Provided that MDSCs and T cells are in close proximity, the factors that mediate MDSC suppressive function (ROS, arginase and NO) can inhibit T-cell proliferation regardless of the antigen specificity of the T cells. Indeed, numerous in vitro studies have demonstrated the antigen nonspecific nature of MDSC-mediated suppression of T cells82 83. However, whether the situation is the same in vivo is not clear, and evidence suggests that MDSC-mediated immunosuppression in peripheral lymphoid organs is mainly antigen-specific. The idea that MDSC-mediated T-cell suppression occurs in an antigen-specific manner is based on findings that antigen-specific interactions between antigen-presenting cells and T cells result in much more stable and more prolonged cell–cell contact than nonspecific interactions82, 84, 85. Such stable contacts are necessary for MDSCderived ROS and peroxynitrite to mediate effects on the molecules on the surface of T cells that render the T cells unresponsive to specific antigen. It should be noted that such modification of cell-surface molecules does not lead to T-cell death nor prevent nonspecific T-cell activation. Other evidence that supports the idea that MDSCs mediate antigen-specific suppression is the finding that that MDSCs can take up soluble antigens, including tumourassociated antigens, and process and present them to T cells17 80; blockade of MDSC–T-cell interactions with a MHC-class-I-specific antibody abrogated MDSC-mediated inhibition of T cell responses in vitro86. The MHC-class-I-restricted nature of MDSC-mediated CD8+ T-cell suppression has also been demonstrated in vivo in tumor models53 and in the model of inflammatory bowel disease 35. This is consistent with the recent observation that large numbers of tumour-induced MDSCs did not inhibit CD8+ T-cell responses specific for unrelated antigens in a model of sporadic cancer87. Notably, it is currently unclear whether similar antigen-specific mechanisms of MDSC-mediated suppression operate on CD4+ T cells, as published studies have only assessed the effects of MDSCs on CD8+ T cells. Addressing this question is complicated by the fact that only a small proportion of MDSCs in many tumour models expresses MHC class II molecules.
The theory that MDSCs suppress T-cell responses in an antigen-specific manner helps to explain the finding that T cells in the peripheral lymphoid organs of tumour-bearing mice and in the peripheral blood of cancer patients can still respond to stimuli other than tumourassociated antigens, including viruses, lectins, co-stimulatory molecules, IL-2 and CD3- and CD28-specific antibodies21, 80, 88-90. Furthermore, even patients with advanced stage cancer do not have systemic immunodeficiency except in cases in which the patient has received high doses of chemotherapy or is at a terminal stage of the disease.
Evidence suggets that the nature of MDSC-mediated suppression at the tumour site is quite different to that which occurs in the periphery. MDSCs actively migrate into the tumour site10, where they upregulate the expression of ARG1 and iNOS, downregulate the production of ROS and/or rapidly differentiate into tumour-associated macrophages (TAMs) 52. The levels of NO and arginase produced by tumour-associated MDSCs and TAMs are much higher than those of MDSCs found in peripheral lymphoid organs of the same animals. In addition, TAMs produce several cytokines (reviewed in REFs91, 92) that suppress T-cell responses in a nonspecific manner (Fig. 4). The mechanisms by which MDSC functions are regulated within the tumour microenvironment, and how they differ from those that operate at peripheral sites, remain unclear. It is possible that tumour stroma, hypoxia and/or the acidophilic environment have a role.
Therapeutic targeting of MDSCs The recognition that immune suppression has a crucial role in promoting tumour progression and contributes to the frequent failure of cancer vaccines to elicit an immune response has resulted in a paradigm shift with respect to approaches for cancer immunotherapy. Indeed, it has become increasingly clear that successful cancer immunotherapy will be possible only with a strategy that involves the elimination of suppressive factors from the body. As MDSCs are one of the main immunosuppressive factors in cancer and other pathological conditions, several different therapeutic strategies that target these cells are currently being explored (Table 2). Although the studies described below were carried out in tumor-bearing hosts, it is likely that the same strategies will be useful in other pathological conditions in which inhibition or elimination of MDSCs is a therapeutic aim.
Promoting myeloid-cell differentiation—One of the most promising approaches by which to target MDSCs for therapy is to promote their differentiation into mature myeloid cells that do not have suppressive abilities. Vitamin A has been identified as a compound that can mediate this effect: vitamin A metabolites such as retinoic acid have been found to stimulate the differentiation of myeloid progenitors into DCs and macrophages 86, 93. Mice that are deficient in vitamin A94 or that have been treated with a pan-retinoic-acid-receptor antagonist95, show an expansion of MDSCs in the bone marrow and spleen. Conversely, therapeutic concentrations of all-trans retinoic acid (ATRA) results in substantial decrease in the presence of MDSCs in cancer patients and tumour-bearing mice. ATRA induced MDSCs to differentiate into DCs and macrophages in vitro and in vivo 12, 86, 96. It is probable that ATRA preferentially induces the differentiation of the monocytic subset of MDSCs, whereas it causes apoptosis of the granulocytic subset. The main mechanism of ATRA-mediated differentiation involved an upregulation of glutathione synthesis and a reduction in ROS levels in MDSCs 97. Decreasing the number of MDSCs in tumour-bearing mice resulted in increased tumour-specific T-cell responses, and the combination of ATRA and two different types of cancer vaccine prolonged the anti-tumour effect of the vaccine treatment in two different tumour models 96. Moreover, administration of ATRA to patients with metastatic renal cell carcinoma resulted in a substantial decrease in the number of MDSCs in the peripheral blood and improved antigen-specific response of T cells 21. Further studies will lead to identification of other agents that have a similar effect. So far, evidence suggests that Vitamin D3 may be another agent with the potential to decrease MDSC numbers in patients with cancer, as it is also known to promote myeloid-cell differentiation98.
Inhibition of MDSC expansion—Because MDSC expansion is known to be regulated by tumour-derived factors (Table 1), several studies have focused on neutralizing the effects of these factors. Recently, SCF has been implicated in causing MDSC expansion in tumourbearing mice39. Inhibition of SCF-mediated signalling by blocking its interaction with its receptor, c-kit, decreased MDSC expansion and tumor angiogenesis39. VEGF, another tumourderived factor that is involved in promoting MDSC expansion, might also be a useful target by which to manipulate MDSC. However, in a clinical trial of 15 patients with refractory solid tumours, treatment with VEGF–trap (a fusion protein that binds all forms of VEGF-A and placental growth factor) showed no effect on MDSC numbers and did not result in increased T-cell responses99. By contrast, treatment of patients with metastatic renal cell cancer with a VEGF-specific blocking antibody (known as avastin) resulted in a decrease in the size of a CD11b+VEGFR1+ population of MDSCs in the peripheral blood 100. However, whether avastatin treatment resulted in an improvement in antitumour responses in these patients has not been determined. Finally, inhibition of matrix metalloproteinase 9 function in tumorbearing mice decreased the number of MDSCs in the spleen and tumour tissues and resulted in a significant delay in the growth of spontaneous NeuT tumours in transgenic BALB/c mice101. However, the mechanism responsible for this outcome remains to be elucidated.
Inhibition of MDSC function—Another approach by which to inhibit MDSCs is to block the signalling pathways that regulate the production of suppressive factors by these cells. One potential target by which this might be achieved is COX2. COX2 is required for the production of prostaglandin E2, which in 3LL tumour cells61 and mammary carcinoma40 has been shown to induce the upregulation of ARG1 expression by MDSCs, thereby inducing their suppressive function. Accordingly, COX2 inhibitors were found to downregulate the expression of ARG1 by MDSCs, which improved antitumour T-cell responses and enhanced the therapeutic efficacy of immunotherapy102, 103. Similarly, phosphodiesterase-5 inhibitors such as sildenafil were found to downregulate the expression of arginase and iNOS expression by MDSCs, thereby inhibiting their suppressive function in growing tumours104. This resulted in the induction of a measurable anti-tumour immune response and a marked delay of tumour progression in several mouse models 104.
ROS inhibitors have also been shown to be effective for decreasing MDSC-mediated immune suppression in tumour-bearing mice. The coupling of a NO-releasing moiety to a conventional non-steroidal anti-inflammatory drug has proven to be an efficient means by which to inhibit the production of ROS. One such drug, nitroaspirin, was found to limit the activity of ARG1 and iNOS in spleen MDSCs105. In combination with vaccination with endogenous retroviral gp70 antigen, nitroaspirin inhibited MDSCs function and increased the number and function of tumour-antigen-specific T cells105.
Elimination of MDSCs—MDSCs can be directly eliminated in pathological settings by using some chemotherapeutic drugs. Administration of one such drug, gemcitabine, to mice that were bearing large tumours resulted in a dramatic reduction in the number of MDSCs in the spleen and resulted in a marked improvement in the anti-tumour response induced by immunotherapy106, 107. This effect was specific to MDSCs, as a significant decrease in the number of T or B cells was not observed in these animals. Furthermore, in a study of 17 patients with early-stage breast cancer that were treated with doxorubicin–cyclophosphamide chemotherapy, a decrease in the level of MDSCs in the peripheral blood was observed22.
Evidence suggests that there is a broad range of methods that will be effective for targeting of the number and/or function of MDSCs in vivo. These strategies will undoubtedly help to further investigate the biology of these cells as well as expedite clinical applications to treat cancer and other pathological conditions.
MDSCs as regulatory myeloid cells? The wealth of information that has accumulated in recent years regarding the biology of MDSCs suggests that these cells might have evolved as a regulatory component of the immune system. These cells are absent under physiological conditions, as IMCs in naive mice are an intrinsic part of normal haematopoiesis that are not immunosuppressive in an unactivated state. In conditions of acute stress, infection or immunization, there is a transient expansion of this IMC population, which then quickly differentiates into mature myeloid cells. This transient IMC population can mediate the suppressive functions that are characteristic of MDSCs but, because the acute conditions are short-lived, the suppressive functions of this transient population have a minimal impact on the overall immune response. However, these cells probably function as important ‘gatekeepers’ that prevent pathological immune-mediated damage.
The role of the MDSC population in settings of chronic infections and cancer is very different. In these pathological conditions, the prolonged and marked expansion of IMCs and their subsequent activation leads to the expansion of a large population of MDSCs with immunosuppressive abilities. MDSCs accumulate in peripheral lymphoid organs and migrate to tumour sites, where they contribute to immunosuppression. Furthermore, some evidence suggests that MDSCs can also induce expansion of regulatory T cells. Future studies will reveal whether MDSCs can be considered part of a natural immune regulatory network.
Concluding remarks The field of MDSC research has more outstanding questions than answers. The roles of specific MDSC subsets in mediating T-cell suppression, and the molecular mechanisms responsible for inhibition of myeloid-cell differentiation, need to be elucidated. The issue of whether Tcell suppression occurs in an antigen-specific manner remains to be clarified, as do the mechanisms that cause MDSC migration to peripheral lymphoid organs. Some of the main priorities in this field should include a better characterization of human MDSCs and a clear understanding of whether targeting these cells in patients with various pathological conditions will be of clinical significance. Conversely, adoptive cellular therapy with MDSCs may be an attractive opportunity by which to inhibit immune responses in the setting of autoimmune disease or transplantation. The challenge for these approaches will be to devise methods by which to generate these cells ex vivo in clinical-grade conditions such that they are suitable for administration to patients. If the past 5–6 years are an indication of the potential for progress in this area, it is safe to estimate that there will soon be significantly more discoveries that further our understanding about the biology and clinical utility of MDSCs.
Box 1. Definition of myeloid-derived suppressor cells (MDSCs)
• a heterogeneous population of cells of myeloid origin that consist of myeloid progenitors and immature macrophages, immature granulocytes and immature dendritic cells
• present in activated state that is characterized by the increased production of reactive oxygen and nitrogen species, and of arginase
• potent suppressors of various T-cell functions • in mice, their phenotype is CD11b+Gr1+, although functionally distinct subsets within this population have been identified (see main text)
• in humans, their phenotype is Lin-HLA-DR-CD33+ or CD11b+CD14-CD33+.
Human cells do not express a marker homologous to mouse Gr1. MDSC have also been identified within a CD15+ population in human peripheral blood.
• in the steady state, immature myeloid cells lack suppressive activity and are present in the bone marrow, but not in secondary lymphoid organs
• accumulation of MDSCs in lymphoid organs and in tumours in response to various growth factors and cytokines is associated with various pathological conditions (most notably cancer)
• in tumour tissues, MDSCs can be differentiated from tumour-associated macrophages (TAMs) by their high expression of Gr1 (not expressed by TAMs) by their low expression of F4/80 (expressed by TAMs), by the fact that a large proportion of MDSCs have a granulocytic morphology and based the upregulated expression of both arginase and inducible nitric oxide synthase by MDSCs but not TAMs.
References
1. Young MRI, Newby M, Wepsic TH. Hematopoiesis and suppressor bone marrow cells in mice bearing large metastatic Lewis lung carcinoma tumors. Cancer Res 1987;47:100–106. [PubMed: 2947676]
2. Buessow SC, Paul RD, Lopez DM. Influence of mammary tumor progression on phenotype and function of spleen and in situ lymphocytes in mice. J Natl Cancer Inst 1984;73:249–255. [PubMed: 6610791]
3. Seung L, Rowley D, Dubeym P, Schreiber H. Synergy between T-cell immunity and inhibition of paracrine stimulation causes tumor rejection. Proc Natl Acad Sci U S A 1995;92:6254–6258. [PubMed: 7603979]
4. Sinha P, Clements VK, Bunt SK, Albelda SM, Ostrand-Rosenberg S. Crosstalk between myeloidderived suppressor cells and macrophages subverts tumor immunity toward a type 2 response. J Immunol 2007;179:977–983. [PubMed: 17617589]
5. Murdoch C, Muthana M, Coffelt SB, Lewis CE. The role of myeloid cells in the promotion of tumour angiogenesis. Nat Rev Cancer 2008;8:618–631. [PubMed: 18633355]
6. Youn JI, Nagaraj S, Collazo M, Gabrilovich DI. Subsets of myeloid-derived suppressor cells in tumorbearing mice. J Immunol 2008;181:5791–5802. [PubMed: 18832739] Together with reference # 17 this paper described functional differences between subsets of MDSC.
7. Bronte V, et al. Identification of a CD11b(+)/Gr-1(+)/CD31(+) myeloid progenitor capable of activating or suppressing CD8(+) T cells. Blood 2000;96:3838. [PubMed: 11090068]
8. Kusmartsev S, Gabrilovich DI. Inhibition of myeloid cell differentiation in cancer: The role of reactive oxygen species. J Leukoc Biol 2003;74:186–196. [PubMed: 12885935]
9. Li Q, Pan PY, Gu P, Xu D, Chen SH. Role of immature myeloid Gr-1+ cells in the development of antitumor immunity. Cancer Res 2004;64:1130–1139. [PubMed: 14871848] …..
“The proto-oncogenic transcription factor Myc is known to promote transcription of genes for the cell cycle as well as aerobic glycolysis and glutamine metabolism. Recently, Myc has been shown to play an essential role to induce the expression of glycolytic and glutamine metabolism genes in the initial hours of T cell activation. In a similar fashion, the transcription factor HIF1a can up-regulate glycolytic genes to allow cancer cells to survive under hypoxic conditions. “
Outsource a part of the T cell’s immune value chain, propose cancer immunotherapy researchers, from patient T cells to donor T cells. The novel allogeneic approach could rely on T-cell receptor gene transfer to generate broad and tumor-specific T-cell immune responses. [NIAID]
A new cancer immunotherapy approach could essentially outsource a crucial T-cell function. This function, T-cell reactivity to specific cancer antigens, is sometimes lacking in cancer patients. Yet, according to a new proof-of-principle study, these patients could benefit from T cells provided by healthy donors. Specifically, the healthy donors’ T cells could be used to broaden the T-cell receptor repertoires of the cancer patients’ T cells.
Ultimately, this approach relies on a cancer immunotherapy technique called T-cell receptor (TCR) transfer, or the genetic transfer of TCR chains. TCR transfer can be used to outsource the T cell’s learning function, the process by which a T cell acquires the ability to recognize foreign antigens—in this case, the sort of proteins that can be expressed on the surface of cancer cells. Because cancer cells harbor faulty proteins, they can also display foreign protein fragments, also known as neoantigens, on their surface, much in the way virus-infected cells express fragments of viral proteins.
The approach was detailed in a paper that appeared May 19 in the journal Science, in an article entitled, “Targeting of Cancer Neoantigens with Donor-Derived T Cell Receptor Repertoires.” This article, by scientists based at the Netherlands Cancer Institute and the University of Oslo, describes a novel strategy to broaden neoantigen-specific T-cell responses. Such a strategy would be useful in overcoming a common limitation seen in the immune response to cancer: Neoantigen-specific T-cell reactivity is generally limited to just a few mutant epitopes, even though the number of predicted epitopes is large.
“We demonstrate that T cell repertoires from healthy donors provide a rich source of T cells that specifically recognize neoantigens present on human tumors,” the study’s authors wrote. “Responses to 11 epitopes were observed, and for the majority of evaluated epitopes, potent and specific recognition of tumor cells endogenously presenting the neoantigens was detected.”
First, the researchers mapped all possible neoantigens on the surface of melanoma cells from three different patients. In all three patients, the cancer cells seemed to display a large number of different neoantigens. But when the researchers tried to match these to the T cells derived from within the patient’s tumors, most of these aberrant protein fragments on the tumor cells went unnoticed.
Next, the researchers tested whether the same neoantigens could be seen by T cells derived from healthy volunteers. Strikingly, these donor-derived T cells could detect a significant number of neoantigens that had not been seen by the patients’ T cells.
“Many of the T cell reactivities [among donor T cells] involved epitopes that in vivo were neglected by patient autologous tumor-infiltrating lymphocytes,” the authors of the Science article continued. “T cells re-directed with T cell receptors identified from donor-derived T cells efficiently recognized patient-derived melanoma cells harboring the relevant mutations, providing a rationale for the use of such ‘outsourced’ immune responses in cancer immunotherapy.”
“In a way, our findings show that the immune response in cancer patients can be strengthened; there is more on the cancer cells that makes them foreign that we can exploit. One way we consider doing this is finding the right donor T cells to match these neoantigens,” said Ton Schumacher, Ph.D., a principal investigator at the Netherlands Cancer Institute. “The receptor that is used by these donor T cells can then be used to genetically modify the patient’s own T cells so these will be able to detect the cancer cells.”
“Our study shows that the principle of outsourcing cancer immunity to a donor is sound,” added Johanna Olweus, M.D., Ph.D., who heads a research group at the University of Oslo. “However, more work needs to be done before patients can benefit from this discovery. Thus, we need to find ways to enhance the throughput.”
“We are currently exploring high-throughput methods to identify the neoantigens that the T cells can ‘see’ on the cancer and isolate the responding cells. But the results showing that we can obtain cancer-specific immunity from the blood of healthy individuals are already very promising.”
Targeting of cancer neoantigens with donor-derived T cell receptor repertoires
Accumulating evidence suggests that clinically efficacious cancer immunotherapies are driven by T cell reactivity against DNA mutation-derived neoantigens. However, among the large number of predicted neoantigens, only a minority is recognized by autologous patient T cells, and strategies to broaden neoantigen specific T cell responses are therefore attractive. Here, we demonstrate that naïve T cell repertoires of healthy blood donors provide a source of neoantigen-specific T cells, responding to 11/57 predicted HLA-A2-binding epitopes from three patients. Many of the T cell reactivities involved epitopes that in vivo were neglected by patient autologous tumor-infiltrating lymphocytes. Finally, T cells re-directed with T cell receptors identified from donor-derived T cells efficiently recognized patient-derived melanoma cells harboring the relevant mutations, providing a rationale for the use of such “outsourced” immune responses in cancer immunotherapy.
Metabolic maintenance of cell asymmetry following division in activated T lymphocytes.
Asymmetric cell division, the partitioning of cellular components in response to polarizing cues during mitosis, has roles in differentiation and development. It is important for the self-renewal of fertilized zygotes in Caenorhabditis elegans and neuroblasts in Drosophila, and in the development of mammalian nervous and digestive systems. T lymphocytes, upon activation by antigen-presenting cells (APCs), can undergo asymmetric cell division, wherein the daughter cell proximal to the APC is more likely to differentiate into an effector-like T cell and the distal daughter is more likely to differentiate into a memory-like T cell. Upon activation and before cell division, expression of the transcription factor c-Myc drives metabolic reprogramming, necessary for the subsequent proliferative burst. Here we find that during the first division of an activated T cell in mice, c-Myc can sort asymmetrically. Asymmetric distribution of amino acid transporters, amino acid content, and activity of mammalian target of rapamycin complex 1 (mTORC1) is correlated with c-Myc expression, and both amino acids and mTORC1 activity sustain the differences in c-Myc expression in one daughter cell compared to the other. Asymmetric c-Myc levels in daughter T cells affect proliferation, metabolism, and differentiation, and these effects are altered by experimental manipulation of mTORC1 activity or c-Myc expression. Therefore, metabolic signalling pathways cooperate with transcription programs to maintain differential cell fates following asymmetric T-cell division.
T cell acute lymphoblastic leukemia (T-ALL) is an aggressive malignancy associated with Notch pathway mutations. While both normal activated and leukemic T cells can utilize aerobic glycolysis to support proliferation, it is unclear to what extent these cell populations are metabolically similar and if differences reveal T-ALL vulnerabilities. Here we show that aerobic glycolysis is surprisingly less active in T-ALL cells than proliferating normal T cells and that T-ALL cells are metabolically distinct. Oncogenic Notch promoted glycolysis but also induced metabolic stress that activated 5′ AMP-activated kinase (AMPK). Unlike stimulated T cells, AMPK actively restrained aerobic glycolysis in T-ALL cells through inhibition of mTORC1 while promoting oxidative metabolism and mitochondrial Complex I activity. Importantly, AMPK deficiency or inhibition of Complex I led to T-ALL cell death and reduced disease burden. Thus, AMPK simultaneously inhibits anabolic growth signaling and is essential to promote mitochondrial pathways that mitigate metabolic stress and apoptosis in T-ALL.
Obesity and diabetes are associated with excessive inflammation and impaired wound healing. Increasing evidence suggests that macrophage dysfunction is responsible for these inflammatory defects. In the setting of excess nutrients, particularly dietary saturated fatty acids (SFAs), activated macrophages develop lysosome dysfunction, which triggers activation of the NLRP3 inflammasome and cell death. The molecular pathways that connect lipid stress to lysosome pathology are not well understood, but may represent a viable target for therapy. Glutamine uptake is increased in activated macrophages leading us to hypothesize that in the context of excess lipids glutamine metabolism could overwhelm the mitochondria and promote the accumulation of toxic metabolites. To investigate this question we assessed macrophage lipotoxicity in the absence of glutamine using LPS-activated peritoneal macrophages exposed to the SFA palmitate. We found that glutamine deficiency reduced lipid induced lysosome dysfunction, inflammasome activation, and cell death. Under glutamine deficient conditions mTOR activation was decreased and autophagy was enhanced; however, autophagy was dispensable for the rescue phenotype. Rather, glutamine deficiency prevented the suppressive effect of the SFA palmitate on mitochondrial respiration and this phenotype was associated with protection from macrophage cell death. Together, these findings reveal that crosstalk between activation-induced metabolic reprogramming and the nutrient microenvironment can dramatically alter macrophage responses to inflammatory stimuli.
Immunoregulatory Protein B7-H3 Reprograms Glucose Metabolism in Cancer Cells by ROS-Mediated Stabilization of HIF1α
CD8(+) T cells can respond to unrelated infections in an Ag-independent manner. This rapid innate-like immune response allows Ag-experienced T cells to alert other immune cell types to pathogenic intruders. In this study, we show that murine CD8(+) T cells can sense TLR2 and TLR7 ligands, resulting in rapid production of IFN-γ but not of TNF-α and IL-2. Importantly, Ag-experienced T cells activated by TLR ligands produce sufficient IFN-γ to augment the activation of macrophages. In contrast to Ag-specific reactivation, TLR-dependent production of IFN-γ by CD8(+) T cells relies exclusively on newly synthesized transcripts without inducing mRNA stability. Furthermore, transcription of IFN-γ upon TLR triggering depends on the activation of PI3K and serine-threonine kinase Akt, and protein synthesis relies on the activation of the mechanistic target of rapamycin. We next investigated which energy source drives the TLR-induced production of IFN-γ. Although Ag-specific cytokine production requires a glycolytic switch for optimal cytokine release, glucose availability does not alter the rate of IFN-γ production upon TLR-mediated activation. Rather, mitochondrial respiration provides sufficient energy for TLR-induced IFN-γ production. To our knowledge, this is the first report describing that TLR-mediated bystander activation elicits a helper phenotype of CD8(+) T cells. It induces a short boost of IFN-γ production that leads to a significant but limited activation of Ag-experienced CD8(+) T cells. This activation suffices to prime macrophages but keeps T cell responses limited to unrelated infections.
The bidirectional interaction between the immune system and whole-body metabolism has been well recognized for many years. Via effects on adipocytes and hepatocytes, immune cells can modulate whole-body metabolism (in metabolic syndromes such as type 2 diabetes and obesity) and, reciprocally, host nutrition and commensal-microbiota-derived metabolites modulate immunological homeostasis. Studies demonstrating the metabolic similarities of proliferating immune cells and cancer cells have helped give birth to the new field of immunometabolism, which focuses on how the cell-intrinsic metabolic properties of lymphocytes and macrophages can themselves dictate the fate and function of the cells and eventually shape an immune response. We focus on this aspect here, particularly as it relates to regulatory T cells.
Figure 1: Proposed model for the metabolic signatures of various Treg cell subsets.
(a) Activated CD4+ T cells that differentiate into the Teff cell lineage (green) (TH1 or TH17 cells) are dependent mainly on carbon substrates such as glucose and glutamine for their anabolic metabolism. In contrast to that, pTreg cells…
T-bet is a key modulator of IL-23-driven pathogenic CD4+ T cell responses in the intestine
IL-23 is a key driver of pathogenic Th17 cell responses. It has been suggested that the transcription factor T-bet is required to facilitate IL-23-driven pathogenic effector functions; however, the precise role of T-bet in intestinal T cell responses remains elusive. Here, we show that T-bet expression by T cells is not required for the induction of colitis or the differentiation of pathogenic Th17 cells but modifies qualitative features of the IL-23-driven colitogenic response by negatively regulating IL-23R expression. Consequently, absence of T-bet leads to unrestrained Th17 cell differentiation and activation characterized by high amounts of IL-17A and IL-22. The combined increase in IL-17A/IL-22 results in enhanced epithelial cell activation and inhibition of either IL-17A or IL-22 leads to disease amelioration. Our study identifies T-bet as a key modulator of IL-23-driven colitogenic responses in the intestine and has important implications for understanding of heterogeneity among inflammatory bowel disease patients.
Th17 cells are enriched at mucosal sites, produce high amounts of IL-17A, IL-17F and IL-22, and have an essential role in mediating host protective immunity against a variety of extracellular pathogens1. However, on the dark side, Th17 cells have also been implicated in a variety of autoimmune and chronic inflammatory conditions, including inflammatory bowel disease (IBD)2. Despite intense interest, the cellular and molecular cues that drive Th17 cells into a pathogenic state in distinct tissue settings remain poorly defined.
The Th17 cell programme is driven by the transcription factor retinoid-related orphan receptor gamma-t (RORγt) (ref. 3), which is also required for the induction and maintenance of the receptor for IL-23 (refs 4, 5). The pro-inflammatory cytokine IL-23, composed of IL-23p19 and IL-12p40 (ref. 6), has been shown to be a key driver of pathology in various murine models of autoimmune and chronic inflammatory disease such as experimental autoimmune encephalomyelitis (EAE)7, collagen induced arthritis8 and intestinal inflammation9, 10, 11, 12. Several lines of evidence, predominantly derived from EAE, suggest that IL-23 promotes the transition of Th17 cells to pathogenic effector cells9, 10, 11, 12. Elegant fate mapping experiments of IL-17A-producing cells during EAE have shown that the majority of IL-17A+IFN-γ+ and IL-17A−IFN-γ+ effector cells arise from Th17 cell progeny13. This transition of Th17 cells into IFN-γ-producing ‘ex’ Th17 cells required IL-23 and correlated with increased expression of T-bet. The T-box transcription factor T-bet drives the Th1 cell differentiation programme14 and directly transactivates the Ifng gene by binding to its promoter as well as multiple enhancer elements15. Indeed, epigenetic analyses have revealed that the loci for T-bet and IFN-γ are associated with permissive histone modifications in Th17 cells suggesting that Th17 cells are poised to express T-bet which could subsequently drive IFN-γ production16, 17.
A similar picture is emerging in the intestine where IL-23 drives T-cell-mediated intestinal pathology which is thought to be dependent on expression of T-bet18 and RORγt (ref. 19) by T cells. In support of this we have recently shown that IL-23 signalling in T cells drives the emergence of IFN-γ producing Th17 cells in the intestine during chronic inflammation20. Collectively these studies suggest a model whereby RORγt drives differentiation of Th17 cells expressing high amounts of IL-23R, and subsequently, induction of T-bet downstream of IL-23 signalling generates IL-17A+IFN-γ+ T cells that are highly pathogenic. Indeed, acquisition of IFN-γ production by Th17 cells has been linked to their pathogenicity in several models of chronic disease13, 21, 22, 23, 24 and a population of T cells capable of producing both IL-17A and IFN-γ has also been described in intestinal biopsies of IBD patients25, 26.
However, in the context of intestinal inflammation, it remains poorly defined whether the requirement for RORγt and T-bet reflects a contribution of Th17 and Th1 cells to disease progression or whether Th17 cells require T-bet co-expression to exert their pathogenic effector functions. Here, we use two distinct models of chronic intestinal inflammation and make the unexpected finding that T-bet is dispensable for IL-23-driven colitis. Rather the presence of T-bet serves to modify the colitogenic response restraining IL-17 and IL-22 driven pathology. These data identify T-bet as a key modulator of IL–23-driven colitogenic effector responses in the intestine and have important implications for understanding of heterogeneous immune pathogenic mechanisms in IBD patients.
Figure 1: IL-23 signalling is required for bacteria-driven T-cell-dependent colitis and the emergence of IL-17A+IFN-γ+ T cells.
C57BL/6 WT and Il23r−/− mice were infected orally with Hh and received weekly i.p. injections of IL-10R blocking antibody. Mice were killed at 4 weeks post infection and assessed for intestinal inflammation. (a) Colitis scores. (b) Typhlitis sores. (c) Representative photomicrographs of colon and caecum (× 10 magnification; scale bars, 200μM). (d) Representative flow cytometry plots of colonic lamina propria gated on viable CD4+ T cells. (e) Frequencies of IL-17A+ and/or IFN-γ+ CD4+ T cells present in the colon. Data represent pooled results from two independent experiments (n=12 for WT, n=10 for Il23r−/−). Bars are the mean and each symbol represents an individual mouse. *P<0.05, ***P<0.001 as calculated by Mann–Whitney U test.
C57BL/6 Rag1−/− mice were injected i.p. with 4 × 105 CD4+CD25−CD45RBhi T cells from C57BL/6 WT,Rorc−/− or Tbx21−/− donors. Mice were killed when recipients of Tbx21−/− T cells developed clinical signs of disease (4–6 weeks) and assessed for intestinal inflammation. (a) Colitis scores. (b) Representative photomicrographs of proximal colon sections (× 10 magnification; scale bars, 200μM). (c) Concentration of cytokines released from colon explants into the medium after overnight culture. Data represent pooled results from two independent experiments (n=14 for WT, n=11 for Rorc−/−, n=14 forTbx21−/−). Bars are the mean and each symbol represents an individual mouse. Bars are the mean and error bars represent s.e.m. *P<0.05, **P<0.01, ***P<0.001 as calculated by Kruskal–Wallis one-way ANOVA with Dunn’s post-test.
C57BL/6 Rag1−/− mice were injected i.p. with 4×105 CD4+CD25−CD45RBhi T cells from C57BL/6 WT,Rorc−/− or Tbx21−/− donors. Mice were killed when recipients of Tbx21−/−T cells developed clinical signs of disease (4–6 weeks). (a) Representative plots of IL-17A and IFN-γ expression in colonic CD4+ T cells. (b) Frequencies of IL-17A+ and/or IFN-γ+ cells among colonic CD4+ T cells. (c) Total numbers of IL-17A+and/or IFN-γ+ CD4+ T cells present in the colon. Data represent pooled results from three independent experiments (n=20 for WT, n=18 for Tbx21−/−, n=12 for Rorc−/−). Bars are the mean and each symbol represents an individual mouse. *P<0.05, **P<0.01, ***P<0.001 as calculated by Kruskal–Wallis one-way ANOVA with Dunn’s post-test.
T-bet deficiency promotes an exacerbated Th17-type response
Our transfer of Tbx21−/− T cells revealed a striking increase in the frequency of IL-17A+IFN-γ−cells (Fig. 3) and we reasoned that T-bet-deficiency could impact on Th17 cell cytokine production. Therefore, we transferred WT or Tbx21−/− CD4+ T cells into Rag1−/− recipients and measured the expression of RORγt, IL-17A, IL-17F and IL-22 by CD4+ T cells isolated from the colon. In agreement with our earlier findings, Tbx21−/− T cells gave rise to significantly increased frequencies of RORγt-expressing T cells capable of producing IL-17A (Fig. 4a). Furthermore, T-bet deficiency also led to a dramatic expansion of IL-17F and IL-22-expressing cells, which constituted only a minor fraction in WT T cells (Fig. 4a,b). By contrast, the frequency of granulocyte-macrophage colony-stimulating factor (GM-CSF) and IFN-γ producing cells was significantly reduced in T-bet-deficient T cells as compared with WT T cells. When analysed in more detail we noted that the production of IL-17A, IL-17F and IL-22 increased specifically in T-bet-deficient IL-17A+IFN-γ+ T cells as compared with WT T cells whereas IFN-γ production decreased overall in the absence of T-bet as expected (Supplementary Fig. 4A). Similarly, GM-CSF production was also generally reduced in Tbx21−/− CD4+ T cells further suggesting a shift in the qualitative nature of the T cell response.
Figure 4: T-bet-deficient CD4+ T cells promote an exacerbated Th17-type inflammatory response.
C57BL/6 Rag1−/− mice were injected i.p. with 4×105 CD4+CD25−CD45RBhi T cells from C57BL/6 WT orTbx21−/− donors. Mice were killed when recipients of Tbx21−/−T cells developed clinical signs of disease (4–6 weeks). (a) Representative plots of cytokines and transcription factors in WT or Tbx21−/− colonic CD4+ T cells. (b) Frequency of IL-17A+, IL-17F+, IL-22+, GM-CSF+ or IFN-γ+ colonic T cells in WT orTbx21−/−. (c) quantitative reverse transcription PCR (qRT-PCR) analysis of mRNA levels of indicated genes in colon tissue homogenates. (d) Total number of neutrophils (CD11b+ Gr1high) in the colon. (e) Primary epithelial cells were isolated from the colon of steady state C57BL/6 Rag1−/− mice and stimulated with 10ngml−1 cytokines for 4h after which cells were harvested and analysed by qRT-PCR for the indicated genes. Data in b–d represent pooled results from two independent experiments (n=14 for WT, n=11 for Tbx21−/−). Bars are the mean and error bars represent s.e.m. Data in e are pooled results from four independent experiments, bars are the mean and error bars represent s.e.m. *P<0.05, **P<0.01,***P<0.001 as calculated by Mann–Whitney U test.
T-bet-deficient colitis depends on IL-23, IL-17A and IL-22
In the present study we show that bacteria-driven colitis is associated with the IL-23-dependent emergence of IFN-γ-producing Th17 cells co-expressing RORγt and T-bet. Strikingly, while RORγt is required for the differentiation of IFN-γ-producing Th17 cells and induction of colitis, T-bet is dispensable for the emergence of IL-17A+IFN-γ+ T cells and intestinal pathology. Our results show that instead of a mandatory role in the colitogenic response, the presence of T-bet modulates the qualitative nature of the IL-23-driven intestinal inflammatory response. In the presence of T-bet, IL-23-driven colitis is multifunctional in nature and not functionally dependent on either IL-17A or IL-22. By contrast, in the absence of T-bet a highly polarized colitogenic Th17 cell response ensues which is functionally dependent on both IL-17A and IL-22. T-bet-deficient T cells are hyper-responsive to IL-23 resulting in enhanced STAT3 activation and downstream cytokine secretion providing a mechanistic basis for the functional changes. These data newly identify T-bet as a key modulator of IL-23-driven colitogenic CD4+ T cell responses.
Contrary to our expectations T-bet expression by CD4 T cells was not required for their pathogenicity. In keeping with the negative effect of T-bet on Th17 differentiation40, 41, 42, we observed highly polarized Th17 responses in T-bet-deficient intestinal T cells. Early studies demonstrated that IFN-γ could suppress the differentiation of Th17 cells40 and thus the reduced IFN-γ production by Tbx21−/−T cells could facilitate Th17 cell generation. However, our co-transfer studies revealed unrestrained Th17 differentiation of Tbx21−/− T cells even in the presence of WT T cells, suggesting a cell autonomous role for T-bet-mediated suppression of the Th17 programme. Indeed, the role of T-bet as a transcriptional repressor of the Th17 cell fate has been described recently. For example, T-bet physically interacts with and sequesters Runx1, thereby preventing Runx1-mediated induction of RORγt and Th17 cell differentiation43. In addition, T-bet binds directly to and negatively regulates expression of many Th17-related genes15, 34 and we identified IL23r to be repressed in a T-bet-dependent manner. In line with this we show here that T-bet-deficient intestinal T cells express higher amounts of Il23r as well as Rorc. This resulted in enhanced IL-23-mediated STAT3 activation and increased production of IL-17A and IL-22. It has also been suggested that T-bet activation downstream of IL-23R signalling is required for pathogenic IL-23-driven T cell responses43, 44. However, we did not find a role for IL-23 in the induction and/or maintenance of T-bet expression and colitis induced by T-bet-deficient T cells was IL-23 dependent. Collectively, these findings demonstrate that T-bet deficiency leads to unrestrained expansion of colitogenic Th17 cells, which is likely mediated through enhanced activation of the IL-23R-STAT3 pathway.
The observation that T-bet-deficient T cells retain their colitogenic potential is in stark contrast to earlier studies. Neurath et al.18 convincingly showed that adoptive transfer of Tbx21−/− CD4+ T cells into severe combined immunodeficiency (SCID) recipients failed to induce colitis and this correlated with reduced IFN-γ and increased IL-4 production. Another study revealed that IL-4 plays a functional role in inhibiting the colitogenic potential of Tbx21−/− T cells, as recipients ofStat6−/−Tbx21−/− T cells developed severe colitis37. Importantly, the intestinal inflammation that developed in recipients of Stat6−/−Tbx21−/− T cells could be blocked by administration of IL-17A neutralizing antibody, suggesting that the potent inhibitory effect of IL-4/STAT6 signals on Th17 differentiation normally prevent colitis induced by Tbx21−/− T cells37. Various explanations could account for the discrepancy between our study and those earlier findings. First, in contrast to the published reports, we used naïve Tbx21−/− CD4+ T cells from C57BL/6 mice instead of BALB/c mice. An important difference between Tbx21−/− CD4+ T cells from these genetic backgrounds appears to be their differential susceptibility to suppression by IL-4/STAT6 signals. We found that transfer of Tbx21−/− T cells induced IL-17A-dependent colitis despite increased frequencies of IL-4-expressing cells in the intestine. This discrepancy may be due to higher amounts of IL-4 produced by activated CD4+ T cells from BALB/c versus C57BL/6 mice45, leading to the well-described Th2-bias of the BALB/c strain45. Second, differences in the composition of the intestinal microbiota between animal facilities can have a substantial effect on skewing CD4+ T cells responses. In particular, the Clostridium-related segmented filamentous bacteria (SFB) have been shown to drive the emergence of IL-17 and IL-22 producing CD4+ T cells in the intestine46. Importantly, the ability of naïve CD4+ T cells to induce colitis is dependent on the presence of intestinal bacteria, as germ-free mice do not develop pathology upon T cell transfer47. In line with this, we previously described that colonization of germ-free mice with intestinal microbiota containing SFB was necessary to restore the development of colitis47. Since our Rag1−/− colony is SFB+ and the presence of SFB was not reported in the previous studies, it is possible that differences in SFB colonization status contributed to the observed differences in pathogenicity ofTbx21−/− T cells.
It is important to note that T-bet-deficient T cells did not induce more severe colitis than WT T cells but rather promoted a distinct mucosal inflammatory response. Colitis induced by WT T cells is characterized by a multifunctional response with high amounts of IFN-γ and GM-CSF and a lower IL-17A and IL-22 response. Consistent with this, we have shown that blockade of GM-CSF abrogates T cell transfer colitis48 as well as bacteria-driven intestinal inflammation49 in T-bet sufficiency whereas blockade of IL-17A or IL-22 fails to do so. By contrast T-bet deficiency leads to production of high amounts of IL-17A and IL-22 in the colon and neutralization of either was sufficient to reduce intestinal pathology. Our in vitro experiments suggest that IL-17A and IL-22 synergise to promote intestinal epithelial cell responses, which may in part explain the efficacy of blocking IL-17A or IL-22 in colitis induced by T-bet-deficient T cells. A similar synergistic interplay has been described in the lung where IL-22 served a tissue protective function in homeostasis but induced airway inflammation in the presence of IL-17A (ref. 50). This highlights the complexity of the system in health and disease, and the need for a controlled production of both cytokines. We describe here only one mechanism of how IL-17A/IL-22 induce a context-specific epithelial cell response that potentially impacts on the order or composition of immune cell infiltration. Overall, these results provide a new perspective on T-bet, revealing its role in shaping the qualitative nature of the IL-23-driven colitogenic T cell response.
We also describe here the unexpected finding that a substantial proportion of T-bet-deficient intestinal T cells retain the ability to express IFN-γ. To investigate the potential mechanisms responsible for T-bet-independent IFN-γ production by intestinal CD4+ T cells we focused on two transcription factors, Runx3 and Eomes. Runx3 has been shown to promote IFN-γ expression directly through binding to the Ifng promoter38 and Eomes is known to compensate for IFN-γproduction in T-bet-deficient Th1 cells37. We found IL-23-mediated induction of Runx3 protein in WT and Tbx21−/− T cells isolated from the intestine, thus identifying Runx3 downstream of IL-23R signalling. By contrast, we could only detect Eomes protein and its induction by IL-23 in T-bet-deficient but not WT T cells. Thus, Runx3 and Eomes are activated in response to IL-23 in T-bet-deficient cells and are likely to be drivers of T-bet-independent IFN-γ production. In support of this we found that the majority of T-bet-deficient IL-17A−IFN-γ+ T cells expressed Eomes. However, only a minor population of IL-17A+IFN-γ+ T cells stained positive for Eomes, suggesting the existence of alternative pathways for IFN-γ production by Th17 cells. Intriguingly, a recent study identified Runx3 and Runx1 as the transcriptional regulators critical for the differentiation of IFN-γ-producing Th17 cells51. The author’s demonstrated that ectopic expression of Runx transcription factors was sufficient to induce IFN-γ production by Th17 cells even in the absence of T-bet. These findings, combined with our data on Runx3 activation downstream of IL-23R signalling strongly suggest that Runx3 rather than Eomes is driving IFN-γ expression by intestinal Th17 cells.
We have not formally addressed the role of IFN-γ in colitis driven by T-bet-deficient T cells. A recent report by Zimmermann et al.52 found that antibody-mediated blockade of IFN-γ ameliorates colitis induced by WT or T-bet-deficient T cells suggesting IFN-γ also contributes to the colitogneic response mediated by T-bet-deficient T cells as originally described for WT T cells53, 54. By contrast with our results the Zimmerman study found that IL-17A blockade exacerbated colitis following transfer of Tbx21−/− T cells. The reason for the differential role of IL-17A in the two studies is not clear but it is notable that the Zimmerman study was performed in the presence of co-infection with SFB and Hh, and this strong inflammatory drive may alter the pathophysiological role of particular cytokines. Together the data indicate that T-bet deficiency in T cells does not impede their colitogenic activity but that the downstream effector cytokines of the response are context dependent.
In conclusion, our data further underline the essential role for IL-23 in intestinal inflammation and demonstrate that T-bet is an important modulator of the IL–23-driven effector T cell response. The colitogenic T cell response in a T-bet sufficient environment is multifunctional with a dominant GM-CSF and IFN-γ response. By contrast T-bet-deficient colitogenic responses are dominated by IL-17A and IL-22-mediated immune pathology. These results may have significant bearing on human IBD where it is now recognized that differential responsiveness to treatment may reflect considerable disease heterogeneity. As such, identification of suitable biomarkers such as immunological parameters, that allow stratification of patient groups, is becoming increasingly important55. Genome-wide association studies have identified polymorphisms in loci related to innate and adaptive immune arms that confer increased susceptibility to IBD. Among these are Th1 (STAT4, IFNG and STAT1) as well as Th17-related genes (RORC, IL23R and STAT3) (refs56, 57). Thus, detailed profiling of the T cell response in IBD patients may help identify appropriate patient groups that are most likely to benefit from therapeutic blockade of certain effector cytokines. Finally, our studies highlight the importance of IL-23 in the intestinal inflammatory hierarchy and suggest that IL-23 could be an effective therapeutic target across a variety of patient groups.
Yale study: How antibodies access neurons to fight infection
Yale scientists have solved a puzzle of the immune system: how antibodies enter the nervous system to control viral infections. Their finding may have implications for the prevention and treatment of a range of conditions, including herpes and Guillain-Barre syndrome, which has been linked to the Zika virus.
Many viruses — such as West Nile, Zika, and the herpes simplex virus — enter the nervous system, where they were thought to be beyond the reach of antibodies. Yale immunobiologists Akiko Iwasaki and Norifumi Iijima used mice models to investigate how antibodies could gain access to nerve tissue in order to control infection.
In mice infected with herpes, they observed a previously under-recognized role of CD4 T cells, a type of white blood cell that guards against infection by sending signals to activate the immune system. In response to herpes infection, CD4 T cells entered the nerve tissue, secreted signaling proteins, and allowed antibody access to infected sites. Combined, CD4 T cells and antibodies limited viral spread.
“This is a very elegant design of the immune system to allow antibodies to go to the sites of infection,” said Iwasaki. “The CD4 T cells will only go to the site where there is a virus. It’s a targeted delivery system for antibodies.”
Access of protective antiviral antibody to neuronal tissues requires CD4 T-cell help
Circulating antibodies can access most tissues to mediate surveillance and elimination of invading pathogens. Immunoprivileged tissues such as the brain and the peripheral nervous system are shielded from plasma proteins by the blood–brain barrier1 and blood–nerve barrier2, respectively. Yet, circulating antibodies must somehow gain access to these tissues to mediate their antimicrobial functions. Here we examine the mechanism by which antibodies gain access to neuronal tissues to control infection. Using a mouse model of genital herpes infection, we demonstrate that both antibodies and CD4 T cells are required to protect the host after immunization at a distal site. We show that memory CD4 T cells migrate to the dorsal root ganglia and spinal cord in response to infection with herpes simplex virus type 2. Once inside these neuronal tissues, CD4 T cells secrete interferon-γ and mediate local increase in vascular permeability, enabling antibody access for viral control. A similar requirement for CD4 T cells for antibody access to the brain is observed after intranasal challenge with vesicular stomatitis virus. Our results reveal a previously unappreciated role of CD4 T cells in mobilizing antibodies to the peripheral sites of infection where they help to limit viral spread.
T Cells Help Reverse Ovarian Cancer Drug Resistance
T cells (red) attack ovarian cancer cells (green). [University of Michigan Health System]
Researchers at the University of Michigan have recently published the results from a new study that they believe underscores why so many ovarian tumors develop resistance to chemotherapy. The tumor microenvironment is made up of an array of cell types, yet effector T cells and fibroblasts constitute the bulk of the tissue. The investigators believe that understanding the interplay between these two cell types holds the key to how ovarian cancer cells develop resistance.
The new study suggests that the fibroblasts surrounding the tumor work to block chemotherapy, which is why nearly every woman with ovarian cancer becomes resistant to treatment. Conversely, the scientists published evidence that T cells in the microenvironment can reverse the resistance phenotype—suggesting a whole different way of thinking about chemotherapy resistance and the potential to harness immunotherapy drugs to treat ovarian cancer.
“Ovarian cancer is often diagnosed at late stages, so chemotherapy is a key part of treatment,” explained co-senior study author J. Rebecca Liu, M.D., associate professor of obstetrics and gynecology at the University of Michigan. “Most patients will respond to it at first, but everybody develops chemoresistance. And that’s when ovarian cancer becomes deadly.”
Dr. Liu continued, stating that “in the past, we’ve thought the resistance was caused by genetic changes in tumor cells. But we found that’s not the whole story.”
The University of Michigan team looked at tissue samples from ovarian cancer patients and separated the cells by type to study the tumor microenvironment in vitro and in mice. More importantly, the scientists linked their findings back to actual patient outcomes.
The results of this study were published recently in Cell through an article entitled “Effector T Cells Abrogate Stroma-Mediated Chemoresistance in Ovarian Cancer.”
Ovarian cancer is typically treated with cisplatin, a platinum-based chemotherapy. The researchers found that fibroblasts blocked platinum. These cells prevented platinum from accumulating in the tumor and protected tumor cells from being killed off by cisplatin.
Diagram depicting how T cells can reverse chemotherapeutic resistance. [Cell, Volume 165, Issue 5, May 19, 2016]
“We show that fibroblasts diminish the nuclear accumulation of platinum in ovarian cancer cells, resulting in resistance to platinum-based chemotherapy,” the authors wrote. “We demonstrate that glutathione and cysteine released by fibroblasts contribute to this resistance.”
T cells, on the other hand, overruled the protection of the fibroblasts. When researchers added the T cells to the fibroblast population, the tumor cells began to die off.
“CD8+ T cells abolish the resistance by altering glutathione and cystine metabolism in fibroblasts,” the authors explained. “CD8+ T-cell-derived interferon (IFN)γ controls fibroblast glutathione and cysteine through upregulation of gamma-glutamyltransferases and transcriptional repression of system xc−cystine and glutamate antiporter via the JAK/STAT1 pathway.”
By boosting the effector T cell numbers, the researchers were able to overcome the chemotherapy resistance in mouse models. Moreover, the team used interferon, an immune cell-secreted cytokine, to manipulate the pathways involved in cisplatin.
“T cells are the soldiers of the immune system,” noted co-senior study author Weiping Zou, M.D., Ph.D., professor of surgery, immunology, and biology at the University of Michigan. “We already know that if you have a lot of T cells in a tumor, you have better outcomes. Now we see that the immune system can also impact chemotherapy resistance.”
The researchers suggest that combining chemotherapy with immunotherapy may be effective against ovarian cancer. Programmed death ligand 1 (PD-L1) and PD-1 pathway blockers are currently FDA-approved treatments for some cancers, although not ovarian cancer.
“We can imagine re-educating the fibroblasts and tumor cells with immune T cells after chemoresistance develops,” Dr. Zou remarked.
“Then we could potentially go back to the same chemotherapy drug that we thought the patient was resistant to. Only now we have reversed that, and it’s effective again,” Dr. Liu concluded.
Effector T Cells Abrogate Stroma-Mediated Chemoresistance in Ovarian Cancer
•Fibroblasts diminish platinum content in cancer cells, resulting in drug resistance
•GSH and cysteine released by fibroblasts contribute to platinum resistance
•T cells alter fibroblast GSH and cystine metabolism and abolish the resistance
•Fibroblasts and CD8+ T cells associate with patient chemotherapy response
Summary
Effector T cells and fibroblasts are major components in the tumor microenvironment. The means through which these cellular interactions affect chemoresistance is unclear. Here, we show that fibroblasts diminish nuclear accumulation of platinum in ovarian cancer cells, resulting in resistance to platinum-based chemotherapy. We demonstrate that glutathione and cysteine released by fibroblasts contribute to this resistance. CD8+ T cells abolish the resistance by altering glutathione and cystine metabolism in fibroblasts. CD8+ T-cell-derived interferon (IFN)γ controls fibroblast glutathione and cysteine through upregulation of gamma-glutamyltransferases and transcriptional repression of system xc− cystine and glutamate antiporter via the JAK/STAT1 pathway. The presence of stromal fibroblasts and CD8+ T cells is negatively and positively associated with ovarian cancer patient survival, respectively. Thus, our work uncovers a mode of action for effector T cells: they abrogate stromal-mediated chemoresistance. Capitalizing upon the interplay between chemotherapy and immunotherapy holds high potential for cancer treatment.
Activation of effect or T cells leads to increased glucose uptake, glycolysis, and lipid synthesis to support growth and proliferation. Activated T cells were identified with CD7, CD5, CD3, CD2, CD4, CD8 and CD45RO. Simultaneously, the expression of CD95 and its ligand causes apoptotic cells death by paracrine or autocrine mechanism, and during inflammation, IL1-β and interferon-1α.. The receptor glucose, Glut 1, is expressed at a low level in naive T cells, and rapidly induced by Myc following T cell receptor (TCR) activation. Glut1 trafficking is also highly regulated, with Glut1 protein remaining in intracellular vesicles until T cell activation. CD28 co-stimulation further activates the PI3K/Akt/mTOR pathway in particular, and provides a signal for Glut1 expression and cell surface localization. Mechanisms that control T cell metabolic reprogramming are now coming to light, and many of the same oncogenes importance in cancer metabolism are also crucial to drive T cell metabolic transformations, most notably Myc, hypoxia inducible factor (HIF)1a, estrogen-related receptor (ERR) a, and the mTOR pathway. The proto-oncogenic transcription factor, Myc, is known to promote transcription of genes for the cell cycle, as well as aerobic glycolysis and glutamine metabolism. Recently, Myc has been shown to play an essential role in inducing the expression of glycolytic and glutamine metabolism genes in the initial hours of T cell activation. In a similar fashion, the transcription factor (HIF)1a can up-regulate glycolytic genes to allow cancer cells to survive under hypoxic conditions
UPDATE 6/11/2021
Bispecific Antibodies Emerging as Effective Cancer Therapeutics
Science 28 May 2021: Vol. 372, Issue 6545, pp. 916-917 DOI: 10.1126/science.abg1209
Bispecific antibodies (bsAbs) bind two different epitopes on the same or different antigens. Through this dual specificity for soluble or cell-surface antigens, bsAbs exert activities beyond those of natural antibodies, offering numerous opportunities for therapeutic applications. Although initially developed for retargeting T cells to tumors, with a first bsAb approved in 2009 (catumaxomab, withdrawn in 2017), exploring new modes of action opened the door to many additional applications beyond those of simply combining the activity of two different antibodies within one molecule. Examples include agonistic “assembly activities” that mimic the activity of natural ligands and cofactors (for example, factor VIII replacement in hemophilia A), inactivation of receptors or ligands, and delivery of payloads to cells or tissues or across biological barriers. Over the past years, the bsAb field transformed from early research to clinical applications and drugs. New developments offer a glimpse into the future promise of this exciting and rapidly progressing field.
Monoclonal antibodies (mAbs) comprise antigen-binding sites formed by the variable domains of the heavy and light chain and an Fc region that mediates immune responses. BsAbs, produced through genetic engineering, combine the antigen-binding sites of two different antibodies within one molecule, with a plethora of formats available (1). Conceptually, one can discriminate between bsAbs with combinatorial modes of action where the antigen-binding sites act independently from each other, and bsAbs with obligate modes of action where activity needs binding of both, either in a sequential (temporal) way or dependent on the physical (spatial) linkage of both (see the figure) (2). BsAbs approved as drugs are so far in the obligate dual-binding category: A T cell recruiter (blinatumomab) against cancer and a factor VIIIa mimetic to treat hemophilia A (emicizumab). Most but not all of the more than 100 bsAbs in clinical development address cancers. Some are in late stage (such as amivantamab, epcoritamab, faricimab, and KNO46), but most are still in early stages (2). Most of these entities enable effector cell retargeting to induce target cell destruction.
An increasing number of programs also explore alternative modes of action. This includes bsAbs that target pathways involved in tumor proliferation (such as amivantamab), invasion, ocular angiogenesis (such as faricimab), or immune regulation by blocking receptors and/or ligands, mainly in a combinatorial manner. Challenges for all of these entities are potential adverse effects, toxicity in normal tissues, and overshooting and systemic immune responses, especially with T cell retargeting or immune-modulating or activating entities. Such issues need to be carefully addressed.
Most of the bispecific T cell engagers comprise a binding site for a tumor-associated antigen and CD3 [a component of the T cell receptor (TCR) activation complex] as trigger molecule on T cells. To prevent or ameliorate “on-target, off-tumor” effects of T cell recruiters, approaches currently investigated include the modulation of target affinities and mechanisms to allow conditional activation upon target cell binding. Thus, a reduced affinity for CD3 increased tolerability by reducing peripheral cytokine concentrations that are associated with nonspecific or overshooting immune reactions (3). Similarly, reduced affinity for the target antigen was shown to ameliorate cytokine release and damage of target-expressing tissues (4). Tumor selectivity can be further increased by implementing avidity effects—for example, by using 2+1 bsAb formats with two low-affinity binding sites for target antigens and monovalent binding to CD3 (4).
In further approaches, binders to CD3 were identified that efficiently trigger target cell destruction without inducing undesired release of cytokines, demonstrating the importance of epitope specificity to potentially uncouple efficacy from cytokine release (5). Complementing these T cell–recruiting principles, the nonclassical T cell subset of γ9d2 T cells with strong cytotoxic activity emerged as potent effectors, which can be retargeted with bsAbs binding to the γ9d2 TCR. Thereby, global activation of all T cells, including inhibitory regulatory T cells (Treg cells), through CD3 binding, may be avoided (6). However, even these approaches might result in a narrow therapeutic window to treat solid tumors because of T cell activation in normal tissues.
Consequently, there are several approaches to conditionally activate T cells within tumors, including a local liberation of the CD3-binding sites or triggering local assembly of CD3-binding sites from two half-molecules. For example, CD3-binding sites have been masked by fusing antigen binding or blocking moieties—such as peptides, aptamers, or anti-idiotypic antibody fragments—to one or both variable domains. These moieties are released within the tumor by tumor-associated proteases, or through biochemical responses to hypoxia or low pH (7). This approach can also be applied to confer specific binding of antibody therapeutics, including bsAbs, to antigens on tumor cells (8).
An on-target restoration of CD3-binding sites requires application of two target-binding entities, each comprising parts of the CD3-binding site, which assemble into functional binding sites upon close binding of both half-antibodies. The feasibility of this approach was recently shown, for example, for a split T cell–engaging antibody derivative (Hemibody) that targets a cell surface antigen (9). Such approaches can also be applied to half-antibodies that recognize two different targets expressed on the same cell, further increasing tumor selectivity.
Regarding T cell engagers, increasing efforts are made to target not only cell-surface antigens expressed on tumor cells but also human leukocyte antigen (HLA)–presented tumor-specific peptides. This expands the target space of bsAbs toward tumor-specific intracellular antigens and can be achieved by using either recombinant TCRs or antibodies with TCR-like specificities combined with, for example, CD3-binding arms to engage T cell responses. A first TCR–anti-CD3 bispecific molecule is in phase I and II trials to treat metastatic melanoma (10). A challenge of this approach is the identification of TCRs or TCR-like antibodies that bind the peptide in the context of HLA with high affinity and specificity, without cross-reacting with related peptides to reduce or avoid off-target activities. Comprehensive screening tools and implementation of computational approaches are being developed to achieve this task.
A rapidly growing area of bsAbs in cancer therapy is their use to foster antitumor immune responses. Here, they are especially applied for dual inhibition of checkpoints that prevent immune responses—for example, programmed cell death protein 1 (PD-1) and its ligand (PD-L1), cytotoxic T lymphocyte–associated antigen 4 (CTLA-4), or lymphocyte activation gene 3 (LAG-3; for example, KNO46). Tumor-targeted bsAbs can also target costimulatory factors such as CD28 or 4-1BB ligand (4-1BBL) to enhance T cell responses when combined with PD-1 blockade or to provide an activity-enhancing costimulatory signal in combination with CD3-based bsAbs (11). Furthermore, bsAbs are being developed for local effects by targeting one arm to antigens that are expressed by tumor cells or cells of the tumor microenvironment (2).
Clinical application of bsAbs now expands to other therapeutic areas, including chronic inflammatory, autoimmune, and neurodegenerative diseases; vascular, ocular, and hematologic disorders; and infections. In contrast to mAbs, bsAbs can inactivate the signaling of different cytokines with one molecule to treat inflammatory diseases (12). Simultaneous dual-target binding is not essential to elicit activity for bsAbs against combinations of proinflammatory cytokines, such as tumor necrosis factor (TNF), interleukin-1α (IL-1α), IL-1β, IL-4, IL-13, IL-17, inducible T cell costimulator ligand (ICOSL), or B cell–activating factor (BAFF). This presumably also applies to blockade of immune cell receptors, although dual targeting might confer increased efficacy due to avidity effects and increased selectivity through simultaneous binding of two different receptors.
A further application of combinatorial dual targeting is in ophthalmology. Loss of vision in wet age-related macular degeneration (AMD) results from abnormal proliferation and leakiness of blood vessels in the macula. This can be treated with antibodies that bind and inactivate factors that stimulate their proliferation (13). In contrast to mAbs or fragments that recognize individual factors, bsAbs bind two such factors. For example, faricimab that binds vascular endothelial growth factor A (VEGF-A) and angiopoietin-2 (ANG2), demonstrated dual efficacy in preclinical studies, and is currently in phase 3 trials.
BsAbs with obligate modes of action that mandate simultaneous dual-target binding are “assemblers” that replace the function of factors necessary to form functional protein complexes. One of these bsAbs with an assembly role (emicizumab, approved in 2018) replaces factor VIIIa in the clotting cascade. Deficiency of factor VIII causes hemophilia A, which can be overcome by substitution with recombinant factor VIII. However, a proportion of patients develop factor VIII–neutralizing immune responses and no longer respond to therapy. To overcome this, a bsAb was developed with binding sites that recognize and physically connect factors IXa and X, a process normally mediated by factor VIIIa. Extensive screening of a large set of bsAbs was required to identify those that combine suitable epitopes with optimized affinities and geometry to serve as functional factor VIIIa mimetics (14). This exemplifies the complexity of identifying the best bsAb for therapeutic applications.
A mode of action requiring sequential binding of two targets is the transport of bsAbs across the blood-brain barrier (BBB). This is a tight barrier of brain capillary endothelial cells that controls the transport of substances between the blood and the cerebrospinal fluid—the brain parenchyma. Passage of large molecules, including antibodies, across the BBB is thereby restricted. Some proteins, such as transferrin or insulin, pass through the BBB by way of transporters on endothelial cells. Antibodies that bind these shuttle molecules, such as the transferrin receptor (TfR), can hitchhike across the BBB. BsAbs that recognize brain targets (such as β-amyloid for Alzheimer’s disease) and TfR with optimized affinities, epitopes, and formats can thereby enter the brain. Such bsAbs are currently in clinical evaluation to treat neurodegenerative diseases (15).
In the past years, there has been a transition from a technology-driven phase, solving hurdles to generate bsAbs with defined composition, toward exploring and extending the modes of action for new therapeutic options. The challenge of generating bsAbs is not only to identify suitable antigen pairs to be targeted in a combined manner. It is now recognized that the molecular composition has a profound impact on bsAb functionality (13). That more than 30 different bsAb formats are in clinical trials proves that development is now driven by a “fit for purpose” or “format defines function” rationale. Many candidates differ in their composition, affecting valency, geometry, flexibility, size, and half-life (1). Not all members of this “zoo of bsAb formats” qualify to become drugs. Strong emphasis is therefore on identifying candidates that exhibit drug-like properties and fulfill safety, developability, and manufacturability criteria. There is likely to be an exciting new wave of bsAb therapeutics available in the coming years.
May 16, 2016
By Alex Keown, BioSpace.com Breaking News Staff
BERKELEY, Calif. – Shares of Aduro Biotech (ADRO) have fallen more than 25 percent this morning following news that the company’s Phase II trial for its combination pancreatic cancer drug, CRS-207 did not meet its primary endpoint of survivability.
Aduro said its Eclipse trial of CRS-207 failed to show an improvement in overall survival for patients with pancreatic cancer who had failed at least two prior therapies in the metastatic setting. Median overall survival was 3.8 months for patients treated with the immunotherapy regimen of CRS-207 and the cancer vaccine GVAX pancreas, 5.4 months for patients treated with CRS-207 alone and 4.6 months for patients administered chemotherapy. Aduro said there were no reported safety concerns during the trial and full study findings will be presented at a later date.
Stephen T. Isaacs, chairman, president and chief executive officer of Aduro, called the findings a disappointing and “unexpected outcome.’
“While we are well aware of the very difficult-to-treat nature of late-stage metastatic pancreatic cancer, we are surprised by the divergence of these data from the results of our Phase IIa study. At the same time, we continue to look forward to the interim results later this year from our ongoing Stellar trial, which is evaluating CRS-207 and GVAX Pancreas with and without the anti-PD1 checkpoint inhibitor nivolumab as a second-line therapy for patients with metastatic pancreatic cancer,” Isaacs said in a statement.
Aduro Biotech says its leading clinical trial for its cancer-fighting combination of GVAX and CRS-207 was a flop. The biotech reported this morning that its combo not only failed to hit the primary endpoint, it did worse than the two solo groups in the study.
“Median overall survival (MOS) in this third-line and greater setting was 3.8 months for patients treated with the immunotherapy regimen of CRS-207 and GVAX Pancreas, 5.4 months for patients treated with CRS-207 alone and 4.6 months for patients administered chemotherapy,” the company reported.
Aduro’s stock ($ADRO) plunged 30% on the news in premarket trading.
“While we are well aware of the very difficult-to-treat nature of late-stage metastatic pancreatic cancer, we are surprised by the divergence of these data from the results of our Phase 2a study,” said CEO Stephen Isaacs. But the company hasn’t given up hope on its lead program.
“In the overall survival analysis, we were intrigued by activity seen with CRS-207 as a single-agent. While the median duration of 5.4 months appears greater for CRS-207, the overall survival curve of CRS-207 alone was comparable to overall survival seen with chemotherapy. Of note, due to a disproportionately high dropout rate in the single-agent chemotherapy arm, most of these patients instead received a variety of combination treatments, including chemotherapies, immunotherapies and targeted therapies,” said Dirk Brockstedt, executive vice president, research and development for Aduro.
In a conference call with analysts Aduro execs noted that they are now shelving plans for a pivotal Phase III study in pancreatic cancer, focusing on an ongoing study in the pipeline that includes a checkpoint inhibitor.
The history of cancer vaccines not customized to individual patients has been a litany of failure, with programs for Stimuvax and others experiencing a string of defeats in the clinic. Celldex joined that circle of failure recently with a Phase III miss for Rintega. Aduro, though, doubled down on the cancer vaccine strategy and was able to strike some big-money pacts along the way on the basis of some promising midstage data.
GVAX Pancreas is based on a pancreatic cell line modified to secrete granulocyte-macrophage colony-stimulating factor (GM-CSF), a cytokine known to stimulate the immune system. CRS-207 is made up of attenuated (deactivated) Listeria monocytogenes that express mesothelin, sparking another immune response to a protein concentrated on pancreatic cancer cells. Together, they’re supposed to provide a one-two punch against cancer, with an option to add on additional drugs to continue to build an attack on cancer cells.
That was the only workable strategy with GVAX, which, like other cancer vaccines, wasn’t able to spur a strong enough response to make a significant difference in the fight against cancer as a solo therapy, allowing Aduro to buy it for a song in early 2013. Monday’s conference call included several skeptical remarks from analysts about GVAX’s future, if any.
Aduro was on hand at the 2013 ASCO confab to review the data from a midstage study involving 93 patients with advanced pancreatic cancer. A combination of chemo plus GVAX pancreas and CRS-207 significantly outperformed GVAX and chemo, bumping up overall survival from 3.9 months to 6.1 months. That’s not a big gain, but it was a sign of progress in a very tough field. And it was good enough for the FDA to grant a breakthrough drug designation.
Now the company is forced into a classic defensive crouch, citing its significant cash reserves as it looks to regroup.
Hello. I’m David Kerr, professor of cancer medicine at University of Oxford.
I’d like to discuss today a really interesting editorial that’s just recently been published in the Journal of the National Cancer Institute by a close friend and colleague of mine, Francesco Pezzella.[1] What he does is challenge one of the basic hallmarks of cancer. We know that Judah Folkman declared in the early 1970s[2] that cancer growth must be preceded by angiogenesis, that there can be no increase in cancer bulk or burden without new vessels dividing, sprouting, supporting, and oxygenating the growth of the cancer, these cancer nodules.
Indeed, angiogenesis has become one of the classic hallmarks of neoplasia, and there are by now a variety of drugs—bevacizumab, ramucirumab, and the tyrosine kinase inhibitors—that seek to prevent new angiogenesis. What Francesco talks about is a different model in which there are some tumors. This is first noted in non–small cell lung cancer[3] and pulmonary metastases, which are nonangiogenic. Rather than requiring the proliferation of new blood vessels, it seems that there are some tumor cells that are capable of co-opting existing blood vessels within organs such as the lungs and liver.
This is a new process, probably an active process. It’s probably cell surface adhesion molecule driven. But there are no clear ideas as yet as to what, mechanistically, the key events are. Of course, this poses a really huge number of really interesting questions. Is it possible that bevacizumab-resistant or ramucirumab-resistant tumors are those which switch from being angiogenic to nonangiogenic, thus devising and developing blood supply through co-option rather than new blood vessel formation?
If we understood more about the mechanism of action, it would lend itself to further drug targeting. If we combined an inhibitor of angiogenesis with an inhibitor of vascular co-option, would it prevent the outgrowth of resistance to the existing antiangiogenic drugs, which are used widely in clinic?
This is a fantastic new area of science, requiring much mechanistic work. It is not yet another hallmark of cancer but one for which I think, over the coming 5-10 years, we’ll see increasingly focused research, more mechanistic insights, and perhaps—if we’re lucky—an idea that can be used on development pathways.
References
Pezzella F, Gatter KC. Evidence showing that tumors can grow without angiogenesis and can switch between angiogenic and nonangiogenic phenotypes. J Natl Cancer Inst. 2016; Apr 8. [Epub ahead of print]
Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med. 1971;285:1182-1186.Abstract
Sardari NP, Colpaert C, Blyweert B, et al. Prognostic value of nonangiogenic and angiogenic growth patterns in non-small-cell lung cancer. Br J Cancer. 2004;91:1293-1300. Abstract
Evidence Showing That Tumors Can Grow Without Angiogenesis and Can Switch Between Angiogenic and Nonangiogenic Phenotypes
Although sorafenib is approved for the treatment of hepatocellular carcinoma (HCC), the ability of this anti-angiogenic tyrosine kinase inhibitor to extend survival in HCC patients is limited because of acquired drug resistance, whose mechanism is poorly understood. In this issue of the Journal, Kuczynski and colleagues (1) report a mechanism of acquired resistance to sorafenib using an orthotopic HCC xenograft model. The authors tell us how, although these HCC are initially angiogenic and respond to sorafenib, resistance occurs because the neoplastic cells switch to a non-angiogenic phenotype and actively co-opt the normal liver vasculature instead of inducing angiogenesis. These results have important implications for understanding this particular form of resistance to anti-angiogenic drugs and the biology of the tumors that can develop such a resistance.
The non-angiogenic growth of tumors has already been hypothesized to be one of the possible reasons for intrinsic and/or acquired cancer resistance to anti-angiogenic treatment (2). In this paper, it is now proven that an angiogenic malignancy can, following treatment with a drug inhibiting sprouting angiogenesis, switch to a non-angiogenic phenotype in order to keep growing.
This finding further supports the notion that neoplasia is not necessarily angiogenesis dependent as some tumors can be completely non-angiogenic while many more can present with a mixture of both angiogenic and non-angiogenic regions (3). Furthermore, it had been already described that the angiogenic status of a tumor is not an absolutely fixed characteristic but can change: eg, primary angiogenic breast carcinomas can relapse as non-angiogenic lung metastases (4) while non-angiogenic primary lung cancers can progress with angiogenic brain secondary (5). Now, the findings of Kuczynksi and coworkers show that a tumor can switch from angiogenic to non-angiogenic growth in response to treatment with an anti-angiogenic drug. Taken together, these observations demonstrate that the angiogenic status of a tumor is not an absolutely fixed characteristic, but can change.
This is in sharp contrast to the concept, first enunciated in 1971 by Judah Folkman (6) and subsequently included among the hallmarks of cancer (7), that tumor growth is always angiogenesis-dependent as “any increase in tumor population must be preceded by an increase in new capillaries converging on the tumor” (8).
Non-angiogenic tumors were first described in histopathology studies of primary non–small cell lung carcinomas (NSCLCs) and carcinoma metastases, from a variety of primaries, in the lung as these tumors fill the air spaces without destroying the parenchyma and co-opt the pre-existing alveolar vessels (9). Non-angiogenic human neoplasms were subsequently reported to occur as brain tumors (10), liver metastases growing by replacing the haepatocytes (11,12) or by colonizing the hepatic sinusoids (13) and lymph node metastases (14,15). Mouse models have now also been established for non-angiogenic malignant growths in brain (16,17) and lung (18).
The demonstration that some tumors do not induce angiogenesis is achieved on the grounds that in these lesions the only vessels present have the distribution and the phenotype of normal vessels and the overall architecture of the organ is preserved (10–12,19,20). This evidence now includes also a recent intravital microscopy study in an animal model (15). A second type of tumor growing without inducing sprouting angiogenesis and without co-opting vessels has also been discovered. This one exploits vascular mimicry, in which the neoplastic cells themselves assemble into channels that act like vessels (21).
The angiogenic NSCLC can also be told apart from non-angiogenic ones by gene transcription analyses. An investigation of differentially transcribed genes in these tumors suggested that metabolic reprogramming, with a switch toward oxidative phosphorylation under the control of selected heat shock proteins, oncogenes, and tumors suppressor genes, could be one of the key issues (22,23).
Another noteworthy piece of information is that the transcription and expression of genes associated with hypoxia and angiogenesis seems to be comparable in both angiogenic and non-angiogenic tumors (15,22,24). Therefore, the sensing of hypoxia and expression of VEGF protein by cancer cells do not invariably lead to new vessel formation.
Only a few studies so far have started to address the mechanisms of vessel co-option. Observations in animal models of brain malignancies indicate that vessel co-option is an active process that involves selected cell adhesion molecules and protection from apoptosis for the cell that is successfully co-opting a vessel (25–28).
All these results have therefore established the study of non-angiogenic tumors as a new field in cancer biology, but so far we have only just scratched the surface. So what now are the most pressing questions we face?
One is: what is the biology underlying the non-angiogenic phenotype, and what are the mechanisms that allow a cancer cell to switch between angiogenic and non-angiogenic phenotypes?
Second, how do the cancer cells interact with and co-opt the pre-existing vessels? Data published so far suggests that this is an active process (26,29). Moreover, how does this process change in different organs?
Third, does vessel co-option also facilitate resistance to other classes of anti-angiogenic drugs, such as the VEGF-neutralizing antibody bevacizumab?
Fourth, given that vessel co-option occurs in many human cancers, including some of the most prevalent (eg, malignancies from breast, colon, rectum, and lung), is vessel co-option also a mechanism of resistance to anti-angiogenic therapy in humans and not just in animal models?
Last, but not least, can vessel co-option be inhibited with drugs? The data of Kuczynski and colleagues shows that the response to sorafenib in HCC might be more durable if sorafenib were to be combined with a drug that targets vessel co-option. However, there are currently no drugs designed to target vessel co-option in humans. In our opinion, this represents a major deficiency in the current portfolio of oncology drugs and needs to be addressed urgently.
Hopefully, this new field of cancer biology will lead to novel therapeutic interventions designed according to the relationship observed between neoplastic cells and vessels in tumor lesions, in the knowledge that tumors can also grow without inducing angiogenesis.
, et al. Co-option of liver vessels and not sprouting angiogenesis drives acquired sorafenib resistance in hepatocellular carcinoma. J Natl Cancer Inst.2016:108(8):djw030.
Quantitative immunohistological analysis of the microvasculature in untreated human glioblastoma multiforme. Computer-assisted image analysis of whole-tumor sections. J Neurosurg.1994;81(6):902–909.
TABLE 1: Antiangiogenic Drugs Approved by FDA (2004–Present)
Anca Chelariu-Raicu, MD, PhD
Robert L. Coleman, MD
Anil K. Sood, MD
Abstract / Synopsis:
Abstract: Angiogenesis is known to play an important role in normal ovarian physiology as well as in growth and progression of ovarian cancer. The first FDA approval of bevacizumab in 2004 was for metastatic colorectal cancer in combination with chemotherapy; this was a key point for several subsequent approvals of antiangiogenic drugs. The efficacy of bevacizumab treatment is modest, however, and most ovarian cancer patients eventually develop acquired resistance, which highlights the need for new targeted therapies and/or combination strategies. Understanding the multitude of variables in response to antiangiogenic therapy would offer potential strategies for selecting patients most likely to benefit from such therapy.
Introduction
The principles of antiangiogenic therapy are rooted in observations made by Folkman and others over 40 years ago.[1] Since then, antiangiogenic therapies have been incorporated into clinical care for many cancer patients. The vascular endothelial growth factor (VEGF)/VEGF receptor (VEGFR) pathway is arguably the most advanced for clinical development. This pathway has been extensively studied for its role in development of malignant ascites and tumor progression.[2] The VEGF molecule is a key angiogenic factor, which is involved in development of physiologic and pathologic neovascularization. VEGF is a growth as well as proliferation factor for endothelial cells and it binds to VEGFR-1 and VEGFR-2 as well as the cofactors neuropilin-1 (NRP-1) and NRP-2.[3] VEGFR-2 is expressed mostly on endothelial cells; VEGFR-1 can be expressed on macrophages, tumor cells, and fibroblasts.[4] While one of the main antiangiogenic approaches is to block VEGF using a monoclonal antibody, other drugs including VEGF pathway inhibitors such as small-molecule tyrosine kinase inhibitors (eg, sunitinib, sorafenib, pazopanib, regorafenib, lenvatinib, vandetanib), soluble VEGF decoy receptor (eg, aflibercept), and human monoclonal antibody against VEGFR-2 (ramucirumab) have also been developed.
Among the various antiangiogenic drugs, bevacizumab, a humanized anti-VEGF monoclonal antibody, is the most widely studied across tumor types and specifically in epithelial ovarian cancer. Beginning in 2004, the US Food and Drug Administration (FDA) granted several approvals for antiangiogenic drugs with a main indication in metastatic disease for colorectal cancer, non–small-cell lung, renal cell, cervical, and ovarian cancers, and glioblastoma. Recently, in June 2018, bevacizumab was approved for the first time also for frontline therapy for ovarian cancer in combination with platinum and taxane-based chemotherapy. Despite positive initial response rates using bevacizumab in advanced ovarian cancer, patients unfortunately develop relapsed disease within weeks to months. Nevertheless, preclinical data suggest that prolonged administration of bevacizumab as maintenance therapy after platinum-based chemotherapy prolongs progression-free survival (PFS).[5] This review summarizes the major clinical trials that led to the approval of antiangiogenic drugs and gives a brief view into novel combinations of bevacizumab with other targeted therapies in an attempt to enhance the efficacy of bevacizumab.
Standard of Care
Ovarian cancer is the most deadly gynecologic malignancy with 5-year survival rates ranging from 47% for all stages compared to only 29% for those with advanced-stage disease (III or IV) and is responsible for approximately 14,000 deaths in the United States annually.[6] The standard-of-care treatment remains primary tumor reductive surgery followed by adjuvant platinum and taxane-based chemotherapy. However, the recurrence rate is approximately 80%, even for patients who respond to initial treatment.[7]
Bevacizumab as Upfront Therapy
GOG-218 and ICON7 were the first two positive advanced-stage frontline ovarian cancer randomized phase III trials that added bevacizumab to chemotherapy.[8,9] In both GOG-218 and ICON7, bevacizumab was added to the standard of care, which consists of 6 cycles of platinum and taxane-based chemotherapy. In GOG-218, the duration of bevacizumab treatment was up to 22 cycles using a dose of 15 mg/kg, and in ICON7, 18 cycles of bevacizumab were given using a dose of 7.5 mg/kg. Although the two trials used different treatment duration and dosing, they both showed an increase in PFS. In GOG-218, the median PFS after adding bevacizumab in frontline and maintenance was increased by 4 months, from 10.3 to 14.1 months (hazard ratio (HR), 0.72; 95% CI, 0.63–0.82).[8] In ICON7, PFS at 36 months was 20.3 months with standard therapy, as compared with 21.8 months with standard therapy plus bevacizumab (HR, 0.81; 95% CI, 0.70–0.94; P = .004).[9] The same study suggested that the benefit of adding bevacizumab was the greatest for patients with high risk of progression (International Federation of Gynecology and Obstetrics [FIGO]) stage III > 1 cm or IV or suboptimally debulked surgery) where the estimated median PFS was 10.5 months with standard therapy, as compared with 15.9 months with bevacizumab (HR, 0.68; 95% CI, 0.55–0.85; P < .001).[9] Another intriguing observation of the study was that the effect on PFS was lost when the therapy with bevacizumab was withdrawn.[9,10] In this context, the optimal strategy for bevacizumab might be to continue the treatment until disease progression, as indicated by the data in the OCEANS trial in recurrent platinum-sensitive setting, where the experimental arm consisted of standard chemotherapy, gemcitabine plus carboplatin, in combination with bevacizumab as maintenance.[11] The same observation was made in the GOG-213 trial where the enrolled patients presenting recurrent platinum-sensitive disease were randomly assigned to standard paclitaxel and carboplatin every 3 weeks with or without bevacizumab. The latter was continued as maintenance every 3 weeks until disease progression or unacceptable toxicity.[12] As already mentioned from the OCEANS trial results, the effects of adding bevacizumab to chemotherapy and continuation as maintenance were reproducible. This was also the case in patients enrolled in the GOG-213 trial, where the median overall survival (OS) in the chemotherapy plus bevacizumab group was 42.2 months (95% CI, 37.7–46.2) vs 37.3 months (95% CI, 32.6–39.7) in the chemotherapy group (HR, 0.829; 95% CI, 0.683–1.005; P = .056).[12] Results from the ENGOT-ov15/AGO-OVAR 17 trial will most probably give an answer to the optimal treatment duration with bevacizumab, as this trial consists of 2 experimental arms, one being frontline chemotherapy combined with bevacizumab for 15 months while the second arm incorporates bevacizumab with the same frontline chemotherapy, but for a longer period (30 months). Considering the increase in PFS and OS after administering bevacizumab in frontline therapy in GOG-218 and ICON7, the European Medicines Agency (EMA) granted first approval of the drug for ovarian cancer in 2011 while the FDA approved it in June 2018.
Other Antiangiogenic Drugs Used as Upfront Therapy
Other multitarget compounds have demonstrated promising results in phase III trials. In the AGO-OVAR 16 trial, pazopanib (a protein kinase inhibitor of VEGFR and platelet-derived growth factor receptor [PDGFR]) maintenance therapy showed that PFS was higher in the experimental arm with a median improvement of 5.6 months (HR, 0.77; 95% CI, 0.64–0.91). Grade 3 or 4 hypertension (30.8%), neutropenia (9.9%), liver-related toxicity (9.4%), and diarrhea (8.2%) were significantly higher in the pazopanib arm.[13] A substudy of the same group of patients looked at the germline BRCA1 or BRCA2 mutation status and explored the effectiveness of maintenance therapy with pazopanib in these patients. Consistent with previous observations, germline BRCA status was prognostic, demonstrating that the median PFS was longer in the placebo arm for the BRCA1 or BRCA2 mutation carriers versus BRCA1 or BRCA2 wild-type patients (30.3 vs 14.1 months) (HR, 0.48; 95% CI, 0.29–0.78).[14] In another study, DNA from tumor and blood samples from patients enrolled in GOG-218 were sequenced, showing that patients with mutations in homologous recombination repair (HRR) had significantly prolonged PFS and OS when compared to those without mutations.[15] These data show that genetic testing plays an important role with regard to prognostic implications and should be discussed with all patients. This is particularly relevant for treatment with poly (ADP-ribose) polymerase (PARP) inhibitors.[16] There was no positive or negative correlation between HRR and the use of bevacizumab as maintenance therapy in this study.[15]
In the AGO-OVAR 12 study, another multitargeted compound, nintedanib (a potent inhibitor of VEGFR, fibroblast growth factor receptor [FGFR], and PDGFR), was investigated. Patients with advanced ovarian cancer were given standard-of-care chemotherapy, carboplatin and paclitaxel, and randomized to nintedanib or placebo. The median PFS was significantly improved in the experimental arm compared with placebo (17.2 vs 16.6 months) (HR, 0.84; 95% CI, 0.72–0.98). Patients treated with nintedanib reported grade 3 adverse effects such as diarrhea (21% vs 2%), thrombocytopenia (12% vs 5%), and anemia (12% vs 6%).[17] Another trial with trebananib, a selective angiopoietin-1 (Ang1) and Ang2 neutralizing peptibody, examined its effects in combination with standard chemotherapy as well as maintenance. This trial was a randomized study, in which patients received trebananib or placebo plus carboplatin and paclitaxel as first-line treatment. The primary endpoint of the study, PFS, did not show any improvement after the combination of trebananib with carboplatin and paclitaxel.[18]
Bevacizumab and Other Antiangiogenic Drugs Used in the Relapse Setting, Platinum Resistant
While the antiangiogenic frontline therapy was seen from different perspectives by the FDA and the EMA, bevacizumab was initially granted FDA approval for use in recurrent ovarian cancer based on the AURELIA trial. The experimental arm of this trial consisted of adding bevacizumab to chemotherapy until disease progression. Patients who received bevacizumab had a median PFS of 6.7 vs 3.4 months in patients receiving chemotherapy alone (HR, 0.48; 95% CI, 0.38–0.60) and median OS of 16.6 vs 13.3 months, respectively (HR, 0.85; 95% CI, 0.66–1.08).[19] Another trial, TRINOVA-1, aimed to determine whether adding trebananib to weekly paclitaxel until disease progression would improve PFS. This trial showed that inhibition of Ang1/Ang2 determined a prolongation of PFS but not over the benefit of bevacizumab.[20] A third randomized phase III trial, ENGOT-ov-6/TRINOVA-2, which had a similar study design to TRINOVA-1, evaluated PFS and OS after adding trebananib to pegylated liposomal doxorubicin (PLD) in patients with recurrent ovarian cancer (platinum sensitive and resistant). Patients in the experimental arm had a median PFS of 7.6 months (95% CI, 7.2–9.0) vs 7.2 months (95% CI, 4.8–8.2) in the placebo arm (HR, 0.92; 95% CI, 0.68–1.24). Trebananib demonstrated anticancer activity indicated by improved objective response rate (46% vs 21% in the placebo arm [odds ratio, 3.43; 95% CI, 1.78–6.64]). Median duration of response was also improved in the trebananib arm (7.4 months; 95% CI, 5.7–7.6) vs placebo (3.9 months; 95% CI, 2.3–6.5).[21]
Bevacizumab and Other Antiangiogenic Drugs Used in the Relapse Setting, Platinum Sensitive
In patients with recurrent platinum-sensitive ovarian cancer, the OCEANS and GOG-213 trials led to important advances. In the OCEANS trial, bevacizumab or placebo was added to gemcitabine and carboplatin for 6 to 10 cycles and then continued until progression. The addition of bevacizumab led to a statistically significant increase in PFS (HR, 0.484; 95% CI, 0.388–0.605). Median PFS was 12.4 months for bevacizumab vs 8.4 months in the placebo group.[11] In the GOG-213 trial, a different chemotherapy backbone (paclitaxel and carboplatin) was used and it was not placebo-controlled due to its primary endpoint being OS. In addition, surgical randomization for candidates deemed appropriate for secondary surgery was done for about 16% of the intent-to-treat population. This trial also demonstrated an increase in the median PFS in the bevacizumab plus chemotherapy arm compared with chemotherapy alone (13.8 months vs 10.4 months). Of note, GOG-213 showed a positive trend in median OS from 37.3 months in the chemotherapy group to 42.2 months in the chemotherapy plus bevacizumab group (HR, 0.829; 95% CI, 0.683–1.005; P = .056), which when adjusted for platinum-free interval and participation in the surgical objective, was significantly associated with OS (HR, 0.823; 95% CI, 0.680–0.996, P = .0447).[12] While the patients in the OCEANS trial did not receive bevacizumab with the frontline treatment, a third trial, MITO16B-MaNGO OV2B-ENGOT OV17, enrolled patients with carboplatin-sensitive relapsed disease who had had previous bevacizumab treatment. They found that bevacizumab in combination with a platinum-based doublet is associated with significantly prolonged PFS and a good safety profile.[22] Results from AGO OVAR 2.21, which evaluated patients with relapsed disease who previously had bevacizumab in frontline, were presented during the ESMO 2018 meeting. In this study, both arms contained bevacizumab added to a platinum-based chemotherapy; one arm consisted of gemcitabine and carboplatin and the other arm consisted of PLD and carboplatin. Being the first phase III trial in ovarian cancer comparing two bevacizumab-containing regimens, the study showed that the carboplatin/PLD/bevacizumab combination resulted in superior PFS compared with carboplatin/gemcitabine/bevacizumab (HR, 0.80; 95% CI, 0.68–0.96; P = .0128).[23]
Only one antiangiogenic VEGF receptor 1-3 inhibitor investigated in recurrent platinum-sensitive ovarian cancer patients so far has shown anti-tumor activity. In the 3-arm ICON6 trial, participants were randomly assigned to receive placebo plus chemotherapy then placebo maintenance (arm A), cediranib 20 mg once daily plus chemotherapy then placebo maintenance (arm B), or cediranib 20 mg once daily plus chemotherapy then cediranib 20 mg once daily for maintenance (arm C). Median PFS was 11 months for arm C vs 8.7 months for arm A (HR, 0.56; 95% CI, 0.44–0.72). The difference in OS was nonsignificant (P = .3) across the 3 arms.[24] Although the improvement in PFS to a median of 11 months with cediranib as maintenance is similar to that reported with bevacizumab maintenance after chemotherapy, the risk of hypertension, fatigue, diarrhea, and nausea in patients taking cediranib in combination with chemotherapy makes this a worse candidate compared to intravenous bevacizumab.
Other Emerging Antiangiogenic Therapies in Combination With Anti-VEGF Drugs
Using antiangiogenic drugs to target the VEGF molecule or angiogenic receptors such as VEGFR, FGFR, and PDGFR proved to be an effective strategy for inhibiting tumor angiogenesis. The effects on PFS and OS are modest, as most patients develop adaptive resistance to anti-VEGF therapy and eventually present with progressive disease. Novel concepts that combine antiangiogenic drugs with other emerging approaches such as Delta-like ligand 4 (DLL4)-blocking antibody,[25,26] and colony stimulating factor 1 receptor (CSF1R) found on macrophages,[27] are showing promising results in decreasing tumor burden in vivo.[25-27] Previous studies that investigated the DLL4 pathway showed that DLL4 blockade can inhibit tumor growth by promoting nonproductive angiogenesis.[25] Furthermore, dual targeting of VEGF and DLL4 showed superior anti-tumor effects (decreased tumor burden, less ascites) in ovarian cancer mouse models compared with either therapy alone.[26] Navicizixumab, a DLL4 and VEGF inhibitor, is a clinical candidate being tested in a phase I/Ib study.[28]
With the genetic ablation of CSF1R and thereby macrophages, it was observed that the macrophages could have a protumoral effect.[29,30] Additional studies have shown that macrophages support tumor growth by production of proangiogenic factors as VEGF and other angiogenic chemokines (eg, CXCL12).[31] After emergence of resistance to anti-VEGF therapy and paclitaxel in an in vivo mouse model, CSF1R inhibitor therapy added to anti-VEGF therapy restored response to antiangiogenic therapy and an 83% lower tumor burden compared to treatment with anti-VEGF therapy and paclitaxel alone.[27]
Other Interesting Combinations
Phase III clinical trials showed that adding PARP inhibitors in maintenance therapy improves PFS for patients with recurrent epithelial ovarian, fallopian-tube, or primary peritoneal cancer who had received prior platinum-based chemotherapy.[32,33] The SOLO-1 study demonstrated that the risk of disease progression or death was 70% lower with olaparib than with placebo (HR, 0.3; 95% CI, 0.23–0.41; P < .001) in patients with newly diagnosed advanced ovarian cancer who have a complete or partial response after platinum-based chemotherapy.[16] Taking into account the response rate to PARP inhibitors, the combination of PARP inhibitor with bevacizumab is the premise of the PAOLA-1 phase III clinical trial. Specifically, olaparib and bevacizumab are used in frontline maintenance in advanced ovarian cancer. Different combinations of PARP inhibitors and antiangiogenic drugs are studied in the NRG-GY005 (NCT02502266) phase II/III and NRG-GY004 (NCT02446600) phase III trials in which a PARP inhibitor is given alone or in combination with cediranib maleate in the experimental arms to determine efficacy compared with standard platinum-based chemotherapy in platinum-sensitive relapsed ovarian cancer.
VEGF inhibitors in combination with immunotherapy are also being investigated. The rationale for combining immunotherapy with VEGF inhibitors is that the latter induce abundant tumor vasculature and inhibit directly T-cell function.[34] There are several promising trials in development evaluating immunotherapy in combination with VEGF inhibitors such as NRG-GY009 (NCT02839707), ATLANTE (NCT02891824), and IMagyn050 (NCT03038100).
Possible Markers of Response to Antiangiogenic Therapy
Treatment with antiangiogenic agents can be quite expensive and can have substantial side effects. One potential solution for optimizing the treatment is to identify useful biomarkers that can allow selection of patients most likely to benefit from such therapy and potentially to detect early escape from anti-VEGF therapy. Circulating molecular and cellular biomarkers in blood would be ideal candidates, as such markers can be followed longitudinally. However, circulating protein levels (eg, VEGF or other angiogenic molecules such as placental growth factor [PIGF]) have not been particularly effective.[35]
Circulating endothelial cells (CECs) are mobilized in murine models as well as in humans in response to VEGF.[36,37] This is especially important because the level of CECs should decrease in response to anti-VEGF therapy. Although the suppression of mobilized endothelial cells was observed in patients with confirmed response to anti-VEGF therapy, an increase in value before clinical progression was not noted.[38]
Some have attempted to identify molecular subgroups of high-grade serous ovarian cancer that could predict response to anti-VEGF therapy. For example, Gourley and colleagues identified three major subgroups in the ICON7 participants based on mRNA analysis of human tissue samples. In two of the subgroups, the angiogenic genes were upregulated, while the third subgroup presented more complex features including repression of the angiogenic genes and upregulation of the immune genes. With regard to OS, the latter group had a superior OS compared to the other two subgroups. However, addition of bevacizumab therapy in this latter group was associated with worse PFS and OS compared to chemotherapy alone. This study suggests that an immune subgroup “geno-signature” with the repressed angiogenic-related expression could better select patients in whom antiangiogenic therapy could be avoided. Addition of bevacizumab in the proangiogenic group was associated with a nonsignificant trend for improved PFS compared with controls (median, 17.4 vs 12.3 months, respectively).[39]
Given the lack of reliable plasma biomarkers, imaging modalities such as CT and MRI scans are the most common assessment tools to evaluate efficacy. However, other functional imaging methods such as dynamic contrast-enhanced (DCE)-MRI and CT perfusion can provide information on tumor perfusion, vascularity, and permeability and could be useful as early markers of treatment efficacy.[38,40,41] The ACRIN 6695 study investigated whether CT perfusion biomarkers are associated with PFS in patients with advanced ovarian cancer treated with carboplatin and dose-dense or conventional paclitaxel. The patients were enrolled from the prospective phase III GOG-0262 clinical trial in which bevacizumab use was left to the physician’s choice and was overwhelmingly preferred based on the results from previous clinical trials in patients with advanced ovarian cancer. The study showed that changes in vasculature parameters within 4 weeks of initiating therapy in one or more CT-perfusion biomarkers were associated with shorter PFS, proving that these biomarkers can be considered good imaging candidates to provide early prognostic information.[41]
Future Directions
The number of antiangiogenic drugs developed during the last 30 years is impressive and is associated with improved patient outcomes. Nevertheless, due to emergence of adaptive resistance, additional therapies are needed. Steps forward would be made with the identification of predictive biomarkers that could help assess the response among patients and a better understanding of mechanisms of adaptive resistance. While neutralization of VEGF was the first approach for targeting the tumor microenvironment, additional approaches (eg, immune therapy) have been also quite successful. In this context, the potential of tumor vessel normalization using antiangiogenic drugs to improve the effectiveness of immunotherapy should be explored further. Collectively, such microenvironment-targeted approaches hold promise for further improving the outcomes of women with ovarian cancer.
FINANCIAL DISCLOSURES:Dr. Chelariu-Raicu has no significant financial interest in or other relationship with the manufacturer of any product or provider of any service mentioned in this article. Dr. Sood has received funding from Merck, Kiyatec, and Bio-Path. Dr. Coleman has been a consultant, speaker, or advisor for AbbVie, Cell Medica, Genmab, MORE Health, Takeda, Roche, Merck, Aravive, ArQule, AstraZeneca, Clovis, Eisai, Genentech, Immunogen, and Janseen.
PERSPECTIVE
ncorporating Antiangiogenic Agents in the Treatment of Advanced Ovarian Cancer
Kristina Frinzi Byers, PharmD, BCOP
The incorporation of antiangiogenic therapy in the treatment of solid tumor malignancies dates back to 2004, when bevacizumab, an anti-vascular endothelial growth factor (VEGF) monoclonal antibody, received US Food and Drug Administration (FDA) approval in advanced colorectal cancer after demonstrating an improvement in both overall and progression-free survival (PFS).[1] Studies in epithelial ovarian cancer have shown a correlation between VEGF expression and more advanced disease leading to worse survival rates.[2] After initial skepticism, bevacizumab was finally granted FDA approval in 2011 for recurrent ovarian cancer and has since received approval in 2018 as front-line therapy after initial surgical resection.[3] Other antiangiogenic agents of interest include pazopanib, nintedanib, cediranib, and navicizumab, all of which are currently being evaluated in clinical trials.
Although bevacizumab demonstrated a modest improvement in PFS, the unique toxicity profile of antiangiogenic therapies and the lack of an overall survival benefit must be considered when selecting patients most appropriate for treatment. Common adverse effects can be divided into these major categories: generalized, cardiovascular, gastrointestinal (GI), and dermatologic. Generalized symptoms primarily include fatigue, headache, dyspnea, arthralgia, and myalgia.[4] In the phase III PALETTE trial that evaluated using pazopanib in treating advanced soft-tissue sarcoma, the incidence of all-grade and grade > 3 fatigue was 65% and 13%, respectively.[5] Although not FDA approved for use in ovarian cancer, the debilitating fatigue associated with pazopanib often warrants dose modification to improve tolerability. Cardiovascular symptoms such as hypertension and venous thromboembolism can be concerning in a primarily postmenopausal population. Frequent blood pressure (BP) monitoring is essential when treating patients with baseline hypertension, and all patients should have adequate BP control prior to initiating treatment with anti-VEGF therapies. Common GI symptoms include diarrhea and abdominal pain. More severe GI adverse events (ie, perforation, fistula, and/or necrosis) have been reported in 2.9% of patients with ovarian cancer, and identifiable risk factors include history of inflammatory bowel disorder and previous bowel resection.[6] Palmar-plantar erythrodysesthesia has been reported in patients receiving anti-VEGF therapies, and early identification of symptoms is essential in preventing dose interruptions. Impaired wound healing can result in serious or fatal complications; therefore, anti-VEGF therapies should be held at least 28 days prior to and after elective invasive procedures.[4] Considering the potentially substantial toxicities associated with bevacizumab and other anti-VEGF agents, their incorporation into the standard treatment of ovarian cancer should be reserved for patients with high-risk clinical features and minimal comorbidities.
FINANCIAL DISCLOSURE:Dr. Byers has served on advisory boards for Pfizer, Tesaro, and Heron Therapeutics, and participated in surveys for The Delham Group.
2. Duncan TJ, Al-Attar A, Rolland P, et al. Vascular endothelial growth factor expression in ovarian cancer: a model for targeted use of novel therapies. Clin Cancer Res. 2008;14:3030-5.
4. Avastin (bevacizumab) [prescribing information]. South San Francisco, CA: Genentech, Inc.; February 2019.
5. van der Graaf WT, Blay JY, Chawla SP, et al; EORTC Soft Tissue and Bone Sarcoma Group; PALETTE study group. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomized, double-blind, placebo-controlled phase 3 trial. Lancet. 2012;379:1879-86.
6. Burger RA, Brady MF, Bookman MA, et al. Risk factors for GI adverse events in a phase III randomized trial of bevacizumab in first-line therapy of advanced ovarian cancer: a gynecologic oncology group study. J Clin Oncol. 2014;32:1210-7.
References:
1. Folkman J. Tumor angiogenesis: Therapeutic implications. N Engl J Med. 1971; 285:1182-6.
2. Graybill W, Sood AK, Monk BJ, Coleman RL. State of the science: emerging therapeutic strategies for targeting angiogenesis in ovarian cancer. Gynecol Oncol. 2015;138:223-6.
3. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature. 2011;473:298-307.
4. Fischer C, Mazzone M, Jonckx B, Carmeliet P.FLT1 and its ligands VEGFB and PlGF: drug targets for anti-angiogenic therapy? Nat Rev Cancer. 2008;8:942-56.
5.Mabuchi S, Terai Y, Morishige K, et al. Maintenance treatment with bevacizumab prolongs survival in an in vivo ovarian cancer model. Clin Cancer Res. 2008;14:7781-9.
6.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7-34.
7.Monk BJ, Herzog TJ, Tewari KS. Evolution of chemosensitivity and resistance assays as predictors of clinical outcomes in epithelial ovarian cancer patients. Curr Pharm Des. 2016;22:4717-28.
8.Burger RA, Brady MF, Bookman MA, et al. Gynecologic Oncology Group. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med. 2011;365:2473-83.
9.Perren TJ, Swart AM, Pfisterer J, et al. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. 2011;365:2484-96.
10.Oza AM, Cook AD, Pfisterer J, et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015;16:928-36.
11.Aghajanian C, Blank SV, Goff BA, et al. OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30:2039-45.
12.Coleman RL, Brady MF, Herzog TJ, et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017;18:779-91.
13.du Bois A, Floquet A, Kim JW, et al. Incorporation of pazopanib in maintenance therapy of ovarian cancer. J Clin Oncol. 2014;32:3374-82.
14.Harter P, Johnson T , Berton-Rigaud D, et al. BRCA1/2 mutations associated with progression-free survival in ovarian cancer patients in the AGO-OVAR 16 study. Gynecol Oncol. 2016;140:443-9.
15.Norquist BM, Brady MF, Harrell MI, et al. Mutations in homologous recombination genes and outcomes in ovarian carcinoma patients in GOG 218: an NRG Oncology/Gynecologic Oncology Group Study. Clin Cancer Res. 2018;24:777-83.
16.Moore K, Colombo N, Scambia G, et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N Engl J Med. 2018;379:2495-505.
17.du Bois A, Kristensen G, Ray-Coquard I, et al. Standard first-line chemotherapy with or without nintedanib for advanced ovarian cancer (AGO-OVAR 12): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet Oncol. 2016;17:78-89.
18.Vergote I, Scambia G, O’Malley DM, et al. Trebananib or placebo plus carboplatin and paclitaxel as first-line treatment for advanced ovarian cancer (TRINOVA-3/ENGOT-ov2/GOG-3001): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019;20:862-76.
19.Pujade-Lauraine E, Hilpert F, Weber B, et al. AURELIA: A randomized phase III trial evaluating bevacizumab (BEV) plus chemotherapy (CT) for platinum (PT)-resistant recurrent ovarian cancer (OC). J Clin Oncol. 2012;30(suppl):abstr LBA5002.
20.Monk BJ, Poveda A, Vergote I, et al. Anti-angiopoietin therapy with trebananib for recurrent ovarian cancer (TRINOVA-1): a randomised, multicentre, double-blind, placebo-controlled phase 3 trial. Lancet Oncol. 2014;15:799-808.
21.Marth C, Vergote I, Scambia G, et al. ENGOT-ov-6/TRINOVA-2: Randomised, double-blind, phase 3 study of pegylated liposomal doxorubicin plus trebananib or placebo in women with recurrent partially platinum-sensitive or resistant ovarian cancer. Eur J Cancer. 2017;70:111-21.
22.Pignata S, Lorusso D, Joly F. et al Chemotherapy plus or minus bevacizumab for platinum-sensitive ovarian cancer patients recurring after a bevacizumab containing first line treatment: the randomized phase 3 trial MITO16B-MaNGO OV2B-ENGOT OV17. J Clin Oncol. 2018;36(suppl):abstr 5506.
23.Pfisterer J, Dean AP, Baumann K. et al. Carboplatin/pegylated liposomal doxorubicin/bevacizumab (CD-BEV) vs. carboplatin/gemcitabine/bevacizumab (CG-BEV) in patients with recurrent ovarian cancer. A prospective randomized phase III ENGOT/GCIG-Intergroup study (AGO Study Group, AGO-Austria, ANZGOG, GINECO, SGCTG). Ann of Oncol. 2018:29(suppl 8):abstr 9330.
24.Ledermann JA, Embleton AC, Raja F, et al. Cediranib in patients with relapsed platinum-sensitive ovarian cancer (ICON6): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2016; 387:1066-74.
25.Noguera-Troise I, Daly C, Papadopoulos NJ, et al. Blockade of Dll4 inhibits tumour growth by promoting non-productive angiogenesis. Nature. 2006;444:1032-1037.
26.Huang J, Hu W, Hu L, et al. Dll4 inhibition plus aflibercept markedly reduces ovarian tumor growth. Mol Cancer Ther. 2016;15:1344-52.
27.Lyons YA, Pradeep S, Wu SY, et al. Macrophage depletion through colony stimulating factor 1 receptor pathway blockade overcomes adaptive resistance to anti-VEGF therapy. Oncotarget. 2017;8:96496-505.
28.Jimeno A, Morre KN, Gordon M, et al. A first-in-human phase 1a study of the bispecific anti-DLL4/anti-VEGF antibody navicixizumab (OMP-305B83) in patients with previously treated solid tumors. Invest New Drugs. 2019;37:461-72.
29.Lin EY, Nguyen AV, Russell RG, Pollard JW. Colony-stimulating factor 1 promotes progression of mammary tumors to malignancy. J Exp. Med. 2001;193,727-40.
30.Lin EY, Pollard JW. Tumor-associated macrophages press the angiogenic switch in breast cancer. Cancer Res. 2007;67:5064-6.
31.Hughes R, Qian BZ, Rowan C, et al. Perivascular M2 macrophages stimulate tumor relapse after chemotherapy. Cancer Res. 2015;75:3479-91.
32.Mirza MR, Monk BJ, Herrstedt J, et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375:2154-64.
33.Coleman RL, Oza AM, Lorusso D, et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390:1949-61.
34.Yang J, Yan J, Liu B. Targeting VEGF/VEGFR to modulate antitumor immunity. Front Immunol. 2018;9:978.
35.Jain RK, Duda DG, Willett CG, et al. Biomarkers of response and resistance to antiangiogenic therapy. Nat Rev Clin Oncol. 2009;6:327-38.
36.Takahashi T, Kalka C, Masuda H, et al. Ischemia- and cytokine-induced mobilization of bone marrow-derived endothelial progenitor cells for neovascularization. Nat Med. 1999;5:434-8.
37.Kalka C, Masuda H, Takahashi T, et al. Vascular endothelial growth factor(165) gene transfer augments circulating endothelial progenitor cells in human subjects. Circ Res. 2000;86:1198-202.
38.Coleman RL, Duska LR, Ramirez PT, et al. Phase 1-2 study of docetaxel plus aflibercept in patients with recurrent ovarian, primary peritoneal, or fallopian tube cancer. Lancet Oncol. 2011;12:1109-17.
39.Gourley C, McCavigan A, Perren T, et al. Molecular subgroup of high-grade serous ovarian cancer (HGSOC) as a predictor of outcome following bevacizumab. J Clin Oncol. 2014;32(suppl):5502.
40.Lockhart AC, Rothenberg ML, Dupont J, et al. Phase I study of intravenous vascular endothelial growth factor trap, aflibercept, in patients with advanced solid tumors. J Clin Oncol. 2010;28:207-14.
41.Ng CS, Zhang Z, Lee SI, et al. CT perfusion as an early biomarker of treatment efficacy in advanced ovarian cancer: an ACRIN and GOG study. Clin Cancer Res. 2017;23:3684-91.
Scientists say they have shown how controlling cholesterol metabolism in pancreatic cancer cells reduces metastasis, pointing to a potential new treatment using drugs previously developed for atherosclerosis.
“We show for the first time that if you control the cholesterol metabolism you could reduce pancreatic cancer spread to other organs,” said Ji-Xin Cheng, Ph.D., a professor in Purdue University’s Weldon School of Biomedical Engineering and Department of Chemistry. “We chose pancreatic cancer to test this approach because it is the most aggressive disease of all the cancers.”
Dr. Cheng had previously led a team of researchers discovering a link between prostate cancer’s aggressiveness and the accumulation of a compound produced when cholesterol is metabolized in cells, findings that could bring new diagnostic and treatment methods. The new study involved researchers at the Purdue Center for Cancer Research and School of Biomedical Engineering, the Indiana University Simon Cancer Center and School of Medicine, and Purdue’s Department of Biological Sciences, Department of Comparative Pathobiology, and Department of Biochemistry.
The findings, detailed in a paper (“Abrogating Cholesterol Esterification Suppresses Growth and Metastasis of Pancreatic Cancer”) just published in Oncogene, suggest that a class of drugs previously developed to treat atherosclerosis could be repurposed for treatment of pancreatic cancer and other forms of cancer. Atherosclerosis is the buildup of fats, cholesterol, and other substances in arteries, restricting blood flow.
The researchers found accumulations of the compound cholesteryl ester in human pancreatic cancer specimens and cell lines, demonstrating a link between cholesterol esterification and metastasis. Excess quantities of cholesterol result in cholesteryl ester being stored in lipid droplets within cancer cells.
“The results of this study demonstrate a new strategy for treating metastatic pancreatic cancer by inhibiting cholesterol esterification,” said Jingwu Xie, Ph.D., the Jonathan and Jennifer Simmons Professor at the Indiana University School of Medicine and a researcher at the Indiana University Melvin and Bren Simon Cancer Center.
The paper’s lead author is Purdue postdoctoral fellow Junjie Li, Ph.D. Purdue researchers have developed an analytical tool, Raman spectromicroscopy, that allows compositional analysis of single lipid droplets in living cells.
“We identified an aberrant accumulation of cholesteryl ester in human pancreatic cancer specimens and cell lines,” Dr. Li said. “Depletion of cholesterol esterification significantly reduced pancreatic tumor growth and metastasis in mice.”
Findings show that drugs like avasimibe, previously developed for treatment of atherosclerosis, reduced the accumulation of cholesteryl ester. Pancreatic cancer usually kills within a few months of diagnosis. It is hoped the potential new treatment might extend life of these patients for a year, Cheng said.
The accumulation of cholesteryl ester is controlled by an enzyme called acyl-coenzyme A acyltransferase-1 (ACAT-1), and findings have correlated a higher expression of the enzyme with a poor survival rate for patients. The researchers analyzed tissue samples from pancreatic cancer patients and then tested the drug treatment in a type of laboratory mice referred to as an orthotopic mouse model, developed at the IU School of Medicine. Specimens of human pancreatic tissues were obtained from the Simon Cancer Center Solid Tissue Bank.
Imaging showed a decrease of the number of lipid droplets, and Raman spectral analysis verified a significant reduction of cholesteryl ester in the lipid droplets, suggesting that avasimibe acted by blocking cholesterol esterification. The drug did not induce weight loss, and there was no apparent organ toxicity in the liver, kidney, lung and spleen, Dr. Cheng said.
Findings also showed that blocking storage of cholesteryl ester causes cancer cells to die, specifically due to damage to the endoplasmic reticulum, a workhorse of protein and lipid synthesis.
“By using avasimibe, a potent inhibitor of ACAT-1, we found that pancreatic cancer cells were much more sensitive to ACAT-1 inhibition than normal cells,” added Dr. Cheng.
Additional research confirmed that the anticancer effect of avasimibe is specific to ACAT-1 inhibition. The researchers performed various biochemical assays and “genetic ablation” to confirm the drug’s anticancer effect.
“The results showed that avasimibe treatment for four weeks remarkably suppressed tumor size and largely reduced tumor growth rate,” said paper co-author Timothy Ratliff, the Robert Wallace Miller Director of Purdue’s Center for Cancer Research. “Metastatic lesions in lymph nodes and distant organs also were assessed at the end of the study. A much higher number of metastatic lesions in lymph nodes were detected in the control group than the avasimibe-treated group.”
Each mouse in the control group showed at least one metastatic lesion in the liver. In contrast, only three mice in the avasimibe-treated group showed single lesion in liver.
Abrogating cholesterol esterification suppresses growth and metastasis of pancreatic cancer
Cancer cells are known to execute reprogramed metabolism of glucose, amino acids and lipids. Here, we report a significant role of cholesterol metabolism in cancer metastasis. By using label-free Raman spectromicroscopy, we found an aberrant accumulation of cholesteryl ester in human pancreatic cancer specimens and cell lines, mediated by acyl-CoA cholesterol acyltransferase-1 (ACAT-1) enzyme. Expression of ACAT-1 showed a correlation with poor patient survival. Abrogation of cholesterol esterification, either by an ACAT-1 inhibitor or by shRNA knockdown, significantly suppressed tumor growth and metastasis in an orthotopic mouse model of pancreatic cancer. Mechanically, ACAT-1 inhibition increased intracellular free cholesterol level, which was associated with elevated endoplasmic reticulum stress and caused apoptosis. Collectively, our results demonstrate a new strategy for treating metastatic pancreatic cancer by inhibiting cholesterol esterification.
Metastasis is the major cause of cancer-related mortality. Though localized tumors can often be treated by surgery or other therapies, treatment options for metastatic diseases are limited. Cancer metastasis has been revealed to be a multiple step process, including cancer cell migration, local invasion, intravasation, circulation through blood and lymph vessels, extravasation, survival and colonization in distant organs.1, 2, 3Mediators identified in these processes have provided the basis for the development of therapies to target metastasis. Current therapeutic strategies for treating metastatic tumors mainly focus on targeting the adhesive molecules and extracellular proteases.4However, these therapeutics have not been proven to be effective in clinical trials, partially owing to the various escape mechanisms used by the metastatic cancer cells.2, 5, 6 Thus, an unmet need exists to develop new therapeutic strategies for treating metastatic cancers.
Recent advances in cancer metabolism have unveiled many potential therapeutic targets for cancer treatment. Metabolic reprogramming, a strategy used by cancer cells to adapt to the rapid proliferation, is being recognized as a new hallmark of cancer.7 Substantial studies have found increased glycolysis, glutaminolysis, nucleotide and lipid synthesis in cancer cells.7, 8, 9,10 Considering that altered metabolic pathways only happen in cancer cells but not in normal cells, targeting these pathways may provide cancer-specific treatments. A number of inhibitors of metabolic enzymes, such as glycolysis inhibitors, are under clinical trials as targeted cancer therapeutics.11
Of various metabolic pathways, lipid metabolism has been suggested to have an important role in cancer cell migration, invasion and metastasis.12 A recent study reported that surrounding adipocytes provide energy source for ovarian cancer cells to promote its rapid growth and metastasis.13 Blocking lipidde novo synthesis pathway has been shown to suppress tumor regrowth and metastasis after anti-angiogenesis treatment withdrawal.14 In parallel, lipolysis by the enzyme monoacylglycerol lipase was shown to regulate the fatty acid network, which promotes cancer cell migration, invasion and growth.15
Cholesterol, a critical component of the plasma membrane, is also implied to be correlated to cancer metastasis.16 It has been shown that prostate cancer bone metastases contain a high level of cholesterol.17 Modulation of cholesterol level in plasma membrane was shown to regulate the capability of cell migration.18, 19Moreover, cholesterol-enriched lipid rafts were shown to have an essential role in cancer cell adhesion and migration.20 Mammalian cells obtain cholesterol either from de novo synthesis or from the uptake of low-density lipoprotein (LDL).21 Inside cells, excess free cholesterol is esterified and stored as cholesteryl ester (CE) in lipid droplets (LDs), which is mediated by acyl-CoA cholesterol acyltransferase (ACAT).22 Increased CE level has been reported in breast cancer,23 leukemia,24 glioma25 and prostate cancer.26Despite these advances, the role of cholesterol esterification in cancer progression, especially in cancer metastasis, is not well understood.
In this article, we report a link between cholesterol esterification and metastasis in pancreatic cancer. Using stimulated Raman scattering (SRS) microscopy and Raman spectroscopy to map LDs stored inside single cells and analyze the composition of individual LDs, we identified an aberrant accumulation of CE in human pancreatic cancer specimens and cell lines. Abrogation of cholesterol esterification, either by inhibiting ACAT-1 enzyme activity or by shRNA knockdown of ACAT-1 expression, significantly reduced pancreatic tumor growth and metastasis in an orthotopic mouse model. Mechanistically, inhibition of cholesterol esterification disturbed cholesterol homeostasis by increasing intracellular free cholesterol level, which was associated with elevated endoplasmic reticulum (ER) stress and eventually led to apoptosis.
In this study, we revealed a link between CE accumulation and pancreatic cancer metastasis. Accumulation of CE via ACAT-1 provides a mechanism to keep high metabolic activity and avoid toxicity from excess free cholesterol. Previously, CE has been reported in breast cancer,23 leukemia,24 glioma25 and prostate cancer.26 Inhibition of cholesterol esterification was shown to suppress tumor growth or cancer cell proliferation.24, 25, 26 Here, we demonstrate that inhibition of cholesterol esterification can be used to treat metastatic pancreatic cancer.
Cholesterol is an essential lipid having important roles in membrane construction, hormone production and signaling.21Aberrant cholesterol metabolism is known to be associated with cardiovascular diseases and cancers.35, 36 Statins, inhibitors of HMG-CoA reductase, have been explored as potential therapies for pancreatic cancer.37 However, statins were not associated with a reduced risk of pancreatic cancer in clinical trials.38 One possible reason is that HMG-CoA reductase is also required for downstream protein prenylation, a critical process for protein activation.39Thus, the effect of statin is not just inhibiting cholesterol synthesis, but also other pathways which may render toxicity to normal cells. This non-specific toxicity is a possible reason for the limited anti-cancer outcome of statin in clinical trials.
Our study identified cholesterol esterification as a novel target for suppression of pancreatic cancer proliferation and metastasis. Inhibitors of ACAT-1 are expected to have great value as cancer-targeting therapeutics, as CE accumulation only occurs in cancer tissues or cell lines. Our animal studies with avasimibe treatment showed no adverse effect to the animals at a dosage of 15mg/kg. More importantly, modulation of cholesterol esterification suppressed not only tumor growth but also tumor metastasis. These results are expected to stimulate further biological studies to fully appreciate the role of cholesterol metabolism in cancer initiation and progression. As CE accumulation happens in several types of aggressive cancer, blocking cholesterol esterification could be pursued as a therapeutic strategy for other types of cancers. By combining with existing chemotherapies, such as gemcitabine, we believe this metabolic treatment possesses high possibilities to extend patients’ survival time by retarding cancer progression and metastasis.
The molecular mechanism that links CE accumulation to cancer aggressiveness needs further studies. One possible mechanism is that cholesterol esterification keeps signaling pathways active by maintaining a low free cholesterol environment. One of the possible targets is the caveolin-1 signaling pathway. Caveolin-1, a regulator of cellular cholesterol homeostasis, is considered as a marker for pancreatic cancer progression.11 Particularly, a promoting role of caveolin-1 in pancreatic cancer metastasis has been reported.40 Our preliminary studies showed ACAT-1 inhibition reduced the expression level of SREBP1, caveolin-1 and phosphorylated ERK1/2 (unpublished data). The effect on caveolin-1 is probably mediated by SREBP1, which senses the intracellular cholesterol homeostasis.41 Meanwhile, caveolin-1 may have an important role in mediating the action of SREBP1 on MAPK pathways,42, 43 which are known to have essential roles in cancer cell metastasis.44 Therefore, it is possible that increased free cholesterol level induced by ACAT-1 inhibition inactivates SREBP1, leading to downregulation of caveolin-1/MAPK pathway, which contributes to the reduced cancer aggressiveness.
Besides the caveolin-1/MAPK signaling, other possibilities include the potential alteration of the membrane composition, such as lipid rafts, by ACAT-1 inhibition. Lipid rafts are known to provide platforms for multiple cellular signaling pathways.20 Thus, modulation of cholesterol metabolism is likely to have more profound effects via other signaling pathways. Future studies are needed to fully elucidate the molecular mechanism.















")



 ncorporating Antiangiogenic Agents in the Treatment of Advanced Ovarian Cancer
ncorporating Antiangiogenic Agents in the Treatment of Advanced Ovarian Cancer
{kind=link}
{kind=link}
{kind=link}
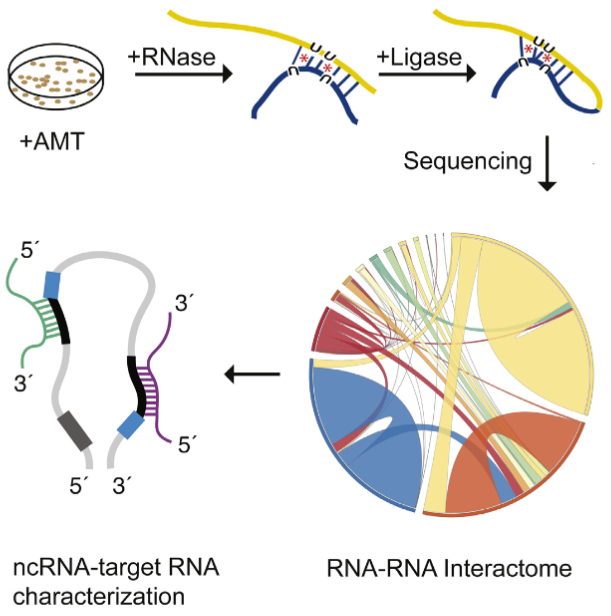{kind=link}
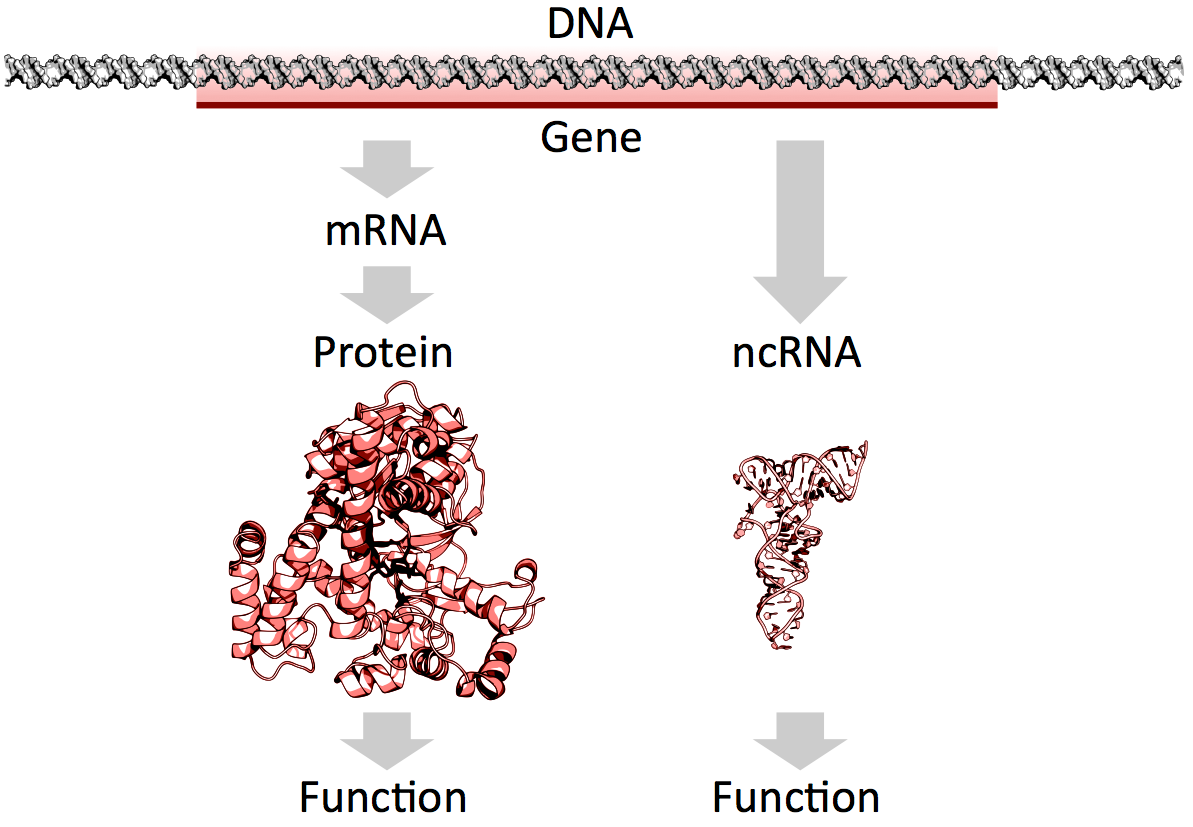{kind=link}
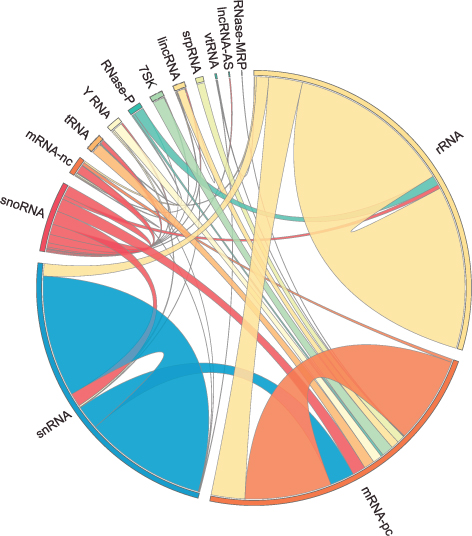{kind=link}
{kind=link}
{kind=link}
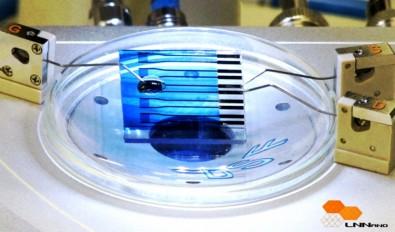{kind=link}
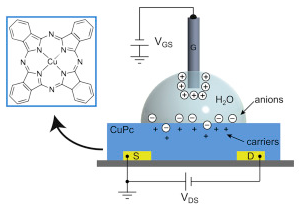{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}