Posts Tagged ‘Hypertension’
Protected: Flywheel iNO, Three Novel Adult Patient Inhaled Nitric Oxide Product Concepts by Justin D. Pearlman MD ME PhD FACC
Posted in Medical Devices R&D Investment, Medical Imaging Technology, Image Processing/Computing, MRI, CT, Nuclear Medicine, Ultra Sound, Nitric Oxide in Health and Disease, Technology Transfer: Biotech and Pharmaceutical, tagged Heart Failure, Hypertension, nitric oxide, Nitric oxide synthase, Pulmonary hypertension, Torr on June 3, 2013|
Imaging Biomarker for Arterial Stiffness: Pathways in Pharmacotherapy for Hypertension and Hypercholesterolemia Management
Posted in Atherogenic Processes & Pathology, Bio Instrumentation in Experimental Life Sciences Research, Chemical Biology and its relations to Metabolic Disease, Disease Biology, Small Molecules in Development of Therapeutic Drugs, Exec Compensation in the Cardiac & Vascular Repair Tools Subsegment, FDA Regulatory Affairs, Frontiers in Cardiology and Cardiovascular Disorders, Health Economics and Outcomes Research, Health Law & Patient Safety, HTN, International Global Work in Pharmaceutical, Molecular Genetics & Pharmaceutical, Nutrition, Nutritional Supplements: Atherogenesis, lipid metabolism, Origins of Cardiovascular Disease, Personalized and Precision Medicine & Genomic Research, Pharmaceutical Analytics, Pharmaceutical Industry Competitive Intelligence, Pharmaceutical R&D Investment, Pharmacotherapy of Cardiovascular Disease, Population Health Management, Genetics & Pharmaceutical, Population Health Management, Nutrition and Phytochemistry, Regulated Clinical Trials: Design, Methods, Components and IRB related issues, Systemic Inflammatory Response Related Disorders, Technology Transfer: Biotech and Pharmaceutical, tagged Arterial stiffness, Aviva Lev-Ari, Biotechnology and Pharmaceuticals, Bosentan, Clinical trial, Hawthorne Effect, Hypertension, Imaging biomarker, Pulse wave velocity on May 24, 2013| 6 Comments »
Imaging Biomarker for Arterial Stiffness: Pathways in Pharmacotherapy for Hypertension and Hypercholesterolemia Management
Author, and Content Consultant to e-SERIES A: Cardiovascular Diseases: Justin Pearlman, MD, PhD, FACC
and
Article Curator: Aviva Lev-Ari, PhD, RN
This article has Four Parts:
Part 1:
Quantification of Arterial Stiffness selected for its Predictive Value for Cardiovascular (CV) Events.
Arterial stiffness can predict cardiovascular adverse events such as stroke and heart attack. While there are various ways to define and estimate arterial stiffness, relatively simple surrogates have clinical advantages and favorable reports regarding predictive accuracy. This article will review in particular carotid-femoral pulse wave velocity (cfPWV) as an imaging-based biomarker of arterial stiffness.
Part II:
Results for Advances and Recent Clinical Trials in Hypertension Management
Caution is required in the interpretation of trial results, due to the Hawthorne Effect: participation in a trial confers benefits to all groups. Usually the Hawthorne effect is attributed to the close attention and is considered transient, but it can have lasting impact. In a retrospective cohort study, the benefits of participation in clinical trials irrespective of the treatment allocation were illustrated by better persistence and adherence to prescribed medication long term.
- Participation in a clinical trial enhances adherence and persistence to treatment: a retrospective cohort study.
Hypertension . 2011 ; 58 : 573 – 578 .
- It is proving more and more difficult to show incremental benefit of new therapies over standard therapy in control groups that are on background therapy marked by high statin, antiplatelet, and other antihypertensive therapy rates, as well as more overweight and obesity and less tobacco use than in the past.
Participation in a Clinical Trial Enhances Adherence and Persistence to Treatment, A Retrospective Cohort Study Chronobiol Int . 2011 ; 28 : 601 – 610.
Cardiorenal end points in a trial of Aliskiren for type 2 diabetes. N Engl J Med . 2012 ; 367 : 2204 – 2213.
Part III:
Pharmacotherapy for Hypertension and Hypercholesterolemia Management: Mechanism of Action of Top 10 Cardio Drugs 2012, published on May 16, 2013. FiercePharma reports the top 10 drugs from expenditure standpoint:
Part IV: Management Aspects of the Global Pharmaceutical Industry
The 20 Highest-Paid Biopharma CEOs of 2012 are also reported by FiersePharma.
-
1
-
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
Part 1:
Quantification of Arterial Stiffness selected for its Predictive Value for Cardiovascular (CV) Events.
based on
Stéphane Laurent, Elie Mousseaux and Pierre Boutouyrie, Arterial Stiffness as an Imaging Biomarker : Are All Pathways Equal?
http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.01372.citation
In a recent meta-analysis,2 Seventeen longitudinal studies totalizing 15,877 subjects with a mean follow-up of 7.7 years showed, for 1 SD increase in PWV, a risk ratio of 1.47 (1.31–1.64) for total mortality, 1.47 (1.29–1.66) for CV mortality, and 1.42 (1.29–1.58) for all-cause mortality.
Aortic stiffness, measured through cfPWV, can thus be considered as a novel imaging biomarker for predicting CV events, although its value as a true surrogate end point requires a large intervention trial to demonstrate that the reduction in arterial stiffness translates into a reduction in CV events.
In this article by Gosse et al7 published in the present issue of Hypertension, the Authors provides an important contribution with regard to the predictive value of arterial stiffness for CV events for the following reasons:
- First, the authors reported that arterial stiffness, measured in a population of 793 patients with hypertension with a mean follow-up of 97 months, was independently related to all CV events, major CV events, and total mortality. Interestingly, the predictive value was significant in all subgroups of CV risk, defined by a low, medium, or high SCORE risk. These findings confirmed those of previous studies.
- Second, the authors took advantage of the simultaneous measurement of 24-hour blood pressure (BP) to include 24-hour mean BP in the multivariate Cox analysis, and this is a novelty. Thus, they were able to provide the demonstration that the predictive value of arterial stiffness is not only independent of office BP, as shown in most epidemiological studies, but also of 24-hour mean BP and pulse pressure (or alternatively 24-hour systolic and diastolic BPs) simultaneously measured.
- Third, among the 793 patients, 519 patients had baseline measurements of arterial stiffness before any antihypertensive treatment, and the remaining 274 patients had measurement during the follow- up period. The independent predictive value of arterial stiffness was significant whether measured before or after the administration of antihypertensive treatment.
- Finally, Gosse et al 7 showed, in a subgroup of 523 patients who had a measurement of left ventricular mass index, that the predictive value of arterial stiffness for major CV events was independent of left ventricular mass index. The authors thus confirmed the very few epidemiological studies which analyzed the predictive value of biomarkers of target organ damages (ie, left ventricular mass index, urinary albumin excretion rate, carotid intimamedia thickness, and arterial stiffness) and found that arterial stiffness retained a significant predictive value when adjusted either to left ventricular mass index6 or carotid intima-media thickness.5
- The method which has been used to determine arterial stiffness. Indeed, Gosse et al 8 proposed, 2 decades ago, to take advantage of an ambulatory measurement of BP and continuous monitoring of ECG >24 hours, to calculate the QKD interval. QKD is the time between the onset of the QRS on the ECG and the detection of the last Korotkoff sound by the microphone placed on the brachial artery. It has 2 components:
- the pre-ejection time, which is influenced by heart rate and
- the pulse transmission time, which is inversely related to PWV, and arterial stiffness.
- BP and QKD are measured repeatedly, and a stiffness parameter is derived from the linear regression of all the measurements of QKD, heart rate, and systolic BP >24 hours. The QKD interval is calculated for a 100-mm Hg BP, thus it gives an isobaric value of arterial stiffness, and for a 60-beats/min heart rate to reduce the influence of the pre-ejection time.
- Most importantly, the arterial pathway of pulse wave transmission includes the ascending aorta, the aortic arch, and muscular arteries (subclavian and brachial), and thus,
- differs from the carotid-femoral pathway of the cfPWV measurement, considered as gold standard for arterial stiffness.9
- cfPWV is calculated as the ratio of the transit time between the feet of the carotid and femoral pressure waveforms, and the carotid-femoral distance, a ratio which is undisputedly recognized as a stiffness parameter. Several studies and a consensus statement have determined the correction factor, which should be applied to the carotid-femoral distance, to take into account the fact that, when the pressure wave is recorded at the carotid level, it has already reached the descending thoracic aorta.
- The pressure wave travels mostly along an aortic segment, including the thoracic descending aorta and the abdominal aorta, and ultimately travels along the iliac and common femoral arteries. This is well exemplified by the Figure, which superimposes the trajectory of the pressure pulse wave on a normal angiogram obtained by magnetic resonance imaging.
VIEW FIGURE
The trajectories of the pressure pulse waves along the arterial segments are superimposed onto an angiogram obtained by computed tomography scan (left anterior oblique). The carotid-femoral pathway is described as dotted line, and the QKD pathway is described as dashed line.

FIGURE SOURCE:
http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.01372.citation
The method developed by Gosse et al 7,8 measures the time delay between the onset of the QRS on the ECG and the detection of the last Korotkoff sound by the microphone placed on the brachial artery. Thus, the pressure pulse wave travels first along the ascending aorta and the aortic arch (ie, a short pathway of elastic arteries) and then along the subclavian and brachial arteries (ie, a much longer pathway of muscular arteries).
Because the stiffness of muscular arteries is little influenced by age and hypertension, Gosse et al8 attributed the difference in QKD duration to ascending aorta and aortic arch. However, a closer look at the Figure shows that the length of the ascending and aortic arch pathway represents a very small part of the total pathway and casts doubt about this statement.
Furthermore, in magnetic resonance imaging studies, the transit time of flow wave along the aortic arch (average 120 mm length) is often found ≈35 ms in young healthy subjects,10 a value which is far from the mean 206 ms QKD duration found in the present study. Thus, part of that QFD duration has to be further explained by both the preejection period and the transit time within muscular arteries.
Alternative Devices
- 2008 – The arteriograph system estimates PWV from a single-site determination of the suprasystolic waveform at the brachial artery site, and measures the time elapsed between the first wave ejected from the left ventricle to the aortic root, and its reflection from the bifurcation as the second systolic wave, with subtraction of the brachial artery transit time.
- 2010 – The Mobil-O-Graph system uses oscillometric recording of brachial artery pressure waveform and reconstructs the central pulse wave by applying a transfer function. Central pulse wave is then decomposed into forward and backward waves, and PWV isestimated from their time difference.
- Device |Method |Arterial Pathway |Predictive Value for CV Events | (Year of First Publication)
1984 Complior Mechanotransducer Carotid-femoral Yes (1999)
1990 Sphygmocor Tonometer Carotid-femoral Yes (2011)
1994 QKD ECG + Korotkoff sounds Aorta + brachial Yes (2005)
1997 Cardiov. Eng. Inc Tonometer Carotid-femoral Yes (2010)
2002 Doppler probes Doppler probe Aortic arch + descending aorta Yes (2002)
2002 VP-1000 Omron Brachial and ankle pressure cuffs Aorta + brachial + lower limbs Yes (2005)
2004 PulsePen Tonometer Carotid-femoral No
2006 CAVI-VaSera ECG + Brachial and ankle pressure cuffs Aorta + brachial + lower limbs No
2008 Arteriograph Arm pressure cuff Aorta + brachial No
2009 MRI-ArtFun MRI Aortic arch No
2009 Vicorder Cuffs Carotid-femoral No
2010 Mobil-O-Graph Arm pressure cuff Aorta No
Conclusions
The measurement of arterial stiffness is increasingly popular among physicians and researchers mainly because its predictive value for cardiovascular (CV) events has been well demonstrated. The largest amount of evidence has been given for aortic stiffness, measured through carotid-femoral pulse wave velocity (cfPWV). This has been initially reported in the late 1990s or early 2000s.1
Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37:1236–1241.
European Network for Non-invasive Investigation of Large Arteries. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588–2605.
Arterial Stiffness as an Imaging Biomarker : Are All Pathways Equal? http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.01372.citation
References for Imaging Biomarker for Arterial Stiffness, at the end of the paper
Part II:
Results for Advances and Recent Clinical Trials in Hypertension Management
Based on
Garry L.R. Jennings, Recent Advances in Hypertension:Recent Clinical Trials of Hypertension Management http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.00863.citation
Trends: tended to drive interest toward equivalence rather than efficacy studies (ie, trials designed to show an investigational agent is as good as, not better than, existing treatment), surrogate end points, including new blood pressure (BP) variables, and studies of combinations and algorithms rather than single interventions. Population studies around the world, however, continue to show that large numbers of people have hypertension that is not treated satisfactorily and are not achieving the goals set by the major national guidelines. These guidelines themselves are under continual scrutiny on the basis of recent data casting doubt on the validity of present BP goals. Guideline committees also face the issue that evidence based on expensive large-scale clinical trials is more often funded by the pharmaceutical or device industries than by government, leaving large evidence gaps in areas of public importance but no direct interest to industry funders. The purpose of the present article is to briefly review clinical trials of interventions in hypertension during the past 2 years.
Subject categories of Last Decade Clinical Trials on Hypertension
- Resistant Hypertension
- Resistant Hypertension and the Sympathetic
- Nervous System
- Trials of Pharmacotherapy
- Old Ground, New Findings
- Are Chlorthalidone and Nonthiazides the Best Diuretics for Treatment of Hypertension?
- BP Targets and Treatment
- Lifestyle and Nonpharmacological Approaches to Hypertension
- Sodium
- Trials of Nutrition and BP
- Resistance Exercise and BP
What Can Be Learned From Clinical Trials Reported in the Present Decade?
- Systems for blood pressure management in the community can be improved because a large treatment gap remains.
- Drug combinations from different classes with different modes of action are useful.
- Drug combinations that include drugs with similar mode of action do not generally enhance efficacy and come at a cost in adverse events.
- Small but important nutritional effects on blood pressure demand further examination.
- The sympathetic nervous system has returned as an important target for therapy of hypertension.
- Blood pressure targets and goals need refining, preferably on the basis of specifically designed clinical trials.
The scene for clinical trials of hypertension management is in transition. The era of mega trials may not be over but is certainly in decline, and in the past 2 years there have been no studies reporting primary outcome data the scale of the
- Antihypertensive and
- Lipid-Lowering Treatment
- Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT),
- The ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial (ONTARGET),
- Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT), and other
- major studies that marked clinical trial activity and informed guideline committees during the past 2 to 3 decades.
This reflects in part the view that the
- present benchmark pharmacological agents for treating hypertension are difficult to improve,
- some systemic issues affecting the pharmaceutical industry influencing the ability to make the large investment required to perform mega trials and
- the quality of the antihypertensive drug pipeline.
http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.00863.citation
References for Clinical Trial on Hypertension, at the end of the paper
Part III:
Mechanism of Action of Top 10 Cardio Drugs 2012, published on May 16, 2013
The top 10 Cardio Drugs in 2012 belong to two drug classes
- Antihypertensive and
- Lipid-Lowering Treatment
Sales % Change 2012 vs 2011 by Drug Class
|
MOA By Drug Class |
Drug Name |
2011 Sales billion |
2012 Sales billion |
% change |
|
Statins |
Crestor |
6.622 |
6.253 |
-6% |
|
Lipitor |
9.577 |
3.948 |
-59% |
|
|
Zetia |
2.428 |
2.567 |
+6% |
|
|
Vytorin |
1.882 |
1.747 |
-7% |
|
|
Total Sales and % change Statins |
20,509 | 14,515 | -29.2% | |
|
ARB |
Diovan |
5.665 |
4.417 |
-22% |
|
ACEII |
Benicar |
2.602 |
2.446 |
-6% |
|
ACEI |
Micardis |
2.217 |
2.098 |
-5% |
|
ARB |
Avapro |
1.797 |
1.422 |
-30% (BMS) |
|
ARB |
Blopress |
1.808 |
1.643 |
-9% |
|
PAH |
Tracleer |
1.721 |
1.6 |
-7% |
|
Total Sales and % change AntiHTN |
15,810 | 13,626 | -13.8% |
Data Source:
http://www.fiercepharma.com/special-reports/top-10-cardio-drugs-2012#ixzz2U9Axh8X4
1 Crestor
Crestor (AstraZeneca)
Patent expiry: July 2016
2012 sales: $6.253 billion
2011 sales: $6.622 billion
Change: (6%)
Crestor – FiercePharma http://www.fiercepharma.com/special-reports/crestor-0#ixzz2UACLZyaa
(rosuvastatin calcium) is indicated as an adjunct to diet to reduce elevated Total-C, LDL-C, ApoB, non-HDL-C, and triglycerides, and to increase HDL-C in adult patients with primary hyperlipidemia or mixed dyslipidemia and to slow the progression of atherosclerosis in adult patients as part of a treatment strategy to lower Total-C and LDL-C to target levels.1
2 Diovan
Diovan (Novartis)
Patent expiry: September 2012
2012 sales: $4.417 billion
2011 sales: $5.665 billion
Change: (22%)
Diovan – FiercePharma http://www.fiercepharma.com/special-reports/diovan#ixzz2UACdBCtZ
Valsartan (Angiotan or Diovan) is an angiotensin II receptor antagonist (more commonly called an “ARB”, or angiotensin receptor blocker), with particularly high affinity for the type I (AT1) angiotensin receptor. By blocking the action of angiotensin, valsartan dilates blood vessels and reduces blood pressure.[1] In the U.S., valsartan is indicated for treatment of high blood pressure, congestive heart failure (CHF), or post-myocardial infarction (MI).[2]
3 Lipitor
Lipitor (Pfizer)
Patent expiry: November 2011
2012 sales: $3.948 billion
2011 sales: $9.577 billion
Change: (59%)
Lipitor – FiercePharma http://www.fiercepharma.com/special-reports/lipitor-2#ixzz2UACsJ2Y2
(atorvastatin calcium) tablets are a prescription medicine that is used along with a low-fat diet. It lowers the LDL (“bad”) cholesterol and triglycerides in your blood. It can raise your HDL (“good”) cholesterol as well. LIPITOR can lower the risk for heart attack, stroke, certain types of heart surgery, and chest pain in patients who have heart disease or risk factors for heart disease such as age, smoking, high blood pressure, low HDL, or family history of early heart disease. LIPITOR can lower the risk for heart attack or stroke in patients with diabetes and risk factors such as diabetic eye or kidney problems, smoking, or high blood pressure.
LIPITOR is a member of the drug class known as statins, used for lowering blood cholesterol. It also stabilizes plaque and prevents strokes through anti-inflammatory and other mechanisms. Like all statins, atorvastatin works by inhibiting HMG-CoA reductase, an enzyme found in liver tissue that plays a key role in production of cholesterol in the body.
Atorvastatin was first synthesized in 1985 by Bruce Roth of Parke-Davis Warner-Lambert Company (now Pfizer). The best selling drug in pharmaceutical history, sales of Lipitor since it was approved in 1996 exceed US$125 billion, and the drug has topped the list of best-selling branded pharmaceuticals in the world for nearly a decade
4 Zetia
Zetia (Merck)
Patent expiry: December 2016
2012 sales: $2.567 billion
2011 sales: $2.428 billion
Change: 6%
Zetia – FiercePharma http://www.fiercepharma.com/special-reports/zetia#ixzz2UADFaGJ0
Ezetimibe (pron.: /ɛˈzɛtɨmɪb/) is a drug that lowers plasma cholesterol levels. It acts by decreasing cholesterol absorption in the intestine. It may be used alone (marketed as Zetia or Ezetrol), when other cholesterol-lowering medications are not tolerated, or together withstatins (e.g., ezetimibe/simvastatin, marketed as Vytorin and Inegy) when statins alone do not control cholesterol.
Ezetimibe decreases cholesterol levels, but has not been shown to improve outcomes in cardiovascular disease patients by decreasing atherosclerotic or vascular events compared to placebo. Ezetimibe is endorsed in the Canadian Lipid Guidelines and is considered a well-tolerated option for an add-on agent to statin, to help patients achieve their LDL (or bad cholesterol) targets. [1] Ezetimibe is the only add-on to statin therapy that has successfully shown cardiovascular benefit when combined with statin, but has not been proven to have an incremental benefit compared to statins alone. [2] Britain’s NICE statement, published in 2007, endorses its use for monotherapy if statins are not tolerated or as add-on therapy.[3]
5 Benicar
Benicar (Daiichi Sankyo)
Patent expiry: October 2016
2012 sales: $2.446 billion
2011 sales: $2.602 billion
Change: (6%)
Benicar – FiercePharma http://www.fiercepharma.com/special-reports/benicar#ixzz2UADYvld5
BENICAR and BENICAR HCT are prescription medicines used to lower high blood pressure (hypertension). They may be used alone or with other medicines used to treat high blood pressure. BENICAR HCT is not for use as the first medicine to treat high blood pressure.
Olmesartan medoxomil is an angiotensin II receptor antagonistused to treat high blood pressure.
Olmesartan is a prodrug that works by blocking the binding of angiotensin II to the AT1 receptors in vascular muscle; it is therefore independent of angiotensin II synthesis pathways, unlike ACE inhibitors. By blocking the binding rather than the synthesis of angiotensin II, olmesartan inhibits the negative regulatory feedback on renin secretion. As a result of this blockage, olmesartan reduces vasoconstriction and the secretion of aldosterone. This lowers blood pressure by producing vasodilation, and decreasing peripheral resistance.
6 Micardis
Micardis (Boehringer Ingelheim)
Patent Expiry: January 2014
2012 Sales: $2.098 billion
2011 Sales: $2.217 billion
Change: (5%)
Micardis – FiercePharma http://www.fiercepharma.com/special-reports/micardis#ixzz2UADpDZeO
Micardis® (telmisartan) tablets are a prescription medicine used to treat high blood pressure (hypertension). Additionally, MICARDIS 80 mg tablets are used in certain high-risk people aged 55 years and older who are unable to take a medicine called an angiotensin converting enzyme inhibitor (ACE-I) to help lower their risk of having certain cardiovascular problems such as stroke, heart attack, or death.
Micardis® (telmisartan) tablets are a prescription medicine used to treat high blood pressure (hypertension).
Telmisartan (INN) (pron.: /tɛlmɪˈsɑrtən/) is an angiotensin II receptor antagonist (angiotensin receptor blocker, ARB) used in the management of hypertension. It is marketed under thetrade name Micardis (by Boehringer Ingelheim), among others.
Telmisartan is an angiotensin II receptor blocker that shows high affinity for the angiotensin II receptor type 1 (AT1), with a binding affinity 3000 times greater for AT1 than AT2. It has the longest half-life of any ARB (24 hours)[1][4] and the largest volume of distribution.
In addition to blocking the RAs, telmisartan acts as a selective modulator of peroxisome proliferator-activated receptor gamma (PPAR-γ), a central regulator of insulin and glucose metabolism. It is believed that telmisartan’s dual mode of action may provide protective benefits against the vascular and renal damage caused by diabetes and cardiovascular disease (CVD).[4]
Telmisartan’s activity at the PPAR-γ receptor has prompted speculation around its potential as a sport doping agent as an alternative to GW 501516.[5] Telmisartan activates PPARδ receptors in several tissues. [6][7][8][9]
7 Avapro
Avapro (Sanofi)
Patent expiry: March 2012
Total 2012 sales: $1.925 billion
2012 sales Sanofi: $1.422 billion
2012 sales BMS: $503 million
Total 2011 sales: $2.749 billion
2011 sales Sanofi: $1.797 billion
2011 sales BMS: $952 million
Total Change: (30%)
Avapro – FiercePharma http://www.fiercepharma.com/special-reports/avapro#ixzz2UAE9iB2E
rbesartan (INN) (pron.: /ɜrbəˈsɑrtən/) is an angiotensin II receptor antagonist used mainly for the treatment of hypertension. Irbesartan was developed by Sanofi Research (now part ofsanofi-aventis). It is jointly marketed by sanofi-aventis and Bristol-Myers Squibb under the trade names Aprovel, Karvea, and Avapro.
As with all angiotensin II receptor antagonists, irbesartan is indicated for the treatment ofhypertension. Irbesartan may also delay progression of diabetic nephropathy and is also indicated for the reduction of renal disease progression in patients with type 2 diabetes,[1]hypertension and microalbuminuria (>30 mg/24 hours) or proteinuria (>900 mg/24 hours).[2]
A large randomized trial following 4100+ men and women with heart failure and normal ejection fraction (>=45%) over 4+ years found no improvement in study outcomes or survival with irbesartan as compared to placebo.[3]
8 Vytorin
Vytorin (Merck)
Patent Expiry: April 2017
2012 sales: $1.747 billion
2011 sales: $1.882 billion
Change: (7%)
Vytorin – FiercePharma http://www.fiercepharma.com/special-reports/vytorin#ixzz2UAEQVcQr
Ezetimibe/simvastatin (pron.: /ɛˈzɛtɨmɪb ˌsɪmvəˈstætɨn/) is a drug combination used for the treatment of dyslipidemia. It is a combination of ezetimibe (best known as Zetia in the United States and Ezetrol elsewhere) and the statin drug simvastatin (best known as Zocor in the U.S.). The combination preparation is marketed by Merck & Co./Schering-PloughPharmaceuticals (joint venture) under the trade names Vytorin and Inegy.
Ezetimibe reduces blood cholesterol by inhibiting absorption of cholesterol by the small intestine by acting at the brush border of the small intestine and inhibits the absorption of cholesterol, leading to a decrease in the delivery of intestinal cholesterol to the liver.
Simvastatin is an HMG-CoA reductase inhibitor or statin. It works by blocking an enzymethat is necessary for the body to make cholesterol.
Even though ezetimibe decreases cholesterol levels, as of 2009 it has not been found to lead to improvement in real world outcomes.[1] The combination of simvastatin and ezetimibe has not been found to be any better than simvastatin alone. A panel of experts thus concluded in 2008 that it should “only be used as a last resort”.[2]
9 Blopress
Blopress (Takeda Pharmaceutical)
Patent expiry: June 2012
2012 sales: $1.643 billion
2011 sales: $1.808 billion
Change: (9%)
Blopress – FiercePharma http://www.fiercepharma.com/special-reports/blopress#ixzz2UAEnxyWy
Candesartan (rINN) (pron.: /ˌkændɨˈsɑrtən/) is an angiotensin II receptor antagonist used mainly for the treatment of hypertension. The prodrug candesartan cilexetil is marketed by AstraZeneca and Takeda Pharmaceuticals, commonly under the trade names Blopress,Atacand, Amias, and Ratacand
As all angiotensin II receptor antagonists, candesartan is indicated for the treatment of hypertension. Results from the CHARM study in the early 2000s demonstrated the morbidity and mortality reduction benefits of candesartan therapy in congestive heart failure.[1] Thus, while ACE inhibitors are still considered first-line therapy in heart failure, candesartan can be used in combination with an ACE to achieve improved mortality and morbidity vs. an ACE alone and additionally is an alternative in patients intolerant of ACE inhibitor therapy.
Prehypertension
In a four-year randomized controlled trial, candesartan was compared to placebo to see whether it could prevent or postpone the development of full-blown hypertension in people with so-called prehypertension. During the first two years of the trial, half of participants were given candesartan, and the others received placebo; candesartan reduced the risk of developing hypertension by nearly two-thirds during this period. In the last two years of the study, all participants were switched to placebo. By the end of the study, candesartan hadsignificantly reduced the risk of hypertension, by more than 15%. Serious side effects were actually more common among participants receiving placebo than in those given candesartan.[2]
Candesartan is also available in a combination formulation with a low dose thiazide diuretic, invariably hydrochlorothiazide, to achieve an additive antihypertensive effect. Candesartan/hydrochlorothiazide combination preparations are marketed under various trade names including Atacand HCT, Hytacand, Blopress Plus, Advantec and Ratacand Plus.
10 Tracleer
Tracleer (Actelion)
Patent expiry: November 2015
2012 sales: $1.600 billion
2011 sales: $1.721 billion
Change: (7%)
Tracleer – FiercePharma http://www.fiercepharma.com/special-reports/tracleer#ixzz2UAF2iIJB
Bosentan is a dual endothelin receptor antagonist used in the treatment of pulmonary artery hypertension (PAH). It is licensed in the United States, the European Union and other countries by Actelion Pharmaceuticals for the management of PAH under the trade name Tracleer.
Bosentan is a competitive antagonist of endothelin-1 at the endothelin-A (ET-A) and endothelin-B (ET-B) receptors. Under normal conditions, endothelin-1 binding of ET-A or ET-B receptors causes pulmonary vasoconstriction. By blocking this interaction, bosentan decreases pulmonary vascular resistance. Bosentan has a slightly higher affinity for ET-A than ET-B.
Clinical uses
Bosentan is indicated mainly for the treatment of pulmonary hypertension. In 2007, bosentan was approved in the European Union also for reducing the number of new digital ulcers in patients with systemic sclerosis and ongoing digital ulcer disease.
In the United States, bosentan is indicated for the treatment of pulmonary arterial hypertension (WHO Group I) in patients with WHO Class II-IV symptoms, to improve exercise capacity and decrease the rate of clinical worsening.[1]
http://www.fiercepharma.com/special-reports/top-10-cardio-drugs-2012
For years, cardio was king. The world’s all-time best-selling drug, Pfizer’s ($PFE) Lipitor, after all, is an antihyperlipidemic drug. Cardio drugs have traditionally made up one of the largest categories of therapeutic treatment in the drug universe.
According to EvaluatePharma‘s World Preview 2018 report, combined sales of antihypertensive drugs and antihyperlipidemics were more than $70 billion in 2011. That would put them at the top of the heap. Sales of antihypertensive drugs alone were more than $40 billion that year, making them the second-largest therapy area defined by the report, behind oncology drugs at $64.4 billion. The list, compiled by EvaluatePharma, includes the theraputic areas categorized as cardio, so it does not include some products sometimes used for heart disease but not in that therapeutic area, including blood thinners like Plavix.
But many of the top cardio drugs are long in the tooth, and generics are now eating their lunch. Did I mention Lipitor? Sales cratered last year, falling nearly 60%. Despite that, the drug placed third among the top 10 cardio drugs of 2012, a reminder of the stature it had achieved. Four of the top 10 have lost patent protection in the last two years, and most will be off patent by 2016, with only Merck’s ($MRK) Vytorin protected until 2017.
Last year, the top 10 cardio drugs racked up sales of $28.644 billion, down 23% from the $37.271 billion they sold in 2011. Still, the group has made a lot of money for its companies for years and, in some cases, completely changed the treatment of heart disease.
It is an interesting list. Only Merck has two drugs in the top 10. The other drugmakers make up a broad swath of the pharma industry. Read our report below, and if you have some insights you would like to share, please do.
Part IV:
20 Highest-Paid Biopharma CEOs of 2012
May 20, 2013
-
1
-
2
-
3
-
4
-
5
-
6
-
7
-
8
-
9
-
10
-
11
-
12
-
13
-
14
-
15
-
16
-
17
-
18
-
19
-
20
http://www.fiercepharma.com/special-reports/20-highest-paid-biopharma-ceos-2012#ixzz2UAGLd93d
 Call it a rite of spring. Every year about this time, FiercePharma takes a look at executive compensation in the industry, and we rank the highest-paid CEOs. If you’re a regular reader, you’ll notice that this year’s list is longer than previous editions. And there’s a reason for that: curiosity.
Call it a rite of spring. Every year about this time, FiercePharma takes a look at executive compensation in the industry, and we rank the highest-paid CEOs. If you’re a regular reader, you’ll notice that this year’s list is longer than previous editions. And there’s a reason for that: curiosity.
As we were beginning to gather numbers from biopharma companies’ proxy statements and annual reports, news surfaced that Valeant Pharmaceuticals ($VRX) and Actavis ($ACT) had been in merger talks. The former CEO of Mylan ($MYL), one of Actavis’ rivals, regularly appeared on our highest-paid executives list, so we looked up the numbers on Actavis. No dice; CEO Paul Bisaro may have pulled off his biggest merger ever last year, but $8.66 million in compensation still didn’t qualify him for our ranking.
Then, we pulled out Valeant’s proxy statement. And while CEO Michael Pearson didn’t earn enough in 2012 to make the cutoff–his compensation just surpassed $6 million–he should have been at the top of the list last year. Pearson’s 2011 pay package broke $36 million. He collected more than $18 million in stock and option awards, plus a special $13.7 million dividend payment, stemming from agreements negotiated years before.
We hate to miss a scoop. Naturally. So, we vowed to avoid making the same mistake this time around. Rather than limit our executive-pay search to the biggest pharma companies and biotechs, plus the usual suspects who often make CEO-pay rankings, we used a bigger net. We collected compensation information from 50 companies, including numbers for CEOs, CFOs, R&D chiefs and other top executives.
Partly because of this search, but mostly because of big bonuses and awards at fast-growing Regeneron ($REGN), we have a brand-new No. 1 on our list. That’s Regeneron CEO Leonard Schleifer, whose 2012 compensation totaled $30.047 million. You’ll notice some other newbies, such as Leonard Bell from Alexion ($ALXN), whose pay bump put him in 12th place. And then there are familiar faces, such as Pfizer ($PFE) CEO Ian Read; Johnson & Johnson’s ($JNJ) former chairman and CEO, William Weldon; and Eli Lilly ($LLY) CEO John Lechleiter, who hung on in 10th place.
Many of the companies we researched pay their top people far less than the $10 million that served as our cutoff figure. Novo Nordisk ($NVO) CEO Lars Sorensen, who has presided over double-digit growth there for several years, collected a package of cash and stock awards worth about $5 million for 2012. GlaxoSmithKline ($GSK) CEO Andrew Witty made less than $6 million himself; he took a pay cut for the year because of Glaxo’s shortfall on certain performance targets.
And then there are others who would have made the list, had their titles been different. There’s Regeneron R&D chief George Yancopoulos, whose extraordinary $81 million in compensation shows how much the company appreciates its newly minted blockbuster, Eylea. There’s Mylan Chairman Robert Coury, who used to be a fixture on our list until Heather Bresch took over as CEO; he made more than $28 million last year. Novartis’ ($NVS) former chairman Daniel Vasella could have qualified for 12th place with his $13.98 million in compensation.
Vasella, then, gives us a quick segue to the ongoing debate over executive pay. In Switzerland, populist dismay at some high-profile compensation figures led to a public vote earlier this year. Citizens voted in new restrictions on common bonuses, such as golden parachutes, and gave shareholders a binding vote on executive pay. And local analysts figure that late-breaking news of Vasella’s behind-the-scenes noncompete agreement–worth some $78 million over 5 years–helped pay activists to get out the vote. (Vasella ended up refusing the deal, by the way.)
In the U.S., where executives are paid more than anywhere else in the world, shareholders at some companies have successfully lobbied for a greater emphasis on performance pay and against extraordinary bonuses, such as change-in-control payments that send top executives on their way with tens of millions after a merger. Other companies have instituted “say-on-pay” advisory votes for shareholders, but those often end up as rubber stamps for the status quo.
Now, we’re interested in what you have to say about executive compensation. Are the CEOs on this list worth their price? What’s a supersuccessful new drug worth? Should CEO pay be docked for R&D failures? What about failed launches? Should other, lower-paid executives earn more? Tweet your opinions to @FiercePharma using the hashtag #FPexecpay, leave your comments below or email us. We’ll collect your thoughts in a future article.
As always, feel free to send us your thoughts on our coverage. And if we missed a well-paid CEO, be sure to let us know.
— Tracy Staton (email | Twitter)
For more:
Top 10 Biotech CEO Pay Packages of 2012
Top 10 Pharma CEO salaries of 2010
Top 10 Pharma CEO salaries of 2009
2012’s 10 highest-paid Med Tech CEOs
Top 10 Medical Device Industry CEO Salaries for 2011
20 Highest-Paid Biopharma CEOs of 2012 – FiercePharma http://www.fiercepharma.com/special-reports/20-highest-paid-biopharma-ceos-2012#ixzz2UAGAlHay
REFERENCES FOR Part I: Arterial Stiffness
1. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L,
Ducimetiere P, Benetos A. Aortic stiffness is an independent predictor
of all-cause and cardiovascular mortality in hypertensive patients.
Hypertension. 2001;37:1236–1241.
2. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular
events and all-cause mortality with arterial stiffness: a systematic
review and meta-analysis. J Am Coll Cardiol. 2010;55:1318–1327.
3. Boutouyrie P, Tropeano AI, Asmar R, Gautier I, Benetos A, Lacolley P,
Laurent S. Aortic stiffness is an independent predictor of primary coronary
events in hypertensive patients: a longitudinal study. Hypertension.
4. Mattace-Raso FU, van der Cammen TJ, Hofman A, van Popele NM, Bos
ML, Schalekamp MA, Asmar R, Reneman RS, Hoeks AP, Breteler MM,
Witteman JC. Arterial stiffness and risk of coronary heart disease and
stroke: the Rotterdam Study. Circulation. 2006;113:657–663.
5. Sehestedt T, Jeppesen J, Hansen TW, Rasmussen S, Wachtell K, Ibsen H,
Torp-Pedersen C, Olsen MH. Risk stratification with the risk chart from
the European Society of Hypertension compared with SCORE in the general
population. J Hypertens. 2009;27:2351–2357.
6. Mitchell GF, Hwang SJ, Vasan RS, Larson MG, Pencina MJ,
Hamburg NM, Vita JA, Levy D, Benjamin EJ. Arterial stiffness and
cardiovascular events: the Framingham Heart Study. Circulation. 2010;
7. Gosse P, Cremer A, Papaioannou G, Yeim S. Arterial stiffness from monitoring
of timing of Korotkoff sounds predicts the occurrence of cardiovascular
events independently of left ventricular mass in hypertensive
patients. HYPERTENSIONAHA.113.01039 Published online before print May 20, 2013,doi: 10.1161/HYPERTENSIONAHA.113.01039
8. Gosse P, Guillo P, Ascher G, Clementy J. Assessment of arterial distensibility
by monitoring the timing of Korotkoff sounds. Am J Hypertens.
9. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C,
Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier
H; European Network for Non-invasive Investigation of Large Arteries.
Expert consensus document on arterial stiffness: methodological issues
and clinical applications. Eur Heart J. 2006;27:2588–2605.
10. Dogui A, Redheuil A, Lefort M, DeCesare A, Kachenoura N, Herment A,
Mousseaux E. Measurement of aortic arch pulse wave velocity in cardiovascular
MR: comparison of transit time estimators and description of a
new approach. J Magn Reson Imaging. 2011;33:1321–1329.
downloaded from
http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.01372.citation
REFERENCES for Part II: Clinical Trials of Hypertension Management
1. Hanselin MR , Saseen JJ , Allen RR , Marrs JC , Nair KV . Description of
antihypertensive use in patients with resistant hypertension prescribed
four or more agents. Hypertension . 2011 ; 58 : 1008 – 1013 .
2. Bakris GL , Lindholm LH , Black HR , Krum H , Linas S , Linseman JV ,
Arterburn S , Sager P , Weber M . Divergent results using clinic and ambulatory
blood pressures: report of a darusentan-resistant hypertension trial.
Hypertension . 2010 ; 56 : 824 – 830 .
3. Smithwick RH , Thompson JE . Splanchnicectomy for essential hypertension;
results in 1,266 cases. J Am Med Assoc . 1953 ; 152 : 1501 – 1504 .
4. Esler M , Ferrier C , Lambert G , Eisenhofer G , Cox H , Jennings G .
Biochemical evidence of sympathetic hyperactivity in human hypertension.
Hypertension . 1991 ; 17 ( 4 Suppl ): III29 – III35 .
5. Esler MD , Krum H , Sobotka PA , Schlaich MP , Schmieder RE , Bohm
M . Symplicity HTN-2 investigators. Renal sympathetic denervation in
patients with treatment-resistant hypertension: a randomized controlled
trial. Lancet 2010 ; 376 : 1903 – 1909 .
6. Brinkmann J , Heusser K , Schmidt BM , Menne J , Klein G , Bauersachs J ,
Haller H , Sweep FC , Diedrich A , Jordan J , Tank J . Catheter-based renal
nerve ablation and centrally generated sympathetic activity in diffi cultto-
control hypertensive patients: prospective case series. Hypertension .
2012 ; 60 : 1485 – 1490 .
7. Mahfoud F , Cremers B , Janker J , et al . Renal hemodynamics and renal
function after catheter-based renal sympathetic denervation in patients
with resistant hypertension. Hypertension . 2012 ; 60 : 419 – 424 .
8. Lambert GW , Hering D , Esler MD , Marusic P , Lambert EA , Tanamas
SK , Shaw J , Krum H , Dixon JB , Barton DA , Schlaich MP . Health-related
quality of life after renal denervation in patients with treatment-resistant
hypertension. Hypertension . 2012 ; 60 : 1479 – 1484 .
9. Daugherty SL , Powers JD , Magid DJ , Masoudi FA , Margolis KL ,
O ’ Connor PJ , Schmittdiel JA , Ho PM . The association between medication
adherence and treatment intensifi cation with blood pressure control
in resistant hypertension. Hypertension . 2012 ; 60 : 303 – 309 .
10. Bobrie G , Frank M , Azizi M , Peyrard S , Boutouyrie P , Chatellier G ,
Laurent S , Menard J , Plouin PF . Sequential nephron blockade versus
sequential renin-angiotensin system blockade in resistant hypertension:
a prospective, randomized, open blinded endpoint study. J Hypertens .
2012 ; 30 : 1656 – 1664 .
11. Mancia G . Additional drug treatment in resistant hypertension: need for
randomized studies. J Hypertens . 2012 ; 30 : 1514 – 1515 .
12. Hermida RC , Ayala DE , Moj ó n A , Fontao MJ , Fern á ndez JR .
Chronotherapy with valsartan/hydrochlorothiazide combination in essential
hypertension: improved sleep-time blood pressure control with bedtime
dosing. Chronobiol Int . 2011 ; 28 : 601 – 610 .
13. Persu A , Renkin J , Thijs L , Staessen JA . Renal denervation: ultima
ratio or standard in treatment-resistant hypertension. Hypertension .
2012 ; 60 : 596 – 606 .
14. Lohmeier TE , Iliescu R . Chronic lowering of blood pressure by carotid
barorefl ex activation: mechanisms and potential for hypertension therapy.
Hypertension . 2011 ; 57 : 880 – 886 .
15. Bisognano JD , Bakris G , Nadim MK , Sanchez L , Kroon AA , Schafer J ,
de Leeuw PW , Sica DA . Barorefl ex activation therapy lowers blood pressure
in patients with resistant hypertension: results from the double-blind,
randomized, placebo-controlled rheos pivotal trial. J Am Coll Cardiol .
2011 ; 58 : 765 – 773 .
16. Parving HH , Brenner BM , McMurray JJ , de Zeeuw D , Haffner SM ,
Solomon SD , Chaturvedi N , Persson F , Desai AS , Nicolaides M , Richard
A , Xiang Z , Brunel P , Pfeffer MA ; ALTITUDE Investigators . Cardiorenal
end points in a trial of aliskiren for type 2 diabetes. N Engl J Med .
2012 ; 367 : 2204 – 2213 .
17. The ONTARGET Investigators . Telmisartan, ramipril, or both in patients
at high risk for vascular events. N Engl J Med . 2008 ; 358 : 1547 – 1559 .
18. Mancia G , Parati G , Bilo G , et al . Ambulatory blood pressure values in
the Ongoing Telmisartan Alone and in Combination with Ramipril Global
Endpoint Trial (ONTARGET). Hypertension . 2012 ; 60 : 1400 – 1406 .
19. Roush GC , Holford TR , Guddati AK . Chlorthalidone compared with
hydrochlorothiazide in reducing cardiovascular events: systematic review
and network meta-analyses. Hypertension . 2012 ; 59 : 1110 – 1117 .
20. Cushman WC , Bakris GL , White WB , Weber MA , Sica D , Roberts A ,
Lloyd E , Kupfer S . Azilsartan medoxomil plus chlorthalidone reduces
blood pressure more effectively than olmesartan plus hydrochlorothiazide
in stage 2 systolic hypertension. Hypertension . 2012 ; 60 : 310 – 318 .
21. Alderman MH , Piller LB , Ford CE , Probstfi eld JL , Oparil S , Cushman WC ,
Einhorn PT , Franklin SS , Papademetriou V , Ong ST , Eckfeldt JH , Furberg
CD , Calhoun DA , Davis BR ; Antihypertensive and Lipid-Lowering
Treatment to Prevent Heart Attack Trial Collaborative Research Group .
Clinical signifi cance of incident hypokalemia and hyperkalemia in treated
hypertensive patients in the antihypertensive and lipid-lowering treatment
to prevent heart attack trial. Hypertension . 2012 ; 59 : 926 – 933 .
22. Kostis WJ , Thijs L , Richart T , Kostis JB , Staessen JA . Persistence of mortality
reduction after the end of randomized therapy in clinical trials of
blood pressure-lowering medications. Hypertension . 2010 ; 56 : 1060 – 1068 .
23. van Onzenoort HA , Menger FE , Neef C , Verberk WJ , Kroon AA , de
Leeuw PW , van der Kuy PH . Participation in a clinical trial enhances
adherence and persistence to treatment: a retrospective cohort study.
Hypertension . 2011 ; 58 : 573 – 578 .
24. Sever PS . The Anglo-Scandinavian Cardiac Outcomes Trial: implications
and further outcomes. Hypertension . 2012 ; 60 : 248 – 259 .
25. Larstorp AC , Ariansen I , Gjesdal K , Olsen MH , Ibsen H , Devereux RB ,
Okin PM , Dahl ö f B , Kjeldsen SE , Wachtell K . Association of pulse pressure
with new-onset atrial fi brillation in patients with hypertension and
left ventricular hypertrophy: the Losartan Intervention For Endpoint
(LIFE) reduction in hypertension study. Hypertension . 2012 ; 60 : 347 – 353 .
26. Rossignol P , Cridlig J , Lehert P , Kessler M , Zannad F . Visit-to-visit blood
pressure variability is a strong predictor of cardiovascular events in hemodialysis:
insights from FOSIDIAL. Hypertension . 2012 ; 60 : 339 – 346 .
27. Matsui Y , O ’ Rourke MF , Hoshide S , Ishikawa J , Shimada K , Kario
K . Combined Effect of Angiotensin II Receptor Blocker and Either a
Calcium Channel Blocker or Diuretic on Day-by-Day Variability of Home
Blood Pressure: The Japan Combined Treatment With Olmesartan and a
Calcium-Channel Blocker Versus Olmesartan and Diuretics Randomized
Effi cacy Study. Hypertension . 2012 ; 59 : 1132 – 1138 .
28. Jennings GL , Sudhir K . Initial therapy of primary hypertension. Med J
Aust . 1990 ; 152 : 198 – 203 .
29. Egan BM , Bandyopadhyay D , Shaftman SR , Wagner CS , Zhao Y ,
Yu-Isenberg KS . Initial monotherapy and combination therapy and hypertension
control the fi rst year. Hypertension . 2012 ; 59 : 1124 – 1131 .
30. Bavry AA , Pepine CJ . Treatment of hypertension: lower is better, or is it?
Hypertension . 2012 ; 60 : 281 – 282 .
31. Mizuno R , Fujimoto S , Saito Y , Okamoto Y . Optimal antihypertensive
level for improvement of coronary microvascular dysfunction: the lower,
the better? Hypertension . 2012 ; 60 : 326 – 332 .
32. Roman MJ , Howard BV , Howard WJ , Mete M , Fleg JL , Lee ET ,
Devereux RB . Differential impacts of blood pressure and lipid lowering
on regression of ventricular and arterial mass: the Stop Atherosclerosis in
Native Diabetics Trial. Hypertension . 2011 ; 58 : 367 – 371 .
33. Bertoia ML , Waring ME , Gupta PS , Roberts MB , Eaton CB . Implications
of new hypertension guidelines in the United States. Hypertension .
2012 ; 60 : 639 – 644 .
34. Stewart S , Carrington MJ , Swemmer CH , et al .; VIPER-BP Study
Investigators . Effect of intensive structured care on individual blood pressure
targets in primary care: multicentre randomised controlled trial. BMJ .
2012 ; 345 : e7156 .
35. Dickinson BD , Havas S ; Council on Science and Public Health, American
Medical Association . Reducing the population burden of cardiovascular
disease by reducing sodium intake: a report of the Council on Science and
Public Health. Arch Intern Med . 2007 ; 167 : 1460 – 1468 .
36. O ’ Donnell MJ , Yusuf S , Mente A , Gao P , Mann JF , Teo K , McQueen M ,
Sleight P , Sharma AM , Dans A , Probstfi eld J , Schmieder RE . Urinary
sodium and potassium excretion and risk of cardiovascular events. JAMA .
2011 ; 306 : 2229 – 2238 .
37. Hummel SL , Seymour EM , Brook RD , Kolias TJ , Sheth SS , Rosenblum
HR , Wells JM , Weder AB . Low-sodium dietary approaches to stop
hypertension diet reduces blood pressure, arterial stiffness, and oxidative
stress in hypertensive heart failure with preserved ejection fraction.
Hypertension . 2012 ; 60 : 1200 – 1206 .
38. Soedamah-Muthu SS , Verberne LD , Ding EL , Engberink MF , Geleijnse JM .
Dairy consumption and incidence of hypertension: a dose-response metaanalysis
of prospective cohort studies. Hypertension . 2012 ; 60 : 1131 – 1137 .
39. West SG , Gebauer SK , Kay CD , Bagshaw DM , Savastano DM ,
Diefenbach C , Kris-Etherton PM . Diets containing pistachios reduce systolic
blood pressure and peripheral vascular responses to stress in adults
with dyslipidemia. Hypertension . 2012 ; 60 : 58 – 63 .
40. Zhang X , Qi Q , Liang J , Hu FB , Sacks FM , Qi L . Neuropeptide Y promoter
polymorphism modifi es effects of a weight-loss diet on 2-year
changes of blood pressure: the preventing overweight using novel dietary
strategies trial. Hypertension . 2012 ; 60 : 1169 – 1175 .
41. Meredith IT , Friberg P , Jennings GL , Dewar EM , Fazio VA , Lambert GW ,
Esler MD . Exercise training lowers resting renal but not cardiac sympathetic
activity in humans. Hypertension . 1991 ; 18 : 575 – 582 .
42. Cornelissen VA , Fagard RH , Coeckelberghs E , Vanhees L . Impact of resistance
training on blood pressure and other cardiovascular risk factors: a metaanalysis
of randomized, controlled trials. Hypertension . 2011 ; 58 : 950 – 958 .
Downloaded from
http://hyper.ahajournals.org/content/early/2013/05/20/HYPERTENSIONAHA.113.00863.citation
RELATED SOURCES:
Aortic pulse pressure is associated with the localization of coronary artery disease based on coronary flow lateralization. American journal of hypertension, 25(10), 1055-1063.
- Georges Khoueiry1,
- Basem Azab2,
- Estelle Torbey2,
- Nidal Abi Rafeh1,
- Jean-Paul Atallah2,
- Kathleen Ahern2,
- James Malpeso1,
- Donald McCord1 and
- Elie R. Chemaly3⇓
Author Affiliations
1Department of Cardiology, Staten Island University Hospital, Staten Island, New York, USA
2Department of Internal Medicine, Staten Island University Hospital, Staten Island, New York, USA
3Cardiovascular Institute, Mount Sinai School of Medicine, New York, New York, USA
Elie R. Chemaly (elie.chemaly@mssm.edu)
Abstract
Background Aortic pulse pressure (APP) is related to arterial stiffness and associated with the presence and extent of coronary artery disease (CAD). Besides, the left coronary artery (LCA) has a predominantly diastolic flow while the right coronary artery (RCA) receives systolic and diastolic flow. Thus, we hypothesized that increased systolic–diastolic pressure difference had a greater atherogenic effect on the RCA than on the LCA.
Methods A random sample of 433 CAD patients (145 females, 288 males, mean age 65.0 ± 11.1 years) undergoing coronary angiography at Staten Island University Hospital between January 2005 and May 2008 was studied. Coronary lesion was defined as a ≥50% luminal stenosis. Patients were divided into three groups, with isolated LCA lesions (n = 154), isolated RCA lesions (n = 36) or mixed LCA and RCA lesions (n = 243).
Results APP differed significantly between groups, being highest when the RCA alone was affected (67.6 ± 20.3 mm Hg for LCA vs. 78.8 ± 22.0 for RCA vs. 72.7 ± 22.6 for mixed, P = 0.008 for analysis of variance (ANOVA)). Age and gender were not associated with CAD location. Heart rate was associated with CAD location, lowest in RCA group, and negatively correlated with APP. However, left ventricular ejection fraction (LVEF) was lower in the mixed CAD group and positively correlated with APP. The association between APP and right-sided CAD persisted in multivariate logistic regression adjusting for confounders, including heart rate, LVEF and medication use. A similar but less significant pattern was seen with brachial arterial pressures.
Conclusions Aortic pulse pressure may affect CAD along with coronary flow phasic patterns.
American Journal of Hypertension, advance online publication 28 June 2012; doi:10.1038/ajh.2012.87
The Relationship Between Diastolic Pressure and Coronary Collateral Circulation in Patients With Stable Angina Pectoris and Chronic Total Occlusion. Am J Hypertens (2013)doi: 10.1093/ajh/hps096
First published online: February 7, 2013
- 1 The Cardiovascular Medical Department of the General Hospital of the Chinese People’s Liberation Army, Beijing, China;
2 The Cardiovascular Medical Department of the Affiliated Hospital of the Chinese People’s Armed Police Logistics College, Tianjin, China.
- ↵Correspondence: Chen Yun Dai (chenyundai2002@163.com).
Abstract
BACKGROUND The most important biomechanical source of activation of the coronary collateral circulation (CCC) is increased tangential fluid shear stress at the arterial endothelial surface. The coronary circulation is unique in that most coronary blood flow occurs in diastole. Consequently, the diastolic blood pressure (DBP) may influence the tangential fluid shear stress on the arterial endothelial surface in diastole, therebyaffecting development of the CCC.
METHODS To investigate this, we conducted a study of 222 patients with stable angina pectoris and chronic total occlusion of coronary arteries. All of the patients had no history of coronary artery interventional therapy, coronary artery bypass surgery, cardiomyopathy, or congenital heart disease. The extent of the collateral vasculature of the area perfused by the artery affected by chronic total occlusion was graded as poor or well-developed according to Rentrop’s classification.
RESULTS Univariate analysis showed a significant difference between the study subgroup with poorly developed collaterals and that with well-developed collaterals in terms of high diastolic blood pressure (DBP) and mean DBP. Multivariate analysis revealed high DBP as the only independent positive predictor of a well-developed collateral circulation.
CONCLUSIONS High DBP is positively related to a well-developed CCC. Differences in development of the CCC may be one of the pathophysiologic mechanisms responsible for the J-curve phenomenon in the relationship between DBP and cardiovascular risk.
http://ajh.oxfordjournals.org/content/early/2013/02/06/ajh.hps096.abstract
Other related articles that were published on this Open Access Online Scientific Journal, include the following:
Synthetic Biology: On Advanced Genome Interpretation for Gene Variants and Pathways: What is the Genetic Base of Atherosclerosis and Loss of Arterial Elasticity with Aging
Aviva Lev-Ari, PhD, RN May 17, 2013
Artherogenesis: Predictor of CVD – the Smaller and Denser LDL Particles
Aviva Lev-Ari, PhD, RN 11/15/2012
Cardiovascular Diseases: Causes, Risks and Management, Volume Two, Risks of Cardiovascular Diseases
Justin D. Pearlman MD ME PhD MA FACC, Editor
Genetics of Conduction Disease: Atrioventricular (AV) Conduction Disease (block): Gene Mutations – Transcription, Excitability, and Energy Homeostasis
Aviva Lev-Ari, PhD, RN 4/28/2013
Genomics & Genetics of Cardiovascular Disease Diagnoses: A Literature Survey of AHA’s Circulation Cardiovascular Genetics, 3/2010 – 3/2013
Aviva Lev-Ari, PhD, RN and Larry H. Bernstein, MD, FCAP 3/7/2013
Hypertriglyceridemia concurrent Hyperlipidemia: Vertical Density Gradient Ultracentrifugation a Better Test to Prevent Undertreatment of High-Risk Cardiac Patients
Aviva Lev-Ari, PhD, RN 4/4/2013
Hypertension and Vascular Compliance: 2013 Thought Frontier – An Arterial Elasticity Focus
Justin D. Pearlman, MD, PhD and Aviva Lev-Ari, PhD, RN 5/11/2013
Prediction of Occurrence of Cardiovascular Events Independently of Left Ventricular Mass in Hypertensive Patients: Monitoring of Timing of Korotkoff Sounds as Indicator of Arterial Stiffness
Posted in Atherogenic Processes & Pathology, Frontiers in Cardiology and Cardiovascular Disorders, HTN, Origins of Cardiovascular Disease, tagged American Heart Association, Antihypertensive drug, Arterial stiffness, Blood pressure, Cardiovascular disease, Hypertension on May 20, 2013| 1 Comment »
Reporter: Aviva Lev-Ari, PhD, RN
- Original Article
HYPERTENSIONAHA.113.01039 Published online before print May 20, 2013,doi: 10.1161/HYPERTENSIONAHA.113.01039
Arterial Stiffness From Monitoring of Timing of Korotkoff Sounds Predicts the Occurrence of Cardiovascular Events Independently of Left Ventricular Mass in Hypertensive Patients
+Author Affiliations
From the Department of Cardiology and Hypertension, University Hospital of Bordeaux, Bordeaux, France.
- Correspondence to Philippe Gosse, Department of Cardiology and Hypertension, University Hospital of Bordeaux, Hopital Saint Andre, 1 Rue Jean Burguet, 33075 Bordeaux, France. E-mail philippe.gosse@chu-bordeaux.fr
Abstract
Several studies have established that the increase in arterial stiffness (AS) is a cardiovascular risk factor but to date no studies have evaluated in hypertensive patients its prognostic value in comparison with another powerful risk factor, left ventricular mass (LVM) as measured by echocardiography. We prospectively evaluated the prognostic value of AS and LVM in patients with essential hypertension. The population studied comprised 793 patients (56% men) aged 54±14 years. For 519 patients, baseline measurements were made before any antihypertensive treatment, for 274 patients, the measurement were obtained during the follow-up period under antihypertensive treatment. AS was assessed from ambulatory monitoring of blood pressure and timing of Korottkoff sounds. Left ventricular mass was measured in 523 patients. After a mean follow-up of 97 months, 122 cardiovascular events were recorded in the whole population and 74 in the group with LVM determination. AS as continuous or discontinuous variable was independently related to cardiovascular events. The existence or not of antihypertensive treatment at the time of its measurement did not affect its prognostic value. When LVM was forced in the model, AS remained significantly related to cardiovascular events. Thus, AS has an independent prognostic value in the hypertensive, whether measured before or after the administration of antihypertensive treatment. This prognostic value persists after taking LVM into account.
Key Words:
- Received January 10, 2013.
- Revision received March 25, 2013.
- Accepted April 22, 2013.
- © 2013 American Heart Association, Inc.
Hypertension and Vascular Compliance: 2013 Thought Frontier – An Arterial Elasticity Focus
Posted in Atherogenic Processes & Pathology, Bio Instrumentation in Experimental Life Sciences Research, Frontiers in Cardiology and Cardiovascular Disorders, HTN, Origins of Cardiovascular Disease, Pharmacotherapy of Cardiovascular Disease, tagged Antihypertensive drug, Artery, Aviva Lev-Ari, Barcelona, Blood pressure, Cardiovascular disease, Cardiovascular Disorders, Circulatory system, Conditions and Diseases, health, Hypertension, Justin D. Pearlman, Lancet, Nitrovasodilator, Oslo, Systolic Hypertension, Tel Aviv University, vasodilation on May 11, 2013| 11 Comments »
Pros and Cons of Drug Stabilizers for Arterial Elasticity as an Alternative or Adjunct to Diuretics and Vasodilators in the Management of Hypertension.
Author, and Content Consultant to e-SERIES A: Cardiovascular Diseases: Justin Pearlman, MD, PhD, FACC
and
Article Curator: Aviva Lev-Ari, PhD, RN
This article presents the 2013 Thought Frontier on Hypertension and Vascular Compliance.
Conceptual development of the subject is presented in the following nine parts:
1. Physiology of Circulation and Role of Arterial Elasticity
2. Isolated Systolic Hypertension caused by Arterial Stiffening may be inadequately treated by Diuretics or Vasodilatation Antihypertensive Medications
3. Physiology of Circulation and Compensatory Mechanism of Arterial Elasticity
4. Vascular Compliance – The Potential for Novel Therapies
- Novel Mechanism for Disease Etiology: Modulation of Nuclear and Cytoskeletal Actin Polymerization.
- Genetic Therapy targeting Vascular Conductivity
- Regenerative Medicine for Vasculature Function Protection
5. In addition to curtailing high pressures, stabilizing BP variability is a potential target for management of hypertension
6. Mathematical Modeling: Arterial stiffening explains much of primary hypertension
7. Classification of Blood Pressure and Hypertensive Treatment Best Practice of Care in the US
8. Genetic Risk for High Blood Pressure
9. Is it Hypertension or Physical Inactivity: Cardiovascular Risk and Mortality – New results in 3/2013.
Summary By Justin D. Pearlman MD ME PhD MA FACC
1. Physiology of Circulation and Role of Arterial Elasticity
- Simplistically, high blood pressure stems from too much volume (salt water) for the vascular space, or conversely, too little space for the volume. Biological signals, such as endothelin, hypoxia, acidosis, nitric oxide, can modify vascular volume by constricting muscles in blood vessel walls. Less simplistically the physics of circulation are governed by numerous factors, with essentials detailed below.
- The vascular space has two major circuits: pulmonary (lungs) and systemic (body).
- Compliance (C) relates change in volume (ΔV) to change in pressure (ΔP) as a measure of the strength of elasticity, where elasticity summarizes the intrinsic forces that return to original shape after deformation: C = ΔV/ΔP . Those values can be estimated by ultrasound imaging with Doppler blood velocity estimation, by MRI, or invasively. Related properties can also be measured, such as wave propagation time or fractional flow reserve.
- The vascular system is dynamic, with frequency components and reactive elements. The fundamental frequency is governed by the heart rate delivering a stroke volume forward into the vasculature; a heart rate of 60/minute corresponds to the frequency of 1 Hertz (1 cycle/second). The pressure rise due to the ejection of stroke volume is called the pulse pressure.
- Numerous factors affect blood flow, including blood composition (affected by anemia or blood dilution), leakiness of vessels, elasticity, wave propagation, streamlines, viscosity, osmotic pressure (affected by protein deficiency and other factors),
- In a static system, the driving force relates linearly flow by way of resistance (R in units of dyn·s·cm−5): V=IR (Ohm’s law).
- Pulmonary:

- Systemic:

- Pulmonary:
- In a dynamic, reactive system, the relation between the driving potential (pressure gradient), and current (blood flow) is governed by a differential equation. However, use of complex numbers and exponentials recovers simplicity similar to Ohm’s law:
- Variables take the form
 , where t is time, s is a complex parameter, and A is a complex scalar. Complex values simply mean two dimensional, e.g., magnitude (as in resistance) plus phase shift (to account for reactive components).
, where t is time, s is a complex parameter, and A is a complex scalar. Complex values simply mean two dimensional, e.g., magnitude (as in resistance) plus phase shift (to account for reactive components). - Complex version of Ohm’s law:
 where V and I are the complex scalars in the voltage and current respectively and Z is the complex impedance.
where V and I are the complex scalars in the voltage and current respectively and Z is the complex impedance. - Frequency dependent “resistance” is captured by the term impedance.
- Variables take the form
- Breathing in increases the return of blood to the heart, adding to pulse variation.
- Dynamic elastance (Eadyn) relates volume variation (VVS) to pressure variation (PPV): Eadyn=PPV/SVV
- PPV(%) = 100% × (PPmax − PPmin)/[(PPmax + PPmin)/2)]
- where PPmax and PPmin are the maximum and minimum pulse pressures determined during a single respiratory cycle
- SVV(%) = 100% × [(SVmax − SVmin)/SVmean]
- where SVmax and SVmin are the maximum and minimum standard deviation of arterial pressure about the mean arterial pressure during a single respiratory cycle
- PPV(%) = 100% × (PPmax − PPmin)/[(PPmax + PPmin)/2)]
- The nervous system provides both stimulants and inhibitors (sympathetic and vagal nerves) to regulate blood vessel wall muscle tone and also heart rate. Many medications, and anesthetic agents in particular, reduce those responses to stimuli, so the vessels dilate, vascular impedance lowers, pressures drop, and autoregulation is impaired.
- Diuretics aim to decrease volume of circulating fluid, vasodilators aim to increase the vascular space, and elasticity treatments will aim to preserve or improve the ability to accommodate changes in volume of fluid.
- Vessel dilation near the skin promotes heat loss.
- Vascular elasticity is impaired by atherosclerosis, menopause, and endothelial dysfunction (impaired nitric oxide signals response, impaired endothelin response).
- Elastance in a cyclic pressure system of systole-diastole (contraction-dilation) presents impedance as a pulsatile load on the heart. Inotropy describes the generation of pressure by cardiac contraction, lusiotropy the compliance of the heart to accept filling with minimal back pressure to the lungs. Chronic exposure to elevated vascular impedance leads to impairment of lusiotropy (diastolic failure, stiff heart) and inotropy (systolic failure, weak heart).
2. Isolated Systolic Hypertension caused by Arterial Stiffening may be inadequately treated by Diuretics or Vasodilatation Antihypertensive Medications
- Stiff or “lead pipe” blood vessels drop pressure precipitously to dangerously low levels in response to diuretics.
- Stiff walls due to fibrosis or scar tissue have limited ability to dilate
- Red clover isoflavones improve vascular compliance loss from menopause.
- Fish oils may improve loss of vascular compliance from diabetes.
3. Physiology of Circulation and Compensatory Mechanism of Arterial Elasticity
Antihypertensive agents have focused on the following approaches:
-
Reduced volume (diuretics)
- Diuretics enhance renal excretion of sodium. Sodium is the major determinant of circulating volume. Too much blood volume for the amount of vascular space elevates blood pressure. Clinical trials show that use of diuretics to lower blood pressure can prevent strokes, non-inferior to vasodilators and recommended as first line agents.
- The most common prescriptions, a mild diuretic, hydrochlorothiazide (HCTZ), is known to improve blood vessel compliance by reducing cell turgor, which explains why its full onset of benefit as well as its slow offset when stopped can take more than one month.
- Chlorthalidone – Some evidence suggests that chlorthalidone may be superior to hydrochlorothiazide for the treatment of hypertension. However, a recent study concluded: chlorthalidone in older adults was not associated with fewer adverse cardiovascular events or deaths than hydrochlorothiazide. However, it was associated with a greater incidence of electrolyte abnormalities, particularly hypokalemia.
-
Increased vascular space (vasodilation)
- Alternatively, the pressure can be lowered by increasing the vascular space for a given vascular volume. Examples of mediators for arterial tone (degree of dilation) include nitric oxide, prostacyclin and endothelin.
|
Class |
Description |
| Hyperpolarization mediated (Calcium channel blocker) | Changes in the resting membrane potential of thecell affects the level of intracellular calciumthrough modulation of voltage sensitive calcium channelsin the plasma membrane. |
| cAMP mediated | Adrenergic stimulation results in elevated levelsof cAMP and protein kinase A, which results inincreasing calcium removal from the cytoplasm. |
| cGMP mediated (Nitrovasodilator) | Through stimulation of protein kinase G.Until 2002, the enzyme for this conversion wasdiscovered to be mitochondrial aldehyde dehydrogenase.Proc. Natl. Acad. Sci. USA 102 (34): 12159–12164. doi:10.1073/pnas.0503723102http://www.pnas.org/content/102/34/12159.long |
|
Class |
Example |
| Hyperpolarization mediated (Calcium channel blocker) | adenosineamlodipine (Norvasc),diltiazem (Cardizem,Dilacor XR) andnifedipine (Adalat, Procardia). |
| cAMP mediated | prostacyclin |
| cGMP mediated (Nitrovasodilator) | nitric oxide |
-
Reduced pulsatile force (beta blockers)
These work by blocking certain nerve and hormonal signals to the heart and blood vessels, thus lowering blood pressure. Frequently prescribed beta blockers include
- metoprolol (Lopressor, Toprol XL)
- carvedilol (Coreg)
- nadolol (Corgard)
- penbutolol (Levatol).
- Metabolized nebivolol increases vascular NO production, involves endothelial ß2-adrenergic receptor ligation, with a subsequent rise in endothelial free [Ca2+]i and endothelial NO synthase–dependent NO production
-
Angiotensin-converting enzyme (ACE) inhibitors
These allow blood vessels to widen by preventing the hormone angiotensin from affecting blood vessels. Frequently prescribed ACE inhibitors include captopril (Capoten), lisinopril (Prinivil, Zestril) and ramipril (Altace).
-
Angiotensin II receptor blockers
These help blood vessels relax by blocking the action of angiotensin. Frequently prescribed angiotensin II receptor blockers include losartan (Cozaar), olmesartan (Benicar) and valsartan (Diovan).
Another very commonly prescribed drug class of medication counteracts hardening of arteries.
Atheroma lipids have enzyme systems that explicitly disassemble cholesterol esters and reconstruct them inside blood vessel walls,e.g., Anacetrapib, Genetic variants that improve cholesterol levels are stimulating development of additional medications.
We can propose that atheroma build up in arterial blood vessel walls constitutes a maladaptive defense against aneurysm and risk of vessel rupture from hypertension.
Arguably, HMG-CoA reductase inhibitors, statin therapy is a second example of a medication that helps protect vascular elasticity, both by its lipid effects and its anti-inflammatory effects.
The best-selling statin is atorvastatin, marketed as Lipitor (manufactured by Pfizer) and Torvast. By 2003, atorvastatin became the best-selling pharmaceutical in history,[4] with Pfizer reporting sales of US$12.4 billion in 2008.[5] As of 2010, a number of statinsare on the market: atorvastatin (Lipitor and Torvast), fluvastatin (Lescol), lovastatin (Mevacor, Altocor, Altoprev), pitavastatin(Livalo, Pitava), pravastatin (Pravachol, Selektine, Lipostat), rosuvastatin (Crestor) and simvastatin (Zocor, Lipex).[6] Several combination preparations of a statin and another agent, such as ezetimibe/simvastatin, are also available.
References for Statins from:
http://en.wikipedia.org/wiki/Statin
Clinical Considerations of Statin Therapy’s manifold effects, in
Compensatory Effects in the Physiology of Circulation
Before declaring vessel elasticity a new and highly desirable treatment target, consider that it is not firmly established that hardening of arteries (loss of elasticity) is entirely maladaptive.
In parallel with any focus on increasing vascular elasticity or compliance, each of the issues discussed, below merits scrutiny and investigation.
Cardiac Circulation Dynamics
Endothelium morphology, rheological properties of intra vasculature fluid dynamics and blood viscosity provided explanation for shear stress of vessels under arterial pressure
and
Aging and Vasculature Diminished Elasticity
While among other reasons for Hypertension increasing prevalence with aging, arterial stiffening is one.
Yet, stiffer vessels are more efficient at transmitting pressure to distal targets. With aging, muscle mass diminishes markedly and the contribution to circulation from skeletal muscle tissue compressions combined with competent venous valves fades.
and
and
Aging and Myocardial Diminished Contractility and Ejection Fraction
With aging heart contractility diminishes. These issues can cause under perfusion of tissues, inadequate nutrient blood delivery (ischemia), lactic acidosis, tissue dysfunction and multi-organ failure. Hardened arteries may compensate. Thus, pharmacotherapy to increase Arterial Elasticity may be counterindicated for patients with mild to progressive CHF.
http://pharmaceuticalintelligence.com/2013/05/05/bioengineering-of-vascular-and-tissue-models/
and
and
http://pharmaceuticalintelligence.com/2012/10/17/chronic-heart-failure-personalized-medicine-two-gene-test-predicts-response-to-beta-blocker-bucindolol/
Our biosystems are highly interdependent, and we cannot leap to conclusions without careful thorough evidence. Increasing arterial elastance will lower vascular impedance and change the frequency components of our pulsatile perfusion system.
MOST comprehensive review of the Human Cardiac Conduction System presented to date:
Diminished contractility will increase the amount of energy needed to maintain circulation. It will change efficiency dramatically – consider the difference between periodically pushing someone sitting on a swing at the resonance frequency if the pendulum versus significantly off resonance.
http://pharmaceuticalintelligence.com/2013/04/14/mitochondrial-metabolism-and-cardiac-function/
and
Increased Arterial Elasticity – Potential Risk to Myocardium
The hypothesis that we should focus on cellular therapies to increase vascular compliance may decrease the circulation efficiency and result in worsening of cardiac right ventricular morphology and development of Dilated cardiomyopathy and hypertrophic cardiomyopathy (muscle thickening and diastolic failure), an undesirable outcome resulting from an attempt to treat the hypertension.
4. Vascular Compliance – The Potential of Noval Therapies
-
Novel Mechanism for Disease Etiology for the Cardiac Phenotype: Modulation of Nuclear and Cytoskeletal Actin Polymerization.
Lamin A/C and emerin regulate MKL1–SRF activity by modulating actin dynamics
Nature (2013) doi:10.1038/nature12105
Published online 05 May 2013
Affiliations
Cornell University, Weill Institute for Cell and Molecular Biology/Department of Biomedical Engineering, Ithaca, New York 14853, USA
Chin Yee Ho &
Jan Lammerding
Brigham and Women’s Hospital/Harvard Medical School, Department of Medicine, Boston 02115, Massachusetts, USA
Chin Yee Ho,
Diana E. Jaalouk &
Jan Lammerding
Institute of Biotechnology, University of Helsinki, 00014 Helsinki, Finland
Maria K. Vartiainen
Present address: American University of Beirut, Department of Biology, Beirut 1107 2020, Lebanon.
Diana E. Jaalouk
Contributions
C.Y.H., D.E.J. and J.L. conceived and designed the overall project, with valuable help from M.K.V. C.Y.H. and D.E.J. performed the experiments. C.Y.H., D.E.J. and J.L. analysed data. C.Y.H. and J.L. wrote the paper.
Corresponding author Jan Lammerding
Laminopathies, caused by mutations in the LMNA gene encoding the nuclear envelope proteins lamins A and C, represent a diverse group of diseases that include Emery–Dreifuss muscular dystrophy (EDMD), dilated cardiomyopathy (DCM), limb-girdle muscular dystrophy, and Hutchison–Gilford progeria syndrome1. Most LMNA mutations affect skeletal and cardiac muscle by mechanisms that remain incompletely understood. Loss of structural function and altered interaction of mutant lamins with (tissue-specific) transcription factors have been proposed to explain the tissue-specific phenotypes1. Here we report in mice that lamin-A/C-deficient (Lmna−/−) and LmnaN195K/N195K mutant cells have impaired nuclear translocation and downstream signalling of the mechanosensitive transcription factor megakaryoblastic leukaemia 1 (MKL1), a myocardin family member that is pivotal in cardiac development and function2. Altered nucleo-cytoplasmic shuttling of MKL1 was caused by altered actin dynamics in Lmna−/− and LmnaN195K/N195K mutant cells. Ectopic expression of the nuclear envelope protein emerin, which is mislocalized in Lmnamutant cells and also linked to EDMD and DCM, restored MKL1 nuclear translocation and rescued actin dynamics in mutant cells. These findings present a novel mechanism that could provide insight into the disease aetiology for the cardiac phenotype in many laminopathies, whereby lamin A/C and emerin regulate gene expression through modulation of nuclear and cytoskeletal actin polymerization.
http://www.nature.com/nature/journal/vaop/ncurrent/full/nature12105.html
-
Genetic Therapy to Conductivity Disease
-
Regenerative Medicine for Vasculature Function Protection
and
and
5. Stabilizing BP Variability is the next Big Target in Hypertension Management
Hypertension caused by Arterial Stiffening is Ineffectively Treated by Diuretics and Vasodilatation Antihypertensives
Barcelona, Spain – An aging population grappling with rising rates of hypertension and other cardiometabolic risk factors should prompt an overhaul of how hypertension is diagnosed and monitored and should spur development of drugs with entirely new mechanisms of action, one expert says. Speaking here at the 2013 International Conference on Prehypertension and Cardiometabolic Syndrome, meeting cochair Dr Reuven Zimlichman (Tel Aviv University, Israel) argued that the definitions of hypertension, as well as the risk-factor tables used to guide treatment, are no longer appropriate for a growing number of patients.
Most antihypertensives today work by producing vasodilation or decreasing blood volume and so are ineffective treatments in ISH patients. In the future, he predicts, “we will have to start looking for a totally different medication that will aim to improve or at least to stabilize arterial elasticity: medication that might affect factors that determine the stiffness of the arteries, like collagen, like fibroblasts. Those are not the aim of any group of antihypertensive medications today.”
Zimlichman believes existing databases could be used to develop algorithms that take this progression of disease into account, in order to better guide hypertension management. He also points out that new ambulatory blood-pressure-monitoring devices also measure arterial elasticity. “Unquestionably, these will improve our ability to diagnose both the status of the arteries and the changes of the arteries with time as a result of our treatment. So if we treat the patient and we see no improvement in arterial elasticity, or the patient is worse, something is wrong, something is not working—either the patient is not taking the medication, or our choice of medication is not appropriate, or the dose is insufficient, etc.”
http://www.theheart.org/article/1502067.do
Oslo, Norway – New research that is only just starting to be digested by the hypertension community indicates that visit-to-visit variability in blood-pressure readings will likely become another way of looking for “at-risk” hypertensive patients and in fact is likely to be more reliable as an indicator of cardiovascular risk than the currently used mean BP.
The Goal of Stabilizing BP variability
June 29, 2010 Lisa Nainggolan
Discussing the importance of this issue for guidelines and clinical practice, Dr Tony Heagerty (University of Manchester, UK) told the recent European Society of Hypertension (ESH) European Meeting on Hypertension 2010: “We are poking around in the dark, offering treatment blankly across a large community, and probably treating a lot of people who don’t need to be treated, while not necessarily treating the highest-risk patients. We should stop being reassured by ‘occasional’ normal BPs. The whole game now is, can we improve the identification of our ‘at-risk’ individuals?”
Heagerty was speaking at a special plenary session on late-breaking research discussing BP variability as a risk factor. This issue has emerged following new analyses reported at the ACC meeting and published in a number of papers in the Lancet and Lancet Neurology earlier this year, which showed that variability in blood pressure is a much stronger determinant of both stroke and coronary disease outcome than average blood pressure.
http://www.theheart.org/article/1093553.do
Three years later, 2/1/2013, Zimlichman also argued that definitions of essential and secondary hypertension have changed very little over the past few decades and have typically only been tweaked up or down related to other CV risk factors. Diastolic hypertension has been the primary goal of treatment, and treatment goals have not adequately taken patient age into account (in whom arterial stiffening plays a larger role), and they have typically relied too heavily on threshold cutoffs, rather than the “linear progression” of risk factors and their impact on organ damage.
6. Mathematical Modeling: Arterial stiffening provides sufficient explanation for primary hypertension
Klas H. Pettersen, Scott M. Bugenhagen, Javaid Nauman, Daniel A. Beard, Stig W. Omholt
(Submitted on 3 May 2013 (v1), last revised 6 May 2013 (this version, v2))
Hypertension is one of the most common age-related chronic diseases and by predisposing individuals for heart failure, stroke and kidney disease, it is a major source of morbidity and mortality. Its etiology remains enigmatic despite intense research efforts over many decades. By use of empirically well-constrained computer models describing the coupled function of the baroreceptor reflex and mechanics of the circulatory system, we demonstrate quantitatively that arterial stiffening seems sufficient to explain age-related emergence of hypertension. Specifically, the empirically observed chronic changes in pulse pressure with age, and the impaired capacity of hypertensive individuals to regulate short-term changes in blood pressure, arise as emergent properties of the integrated system. Results are consistent with available experimental data from chemical and surgical manipulation of the cardio-vascular system. In contrast to widely held opinions, the results suggest that primary hypertension can be attributed to a mechanogenic etiology without challenging current conceptions of renal and sympathetic nervous system function. The results support the view that a major target for treating chronic hypertension in the elderly is the reestablishment of a proper baroreflex response.
Klas H. Pettersen1, Scott M. Bugenhagen2, Javaid Nauman3, Daniel A. Beard2 & Stig W. Omholt3
1Department of Mathematical and Technological Sciences, Norwegian University of Life Science, Norway
2Department of Physiology, Medical College of Wisconsin, Milwaukee, Wisconsin, USA
3NTNU Norwegian University of Science and Technology, Department of Circulation and Medical Imaging, Cardiac Exercise Research Group, Trondheim, Norway
Correspondence should be addressed to: KHP (klas.pettersen@gmail.com)
Keywords: hypertension, mechanogenic, baroreceptor signaling, cardiovascular model, arterial stiffening
Author contributions: K.H.P. and S.W.O. designed the study. K.H.P. constructed the
integrated model and performed the numerical experiments with contributions from
D.A.B. and S.M.B.. J.N. extracted and compiled empirical test data from the HUNT2
Survey. S.W.O, K.H.P. and D.A.B. wrote the paper.
7. Classification of Blood Pressure and Hypertensive Treatment:
Best Practice of Care in the US
8. Genetic Risk for High Blood Pressure
Hypertension.2013; 61: 931doi: 10.1161/HYP.0b013e31829399b2
Blood Pressure Single-Nucleotide Polymorphisms and Coronary Artery Sisease (page 995)
Blood pressure (BP) is considered a major cardiovascular risk factor that is influenced by multiple genetic and environmental factors. However, the precise genetic underpinning influencing interindividual BP variation is not well characterized; and it is unclear whether BP-associated genetic variants also predispose to clinically apparent cardiovascular disease. Such an association of BP-related variants with cardiovascular disease would strengthen the concept of BP as a causal risk factor for cardiovascular disease. In this issue of Hypertension, analyses within the Coronary ARtery DIsease Genome-Wide Replication And Meta-Analysis consortium indicate that common genetic variants associated with BP in the population, indeed, contribute to the susceptibility for coronary artery disease (CAD). Lieb et al tested 30 single-nucleotide polymorphisms—that based on prior studies were known to affect BP—for their association with CAD. In total, data from 22 233 CAD cases and 64 762 controls were analyzed. The vast majority (88%) of BP-related single-nucleotide polymorphisms were also shown to increase the risk of CAD (as defined by an odds ratio for CAD >1; Figure). On average, each of the multiple BP-raising alleles was associated with a 3% (95% confidence interval, 1.8%–4.3%) risk increase for CAD.
Masked Hypertension in Diabetes Mellitus (page 964)
The first important finding in the IDACO study of masked hypertension (MH) in the population with diabetes mellitus and non–diabetes mellitus was that antihypertensive treatment converted some sustained hypertensives into sustained normotensives; this resulted in an increased cardiovascular disease risk in the treated versus untreated normotensive comparator group (Figure). Not surprisingly, normalization of blood pressure (BP) with treatment did not eliminate the lifetime cardiovascular disease burden associated with prior elevated BP nor did it correct other cardiometabolic risk factors that clustered with the hypertensive state.
The second important IDACO finding was that treatment increased the prevalence of MH by decreasing conventional BP versus daytime ambulatory BP (ABP) by a ratio of ≈3 to 2. The clinical implication of increased prevalence of MH with therapy in the population of both diabetes mellitus and non–diabetes mellitus was that these subjects did not receive sufficient antihypertensive therapy to convert MH into normalized ABP (ie, treated, normalized ABP being the gold standard for minimizing cardiovascular disease risk). Indeed, there is a transformation-continuum from sustained hypertension to MH and finally to sustained normotension with increasing antihypertensive therapy. These IDACO findings strongly suggest that many physicians mistakenly have their primary focus on normalizing in-office rather than out-of-office home BP and/or 24-hour ABP values and this results in an increased prevalence of MH. However, what constitutes optimal normalized ABP will remain empirical until established in randomized controlled trials.
Genetic Risk Score for Blood Pressure (page 987)
Elevated blood pressure (BP) is a strong, independent, and modifiable risk factor for stroke and heart disease. BP is a heritable trait, and genome-wide association studies have identified several genetic loci that are associated with systolic BP, diastolic BP, or both. Although the variants have modest effects on BP, typically 0.5 to 1.0 mm Hg, their presence may act over the entire life course and, therefore, lead to substantial increase in risk of cardiovascular disease (CVD). However, the independent impact of these variants on CVD risk has not been established in a prospective setting. Havulinna et al genotyped 32 common single-nucleotide polymorphisms in several Finnish cohorts, with up to 32 669 individuals after exclusion of prevalent CVD cases. The median follow-up was 9.8 years, during which 2295 incident CVD events occurred. Genetic risk scores were created for systolic BP and diastolic BP by multiplying the risk allele count of each single-nucleotide polymorphism by the effect size estimated in published genome-wide association studies on BP traits. The GRSs were strongly associated with baseline systolic BP, diastolic BP, and hypertension (all P<10–62). Hazard ratios for incident CVD increased roughly linearly by quintile of systolic BP or diastolic BP GRS (Figure). GRSs remained significant predictors of CVD risk after adjustment for traditional risk factors, even including BP and use of antihypertensive medication. These findings are consistent with a lifelong effect of these variants on BP and CVD risk.
Related Articles on Genetics and Blood Pressure
Genetic Predisposition to Higher Blood Pressure Increases Coronary Artery Disease Risk
- Wolfgang Lieb,
- Henning Jansen,
- Christina Loley,
- Michael J. Pencina,
- Christopher P. Nelson,
- Christopher Newton-Cheh,
- Sekar Kathiresan,
- Muredach P. Reilly,
- Themistocles L. Assimes,
- Eric Boerwinkle,
- Alistair S. Hall,
- Christian Hengstenberg,
- Reijo Laaksonen,
- Ruth McPherson,
- Unnur Thorsteinsdottir,
- Andreas Ziegler,
- Annette Peters,
- John R. Thompson,
- Inke R. König,
- Jeanette Erdmann,
- Nilesh J. Samani,
- Ramachandran S. Vasan,
- andHeribert Schunkert
- , on behalf of CARDIoGRAM
Hypertension. 2013;61:995-1001, published online before print March 11 2013,doi:10.1161/HYPERTENSIONAHA.111.00275
Masked Hypertension in Diabetes Mellitus: Treatment Implications for Clinical Practice
- Stanley S. Franklin,
- Lutgarde Thijs,
- Yan Li,
- Tine W. Hansen,
- José Boggia,
- Yanping Liu,
- Kei Asayama,
- Kristina Björklund-Bodegård,
- Takayoshi Ohkubo,
- Jørgen Jeppesen,
- Christian Torp-Pedersen,
- Eamon Dolan,
- Tatiana Kuznetsova,
- Katarzyna Stolarz-Skrzypek,
- Valérie Tikhonoff,
- Sofia Malyutina,
- Edoardo Casiglia,
- Yuri Nikitin,
- Lars Lind,
- Edgardo Sandoya,
- Kalina Kawecka-Jaszcz,
- Jan Filipovský,
- Yutaka Imai,
- Jiguang Wang,
- Hans Ibsen,
- Eoin O’Brien,
- and Jan A. Staessen
- , on behalf of the International Database on Ambulatory blood pressure in relation to Cardiovascular Outcomes (IDACO) Investigators
Hypertension. 2013;61:964-971, published online before print March 11 2013,doi:10.1161/HYPERTENSIONAHA.111.00289
A Blood Pressure Genetic Risk Score Is a Significant Predictor of Incident Cardiovascular Events in 32 669 Individuals
- Aki S. Havulinna,
- Johannes Kettunen,
- Olavi Ukkola,
- Clive Osmond,
- Johan G. Eriksson,
- Y. Antero Kesäniemi,
- Antti Jula,
- Leena Peltonen,
- Kimmo Kontula,
- Veikko Salomaa,
- and Christopher Newton-Cheh
Hypertension. 2013;61:987-994, published online before print March 18 2013,doi:10.1161/HYPERTENSIONAHA.111.00649
9. Is it Hypertension or Physical Inactivity: Cardiovascular Risk and Mortality – New results in 3/2013.
Heart doi:10.1136/heartjnl-2012-303461
- Epidemiology
- Original article
Estimating the effect of long-term physical activity on cardiovascular disease and mortality: evidence from the Framingham Heart Study
+Author Affiliations
1Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia
2Biostatistics Unit, Group Health Research Institute, Seattle, Washington, USA
3Obesity and Population Health Unit, Baker IDI Heart and Diabetes Institute, Melbourne, Australia
Correspondence toDr Susan M Shortreed, Biostatistics Unit, Group Health Research Institute, 1730 Minor Avenue, Suite 1600, Seattle, WA 98101, USA; shortreed.s@ghc.org
- Published Online First 8 March 2013
Abstract
Objective In the majority of studies, the effect of physical activity (PA) on cardiovascular disease (CVD) and mortality is estimated at a single time point. The impact of long-term PA is likely to differ. Our study objective was to estimate the effect of long-term adult-life PA compared with long-term inactivity on the risk of incident CVD, all-cause mortality and CVD-attributable mortality.
Design Observational cohort study.
Setting Framingham, MA, USA.
Patients 4729 Framingham Heart Study participants who were alive and CVD-free in 1956.
Exposures PA was measured at three visits over 30 years along with a variety of risk factors for CVD. Cumulative PA was defined as long-term active versus long-term inactive.
Main outcome measures Incident CVD, all-cause mortality and CVD-attributable mortality.
Results During 40 years of follow-up there were 2594 cases of incident CVD, 1313 CVD-attributable deaths and 3521 deaths. Compared with long-term physical inactivity, the rate ratio of long-term PA was 0.95 (95% CI 0.84 to 1.07) for CVD, 0.81 (0.71 to 0.93) for all-cause mortality and 0.83 (0.72 to 0.97) for CVD-attributable mortality. Assessment of effect modification by sex suggests greater protective effect of long-term PA on CVD incidence (p value for interaction=0.004) in men (0.79 (0.66 to 0.93)) than in women (1.15 (0.97 to 1.37)).
Conclusions
- Cumulative long-term PA has a protective effect on incidence of all-cause and CVD-attributable mortality compared with long-term physical inactivity.
- In men, but not women, long-term PA also appears to have a protective effect on incidence of CVD.
Summary – PENDING
REFERENCES
1. Kannel WB, Gordan T (1978) Evaluation of cardiovascular risk in the elderly: the Framingham study. Bull N Y Acad Med 54:573–591.
1. Kannel WB, Gordan T (1978) Evaluation of cardiovascular risk in the elderly: the Framingham study. Bull N Y Acad Med 54:573–591.
2. Franklin SS, Khan SA, Wong ND, Larson MG, Levy D (1999) Is pulse pressure useful in predicting risk for coronary heart disease?: The Framingham Heart Study. Circulation 100:354–360.
3. Mitchell GF et al. (2010) Hemodynamic Correlates of Blood Pressure Across the Adult Age Spectrum: Noninvasive Evaluation in the Framingham Heart Study. Circulation 122:1379–1386.
4. Khattar RS, Swales JD, Dore C, Senior R, Lahiri A (2001) Effect of Aging on the Prognostic Significance of Ambulatory Systolic, Diastolic, and Pulse Pressure in Essential Hypertension. Circulation 104:783–789.
5. Franklin SS et al. (1997) Hemodynamic patterns of age-related changes in blood pressure: the Framingham Heart Study. Circulation 96:308.
6. Guyenet PG (2006) The sympathetic control of blood pressure. Nat Rev Neurosci 7:335–346.
7. Monahan KD (2007) Effect of aging on baroreflex function in humans. Am J Physiol Regul Integr Comp Physiol 293:R3–R12.
8. Zieman SJ (2005) Mechanisms, Pathophysiology, and Therapy of Arterial Stiffness. Arterioscler Thromb Vasc Biol 25:932–943.
9. McVeigh GE, Bank AJ, Cohn JN (2007) Arterial compliance. Cardiovasc Med:1811–1831.
10. Guyton AC (1991) Blood pressure control–special role of the kidneys and body fluids. Science 252:1813–1816.
11. Smith BW, Chase JG, Nokes RI, Shaw GM, Wake G (2004) Minimal haemodynamic system model including ventricular interaction and valve dynamics. Med Eng Phys 26:131–139.
12. Smith BW, Geoffrey Chase J, Shaw GM, Nokes RI (2005) Experimentally verified minimal cardiovascular system model for rapid diagnostic assistance. Control Eng Pract 13:1183–1193.13. Bugenhagen SM, Cowley AW, Beard DA (2010) Identifying physiological origins of baroreflex dysfunction in salt-sensitive hypertension in the Dahl SS rat. Physiol Genomics 42:23–41.14. Beard DA et al. (2012) Multiscale Modeling and Data Integration in the Virtual Physiological Rat Project. Ann Biomed Eng.15. King AL (1946) Pressure-Volume Relation for Cylindrical Tubes with Elastomeric Walls: The Human Aorta. J Appl Phys 17:501.16. Dayan P, Abbott LF (2001) Theoretical Neuroscience: Computational and Mathematical Modeling of Neural Systems (Computational Neuroscience) (The MIT Press). 1st Ed.17. Andresen MC, Krauhs JM, Brown AM (1978) Relationship of aortic wall and baroreceptor properties during development in normotensive and spontaneously hypertensive rats. Circ Res 43:728–738.18. Hallock P, Benson IC (1937) Studies on the elastic properties of human isolated aorta. J Clin Invest 16:595–602.19. Coffman TM (2011) Under pressure: the search for the essential mechanisms of hypertension. Nat Med 17:1402–1409.20. Proctor DN et al. (1998) Influence of age and gender on cardiac output-V O 2 relationships during submaximal cycle ergometry. J Appl Physiol 84:599–605.21. Fagard R, Thijs L, AMERY A (1993) Age and the Hemodynamic Response to Posture and Exercise. Am J Geriatr Cardiol 2:23–40.22. Stratton JR, Levy WC, Cerqueira MD, Schwartz RS, Abrass IB (1994) Cardiovascular responses to exercise. Effects of aging and exercise training in healthy men. Circulation 89:1648–1655.23. Holmen J et al. (2003) The Nord-Trøndelag Health Study 1995–97 (HUNT 2): objectives, contents, methods and participation. Norsk epidemiologi 13:19–32.24. Chobanian AV et al. (2003) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 289:2560–2572.25. Cowley AW, LIARD JF, Guyton AC (1973) Role of the Baroreceptor Reflex in Daily Control of Arterial Blood Pressure and Other Variables in Dogs. Circ Res 32:564–576.26. Schreihofer AM, Sved AF (1992) Nucleus tractus solitarius and control of blood pressure in chronic sinoaortic denervated rats. Am J Physiol 263:R258–66.27. Ito S, Sved AF (1997) Influence of GABA in the nucleus of the solitary tract on blood pressure in baroreceptor-denervated rats. Am J Physiol Regul Integr Comp Physiol 273:R1657–R1662.28. Thrasher TN (2004) Baroreceptors, baroreceptor unloading, and the long-term control of blood pressure. Am J Physiol Regul Integr Comp Physiol 288:R819– R827.29. Monahan KD et al. (2001) Age-associated changes in cardiovagal baroreflex sensitivity are related to central arterial compliance. Am J Physiol Heart Circ Physiol 281:H284–H289.30. Malpas S (2009) Editorial comment: Montani versus Osborn exchange of views. Experimental Physiology 94:381–382.31. Mori T et al. (2008) High Perfusion Pressure Accelerates Renal Injury in Salt-Sensitive Hypertension. Journal of the American Society of Nephrology 19:1472–1482.32. Beard DA, Mescam M (2012) Mechanisms of pressure-diuresis and pressurenatriuresis in Dahl salt-resistant and Dahl salt-sensitive rats. BMC Physiol 12:6.33. Iliescu R, Irwin ED, Georgakopoulos D, Lohmeier TE (2012) Renal Responses to Chronic Suppression of Central Sympathetic Outflow. Hypertension 60:749–756.34. Krum H et al. (2009) Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 373:1275–1281.35. Mahfoud F et al. (2012) Renal Hemodynamics and Renal Function After Catheter-Based Renal Sympathetic Denervation in Patients With Resistant Hypertension. Hypertension 60:419–424.36. Vink EE, Blankestijn PJ (2012) Evidence and Consequences of the Central Role of the Kidneys in the Pathophysiology of Sympathetic Hyperactivity. Front Physio 3.37. Cowley A Jr (1992) Long-term control of arterial blood pressure. Physiol Rev 72:231–300.38. Mancia G, Ludbrook J, Ferrari A, Gregorini L, Zanchetti A (1978) Baroreceptor reflexes in human hypertension. Circ Res 43:170–177.39. Kaess BM et al. (2012) Aortic stiffness, blood pressure progression, and incident hypertension. JAMA 308:875–881.
40. Kirkwood TBL (1977) Evolution of ageing. Nature 270:301–304.
41. Nakayama Y et al. (2001) Heart Rate-Independent Vagal Effect on End-Systolic Elastance of the Canine Left Ventricle Under Various Levels of Sympathetic Tone. Circulation 104:2277–2279.
42. Cohen A (1991) A Padé approximant to the inverse Langevin function. Rheologic Acta 30:270–273.
43. Brown AM, Saum WR, Tuley FH (1976) A comparison of aortic baroreceptor discharge in normotensive and spontaneously hypertensive rats. Circ Res 39:488–496.
44. Smith H (2011) in Texts in Applied Mathematics, Texts in Applied Mathematics. (Springer New York, New York, NY), pp 119–130.
Other related articles were published on this Open Access Online Scientific Journal including the following:
Pearlman, JD and A. Lev-Ari 5/24/2013 Imaging Biomarker for Arterial Stiffness: Pathways in Pharmacotherapy for Hypertension and Hypercholesterolemia Management
Lev-Ari, A. 5/17/2013 Synthetic Biology: On Advanced Genome Interpretation for Gene Variants and Pathways: What is the Genetic Base of Atherosclerosis and Loss of Arterial Elasticity with Aging
Bernstein, HL and A. Lev-Ari 5/15/2013 Diagnosis of Cardiovascular Disease, Treatment and Prevention: Current & Predicted Cost of Care and the Promise of Individualized Medicine Using Clinical Decision Support Systems
Pearlman, JD and A. Lev-Ari 5/7/2013 On Devices and On Algorithms: Arrhythmia after Cardiac Surgery Prediction and ECG Prediction of Paroxysmal Atrial Fibrillation Onset
Pearlman, JD and A. Lev-Ari 5/4/2013 Cardiovascular Diseases: Decision Support Systems for Disease Management Decision Making
Larry H Bernstein, MD, FACP, 12/10/2012
Aviva Lev-Ari, PhD, RN and Larry H. Bernstein, MD, FACP, 3/7/2013
Aviva Lev-Ari, PhD, RN, 4/28/2013
Aviva Lev-Ari, PhD, RN, 4/4/2013
Manuela Stoicescu, MD, PhD, 2/9/2013
Aviva Lev-Ari, PhD, RN, 1/14/2013
Aviva Lev-Ari, PhD, RN, 6/13/2012
Aviva Lev-Ari, PhD, RN, 5/29/2012
Mitochondrial Dysfunction and Cardiac Disorders
Curator: Larry H Bernstein, MD, FACP
Aviva Lev-Ari, PhD, RN, 4/7/2013
Walking and Running: Similar Risk Reductions for Hypertension, Hypercholesterolemia, DM, and possibly CAD
Posted in Atherogenic Processes & Pathology, Frontiers in Cardiology and Cardiovascular Disorders, HTN, Origins of Cardiovascular Disease, tagged CHD, Coronary disease, Diabetes Mellitus, Hartford Hospital, Hypercholesterolemia, Hypertension, Lawrence Berkeley National Laboratory on April 4, 2013| 2 Comments »
Reporter: Aviva Lev-Ari, PhD, RN
Walking Versus Running for Hypertension, Cholesterol, and Diabetes Mellitus Risk Reduction
From the Life Sciences Division, Lawrence Berkeley National Laboratory, Berkeley, CA (P.T.W.); and Division of Cardiology, Hartford Hospital, Hartford, CT (P.D.T.).
Correspondence to Paul T. Williams, PhD, Life Sciences Division, Lawrence Berkeley National Laboratory, Donner 464, 1 Cycloton Rd, Berkeley, CA 94720. E-mailptwilliams@lbl.gov
Abstract
Objective—To test whether equivalent energy expenditure by moderate-intensity (eg, walking) and vigorous-intensity exercise (eg, running) provides equivalent health benefits.
Approach and Results—We used the National Runners’ (n=33 060) and Walkers’ (n=15 945) Health Study cohorts to examine the effect of differences in exercise mode and thereby exercise intensity on coronary heart disease (CHD) risk factors. Baseline expenditure (metabolic equivant hours per day [METh/d]) was compared with self-reported, physician-diagnosed incident hypertension, hypercholesterolemia, diabetes mellitus, and CHD during 6.2 years follow-up. Running significantly decreased the risks for incident hypertension by 4.2% (P<10−7), hypercholesterolemia by 4.3% (P<10−14), diabetes mellitus by 12.1% (P<10−5), and CHD by 4.5% per METh/d (P=0.05). The corresponding reductions for walking were 7.2% (P<10−7), 7.0% (P<10−8), 12.3% (P<10−4), and 9.3% (P=0.01). Relative to <1.8 METh/d, the risk reductions for 1.8 to 3.6, 3.6 to 5.4, 5.4 to 7.2, and ≥7.2 METh/d were as follows: (1) 10.0%, 17.7%, 25.1%, and 34.9% from running and 14.0%, 23.8%, 21.8%, and 38.3% from walking for hypercholesterolemia; (2) 19.7%, 19.4%, 26.8%, and 39.8% from running and 14.7%, 19.1%, 23.6%, and 13.3% from walking for hypertension; and (3) 43.5%, 44.1%, 47.7%, and 68.2% from running, and 34.1%, 44.2% and 23.6% from walking for diabetes mellitus (walking >5.4 METh/d excluded for too few cases). The risk reductions were not significantly different for running than walking for diabetes mellitus (P=0.94), hypercholesterolemia (P=0.06), or CHD (P=0.26), and only marginally greater for walking than running for hypercholesterolemia (P=0.04).
Conclusions—Equivalent energy expenditures by moderate (walking) and vigorous (running) exercise produced similar risk reductions for hypertension, hypercholesterolemia, diabetes mellitus, and possibly CHD.
http://atvb.ahajournals.org/content/early/2013/04/04/ATVBAHA.112.300878.abstract.html?papetoc
Secondary Hypertension caused by Aldosterone-producing Adenomas caused by Somatic Mutations in ATP1A1 and ATP2B3
Posted in Biological Networks, Gene Regulation and Evolution, Biomarkers & Medical Diagnostics, CANCER BIOLOGY & Innovations in Cancer Therapy, Cardiovascular Pharmacogenomics, Cell Biology, Signaling & Cell Circuits, Chemical Genetics, Computational Biology/Systems and Bioinformatics, Frontiers in Cardiology and Cardiovascular Disorders, Genome Biology, Genomic Testing: Methodology for Diagnosis, HTN, Molecular Genetics & Pharmaceutical, Personalized and Precision Medicine & Genomic Research, tagged adenoma, Cancer - General, Conditions and Diseases, Hypertension, mutation, Secondary hypertension on February 21, 2013| Leave a Comment »
Reporter: Aviva Lev-Ari, PhD, RN
Somatic mutations in ATP1A1 and ATP2B3 lead to aldosterone-producing adenomas and secondary hypertension
- Felix Beuschlein,
- Sheerazed Boulkroun,
- Andrea Osswald,
- Thomas Wieland,
- Hang N Nielsen,
- Urs D Lichtenauer,
- David Penton,
- Vivien R Schack,
- Laurence Amar,
- Evelyn Fischer,
- Anett Walther,
- Philipp Tauber,
- Thomas Schwarzmayr,
- Susanne Diener,
- Elisabeth Graf,
- Bruno Allolio,
- Benoit Samson-Couterie,
- Arndt Benecke,
- Marcus Quinkler,
- Francesco Fallo,
- Pierre-Francois Plouin,
- Franco Mantero,
- Thomas Meitinger,
- Paolo Mulatero,
- Xavier Jeunemaitre,
- Richard Warth,
- Bente Vilsen,
- Maria-Christina Zennaro,
- Tim M Strom
- & Martin Reincke
- Published online 17 February 2013
- Mutations affecting a pair of related enzyme-coding genes can contribute to the
risk of benign glandular tumors
- called adenomas and secondary hypertension, a new
- study suggests. An international team led by investigators in Germany performed
- on matched tumor and normal samples from nine individuals with forms of adenoma that enhance aldosterone hormone production. This leads to a type of so-called aldosteronism that can bump up blood pressure and cause other adverse symptoms.
When researchers sorted through the exome sequence data, they saw ties between aldosterone-producing adenoma and mutations in two ATPase genes — ATP1A1 and ATP2B3 — that participate in sodium/potassium and calcium signaling, respectively. Somatic ATP1A1 mutations turned up in more than 5 percent of 308 aldosterone-producing adenoma samples screened subsequently, the team noted, while 1.6 percent of those tumors contained ATP2B3 alterations.
“[T]hese findings expand the spectrum of somatic alterations leading to [aldosterone-producing adenomas] to two members of the P-type ATPase pump family, extend knowledge of the molecular mechanism leading to [aldosterone-producing adenoma],” the Ludwig Maximilian University of Munich researcher Martin Reincke, the study’s corresponding author, and colleagues wrote, “and indicate new potential therapeutic targets for the most frequent secondary form of arterial hypertension.”
SOURCE:
http://www.genomeweb.com//node/1194476?hq_e=el&hq_m=1505701&hq_l=6&hq_v=6fcaf1aef4
Somatic mutations in ATP1A1 and ATP2B3 lead to aldosterone-producing adenomas and secondary hypertension
Primary aldosteronism is the most prevalent form of secondary hypertension. To explore molecular mechanisms of autonomous aldosterone secretion, we performed exome sequencing of aldosterone-producing adenomas (APAs). We identified somatic hotspot mutations in the ATP1A1 (encoding an Na+/K+ ATPase α subunit) and ATP2B3 (encoding a Ca2+ ATPase) genes in three and two of the nine APAs, respectively. These ATPases are expressed in adrenal cells and control sodium, potassium and calcium ion homeostasis. Functional in vitro studies of ATP1A1 mutants showed loss of pump activity and strongly reduced affinity for potassium. Electrophysiological ex vivo studies on primary adrenal adenoma cells provided further evidence for inappropriate depolarization of cells with ATPase alterations. In a collection of 308 APAs, we found 16 (5.2%) somatic mutations in ATP1A1 and 5 (1.6%) in ATP2B3.
Mutation-positive cases showed
- male dominance,
- increased plasma aldosterone concentrations and
- lower potassium concentrations compared with mutation-negative cases.
In summary, dominant somatic alterations in two members of the ATPase gene family result in autonomous aldosterone secretion.
Author information
SOURCE:
http://www.nature.com/ng/journal/vaop/ncurrent/full/ng.2550.html
An Important Marker of Hypertension in Young Adults: Plasma Renin
Posted in Biomarkers & Medical Diagnostics, HTN in Youth, tagged Conditions and Diseases, Hypertension, Pheochromocytoma on February 9, 2013| 5 Comments »
An Important Marker of Hypertension in Young Adults: Plasma Renin
Author: Manuela Stoicescu, MD, PhD
Original research
Manuela Stoicescu, MD, PhD
Consultant Internal Medicine, Assistant Professor
Faculty of Medicine and Pharmacy, Medical Disciplines Department
University of Oradea, Romania
ABSTRACT
Introduction: Plasma renin level is an important marker of hypertension in the young adults. The purpose of this study was to determine the role of increased levels of plasmatic renin in the pathogenesis of hypertension in the young adults and to highlight the main conditions underlying the pathogenesis of hypertension in the young people in these circumstances.
Material and methods: The group of patients taking part in the study was of 121 young hypertensive adults (selected from a group of 321 young hypertensive adults), with the age between 18-35 years, with elevated blood pressure exceeding 140/90mmHg in at least three repeated measurements at intervals of one week to exclude white coat phenomenon, or had a blood pressure value greater than 170/100mmHg at the first measurement and increased plasma renin levels above the 4,3ng/ml.
Results and discussion: Of the 121 young hypertensive patients with increased plasma renin levels, 49 were cases of renal artery stenosis representing 40.50% (p<0.001), 8 cases were represented by small unilateral kidneys representing 6.61% (p<0.001), renal cell carcinoma (previously known as “hypernephron” – Grawitz tumor) was responsible for the younger group of patients studied of 4 cases representing 3.30% (p <0.001) of the cases of hypertension in the young adults, and 60 cases representing 49.59% were represented by pheochromocytoma.
Conclusions: The results show the role of plasma renin dosing as being particularly important in the pathogenesis of secondary hypertension in the young adults
Keywords: Renin, arterial hypertension (HBP), young adults
INTRODUCTION
Renin is an enzyme secreted by the juxtaglomerular apparatus to maintain electrolyte balance and blood pressure in the appropriate limits. Plasma renin level is an important marker of hypertension in the young adults. The purpose of this study was to determine the role of increased levels of plasma renin in the pathogenesis of hypertension in the young adults and highlight the main conditions underlying the pathogenesis of hypertension in the young adults with increased plasmatic renin. The principal diseases which had increased plasma renin levels were: renal artery stenosis, pheochromocytoma, congenital unilateral small kidney, primary reninoma (renal cell carcinoma or Grawitz tumor), situations in which renin is secreted in excess, the highest values being in cases of renal cell carcinoma, of 320ng/ml.
MATERIAL AND METHODS
The group of patients taking parts in the study was of 121 hypertensive young adults, with the ages between 18-35 years with elevated blood pressure over 140/90mmHg in at least three repeated measurements at intervals of one week to exclude white coat phenomenon frequently encountered in the young, or had a severely increased blood pressure of >170/100mmHg on the first measurement and plasma renin levels greater than 4,3 ng/ml.
Parameters for assessment of the diseases which had increased plasma rennin levels were clinical, radiological, biological and histopathological. The study was done after the diagnosis of hypertension and staging according OMS. All patients were investigated clinically and fully analyzed paraclinically. They agreed to participate in the trial after they were explained the criteria of professional ethics, scientific and terms of confidentiality. All patients participating in the study had plasmatic renin levels above 4.3ng /ml. The statistical analysis was done with the help of EPIINFO application, version 6.0, program of the Center for Disease Control and Prevention-CDC in Atlanta, suitable for processing of medical statistics. Averages were calculated for the parameters, frequency ranges, standard deviations, tests of statistical significance by Student method (t test) and χ ².
RESULTS
The group of young hypertensive patients with ages 18-35 years, with elevated blood pressure >140/90mmHg, with increased plasma renin levels over 4.3ng/ml we found 49 cases of renal artery stenosis representing 40.50%, 8 cases of congenital small kidney representing 6.61%, 4 cases of Grawitz tumors (renal cell carcinoma) representing 3.30% and 60 cases of pheochromocytoma representing 49.59%. Table No.1
Table 1. The main conditions that were present in the group of young hypertensive patients with increased plasma renin level.
|
Diseases |
No. of cases |
Percentage of cases [%] |
|
Vascular pathology |
49 |
40.50% |
|
Renal parenchymatous pathology Congenital small kidney |
8 |
6.61% |
|
Renal carcinoma (Gravitz tumor) |
4 |
3.30% |
|
60 |
49.59% |
The positive criteria’s of diagnostic for the diseases were included in the study was:
I. Renal artery stenosis
- The increased value of diastolic blood pressure over 110mmHg.
- Paraombilical systolic murmur.
- Imaging of arteriography.
- Increased plasmatic renin level > 4.3 ng / ml.
II. Congenital small kidney
- Values of blood pressure over 140/90mmHg.
- Arteriography – put in evidence the small kidney
- The abdominal MRI
- Increased plasmatic renin level > 4.3 ng / ml.
III. Renal carcinoma (Gravitz tumor)
- Unilateral lumbar pain
- Loss of appetite
- Weight loss
- Macroscopic hematuria (blood in the urine)
- The value of plasma rennin level increased > 4.3ng /ml, mentioning that in this situation the plasma renin values reached the highest values up to 320ng/ml
- The abdominal MRI
- The renal biopsy
IV. Pheochromocytoma
- The paroxysmal outbursts of severe blood pressure over 220/120mmHg
- Headache
- Tremor of extremities
- Nervousness
- Increased serum catecholamine levels above 260pg/ml
- Increased urinary catecholamine values above the 7.4 mg/24 hrs
- Increased plasmatic renin level > 4.3 ng/ml.
- The abdominal MRI used in the detection of adrenal tumors .
Table 2. Diagnostic criteria’s met by patients
|
Diseases |
No. of cases |
Diagnostic criteria’s met by patients |
|
Vascular pathology Renal artery stenosis |
49 |
24 cases 4 of 4 25 cases 3 of 4 |
|
Renal parenchymatous pathology Congenital small kidney |
8 |
8 cases 4 of 4
|
|
Renal carcinoma (Gravitz tumor) |
4 |
2 cases 7 of 7 2 cases 6 of 7 |
|
Pheochromocytoma |
60 |
38 cases 8 of 8 12 cases 7 of 8 10 cases 6 of 8 |
Of the group of young hypertensive patients studied with increased plasma renin activity, 49 of the cases were renal artery stenosis representing 40.50% (p <0.001). The parameters of the clinical assessment were the increased value of diastolic blood pressure over 110mmHg, paraombilical systolic murmur and an imaging of arteriography. Figure 1.
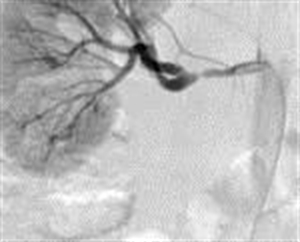
Figure 1. Arteriography of the right renal artery stenosis (M.I. aged 21 years with HBP = 170/120mmHg)
Of the group of young patients participating in the study, we found 8 cases of unilateral small kidney representing 6.61% (p<0.001). The pathogenic mechanism of hypertension was ischemic, in that all cases arterial high blood pressure evolved along with hyperreninemia in congenital unilateral small kidney. The early diagnosis of renal disease is very important, in the best cases before the hypertension causes severe nephroangiosclerosis on the contralateral kidney, leading to nephrectomy which then can then lead to the disappearance of hypertension. The parameters of assessment in this case were the clinical blood pressure values above 140/90mmHg, imaging methods to put in evidence the small kidney: arteriography Figure2 abdominal MRI Figura3 and biological-increased plasmatic renin activity> 4.3 ng / ml.
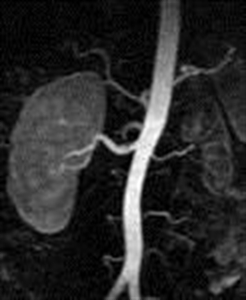
Figure2. Arteriography evidence the congenital small left kidney (D.R. of 19 years old with HBP = 165/110mmHg)

Figure 3. MRI – scan with contrast substance putting in evidence the left renal hypoplasia (D.R. of 19 years old with HBP = 165/110mmHg)
Renal cell carcinoma (renal carcinoma, previously “hypernephroma” – Grawitz tumor) was responsible for the younger group of patients studied, 4 cases representing 3,30% (p<0.001) of the HBP young cases. All had severely elevated blood pressure values over 200/100mmHg. The diagnostic was based on clinical parameters: unilateral lumbar pain, loss of appetite, weight loss, but only two cases had macroscopic hematuria (blood in the urine), biological – the value of increased plasma rennin level > 4.3ng /ml, mentioning that in this situation the plasma renin values reached the highest values up to 320ng/ml. Imaging parameters are represented in the abdominal MRI by Figure 4.

Figure 4. MRI-scan with bilateral renal tumor (F.R.of 34 years with malignant HBP=220/130mmHg — worked with pesticides)
Histopathological parameters were put into evidence in all four cases in which renal biopsy was performed and the histopathological results of which are outlined below:
Two cases were clear cell renal carcinoma based on the histopathology results after renal biopsy – histological preparation with H&E staining with the objective of 10X is shown in (Figure 5a) and (Figure 5b)
Figure 5a. Clear cell renal carcinoma (objective 10x) – H&E stain (M.I. 21 years with paroxysmal HBP=200/110mmHg)
Figure 5b. Clear cell renal carcinoma (objective 10x) – H&E stain (P.R. 28 years with severe form HBP=210/110mmhHg)
The other two cases of renal carcinoma are represented in the following H&E stained images, after the renal biopsy (Figure 6) and (Figure 7).
Figure 6. Renal carcinoma (objective 10x). H & E stain (I.G. 31 years with paroxysmal HBP=210/115 mmHg)
Figure 7. Renal carcinoma (objective 10x). H & E stain (F.R. 34 years with malignant HBP=220/130mmHg — worked with pesticides)
Hypertension in the young patients with renal cell carcinoma took the form of severe paroxysmal HBP=200/110mmHg or above in all four cases, due to excessive secretion of renin produced in large quantities by the tumor and it was the one form which attracted most the clinical attention when it was not manifested by macroscopic hematuria.
Of the group of hypertensive young adults studied, 60 of the cases were of pheochromocytoma representing 49.59%.
The diagnostic criteria used in this clinical situation were: paroxysmal outbursts of severe blood pressure values over 220/120mmHg accompanied by headache, tremor of extremities, nervousness, biological parameters represented by increased serum catecholamine levels above 260pg/ml, increased urinary catecholamine values above the 7.4 mg/24 hrs, imaging parameters which were used in the detection of adrenal tumors by performing an abdominal MRI. Figure 8.
Figure 8. Abdominal MRI-scan with pheochromocytoma of the right adrenal gland (G.R. 24 years with paroxysmal HBP=220/130mmHg)
DISCUSSIONS
The importance of this study was to measure the level of plasma renin of hypertensive young patients with ages between 18-35 years to determine its role in the pathogenesis of secondary hypertension in the young adults. Also the conditions in which plasma renin level is increased in the context of secondary hypertension in the young patients.
Renovascular hypertension was one of the important causes of secondary hypertension in the young, its frequency in the group of patients studied was of 49 cases with renal artery stenosis representing 40.50% (p <0.001), in all these cases the renin plasma level was increased above 4,3ng/ml.
Safian R.D. and Textor S.C. [1] found the frequency of renal artery stenosis in a group of young hypertensive patients with increased plasma renin activity, as being 42.36%, which is slightly higher than in our study, this difference could be explained by a better paraclinical investigation of the young patients with hypertension.
Of the group of young hypertensive patients participating in the study we found 8 cases of unilateral congenital small kidney, representing 6.61% (p<0.001).
Goddard C, et al. [2] found that the incidence of hypertension in young people with kidney hypoplasia was 25%. They suggested that the renin-angiotensin-aldosterone system plays an important role in the pathogenesis of hypertension in the situation of renal hypoplasia. This difference could be explained by the fact that young patients in other countries had an increased teratogenic risk compared with the young in our country.
Renal cell carcinoma (Grawitz tumor) was responsible for the younger group of patients studied, 4 cases representing 3.30% (p<0.001) of all the young hypertensive patients. Two cases were clear cell renal cell carcinoma histopathology analyzed after a renal biopsy. The data obtained are slightly lower than those in the literature (5%) Sukarochana [3] and (4%) Gangurly [4]. This difference could be explained by the fact that our country carcinogenic risk factors are lower.
Rose HJ, Pruitt AW [5] reported the case of a young patient with severe hypertension of 190/110mmHg, which after further investigations had found increased plasma renin levels and after paraclinical investigations a solitary simple kidney cyst was found.
DW Robertson et al. [6] reported the case of a young man who had elevated blood pressure (HBP=180/120mmHg) and after investigations increased plasma renin level was found and a left renal tumor (primary reninoma) was found, whose blood pressure values were normalized after tumor resection.
Pheochromocytoma was found in 60 of the cases representing 49.59% of cases of the young hypertensive adults.
Abrams HL [7] found that the incidence of pheochromocytoma in the young hypertensive cases was 21.03%, Bravo EL [8] found 42.38% cases of pheochromocytoma, and Bravo EL, Gifford RWJr [9] 46.03 % of young hypertensive patients with pheochromocytoma. These results are lower than those obtained in our study. This could be explained by the risk factors in this geographical area and dominant genetic factor has an important role in the etiology of pheochromocytoma.
CONCLUSIONS
- Plasmatic renin level is an important marker of hypertension in the young adults.
- The highest plasmatic renin levels up to 320ng/ml were found in the cases of renal cell carcinoma, because the kidney tumor cells secrete increased amounts of renin.
- This situation suggests that hypertension in the young adults is hyperreninemia hypertension in the most cases dominated by a vasoconstriction and increased peripheral vascular resistance due hyperactivity of the sympathetic nervous system, being a rapidly evolving form of hypertension with vascular complications.
- The results of plasma renin dosing shows its important role in the pathogenesis in secondary hypertension of the young adults, these conditions are not quite as rare as one might think but not enough investigated.
- This marker should be routinely performed in young patients with hypertension, especially those with medium and severe forms of blood pressure > 170/100mmHg, having a role in establishing the etiology of hypertension in the young, however presently it is still not made often enough, but situation must to be change in the future.
REFERENCES:
[1] Safian R.D, Textor S.C, Renal-artery stenosis, N Engl J Med 2001, 344(6):431-42.
[2] Goddard C , Vallothon MB, Broyer M, Plasma rennin activity in segmental hypoplasia of kidneys with hypertension, Nephron 2003, 11:308-17.
[3] Sukarochana K, Nephroblastoma and hypertension J Surg 2005, 7- 573.
[5] Rose HJ, Pruitt AW, Hypertension, hyperreninemia and a solitary renal cyst in an adolescent, Am J Med 2004, 61; 579-82.
[6] Robertson DW, Klidjiana A, Harding KK, Walters G, Lee MR, Robb-Smith AHT, Hypertension due to a renin-secreting renal tumor, Am Med 2005, 43 (9) 63-76.
[8] Bravo EL, Pheochromocytoma: New concepts and future trends, Kidney Int 1991, 40:544-556.
[9] Bravo EL, Gifford RWJr, Pheochromocytoma: Diagnosis, localization and management, N Engl J. Med 1984, 311-1298.
Corresponding author
Manuela Stoicescu, Internal Medicine Department, University of Oradea, Faculty of Medicine and Pharmacy, Oradea, Romania: County Hospital of Oradea, Phone 0723019951, e-mail: manuela_stoicescu@yahoo.com
Arterial Hypertension in Young Adults: An Ignored Chronic Problem
Posted in Biomarkers & Medical Diagnostics, HTN in Youth, tagged Blood pressure, Cardiovascular Disorders, Conditions and Diseases, Hypertension on February 9, 2013| 4 Comments »
Arterial Hypertension in Young Adults: An Ignored Chronic Problem
Author: Manuela Stoicescu, MD, PhD
Manuela Stoicescu, MD, PhD
Consultant Internal Medicine, Assistant Professor
Faculty of Medicine and Pharmacy, Medical Disciplines Department
University of Oradea, Romania
ABSTRACT
Introduction:
Don’t ignore the young patients: being young does not necessary mean being healthy.
Objectives:
The objectives in this study was to analyzed the principal clinical aspects and conduct laboratory investigations with young people in group of age 18-35 years. Attracting attention to the diagnosis of hypertension in the young in the early stages of life. I choice this topic because high blood pressure in the young, in particularly, in this group age was insufficiently studied while a high frequency of cases presented every day was continuously increasing.
Material and method:
The study was performed in the Ambulatory Specialty of the Internal Diseases Department in the County Hospital in Oradea, Romania. Study period was 1 October 2006 to 31 July 2009. Included in the study were 321 patients with hypertension exceeding 140/90 mmHg which was maintained higher after three consecutive determinations in intervals of one week to exclude the “white coat phenomenon”, an effect noted very frequent in young people, especially in young women, because a young persons have hyperactivity of simpatico nervous systemic, or the value of blood pressure was higher more than 170/110 mmHg from first determination.
Results
1. Importance of the genetic factors in the etiologies of disease was suggests that family prevalence of hypertension in the young people and another family diseases like hyperaldosteronism, polycystic kidney and multiple endocrine neoplasias MEN2a.
2. Importance of personal pathologic antecedents demonstrated in my study that repetitive Streptococcus angina with Streptococcus β hemolytic group A originated in the first place as a cause in hypertension in the young people in context of acute streptococcal renal parenchymatous diseases.
3. Renin plasmatic level is a very important marker of high blood pressure in the young. It was high in 121 cases (37.69%). This situation suggests that hypertension in the young is hyperreninemic hypertension in many cases because a young person has a systemic hyperactivity of simpatico nervous.
4. Left ventricular hypertrophy is been detected in X-ray, ECG and echocardiography. In my studied I detected left ventricular hypertrophy in 35 patients representing 10.49%.
5. Proteinuria was represented in 96 cases (29.90%) has two meanings:
- nephropathy complication of hypertension or
- acute glomerulonephritis or
- nephritis syndrome accompaniment with hematuria 38 cases (11.83%).
6. The eye ground findings of young people with hypertension are frequently normal. In the absence of prior readings, one needs to look for evidence of target organ damage that may suggest chronicity. In my study this changes appeared for 86 cases 23.3 %, hemorrhages and exudates I rarely found in 9 cases represent 2.8% and papilla edema was presented in 2 cases even when hypertension was very severe more than 200/120 mmHg and complicate with hypertensive encephalopathy.
Conclusions: Guidelines for hypertension treatment with young patients group of ages 18-35 was developed, which I hope will help the activity of physicians in general specialties in their practice, to use for diagnosis and easy work. This is new and hypertension in the young in this group of ages was insufficiently studied.
Key words: hypertension diagnosis, young adults.
INTRODUCTION
Prior to the last twenty years it was impossible to accept the idea that hypertension and atherosclerosis begin in adolescence and even earlier in childhood. Current concepts concerning the nature of hypertension in the young are changing. Earlier clinical impressions indicated that hypertension in the young was secondary and the essential hypertension occurred only rarely.
In my recent study, involving young people, of the age group of age 18-35 year old, indicated that young with high levels of blood pressure often the cause is known and often is unknown. When high BP (HBP) is found in the young the young compared with their peers, it is likely that the HBP will continue to Adulthood. My study has indicated that the level of blood pressure in young is closely related to the occurrence of hypertension in adulthood. Thus, changing concepts suggest that essential hypertension begins in early life. Considerable information is now known about the clinical and pathologic features of hypertension in adults.
We understand clinical diagnoses, the pathophysiology and humoral background, and the consequences of end stage renal disease (ESRD). We are even beginning to consider that essential hypertension may represent more than one disease. By contrast, little is known about the early natural development of essential hypertension. For example, how can hypertension in young be defined? We cannot equate level of blood pressure with cardiovascular damage as in adults (cardiovascular, cerebral, and renal disease). Furthermore, there is little specific information that can be used to predict development of adult hypertension. As a beginning, descriptive studies of the early natural development of essential hypertension are needed. It is logical to assume that prevention would be most successful if the disease process could be understood and treated in its earliest phase.
OBJECTIVES
Don’t ignore the young adult patient. Being young does not necessary means being healthy. Key objectives in my study was to analyze the principal clinical aspects and laboratory tests performed on young adults in the group age 18-35 year old, to advocate for the attention needed for diagnosis of hypertension in the young adults in the early stages of the disease.
MATERIAL AND METHOD
The study was performed in the Ambulatory Specialty of the Internal Diseases Department at the County Hospital in Oradea, Romana. Study period was 1 October 2006 to 31 July 2009. Study participants:
- 321 young patients,
- group of ages 18-35, patients with high blood pressure more than 140/90 mmHg
- after three consecutive determinations in interval one week maintain higher than 140/90 mmHg to exclude the “white coat phenomenon”, effect very frequently encountered with young adults especially with young women, because young person have a hyperactivity of sympathetic nervous system, or
- the value of blood pressure was high more than 170/110mmHg from first determination.
The patients had a comprehensive physical examination (clinical and par clinical) and diagnosed with hypertension in different stages.
The study consideration was done after having confirmed the diagnosis of hypertension and the standardization according to the phenomenon of high blood pressure and the classification of OMS.
The patients agreed to participate after being introduced in the study after they have been explained the deontological and preserving of the confidentiality criteria.
For statistics data I has been used the EPIINFO application, 6.0 version, a program of The Center of Disease Control and Prevention- Atlanta, with the Student method (test t) and χ²
RESULTS AND DISCUSSIONS
We observed that a 1/5 of the patients studied have in family antecedents of young adults hypertensive member of the family:hypertension in 70 cases (21.80%), stroke in 46 cases (14.33%), myocardial infarction in 55 cases (17.13%), peripheral vascular disease in 23 cases ( 7.16%) obesity 38 (11.83%), pre-eclamptic toxemia in 31 cases(9.65% ), hyperaldosteronism in 18 cases (5.60%), polycystic kidney in 26 cases (8.09%), multiple endocrine neoplasias MEN2a in 14 cases (4.36%) Distribution of cases according to family history. See, Table 1.
Table 1: Distribution of Cases according to Family History
|
Consideration |
No. of cases |
Percent |
|
Hypertension for parents, grandparents, aunts, uncles and cousins |
70 |
21.80% |
|
Family antecedents of stroke |
46 |
14.33 % |
|
Family antecedents of myocardial infarction |
55 |
17.13% |
|
Family antecedents of peripheral vascular disease |
23 |
7.16% |
|
Family antecedents of obesity |
38 |
11.83% |
|
Pre-eclamptic toxemia |
31 |
9.65% |
|
Hyperaldosteronism |
18 |
5.60% |
|
Polycystic kidney |
26 |
8.09% |
|
Multiple endocrine neoplasias MEN2a |
14 |
4.36% |
A significant numbers of patients in my studies did not have any antecedents of hypertension in their family history. That fact demonstrates that not only genetic factors have an important role in the etiology of the disease.ENvironmental factors count.
Significant number of hypertensive young patients had diseases in their personal history: Scarlatti in 27 (8.41%), repetitive angina with Streptococcus β hemolytic group A in 88 (27.41%), chronic ORAL infection focus in 35 (10.90%) chronic stomathological focus infections in 19 (5.91%), nephritis in 34(10.59%), endocrine disorders in 16 (4.98% ), physical and psychological in 22 (6.85%), head trauma in 11 (3.42%), therapy with corticosteroids secondary to another disease (for example erythematous systemic lupus) in 5 (1.55%), therapy with AINS drugs in 21 (6.54%), use decongestion nasal in 4 (1.24%) repetitive urinary tract infection in 28 (8.72%), syphilis in 11 (3.42%). See, Table II.
Table II: Distribution of Cases by Illnesses in Personal History
|
Consideration |
No. of cases |
Percent |
|
Scarlatti |
27 |
8.41% |
|
Repetitive Streptococcus angina with Streptococcus β hemolytic group A |
88 |
27.41% |
|
Chronic ORAL infection focus |
35 |
10.90% |
|
Chronic stomathological infection focus |
19 |
5.91% |
|
Nephritis |
34 |
10.59% |
|
Endocrine disorders |
16 |
4.98% |
|
Physical and psychical suprademanding |
22 |
6,85% |
|
Head trauma |
11 |
3,42% |
|
Therapy with corticosteroids |
5 |
1.55% |
|
Therapy with AINS |
21 |
6.54% |
|
Use decongestion at nasal |
4 |
1.24% |
|
Repetitive urinary tract infections |
28 |
8.72% |
|
Syphilis |
11 |
3.42% |
Fig.1: Principal Diseases Etiology for Young Hypertensive Patients
Table III: Laboratory Results
|
Hemoglobin value ↑ |
18 |
5.60% |
|
Hematocrit ↑ |
18 |
5.60% |
|
Value of glucose ↑ |
68 |
21.18% |
|
Cholesterol ↑ |
78 |
24.29% |
|
HDL cholesterol ↑ |
86 |
26.79% |
|
LDL cholesterol ↑ |
77 |
23.67% |
|
Triglycerides ↑ |
105 |
32.71% |
|
Uric acid ↑ |
57 |
17.75% |
|
Creatinina ↑ |
38 |
11.83% |
|
Urea ↑ |
36 |
11.21% |
|
Serum sodium ↑ |
42 |
13.08% |
|
Serum potassium↓ |
42 |
13.08% |
|
Urinalysis -albuminuria+ -hematuria+ |
96 |
29.90% |
|
38 |
11.83% |
|
|
Urine culture with female + |
104 |
32.29% |
Table IV: Laboratory Special Tests
|
Rennin plasmatic↑ |
121 |
37.69% |
|
Vanillyl Mandelic Acid testing (VMA): in urine↑ |
18 |
5.60% |
|
Catecholamine urine↑ |
18 |
5.60% |
|
Cortisol urine ↑ |
9 |
2.80% |
|
Cortisolemia ↑ |
9 |
2.80% |
|
TSH ↑ |
16 |
4.98% |
|
T3 ↑ |
16 |
4.98% |
|
T4 ↑ |
16 |
4.98% |
|
CT abdominal |
114 |
35.51% |
|
RMN abdominal |
158 |
49.92% |
|
Intravenous urogrography |
102 |
31.77% |
Observations on Eye Exam and Retinopathy [The eye ground (eye ground findings)]
Clearly, the most helpful information to have when one is attempting to establish the chronicity of hypertension is past blood pressure readings. Unfortunately, these are by no means always available since routine blood pressure measurement in young adults is not yet uniformly obtained. In the absence of prior readings, one needs to look for evidence of target organ damage that may suggest chronicity. In adolescent with even severe chronic hypertension or hypertensive encephalopathy. In my study this changes appear for the optic fund may show no more than retinal arteriolar narrowing in 103 cases represent 32.09% and arterio-venous nicking in 98 cases represent 30.53%, hemorrhages and exudates I rarely found in 9 cases represent 2.8%, papilla edema may be absent except in 2 cases even when hypertension was very severe more than 200/120 mmHg with complications of encephalopathy and in 109 cases represent 33.96 was normal result of eye ground examination. See Table V and Fig. 2
Just as there may be minimal eye ground findings, there are infrequently cardiac findings that suggest chronicity.
Table V Distribution of Cases by Eye Exam Findings
|
Normal |
109 |
33.96% |
|
Arteriolar narrowing |
103 |
32.09% |
|
Arterio-venous nicking |
98 |
30.53% |
|
Exudates and hemorrhages |
9 |
2.80% |
|
Papilla edema |
2 |
0.62% |
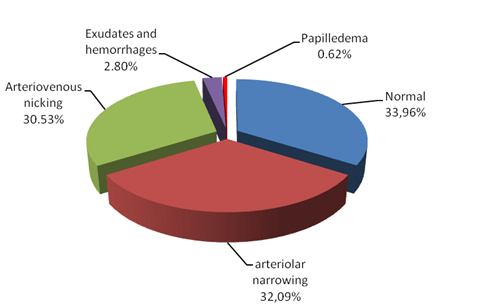
Fig. 2: Distribution of Cases by Changes of Eye Ground Findings
The heart morphology was not clinically enlarged in many cases and the ECG and chest X-ray were usually unhelpful in detecting left ventricular hypertrophy unless hypertension has been prolonged and severe. In my studies left ventricular hypertrophy was present in 35 cases (10.49%), they are helpful in determining chronicity of hypertension and in 206 cases (64.18%) left ventricular hypertrophy was absent. If negative suggesting nothing about the duration of hypertension. See Table VI and Fig 3
Table VI: Distribution of Cases by Changes in Chest X-Ray
|
Normal |
206 |
64.18% |
|
Elongation and elevated of left inferior arcos |
99 |
30.85% |
|
Cardiomegaly |
12 |
3.73% |
|
Aneurism of thoracic aorta |
4 |
1.24% |
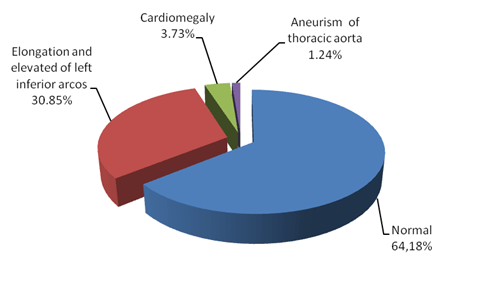
Fig. 3: Distribution of Cases by Changes of chest X-Ray
The echocardiography seems to be more sensitive for evaluating chamber size and wall thickness than the ECG and can be helpful. Left atria hypertrophy and left ventricular hypertrophy (Sokolow -Lyon index) and left axial deviation was possible to detect. In my studies I found 35 cases (10.49%) with LVH, 36 cases (11.21%) with LAH and 35 cases (10.49%) with left axial deviation. Secondary changes of depolarization like ST segment sub elevated and negative T wave I found in 35 cases represent 10.49%. See Table VII and Fig. 4
Table 7: Distribution of Cases by Changes in ECG
|
Normal |
180 |
56.07% |
|
Left axial deviation> -30 |
35 |
10.90% |
|
Left atria hypertrophy |
36 |
11.21% |
|
Left ventricular hypertrophy Sokolov -Lyon index(SV1+RV5/V6>35mm) |
35 |
10.90% |
|
Secondary changes of depolarization – ST segment sub elevated and T wave negative |
35 |
10.90% |
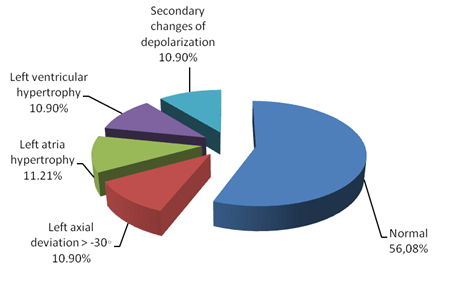
Fig. 4: Distribution of Cases by Changes in ECG
Table VIII: Distribution of cases by Echocardiography of Hearth Examination
|
Normal |
226 |
70.40% |
|
Left ventricular hypertrophy |
40 |
12.46% |
|
Ejection fraction(FE) of left ventricular<55% |
27 |
8.41% |
|
Aortic coarctation |
28 |
8.72% |
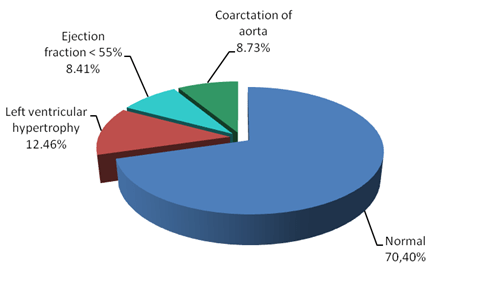
Fig. 5: Distribution of cases by Changes in Echocardiography
Table IX: Distribution of Cases by Urine Analysis Results
|
Normal |
187 |
58.27% |
|
Proteinuria |
96 |
29.90% |
|
Hematuria |
38 |
11.83 % |
Proteinuria I detect in 96 cases (29.90%) and hematuria in 38 cases (11.83%). See Fig. 6
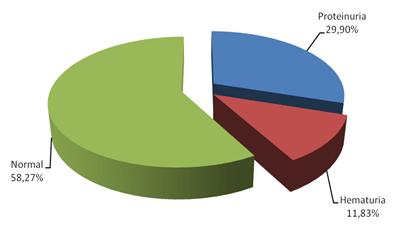
Fig.6: Distribution of cases by Urine Analysis Results
OMS stadialization classification high blood pressure in three stages. In my study about hypertension in the young adults, the results are as follows:
- Stages I: 270 cases represents 84.11%,
- Stages II: 40 cases represents 12.46%,
- Stages III: 9 cases (2.80%) and
- Stage IV: malign hypertension 2 cases represents 0.62%.
See, Table IX and Fig.7
Table IX: Distribution of Cases by Stadialization
|
Stages I |
270 |
84.11% |
|
Stages II |
40 |
12.46% |
|
Stages III |
9 |
2.81% |
|
Stages IV |
2 |
0.62% |
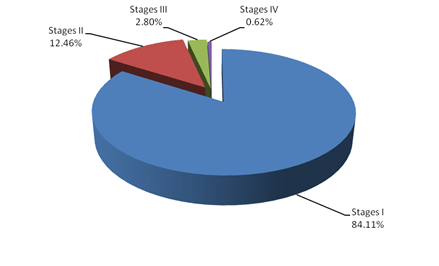
Fig. 7: Distribution of Cases by Stadialization
DISCUSSION
1. A 1/5 of group of patients studied have in family antecedents of young hypertensive family member with the following diseases:
- stroke 46 cases (14.33%),
- myocardial infarction 55 cases (17.13%),
- peripheral vascular disease 23 cases (7.16%),
- obesity 38 (11.83%),
- pre-eclamptic toxemia 31 cases (9.65%),
- hiperaldosteronism in 18 cases (5.60%),
- polycystic kidney 26cases (8.09%),
- multiple endocrine diseases II 14 cases (4.36%).
These results are in concordance with observations of Kotchen JM [1] which in a studies about young hypertensive patients concluded that family aggregation of hypertension was very frequent 20.2% (p<0,001) suggesting the importance of a genetic factor in the etiology of hypertension in the young adults.
2. An important number of hypertensive young patients were present in personal pathological antecedents: Scarlatti 27 (8.41%), repetitive angina with Streptococcus β hemolytic group A 88 (27.41%),chronic ORL infection focus 35 (10.90%) chronic stomathological focus infections 19 (5.91%), nephritis 34 (10.59%), endocrine disorders 16 (4.98% ), physical and psychical supra solicitation 22 (6.85%), head trauma 11 ( 3.42% ), therapy with corticosteroizi from another disease (for example erithematous systemic lupus) 5 (1.55%) therapy with AINS drugs 21 (6.54%), use decongestion nasal 4 (1.24%) repetitive urinary tract infection 28 (8.72%), syphilis 11 (3.42%)(p<0,001). Loggie JMH [2] in a studies with hypertension in the young reported the streptococcus infection with Streptococcus β hemolytic group A was 18.2% , chronic ORAL infection focus was 8.9%, chronic stomathological focus infections was 3.98%, glomerulonephritis was 6.2% and physical and psychical supra solicitation was 12.43% in personal pathological antecedents.
3. Changes of retinal vascular were insufficiently studied in young adults. In my study this changes appear for the optic fund may show no more than retinal arteriolar narrowing 103 cases represent 32.09% and arterio venous nicking 98 cases represent 30.53% , hemorrhages and exudates I rarely found from 9 cases represent 2.8%, papilla edema may be absent except 2 cases even with hypertension was very severe more than 200/120mmHg and complicate with encephalopathy and 109 cases represent 33.96% was normal result of funduoscopic examination (p<0.001).
Skalina MEL et al. [3] observations: 281 hypertensive young patients 140 have changes for the optic fund arterio venous nicking 93 cases, hemorrhages found from 7 cases and exudates appear from 40 patients. 141 patients have the optic fund examination normal.
4. The heart is not often clinically enlarged and the ECG and chest X-ray are usually unhelpful in detecting left ventricular hypertrophy unless hypertension has been prolonged and severe. In my studies left ventricular hypertrophy was present in 35 cases (10.49%), they are helpful in determining chronicity of hypertension and from 206 cases (64.174%) left ventricular hypertrophy was absent, that suggest that if negative, they tell one nothing about the duration of hypertension. The results are in concordance with observation with Laird WP and Fixler DE [4] who reports after performing chest X-ray for 210 young hypertensive, 103 have normal results, 78 have elongation and elevated of left inferior arcos and 29 present’s cardiomegaly.
5. The echocardiogram seems to be more sensitive for evaluating chamber size and wall thickness than the ECG and can be helpful. Left atria hypertrophy and left ventricular hypertrophy (Sokolow-Lyon index) and left axial deviation it’s possible to detect. In my studies I found 35 cases (10.49%) with LVH, 36 cases (11.21%) with LAH and 35 cases (10.49%) with left axial deviation. Secondary changes of depolarization like ST segment sub elevated and negative T wave I found from 35 cases represent 10.49% (p<0,001).The results are in concordance with observation with Laird WP and Fixler DE [4], who reports than 18% from young hypertensive subject, presents left ventricular hypertrophy detected after echocardiography examination, end in concordance with observation with Schieken RM et al. [5] in Muscatine studies who reports more than 14% from young hypertensive subjects have left ventricular hypertrophy after make echocardiography examination.
6. Proteinuria I detect in 96 cases (29.90%) and hematuria in 38 cases (11.83%).This changes appear in context of acute glomerulonephritis and hypertension was secondary renal.
Schmider et al. [6] sustained that glomerular hyperfiltration is a early marker for nefroangiosclerosis and a sign for subclinical organ affected.
7. OMS stadialization classification high blood pressure in three stages. In my study about hypertension in young adults the results are: in stages I found 270 cases represents 84.11%, in stages II 40 cases represents 12.46%, in stages III 9 cases (2.80%) and malign hypertension 2 cases represents 0.62%.
CONCLUSIONS
- 1. Importance of genetic factors in etiologies of disease is suggested that family aggregation of hypertension in young adults and another familial diseases like hyperaldosteronism, polycystic kidney and multiple endocrine diseases II.
- 2. Importance of personal pathologic antecedents demonstrated in my study that repetitive Streptococcus angina with Streptococcus β hemolytic group A was found in the first place as a cause of hypertension in the young people in context of acute streptococcal renal parenchymatous diseases.
- 3. Except nonspecific symptoms of high blood pressure exist specifically symptoms who suggest etiology of hypertension with young people.
- 4. The fundoscopic findings in the young adult with hypertension are frequently normal. In the absence of prior readings, one needs to look for evidence of target organ damage that may suggest chronicity. In my study this changes appear for 86 cases 23.3 % and hemorrhages and exudates I rarely found from 9 cases represent 2.8% and papilla edema may be absent except 2 cases even with hypertension is very severe more than 200/120mmHg and complication of encephalopathy.
- 5. Left ventricular hypertrophy is possible to detect X-ray, ECG and echocardiography. In my studied I detected left ventricular hypertrophy from 35 patients represent 10.49%.
- 6. Proteinuria 96 cases (29.90%) have two significance: nephropathy complication of high blood pressure, or etiology in context or glomerulonephritis alone or accompaniment with hematuria 38 cases (11.83%) in nephritis syndrome.
- 7. Renin plasmatic level is very important marker of high blood pressure in the young. Was high in 121 cases (37.69%).This situation suggests that hypertension in the young is hiperreninemic hypertension in many cases because young adults have hyperactivity of sympatetic nervous system.
- 8. OMS classification evaluated stages I 270 cases (84.11%), stages II 40 cases (12.46%) in stages III 9 cases (2.80%) and malign hypertension (stages IV) 2 cases (0.62%)
- 9. Finally I make a small guideline about hypertension with young patients group of ages 18-35, which I hope to help activity of every physician indifferent specialties in your practice, to use for diagnosis and easy work.
REFERENCES
1. Kotchen JM “Effect of relative weight on familial blood pressure aggregations“ Am J Epidemiol.1987 105-214.
2. Loggie JMH. “The diagnostic evaluation of adolescents with hypertension.” In Hunt JC, Dreifus LS, Dustan HP et al, eds Dialogues in Hypertension Update II vol 1. Lyndhurst, NJ: Health Learning Systems 1984:43-56.
3. Skalina MEL et al.: Annable WL, Kleigman RM, Fanaroff AA “ Hypertensive retinopathy in the adolescent“ J Adolesc. 1983:103:781-6.
4. Laird WP and Fixler DE. “Left ventricular hypertrophy in adolescents with elevated blood pressure: assessment by chest roentgenography, electrocardiography and echocardiography.” Adolescents 2001;67:255-9.
5.Schieken RM and coauthors: Clarke WR, Lauer RM, “Left ventricular hypertrophy in the young with blood pressures in the upper quin-tile of the distribution: the Muscatine study.” Hypertenesion 2004;3:669-75.
6. Schmider and coauthors: Messerli FH, Garavaglia GE, Nunez BD “Glomerular hyperfiltration indicates target organ disease in essential hypertension.” Circulation 2003; 76: III-273.
Follow Blog via Email
Join 2,056 other subscribers-
Recent Posts
- Grok thinks like PhDs – Hybrid Model for Autonomous Update of Doctoral Dissertations with Original PhD Student Author editing and acceptance of Grok’s updated output. 3rd Joint article, a pilot study for Validation of an Autonomous Journal Articles Updating System (AJAUS) tested on Autonomous Update of Aviva Lev-Ari, PhD, RN Doctoral Thesis, UC, Berkeley, 1983. January 31, 2026
- 2026 World Economic Forum, 1/19 – 1/23/2026, Davos, Switzerland, LPBI Group’s KOLs interpretation of AI in Health Videos January 24, 2026
- Evolving LPBI Group’s Portfolio of Intellectual Properties (IP): From 2021 Vision to 2026 Reality January 12, 2026
- Aviva Lev-Ari, PhD, RN – Biography ->> Grokepedia Entry January 11, 2026
- List of Articles included in the Article SELECTION from Collection of Aviva Lev-Ari, PhD, RN Scientific Articles on PULSE on LinkedIn.com for Training Small Language Models (SLMs) in Domain-aware Content of Medical, Pharmaceutical, Life Sciences and Healthcare by 15 Subjects Matter January 10, 2026
- Article SELECTION from Collection of Aviva Lev-Ari, PhD, RN Scientific Articles on PULSE on LinkedIn.com for Training Small Language Models (SLMs) in Domain-aware Content of Medical, Pharmaceutical, Life Sciences and Healthcare by 15 Subjects Matter January 10, 2026
- Collection of Aviva Lev-Ari, PhD, RN Scientific Articles on PULSE on LinkedIn.com January 10, 2026
- The youngest leader in AI in Health: Tanishq Mathew Abraham, Ph.D. (@iScienceLuvr) January 8, 2026
- 2026 Grok Multimodal Causal Reasoning on Proprietary Cariovascular Corpus: From 2021 Wolfram NLP Baseline to Thousands of Novel Relationships – A Second Head-to-Head Validation of LPBI’s Domain-Aware Training Advantage January 6, 2026
- Workflow for Dynamic Linkage and Transition between two Authoring Systems: LPBI Group’s WordPress.com Multi-Authors Authoring System and Microsoft PowerPoint product for Slide show presentation – Part 10.1 in Composition of Methods January 6, 2026
Archives
Categories
Meta