Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
Remote control of hormone release using magnetic nanoparticles
Reporter: Irina Robu, PhD
Depression and post-traumatic stress disorder can increase abnormal levels of stress hormones such as adrenaline and cortisol. Adrenaline and cortisol are steroids hormones, produced in the adrenal glands and is released into the blood stream and serve as chemical mediators. Scientists at MIT invented a way to remotely control the release of these hormones from the adrenal gland, using magnetic nanoparticles.
Magnetic nanoparticles are nanoparticles consist of magnetic elements such as iron, nickel, cobalt, chromium, manganese, gadolinium and their chemical compounds. These nanoparticles are super magnetic due to their nanoscale size and can be selectively attached to a functional molecule and allow transportation to a targeted location under external magnetic field from an electromagnet. In an effort to avert aggregation and minimize the interaction of particles with the system environment.
This method can aid researchers to study more about how hormone release influences mental health and can ultimately bargain a new way to treat hormone-linked disorders. To obtain a control over hormone release Dekel Rosenfeld, an MIT-Technion postdoc has developed specialized magnetic nanoparticles that can be injected into the adrenal gland. When exposed to a weak magnetic field, the particles heat up slightly, activating heat-responsive channels that trigger hormone release. This technique can be used to stimulate an organ deep in the body with minimal invasiveness.
In the new study, the exploration team desired to discover the idea of treating disorders of the brain by manipulating organs that are outside the central nervous system but impact it through hormone release. Hormones secreted by the adrenal gland, including cortisol and adrenaline, play vital roles in depression, stress, and anxiety.
The researchers decided on ion channels that control the flow of calcium into adrenal glands as a target to stimulate hormone release. When calcium flows through the open channels into adrenal cells, the cells begin pumping out hormones. To stimulate these heat-sensitive channels, scientists designed nanoparticles made of magnetite. In rats, they found these particles could be injected directly into the adrenal glands and remain there for at least six months. When the rats were exposed to a weak magnetic field—about 50 millitesla (100 times weaker than the fields used for MRI), the particles heated up by about 6 degrees Celsius, enough to activate the calcium channels to open without damaging any surrounding tissue.
TRPV, the heat-sensitive channel that they targeted found in numerous sensory neurons throughout the body, including pain receptors. TRPV1 channels can be activated by capsaicin as well as by temperature and are found across mammalian species.This stimulation triggered a hormone rush, doubling cortisol production and boosting noradrenaline by about 25 percent which can lead to a measurable increase in the animals’ heart rates.
The investigators are now planning to use this method to investigate how hormone release affects PTSD and other disorders, and this technique would propose a much less invasive alternative to potential treatments that include implanting a medical device to electrically stimulate hormone release, which is not practicable in organs such as the adrenal glands that are soft and highly vascularized.
When Will Life Be Normal Again? We Just Don’t Know
Reporter: Joel T. Shertok, PhD
Many Americans have been living under lockdown for a month or more. We’re all getting antsy. The president is talking about a “light at the end of the tunnel.” People are looking for hope and reasons to plan a return to something — anything — approximating normalcy. Experts are starting to speculate on what lifting restrictions will look like. Despite the relentless, heroic work of doctors and scientists around the world, there’s so much we don’t know.
We don’t know how many people have been infected with Covid-19.
We don’t know the full range of symptoms.
We don’t always know why some infections develop into severe disease.
We don’t know the full range of risk factors.
We don’t know exactly how deadly the disease is.
We don’t have answers to more detailed questions about how the virus spreads, including: “How many virus particles does it even take to launch an infection? How far does the virus travel in outdoor spaces, or in indoor settings? Have these airborne movements affected the course of the pandemic?”
We don’t know for sure how this coronavirus first emerged.
We don’t know how much China has concealed the extent of the coronavirus outbreak in that country.
We don’t know what percentage of adults are asymptomatic. Or what percentage of children are asymptomatic.
We don’t know the strength and duration of immunity. Though people who recover from Covid-19 likely have some degree of immunity for some period of time, the specifics are unknown.
We don’t yet know why some who’ve been diagnosed as “fully recovered” from the virus have tested positive a second time after leaving quarantine.
We don’t know the long-term health effects of a severe Covid-19 infection. What are the consequences to the lungs of those who survive intensive care?
We don’t yet know if any treatments are truly effective. While there are many therapies in trials, there are no clinically proven therapies aside from supportive care.
We don’t know for certain if the virus was in the United States before the first documented case.
We don’t know when supply chains will strengthen to provide health care workers with enough masks, gowns and face shields to protect them.
In America, we don’t know the full extent to which black people are disproportionately suffering. Fewer than a dozen states have published data on the race and ethnic patterns of Covid-19.
We don’t know if people will continue to adhere to social distancing guidelines once infections go down.
We don’t know when states will be able to test everyone who has symptoms.
We don’t know if the United States could ever deploy the number of tests — as many as 22 million per day — needed to implement mass testing and quarantining.
We don’t know if full-scale serological testing will accurately determine immunity.
We don’t know if we can implement “test and trace” contact tracing at scale.
We don’t know whether smartphone location tracking could be implemented without destroying our privacy.
We don’t know if or when researchers will develop a successful vaccine.
We don’t know how many vaccines can be deployed and administered in the first months after a vaccine becomes available.
We don’t know how a vaccine will be administered — who will get it first?
We don’t know if a vaccine will be free or costly.
We don’t know if a vaccine will need to be updated every year.
We don’t know how, when we do open things up again, we will do it.
We don’t know if people will be afraid to gather in crowds.
We don’t know if people will be too eager to gather in crowds.
We don’t know what socially distanced professional sports will look like.
We don’t know what socially distanced workplaces will look like.
We don’t know what socially distanced bars and restaurants will look like.
We don’t know what a general election in a pandemic will look like.
We don’t know when schools will reopen.
We don’t know what a general election in a pandemic will look like.
We don’t know what effects lost school time will have on children.
We don’t know if the United States’s current and future government stimulus will stave off an economic collapse.
We don’t know whether the economy will bounce back in the form of a “v curve”
Or whether it’ll be a long recession.
Or whether it’ll be a Great Depression.
Or whether it’ll be a “Greater Depression.”We don’t know when we might be able to return to a new normal.We don’t know when any of this will end for good.There is, at present, no plan from the Trump White House on the way forward.
As an umbrella organization we feel obliged to take action in the outbreak of the COVID-19 in the developing world. In order to address if and how the Israeli and Jewish aid community should act and understand the needs of the developing world. The agenda included a short review from executives in international organizations, leading institutions in the developing world, and various civil society and business representatives in Israel who are active in the developing world The webinar was moderated by
Dr Bruria Adini- head of the Department of Emergency Management and Disaster Medicine in the Tel Aviv University
Was listening to SID Israel preparatory information session on COVID-19 preparations for developing countries from March 31, which is centuries ago in the development of this crisis.
Reminder Europe was in a crisis, the USA and the UK were showing a sign they will join but not have quiet caught up.
WATCH VIDEO
with historical perspectives a first world – developing world perspective is no longer relevant in many ways. Some of the issues that were raised in way the “first” world was reacting to the shock the situation has caused the European nations were affecting smaller nations within Europe already; yet the intensity of the situation and the speed this crisis is developing has not allowed us to free our minds to understand it.
While Europe has suffered dramatically, and Spain, Italy and France are at the heat of the pandemics Europe has not come to it as a unified community/country and the outcome of which are already staggering, The “brutal fight” for protective gear and all kind of panic based measures taken by countries such as Germany, have caused havoc in countries in Europe that are mostly dependent on neighbor countries for their supplies in what looked like the open borders of Europe.
The evidence for this is not in cries from these countries but in the numbers: San Marino is the country with the highest death and illness rates (per Million) in Europe, 5-20 times the numbers of surrounding Italy, and So is Andorra, Luxembourg, Gibraltar, Monaco and even Liechtenstein, be it masks, tests or other measures that where missing, be it sanitation, disinfection or missing food essentials that depended on neighboring countries the outcomes are still outrageous.
Outside of this there are major challenges that developing countries are facing in some of the paradigms regardless of the major impacts of border closures, flight restrictions, custom restrictions and general crisis based regulation and bureaucratic hurdles added to normal limitations of working over borders
Some issues raised were issues of cultural and economical differences but to many of those the solutions are those that were already worked before: collaboration on community level across organizations and aid sectors, exchange of information, and working with local leadership
the panel was in a way on putting borders between humanity and virus and not between us human.
It was meant as a brain-storm and not a lecture.
The rep of WHO Europe HQ in Denmark shared their sometimes frustration over border limits and human/supply movement amid urgent need as well as the price war between countries and organizations.
But had pride in their success in putting together efforts and using long term relations to overcome and set up regional labs as preparatory measure.
Covid-19 is a challenge since it so far hit the hardest in Europe and the USA the epicenters of humanitarian aid and understanding that there is a “we are all in it together” takes a bigger perspectives (e.g. we have to dea with covid 19 in prisons and detention centers, refugee camps and other “off the map” places even in the US-Mexico borders, across war borders and in communities of great marginalization.
Yet often a small effort can make miracles, an advice on who to talk to and who to work with on a school, religion, community leadership can be more important then a box of gloves.
Another issue is the balance of disease mitigation in a community with zero margins on the hunger front, with a hard balance on the sanitation issues nad the innability to inflict stricter clossure on the camps that are already suffering form over closures to the brink of disaster.
I recommend listening albeit long discussion, you may skip the first ten mins intro if short in time.
Worldwide trial uses AI to quickly identify ideal Covid-19 treatments
Reporter : Irina Robu, PhD
The novel coronavirus, SARS-CoV-2 that has been spreading around the world can cause a respiratory illness that can be severe. The disease, COVID-19 appears to have a fatality rate of less than 2 percent and forcing doctors to choose between two equally revolting options: try an unproven therapy and anticipate that it works or treat patients with standard supportive care for severe respiratory disease until a vaccine is developed.
Currently, randomized controlled trials have started in dozens of hospitals around the world by fusing two approaches together, using artificial intelligence to home in or using the most effective treatments for respiratory infections. The randomized trials, also known as an adaptive trial, in which scientists adjust the treatment protocols and/or statistical procedures based on the outcomes of participants. The trials are seen as a way to detect promising treatments and brand trials more flexible than traditional randomized trials and force patients, trial sponsors to wait for an outcome that often turns out to be disappointing. The inadequacies of the randomized approach have been taken into sharp relief during the pandemic, as thousands of patients can’t wait for gold-standard science to play out as they lay dying in intensive care of units.
However, analyzing data from more than 50 hospitals, researchers hope to supply quick answers to pressing questions such as the fact that the antimalarial drug hydroxychloroquine is an effective therapy and, if so, for which types of patients. The trial will also allow the researchers to test multiple therapies at once. Since the approach seems reasonable to give answers during a pandemic, it still has a lot of challenges, plus the necessity to rapidly assemble and analyze data from several hospitals with various record-keeping systems on three continents. Then update the protocols in accord during a crisis that is draining clinical resources.
Since several treatments are being tested, carrying out these trials is predominantly complicated. But progress in computing resources required to share data and analyze it swiftly using artificial intelligence have started to make these designs more practical.
The World Health Organization and the U.S. Food and Drug Administration, along with groups like the Gates Foundation, have offered increasing support for adaptive trial designs in recent years, particularly as a way to evaluate therapies during epidemics.
Nonetheless that doesn’t mean this specific effort is going to yield results in time to save the first wave of extremely ill patients. Once a promising treatment is recognized more patients will be allocated to receive it during each successive round of therapy. So far, about 130 ICU patients with Covid-19 have been enrolled, furthermore to hundreds of other hospitalized patients.
The goal in the REMAP-CAP trial, once all the trial sites are up and running, is to analyze results and change treatments on a weekly basis.
Recombinant Coronavirus Vaccines Delivered via Microneedle Array
Curator: Irina Robu, PhD
Coronavirus is an evolving pathogen with exponentially increasing significance due to the high case fatality rate, the large distribution of reservoir, and the lack of medical countermeasures. The public health emergencies triggered by coronaviruses, including SARS-CoV and SARS-CoV-2, obviously validate the urgency to assess candidate vaccines to fight these outbreaks. Continuous research contributes to the efforts of scientists to quickly progress safe vaccines against these developing infections. The recent COVID-19 pandemic indicates a vital need for the rapid design, production, testing, and clinical translation of candidate vaccines.
Coronavirus virus particles contain four main structural proteins. These are the spike, membrane, envelope, and nucleocapsid proteins, all of which are encoded within the 3′ end of the viral genome. Coronaviruses contain a non-segmented, positive-sense RNA genome, which contains a 5′ cap structure along with a 3′ poly (A) tail, allowing it to act as a mRNA for translation of the replicase polyproteins. The replicase gene encoding the nonstructural proteins inhabits two-thirds of the genome, which make up only about 10 kb of the viral genome. The 5′ end of the genome contains a leader sequence and untranslated region that encompasses multiple stem loop structures required for RNA replication and transcription. Furthermore, at the start of each structural gene are the transcriptional regulatory sequences that are essential for expression of each of these genes.
Researchers at U of Pittsburg generated codon optimized MERS-S1 subunit vaccines fused with a foldon trimerization domain to mimic the native viral structure. They engineered immune stimulants (RS09 or flagellin, as TLR4 or TLR5 agonists) into this trimeric design and tested the pre-clinical immunogenicity of MERS-CoV vaccines in mice, distributed subcutaneously by needle injection or intracutaneously by dissolving microneedle arrays by assessing virus specific IgG antibodies in the serum of vaccinated mice by ELISA and using virus neutralization assays.
Microneedle array mediated immunization has several mechanistic differences from traditional intramuscular needle injections, which could clarify the variations in the magnitude and kinetics of the ensuing responses. Due to the urgent need for COVID-19 vaccines, they used this approach to quickly advance MNA SARS-CoV-2 subunit vaccines and tested their pre-clinical immunogenicity in-vivo by manipulating the previous research on MNA MERS-CoV vaccines.
Even though it is still premature to predict whether humans immunized with these vaccine candidates will have similar responses and be protected from SARS-CoV-2 infections, their previous research show that development, production, and initial animal testing of clinically translatable MNA vaccine candidates against SARS-CoV-2. Incidentally it will be vital to determine whether antibodies from MNA-SARS-CoV-2 immunized animals will neutralize virus infectivity.
Finally, we note that the immunogenicity differences between MNA coronavirus vaccines and coronavirus vaccines delivered by traditional needle injection that we observe will need to be evaluated in clinical trials to establish the clinical advantages of MNA delivery.
SOURCE
E. Kim et al., Microneedle array delivered recombinant coronavirus vaccines: Immunogenicity and rapid translational development, EBioMedicine (2020).
Fehr, Anthony R, and Stanley Perlman. Coronaviruses: an overview of their replication and pathogenesis. Methods in molecular biology, vol. 1282 (2015): 1-23.
Susan R. Weiss, Sonia Navas-Martin. Coronavirus Pathogenesis and the Emerging Pathogen Severe Acute Respiratory Syndrome Coronavirus. Microbiology and Molecular Biology Reviews Dec 2005, 69 (4) 635-664.
Asset Class I-X, Type, Quantity, Business Model, Protection, Transaction Type, Unique Value Proposition, Key Paying Customers, Key Stakeholders and Unique Selling Point
Author: Aviva Lev-Ari, PhD, RN
Asset
Classes
Type
Quantity
Business Model
Asset Protection
Transaction Type
Asset Class I
The Journal 3/3/2020 Views 1,723,051
5,742 articles on 3/3/2020
Valuation [$40M] done by Joel on Alex WP Data
Revenue Potential: Partnership Programs – Subscription/Access fee Legal and Pharma, free for Academia
Revenue Potential: Partnership Programs – Subscription/Access fee Legal and Pharma, free for Academia
Copyright Law
B2B & B2B & B2C
Asset Class IV
Platform, composition of methods and workflows for the content creation of scientific curations
TBD
Customized Platform Infrastructure, Building Tools for new products, venturing to new Disciplines beyond HealthCare,knowhow contracts in new geographies
Copyright Law and Proprietary Knowhow
internal and contracts
Asset
Classes
Type
Quantity
Business Model
Asset Protection
Transaction Type
Asset Class V
Gallery of Biological Images in use in Articles and Books
TBD
Artifacts in the of Content Creation of PRIOR ART
Copyright upon EMBEDDED
in original curations
Internal Use – subsets per BioMed e- Series in Medical Specialties
Asset Class VI
Team of Experts
BIOs Final Improvement Team (FIT)
Factor of Content Creation
Personal Agreement s to become Employment Contracts Post-Exit
Internal
Asset Class VII
Royalties on BioMed e- Series:Page downloads, Book borrowings and Book sale
111,645 page downloads in total on 3/9/2020
Current Account Receivables
Royalties Agreement with KDP
@Amazon
Derivative of Interest in Content (120,000
Pages download in 16 books
Asset Class VIII
Subscribers to the Website
2,554 on 3/29/2020
Potential Account Receivables
n/a
Drivers of Loyalty & Success
Asset Class IX
INTANGIBLE ASSETS
& Intrinsic Value = Good Will
TBD
Potential Account Receivables
Copyright Law
External
e-Reputation
Asset Class X
e-VOICE PODCASTS
Audio Library
TBD
Potential Account Receivables
Copyright Law
B2B & B2B & B2C
Asset
Classes
Type
Quantity
Business Model
Asset Protection
Transaction Type
Asset Classes
Unique Value Proposition
Key Paying Customers
Key Stakeholders
Unique Selling Point
Asset Class I
We create a new level of knowledge that is current and lively on the current issues and based on a discussion of multiple KOL
in depth as of day of publication knowledge collection of topic, background, good as a course or a journal club guide. State of the art, science based, outcome oriented KOL based perspective.
Legal, regulatory, pharma R&D, non academia, Gov, journalists and media, premium audience
Universities, Patient advocacy groups, Professional associations, Curriculum developers
current highly multiple domain specialized accessible knowledge
Asset Class III
In depth on publication day, knowledge collection of topic, depicts event spirit and highlights with KOL perspective and annotation, scientific documents and historical state of Science
Global Biotech & Healthcare Conference Organizers + Customers of Asset Class I+II
platform that allow harnessing the state of knowledge to produce a state of the art coverage of eventual or topic based current knowledge products to a specific targeted audience
New topics, new geographies knowledge community makers, LPBI new products pipeline
the global KOL community in health, life- sciences and pharma
unique, easy, proven, state of the art
Transaction Type
Unique Value Proposition
Key Paying Customers
Key Stakeholders
Unique Selling Point
Asset Class V
Selection done by Domain Experts for IP creation of original content
Article ID #273: Live Notes and Conference Coverage in Real Time. COVID19 And The Impact on Cancer Patients Town Hall with Leading Oncologists; April 4, 2020. Published 4/4/2020
This update is the video from the COVID-19 Series 4.
UPDATED 4/08/2020 see below
The Second in a Series of Virtual Town Halls with Leading Oncologist on Cancer Patient Care during COVID-19 Pandemic: What you need to know
The second virtual Town Hall with Leading International Oncologist, discussing the impact that the worldwide COVID-19 outbreak has on cancer care and patient care issues will be held this Saturday April 4, 2020. This Town Hall Series is led by Dr. Roy Herbst and Dr. Hossain Borghaei who will present a panel of experts to discuss issues pertaining to oncology practice as well as addressing physicians and patients concerns surrounding the risk COVID-19 presents to cancer care. Some speakers on the panel represent oncologist from France and Italy, and will give their views of the situation in these countries.
Speakers include:
Roy S. Herbst, MD, PhD, Ensign Professor of Medicine (Medical Oncology) and Professor of Pharmacology; Chief of Medical Oncology, Yale Cancer Center and Smilow Cancer Hospital; Associate Cancer Center Director for Translational Research, Yale Cancer Center
Hossain Borghaei, DO, MS , Chief of Thoracic Medical Oncology and Director of Lung Cancer Risk Assessment, Fox Chase Cancer Center
Giuseppe Curigliano, MD, PhD, University of Milan and Head of Phase I Division at IEO, European Institute of Oncology
Paolo Ascierto, MD National Tumor Institute Fondazione G. Pascale, Medical oncologist from National Cancer Institute of Naples, Italy
Dr. Jack West from City of Hope talked about telemedicine: Coordination of the patient experience, which used to be face to face now moved to a telemedicine alternative. For example a patient doing well on personalized therapy, many patients are well suited for a telemedicine experience. A benefit for both patient and physician.
Dr. Rohit Kumar: In small cancer hospitals, can be a bit difficult to determine which patient needs to come in and which do not. For outpatients testing for COVID is becoming very pertinent as these tests need to come back faster than it is currently. For inpatients the issue is personal protection equipment. They are starting to reuse masks after sterilization with dry heat. Best to restructure the system of seeing patients and scheduling procedures.
Dr. Christopher Manley: hypoxia was an issue for COVID19 patients but seeing GI symptoms in 5% of patients. Nebulizers have potential to aerosolize. For patients in surgery prep room surgical masks are fine. Ventilating these patients are a challenge as hypoxia a problem. Myocarditis is a problem in some patients. Diffuse encephalopathy and kidney problems are being seen. So Interleukin 6 (IL6) inhibitors are being used to reduce the cytokine storm presented in patients suffering from COVID19.
Dr. Hope Rugo from UCSF: Breast cancer treatment during this pandemic has been challenging, even though they don’t use too much immuno-suppressive drugs. How we decide on timing of therapy and future visits is crucial. For early stage breast cancer, neoadjuvant therapy is being used to delay surgeries. Endocrine therapy is more often being used. In patients that need chemotherapy, they are using growth factor therapy according to current guidelines. Although that growth factor therapy might antagonize some lung problems, there is less need for multiple visits.
For metastatic breast cancer, high risk ER positive are receiving endocrine therapy and using telemedicine for followups. For chemotherapy they are trying to reduce the schedules or frequency it is given. Clinical trials have been put on hold, mostly pharmokinetic studies are hard to carry out unless patients can come in, so as they are limiting patient visits they are putting these type of clinical studies on hold.
Dr. Harriet Kluger: Melanoma community of oncologists gathered together two weeks ago to discuss guidelines and best practices during this pandemic. The discussed that there is a lack of data on immunotherapy long term benefit and don’t know the effectiveness of neoadjuvant therapy. She noted that many patients on BRAF inhibitors like Taflinar (dabrafenib) or Zelboraf (vemurafenib) might get fevers as a side effect from these inhibitors and telling them to just monitor themselves and get tested if they want. Yale has also instituted a practice that, if a patient tests positive for COVID19, Yale wants 24 hours between the next patient visit to limit spread and decontaminate.
Marianne Davies: Blood work is now being done at satellite sites to limit number of in person visits to Yale. Usually they did biopsies to determine resistance to therapy but now relying on liquid biopsies (if insurance isn’t covering it they are working with patient to assist). For mesothelioma they are dropping chemotherapy that is very immunosuppressive and going with maintenance pembrolizumab (Keytruda). It is challenging in that COPD mimics the symptoms of COVID and patients are finding it difficult to get nebulizers at the pharmacy because of shortages; these patients that develop COPD are also worried they will not get the respirators they need because of rationing.
Dr. Barbara Burtness: Head and neck cancer. Dr. Burtness stresses to patients that the survival rate now for HPV positive head and neck is much better and leaves patients with extra information on their individual cancers. She also noted a registry or database that is being formed to track data on COVID in patients undergoing surgery and can be found here at https://globalsurg.org/covidsurg/
About CovidSurg
There is an urgent need to understand the outcomes of COVID-19 infected patients who undergo surgery.
Capturing real-world data and sharing international experience will inform the management of this complex group of patients who undergo surgery throughout the COVID-19 pandemic, improving their clinical care.
CovidSurg has been designed by an international collaborating group of surgeons and anesthetists, with representation from Canada, China, Germany, Hong Kong, Italy, Korea, Singapore, Spain, United Kingdom, and the United States.
Dr. Burtness had noted that healthcare care workers are at high risk of COVID exposure during ear nose and throat (ENT) procedures as the coronavirus resides in the upper respiratory tract. As for therapy for head and neck cancers, they are staying away from high dose cisplatin because of the nephrotoxicity seen with high dose cisplatin. An alternative is carboplatin which generally you do not see nephrotoxicity as an adverse event (a weekly carboplatin). Changing or increasing dose schedule (like 6 weeks Keytruda) helps reduce immunologic problems related to immunosupression and patients do not have to come in as often.
Italy and France
Dr. Paolo Ascierto: with braf inhibitors, using in tablet form so patients can take from home. Also they are moving chemo schedules for inpatients so longer dosing schedules. Fever still a side effect from braf inhibitors and they require a swab to be performed to ascertain patient is COVID19 negative. Also seeing pneumonitis as this is an adverse event from checkpoint inhibitors so looking at CT scans and nasal swab to determine if just side effect of I/O drugs or a COVID19 case. He mentioned that their area is now doing okay with resources.
Dr. Guiseppe Curigliano mentioned about the redesign of the Italian health system with spokes and hubs of health care. Spokes are generalized medicine while the hubs represent more specialized centers like CV hubs or cancer hubs. So for instance, if a melanoma patient in a spoke area with COVID cases they will be referred to a hub. He says they are doing better in his area
In the question and answer period, Dr. West mentioned that they are relaxing many HIPAA regulations concerning telemedicine. There is a website on the Centers for Connective Health Policy that shows state by state policy on conducting telemedicine. On immuno oncology therapy, many in the panel had many questions concerning the long term risk to COVID associated with this type of therapy. Fabrice mentioned they try to postpone use of I/O and although Dr. Kluger said there was an idea floating around that PD1/PDL1 inhibitors could be used as a prophylactic agent more data was needed.
Please revisit this page as the recording of this Town Hall will be made available next week.
UPDATED 4/08/2020
Below find theLIVE RECORDING and TAKEAWAYSby the speakers
Town Hall Takeaways
Utilize Telehealth to Its Fullest Benefit
· Patients doing well on targeted therapy or routine surveillance are well suited to telemedicine
· Most patients are amenable to this, as it is more convenient for them and minimizes their exposure
· A patient can speak to multiple specialists with an ease that was not previously possible
· CMS has relaxed some rules to accommodate telehealth, though private insurers have not moved as quickly, and the Center for Connected Health Policy maintains a repository of current state-by-state regulations: https://www.cchpca.org/
Practice Management Strategies
· In the face of PPE shortages, N95 masks can be decontaminated using UV light, hydrogen peroxide, or autoclaving with dry heat; the masks can be returned to the original user until the masks are no longer suitable for use
· For blood work or scans, the use of external satellite facilities should be explored
· Keep pumps outside of the room so nurses can attend to them quickly
· Limit the use of nebulizers, CPAPs, and BiPAPs due to risk of aerosolization
· Caution is urged in the presence of cardiac complications, as ventilated patients may appear to improve, only to suffer severe myocarditis and cardiac arrest following extubation
· When the decision is made to intubate, intubate quickly, as less invasive methods result in aerosolization and increased risks to staff
Study the Lessons of Europe
· The health care system in Italy has been reorganized into “spokes” and “hubs,” with a number of cancer hubs; if there is a cancer patient in a spoke hospital with many COVID patients, this patient may be referred to a hub hospital
· Postpone adjuvant treatments whenever possible
· Oral therapies, which can be managed at home, are preferred over therapies that must be administered in a healthcare setting
· Pneumonitis patients without fevers may be treated with steroids, but nasal swab testing is needed in the presence of concomitant fever
· Any staff who are not needed on site should be working from home, and rotating schedules can be used to keep people healthy
· Devise an annual epidemic control plan now that we have new lessons from COVID
We Must Be Advocates for Our Cancer Patients
· Be proactive with other healthcare providers on behalf of patients with a good prognosis
· Consider writing letters for cancer patients for inclusion into their chart, or addendums on notes, then encourage patients to print these out, or give it to them during their visit
· The potential exists for a patient to be physiologically stable on a ventilator, but intolerant of decannulation; early discussions are necessary to determine reasonable expectations of care
· Be sure to anticipate a second wave of patients, comprised of cancer patients for whom treatments and surgery have been delayed!
Tumor-Specific Learnings
Ø Strategies in Breast Cancer:
· In patients with early-stage disease, promote the use of neoadjuvant therapy where possible to delay the need for surgery
· For patients with metastatic disease in the palliative setting, transition to less frequent chemotherapy dosing if possible
· While growth factors may pose a risk in interstitial lung disease, new guidelines are emerging
· The use of BRAF/MEK inhibitors can cause fevers that are drug-related, and access to an alternate clinic where patients can be assessed is a useful resource
Ø Strategies in Lung Cancer:
· For patients who are stable on an oral, targeted therapy, telehealth check-in is a good option
· For patients who progress on targeted therapies, increased use of liquid biopsies when appropriate can minimize use of bronchoscopy suites and other resources
· For patients on pembrolizumab monotherapy, consider switching to a six-week dosing of 400 mg
· Many lung cancer patients worry about “discrimination” should they develop a COVID infection; it is important to support patients and help manage expectations and concerns
UPDATED 5/11/2020
Townhall on COVID-19 and Cancer Care with Leading Oncologists Series 4
Addressing the Challenges of Cancer Care in the Community
The second virtual Town Hall with Leading International Oncologist, discussing the impact that the worldwide COVID-19 outbreak has on cancer care and patient care issues will be held this Saturday April 4, 2020. This Town Hall Series is led by Dr. Roy Herbst and Dr. Hossein Borghaei who will present a panel of experts to discuss issues pertaining to oncology practice as well as addressing physicians and patients concerns surrounding the risk COVID-19 presents to cancer care. Some speakers on the panel represent oncologist from France and Italy, and will give their views of the situation in these countries.
This series is being hosted in partnership with Axiom Healthcare Strategies, Inc..
The Town Hall proceedings and live notes will be made available on this site and Live Notes will be Tweeted in Real Time using the #CancerCareandCOVID19 and @pharma_BI
The goal of these town halls is to improve outcomes of cancer patients across the globe, by sharing insights and lessons learned from oncologists fighting COVID-19. Dr. Roy Herbst and Dr. Hossein Borghaei will be joined by a panel of thought leaders with expertise in a variety of solid tumors to discuss how COVID-19 has impacted patient care in oncology.
Following the session, a video, transcript, and key takeaways will be released on Monday 4/6.
Time
For Live Notes From the Last Town Hall Meeting Specifically on Lung Cancer and COVID19 please go to
3D-Printed Brain Clear the Way to Find Cancer Treatments
Reported by: Irina Robu, PhD
Glioblastomas are aggressive and malignant grade IV brain tumors and can located wherever in the brain and do not regularly spread outside of the brain. Common symptoms patients with glioblastoma experience include headaches, seizures, confusion, memory loss, muscle weakness, visual changes, language deficit, and cognitive changes. Glioblastomas tend to affect older individuals (age 45 to 70) with rare occurrences in children. Treatment methods typically include a combination of surgery, chemotherapy, radiation therapy, and alternating electric fields therapy.
Scientists at Northwestern University developed a technique to study their fast spreading cancer using a 3D structure made of agglomeration of human brain cells and biomaterials, which can help doctors better understand how the tumor grows and speed up the potential discovery of novel drugs to fight it. A water-based substance serves as a matrix to hold the cells into place. However, inside the living brain, scientists can’t observe how the tumor cells grow or respond the treatment and they have to use mice/rats to understand tumor development. Animal studies are expensive and time consuming, but the 3D printed live tissue allows researchers to study glioblastoma to be studied more directly.
To understand what happens inside the 3D model, the researchers used a laser to scan the sample and create a snapshot of the cellular structure. This combination allows them to assess the effectiveness of a commonly used chemotherapy drug, temozolomide. The drug, temozolomide kills glioblastoma cells in two-dimensional models, but when put into a three-dimensional one, the tumor rebounded which implies that the drug did not work in the long term.
This 3D model may be able to speed up that process to weed out ineffective drugs first, confirming that only the most promising ones move to animal, and eventually human, trials.
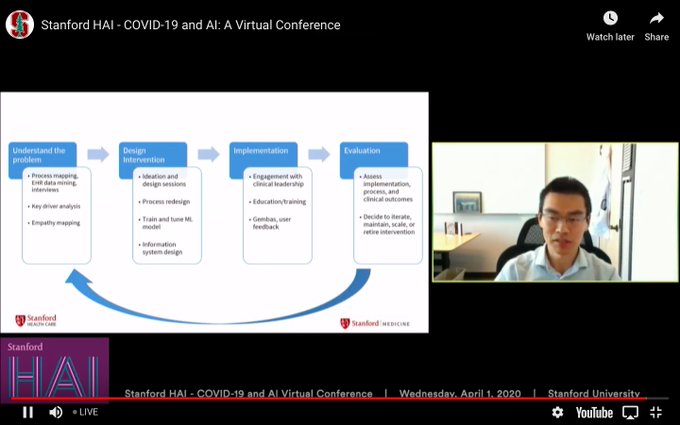
Tweets and Retweets @ COVID-19 and AI: A Virtual Conference – Human-Centered Artificial Intelligence Institute, Stanford University, 4/1/2020, 9AM PST – 3:30PM PST @StanfordHAI BY @pharma_BI and @AVIVA1950
COVID-19 and AI: A Virtual Conference – Human-Centered Artificial Intelligence Institute, Stanford University, 4/1/2020, 9AM PST – 3:30PM PST @StanfordHAI @pharma_BI @AVIVA1950
@StanfordHAI@pharma_BI@AVIVA1950https://pharmaceuticalintelligence.com/coronavirus-portal/… Fei-Fei Li AGE Fatality rate and infection rate of the aged Interaction between Acute Infection and Chronic Disease Safety of home – AI sensors at home Sensors data on secure systems clinically data recognized detection
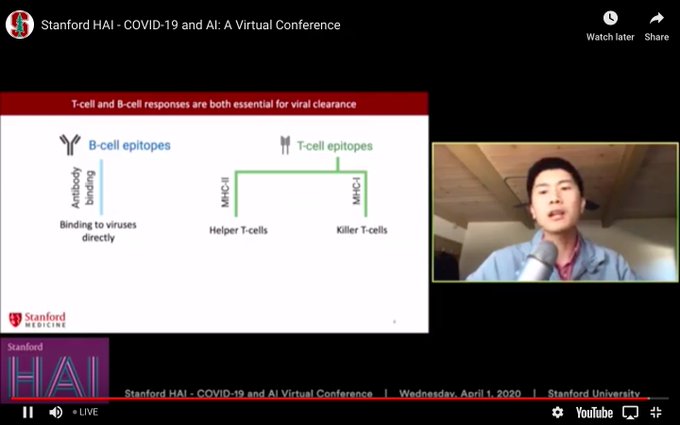
@StanfordHAI@pharma_BI@AVIVA1950https://pharmaceuticalintelligence.com/coronavirus-portal/… Identifying COVID-19 Vaccine Candidates with ML Binbin Chen, MD and Ph.D. Student, Department of Genetics, Stanford University Immunogenic component of vaccine for COVID-19 spike protein bind epitome
@StanfordHAI@pharma_BI@AVIVA1950https://pharmaceuticalintelligence.com/coronavirus-portal/… Repurposing Existing Drugs to Fight COVID-19 Stefano Rensi #NLP Mine the literature for Proteins: Genomes genes proteins Biophysics #docking simulations for energy of 18 molecules as inhibitors Selection of candidate
@StanfordHAI@pharma_BI@AVIVA1950https://pharmaceuticalintelligence.com/coronavirus-portal/…#ML can be helpful in critical care navigate complexity by automating processes vaccine mutations in the spike protein binding ACE2
@StanfordHAI@pharma_BI@AVIVA1950https://pharmaceuticalintelligence.com/coronavirus-portal/… Mining article on sample size domain ares expert add to the challenges vs CS expertise alone
@StanfordHAI@pharma_BI@AVIVA1950https://pharmaceuticalintelligence.com/coronavirus-portal/…#Virtual#informed#consent of #patient to accelerate ##clinical#trials
https://pharmaceuticalintelligence.com/coronavirus-portal/… Xavier Amatriain Lack accessibility to health care systems HC Accessibility and Scalability AI based HC IT System PDA – Personalized Diagnostics Assessment – for self reporting AI Automations + Physicians home testing
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Tina White, Ph.D. Candidate, Department of Mechanical Engineering, Stanford University China death toll >1000 China launched App to monitor quarantine early 1/2020 GPS based new App for contact tracing regulation on data
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… John Brownstein Late December 2019 collecting dat a HealthMap – public domain Baidu – has movement information connected with cases Temperature Data published Buoy data base customized to collect MA data on Temperature
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Jason Wang commend center in December 2019 All flight entering the country – Level 3 alert country: China Huhan, Hubei Quarantine all arriving from Level 3 alert country National STOKE PILES Activated x5 mask production
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Jason Wang Since 2003 Taiwan is preparing for a Pangemic JAMA paper on the topic is beebn reported Location of patient Taiwan National Epidemic Center 100 persons 24×7 in the Command Center Taiwan activated
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Michele Barry,TRACE together – Bluetooth tool on distance among people CHINA – contact racing surveillence scanning temp strict social distancing Hong Kong – tracing bracelets for quarantine Street locations of infected
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Michele Barry 5Million people travel out of Huhan Singapore – Free testing 1st country Temp testing stay at home, text phone from Authorities, show picture they are in quarantine for 5 days if negative TRACE together
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Seema Yasmin March 7, 2020 Italy news quarantine of 16 million lockdown large movement of people moving out of lockeddown areas, this movement based on information lead to spread of the viral spread
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
Stanford HAI – COVID-19 and AI: A Virtual Conference
COVID-19 and AI: A Virtual Conference will address a developing public health crisis. Sponsored by the Stanford Institute for Human-Centered Artificial Intel…
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
Stanford HAI – COVID-19 and AI: A Virtual Conference
COVID-19 and AI: A Virtual Conference will address a developing public health crisis. Sponsored by the Stanford Institute for Human-Centered Artificial Intel…
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
Stanford HAI – COVID-19 and AI: A Virtual Conference
COVID-19 and AI: A Virtual Conference will address a developing public health crisis. Sponsored by the Stanford Institute for Human-Centered Artificial Intel…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Stanford Institute for Human-Centered Artificial Intelligence (HAI) Conference on COVID-19 and AI: A Virtual Conference on April 1, 2020 beginning at 9:00am (PDT). event covered in real time
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
says. He discusses how AI tools built upon immunology knowledge and data can increase the chances of finding an effective vaccine. https://stanford.io/3aBidgh
Treatments for COVID-19 are urgently needed. “The fastest way to develop drugs is to repurpose existing drugs already on the market or in clinical trials.” – Stefano Rensi (
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
Stanford HAI – COVID-19 and AI: A Virtual Conference
COVID-19 and AI: A Virtual Conference will address a developing public health crisis. Sponsored by the Stanford Institute for Human-Centered Artificial Intel…
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…
Stanford HAI – COVID-19 and AI: A Virtual Conference
COVID-19 and AI: A Virtual Conference will address a developing public health crisis. Sponsored by the Stanford Institute for Human-Centered Artificial Intel…
https://pharmaceuticalintelligence.com/coronavirus-portal/… Stanford Institute for Human-Centered Artificial Intelligence (HAI) Conference on COVID-19 and AI: A Virtual Conference on April 1, 2020 beginning at 9:00am (PDT). event covered in real time
Coronavirus Portal
CORONAVIRUS PORTAL @LPBI Launched on 3/14/2020 OPEN TO GUEST AUTHORS on Seven Selected Topics & Lead Curator for Contact: Development of Medical Counter-measures for 2019-nCoV, Co…