Rapid diagnosis of septicemia
Larry H. Bernstein, MD, FCAP, Curator
LPBI
Rapid Diagnosis of Infection in the Critically Ill, a Multicenter Study of Molecular Detection in Bloodstream Infections, Pneumonia, and Sterile Site Infections
Objective: Early identification of causative microorganism(s) in patients with severe infection is crucial to optimize antimicrobial use and patient survival. However, current culture-based pathogen identification is slow and unreliable such that broad-spectrum antibiotics are often used to insure coverage of all potential organisms, carrying risks of overtreatment, toxicity, and selection of multidrug-resistant bacteria. We compared the results obtained using a novel, culture-independent polymerase chain reaction/electrospray ionization-mass spectrometry technology with those obtained by standard microbiological testing and evaluated the potential clinical implications of this technique.
Design: Observational study.
Setting: Nine ICUs in six European countries.
Patients: Patients admitted between October 2013 and June 2014 with suspected or proven bloodstream infection, pneumonia, or sterile fluid and tissue infection were considered for inclusion.
Interventions: None.
Measurements and Main Results: We tested 616 bloodstream infection, 185 pneumonia, and 110 sterile fluid and tissue specimens from 529 patients. From the 616 bloodstream infection samples, polymerase chain reaction/electrospray ionization-mass spectrometry identified a pathogen in 228 cases (37%) and culture in just 68 (11%). Culture was positive and polymerase chain reaction/electrospray ionization-mass spectrometry negative in 13 cases, and both were negative in 384 cases, giving polymerase chain reaction/electrospray ionization-mass spectrometry a sensitivity of 81%, specificity of 69%, and negative predictive value of 97% at 6 hours from sample acquisition. The distribution of organisms was similar with both techniques. Similar observations were made for pneumonia and sterile fluid and tissue specimens. Independent clinical analysis of results suggested that polymerase chain reaction/electrospray ionization-mass spectrometry technology could potentially have resulted in altered treatment in up to 57% of patients.
Conclusions: Polymerase chain reaction/electrospray ionization-mass spectrometry provides rapid pathogen identification in critically ill patients. The ability to rule out infection within 6 hours has potential clinical and economic benefits.
Introduction
The availability of rapid and reliable infectious disease diagnostics that can provide results directly from patient specimens represents a major unmet need in managing critically ill patients. Current sepsis guidelines recommend initiation of IV antibiotic therapy as early as possible, ideally within the first hour,[1] as any delay in effective antimicrobial therapy may result in decreased survival.[2] Effective therapy requires that the identity of causative pathogens and their resistance patterns are known. However, the current standard-of-care, which depends on blood culture-based initial diagnosis, often takes at least 48–72 hours to provide a result. Furthermore, cultures often remain negative even when bacterial or fungal infections are strongly suspected,[3] in part, related to concurrent antibiotic treatment.[4]
Molecular diagnostic techniques that do not depend on growth of organisms in culture may offer a distinct advantage over current methods. Most of the recently described molecular methods, however, rely on culture amplification as a precursor to diagnosis.[5–8] Although these techniques may accelerate diagnosis for positive cultures, they do not address the significant proportion of false-negative cultures observed in patients with sepsis. In addition, many of these methods also use targeted pathogen detection with limited pathogen coverage such that negative results are often not highly predictive.
Polymerase chain reaction followed by electrospray ionization-mass spectrometry (PCR/ESI-MS) can detect more than 800 bloodstream infection (BSI)-relevant pathogens in a single assay and in approximately 6 hours.[9–13] It can also identify three classes of antibiotic resistance markers associated with resistance to methicillin (mecA), vancomycin (vanA/vanB), and carbapenems (KPC). Using this technique, we recently demonstrated 83% sensitivity and 94% specificity compared with culture for direct detection of pathogens in whole-blood specimens from patients with suspected BSIs.[13]
Here, we describe findings from the multicenter observational Rapid Diagnosis of Infections in the Critically Ill (RADICAL) study. The primary objective was to compare results obtained using the novel culture-independent PCR/ESI-MS technology with those obtained from standard microbiological testing as a measure of clinical performance. Secondarily, to broadly address the clinical value of PCR/ESI-MS detections, a panel of independent clinical adjudicators was used to identify changes in patient management that may have occurred had the results from the PCR/ESI-MS technology been available for clinical use and assumed to be correct.
Patient Inclusion and Exclusion Criteria
Patients were considered for inclusion if they had 1) suspected or proven severe infection or sepsis and or 2) suspected or proven healthcare-associated pneumonia (HAP/HCAP), ventilator-associated pneumonia (VAP), or severe community-acquired pneumonia (sCAP). Because pneumonia is the most common precipitating cause of sepsis, there may be an overlap between these two populations, but patients were included in one of the two groups, not both. Pneumonia (HAP/HCAP, VAP, and sCAP) was diagnosed in patients with an endotracheal tube in situ and a new infiltrate on chest radiograph plus temperature more than 38°C or less than 35°C, increased sputum production, increased or decreased WBC count (> 12 or < 4 cells/mL3), or a clinical suspicion of pneumonia, and the treating clinician expected the patient to still be intubated the next day.
The following exclusion criteria were used: the treating clinician expected the patient to be discharged from the ICU on the day of evaluation or the following day, the treatment intent was palliative, the clinician was not committed to aggressive treatment, or death was deemed imminent and inevitable. Patients who had previously been included, but were readmitted to the ICU during the same hospitalization, were not included a second time.
Data Analysis
Results obtained with the PCR/ESI-MS technology for each specimen were compared with those obtained using conventional microbiology methods for the same sample. If multiple specimens were taken from a patient per standard-of-care protocols, each was independently analyzed in this study. Agreement and concordance were assessed using a McNemar test[16] and Cohen κ.[17] All percentages and CIs for proportions were calculated using the exact method and are rounded to the nearest percentage. Direct comparison of positive and negative results was conducted with organism identification for each method (conventional microbiology vs PCR/ESI-MS) for each specimen type. Coagulase-negative staphylococcus and other common skin contaminants were annotated as “potential contaminants” for both methods and excluded from the overall analysis, as previously described.[13]
Discrepant results between the PCR/ESI-MS and culture cannot be directly confirmed by an independent method, as previously described.[13] Two approaches were used to resolve discrepancies. In a subset of patients, multiple samples were collected per standard-of-care. This included two independent fresh venipunctures (left arm vs right arm) or one venipuncture plus one sample collected from an indwelling line. Paired analysis of PCR/ESI-MS testing results between these independently collected samples was conducted to indicate the likelihood of true infection. In addition, independent clinical adjudication (described below) was performed using all the clinical data collected as part of the study, including standard-of-care microbiology results and PCR/ESI-MS results.
Results
Of 543 patients enrolled in the study, 14 did not have matching PCR/ESI-MS or standard-of-care microbiology results and were excluded from the final analysis. Table 1 shows the patient demographics, reflecting a typically heterogeneous ICU population: one third of the patients were admitted from the emergency department; 75% were exposed to one or more antibiotics prior to study enrolment. Overall mortality was 29%, with cardiac arrest, septic shock, multiple organ failure, and acute respiratory distress syndrome accounting for ~62% of deaths.
BSI Analysis
A total of 616 direct whole-blood specimens from the 529 patients were tested to assess the accuracy of organism identification. PCR/ESI-MS results from analysis of blood using the bacteria, antibiotic resistance, and Candida BSI assay were compared with results from standard clinical microbiology cultures. As shown in Table 2, there were 228 PCR/ESI-MS positive specimens (36.5%) for at least one pathogen compared with 68 positive specimens by culture (10.9%). The total number of positive tests for each method was statistically different (McNemar test statistic = 137.6; df = 1; p < 0.0001). There were 55 samples that were positive for the same organism with both techniques (Table 2), yielding an overall concordance of identification (calculated sensitivity) of 81% (95% CI, 70–89%) and a κ value of 0.25 (95% CI, 0.18–0.31). In 13 instances, culture identified an organism that was either negative by PCR/ESI-MS (6/13) or the identity of the organism reported by PCR/ESI-MS did not match the organism identified by microbiology testing (7/13) (Table S1, Supplemental Digital Content 1,http://links.lww.com/CCM/B418). In contrast, PCR/ESI-MS reported a BSI-relevant organism in 173 additional specimens that were culture negative, resulting in a calculated assay specificity of 69% (Table S2, Supplemental Digital Content 1, http://links.lww.com/CCM/B418). Finally, there were 384 concordant negative specimens, yielding a negative predictive value (NPV) of ~97% (95% CI, 94–98%).
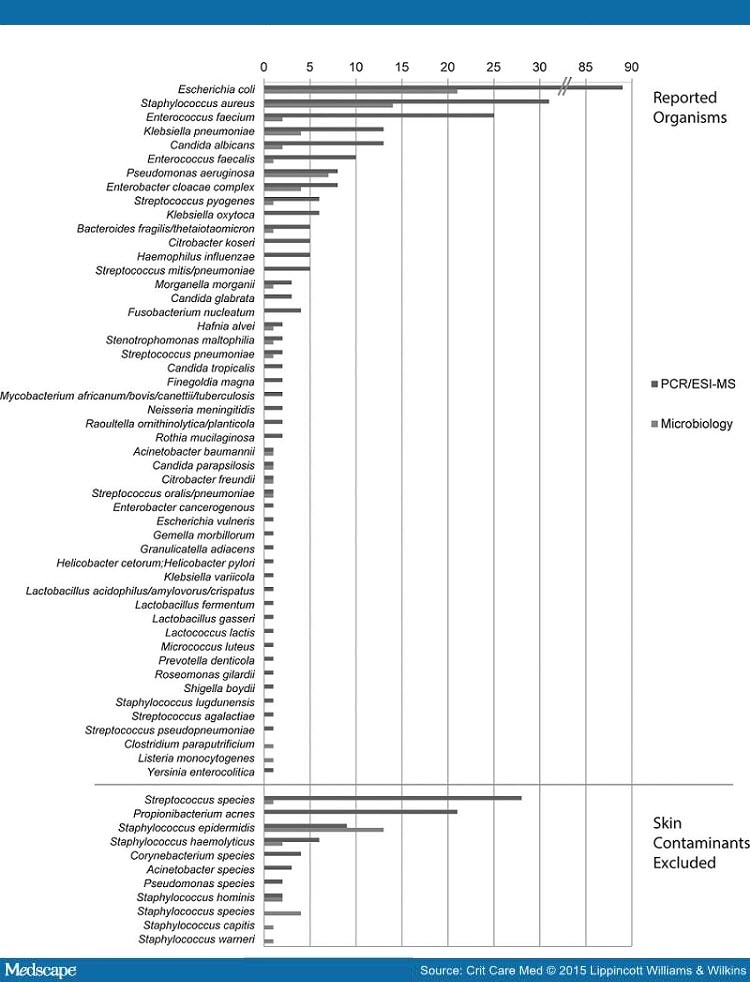
The frequencies of organisms detected from BSI specimens are shown in Figure 1. The distributions of the top 10 species detected by microbiology and those detected by PCR/ESI-MS were similar. The largest single discrepancy between the two methods by sheer volume of detections was in the identification of Escherichia coli. Although culture and PCR/ESI-MS techniques both reported E. coli as the most abundant species, PCR/ESI-MS detection was 4-fold higher (89 vs 21). Other organisms in which blood culture performed less well included the enterococcus species, Enterococcus faecalis (1 vs 10) and Enterococcus faecium (2 vs 25), Candida albicans (2 vs 13), and Staphylococcus aureus (14 vs 31). In contrast, Pseudomonas aeruginosa detection was comparable between the two methods (6 vs 8). Additional analysis of the PCR/ESI-MS results showed that the levels (genome equivalent/mL) of organisms reported in the majority of these PCR/ESI-MS positive, but culture-negative, cases were similar to cases in which culture matched PCR/ESI-MS detections (data not shown).

Figure 1.
http://img.medscape.com/article/853/105/853105-fig1.jpg
{kind=link}
Bacteria and Candida detected in the Rapid Diagnosis of Infections in the Critically Ill (RADICAL) study. Distribution of organisms reported by polymerase chain reaction/electrospray ionization-mass spectrometry (PCR/ESI-MS) (blue bar) and culture (red bar) observed in the RADICAL study are shown, sorted by decreasing order of PCR/ESI-MS reported organisms. Both methods showed similar distribution for the top eight reportable organisms that were seen >5 times by PCR/ESI-MS, with some minor reshuffling of the order. PCR/ESI-MS showed a longer tail of reportable organisms that were infrequent (≤5 times). Normal skin flora are shown below the line were not included in further analysis by either method.
Nonbloodstream Infections
Heterogeneous samples from patients with suspected pneumonia or sterile site infections were also obtained in several cases. Overall, there were 185 LRT samples (88 BAL, 96 ETA, and 1 other) and 110 SF&T samples (36 intraperitoneal fluid, 14 pleural fluid, 11 CSF, 13 tissue, and 36 other fluid types). Results from the analysis of these specimens are shown in Table 3. LRT and SF&T specimens often had multiple detections reported by both methods in several samples. Only the primary detections by either method were included in the analysis. The overall sensitivities for concordance between standard-of-care and PCR/ESI-MS were 84% (95% CI, 74–91%) and 85% (95% CI, 72–93%), respectively. As for the bloodstream infection data, the McNemar test for both the LRT and the SF&T sample data showed that the total number of samples considered positive was significantly different for culture versus PCR/ESI-MS (McNemar test statistic = 20.9 for LRT and 15.2 for SF&T; p < 0.0001 in both cases). Also similar to the bloodstream infection data, there was more agreement in the contingency table comparing culture to PCR/ESI-MS than would be expected by chance (LRT κ = 0.35; 95% confidence limits, 0.23, 0.47 and SF&T κ = 0.27; 95% confidence limits, 0.11, 0.43). For LRT specimens, there was no statistically significant difference in sensitivity (p = 0.677) or specificity (p = 0.444) when testing the hypothesis that the BAL proportion – the ETA proportion was equal to zero.
In 151 patients, two or more specimen types (BSI plus LRT and/or SF&T) were obtained and analyzed. In 86 of these 151 cases (57%), the same organisms were reported by PCR/ESI-MS in all samples tested from an individual patient (data not shown). In comparison, culture concordance between the sample types was seen in only 19 cases (12%), driven largely by no detection reported in the BSI culture results.
Resistance Markers
There were no identified cases of Klebsiella-associated carbapenemase. There was a single report of vancomycin-resistant Enterococci, which was matched across the two methods. There were 23 reports of mecA+ staphylococcus organisms (seven in BSI samples, 13 in LRT samples, and three in SF&T samples), with the following agreement between PCR/ESI-MS and culture: for BSI samples, results were concordant in four cases, and PCR/ESI-MS was positive and culture negative in three; for LRT samples, results were concordant in three cases, PCR/ESI-MS was positive with culture negative in nine, and PCR/ESI-MS was negative with culture positive in one; and the three cases in the SF&T samples were concordant across PCR/ESI-MS and culture.
Discussion
The important findings of the RADICAL study are that PCR/ESI-MS detected BSI pathogens with high overall sensitivity and NPV; PCR/ESI-MS was three times more likely to identify an organism than standard culture; and, if available, PCR/ESI-MS results may have altered the treatment regimen in as many as 57% of patients.
Sepsis affects a large proportion of the critically ill population. Despite improvements in recent years, morbidity and mortality rates remain high.[18] The importance of initiating treatment as soon as possible has been highlighted and shown to be associated with improved outcomes,[2] yet this finding needs to be balanced against the direct risks and stewardship issues arising from overzealous or inappropriate antibiotic use.
Rapid diagnosis of severe infection or sepsis is thus crucial not only to optimize a patient’s chances of survival but also to encourage responsible antibiotic use. However, diagnosing infection accurately in critically ill patients is challenging. Characteristic clinical and laboratory signs of severe infection, such as tachycardia, fever, and altered WBC count, are nonspecific and are often present in other acute conditions. Biomarkers, such as C-reactive protein and procalcitonin, are also nonspecific and are of more value in ruling out infection than in making a definite diagnosis.[19] Microbiological culture results are negative in many patients with sepsis, largely because prior antimicrobial therapy affects ex vivo growth in culture medium.[1] Certain microorganisms are also particularly difficult to culture, requiring specific growth media or a particular environment. As culture results often require several days to become available, patients with suspected severe infection are, therefore, often started on empiric broad-spectrum antibiotics to increase the likelihood that a pathogenic organism will be adequately covered. This approach, although valid in terms of preventing delays in starting treatment with currently available diagnostic techniques, has several negative aspects, including the potential for toxicity with multiple antibiotics, the high-associated costs, and the effects of antibiotic pressure on the development of antimicrobial resistance.[20]
Availability of a technique that could provide more rapid pathogen identification directly from patient samples could, therefore, represent a marked improvement in terms of enabling more rapid diagnosis and earlier initiation of appropriate antimicrobial therapy, with associated beneficial effects on outcomes, antimicrobial resistance, costs, and toxicity. Various methods have been suggested for this purpose, including single pathogen assays, which are of limited use in patients with suspected sepsis in whom multiple organisms may be involved; selected-pathogen assays, which use specific molecular targets to identify some 20–35 species;[21–23] and broad-range pathogen assays, which use universal or conserved targets to identify many hundreds of species, but for which earlier versions lacked sensitivity due to the small volumes of blood extracted for analysis.[24,25]
Importantly, in 41% of cases, the panel of independent experts would have recommended a change in management, including initiation of therapy, altered antimicrobial spectrum, and/or change in duration of therapy, based on the PCR/ESI-MS results. This percentage increased to 57 when PCR/ESI-MS tests were positive.
Second, the greater detection rate of E. coli, S. aureus, E. faecium, C. albicans, and Klebsiella pneumoniae by PCR/ESI-MS compared with routine culture was unanticipated, and the explanation is unclear. Prior to study inclusion, most patients were exposed to combinations of two or more antibiotics active against Gram-positive and Gram-negative organisms and were often receiving one or more antifungals in addition. As stated above, the bacterium/fungus may have been largely cleared with preexisting antibiotics, hence the negative culture results, but remaining DNA remnants in the circulation may have been sufficient to give a positive PCR/ESI-MS. The sensitivity of the technique increases the risk of identifying contaminants and commensals; however, the pathogens most frequently detected in the study are those associated with infection. Accepting the validity of these data, the PCR/ESI-MS test could be of importance to help target antimicrobial therapy in patients who have already started antimicrobials and have negative cultures (salvage microbiology).[29] Further, ideally interventional, studies are warranted to confirm and further explore these findings.
Leave a Reply