Apixaban (Eliquis): Mechanism of Action, Drug Comparison and Additional Indications
Curator: Aviva Lev-Ari, PhD, RN

WordCloud by Zach Day; Article Title: Apixaban (Eliquis): Mechanism of Action, Drug Comparison and Additional Indications
Updated on 9/30/2022
PROACT Xa Trial of Apixaban With On-X Heart Valve Stopped
Artivion Inc. has halted the PROACT Xa clinical trial that was testing whether patients with an On-X mechanical aortic valve could be safely and effectively managed with the direct oral anticoagulant (DOAC) apixaban (Eliquis) rather than warfarin.
The decision to stop the trial was based on the recommendation of the independent data and safety monitoring board (DSMB), which cited a lack of evidence supporting noninferiority of apixaban over warfarin for valve thrombosis and thromboembolism.
Currently, warfarin is the only approved anticoagulant for patients with mechanical valves.
In the PROACT Xa trial, which began enrollment in April 2020, patients with an On-X mechanical aortic valve were randomly allocated to receive anticoagulation with warfarin or apixaban.
“The DSMB found that blood clots, resulting in stroke, occurred more frequently in patients receiving apixaban and that continuing the trial was unlikely to achieve the primary endpoint while possibly exposing patients to increased risk,” Artivion said in a statement.
“The PROACT Xa trial was designed to determine whether apixaban would yield equivalent safety to the standard anticoagulant, warfarin. Unfortunately, it appears that it does not,” John Alexander, MD, chair of the PROACT Xa trial and professor of medicine/cardiology at Duke University School of Medicine, Durham, North Carolina, said in the statement.
SOURCE
@@@@
During the past 20 years, the approval of anticoagulants such as low-molecular-weight heparins (LMWHs), indirect factor Xa inhibitors (eg, fondaparinux), and direct thrombin inhibitors (eg, argatroban, bivalirudin, lepirudin, and desirudin) has signaled a growing interest in antithrombotic compounds that have relatively discrete targets within the coagulation pathway. Although these medications offer several potential advantages over unfractionated heparin, they all require parenteral administration and are substantially more expensive than oral vitamin K antagonists (VKAs). Thus VKAs, despite disadvantages such as variability in dose response, a narrow therapeutic index, and numerous drug and dietary interactions, are the only option for most patients requiring chronic anticoagulation.
http://bloodjournal.hematologylibrary.org/content/115/1/15.full
Eliquis Approval History
-
FDA approved: Yes (First approved December 28th, 2012)
- Brand name: Eliquis
- Generic name: apixaban
- Company: Bristol-Myers Squibb Company and Pfizer Inc.
- Treatment for: Prevention of Thromboembolism in Atrial Fibrillation, Deep Vein Thrombosis Prophylaxis after Knee Replacement Surgery, Deep Vein Thrombosis Prophylaxis after Hip Replacement Surgery
Eliquis (apixaban) is a factor Xa inhibitor anticoagulant indicated to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, and for the prophylaxis of deep vein thrombosis (DVT) in patients who have undergone hip or knee replacement surgery .
.
FDA Approval History for Eliquis
http://www.drugs.com/history/eliquis.html
Indirect Comparisons of New Oral Anticoagulant Drugs for Efficacy and Safety When Used for Stroke Prevention in Atrial Fibrillation
Results There was a significantly lower risk of stroke and systemic embolism (by 26%) for dabigatran (150 mg BID) compared with rivaroxaban, as well as hemorrhagic stroke and nondisabling stroke. There were no significant differences for apixaban versus dabigatran (both doses) or rivaroxaban; or rivaroxaban versus dabigatran 110 mg BID in preventing stroke and systemic embolism. For ischemic stroke, there were no significant differences between the new OACs. Major bleeding was significantly lower with apixaban compared with dabigatran 150 mg BID (by 26%) and rivaroxaban (by 34%), but not significantly different from dabigatran 110 mg BID. There were no significant differences between apixaban and dabigatran 110 mg BID in safety endpoints. Apixaban also had lower major or clinically relevant bleeding (by 34%) compared with rivaroxaban. When compared with rivaroxaban, dabigatran 110 mg BID was associated with less major bleeding (by 23%) and intracranial bleeding (by 54%). There were no significant differences in myocardial infarction events between the dabigatran (both doses) and apixaban.
Conclusions Notwithstanding the limitations of an indirect comparison study, we found no profound significant differences in efficacy between apixaban and dabigatran etexilate (both doses) or rivaroxaban. Dabigatran 150 mg BID was superior to rivaroxaban for some efficacy endpoints, whereas major bleeding was significantly lower with dabigatran 110 mg BID or apixaban. Only a head-to-head direct comparison of the different new OACs would fully answer the question of efficacy/safety differences between the new drugs for stroke prevention in AF.
http://content.onlinejacc.org/article.aspx?articleid=1182715
Clinical trials with new oral anticoagulants |
| Journal: | Hämostaseologie |
| ISSN: | 0720-9355 |
| Topic: | 57. Jahrestagung der Gesellschaft für Hämostase- und Thromboseforschung e.V. HÄMOSTASEOLOGIE INTERDISZIPLINÄR |
| DOI: | http://dx.doi.org/10.5482/HAMO-12-11-0021 |
| Issue: | Issues of 2013 (Vol. 33): Issue 1 2013 (1-76) |
| Pages: | 62-70 |
New Eliquis® (apixaban) Post-hoc Subanalysis of the Phase III ARISTOTLE trial Demonstrated that within 30 Days of a Procedure, Stroke or Systemic Embolism and Major Bleeding were Uncommon –
About ARISTOTLE
The ARISTOTLE study was designed to demonstrate the efficacy and safety of Eliquis versus warfarin for the prevention of stroke or systemic embolism. In ARISTOTLE, 18,201 patients were randomized (9,120 patients to Eliquis and 9,081 to warfarin). ARISTOTLE was an active-controlled, randomized, double-blind, multi-national trial in patients with nonvalvular atrial fibrillation or atrial flutter, and at least one additional risk factor for stroke. Patients were randomized to treatment with Eliquis 5 mg orally twice daily (or 2.5 mg twice daily in selected patients, representing 4.7 percent of all patients) or warfarin (target INR range 2.0-3.0), and followed for a median of 1.8 years.
Results presented today at the ESC Congress 2013
The new oral anticoagulants
Apixaban
Phase 2 data for apixaban in the prevention and treatment of venous thromboembolism (VTE) suggested that this compound may be a safe and effective anticoagulant over a wide range of doses.16,17 The first phase 3 orthopedic prophylaxis trial (ADVANCE-1) randomized 3195 patients, in double-blind fashion, to either apixaban (2.5 mg orally twice a day) or enoxaparin (30 mg subcutaneously every 12 hours). In both arms, treatments were begun 12 to 24 hours after surgery; all patients underwent venography approximately 2 weeks later. The proportion of patients who reached the primary endpoint (VTE, both symptomatic and venographically detected, or death from any cause) was similar for the apixaban (8.99%) and enoxaparin (8.85%) arms; however, the predetermined noninferiority endpoint was not met.7 It is unclear whether the failure to prove noninferiority can be explained by inaccurately low prestudy estimates of event rates, the dose/timing of apixaban, or some other cause. In any case, the comparable event rates (neither regimen was found superior to the other), along with less clinically relevant bleeding in the apixaban arm, strongly suggest that apixaban is an effective anticoagulant. Results from ADVANCE-2, a randomized double-blind multicenter trial comparing apixaban 2.5 mg orally twice a day with enoxaparin 40 mg subcutaneously once daily for preventing VTE after total knee replacement were presented at the congress of the International Society of Thrombosis and Hemostasis in July 2009. The primary efficacy outcome (all VTE) occurred in 147 of 976 evaluable patients (15.1%) in the apixaban group and 243 of 997 evaluable patients (24.4%) in the enoxaparin group (relative risk = 0.62; 95% confidence interval, 0.51-0.74, 1-sidedP < .001). A nonsignificant trend toward less clinically relevant bleeding also favored apixaban (53 patients, 3.5% vs 72 patients, 4.8%; P = .09).
A phase 3 study (AMPLIFY) of patients with acute VTE (deep vein thrombosis [DVT] and/or pulmonary embolism [PE]) will compare apixaban (10 mg twice daily for 7 days, followed by apixaban 5 mg, twice daily for 6 months) to a standard strategy using enoxaparin followed by VKA. A phase 3 “extension” study will enroll patients for whom there is clinical uncertainty about whether to continue oral anticoagulation after 6 months of routine treatment with a VKA. Participants will be randomly assigned to receive 1 of 3 possible interventions for 12 months: placebo, apixaban 2.5 mg twice daily, or apixaban 5 mg twice daily. In both trials, the primary outcome measure will be a composite of symptomatic, objectively confirmed recurrent VTE or death during the treatment period.
The APPRAISE trial was a phase 2 dose-finding study in which 1700 patients were randomized to receive placebo or 1 of 4 apixaban doses for the 6 months after standard acute therapy for acute coronary syndrome.18 For patients receiving the 2 highest doses of apixaban, the trial was terminated prematurely because of excess bleeding. In this population of patients receiving one or more concomitant antiplatelet agents, the 2 lower-dose apixaban arms had higher rates of the primary endpoint (major bleeding plus clinically relevant nonmajor bleeding) than did the placebo group. The trial was not powered to detect a statistically significant difference in the rates in the composite efficacy endpoint of cardiovascular death, nonfatal heart attack, severe recurrent ischemia, and nonhemorrhagic stroke but showed trends favoring apixaban over placebo for these endpoints. A phase 3 trial (APPRAISE-2) comparing apixaban 5 mg twice daily versus placebo in this clinical setting is under way.
Finally, apixaban is being studied as a stroke prevention strategy for patients with atrial fibrillation (AF). When completed, the ARISTOTLE trial will randomize approximately 18 000 patients with chronic nonvalvular AF to apixaban 5 mg orally twice daily or warfarin, target international normalized ratio (INR) 2.0 to 3.0. This event-driven, double-blind, parallel arm study is designed to show that apixaban is noninferior to well-managed warfarin in the prevention of stroke or systemic embolism. In a different randomized, double-blind study (AVERROES), apixaban (5 mg orally twice daily) is being compared with aspirin (81-324 mg daily) among AF patients who have failed or are unsuitable for VKA treatment. This trial will include 5000 to 6000 patients; follow-up will be up to 36 months.
http://bloodjournal.hematologylibrary.org/content/115/1/15.full
Clinical Studies
Reduction Of Risk Of Stroke And Systemic Embolism In Nonvalvular Atrial Fibrillation
ARISTOTLE
Evidence for the efficacy and safety of ELIQUIS was derived from ARISTOTLE, a multinational, double-blind study in patients with nonvalvular AF comparing the effects of ELIQUIS and warfarin on the risk of stroke and non-central nervous system (CNS) systemic embolism. In ARISTOTLE, patients were randomized to ELIQUIS 5 mg orally twice daily (or 2.5 mg twice daily in subjects with at least 2 of the following characteristics: age ≥ 80 years, body weight ≤ 60 kg, or serum creatinine ≥ 1.5 mg/dL) or to warfarin (targeted to an INR range of 2.0–3.0). Patients had to have one or more of the following additional risk factors for stroke:
- prior stroke or transient ischemic attack (TIA)
- prior systemic embolism
- age ≥ 75 years
- arterial hypertension requiring treatment
- diabetes mellitus
- heart failure ≥ New York Heart Association Class 2
- left ventricular ejection fraction ≤ 40%
The primary objective of ARISTOTLE was to determine whether ELIQUIS 5 mg twice daily (or 2.5 mg twice daily) was effective (noninferior to warfarin) in reducing the risk of stroke (ischemic or hemorrhagic) and systemic embolism. Superiority of ELIQUIS to warfarin was also examined for the primary endpoint (rate of stroke and systemic embolism), major bleeding, and death from any cause.
A total of 18,201 patients were randomized and followed on study treatment for a median of 89 weeks. Forty-three percent of patients were vitamin Kantagonist (VKA) “naive,” defined as having received ≤ 30 consecutive days of treatment with warfarin or another VKA before entering the study. The mean age was 69 years and the mean CHADS2 score (a scale from 0 to 6 used to estimate risk of stroke, with higher scores predicting greater risk) was 2.1. The population was 65% male, 83% Caucasian, 14% Asian, and 1% Black. There was a history of stroke, TIA, or non-CNS systemic embolism in 19% of patients. Concomitant diseases of patients in this study included hypertension 88%, diabetes 25%, congestive heart failure (or left ventricular ejection fraction ≤ 40%) 35%, and prior myocardial infarction14%. Patients treated with warfarin in ARISTOTLE had a mean percentage of time in therapeutic range (INR 2.0–3.0) of 62%.
ELIQUIS was superior to warfarin for the primary endpoint of reducing the risk of stroke and systemic embolism (Table 5 and Figure 4). Superiority to warfarin was primarily attributable to a reduction in hemorrhagic stroke and ischemic strokes with hemorrhagic conversion compared to warfarin. Purely ischemic strokes occurred with similar rates on both drugs.
ELIQUIS also showed significantly fewer major bleeds than warfarin [seeADVERSE REACTIONS].
Table 5: Key Efficacy Outcomes in Patients with Nonvalvular Atrial Fibrillation in ARISTOTLE (Intent-to-Treat Analysis)
| ELIQUIS N=9120 N (%/YEAR) |
WARFARIN N=9081 N (%/YEAR) |
HAZARD RATIO (95% CI) | P-VALUE | |
| Stroke or systemic embolism | 212 (1.27) | 265 (1.60) | 0.79 (0.66, 0.95) | 0.01 |
| Stroke | 199 (1.19) | 250 (1.51) | 0.79 (0.65, 0.95) | |
| Ischemic without hemorrhage | 140 (0.83) | 136 (0.82) | 1.02 (0.81, 1.29) | |
| Ischemic with hemorrhagic conversion | 12 (0.07) | 20 (0.12) | 0.60 (0.29, 1.23) | |
| Hemorrhagic | 40 (0.24) | 78 (0.47) | 0.51 (0.35, 0.75) | |
| Unknown | 14 (0.08) | 21 (0.13) | 0.65 (0.33, 1.29) | |
| Systemic embolism | 15 (0.09) | 17 (0.10) | 0.87 (0.44, 1.75) | |
| The primary endpoint was based on the time to first event (one per subject). Component counts are for subjects with any event, not necessarily the first. | ||||
Figure 4: Kaplan-Meier Estimate of Time to First Stroke or Systemic Embolism in ARISTOTLE (Intent-to-Treat Population)
http://www.rxlist.com/eliquis-drug/clinical-pharmacology.htm
Apixaban, a direct factor Xa inhibitor, inhibits tissue-factor induced human platelet aggregation in vitro : Comparison with direct inhibitors of factor VIIa, XIa and thrombin
P. C. Wong (1), X. Jiang (1)
(1) Thrombosis Research, Bristol-Myers Squibb Company, Pennington, New Jersey, USA
Keywords
Tissue factor, platelet aggregation, rivaroxaban, direct factor Xa inhibitor, dabigatran, Apixaban
Summary
Apixaban is an oral, direct and highly selective factor Xa (FXa) inhibitor in late-stage clinical development. This study evaluated the in vitro effect of apixaban on human platelet aggregation induced by thrombin derived via the extrinsic pathway. Direct inhibitors of FXa (rivaroxaban), FVIIa (BMS-593214), thrombin (dabigatran, argatroban) and FXIa (BMS-262084) were included for comparison. Citrated human platelets-rich plasma (PRP) was treated with 50 mg/ml corn trypsin inhibitor (to block the contact factor pathway) and 3 mM H-Gly-Pro-Arg-Pro-OH-AcOH (to prevent fibrin polymerisation). Human tissue factor (TF) (Innovin®; dilution 1:1,000 to 1:1,500) plus 7.5 mM CaCl2 was added to PRP pre-incubated with vehicle or increasing concentrations of inhibitors. The TF-induced platelet aggregation was measured by optical aggregometry. TF produced 85 ± 3% aggregation of human platelets in the vehicle-treated group (n=10). Apixaban and other factor inhibitors, except the FXIa inhibitor, inhibited TF-induced platelet aggregation with IC50 (nM) values as follows: 4 ± 1 (apixaban), 8 ± 2 (rivaroxaban), 13 ± 1 (BMS-593214), 46 ± 1 (dabigatran) and 79 ± 1 (argatroban). BMS-262084 (IC50 = 2.8 nM vs. human FXIa) had no effect on TF-induced platelet aggregation at 10 μM. These inhibitors at 10 μM had no effect on platelet aggregation induced by ADP and collagen, as expected from their mechanism of action. This study demonstrates that inhibition of thrombin generation by blocking upstream proteases (FVIIa and FXa) in the blood coagulation cascade is as effective as direct thrombin inhibition in preventing TF-induced platelet aggregation. Under these experimental conditions, a FXIa inhibitor did not prevent TF-induced platelet aggregation.
http://th.schattauer.de/en/contents/archive/issue/1099/manuscript/13269.html
Mechanism Of Action
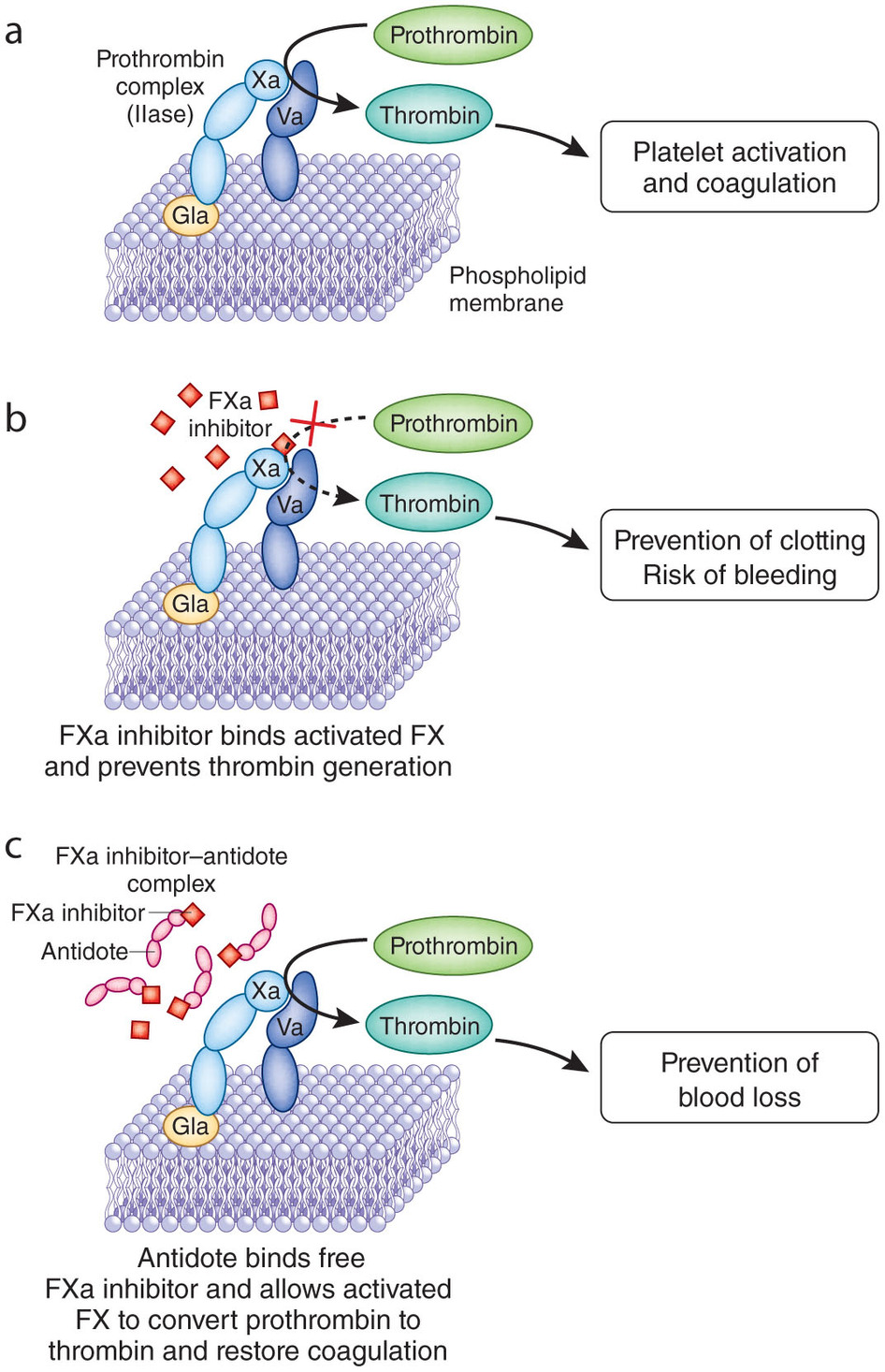
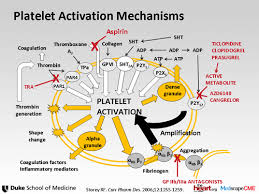
Apixaban is a selective inhibitor of FXa. It does not require antithrombin III for antithrombotic activity. Apixaban inhibits free and clot-bound FXa, and prothrombinase activity. Apixaban has no direct effect on platelet aggregation, but indirectly inhibits platelet aggregation induced by thrombin. By inhibiting FXa, apixaban decreases thrombin generation and thrombusdevelopment.
Pharmacodynamics
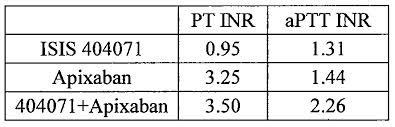
As a result of FXa inhibition, apixaban prolongs clotting tests such asprothrombin time (PT), INR, and activated partial thromboplastin time (aPTT). Changes observed in these clotting tests at the expected therapeutic dose, however, are small, subject to a high degree of variability, and not useful in monitoring the anticoagulation effect of apixaban.
The Rotachrom® Heparin chromogenic assay was used to measure the effect of apixaban on FXa activity in humans during the apixaban development program. A concentration-dependent increase in anti-FXa activity was observed in the dose range tested and was similar in healthy subjects and patients with AF.
This test is not recommended for assessing the anticoagulant effect of apixaban.
Pharmacodynamic Drug Interaction Studies
Pharmacodynamic drug interaction studies with aspirin, clopidogrel, aspirin and clopidogrel, prasugrel, enoxaparin, and naproxen were conducted. No pharmacodynamic interactions were observed with aspirin, clopidogrel, or prasugrel [see WARNINGS AND PRECAUTIONS]. A 50% to 60% increase in anti-FXa activity was observed when apixaban was coadministered with enoxaparin or naproxen.
Specific Populations
Renal impairment: Anti-FXa activity adjusted for exposure to apixaban was similar across renal function categories.
Hepatic impairment: Changes in anti-FXa activity were similar in patients with mild-tomoderate hepatic impairment and healthy subjects. However, in patients with moderate hepatic impairment, there is no clear understanding of the impact of this degree of hepatic function impairment on the coagulation cascade and its relationship to efficacy and bleeding. Patients with severe hepatic impairment were not studied.
Cardiac Electrophysiology
Apixaban has no effect on the QTc interval in humans at doses up to 50 mg.
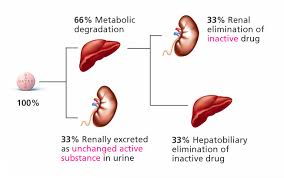
Pharmacokinetics
Apixaban demonstrates linear pharmacokinetics with dose-proportional increases in exposure for oral doses up to 10 mg.
Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials
Dr Christian T Ruff MD a 
 ,
,
Correspondence to: Dr Christian T Ruff, Thrombolysis in Myocardial Infarction (TIMI) Study Group, 350 Longwood Avenue, 1st Floor Offices, Boston, MA 02115, USABackground
Methods
Findings
Interpretation
Funding
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)62343-0/abstract
Comparative effectiveness of novel oral anticoagulants for atrial fibrillation: evidence from pair-wise and warfarin-controlled network meta-analyses
Table 1

Introduction
Novel oral anticoagulants have been tested against warfarin for atrial fibrillation, yet no direct comparison is available. We thus aimed to perform pair-wise (direct) and warfarin-adjusted network (i.e. indirect) meta-analyses of novel oral anticoagulants for atrial fibrillation.
Methods
Databases were searched for randomized warfarin-controlled trials of novel anticoagulants for non-valvular atrial fibrillation. The primary end-point was long-term stroke/systemic embolism. Odds ratios (95% intervals) were computed with RevMan and WinBUGS.
Results
Seven trials (52701 patients) were included, focusing on apixaban, dabigatran, edoxaban and rivaroxaban. Pair-wise meta-analysis showed that after a weighted average of 23 months these novel anticoagulants lead to significant reductions in the risk of stroke/systemic embolism (odds ratio=0.81 [0.71-0.92], I2=23%) and all cause death (odds ratio=0.88 [0.82-0.95], I2=0%) in comparison to warfarin. Network meta-analysis showed that apixaban and dabigatran proved similarly superior to warfarin in preventing stroke/systemic embolism (odds ratio=0.78 [0.62-0.96] for apixaban vs warfarin; odds ratio=0.66 [0.52-0.84] for high-dose dabigatran vs warfarin; odds ratio for apixaban vs high-dose dabigatran=1.17 [0.85-1.63]), but apixaban was associated with fewer major bleedings (odds ratio=0.73 [0.57-0.93]) and drug discontinuations (odds ratio=0.64 [0.52-0.78]) than dabigatran. Rivaroxaban did not reduce stroke/systemic embolism (odds ratio=0.87 [0.71-1.07]) or major bleedings in comparison to warfarin (odds ratio=0.87 [0.71-1.07]) and was associated with more major bleedings in comparison to apixaban (odds ratio=1.52 [1.19-1.92]). Data for edoxaban were inconclusive.
Conclusions
Novel oral anticoagulants appear as a very promising treatment option for atrial fibrillation.

Source: Google images
 Source: Google images
Source: Google images

SOURCE: Google Images

SOURCE
Google Images
SOURCE
Google Images
SOURCE
Google Images

SOURCE
Google Images

REFERENCES
| 1. |
Additive value of indirect comparisons (network meta-analyses) |
|
| Free download of English version
J. Harenberg (1), C. Weiss (2), S. Marx (1), S. Zolfaghari (1) Phlebologie 2013 42 3: 139-148 |
||
| 2. |
An indirect comparison analysis |
|
| Online Supplementary Material
F. Skjøth (1, 2), T. B. Larsen (1, 2), L. H. Rasmussen (1, 2), G. Y. H. Lip (1, 3) Thromb Haemost 2014 111 5: 981-988 |
||
| 3. |
Ready to be replaced? |
|
|
J. Steffel (1), T. F. Luscher (1) Hämostaseologie 2012 32 4: 249-257 |
||
- Roskell NS, Lip GY, Noack H et al. Treatments for stroke prevention in atrial fibrillation: a network meta-analysis and indirect comparisons versus dabigatran etexilate. Thromb Haemost 2010; 104: 1106-1115.DOI:10.1160/TH10-10-0642
- Hart RG, Pearce LA, Aguilar MI. Adjusted-dose warfarin versus aspirin for preventing stroke in patients with atrial fibrillation. Ann Intern Med 2007; 147: 590-592.
- Lip GY, Andreotti F, Fauchier L et al. Bleeding risk assessment and management in atrial fibrillation patients. Thromb Haemost 2011; 106: 997-1011. DOI:10.1160/TH11-10-0690
- Ansell J, Hirsh J, Hylek E et al. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8 th ed). Chest 2008; 133 (6 Suppl): 160S-198S. DOI:10.1378/chest.08-0670
- Ogilvie IM, Newton N, Welner SA et al. Underuse of oral anticoagulants in atrial fibrillation: a systematic review. Am J Med 2010; 123: 638-645.DOI:10.1016/j.amjmed.2009.11.025
- Tasker A, Harbord R, Bannister GC. Meta-analysis of low molecular weight heparin versus placebo in patients undergoing total hip replacement and post-operative morbidity and mortality since their introduction. Hip Int 2010; 20: 64-74.
- Falck-Ytter Y, Francis CW, Johanson NA et al. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9 th ed. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2 Suppl): e278S-325S. DOI:10.1378/chest.11-2404
- Linkins LA, Dans AL, Moores LK et al. Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9 th ed. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141 (2 Suppl): e495S-530S. DOI:10.1378/chest.11-2303
- Harenberg J, Wehling M. Current and future prospects for anticoagulant therapy: inhibitors of factor Xa and factor IIa. Semin Thromb Hemost 2008; 34: 39-57. DOI:10.1055/s-2008-1066023
- Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009; 361: 1139-1151.DOI:10.1056/NEJMoa0905561
- Connolly SJ, Ezekowitz MD, Yusuf S et al. Newly identified events in the RE-LY trial. N Engl J Med 2010; 363: 1875-1876.DOI:10.1056/NEJMc1007378
- Patel MR, Mahaffey KW, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365: 883-891.DOI:10.1056/NEJMoa1009638
- Granger CB, Alexander JH, McMurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011; 365: 981-992.DOI:10.1056/NEJMoa1107039
- Glenny AM, Altman DG, Song F et al. Indirect comparisons of competing interventions. Health Technol Assess 2005; 9: 1-134.
- Lumley T. Network meta-analysis for indirect treatment comparisons. Stat Med 2002; 21: 2313-2324. DOI:10.1002/sim.1201
- Ades AE, Madan J, Welton NJ. Indirect and mixed treatment comparisons in arthritis research. Rheumatology 2011; 50 (Suppl 4): iv5-9.DOI:10.1093/rheumatology/ker241
- Cooper NJ, Sutton AJ, Morris D et al. Addressing between-study heterogeneity and inconsistency in mixed treatment comparisons: application to stroke prevention treatments in individuals with nonrheumatic atrial fibrillation. Stat Med 2009; 28: 1861-1881.DOI:10.1002/sim.3594
- Salanti G, Higgins JP, Ades AE, Ioannidis JP. Evaluation of networks of randomized trials. Stat Methods Med Res 2008; 17: 279-301.DOI:10.1177/0962280207080643
- Jansen JP, Fleurence R, Devine B et al. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 1. Value Health. 2011; 14: 417-428.DOI:10.1016/j.jval.2011.04.002
- Hoaglin DC, Hawkins N, Jansen JP et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 2. Value Health 2011; 14: 429-437. DOI:10.1016/j.jval.2011.01.011
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009; 151: 264-269.
- Harenberg J, Marx S, Diener HC et al. Comparison of efficacy and safety of dabigatran, rivaroxaban and apixaban in patients with atrial fibrillation using network meta-analysis. Int Angiol 2012; 31: 330-339.
- Lip GY, Larsen TB, Skjøth F et al. Indirect comparisons of new oral anticoagulant drugs for efficacy and safety when used for stroke prevention in atrial fibrillation. J Am Coll Cardiol 2012; 60: 738-746.DOI:10.1016/j.jacc.2012.03.019
- Mantha S, Ansell J. An indirect comparison of dabigatran, rivaroxaban and apixaban for atrial fibrillation. Thromb Haemost 2012; 108: 476-484.DOI:10.1160/TH12-02-0093
- Wells GA, Coyle D, Cameron C et al. Safety, effectiveness, and cost-effectiveness of new oral anticoagulants compared with warfarin in preventing stroke and other cardiovascular events in patients with atrial fibrillation. http://www.cadth.ca/media/pdf/NOAC_Therapeutic_Review_final_report.pdf (assessed Dec 22, 2012)
- Harenberg J, Marx S, Wehling M. Head-to-head or indirect comparisons of the novel oral anticoagulants in atrial fibrillation: what’s next? Thromb Haemost 2012; 108: 407-409. DOI:10.1160/TH12-07-0463
- Schneeweiss S, Gagne JJ, Patrick AR et al. Comparative efficacy and safety of new oral anticoagulants in patients with atrial fibrillation. Circ Cardiovasc Qual Outcomes 2012; 5: 480-486.DOI:10.1161/CIRCOUTCOMES.112.965988
- Camm AJ, Kirchhof P, Lip GY et al. Guidelines for the management of atrial fibrillation: The task force for the management of atrial fibrillation of the European Society of Cardiology. Europace 2010; 12: 1360-1420.DOI:10.1093/europace/euq160
- You JJ, Singer DE, Howard PA et al. Antithrombotic therapy for atrial fibrillation: Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2012; 141: e531S-575S. DOI:10.1378/chest.11-2304
- Harenberg J, Lip GY. Differences between indirect comparison studies of the oral anticoagulants for stroke prevention in atrial fibrillation: where do we go next? QJM 2013; 106: 95-96. DOI:10.1093/qjmed/hcs224
- Testa L, Agnifili M, Latini RA et al. Adjusted indirect comparison of new oral anticoagulants for stroke prevention in atrial fibrillation. QJM 2012; 105: 949-957. DOI:10.1093/qjmed/hcs114
- Miller CS, Grandi SM, Shimony A et al. Meta-analysis ofefficacy and safety of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus warfarin in patients with atrial fibrillation. Am J Cardiol 2012; 110: 453-460. DOI:10.1016/j.amjcard.2012.03.049
- Dentali F, Riva N, Crowther M et al. Efficacy and safety of the novel oral anticoagulants in atrial fibrillation: a systematic review and meta-analysis of the literature. Circulation 2012; 126: 2381-2391.DOI:10.1161/CIRCULATIONAHA.112.115410
- Rasmussen LH, Larsen TB, Graungaard T et al. Primary and secondary prevention with new oral anticoagulant drugs for stroke prevention in atrial fibrillation: indirect comparison analysis. BMJ 2012; 345: e7097.DOI:10.1136/bmj.e7097
- Alonso-Coello P, Zhou Q, Guyatt G. Home-monitoring of oral anticoagulation vs. dabigatran. An indirect comparison. Thromb Haemost 2012; 108: 647-653. DOI:10.1160/TH12-01-0027
- Trkulja V, Kolundzic R. Rivaroxaban vs dabigatran for thromboprophylaxis after joint-replacement surgery: exploratory indirect comparison based on meta-analysis of pivotal clinical trials. Croat Med J 2010; 51: 113-123.DOI:10.3325/cmj.2010.51.113
- Lereun C, Wells P, Diamantopoulos A et al. An indirect comparison, via enoxaparin, of rivaroxaban with dabigatran in the prevention of venous thromboembolism after hip or knee replacement. J Med Econ 2011; 14: 238-244. DOI:10.3111/13696998.2011.564699
- Loke YK, Kwok CS. Dabigatran and rivaroxaban for prevention of venous thromboembolism–systematic review and adjusted indirect comparison. J Clin Pharm Ther 2011; 36: 111-124. DOI:10.1111/j.1365-2710.2010.01162.x
- Cohen A, Drost P, Marchant N et al. The Efficacy and Safety of Pharmacological Prophylaxis of Venous Thromboembolism Following Elective Knee or Hip Replacement: Systematic Review and Network Meta-Analysis. Clin Appl Thromb Hemost 2012; 18: 611-627.DOI:10.1177/1076029612437579
- Dahl OE, Quinlan DJ, Bergqvist D et al. A critical appraisal of bleeding events reported in venous thromboembolism prevention trials of patients undergoing hip and knee arthroplasty. J Thromb Haemost 2010; 8: 1966-1975. DOI:10.1111/j.1538-7836.2010.03965.x
- Maratea D, Fadda V, Trippoli S, Messori A. Prevention of venous thromboembolism after major orthopedic surgery: indirect comparison of three new oral anticoagulants. J Thromb Haemost 2011; 9: 1868-1870.DOI:10.1111/j.1538-7836.2011.04421.x
- Gómez-Outes A, Terleira-Fernández AI, Suárez-Gea ML, Vargas-Castrillón E. Dabigatran, rivaroxaban, or apixaban versus enoxaparin for thromboprophylaxis after total hip or knee replacement: systematic review, meta-analysis, and indirect treatment comparisons. BMJ 2012; 344: e3675. DOI:10.1136/bmj.e3675
- Harenberg J, Marx S, Dahl OE et al. Interpretation of endpoints in a network meta-analysis of new oral anticoagulants following total hip or total knee replacement surgery. Thromb Haemost 2012; 108: 903-912.DOI:10.1160/TH12-07-0482
- Hamid JS, Meaney C, Crowcroft NS, Granerod J, Beyene J; UK Etiology of Encephalitis Study Group. Cluster analysis for identifying sub-groups and selecting potential discriminatory variables in human encephalitis. BMC Infect Dis 2010; 10: 364-374. DOI:10.1186/1471-2334-10-364
- Song EK, Moser DK, Rayens MK, Lennie TA. Symptom clusters predict event-free survival in patients with heart failure. J Cardiovasc Nurs 2010; 25: 284-291.
- McLachlan GJ. Cluster analysis and related techniques in medical research. Stat Methods Med Res 1992; 1: 27-48.DOI:10.1177/096228029200100103
- Schulman S. Is the network meta-analysis (NETMA) bringing us closer to the truth? Insights from recent antithrombotic drug data. Thromb Haemost 2012; 108: 872-875. DOI:10.1160/TH12-10-0730
- Fox BD, Kahn SR, Langleben D et al. Efficacy and safety of novel oral anticoagulants for treatment of acute venous thromboembolism: direct and adjusted indirect meta-analysis of randomised controlled trials. BMJ 2012; 345: e7498. DOI:10.1136/bmj.e7498
- Freeman JV, Zhu RP, Owens DK et al. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Int Med 2011; 154: 1-11.
- Kansal AR, Sorensen SV, Gani R et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in UK patients with atrial fibrillation. Heart 2012; 98: 573-578.DOI:10.1136/heartjnl-2011-300646
- Lee S, Anglade MW, Pham D et al. Cost-effectiveness of rivaroxaban compared to warfarin for stroke prevention in atrial fibrillation. Am J Cardiol 2012; 110: 845-851. DOI:10.1016/j.amjcard.2012.05.011
- Deitelzweig S, Amin A, Jing Y et al. Medical cost reductions associated with the usage of novel oral anticoagulants vs warfarin among atrial fibrillation patients, based on the RE-LY, ROCKET-AF, and ARISTOTLE trials. J Med Econ 2012; 15: 776-785.DOI:10.3111/13696998.2012.680555
- Krejczy M, Harenberg J, Marx S et al. Comparison of cost-effectiveness of anticoagulation with dabigatran, rivaroxaban and apixaban in patients with non-valvular atrial fibrillation across countries. Blood 2012; 120 (Suppl): P1164.