Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
NEW YORK (GenomeWeb News) – PDI and Transgenomic today announced a collaboration to commercialize Transgenomic’s molecular diagnostic test that identifies specific genes that influence the safety and effectiveness of commonly used cardiovascular drugs.
Under the terms of the deal, PDI will market and promote the test called CardioPredict in the US. Transgenomic will process the test, which launches later this month, in its CLIA laboratory and be responsible for customer support. The firms will bear their respective costs and will divide profits based on an undisclosed formula. PDI will also provide funding to Transgenomic “principally to mitigate working capital requirements.”
Other financial terms were not disclosed.
“With an experienced sales team and a demonstrated record of success in sales and marketing in the life sciences, PDI is the right partner for the launch and long-term growth of CardioPredict,” Transgenomic President and CEO Paul Kinnon said in a statement. Kinnon replaced Craig Tuttle in those positions earlier this month.
“This collaboration with Transgenomic is another step in our pursuit of commercialization opportunities for clinically valuable products aimed at adding more predictable, higher growth, higher margin businesses that can leverage the substantial full commercialization capabilities of PDI,” PDI CEO Nancy Lurker added.
Based in Parsippany, NJ, PDI is a healthcare commercialization company.
“There is a large market, a well-defined patient population, and a clearly identified physician base treating these patients that should allow for a very efficient use of PDI’s broad base of commercialization capabilities,” Lurker said.
BALTIMORE — Two new studies contribute further to the debate over the cardiovascular risk associated with supplementary or dietary calcium, each decidedly coming down on the side of no significant risk — to men or women.
“[Based on these findings], clinicians should continue to evaluate calcium intake, encourage adequate dietary intake, and if necessary, use supplements to reach but not exceed recommended intakes,” Douglas C. Bauer, MD, from the University of California, San Francisco, the lead author of the first study, told Medscape Medical News.
Results of both studies were reported at the recent American Society for Bone and Mineral Research (ASBMR) 2013 Annual Meeting.
Dr. Bauer’s observational trial is one of few contemporary studies to evaluate the level of risk among men, who are often poorly represented in calcium studies, he noted. The results showed no association between calcium dietary intake or supplementation and total or cardiovascular mortality. The second study was an updated meta-analysis of calcium supplementation among women and similarly demonstrated no increased risk for ischemic heart disease (with adjudicated outcomes) or total mortality in elderly women. It did draw some criticism for potential bias and contamination, however.
Nevertheless, says Robert Marcus, MD, a retired Stanford University bone specialist, the 2 studies are “powerful. The one involving men had very elegant, accurate reports of death and validated diagnosis of myocardial infarction, and the [study involving women] was also excellent work,” he commented.
“This field has been the subject of an enormous amount of controversy, ambiguity, and confusion for the past several years, and I think the most important thing is to help us come up with what is true,” he said. The quality of data to suggest an adverse effect of calcium is “very poor,” and there is now compelling evidence that there is little to substantiate this, he noted. But despite these reassuring new findings, public anxiety over a potential risk with calcium is unlikely to go away, he believes.
In recommendations issued in 2010, the ASBMR said that most adults 19 years of age and older require about 600 to 800 IUs of vitamin D daily and 1000 to 1200 mg of calcium daily through food and with supplements, if needed.
Contemporary Data on Calcium Intake in Men
The use of calcium supplements, predominantly with vitamin D, is an important therapy for the prevention of osteoporosis and its clinical consequences. But concerns about the cardiovascular safety of calcium have emerged periodically; in 2 alarming meta-analyses published in 2010 and 2011 by Dr. Mark Bolland and colleagues, for example, there was a 27% increase in MI among individuals allocated to calcium supplements in the first study and a 24% increased risk in the second.
More recently, a 40% increase in total mortality and up to a 50% increase in cardiovascular mortality was seen among women from a Swedish mammography cohort with a calcium intake exceeding 1400 mg per day. In that study, the effect on mortality appeared to be especially strong if a high dietary intake of calcium was combined with calcium supplements.
In their new study, Dr. Bauer and his colleagues set out to assess rates of dietary calcium intake, use of supplements, and mortality in a prospective cohort of 5967 men over the age of 65 years in the Osteoporotic Fractures in Men (MrOS) study.
The participants completed extensive surveys at baseline on their dietary calcium intake, and supplementation was verified by a review of pill bottles by trained staff.
Mean dietary calcium intake was 1142 ± 590 mg/day, with more than half — 65% — of participants reporting use of calcium supplements.
Over the 10-year follow-up, among 2022 men who died, 687 deaths were caused by cardiovascular disease. The highest mortality for CVD was seen in the quartile with the lowest intake from calcium supplementation.
And in models that adjusted for age, energy intake, and calcium use, men in the lowest quartile of total calcium intake (less than 621 mg per day) had higher total mortality compared with those in the highest quartile (more than 1565 mg of calcium per day).
Adjustment for additional confounding factors showed no association between calcium dietary intake and total or cardiovascular mortality (P for trend .51 and .79, respectfully). Likewise, there was no association between calcium supplementation and total or cardiovascular mortality.
The authors also conducted an additional analysis of calcium intake and adjudicated cardiovascular disease events in a subcohort of the study, MrOS Sleep, involving 3120 patients who took part in a 7-year follow-up, and again there was no higher risk for cardiovascular events associated with calcium intake.
The study did have is limitations, Dr. Bauer acknowledged, including the observational design, calcium intake being assessed with a food frequency questionnaire, and cause of death not being formally adjudicated. Nevertheless, the findings are important in demonstrating the level of risk among men in a contemporary setting, he pointed out.
“Contrary to the Swedish study of women, we found no evidence that calcium supplementation is harmful to men, even among those with the highest dietary calcium intake,” he concluded, recommending that future studies should include adjudicated outcomes.
Study in Men as Expected, but Female Research Questioned
In the second study reported at the ASBMR meeting, Joshua Lewis, MD, PhD, from the University of Western Australia, Perth, and colleagues reported a meta-analysis of 19 randomized controlled trials involving women over the age of 50 years who had received calcium supplementation for more than a year.
Importantly, the analysis included reports of adjudicated cardiovascular outcomes, which the researchers note is important because gastrointestinal events can be misreported as cardiac ones. They also assessed all-cause mortality.
Among 59,844 participants in the studies, there were 4646 deaths, and the relative risk for death among those randomized to calcium supplements was 0.96 (P = .18).
The relative risk for 3334 ischemic heart disease events among 46,843 participants was 1.02 (P = .053), and the risk for 1097 MI events among 49,048 participants was 1.09 (P =.21).
“The data from this meta-analysis does not support the concept that calcium supplementation with or without vitamin D increases the risk of ischemic heart disease or total mortality in elderly women,” concluded Dr. Lewis.
But bone specialist Ian Reid, MD, from the University of Auckland, New Zealand, who was a coauthor on some of the Bolland studies, said this analysis essentially repeats previous ones, but with the inclusion of 20,000 patients from the Women’s Health Initiative (WHI), many of whom continued to take their own calcium tablets, regardless of whether they were randomized to calcium or placebo.
These “contaminated” WHI data have the potential to mask the effect of calcium, he told Medscape Medical News. In addition, in a study from Denmark also included in the meta-analysis, subjects were not properly blinded to treatment assignment and the calcium and control groups were not comparable at baseline for cardiovascular risk, which introduced “major potential bias,” he added.
Regarding the results from the study in men by Dr. Bauer and colleagues, Dr. Reid said they were not surprising to him. “Generally, people who take calcium supplements have more health-conscious behaviors than those who do not and so have a lower baseline risk of heart disease” that can “obscure small adverse effects of drugs such as calcium,” he observed.
An effect has to be “very substantial” before it can be picked up in an observational study, because of the many confounders that can obscure such an effect, he concluded.
Dr. Bauer, Dr. Lewis, Dr. Reid, and Dr. Marcus have reported no financial relationships. MrOS is supported by funding from the National Institutes of Health.
American Society for Bone and Mineral Research 2013 Annual Meeting. Abstracts 1001 and 1002, presented October 4, 2013.
Carotid Ultrasound more sensitive for Detecting Subclinical Atherosclerosis in patients with rheumatoid arthritis (RA) than CT with calculation of Coronary Artery Calcification Scores
Carotid ultrasound was more sensitive for detecting subclinical atherosclerosis in patients with rheumatoid arthritis (RA) than CT with calculation of coronary artery calcification scores, Spanish researchers found.
Among a group of 60 patients classified as being at moderate cardiovascular risk on a conventional scoring system, the presence of severe abnormalities on ultrasound reclassified 51 as being at high or very high risk, according to Miguel A. Gonzalez-Gay, MD, of Universitario Marques de Valdecilla in Santander, and colleagues.
Patients with RA are at markedly increased risk for cardiovascular disease (CVD), both from conventional risk factors and the ongoing systemic inflammation associated with RA.
Comprehensive management of these patients therefore should include risk assessment and appropriate interventions, but “adequate stratification of the CV risk in patients with RA is still far from being completely established,” Gonzalez-Gay and colleagues noted.
The insensitivity of conventional risk assessments such as the Systematic Coronary Risk Evaluation (SCORE), even when modified by the European League Against Rheumatism(mSCORE) to account for the increased background risk in RA, has been confirmed byreports of ischemic heart disease among patients not considered to be at elevated risk on these measures.
Therefore, they enrolled 95 rheumatoid arthritis patients with no history of cardiovascular events and no diabetes or chronic renal disease.
Most were women, mean age was 59, and mean disease duration was 11 years.
Rheumatoid factor and/or anticyclic citrullinated peptide was present in 72%, and extra-articular manifestations in 16%.
All patients had carotid ultrasonography to assess for plaque and multi-detector CT scanning to detect coronary artery calcification.
Carotid intima-media thickness of 0.90 or the presence of plaque was considered predictive of CVD on ultrasound.
A coronary artery calcification score of zero was considered normal, and a score over 100 indicated a high likelihood of coronary artery disease.
Patients also were given conventional SCORE ratings, based on factors such as age, sex, smoking, blood pressure, and atherogenic index, as well as mSCORE ratings, to estimate the 10-year risk for a fatal cardiovascular event.
The mean SCORE was 2.30, and the mean mSCORE was 2.78.
Cardiovascular risk according to mSCORE was low in 21, moderate in 60, and high or very high in 14.
Most patients with low mSCOREs also had scores of zero for coronary artery calcification, and none of the low mSCORE patients had calcification scores above 100.
But 57% of patients with calcification scores of zero had carotid plaques identified on ultrasound, as did 76.3% of patients with calcification scores between 1 and 100.
While calcification scores above 100 weren’t much more sensitive than mSCOREs for detection of high risk (23.6% versus 19.4%), almost all (70 of 72) patients with high or very high risk were identified with carotid ultrasound, for a sensitivity of 97.2% (95% CI 90.3-99.7).
And when the ultrasound model of intima-media thickness above 0.9 mm and/or carotid plaque also included mSCOREs above 5%, all 72 were correctly identified, for a sensitivity of 100% (95% CI 95-100).
This lack of sensitivity for calcification scores likely reflects the finding that arterial calcification is a later vascular development, and its absence doesn’t rule out the presence of the more vulnerable noncalcified plaques, the researchers explained.
“These results support the use of carotid ultrasonography as the imaging technique of choice for detection of high/very high CV risk in RA patients with moderate mSCORE,” they said.
In an editorial accompanying the study, Patrick H. Dessein, MD, of the University of Witwatersrand in Johannesburg, South Africa, and Anne G. Semb, MD, of Diakonhjemmet Hospital in Oslo, Norway, noted that the use of ultrasound more than tripled the number of patients considered to be at high risk.
If only mSCORE was used for risk stratification, they pointed out, many patients “in routine clinical settings” would be unlikely to receive preventive treatments, “with the serious consequences this has.”
Dessein and Semb also noted that there were certain limitations to this study, including its cross-sectional design and inclusion of patients with long disease duration.
“It remains to be clarified whether carotid ultrasound is as helpful among patients with early disease versus those with longstanding disease in enhancing CVD risk stratification,” the editorialists wrote.
To conduct a multicenter study of the relationship between insulin resistance and cardiovascular disease (CVD) and its risk factors in a tri-ethnic (African-American, Hispanic, and non-Hispanic white) population aged 40 to 69 years at baseline. Also, to identify the genetic determinants of insulin resistance and visceral adiposity.
IRAS enrolled 863 nondiabetic subjects (age 40–69) at four centers. Insulin sensitivity and acute insulin response were measured at baseline and at regular intervals over a five-year follow-up period. Diabetes and IGT were defined by
current fasting and
two-hour plasma glucose criteria
and/or use of glucose-lowering medications
Of the 863 subjects, the number of people in IRAS who fell into this high-calcium group was relatively small—about 15% to 17% of the study population.
Respectively, Serum Calcium in Upper-Normal Range (>2.5 mmol/L) as a New Biomarker for Diabetes-risk Forecasts is applicable for 15% -17% of the Patient population, thus, the prediction power of the new Biomarker is defined by this percentage.
#2
Comorbidities
Cardiovascular disease and diabetes share many of the same risk factors and that calcium has also been linked with
lower insulin sensitivity,
impaired glucose tolerance (IGT), and the
metabolic syndrome
#3
Tree Key factors involved in Calcium Regulation NOT studies by Insulin Resistance Atherosclerosis Study (IRAS)
The study did not address
vitamin D – involved in calcium regulation
parathyroid hormone levels – involved in calcium regulation
physical-activity levels, which are also known to have an impact on serum calcium
#4
Hypothesis was that serum calcium may also play some role in the development of diabetes
Dr. Lorenzo told heartwire:
Whether serum calcium plays a causative role in the development of diabetes or is a marker for other adverse processes remains unclear; “we can’t answer that question,” “There is a relationship, but we can’t yet determine why this is happening.”
Study Results Highlights
High concentrations of serum calcium—but not necessarily calcium intake—are associated with an increased risk of developing type 2 diabetes, results from the Insulin Resistance Atherosclerosis Study(IRAS) show. Moreover, calcium concentration appears to act independently of glucose, insulin secretion, and insulin resistance
relationship between calcium concentration and incident diabetes was statistically significant but did not follow a linear relationship. Only subjects with the highest concentrations of calcium (>2.38 mmol/L) had a significantly increased risk of developing diabetes. After controlling for
researchers found that only patients at the highest levels of serum calcium (>2.5 mmol/L) showed a statistically significant increase in incident diabetes.
A similar, nonlinear relationship was seen between the highest category of serum calcium and impaired fasting glucose.
Of note, in models that looked at albumin-adjusted calcium concentration as well as total calcium intake, no statistically significant relationship with five-year diabetes risk was seen
In the past, explained Lorenzo, researchers have speculated that the link between calcium and diabetes is related to insulin resistance or insulin secretion. “Our study shows that people with serum calcium that is pretty much in the normal range, but in the upper-normal range—those people are at higher risk for diabetes. And that, most probably, is not related to their metabolic status defined by their obesity or their insulin resistance or their insulin secretion.”
Calcium Intake Not Linked With Diabetes IncidenceThe findings on calcium intake are also important, he noted, since it shows that high calcium intake, per se, is not problematic; rather, it is the body’s ability toregulate calcium that seems to be at issue.
Dr, Lorenzo suspect [serum calcium levels] won’t add much to their prediction equations, but “if you have someone in the clinic who has those levels of calcium, that person is going to be at higher risk for diabetes,” he concluded.
Other RELATED articles published on this Open Access Online Scientific Journal, include the following:
Critical Gene in Calcium Reabsorption: Variants in the KCNJ and SLC12A1 genes – Calcium Intake and Cancer Protection
Part IV: The Centrality of Ca(2+) Signaling and Cytoskeleton Involving Calmodulin Kinases and Ryanodine Receptors in Cardiac Failure, Arterial Smooth Muscle, Post-ischemic Arrhythmia, Similarities and Differences, and Pharmaceutical Targets
Larry H Bernstein, MD, FCAP, Justin Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
Part VI: Calcium Cycling (ATPase Pump) in Cardiac Gene Therapy: Inhalable Gene Therapy for Pulmonary Arterial Hypertension and Percutaneous Intra-coronary Artery Infusion for Heart Failure: Contributions by Roger J. Hajjar, MD
Part VIII: Disruption of Calcium Homeostasis: Cardiomyocytes and Vascular Smooth Muscle Cells: The Cardiac and Cardiovascular Calcium Signaling Mechanism
Justin Pearlman, MD, PhD, FACC, Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Since 4/2012, Leaders in Pharmaceutical Business Intelligence, is developing an innovative methodology for the facilitation of Global access to Biomedical knowledge rather than the access to sheer search results on Scientific subject matters in the Life Sciences and Medicine. For the methodology to attain this complex goal it is to be dealing with popularization of ORIGINAL Scientific Research via Content Curation of Scientific Research Results by Experts, Authors, Writers using the critical thinking process of expert interpretation of the original research results. We demonstrate in this article two approaches to the process of reaching that goal successfully.
Editorial Team Members and Five Series of e-Bookd in BioMed
Part I: The Curator as a Scientific Content Critique for the Architecture of Knowledge, its meaning and its societal implications.
Part II: Cases in Co-Curation and Scientific Content Critique
In Part I, one curator edifies the e-Reader via his/hers OWN creative mental processes of knowledge synthesis following the creative mental process of analytical critique. The outcome is a new FORM of writing Science and of writing about Science, as well as, a new FORM of framework been created for the organization of the interrelations exposed in the analytical phase of a dialectically generated original synthesis, the process of which is manifold: the structure of the knowledge presented, culling in the midst of inclusion/exclusion dialectics and finally the Curator’s own original synthetic statements of the new Art, a new conceptual perspective on Science.
In part Part II: Cases in Co-Curation and Scientific Content Critique, are presented. A similarprocess to the one in Part I, is been applied. However, the Co-Curation, brings on stage several players. The Actors in the Scientific Writers Theater, all own scientific knowledge and master the process of creation of a new Synthesis for most writing engagements. Since the Co-curators are educated in different disciplines, they are skillfully providing interpretations for others’ and their own new conception of ideas. Thus, they are developing new views of the original scientific results presented in peer reviewed journals, just the leading ones in every field. The Co-Curators, their creation is a new layer of comprehension for the processes at hand.
Example #1:
Action Potential, a well define concept in Physiology. For us, Action Potential was a conceptual creation for the process of Co-Curation. Dr. Lev-Ari, requesting Dr. Bernstein to elaborate creatively, on the function of actin in cytoskeleton mobility, he did, THEN a new conceptual creation process emerged and had YIELDED the following article:
Identification of Biomarkers that are Related to the Actin Cytoskeleton
The e-Reader will compare which of the two is more beneficial for the e-Reader.
We believe that the curation of the Source Interview has remarkable value added analysis that the Reader can benefit from.
The unique process as described for Part I and for Part II, above, will be demonstrated, below, in concrete cases, as we applied the methodology of curation by one or by several Experts, Authors, Writers in the field of Cardiovascular Diseases.
The Process: We culled the scene for Cardiovascular Original Research in +24 Journals, we pre-select domains of research to cover: The Etiology of the Disease, the Risks of dysfunction at cellular, tissue, organelle, organ, anatomy, physiology, pathophysiology and diagnostics for all of the above. We interpret the Disease Management Options in a comprehensive fashion, exposing the e-Reader to an integrative approach for the treatment of Cardiovascular Disease.
Below, the e-Reader finds selective cases exemplifying the methodology described, making
Lev-Ari, A. 8/1/2013 Calcium Cycling (ATPase Pump) in Cardiac Gene Therapy: Inhalable Gene Therapy for Pulmonary Arterial Hypertension and Percutaneous Intra-coronary Artery Infusion for Heart Failure: Contributions by Roger J. Hajjar, MD
Lev-Ari, A. 7/14/2013 Vascular Surgery: International, Multispecialty Position Statement on Carotid Stenting, 2013 and Contributions of a Vascular Surgeon at Peak Career – Richard Paul Cambria, MD
Lev-Ari, A. 7/9/2013 Heart Transplant (HT) Indication for Heart Failure (HF): Procedure Outcomes and Research on HF, HT @ Two Nation’s Leading HF & HT Centers
Lev-Ari, A. 6/3/2013 Clinical Indications for Use of Inhaled Nitric Oxide (iNO) in the Adult Patient Market: Clinical Outcomes after Use, Therapy Demand and Cost of Care
Lev-Ari, A. 5/17/2013 Synthetic Biology: On Advanced Genome Interpretation for Gene Variants and Pathways: What is the Genetic Base of Atherosclerosis and Loss of Arterial Elasticity with Aging
Lev-Ari, A. 4/28/2013 Genetics of Conduction Disease: Atrioventricular (AV) Conduction Disease (block): Gene Mutations – Transcription, Excitability, and Energy Homeostasis
Bernstein LH, Pearlman JD and A. Lev-Ari, 9/8/2013
Part IV: The Centrality of Ca(2+) Signaling and Cytoskeleton Involving Calmodulin Kinases and Ryanodine Receptors in Cardiac Failure, Arterial Smooth Muscle, Post-ischemic Arrhythmia, Similarities and Differences, and Pharmaceutical Targets
Pearlman, JD, Bernstein, LH and A. Lev-Ari, 9/12/2013
Part VIII: Disruption of Calcium Homeostasis: Cardiomyocytes and Vascular Smooth Muscle Cells: The Cardiac and Cardiovascular Calcium Signaling Mechanism
Pearlman, JD, Bernstein, LH and A. Lev-Ari 8/5/2013
Alternative Designs for the Human Artificial Heart: The Patients in Heart Failure – Outcomes of Transplant (donor)/Implantation (artificial) and Monitoring Technologies for the Transplant/Implant Patient in the Community. To be submitted to Heart Failure Society of America (HFSA)
Cardiovascular Complications: Death from Reoperative Sternotomy after prior CABG, MVR, AVR, or Radiation; Complications of PCI; Sepsis from Cardiovascular Interventions
Pearlman JD, LH Bernstein and A. Lev-Ari 5/15/2013
Diagnosis of Cardiovascular Disease, Treatment and Prevention: Current & Predicted Cost of Care and the Promise of Individualized Medicine Using Clinical Decision Support Systems
The voice of Series A Content Consultant, Justin D Pearlman, MD, PhD, FACC
The leading cause of death and disability from any cause is cardiovascular disease, principally, heart attacks and strokes. Both the heart and brain typically allow only 10 minutes or so of inadequate blood supply before starting a committed course of permanent tissue injury, progressing in severity as time goes by without successful interruption of the disease process. Thus there is great time urgency to get patients to a definitive treatment that can stop the injury and restore adequate nutrient blood supply. Many patients can benefit from a catheterization to identify blockages and insert a small balloon within the blockage to expand the narrow channel, often followed by placement of a stent (wire cage) to maintain the expanded vessel diameter. Chemicals released over time from drug-eluting stents can prevent tissue in growth that may obstruct stents. These emergeny interventions are not always successful. There may be complications from the attempt to access an entry artery, and the blockages may not be amenable to a balloon. When such limitations are encountered, the next chance to help is surgical, with continued time pressure.
The fastest way to make the transition from a diagnostic catheterization to a timely intervention is a hybrid intervention suite that offers non-invasive imaging, catheterization and surgery all in one location. The following articles present the current state of hybrid “do it all” intervention suites. Additional articles address the risks of bad outcomes from such interventions.
Part One
Hybrid Cath Lab/OR Suite for Hybrid Surgery
In ACC.10 and i2 Summit, 59th Annual Scientific Session, 3/14-3/16, 2010, Alfred A. Bove, M.D., Ph.D., F.A.C.C., ACC President addressed the conference attendees:
Welcome to the all-new Hybrid Cath Lab/OR and 3D CV Theater. Recent developments in cardiac surgery and interventional cardiology have led to the creation of integrated, hybrid cath lab/operating rooms (OR), which provide significant advantages in the diagnosis and treatment of patients requiring cardiac procedures—helping to facilitate a rapid-response approach. These multimodality rooms are designed to support a variety of integrated surgical and endovascular procedures. We are excited to provide you with this opportunity to get a first-hand look—and feel—of the latest technologies. We hope you take the time to explore this interactive, multivendor venue. Learning is at the core of the ACC Annual Scientific Session and we invite you to expand your educational experience in this dynamic learning environment.
In the Hybrid Cath Lab/OR Suite, you’ll discover how integrating cutting edge angiographic and surgical equipment and technologies can facilitate a broad range of procedures within one location. Additionally, you will learn how hybrid suites are providing solutions that enable interventionalists and surgeons to work collaboratively to provide the best treatment options for patients. The adjoining 3D CV Theater features presentations by physicians currently performing intravascular and surgical procedures in hybrid suites. Each live presentation pairs a cardiologist with a surgeon, allowing you to hear perspectives from both sides on a variety of hybrid suite procedures and cases. In addition, the Theater offers video presentations of cases from around the world.
The ACC thanks the supporters of the Hybrid Suite for providing us with the opportunity to share this unique learning destination with you.
are perfect examples of procedures that could, and should, be carried out in a hybrid OR. High-risk patients who require less invasive interventions are the best candidates for treatment in a hybrid suite.
As cardiac surgery becomes less invasive, incisions are becoming smaller and smaller, and even totally endoscopic heart surgery is now possible. Cardiac surgeons have started to perform procedures that include catheter-based skills, such as transapical valve replacement. For these operations, surgeons need more sophisticated imaging techniques, fluoroscopy and contrast injections. The hybrid OR offers all these facilities. Perhaps the most obvious and easiest procedure that can be performed in a hybrid OR is coronary revascularization combining coronary artery bypass grafting with on-table intra-operative completion angiography for quality control. If the surgeon detects a problem during the procedure, he or she can revise the graft immediately and thereby prevent potential perioperative and long-term complications. Currently, cardiologists and cardiovascular surgeons have shown special interest in so-called hybrid coronary interventions, which are combinations of minimally invasive coronary artery bypass grafting and percutaneous coronary interventions. In these procedures, cardiovascular surgeons place a left-internal mammary artery bypass graft to the left-anterior descending artery through small incisions (MIDCAB) or completely endoscopically (TECAB), while any remaining obstructed coronary arteries are treated with stents by an interventional cardiologist. This procedure is an attractive alternative to multivessel open coronary artery bypass grafting. Transcatheter heart-valve replacement and repair are especially suited to a hybrid suite because percutaneoustransfemoral and transapical aortic valve repairs include risks that can only be treated successfully by immediate surgical intervention, such as coronary artery obstruction, aortic dissection and aortic perforations.
In addition, endovascular aortic stent grafting for the repair of abdominal aortic aneurysms is a suitable procedure for a hybrid operating room. Endovascular aneurysm repair has become an established alternative to open repair and is increasingly used for thoracic aorta repair as well. Some
emergency procedures for traumatic lesions of the thoracic aorta and
fulminant pulmonary embolism may also be performed in a hybrid OR. Several
pediatric interventions can be carried out in a hybrid suite as well, such as implantation of closure devices for atrial and ventricular septal defects in small children and
In a recent article we reported on the Change in Requirement for Surgical Support by Cath Labs for performance of Nonemergent PCI without Surgical Backup, that increases the autonomy of Interventional Cardiologists. In the Hybrid OR that change is irrelevant since the presence of a Cardiac Surgeon is a fact of the division of labor between the two types of specialties. Cardiac Surgeons are involved with percutaneous transfemoral and transapical aortic valve repairs and intervention for endoscopic aorta, AAA and Thoracic AA grafting.
Cardiovascular hybrid suite is a state-of-the-art operating room equipped with a fully functional catheterization laboratory, thus allowing surgical procedures and catheter-based interventions to be carried out in the same room. Hybrid suites provide a place where treatments traditionally available only in a cath lab and procedures only available in an operating room can be performed together to provide patients with the best available combination of therapies for cardiovascular disease. These multidisciplinary, integrated cardiovascular procedural suites bring the best of two worlds together by combining all the advantages of a modern cath lab with an up-to-date cardiovascular surgery operating room (OR).
Hybrid suites began to evolve in the mid to late 1990s, when some groups of interventional cardiologists started sharing operating rooms with cardiovascular surgeons. The appeal of the hybrid suite concept has grown as have catheter based devices (stents, coils, balloons and lasers) have been developed that enable interventional cardiologists to advance the invasiveness and effectiveness and applications of percutaneous transcatheter interventions. The interest in these suites has also increased as cardiovascular surgeons have developed a variety of techniques for
Minimally invasive procedures, such as minimally invasive direct coronary artery bypass grafting (MIDCAB) or
With the advent of more tools, interventional cardiologists are becoming more like surgeons, and with less invasive tools, cardiovascular surgeons are becoming more like interventionalists. Rather than separating surgical procedures from interventional procedures performed in traditional operating rooms and cath labs, hybrid suites provide a high-tech environment that allows cardiologists and surgeons to work together to offer patients complex, minimally invasive therapies.
Some experts believe that hybrid suites represent the wave of the future in cardiovascular care and that most heart centers will eventually install hybrid suites to offer patients the latest cardiovascular procedures safely and effectively with minimal surgical trauma. The rooms can be costly to build and equip, but if a medical center is considering building a new operating room or cath lab, setting up a hybrid suite makes sense. Medical centers that have a hybrid suite available can clearly differentiate themselves in a positive way from centers that do not have such capabilities.
The Benefits of a Hybrid Suite for Medical Centers
While building a hybrid suite is more expensive than building a traditional operating room or cath lab, a hybrid suite can potentially be used for all types of cardiovascular procedures, including
traditional cardiac and vascular surgery,
interventional coronary procedures,
endovascular aortic procedures and
electrophysiology procedures.
Hybrid suites reinforce the trend in cardiovascular care toward less invasive, comprehensive hybrid procedures. Once a hybrid suite is in place, the demand for its use will likely grow due to increasing indications and referrals for these innovative treatments, many of which are increasingly covered by third-party payers.
Interventional cath labs usually have excellent imaging capabilities but lack the sterile facilities and staff needed for a formal OR, while operating rooms frequently lack high-level imaging equipment. Some of the essential equipment for a hybrid suite includes:
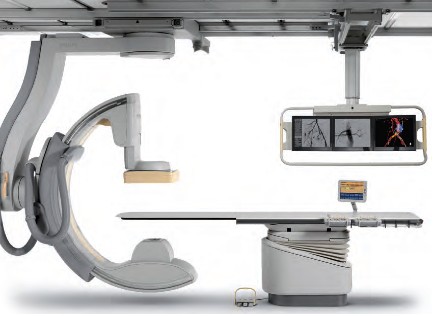
• A state-of-the-art imaging system capable of performing 3D rotational angiography, CT scanning, and ultrasound is advantageous. Floor-mounted and ceiling-mounted systems are available, but many hospitals use ceiling-mounted systems because access to the patient is slightly easier. Some ceiling-mounted systems provide 3D imaging from the surgeon’s position perpendicular to the patient. However, some hospitals prefer floor-mounted systems because having mechanical parts running above the operative field may cause dust to fall, resulting in infections. An important aspect is that the C-arm can be parked away when it is not used. This especially enhances access of the anesthesia team to the patient.
• An operating table that meets the needs of both surgeons and interventionalists by electronically integrating the table with the imaging system is also essential. These tables should have retractable rails for retractors and other surgical tools. To perform 3D imaging on the operating table, the C-arm of the imaging system should allow fast and precise rotation around the patient.
• A variety of other surgical and interventional systems and equipment may also be needed, including a robotic surgical system, a heart-lung machine, an image integration system, an endoscopic imaging system, a radiology display system, an audiovisual system to move images to different monitors and an anesthesia monitoring system, including transesophageal echocardiography. Some equipment like the integrated OR table and the angiography unit need to be fixed parts of the hybrid OR. Some equipment will be mobile in order to maintain some flexibility in workflow.
Philips is one of the world’s leading technology companies, with a long history of practical innovation and visionary design. In healthcare, we are committed to understanding the human and technological needs of patients and caregivers. We believe this understanding will help us deliver solutions that not only enable more confident diagnoses and more efficient delivery of care, but also improve the overall experience of care. We offer equipment, software and services for imaging, patient monitoring, resuscitation and much more. A Hybrid OR can help make life simpler for the interdisciplinary teams who operate in this environment every day. As a world leader in cardiovascular X-ray, Philips has the experience and expertise to deliver the first class technology you need to perform minimally invasive procedures with speed, accuracy and confidence. A long history of innovation has enabled Philips to develop pioneering imaging solutions that really make a difference.
For example, Philips Allura Xper cardiovascular X-ray systems are designed to deliver enhanced imaging with superb performance for all cardiac projections, and our iE33 ultrasound system with Live 3D TEE and QLAB can assist interventional procedures and provide comprehensive quantitative information to support critical decisions. Our cardiology informatics solutions help you manage patient information throughout the cardiovascular care continuum. Philips solutions allow minimally invasive and catheter-based procedures to take place in the same suite as conventional cardiac surgery.
Phillips EchoNavigator – X-Ray and 3-D Ultrasound is described in:
Intuitive Surgical, Inc. is the global technology leader in robotic-assisted, minimally invasive surgery. The company’s da Vinci® Surgical System offers breakthrough capabilities that enable cardiac surgeons to use a minimally invasive approach and avoid median sternotomy.
Content of FDA Warning Letter, following FDA Inspection on dates 04/01/2013 – 05/30/2013 – it discussed in
MAVIG’s specialty is ceiling/boom suspension systems for lighting (exam, surgical and LED), monitor-suspension systems—single, multibank (one to eight) systems and widescreen, overhead radiation shielding and contrast injector adapters. MAVIG also manufactures radiation protection products such as aprons, gloves, table-attachable lower body shields, adjustable- and fixed-height mobile and modular barriers.
Creating a hybrid lab may be complicated, but having an experienced partner that listens makes all the difference. Toshiba’s unique blend of hybrid experience and industry recognized Infinix™-i imaging systems for the Cath Lab.
Hybrid Cath Lab/OR Suite in Leading Hospitals in the US
The Hybrid Cath Lab/OR Suite at New York Presbyterian Hospital/Columbia University Medical Center, New York, NY is presented in
Speakers at 3D CV Theater, 2010 are working in Hospitals where Hybrid Cath Lab/OR Suite are in operations at the present time. The list include the following Hospitals with a Hybrid Cath Lab/OR Suite:
Vanderbilt Medical Center, Nashville, TN
University of Maryland Heart Center, Baltimore, MD
The Heart Center at Nationwide Children’s Hospital, Columbus, Ohio
The Robotic Surgical Center, East Carolina University Department of Surgery, Greenville, N.C.
University of Washington Medicine Regional Heart Center, Seattle, WA
Brigham and Women’s Hospital, Boston, MA
Saint Joseph’s Hospital and Peachtree Cardiovascular and Thoracic Surgery, Atlanta, GA
Emory University Hospital, Atlanta, GA
Beth Israel Deaconess Medical Center, Boston, MA
Boston Medical Center, Boston, MA
Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN
Lankenau Hospital, Lancaster, PA
Cardiac Non-Invasive Laboratory at Cedars-Sinai Medical Center, Los Angeles, CA
Robotic Surgery at St. Joseph’s Hospital, Atlanta, GA
Speakers at 3D CV Theater, 2010, included the following Cardiovascular Interventionists leading the adoption process of Hybrid Surgery in Hybrid Cath Lab/OR Suite into care modalities for cardiovascular disease:
Johannes O. Bonatti, M.D., is professor of surgery and director of coronary surgery and advanced coronary interventions at the University of Maryland Heart Center, Baltimore. He received his training in general surgery and cardiac surgery at the department of surgery at Innsbruck Medical University in Austria. Prior to his arrival at the University of Maryland, he worked at this institution as an attending surgeon and associate professor. Dr. Bonatti’s main interest is the development of minimally invasive, totally endoscopic coronary artery bypass grafting (TECAB) procedures using robotic technology.
As one of the international leaders in this field, he performed the largest series of robotic TECAB on the arrested heart, including single-, double- and triple-vessel TECAB. He has published significantly on procedure development and the implementation process of completely endoscopic coronary surgery using the da Vinci robotic system. Together with colleagues from interventional cardiology, Dr. Bonatti is working on integrated concepts for treatment of coronary artery disease. He was the first to perform a simultaneous hybrid coronary intervention using TECAB and placement of a coronary stent. He is organizing international meetings on hybrid interventions in cardiovascular medicine (http://www.icrworkshop.com). He has trained heart surgeons from around the world in the use of the da Vinci robot for heart surgery and he has introduced TECAB procedures in Austria, the Czech Republic, Greece, Turkey, India and Australia.
John G. Byrne, M.D., is the William S. Stoney Professor of Cardiac Surgery at Vanderbilt University School of Medicine and chair of the department of cardiac surgery at Vanderbilt Medical Center, Nashville, TN.
Before moving to Vanderbilt, he was associate chief and residency program director in the division of cardiac surgery at Brigham and Women’s Hospital, and associate professor of surgery at Harvard Medical School, Cambridge, MA. A graduate of the University of California, Davis, he received his medical degree in 1987 from Boston University. His postdoctoral training was completed at the University of Illinois affiliated hospitals and Brigham and Women’s Hospital in Boston.
Dr. Byrne is the author of more than 100 scientific articles on cardiac surgery and related areas. His patient care emphasis is
aortic root surgery,
coronary artery disease and
valve surgery
He is board-certified in general surgery and thoracic surgery.
John P. Cheatham, M.D., is director of cardiac catheterization and interventional therapy and codirector of The Heart Center at Nationwide Children’s Hospital, Columbus, Ohio. He is also the George H. Dunlap Endowed Chair in Interventional Cardiology and professor of pediatrics and internal medicine at The Ohio State University College of Medicine. Dr. Cheatham’s area of expertise is transcatheter intervention and hybrid therapy of newborns, children and adults with complex congenital heart disease. He has pioneered several new techniques and devices in non-surgical intervention and is a leader in developing hybrid therapies. He has been a principal investigator in numerous FDA-sponsored clinical trials evaluating non-surgical closure devices and stent therapy over the past two decades. Additionally, Dr. Cheatham designed the first hybrid cardiac catheterization suites and advanced imaging equipment at Nationwide Children’s Hospital. He serves as a consultant to various medical companies and proctors new transcatheter techniques and devices to other physicians around the world. Dr. Cheatham has implemented a formal physician exchange program with two of the leading medical institutions in China. In cooperation with China Red Cross, he is also the foreign director of the International Training Center for treatment of congenital heart disease in poor children. Dr. Cheatham has written more than 120 manuscripts, 16 book chapters, 300 national and international presentations and is co-editor of the book, Complications in Percutaneous Interventions for Congenital and Structural Heart Disease. After graduating from the University of Oklahoma College of Medicine, he completed his residency at Boston Children’s Hospital, followed by a fellowship in Pediatric Cardiology at Texas Children’s Hospital in Houston.
W. Randolph Chitwood, Jr., M.D., is senior associate vice chancellor for health sciences and chief of cardiovascular services at East Carolina University Department of Surgery, Greenville, N.C. Dr. Chitwood is a leading international pioneer in minimally invasive and robotic heart surgery. The Robotic Surgical Center at East Carolina University has trained more than 350 surgeons. His research activities relate to myocardial preservation, simulation in surgery and endoscopic/robotic cardiac surgery. He was the principal investigator of the FDA robotic mitral valve trials that led to approval for use in the U.S. He is the son and grandson of “southwestern Virginia mountain doctors” who set the guidelines for his professional life. He graduated from Hampden-Sydney College and received his medical degree from the University of Virginia. After medical school, he completed the surgical residency at Duke University Medical Center under David C. Sabiston, M.D., an influential surgical educator of the era. At Duke he spent 10 years training in general and cardiothoracic surgery, as well as basic science research.
After his chief residency at Duke in 1984, he was selected to begin and head the new cardiac surgery program at the East Carolina University School of Medicine. Because of his prolific publication record as a resident and clinical acumen, his initial appointment was as a full professor of surgery. Except for a two-year hiatus as the chief of cardiothoracic surgery at the University of Kentucky, he has spent his entire career at East Carolina University, where he also served as chairman of the department of surgery. In 2003, he was named to be in charge of the development of the East Carolina Heart Institute, which now includes an integrated department of cardiovascular sciences as well as a $200 million heart hospital, outpatient, research and education center.
Larry S. Dean, M.D., is director of the University of Washington Medicine Regional Heart Center and is professor of medicine and of surgery at the University of Washington School of Medicine, Seattle. In addition to general cardiology, he is an expert in cardiac catheterization and interventional cardiology. He also conducts research on stents to keep blocked heart arteries open and on ways to prevent restenosis after stents are inserted. He is currently involved in the evaluation of percutaneous aortic valve replacement. Dr. Dean earned his M.D. from the University of Alabama School of Medicine, Birmingham, and served his internship and residency at the University of Washington. He then returned to the University of Alabama Hospital for fellowships in cardiovascular disease and in angioplasty. After nearly 15 years as a faculty member at the University of Alabama, he returned to the University of Washington to direct the Regional Heart Center. He is a fellow of the American College of Cardiology and is board-certified in internal medicine, cardiovascular disease and interventional cardiology. He is also a fellow of the American Heart Association and president-elect of the Society of Cardiovascular Angiography and Interventions.
Andrew Craig Eisenhauer, M.D., is director of the interventional cardiovascular medicine service at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School. His specialties are
interventional cardiology,
vascular medicine and
congenital and inherited diseases.
He earned his medical degree at New York University School of Medicine and served a residency at Peter Bent Brigham Hospital and a fellowship at Massachusetts General Hospital. He is certified in internal medicine, cardiovascular disease and interventional cardiology. His clinical interests are
endovascular therapy,
complex coronary disease,
peripheral vascular disease,
cerebrovascular disease,
congenital heart disease and structural heart disease
Douglas A. Murphy, M.D., is chief of cardiothoracic surgery at Saint Joseph’s Hospital and a cardiothoracic surgeon at Peachtree Cardiovascular and Thoracic Surgery, Atlanta. His areas of interest are robotically assisted heart surgery with an emphasis on repairing the mitral valve rather than replacing it. A graduate of the University of Pennsylvania Medical School, Philadelphia, he served an internship and residency at Massachusetts General Hospital, Boston, and at Emory University, Atlanta.
Khusrow Niazi, M.D., is an assistant professor at Emory University School of Medicine and director of peripheral and carotid intervention at Emory University Hospital Midtown, Atlanta. He earned his medical degree at King Edward Medical College, Lahore, Pakistan, and served an internship at Kettering Medical Center, Dayton, Ohio, and a fellowship at William Beaumont Hospital, Royal Oak, MI. He has published papers on stenting following rotational atherectomy, small vessel stenting for coronary arteries, imaging of lower extremities and treatment of peripheral arterial disease.
Jeffrey J. Popma, M.D., is director of innovations in interventional cardiology, a senior attending physician at Beth Israel Deaconess Medical Center and an associate professor of medicine at Harvard Medical School in Boston. Dr. Popma received his bachelor’s degree in economics from Stanford University, and his M.D. from Indiana University School of Medicine. He completed his internship, residency, chief residency and fellowship at University of Texas Southwestern Medical Center. He also completed an interventional cardiology fellowship at the University of Michigan. Dr. Popma is the past president of the Society for Cardiac Angiography and Intervention and is the co-chair of the ACC Interventional Council. He sits on the editorial boards of several publications, and reviews for several cardiology periodicals. Dr. Popma has more than 300 published peer-reviewed manuscripts.
Dr. Popma also directs the BIDMC Angiographic Core Laboratory and is principal investigator for more than 65 ongoing multicenter device studies within the research laboratory. Over the past 15 years, these trials have included a broad array of new technology, including bare-metal stents, drug-eluting stents, distal-protection devices, total-occlusion devices and carotid and peripheral revascularization procedures. His primary clinical interest currently is the use of percutaneous aortic valve replacement for patients with high-risk aortic stenosis.
Robert S. Poston, M.D., is chief of cardiac surgery at Boston Medical Center and associate professor of cardiothoracic surgery at Boston University School of Medicine. He has a strong background in minimally invasive cardiac bypass surgery and is a pioneer in using robotics, specifically the da Vinci Surgical System, to treat coronary artery disease. A graduate of the Johns Hopkins School of Medicine, Baltimore, Dr. Poston completed a residency in general surgery at the University of California, San Francisco, and continued his training with a research fellowship in cardiothoracic surgery at Stanford University School of Medicine, Palo Alto, CA, and a cardiothoracic residency at the University of Pittsburgh Medical Center.
Charanjit S. Rihal, M.D., is professor of medicine and director of the cardiac catheterization laboratory at Mayo Graduate School of Medicine, Mayo Clinic, Rochester, MN. A graduate of the University of Winnipeg, Dr. Rihal did his residency and fellowship at the Mayo Graduate School of Medicine and also earned an MBA at the Carlson School of Management, University of Minnesota. His medical interests are interventional cardiology, structural heart disease interventions and the management of quality and costs in healthcare.
Timothy A. Shapiro, M.D., is director of the Interventional Cardiology Fellowship Program and campus chief, interventional cardiology, at Lankenau Hospital, Lancaster, PA. A graduate of Yale University School of Medicine, he served his residency and a fellowship at the Hospital of the University of Pennsylvania.
Robert J. Siegel, M.D., is director of the Cardiac Non-Invasive Laboratory at Cedars-Sinai Medical Center, cardiology director of the Cedars-Sinai Marfan Center, and Rexford S. Kennamer, M.D., chair in cardiac ultrasound at Cedars-Sinai Medical Center, Los Angeles. Dr. Siegel is also professor of medicine in residence at the David Geffen School of Medicine at University of California, Los Angeles. He previously served as senior staff fellow in cardiac pathology at the Heart, Lung and Blood Institute of the National Institutes of Health, Bethesda, MD. Internationally recognized as one of the leading experts in the field of cardiovascular ultrasound, Dr. Siegel specializes in cardiovascular ultrasound, including transthoracic, transesophageal and intravascular methodologies. His research interests include
valvular heart disease,
therapeutic applications of ultrasound energy,
transesophageal and intraoperative echocardiography, and the
development and use of hand-held portable echocardiographic systems for clinical innovations.
In addition, he is involved with clinical research studies related to the diagnosis, assessment and management of patients with
Marfan syndrome,
hypertrophic cardiomyopathy and
pericardial and valvular heart disease.
Dr. Siegel is a fellow, and has previously served as the president of the California Chapter of the American College of Cardiology and president of the Los Angeles Society of Echocardiography. He has been active in numerous cardiovascular societies, including the American Heart Association, the American College of Cardiology and the American Society of Echocardiography. Dr. Siegel received his medical degree at Baylor College of Medicine, Houston, where he developed an interest in cardiology. He completed his medical residency at Emory University and at Los Angeles County + USC Medical Center. He completed his cardiology fellowship at Harbor-UCLA Medical Center.
Over the last two years Dr. Siegel has worked extensively with live 3D transesophageal echo in the cardiac intervention center and the operating room. He and his echocardiologist colleagues, doctors Shiota, Biner, Tolstrup and Gurudevan, have worked closely at Cedars-Sinai Medical Center in Los Angeles with the interventional cardiologists, doctors Kar and Makkar, as well as with the cardiac surgeons, doctors Trento and Fontana. They use live 3D TEE extensively for the assessment of structural heart disease. In addition, it is used on a regular basis for the guidance of percutaneous procedures for mitral valve e-clip repair, mitral balloon valvuloplasty, aortic and pulmonic valve replacement, left atrial appendage exclusion by the Watchman device as well as for ASD closure.
Sudhir P. Srivastava, M.D., president of the International College of Robotic Surgery at St. Joseph’s Hospital, Atlanta, is a pioneer in performing beating heart totally endoscopic coronary artery bypass surgeries. Previously, he was assistant professor of surgery and director of robotic and minimally invasive cardiac surgery at the University of Chicago Medical Center. Dr. Srivastava specializes in robotically assisted totally endoscopic coronary artery bypass surgery. He has performed approximately 1,000 robotic cardiothoracic surgical procedures, of which 450 have been single- and multivessel beating heart totally endoscopic coronary bypass (BH TECAB) procedures. He has keen interest in hybrid coronary revascularization in TECAB patients to achieve complete revascularization.
Dr. Srivastava has helped launch robotic revascularization programs throughout the world. He has performed numerous live BH TECAB demonstrations both in the U.S. and abroad, and continues to be a presenter and invited speaker at numerous national and international scientific meetings. He earned his medical degree at the Jawahar Lal Nehru Medical College in Ajmer, India and immigrated to the U.S. in 1972. He completed his cardiothoracic surgery residency at the hospitals associated with the University of British Columbia, Vancouver, Canada.
Francis P. Sutter, D.O., F.A.C.S., is clinical professor of surgery at Thomas Jefferson University-Jefferson Medical College, Philadelphia, and chief of cardiothoracic surgery at Lankenau Hospital, Main Line Health System, Wynnewood, PA. A graduate of Philadelphia College of Osteopathic Medicine, his surgical residency and a cardiothoracic fellowship were completed at Thomas Jefferson University Hospital.
Mark R. Vesely, M.D., is an assistant professor of medicine at the University of Maryland School of Medicine. He completed medical school at the George Washington University and postgraduate training—an internal medicine residency and fellowships in cardiovascular disease and interventional cardiology—at the University of Maryland. He is board-certified in internal medicine, cardiovascular disease, nuclear cardiology and interventional cardiology. Dr. Vesely is the associate program director of the Interventional Cardiology fellowship at University of Maryland. His special interests include the partnered approach (interventional cardiologists and cardiac surgeons) for hybrid coronary revascularization and structural heart disease interventions. Additional research interests include investigation of techniques to minimize acute myocardial infarction injury with ventricular-assist devices and adult stem cell therapies.
David X. M. Zhao, M.D., Ph.D., is an associate professor of medicine and cardiac surgery, Harry and Shelley Page Chair in Interventional Cardiology, director of the Cardiac Catheterization Laboratories and interventional cardiology director of the Interventional Cardiology Fellowship Training Program, Vanderbilt University School of Medicine, Nashville, TN. He earned his medical degree at Shanghai Medical University, Shanghai, P.R. China, and his Ph.D. in immunology at Queensland University, Brisbane, Australia. His postdoctoral training was at Zhongshan Hospital, Shanghai Medical University, Shanghai, P.R. China, The Prince Charles Hospital, Brisbane, Australia, and Brigham and Women’s Hospital, Boston.
Cardiac Surgery @ Cleveland Clinic: Traditional OR & Hybrid Cath Lab/OR Suite
Nation #1 for 19 consecutive years – The Heart Center: Miller Family Heart & Vascular Institute @ Cleveland Clinic
The Sydell and Arnold Miller Family Heart & Vascular Institute is one of the largest, most experienced cardiovascular specialty groups in the world. Our physicians are committed to providing the most advanced diagnostic and treatment options, better outcomes and improved quality of life. U.S.News & World Reporthas ranked Cleveland Clinic as the No.1 heart program in America every year since 1995.
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Comparison of the 10-year and 15-year survivals after CABG demonstrated benefit from a change in graft sources used at the Mayo Clinic and widely adapted by others: vascular grafts from the left internal mammary artery (LIMA) instead of just leg veins, for multiple grafts (up to 3), LIMA-to-LAD plus grafts using LIMA or radial artery vs LIMA/saphenous vein (SV).
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part Three
Invasive Interventions with Complications
In the following article we covered multiple etiologies for cardiovascular complications related to invasive interventions: cardiovascular and peripheral arterial or peri- and post- cardiac surgery of the open heart type.
Cardiovascular Complications: Death from Reoperative Sternotomy after prior CABG, MVR, AVR, or Radiation; Complications of PCI; Sepsis from Cardiovascular Interventions
Justin D Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
This article covers types of Cardiovascular Complications derived from the following THREE types of assault on the Human body, two related to cardiac invasive interventions, the last due to its systemic nature is taking a fatal Cardiac toll: the Sepsis condition causing cardiac failure.
2. Surgical Complication of Non-cardiac surgery type causing cardiac arrest, i.e, Surgery of Joint Replacement causing sepsis causing death or death caused by complications of surgery i.e., blood loss, viral infection, emboli, thrombus, stroke, or cardiogenic shock not related to Cardiovascular and Cardiac invasive interventions
The e-Reader is advised to consider the following expansion on the subject matter carrying the discussion to additional related clinical issues:
Larry H Bernstein, Advanced Topics in Sepsis and the Cardiovascular System at its End Stage
Bernstein, HL, Pearlman, JD and A. Lev-Ari Alternative Designs for the Human Artificial Heart: The Patients in Heart Failure – Outcomes of Transplant (donor)/Implantation (artificial) and Monitoring Technologies for the Transplant/Implant Patient in the Community
2013 ACCF/AHA Guideline for the Management of Heart FailureA Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
Clyde W. Yancy, MD, MSc, FACC, FAHA; Mariell Jessup, MD, FACC, FAHA; Biykem Bozkurt, MD, PhD, FACC, FAHA; Javed Butler, MBBS, FACC, FAHA; Donald E. Casey, MD, MPH, MBA, FACP, FAHA; Mark H. Drazner, MD, MSc, FACC, FAHA; Gregg C. Fonarow, MD, FACC, FAHA; Stephen A. Geraci, MD, FACC, FAHA, FCCP; Tamara Horwich, MD, FACC; James L. Januzzi, MD, FACC; Maryl R. Johnson, MD, FACC, FAHA; Edward K. Kasper, MD, FACC, FAHA; Wayne C. Levy, MD, FACC; Frederick A. Masoudi, MD, MSPH, FACC, FAHA; Patrick E. McBride, MD, MPH, FACC; John J.V. McMurray, MD, FACC; Judith E. Mitchell, MD, FACC, FAHA; Pamela N. Peterson, MD, MSPH, FACC, FAHA; Barbara Riegel, DNSc, RN, FAHA; Flora Sam, MD, FACC, FAHA; Lynne W. Stevenson, MD, FACC; W.H. Wilson Tang, MD, FACC; Emily J. Tsai, MD, FACC; Bruce L. Wilkoff, MD, FACC, FHRS
We present below four National institutions with pubic mandate to promote all Healthcare aspects of Cardiovascular Diseases.
A. 2020 Vision of the Heart Failure Society of America (HFSA)
Special Communication: The Heart Failure Society of America in 2020: A Vision for the Future
Journal of Cardiac Failure Vol. 18 No. 2 2012 written by BARRY H. GREENBERG, MD,1,3 INDER S. ANAND, MD, PhD,2 JOHN C. BURNETT JR, MD,2,3 JOHN CHIN, MD,2,3 KATHLEEN A. DRACUP, RN, DNSc,3 ARTHUR M. FELDMAN, MD, PhD,3 THOMAS FORCE, MD,2,3 GARY S. FRANCIS, MD,3 STEVEN R. HOUSER, PhD,2 SHARON A. HUNT, MD,2 MARVIN A. KONSTAM, MD,3 JOANN LINDENFELD, MD,2,3 DOUGLAS L. MANN, MD,2,3 MANDEEP R. MEHRA, MD,2,3 SARA C. PAUL, RN, DNP, FNP,2,3 MARIANN R. PIANO, RN, PhD,2 HEATHER J. ROSS, MD,2 HANI N. SABBAH, PhD,2 RANDALL C. STARLING, MD, MPH,2 JAMES E. UDELSON, MD,2 CLYDE W. YANCY, MD, MSc,3 MICHAEL R. ZILE, MD,2 AND BARRY M. MASSIE, MD2,3
From the 1Chair, ad hoc Committee for Strategic Development, Heart Failure Society of America; 2Member of Executive Council, Heart Failure Society of America and 3Member, ad hoc Committee for Strategic Development, Heart Failure Society of America.
They write:
The preceding 2 decades had been marked by unprecedented insights into the underlying pathophysiology of cardiac dysfunction that were paralleled by therapeutic advances that, for the first time, were shown to clearly improve outcomes in heart failure patients. At the same time, heart failure prevalence was rapidly increasing throughout the world because of the aging of the population, improved survival of patients with myocardial infarction and other cardiac conditions, and inadequate treatment of common risk factors such as hypertension.
More recently the Heart Failure Society successfully promoted establishment of Advanced Heart Failure and Transplant Cardiology as an American Board of Internal Medicine recognized secondary subspecialty of cardiology developed a board review course to help physicians prepare for the certification examination for the new subspecialty and created a national heart failure review course.
The Society has Advocacy goals, membership goals – to increase by 10% per year for 3 years from all disciplines of Heart Failure.
Education Goals:
The Heart Failure Society of America will be recognized for its innovative approaches to educating and content dissemination on heart failure targeting
healthcare professionals and patients
Grow and enhance the annual meeting through innovative approaches
Continue board review course
Increase web-based programs for patients and health care providers
Enhance the website as a portal for information dissemination for health care professionals and patients
Grow and enhance the relevance and value of the Journal of Cardiac Failure
Conceptual analysis of projection done by the AHA regarding the increase in the Cost of Care for the the American Patient in Heart Failure were developed in the following two articles:
National Heart, Lung, And Blood Institute Working Group identified the most urgent knowledge gaps in Heart Transplantation Research. These gaps require to address the following 4 specific research directions:
enhanced phenotypic characterization of the pre-transplant population
donor-recipient optimization strategies
individualized immunosuppression therapy, and
investigations of immune and non-immune factors affecting late cardiac allograft outcomes.
D. Donor-Recipient Optimization Strategies – 33,640 Cases in the United Network for Organ Sharing database – Organ Donor’s Age is BEST predictor for survival after Heart Transplant
IF the donor age is in the 0- to 19-year-old group the median survival of 11.4 years follows the Heart Transplant.
The effect of ischemic time on survival after heart transplantation varies by donor age: An analysis of the United Network for Organ Sharing database
The Journal of Thoracic and Cardiovascular Surgery ● February 2007
Mark J. Russo, MD, MS,a,b Jonathan M. Chen, MD,a Robert A. Sorabella, BA,a Timothy P. Martens, MD,a
Mauricio Garrido, MD,a Ryan R. Davies, MD,a Isaac George, MD,a Faisal H. Cheema, MD,a Ralph S. Mosca, MD,a Seema Mital, MD,c Deborah D. Ascheim, MD,b,d Michael Argenziano, MD,a Allan S. Stewart, MD,a Mehmet C. Oz, MD,a and Yoshifumi Naka, MD, PhDa
Objectives:
(1) To examine the interaction of donor age with ischemic time and their effect on survival and
(2) to define ranges of ischemic time associated with differences in survival.
Methods: The United Network for Organ Sharing provided de-identified patientlevel data. The study population included 33,640 recipients undergoing heart transplantation between October 1, 1987, and December 31, 2004. Recipients were divided by donor age into terciles: 0 to 19 years (n 10,814; 32.1%), 20 to 33 years (11,410, 33.9%), and 34 years or more (11,416, 33.9%). Kaplan-Meier survival functions and Cox regression were used for time-to-event analysis. Receiver operating characteristic curves and stratum-specific likelihood ratios were generated to compare 5-year survival at various thresholds for ischemic time.
Results: In univariate Cox proportional hazards regression, the effect of ischemic time on survival varied by donor age tercile: 0 to 19 years (P .141), 20 to 33 years (P .001), and 34 years or more (P .001). These relationships persisted in multivariable regression. Threshold analysis generated a single stratum (0.37-12.00 hours) in the 0- to 19-year-old group with a median survival of 11.4 years. However, in the 20- to 33-year-old-group, 3 strata were generated: 0.00 to 3.49 hours (limited), 3.50 to 6.24 hours (prolonged), and 6.25 hours or more (extended), with median survivals of 10.6, 9.9, and 7.3 years, respectively. Likewise, 3 strata were generated in the group aged 34 years or more: 0.00 to 3.49 (limited), 3.50 to 5.49 (prolonged), and 5.50 or more (extended), with median survivals of 9.1, 8.5, and 6.3 years, respectively.
Conclusions: The effect of ischemic time on survival after heart transplantation is dependent on donor age, with greater tolerance for prolonged ischemic times among grafts from younger donors. Both donor age and anticipated ischemic time must be considered when assessing a potential donor.
Procedures Outcomes of Heart Transplant (HT) Indication for Heart Failure (HF)
Center for Heart Failure @Cleveland Clinic, and
Transplant Center @Mayo Clinic
Center for Heart Failure @Cleveland Clinic: Institution Profile
Heart failure (sometimes called congestive heart failure or ventricular dysfunction) means your heart muscle is not functioning as well as it should. Either the left ventricle (lower chamber of the heart) is not contracting with enough force (systolic heart failure), or the ventricles are stiff and do not relax and fill properly (diastolic heart failure). The treatment of heart failure requires a specialized multidisciplinary approach to manage the overall patient care plan.
The George M and Linda H Kaufman Center for Heart Failure is one of the premier facilities in the United States for the care of people with heart failure.
The Kaufman Center Heart Failure Intensive Care was the recipient of the Beacon Award of Excellence for continuing improvements in providing the highest quality of care for patients. With over 6,000 ICUs in the Unites States, the Center joins a distinguished group of just 300 to receive this honor that recognizes the highest level of standards in patient safety and quality in acute and critical care.
In 2011, Cleveland Clinic received the American Heart Association’s Get With The Guidelines Heart Failure GOLD Plus Certification for improving the quality of care for heart failure patients. Gold Plus distinction recognizes hospitals for their success in using Get With The Guidelines treatment interventions. This quality improvement program provides tools that follow proven, evidence-based guidelines and procedures in caring for heart failure patients to prevent future hospitalizations.
The Kaufman Center for Heart Failure Team brings together clinicians that specialize in cardiomyopathies and ischemic heart failure. The team includes physicians and nurses from Cardiovascular Medicine, Cardiothoracic Surgery, Radiology, Infectious Disease, Immunology, Pathology, Pharmacy, Biothetics and Social Work with expertise in diagnostic testing, medical and lifestyle management, surgical procedures, and psychosocial support for patients with:
Patients at Cleveland Clinic Kaufman Center for Heart Failure have available to them the full array of diagnostic testing, treatments and specialized programs.
Outcomes of Heart Failure and Heart Transplant @Cleveland Clinic
1,570 Number of heart transplants performed at Cleveland Clinic since inception of the Cardiac Transplant Program in 1984.
The survival rates among patients who have heart transplants at Cleveland Clinic exceeds the expected rates. Of the 150 transplant centers in the United States, Cleveland Clinic is one of only three that had better-than-expected one-year survival rates in 2011.
Ventricular Assist Device Volume 2007 – 2011
2007 – N = 23
2008 – N = 48
2009 – N = 76
2010 – N = 51
2011 – N = 56
Mechanical circulatory support (MCS) devices are used in patients with heart failure to preserve heart function until transplantation (bridge-to-transplant) or as a final treatment option (destination therapy). Cleveland Clinic has more than 20 years of experience with MCS devices for both types of therapy.
LVAD In-Hospital Mortality 2007 – 2011
Cleveland Clinic continues to make improvements to reduce mortality rates among patients who are placed on mechanical circulatory support. The mortality rate among patients who have a left ventricular assist device (LVAD) has been drastically reduced over the past five years.5% in 2011
VAD Mortality 2011
The mortality rate among Cleveland Clinic patients placed on ventricular assist devices (VADs) was much lower than expected in 2011. Observed 10%, Expected 17.5%
Heart Failure – National Hospital Quality Measures
This composite metric, based on four heart failure hospital quality process measures developed by the Centers for Medicare and Medicaid Services (CMS), shows the percentage of patients who received all the recommended care for which they were eligible. Cleveland Clinic has set a target of UHC’s 90th percentile.
Cleveland Clinic, 2010 (N = 1,194) 93.9%
Cleveland Clinic, 2011 (N = 1,163) 96.9%
UHC Top Decile, 2011 99.2%
SOURCE
University HealthSystem Consortium (UHC) Comparative Database, January through November 2011 discharges.
The Centers for Medicare and Medicaid Services (CMS) calculates two heart failure outcome measures: all-cause mortality and all-cause readmission rates, each based on Medicare claims and enrollment information. Cleveland Clinic’s performance appears below.
Heart Failure All-Cause 30-Day Mortality (N = 762) July 2008 – June 2011
Cleveland Clinic 9.2%
National Average 11.6%
Heart Failure All-Cause 30-Day Readmission (N = 1,029) July 2008 – June 2011
Cleveland Clinic 27.3%
National Average 24.7%
SOURCE:
hospitalcompare.hhs.gov
Cleveland Clinic’s heart failure risk-adjusted 30-day mortality rate is below the national average; the difference is statistically significant. Our heart failure risk-adjusted readmission rate is higher than the national average; that difference is also statistically significant. To further reduce this rate, a multidisciplinary team was tasked with improving transitions from hospital to home or post-acute care facility. Specific initiatives have been implemented in each of these focus areas: communication, education and follow-up.
In 2011, 51% of lung transplant patients were from outside the state of Ohio.
Cleveland Clinic surgeons transplanted 111 lungs in 2011. Our Lung and Heart-Lung Transplant
Program is the leader in Ohio and among the best programs in the country.
July 2010 – June 2011
160 Performed in 2009
Liver-Lung
Heart-Lung
Double Lung
Single Lung
53.5% Idiopathic
Primary Disease of Lung Transplant Recipients (N = 101)
Source: Scientific Registry of Transplant Recipients. March 2011. Ohio, Lung Centers, Cleveland Clinic. Table 7
Cleveland Clinic surgeons transplanted 111 lungs in 2011. Our Lung and Heart-Lung Transplant Program is the leader in Ohio and among the best programs in the country.
Transplant Center @Mayo Clinic: Heart Transplant Procedures Outcomes
Mayo Clinic History
Dr. W.W. Mayo
Drs. William (left) and Charles Mayo
Mayo Clinic developed gradually from the medical practice of a pioneer doctor, Dr. William Worrall Mayo, who settled in Rochester, Minn., in 1863. His dedication to medicine became a family tradition when his sons, Drs. William James Mayo and Charles Horace Mayo, joined his practice in 1883 and 1888, respectively.
From the beginning, innovation was their standard and they shared a pioneering zeal for medicine. As the demand for their services increased, they asked other doctors and basic science researchers to join them in the world’s first private integrated group practice.
Although the Mayo doctors were initially viewed as unconventional for practicing medicine through this teamwork approach, the benefits of a private group practice were undeniable.
As the success of their method of practice became evident, so did its acceptance. Patients discovered the advantages to a “pooled resource” of knowledge and skills among doctors. In fact, the group practice concept that the Mayo family originated has influenced the structure and function of medical practice throughout the world.
Along with its recognition as a model for integrated group practice, “the Mayos’ Clinic” developed a reputation for excellence in individual patient care. Doctors and students came from around the world to learn new techniques from the Mayo doctors, and patients came from around the world for diagnosis and treatment. What attracted them was not only technologically advanced medicine, but also the caring attitude of the doctors.
Through the years, Mayo Clinic has nurtured and developed its founders’ style of working together as a team. Shared responsibility and consensus still provide the framework for decision making at Mayo.
That teamwork in medicine is carried out today by more than 55,000 doctors, nurses, scientists, students and allied health staff at Mayo Clinic locations in the Midwest, Arizona and Florida.
Alternative Solutions to Treatment of Heart Failure
Mayo Clinic, with transplant services in Arizona, Florida and Minnesota, performs more transplants than any other medical center in the world. Mayo Clinic has pre-eminent adult and pediatric transplant programs, offering cardiac, liver, kidney, pancreas and bone marrow transplant services. Since performing the first clinical transplant in 1963, Mayo’s efforts to continually improve and expand organ transplantation have placed Mayo at the leading edge of clinical and basic transplant research worldwide. Research activities in the Transplant Center at Mayo Clinic have contributed significantly to the current successful outcomes of organ transplantation.
People who survive a heart attack face the greatest risk of dying from sudden cardiac death (SCD) during the first month after leaving the hospital, according to a long-term community study by Mayo Clinic researchers of nearly 3,000 heart attack survivors.
Sudden cardiac death can happen when the hearts electrical system malfunctions; if treatment — cardiopulmonary resuscitation and defibrillation — does not happen fast, a person dies.
After that first month, the risk of sudden cardiac death drops significantly — but rises again if a person experiences signs of heart failure. The research results appear in the Nov. 5 edition of Journal of the American Medical Association.
Veronique Roger, M.D., a Mayo Clinic cardiologist provides an overview of the study and it’s findings.
For more information on heart attacks, click on the following link:http://www.mayoclinic.org/heart-attack/
VIEW VIDEOon Mayo Clinic Regenerative Medicine Consult Service – Stem Cell Transplantation post MI
In a proof-of-concept study, Mayo Clinic investigators have demonstrated that induced pluripotent stem (iPS) cells can be used to treat heart disease. iPS cells are stem cells converted from adult cells. In this study, the researchers reprogrammed ordinary fibroblasts, cells that contribute to scars such as those resulting from a heart attack, converting them into stem cells that fix heart damage caused by infarction. The findings appear in the current online issue of the journal Circulation.
Timothy Nelson, M.D., Ph.D., first author on the Mayo Clinic study, talks about the study and it’s findings.
Heart Transplant: Volumes and success measures Transplant Center@ Mayo Clinic
Mayo Clinic doctors’ experience and integrated team approach results in transplant outcomes that compare favorably with national averages. Teams work with transplant recipients before, during and after surgery to ensure the greatest likelihood of superior results.
Volumes and statistics are maintained separately for the three Mayo Clinic locations. Taken together or separately, transplant recipients at Mayo Clinic enjoy excellent results.
Volumes
Arizona
More than 100 heart transplants have been completed since the program began in 2005.
Florida
Surgeons at Mayo Clinic in Florida have performed more than 167 heart transplants and eight heart-lung transplants since the program began in 2001. Mayo surgeons have performed combined transplants, such as heart-kidney and heart-lung-liver transplants.
Minnesota
Mayo Clinic’s outcomes for heart transplantation compare favorably with national norms. Doctors at Mayo Clinic in Minnesota have transplanted more than 450 adult and pediatric patients, including both isolated heart transplants and combined transplants such as heart-liver, heart-kidney and others.
The Center for Heart Failure @Cleveland Clinic’s, and the Transplant Center @Mayo Clinic’s Institutions Profiles, Procedures Outcomes and Selection of their Research are now in:
Molecular biomarkers could detect biochemical changes associated with disease processes. The key metabolites have become an important part for improving the diagnosis, prognosis, and therapy of diseases. Because of the chemical diversity and dynamic concentration range, the analysis of metabolites remains a challenge. Assessment of fluctuations on the levels of endogenous metabolites by advanced NMR spectroscopy technique combined with multivariate statistics, the so-called metabolomics approach, has proved to be exquisitely valuable in human disease diagnosis. Because of its ability to detect a large number of metabolites in intact biological samples with isotope labeling of metabolites using nuclei such as H, C, N, and P, NMR has emerged as one of the most powerful analytical techniques in metabolomics and has dramatically improved the ability to identify low concentration metabolites and trace important metabolic pathways. Multivariate statistical methods or pattern recognition programs have been developed to handle the acquired data and to search for the discriminating features from biosample sets. Furthermore, the combination of NMR with pattern recognition methods has proven highly effective at identifying unknown metabolites that correlate with changes in genotype or phenotype. The research and clinical results achieved through NMR investigations during the first 13 years of the 21st century illustrate areas where this technology can be best translated into clinical practice.
In the last decade, proteomics and metabolomics have contributed substantially to our understanding of cardiovascular diseases. The unbiased assessment of pathophysiological processes without a priori assumptions complements other molecular biology techniques that are currently used in a reductionist approach. A discrete biological function is very rarely attributed to a single molecule; more often it is the combined input of many proteins. In contrast to the reductionist approach, in which molecules are studied individually, “omics” platforms allow the study of more complex interactions in biological systems. Combining proteomics and metabolomics to quantify changes in metabolites and their corresponding enzymes will advance our understanding of pathophysiological mechanisms and aid the identification of novel biomarkers for cardiovascular disease.
Marginal deficiency of vitamin B-6 is common among segments of the population worldwide. Because pyridoxal 5′-phosphate serves as a coenzyme in the metabolism of amino acids, carbohydrates, organic acids, and neurotransmitters, as well as in aspects of one-carbon metabolism, vitamin B-6 deficiency could have many effects. NMR spectral features of selected metabolites indicated that vitamin B-6 restriction significantly increased the ratios of glutamine/glutamate and 2-oxoglutarate/glutamate and tended to increase concentrations of acetate, pyruvate, and trimethylamine-N-oxide. Tandem MS showed significantly greater plasma proline after vitamin B-6 restriction, but there were no effects on the profile of 14 other amino acids and 45 acylcarnitines. These findings demonstrate that marginal vitamin B-6 deficiency has widespread metabolic perturbations and illustrate the utility of metabolomics in evaluating complex effects of altered vitamin B-6 intake.
Hepatocellular carcinoma is one of the most common malignancies worldwide, and it has a poor prognosis due to its rapid development and early metastasis. An understanding of tumor metabolism would be helpful for the clinical diagnosis and therapy of hepatocellular carcinoma. To investigate the metabolic features of hepatocellular carcinoma, a non-targeted metabolic profiling strategy based on liquid chromatography-mass spectrometry was performed. The results revealed multiple metabolic changes in the tumor, and the principal changes included elevated glycolysis, inhibition of the tricarboxylic acid cycle, accelerated gluconeogenesis and β-oxidation for energy supply and down-regulated Δ-12 desaturase. Furthermore, increased levels of anti-oxidative molecules, such as glutathione, and decreased levels of inflammatory-related polyunsaturated fatty acids and the phospholipase A2 enzyme were also observed. The differential metabolites found in the tissue were tested in serum samples from the chronic hepatitis, cirrhosis and hepatocellular carcinoma patients. The combination of betaine and propionylcarnitine was confirmed to have a good diagnostic potential to distinguish hepatocellular carcinoma from chronic hepatitis and cirrhosis. External validation of cirrhosis and hepatocellular carcinoma serum samples further shows the combination biomarker is useful for hepatocellular carcinoma diagnosis.
Current diagnostic techniques have increased the detection of prostate cancer; however, these tools inadequately stratify patients to minimize mortality. Recent studies have identified a biochemical signature of prostate cancer metastasis, including increased sarcosine abundance. Prostate tumors had significantly altered metabolite profiles compared to cancer-free prostate tissues, including biochemicals associated with cell growth, energetics, stress, and loss of prostate-specific biochemistry. Many metabolites were further associated with clinical findings of aggressive disease. Aggressiveness-associated metabolites stratified prostate tumor tissues with high abundances of compounds associated with normal prostate function (e.g., citrate and polyamines) from more clinically advanced prostate tumors. These aggressive prostate tumors were further subdivided by abundance profiles of metabolites including NAD+ and kynurenine. When added to multiparametric nomograms, metabolites improved prediction of organ confinement and 5-year recurrence. These findings support and extend earlier metabolomic studies in prostate cancer and studies where metabolic enzymes have been associated with carcinogenesis and/or outcome. Furthermore, it suggests that panels of analytes may be valuable to translate metabolomic findings to clinically useful diagnostic tests.
Article ID #65: Becoming a Cardiothoracic Surgeon: An Emerging Profile in the Surgery Theater and through Scientific Publications. Published on 7/8/2013
WordCloud Image Produced by Adam Tubman
Two components of an Emerging Profile of a Young Cardiothoracic Surgeon were researched by the Author for the case of Dr. Isaac George, Assistant Professor of Surgery, Division of Cardiothoracic Surgery, Department of Surgery, New York Presbyterian Hospital/Columbia University Medical Center , New York, NY.
The two components being:
1. the Cardiothoracic Surgery Theater
2. the Scientific Publications
I noted with interest Dr. George’s second publication, to be about a very well known surgeon in the US and Europe, John Benjamin Murphy. written by Dr. George and two other colleagues, George I, Hardy MA, Widmann WD. published in Curr Surg. 2004 Sep-Oct;61(5):439-41.
I assume that Dr. Murphy’s contributions to Thoracic surgery were of interest to Dr. George to inspire him to write on the subject and elect that Specialty in Surgery.
Murphy was first in the U.S. to induce (1898) artificial immobilization and collapse of the lung in treatment of pulmonary tuberculosis. He was a pioneer in the use of bone grafting and made contributions to the understanding and management of ankylosis as well as independently proposing artificial pneumothorax to manage unilateral lung disease in tuberculosis.
«It is the purpose of every man’s life to do something worthy of the recognition and appreciation of his fellow men. . . . By their superior intellectual qualifications, their fidelity to purpose and above all their indefatigable labour the few become leaders.»
SOURCEWhonamedit? A dictionary of medical eponyms, John Benjamin Murphy
I came across Dr. Isaac George’s name while researching clinical indications for Inhaled Nitric Oxide in June 2013, upon the recent publication of Leaders in Pharmaceutical Business Intelligence FIRST e-Book on Amazon (Biomed e-Books) [Kindle Edition]
Being myself in Analytics and quantitative model design, 1976-2004, I found of particular interest the range of quantitative methodologies used in the following article by Isaac George, assuming that his days at MIT, came very handy in 2006:
George, Isaac, Xydas, Steve, Topkara, Veli K., Ferdinando, Corrina, Barnwell, Eileen C., Gableman, Larissa, Sladen, Robert N., Naka, Yoshifumi, Oz, Mehmet C. Clinical Indication for Use and Outcomes After Inhaled Nitric Oxide Therapy Ann Thorac Surg 2006 82: 2161-2169
As a result of studying this article, I became aware that it has impacted favorably my 6/2013, Editorial decision, for a forthcoming book on Cardiovascular Disease in 2013. The Editorial decision regarding the selection and representation of prominent Cardiothoracic Surgery Theater in the US, and my personal decision to select a Young Cardiothoracic Surgeon
Dr. Isaac George, Assistant Professor of Surgery, Division of Cardiothoracic Surgery, Department of Surgery, New York Presbyterian Hospital/Columbia University Medical Center, New York, NY
Education Profile and Medical Training of a Cardiac Surgeon
NewYork-Presbyterian Hospital/Columbia University Medical Center, New York, NY
2012-present
Assistant Professor of Surgery
Division of Cardiothoracic Surgery, Department of Surgery, New York Presbyterian Hospital/Columbia University Medical Center , New York, NY
Clinical Specialties
Adult aortic and mitral valve surgery
Transcatheter aortic and mitral valve implantation
Hybrid coronary artery bypass surgery
Complex aortic surgery
Complex valvular surgery
Heart failure and transplant surgery
Reoperative cardiac surgery
Thoracic aortic endograft implantation
1. Regulation of myostatin signaling in human cardiomyopathy
2. TGFB regulation in non-syndromic aortic aneurysm formation
3. Valve interstitial cell activation mechanisms after surgical and transcatheter valve replacement
4. Clinical outcomes after valve and hybrid surgery
Education and Training
2011-2012
Interventional Cardiology/Hybrid Cardiac Surgery Fellowship
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2011
Ventricular Assist Device/Cardiac Transplant Fellowship, Minimally Invasive, Cardiac Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2009-2011
Fellow, Cardiothoracic Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2008-2009
Post-Doctoral Clinical Fellow, Cardiothoracic Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2006-2008
Resident, General Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2004-2006
Research Fellow, Cardiothoracic Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2002-2004
Resident, General Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
2001-2002
Internship, General Surgery
New York Presbyterian Hospital – Columbia University Medical Center, New York, NY
1997-2001
MD, Medicine
Duke University School of Medicine, Durham, NC
1993-1997
BS, Mechanical Engineering
Massachusetts Institute of Technology, Cambridge, MA
Board Certifications
American Board of Thoracic Surgery, 2012-
American Board of Surgery, 2008-
Certification, Pediatric Advanced Life Support, 2008-
Certification, Advanced Trauma Life Support, 2006-
MD, State of New York, 2005-
Certification, Advanced Cardiac Life Support/Basic Life Support, 2001-
United States Medical Licensing Examination Step 3, 2004
United States Medical Licensing Examination Step 2, 2001
United States Medical Licensing Examination Step 1, 2000
Professional Honors
2008 Blakemore Prize – Best Resident Research Award, Columbia University College of Physicians and Surgeons
2007 Blakemore Award – Best Resident Research Award, Columbia University College of Physicians and Surgeons
2006 Blakemore Award – Best Resident Research Award, Columbia University College of Physicians and Surgeons
2004 New Era Cardiac Surgery Conference Scholarship
1995 Pi Tau Sigma, Mechanical Engineering Honor Society
1993 Duke University Comprehensive Cancer Center Fellowship
The decision to focus on Cardiothoracic Surgery @Presbeterian as described in Dr. Isaac George’s research had yielded one Sub-Chapter (4.1) in Chapter 4
Cardiac Surgery, Cardiothoracic Surgical Procedures and Percutaneous Coronary Intervention (PCI)/Coronary Angioplasty – Heart and Cardiovascular Medical Devices in Use in Operating Rooms and in Catheterization Labs in the US
in Volume Three in a forthcoming three volume Series of e-Books on Cardiovascular Diseases
This very Sub-Chapter represents milestones in Dr. Isaac George – Becoming a Cardiothoracic Surgeon: An Emerging Profile through Scientific Publications, This profile is now in:
VIEW VIDEOon Mitral Valve Repair and Replacement – Dr. Karl H. Krieger
Dr. Karl H. Krieger, the Vice Chairman of the Department of Cardiothoracic Surgery at NewYork-Presbyterian Hospital/Weill Cornell Medical Center in New York City, discusses treatment for Mitral Valve Disease. Specifically, Dr. Krieger compares the options of Mitral Valve Repair with Mitral Valve Replacement.
This video with Dr. Krieger is from a web cast at the Ronald O. Perelman Heart Institute at NewYork-Presbyterian.
VIEW VIDEOon Left Ventricular Assist Devices (LVADs) – Dr. Jonathan Chen
Dr. Jonathan Chen, the Site Chief for Pediatric Cardiac Surgery at NewYork-Presbyterian Hospital/Weill Cornell Medical Center in New York City, explains how Left Ventricular Assist Devices (LVADs) work and how they can benefit patients with heart failure.
LVADs are implantable devices that help the heart pump blood. They can be used as a temporary therapy, allowing patients’ hearts to rest while they recover from cardiac events such as heart attacks, or while they wait for hearts to become available for transplants. For some patients whose hearts are unlikely to recover and are not candidates for heart transplants, the devices may be used as a permanent therapy. Heart failure, especially in severe forms, can force patients to lead restricted lives because often even very limited physical activity, such as walking from one room to another, will leave them breathless.
Dr. Chen is a pediatric cardiothoracic surgeon, yet the information in the video is applicable to adult patients as well.
Organ transplantation that prolongs and dramatically improves quality of life is nearly a daily occurrence at Columbia University Medical Center.
The success of solid organ transplantation – with improved surgical techniques, replacement organ procurement, and medical management – is advancing each year. Many of these advances have resulted from scientific and clinical research conducted at Columbia University Medical Center.
A Brief History of Transplantation at Columbia
Transplantation: Where we’ve been, where we’re going
Eric A. Rose, MD, former chairman of the department of surgery, left center, performing the first successful pediatric heart transplant in 1984. Transplant pioneer Keith Reemtsma, MD, who is overseeing the operating field (top of photo).
When he transplanted a chimpanzee kidney into a human patient in the late 1960’s, the late Keith Reemtsma, MD, then Department of Surgery Chairman at Tulane University, revolutionized treatment of end-stage organ failure and initiated an era of unprecedented exploration into organ transplantation that would affect the lives of patients around the world.
Transferring to Columbia-Presbyterian Medical Center in 1971, Dr. Reemtsma recruited Mark A. Hardy, MD, who laid another cornerstone of organ transplant medicine by founding the program for dialysis and kidney transplantation. Dr. Hardy based the new program on the principle of collaborative clinical care between surgeons and nephrologists. During a time when renal transplant programs were managed by one or the other discipline but never by both simultaneously, the medical community regarded the concept as folly. Yet the program grew steadily, as did the program’s immune tolerance research initiatives to induce the transplant recipient’s body to accept a donor organ. This multidisciplinary cooperation also led to major contributions in immunogenetics, immunosuppression, and treatment of autoimmune diseases and lymphoma — and it ultimately became the overarching principle for all the NewYork-Presbyterian Hospital transplant services.
Colleagues universally give credit to Eric A. Rose, MD, who co-founded the heart transplantation program with Dr. Reemtsma, for his successful transformation of the program into the outstanding center it is today. A parade of achievements marks the history of the heart transplant program, including the first mechanical bridge-totransplantation using intra-aortic balloon pumps in the 1970’s, and the first successful pediatric heart transplant, performed by Dr. Rose in 1984. Under the guidance of Dr. Rose and his successors, the program has pioneered research in immunosuppressant medications, mechanical assist devices, and minimally invasive surgical procedures. It currently performs over 100 heart transplants yearly, with among the highest success rates in the nation.
Also in 2004, Lloyd E. Ratner, MD, succeeded Dr. Hardy as director of the renal and pancreas transplant program. One of the first to perform laparoscopic donor operations, Dr. Ratner has found creative solutions to overcome immune barriers to kidney transplantation. The program now routinely uses extended-criteria donor organs, performs transplants among incompatible donors, and is a leader in coordinating “donor swaps” to maximize availability of compatible donor organs. Since Dr. Ratner’s arrival, Columbia has been designated one of ten regional islet resource centers in the U.S. that isolate and transplant pancreatic cells to treat type 1 diabetes as part of a limited protocol controlled by the FDA. Recent progress in visualization of pancreatic islets using PET technology, under the guidance of Paul Harris, PhD, has been recognized by the scientific community as a milestone in this developing field.
NYPH/Columbia received UNOS approval for pancreatic transplantation in January 2008. Our premier kidney transplant program is facilitating rapid growth of the new pancreatic transplantation program, which overlaps both in its patient population and its surgical and medical expertise. The northeast region of the U.S. has been consistently underserved as far as access to pancreatic transplantation, with relatively few centers serving a disproportionately large metropolitan population. The expanding program at NewYork-Presbyterian now provides much-needed access to patients with end-stage pancreatic disease in New York state, particularly those with the most complex medical and surgical challenges.
Transplantation of cells, rather than organs, is emerging as a therapy with enormous potential. Transplantation of either a patient’s own or a foreign donor’s bone marrow cells, for example, offers hope of regenerating the heart so that patients with heart failure may be able to avoid heart transplantation.
In introducing the transplantation programs, it would be remiss to neglect mention of the yet another dimension in which they excel — education. Physician training is a top priority, and NYPH/Columbia has trained many of the greatest transplant surgeons over the last 20 years, including many of the leaders of transplant programs throughout the U.S.
At NewYork-Presbyterian Hospital/Columbia University Medical Center, the Transplant Initiative (TI) has been launched to drive the growth of both clinical and research aspects of transplantation. This multi-year undertaking will involve Departments of Medicine, Pathology, Pediatrics, and Surgery and all of the solid organ transplantation programs, both adult and pediatrics. It is led by its Executive Director, Jean C. Emond, MD.
Although NYP/Columbia is already a national leader in clinical transplantation with respect to volume and patient outcomes, this initiative will further leverage the diverse expertise of its transplant scientists and clinicians.
Approximately 2,200 heart transplants are now performed each year in more than 150 heart transplant centers in the United States. The surgeons and cardiologists of Columbia University Medical Center of NYPH have a long and distinguished history of advancing “standards of care” and the survival rates of our patients by using innovative surgical techniques, by applying our basic scientific research in immunosuppression to the clinical setting, and by inventing and perfecting life-sustaining cardiac assist devices that prolong life while waiting for organ availability.
Columbia University Medical Center’s lung and heart-lung transplantation program, which began in 1985, is fast approaching its 200th transplant. Performing more than 30 transplants each year, the lung and heart-lung transplant teams have earned a national reputation for excellence. Our world-renowned transplantation researchers have helped lead the way to improvements in care that, nationwide, have increased the long-term survival rate for lung transplantation by 50% over the past seven years. Among those improvements are new immunosuppressive agents, new antibiotics, refined surgical techniques, and a more comprehensive understanding of follow-up care.
It is the combination of basic research at the molecular cardiology level, biomaterial, surgical procedures and PUBLICATION of Cases and research results that found me in Dr. George’s territory as a renewed inspiration.
For Author’s training & experience @ MGH – Cardiac Floor – Ellison 11, BWH – CCU, Tower 3 – 12Fl, BIDMC – Acute Surgery, Farr 9, and Texas Heart Institute, Perfusion, Faulkner Hospital – ICU
Russo MJ, Chen JM, Sorabella RA, Martens TP, Garrido M, Davies RR, George I, Cheema FH, Mosca RS, Mital S, Ascheim DD, Argenziano M, Stewart AS, Oz MC, Naka Y.
Coronary Reperfusion Therapies: CABG vs PCI – Mayo Clinic preprocedure Risk Score (MCRS) for Prediction of in-Hospital Mortality after CABG or PCI
Author and Curator: Larry H. Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN
Published on Mar 27, 2012
Mayo Clinic cardiologist Charanjit Rihal, M.D. discusses a recent study conducted by Mayo Clinic that focuses on predicting operator outcomes in coronary angioplasty procedures.
“We’ve been interested in prediction of outcomes after coronary angioplasty and stent procedures for some time,” says Dr. Rihal. “Almost ten years ago, we published a paper called ‘The Mayo Clinic Risk Score for Prediction of Adverse Events following Coronary Angioplasty and Stent Procedures’. We’ve since refined into the ‘New Mayo Clinic Risk Score’, which includes seven key variables that predict bad outcomes following PCI procedures.”
The study, which was presented at the 2012 ACC Annual Scientific Session & Expo, presents a novel application of the Mayo Clinic Risk Score to predict operator specific outcomes in coronary angioplasty procedures.
“We looked at the outcomes of over 8000 procedures performed by 21 Mayo Clinic interventional cardiologists as predicted by the Mayo Clinic Risk Score,” says Dr. Rihal. “On an individual basis, we were able to calculate the expected mortality and adverse event rate and compare that to the actual observed mortality and adverse event rate. We were able to show that in our clinical practice of PCI, this risk score was very useful as a performance measure.
In a pleasant surprise, the study also discovered an outlier whose outcomes for instances of adverse event rates were much better than expected. “We don’t know exactly why this operator has such good results,” remarks Dr. Rihal, “But that will be the next phase of this analysis. We can compare procedural, pre-procedural, and post procedural practices of this operator and see if there are things that are translatable to the rest of us.”
VIEW VIDEO
Singh M, Gersh BJ, Li S, Rumsfeld JS, Spertus JA, O’Brien SM, Suri RM, Peterson ED.
BACKGROUND: Current risk models predict in-hospital mortality after either coronary artery bypass graft surgery or percutaneous coronary interventions. The overlap of models suggests that the same variables can define the risks of alternative coronary reperfusion therapies. We sought a preprocedure risk model that can predict in-hospital mortality after either percutaneous coronary intervention or coronary artery bypass graft surgery.
METHODS AND RESULTS: We tested the ability of the recently validated, integer-based Mayo Clinic Risk Score (MCRS) for percutaneous coronary intervention, which is based solely on preprocedure variables:
age,
creatinine,
ejection fraction,
myocardial infarction < or = 24 hours,
shock,
congestive heart failure
peripheral vascular disease
to predict in-hospital mortality among 370,793 patients in the Society of Thoracic Surgeons (STS) database undergoing isolated coronary artery bypass graft surgery from 2004 to 2006. The median age of the STS database patients was 66 years (quartiles 1 to 3, 57 to 74 years), with 37.2% of patients > or = 70 years old. The high prevalence of comorbid conditions included
diabetes mellitus (37.1%)
hypertension (80.5%)
peripheral vascular disease (15.3%)
renal disease (creatinine > or = 1.4 mg/dL; 11.8%).
A strong association existed between the MCRS and the observed mortality in the STS database. The in-hospital mortality ranged between 0.3% (95% confidence interval 0.3% to 0.4%) with a score of 0 on the MCRS and 33.8% (95% confidence interval 27.3% to 40.3%) with an MCRS score of 20 to 24. The discriminatory ability of the MCRS was moderate, as measured by the area under the receiver operating characteristic curve(C-statistic = 0.715 to 0.784 among various subgroups); performance was inferior to the STS model for most categories tested.
CONCLUSIONS: This model is based on the 7 preprocedure risk variables listed above. However, it may be useful for providing patients with individualized, evidence-based estimates of procedural risk as part of the informed consent process before percutaneous or surgical revascularization.
It appears to this reviewer that the model might provide a better AUC if it were reconstructed as follows:
age
estimated creatinine clearance (which has been improved substantially by the Mayo Clinic)
There is another question that This reviewer has about the approach to prediction of post-procedural survival from pre-procedural information.
Age falls into interval classes that would suffice for use as classification variables.
Creatinine is a measurement that is a continuous variable, but I call attention to the fact that eGFR would be preferred, as physicians tend to look at the creatinine roughly in relationship to age, gender, and body size or BMI.
The laboratory contribution as powerful information is underutilized.
On the one hand, CHF is important, but how is the distinction made between
stable CHF and
decompensated CHF, or degrees in between?
This is where the amino-terminal pro b-type natriuretic perptide, or the BNP has been used in isolation, but not in a multivariate model such as described. There is a difference between them, but whether the difference makes a difference is unproved.
The BNP, derived from the propeptide is made by the myocardium as a hormonal mediator of sodium retention. The BNP is degraded by the vascular endothelium, so it’s half time of disappearance would not reflect renal dysfunction, which is not the case for the NT proBNP. This observation has nothing to do with the medical use of BNP.
Three coronary artery bypass grafts, a LIMA to LAD and two saphenous vein grafts – one to the right coronary artery (RCA) system and one to the obtuse marginal (OM) system. (Photo credit: Wikipedia)
Forrester-classification for classification of Congestive heart failure ; Forrester-Klassifikation zur Einteilung einer akuten Herzinsuffizienz (Photo credit: Wikipedia)