See on Scoop.it – Cardiovascular and vascular imaging
Academic Radiology
See on www.mdlinx.com
Posted in Uncategorized | Leave a Comment »
See on Scoop.it – Cardiovascular and vascular imaging
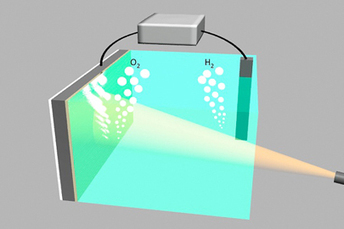
The new device uses light to split water into oxygen and hydrogen, a clean-burning fuel that can be used to generate electricity on demand.
Stanford University scientists have created a silicon-based water splitter that is both low-cost and corrosion-free. The novel device – a silicon semiconductor coated in an ultrathin layer of nickel – could help pave the way for large-scale production of clean hydrogen fuel from sunlight, according to the scientists. Their results are published in the Nov. 15, 2013, issue of the journal Science.
“Solar cells only work when the sun is shining,” said study co-author Hongjie Dai, a professor of chemistry at Stanford. “When there’s no sunlight, utilities often have to rely on electricity from conventional power plants that run on coal or natural gas.”
A greener solution, Dai explained, is to supplement the solar cells with hydrogen-powered fuel cells that generate electricity at night or when demand is especially high.
To produce clean hydrogen for fuel cells, scientists have turned to an emerging technology called water splitting. Two semiconducting electrodes are connected and placed in water. The electrodes absorb light and use the energy to split the water into its basic components, oxygen and hydrogen. The oxygen is released into the atmosphere, and the hydrogen is stored as fuel.
When energy is needed, the process is reversed. The stored hydrogen and atmospheric oxygen are combined in a fuel cell to generate electricity and pure water.
The entire process is sustainable and emits no greenhouse gases. But finding a cheap way to split water has been a major challenge. Today, researchers continue searching for inexpensive materials that can be used to build water splitters efficient enough to be of practical use.
See on news.stanford.edu
Posted in Uncategorized | Leave a Comment »
See on Scoop.it – Cardiovascular and vascular imaging
Journal of Nuclear Cardiology
See on www.mdlinx.com
Posted in Uncategorized | Leave a Comment »
Reporter: Aviva Lev-Ari, PhD, RN
See on Scoop.it – Cardiovascular and vascular imaging
DALLAS — Two studies evaluating therapeutic hypothermia strategies in patients who had experienced an out-of-hospital cardiac arrest — one looking at the timing of induction and one looking at diffe…
See on www.medpagetoday.com
Posted in Cardiogenic Shock, Frontiers in Cardiology and Cardiovascular Disorders | Leave a Comment »
Reporter: Aviva Lev-Ari, PhD, RN
See on Scoop.it – Cardiovascular and vascular imaging
DALLAS — Use of antihypertensive drugs to lower systolic blood pressure by close to 13% as part of acute treatment of ischemic stroke did not reduce early mortality or disability compared with patien…
See on www.medpagetoday.com
Posted in Frontiers in Cardiology and Cardiovascular Disorders, HTN, Origins of Cardiovascular Disease | Leave a Comment »
Posted in Uncategorized | Leave a Comment »
See on Scoop.it – Cardiovascular Disease: PHARMACO-THERAPY
A Clear Choice for Diabetes Patients with Hypertension Diabetes In Control The results from these studies show that ACE inhibitors significantly decreased the doubling of creatinine compared with placebo (OR=0.58; 95% credible interval, 0.32-0.9),…
See on www.diabetesincontrol.com
Posted in Uncategorized | Leave a Comment »
Reporter: Aviva Lev-Ari, PhD, RN
December 11, 2013: 5:30pm – 8:30pm
Over the past decade, the genomics revolution has led to the creation of numerous groundbreaking personalized therapies as well as multiple diagnostic and therapeutic targets. But what will the next field of biology be similar to that which created the genomics revolution? Join us to learn from thought leaders of several Cambridge-based “’omics” companies and institutions as they discuss their role in improving therapeutic effectiveness, realizing potential reductions in adverse effects, and the related promises of cost-effectiveness and efficiencies associated with these advances. We will gain insight from viewing the unique application of epigenetics, metabolomics, microbiomics, proteomics and more from these players to address our individual targeted medical needs and challenges. What are the challenges of commercializing new technologies and new areas of basic biological research? Will the next group of ‘omics contribute to the future of personalized therapies and ultimately improve healthcare outcomes and cost-effectiveness in our complex, expensive healthcare system?
Register
Panelists:
Clary Clish, PhD, Director of Metabolite Profiling, Broad Institute
Bernat Olle, PhD, Principal, PureTech
Robert Copeland, PhD, Executive Vice President and Chief Scientific Officer, Epizyme, Inc.
Edward Driggers, PhD, Senior Director, Cell Metabolism, Agios Pharmaceuticals, Inc.
Posted in Genome Biology | Tagged Agios Pharmaceuticals, genomics, national cancer institute, Proteomics | Leave a Comment »
Reporter: Aviva Lev-Ari, PhD, RN
VIEW VIDEO
Students in Hebrew University-Hadassah Medical Center program develop “science fiction gadgets”
Biodesign entrepreneurship program is Israel’s first medical innovation accelerator
Jerusalem — As health costs spiraled over the last decade, the need for more cost-effective health care systems has become increasingly urgent. Medical innovation plays a vital role in making medicine both efficient and affordable — not to mention improving the quality of patient care and ensuring positive outcomes. However, the process of creating new medical devices requires an in-depth understanding of multiple disciplines including medicine, engineering, and finance that few could master alone. As a result, most aspiring medical innovators face disappointment as the vast majority of ideas fail before reaching the market.
According to Dr. Yaakov Nahmias, the director of The Hebrew University of Jerusalem’s Center for Bioengineering, “When it comes to bringing an idea to market, there is a huge disparity between Hi-Tech, where a few programmers can succeed, and Bio-Tech, where clinicians, engineers, and business experts must all work together to bring a product to the market.”
To solve this problem, Nahmias partnered with Professor Chaim Lotan, the director of Hadassah Medical Center’s Heart Institute and an expert in clinical innovation. According to Prof. Lotan, “We knew that Stanford University’s Biodesign program was the most successful medical innovation program to date, and considering the outstanding students at The Hebrew University and Hadassah we were certain we could give them a run for their money.”

The two partnered with Professor Dan Galai, the former Dean of the Business School at The Hebrew University, and with the help of Dr. Todd Brighton, a Biodesign program director at Stanford University, established The Hebrew University’s Biodesign Medical Innovation Program, the first academic medical innovation accelerator in Israel.
View videos on the innovations
Biodesign is a multi-disciplinary, team-based approach to medical innovation. The program takes outstanding medical fellows, bioengineering and business graduate students, and tutors them in the science and practice of bringing a medical innovation to the market. The teams receive a list of clinical problems, collected from Israeli and American hospitals, and critically evaluate their commercial potential. Once they identify a clinical need with commercial potential, they find an engineering solution that can be protected by a patent application.

The students are mentored by some of Israel’s best and brightest academic and industrial experts, who bring their experience in scientific discovery, clinical applications, and business development.
According to the Hebrew University’s Nahmias, “This isn’t a pure academic exercise. We have students and clinicians who are eager to bring innovation to the market. The program generated quite of lot of excitement with the business and academic environment. It is exactly this drive that makes Israel a start-up nation.”
One year after starting with 20 students and medical fellows, the program has already produced four projects that passed through the proof-of-concept stage, are protected by provisional patent applications, and are showing excellent market potential.
One of the projects, called SAGIV, is a semi-automatic handheld device for rapid and safe IV insertion, using infrared sights and electrical sensing. SAGIV targets a $900 million market with elements already tested on difficult IV insertion cases at the Hadassah Medical Center.
Another project, called GuideIN Tube, is a robotic intubation device which automatically navigates towards the lungs, targeting a $3 billion market.
“The projects really look like science fiction gadgets,” said Dr. Nahmias. “Even if just a few Biodesign companies succeed, they can completely transform the Israeli medical device sector.”
“We have incredibly driven students at The Hebrew University, and Biodesign gives them critical tools they need to succeed,” added Prof. Lotan. Both directors noted that students accomplished in one academic year what many start-up companies take 2 to 3 years to complete, advancing to the point of having proof-of-principle prototypes.
Yehuda Zisapel, president of RAD-Bynet Group, one of the largest investment groups in Israel, said: “Biodesign is a truly innovative approach to generate and accelerate new ideas. The cooperative efforts of physicians, scientists, engineers and business development people allows for a multidimensional approach which encourages the creation and development of new ideas. I was really impressed by the team work and the spirit created by the program, and also by the impressive achievements of the projects.”
Hadassah Medical Center’s Prof. Lotan attributes the program’s success to several additional factors: “We are based in Jerusalem, where biotechnology ventures are buoyed by sustained government support. We are backed by the strong track record of Yissum and Hadasit, the technology transfer companies of The Hebrew University and Hadassah Medical Center. And we have an important relationship with Stanford’s Biodesign program, which offers knowledge, experience and course materials. The Biodesign program has increased Stanford University biomed startup success rates by 4 to 5 folds over the last decade. We envision a similar revolution in Jerusalem, where 50% of the medical research in Israel is already taking place.”
http://www.afhu.org/Israels-first-biodesign-program-produces-four-startups-after-one-year
Posted in Technology Transfer: Biotech and Pharmaceutical | Tagged Hadassah Medical Center, Hebrew University, Hebrew University of Jerusalem, Israel, Stanford University | Leave a Comment »
Larry H Bernstein, MD, FCAP, Reporter Reblog

Article ID #85: Cancer Biomarkers. Published on 11/18/2013
WordCloud Image Produced by Adam Tubman
http://pharmaceuticalintelligence.org/2013-11-17/larryhbern/cancer-biomarkers
Clinical Laboratory News Nov 2013; 39( 11)
By Genna Rollins
It’s a classic conundrum: biomarkers are essential to
yet despite an explosion of research, only a trickle have made it into clinical practice. The factors behind this less-than-desirable circumstance are complex at best, but according to some observers, boil down to the healthcare system’s placing
Without a better means of demonstrating the difference biomarkers make in clinical outcomes or management, they remain stuck in a loop of low value:
A panel of leading scholars, clinicians, and executives recently collaborated about this dilemma in the hopes of starting a national dialogue toward breaking what they call a vicious cycle. Their proposed solutions—as ambitious as the problem is convoluted—can be implemented if the industry has the will to do so, they contend.
“People don’t value tumor biomarkers. They value therapeutics. We all talk about personalized medicine but we don’t really mean it if we’re not willing to value biomarkers the way we value therapeutics,” said Daniel Hayes, MD, Stuart B. Padnos professor of breast cancer research and clinical director of the breast oncology program at the University of Michigan Comprehensive Cancer Center in Ann Arbor. “However,
But without putting the kind of money and research into it that’s necessary to determine clinical utility, payers don’t want to pay as much for a diagnostic as a therapeutic, and we’re stuck in this vicious cycle.”
Hayes has been on the forefront of thinking about how to bring more clinically meaningful biomarkers into cancer care, and he was the lead author of the group’s commentary, which was published
Whether or not they concur with all elements of Hayes’ and his colleagues’ vicious cycle concept, many in the cancer field agree that biomarkers have an anemic batting average. The scientific literature is replete with reports of promising cancer biomarkers, but
While some paradigm-shifting cancer biomarkers with obvious clinical utility have been implemented rapidly in practice, others—be they FDA-cleared or LDTs—never really have found a niche. An example of the latter is
Individuals who are homozygous for the UGT1A1*28 allele are at increased risk for neutropenia when taking irinotecan, but this testing just hasn’t caught on, according to Hayes’ co-author, Richard L. Schilsky, MD, chief medical officer of the American Society of Clinical Oncology (ASCO). “Practically no oncologist orders the test because
There’s not a specific recommendation about whether you’re supposed to
On the other end of the spectrum is KRAS genetic testing in metastatic colon cancer. After seminal research published in 2008 showed that
the test, even as an LDT, quickly became the de facto standard-of-care.
“A wealth of data came out all at the same time, and almost overnight
“That was a clear example of where if the tumor has a mutation,
That’s the kind of discrete information that oncologists are always looking for.”
The KRAS test also hit the medical economics jackpot:
At the same time, the cost of KRAS testing, about $400, speaks to Hayes’ and his colleagues’ arguments about the vicious cycle. If the test has that much clinical impact, shouldn’t it be valued higher in the medical system?
“The pharmaceutical industry
But then we’d have to charge a whole lot more for the tests, which everybody sees as commodities right now,” said Hayes’ co-author Debra Leonard, MD, PhD, professor and chair of pathology at the University of Vermont College of Medicine in Burlington.
That’s why drug companies can charge so much, because all the cost of generating evidence is built into the price of a drug when it comes onto the market. There’s also good evidence to say that it does or doesn’t work, and
To Leonard’s point about evidence, the authors cited one cause of the vicious cycle as how FDA regulates approvals for diagnostic tests (See Figure, below). The agency by statute does not have authority to require that
but that is exactly what the authors would like to see. “In the current regulatory environment, many tumor-biomarker tests
leaving healthcare professionals or third-party payers unsure of whether and how to use the tests or how much to pay for them,” they wrote.
A. Vicious Cycle
B. Virtuous Cycle
(A) The vicious cycle of tumor-biomarker research and clinical utility.
(B) A proposed virtuous cycle of tumor-biomarker research and clinical utility based on proposals herein.
Used with permission of Science Translational Medicine
The authors proposed several solutions to this challenge, some more audacious than others. On the bold side, they suggested that
If those recommendations might be long-term goals, possibly even requiring Congressional approval, others seem more approachable, but perhaps no less controversial. One is that
This contentious topic, under review for more than 3 years at FDA, would, the authors suggest, subject all proposed tests to a risk-based review process, regardless of the manufacturer or commercialization strategy behind them. However, not even all the authors back the idea.
“I don’t believe we can do away with LDTs,” said Leonard. “If the FDA had a better mechanism for looking at LDTs in their risk-based system, that might be helpful. But I worry about everything having to go through FDA because of the slowness of the FDA process and the expense of using the FDA process. There also doesn’t seem to be any idea of how we’re going to get from where we are today to an FDA approval process that actually works.”
Leonard also expressed skepticism that the FDA approval process inherently produces better or more clinically useful tests than do LDTs. “The FDA process does not look at
citing the Health and Human Services Secretary’s Advisory Committee on Genetics, Health, and Society, which, in its 2008 report on the U.S. system of overseeing genetic testing found
Other researchers who have thought about how to speed up the biomarker pipeline also find this recommendation troubling. “Basically eliminating LDTs, especially if this were not accompanied by a prior increase in reimbursement and research dollars, would be extremely negative,” said Leigh Anderson, PhD, CEO of Washington, D.C.-based SISCAPA Assay Technologies. “I’m involved in collaborative work with a number of groups trying to develop new tests mainly in the cancer area and I don’t think any of them would be in the position
They would have to raise hundreds of millions of additional dollars to take that approach. It’s not trivial to develop an LDT, but to say
Although Anderson wasn’t on board with the authors’ proposal about LDTs, he lauded their recommendation that
In fact, writing in a Clinical Chemistry opinion piece along with the journal’s editor-in-chief Nader Rifai, PhD, he recommended that
This “would allow
Along with the need to provide higher levels of evidence for candidate cancer biomarkers, the authors called for a significant
In addition, they recommended that
Finally, they proposed that guideline bodies follow evidence-based recommendations for tumor biomarker test use.
To up the ante on these sweeping reforms, the authors believe addressing them in concert is the only way to break the vicious cycle. But how can the healthcare industry essentially reinvent a new paradigm for better valuing cancer biomarkers when the elements of doing so are like a gyrating Medusa’s head of knotty, seemingly intractable challenges? The authors agree the problem is too daunting if considered only in its entirety. But they and other experts suggest that several tangible actions could move the field along substantially without too much chaos or pain.
For example, in the area of building evidence that would open the door for better reimbursement for cancer biomarker tests,
This ground-breaking initiative managed by the American College of Radiology (ACR) and the ACR Imaging Network developed evidence for Medicare to reimburse PET scanning with F-18 fluorodeoxyglucose when it wasn’t covered at all. NOPR enabled reimbursement for this testing in cancer patients on the proviso that physicians agreed to enter data in a registry that would enable a fair assessment of the impact PET had on cancer patient management. Started in 2006, NOPR led in 2009 to coverage of PET scans as part of the initial treatment strategy for most solid tumors, coverage that recently
By doing the same thing with selected tumor biomarkers, Schilsky suggested, “we immediately begin to capture information that we’re not currently getting on
he explained. “Then, for payers, it becomes much less of a Wild West environment. They will have information they can analyze and use to inform their coverage decisions.” Such a system also would differentiate the most clinically useful tests from less relevant ones, enabling payers to shift resources to the winning tests. This, in turn, would incentivize test developers “to put tests out that are likely to perform well,” Schilsky added.
The authors also point to efforts like the National Human Genome Research Institute’s recent decision to fund more than $25 million over 4 years to develop the Clinical Genome Resource for
The National Cancer Institute (NCI) also is planning a
Anderson believes the authors overlooked the impact technological advances could have on the vicious cycle, by speeding up the process of vetting candidate biomarkers. “An alternative way of doing mass spectrometry [MS]-based protein assays is
“Those kinds of directed assay methods which are not looking for everything, but instead for specific things that you hypothesize are important biomarkers, can be run
That then removes the primary technological limitation to getting the validation of biomarkers done.”
Anderson added that this type of MS-based directed protein analysis also could speed up the bench-to-bedside time for biomarkers. “The advantage is that the same method used in biomarker verification studies at the research stage can be
“That it can be taken all the way from research to LDT in a capable reference lab takes a lot of delay out of the introduction into clinical practice. That’s because you don’t need to redevelop immunoassays for different platforms. Eventually you might not even need to redevelop it for an IVD platform, once mass spectrometry IVD platforms exist.” He predicted that this approach could shave 5–10 years from the biomarker development process. Anderson’s company, SISCAPA Assay Technologies, provides mass-spec-based specific assays for biomarker proteins.
Researchers also have a responsibility to think about the clinical need they want to address before diving deep into discovery, suggested Ivan Blasutig, PhD, a clinical biochemist and assistant professor at Toronto General Hospital and the University of Toronto. “Many of the biomarkers discovered may have statistically significant results but when it comes to actual clinical use they don’t cut it. That’s one of the biggest issues,” he said.
Blasutig collaborates closely with Eleftherios Diamandis, MD, PhD, who has written extensively about the challenges of bringing proposed cancer biomarkers into clinical practice. He, Diamandis, and others have emphasized how important robust analytics are in the early stages of biomarker discovery. In fact Blasutig and Diamandis recently wrote about how using what turned out to be an unreliable commercial kit for CUZD1 detection set back their research team by 2 years and about $500,000 in their quest to find a new pancreatic cancer biomarker (Clin Chem 2013 doi:10.1373/clinchem.2013.215236).
Blasutig and others encouraged clinical laboratorians to participate actively in biomarker discovery, as they bring a wealth of knowledge about analytical issues in validation that research chemists don’t necessarily share. Laboratorians also are more likely to be aware of resources like the NCI’s Early Detection Research Network, which gives guidance on topics such as completing sample collections and avoiding analytical bias, Blasutig suggested.
If the vicious cycle seems completely unwieldy and unrepairable, each person CLN contacted expressed confidence that even in the face of long odds, it can be changed. Leonard spoke for many: “I’m optimistic that we have to do this for our patients, and for our healthcare delivery system. There are a lot of good people around who are interested in having this conversation. So if we can just get all the parties at the table and see if there are some concrete steps that we can take, that would be a major step in the right direction.”
The clinical laboratory has been concentrating on technical accuracy considerably beyond the clinical utility of many observations in clinical medicine. This is not necessarily appreciated, so when a test is inconsistent with the clinical hypothesis, it may be rejected as error. Errors may occur, but are rare, except if there is specimen misidentification. However, we are still focused on a “silver bullet” approach to use of diagnostic tests. There is some variability of the expression of cancer cells, so that there are subclusters to be expected within a major class. The level of applied mathematics that is needed to analyze this data has been refined enormously in the last decade, and has to be used on the selected groups of tests referred to with all due respect by Leigh Anderson, who has the imagination to pursue the highest accuracy in large scale MS analysis that his laboratory has pursued for many years. This reviewer is interested in the “information content” of a combination of tests, when the accuracy of testing is no longer an issue. By combining the high throuput and lower cost of processing, with vastly better mathematical technology than is customary – on the fly – would be a breakthrough. That would not be the end of this journey because there would have to be centers for analysis distributed within a few hours of the treatment centers (or at those sites), so that testing and processing would enable better facilitation of treatment.
Posted in Biomarkers & Medical Diagnostics, CANCER BIOLOGY & Innovations in Cancer Therapy, Cancer Prevention: Research & Programs, Cell Biology, Signaling & Cell Circuits, Genome Biology, Genomic Testing: Methodology for Diagnosis, Health Economics and Outcomes Research, Interviews with Scientific Leaders, Molecular Genetics & Pharmaceutical, Personalized and Precision Medicine & Genomic Research, Population Health Management, Genetics & Pharmaceutical | Tagged best practice, biomarkers, Cancer - General, diagnostic testing, FDA 510K, FDA clearance, FDA innovation route, R&D, test utilization | Leave a Comment »