3D Cardiovascular Theater – Hybrid Cath Lab/OR Suite, Hybrid Surgery, Complications Post PCI and Repeat Sternotomy
Curator: Aviva Lev-Ari, PhD, RN

Article ID #70: Cardiovascular Original Research: Cases in Methodology Design for Content Curation and Co-Curation. Published on 7/19/2013
WordCloud Image Produced by Adam Tubman
This article has THREE Parts:
Part One: Hybrid Cath Lab/OR Suite for Hybrid Surgery
Part Two: Cardiac Surgery
Part Three: Invasive Interventions with Complications
1. Repeat Sternotomy Post CABG and/or Aortic Valve Replacement
2. Complications Post PCI – Pump Catheter in Use
The voice of Series A Content Consultant, Justin D Pearlman, MD, PhD, FACC
The leading cause of death and disability from any cause is cardiovascular disease, principally, heart attacks and strokes. Both the heart and brain typically allow only 10 minutes or so of inadequate blood supply before starting a committed course of permanent tissue injury, progressing in severity as time goes by without successful interruption of the disease process. Thus there is great time urgency to get patients to a definitive treatment that can stop the injury and restore adequate nutrient blood supply. Many patients can benefit from a catheterization to identify blockages and insert a small balloon within the blockage to expand the narrow channel, often followed by placement of a stent (wire cage) to maintain the expanded vessel diameter. Chemicals released over time from drug-eluting stents can prevent tissue in growth that may obstruct stents. These emergeny interventions are not always successful. There may be complications from the attempt to access an entry artery, and the blockages may not be amenable to a balloon. When such limitations are encountered, the next chance to help is surgical, with continued time pressure.
The fastest way to make the transition from a diagnostic catheterization to a timely intervention is a hybrid intervention suite that offers non-invasive imaging, catheterization and surgery all in one location. The following articles present the current state of hybrid “do it all” intervention suites. Additional articles address the risks of bad outcomes from such interventions.
Part One
Hybrid Cath Lab/OR Suite for Hybrid Surgery
In ACC.10 and i2 Summit, 59th Annual Scientific Session, 3/14-3/16, 2010, Alfred A. Bove, M.D., Ph.D., F.A.C.C., ACC President addressed the conference attendees:
Welcome to the all-new Hybrid Cath Lab/OR and 3D CV Theater. Recent developments in cardiac surgery and interventional cardiology have led to the creation of integrated, hybrid cath lab/operating rooms (OR), which provide significant advantages in the diagnosis and treatment of patients requiring cardiac procedures—helping to facilitate a rapid-response approach. These multimodality rooms are designed to support a variety of integrated surgical and endovascular procedures. We are excited to provide you with this opportunity to get a first-hand look—and feel—of the latest technologies. We hope you take the time to explore this interactive, multivendor venue. Learning is at the core of the ACC Annual Scientific Session and we invite you to expand your educational experience in this dynamic learning environment.
In the Hybrid Cath Lab/OR Suite, you’ll discover how integrating cutting edge angiographic and surgical equipment and technologies can facilitate a broad range of procedures within one location. Additionally, you will learn how hybrid suites are providing solutions that enable interventionalists and surgeons to work collaboratively to provide the best treatment options for patients. The adjoining 3D CV Theater features presentations by physicians currently performing intravascular and surgical procedures in hybrid suites. Each live presentation pairs a cardiologist with a surgeon, allowing you to hear perspectives from both sides on a variety of hybrid suite procedures and cases. In addition, the Theater offers video presentations of cases from around the world.
The ACC thanks the supporters of the Hybrid Suite for providing us with the opportunity to share this unique learning destination with you.
http://www.expo.acc.org/acc12/CUSTOM/images/ACC12/ACC.10%20Hybrid%20Suite%20Directory.pdf
Hybrid Cath Lab/OR Suite for Hybrid Surgery
Procedures Performed in a Hybrid Suite
The treatment of cardiovascular diseases has undergone a paradigm shift within the last few years, from
- open surgery to minimally invasive surgical procedures and from
- limited percutaneous catheter-based interventions to hybrid interventions for the entire cardiovascular tree.
The Hybrid Suite
are perfect examples of procedures that could, and should, be carried out in a hybrid OR. High-risk patients who require less invasive interventions are the best candidates for treatment in a hybrid suite.
As cardiac surgery becomes less invasive, incisions are becoming smaller and smaller, and even totally endoscopic heart surgery is now possible. Cardiac surgeons have started to perform procedures that include catheter-based skills, such as transapical valve replacement. For these operations, surgeons need more sophisticated imaging techniques, fluoroscopy and contrast injections. The hybrid OR offers all these facilities. Perhaps the most obvious and easiest procedure that can be performed in a hybrid OR is coronary revascularization combining coronary artery bypass grafting with on-table intra-operative completion angiography for quality control. If the surgeon detects a problem during the procedure, he or she can revise the graft immediately and thereby prevent potential perioperative and long-term complications. Currently, cardiologists and cardiovascular surgeons have shown special interest in so-called hybrid coronary interventions, which are combinations of minimally invasive coronary artery bypass grafting and percutaneous coronary interventions. In these procedures, cardiovascular surgeons place a left-internal mammary artery bypass graft to the left-anterior descending artery through small incisions (MIDCAB) or completely endoscopically (TECAB), while any remaining obstructed coronary arteries are treated with stents by an interventional cardiologist. This procedure is an attractive alternative to multivessel open coronary artery bypass grafting. Transcatheter heart-valve replacement and repair are especially suited to a hybrid suite because percutaneous transfemoral and transapical aortic valve repairs include risks that can only be treated successfully by immediate surgical intervention, such as coronary artery obstruction, aortic dissection and aortic perforations.
In addition, endovascular aortic stent grafting for the repair of abdominal aortic aneurysms is a suitable procedure for a hybrid operating room. Endovascular aneurysm repair has become an established alternative to open repair and is increasingly used for thoracic aorta repair as well. Some
- emergency procedures for traumatic lesions of the thoracic aorta and
- fulminant pulmonary embolism may also be performed in a hybrid OR. Several
- pediatric interventions can be carried out in a hybrid suite as well, such as implantation of closure devices for atrial and ventricular septal defects in small children and
- treatments for hypoplastic left-heart syndrome.
http://www.expo.acc.org/acc12/CUSTOM/images/ACC12/ACC.10%20Hybrid%20Suite%20Directory.pdf
In a recent article we reported on the Change in Requirement for Surgical Support by Cath Labs for performance of Nonemergent PCI without Surgical Backup, that increases the autonomy of Interventional Cardiologists. In the Hybrid OR that change is irrelevant since the presence of a Cardiac Surgeon is a fact of the division of labor between the two types of specialties. Cardiac Surgeons are involved with percutaneous transfemoral and transapical aortic valve repairs and intervention for endoscopic aorta, AAA and Thoracic AA grafting.
AHA, ACC Change in Requirement for Surgical Support: Class IIb -> Class III, Level of Evidence A: Supports Nonemergent PCI without Surgical Backup (Change of class IIb, level of Evidence B).
What is a Cardiovascular Hybrid Suite?
Cardiovascular hybrid suite is a state-of-the-art operating room equipped with a fully functional catheterization laboratory, thus allowing surgical procedures and catheter-based interventions to be carried out in the same room. Hybrid suites provide a place where treatments traditionally available only in a cath lab and procedures only available in an operating room can be performed together to provide patients with the best available combination of therapies for cardiovascular disease. These multidisciplinary, integrated cardiovascular procedural suites bring the best of two worlds together by combining all the advantages of a modern cath lab with an up-to-date cardiovascular surgery operating room (OR).
Hybrid suites began to evolve in the mid to late 1990s, when some groups of interventional cardiologists started sharing operating rooms with cardiovascular surgeons. The appeal of the hybrid suite concept has grown as have catheter based devices (stents, coils, balloons and lasers) have been developed that enable interventional cardiologists to advance the invasiveness and effectiveness and applications of percutaneous transcatheter interventions. The interest in these suites has also increased as cardiovascular surgeons have developed a variety of techniques for
- Minimally invasive procedures, such as minimally invasive direct coronary artery bypass grafting (MIDCAB) or
- Totally endoscopic coronary artery bypass grafting (TECAB).
With the advent of more tools, interventional cardiologists are becoming more like surgeons, and with less invasive tools, cardiovascular surgeons are becoming more like interventionalists. Rather than separating surgical procedures from interventional procedures performed in traditional operating rooms and cath labs, hybrid suites provide a high-tech environment that allows cardiologists and surgeons to work together to offer patients complex, minimally invasive therapies.
Some experts believe that hybrid suites represent the wave of the future in cardiovascular care and that most heart centers will eventually install hybrid suites to offer patients the latest cardiovascular procedures safely and effectively with minimal surgical trauma. The rooms can be costly to build and equip, but if a medical center is considering building a new operating room or cath lab, setting up a hybrid suite makes sense. Medical centers that have a hybrid suite available can clearly differentiate themselves in a positive way from centers that do not have such capabilities.
The Benefits of a Hybrid Suite for Medical Centers
While building a hybrid suite is more expensive than building a traditional operating room or cath lab, a hybrid suite can potentially be used for all types of cardiovascular procedures, including
- traditional cardiac and vascular surgery,
- interventional coronary procedures,
- endovascular aortic procedures and
- electrophysiology procedures.
Hybrid suites reinforce the trend in cardiovascular care toward less invasive, comprehensive hybrid procedures. Once a hybrid suite is in place, the demand for its use will likely grow due to increasing indications and referrals for these innovative treatments, many of which are increasingly covered by third-party payers.
http://www.expo.acc.org/acc12/CUSTOM/images/ACC12/ACC.10%20Hybrid%20Suite%20Directory.pdf
What Equipment is Needed?
Interventional cath labs usually have excellent imaging capabilities but lack the sterile facilities and staff needed for a formal OR, while operating rooms frequently lack high-level imaging equipment. Some of the essential equipment for a hybrid suite includes:
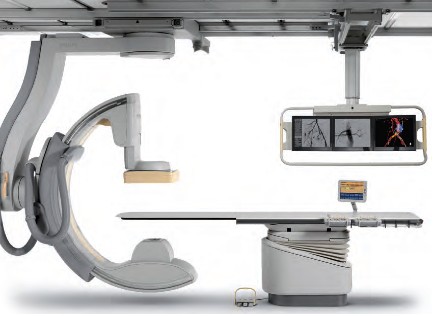
• A state-of-the-art imaging system capable of performing 3D rotational angiography, CT scanning, and ultrasound is advantageous. Floor-mounted and ceiling-mounted systems are available, but many hospitals use ceiling-mounted systems because access to the patient is slightly easier. Some ceiling-mounted systems provide 3D imaging from the surgeon’s position perpendicular to the patient. However, some hospitals prefer floor-mounted systems because having mechanical parts running above the operative field may cause dust to fall, resulting in infections. An important aspect is that the C-arm can be parked away when it is not used. This especially enhances access of the anesthesia team to the patient.
• An operating table that meets the needs of both surgeons and interventionalists by electronically integrating the table with the imaging system is also essential. These tables should have retractable rails for retractors and other surgical tools. To perform 3D imaging on the operating table, the C-arm of the imaging system should allow fast and precise rotation around the patient.
• A variety of other surgical and interventional systems and equipment may also be needed, including a robotic surgical system, a heart-lung machine, an image integration system, an endoscopic imaging system, a radiology display system, an audiovisual system to move images to different monitors and an anesthesia monitoring system, including transesophageal echocardiography. Some equipment like the integrated OR table and the angiography unit need to be fixed parts of the hybrid OR. Some equipment will be mobile in order to maintain some flexibility in workflow.





Who are the Equipment Vendors?
Philips Healthcare
Phone: 800-934-7372
Email: healthcare@philips.com
Web: http://www.philips.com/healthcare
Philips is one of the world’s leading technology companies, with a long history of practical innovation and visionary design. In healthcare, we are committed to understanding the human and technological needs of patients and caregivers. We believe this understanding will help us deliver solutions that not only enable more confident diagnoses and more efficient delivery of care, but also improve the overall experience of care. We offer equipment, software and services for imaging, patient monitoring, resuscitation and much more. A Hybrid OR can help make life simpler for the interdisciplinary teams who operate in this environment every day. As a world leader in cardiovascular X-ray, Philips has the experience and expertise to deliver the first class technology you need to perform minimally invasive procedures with speed, accuracy and confidence. A long history of innovation has enabled Philips to develop pioneering imaging solutions that really make a difference.
For example, Philips Allura Xper cardiovascular X-ray systems are designed to deliver enhanced imaging with superb performance for all cardiac projections, and our iE33 ultrasound system with Live 3D TEE and QLAB can assist interventional procedures and provide comprehensive quantitative information to support critical decisions. Our cardiology informatics solutions help you manage patient information throughout the cardiovascular care continuum. Philips solutions allow minimally invasive and catheter-based procedures to take place in the same suite as conventional cardiac surgery.
Phillips EchoNavigator – X-Ray and 3-D Ultrasound is described in:
Minimally Invasive Structural CVD Repairs: FDA grants 510(k) Clearance to Philips’ EchoNavigator – X-ray and 3-D Ultrasound Image Fused.
Intuitive Surgical, Inc.
da Vinci.Surgery by Intuitive Surgical, Inc.
Phone: 800-876-1310
Email: info@intusurg.com
Web: http://www.intuitivesurgical.com
Intuitive Surgical, Inc. is the global technology leader in robotic-assisted, minimally invasive surgery. The company’s da Vinci® Surgical System offers breakthrough capabilities that enable cardiac surgeons to use a minimally invasive approach and avoid median sternotomy.
Content of FDA Warning Letter, following FDA Inspection on dates 04/01/2013 – 05/30/2013 – it discussed in
Hybrid Cath Lab/OR Suite’s da Vinci Surgical Robot of Intuitive Surgical gets FDA Warning Letter on Robot Track Record
MAVIG GmbH
Phone: 631-266-2229,
585-247-1212 ext. 60
Email: info@mavig.com
Web: http://www.mavig.com
MAVIG’s specialty is ceiling/boom suspension systems for lighting (exam, surgical and LED), monitor-suspension systems—single, multibank (one to eight) systems and widescreen, overhead radiation shielding and contrast injector adapters. MAVIG also manufactures radiation protection products such as aprons, gloves, table-attachable lower body shields, adjustable- and fixed-height mobile and modular barriers.
Toshiba America Medical Systems, Inc.
Phone: 714-730-5000
Email: mktgcomm@tams.com
Web: http://www.medical.toshiba.com
Creating a hybrid lab may be complicated, but having an experienced partner that listens makes all the difference. Toshiba’s unique blend of hybrid experience and industry recognized Infinix™-i imaging systems for the Cath Lab.
Hybrid Cath Lab/OR Suite in Leading Hospitals in the US
- The Hybrid Cath Lab/OR Suite at New York Presbyterian Hospital/Columbia University Medical Center, New York, NY is presented in
Becoming a Cardiothoracic Surgeon: An Emerging Profile in the Surgery Theater and through Scientific Publications
- The Hybrid Cath Lab/OR Suite at Cleveland Clinic, Cleveland, Ohio is presented in
Heart Transplant (HT) Indication for Heart Failure (HF): Procedure Outcomes and Research on HF, HT @ Two Nation’s Leading HF & HT Centers
Speakers at 3D CV Theater, 2010 are working in Hospitals where Hybrid Cath Lab/OR Suite are in operations at the present time. The list include the following Hospitals with a Hybrid Cath Lab/OR Suite:
- Vanderbilt Medical Center, Nashville, TN
- University of Maryland Heart Center, Baltimore, MD
- The Heart Center at Nationwide Children’s Hospital, Columbus, Ohio
- The Robotic Surgical Center, East Carolina University Department of Surgery, Greenville, N.C.
- University of Washington Medicine Regional Heart Center, Seattle, WA
- Brigham and Women’s Hospital, Boston, MA
- Saint Joseph’s Hospital and Peachtree Cardiovascular and Thoracic Surgery, Atlanta, GA
- Emory University Hospital, Atlanta, GA
- Beth Israel Deaconess Medical Center, Boston, MA
- Boston Medical Center, Boston, MA
- Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN
- Lankenau Hospital, Lancaster, PA
- Cardiac Non-Invasive Laboratory at Cedars-Sinai Medical Center, Los Angeles, CA
- Robotic Surgery at St. Joseph’s Hospital, Atlanta, GA
Speakers at 3D CV Theater, 2010, included the following Cardiovascular Interventionists leading the adoption process of Hybrid Surgery in Hybrid Cath Lab/OR Suite into care modalities for cardiovascular disease:
Johannes O. Bonatti, M.D., is professor of surgery and director of coronary surgery and advanced coronary interventions at the University of Maryland Heart Center, Baltimore. He received his training in general surgery and cardiac surgery at the department of surgery at Innsbruck Medical University in Austria. Prior to his arrival at the University of Maryland, he worked at this institution as an attending surgeon and associate professor. Dr. Bonatti’s main interest is the development of minimally invasive, totally endoscopic coronary artery bypass grafting (TECAB) procedures using robotic technology.
As one of the international leaders in this field, he performed the largest series of robotic TECAB on the arrested heart, including single-, double- and triple-vessel TECAB. He has published significantly on procedure development and the implementation process of completely endoscopic coronary surgery using the da Vinci robotic system. Together with colleagues from interventional cardiology, Dr. Bonatti is working on integrated concepts for treatment of coronary artery disease. He was the first to perform a simultaneous hybrid coronary intervention using TECAB and placement of a coronary stent. He is organizing international meetings on hybrid interventions in cardiovascular medicine (http://www.icrworkshop.com). He has trained heart surgeons from around the world in the use of the da Vinci robot for heart surgery and he has introduced TECAB procedures in Austria, the Czech Republic, Greece, Turkey, India and Australia.
John G. Byrne, M.D., is the William S. Stoney Professor of Cardiac Surgery at Vanderbilt University School of Medicine and chair of the department of cardiac surgery at Vanderbilt Medical Center, Nashville, TN.
Before moving to Vanderbilt, he was associate chief and residency program director in the division of cardiac surgery at Brigham and Women’s Hospital, and associate professor of surgery at Harvard Medical School, Cambridge, MA. A graduate of the University of California, Davis, he received his medical degree in 1987 from Boston University. His postdoctoral training was completed at the University of Illinois affiliated hospitals and Brigham and Women’s Hospital in Boston.
Dr. Byrne is the author of more than 100 scientific articles on cardiac surgery and related areas. His patient care emphasis is
- aortic root surgery,
- coronary artery disease and
- valve surgery
He is board-certified in general surgery and thoracic surgery.
John P. Cheatham, M.D., is director of cardiac catheterization and interventional therapy and codirector of The Heart Center at Nationwide Children’s Hospital, Columbus, Ohio. He is also the George H. Dunlap Endowed Chair in Interventional Cardiology and professor of pediatrics and internal medicine at The Ohio State University College of Medicine. Dr. Cheatham’s area of expertise is transcatheter intervention and hybrid therapy of newborns, children and adults with complex congenital heart disease. He has pioneered several new techniques and devices in non-surgical intervention and is a leader in developing hybrid therapies. He has been a principal investigator in numerous FDA-sponsored clinical trials evaluating non-surgical closure devices and stent therapy over the past two decades. Additionally, Dr. Cheatham designed the first hybrid cardiac catheterization suites and advanced imaging equipment at Nationwide Children’s Hospital. He serves as a consultant to various medical companies and proctors new transcatheter techniques and devices to other physicians around the world. Dr. Cheatham has implemented a formal physician exchange program with two of the leading medical institutions in China. In cooperation with China Red Cross, he is also the foreign director of the International Training Center for treatment of congenital heart disease in poor children. Dr. Cheatham has written more than 120 manuscripts, 16 book chapters, 300 national and international presentations and is co-editor of the book, Complications in Percutaneous Interventions for Congenital and Structural Heart Disease. After graduating from the University of Oklahoma College of Medicine, he completed his residency at Boston Children’s Hospital, followed by a fellowship in Pediatric Cardiology at Texas Children’s Hospital in Houston.
W. Randolph Chitwood, Jr., M.D., is senior associate vice chancellor for health sciences and chief of cardiovascular services at East Carolina University Department of Surgery, Greenville, N.C. Dr. Chitwood is a leading international pioneer in minimally invasive and robotic heart surgery. The Robotic Surgical Center at East Carolina University has trained more than 350 surgeons. His research activities relate to myocardial preservation, simulation in surgery and endoscopic/robotic cardiac surgery. He was the principal investigator of the FDA robotic mitral valve trials that led to approval for use in the U.S. He is the son and grandson of “southwestern Virginia mountain doctors” who set the guidelines for his professional life. He graduated from Hampden-Sydney College and received his medical degree from the University of Virginia. After medical school, he completed the surgical residency at Duke University Medical Center under David C. Sabiston, M.D., an influential surgical educator of the era. At Duke he spent 10 years training in general and cardiothoracic surgery, as well as basic science research.
After his chief residency at Duke in 1984, he was selected to begin and head the new cardiac surgery program at the East Carolina University School of Medicine. Because of his prolific publication record as a resident and clinical acumen, his initial appointment was as a full professor of surgery. Except for a two-year hiatus as the chief of cardiothoracic surgery at the University of Kentucky, he has spent his entire career at East Carolina University, where he also served as chairman of the department of surgery. In 2003, he was named to be in charge of the development of the East Carolina Heart Institute, which now includes an integrated department of cardiovascular sciences as well as a $200 million heart hospital, outpatient, research and education center.
Larry S. Dean, M.D., is director of the University of Washington Medicine Regional Heart Center and is professor of medicine and of surgery at the University of Washington School of Medicine, Seattle. In addition to general cardiology, he is an expert in cardiac catheterization and interventional cardiology. He also conducts research on stents to keep blocked heart arteries open and on ways to prevent restenosis after stents are inserted. He is currently involved in the evaluation of percutaneous aortic valve replacement. Dr. Dean earned his M.D. from the University of Alabama School of Medicine, Birmingham, and served his internship and residency at the University of Washington. He then returned to the University of Alabama Hospital for fellowships in cardiovascular disease and in angioplasty. After nearly 15 years as a faculty member at the University of Alabama, he returned to the University of Washington to direct the Regional Heart Center. He is a fellow of the American College of Cardiology and is board-certified in internal medicine, cardiovascular disease and interventional cardiology. He is also a fellow of the American Heart Association and president-elect of the Society of Cardiovascular Angiography and Interventions.
Andrew Craig Eisenhauer, M.D., is director of the interventional cardiovascular medicine service at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School. His specialties are
- interventional cardiology,
- vascular medicine and
- congenital and inherited diseases.
He earned his medical degree at New York University School of Medicine and served a residency at Peter Bent Brigham Hospital and a fellowship at Massachusetts General Hospital. He is certified in internal medicine, cardiovascular disease and interventional cardiology. His clinical interests are
- endovascular therapy,
- complex coronary disease,
- peripheral vascular disease,
- cerebrovascular disease,
- congenital heart disease and structural heart disease
Douglas A. Murphy, M.D., is chief of cardiothoracic surgery at Saint Joseph’s Hospital and a cardiothoracic surgeon at Peachtree Cardiovascular and Thoracic Surgery, Atlanta. His areas of interest are robotically assisted heart surgery with an emphasis on repairing the mitral valve rather than replacing it. A graduate of the University of Pennsylvania Medical School, Philadelphia, he served an internship and residency at Massachusetts General Hospital, Boston, and at Emory University, Atlanta.
Khusrow Niazi, M.D., is an assistant professor at Emory University School of Medicine and director of peripheral and carotid intervention at Emory University Hospital Midtown, Atlanta. He earned his medical degree at King Edward Medical College, Lahore, Pakistan, and served an internship at Kettering Medical Center, Dayton, Ohio, and a fellowship at William Beaumont Hospital, Royal Oak, MI. He has published papers on stenting following rotational atherectomy, small vessel stenting for coronary arteries, imaging of lower extremities and treatment of peripheral arterial disease.
Jeffrey J. Popma, M.D., is director of innovations in interventional cardiology, a senior attending physician at Beth Israel Deaconess Medical Center and an associate professor of medicine at Harvard Medical School in Boston. Dr. Popma received his bachelor’s degree in economics from Stanford University, and his M.D. from Indiana University School of Medicine. He completed his internship, residency, chief residency and fellowship at University of Texas Southwestern Medical Center. He also completed an interventional cardiology fellowship at the University of Michigan. Dr. Popma is the past president of the Society for Cardiac Angiography and Intervention and is the co-chair of the ACC Interventional Council. He sits on the editorial boards of several publications, and reviews for several cardiology periodicals. Dr. Popma has more than 300 published peer-reviewed manuscripts.
Dr. Popma also directs the BIDMC Angiographic Core Laboratory and is principal investigator for more than 65 ongoing multicenter device studies within the research laboratory. Over the past 15 years, these trials have included a broad array of new technology, including bare-metal stents, drug-eluting stents, distal-protection devices, total-occlusion devices and carotid and peripheral revascularization procedures. His primary clinical interest currently is the use of percutaneous aortic valve replacement for patients with high-risk aortic stenosis.
Robert S. Poston, M.D., is chief of cardiac surgery at Boston Medical Center and associate professor of cardiothoracic surgery at Boston University School of Medicine. He has a strong background in minimally invasive cardiac bypass surgery and is a pioneer in using robotics, specifically the da Vinci Surgical System, to treat coronary artery disease. A graduate of the Johns Hopkins School of Medicine, Baltimore, Dr. Poston completed a residency in general surgery at the University of California, San Francisco, and continued his training with a research fellowship in cardiothoracic surgery at Stanford University School of Medicine, Palo Alto, CA, and a cardiothoracic residency at the University of Pittsburgh Medical Center.
Charanjit S. Rihal, M.D., is professor of medicine and director of the cardiac catheterization laboratory at Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN. A graduate of the University of Winnipeg, Dr. Rihal did his residency and fellowship at the Mayo Graduate School of Medicine and also earned an MBA at the Carlson School of Management, University of Minnesota. His medical interests are interventional cardiology, structural heart disease interventions and the management of quality and costs in healthcare.
Timothy A. Shapiro, M.D., is director of the Interventional Cardiology Fellowship Program and campus chief, interventional cardiology, at Lankenau Hospital, Lancaster, PA. A graduate of Yale University School of Medicine, he served his residency and a fellowship at the Hospital of the University of Pennsylvania.
Robert J. Siegel, M.D., is director of the Cardiac Non-Invasive Laboratory at Cedars-Sinai Medical Center, cardiology director of the Cedars-Sinai Marfan Center, and Rexford S. Kennamer, M.D., chair in cardiac ultrasound at Cedars-Sinai Medical Center, Los Angeles. Dr. Siegel is also professor of medicine in residence at the David Geffen School of Medicine at University of California, Los Angeles. He previously served as senior staff fellow in cardiac pathology at the Heart, Lung and Blood Institute of the National Institutes of Health, Bethesda, MD. Internationally recognized as one of the leading experts in the field of cardiovascular ultrasound, Dr. Siegel specializes in cardiovascular ultrasound, including transthoracic, transesophageal and intravascular methodologies. His research interests include
- valvular heart disease,
- therapeutic applications of ultrasound energy,
- transesophageal and intraoperative echocardiography, and the
- development and use of hand-held portable echocardiographic systems for clinical innovations.
In addition, he is involved with clinical research studies related to the diagnosis, assessment and management of patients with
- Marfan syndrome,
- hypertrophic cardiomyopathy and
- pericardial and valvular heart disease.
Dr. Siegel is a fellow, and has previously served as the president of the California Chapter of the American College of Cardiology and president of the Los Angeles Society of Echocardiography. He has been active in numerous cardiovascular societies, including the American Heart Association, the American College of Cardiology and the American Society of Echocardiography. Dr. Siegel received his medical degree at Baylor College of Medicine, Houston, where he developed an interest in cardiology. He completed his medical residency at Emory University and at Los Angeles County + USC Medical Center. He completed his cardiology fellowship at Harbor-UCLA Medical Center.
Over the last two years Dr. Siegel has worked extensively with live 3D transesophageal echo in the cardiac intervention center and the operating room. He and his echocardiologist colleagues, doctors Shiota, Biner, Tolstrup and Gurudevan, have worked closely at Cedars-Sinai Medical Center in Los Angeles with the interventional cardiologists, doctors Kar and Makkar, as well as with the cardiac surgeons, doctors Trento and Fontana. They use live 3D TEE extensively for the assessment of structural heart disease. In addition, it is used on a regular basis for the guidance of percutaneous procedures for mitral valve e-clip repair, mitral balloon valvuloplasty, aortic and pulmonic valve replacement, left atrial appendage exclusion by the Watchman device as well as for ASD closure.
Sudhir P. Srivastava, M.D., president of the International College of Robotic Surgery at St. Joseph’s Hospital, Atlanta, is a pioneer in performing beating heart totally endoscopic coronary artery bypass surgeries. Previously, he was assistant professor of surgery and director of robotic and minimally invasive cardiac surgery at the University of Chicago Medical Center. Dr. Srivastava specializes in robotically assisted totally endoscopic coronary artery bypass surgery. He has performed approximately 1,000 robotic cardiothoracic surgical procedures, of which 450 have been single- and multivessel beating heart totally endoscopic coronary bypass (BH TECAB) procedures. He has keen interest in hybrid coronary revascularization in TECAB patients to achieve complete revascularization.
Dr. Srivastava has helped launch robotic revascularization programs throughout the world. He has performed numerous live BH TECAB demonstrations both in the U.S. and abroad, and continues to be a presenter and invited speaker at numerous national and international scientific meetings. He earned his medical degree at the Jawahar Lal Nehru Medical College in Ajmer, India and immigrated to the U.S. in 1972. He completed his cardiothoracic surgery residency at the hospitals associated with the University of British Columbia, Vancouver, Canada.
Francis P. Sutter, D.O., F.A.C.S., is clinical professor of surgery at Thomas Jefferson University-Jefferson Medical College, Philadelphia, and chief of cardiothoracic surgery at Lankenau Hospital, Main Line Health System, Wynnewood, PA. A graduate of Philadelphia College of Osteopathic Medicine, his surgical residency and a cardiothoracic fellowship were completed at Thomas Jefferson University Hospital.
Mark R. Vesely, M.D., is an assistant professor of medicine at the University of Maryland School of Medicine. He completed medical school at the George Washington University and postgraduate training—an internal medicine residency and fellowships in cardiovascular disease and interventional cardiology—at the University of Maryland. He is board-certified in internal medicine, cardiovascular disease, nuclear cardiology and interventional cardiology. Dr. Vesely is the associate program director of the Interventional Cardiology fellowship at University of Maryland. His special interests include the partnered approach (interventional cardiologists and cardiac surgeons) for hybrid coronary revascularization and structural heart disease interventions. Additional research interests include investigation of techniques to minimize acute myocardial infarction injury with ventricular-assist devices and adult stem cell therapies.
David X. M. Zhao, M.D., Ph.D., is an associate professor of medicine and cardiac surgery, Harry and Shelley Page Chair in Interventional Cardiology, director of the Cardiac Catheterization Laboratories and interventional cardiology director of the Interventional Cardiology Fellowship Training Program, Vanderbilt University School of Medicine, Nashville, TN. He earned his medical degree at Shanghai Medical University, Shanghai, P.R. China, and his Ph.D. in immunology at Queensland University, Brisbane, Australia. His postdoctoral training was at Zhongshan Hospital, Shanghai Medical University, Shanghai, P.R. China, The Prince Charles Hospital, Brisbane, Australia, and Brigham and Women’s Hospital, Boston.
http://www.expo.acc.org/acc12/CUSTOM/images/ACC12/ACC.10%20Hybrid%20Suite%20Directory.pdf
Part Two
Cardiac Surgery
Cardiac Surgery @ Cleveland Clinic: Traditional OR & Hybrid Cath Lab/OR Suite
Nation #1 for 19 consecutive years – The Heart Center: Miller Family Heart & Vascular Institute @ Cleveland Clinic
The Sydell and Arnold Miller Family Heart & Vascular Institute is one of the largest, most experienced cardiovascular specialty groups in the world. Our physicians are committed to providing the most advanced diagnostic and treatment options, better outcomes and improved quality of life. U.S.News & World Reporthas ranked Cleveland Clinic as the No.1 heart program in America every year since 1995.
Departments & Centers:
Below we present two articles on Cardiac Surgery @ Mayo Clinic
Cardiac Surgery @ Mayo Clinic: Traditional OR & Hybrid Cath Lab/OR Suite
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Comparison of the 10-year and 15-year survivals after CABG demonstrated benefit from a change in graft sources used at the Mayo Clinic and widely adapted by others: vascular grafts from the left internal mammary artery (LIMA) instead of just leg veins, for multiple grafts (up to 3), LIMA-to-LAD plus grafts using LIMA or radial artery vs LIMA/saphenous vein (SV).
CABG Survival in Multivessel Disease Patients: Comparison of Arterial Bypass Grafts vs Saphenous Venous Grafts
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part Three
Invasive Interventions with Complications
In the following article we covered multiple etiologies for cardiovascular complications related to invasive interventions: cardiovascular and peripheral arterial or peri- and post- cardiac surgery of the open heart type.
Cardiovascular Complications: Death from Reoperative Sternotomy after prior CABG, MVR, AVR, or Radiation; Complications of PCI; Sepsis from Cardiovascular Interventions
Justin D Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
http://pharmaceuticalintelligence.com/2013/07/23/cardiovascular-complications-of-multiple-etiologies-repeat-sternotomy-post-cabg-or-avr-post-pci-pad-endoscopy-andor-resultant-of-systemic-sepsis/
This article covers types of Cardiovascular Complications derived from the following THREE types of assault on the Human body, two related to cardiac invasive interventions, the last due to its systemic nature is taking a fatal Cardiac toll: the Sepsis condition causing cardiac failure.
Three types of Cardiovascular Complications:
- (a) Post PCI, and
- (b) PAD Endovascular Interventions: Carotid Artery Endarterectomy
This article does NOT cover the following two types of Cardiovascular Complications:
1. Trauma Injury causing cardiac arrest, lung collapse or cardiogenic shock
2. Surgical Complication of Non-cardiac surgery type causing cardiac arrest, i.e, Surgery of Joint Replacement causing sepsis causing death or death caused by complications of surgery i.e., blood loss, viral infection, emboli, thrombus, stroke, or cardiogenic shock not related to Cardiovascular and Cardiac invasive interventions
The e-Reader is advised to consider the following expansion on the subject matter carrying the discussion to additional related clinical issues:
Larry H Bernstein, Advanced Topics in Sepsis and the Cardiovascular System at its End Stage
http://pharmaceuticalintelligence.com/2013/08/18/advanced-topics-in-sepsis-and-the-cardiovascular-system-at-its-end-stage/
Read Full Post »

























































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}