Voices of Americans during the Coronavirus Pandemic
9/8/2020
Food insecurity, COVID-19, and eating disorders
Reporter: Gail S. Thornton, M.A.

Every human in the United States can attest that COVID-19 has changed our way of life. In addition to shining a light on the prevalence of racial and ethnic disparities, socioeconomic status, and weight status on outcomes in COVID-19, the pandemic is driving food insecurity to an all-time high.
So, what is food insecurity?
Food insecurity is a disruption in food intake or eating patterns because of lack of money and other resources. The United States Department of Agriculture (USDA) divides food insecurity into two categories:
- Low food security: Quality, variety, or desired foods are being reduced by necessity. However, low food security is linked to little or no paring back in food intake.
- Very low food security: Multiple indicators of disrupted eating patterns — such as having no food in the fridge — and reduced food intake due to not having access to food.
How does food insecurity drive eating disorders?
One of the first studies to address the full spectrum of eating disorders in people living with food insecurity was published in the International Journal of Eating Disorders in 2017. In this study, participants with the highest level of food insecurity experienced:
- higher levels of binge eating (uncontrollable eating)
- a higher likelihood of having any type of eating disorder, such as anorexia or bulimia
- dietary restraint for any reason, for example, avoiding a food group, such as carbohydrates, or types of foods, such as desserts
- weight self-stigma, assessed through responses to a questionnaire that measured self-devaluation and fear of experiencing stigma (sample statement: “I would never have any problems with weight if I were stronger”)
- high levels of worry, also measured through responses to a questionnaire (sample statement: “My worries overwhelm me”).
A 2020 study in Eating Disorders points to high levels of dietary restraint in racially and ethnically diverse, low-income urban populations. The primary reasons people reported holding back on eating were:
- minimizing the effect of hunger on children and other family members
- stretching food by eating less to make it last longer
- prioritizing medical expenses over food.
Stretching the limits of food banks
Unfortunately, in the wake of COVID-19, unemployment rates are higher than those at the peak of the Great Depression. With this rise in unemployment, consistent access to nutritious food is elusive for many people. Food banks throughout the country are seeing higher rates of attendance than ever before.
As a woman who was raised serving as a worker in the food bank at my home church in Atlanta, I am encouraged by my parents’ consistent service as the leads of this food bank. They show up every week to make sure the hundreds of families that need food receive food, despite their fears of the COVID-19 pandemic, which has disproportionately impacted the Black community — especially those over the age of 65 like themselves. They show up because they care, but they realize that their efforts will likely fall short of solving food insecurity in their community. Only a coordinated multi-sector approach can solve this issue.
Impact on health and well-being
One public sector approach is the current HEROES bill, which has provisions to address food insecurity, as discussed in a recent blog post. But whether or not a fully-funded HEROES bill becomes law, we must address the role of food insecurity in eating disorders. The research is clear: food insecurity is linked to eating disorders that undermine health. Food insecurity has intensified in the middle of the most significant pandemic of our lifetime, COVID-19. Racial and ethnic minorities continue to face the brunt of the compounded issues of food insecurity, COVID-19, disordered eating, and excess weight. Indeed, food insecurity has increased since 1999 to affect about 20% of the US adult population. We must remain vigilant in efforts to address the intersectionality of these major issues, which have a tremendous impact on the health and well-being of our communities.
SOURCE
9/2/2020
For some, COVID-19 symptoms linger for months
Known as “long-haulers,” these patients call for more research, especially in the Boston area.
Reporter: Gail S. Thornton, M.A.
 Lauren Nichols, who tested positive for COVID-19 on March 17. Five months later, she is still suffering from a variety of symptoms, including nausea and fatigue.BARRY CHIN/GLOBE STAFF
Lauren Nichols, who tested positive for COVID-19 on March 17. Five months later, she is still suffering from a variety of symptoms, including nausea and fatigue.BARRY CHIN/GLOBE STAFFAt least four days a week, Kate Porter feels the heat rising within her, the inevitable return of the fevers that have plagued her for months. Merely walking from one room to another in her Beverly home can set her heart pattering at 140 beats per minute. Mounting a flight of stairs leaves her breathless.
Porter, 35, was healthy and active until mid-March, when she came down with COVID-19.
“So many people think it’s just life or death,” she said. But Porter, and others like her, are stuck in between — alive but unable to return to their previous lives.
No one knows how many people there are like Porter, but many thousands have gathered in social media groups, often conducting their own research.
 Kate Porter works on her laptop in her living room. Porter came down with COVID-19 on March 17, and she’s still suffering from fevers, shortness of breath, exercise intolerance, and terrible fatigue. JESSICA RINALDI/GLOBE STAFF
Kate Porter works on her laptop in her living room. Porter came down with COVID-19 on March 17, and she’s still suffering from fevers, shortness of breath, exercise intolerance, and terrible fatigue. JESSICA RINALDI/GLOBE STAFFThey call themselves “long-haulers”: COVID-19 patients who continue to endure symptoms weeks and months after their initial infection, despite no sign of the virus remaining in their bodies. Most were never hospitalized, so their lingering symptoms cannot be attributed to the effects of prolonged hospital stays.
The list of symptoms they report in patient-run surveys is long — longer than the government’s official list. Among the most common are fatigue, body aches, shortness of breath, and difficulty concentrating. But some people have chest pain and palpitations, or numbness and tremors in a limb, or intermittent fevers, dizziness, even hallucinations. It’s common to start to get better, and then suddenly get hit with new symptoms.
Lauren Nichols, a 32-year-old long-hauler who has been suffering with nausea, vertigo, painful breathing, and other symptoms for more than five months, puts it this way: “You trust your body. You think your body is going to bounce back because it always had. You trust the medical system, because it always had answers. Now you can’t trust either.”
Nichols and Porter both expressed surprise at how little interest the long-haulers’ plight has sparked among Boston’s esteemed medical centers. Nichols, who works for the federal government from her home in Back Bay, said she has enrolled in several studies based in California, but has found nothing local. Porter, a marketing director for a Boston company, has created a website listing resources and current research projects, many based in the United Kingdom.
The Globe contacted all of the region’s teaching hospitals and found no one specifically studying long-haulers, although a couple of researchers are planning to gather data on COVID-19 symptoms over time.
Spaulding Rehabilitation Hospital recently opened a clinic offering post-COVID-19 care, but so far it has only seen patients who had previously been hospitalized, according to a spokesman. Most long-haulers — 93 percent in one patient-led survey — were never sick enough to need hospital care.
Dr. Zeina Chemali, a behavioral neurologist and neuropsychiatrist who heads Massachusetts General Hospital’s McCance Center for Brain Health, said she has treated post-COVID-19 patients with persistent problems, most commonly fatigue and brain fog. Former go-getters who never napped suddenly find themselves unable to get off the couch, never mind navigate the complexities of their jobs. Chemali refers some of her patients for cognitive rehabilitation, where they do brain exercises. Some have taken stimulants to help them regain focus.
“People do get better,” Chemali said. “Some people, after a couple of months, reported feeling better and wanting to go back to work. Some people are making micro-achievements in their goals. I’m sure there is a huge population out there not coming to be seen, just staying at home.”
That’s one of the reasons why, despite multiple reports in the media, long-haulers can feel invisible to the medical system.
For those never admitted to the hospital, “nobody even knows we’re here,” said Jenny Berz, a Brookline psychologist and long-hauler. “For all of us who have this, we each have our own doctor. There’s no COVID doctor we can go to.”
Even the patients themselves may not recognize the source of their difficulties. “I know people who got COVID, recovered, and had a relapse. They didn’t realize it could still be COVID,” Berz said.
In July, the US Centers for Disease Control and Prevention reported that 35 percent of symptomatic COVID-19 patients said in a survey that they had not returned to their “usual state of health” two to three weeks after infection, including one-fifth of those ages 18 to 34 with no chronic illnesses.
Much less is known about what happens months after infection.
But there are many stories.
Nicole Ricker is starting to recover from the diarrhea, acid reflux, cough, body aches, and fevers that she had endured for weeks. But now, she’s confronting a puzzling new symptom: numbness on the right side of her body, particularly in her heel. Ricker, who is 34 and lives in Fall River, wants to return to work as an activities assistant at a nursing home, but isn’t sure she can be on her feet for eight hours.
In contrast, 75-year-old David Rose of Lexington had a mild case of COVID-19, just a fever for 10 days in March, plus fatigue. “I never felt in danger,” he said.
Months later, though, he’s still tired.
Although he has retired from his work as director of a nonprofit, he continues to write papers and give talks. But these days he feels less sharp. In one recent talk, Rose found himself dragging, barely able to keep going, instead of eagerly trying to convince people as he normally would.
Recently he had a pacemaker installed because his heart would periodically stop beating for several seconds. His cardiologist hasn’t ruled out the possibility that COVID-19, which is known to attack the heart, caused the problem.
“The thing is, nobody knows,” Rose said. “We all feel greater risk about everything.”
Some experts draw parallels between long-haulers and people suffering from myalgic encephalomyelitis/chronic fatigue syndrome, a chronic condition whose chief symptoms include extreme fatigue that gets worse after mental or physical activity, sleep difficulties, and problems with thinking and memory. ME/CFS has been known to occur after a viral infection, and many long-haulers describe similar symptoms.
But Dr. Zijian Chen, an endocrinologist who is medical director of the Mount Sinai Center for Post-COVID Care in New York City, said the convergence of so many different symptoms makes COVID-19 “very, very different from anything that we’ve seen before. … Every day we see a patient it seems like we’re looking at something new.”
The Mount Sinai clinic, which opened in May and has seen about 300 patients, was the nation’s first clinic devoted to long-haulers.
Some patients, Chen said, have evidence of physical damage to an organ such as the lungs or heart that explains their symptoms. For others, pulmonary function tests, echocardiograms, or CT scans find nothing amiss. “Those patients are puzzling, but they have very real symptoms,” he said.
One hypothesis holds that “a continually activated immune system” is producing the symptoms, but “there’s no good way to test that theory,” Chen said. Another theory posits that the virus attacked the autonomic nervous system, which controls involuntary functions like breathing and heart rate.
Dr. Richard Schwartzstein, chief of the Division of Pulmonary, Critical Care and Sleep Medicine at Beth Israel Deaconess Medical Center, said he’s seen about a dozen patients with prolonged COVID-19 symptoms, mostly fatigue. Some patients, he said, may be out of shape from prolonged inactivity while sick. And others may be drained by stress of the pandemic. “Their world has been thrown upside down,” he said. “For those people who have been sick, their ability to recover emotionally is not as readily done.”
At the Cambridge Health Alliance, providers at a clinic for COVID-19 patients found that a few complained of persistent symptoms eight to 10 weeks after getting infected. But as the virus has waned in the region, such patients have stopped coming in, said Neha Sandeep, a physician assistant at the clinic. She believes they recovered, but acknowledges some may have simply adjusted to a new normal.
Berz, the Brookline psychologist, has been active in patient groups, and said she hasn’t heard of anyone getting better.
“That’s the hardest part. I don’t know if this will ever change,” she said. “I don’t know if I’m ever going to be well.”
Felice J. Freyer can be reached at felice.freyer@globe.com. Follow her on Twitter @felicejfreyer
SOURCE
###
9/2/2020
Americans see hospitals as more trustworthy than FDA or CDC on COVID-19 vaccine information, poll finds

SOURCE
###
8/24/2020
How COVID-19 is shaking up medical education—for good
As the wave of closures swept across the U.S. due to the COVID-19 pandemic this spring, Jason Rosenstock, M.D. found himself among the educators scrambling to totally rethink how school would work.
For the interim associate dean for medical education at the Univeristy of Pittsburgh School of Medicine, that meant rethinking the delivery of medical education using pre-recorded classes while lecturers connected with students in active discussions through online platforms like Zoom, Rosenstock said.
“It was okay, but it really wasn’t as good as doing synchronous discussions,” he said.
With COVID-19 shows no signs of letting up soon, leaders at medical schools like Rosenstock are adapting their plans for education in the fall to meet the new demands of the pandemic. That means going digital in an unprecedented way—both in terms of classes and in terms of the type of clinical care students are learning about.
“It’s the new normal, and we’re going to need to tailor our medical education curriculum and other health professions’ education curricula to train our students for that new normal,” Stephen Spann, M.D., founding dean of the College of Medicine and vice president for medical affairs at the University of Houston, told Fierce Healthcare.
At UH, Spann and his team have welcomed the university’s first class of medical students in July, saying they tried to strike a balance between the need for in-person clinical education with social distancing and the growing use of telehealth.
The challenges facing UH are emblematic of the same hurdles that medical schools across the country are navigating.
Alison Whelan, M.D., chief medical education officer at the Association of American Medical Colleges, told Fierce Healthcare that the pandemic has forced medical colleges to get back to basics and really suss out the key competencies that students must learn in reshaping the education experience.
“It’s taken a lot of sort of creative jimmying,” she said.
Zoom versus in-room learning
Medical schools were not alone in moving to remote learning in the spring as the novel coronavirus first began to spread in the U.S. Schools at all levels grappled with the same challenge, and are eyeing it again as we move into the fall.
Medical students in their first two years are largely engaged in more classroom-based activities so going online was a logical transition, Rosentock said about Pitt’s move to online. But, he said, students miss something in being able to get together for a conversation so looking ahead to the fall, greater emphasis will be placed on active learning opportunities.
The bigger challenge, Rosenstock said, is effectively providing the hands-on clinical care for third- and fourth-year medical students, who engage more directly with patients. Pitt pulled its students out of clinical sites in the spring, a decision he said was “very hard.”
There are ways to conduct such training remotely—such as talk-through sessions or simulations—but it’s far less effective than conducting a physical exam in-person. Rosenstock said Pitt provided additional coaching and advising to students at all levels to help them through the shift to virtual education.
David Muller, M.D., dean of medical education at the Icahn School of Medicine at Mount Sinai, told Fierce Healthcare that Mount Sinai students have continued to conduct clinical education in-person for its third and fourth year students, as there are few viable alternatives.
And, he said, these students must realize that COVID-19 will be something they need to prepare for as physicians themselves.
“COVID is here to stay,” Muller said. “Even once we’re all miraculously vaccinated, this is going to become part of their clinical practice.”
The telehealth transition
As telehealth takes on an outsized role in navigating the pandemic, it’s also becoming a focal point in medical education. At the University of Houston, for example, nursing students that predated its first class of medical students were shadowing nurses on virtual visits as part of their clinical training, said Tray Cockerell, director of strategic relationships at Humana.
Humana and UH co-founded the medical school together, and it is under the university’s Humana Integrated Health Systems Science Institute.
Cockerell said that nursing students would join Humana nurses on in-home visits, so transitioning that experience to the virtual space was the logical step. He said there’s an interest from students in learning more about this kind of care.
“I think that’s something that is emerging and has been certainly an interest of all the clinical colleges to learn more about how we bring telehealth into education and leverage opportunities like this,” he said.
Spann said that interest extends to the new class of physician trainees as well. Pretty much all their educational journey has been influenced by the digital demands of COVID-19, starting with their admission interviews in the beginning of the year.
For the 170 applicants who made it to the interview stage, only 48 in-person interviews were conducted before the pandemic forced UH to take the interviews virtual.
And, as more practicing physicians expand their use of telehealth, it will become a critical piece of curricula moving forward, Spann said.
“This sounds strange to think there could be any benefits to this COVID pandemic,” he said. “One of the good outcomes, I think, is going to be expanding the use of telehealth in clinical care, and we’re going to need to teach students about that.”
Even before the pandemic began, the AAMC was looking at ways to assist medical schools in integrating telehealth into their curricula, Whelan said. The group assembled a group of clinicians and experts to outline a list of core competencies around telemedicine.
AAMC expects the guide to be released this fall, she said.
“That is where patient care is going to be happening,” she said.
Putting health disparities front and center
Cockerell said the pandemic is also putting a huge spotlight on another key focus area at the Humana Institute—the social determinants of health. One of the Institute’s goals is to integrate thinking about these social needs into the medical education it provides, and he said the pandemic is proving the value in that effort.
They also aim to show patients how to engage with companies like Humana and community partners “to think about how we work to help solve some of those issues,” he said. That includes, for example, providing training on how to use data to track referrals and patients’ use of services they need, including non-clinical services.
“Being able to close that loop is something we’re very interested in doing,” Cockerell said.
Spann said that education entails making students understand that non-clinical workers are a critical part of the care team in tackling these issues. For instance, if a child presents repeatedly to the emergency department with asthma issues, they can receive any number of medicines and treatments, but will continue to struggle if they’re returning to a home infested with mold and cockroaches.
Getting at that issue, he said, will require the assistance of a lawyer to hold a neglectful landlord accountable—a potential partner in medical care that most would not think of.
“It’s all about a team sport, and there are members of that team that we don’t typically think about as healthcare providers,” Spann said.
Muller said that the pandemic is also putting greater strain on the socioeconomic challenges the students themselves may be facing, and that must also be a greater consideration moving forward.
Mount Sinai, for example, accepts a number of students who are living in the U.S. under the Deferred Action for Childhood Arrivals (DACA) program. On top of trying to complete their medical education, many of these students are dealing with the pandemic having a disproportionate impact on their communities and any undocumented family members trying to seek care if they need while avoiding detection by Immigration and Customs Enforcement (ICE).
Muller said students like these may require greater resources and for their schools to better meet them whether they are.
“Medical schools need to acknowledge that and be cognizant of it,” he said.
Looking to the future
It’s likely that some of the changes brought on by the pandemic are here to stay in medical education. Industry experts largely agree that the telehealth boom is here to stay, which means the demand for training will stay in tandem.
Rosenstock said that the pandemic response has made a case at Pitt for continued use of remote assessment and learning, which is more convenient and effective for some students. Adjusting to digital learning was difficult, but the students did settle in, he said.
“We’re in a much better place now,” he said. “We’re used now to this hybrid of tele and in-person.”
He added that transitioning to providing education virtually has also required additional training for the educators, and planning for how to best integrate telehealth training into certain specialties.
Spann said that the pandemic has also proved the need to better educate students on public health and epidemiology so the clinical workforce has experience in those areas should another health crisis like COVID-19 emerge.
Muller said that going digital due to the pandemic has also emphasized that some of the more traditional approaches to education were on the way out, anyway, with or without the novel coronavirus.
Lecture attendance, for example, was already declining as students would instead listen to recordings on their own time, which was more convenient, he said. It’s also bringing back up longstanding questions about standardized testing—a method that has been criticized for decades as disadvantaging certain populations and for biases.
As students avoid testing centers for these exams amid social distancing, it proves that other ways to assess performance are just as workable, Muller said.
“The pandemic has revealed how really ridiculous all of that has always been,” he said.
SOURCE
###
7/26/2020
Laurie Lipton: Drawing from the Darkness
Reporter: Gail S. Thornton, M.A.
JULY 22, 2020
The American artist likes drawing more than anything else in the world and uses it to create dystopian scenes combining past and present to deal with the insanity going on around us.
Recently, her subject has become the disquieting and real presence of the pervasive network of computerized surveillance devices, which is used to observe our movements, our faces, our purchases, and our language – the multiplying sneaky, spying network of cameras, which permanently watches our streets and stores; the algorithms cleverly programmed into super-computers, silently listening for trigger words in a billion telephone conversations; the on-line trackers used to refine personalized and carefully pinpointed advertising and to exploit our digital addiction to purchasing processed pleasures – these seeping violations excused by functionary servants of the state with bland utilitarian apologies as the expediencies of the war on terror, the war on drugs, or the war on Covid-19; these infectious intrusions, justified by manipulating our fear of violence, of harm to our families, of sickness and death. “My work evolves,” Lipton says, “but has always been about the world I live in. Like Goya, I am reacting, in a symbolic way, to the insanity around me. What do I think should be done about it? Make more drawings.”
Lipton works with neurotic discipline, religious in its repetitive and meditative observance. Like a solitary medieval monk, she follows a strict regime of drawing in the isolation of her studio, which is in her home in suburban Los Angeles. “The ‘devotion’ to my work comes through joy,” she says, “I adore drawing. I like doing it more than anything else on earth, which is why I’m so good at it.”
But what species of joy is this? The scale of the drawings, and the fanatical dedication she takes in producing them, with millions of strokes of graphite to paper, are these the marks of obsession, a religious observation, like the joy of self-inflicted penitence for the sins of the world? Christian icons share the same quality of self-sacrifice. When asked about her religious thoughts, she replies dismissively, “What do I think about spirituality today? If anyone finds any, good for them.” And although conceived with the fidelity and self-mortifying dedication of an aesthetic stylite, her drawings offer no expiation for our collective guilt for allowing culture to become what it has become, and they lack the appeal that the iconographers made for forgiveness, for they make no connection to the numinous.
She has a fanatical following of collectors, including Terry Gilliam, whose brilliantly imaginative, bizarre and funny movies 12 Monkeys, and Brazil, share the same obsessive observation of a society infected with bureaucratic evil. Lipton met the great director and former Python in London through a mutual friend. “We also mutually adore each other’s work & have kept in touch,” she says. Unlike Gilliam’s films, in which we are released from the darkness by laughter and the truth of human affection, there’s little comedic redemption in Lipton’s work, which bleakly peers into the void as a grim affirmation of the tragic failure of modern communication. Her cacotopic drawings linger in the imagination like a dark patch on an x-ray, like the undead shadow on the staircase, like an eclipse.
SOURCE:
###
7/18/2020
A funeral and a birthday party: CDC traces Chicago coronavirus outbreak to two family gatherings
Reporter: Gail S. Thornton, M.A.
The case study, published Wednesday by the Centers for Disease Control and Prevention, is one of the most detailed looks at how covid-19 moves through communities and shows how a single person can set off a chain reaction of infections. The transmissions — traced to a funeral and birthday party held three days apart — took place before major social distancing policies were implemented and may have facilitated transmission of covid-19 to the broader Chicago community. (The CDC also previously investigated how those aboard the Diamond Princess cruise ship that had docked in Japan became infected.)
The CDC report begins the night before the funeral. The traveling friend — dubbed “Patient A1.1” as the first patient in the first transmission “generation” in the first cluster discovered — shared a takeout meal eaten from common serving dishes with two family members of the deceased at their home. The meal lasted about three hours.
At the funeral, Patient A1.1 hugged the friends who had been at the dinner and other family members to “express condolences.”
Two days later, one of the dinner hosts showed symptoms of the coronavirus. Two days after that, the other host got sick, too. A third family member who had hugged Patient A1.1 at the funeral also got sick.
Around the same time, Patient A1.1, who was then still experiencing mild respiratory symptoms, attended a birthday party with nine other people. They hugged and shared food at the three-hour party. Seven of the attendees soon became ill.
Within about a week of the onset of symptoms, the condition of the first dinner host deteriorated. The person was hospitalized, put on a ventilator and subsequently died.
Another family member visited the dinner host at the hospital and — without any personal protective equipment, according to the CDC — provided “personal care” and gave hugs. Three days later, that person developed a fever and cough, too.
Meanwhile, two of the birthday party attendees became critically ill and were put on ventilators. Both died. The five others experienced mild symptoms of cough and low-grade fever.
While one of the critically ill patients was hospitalized, a family member and a home-care professional who visited that person developed probable covid-19, the CDC said. The visiting family member, in turn, probably transmitted it to a household contact.
Three of the symptomatic birthday party attendees went to church six days after developing their first symptoms. Another church attendee who sat within one row for 90 minutes, talked to them and passed the offering plate with them also developed symptoms.
The CDC hypothesizes that these clusters may have facilitated transmission of covid-19 more broadly in Chicago and that they show why social distancing measures — and in particular, avoiding gatherings with multiple people — have been critical as the virus moved out of retirement communities, cruise ships and other more contained places. In New Orleans, local officials blamed another type of “super-spreading” event, Mardi Gras, for accelerating the transmission there. Outbreaks also have been traced to a French ski resort and an Italian soccer game.
“[T]hese findings highlight the importance of adhering to current social distancing recommendations, including guidance to avoid any gatherings with persons from multiple households and following state or local stay-at-home orders,” the CDC said.
SOURCE:
###
7/18/2020
COVID-19 and gender equality: Countering the regressive effects
Reporter: Gail S. Thornton, M.A.
July 15, 2020
Given trends we have observed over the past few months, in a gender-regressive scenario in which no action is taken to counter these effects, we estimate that global GDP growth could be $1 trillion lower in 2030 than it would be if women’s unemployment simply tracked that of men in each sector. (It is important to note that the impact could be more severe than the one we have modeled here if factors such as increased childcare burdens, attitudinal bias, a slower recovery, or reduced public and private spending on services such as education or childcare make women leave the labor market permanently.) Conversely, taking action now to advance gender equality could be valuable, adding $13 trillion to global GDP in 2030 compared with the gender-regressive scenario. A middle path—taking action only after the crisis has subsided rather than now—would reduce the potential opportunity by more than $5 trillion. The cost of that delay amounts to three-fourths of the total global GDP we could potentially lose to COVID-19 this year.
These estimates build on the McKinsey Global Institute’s (MGI’s) Power of Parity work since 2015. This research maps 15 gender-equality indicators across four categories: equality in work, essential services and enablers of economic opportunity, legal protection and political voice, and physical security and autonomy. (The latter three categories together indicate equality in society.) Using a Gender Parity Score, or GPS, calculated using these indicators, MGI has established a strong link between gender equality in society and gender equality in work—and shown that the latter is not achievable without the former.
Even before the coronavirus, our 15 indicators showed that tangible progress toward gender parity had been uneven and that large gender gaps remained across the world. Now, without intervention to address the disproportionate impact of COVID-19 on women, there’s a risk that progress could go into reverse. This would not just set back the cause of gender equality but also hold back the global economy. Conversely, taking steps to redress the balance now could improve social and economic outcomes for millions of women globally and help boost economic growth.
While most people’s lives and work have been negatively affected by the crisis, our analysis shows that, overall, women’s jobs and livelihoods are more vulnerable to the COVID-19 pandemic. The magnitude of the inequality is striking: Using data and trends from unemployment surveys in the United States and India, where gender-disaggregated data are available, we estimate that female job loss rates due to COVID-19 are about 1.8 times higher than male job loss rates globally, at 5.7 percent versus 3.1 percent respectively.
At a country level, the data suggest that in the United States, women made up 46 percent of workers before COVID-19. Factoring in industry-mix effects suggests that women would make up 43 percent of job losses. However, unemployment data indicate that women make up 54 percent of the overall job losses to date. Similarly, in India women made up 20 percent of the workforce before COVID-19; their share of job losses resulting from the industry mix alone is estimated at 17 percent, but unemployment surveys suggest that they actually account for 23 percent of overall job losses. Our analysis finds that the gendered nature of work across industries explains one-fourth of the difference between job-loss rates for men and women. The lack of systemic progress to resolve other societal barriers for women explains the rest.
The nature of work remains significantly gender specific: women and men tend to cluster in different occupations in both mature and emerging economies. This, in turn, shapes the gender implications of the pandemic: our analysis shows that female jobs are 19 percent more at risk than male ones simply because women are disproportionately represented in sectors negatively affected by the COVID-19 crisis. We estimate that 4.5 percent of women’s employment is at risk in the pandemic globally, compared with 3.8 percent of men’s employment, just given the industries that men and women participate in. As Exhibit 1 shows, the reason is that women have more than the average share of employment in three of the four most affected sectors, as measured by employment declines globally. Compared with the aggregate share of women in global employment—39 percent—women have 54 percent of global jobs in accommodations and food service, which are among the sectors worst affected by the crisis; 43 percent of jobs in retail and wholesale trade; and 46 percent in other services, including the arts, recreation, and public administration. Some sectors, such as manufacturing, in which men are a large majority of those employed have also been severely affected. Other sectors, such as education and healthcare, where women are the majority have suffered relatively little impact.
In examining labor-market effects and other factors for six countries—France, India, Indonesia, Kenya, Nigeria, and the United States—we find that these labor-market and industry-mix effects play out differently across countries. In Nigeria, for example, women are disproportionately represented in industries that are more affected by COVID-19 than men, while in France the opposite is true. In the United States, the gap between the sexes is less marked.
As noted, the industry-mix and labor-market specifics explain just one-quarter of the gender gap in vulnerability to job losses in the pandemic. What factors drive the other three-quarters? An important one is the burden of unpaid care, the demands of which have grown substantially during the pandemic. Women are on the front lines here; they do an average of 75 percent of the world’s total unpaid-care work, including childcare, caring for the elderly, cooking, and cleaning. In some regions, such as South Asia and the Middle East and North Africa (MENA), women’s share of unpaid-care work is as high as 80 to 90 percent. Our Power of Parity research found that the share of women in unpaid-care work has a high and negative correlation with female labor-force participation rates and a moderately negative correlation with women’s chances of participating in professional and technical jobs or of assuming leadership positions. Other research has found similar trends. As COVID-19 has disproportionately increased the time women spend on family responsibilities—by an estimated 30 percent in India, according to one survey, and by 1.5 to 2.0 hours in the United States—it is not surprising that women have dropped out of the workforce at a higher rate than explained by labor-market dynamics alone.
Another factor could be COVID-19’s disproportionate impact on female entrepreneurship, including women-owned microenterprises in developing countries (where such enterprises account for a high share of female labor-force participation). The crisis may have made some family resources scarce, such as financial capital to invest in businesses or digital devices that families must now share as children’s schooling has gone online. Our Power of Parity research showed that both digital and financial inclusion, notably access to credit from financial institutions and access to mobile banking, are closely related to the presence of women in the labor force.
Attitudes also shape how women experience the economic consequences of a crisis relative to men. These aren’t new beliefs but rather traditional societal mindsets about the role of women. They may be reflected in current decisions, at the organizational level or indeed within the family, about who gets to keep their jobs. For example, according to the global World Values Survey, more than half the respondents in many countries in South Asia and MENA agreed that men have more right to a job than women when jobs are scarce. About one in six respondents in developed countries said the same.
Looking ahead, other structural forces could further compound gender inequality. Our previous research on the impact of long-term automation trends on work concluded that, worldwide, 40 million to 160 million women—7 to 24 percent of those currently employed—may need to transition across occupations by 2030 as automation transforms the nature of work. (The range reflects different paces of automation.) This is roughly the same level of impact that automation would have on men. However, long-established barriers to acquiring new skills and making midcareer shifts, as well as other factors, make the transition harder for women.
The gender effects of the COVID-19 crisis highlight the uneven progress toward gender equality. Indeed, in the aggregate, progress toward equality in work and society has stayed relatively flat in the five years between 2014 and 2019. In 2014, the global GPS score was 0.60; today, it is 0.61 (on a scale of 0 to 1, where 1 signifies full parity between women and men). Gender equality in work continues to lag behind gender equality in society, with a GPS of 0.52 versus 0.67, respectively. The world has made progress on a few aspects of gender equality, such as maternal mortality, the share of women in professional and technical jobs, and political representation. However, the level of female participation in the labor force is about two-thirds that of men and has hardly budged in that period (Exhibit 2). Within this overall picture, countries and regions can vary significantly. India has seen a slight decrease in female labor-force participation in the past five years, for example, while Indonesia has registered a small increase.
For additional information, please click on the link below to read more of the article.
Anu Madgavkar, based in McKinsey’s Mumbai office, is a partner with the McKinsey Global Institute, where Mekala Krishnan, based in the Boston office, is a senior fellow. Olivia White and Deepa Mahajan are McKinsey partners in the San Francisco office, and Xavier Azcue is a consultant in the New Jersey office.
The authors wish to thank Rishi Arora, Ryan Luby, James Manyika, Mackenzie Nolan, Tracy Nowski, Jose Maria Quiros, and Jonathan Woetzel for their contributions to this article.
This article was edited by Peter Gumbel, the editorial director of the McKinsey Global Institute.
SOURCE:
###
7/9/2020
Rural Matters — Coronavirus and the Navajo Nation
SOURCE:
https://www.nejm.org/doi/full/10.1056/NEJMp2012114?query=TOC
###
7/1/2020
19/ Assaid today, 19 CA counties (~70% of state population) now on watchlist because of surges. Bars closing in ~15 counties (incl. LA, Orange). Imperial returning to SIP, LA beaches closing bit.ly/2AfESlD. Expect more use of “dimmer switch” in coming wks.
9101631
20/ The message from the governor was crystal clear: if we don’t turn things around, we may find ourselves back to widespread shelter-in-place soon. It wasn’t a-esque “Don’t make me come down there” moment bit.ly/3dL3qAL, but the resolve was unmistakable.
397780
21/ Trust is key, and Newsom & CA mayors have mostly earned it. Here’s a fun PSA on masks from past 4 governors, GOP & Dems (incl. Ahnold) bit.ly/3eWHaW1. This kind of thing will be harder to do in red states, since it’ll involve a lot of walking back past fictions.592875
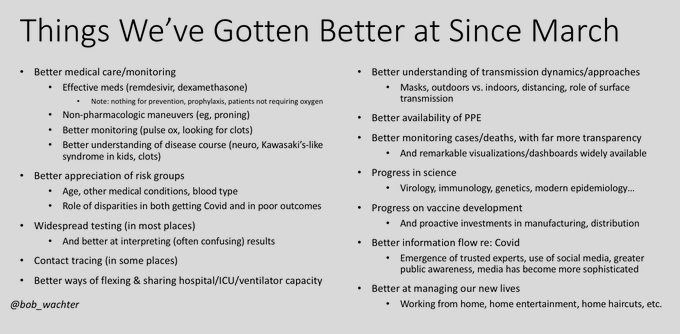
22/ As I said last week, we enter this crisis in better shape than we were in March (Fig again below). We’re catching the surges early through testing (not ICU admits), we have some effective treatments, & we’ve built hospital, ICU, & PPE capacity. We should feel good about that.
62211.1K
23/ I don’t know about you, but in March I was scared; now I’m mostly depressed – depressed that we’ve collectively allowed this to happen, depressed that the light at the end of the tunnel may prove to be an oncoming train. But if any state can turn this around, I’d bet on CA.445723.3K
Hello, here is your unroll:: 1/ Covid (
) Chronicles, Day 104 Let’s talk California. Until recently, our state managed to do so… threadreaderapp.com/thread/1277797 Share this if you think it’s interesting.