Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
The UK Biobank (UKBB) this week unveiled to scientists the entire genomes of 200,000 people who are part of a long-term British health study.
The trove of genomes, each linked to anonymized medical information, will allow biomedical scientists to scour the full 3 billion base pairs of human DNA for insights into the interplay of genes and health that could not be gleaned from partial sequences or scans of genome markers. “It is thrilling to see the release of this long-awaited resource,” says Stephen Glatt, a psychiatric geneticist at the State University of New York Upstate Medical University.
Other biobanks have also begun to compile vast numbers of whole genomes, 100,000 or more in some cases (see table, below). But UKBB stands out because it offers easy access to the genomic information, according to some of the more than 20,000 researchers in 90 countries who have signed up to use the data. “In terms of availability and data quality, [UKBB] surpasses all others,” says physician and statistician Omar Yaxmehen Bello-Chavolla of the National Institute for Geriatrics in Mexico City.
Enabling your vision to improve public health
Data drives discovery. We have curated a uniquely powerful biomedical database that can be accessed globally for public health research. Explore data from half a million UK Biobank participants to enable new discoveries to improve public health.
This UKBB biobank represents genomes collected from 500,000 middle-age and elderly participants for 2006 to 2010. The genomes are mostly of a European descent. Other large scale genome sequencing ventures like Iceland’s DECODE, which collected over 100,000 genomes, is now a subsidiary of Amgen, and mostly behind IP protection, not Open Access as this database represents.
UK Biobank is a large-scale biomedical database and research resource, containing in-depth genetic and health information from half a million UK participants. The database is regularly augmented with additional data and is globally accessible to approved researchers undertaking vital research into the most common and life-threatening diseases. It is a major contributor to the advancement of modern medicine and treatment and has enabled several scientific discoveries that improve human health.
A summary of some large scale genome sequencing projects are show in the table below:
Biobank
Completed Whole Genomes
Release Information
UK Biobank
200,000
300,000 more in early 2023
TransOmics for Precision Medicien
161,000
NIH requires project specific request
Million Veterans Program
125,000
Non-Veterans Affairs researchers get first access
100,000 Genomes Project
120,000
Researchers must join Genomics England collaboration
All of Us
90,000
NIH expects to release 2022
Other Related Articles on Genome Biobank Projects in this Open Access Online Scientific Journal Include the Following:
Why do some people with COVID-19 get sicker than others? Maybe exposure to a particularly high dose of the causative virus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), accounts for the difference. Perhaps deficiencies in diet, exercise, or sleep contribute to worse illness. Although many factors govern how sick people become, a key driver of the severity of COVID-19 appears to be genetic, which is common for other human viruses and infectious agents (1). On page 579 of this issue, Wickenhagen et al. (2) show that susceptibility to severe COVID-19 is associated with a single-nucleotide polymorphism (SNP) in the human gene 2′-5′-oligoadenylate synthetase 1 (OAS1).The authors reasoned that SARS-CoV-2 should be inhibited by interferon-mediated antiviral responses, which are among the first cellular defense mechanisms produced in response to a viral infection. Interferons are a group of cytokines that induce the transcription of a large cadre of genes, many of which encode proteins with the potential to directly inhibit the invading virus. Wickenhagen et al. interrogated many hundreds of these putative antiviral proteins for their ability to suppress SARS-CoV-2 in cultured cells and found that OAS1 was particularly potent against SARS-CoV-2.OAS1 is an enzyme that is activated in the presence of double-stranded RNA, which is scattered along an otherwise singlestranded SARS-CoV-2 genome because of an assortment of RNA hairpins and other secondary structures. Once activated, OAS1 catalyzes the polymerization of adenosine triphosphate (ATP) into a second messenger, 2′-5′-oligoadenylate. This then triggers the conversion of ribonuclease L (RNaseL) into its active form so that it can cleave viral RNA, effectively blunting viral replication (3). Wickenhagen et al. found that OAS1 is expressed in respiratory tissues of healthy donors and COVID-19 patients and that it interacts with a region of the SARS-CoV-2 genome that contains double-stranded RNA secondary structures (see the figure).OAS1 exists predominantly as two isoforms in humans—a longer isoform (p46) and a shorter version (p42). Genetic variation dictates which isoform will be expressed. In humans, p46 is expressed in people who have a SNP that causes alternative splicing of the OAS1 messenger RNA (mRNA). This results in the utilization of a terminal exon that is not used to translate p42. Thus, the carboxyl terminus of the p46 OAS1 protein contains a distinct four–amino acid motif that forms a prenylation site. Prenylation is a posttranslational modification that targets proteins to membranes. In cell culture experiments, Wickenhagen et al. showed that only OAS1 p46, but not p42, could inhibit SARS-CoV-2. However, when the prenylation site of p46 was engineered into p42, this chimeric p42 protein was able to inhibit SARS-CoV-2, which strongly implicates a role for OAS1 specifically at membranes.Why are membranes important? SARS-CoV-2, like all coronaviruses, co-opts cellular membranes at the endoplasmic reticulum to form double-membrane vesicles, in which the virus replicates its genome. Thus, membrane-bound OAS1 p46 may be specifically activated by RNA viruses that form membrane-bound vesicles for replication. Indeed, the unrelated cardiovirus A, which also forms vesicular membranous structures, was inhibited by OAS1. Conversely, other respiratory RNA viruses, such as human parainfluenza virus type 3 and human respiratory syncytial virus, which do not use membrane-tethered vesicles for replication, were not inhibited by p46.Wickenhagen et al. examined a cohort of 499 COVID-19 patients hospitalized in the UK. Whereas all patients expressed OAS1, 42.5% of them did not express the antiviral p46 isoform. These patients were statistically more likely to have severe COVID-19 (be admitted to the intensive care unit). This suggests that OAS1 is an important antiviral factor in the control of SARS-CoV-2 infection and that its inability to activate RNaseL results in prolonged infections and severe disease, although other factors likely contribute. The authors also examined animals known to harbor different coronaviruses. They found evidence for prenylated OAS1 proteins in mice, cows, and camels. Notably, horseshoe bats, which are considered a possible reservoir for SARS-related coronaviruses (4), lack a prenylation motif in their OAS1 because of genomic changes that eliminated the critical four-amino acid motif. A horseshoe bat (Rhinolophus ferrumequinum) OAS1 was unable to inhibit SARS-CoV-2 infection in cell culture. Conversely, the black flying fox (Pteropus alecto)—a pteropid bat that is a reservoir for the Nipah and Hendra viruses, which can also infect humans—possesses a prenylated OAS1 that can inhibit SARS-CoV-2. These findings indicate that horseshoe bats may be genetically and evolutionarily primed to be optimal reservoir hosts for certain coronaviruses, like SARS-CoV-2.Other studies have now shown that the p46 OAS1 variant, which resides in a genomic locus inherited from Neanderthals (5–7), correlates with protection from COVID-19 severity in various populations (8, 9). These findings mirror previous studies indicating that outcomes with West Nile virus (10) and hepatitis C virus (11) infection, both of which also use membrane vesicles for replication, are also associated with genetic variation at the human OAS1 locus. Another elegant functional study complements the findings of Wickenhagen et al. by also demonstrating that prenylated OAS1 inhibits multiple viruses, including SARS-CoV-2, and is associated with protection from severe COVID-19 in patients (12).There is a growing body of evidence that provides critical understanding of how human genetic variation shapes the outcome of infectious diseases like COVID-19. In addition to OAS1, genetic variation in another viral RNA sensor, Toll-like receptor 7 (TLR7), is associated with severe COVID-19 (13–15). The effects appear to be exclusive to males, because TLR7 is on the X chromosome, so inherited deleterious mutations in TLR7 therefore result in immune cells that fail to produce normal amounts of interferon, which correlates with more severe COVID-19. Our knowledge of the host cellular factors that control SARS-CoV-2 is rapidly increasing. These findings will undoubtedly open new avenues into SARS-CoV-2 antiviral immunity and may also be beneficial for the development of strategies to treat or prevent severe COVID-19.
Degrading viral RNAOnce inside a host cell, coronaviruses form double-membrane vesicles (DMVs) to replicate their RNA genome. When anchored to membranes, 2′-5′-oligoadenylate synthetase 1 (OAS1) detects double-stranded RNA (dsRNA) secondary structure and activates ribonuclease L (RNaseL), which degrades viral RNA. The OAS1 p42 isoform lacks the prenylation motif, so it is not membrane bound and RNaseL is not activated, leading to unrestrained viral replication and correlating with severe COVID-19.GRAPHIC: KELLIE HOLOSKI/SCIENCE Source: Shroggins SCIENCE
28 Oct 2021
Vol 374, Issue 6567
pp. 535-536
DOI: 10.1126/science.abm3921
Moderna Vaccine Patent Application needs to include Names of Three NIH Scientists that Shared the Genome Sequence of SAR-Cov-2 with Moderna Early on
Reporter: Aviva Lev-Ari, PhD, RN
UPDATED on 11/12/2021
Within the filing, Moderna said it had “reached the good-faith determination” that three NIH scientists — John Mascola, Barney Graham and Kizzmekia Corbett — “did not co-invent” the sequence that prompts the body’s immune response to the coronavirus spike protein. The NIH, meanwhile, says the trio worked with Moderna at the outset of the pandemic to design the component in question.
In response to an Endpoints News request for comment, a Moderna spokesperson said the company has “all along” recognized the role the NIH played in developing the Covid-19 shot. But the spokesperson insisted only Moderna scientists invented mRNA-1273 — the codename for the company’s vaccine.
In the new book A Shot to Save the World out last month detailing the inventions of the mRNA Covid-19 vaccines, Wall Street Journal reporter Gregory Zuckerman wrote the three NIH scientists in question designed a sequence for a vaccine and sent it to Moderna. The biotech then used it to confirm their own designs and produce that vaccine.
Zuckerman wrote:
On Thursday, January 23, Wang packed his material in a container, trying hard to ensure it didn’t leak, and shipped it all to Kizzmekia Corbett, the government scientist who was doing similar work with other’s in Graham’s lab. Corbett, Graham and John Mascola chose an ideal spike-protein design and sent it to Moderna. The company’s scientists, relying on McLellan and Wang’s earlier work, had built their own spike-protein design. It matched the one from the government scientists, confirming they made the right choice. Moderna took their chosen sequence, employed some sophisticated computer software, and built an mRNA molecule capable of producing the stabilized spike protein. This would become Moderna’s vaccine antigen.
What Moderna says: The company argues that the NIH scientists — John Mascola, Barney Graham and Kizzmekia Corbett — were not part of selecting the messenger RNA sequence that became the Covid-19 shot authorized today. That sequence patent is essentially the heart of the product.
Moderna “has recognized the substantial role that the NIAID has played” in the vaccine development by including those scientists on other patents but “just because someone is an inventor on one patent application relating to our COVID-19 vaccine does not mean they are an inventor on every patent application relating to the vaccine,” it tweeted.
“Moderna remains the only company to have pledged not to enforce its COVID-19 intellectual property during the pandemic,” the company added.
It’s far from over: Moderna, which never brought a product to market before its effective Covid-19 shot, has received nearly $10 billion in government funding for the vaccine — a figure that advocates return to repeatedly when pressing for global access to patents and production.
SOURCE
From: POLITICO Pulse <pulse@email.politico.com> Reply-To: “POLITICO, LLC” <reply-fe8c1d737662017574-630320_HTML-638333449-1376319-0@politicoemail.com> Date: Friday, November 12, 2021 at 10:02 AM To: Aviva Lev-Ari <Avivalev-ari@alum.Berkeley.edu> Subject: Moderna vs. The Government
11/9/2021and 11/11/2021
The NIH told the New York Times earlier this week that three of its scientists — John Mascola, Barney Graham, who recently retired, and Kizzmekia Corbett, who has since moved over to Harvard — worked with Moderna to design the genetic sequence that prompts the vaccine to produce an immune response.
“I think Moderna has made a serious mistake here in not providing the kind of co-inventorship credit to the people who played a major role in the development of the vaccine that they are now making a fair amount of money on. We did our best to try to resolve this and ultimately failed but we are not done,” NIH Director Francis Collins told Reuters in an interview yesterday.
Dr. Barney Graham, left, and his colleague at the time, Dr. Kizzmekia Corbett, right, explaining the role of spike proteins to President Biden at the National Institutes of Health in Bethesda, Md., in February 2021
The vaccine grew out of a four-year collaboration between Moderna and the N.I.H., the government’s biomedical research agency — a partnership that was widely hailed when the shot was found to be highly effective. A year ago this month, the government called it the “N.I.H.-Moderna Covid-19 vaccine.”
The agency says three scientists at its Vaccine Research Center — Dr. John R. Mascola, the center’s director; Dr. Barney S. Graham, who recently retired; and Dr. Kizzmekia S. Corbett, who is now at Harvard — worked with Moderna scientists to design the genetic sequence that prompts the vaccine to produce an immune response, and should be named on the “principal patent application.”
If the three agency scientists are named on the patent along with the Moderna employees, the federal government could have more of a say in which companies manufacture the vaccine, which in turn could influence which countries get access. It would also secure a nearly unfettered right to license the technology, which could bring millions into the federal treasury.
“Omitting N.I.H. inventors from the principal patent application deprives N.I.H. of a co-ownership interest in that application and the patent that will eventually issue from it.”
According to the NYT article,
But experts said the disputed patent was the most important one in Moderna’s growing intellectual property portfolio. It seeks to patent the genetic sequence that instructs the body’s cells to make a harmless version of the spike proteins that stud the surface of the coronavirus, which triggers an immune response.
While it has not publicly acknowledged the rift until now, the Biden administration has expressed frustration that Moderna has not done more to provide its vaccine to poorer nations even as it racks up huge profits.
Accurate and near real-time data about the trajectory of the COVID-19 pandemic have been crucial in informing mitigation policies. Because choosing the right mitigation policies relies on an accurate assessment of the current state of the local epidemic, the potential ramifications of misinterpreting data are serious. Each data source has inherent biases and pitfalls in interpretation. The more data sources that are interpreted in combination, the easier it is to detect genuine changes in an epidemic. Recently, in many countries, this has involved disentangling the varying impact of rising but heterogeneous vaccination rates, relaxation of mitigations, and the emergence of new variants such as Delta.The exact data collected and their accuracy will vary by country. Typical data common to many countries are numbers of tests, confirmed cases, hospital and intensive care unit (ICU) admissions and occupancy, deaths, and vaccinations (1). Many countries additionally sequence a proportion of new positive tests to identify and track emerging variants. Some countries also now collect and publish data on infections, hospitalizations, and deaths by vaccination status (e.g., Israel and the UK). Stratifying all available data by different demographic factors (e.g., age, location, measures of deprivation, and ethnicity) is crucial for understanding patterns of spread, potential impact of policies, and efficacy of vaccines (age, timing of breakthrough infections, and prevalent variants).It is also necessary to be aware of what data are not being collected. For example, persistent symptoms of COVID-19 (Long Covid) were recognized as a long-term adverse outcome by the autumn of 2020. However, no simple diagnostic test has been associated with the up to 200 different reported symptoms (2). Counting Long Covid relies on a clinical diagnosis, based on a history of having had COVID-19 and a failure to fully recover, with development of some characteristic symptoms and with no obvious alternative cause (3). These features make it very difficult to measure routinely, and so it rarely is. As a result, Long Covid is often neglected in decision-making. Failure to account for the disease load associated with Long Covid may lead to an unnecessary long-term societal health burden.The feedback between different types of outcomes, different severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants, different mitigation policies (including vaccination), and individual risks (a combination of exposure and clinical risk) is complex and must be factored into both interpretation of data and the development of policy. Using all available data to quantify transmission is crucial to ensuring rapid and effective responses to early phases of renewed exponential growth and to evaluating mitigation measures. Relying too much on a single data source, or without disaggregating data, risks fundamentally misunderstanding the state of the epidemic.The inherent biases and lags in data are particularly important to understand from the point of view of policy-makers. Because of the natural time scales of COVID-19 disease progression (see the figure), policy changes can take several weeks to show up in the data. Purely reactive policy-making is likely to be ineffective. When cases are rising, increases in hospital admissions and deaths will follow. When a new variant is outcompeting existing strains, it is likely to become dominant without action to suppress. The precautionary principle suggests acting early and emphatically. Conversely, when releasing restrictions, governments must wait long enough to assess them before continuing with re-opening.The most up-to-date indicator of the state of the epidemic is typically the number of confirmed cases, as ascertained through testing of both symptomatic individuals and those tested frequently regardless of symptoms. Symptom-based testing is likely to pick up more adults and fewer younger individuals (4). Infections in children are harder to detect: children are more likely to be asymptomatic than adults, are harder to administer tests to (particularly young children), are often exposed to other viruses with similar symptoms, and can present with symptoms that are atypical in adults (e.g., abdominal pain or nausea). Children under 12 are not routinely offered the COVID-19 vaccination, and their mixing in schools provides ongoing opportunities for the virus to circulate, so it will be important for countries to track infections in children as accurately as possible. Other testing biases include accessibility, reporting lags, and the ability to act lawfully upon receiving a positive result. Substantial changes in the number of people seeking tests may further confound case figures (5). Case positivity rates may provide a more accurate reflection of the state of the epidemic (6) but are dependent on the mix of symptomatic and asymptomatic people being tested.SARS-CoV-2 variants have been an important driver of local epidemics in 2021. The four main SARS-CoV-2 variants of concern, to date, are B.1.1.7 (Alpha), B.1.351 (Beta), P.1 (Gamma), and B.1.617.2 (Delta). Some have been more transmissible (Alpha), some have substantial resistance to previous infection or vaccines (Beta), and some have elements of both (Gamma and Delta) (7). Currently, the high transmissibility of Delta combined with some immune evasion has made it the world’s dominant variant. Determining which variants pose a substantial threat is difficult and takes time, particularly when many variants cocirculate. This is especially true for situations in which a dominant variant is declining, and a new one growing. While the declining variant remains dominant, its decrease masks increases in the new variant because case numbers remain unchanged or fall overall. Only when a new variant becomes dominant does its growth become apparent in aggregated case data, by which time it is, by definition, too late to contain its spread. This dynamic has been observed across the world with Delta over the latter half of 2021.With multiple variants circulating, there are, effectively, multiple epidemics occurring in parallel, and they must be tracked separately. This typically requires the availability of sequencing data, which is unfortunately limited in most countries. Sequencing takes time and so is typically a few weeks out of date. These lags, and the uncertainty in sampling, can lead to hesitancy in acting. The rapid path to dominance of the Delta variant in the UK highlights the need for action when a quickly growing variant represents a few percent (or less) of overall cases.Hospital admissions or occupancy data do not suffer the same biases associated with testing behaviors and provide unequivocal evidence of widespread transmission, its geography, and demographics. However, hospital admissions lag infections more than reported cases do, rendering these data less useful for proactive decision-making. Hospital data are also biased toward older people, who are more likely to suffer severe COVID-19, and now, unvaccinated populations. ICU occupancy data show a younger age profile than admissions because younger patients have a better chance of benefitting from the invasive treatment procedures (8).Deaths are the most lagged indicator, typically occurring 3 or more weeks after infection and with an additional lag in registration and reporting. Death data should never be used to inform real-time policy decisions. Instead, death figures can act as an eventual measure of the success of a country’s epidemic strategy and implementation. The age distribution of those who eventually die from COVID-19 is different from other metrics of the epidemic—skewed furthest toward older age groups (9). Those with clinical risk factors (such as immunodeficiency, obesity, or existing lung conditions), high exposure (health care workers and low-income workers), and the unvaccinated are overrepresented in COVID-19 deaths.In countries with high vaccination rates, vaccination has had a substantial impact—reducing COVID-19 cases, hospitalizations, and deaths. However, when looking at the raw numbers in highly vaccinated populations, it can be the case that more fully vaccinated people are dying of COVID-19 than unvaccinated. If these raw statistics are misinterpreted—or worse, deliberately misused—they can damage vaccine confidence. More vaccinated people may die than unvaccinated because such a high proportion of people are vaccinated (10). This does not mean vaccines are not effective at preventing death. Looking at the rates of death in vaccinated and unvaccinated individuals separately within age groups demonstrates that vaccines provide considerable protection against severe disease and death. This example illustrates how important it is to curate and manage the way in which data are presented.
COVID-19 progressionAn approximate timeline from infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) to various outcomes. When current infections show up in different data sources depends on this timeline. Collecting data for Long Covid, asymptomatic infection, and vaccine history will improve understanding of the pandemic.GRAPHIC: N. CARY/SCIENCE
Each country has established its own vaccination priority lists and dosing schedules to best achieve its goals (11, 12). Each of these strategies will manifest differently in the data. Additionally, many countries are using multiple vaccines in tandem and administer them differently for different demographics. Some countries are vaccinating adolescents, and others are not or not offering them the full approved dose. Most vaccines require two doses, spaced between 3 and 12 weeks apart, except for the Johnson & Johnson single-dose vaccine. This matters, particularly as variants spread, because different vaccines have different effectiveness after one and two doses, different timelines to full effectiveness, and different effectiveness against variants (13).Data published on the vaccination delivery itself must thus go beyond the raw numbers of people vaccinated. Vaccine uptake must be reported by whether fully or partially (one-dose in a two-dose regimen) vaccinated and using the whole population as a denominator. It is vital to disaggregate vaccine data by age, gender, and ethnicity as well as location so that it is possible, for example, to understand the impact of deprivation on vaccine coverage or vaccine hesitancy in particular demographics. When interpreting vaccination data, it is important to remember that there is also a lag between delivery and the build-up of immunity.Data on reinfection and post-vaccination (breakthrough) infection are also important to determine the relative benefits of infection-mediated and vaccine-mediated immunity and the length of protection offered. Studies that show those who were immunized earlier were acquiring COVID-19 with higher rates than those vaccinated more recently may suggest waning vaccine protection (14). Such studies have already prompted vaccine booster programs in some countries. However, any study that suggests waning immunity must be extremely careful to ensure that the “early” and “recent” subgroups are properly controlled. Differences in prior exposure, affluence, education level, age, and other demographic factors between these cohorts may be enough to explain the disparities in SARS-CoV-2 infection rates, even in the absence of waning immunity. Waning immunity must also be reported separately for different outcomes; for example, there might be waning in terms of preventing symptomatic infection but far less or none in preventing death (15). Additionally, there are ethical concerns about mass booster programs in high-income countries while many lower-income countries have been unable to procure vaccines.Moving into the vaccination era, reported cases, hospitalizations, and deaths should also be disaggregated by vaccination status (and by which vaccine), which will be easier in countries where national linked datasets exist. Additionally, incorporating Long Covid into routine reporting and policy-making is crucial. Consistent diagnostic criteria and well-controlled studies will be vital to this effort. These elusive data will be of critical importance to navigate our way successfully out of the pandemic.
Comparative Study: Four SARS-CoV-2 vaccines induce quantitatively different antibody responses against SARS-CoV-2 variants
Reporter: Aviva Lev- Ari, PhD, RN
Marit J. van Gils, A. H. Ayesha Lavell, Karlijn van der Straten, Brent Appelman, Ilja Bontjer, Meliawati Poniman, Judith A. Burger, Melissa Oomen, Joey H. Bouhuijs, Lonneke A. van Vught, Marleen A. Slim, Michiel Schinkel, Elke Wynberg, Hugo D.G. van Willigen, Marloes Grobben, Khadija Tejjani, Jonne Snitselaar, Tom G. Caniels, Amsterdam UMC COVID-19 S3/HCW study group, Alexander P. J. Vlaar, Maria Prins, Menno D. de Jong, Godelieve J. de Bree, Jonne J. Sikkens, Marije K. Bomers, Rogier W. Sanders doi:https://doi.org/10.1101/2021.09.27.21264163
Abstract
Emerging and future SARS-CoV-2 variants may jeopardize the effectiveness of vaccination campaigns. We performed a head-to-head comparison of the ability of sera from individuals vaccinated with either one of four vaccines (BNT162b2, mRNA-1273, AZD1222 or Ad26.COV2.S) to recognize and neutralize the four SARS-CoV-2 variants of concern (VOCs; Alpha, Beta, Gamma and Delta). Four weeks after completing the vaccination series, SARS-CoV-2 wild-type neutralizing antibody titers were highest in recipients of BNT162b2 and mRNA-1273 (median titers of 1891 and 3061, respectively), and substantially lower in those vaccinated with the adenovirus vector-based vaccines AZD1222 and Ad26.COV2.S (median titers of 241 and 119, respectively). VOCs neutralization was reduced in all vaccine groups, with the largest (5.8-fold) reduction in neutralization being observed against the Beta variant. Overall, the mRNA vaccines appear superior to adenovirus vector-based vaccines in inducing neutralizing antibodies against VOCs four weeks after the final vaccination.
Figure 2:Binding and neutralization titers post-vaccination against VOCs.
(A) Median with interquartile range of binding titers to wild-type and VOCs S proteins represented as mean fluorescence intensity (MFI) of 1:100,000 diluted sera collected four-five weeks after full vaccination for the four vaccination groups. The lower cutoff for binding was set at an MFI of 10 (grey shading). Vaccine groups are indicated by colors with BNT162b2 in green, mRNA-1273 in purple, AZD1222 in orange and Ad26.COV2.S in blue. (B) Median with interquartile range of half-maximal neutralization (ID50) titers of D614G and VOCs pseudoviruses for sera collected after full vaccination for the four vaccination groups. The lower cutoff for neutralization was set at an ID50 of 100 (grey shading). Vaccine groups are indicated by colors with BNT162b2 in green, mRNA-1273 in purple, AZD1222 in orange and Ad26.COV2.S in blue. (C) Median ID50 neutralization of D614G and VOCs plotted against the reported vaccine efficacy against symptomatic infection2–5,12–17. Vaccine groups are indicated by colors with BNT162b2 in green, mRNA-1273 in purple, AZD1222 in orange and Ad26.COV2.S in blue. Circles represent WT data, squares for Alpha, diamond for Beta, nabla triangle for Gamma and delta triangle for Delta. Spearman’s rank correlation coefficient with p value are indicated. The result of the AZD1222 phase 3 trial conducted in South Africa, demonstrating poor (10%) efficacy against Beta variant, is not shown.
Can the Public Benefit Company Structure Save US Healthcare?
Curator: Stephen J. Williams, Ph.D.
UPDATED 11/05/2023
Public Benefit Corporation structure in healthcare has actually been around since the 1970s in New Yourk State, when New York City’s new Health and Hospitals Corporation took over the city Department of Hospitals and today runs 11 hospitals and four long-term care facitlites in the city. The following link to an article describes however the problems occuring with Nassau and Westchester hosptial systems, which were converted to New York PBC status in the 1990s. As the article states the financial problems in 2004 which these hospitals encountered
do not stem from their unusual status as public benefit corporations, and might have been even worse off had they not converted
The New York Times article of 2004 “At 2 Hospitals, Fiscal Troubles in the Glare of Public View” highlight in fact the growing problem that all hospitals are encountering, especially on the fiscal side. But it does highlight how to better structure these entities and why full commitment to the PBC structure is necessary.
In 2003 New York State had a record closure of hospitals, and in 2004 Nassau and WestChester were having such fiscal problems it threatened the bond status of those counties. Despite the regular problems hospitals had, critics had said there were two major contributing factors to their woes
the two agencies had not completed their transition from government operations to fully competitve hospitals
as a PBC they bear a costly mission of serving the uninsured
As a PBC the structure allows one to shed cumbersome government rules, giving them the flexibility to conduct business like other hospitals.
In addition they are no longer dependent, in fact now forced, to forgo dependence on public funding and look for independent means of investment. With their semi-independence from government the agencies also are more insulted from political pressure.
However this seemed to be the problem. These agencies were still to dependent on their local government and there was still local political influence on their boards.
UPDATED 3/15/2023
According to Centers for Medicare and Medicare Services (CMS.gov) healthcare spending per capita has reached 17.7percent of GDP with, according to CMS data:
From 1960 through 2013, health spending rose from $147 per person to $9,255 per person, an average annual increase of 8.1 percent.
the National Health Expenditure Accounts (NHEA) are the official estimates of total health care spending in the United States. Dating back to 1960, the NHEA measures annual U.S. expenditures for health care goods and services, public health activities, government administration, the net cost of health insurance, and investment related to health care. The data are presented by type of service, sources of funding, and type of sponsor.
Graph: US National Healthcare Expenditures as a percent of Gross Domestic Product from 1960 to current. Recession periods are shown in bars. Note that the general trend has been increasing healthcare expenditures with only small times of decrease for example 2020 in year of COVID19 pandemic. In addition most of the years have been inflationary with almost no deflationary periods, either according to CPI or healthcare costs, specifically.
U.S. health care spending grew 4.6 percent in 2019, reaching $3.8 trillion or $11,582 per person. As a share of the nation’s Gross Domestic Product, health spending accounted for 17.7 percent.
And as this spending grew (demand for health care services) associated costs also rose but as the statistical analyses shows there was little improvement in many health outcome metrics during the same time.
Graph of the Growth of National Health Expenditures (NHE) versus the growth of GDP. Note most years from 1960 growth rate of NHE has always been higher than GDP, resulting in a seemingly hyperinflationary effect of healthcare. Also note how there are years when this disconnect is even greater, as there were years when NHE grew while there were recessionary periods in the general economy.
It appears that US healthcare may be on the precipice of a transformational shift, but what will this shift look like? The following post examines if the corporate structure of US healthcare needs to be changed and what role does a Public Benefit Company have in this much needed transformation.
Hippocratic Oath
I swear by Apollo the physician, and Asclepius, and Hygieia and Panacea and all the gods and goddesses as my witnesses, that, according to my ability and judgement, I will keep this Oath and this contract:
To hold him who taught me this art equally dear to me as my parents, to be a partner in life with him, and to fulfill his needs when required; to look upon his offspring as equals to my own siblings, and to teach them this art, if they shall wish to learn it, without fee or contract; and that by the set rules, lectures, and every other mode of instruction, I will impart a knowledge of the art to my own sons, and those of my teachers, and to students bound by this contract and having sworn this Oath to the law of medicine, but to no others.
I will use those dietary regimens which will benefit my patients according to my greatest ability and judgement, and I will do no harm or injustice to them.
I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; and similarly I will not give a woman a pessary to cause an abortion.
In purity and according to divine law will I carry out my life and my art.
I will not use the knife, even upon those suffering from stones, but I will leave this to those who are trained in this craft.
Into whatever homes I go, I will enter them for the benefit of the sick, avoiding any voluntary act of impropriety or corruption, including the seduction of women or men, whether they are free men or slaves.
Whatever I see or hear in the lives of my patients, whether in connection with my professional practice or not, which ought not to be spoken of outside, I will keep secret, as considering all such things to be private.
So long as I maintain this Oath faithfully and without corruption, may it be granted to me to partake of life fully and the practice of my art, gaining the respect of all men for all time. However, should I transgress this Oath and violate it, may the opposite be my fate.
Translated by Michael North, National Library of Medicine, 2002.
Much of the following information can be found on the Health AffairsBlog in a post entitled
Limitations of For Profit and Non-Profit Hospitals
For profit represent ~ 25% of US hospitals and are owned and governed by shareholders, and can raise equity through stock and bond markets.
According to most annual reports, the CEOs incorrectly assume they are legally bound as fiduciaries to maximize shareholder value. This was a paradigm shift in priorities of companies which started around the mid 1980s,aphenomenon discussed below.
A by-product of this business goal, to maximize shareholder value, is that CEO pay and compensation is naturally tied to equity markets. A means for this is promoting cost efficiencies, even in the midst of financial hardships.
A clear example of the failure of this system can be seen during the 2020- current COVID19 pandemic in the US. According to the Medicare Payment Advisory Commission, four large US hospitals were able to decrease their operating expenses by $2.3 billion just in Q2 2020. This amounted to 65% of their revenue; in comparison three large NONPROFIT hospitals reduced their operating expense by an aggregate $13 million (only 1% of their revenue), evident that in lean times for-profit will resort to drastic cost cutting at expense of service, even in times of critical demands for healthcare.
Because of their tax structure and perceived fiduciary responsibilities, for-profit organizations (unlike non-profit and public benefit corporations) are not legally required to conduct community health need assessments, establish financial assistance policies, nor limit hospital charges for those eligible for financial assistance. In addition to the difference in tax liability, for-profit, unlike their non-profit counterparts, at least with hospitals, are not funded in part by state or local government. As we will see, a large part of operating revenue for non-profit university based hospitals is state and city funding.
Therefore risk for financial responsibility is usually assumed by the patient, and in worst case, by the marginalized patient populations on to the public sector.
Tax Structure Considerations of for-profit healthcare
Financials of major for-profit healthcare entities (2020 annual)
Non-profit Healthcare systems
Nonprofits represent about half of all hospitals in the US. Most of these exist as a university structure, so retain the benefits of being private health systems and retaining the funding and tax benefits attributed to most systems of higher education. And these nonprofits can be very profitable. After taking in consideration the state, local, and federal tax exemptions these nonprofits enjoy, as well as tax-free donations from contributors (including large personal trust funds), a nonprofit can accumulate a large amount of revenue after expenses. In fact 82 nonprofit hospitals had $33 billion of net asset increase year-over-year (20% increase) from 2016 to 2017. The caveat is that this revenue over expenses is usually spent on research or increased patient services (this may mean expanding the physical infrastructure of the hospital or disseminating internal grant money to clinical investigators, expanding the hospital/university research assets which could result in securing even larger amount of external funding from government sources.
And although this model may work well for intercity university/healthcare systems, it is usually a struggle for the rural nonprofit hospitals. In 2020, ten out of 17 rural hospitals that went under were nonprofits. And this is not just true in the tough pandemic year. Over the past two decades multitude of nonprofit rural hospitals had to sell and be taken over by larger for-profit entities.
Hospital consolidation has led to a worse patient experience and no real significant changes in readmission or mortality data. (The article below is how over 130 rural hospitals have closed since 2010, creating a medical emergency in rural US healthcare)
And according to the article below it is only to get worse
The authors of the Health Affairs blog feel a major disadvantage of both the for-profit and non-profit healthcare systems is “that both face limited accountability with respect to anticompettive mergers and acquisitions.”
More hospital consolidation is expected post-pandemic
Hospital deal volume is likely to accelerate due to the financial damage inflicted by the coronavirus pandemic.
The anticipated increase in volume did not show up in the latest quarter, when deals were sharply down.
The pandemic may have given hospitals leverage in coming policy fights over billing and the creation of “public option” health plans.
Hospital consolidation is likely to increase after the COVID-19 pandemic, say both critics and supporters of the merger-and-acquisition (M&A) trend.
The financial effects of the coronavirus pandemic are expected to drive more consolidation between and among hospitals and physician practices, a group of policy professionals told a recent Washington, D.C.-based web briefing sponsored by the Alliance for Health Policy.
“There is a real danger that this could lead to more consolidation, which if we’re not careful could lead to higher prices,” said Karyn Schwartz, a senior fellow at the Kaiser Family Foundation (KFF).
Schwartz cited a recent KFF analysis of available research that concluded “provider consolidation leads to higher health care prices for private insurance; this is true for both horizontal and vertical consolidation.”
Kenneth Kaufman, managing director and chair of Kaufman Hall, noted that crises tend to push financially struggling organizations “further behind.”
“I wouldn’t be surprised at all if that happens,” Kaufman said. “That will lead to further consolidation in the provider market.”
The initial rounds of federal assistance from the CARES Act, which were based first on Medicare revenue and then on net patient revenue, may fuel consolidation, said Mark Miller, PhD, executive vice president of healthcare for Arnold Ventures. That’s because the funding formulas favored organizations that already had higher revenues, he said, and provided less assistance to low-revenue organizations.
HHS has distributed $116.2 billion from the $175 billion in provider funding available through the CARES Act and the Paycheck Protection Program and Health Care Enhancement Act. The largest distributions used the two revenue formulas cited by Miller.
No surge in M&A yet
The expected burst in hospital M&A activity has yet to occur. Kaufman Hall identified 14 transactions in the second quarter of 2020, far fewer than in the same quarter in any of the four preceding years, when second-quarter transactions totaled between 19 and 31. The latest deals were not focused on small hospitals, with average seller revenue of more than $800 million — far larger than the previous second-quarter high of $409 million in 2018.
Six of the 14 announced transactions were divestitures by major for-profit health systems, including Community Health Systems, Quorum and HCA.
Kaufman Hall’s analysis of the recent deals identified another pandemic-related factor that may fuel hospital M&A: closer ties between hospitals. The analysis cited the example of Lifespan and Care New England, which had suspended merger talks in 2019. More recently, in a joint announcement, the CEOs of the two systems noted that because of the COVID-19 crisis, the two systems “have been working together in unprecedented ways” and “have agreed to enter into an exploration process to understand the pros and cons of what a formal continuation of this collaboration could look like in the future.”
The M&A outlook for rural hospitals
The pandemic has had less of a negative effect on the finances of rural hospitals that previously joined larger health systems, said Suzie Desai, senior director of not-for-profit healthcare for S&P Global.
A CEO of a health system with a large rural network told Kaufman the federal grants that the system received for its rural hospitals were much larger than the grants paid through the general provider fund.
“If that was true across the board, then the federal government recognized that many rural hospitals could be at risk of not being able to make payroll; actually running out of money,” Kaufman said. “And they seem to have bent over backwards to make sure that didn’t happen.”
Other CARES Act funding distributed to providers included:
$12.8 billion for 959 safety net hospitals
$11 billion to almost 4,000 rural healthcare providers and hospitals in urban areas that have certain special rural designations in Medicare
Telehealth has helped rural hospitals but has not been sufficient to address the financial losses inflicted by the pandemic, Desai said.
Other coming trends include a sharper cost focus
Desai expects an increasing focus “over the next couple years” on hospital costs because of the rising share of revenue received from Medicare and Medicaid. She expects increased efforts to use technology and data to lower costs.
Billy Wynne, JD, chairman of Wynne Health Group, expects telehealth restrictions to remain relaxed after the pandemic.
Also, the perceptions of the public and politicians about the financial health of hospitals are likely to give those organizations leverage in coming policy fights over changes such as banning surprise billing and creating so-called public-option health plans, Wynne said. As an example, he cited the Colorado legislature’s suspension of the launch of a public option “in part because of sensitivities around hospital finances in the COVID pandemic.”
“Once the dust settles, it’ll be interesting to see if their leverage has increased or decreased due to what we’ve been through,” Wynne said.
About the Author
Rich Daly, HFMA Senior Writer and Editor,
is based in the Washington, D.C., office. Follow Rich on Twitter: @rdalyhealthcare
The quality of care at hospitals acquired during a recent wave of consolidations has gotten worse or stayed the same, according to a study led by Harvard Medical School scientists published Jan. 2 in NEJM.
The findings deal a blow to the often-cited arguments that hospital consolidation would improve care. A flurry of earlier studies showed that mergers increase prices. Now after analyzing patient outcomes after hundreds of hospital mergers, the new research also dashes the hopes that this more expensive care might be of higher quality.
Get more HMS news here
“Our findings call into question claims that hospital mergers are good for patients—and beg the question of what we are getting from higher hospital prices,” said study senior author J. Michael McWilliams, the Warren Alpert Foundation Professor of Health Care Policy in the Blavatnik Institute at HMS and an HMS professor of medicine and a practicing general internist at Brigham and Women’s Hospital.
McWilliams noted that rising hospital prices have been one of the leading drivers of unsustainable growth in U.S. health spending.
To examine the impact of hospital mergers on quality of care, researchers from HMS and Harvard Business School examined patient outcomes from nearly 250 hospital mergers that took place between 2009 and 2013. Using data collected by the Centers for Medicare and Medicaid Services, they analyzed variables such as 30-day readmission and mortality rates among patients discharged from a hospital, as well as clinical measures such as timely antibiotic treatment of patients with bacterial pneumonia. The researchers also factored in patient experiences, such as whether those who received care at a given hospital would recommend it to others. For their analysis, the team compared trends in these indicators between 246 hospitals acquired in merger transactions and unaffected hospitals.
The verdict? Consolidation did not improve hospital performance, and patient-experience scores deteriorated somewhat after the mergers.
The study was not designed to examine the reasons behind the worsening in patient experience. Weakening of competition due to hospital mergers could have contributed, the researchers said, but deeper exploration suggested other potential mechanisms. Notably, the analysis found the decline in patient-experience scores occurred mainly in hospitals acquired by hospitals that already had a poor patient-experience score—a finding that suggests acquisitions facilitate the spread of low quality care but not of high quality care.
The researchers caution that isolated, individual mergers may have still yielded positive results—something that an aggregate analysis is not powered to capture. And the researchers could only examine measurable aspects of quality. The trend in hospital performance on these standard measures, however, appears to point to a net effect of overall decline, the team said.
“Since our study estimated the average effects of mergers, we can’t rule out the possibility that some mergers are good for patient care,” said first author Nancy Beaulieu, research associate in health care policy at HMS. “But this evidence should give us pause when considering arguments for hospitals mergers.”
The work was supported by the Agency for Healthcare Research and Quality (grant no. U19HS024072).
Co-investigators included Bruce Landon and Jesse Dalton from HMS, Ifedayo Kuye, from the University of California, San Francisco, and Leemore Dafny from Harvard Business School and the National Bureau of Economic Research.
Public benefit corporations (versus Benefit Corporate status, which is more of a pledge) are separate legal entities which exist as a hybrid, for-profit/nonprofit company but is mandated to
Pursue a general or specific public benefit
Consider the non-financial interests of its shareholders and other STAKEHOLDERS when making decision
report how well it is achieving its overall public benefit objectives
Have limited fiduciary responsibility to investors that remains IN SCOPE of public benefit goal
In essence, the public benefit corporations executives are mandated to run the company for the benefit of STAKEHOLDERS first, if those STAKEHOLDERS are the public beneficiary of the company’s goals. This in essence moves the needle away from the traditional C-Corp overvaluing the needs of shareholders and brings back the mission of the company and in the case of healthcare, the needs of its stakeholders, the consumers of healthcare.
PBCs are legal entities recognized by states rather than by the federal government. So far, in 2020 about 37 states allow companies to incorporate as a PBC. Stipulations of the charter include semiannual reporting of the public benefits bestowed by the company and how well it is achieving its public benefit mandate. There are about 3,000 US PBCs. Some companies have felt it was in their company mission and financial interest to change incorporation as a PBC.
Some well known PBCs include
Ben and Jerry’s Ice Cream
American Red Cross
Susan B. Komen Foundation
Allbirds (a shoe startup valued at $1.7 billion when made switch)
Bombas (the sock company that donates extra socks when you buy a pair)
Lemonade (a publicly traded insurance PBC that has beneficiaries select a nonprofit that the company will donate to)
Although the number of PBCs in the healthcare arena is increasing
Not many PBCs are in the area of healthcare delivery
Noone is quite sure what the economic model would look like for a healthcare delivery PBC
Some example of hospital PBC include NYC Health + Hospitals and Community First Medical Center in Chicago.
Benefits of moving a hospital to PBC Status
PBCs are held legally accountable to a predefined public benefit. For hospitals this could be delivering cost-effective quality of care and affordable to a local citizenry or an economically disadvantaged population. PBCs must produce at least an annual report on the public benefits it has achieved contrasted against a third party standard. For example a hospital could include data of Medicaid related mortality risks, data neither the C-corp nor the nonprofit 501c would have to report on. Most nonprofits and charities report their taxes on a schedule H or Form 990, which only has to report the officer’s compensation as well as monies given to charitable organizations, or other 501 organizations. The nonprofit would show a balance of zero as the donated money for that year would be allocated out for various purposes. Hospitals, even as nonprofits, are not required to submit all this data. Right now in US the ACA just requires any hospital that receives government or ACA insurance payments to report certain outcome statistics. Although varying state by state, a PBC should have a “benefit officer” to make sure the mandate is being met. In some cases a PBC benefit officer could sue the board for putting shareholder interest over the public benefit mandate.
A PBC can include community stakeholders in the articles of incorporation thus giving a voice to local community members. This would be especially beneficial for a hospital serving, say, a rural community.
PBCs do have advantages of the for-profit companies as they are not limited to non-equity forms of investment. A PBC can raise money in the equity markets or take on debt and finance it. These financial instruments are unavailable to the non-profit. Yet one interesting aspect is that PBCs require a HIGHER voting threshold by shareholders than a traditional for profit company in the ability to change their public benefit or convert their PBC back to a for-profit.
Limitations of the PBC
Little incentive financially for current and future hospitals to incorporate as a PBC. Herein lies a huge roadblock given the state of our reimbursement structure in this country. Although there may be an incentive with regard to hiring and retention of staff drawn to the organization’s social purpose. There have been, in the past, suggestions to allow hospitals that incorporate at PBC to receive some tax benefit, but this legislation has not gone through either at state or federal level. (put link to tax article).
In order for there to be value to constituents (patients) there must be strong accountability measures. This will require the utmost in ethical behavior by a board and executives. We have witnessed, through M&A by large health groups, anticompetitive and near monopoly behavior.
There are no federal guidelines but varying guidelines from state to state. There must be some federal recognition of the PBC status when it comes to healthcare, such as that the government is one of the biggest payers of US healthcare.
This is a great interview with ArcHealth, a PBC healthcare system.
Arc Health PBC is a public benefit corporation, a mission-driven for-profit company that utilizes a market-driven approach to achieving our short and long-term social goals. As a public benefit corporation, Arc Health is also a social enterprise working to further our mission of providing healthcare to rural, underserved, and indigenous communities through business practices that improve the recruitment and retention of quality healthcare providers.
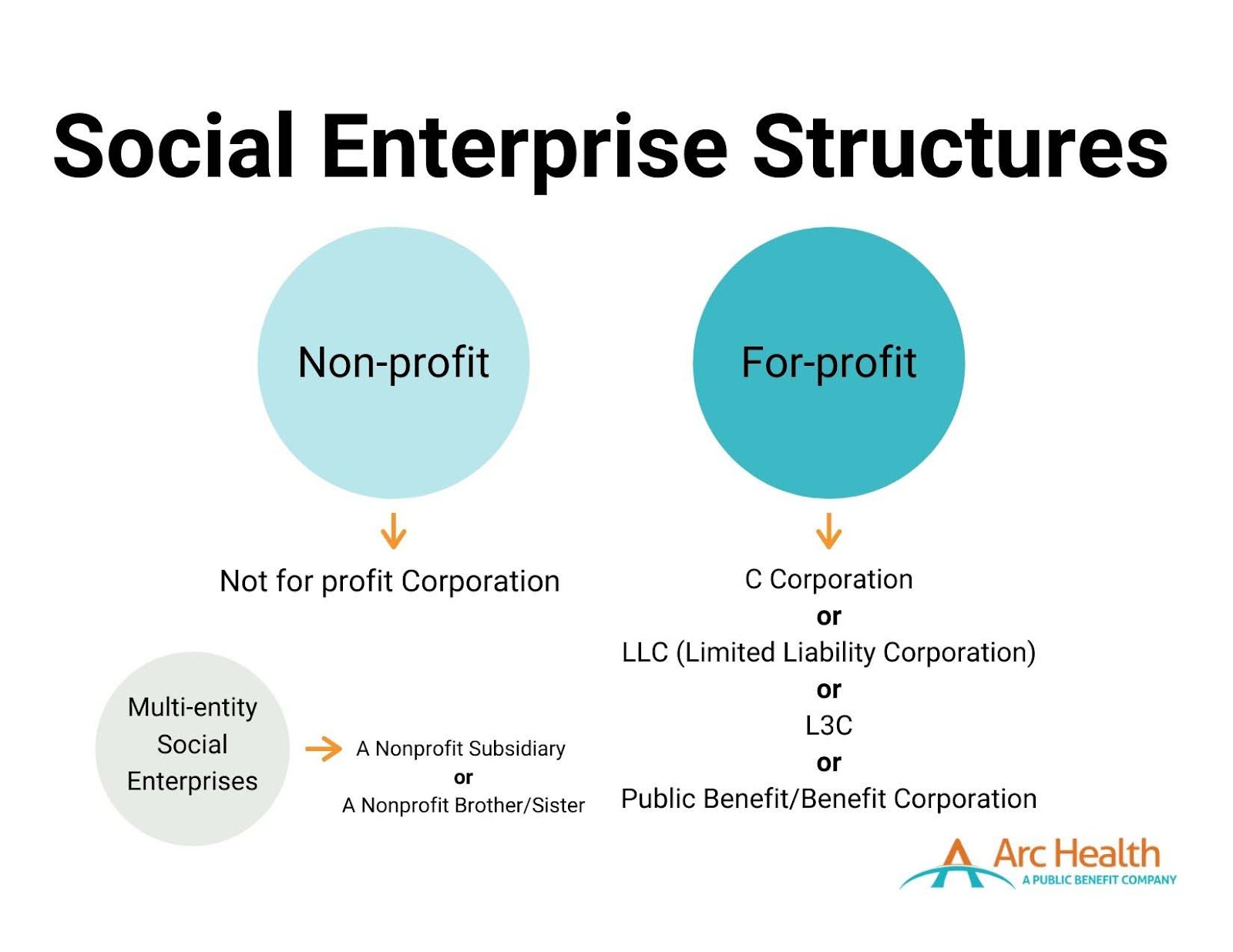
What is a Social Enterprise?
While there is no one exact definition, according to the Social Enterprise Alliance, a social enterprise is an “organization that addresses a basic unmet need or solves a social or environmental problem through a market-driven approach.” A social enterprise is not a distinct legal entity, but instead, an “ideological spectrum marrying commercial approaches with social good.” Social enterprises foster a dual-bottom-line – simultaneously seeking profits and social impact. Arc Health, like many social enterprises, seeks to be self–sustainable.
Two primary structures fall under the social enterprise umbrella: nonprofits and for-profit organizations. There are also related entities within both structures that could be considered social enterprises. Any of these listed structures can be regarded as a social enterprise depending on if and how involved they are with socially beneficial programs.
What is a Public Benefit Corporation?
Public Benefit Corporations (PBCs), also known as benefit corporations, are “for-profit companies that balance maximizing value to stakeholders with a legally binding commitment to a social or environmental mission.” PBCs operate as for-profit entities with no tax advantages or exemptions. Still, they must have a “purpose of creating general public benefit,” such as promoting the arts or science, preserving the environment, or providing benefits to underserved communities. PBCs must attain a higher degree of corporate purpose, expanded accountability, and expected transparency.
There are now over 3,000 registered PBCs, comprising approximately 0.1% of American businesses.
As a PBC, Arc Health expects to access capital through individual investors who seek financial returns, rather than through donations. Arc Health’s investors make investments with a clear understanding of the balance the company must strike between financial returns (I.e., profitability) and social purpose. Therefore, investors expect the company to be operationally profitable to ensure a financial return on their investments, while also making clear to all stakeholders and the public that generating social impact is the priority.
What is the difference between a Social Enterprise and PBC?
Social enterprises and PBCs emulate similar ideals that value the importance and need to invoke social change vis-a-vis working in a market-driven industry. Public benefit corporations fall under the social enterprise umbrella. An organization may choose to use a social enterprise model and incorporate itself as either a not-for-profit, C-Corp, PBC, or other corporate structure.
How did Arc Health Become a Public Benefit Corporation?
Arc Health was initially formed as a C-Corp. In 2019, Arc Health’s CEO and Co-Founder, Dave Shaffer, guided the conversion from a C-Corp to a PBC, incorporated in Delaware. Today, Arc Health follows guidelines and expectations for PBCs, including adhering to the State of Delaware’s requirements for PBCs.
Why is Arc Health a Social Enterprise and Public Benefit Corporation?
Arc Health believes it is essential to commit ourselves to our mission and demonstrate our dedication through our actions. We work to adhere to the core values of accountability, transparency, and purpose. As a registered public benefit company and a social enterprise, we execute our drive to achieve health equity in tangible and effective ways that the communities we work with, our stakeholders, and our providers expect of us.
90% of Americans say that companies must not only say a product or service is beneficial, but they also need to prove its benefit.
When we partner with health clinics and hospitals, we aim to provide services that enact lasting change. For example, we work with healthcare providers who desire to contribute both clinical and non-clinical skills. In 2020, Arc Health clinicians developed COVID-19 response protocols and educational materials about the vaccines. They participated in pain management working groups. They identified and followed up with kids in the community who were overdue for a well-child check. Arc Health providers should be driven by a desire to develop a long-term relationship with a healthcare service provider and participate in its successes and challenges.
Paradigm Shift in the 1980’s: Companies Start to Emphasize Shareholders Over Stakeholders
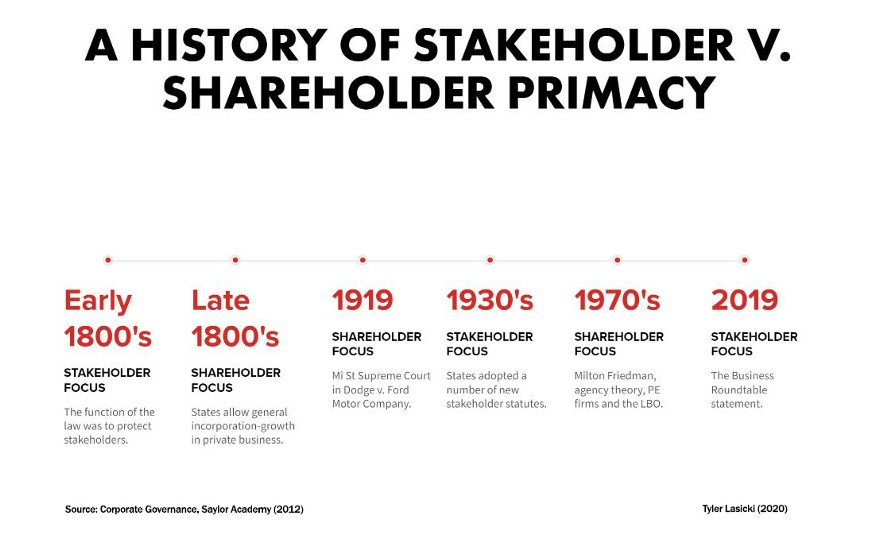
So earlier in this post we had mentioned about a shift in philosophy at the corporate boardroom that affected how comparate thought, value, and responsibility: Companies in the 1980s started to shift their focus and value only the needs of corporate ShAREHOLDERS at the expense of their traditional STAKEHOLDERS (customers, clients). Many movies and books have been written on this and debatable if deliberate or a by-product of M&A, hostile takeovers, and the stock market in general but the effect was that the consumer was relegated as having less value, even though marketing budgets are very high. The fiduciary responsibility of the executive was now defined in terms of satisfying shareholders, who were now big huge and powerful brokerage houses, private equity, and hedge funds. A good explanation by Medium.com Tyler Lasicki is given below.
In a famous 1970 New York Times Article, Milton Friedman postulated that the CEO, as an employee of the shareholder, must strive to provide the highest possible return for all shareholders. Since that article, the United States has embraced this idea as the fundamental philosophy supporting the ultimate purpose of businesses — The Shareholders Come First.
In August of 2019, the Business Roundtable, a group made up of the most influential U.S CEOs, published a letter shifting their stance on the purpose of a corporation. Regardless of whether this piece of paper will actually result in any systematic changes has yet to be seen, however this newly stated purpose of business is a dramatic shift from the position Milton Friedman took in 1970. According to the statement, these corporations will no longer prioritize maximizing profits for shareholders, but instead turn their focus to benefiting all stakeholders — including citizens, customers, suppliers, employees, on par with shareholders.
Now the social responsibility of a company and the CEO was to maxiimize the profits even at the expense of any previous social responsibility they once had.
Small sample of the 181 Signatures attached to the Business Roundtable’s letter
What has happened over the past 50 years that has led to such a fundamental change in ideology? What has happened to make the CEO’s of America’s largest corporations suddenly change their stance on such a foundational principle of what it means to be an American business?
Since diving into this subject, I have come to find that the “American fundamental principle” of putting shareholders first is one that is actually not all that fundamental. In fact, for a large portion of our nation’s history this ideology was actually seen as the unpopular position.
Key ideological shifts in U.S. history
This post dives into a brief history of these two contrasting ideological viewpoints in an attempt to contextualize the forces behind both sides — specifically, the most recent shift (1970–2019). This basic idea of what is most important; the stakeholder or the shareholder, is the underlying reason as to why many things are the way they are today. A corporation’s priority of shareholder or stakeholder ultimately impacts employee salaries, benefits, quality of life within communities, environmental conditions, even the access to education children can receive. It affects our lives in a breadth and depth of ways and now that corporations may be changing positions (yet again) to focus on a model that prioritizes the stakeholder, it is important to understand why.
Looking forward, if stakeholder priority ends up being the popular position among American businesses, how long will it last for? What could lead to its downfall? And what will managers do to ensure a long term stakeholder-friendly business model?
It is clear to me the reasons that have led to these shifts in ideology are rather nuanced, however I want to highlight a few trends that have had a major impact on businesses changing their priorities while also providing context as to why things have shifted.
The Ascendancy of Shareholder Value
Following the 1929 stock market crash and the Great Depression, stakeholder primacy became the popular perspective within corporate America. Stakeholder primacy is the idea that corporations are to consider a wider group of interested parties (not just shareholders) whose positions need to be taken into consideration by corporate governance. According to this point of view, rather than solely being an agent for shareholders, management’s responsibilities were to be dispersed among all of its constituencies, even if it meant a reduction in shareholder value. This ideology lasted as the dominant position for roughly 40 years, in part due to public opinion and strong views on corporate responsibility, but also through state adoption of stakeholder laws.
By the mid-1970s, falling corporate profitability and stagnant share prices had been the norm for a decade. This poor economic performance influenced a growing concern in the U.S. regarding the perceived divergence between manager and shareholder interest. Many held the position that profits and share prices were suffering as a result of corporation’s increased attention on stakeholder groups.
This noticeable divergence in interests sparked many academics to focus their research on corporate management’s motivations in decision making regarding their allocation of resources. This branch of research would later be known as agency theory, which focused on the relationship between principals (shareholders) and their agents (management). Research at the time outlined how over the previous decades corporate management had pursued strategies that were not likely to optimize resources from a shareholder’s perspective. These findings were part of a seismic shift of corporate philosophy, changing priority from the stakeholders of a business to the shareholders.
By 1982, the U.S. economy started to recover from a prolonged period of high inflation and low economic growth. This recovery acted as a catalyst for change in many industries, leaving many corporate management teams to struggle in response to these changes. Their business performance suffered as a result. These distressed businesses became targets for a group of new investors…private equity firms.
Now the paradigm shift had its biggest backer…. private equity! And private equity care about ONE thing….. THEIR OWN SHARE VALUE and subsequently meaning corporate profit, which became the most important directive for the CEO.
So it is all hopeless now? Can there be a shift back to the good ‘ol days?
Well some changes are taking place at top corporate levels which may help the stakeholders to have a voice at the table, as the following IRMagazine article states.
And once again this is being led by the Business Roundtable, the same Business Roundtable that proposed the shift back in the 1970s.
n a major corporate shift, shareholder value is no longer the main objective of the US’ top company CEOs, according to the Business Roundtable, which instead emphasizes the ‘purpose of a corporation’ and a stakeholder-focused model.
The influential body – a group of chief executive officers from major US corporations – has stressed the idea of a corporation dropping the age-old notion that corporations function first and foremost to serve their shareholders and maximize profits.
Rather, the focus should be on investing in employees, delivering value to customers, dealing ethically with suppliers and supporting outside communities as the vanguard of American business, according to a Business Roundtable statement.
‘While each of our individual companies serves its own corporate purpose, we share a fundamental commitment to all of our stakeholders,’ reads the statement, signed by 181 CEOs. ‘We commit to deliver value to all of them, for the future success of our companies, our communities and our country.’
Gary LaBranche, president and CEO of NIRI, tells IR Magazine that this is part of a wider trend: ‘The redefinition of purpose from shareholder-focused to stakeholder-focused is not new to NIRI members. For example, a 2014 IR Update article by the late Professor Lynn Stout urges a more inclusive way of thinking about corporate purpose.’
NIRI has also addressed this concept at many venues, including the senior roundtable annual meeting and the NIRI Annual Conference, adds LaBranche. This trend was further seen in the NIRI policy statement on ESG disclosure, released in January this year.
Analyzing the meaning of this change in more detail, LaBranche adds: ‘The statement is a revolutionary break with the Business Roundtable’s previous position that the purpose of the corporation is to create value for shareholders, which was a long-held position championed by Milton Friedman.
‘The challenge is that Friedman’s thought leadership helped to inspire the legal and regulatory regime that places wealth creation for shareholders as the ‘prime directive’ for corporate executives.
‘Thus, commentators like Mike Allen of Axios are quick to point out that some shareholders may actually use the new statement to accuse CEOs of worrying about things beyond increasing the value of their shares, which, Allen reminds us, is the CEOs’ fiduciary responsibility.
‘So while the new Business Roundtable statement reflects a much-needed rebalancing and modernization that speaks to the comprehensive responsibilities of corporate citizens, we can expect that some shareholders will push back on this more inclusive view of who should benefit from corporate efforts and the capital that makes it happen. The new statement may not mark the dawn of a new day, but it perhaps signals the twilight of the Friedman era.’
In a similarly reflective way, Jamie Dimon, chairman and CEO of JPMorgan Chase & Co and chairman of the Business Roundtable, says: ‘The American dream is alive, but fraying. Major employers are investing in their workers and communities because they know it is the only way to be successful over the long term. These modernized principles reflect the business community’s unwavering commitment to continue to push for an economy that serves all Americans.’
Note: Mr Dimon has been very vocal for many years on corporate social responsibility, especially since the financial troubles of 2009.
Impact of New Regulatory Trends in M&A Deals
The following podcast from Pricewaterhouse Cooper Health Research Institute (called Next in Health) discusses some of the trends in healthcare M&A and is a great listen. However from 6:30 on the podcast discusses a new trend which is occuring in the healthcare company boardroom, which is this new focus on integrating companies that have proven ESG (or environmental, social, governance) functions within their organzations. As stated, doing an M&A deal with a company with strong ESG is looked favorably among regulators now.
Please click on the following link to hear a Google Podcast Next in Health episode
Heather shows the feasability of this model with multiple biotech and healthtech startups, including one founded by Mark Cuban.
Health tech unicorn Aledade recently announced that it made the strategic decision to become a public benefit corporation (PBC).
The company joins just a handful of others in healthcare that are structured this way.
So what exactly is a PBC, and why does it matter?
PBCs are a type of for-profit corporate entity that has also adopted a public benefit purpose and is currently authorized by 35 states and the District of Columbia. A PBC must consider the nonfinancial interests of its shareholders and other stakeholders when making decisions. As a public benefit corporation, companies have to weigh their social/environmental objectives alongside maximizing value for shareholders.
While PBC and B Corp. are often used interchangeably, they are not the same. A B Corp. is a certification provided to eligible companies by the nonprofit, B Lab. A PBC is an actual legal entity that bakes into its certificate of incorporation a “public benefit,” according to Rubicon Law Group.
“I don’t think that there is a trade-off between either you do things that are good for society or you make profits in your business.” —Farzad Mostashari, M.D.
PBCs also are required to provide a report to shareholders every two years that detail how well the company is achieving its overall public benefit objectives. In some states, the report must be assessed against a third-party standard and be made publicly available. Delaware PBCs are not required to report publicly or against a third-party standard.
Aledade launched in 2014 and uses data analytics to help independent doctors’ offices transition to value-based care models. The company currently partners with more than 1,000 independent primary care practices comprising over 11,000 physicians and has nearly 150 contracts covering more than 1.7 million patients and $17 billion in total healthcare spending. Last June, the company raised $123 million in a series E round, boosting its valuation to $3.1 billion.
In a blog post, Aledade CEO and co-founder Farzad Mostashari, M.D., explained the company’s reasoning behind the move and said the corporate structure of a PBC is “well suited to mission-oriented companies where alignment with stakeholders is a key driver of the business model.”
“Aledade’s public benefit purpose means that we must weigh the interests of our primary care practice partners, their patients, our employees, and those who bear the burden of rising health care costs, alongside those of our shareholders, when we make decisions,” Mostashari said in an interview. This duty extends to all significant board decisions, including decisions on whether to go public, to make acquisitions or to sell the company, he noted.
The PBC structure helps create alignment among stakeholders and build trust, he said. “I don’t think that there is a trade-off between either you do things that are good for society or you make profits in your business. That might be true for fee-for-service businesses. It’s not true for Aledade,” he said.
He added, “For businesses that are built on trust and alignment, not considering stakeholder benefits gets you neither social good nor profits. If you’re in a business like our business where it’s actually really important that everybody have faith and belief that you are doing what’s best for patients, that you are actually in it for the long-term for practices, that’s what makes us successful as a business.”
Mark Cuban Cost Plus Drugs, which launched in January 2022 to offer low-cost rivals to overpriced generic drugs, also is structured as a public benefit corporation. The company’s founder and CEO Alexander Oshmyansky started the company in 2015 as a nonprofit, according to a feature story in D Magazine. Through Y Combinator, investors told Oshmyansky that the nonprofit model wouldn’t be able to raise the needed funds. He then reworked the business model to a PBC and launched Osh’s Affordable Pharmaceuticals in 2018.
Some other companies that are biotech drug development companies that operate under the PBC model include
Even a traditional for-profit C corporation can work toward a public mission without becoming a PBC. But, in an industry like healthcare, too often the duty to maximize financial returns for shareholders or investors can be in conflict with what is best for patients, executives say.
“With a startup, it might limit the ability to sell their business to a larger company in the future because there might be some limitations on what the larger company could do with the organization.”—Jodi Daniel, a partner in Crowell & Moring’s Health Care Group
According to some healthcare experts, PBCs offer a promising alternative as a business model for healthcare companies by providing a “North Star” by which a company can navigate critical business decisions.
“I think it really helps to drive accountability,” Huang, Osmind’s chief executive, said. “I think that’s important, especially in healthcare where it’s easy sometimes to get misaligned with all the different stakeholders that are involved in the industry. We wanted to make sure we had something to be accountable to. Second, it’s ingrained in the culture. The third element of why it was so helpful for us from the beginning is just on focus and alignment. I think we can be much more clear and transparent about what we’re focused on, our values, how we try to use that transparently to influence our decisions and how we can build a business that really ties all of that together.”
In a Health Affairs article, medical researchers at Stanford, including Jimmy Qian, a co-founder of Osmind, laid out the case for why PBCs may simultaneously improve individual patient outcomes and collective benefit without sacrificing institutions’ financial stability.
PBCs are held legally accountable to a predefined public benefit, which, for hospitals, could involve delivering high-quality, affordable care to local populations. PBCs are required to produce annual benefits reports that are assessed against a third-party standard. “These reports could be used by regulatory agencies such as the Centers for Medicare and Medicaid Services (CMS) or local health authorities to evaluate whether the PBC is making progress toward its stated mission and respond accordingly,” the researchers wrote.
But are there any trade-offs?
Having a public benefit obligation could potentially “tie the hands” of board members who can’t just focus on profits and must focus on those dual responsibilities, noted Jodi Daniel, a partner in Crowell & Moring’s Health Care Group.
“Companies that transition to being a public benefit corporation are intentionally trying to ensure that that the company’s mission doesn’t get diminished over time because it’s in their charter. So it helps [the mission] to endure. But there are pros and cons to that. It is somewhat binding the future board members and executives to follow that mission,” she said.
Daniel said she has spoken with several healthcare companies recently that are weighing the possibility of transitioning to a PBC. “Companies often don’t want to necessarily limit their options in their decision-making in the future. With a startup, it might limit the ability to sell their business to a larger company in the future because there might be some limitations on what the larger company could do with the organization,” she said in an interview.
By making decisions based on interests outside of financial ones, organizations may put themselves at a margin disadvantage as compared to pure for-profit players in the space, wrote Hospitalogy founder Blake Madden.
Faddis with Veeva said the company hasn’t seen any financial or performance trade-off as a result of operating as a PBC. He noted that the move has been good for recruiting, spurred more long-term conversations with customers and has been a source of new ideas.
“Prior to the conversion, you had employees who were thinking of new products or new functionality with the mindset of getting to be commercially successful,” Faddis said. “Now, you also have people thinking about it from the angle of, ‘Does it further one of our PBC purposes and then maybe it’s also going to be commercially successful?'”
Converting to a PBC also can be a tactic to build trust, Daniel noted, especially in healthcare, and that holds the potential to drive business.
One factor that isn’t clear is whether there is sufficient oversight to hold these companies accountable to their stated public mission. Who checks to make sure companies are making progress toward their objectives to improve healthcare?
Osmind publishes its benefit corporation report on its website to make it available to the public even though it is not required to do so. “I think that really highlights the accountability piece of you need to tell the world or at least tell your shareholders how you’re really trying to uphold your public benefit,” Huang said.
Other related articles published on this Open Access Online Scientific Journal on Healthcare Issues include the following:
Reporter: Danielle Smolyar, Research Assistant 3 – Text Analysis for 2.0 LPBI Group’s TNS #1 – 2020/2021 Academic Internship in Medical Text Analysis (MTA)
An increase of infections among youth who are unvaccinated in countries with high vaccination rates is getting noticed in the role of young people in the pandemic.
On June 21 is Ross Ministry of health recommended that all individuals between the ages of 12 and 15 should be vaccinated. This makes the nation one of the few that have been approved vaccinations for younger kids. This decision came about in response too many other countries with high rates of vaccination are experiencing an increase in numbers of infections that are found to be in younger age groups.
Israel’s vaccination campaign which has reached to more than 85% of the adult population to be vaccinated noticed that case numbers are dropping around a dozen daily in the month of June. At the end of June, they have realized that the cases began to rise to more than 100 cases a day. These cases were found in kids under the age of 16 which is why the government decided to allow vaccinations.
Ran Balicer, and epidemiologists at Israel’s largest healthcare provider in Tel Aviv said that the younger profile is not surprising.
This trend that Israel started to notice is not just happening in Israel. The United States and the United Kingdom COVID-19, “become a disease of the unvaccinated, who are predominantly young”, says Joshua Goldstein, a demographer at the University of California, Berkeley. Stated in the article.
This trend has been occurring in the countries where the older population were being vaccinated first. Follow the drop in age because they were vaccinating older people who are the most at risk for the disease.
This shift has shut attention to the studies of transmission in the younger age groups. Karin Magnusson immunologist said that it has come very important to understand the burden of the disease among the younger children.
Magnusson on the impact of COVID-19 in children in Norway. On June 5 pre-print she reported that children see their doctor regularly up to six months after contracting Covid-19.
Balicer, is studying the virus spread in multi-generational households in Israel. Going beyond whether vaccinating children or not the patterns of COVID-19 infection have caused discussions about mask wearing to adolescence and kids in Israel.
As stated in the article, “As the burden of cases shifts towards younger people, arguments for vaccinating adolescents will become slightly more compelling,” agrees Nick Bundle, an epidemiologist at the European Centre for Disease Prevention and Control in Stockholm.” However, the risk of disease in children still is low and in other countries the total number of cases have declined.
Countries also need to consider the global contacts. As stated in the article, “Are we really better off giving the vaccine to kids in rich countries than to older people [in less wealthy countries] where it might have a much bigger impact on people’s lives?” says Jennie Lavine, who studies infectious-disease dynamics at Emory University in Atlanta, Georgia. “It seems hard for me to imagine a really good argument for that.”
Oh there is a downward shift and the average age of infected with COVID-19 in countries with high COVID-19 vaccination rates it may be short-lived. There could be a few scenarios where the shift could bounce back says Henrik Salje, who is an infectious disease epidemiologist at the University of Cambridge, UK. Many of the countries could start vaccinating the adolescence just like Israel and the United States are already doing so.
Bundle says that COVID- 19 can still be present in younger kids. “But how big a problem that is, is not a simple thing to respond to.”
New evidence has shown how coronavirus has caused much damage to the brain. There is a new evidence that shows that COVID-19 assault on the brain I has the power to be multipronged. What this means is that it can attack on certain Brain cells such as reduce the amount of blood flow that the brain needs to the brain tissue.
Along with brain damage COVID-19 has also caused strokes and memory loss. A neurologist at yell University Serena Spudich says, “Can we intervene early to address these abnormalities so that people don’t have long-term problems?”
We’re on 80% of the people who have been hospitalized due to COVID-19 have showed brain symptoms which seem to be correlated to coronavirus.
At the start of the pandemic a group of researchers speculated that coronavirus they can damage the brain by infecting the neurons in the cells which are important in the process of transmitting information. After further studies they found out that coronavirus has a harder time getting past the brains defense system and the brain barrier and that it does not affect the neurons in anyway.
An expert in this study indicated that a way in which SARS-CoV-2 may be able to get to the brain is by going through the olfactory mucosa which is the lining of the nasal cavity. It is found that this virus can be found in the nasal cavity which is why we swab the nose one getting tested for COVID-19.
Spudich quotes, “there’s not a tonne of virus in the brain”.
Recent studies indicate that SARS-CoV-2 have ability to infect astrocytes which is a type of cell found in the brain. Astrocytes do quite a lot that supports normal brain function,” including providing nutrients to neurons to keep them working, says Arnold Kriegstein, a neurologist at the University of California, San Francisco.
Astrocytes are star-shaped cells in the central nervous system that perform many functions, including providing nutrients to neurons.
Kriegstein and his fellow colleagues have found that SARS-CoV-2 I mostly infects the astrocytes over any of the other brain cells present. In this research they expose brain organoids which is a miniature brain that are grown from stem cells into the virus.
As quoted in the article” a group including Daniel Martins-de-Souza, head of proteomics at the University of Campinas in Brazil, reported6 in a February preprint that it had analysed brain samples from 26 people who died with COVID-19. In the five whose brain cells showed evidence of SARS-CoV-2 infection, 66% of the affected cells were astrocytes.”
The infected astrocytes could indicate the reasoning behind some of the neurological symptoms that come with COVID-19. Specifically, depression, brain fog and fatigue. Kreigstein quotes, “Those kinds of symptoms may not be reflective of neuronal damage but could be reflective of dysfunctions of some sort. That could be consistent with astrocyte vulnerability.”
A study that was published on June 21 they compared eight different brands of deceased people who did have COVID-19 along with 14 brains as the control. The results of this research were that they found that there was no trace of coronavirus Brain infected but they found that the gene expression was affected in some of the astrocytes.
As a result of doing all this research and the findings the researchers want to know more about this topic and how many brain cells need to be infected for there to be neurological symptoms says Ricardo Costa.
Further evidence has also been done on how SARS-CoV-2 can affect the brain by reducing its blood flow which impairs the neurons’ function which ends up killing them.
Pericytes can be found on the small blood vessels which are called capillaries and are found all throughout the body and in the brain. In a February pre-print there was a report about how SARS-CoV-2 can infect the pericyte in the brain organoids.
David Atwell, a neuroscientist at the University College London, along with his other colleagues had published a pre-print which has evidence to show that SARS-CoV-2 odes In fact pericytes behavior. I researchers saw that in the different part of the hamsters brain SARS-CoV-2 blocks the function of receptors on the pericytes which ultimately causes the capillaries found inside the tissues to constrict.
As stated in the article, It’s a “really cool” study, says Spudich. “It could be something that is determining some of the permanent injury we see — some of these small- vessel strokes.”
Attwell brought to the attention that the drugs that are used to treat high blood pressure may in fact be used in some cases of COVID-19. Currently there are two clinical trials that are being done to further investigate this idea.
There is further evidence showing that the neurological symptoms and damage could in fact be happening because of the bodies on immune system reacting or misfiring after having COVID-19.
Over the past 15 years it has become evident that people’s immune system’s make auto antibodies which attack their own tissues says Harald Prüss in the article who has a Neuroimmunologist at the German Center for neurogenerative Diseases in Berlin. This may cause neuromyelitis optica which is when you can experience loss of vision or weakness in limbs. Harald Prüss summarized that the autoantibodies can pass through the blood brain barrier and ultimately impact neurological disorders such as psychosis.
Prüss and his colleagues published a study last year that focused on them isolating antibodies against SARS-CoV-2 from people. They found that one was able to protect hamsters from lung damage and other infections. The purpose of this was to come up with and create new treatments. During this research they found that some of the antibodies from people. They found that one was able to protect hamsters from lung damage and other infections. The purpose of this was to come up with and create new treatments. During this research they found that some of the antibodies can bind to the brain tissue which can ultimately damage it. Prüss states, “We’re currently trying to prove that clinically and experimentally,” says Prüss.
Was published online in December including Prüss sorry the blood and cerebrospinal fluid of 11 people who were extremely sick with COVID-19. These 11 people had neurological symptoms as well. All these people were able to produce auto antibodies which combined to neurons. There is evidence that when the patients were given intravenous immunoglobin which is a type of antibody it was successful.
Astrocytes, pericytes and autoantibodies we’re not the only pathways. However it is likely that people with COVID-19 experience article symptoms for many reasons. As stated, In the article, Prüss says a key question is what proportion of cases is caused by each of the pathways. “That will determine treatment,” he says.
Comparing COVID-19 Vaccine Schedule Combinations, or “Com-COV” – First-of-its-Kind Study will explore the Impact of using eight different Combinations of Doses and Dosing Intervals for Different COVID-19 Vaccines
Ramatroban, a Thromboxane A2/TPr and PGD2/DPr2 receptor antagonist for Acute and Long haul COVID-19
Author: Ajay Gupta, MD
From: “Gupta, Ajay” <ajayg1@hs.uci.edu> Date: Wednesday, July 7, 2021 at 1:10 PM To: Aviva Lev-Ari <AvivaLev-Ari@alum.berkeley.edu> Cc: “Dr. Saul Yedgar” <saulye@ekmd.huji.ac.il> Subject: Ramatroban, a Thromboxane A2/TPr and PGD2/DPr2 receptor antagonist for Acute and Long haul COVID-19
While corticosteroids may have a role in about 5% of hospitalized patients who have the cytokine storm, currently there is no effective treatment for mild or moderate COVID and long haul COVID. Massive increase in respiratory and plasma thromboxane A2 (TxA2) plays a key role in thromboinflammation and microvascular thrombosis, while an increase in respiratory and plasma PGD2 potentially suppresses innate interferon response, and acquired Th1 anti-viral response, while promoting a maladaptive type 2, anti-helminthic like immune response. Ramatroban is a potent dual receptor antagonist of Thromboxane A2/TPr and PGD2/DPr2 that has been used in Japan for the treatment of allergic rhinitis for past 20 years (Baynas®, Bayer Japan). We first disclosed use of ramatroban for COVID in a provisional patent application filed on 31st March, 2020; followed by the publication Gupta et al, J Mol Genet Med, 2020
Several experts, as outlined below in yellow highlighted text, have supported the idea of using ramatroban as an anti-thrombotic and immunomodulator in COVID-19.
1. Prof. Louis Flamand, Nicolas Flamand, Eric Boilard Laval Univ. Quebec, Canada: There is a lipid-mediator storm in COVID-19 characterized by massive increases in thromboxane A2 and PGD2 in the lungs and plasma. “Blocking the deleterious effects of PGD2 and TxA2 with the dual DPr2/TPr antagonist Ramatroban might be beneficial in COVID-19Archambault et al, FASEB, June 2021, doi: https://doi.org/10.1096/fj.202100540R
2. Prof. Garret A FitzGerald, Univ. Of Pennsylvania, Member National Academy of Sciences.https://en.wikipedia.org/wiki/Garret_A._FitzGerald “In the current pandemic there may be utility in targeting eicosanoids with existing drugs. These approaches would likely be most effective early in the disease before the development of ARDS, where cytokines and chemokines dominate. Dexamethasone limits COX-2 expression and might diminish COVID-19 severity and mortality at least in part, by diminishing COX metabolites… Dexamethasone might improve severe COVID-19 by diminishing the prostaglandins / thromboxane storm in the lungs”. “Treatment with a PGD2/DPr2 inhibitor decreased viral load and improved morbidity by upregulating IFN-lambda expression. ….. Antagonism of the thromboxane receptor (TPr) prevents ARDS…. Early administration of well-tolerated TPr antagonists may limit progress to severe COVID-19 (Theken and FitzGerald, Science, 2021)
4. Prof. Simon Phipps, Univ. of Queensland, Brisbane Australia “It has been hypothesized that DP2 antagonists be repurposed as a novel immunotherapy for the treatment of COVID-19, and this may be appropriate in mild to moderate cases where Th1 immunity is impaired.” (Ullah et al, Mucosal Immunology, 2021)
5. Prof. Bruce D. Hammock, Distinguished Professor, Univ of California Davis, Member US National Academy of Sciences and National Academy of Inventors; April 25, 2021. https://www.entsoc.org/fellows/hammock “I find your idea of blocking specific thromboxane receptors in preventing or reducing some of the devastating co-morbidity of COVID-19 very compelling. … A DPr2 receptor blocker is conceptually attractive in offering the potential of effective therapy and low risk due to a high therapeutic index.” E mail dated April 25, 2021.(https://ajp.amjpathol.org/action/showPdf?pii=S0002-9440%2820%2930332-1 and http://ucanr.edu/sites/hammocklab/files/328012.pdf)
6. Ann E Eakin, PhD, Senior Scientific Officer, NIH-NIAID “very compelling data supporting potential benefits of ramatroban in both reducing viral load as well as modulating host responses” E Mail dated Nov 20, 2020
Ramatroban is expected to reduce lung fibrosis in COVID-19 and therefore diminish clinical manifestations of Long haul COVID. Pang et al, 2021 “examined the effect of Ramatroban, a clinical antagonist of both PGD2 and TXA2 receptors, on treating silicosis using a mouse model. The results showed that Ramatroban significantly alleviated silica-induced pulmonary inflammation, fibrosis, and cardiopulmonary dysfunction compared with the control group.” https://www.thno.org/v11p2381.htm
Unfortunately, the animal models of COVID-19 are harsh, lack microvascular thrombosis and immune perturbations characteristic of human disease. These models may be good for testing antivirals but not for testing immunomodulators or anti-thrombotics. There is highly positive anecdotal experience with use of ramatroban in moderately severe COVID-19 (https://www.researchsquare.com/article/rs-474882/v1
Ending a global pandemic demands a global response. I am thrilled that a novel vaccine adjuvant developed in the United States with NIAID support is now included in an effective COVID-19 vaccine that is available to individuals in India.”
Adjuvants are components that are created as part of a vaccine to improve immune responses and increase the efficiency of the vaccine. COVAXIN was developed and is manufactured in India, which is currently experiencing a terrible health catastrophe as a result of COVID-19. An adjuvant designed with NIH funding has contributed to the success of the extremely effective COVAXIN-COVID-19 vaccine, which has been administered to about 25 million individuals in India and internationally.
Alhydroxiquim-II is the adjuvant utilized in COVAXIN, was discovered and validated in the laboratory by the biotech company ViroVax LLCof Lawrence, Kansas, with funding provided solely by the NIAID Adjuvant Development Program. The adjuvant is formed of a small molecule that is uniquely bonded to Alhydrogel, often known as alum and the most regularly used adjuvant in human vaccines. Alhydroxiquim-II enters lymph nodes, where it detaches from alum and triggers two cellular receptors. TLR7 and TLR8 receptors are essential in the immunological response to viruses. Alhydroxiquim-II is the first adjuvant to activate TLR7 and TLR8 in an approved vaccine against an infectious disease. Additionally, the alum in Alhydroxiquim-II activates the immune system to look for an infiltrating pathogen.
Although molecules that activate TLR receptors strongly stimulate the immune system, the adverse effects of Alhydroxiquim-II are modest. This is due to the fact that after COVAXIN is injected, the adjuvant travels directly to adjacent lymph nodes, which contain white blood cells that are crucial in recognizing pathogens and combating infections. As a result, just a minimal amount of Alhydroxiquim-II is required in each vaccination dosage, and the adjuvant does not circulate throughout the body, avoiding more widespread inflammation and unwanted side effects.
This scanning electron microscope image shows SARS-CoV-2 (round gold particles) emerging from the surface of a cell cultured in the lab. SARS-CoV-2, also known as 2019-nCoV, is the virus that causes COVID-19. Image Source: NIAID
COVAXIN is made up of a crippled version of SARS-CoV-2 that cannot replicate but yet encourages the immune system to produce antibodies against the virus. The NIH stated that COVAXIN is “safe and well tolerated,” citing the results of a phase 2 clinical investigation. COVAXIN safety results from a Phase 3 trial with 25,800 participants in India will be released later this year. Meanwhile, unpublished interim data from the Phase 3 trial show that the vaccine is 78% effective against symptomatic sickness, 100% effective against severe COVID-19, including hospitalization, and 70% effective against asymptomatic infection with SARS-CoV-2, the virus that causes COVID-19. Two tests of blood serum from persons who had received COVAXIN suggest that the vaccine creates antibodies that efficiently neutralize the SARS-CoV-2 B.1.1.7 (Alpha) and B.1.617 (Delta) variants (1) and (2), which were originally identified in the United Kingdom and India, respectively.
Since 2009, the NIAID Adjuvant Program has supported the research of ViroVax’s founder and CEO,Sunil David, M.D., Ph.D. His research has focused on the emergence of new compounds that activate innate immune receptors and their application as vaccination adjuvants.
Dr. David’s engagement with Bharat Biotech International Ltd. of Hyderabad, which manufactures COVAXIN, began during a 2019 meeting in India organized by the NIAID Office of Global Research under the auspices of the NIAID’s Indo-US Vaccine Action Program. Five NIAID-funded adjuvant investigators, including Dr. David, two representatives of the NIAID Division of Allergy, Immunology, and Transplantation, and the NIAID India representative, visited 4 top biotechnology companies to learn about their work and discuss future collaborations. The delegation also attended a consultation in New Delhi, which was co-organized by the NIAID and India’s Department of Biotechnology and hosted by the National Institute of Immunology.
Among the scientific collaborations spawned by these endeavors was a licensing deal between Bharat Biotech and Dr. David to use Alhydroxiquim-II in their candidate vaccines. During the COVID-19 outbreak, this license was expanded to cover COVAXIN, which has Emergency Use Authorization in India and more than a dozen additional countries. COVAXIN was developed by Bharat Biotech in partnership with the Indian Council of Medical Research’sNational Institute of Virology. The company conducted thorough safety research on Alhydroxiquim-II and undertook the arduous process of scaling up production of the adjuvant in accordance with Good Manufacturing Practice standards. Bharat Biotech aims to generate 700 million doses of COVAXIN by the end of 2021.
NIAID conducts and supports research at the National Institutes of Health, across the United States, and across the world to better understand the causes of infectious and immune-mediated diseases and to develop better methods of preventing, detecting, and treating these illnesses. The NIAID website contains news releases, info sheets, and other NIAID-related materials.
Other Related Articles published in this Open Access Online Scientific Journal include the following:
Comparing COVID-19 Vaccine Schedule Combinations, or “Com-COV” – First-of-its-Kind Study will explore the Impact of using eight different Combinations of Doses and Dosing Intervals for Different COVID-19 Vaccines