Heart-Failure–Related Mortality Rate: CDC Reports comparison of 2000, 2012, 2014 – the decease is steadily reversed
Reporter: Aviva Lev-Ari, PhD, RN
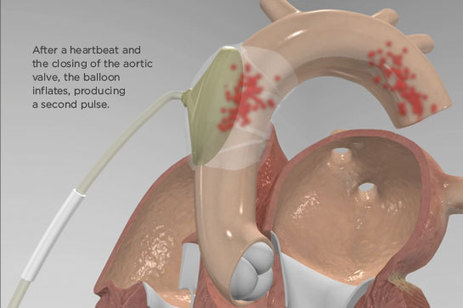
The report, which examined heart-failure trends between 2000 and 2014, showed that the age-adjusted rate for HF-related mortality was 105.4 per 100,000 population in 2000 and only 81.4 per 100,000 in 2012 (P<0.05). However, the rate then started a slow but steady climb, reaching 84.0 per 100,000 in 2014.
Not so surprising: men of all ages still had a higher death rate vs women in 2014, and black individuals had a higher rate than whites (91.5 vs 87.3 deaths per 100,000) and Hispanics (53.3 per 100,000).
CDC: Heart-Failure–Related Mortality Rate Climbs After Decade-Long Decrease
NCHS Data Brief
Number 231, December 2015
Recent Trends in Heart Failure-related Mortality: United States, 2000–2014
- Key findings
- The age-adjusted rates for heart failure-related deaths declined from 2000 through 2012 but increased from 2012 through 2014.
- The age-adjusted rate for heart failure-related deaths was higher for the non-Hispanic black population than for the non-Hispanic white and Hispanic populations.
- Heart failure-related death rates declined for all selected age and sex groups from 2000 through 2012 but increased from 2012 through 2014.
- The percentage of heart failure-related deaths occurring in a hospital decreased from 2000 through 2014.
- Non-cardiovascular disease was the underlying cause of death for more than one-third of heart failure-related deaths of adults aged 45 and over in 2014.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version ![]() (351 KB)
(351 KB)
Hanyu Ni, Ph.D.; and Jiaquan Xu, M.D.
Key findings
Data from the National Vital Statistics System, Mortality
- The age-adjusted rate for heart failure-related deaths decreased from 2000 through 2012 but increased from 2012 through 2014.
- The death rate for heart failure was higher for the
non-Hispanic black population than for the non-Hispanic white and Hispanic populations. - The death rate was higher for men than for women in all age groups. The gap in the death rate for adults aged 45–64 and 85 and over increased over time.
- The percentage of heart failure-related deaths that occurred in a hospital decreased from 2000 through 2014.
- The percentage of heart failure-related deaths for adults aged 45 and over with coronary heart disease as the underlying cause of death decreased 32%, from 34.9% in 2000 to 23.9% in 2014.
Heart failure is a major public health problem associated with significant hospital admission rates, mortality, and costly health care expenditures, despite advances in the treatment and management of heart failure and heart failure-related risk factors (1–4). Using data from the multiple cause of death files, this report describes the trends in heart failure-related mortality from 2000 through 2014 for the U.S. population, by age, sex, race and Hispanic origin, and place of death. Heart failure-related deaths were identified as those with heart failure reported anywhere on the death certificate, either as an underlying or contributing cause of death. Changes in the underlying causes of heart failure-related deaths are also described in this report.
Keywords: mortality, heart failure, trend, National Vital Statistics System
SOURCE
http://www.cdc.gov/nchs/data/databriefs/db231.htm