Brain and Cognition
Larry H. Bernstein, MD, FCAP, Curator
LPBI
Brain activity may be as unique as fingerprints
Tue, 10/13/2015 – Bill Hathaway, Yale Univ.
Image: Michael S. Helfenbeing/Shutterstock
A person’s brain activity appears to be as unique as his or her fingerprints, a new Yale Univ.-led imaging study shows. These brain “connectivity profiles” alone allow researchers to identify individuals from the fMRI images of brain activity of more than 100 people, according to the study published in Nature Neuroscience.
“In most past studies, fMRI data have been used to draw contrasts between, say, patients and healthy controls,” said Emily Finn, a PhD student in neuroscience and co-first author of the paper. “We have learned a lot from these sorts of studies, but they tend to obscure individual differences which may be important.”
Finn and co-first author Xilin Shen, under the direction of R. Todd Constable, professor of diagnostic radiology and neurosurgery at Yale, compiled fMRI data from 126 subjects who underwent six scan sessions over two days. Subjects performed different cognitive tasks during four of the sessions. In the other two, they simply rested. Researchers looked at activity in 268 brain regions: specifically, coordinated activity between pairs of regions. Highly coordinated activity implies two regions are functionally connected. Using the strength of these connections across the whole brain, the researchers were able to identify individuals from fMRI data alone, whether the subject was at rest or engaged in a task. They were also able to predict how subjects would perform on tasks.
Finn said she hopes that this ability might one day help clinicians predict or even treat neuropsychiatric diseases based on individual brain connectivity profiles.
Brain Activity Identifies Individuals
By Kerry Grens
Neural connectome patterns differ enough between people to use them as a fingerprint.
New Alzheimer’s Gene Identified
Megan Brooks
http://www.medscape.com/viewarticle/852556
Researchers have identified a new gene involved in the immune system that increases the risk for Alzheimer’s disease (AD), providing a potential new target for prevention and treatment.
They found that older adults at risk for AD and those with the disease who carry a specific variant in the interleukin-1 receptor accessory protein (IL1RAP) had higher rates of amyloid plaque accumulation in the brain over 2 years. The effect of the variant was stronger than the well-known AD risk allele APOE ε4.
“These findings suggest that targeting the IL1RAP immune pathway may be a viable approach for promoting the clearance of amyloid deposits and fighting an important cause of progression in Alzheimer’s disease,” Andrew J. Saykin, PsyD, director of the Indiana Alzheimer Disease Center, Indianapolis, and the national Alzheimer’s Disease Neuroimaging Initiative Genetics Core, said in a statement.
The study was published in the October 1 issue of Brain.
Novel Association
The researchers conducted a genome-wide association study of longitudinal changes in brain amyloid burden measured by florbetapir positron emission tomography (PET) in nearly 500 individuals. They assessed the levels of brain amyloid deposits at an initial visit and again 2 years later.
Study participants came from the Alzheimer’s Disease Neuroimaging Initiative, the Indiana Memory and Aging Study, the Religious Orders Study, and the Rush Memory and Aging Project, all longitudinal studies of older adults representing clinical stages along the continuum from normal aging to AD.
As expected, APOE ε4 was associated with higher rates of amyloid plaque buildup. However, they also identified a novel association between a single nucleotide polymorphism in IL1RAP (rs12053868-G) and higher rates of amyloid accumulation, independent of APOE ε4.
Carriers of the IL1RAP rs12053868-G variant showed accelerated cognitive decline and were more likely to progress from mild cognitive impairment to AD. They also showed greater longitudinal atrophy of the temporal cortex, which is involved in memory and had a lower level of microglial activity as measured by PET scans, the researchers report.
“This was an intriguing finding because IL1RAP is known to play a central role in the activity of microglia, the immune system cells that act as the brain’s ‘garbage disposal system’ and the focus of heavy investigation in a variety of neurodegenerative diseases,” Vijay K. Ramanan, MD, PhD, postdoctoral researcher at the Indiana University School of Medicine, Indianapolis, who worked on the study, said in the statement.
“These results suggest a crucial role of activated microglia in limiting amyloid accumulation and nominate the IL-1/IL1RAP pathway as a potential target for modulating this process,” the investigators write.
The study was supported by the National Institute on Aging and a consortium of private partners through the Foundation for the National Institutes of Health. Several authors disclosed relationships with pharmaceutical companies. A complete list can be found with the original article.
Brain. 2015;138:3076-3088. Abstract
Cognitive Impairments in Elderly Diabetic Patients: Understanding the Risks for Better Management
Medscape Medical News from the
Visit Medscape in Hall B Booth #B13:31
Medscape Diabetes & Endocrinology
COMMENTARY
Lyse Bordier, MD
http://www.medscape.com/viewarticle/852112
Editor’s Note: The following is an edited, translated transcript of a presentation by Professor Lyse Bordier, a diabetologist at Military Hospital Bégin, Saint-Mandé, France, summarizing her lecture at the European Association for the Study of Diabetes (EASD) 2015 AnnualMeeting in Stockholm, Sweden.
Hello. I am Professor Lyse Bordier. I work at the Bégin Military Hospital, in Saint-Mandé, France, and I had the pleasure of participating in a symposium organized by the EASD 2015 conference in Stockholm on elderly patients, specifically on cognitive impairments.
A Public Health Problem
Dementia and cognitive impairments are a major problem; Alzheimer disease accounts for 70% of all cases of dementia. The other main causes are vascular dementias and mixed dementias. They are a real public health problem; it is estimated that, in the United States, 5.2 million people have this condition, and worldwide, every 7 seconds, a new case of dementia is diagnosed.[1,2] In France, for example, it was estimated in 2010 that 750,000-850,000 people had dementia and that this figure will increase by a factor of 2.4 by the year 2050.
Diabetes is an important contributor to the development of cognitive impairments, all the way up to dementia. In Europe, it is estimated that nearly 25% of people over age 85 years have dementia. Its prevalence and incidence are higher in women than in men.[2] We know that the complications of diabetes have changed over the years and that acute metabolic complications are, in the end, much less important. With the improvement in life expectancy in our diabetic patients, who are now better treated thanks to better therapeutic management, new complications have arisen, such as renal failure, heart failure, and, of course, geriatric complications, which are, in large part, cognitive disorders.[3]
Prevalence Underestimated by Physicians
These cognitive impairments are common and largely underestimated. This was clearly shown in the GERODIAB study,[4] which included a cohort of 987 patients over the age of 70 years. At inclusion, the physicians reported that 11% of their patients had cognitive impairments and that 3% had dementia. In actual fact, 25% of the patients had impaired cognitive functions, with a Mini-Mental State Examination (MMSE) score under 25. The prevalence is therefore significantly underestimated by physicians.
Cognitive impairments are more prevalent and more severe in diabetics than in nondiabetics. It is estimated that the risk for cognitive impairments and that for dementia are 20% to 70% and 60% higher, respectively, in the presence of diabetes.[5] Furthermore, the risk for Alzheimer dementia is considerable, it being 40% higher in diabetics. As expected (given the combination of the other cardiovascular risk factors), the increase in the risk is even greater for vascular dementia, with an odds ratio of 2.38.[6]
Mechanisms
What are the mechanisms in the development of cognitive impairments and dementia? There are many mechanisms, and they are often poorly understood. Hyperglycemia plays a very important role as a direct result of oxidative stress, of advanced glycation end-products, but also as a result of micro- and macroangiopathy, hypertension, and dyslipidemia.[7,8] Other major factors, such as hypoglycemia,[9-12]play an extremely important role in the development of cognitive impairments. As well, a great deal of literature has been published lately on the role of inflammation[13] and genetic factors. Another widely known aspect is insulin resistance, which increases the risk for dementia at a fairly early stage by 40%[14,15]; this already during the metabolic syndrome, even before the onset of type 2 diabetes.
http://img.medscape.com/article/852/112/852112-Figure1.jpg
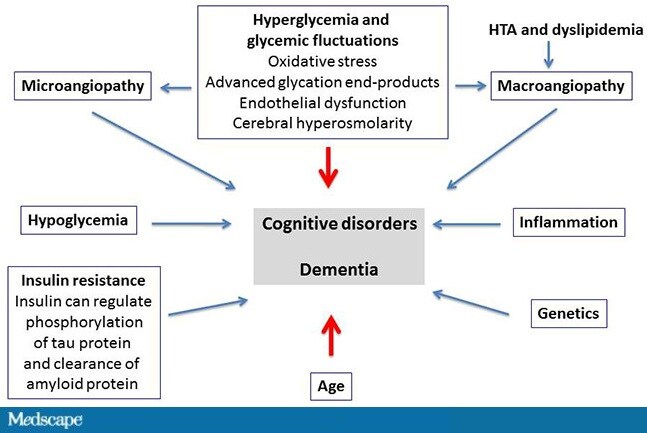{kind=link}
Figure. Multiple and poorly understood mechanisms of cognitive impairments and dementia. HTA = arterial hypertension. Adapted from Buysschaert M, et al.[16]
What Are the Consequences of Cognitive Impairments?
Cognitive impairments lead to a number of complications, including a reduction in life expectancy. In the GERODIAB cohort, we found, after 2 years of follow-up, that the mortality rate was twice as high in the patients with an MMSE score <24 compared with those with an MMSE score >24. In this study, the patients with a lower MMSE score had less well-controlled diabetes, were usually treated with insulin, and had heart failure and cerebrovascular complications more often. Very surprisingly, hypoglycemia was not more prevalent in these patients, perhaps because, being less independent, they were better managed by care teams.[17]
Cognitive impairments lead to geriatric complications, such as malnutrition, falls, and a loss of autonomy. They also promote social and family isolation and iatrogenic accidents, as well as depression, which can both mask cognitive impairments and exacerbate an underlying dementia. Another important aspect is that cognitive impairments increase the risk for hypoglycemia. This has been shown very clearly in all of the studies. There is, in fact, a bidirectional link between dementia and hypoglycemia: Hypoglycemia doubles the risk for dementia, and dementia triples the risk for hypoglycemia.[18]
Screening and Management
What do we do when a patient presents with cognitive impairments? First, they should be identified so that they can be managed. We need to be vigilant for certain little signs: changes in the patient’s behavior (eg, a patient who forgets his appointments, whose personal hygiene has declined, who is less diligent in keeping his blood glucose diary, and, lastly, who has an unexplained diabetic imbalance). We should also know how to use simple tests, such as the MMSE, which provides an overall assessment of space-time orientation, cognitive functions, language functions, and calculation, and how to assess the patient’s autonomy and loss of autonomy.[19] Next, we should, as per the recommendations of the American Diabetes Association[20] and the EASD, individualize the glycemic goals, taking into account, in the most fragile, elderly patients, cognitive status, the level of autonomy, depression, nutritional status—in particular, sarcopenia, which can coexist with obesity, and the risk for hypoglycemia.[21]
We should therefore avoid overtreating the most fragile patients (those at greatest risk for hypoglycemia), but neither should we undertreat patients who have a long life expectancy and who could develop micro- and macroangiopathic complications.
One last aspect, which is very important, is the family. Help needs to be provided to prevent the patient’s loss of autonomy.[21] Lastly, I think that cognitive decline should be added to the already long list of degenerative complications of diabetes.
| PDGFR-ß Plays a Key Role in the Ectopic Migration of Neuroblasts in Cerebral Stroke
Hikari Sato et al. |
| The neuroprotective agents and induction of endogenous neurogenesis remain as the urgent issues to be established for the care of cerebral stroke. Platelet-derived growth factor receptor beta (PDGFR-ß) is mainly expressed in neural stem/progenitor cells (NSPCs), neurons and vascular pericytes of the brain; however, the role in pathological neurogenesis remains elusive. This review examined the role of PDGFR-ß in the migration and proliferation of NSPCs after stroke. |
Leave a Reply