Cancer Immunotherapy
Curator: Larry H. Bernstein, MD, FCAP, Curator
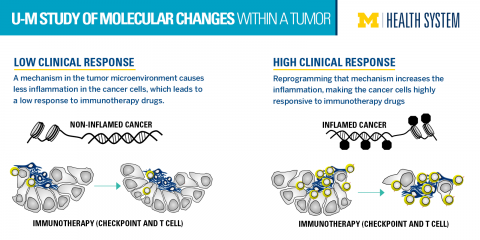
Research explains limits of cancer immunotherapy drugs
Finding offers possibility to improve response to therapies
http://www.uofmhealth.org/news/archive/201510/research-explains-limits-cancer-immunotherapy-drugs
A new study from the University of Michigan Comprehensive Cancer Center reveals molecular changes within the tumor that are preventing the immunotherapy drugs from killing off the cancer.
Clinical trials with PD-L1 and PD-1 blockade suggested that tumors with a high number of inflammation-causing T cells were more responsive to the immunotherapy-based PD-L1 and PD-1 inhibitors. Tumors with low inflammation, or low T cells, were less responsive. But what controls T cells in the tumor microenvironment is poorly understood.

http://www.uofmhealth.org/sites/default/files/styles/large/public/Immunotherapy.png?itok=_oihl0jj
{kind=link}
“We defined a molecular mechanism to explain why some tumors are inflamed and others are not – and consequently why some patients will be responsive to therapy and others not,” says senior author Weiping Zou, M.D., Ph.D.
“If we can reprogram this epigenetic mechanism, then the therapy might work for more patients,” says Zou, Charles B. de Nancrede Professor of Surgery, Immunology and Biology at the University of Michigan Medical School.
Zou’s group was the first to show PD-L1 expression, regulation and functional blockade in dendritic cells in the human cancer microenvironment.
In this study, published in Nature, researchers studied human and mouse models of ovarian cancer cells. They applied epigenetic drugs and found that the numbers of T cells in the tumor increased. They also saw that the epigenetic drugs synergized the anti-tumor effect of PD-L1 blockade in their models.
“We hope this could be developed into a clinical trial testing a combination of PD-L1 and PD-1 blockade with epigenetic therapy. We want to see if we can make the responders more responsive and turn the non-responders into responders,” Zou says.
Additional authors: From U-M: Dongjun Pen, Ilona Kryczek, Nisha Nagarsheth, Lili Zhao, Shuang Wei, Weimin Wang, Yuqing Sun, Ende Zhao, Linda Vatan, Wojciech Szeliga, Yali Dou, Kathleen Cho, Rebecca Liu; from Medical University in Lublin, Poland: Jan Kotarski, Rafal Tarkowski; from Henry Ford Health System: Sharon Hensley-Alford, Adnan Munkarah
Funding: National Institutes of Health grants CA190176, CA123088, CA099985, CA193136, CA152470, CA171306, 5P30 CA46592; Rivkin Ovarian Cancer Center, Ovarian Cancer Research Fund, Barbara and Don Leclair
Cancer immunotherapy research is evolving to more targeted strategies
Discoveries in immune pathway research have helped refine cancer immunotherapy strategies to become more targeted.1,2

http://www.researchcancerimmunotherapy.com/overview/targeted-cancer-research
- CAR=chimeric antigen receptor;
- CSF-1R=colony-stimulating factor 1; CTLA4=cytotoxic
- T-lymphocyte antigen-4; IDO=indoleamine
- 2,3-dioxygenase; PD-1=programmed death-1; PD-L1=programmed death-ligand 1.
{kind=link}
Engaging the immune response: a unique approach to cancer management
Cancer immunotherapy strategies are designed to engage the immune system against tumors. This approach is unique in the oncology setting and introduces new considerations for cancer management.1,2
-

TARGETED
to tumor-specific antigens
-

RAPID
activation of the immune response
-

ADAPTABLE
as the tumor mutates and evolves
-

SELF-PROPAGATING
with each revolution of the cancer immunity cycle
-

DURABLE
response over time
CONSIDERATIONS FOR CANCER IMMUNOLOGY
Duration of response
The immune response has the ability to adapt with cancer as it evolves, and can become self-propagating once the cancer immunity cycle is initiated. Immune-directed strategies aim to leverage these attributes, with the goal of inducing a durable antitumor effect.3-5
Pseudo-progression
T-cell infiltration to the tumor site may cause an apparent increase in tumor size or the appearance of new lesions. This inflammatory effect can be misinterpreted as progressive disease, as it can be difficult to differentiate the different cell types in radiographic imaging. New criteria have been developed to better capture immune-related response patterns, and may guide evaluation of immunotherapies in clinical trials, and potentially in clinical care.1,2,6
![Image showing T-cell infiltration into the tumor site can cause pseudoprogression]](https://i0.wp.com/www.researchcancerimmunotherapy.com/images/overview/immune-response/pseudo-progression.png?w=500)
REFERENCES
- Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39:1-10. PMID: 23890059
- Mellman I, Coukos G, Dranoff G. Cancer immunotherapy comes of age. Nature. 2011;480:480-489. PMID: 22193102
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144:646-674. PMID: 21376230
Immune-related adverse events
While the goal of cancer immunotherapy research is to understand how to activate specific components of the immune response, the potential for off-target effects exists. Adverse event profiles may vary among different immune-directed strategies. As strategies grow more targeted, the recognition and management of immune-related adverse events will evolve.1,3
REFERENCES
- Mellman I, Coukos G, Dranoff G. Cancer immunotherapy comes of age. Nature. 2011;480:480-489. PMID: 22193102
- Hoos A, Eggermont AM, Janetzki S, et al. Improved endpoints for cancer immunotherapy trials. J Natl Cancer Inst. 2010;102:1388-1397.PMID: 20826737
- Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39:1-10. PMID: 23890059
- Topalian SL, Weiner GJ, Pardoll DM. Cancer immunotherapy comes of age. J Clin Oncol. 2011;29:4828-4836. PMID: 22042955
- Chen DS, Irving BA, Hodi FS. Molecular pathways: next-generation immunotherapy—inhibiting programmed death-ligand 1 and programmed death-1. Clin Cancer Res. 2012;18:6580-6587. PMID: 23087408
- Wolchok JD, Hoos A, O’Day S, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009;15:7412-7420. PMID: 19934295
Tumors can evade immune destruction
By disrupting the processes of the cancer immunity cycle throughout the body, tumors can avoid detection by the immune system and limit the extent of immune destruction.1-3

Tumor microenvironment
Disrupting antigen detection
{kind=link}

Lymph node
Inhibiting T-cell activation by dendritic cells
http://www.researchcancerimmunotherapy.com/images/overview/evading-immune-destruction/lymph-node.png
{kind=link}

Blood vessel
Blocking T-cell infiltration into tumor
{kind=link}

Tumor microenvironment
Suppressing cytotoxic T-cell activity
{kind=link}
EVADING IMMUNE DESTRUCTION IS AN EMERGING HALLMARK OF CANCER

{kind=link}
The growing body of research into the mechanisms of immune evasion has led to its addition as an emerging hallmark of cancer, a distinct biological capability that enables tumors to grow and metastasize.3
MUTATION RATE BY CANCER TYPE4

{kind=link}
REFERENCES
- Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39:1-10. PMID: 23890059
- Chen DS, Irving BA, Hodi FS. Molecular pathways: next-generation immunotherapy—inhibiting programmed death-ligand 1 and programmed death-1. Clin Cancer Res. 2012;18:6580-6587. PMID: 23087408
- Rajasagi M, Shokla SA, Fritsch EF, et al. Systematic identification of personal tumor-specific neoantigens in chronic lymphocytic leukemia.Blood. 2014;124:453-462. PMID: 24891321
- Lawrence MS, Stojanov P, Polak P, et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature.2013;499:214-218. PMID: 23770567
Atezolizumab (Anti-PDL1) clinical trials
Atezolizumab clinical trials are being conducted for the following types of cancers: lung, bladder, kidney, hematological malignancies, and breast cancer. Please check back for updates or search clinicaltrials.gov with the search term “Atezolizumab.”
EXPLORING A MORE PERSONALIZED APPROACH TO CANCER IMMUNOTHERAPY RESEARCH
With the evolution to more targeted strategies, research is focusing on identifying predictors of individual immune response through specific tumor characteristics and factors in the tumor microenvironment, such as
- The presence of tumor-infiltrating immune cells8
- The ability of immune cells to infiltrate the tumor microenvironment may be a key criterion for a variety of immune-directed strategies, and could indicate which tumors are more likely to respond
- Gene expression patterns in tumors, particularly the genes involved in immune response9
- Cell surface protein expression
- PD-L1 expression on tumor cells and tumor-infiltrating immune cells10,11
- MUC1 expression on tumor cells12
REFERENCES
- Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39:1-10. PMID: 23890059
- Mellman I, Coukos G, Dranoff G. Cancer immunotherapy comes of age. Nature. 2011;480:480-489. PMID: 22193102
- Lesterhuis WJ, Haanen JB, Punt CJ. Cancer immunotherapy—revisited. Nat Rev Drug Discov. 2011;10:591-600. PMID: 21804596
- National Institutes of Health ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT01494688. Accessed March 4, 2015.
- National Institutes of Health ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT00739609. Accessed March 4, 2015.
- Glienke W, Esser R, Priesner C, et al. Advantages and applications of CAR-expressing natural killer cells. Front Pharmacol. 2015;6:21. doi: 10.3389/fphar.2015.00021. PMID: 25729364
- National Institutes of Health ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT01303705. Accessed March 4, 2015.
- Gajewski TF, Schreiber H, Fu YX. Innate and adaptive immune cells in the tumor microenvironment. Nat Immunol. 2013;14:1014-1022.PMID: 24048123
- Ji RR, Chasalow SD, Wang L, et al. An immune-active tumor microenvironment favors clinical response to ipilimumab. Cancer Immunol Immunother. 2012;61:1019-1031. PMID: 22146893
- Taube JM, Anders RA, Young GD, et al. Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci Transl Med. 2012;4:127ra37. PMID: 22461641
- Chen DS, Irving BA, Hodi FS. Molecular pathways: next-generation immunotherapy—inhibiting programmed death-ligand 1 and programmed death-1. Clin Cancer Res. 2012;18:6580-6587. PMID: 23087408
- Stojnev S, Ristic-Petrovic A, Velickovic LJ, et al. Prognostic significance of mucin expression in urothelial bladder cancer. Int J Clin Exp Pathol. 2014;7:4945-4958. PMID: 25197366
- Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12:252-264. PMID: 22437870
- Taylor RC, Patel A, Panageas KS, Busam KJ, Brady MS. Tumor-infiltrating lymphocytes predict sentinel lymph node positivity in patients with cutaneous melanoma. J Clin Oncol. 2007;25:869-875. PMID: 17327608