Update on FDA Policy Regarding 3D Bioprinted Material
Curator: Stephen J. Williams, Ph.D.
Last year (2015) in late October the FDA met to finalize a year long process of drafting guidances for bioprinting human tissue and/or medical devices such as orthopedic devices. This importance of the development of these draft guidances was highlighted in a series of articles below, namely that
- there were no standards as a manufacturing process
- use of human tissues and materials could have certain unforseen adverse events associated with the bioprinting process
In the last section of this post a recent presentation by the FDA is given as well as an excellent pdf here BioprintingGwinnfinal written by a student at University of Kentucky James Gwinn on regulatory concerns of bioprinting.
Bio-Printing Could Be Banned Or Regulated In Two Years
3D Printing News January 30, 2014 No Comments 3dprinterplans

Cross-section of multi-cellular bioprinted human liver tissue Credit: organovo.com
Bio-printing has been touted as the pinnacle of additive manufacturing and medical science, but what if it might be shut down before it splashes onto the medical scene. Research firm, Gartner Inc believes that the rapid development of bio-printing will spark calls to ban the technology for human and non-human tissue within two years.
A report released by Gartner predicts that the time is drawing near when 3D-bioprinted human organs will be readily available, causing widespread debate. They use an example of 3D printed liver tissue by a San Diego-based company named Organovo.
“At one university, they’re actually using cells from human and non-human organs,” said Pete Basiliere, a Gartner Research Director. “In this example, there was human amniotic fluid, canine smooth muscle cells, and bovine cells all being used. Some may feel those constructs are of concern.”
Bio-printing
Bio-printing uses extruder needles or inkjet-like printers to lay down rows of living cells. Major challenges still face the technology, such as creating vascular structures to support tissue with oxygen and nutrients. Additionally, creating the connective tissue or scaffolding-like structures to support functional tissue is still a barrier that bio-printing will have to overcome.
Organovo has worked around a number of issues and they hope to print a fully functioning liver for pharmaceutical industry by the end of this year. “We have achieved thicknesses of greater than 500 microns, and have maintained liver tissue in a fully functional state with native phenotypic behavior for at least 40 days,” said Mike Renard, Organovo’s executive vice president of commercial operations.
clinical trails and testing of organs could take over a decade in the U.S. This is because of the strict rules the U.S. Food and Drug Administration (FDA) places on any new technology. Bio-printing research could outplace regulatory agencies ability to keep up.
“What’s going to happen, in some respects, is the research going on worldwide is outpacing regulatory agencies ability to keep up,” Basiliere said. “3D bio-printing facilities with the ability to print human organs and tissue will advance far faster than general understanding and acceptance of the ramifications of this technology.”
Other companies have been successful with bio-printing as well. Munich-based EnvisionTEC is already selling a printer called a Bioplotter that sells for $188,000 and can print 3D pieces of human tissue. China’s Hangzhou Dianzi University has developed a printer called Regenovo, which printed a small working kidney that lasted four months.
“These initiatives are well-intentioned, but raise a number of questions that remain unanswered. What happens when complex enhanced organs involving nonhuman cells are made? Who will control the ability to produce them? Who will ensure the quality of the resulting organs?” Basiliere said.
Gartner believes demand for bio-printing will explode in 2015, due to a burgeoning population and insufficient levels of healthcare in emerging markets. “The overall success rates of 3D printing use cases in emerging regions will escalate for three main reasons: the increasing ease of access and commoditization of the technology; ROI; and because it simplifies supply chain issues with getting medical devices to these regions,” Basiliere said. “Other primary drivers are a large population base with inadequate access to healthcare in regions often marred by internal conflicts, wars or terrorism.”
It’s interesting to hear Gartner’s bold predictions for bio-printing. Some of the experts we have talked to seem to think bio-printing is further off than many expect, possibly even 20 or 30 years away for fully functioning organs used in transplants on humans. However, less complicated bio-printing procedures and tissue is only a few years away.
FDA examining regulations for 3‑D printed medical devices
Renee Eaton Monday, October 27, 2014

The official purpose of a recent FDA-sponsored workshop was “to provide a forum for FDA, medical device manufacturers, additive manufacturing companies and academia to discuss technical challenges and solutions of 3-D printing.” The FDA wants “input to help it determine technical assessments that should be considered for additively manufactured devices to provide a transparent evaluation process for future submissions.”
Simply put, the FDA is trying to stay current with advanced manufacturing technologies that are revolutionizing patient care and, in some cases, democratizing its availability. When a next-door neighbor can print a medical device in his or her basement, it clearly has many positive and negative implications that need to be considered.
Ignoring the regulatory implications for a moment, the presentations at the workshop were fascinating.
STERIS representative Dr. Bill Brodbeck cautioned that the complex designs and materials now being created with additive manufacturing make sterilization practices challenging. For example, how will the manufacturer know if the implant is sterile or if the agent has been adequately removed? Also, some materials and designs cannot tolerate acids, heat or pressure, making sterilization more difficult.
Dr. Thomas Boland from the University of Texas at El Paso shared his team’s work on 3-D-printed tissues. Using inkjet technology, the researchers are evaluating the variables involved in successfully printing skin. Another bio-printing project being undertaken at Wake Forest by Dr. James Yoo involves constructing bladder-shaped prints using bladder cell biopsies and scaffolding.
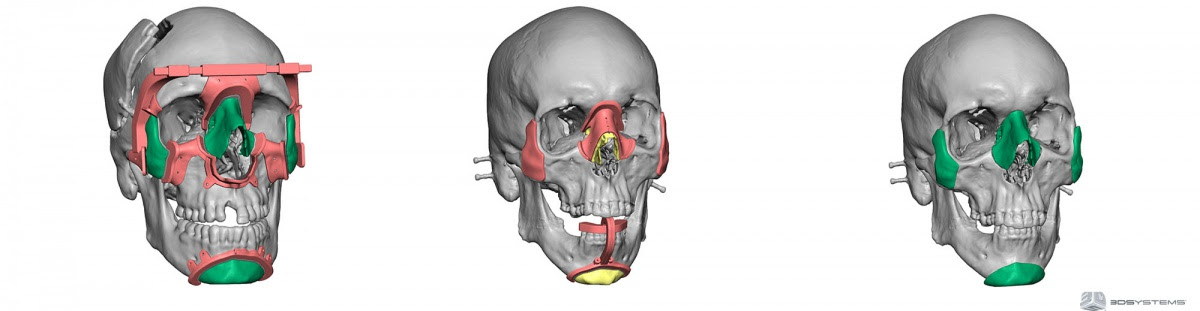
Dr. Peter Liacouras at Walter Reed discussed his institution’s practice of using 3-D printing to create surgical guides and custom implants. In another biomedical project, work done at Children’s National Hospital by Drs. Axel Krieger and Laura Olivieri involves the physicians using printed cardiac models to “inform clinical decisions,” i.e. evaluate conditions, plan surgeries and reduce operating time.
As interesting as the presentations were, the subsequent discussions were arguably more important. In an attempt to identify and address all significant impacts of additive manufacturing on medical device production, the subject was organized into preprinting (input), printing (process) and post-printing (output) considerations. Panelists and other stakeholders shared their concerns and viewpoints on each topic in an attempt to inform and persuade FDA decision-makers.
An interesting (but expected) outcome was the relative positions of the various stakeholders. Well-established and large manufacturers proposed validation procedures: material testing, process operating guidelines, quality control, traceability programs, etc. Independent makers argued that this approach would impede, if not eliminate, their ability to provide low-cost prosthetic devices.
Comparing practices to the highly regulated food industry, one can understand and accept the need to adopt similar measures for some additively manufactured medical devices. An implant is going into someone’s body, so the manufacturer needs to evaluate and assure the quality of raw materials, processing procedures and finished product.
But, as in the food industry, this means the producer needs to know the composition of materials. Suppliers cannot hide behind proprietary formulations. If manufacturers are expected to certify that a device is safe, they need to know what ingredients are in the materials they are using.
Many in the industry are also lobbying the FDA to agree that manufacturers should be expected to certify the components and not the additive manufacturing process itself. They argue that what matters is whether the device is safe, not what process was used to make it.
Another distinction should be the product’s risk level. Devices should continue to be classified as I, II or III and that classification, not the process used, should determine its level of regulation.
Will the FDA Regulate Bioprinting?
Published by Sandra Helsel, May 21, 2014 10:20 am
(3DPrintingChannel) The FDA currently assesses 3D printed medical devices and conventionally made products under the same guidelines, despite the different manufacturing methods involved. To receive device approval, manufacturers must prove that the device is equivalent to a product already on the market for the same use, or the device must undergo the process of attaining pre-market approval. However, the approval process for 3D printed devices could become complicated because the devices are manufactured differently and can be customizable. Two teams at the agency are now trying to determine how approval process should be tweaked to account for the changes.
3D Printing and 3D Bioprinting – Will the FDA Regulate Bioprinting?
This entry was posted by Bill Decker on May 20, 2014 at 8:52 am

VIEW VIDEO
https://www.youtube.com/watch?v=5KY-JZCXKXQ#action=share
The 3d printing revolution came to medicine and is making people happy while scaring them at the same time!
3-D printing—the process of making a solid object of any shape from a digital model—has grown increasingly common in recent years, allowing doctors to craft customized devices like hearing aids, dental implants, and surgical instruments. For example, University of Michigan researchers last year used a 3-D laser printer to create an airway splint out of plastic particles. In another case, a patient had 75% of his skull replaced with a 3-D printed implant customized to fit his head. The 3d printing revolution came to medicine and is making people happy while scaring them at the same time!
Printed hearts? Doctors are getting there
FDA currently treats assesses 3-D printed medical devices and conventionally made products under the same guidelines, despite the different manufacturing methods involved. To receive device approval, manufacturers must prove that the device is equivalent to a product already on the market for the same use, or the device must undergo the process of attaining pre-market approval.
“We evaluate all devices, including any that utilize 3-D printing technology, for safety and effectiveness, and appropriate benefit and risk determination, regardless of the manufacturing technologies used,” FDA spokesperson Susan Laine said.
However, the approval process for 3-D printed devices could become complicated because the devices are manufactured differently and can be customizable. Two teams at the agency now are trying to determine how approval process should be tweaked to account for the changes:
The Stuff of Innovation – 3D Bioprinting and FDA’s Possible Reorganization
Weil Product Liability Monitor on September 10, 2013 ·
Posted in News
Contributing Author: Meghan A. McCaffrey
With 3D printers, what used to exist only in the realm of science fiction — who doesn’t remember the Star Trek food replicator that could materialize a drink or meal with the mere press of a button — is now becoming more widely available with food on demand, prosthetic devices, tracheal splints, skull implants, and even liver tissue all having recently been printed, used, implanted or consumed. 3D printing, while exciting, also presents a unique hybrid of technology and biology, making it a potentially unique and difficult area to regulate and oversee. With all of the recent technological advances surround 3D printer technology, the FDA recently announced in a blog post that it too was going 3D, using it to “expand our research efforts and expand our capabilities to review innovative medical products.” In addition, the agency will be investigating how 3D printing technology impacts medical devices and manufacturing processes. This will, in turn, raise the additional question of how such technology — one of the goals of which, at least in the medical world, is to create unique and custom printed devices, tissue and other living organs for use in medical procedures — can be properly evaluated, regulated and monitored.
In medicine, 3D printing is known as “bioprinting,” where so-called bioprinters print cells in liquid or gel format in an attempt to engineer cartilage, bone, skin, blood vessels, and even small pieces of liver and other human tissues [see a recent New York Times article here]. Not to overstate the obvious, but this is truly cutting edge science that could have significant health and safety ramifications for end users. And more importantly for regulatory purposes, such bioprinting does not fit within the traditional category of a “device” or a “biologic.” As was noted in Forbes, “more of the products that FDA is tasked with regulating don’t fit into the traditional categories in which FDA has historically divided its work. Many new medical products transcend boundaries between drugs, devices, and biologics…In such a world, the boundaries between FDA’s different centers may no longer make as much sense.” To that end, Forbes reported that FDA Commissioner Peggy Hamburg announced Friday the formation of a “Program Alignment Group” at the FDA whose goal is to identify and develop plans “to best adapt to the ongoing rapid changes in the regulatory environment, driven by scientific innovation, globalization, the increasing complexity of regulated products, new legal authorities and additional user fee programs.”
It will be interesting to see if the FDA can retool the agency to make it a more flexible, responsive, and function-specific organization. In the short term, the FDA has tasked two laboratories in the Office of Science and Engineering Laboratories with investigating how the new 3D technology can impact the safety and efficacy of devices and materials manufactured using the technology. The Functional Performance and Device Use Laboratory is evaluating “the effect of design changes on the safety and performance of devices when used in different patient populations” while the Laboratory for Solid Mechanics is assessing “how different printing techniques and processes affect the strength and durability of the materials used in medical devices.” Presumably, all of this information will help the FDA evaluate at some point in the future whether a 3D printed heart is safe and effective for use in the patient population.
In any case, this type of hybrid technology can present a risk for companies and manufacturers creating and using such devices. It remains to be seen what sort of regulations will be put in place to determine, for example, what types of clinical trials and information will have to be provided before a 3D printer capable of printing a human heart is approved for use by the FDA. Or even on a different scale, what regulatory hurdles (and on-going monitoring, reporting, and studies) will be required before bioprinted cartilage can be implanted in a patient’s knee. Are food replicators and holodecks far behind?
http://www.raps.org/regulatory-focus/news/2014/05/19000/FDA-3D-Printing-Guidance-and-Meeting/
- Education & Training
- Jobs & Careers
- Global Network & Community
- News & Trends
- Be Credentialed
- Join RAPS
- Shop RAPS
Home / Regulatory Focus / News
FDA Plans Meeting to Explore Regulation, Medical Uses of 3D Printing Technology
Posted 16 May 2014 By Alexander Gaffney, RAC
The US Food and Drug Administration (FDA) plans to soon hold a meeting to discuss the future of regulating medical products made using 3D printing techniques, it has announced.

Background
3D printing is a manufacturing process which layers printed materials on top of one another, creating three-dimensional parts (as opposed to injection molding or routing materials).
The manufacturing method has recently come into vogue with hobbyists, who have been driven by several factors only likely to accelerate in the near future:
- The cost of 3D printers has come down considerably.
- Electronic files which automate the printing process are shareable over the Internet, allowing anyone with the sufficient raw materials to build a part.
- The technology behind 3D printing is becoming more advanced, allowing for the manufacture of increasingly durable parts.
While the technology has some alarming components—the manufacture of untraceable weapons, for example—it’s increasingly being looked at as the future source of medical product innovation, and in particular for medical devices like prosthetics.
Promise and Problems
But while 3D printing holds promise for patients, it poses immense challenges for regulators, who must assess how to—or whether to—regulate the burgeoning sector.
In a recent FDA Voice blog posting, FDA regulators noted that 3D-printed medical devices have already been used in FDA-cleared clinical interventions, and that it expects more devices to emerge in the future.
Already, FDA’s Office of Science and Engineering laboratories are working to investigate how the technology will affect the future of device manufacturing, and CDRH’s Functional Performance and Device Use Laboratory is developing and adapting computer modeling methods to help determine how small design changes could affect the safety of a device. And at the Laboratory for Solid Mechanics, FDA said it is investigating the materials used in the printing process and how those might affect durability and strength of building materials.
And as Focus noted in August 2013, there are myriad regulatory challenges to confront as well. For example: If a 3D printer makes a medical device, will that device be considered adulterated since it was not manufactured under Quality System Regulation-compliant conditions? Would each device be required to be registered with FDA? And would FDA treat shared design files as unauthorized promotion if they failed to make proper note of the device’s benefits and risks? What happens if a device was never cleared or approved by FDA?
The difficulties for FDA are seemingly endless.
Plans for a Guidance Document
But there have been indications that FDA has been thinking about this issue extensively.
In September 2013, Focus first reported that CDRH Director Jeffery Shuren was planning to release a guidance on 3D printing in “less than two years.”
Responding to Focus, Shuren said the guidance would be primarily focused on the “manufacturing side,” and probably on how 3D printing occurs and the materials used rather than some of the loftier questions posed above.
“What you’re making, and how you’re making it, may have implications for how safe and effective that device is,” he said, explaining how various methods of building materials can lead to various weaknesses or problems.
“Those are the kinds of things we’re working through. ‘What are the considerations to take into account?'”
“We’re not looking to get in the way of 3D printing,” Shuren continued, noting the parallel between 3D printing and personalized medicine. “We’d love to see that.”
Guidance Coming ‘Soon’
In recent weeks there have been indications that the guidance could soon see a public release. Plastics News reported that CDRH’s Benita Dair, deputy director of the Division of Chemistry and Materials Science, said the 3D printing guidance would be announced “soon.”
“In terms of 3-D printing, I think we will soon put out a communication to the public about FDA’s thoughts,” Dair said, according to Plastics News. “We hope to help the market bring new devices to patients and bring them to the United States first. And we hope to play an integral part in that.”
Public Meeting
But FDA has now announced that it may be awaiting public input before it puts out that guidance document. In a 16 May 2014 Federal Register announcement, the agency said it will hold a meeting in October 2014 on the “technical considerations of 3D printing.”
“The purpose of this workshop is to provide a forum for FDA, medical device manufacturers, additive manufacturing companies, and academia to discuss technical challenges and solutions of 3-D printing. The Agency would like input regarding technical assessments that should be considered for additively manufactured devices to provide a transparent evaluation process for future submissions.”
That language—”transparent evaluation process for future submissions”—indicates that at least one level, FDA plans to treat 3D printing no differently than any other medical device, subjecting the products to the same rigorous premarket assessments that many devices now undergo.
FDA’s notice seems to focus on industrial applications for the technology—not individual ones. The agency notes that it has already “begun to receive submissions using additive manufacturing for both traditional and patient-matched devices,” and says it sees “many more on the horizon.”
Among FDA’s chief concerns, it said, are process verification and validation, which are both key parts of the medical device quality manufacturing regulations.
But the notice also indicates that existing guidance documents, such as those specific to medical device types, will still be in effect regardless of the 3D printing guidance.
Discussion Points
FDA’s proposed list of discussion topics include:
- Preprinting considerations, including but not limited to:
- material chemistry
- physical properties
- recyclability
- part reproducibility
- process validation
- Printing considerations, including but not limited to:
- printing process characterization
- software used in the process
- post-processing steps (hot isostatic pressing, curing)
- additional machining
- Post-printing considerations, including but not limited to:
- cleaning/excess material removal
- effect of complexity on sterilization and biocompatibility
- final device mechanics
- design envelope
- verification
– See more at: http://www.raps.org/regulatory-focus/news/2014/05/19000/FDA-3D-Printing-Guidance-and-Meeting/#sthash.cDg4Utln.dpuf
FDA examining regulations for 3‑D printed medical devices
Renee Eaton Monday, October 27, 2014
Share this article
The official purpose of a recent FDA-sponsored workshop was “to provide a forum for FDA, medical device manufacturers, additive manufacturing companies and academia to discuss technical challenges and solutions of 3-D printing.” The FDA wants “input to help it determine technical assessments that should be considered for additively manufactured devices to provide a transparent evaluation process for future submissions.”
Simply put, the FDA is trying to stay current with advanced manufacturing technologies that are revolutionizing patient care and, in some cases, democratizing its availability. When a next-door neighbor can print a medical device in his or her basement, it clearly has many positive and negative implications that need to be considered.
Ignoring the regulatory implications for a moment, the presentations at the workshop were fascinating.
STERIS representative Dr. Bill Brodbeck cautioned that the complex designs and materials now being created with additive manufacturing make sterilization practices challenging. For example, how will the manufacturer know if the implant is sterile or if the agent has been adequately removed? Also, some materials and designs cannot tolerate acids, heat or pressure, making sterilization more difficult.
Dr. Thomas Boland from the University of Texas at El Paso shared his team’s work on 3-D-printed tissues. Using inkjet technology, the researchers are evaluating the variables involved in successfully printing skin. Another bio-printing project being undertaken at Wake Forest by Dr. James Yoo involves constructing bladder-shaped prints using bladder cell biopsies and scaffolding.
Dr. Peter Liacouras at Walter Reed discussed his institution’s practice of using 3-D printing to create surgical guides and custom implants. In another biomedical project, work done at Children’s National Hospital by Drs. Axel Krieger and Laura Olivieri involves the physicians using printed cardiac models to “inform clinical decisions,” i.e. evaluate conditions, plan surgeries and reduce operating time.
As interesting as the presentations were, the subsequent discussions were arguably more important. In an attempt to identify and address all significant impacts of additive manufacturing on medical device production, the subject was organized into preprinting (input), printing (process) and post-printing (output) considerations. Panelists and other stakeholders shared their concerns and viewpoints on each topic in an attempt to inform and persuade FDA decision-makers.
An interesting (but expected) outcome was the relative positions of the various stakeholders. Well-established and large manufacturers proposed validation procedures: material testing, process operating guidelines, quality control, traceability programs, etc. Independent makers argued that this approach would impede, if not eliminate, their ability to provide low-cost prosthetic devices.
Comparing practices to the highly regulated food industry, one can understand and accept the need to adopt similar measures for some additively manufactured medical devices. An implant is going into someone’s body, so the manufacturer needs to evaluate and assure the quality of raw materials, processing procedures and finished product.
But, as in the food industry, this means the producer needs to know the composition of materials. Suppliers cannot hide behind proprietary formulations. If manufacturers are expected to certify that a device is safe, they need to know what ingredients are in the materials they are using.
Many in the industry are also lobbying the FDA to agree that manufacturers should be expected to certify the components and not the additive manufacturing process itself. They argue that what matters is whether the device is safe, not what process was used to make it.
Another distinction should be the product’s risk level. Devices should continue to be classified as I, II or III and that classification, not the process used, should determine its level of regulation.
If you are interested in submitting comments to the FDA on this topic, post them by Nov. 10.
FDA Guidance Summary on 3D BioPrinting






















 BY
BY 




{kind=link}
{kind=link}
{kind=link}