Healthcare analytics, AI solutions for biological big data, providing an AI platform for the biotech, life sciences, medical and pharmaceutical industries, as well as for related technological approaches, i.e., curation and text analysis with machine learning and other activities related to AI applications to these industries.
1:15PM 11/12/2014 – 10th Annual Personalized Medicine Conference at the Harvard Medical School, Boston
Reporter: Aviva Lev-Ari, PhD, RN
REAL TIME Coverage of this Conference by Dr. Aviva Lev-Ari, PhD, RN – Director and Founder of LEADERS in PHARMACEUTICAL BUSINESS INTELLIGENCE, Boston http://pharmaceuticalintelligence.com
1:15 p.m. – Keynote Speaker – International Genetics Health and Disease
International Genetics Health and Disease
The principles of personalized medicine and how they affect the lives of people acknowledge no national boundaries. Although there are some differences among the diverse populations around the world in terms of their genetic variation, the general principles of personalized medicine apply uniformly across many populations. Dr. Periz will discuss how personalized medicine is viewed across the many European countries with particular emphasis on how Spain is implementing it into its medical care.
11:30AM 11/12/2014 – 10th Annual Personalized Medicine Conference at the Harvard Medical School, Boston
Reporter: Aviva Lev-Ari, PhD, RN
REAL TIME Coverage of this Conference by Dr. Aviva Lev-Ari, PhD, RN – Director and Founder of LEADERS in PHARMACEUTICAL BUSINESS INTELLIGENCE, Boston http://pharmaceuticalintelligence.com
11:30 Personalized Medicine Coalition Award & Award Recipient Speech
Presentation of Personalized Medicine Coalition’s 10th Annual Award for Leadership in Personalized Medicine.
Brian Munroe PMC Founder and Senior Vice President, Government Affairs
Endo
Award in Science, Business Policy to individual to lead PM – Mark Levin
was at Ely Lilly in the 70s leading supplier of Insulin in the 20s and antibiotics in the 30s,Factor 8, pain drugs, chemotherapy
was at Genentech – Human growth Hormone and Human Insulin — both are PM, Interferon,
was at Mayfield Ventures
was at Millenium, CEO, early 90s, monoclonal antibodies
2000 discussion on the need for PMC
Founder of Foundation Medicine – molecular informatics – expands therapeutics and PM
NOW — with Third Rock Ventures, LLC
Mark Levin – award acceptance speech – Team accomplishments most important
We need to thank the patients participating in Clinical Trials
How I got involved in personalized medicine (PM): High School – Human Biology
Genetics – drive
PM – All diseases – genetic disorders — combination with extreme phenotyping, Muscular Dystrophy – splicing a gene for treatment
Drugability and PM – gene therapy, replace factor, deliver a gene to the brain and the drug. inside CSF
Gene editing – deliver to the Brain correct the gene in the Brain – therapy for ALS, Schizophrenia – understanding the genes involved in this disease, same
Cancer cure – treatment of combination therapies several at the same time vs present time treat one other emerges
cancer vaccine
Sample of blood – proteomics — in Annual Exams at MDs Annual physical
Convergent — comparison of Mutation across to 1000 patient’s mutations
Future is MOST exciting
Challenges of the Future: Biology and Technology, cells in microbiome, 10 million genes, SYSTEM BIOLOGY — will lead the way,
FUNDING SCIENCE via NIH Scientist is the most important National task
Preventative and Prognostics Medicine -need be part of DRUG development
Justification – maximize value for patient vs $$ spent – maximum value – waste and no leadership
Concern — Affordability of Healthcare to All, access to care vs economic Inequality
Leadership and Management: We truly need NATIONAL CONVERSATION — with a Leader with set of goals to solve a problem in certain time
Insurance, Pharma, HMO — budget challenge — attendees inn the room, need to provide leadership at the National Level
9:20AM 11/12/2014 – 10th Annual Personalized Medicine Conference at the Harvard Medical School, Boston
Reporter: Aviva Lev-Ari, PhD, RN
REAL TIME Coverage of this Conference by Dr. Aviva Lev-Ari, PhD, RN – Director and Founder of LEADERS in PHARMACEUTICAL BUSINESS INTELLIGENCE, Boston http://pharmaceuticalintelligence.com
9:20 a.m. Panel Discussion – Genomic Technologies
Genomic Technologies
The greatest impetus for personalized medicine is the initial sequencing of the human genome at the beginning of this Century. As we began to recognize the importance of genetic factors in human health and disease, efforts to understand genetic variation and its impact on health have accelerated. It was estimated that it cost more than two billion dollars to sequence the first human genome and reduction in the cost of sequence became an imperative to apply this technology to many facets of risk assessment, diagnosis, prognosis and therapeutic intervention. This panel will take a brief historical look back at how the technologies have evolved over the last 15 years and what the future holds and how these technologies are being applied to patient care.
Genomic Technologies
Opening Speaker and Moderator:
George Church, Ph.D. Professor of Genetics, Harvard Medical School; Director, Personal Genomics
Genomic Technologies and Sequencing
highly predictive, preventative
non predictive
Shareable Human Genomes Omics Standards
$800 Human Genome Sequence – Moore’s Law does not account for the rapid decrease in cost of Genome Sequencing
Genome Technologies and Applications
Genia nanopore – battery operated device
RNA & protein traffic
Molecular Stratification Methods – more than one read, sequence ties
The meeting, as described by meeting organizer and Steering Committee member of Mid Atlantic Bio Angels Lorraine Marchand, as a “benevolent sharktank”, where presenters get open and honest feedback from experienced venture capitalists on how to improve their pitch and business. The meeting here in Philadelphia was well attended with” over 70 attendants compareable to the 130 we get in New york”, according to MABA Founder Yaniv Sneor.
A few key points were discussed to improve the presenters future pitches to VC.
Define your technology/product, its purpose, how it fills an unmet need, and how you are unique.
Timelines and Milestones VERY IMPORTANT to have specific dates on when and what you will accomplish.
If your EXIT Strategy involves OUT-LICENSING, it is important to keep this in mind when framing your patent
VC’s want to see a STRONG MANAGEMENT TEAM, preferably a CEO from big pharma if you need to deal with them later
if PITCH sounds too much like a science project VC’s would NOT be interested. Show also the BUSINESS not just science
know the REGULATORY RISK – talk with the FDA
if market is small, son’t fret, show PROOF OF CONCEPT then show how relates to other markets
show your TANGIBLE ASSETS in your pitch – if you use a new equipment show it,
Other posts related to this meeting are included below
New Imaging device bears a promise for better quality control of breast-cancer lumpectomies – considering the cost impact
Author and Curator: Dror Nir, PhD
Article 11.5.2 New Imaging device bears a promise for better quality control of breast cancer lumpectomies considering the cost impact
Couple of days ago I have posted on breast-cancer mammography screening and associated costs;Not applying evidence-based medicine drives up the costs of screening for breast-cancer in the USA.Treatment of breast-cancer represents much heavier cost-burden. According to the following publication: Variability in Reexcision Following Breast Conservation Surgery made in JAMA: “Failure to achieve appropriate margins at the initial operation will require additional surgery with re-excision rate estimates ranging from 30% to 60%. These additional operations can produce considerable psychological, physical, and economic stress for patients and delay use of recommended adjuvant therapies. A high percentage (10%-36%) of women requiring reexcision undergo total mastectomy. Thus, the effect of reexcision on altering a patient’s initial treatment of choice is significant.”
Considering that ~70% of the 285,000 new patients diagnosed with breast cancer each year undergoes lumpectomy, this data represents significant cost. Not to mention morbidity, stress and reduce quality of life for the patients. In my post Optical Coherent Tomography – emerging technology in cancer patient managementI discussed the potential of OCT in controlling the quality of lumpectomies in-situ. A workflow that represents potential to reduce the costs of repeated lumpectomies.
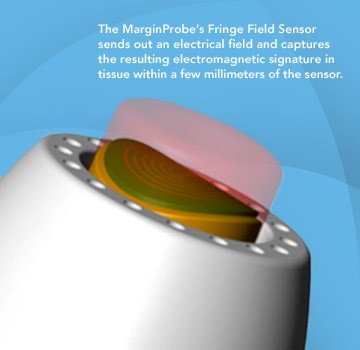
Last week, Dune Medical Devices, Inc., the company that developed the MarginProbeTM System, an intra-operative tissue assessment device to be used as accessory during lumpectomies of early-stage breast cancer, has received Premarket Approval (PMA) by the United States Food and Drug Administration.
FDA approval of the MarginProbe System was based on a 664 patient prospective, multi-center, randomized, double arm study to evaluate the effectiveness of MarginProbe in identifying cancerous tissue along the margins of removed breast tissue during initial lumpectomy procedures. MarginProbe, which uses electromagnetic “signatures” to identify healthy and cancerous tissue, was found to be over three times more effective in finding cancer on the margin during lumpectomy, compared to traditional intra-operative imaging and palpation assessment. This enabled surgeons to significantly reduce the number of patients with positive margins following initial surgery.
The following publication gives an idea on the clinical performance of MarginProbe:
“J Surg Res.2010 May 15;160(2):277-81. doi: 10.1016/j.jss.2009.02.025. Epub 2009 Mar 31.
Diagnostic performance of a novel device for real-time margin assessment in lumpectomy specimens.
Department of General Surgery, Assaf Harofeh Medical Center, Zrifin, Israel. pappo@zahav.net.il
Abstract
BACKGROUND:
Margin status in breast lumpectomy procedures is a prognostic factor for local recurrence and the need to obtain clear margins is often a cause for repeated surgical procedures. A recently developed device for real-time intraoperative margin assessment (MarginProbe; Dune Medical Devices, Caesarea, Israel), was clinically tested. The work presented here looks at the diagnostic performance of the device.
METHODS:
The device was applied to freshly excised lumpectomy and mastectomy specimens at specific tissue measurement sites. These measurement sites were accurately marked, cut out, and sent for histopathologic analysis. Device readings (positive or negative) were compared with histology findings (namely malignant, containing any microscopically detected tumor, or nonmalignant) on a per measurement site basis. The sensitivity and specificity of the device was computed for the full dataset and for additional relevant subgroups.
RESULTS:
A total of 869 tissue measurement sites were obtained from 76 patients, 753 were analyzed, of which 165 were cancerous and 588 were nonmalignant. Device performance on relatively homogeneous sites was: sensitivity 1.00 (95% CI: 0.85-1), specificity 0.87 (95% CI: 0.83-0.90). Performance for the full dataset was: sensitivity 0.70 (95% CI: 0.63-0.77), specificity 0.70 (95% CI: 0.67-0.74). Device sensitivity was estimated to change from 56% to 97% as the cancer feature size increased from 0.7 mm to 6.6 mm. Detection rate of samples containing pure DCIS clusters was not different from rates of samples containing IDC.
CONCLUSIONS:
The device has high sensitivity and specificity in distinguishing between normal and cancer tissue even down to small cancer features.
Copyright (c) 2010 Elsevier Inc. All rights reserved.
PMID: 19628225”
Imagine how cost effective breast cancer management can be if it will involve systems such as these in addition to the systems I discussed in some of my previous posts, for example: What could transform an underdog into a winner?
Not applying evidence-based medicine drives up the costs of screening for breast-cancer in the USA
Author: Dror Nir
Costs for breast screening are being driven higher by increased use of new imaging technologies such as digital mammography and MRI, workflows incorporating 2nd and 3rd remote-readings as quality control measure, use of computer-aided detection (CAD) applications and growth in aged population.
According to recent publication in JAMA, 40% of the annual spending is for screening women ages 75 and older. Under existing guidelines routine screening is not recommended for this age group since “There is insufficient evidence to assess the benefits and harms of screening mammography”
The study population comprised women of 66 to 100 years old. “Forty-two percent of the women in the study were younger than age 75, and almost 60% of this group had one or more screening mammograms. Women ages 75 to 85 represented 40% of the total; 42% of this group had mammograms. Women 85 years and older represented 18% of the total; only 15% of this group had mammograms. Women with multiple chronic health conditions were much less likely to have a mammogram (26.6%) than healthy women (47.4%).”
“Abstract
The Cost of Breast Cancer Screening in the Medicare Population.
Cary P. Gross, MD; Jessica B. Long, MPH; Joseph S. Ross, MD, MHS; Maysa M. Abu-Khalaf, MD; Rong Wang, PhD; Brigid K. Killelea, MD, MPH; Heather T. Gold, PhD; Anees B. Chagpar, MD, MA, MPH, MSc; Xiaomei Ma, PhD
JAMA Intern Med. 2013;():1-7. doi:10.1001/jamainternmed.2013.1397. Published online January 7, 2013
Background Little is known about the cost to Medicare of breast cancer screening or whether regional-level screening expenditures are associated with cancer stage at diagnosis or treatment costs, particularly because newer breast cancer screening technologies, like digital mammography and computer-aided detection (CAD), have diffused into the care of older women.
Methods Using the linked Surveillance, Epidemiology, and End Results–Medicare database, we identified 137 274 women ages 66 to 100 years who had not had breast cancer and assessed the cost to fee-for-service Medicare of breast cancer screening and workup during 2006 to 2007. For women who developed cancer, we calculated initial treatment cost. We then assessed screening-related cost at the Hospital Referral Region (HRR) level and evaluated the association between regional expenditures and workup test utilization, cancer incidence, and treatment costs.
Results In the United States, the annual costs to fee-for-service Medicare for breast cancer screening-related procedures (comprising screening plus workup) and treatment expenditures were $1.08 billion and $1.36 billion, respectively. For women 75 years or older, annual screening-related expenditures exceeded $410 million. Age-standardized screening-related cost per beneficiary varied more than 2-fold across regions (from $42 to $107 per beneficiary); digital screening mammography and CAD accounted for 65% of the difference in screening-related cost between HRRs in the highest and lowest quartiles of cost. Women residing in HRRs with high screening costs were more likely to be diagnosed as having early-stage cancer (incidence rate ratio, 1.78 [95% CI, 1.40-2.26]). There was no significant difference in the cost of initial cancer treatment per beneficiary between the highest and lowest screening cost HRRs ($151 vs $115; P = .20).
Conclusions The cost to Medicare of breast cancer screening exceeds $1 billion annually in the fee-for-service program. Regional variation is substantial and driven by the use of newer and more expensive technologies; it is unclear whether higher screening expenditures are achieving better breast cancer outcomes.”
The study is mainly addressing the difference in costs between different regions of referrals. It would be interesting to explore the situation in the age group of 40 to 66 years old.
The unfortunate ending of the Tower of Babel construction project and its effect on modern imaging-based cancer patients’ management
Curator: Dror Nir, PhD
The story of the city of Babel is recorded in the book of Genesis 11 1-9. At that time, everyone on earth spoke the same language.
Picture: Pieter Bruegel the Elder: The Tower of Babel_(Vienna)
It is probably safe to assume that medical practitioners at that time were reporting the status of their patients in a standard manner. Although not mentioned, one might imagine that, at that time, ultrasound or MRI scans were also reported in a standard and transferrable manner. The people of Babel noticed the potential in uniform communication and tried to build a tower so high that it would reach the gods. Unfortunately, God did not like that, so he went down (in person) and confounded people’s speech, so that they could not understand each another. Genesis 11:7–8.
This must be the explanation for our inability to come to a consensus on reporting of patients’ imaging-outcome. Progress in development of efficient imaging protocols and in clinical management of patients is withheld due to high variability and subjectivity of clinicians’ approach to this issue.
Clearly, a justification could be found for not reaching a consensus on imaging protocols: since the way imaging is performed affects the outcome, (i.e. the image and its interpretation) it takes a long process of trial-and-error to come up with the best protocol. But, one might wonder, wouldn’t the search for the ultimate protocol converge faster if all practitioners around the world, who are conducting hundreds of clinical studies related to imaging-based management of cancer patients, report their results in a standardized and comparable manner?
Is there a reason for not reaching a consensus on imaging reporting? And I’m not referring only to intra-modality consensus, e.g. standardizing all MRI reports. I’m referring also to inter-modality consensus to enable comparison and matching of reports generated from scans of the same organ by different modalities, e.g. MRI, CT and ultrasound.
As developer of new imaging-based technologies, my personal contribution to promoting standardized and objective reporting was the implementation of preset reporting as part of the prostate-HistoScanning product design. For use-cases, as demonstrated below, in which prostate cancer patients were also scanned by MRI a dedicated reporting scheme enabled matching of the HistoScanning scan results with the prostate’s MRI results.
The MRI reporting scheme used as a reference is one of the schemes offered in a report by Miss Louise Dickinson on the following European consensus meeting : Magnetic Resonance Imaging for the Detection, Localisation, and Characterisation of Prostate Cancer: Recommendations from a European Consensus Meeting,Louise Dickinson a,b,c,*, Hashim U. Ahmed a,b, Clare Allen d, Jelle O. Barentsz e, Brendan Careyf, Jurgen J. Futterer e, Stijn W. Heijmink e, Peter J. Hoskin g, Alex Kirkham d, Anwar R. Padhani h, Raj Persad i, Philippe Puech j, Shonit Punwani d, Aslam S. Sohaib k, Bertrand Tomball,Arnauld Villers m, Jan van der Meulen c,n, Mark Emberton a,b,c,
Image of MRI reporting scheme taken from the report by Miss Louise Dickinson
The corresponding HistoScanning report is following the same prostate segmentation and the same analysis plans:
Preset reporting enabling matching of HistoScanning and MRI reporting of the same case.
It is my wish that already in the near-future, the main radiology societies (RSNA, ESR, etc..) will join together to build the clinical Imaging’s “Tower of Babel” to effectively address the issue of standardizing reporting of imaging procedures. This time it will not be destroyed…:-)
Knowing the tumor’s size and location, could we target treatment to THE ROI by applying imaging-guided intervention?
Author: Dror Nir, PhD
Article 9.6.Knowing the tumor’s size and location, could we target treatment to THE ROI by applying imaging-guided intervention?
Advances in techniques for cancer lesions’ detection and localisation [1-6] opened the road to methods of localised (“focused”) cancer treatment [7-10]. An obvious challenge on the road is reassuring that the imaging-guided treatment device indeed treats the region of interest and preferably, only it.
A step in that direction was taken by a group of investigators from Sunnybrook Health Sciences Centre, University of Toronto, Ontario, Canada who evaluate the feasibility and safety of magnetic resonance (MR) imaging–controlled transurethral ultrasound therapy for prostate cancer in humans [7]. Their study’s objective was to prove that using real-time MRI guidance of HIFU treatment is possible and it guarantees that the location of ablated tissue indeed corresponds to the locations planned for treatment. Eight eligible patients were recruited.
The setup
Treatment protocol
The result
“There was excellent agreement between the zone targeted for treatment and the zone of thermal injury, with a targeting accuracy of ±2.6 mm. In addition, the temporal evolution of heating was very consistent across all patients, in part because of the ability of the system to adapt to changes in perfusion or absorption properties according to the temperature measurements along the target boundary.”
Technological problems to be resolved in the future:
“Future device designs could incorporate urinary drainage during the procedure, given the accumulation of urine in the bladder during treatment.”
“Sufficient temperature resolution could be achieved only by using 10-mm-thick sections. Our numeric studies suggest that 5-mm-thick sections are necessary for optimal three-dimensional conformal heating and are achievable by using endorectal imaging coils or by performing the treatment with a 3.0-T platform.”
Major limitation: “One of the limitations of the study was the inability to evaluate the efficacy of this treatment; however, because this represents, to our knowledge, the first use of this technology in human prostate, feasibility and safety were emphasized. In addition, the ability to target the entire prostate gland was not assessed, again for safety considerations. We have not attempted to evaluate the effectiveness of this treatment for eradicating cancer or achieving durable biochemical non-evidence of disease status.”
References
SIMMONS (L.A.M.), AUTIER (P.), ZATURA (F.), BRAECKMAN (J.G.), PELTIER (A.), ROMICS (I.), STENZL (A.), TREURNICHT (K.), WALKER (T.), NIR (D.), MOORE (C.M.), EMBERTON (M.). Detection, localisation and characterisation of prostate cancer by Prostate HistoScanning.. British Journal of Urology International (BJUI). Issue 1 (July). Vol. 110, Page(s): 28-35
WILKINSON (L.S.), COLEMAN (C.), SKIPPAGE (P.), GIVEN-WILSON (R.), THOMAS (V.). Breast HistoScanning: The development of a novel technique to improve tissue characterization during breast ultrasound. European Congress of Radiology (ECR), A.4030, C-0596, 03-07/03/2011.
Wendie A. Berg, Kathleen S. Madsen, Kathy Schilling, Marie Tartar, Etta D. Pisano, Linda Hovanessian Larsen, Deepa Narayanan, Al Ozonoff, Joel P. Miller, and Judith E. Kalinyak Breast Cancer: Comparative Effectiveness of Positron Emission Mammography and MR Imaging in Presurgical Planning for the Ipsilateral Breast Radiology January 2011 258:1 59-72.
Anwar R. Padhani, Dow-Mu Koh, and David J. Collins Reviews and Commentary – State of the Art: Whole-Body Diffusion-weighted MR Imaging in Cancer: Current Status and Research Directions Radiology December 2011 261:3 700-718
Eggener S, Salomon G, Scardino PT, De la Rosette J, Polascik TJ, Brewster S. Focal therapy for prostate cancer: possibilities and limitations. Eur Urol 2010;58(1):57–64).
Black, Peter McL. M.D., Ph.D.; Alexander, Eben III M.D.; Martin, Claudia M.D.; Moriarty, Thomas M.D., Ph.D.; Nabavi, Arya M.D.; Wong, Terence Z. M.D., Ph.D.; Schwartz, Richard B. M.D., Ph.D.; Jolesz, Ferenc M.D. Craniotomy for Tumor Treatment in an Intraoperative Magnetic Resonance Imaging Unit. Neurosurgery: September 1999 – Volume 45 – Issue 3 – p 423
Medel, Ricky MD, Monteith, Stephen J. MD, Elias, W. Jeffrey MD, Eames, Matthew PhD, Snell, John PhD, Sheehan, Jason P. MD, PhD, Wintermark, Max MD, MAS, Jolesz, Ferenc A. MD, Kassell, Neal F. MD. Neurosurgery: Magnetic Resonance–Guided Focused Ultrasound Surgery: Part 2: A Review of Current and Future Applications. October 2012 – Volume 71 – Issue 4 – p 755–763
Bruno Quesson PhD, Jacco A. de Zwart PhD, Chrit T.W. Moonen PhD. Magnetic resonance temperature imaging for guidance of thermotherapy. Journal of Magnetic Resonance Imaging, Special Issue: Interventional MRI, Part 1, Volume 12, Issue 4, pages 525–533, October 2000
Introducing smart-imaging into radiologists’ daily practice.
Author and Curator: Dror Nir, PhD
Article 11.3.1 Introducing smart imaging into radiologists daily practice
Radiology congresses are all about imaging in medicine. Interestingly, radiology originates from radiation. It was the discovery of X-ray radiation at the beginning of the 20th century that opened the road to “seeing” the inside of the human body without harming it (at that time that meant cutting into the body).
Radiology meetings are about sharing experience and knowhow on imaging-based management patients. The main topic is always image-interpretation: the bottom line of clinical radiology! This year’s European Congress of Radiology (ECR) dedicated few of its sessions to recent developments in image-interpretation tools. I chose to discuss the one that I consider contributing the most to the future of cancer patients’ management.
In the refresher course dedicated to computer application the discussion was aimed at understanding the question “How do image processing and CAD impact radiological daily practice?” Experts’ reviews gave the audience some background information on the following subjects:
A. The link between image reconstruction and image analysis.
B. Semantic web technologies for sharing and reusing imaging-related information
C. Image processing and CAD: workflow in clinical practice.
I find item A to be a fundamental education item. Not once did I hear a radiologist saying: “I know this is the lesion because it’s different on the image”. Being aware of the computational concepts behind image rendering, even if it is at a very high level and lacking deep understanding of the computational processes, will contribute to more balanced interpretations.
Item B is addressing the dream of investigators worldwide. Imagine that we could perform a web search and find educating, curated materials linking visuals and related clinical information, including standardized pathology reporting. We would only need to remember that search engines used certain search methods and agree, worldwide, on the method and language to be used when describing things. Having such tools is a pre-requisite to successful pharmaceutical and bio-tech development.
I find item C strongly linked to A, as all methods for better image interpretation must fit into a workflow. This is a design goal that is not trivial to achieve. To understand what I mean by that, try to think about how you could integrate the following examples in your daily workflow: i.e. what kind of expertise is needed for execution, how much time it will take, do you have the infrastructure?
In the rest of this post, I would like to highlight, through examples that were discussed during ECR 2012, the aspect of improving cancer patients’ clinical assessment by using information fusion to support better image interpretation.
Adding up quantitative information from MR spectroscopy (quantifies biochemical property of a target lesion) and Dynamic Contrast Enhanced MR imaging (highlights lesion vasculature).
Image provided by: Dr. Pascal Baltzer, director of mammography at the centre for radiology at Friedrich Schiller University in Jena, Germany
Registration of images generated by different imaging modalities (Multi-modal imaging registration).
The following examples: Fig 2 demonstrates registration of a mammography image of a breast lesion to an MRI image of this lesion. Fig3 demonstrates registration of an ultrasound image of a breast lesion scanned by an Automatic Breast Ultrasound (ABUS) system and an MRI image of the same lesion.
Images provided by members of the HAMAM project (an EU, FP7 funded research project: Highly Accurate Breast Cancer Diagnosis through Integration of Biological Knowledge, Novel Imaging Modalities, and Modelling): http://www.hamam-project.org
Multi-modality image registration is usually based on the alignment of image-features apparent in the scanned regions. For ABUS-MRI matching these were: the location of the nipple and the breast thickness; the posterior of the nipple in both modalities; the medial-lateral distance of the nipple to the breast edge on ultrasound; and an approximation of the ribcage using a cylinder on the MRI. A mean accuracy of 14mm was achieved.
Also from the HAMAM project, registration of ABUS image to a mammography image:
registration of ABUS image to a mammography image, Image provided by members of the HAMAM project (an EU, FP7 funded research project: Highly Accurate Breast Cancer Diagnosis through Integration of Biological Knowledge, Novel Imaging Modalities, and Modelling): http://www.hamam-project.org
Automatic segmentation of suspicious regions of interest seen in breast MRI images
Segmentation of suspicious the lesions on the image is the preliminary step in tumor evaluation; e.g. finding its size and location. Since lesions have different signal/image characteristics to the rest of the breast tissue, it gives hope for the development of computerized segmentation techniques. If successful, such techniques bear the promise of enhancing standardization in the reporting of lesions size and location: Very important information for the success of the treatment step.
Roberta Fusco of the National Cancer Institute of Naples Pascal Foundation, Naples/IT suggested the following automatic method for suspicious ROI selection within the breast using dynamic-derived information from DCE-MRI data.
Automatic segmentation of suspicious ROI in breast MRI images, image provided by Roberta Fusco of the National Cancer Institute of Naples Pascal Foundation, Naples/IT
Her algorithm includes three steps (Figure 2): (i) breast mask extraction by means of automatic intensity threshold estimation (Otsu Thresh-holding) on the parametric map obtained through the sum of intensity differences (SOD) calculated pixel by pixel; (ii) hole-filling and leakage repair by means of morphological operators: closing is required to fill the holes on the boundaries of breast mask, filling is required to fill the holes within the breasts, erosion is required to reduce the dilation obtained by the closing operation; (iii) suspicious ROIs extraction: a pixel is assigned to a suspicious ROI if it satisfies two conditions: the maximum of its normalized time-intensity curve should be greater than 0.3 and the maximum signal intensity should be reached before the end of the scan time. The first condition assures that the pixels within the ROI have a significant contrast agent uptake (thus excluding type I and type II curves) and the second condition is required for the time-intensity pattern to be of type IV or V (thus excluding type III curves).


")













{kind=link}