Arterial Hypertension in Young Adults: An Ignored Chronic Problem
Author: Manuela Stoicescu, MD, PhD
Manuela Stoicescu, MD, PhD
Consultant Internal Medicine, Assistant Professor
Faculty of Medicine and Pharmacy, Medical Disciplines Department
University of Oradea, Romania
ABSTRACT
Introduction:
Don’t ignore the young patients: being young does not necessary mean being healthy.
Objectives:
The objectives in this study was to analyzed the principal clinical aspects and conduct laboratory investigations with young people in group of age 18-35 years. Attracting attention to the diagnosis of hypertension in the young in the early stages of life. I choice this topic because high blood pressure in the young, in particularly, in this group age was insufficiently studied while a high frequency of cases presented every day was continuously increasing.
Material and method:
The study was performed in the Ambulatory Specialty of the Internal Diseases Department in the County Hospital in Oradea, Romania. Study period was 1 October 2006 to 31 July 2009. Included in the study were 321 patients with hypertension exceeding 140/90 mmHg which was maintained higher after three consecutive determinations in intervals of one week to exclude the “white coat phenomenon”, an effect noted very frequent in young people, especially in young women, because a young persons have hyperactivity of simpatico nervous systemic, or the value of blood pressure was higher more than 170/110 mmHg from first determination.
Results
1. Importance of the genetic factors in the etiologies of disease was suggests that family prevalence of hypertension in the young people and another family diseases like hyperaldosteronism, polycystic kidney and multiple endocrine neoplasias MEN2a.
2. Importance of personal pathologic antecedents demonstrated in my study that repetitive Streptococcus angina with Streptococcus β hemolytic group A originated in the first place as a cause in hypertension in the young people in context of acute streptococcal renal parenchymatous diseases.
3. Renin plasmatic level is a very important marker of high blood pressure in the young. It was high in 121 cases (37.69%). This situation suggests that hypertension in the young is hyperreninemic hypertension in many cases because a young person has a systemic hyperactivity of simpatico nervous.
4. Left ventricular hypertrophy is been detected in X-ray, ECG and echocardiography. In my studied I detected left ventricular hypertrophy in 35 patients representing 10.49%.
5. Proteinuria was represented in 96 cases (29.90%) has two meanings:
- nephropathy complication of hypertension or
- acute glomerulonephritis or
- nephritis syndrome accompaniment with hematuria 38 cases (11.83%).
6. The eye ground findings of young people with hypertension are frequently normal. In the absence of prior readings, one needs to look for evidence of target organ damage that may suggest chronicity. In my study this changes appeared for 86 cases 23.3 %, hemorrhages and exudates I rarely found in 9 cases represent 2.8% and papilla edema was presented in 2 cases even when hypertension was very severe more than 200/120 mmHg and complicate with hypertensive encephalopathy.
Conclusions: Guidelines for hypertension treatment with young patients group of ages 18-35 was developed, which I hope will help the activity of physicians in general specialties in their practice, to use for diagnosis and easy work. This is new and hypertension in the young in this group of ages was insufficiently studied.
Key words: hypertension diagnosis, young adults.
INTRODUCTION
Prior to the last twenty years it was impossible to accept the idea that hypertension and atherosclerosis begin in adolescence and even earlier in childhood. Current concepts concerning the nature of hypertension in the young are changing. Earlier clinical impressions indicated that hypertension in the young was secondary and the essential hypertension occurred only rarely.
In my recent study, involving young people, of the age group of age 18-35 year old, indicated that young with high levels of blood pressure often the cause is known and often is unknown. When high BP (HBP) is found in the young the young compared with their peers, it is likely that the HBP will continue to Adulthood. My study has indicated that the level of blood pressure in young is closely related to the occurrence of hypertension in adulthood. Thus, changing concepts suggest that essential hypertension begins in early life. Considerable information is now known about the clinical and pathologic features of hypertension in adults.
We understand clinical diagnoses, the pathophysiology and humoral background, and the consequences of end stage renal disease (ESRD). We are even beginning to consider that essential hypertension may represent more than one disease. By contrast, little is known about the early natural development of essential hypertension. For example, how can hypertension in young be defined? We cannot equate level of blood pressure with cardiovascular damage as in adults (cardiovascular, cerebral, and renal disease). Furthermore, there is little specific information that can be used to predict development of adult hypertension. As a beginning, descriptive studies of the early natural development of essential hypertension are needed. It is logical to assume that prevention would be most successful if the disease process could be understood and treated in its earliest phase.
OBJECTIVES
Don’t ignore the young adult patient. Being young does not necessary means being healthy. Key objectives in my study was to analyze the principal clinical aspects and laboratory tests performed on young adults in the group age 18-35 year old, to advocate for the attention needed for diagnosis of hypertension in the young adults in the early stages of the disease.
MATERIAL AND METHOD
The study was performed in the Ambulatory Specialty of the Internal Diseases Department at the County Hospital in Oradea, Romana. Study period was 1 October 2006 to 31 July 2009. Study participants:
- 321 young patients,
- group of ages 18-35, patients with high blood pressure more than 140/90 mmHg
- after three consecutive determinations in interval one week maintain higher than 140/90 mmHg to exclude the “white coat phenomenon”, effect very frequently encountered with young adults especially with young women, because young person have a hyperactivity of sympathetic nervous system, or
- the value of blood pressure was high more than 170/110mmHg from first determination.
The patients had a comprehensive physical examination (clinical and par clinical) and diagnosed with hypertension in different stages.
The study consideration was done after having confirmed the diagnosis of hypertension and the standardization according to the phenomenon of high blood pressure and the classification of OMS.
The patients agreed to participate after being introduced in the study after they have been explained the deontological and preserving of the confidentiality criteria.
For statistics data I has been used the EPIINFO application, 6.0 version, a program of The Center of Disease Control and Prevention- Atlanta, with the Student method (test t) and χ²
RESULTS AND DISCUSSIONS
We observed that a 1/5 of the patients studied have in family antecedents of young adults hypertensive member of the family:hypertension in 70 cases (21.80%), stroke in 46 cases (14.33%), myocardial infarction in 55 cases (17.13%), peripheral vascular disease in 23 cases ( 7.16%) obesity 38 (11.83%), pre-eclamptic toxemia in 31 cases(9.65% ), hyperaldosteronism in 18 cases (5.60%), polycystic kidney in 26 cases (8.09%), multiple endocrine neoplasias MEN2a in 14 cases (4.36%) Distribution of cases according to family history. See, Table 1.
Table 1: Distribution of Cases according to Family History
|
Consideration |
No. of cases |
Percent |
|
Hypertension for parents, grandparents, aunts, uncles and cousins |
70 |
21.80% |
|
Family antecedents of stroke |
46 |
14.33 % |
|
Family antecedents of myocardial infarction |
55 |
17.13% |
|
Family antecedents of peripheral vascular disease |
23 |
7.16% |
|
Family antecedents of obesity |
38 |
11.83% |
|
Pre-eclamptic toxemia |
31 |
9.65% |
|
Hyperaldosteronism |
18 |
5.60% |
|
Polycystic kidney |
26 |
8.09% |
|
Multiple endocrine neoplasias MEN2a |
14 |
4.36% |
A significant numbers of patients in my studies did not have any antecedents of hypertension in their family history. That fact demonstrates that not only genetic factors have an important role in the etiology of the disease.ENvironmental factors count.
Significant number of hypertensive young patients had diseases in their personal history: Scarlatti in 27 (8.41%), repetitive angina with Streptococcus β hemolytic group A in 88 (27.41%), chronic ORAL infection focus in 35 (10.90%) chronic stomathological focus infections in 19 (5.91%), nephritis in 34(10.59%), endocrine disorders in 16 (4.98% ), physical and psychological in 22 (6.85%), head trauma in 11 (3.42%), therapy with corticosteroids secondary to another disease (for example erythematous systemic lupus) in 5 (1.55%), therapy with AINS drugs in 21 (6.54%), use decongestion nasal in 4 (1.24%) repetitive urinary tract infection in 28 (8.72%), syphilis in 11 (3.42%). See, Table II.
Table II: Distribution of Cases by Illnesses in Personal History
|
Consideration |
No. of cases |
Percent |
|
Scarlatti |
27 |
8.41% |
|
Repetitive Streptococcus angina with Streptococcus β hemolytic group A |
88 |
27.41% |
|
Chronic ORAL infection focus |
35 |
10.90% |
|
Chronic stomathological infection focus |
19 |
5.91% |
|
Nephritis |
34 |
10.59% |
|
Endocrine disorders |
16 |
4.98% |
|
Physical and psychical suprademanding |
22 |
6,85% |
|
Head trauma |
11 |
3,42% |
|
Therapy with corticosteroids |
5 |
1.55% |
|
Therapy with AINS |
21 |
6.54% |
|
Use decongestion at nasal |
4 |
1.24% |
|
Repetitive urinary tract infections |
28 |
8.72% |
|
Syphilis |
11 |
3.42% |
Fig.1: Principal Diseases Etiology for Young Hypertensive Patients
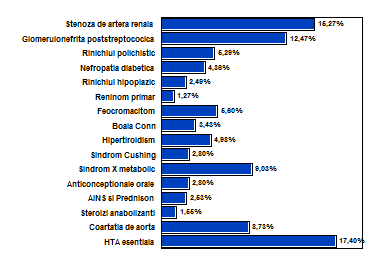
Table III: Laboratory Results
|
Hemoglobin value ↑ |
18 |
5.60% |
|
Hematocrit ↑ |
18 |
5.60% |
|
Value of glucose ↑ |
68 |
21.18% |
|
Cholesterol ↑ |
78 |
24.29% |
|
HDL cholesterol ↑ |
86 |
26.79% |
|
LDL cholesterol ↑ |
77 |
23.67% |
|
Triglycerides ↑ |
105 |
32.71% |
|
Uric acid ↑ |
57 |
17.75% |
|
Creatinina ↑ |
38 |
11.83% |
|
Urea ↑ |
36 |
11.21% |
|
Serum sodium ↑ |
42 |
13.08% |
|
Serum potassium↓ |
42 |
13.08% |
|
Urinalysis -albuminuria+ -hematuria+ |
96 |
29.90% |
|
38 |
11.83% |
|
|
Urine culture with female + |
104 |
32.29% |
Table IV: Laboratory Special Tests
|
Rennin plasmatic↑ |
121 |
37.69% |
|
Vanillyl Mandelic Acid testing (VMA): in urine↑ |
18 |
5.60% |
|
Catecholamine urine↑ |
18 |
5.60% |
|
Cortisol urine ↑ |
9 |
2.80% |
|
Cortisolemia ↑ |
9 |
2.80% |
|
TSH ↑ |
16 |
4.98% |
|
T3 ↑ |
16 |
4.98% |
|
T4 ↑ |
16 |
4.98% |
|
CT abdominal |
114 |
35.51% |
|
RMN abdominal |
158 |
49.92% |
|
Intravenous urogrography |
102 |
31.77% |
Observations on Eye Exam and Retinopathy [The eye ground (eye ground findings)]
Clearly, the most helpful information to have when one is attempting to establish the chronicity of hypertension is past blood pressure readings. Unfortunately, these are by no means always available since routine blood pressure measurement in young adults is not yet uniformly obtained. In the absence of prior readings, one needs to look for evidence of target organ damage that may suggest chronicity. In adolescent with even severe chronic hypertension or hypertensive encephalopathy. In my study this changes appear for the optic fund may show no more than retinal arteriolar narrowing in 103 cases represent 32.09% and arterio-venous nicking in 98 cases represent 30.53%, hemorrhages and exudates I rarely found in 9 cases represent 2.8%, papilla edema may be absent except in 2 cases even when hypertension was very severe more than 200/120 mmHg with complications of encephalopathy and in 109 cases represent 33.96 was normal result of eye ground examination. See Table V and Fig. 2
Just as there may be minimal eye ground findings, there are infrequently cardiac findings that suggest chronicity.
Table V Distribution of Cases by Eye Exam Findings
|
Normal |
109 |
33.96% |
|
Arteriolar narrowing |
103 |
32.09% |
|
Arterio-venous nicking |
98 |
30.53% |
|
Exudates and hemorrhages |
9 |
2.80% |
|
Papilla edema |
2 |
0.62% |
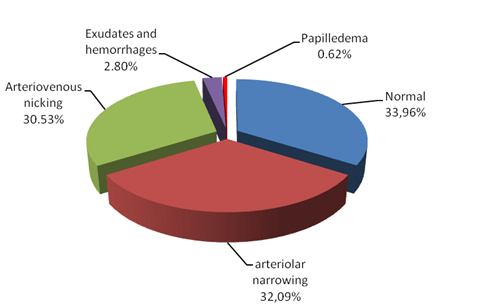
Fig. 2: Distribution of Cases by Changes of Eye Ground Findings
The heart morphology was not clinically enlarged in many cases and the ECG and chest X-ray were usually unhelpful in detecting left ventricular hypertrophy unless hypertension has been prolonged and severe. In my studies left ventricular hypertrophy was present in 35 cases (10.49%), they are helpful in determining chronicity of hypertension and in 206 cases (64.18%) left ventricular hypertrophy was absent. If negative suggesting nothing about the duration of hypertension. See Table VI and Fig 3
Table VI: Distribution of Cases by Changes in Chest X-Ray
|
Normal |
206 |
64.18% |
|
Elongation and elevated of left inferior arcos |
99 |
30.85% |
|
Cardiomegaly |
12 |
3.73% |
|
Aneurism of thoracic aorta |
4 |
1.24% |
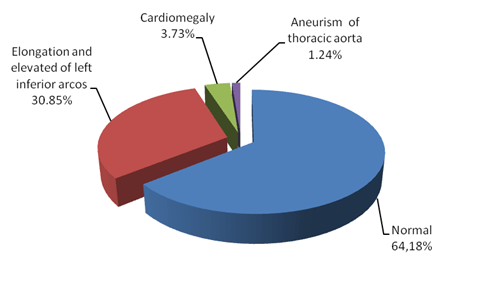
Fig. 3: Distribution of Cases by Changes of chest X-Ray
The echocardiography seems to be more sensitive for evaluating chamber size and wall thickness than the ECG and can be helpful. Left atria hypertrophy and left ventricular hypertrophy (Sokolow -Lyon index) and left axial deviation was possible to detect. In my studies I found 35 cases (10.49%) with LVH, 36 cases (11.21%) with LAH and 35 cases (10.49%) with left axial deviation. Secondary changes of depolarization like ST segment sub elevated and negative T wave I found in 35 cases represent 10.49%. See Table VII and Fig. 4
Table 7: Distribution of Cases by Changes in ECG
|
Normal |
180 |
56.07% |
|
Left axial deviation> -30 |
35 |
10.90% |
|
Left atria hypertrophy |
36 |
11.21% |
|
Left ventricular hypertrophy Sokolov -Lyon index(SV1+RV5/V6>35mm) |
35 |
10.90% |
|
Secondary changes of depolarization – ST segment sub elevated and T wave negative |
35 |
10.90% |
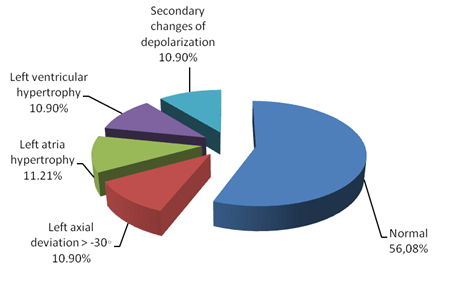
Fig. 4: Distribution of Cases by Changes in ECG
Table VIII: Distribution of cases by Echocardiography of Hearth Examination
|
Normal |
226 |
70.40% |
|
Left ventricular hypertrophy |
40 |
12.46% |
|
Ejection fraction(FE) of left ventricular<55% |
27 |
8.41% |
|
Aortic coarctation |
28 |
8.72% |
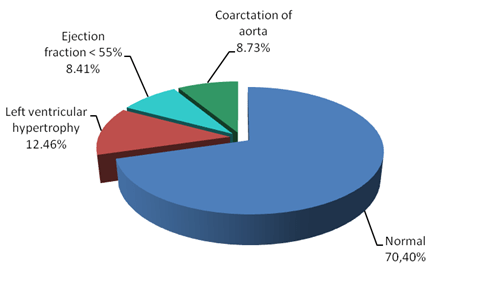
Fig. 5: Distribution of cases by Changes in Echocardiography
Table IX: Distribution of Cases by Urine Analysis Results
|
Normal |
187 |
58.27% |
|
Proteinuria |
96 |
29.90% |
|
Hematuria |
38 |
11.83 % |
Proteinuria I detect in 96 cases (29.90%) and hematuria in 38 cases (11.83%). See Fig. 6
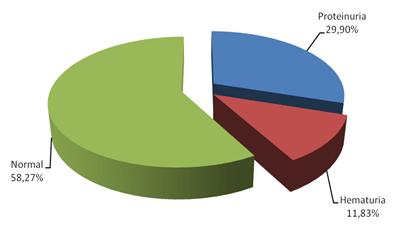
Fig.6: Distribution of cases by Urine Analysis Results
OMS stadialization classification high blood pressure in three stages. In my study about hypertension in the young adults, the results are as follows:
- Stages I: 270 cases represents 84.11%,
- Stages II: 40 cases represents 12.46%,
- Stages III: 9 cases (2.80%) and
- Stage IV: malign hypertension 2 cases represents 0.62%.
See, Table IX and Fig.7
Table IX: Distribution of Cases by Stadialization
|
Stages I |
270 |
84.11% |
|
Stages II |
40 |
12.46% |
|
Stages III |
9 |
2.81% |
|
Stages IV |
2 |
0.62% |
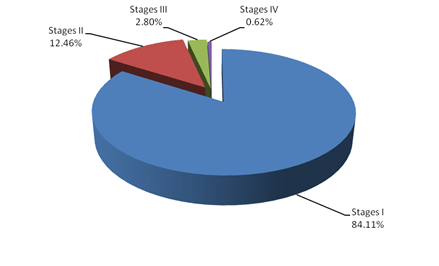
Fig. 7: Distribution of Cases by Stadialization
DISCUSSION
1. A 1/5 of group of patients studied have in family antecedents of young hypertensive family member with the following diseases:
- stroke 46 cases (14.33%),
- myocardial infarction 55 cases (17.13%),
- peripheral vascular disease 23 cases (7.16%),
- obesity 38 (11.83%),
- pre-eclamptic toxemia 31 cases (9.65%),
- hiperaldosteronism in 18 cases (5.60%),
- polycystic kidney 26cases (8.09%),
- multiple endocrine diseases II 14 cases (4.36%).
These results are in concordance with observations of Kotchen JM [1] which in a studies about young hypertensive patients concluded that family aggregation of hypertension was very frequent 20.2% (p<0,001) suggesting the importance of a genetic factor in the etiology of hypertension in the young adults.
2. An important number of hypertensive young patients were present in personal pathological antecedents: Scarlatti 27 (8.41%), repetitive angina with Streptococcus β hemolytic group A 88 (27.41%),chronic ORL infection focus 35 (10.90%) chronic stomathological focus infections 19 (5.91%), nephritis 34 (10.59%), endocrine disorders 16 (4.98% ), physical and psychical supra solicitation 22 (6.85%), head trauma 11 ( 3.42% ), therapy with corticosteroizi from another disease (for example erithematous systemic lupus) 5 (1.55%) therapy with AINS drugs 21 (6.54%), use decongestion nasal 4 (1.24%) repetitive urinary tract infection 28 (8.72%), syphilis 11 (3.42%)(p<0,001). Loggie JMH [2] in a studies with hypertension in the young reported the streptococcus infection with Streptococcus β hemolytic group A was 18.2% , chronic ORAL infection focus was 8.9%, chronic stomathological focus infections was 3.98%, glomerulonephritis was 6.2% and physical and psychical supra solicitation was 12.43% in personal pathological antecedents.
3. Changes of retinal vascular were insufficiently studied in young adults. In my study this changes appear for the optic fund may show no more than retinal arteriolar narrowing 103 cases represent 32.09% and arterio venous nicking 98 cases represent 30.53% , hemorrhages and exudates I rarely found from 9 cases represent 2.8%, papilla edema may be absent except 2 cases even with hypertension was very severe more than 200/120mmHg and complicate with encephalopathy and 109 cases represent 33.96% was normal result of funduoscopic examination (p<0.001).
Skalina MEL et al. [3] observations: 281 hypertensive young patients 140 have changes for the optic fund arterio venous nicking 93 cases, hemorrhages found from 7 cases and exudates appear from 40 patients. 141 patients have the optic fund examination normal.
4. The heart is not often clinically enlarged and the ECG and chest X-ray are usually unhelpful in detecting left ventricular hypertrophy unless hypertension has been prolonged and severe. In my studies left ventricular hypertrophy was present in 35 cases (10.49%), they are helpful in determining chronicity of hypertension and from 206 cases (64.174%) left ventricular hypertrophy was absent, that suggest that if negative, they tell one nothing about the duration of hypertension. The results are in concordance with observation with Laird WP and Fixler DE [4] who reports after performing chest X-ray for 210 young hypertensive, 103 have normal results, 78 have elongation and elevated of left inferior arcos and 29 present’s cardiomegaly.
5. The echocardiogram seems to be more sensitive for evaluating chamber size and wall thickness than the ECG and can be helpful. Left atria hypertrophy and left ventricular hypertrophy (Sokolow-Lyon index) and left axial deviation it’s possible to detect. In my studies I found 35 cases (10.49%) with LVH, 36 cases (11.21%) with LAH and 35 cases (10.49%) with left axial deviation. Secondary changes of depolarization like ST segment sub elevated and negative T wave I found from 35 cases represent 10.49% (p<0,001).The results are in concordance with observation with Laird WP and Fixler DE [4], who reports than 18% from young hypertensive subject, presents left ventricular hypertrophy detected after echocardiography examination, end in concordance with observation with Schieken RM et al. [5] in Muscatine studies who reports more than 14% from young hypertensive subjects have left ventricular hypertrophy after make echocardiography examination.
6. Proteinuria I detect in 96 cases (29.90%) and hematuria in 38 cases (11.83%).This changes appear in context of acute glomerulonephritis and hypertension was secondary renal.
Schmider et al. [6] sustained that glomerular hyperfiltration is a early marker for nefroangiosclerosis and a sign for subclinical organ affected.
7. OMS stadialization classification high blood pressure in three stages. In my study about hypertension in young adults the results are: in stages I found 270 cases represents 84.11%, in stages II 40 cases represents 12.46%, in stages III 9 cases (2.80%) and malign hypertension 2 cases represents 0.62%.
CONCLUSIONS
- 1. Importance of genetic factors in etiologies of disease is suggested that family aggregation of hypertension in young adults and another familial diseases like hyperaldosteronism, polycystic kidney and multiple endocrine diseases II.
- 2. Importance of personal pathologic antecedents demonstrated in my study that repetitive Streptococcus angina with Streptococcus β hemolytic group A was found in the first place as a cause of hypertension in the young people in context of acute streptococcal renal parenchymatous diseases.
- 3. Except nonspecific symptoms of high blood pressure exist specifically symptoms who suggest etiology of hypertension with young people.
- 4. The fundoscopic findings in the young adult with hypertension are frequently normal. In the absence of prior readings, one needs to look for evidence of target organ damage that may suggest chronicity. In my study this changes appear for 86 cases 23.3 % and hemorrhages and exudates I rarely found from 9 cases represent 2.8% and papilla edema may be absent except 2 cases even with hypertension is very severe more than 200/120mmHg and complication of encephalopathy.
- 5. Left ventricular hypertrophy is possible to detect X-ray, ECG and echocardiography. In my studied I detected left ventricular hypertrophy from 35 patients represent 10.49%.
- 6. Proteinuria 96 cases (29.90%) have two significance: nephropathy complication of high blood pressure, or etiology in context or glomerulonephritis alone or accompaniment with hematuria 38 cases (11.83%) in nephritis syndrome.
- 7. Renin plasmatic level is very important marker of high blood pressure in the young. Was high in 121 cases (37.69%).This situation suggests that hypertension in the young is hiperreninemic hypertension in many cases because young adults have hyperactivity of sympatetic nervous system.
- 8. OMS classification evaluated stages I 270 cases (84.11%), stages II 40 cases (12.46%) in stages III 9 cases (2.80%) and malign hypertension (stages IV) 2 cases (0.62%)
- 9. Finally I make a small guideline about hypertension with young patients group of ages 18-35, which I hope to help activity of every physician indifferent specialties in your practice, to use for diagnosis and easy work.
REFERENCES
1. Kotchen JM “Effect of relative weight on familial blood pressure aggregations“ Am J Epidemiol.1987 105-214.
2. Loggie JMH. “The diagnostic evaluation of adolescents with hypertension.” In Hunt JC, Dreifus LS, Dustan HP et al, eds Dialogues in Hypertension Update II vol 1. Lyndhurst, NJ: Health Learning Systems 1984:43-56.
3. Skalina MEL et al.: Annable WL, Kleigman RM, Fanaroff AA “ Hypertensive retinopathy in the adolescent“ J Adolesc. 1983:103:781-6.
4. Laird WP and Fixler DE. “Left ventricular hypertrophy in adolescents with elevated blood pressure: assessment by chest roentgenography, electrocardiography and echocardiography.” Adolescents 2001;67:255-9.
5.Schieken RM and coauthors: Clarke WR, Lauer RM, “Left ventricular hypertrophy in the young with blood pressures in the upper quin-tile of the distribution: the Muscatine study.” Hypertenesion 2004;3:669-75.
6. Schmider and coauthors: Messerli FH, Garavaglia GE, Nunez BD “Glomerular hyperfiltration indicates target organ disease in essential hypertension.” Circulation 2003; 76: III-273.
PUT IT IN CONTEXT OF CANCER CELL MOVEMENT
The contraction of skeletal muscle is triggered by nerve impulses, which stimulate the release of Ca2+ from the sarcoplasmic reticuluma specialized network of internal membranes, similar to the endoplasmic reticulum, that stores high concentrations of Ca2+ ions. The release of Ca2+ from the sarcoplasmic reticulum increases the concentration of Ca2+ in the cytosol from approximately 10-7 to 10-5 M. The increased Ca2+ concentration signals muscle contraction via the action of two accessory proteins bound to the actin filaments: tropomyosin and troponin (Figure 11.25). Tropomyosin is a fibrous protein that binds lengthwise along the groove of actin filaments. In striated muscle, each tropomyosin molecule is bound to troponin, which is a complex of three polypeptides: troponin C (Ca2+-binding), troponin I (inhibitory), and troponin T (tropomyosin-binding). When the concentration of Ca2+ is low, the complex of the troponins with tropomyosin blocks the interaction of actin and myosin, so the muscle does not contract. At high concentrations, Ca2+ binding to troponin C shifts the position of the complex, relieving this inhibition and allowing contraction to proceed.
Figure 11.25
Association of tropomyosin and troponins with actin filaments. (A) Tropomyosin binds lengthwise along actin filaments and, in striated muscle, is associated with a complex of three troponins: troponin I (TnI), troponin C (TnC), and troponin T (TnT). In (more ) Contractile Assemblies of Actin and Myosin in Nonmuscle Cells
Contractile assemblies of actin and myosin, resembling small-scale versions of muscle fibers, are present also in nonmuscle cells. As in muscle, the actin filaments in these contractile assemblies are interdigitated with bipolar filaments of myosin II, consisting of 15 to 20 myosin II molecules, which produce contraction by sliding the actin filaments relative to one another (Figure 11.26). The actin filaments in contractile bundles in nonmuscle cells are also associated with tropomyosin, which facilitates their interaction with myosin II, probably by competing with filamin for binding sites on actin.
Figure 11.26
Contractile assemblies in nonmuscle cells. Bipolar filaments of myosin II produce contraction by sliding actin filaments in opposite directions. Two examples of contractile assemblies in nonmuscle cells, stress fibers and adhesion belts, were discussed earlier with respect to attachment of the actin cytoskeleton to regions of cell-substrate and cell-cell contacts (see Figures 11.13 and 11.14). The contraction of stress fibers produces tension across the cell, allowing the cell to pull on a substrate (e.g., the extracellular matrix) to which it is anchored. The contraction of adhesion belts alters the shape of epithelial cell sheets: a process that is particularly important during embryonic development, when sheets of epithelial cells fold into structures such as tubes.
The most dramatic example of actin-myosin contraction in nonmuscle cells, however, is provided by cytokinesisthe division of a cell into two following mitosis (Figure 11.27). Toward the end of mitosis in animal cells, a contractile ring consisting of actin filaments and myosin II assembles just underneath the plasma membrane. Its contraction pulls the plasma membrane progressively inward, constricting the center of the cell and pinching it in two. Interestingly, the thickness of the contractile ring remains constant as it contracts, implying that actin filaments disassemble as contraction proceeds. The ring then disperses completely following cell division.
Figure 11.27
Cytokinesis. Following completion of mitosis (nuclear division), a contractile ring consisting of actin filaments and myosin II divides the cell in two.
http://www.ncbi.nlm.nih.gov/books/NBK9961/
This is good. I don’t recall seeing it in the original comment. I am very aware of the actin myosin troponin connection in heart and in skeletal muscle, and I did know about the nonmuscle work. I won’t deal with it now, and I have been working with Aviral now online for 2 hours.
I have had a considerable background from way back in atomic orbital theory, physical chemistry, organic chemistry, and the equilibrium necessary for cations and anions. Despite the calcium role in contraction, I would not discount hypomagnesemia in having a disease role because of the intracellular-extracellular connection. The description you pasted reminds me also of a lecture given a few years ago by the Nobel Laureate that year on the mechanism of cell division.
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette
I actually consider this amazing blog , âSAME SCIENTIFIC IMPACT: Scientific Publishing –
Open Journals vs. Subscription-based « Pharmaceutical Intelligenceâ, very compelling plus the blog post ended up being a good read.
Many thanks,Annette