Atherosclerosis Independence: Genetic Polymorphisms of Ion Channels Role in the Pathogenesis of Coronary Microvascular Dysfunction and Myocardial Ischemia (Coronary Artery Disease (CAD))
Reviewer and Co-Curator: Larry H Bernstein, MD, FCAP
and
Curator: Aviva Lev-Ari, PhD, RN

Image created by Adina Hazan 06/30/2021
The role of ion channels in Na(+)-K(+)-ATPase: regulation of ion transport across the plasma membrane has been studied by our Team in 2012 and 2013. This is article TWELVE in a 13 article series listed at the end of this article.
Chiefly, our sources of inspiration were the following:
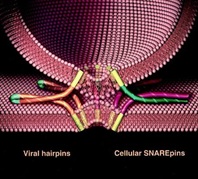
1. 2013 Nobel work on vesicles and calcium flux at the neuromuscular junction
Machinery Regulating Vesicle Traffic, A Major Transport System in our Cells
The 2013 Nobel Prize in Physiology or Medicine is awarded to Dr. James E. Rothman, Dr. Randy W. Schekman and Dr. Thomas C. Südhof for their discoveries of machinery regulating vesicle traffic, a major transport system in our cells. This represents a paradigm shift in our understanding of how the eukaryotic cell, with its complex internal compartmentalization, organizes the routing of molecules packaged in vesicles to various intracellular destinations, as well as to the outside of the cell. Specificity in the delivery of molecular cargo is essential for cell function and survival.
http://www.nobelprize.org/nobel_prizes/medicine/laureates/2013/advanced-medicineprize2013.pdf
Synaptotagmin functions as a Calcium Sensor: How Calcium Ions Regulate the fusion of vesicles with cell membranes during Neurotransmission
Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
2. Perspectives on Nitric Oxide in Disease Mechanisms
available on Kindle Store @ Amazon.com
http://www.amazon.com/dp/B00DINFFYC
3. Professor David Lichtstein, Hebrew University of Jerusalem, Dean, School of Medicine
Lichtstein’s main research focus is the regulation of ion transport across the plasma membrane of eukaryotic cells. His work led to the discovery that specific steroids that have crucial roles, as the regulation of cell viability, heart contractility, blood pressure and brain function. His research has implications for the fundamental understanding of body functions, as well as for several pathological states such as heart failure, hypertension and neurological and psychiatric diseases.
Physiologist, Professor Lichtstein, Chair in Heart Studies at The Hebrew University elected Dean of the Faculty of Medicine at The Hebrew University of Jerusalem
Reporter: Aviva Lev-Ari, PhD, RN
4. Professor Roger J. Hajjar, MD at Mount Sinai School of Medicine
Calcium Cycling (ATPase Pump) in Cardiac Gene Therapy: Inhalable Gene Therapy for Pulmonary Arterial Hypertension and Percutaneous Intra-coronary Artery Infusion for Heart Failure: Contributions by Roger J. Hajjar, MD
Aviva Lev-Ari, PhD, RN
5. Seminal Curations by Dr. Aviva Lev-Ari on Genetics and Genomics of Cardiovascular Diseases with a focus on Conduction and Cardiac Contractility
Aviva Lev-Ari, PhD, RN
Aviva Lev-Ari, PhD, RN
Aviva Lev-Ari, PhD, RN and Larry H. Bernstein, MD, FCAP
Justin Pearlman, MD, PhD, FACC, Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Other related research by the Team of Leaders in Pharmaceutical Business Intelligence published on the Open Access Online Scientific Journal
http://pharmaceuticalintelligence.com
See References to articles at the end of this article on
- ION CHANNEL and Cardiovascular Diseases
http://pharmaceuticalintelligence.com/?s=Ion+Channel
- Calcium Role in Cardiovascular Diseases – The Role of Calcium Calmodulin Kinase (CKCaII) and Ca(2) flux
- Mitochondria and Oxidative Stress Role in Cardiovascular Diseases
Thus, the following article follows a series of articles on ion-channels and cardiac contractility mentioned, above. The following article is closely related to the work of Prof. Lichtstein.
These investigators studied the possible correlation between
- Myocardial Ischemia (Coronary Artery Disease (CAD)) aka Ischemic Heart Disease (IHD) and
- single-nucleotide polymorphisms (SNPs) genes encoding several regulators involved in Coronary Blood Flow Regulation (CBFR), including
- ion channels acting in vascular smooth muscle and/or
- endothelial cells of coronary arteries.
They completely analyzed exon 3 of both KCNJ8 and KCNJ11 genes (Kir6.1 and Kir6.2 subunit, respectively) as well as
- the whole coding region of KCN5A gene (Kv1.5 channel).
- to identify individuals at relatively low-risk for cardiovascular disease
- an independent protective role of the
- rs5215_GG against developing CAD and
- a trend for rs5219_AA to be associated with protection against coronary microvascular dysfunction
Their findings are a lead into further investigations on ion channels and IHD affecting the microvasculature.
Role of genetic polymorphisms of ion channels in the pathophysiology of coronary microvascular dysfunction and ischemic heart disease
BasicResCardiol(2013)108:387 http//dx.dio.org/10.1007/s00395-013-0387-4
F Fedele1•M Mancone1•WM Chilian2•P Severino2•E Canali•S Logan•ML DeMarchis3•M Volterrani4•R Palmirotta3•F Guadagni3
1Department of Cardiovascular, Respiratory, Nephrology, Anesthesiology and Geriatric Sciences,Sapienza University of Rome, UmbertoI Policlinic, Rome, Italy e-mail:francesco.fedele@uniroma1.it
2Department of Integrative Medical Sciences, Northeastern Ohio Universities College of Medicine, Rootstown,OH
3Department of Advanced Biotechnologies and Bioimaging, IRCCS San Raffaele Pisana,Rome,It
4Cardiovascular Research Unit, Department of Medical Sciences, Centre for Clinical and Basic Research, Raffaele Pisana, Rome, Italy (CBFR)
BasicResCardiol(2013)108:387 http//dx.dio.org/10.1007/s00395-013-0387-4
This article is published with open access at Springerlink.com
Abstract
Conventionally,ischemic heart disease (IHD) study is equated with large vessel coronary disease (CAD). However, recent evidence has suggested
- a role of compromised microvascular regulation in the etiology of IHD.
Because regulation of coronary blood flow likely involves
- activity of specific ion-channels, and
- key factors involved in endothelium-dependent dilation,
genetic anomalies of ion-channels or specific endothelial-regulators may underlie coronary microvascular disease.
We aimed to evaluate the clinical impact of single-nucleotide polymorphisms in genes encoding for
- ion-channels expressed in the coronary vasculature and the possible
- correlation with IHD resulting from microvascular dysfunction.
242 consecutive patients who were candidates for coronary angiography were enrolled. A prospective, observational, single-center study was conducted,
- analyzing genetic polymorphisms relative to
(1) NOS3 encoding for endothelial nitric oxide synthase (eNOS);
(2) ATP2A2 encoding for the Ca/H-ATP-ase pump (SERCA);
(3) SCN5A encoding for the voltage-dependent Na channel (Nav1.5);
(4) KCNJ8 and in KCNJ11 encoding for the Kir6.1and Kir6.2 subunits
of genetic K-ATP channels, respectively;and
(5) KCN5A encoding for the voltage-gated K channel (Kv1.5).
No significant associations between clinical IHD manifestations and
- polymorphisms for SERCA, Kir6.1, and Kv1.5. were observed (p[0.05),
whereas specific polymorphisms detected in eNOS, as well as in Kir6.2 and Nav1.5 were found to be correlated with
- IHD and microvascular dysfunction.
Interestingly, genetic polymorphisms of ion-channels seem to have an important clinical impact
- influencing the susceptibility for microvascular dysfunction and (IHD,
- independent of the presence of classic cardiovascular risk factors: atherosclerosis
http//dx.dio.org/10.1007/s00395-013-0387-4
Keywords: Ion-channels, Genetic polymorphisms, Coronary microcirculation, Endothelium, Atherosclerosis Ischemic heart disease
Introduction
Historically, in the interrogation of altered vascular function in patientswith ischemic heart disease (IHD), scientists have focused their attention on the correlation between
- endothelial dysfunction and
- atherosclerosis [11, 53, 65, 67].
The endothelium-independent dysfunction in coronary microcirculation and its possible correlations with
- atherosclerotic disease and
- myocardial ischemia has not been extensively investigated.
In normal conditions, coronary blood flow regulation (CBFR) is mediated by several different systems, including
- endothelial,
- nervous,
- neurohumoral,
- myogenic, and
- metabolic mechanisms [2, 10, 14, 15, 63, 64, 69].
Physiologic CBFR depends also on several ion channels, such as
- ATP-sensitive potassium (KATP) channels,
- voltage-gated potassium (Kv) channels,
- voltage-gated sodium (Nav) channels, and others.
Ion channels regulate the concentration of calcium in both
- coronary smooth muscle and endothelial cells, which
- modulates the degree of contractile tone in vascular muscle and
- the amount of nitric oxide that is produced by the endothelium
Ion channels play a primary role in the rapid response of both
- the endothelium and vascular smooth muscle cells of coronary arterioles
- to the perpetually fluctuating demands of the myocardium for blood flow
[5, 6, 13, 18, 33, 45, 46, 51, 52, 61, 73, 75].
Despite this knowledge, there still exists an important gap about
- the clinical relevance and
- causes of microvascular dysfunction in IHD.
By altering the overall
- regulation of blood flow in the coronary system,
- microvascular dysfunction could alter the normal distribution of shear forces in large coronary arteries
Proximal coronary artery stenosis could
- contribute to microvascular dysfunction [29, 60]. But
- ion channels play a critical role in microvascular endothelial
- and smooth muscle function.
Therefore, we hypothesized that alterations of coronary ion channels could be the primary cause in a chain of events leading to
- microvascular dysfunction and
- myocardial ischemia,
independent of the presence of atherosclerosis.
Therefore, the objective of our study was to evaluate the possible correlation between
- IHD and single-nucleotide polymorphisms (SNPs) for genes encoding several regulators involved in CBFR, including
- ion channels acting in vascular smooth muscle and/or
- endothelial cells of coronary arteries.
Discussion
Implications of the present work. This study describes the possible correlation of polymorphisms in genes encoding for CBFR effectors (i.e., ion channels, nitric oxide synthase, and SERCA) with the susceptibility for microcirculation dysfunction and IHD.
Our main findings are as follows: (Group 3 – Normal Patients – anatomically and functionally normal coronary arteries).
- In Group 3, the genotype distribution of SNP rs5215 (Kir6.2/KCNJ11) moderately deviates from the HW equilibrium (p = 0.05).
- In Group 1 (CAD), the polymorphism rs6599230 of Nav1.5/SCN5A showed deviation from HW equilibrium (p = 0.017).
- The genotypic distribution of rs1799983 polymorphism for eNOS/NOS3 is inconsistent with the HW equilibrium in groups 1, 2, and 3 (p = 0.0001, p = 0.0012 and p = 0.0001, respectively).
Haplotype analyses revealed that there is no linkage disequilibrium between polymorphisms of the analyzed genes. There was no significant difference in the prevalence of T2DM (p = 0.185) or dyslipidemia (p = 0.271) between groups, as shown in Table2. In regards to genetic characteristics, no significant differences between the three.
1. A marked HW disequilibrium in the genotypic distribution of rs1799983 polymorphism for eNOS/NOS3 was observed in all three populations. Moreover, this SNP seems to be an independent risk factor for microvascular dysfunction, as evidenced by multivariate analysis;
2. The SNPs rs5215_GG, rs5218_CT, and rs5219_AA for Kir6.2/KCJ11 could reduce susceptibility to IHD, since they were present more frequently in patients with anatomically and functionally normal coronary arteries;
3. In particular, with regard to rs5215 for Kir6.2/KCJ11, we observed a moderate deviation from the HW equilibrium in the genotypic
distribution in the control group. In addition, this genotype appears to be an independent protective factor in the development of IHD, as evidenced by multivariate analysis;
4. Furthermore, the trend observed for the SNP rs5219_AA of Kir6.2/KCNJ11 may suggest an independent protective factor in the development of coronary microvascular dysfunction
5. The rs1805124_GG genotype of Nav1.5/SCN5A seems to play a role against CAD;
6. No association seems to exist between the polymorphisms of SERCA/ATP2A2, Kir6.1/KCNJ8, and Kv1.5/KCNA5 and the presence of IHD;
7. All groups are comparable regarding the cardiovascular risk factors of T2DM and dyslipidemia, illustrating a potentially important implication of genetic polymorphisms in the susceptibility to IHD.
It is important to underline that the control group (Group 3) is a high-risk population, because of their cardiovascular risk factors
- hypertension = 17 %,
- T2DM = 34.1 %,
- dyslipidemia = 41.4 %,
with an appropriate indication for coronary angiography, in accordance with current guidelines. Nevertheless, these patients were demonstrated to have both anatomically and functionally normal coronary arteries. Moreover, as shown in Tables 2 and 3, we observed that
- rs5215_GG, rs5218_CT and rs5219_AA for Kir6.2/KCNJ11 had a higher prevalence in this group,compared to patients with CAD
- and patients with microvascular dysfunction.
Moreover, as shown in Table 4, the presence of the rs5215_GG polymorphism for the Kir6.2 subunit was
- inversely correlated with the prevalence of cardiovascular risk factors and CAD,whereas
- rs5219_AA of the Kir6.2 subunit trended towards an inverse correlation with coronary microvascular dysfunction.
On the other hand, the SNP rs1799983_GT of eNOS was
- confirmed to be an independent risk factor for microvascular dysfunction.
Our data suggest that the presence of certain genetic polymorphisms may represent a non-modifiable protective factor that could be used
- to identify individuals at relatively low-risk for cardiovascular disease,
- regardless of the presence of T2DM and dyslipidemia.
Current Clinical and Research Context
In normal coronary arteries, particularly the coronary microcirculation, there are several different mechanisms of CBFR, including
- endothelial, neural, myogenic, and metabolic mediators [2, 8, 10, 12, 14, 15, 37, 55, 63, 64, 69].
In particular, endothelium-dependent vasodilation acts mainly via eNOS-derived nitric oxide (NO) in response to acetylcholine and shear stress.
- NO increases intracellular cyclic guanosine monophosphate. It also causes vasodilation via
- activation of both K-Ca channels and K-ATP channels.
Recent data suggested a pathophysiologically relevant role for the polymorphisms of eNOS/NOS3 in human coronary vasomotion [40–43]. Our data suggest that rs1799983_GT at exon 7 (Glu298Asp, GAG-GAT) of eNOS/NOS3 represents
- an independent risk factor for coronary micro-vascular dysfunction, which agrees with a recent meta-analysis reporting an
- association of this SNP with CAD in Asian populations [74]. In addition,
- this SNP has been associated with endothelial dysfunction, although the mechanisms are not well defined [30].
Consistently, a recent study performed on 60 Indian patients with documented history of CAD reported a significantly higher frequency of rs1799983 (p.05) compared to control subjects, indicating that
- variations in NOS3 gene may be useful clinical markers of endothelial dysfunction in CAD [54].
- high-grade coronary stenosis or occlusion [19].
- potassium channels determine the resting membrane potential (Em) and serve as targets of endogenous and therapeutic vasodilators [9, 27].
- The K-ATP channels couple cell metabolic demand to conductance, via pore-forming (Kir6.1 and/or Kir6.2) subunits and regulatory
[sulphonylurea-binding (SUR 1, 2A, or 2B)] subunits. - Kir6.x allows for channel inhibition by ATP, while SURx is responsible for channel activation by ADP and Mg2+.
- consequent hyperpolarization, resulting in
- voltage-gated calcium channel closure,
- decreased Ca2+ influx, and ultimately
- vasodilation [1, 5, 18, 20, 21, 33, 61, 62, 73, 75].
Our data do not support any significant difference regarding the Kir6.1 subunit of the K-ATP channel. On the other hand, this study suggests
- an important role of specific SNPs for the Kir6.2 subunit (Tables 2, 3)—i.e., rs5215, rs5219, and rs5218—
in the susceptibility to IHD and microvascular dysfunction. These SNPs are among the most studied K-ATP channel polymorphisms, especially in the context of diabetes mellitus. In fact, in both Caucasian and Asian populations, these three SNPs as well as other genetic polymorphisms for the KCNJ11 gene have been associated with diabetes mellitus [34, 35, 44, 50, 57, 58, 70].
Nevertheless, the precise
- structure–function impacts of the various amino acid substitutions remain unclear.
The rs5215 and rs5219 polymorphisms, also known as I337V and E23K, respectively, are highly linked with reported
- concordance rates between 72 and 100 % [22, 23, 56].
The high concordance between rs5219 and rs5215 suggests that these polymorphisms
- may have originated in a common ancestor, further indicating a
- possible evolutionary advantage to their maintenance in the general population [49].
In our study, multivariate analysis suggests both an independent protective role of the
- rs5215_GG against developing CAD and
- a trend for rs5219_AA to be associated with protection against coronary microvascular dysfunction (Table 4a, b).
- The variant rs5215_GG is a missense SNP located in the gene KCNJ11 at exon 1009 (ATC-GTC) and results in
the substitution of isoleucine (I) residue with valine (V) [23].
Future studies are necessary to better understand the influence of this single amino acid variant on the function of the channel.
- are both impaired in diabetes mellitus [39].
- independent of the presence of either diabetes mellitus or dyslipidemia.
- regardless of the presence of T2DM and/or dyslipidemia.
However, further studies are necessary to confirm these findings. In this context, to better investigate the implications of genetic variation in the K-ATP channel,
- future studies should include ion channel’s functional modification due to the SNPs and analysis of SUR subunits.
More than 40-kV channel subunits have been identified in the heart, and sections of human coronary smooth muscle cells demonstrate Kv1.5 immunoreactivity [16, 17, 27, 38]. Through constant regulation of smooth muscle tone, Kv channels contribute to the control of coronary microvascular resistance [4, 7]. Pharmacologic molecules that inhibit Kv1.5 channels such as
- pergolide [25],
- 4-amino-pyridine [32], and
- correolide [17]
lead to coronary smooth muscle cell contraction and block the coupling between
- cardiac metabolic demand and
- coronary blood flow.
However, no significant differences were identified between the study groups in terms of the particular polymorphisms for Kv1.5 that were analyzed in this study. Expression of
- the voltage-dependent Na+ channel (Nav) has been demonstrated in coronary microvascular endothelia cells [3, 66].
Our analysis reveals a possible implication of the polymorphism rs1805124_GG for Nav1.5 channel with the presence of anatomically and functionally normal coronary arteries. This SNP leads to a homozygous 1673A-G transition, resulting in a His558-to-Arg (H558R) substitution. It is important to underline that
- our data are the first to correlate the polymorphism rs1805124_GG with IHD.
Further research is necessary to confirm the observed implication.
Finally, we have analyzed the sarco/endoplasmic reticulum calcium transporting Ca2+-ATPase (SERCA), which is fundamental in the regulation of intracellular Ca2+ concentration [6].
SERCA is an intracellular pump that
- catalyzes the hydrolysis of ATP coupled with the
- translocation of calcium from the cytosol into the lumen of the sarcoplasmic reticulum.
Although this pump plays a critical role in regulation of the contraction/relaxation cycle, our analysis did not reveal any apparent association between
- genetic variants of SERCA and the
- prevalence of microvascular dysfunction or IHD.
Conclusions
- with CAD or microvascular dysfunction and those with both anatomically and functionally normal coronary arteries.
- the precise manners by which specific genetic polymorphisms affect ion channel function and expression
Limitations and future perspectives
Notable limitations of this pilot study are as follows:
- sulfonylurea receptor, SURx and further coronary ion channels (e.g., calcium-dependent K channels), as well as
- in vitro evaluation of ion channel activity by patch clamp and analysis of channel expression in the human cardiac tissue.
Moreover, to better address the significance of microvascular dysfunction in IHD, it could be interesting to analyze
- typical atherosclerosis susceptibility genes (e.g., PPAP2B, ICAM1, et al.).
Methods
In this prospective, observational, single-center study – 242 consecutive patients admitted to our department were enrolled with
- the indication to undergo coronary angiography .
All patients matched inclusion criteria
- age [18];
- suspected or documented diagnosis of acute coronary syndrome or stable angina
- with indication(s) for coronary angiography, in accordance with current guidelines [36, 68], and
- the same ethno-geographic Caucasian origin) and
Exclusion Criteria
- previous allergic reaction to iodine contrast,
- renal failure,
- simultaneous genetic disease,
- cardiogenic shock,
- non- ischemic cardiomyopathy
All patients signed an informed consent document –
prior to participation in the study, which included
- acknowledgement of the testing procedures to be performed
(i.e., coronary angiography; intracoronary tests; genetic analysis, and processing of personal data).
The study was approved by the Institution’s Ethics Committee.
All clinical and instrumental characteristics were collected in a dedicated database.
Study Design
(a) Standard therapies were administered, according to current guidelines [36, 68].
(b) An echocardiography was performed before and after coronary angiography
(c) Coronary angiography was performed using radial artery or femoral artery
Judkins approach via sheath insertion.
(d) In patients showing normal epicardial arteries, intracoronary functional tests
were performed through Doppler flow wire to evaluate
- both endothelium-dependent microvascular function
[via intracoronary (IC) infusion of acetylcholine (2.5–10 lg)] and - nonendothelium-dependent microvascular function
[via IC infusion of adenosine (5 lg)] [31].
(e) In all enrolled patients, a peripheral blood sample for genetic analysis was taken.
On the basis of the coronary angiography and the intracoronary functional tests,
- the 242 patients were divided into three groups (see also Fig. 1).
- Group 1: 155 patients with anatomic coronary alteration
(comprising patients with acute coronary syndrome and chronic stable angina).- microvascular dysfunction defined as coronary flow reserve (CFR) \ 2.5
- after IC infusion of acetylcholine and adenosine].
- Group 2: 46 patients with functional coronary alteration
[normal coronary arteries as assessed by angiography, and- as assessed by angiography and with normal functional tests
(CFR C 2.5 after intracoronary infusion of acetylcholine and adenosine) (Fig. 1).
- as assessed by angiography and with normal functional tests
- Group 3: 41 patients with anatomically and functionally normal coronary arteries

Fig. 1 Study design: 242 consecutive not randomized patients matching inclusion and exclusion criteria were enrolled.
In all patients, coronary angiography was performed, according to current ESC/ACC/AHA guidelines. In patients with
angiographically normal coronary artery, intracoronary functional tests were performed. In 242 patients
(155 with coronary artery disease, 46 patients with micro-vascular dysfunction, endothelium and/or non-endothelium
dependent, and 41 patients with anatomically and functionally normal coronary arteries) genetic analysis was performed.
Genetic Analysis
In conformity with the study protocol, ethylenediaminetetraacetic acid (EDTA) whole blood samples were collected according
to the international guidelines reported in the literature [48]. Samples were transferred to the Interinstitutional Multidisciplinary
BioBank (BioBIM) of IRCCS San Raffaele Pisana (Rome) and stored at -80 C until DNA extraction. Bibliographic research by
PubMed and web tools OMIM (http://www.ncbi.nlm.nih.gov/omim), Entrez SNP (http://www.ncbi.nlm.nih.gov/snp), and
Ensembl (http://www.ensembl.org/index.html) were used to select variants of genes involved in signaling pathways
- related to ion channels and/or reported to be associated with
- microvascular dysfunction and/or myocardial ischemia and/or
- diseases correlated to IHD, such as diabetes mellitus.
- NOS3 (endothelial nitric oxide synthase, eNOS),
- ATP2A2 (Ca2+/H+-ATPase pump, SERCA2),
- SCN5A (voltage-dependent Na+ channel,
- Nav1.5),
- KCNJ11 (ATP-sensitive K+ channel, Kir6.2 subunit),
- KCNJ8 (ATP-sensitive K+ channel, Kir6.1 subunit) and
- KCNA5 (voltage-gated K+ channel, Kv1.5).
In particular, we completely analyzed by direct sequencing
- exon 3 of KCNJ8 (Kir6.1 subunit), which includes eight SNPs, as well as
- the whole coding region of KCNA5 (Kv1.5 channel), which includes 32 SNPs and
- four previously described variants [26, 47, 71, 72].
- the whole coding region of KCNJ11 (Kir6.2 subunit), for which sequence variants are described [26, 28].
All SNPs and sequence variants analyzed—a total of 62 variants of 6 genes—are listed in Table 1.


DNA was isolated from EDTA anticoagulated whole blood using the MagNA Pure LC instrument and theMagNA Pure LC
total DNA isolation kit I (Roche Diagnostics, Mannheim, Germany) according to the manufacturer’s instructions. Standard
PCR was performed in a GeneAmp PCR System 9700 (Applied Biosystems, CA) using HotStarTaq Master Mix
(HotStarTaq Master Mix Kit, QIAGEN Inc, CA). PCR conditions and primer sequences are listed in Table 1.
In order to exclude preanalytical and analytical errors, all direct sequencing analyses were carried out on both
strands using Big Dye Terminator v3.1 Cycle Sequencing kit (Applied Biosystems), run on an ABI 3130
Genetic Analyzer (Applied Biosystems), and repeated on PCR products obtained from new nucleic acid extractions.
All data analyses were performed in a blind fashion.
Statistical Analysis
This report, intended as pilot study, is the first to compare
- the prevalence of SNPs in genes encoding several effectors (including ion channels)
- involved in CBFR between these groups of patients.
No definite sample size could be calculated to establish a power analysis. groups of patients. However, assuming
- a 15 % prevalence of normal macrovascular and microvascular coronary findings in unselected patients
undergoing coronary angiography,
we estimated that
- a sample size of at least 150 patients could enable the computation of two-sided 95 % confidence intervals for
- such prevalence estimates ranging between -5.0 and + 5.0 %.
The significance of the differences of observed alleles and genotypes between groups, as well as
- analysis of multiple inheritance models for SNPs were also tested
(co-dominant, dominant, recessive, over-dominant and log-additive) - using a free web-based application (http://213. 151.99.166/index.php?module=Snpstats)
- designed from a genetic epidemiology point of view to analyze association studies.
Akaike Information Criterion (AIC) was used to determine the best-fitting inheritance model for analyzed SNPs,
- with the model with the lowest AIC reflecting the best balance of goodness-of-fit and parsimony.
Moreover, the allelic frequencies were estimated by gene counting, and the genotypes were scored. For each gene,
- the observed numbers of each genotype were compared with those expected for a population in Hardy–Weinberg (HW) equilibrium
- using a free web-based application (http://213.151.99.166/index.php?module=Snpstats) [59].
Linkage disequilibrium coefficient (D0) and haplotype analyses were assessed using the Haploview 4.1 program.
Statistical analysis was performed using SPSS software package for Windows v.16.0 (SPSS Inc., Chicago, IL).
All categorical variables are expressed as percentages, and all continuous variables as mean ± standard deviation.
Differences between categorical variables
- were analyzed by Pearson’s Chi-SQ test.
Given the presence of three groups, differences between continuous variables, were calculated using
(including the number of SNPs tested),
- one-way ANOVA; a post-hoc analysis with Bonferroni correction was made for multiple comparisons.
Univariate and multivariate logistic regression analyses
- the independent impact of genetic polymorphisms on
- coronary artery disease and microvascular dysfunction,
were performed to assess the independent impact of
- genetic polymorphisms on coronary artery disease
and microvascular dysfunction,
while adjusting for other confounding variables. The following parameters were entered into the model:
- age,
- male gender,
- type 2 diabetes mellitus (T2DM),
- systemic arterial hypertension,
- dyslipidemia,
- smoking status, and
- family history of myocardial infarction (MI).
Only variables with a p value < 0.10 after univariate analysis were entered
- into the multivariable model as covariates.
A two-tailed p < 0.05 was considered statistically significant.
Definition of Cardiovascular Risk Factors
Patients were classified as having T2DM if they had
- fasting levels of glucose of >126 mg/dL in two separate measurements or
- if they were taking hypoglycemic drugs.
Systemic arterial hypertension was defined as
- systolic blood pressure > 140 mmHg / diastolic blood pressure > 90 mmHg
- in two separate measurements or
- if the patient was currently taking antihypertensive drugs.
Dyslipidemia was considered to be present if
- serum cholesterol levels were>220 mg/dL or
- if the patient was being treated with cholesterol-lowering drugs.
Family history of MI was defined as a first-degree relative with MI before the age of 60 years.
Results
- nitric oxide synthase,
- the SERCA pump, and
- ion channels
- were screened for sequence variations using PCR amplification and
- direct DNA sequencing analysis
in the population of
- 155 patients with CAD (group 1),
- 46 patients with microvascular dysfunction (group 2), and
- 41 patients with normal coronary arteries and
- normal endothelium dependent and endothelium-independent vasodilation (group 3).
- SNP rs5215 (Kir6.2/KCNJ11) moderately deviates from the HW equilibrium (p = 0.05).
- rs6599230 of Nav1.5/SCN5A showed deviation from HW equilibrium (p = 0.017).
- eNOS/NOS3, SERCA/ATP2A2, Nav1.5/SCN5A, Kir6.1/KCNJ8, or Kv1.5/KCNA5
- rs5215_GG, and
- rs5219_AA of Kir6.2/KCNJ11 were observed,
Table 3 displays significant differences between normal subjects (group 3) and
- patients with either CAD (group 1) or microvascular dysfunction (group 2).

When correcting for other covariates as risk factors, the rs5215_GG genotype of Kir6.2/KCNJ11 was found to be
- significantly associated with CAD after multivariate analysis (OR = 0.319, p = 0.047, 95 % CI = 0.100–0.991), evidencing
- a ‘‘protective’’ role of this genotype, as shown in Table 4a.
Similarly, a trend that supports this role of Kir6.2/KCNJ11 was also observed
- in microvascular dysfunction for rs5219 AA. In contrast,
- rs1799983_GT for eNOS/NOS3 was identified as an independent risk factor
following multivariate analysis (Table 4b), which agrees with literature findings as described below.

SOURCE for TABLES
BasicResCardiol(2013)108:387 http//dx.dio.org/10.1007/s00395-013-0387-4
Conflict of interest On behalf of all authors, the corresponding author states that there is no conflict of interest.
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
REFERENCES
1. Alekseev AE, Hodgson DM, Karger AB, Park S, Zingman LV, Terzic A (2005) ATP-sensitive K? channel channel/enzyme multimer: metabolic gating in the heart. J Mol
Cell Cardiol 38:895–905. doi:10.1016/j.yjmcc.2005.02.022
2. Baumgart D, Naber C, Haude M, Oldenburg O, Erbel R, Heusch G, Siffert W (1999) G protein beta3 subunit 825T allele and enhanced coronary vasoconstriction on
alpha(2)-adrenoceptor activation. Circ Res 85:965–969. doi:10.1161/01.RES.85.10.965
3. Belardinelli L, Shryock JC, Fraser H (2006) Inhibition of the late sodium current as a potential cardioprotective principle: effects of the late sodium current inhibitor
ranolazine. Heart 92:6–14. doi:10.1136/hrt.2005.078790
4. Berwick ZC, Moberly SP, Kohr MC, Morrical EB, Kurian MM, Dick GM, Tune JD (2012) Contribution of voltage-dependent K+ and Ca2+ channels to coronary pressure-
flow autoregulation. Basic Res Cardiol 107:264. doi:10.1007/s00395-012-0264-6
5. Brayden JE (2002) Functional roles of KATP channels in vascular smooth muscle. Clin Exp Pharmacol Physiol 29:312–316. doi:10.1046/j.1440-1681.2002.03650.x
6. Brini M, Carafoli E (2009) Calcium pumps in health and disease. Physiol Rev 89:1341–1378. doi:10.1152/physrev.00032.2008
7. Chen TT, Luykenaar KD, Walsh EJ, Walsh MP, Cole WC (2006) Key role of Kv1 channels in vasoregulation. Circ Res 99:53–60. doi:10.1161/01.RES.0000229654.45090.57
8. Cohen KD, Jackson WF (2005) Membrane hyperpolarization is not required for sustained muscarinic agonist-induced increases in intracellular Ca2+ in arteriolar endothelial
cells. Microcirculation 12:169–182. doi:10.1080/10739680590904973
9. Daut J, Maier-Rudolph W, von Beckerath N, Mehrke G, Gu¨nter K, Goedel-Meinen L (1990) Hypoxic dilation of coronary arteries is mediated by ATP-sensitive potassium
channels. Science 247:1341–1344. doi:10.1126/science.2107575
10. Davidson SM, Duchen MR (2007) Endothelial mitochondria: contributing to vascular function and disease. Circ Res 100:1128–1141. doi:10.1161/01.RES.0000261970.18328.1d
…. 75
SOURCE for References 1-75
Basic Res Cardiol (2013) 108:387 http://dx.doi.org/10.1007/s00395-013-0387-4
Other related articles published on this Open Access Online Scientific Journal include the following:
ION CHANNEL and Cardiovascular Diseases
http://pharmaceuticalintelligence.com/?s=Ion+Channel
Calcium Role in Cardiovascular Diseases
Part I: Identification of Biomarkers that are Related to the Actin Cytoskeleton
Larry H Bernstein, MD, FCAP
Part II: Role of Calcium, the Actin Skeleton, and Lipid Structures in Signaling and Cell Motility
Larry H. Bernstein, MD, FCAP, Stephen Williams, PhD and Aviva Lev-Ari, PhD, RN
Part III: Renal Distal Tubular Ca2+ Exchange Mechanism in Health and Disease
Larry H. Bernstein, MD, FCAP, Stephen J. Williams, PhD and Aviva Lev-Ari, PhD, RN
Part IV: The Centrality of Ca(2+) Signaling and Cytoskeleton Involving Calmodulin Kinases and Ryanodine Receptors in Cardiac Failure, Arterial Smooth Muscle, Post-ischemic Arrhythmia, Similarities and Differences, and Pharmaceutical Targets
Larry H Bernstein, MD, FCAP, Justin Pearlman, MD, PhD, FACC and Aviva Lev-Ari, PhD, RN
Part V: Ca2+-Stimulated Exocytosis: The Role of Calmodulin and Protein Kinase C in Ca2+ Regulation of Hormone and Neurotransmitter
Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part VI: Calcium Cycling (ATPase Pump) in Cardiac Gene Therapy: Inhalable Gene Therapy for Pulmonary Arterial Hypertension and Percutaneous Intra-coronary Artery Infusion for Heart Failure: Contributions by Roger J. Hajjar, MD
Aviva Lev-Ari, PhD, RN
Part VII: Cardiac Contractility & Myocardium Performance: Ventricular Arrhythmias and Non-ischemic Heart Failure – Therapeutic Implications for Cardiomyocyte Ryanopathy (Calcium Release-related Contractile Dysfunction) and Catecholamine Responses
Justin Pearlman, MD, PhD, FACC, Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part VIII: Disruption of Calcium Homeostasis: Cardiomyocytes and Vascular Smooth Muscle Cells: The Cardiac and Cardiovascular Calcium Signaling Mechanism
Justin Pearlman, MD, PhD, FACC, Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part IX: Calcium-Channel Blockers, Calcium Release-related Contractile Dysfunction (Ryanopathy) and Calcium as Neurotransmitter Sensor
Justin Pearlman, MD, PhD, FACC, Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part X: Synaptotagmin functions as a Calcium Sensor: How Calcium Ions Regulate the fusion of vesicles with cell membranes during Neurotransmission
Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Part XI: Sensors and Signaling in Oxidative Stress
Larry H. Bernstein, MD, FCAP
http://pharmaceuticalintelligence.com/2013/11/01/sensors-and-signaling-in-oxidative-stress/
Part XII: Atherosclerosis Independence: Genetic Polymorphisms of Ion Channels Role in the Pathogenesis of Coronary Microvascular Dysfunction and Myocardial Ischemia (Coronary Artery Disease (CAD))
Larry H Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Mitochondria and Oxidative Stress Role in Cardiovascular Diseases
Reversal of Cardiac Mitochondrial Dysfunction
Larry H. Bernstein, MD, FCAP
http://pharmaceuticalintelligence.com/2013/04/14/reversal-of-cardiac-mitochondrial-dysfunction/
Calcium Signaling, Cardiac Mitochondria and Metabolic Syndrome
Larry H. Bernstein, MD, FCAP and Aviva Lev-Ari, PhD, RN
Mitochondrial Dysfunction and Cardiac Disorders
Larry H. Bernstein, MD, FCAP http://pharmaceuticalintelligence.com/2013/04/14/mitochondrial-dysfunction-and-cardiac-disorders/
Mitochondrial Metabolism and Cardiac Function
Larry H. Bernstein, MD, FCAP
http://pharmaceuticalintelligence.com/2013/04/14/mitochondrial-metabolism-and-cardiac-function/
Mitochondria and Cardiovascular Disease: A Tribute to Richard Bing
Larry H. Bernstein, MD, FCAP
http://pharmaceuticalintelligence.com/2013/04/14/chapter-5-mitochondria-and-cardiovascular-disease/
MIT Scientists on Proteomics: All the Proteins in the Mitochondrial Matrix Identified
Aviva Lev-Ari, PhD, RN
Mitochondrial Dynamics and Cardiovascular Diseases
Ritu Saxena, Ph.D.
http://pharmaceuticalintelligence.com/2012/11/14/mitochondrial-dynamics-and-cardiovascular-diseases/
Mitochondrial Damage and Repair under Oxidative Stress
Larry H Bernstein, MD, FCAP
Nitric Oxide has a Ubiquitous Role in the Regulation of Glycolysis -with a Concomitant Influence on Mitochondrial Function
Larry H. Bernstein, MD, FACP
Mitochondrial Mechanisms of Disease in Diabetes Mellitus
Aviva Lev-Ari, PhD, RN
Mitochondria Dysfunction and Cardiovascular Disease – Mitochondria: More than just the “Powerhouse of the Cell”
Ritu Saxena, PhD
 Randy Schekman, who will share the 2013 Nobel Prize in Physiology or Medicine (Peg Skorpinski photo)
Randy Schekman, who will share the 2013 Nobel Prize in Physiology or Medicine (Peg Skorpinski photo) Schekman takes a call at home after getting the news. (Carol Ness photo)
Schekman takes a call at home after getting the news. (Carol Ness photo)



{kind=link}